
Submitted:
09 November 2023
Posted:
10 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Adolescence is a stage of change and transition, which together with the COVID-19 situation, has been a huge source of vulnerability and facilitated the development of emotional disorders. This study aims to analyse internalising (anxiety and depression) and externalising (anger and aggression) symptoms in adolescence according to gender, as well as personal resources (self-esteem, social competence and integration, and awareness of problems) put in place as a mechanism of protection and coping after the situation of the pandemic. The study population encompassed 445 adolescents, of whom 230 were boys and 215 were girls, between the ages of 12 and 17. A self-reported Likert-type test was used. Findings indicate that girls show greater levels of internalising (anxiety and depression) and externalising problems (anger), finding no differences for the variable aggression between the two groups. Personal resources are closely linked to emotional symptomatology, providing a source of protection in both genders. The findings indicate a maladaptive pattern for adolescents that requires early intervention within the field of education.
Keywords:
internalising
; externalising
; personal resources
; gender
; adolescence.
1. Introduction
Adolescence is a transitional stage between childhood and adulthood, covering approximately between 10 and 19 years of age, and is based on a social construct where the formation of identity, formal thinking, and sexual maturity occurs. It is a growth phase exposed to various risk factors [1] and can be conceived of as a vulnerable stage, due to constant changes in biological, cognitive, social and family functioning. Adolescents are exposed to greater sources of stress and intense emotions, such as separation from parents, bullying, academic performance, interaction with peers, etc., among many others [2].
Another vulnerable situation has been the COVID-19 pandemic, as a historic event that has had an uneven impact on various spheres of personal and social life. The major unprecedented health measures included social distancing and quarantining, dictated in Spain through Royal Decree 463/2020 [3], which has had a great impact on people in terms of their physical, mental, social, behavioural, learning and developmental health. The duration of restrictions, uncertainty, lack of information, family economic stress, lack of space in the home and lack of essential supplies acted as key factors in the emergence of psychological reactions [4,5]. In the adolescent population, this situation has had a significant effect [6,7]. Even after the restrictions were lifted, risk factors such as illness or loss of loved ones, insomnia, irritability, difficulty concentrating, post-traumatic stress disorder, substance use, as well as the appearance of depressive symptoms or anxiety have persisted after the pandemic. This situation has increased the possibility that a section of the population presents psycho-pathological disorders both in the present and in the future, considering their level of vulnerability [8].
Adolescents have a high prevalence of mental disorders, around 20%, and the possibility that individuals’ experiences can be perpetuated in adulthood, greatly influencing and shaping their future social interactions and emotional well-being [6,7,9,10]. Emotional difficulties can have serious consequences on the lives of adolescents, including mental health problems and difficulties in establishing healthy relationships [11].
The transdiagnostic approach does not draw a specific line of separation between internalising and externalising symptoms, since it emphasises the mechanisms or cross-cutting factors that may be present in both disorders, such as negative thinking patterns, emotional regulation skills or difficulties in interpersonal relationships [12].
However, other researchers divide mental health problems according to whether they are internalising or externalising [13]. Internalising symptomatology refers to difficulties experienced internally and manifested at a cognitive or emotional level, such as anxiety and depression. While anxiety can be defined as our body’s response to certain stimuli triggered by a reaction that activates our nervous system [14,15,16], depression is characterised by sadness, loss of interest, fatigue, changes in appetite or sleep and lack of concentration [16]. Between 13 and 17% of the population presents anxiety and up to 67% could manifest depressive symptoms [10,17]. Externalising symptomatology, on the other hand, is characterised by disruptive and aggressive behaviour that is directed towards other people or the environment, such as anger and aggression [16]. While anger is defined as a normal and common emotion that can occur in varying degrees of intensity [18], aggressiveness refers to the ability and intent to cause harm, whether physical or psychological, to another person, and can manifest itself through kicking, scratching, screaming, pushing, swearing, etc. among other behaviours. Externalising symptomatology usually has a prevalence of around 6 to 10% of the population [10,19]. This type of behaviour has a great impact on the life of the child or adolescent and on their school development [20], and is crucial in the mental health of the child and adolescent population, as they can have a significant impact on the development and well-being of the person, due to the strong impact on their immediate social and family context, as well as on their socio-affective development [21].
Some research indicates that there are relevant differences between genders, so it could be a modulating variable in early adolescence [14]. Specifically, women would be up to four times more likely to develop emotional imbalances than men and experience a greater incidence of mental health disorders [22]. On the one hand, women would have higher scores in internalising symptomatology than men [14,22,23]. In contrast, some studies do not find any gender differences in anxiety and depression in adolescence [24,25] and others do not find these differences in early adolescence [9]. On the other hand, men tend to present higher levels of aggressiveness as a manifestation of emotional imbalances [24,25] while women tend to manifest contained rage or anger, without reaching behavioural manifestations [28]. In this regard, there could be gender differences in externalising symptomatology. Other research, in contrast, does not find these differences in anger or aggressiveness between genders [22].
Adolescents also have psychological resources that enable them to face these challenges effectively and adaptively [19,29], and these play a fundamental role in coping and psychological protection, life satisfaction and emotional well-being [29], such as self-esteem, social competence and awareness of problems, among others. Self-esteem is a person’s subjective and global perception of their own abilities, competences and personal traits, and this influences the way we see ourselves and how we relate to others [30]. In adolescence, self-esteem has been found to play an important role in the generation of emotional stability and lasting well-being [29]. Specifically, it appears that women have a lower level of self-esteem than men [31], both in the global and in the specific dimension for the physical, social or academic domain, which indicates that girls could have more negative visions of themselves than boys. In contrast, other studies carried out after the pandemic do not record this clear pattern, but it may be mediated by other variables, such as the self-perceived needs of boys and girls [32]. Social competence and integration is the ability to adapt to the norms and rules of a community and apply social skills in social interactions with others [33]. Adolescents with a greater repertoire of social skills have higher self-esteem, fewer negative feelings, better school performance, and fewer behavioural disorders [34]. In particular, women may have greater difficulty in communicating and expressing their emotions, which could have an impact on having more unstable social networks [35]. However, other studies do not find any gender differences in terms of social competence [36], so boys and girls would not display any differences in the social skills they bring into play in their social relationships. Finally, awareness of problems is related to the ability of people to realise the difficulties they have in their day to day lives, being aware that they must change and seeking help from others to be able to do so [37]. Women tend to be more aware of their difficulties [31], perceive and understand emotions better than boys, and this may be associated with a higher risk of developing emotional problems [38].
Thus, self-esteem and social competence and integration are considered positive protective factors, since they predict psychological well-being in this age group, mainly because they promote more rewarding interpersonal relationships and bolster the subject’s ability to deal with everyday difficulties [30,34,35].
In summary, internalising and externalising symptomatology may be frequent in adolescents after COVID-19 experiences, and may have a significant impact on their personal development and psychological well-being. On the other hand, personal resources, such as self-esteem, social competence and integration, and awareness of problems can act as a protector against these emotional difficulties. Some research indicates that there may be differences in the expression of these emotional difficulties according to gender [31,34,35,38] or not [22,24,25,36]
Therefore, the objective of the research is to analyse the socio-emotional difficulties (internalising and externalising) as well as the relationship with personal resources (self-esteem, social competence and integration, and awareness of problems) according to gender in adolescence after the situation created by COVID-19. Firstly, girls are expected to have a higher incidence of internalising and less externalising symptomatology compared to boys, and secondly, socioemotional difficulties and personal resources are expected to be related in both adolescent boys and girls.
2. Materials and Methods
2.1. Participants
The study sample was composed of 445 adolescents attending compulsory secondary education. There were 215 female students (48.3%), with ages ranging from 12 to 17 (M = 13.59; SD = 1.14). The male group consisted of 230 students (51.7%), whose ages ranged from 12 to 17 (M = 13.60; SD = 1.24). There were no significant differences between groups in terms of age [t(433) = 0.54 and p = .957)].
The distribution of participants between the groups was gender-balanced, as shown in Table 1. There were no significant differences in the number of subjects in each group or sex [λ2(445) = 0,733 and p = .655)]. The second year of compulsory secondary schooling was the largest group in the sample, representing 47.2% of the total participants.
2.2. Tools
The Evaluation of Children and Adolescents questionnaire (SENA) developed by Fernández-Pinto et al. [37] for secondary education students (12-18 years old) was used to record internalising symptomatology, externalising symptomatology and personal resources.
Internalising symptomatology was measured as Anxiety and Depression. The variable Anxiety (ANX) implies the presence of persistent ideas or feelings such as worries, fears, nervousness or overactivation. The items included “I’m told I worry too much” and “I’m fearful.” The variable Depression (DEP) refers to the presence of a dysphoric, anhedonian and anergic mood, with items such as “I am sad” and “I enjoy things less than before”.
Externalising symptomatology was evaluated as Aggression (AGR) and Anger (ANG). The variable Aggression (AGR) is focused on interpersonal aggression and evaluates the presence of behaviours that denote low empathy and which can manifest, in more serious situations, a certain cruelty towards others [37]. It was evaluated using items such as: “I insult others during arguments,” and “I take advantage of others if I can.” The variable Anger (ANG) is defined as an exaggerated and inappropriate experience or expression of anger, manifesting itself in aggressive-impulsive behaviours, feelings of anger and a perceived loss of control, and is evaluated with items such as: “when I am furious I throw or break things,” and “I fly off the handle easily.” [37]
The personal resources evaluated were Self-esteem (SEL), Social competence and integration (SOC) and Awareness of problems (AWE). The variable Self-esteem (SEL) refers to the person’s degree of satisfaction with themselves, their valuation and personal adjustment. High scores on this scale would be described as an assessment of a positive person with good personal adjustment. Some examples of items on this scale are: “I trust myself” and “I like how I am” [37]. The variable Social integration and competence (SOC) evaluates the ability to relate effectively to others, integrate into peer groups and thus get support and reinforcement. These variables imply a good level of personal and social adaptation that is beneficial to minimise possible emotional deficits. Some of the items on this scale are: “I get on well with people” and “I make new friends easily” [37]. Finally, the variable Awareness of problems (AWE) reflects the degree to which the person can perceive difficulties in their day-to-day life, is aware of what is happening and that they should ask for help. A high score on this scale signifies a good disposition to personal and emotional changes, so it is an indication of good prognosis. Some examples of items on this scale are: “There are things that go wrong for me in my life, and I would need help” and “I think I have to change, even if I find it very hard” [37].
The reliability of the SENA questionnaire [37] was calculated through internal consistency (A = .82 and .85, according to the scales) and temporal stability (r = .88 and .90) (see Table 2). In terms of validity, the BASC test [39] was used, which reaches high mean values (r =.70), as well as Morey’s Personality Assessment Inventory-Adolescent PAI-A [40] which corroborated a mean correlation (r = .60).
2.3. Procedure
2.3.1. Description
We selected participating schools through stratified sampling by catchment areas in the province of Malaga, according to the Junta de Andalucia [41], randomly selecting four schools that agreed to participate voluntarily, three from the city of Malaga and one from the wider province.
The exclusion criteria for students from the study sample were those with previous clinical disorders, disabilities, high abilities and/or socio-educational disadvantages.
The next step was to obtain the consent of the school management team to carry out the study. We then requested authorisation from parents and/or legal guardians and gained the consent of the participating students about the study.
The students completed the questionnaire during school hours in their respective classrooms, after the instructions were explained and the necessary material was provided. The assessment was conducted during a 45-minute session, assuring the students of the confidentiality of their responses. The evaluation was carried out individually.
The evaluation was carried out in November 2021, when social distancing and health measures were in still place for COVID-19, and it had been a year and eight months since the lock-down and social isolation enacted by Royal Decree 463/2020 of 14 March [3].
This paper is part of the research project “Psychoeducational Evaluation of Socio-Emotional Adjustment in Adolescents” and is governed by the code of ethics of Helsinki [16] and the University of Malaga, having been evaluated by the Malaga Experimentation Ethics Committee.
2.3.2. Statistical Design and Analysis
This a basic research project, which applies a descriptive, correlational and observational design. The study variables were internalising symptoms (anxiety and depression), externalising symptoms (aggression and anger), personal resources (self-esteem, social competence and integration, and awareness of problems), and gender (female and male).
The variables were recoded to avoid the difference between the number of items in the different scales and to be able to compare the results in the same range of scores. To do this, we added the scores of the different items (Itn), and divided it by the number of items on the scale (Nit), on the range between 1 and 5 points (see Equation 1).
Firstly, we applied the corresponding descriptive statistics to the study variables. Next, we calculated non-parametric Spearman correlations between the study variables.
Subsequently, we carried out comparisons of statistical means between the groups of male and female participants using Mann-Whitney’s U test for independent non-parametric samples.
If the differences between the means are significant, the effect size is calculated using the statistics programme G*power [42] following Cohen’s criterion [43], which classes as small, moderate or strong effect sizes d = |.10|, d = |.30|, d = |.50| or greater, respectively.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 29 [44].
3. Results
3.1. Descriptive Statistics
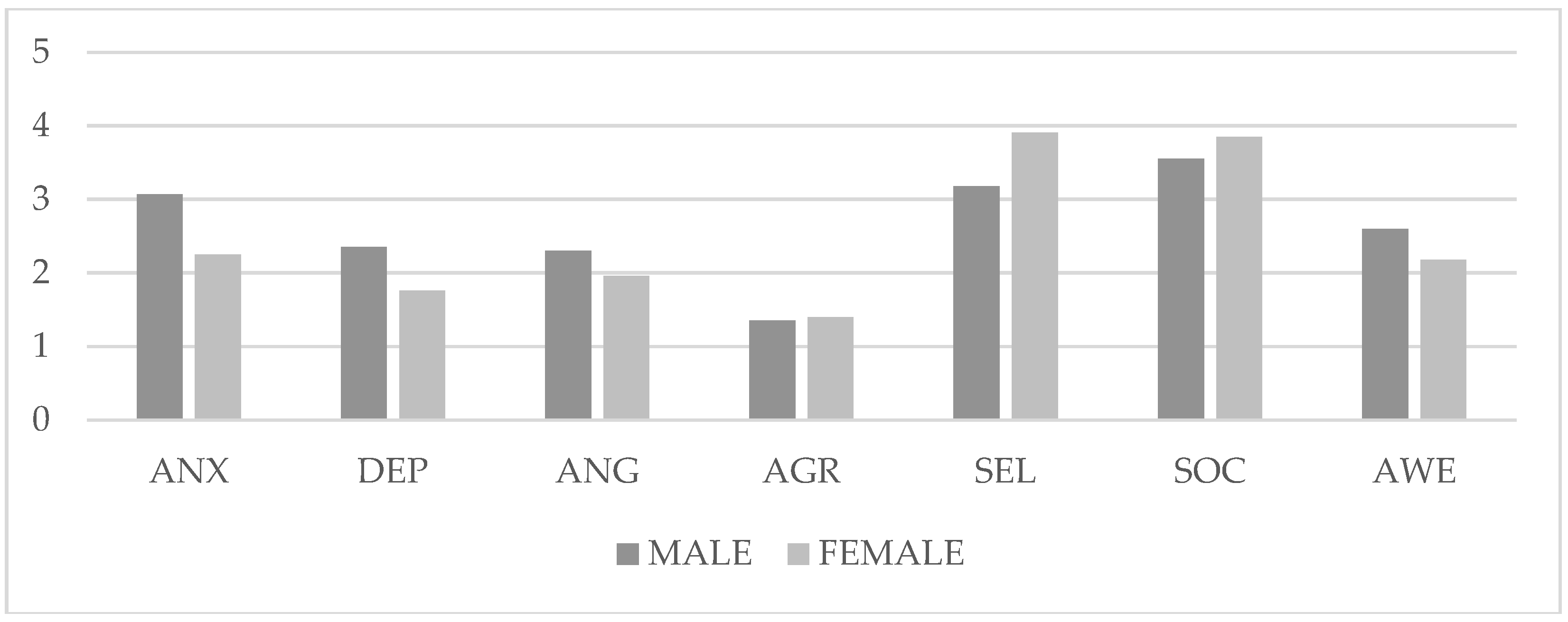
Table 3 presents the descriptive statistics for the internalising symptoms. The group of female participants obtained higher scores in ANX (M = 3.07; SD = 0.96) and DEP (M = 2.35; SD = 0.99) than the group of male participants [ANX (M = 2.25; SD = 0.82) and DEP (M = 1.76; SD = 0.75)]. Furthermore, in externalising symptoms (see Table 3), the group of female participants obtained higher scores for ANG (M = 2.30; SD = 0.92) than the group of male participants (M = 1.96; SD = 0.86). In contrast, the male participants obtained higher scores in AGR (M = 1.40; SD = 0.53) compared to the female participants (M = 1.35; SD = 0.45).
As for personal resources, the group of male participants obtained higher scores in SEL (M = 3.91; SD = 0.87) and SOC (M = 3.85; SD = 0.76) than the group of female participants [SEL (M = 3.18; SD = 1.07) and SOC (M = 3.55; SD = 0.79)]. In contrast, the female participants obtained higher scores in AWE (M = 2.60; SD = 0.89) compared to the male participants (M = 2.18; SD = 0.78).
Figure 1.
Average scores of the groups in the different variables. Note: ANX (anxiety), DEP (depression), ANG (anger), AGR (Aggression), SEL (Self-Esteem), SOC (Social Competence and Integration), AWE (Awareness of Problems).
Figure 1.
Average scores of the groups in the different variables. Note: ANX (anxiety), DEP (depression), ANG (anger), AGR (Aggression), SEL (Self-Esteem), SOC (Social Competence and Integration), AWE (Awareness of Problems).
3.2. Correlational Analysis
Firstly, the Female participants present statistically significant correlations in most variables (see Table 4). In particular, internalising variables such as ANX and DEP (rho = .815 and p < .01) have a high index, as do the externalising variables ANG and AGR (rho = .635 and p < .01), but more moderate in the latter case. The correlations between internalising and externalising variables are significant but more moderate, such as ANX and AGR (rho = .235 and p < .01), ANX and ANG (rho = .445 and p < .01), DEP and AGR (rho = .309 and p < .01), or DEP and ANG (rho = .471 and p < .01). On the other hand, personal resources show positive correlations between SOC and AWE (rho = .537 and p < .01) and negative between AWE and SEL [rho = -.676 and p < .01]), and AWE and SOC (rho = -.410 and p < .01). Personal resources and internalising symptomatology show negative correlations between SOC and ANX (rho = -.349 and p < .01) and SOC and DEP (rho = -.488 and p < .05), SEL and ANX (rho = -.687 and p < .01) or SEL and DEP (rho = -.798 and p < .01) and positive between AWE and ANX (rho = .750 and p < .01) or AWE and DEP (rho = .775 and p < .01). Finally, personal resources also have correlations with externalising variables, but they are not significant between SOC and AGR (rho = .020 and p > .05), or negative between SOC and ANG (rho = -.160 and p > .05), SEL and AGR (rho = -.257 and p < .01) and ANG and SEL (rho = -.388 and p < .01), or positive between AWE and AGR (rho = .318 p < .01) and AWE and ANG (rho = .440 and p < .01).
The group of male participants, on the other hand, presents statistically significant correlations in most variables. In particular, internalising variables ANX and DEP (rho = .724 and p < .01) have a high index, as do the externalising variables ANG and AGR (rho = .626 and p < .01), but more moderate in the latter case. The correlations between internalising and externalising variables are more moderate in ANX and DEP (rho = .366 and p < .01), DEP and ANG (rho = .427 and p < .01), ANX and ANG (rho = .456 and p < .01), or DEP and ANG (rho = .553 and p < .01). On the other hand, personal resources show statistically significant correlations between SEL and SOC (rho = .613 and p < .01) and negative more moderate correlations between AWE and SOC (rho = -.231 and p < .01), and AWE and SEL (rho = -.442 and p < .01). Internalising symptomatology and personal resources also show negative correlations between SOC and ANX (rho = -.247 and p < .01) and SOC and DEP (rho = -.422 and p < .05), SEL and ANX (rho = -.528 and p < .01) or SEL and DEP (rho = -.664 and p < .01) and positive between AWE and DEP (rho = .673 and p < .01) or AWE and ANX (rho = .598 and p < .01). Personal resources also present correlations with externalising variables, but they are not significant between SOC and AGR (rho = .078 and p > .05), or SOC and ANG (rho = -.093 and p > .05), and negative between SEL and AGR (rho = -.271 and p < .01) and ANG and SEL (rho = -.277 and p < .01), or positive between AWE and AGR (rho = .422 p < .01) and AWE and ANG (rho = .440 and p < .01).
3.3. Contrast of Means
We then went on to contrast the means between groups in the variables by statistically testing the analysis of variance (see Table 5).
The variable Anxiety presents statistically significant differences between the groups [U = 12582 and p < .001], so the scores in the group of female participants are higher than the male participants, with a medium effect size (d = 0.49). We also found significant differences between the groups in the variable Depression [U = 15680 and p < .001], with higher scores among the female than the male participants, showing a medium effect size (d = 0.36). The variable Anger presents statistically significant differences between groups [U = 18971 and p < .001], with higher scores among the female than the male participants, and a moderate effect size (d = 0.23). Regarding the variable Aggression, the differences between the groups [U = 24553 and p > 05] are not statistically significant. The variable Self-esteem presents significant differences [U = 14897 and p < .001], with higher scores among the male than the female participants and a moderate effect size (d = 0.39). The variable Social competence and integration also shows significant differences between groups [U = 19201 and p < .001], with higher scores among the male than the female participants and a moderate effect size (d = .0.22). Finally, the variable Awareness of problems shows significant differences [U = 17983 and p < .001] in favour of the group of female participants with a high effect size (d = 0.27).
4. Discussion
The objective of this study is to analyse the internalising and externalising symptomatology according to gender and the relationship with personal resources in adolescence after the COVID-19 pandemic.
The first hypothesis expected to find a higher incidence of internalising symptoms and lower externalising symptoms among the female participants. The results of this study indicate that the group of female participants has higher scores in anxiety, depression and anger than the male participants, while there are no statistically significant differences between the groups in terms of aggression, so the hypothesis cannot be partially maintained.
On the one hand, the female participants score higher in internalising emotional symptomatology (anxiety or depression) than the male participants, which coincides with several studies [15,22,23,45]. It seems that women tend to have higher scores in internalising variables than men, since they do not usually manifest emotional problems, but develop other cognitive patterns of internalisation of emotional difficulties. On the other hand, some studies [21,26,27,46] conclude that men are more likely to exhibit aggressive behaviours, and that women tend to experience fewer externalising behaviours than men. This study differs, since higher levels of anger have been found among the female participants who, although they might not engage in transgressive external behaviour, may engage in explosive verbal violence, as other studies find. For example, Oliva et al. [28] examined gender differences in behaviour disorders in adolescents and found that women showed higher levels of defiant behaviour and anger. Other studies have also not found differences in aggressive behaviour between genders [26,27]. This maladaptive pattern present in women is detrimental to their mental health and emotional well-being, since it implies not manifesting their emotions and ideations, which prevents them from being helped by others and without possibilities for improvement.
These differences found between genders can be attributed, for example, to biological, social and cultural influences [21]. Some authors [47] examine neurobiological differences between men and women, finding that higher testosterone levels in men may be associated with an increased propensity towards physical aggression. However, in our study, there are no differences in this variable, but rather they could indicate a gender gap, since women would tend to internalise the daily setbacks and not manifest them, as expected in the case of men [14,23,28]. Social and contextual factors, such as the influence of family, peers and culture, could contribute to gender differences in emotional difficulties. Adolescents might perceive as normative various permitted forms of expression of internal or external symptoms as more appropriate according to the role assigned in society. For example, experiences of differential socialisation, where certain behaviours are reinforced based on gender, can influence the way men and women express anger or aggression [48].
The second hypothesis states that internalising and externalising symptomatology and personal resources are related in male and female adolescents. The results of the study indicate that there is a high and significant relationship between socioemotional difficulties and personal resources, although in the group of male participants the indexes are higher than among the female participants, so the initial hypothesis could be maintained.
Regarding the relationship of personal resources with internalising symptomatology according to gender, [15] conducted a study that included the variables self-esteem and anxiety, and determined that there was a negative relationship between both variables, since, at higher levels of self-esteem, lower levels of anxiety as a state and trait were exhibited. In addition, if adolescents display a very intense level of anxiety, it would trigger excessive sensitivity, which would lead to a decrease in self-esteem. Likewise, these authors argue that the anxiety presented by students depends on their ideas about the task that is demanded of them, but also on their ability for understanding and self-control.
There is also a high relationship between self-esteem and depression in adolescents, since having low self-esteem can lead them to feel devalued and experience negative feelings of self-worth, affecting their emotional and mental state, causing symptoms of depression such as sadness, irritability or feelings of guilt [17].
Thus, internalising difficulties are related to personal resources since coping resources favour the balance between the demands of the environment and the internal needs of the adolescent according to gender. Hence, the group of male participants presents lower levels of emotional problems because they have higher levels of self-esteem and social competence than the group of female participants. Aguilar [35] describes a difference between adolescent boys and girls regarding their psychosocial adjustment and points out that adolescent girls have less self-esteem, perceive their own conflicts to a greater extent, and participate less socially. The fact that women communicate less with their support networks and are less socially active can be considered a risk factor since being able to talk safely about their feelings with their parents or people close to them can be a protection factor when developing a more positive self-perception and better coping styles [29,31,34].
Stegge and Terwogt [49] examine the role of emotional intelligence and self-esteem as mediators of externalising symptomatology in early adolescence. The results showed that self-esteem partially mediated the relationship between emotional intelligence and behavioural disorders, suggesting that positive self-esteem may help mitigate them.
Associations between externalising problems in adolescence, mental health and social competence and integration were also investigated. The results showed that social competence and integration act as a mediator in the relationship between externalising behaviours and mental health, suggesting that having adequate social skills can reduce socioemotional difficulties and improve emotional well-being [50]. They also examined its role as a mediator in the relationship between aggression and substance use in early adolescence. The results showed that social competence and integration mediate the relationship between aggression and substance use, indicating that the lack of this factor can contribute to the manifestation of aggression and the consumption of toxic substances [51].
Some studies indicate that there are gender differences from early adolescence onwards. [45,50] explain that the self-perception of boys interacts with their anxiety levels in a U shape; that is, during early adolescence they have higher levels of anxiety and lower levels of self-confidence; however, when they reach the stage of full adolescence the relationship becomes inverse, that is, self-confidence increases and anxiety decreases. However, in the case of girls it does not happen in the same way. Girls from early adolescence onwards begin to show high levels of anxiety and a decrease in self-confidence that will gradually increase until the critical stage of adolescence. Therefore, girls will have a poorer perception of themselves and greater awareness of their difficulties, accompanied by higher levels of anxiety, from the middle stage of childhood compared to boys. Thus, the evolution of gender differences throughout adolescence could be different for girls and boys, since some studies indicate that at the beginning of adolescence girls are twice as likely to present emotional disorders, which then triples between 13 and 15 years of age, decreasing from the age of 16 and remaining stable in adulthood [52].
The socio-emotional problems of adolescents have also been aggravated by the recent pandemic, and social patterns have even changed. According to Resa’s study [53], having been isolated at home has caused some intense emotions to overflow, and teens have had to connect with unpleasant emotions. All this causes a series of bodily sensations that can manifest in muscle tension or even anxiety. Many adolescents have shown social and emotional vulnerability after this health crisis, so it has directly affected the socioemotional adjustment of adolescents, causing them higher levels of anxiety and depression.
5. Conclusions
In conclusion, women and men have socioemotional difficulties, but different kinds, since women tend to express more anxiety, depression, and anger than men, with no differences in aggression, showing a more maladaptive pattern. These differences may be due to biological, social and cultural influences, as well as COVID 19 situations of vulnerability. In addition, personal resources such as self-esteem, social competence and integration, and awareness of problems, have a negative relationship with them. A higher level of these resources is associated with a lower incidence of emotional deficits, so they play a protective role for adolescents.
It is important to mention some limitations of this study. Firstly, the research was based on samples from the same province, which may not be generalisable to the rest of the population. In addition, a self-reporting approach was used, which may be subject to biases and limitations in the accuracy of the data collected.
Future research could be aimed at conducting longitudinal studies, to record the evolution of socio-emotional problems and personal resources throughout adolescence and young adulthood, and to see if these patterns are maintained or vary. It would also be interesting to triangulate information from adolescents with data collected by family and teachers, especially in internalised symptomatology.
The findings of this study have significant educational implications. The results highlight the importance of promoting the development of personal resources in adolescents of both genders, as part of the support and prevention programmes delivered in schools [10,12]. Social skills training programmes can be implemented to help teens improve their ability to communicate, resolve conflicts, and relate to others in a healthy way. The promotion of positive self-esteem, social integration and competence, as well as awareness of problems, can help reduce emotional difficulties and promote healthy adjustment in adolescence in both genders.
Author Contributions
Conceptualisation, ISAIAS MARTIN-RUIZ; methodology, ISAIAS MARTIN-RUIZ AND ANA HERRERA-GARCÍA.; formal analysis, ISAIAS MARTIN- RUIZ AND CRISTINA GARCÍA-PEREZ.; investigation, resources, and data curation, ANA HERRERA-GARCIAND CRISTINA GARCÍA-PEREZ.; writing—original draft preparation ISAIAS MARTIN-RUIZ.; writing—review and editing, ISAIAS MARTIN-RUIZ. All authors have read and added to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by UNIVERSIDAD DE MALAGA.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of UNIVERSIDAD DE MALAGA.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Conflicts of Interest
The authors declare no conflict of interest.
References
- García, A.D.; Hernández, L.J.; Espinosa, C.J.F.; Soler, M.J. Salud mental en la adolescencia montevideana: una mirada desde el bienestar psicológico. Arch Venez Farmacol Ter 2020, 39, 182–190. [Google Scholar] [CrossRef]
- Bailen, N.H.; Green, L.M.; Thompson, R.J. Understanding emotion in adolescents: A review of emotional frequency, intensity, instability, and clarity. Emot Rev 2019, 11, 63–73. [Google Scholar] [CrossRef]
- Gobierno de España. Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. «BOE» núm. 67, de 14 de marzo de 2020.
- Anglim, J.; Horwood, S.; Smillie, L.D.; Marrero, R.J.; Wood, J.K. Predicting psychological and subjective well-being from personality: A meta-analysis. Psychol Bull 2020, 146, 279–323. [Google Scholar] [CrossRef]
- Holzer, J.; Lüftenegger, M.; Käser, U.; Korlat, S.; Pelikan, E.; Schultze-Krumbholz, A.; Spiel, C.; Wachs, S.; Schober, B. Students’ basic needs and well-being during the COVID-19 pandemic: A two-country study of basic psychological need satisfaction, intrinsic learning motivation, positive emotion and the moderating role of self-regulated learning. Int J Psychol 2021, 56, 843–852. [Google Scholar] [CrossRef]
- Orgilés, M.; Tomczyk, S.; Amorós-Reche, V.; Espada, J.P.; Morales, A. Stressful Life Events in Children Aged 3 to 15 Years During the COVID-19 Pandemic: A Latent Class Analysis. Psicothema 2023, 35, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Tamarit, A.; de la Barrera, U.; Mónaco, E.; Schoeps, K.; Montoya-Castilla, I. Psychological impact of COVID-19 pandemic in Spanish adolescents: Risk and protective factors of emotional symptoms. Rev Psicol Clín Niños Adolesc 2020, 7, 73–80. [Google Scholar] [CrossRef]
- Galiano, R.M.; Prado, R.F.; Mustelier, B.RG. Salud mental en la infancia y adolescencia durante la pandemia de COVID-19. Rev Cubana Pediatr 2020, 92. [Google Scholar]
- Chen, F.; Zheng, D.; Liu, J.; Gong, Y.; Guan, Z.; Lou, D. Depression and anxiety among adolescents during COVID-19: A cross-sectional study. Brain Behav Immun 2020, 88, 36–38. [Google Scholar] [CrossRef]
- Martín, I.; Barba, M.J.; Lázaro, C.; Cuenca, J.; Samaniego, E. Prevención de los problemas socioemocionales en los centros educativos. Una propuesta de intervención psicoeducativa. Rev Orient Educ AOSMA 2022, 31, 36–66. [Google Scholar]
- Oram, R.; Ryan, J.; Rogers, M.; Heath, N. Emotion regulation and academic perceptions in adolescence. Emot Behav Diffic 2017, 22, 162–173. [Google Scholar] [CrossRef]
- Ehrenreich-May J, Kennedy SM, Sherman JA, Bennett SM, Barlow DH. Protocolo unificado para el tratamiento transdiagnóstico de los trastornos emocionales en adolescentes. Manual del terapeuta. Pirámide. 2022.
- Achenbach, T.M. International findings with the Achenbach System of Empirically Based Assessment (ASEBA): applications to clinical services, research, and training. Child Adolesc Psychiatry Ment Healt 2019, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alarcón, P.D.; Bárrig, J.P.S. Internalizing and externalizing behaviors in adolescents. Liberabit. Rev Peru Psicol 2015, 21, 253–259. [Google Scholar]
- Hernández, P.M.A.; Belmonte, G.L.; Martínez, A.M.M. Autoestima y ansiedad en los adolescentes. ReiDoCrea 2018, 7, 269–278. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud, OMS. Clasificación Internacional de Enfermedades, undécima revisión (CIE-11). 2019. https://icd.who.int/browse11.
- Lizano, O.J. Autoestima y depresión en adolescentes del distrito de San Vicente. Tesis doctoral. Universidad Católica de los Ángeles. 2023. https://hdl.handle.net/20.500.13032/31999. 1303.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Association. 2014.
- Lohmann, M.J.; Boothe, K.A.; Nenovich, N.M. Using Classroom Design to Reduce Challenging Behaviors in the Elementary Classroom. Classroom Manag Ser 2017, 17, 1–8. [Google Scholar]
- Salavera, C.; Usán, S.P. Influencia de los problemas internalizantes y externalizantes en la autoeficacia en estudiantes de Secundaria. Rev Investig Educ 2019, 37, 413–429. [Google Scholar] [CrossRef]
- Caqueo, U.A.; Mena, C.P.; Flores, J.; Narea, M.; Irarrázaval, M. Problemas de regulación emocional y salud mental en adolescentes del norte de Chile. Ter Psicol 2020, 38, 203–222. [Google Scholar] [CrossRef]
- Mesurado, B.; Vidal, E.M.; Mestre, A.L. Negative emotions and behaviour: The role of regulatory emotional self-efficacy. J Adolesc 2018, 64, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Rey, B.M.; Calonge, R.I.; Martínez, A.M.; Thomas, C.H. Sexo como variable moderadora de la sintomatología internalizante y externalizante en la infancia. Rev. esp. salud pública 2023, e202303022-e202303022.
- Carapeto, M.J.; Domingos, R.; Veiga, G. Attachment and Depressive Symptoms in Adolescence: The Mediatory Role of Emotion Awareness. Behav Sci 2022, 12, 405. [Google Scholar] [CrossRef] [PubMed]
- Peter, F.; Dalbert, C.; Kloeckner, N.; Radant, M. Personal belief in a just world, experience of teacher justice, and school distress in different class contexts. Eur J Psychol Educ 2013, 28, 1221–1235. [Google Scholar] [CrossRef]
- Baker, A.W.; Roker, R.; Bowling, A. Gender differences in the association between aggression and substance use among African American adolescents. J Child Adolesc Subst Abuse 2020, 29, 135–143. [Google Scholar] [CrossRef]
- Yancey, T.J.; Bennett, D.C.; Benner, A.D.; Li, F. Gender differences in behavioral and academic trajectories from kindergarten to eighth grade. Dev Psychol 2019, 55, 1004–1017. [Google Scholar]
- Oliva, A.; Antolín, L.; Pertegal, M.A.; Ríos, M.; Parra, Á.; Hernando, A.; Hernández, J.A. Gender differences in aggressive behavior among adolescents and young adults: A study from the Canary Islands. International Journal of Clinical and Health Psychology 2017, 17, 125–132. [Google Scholar]
- Núñez, A.; Álvarez, G.D.; Pérez, F.M.C. Ansiedad y autoestima en los perfiles de cibervictimización de los adolescentes. Comunicar 2021, 29, 47–59. [Google Scholar] [CrossRef]
- Farías, Á.D.R.; Urra, R.G. Funcionalidad familiar y autoestima en adolescentes durante la pandemia por COVID-19. Rev PSIDIAL Psicol Diálogo Saberes 2022, 1, 1–18. [Google Scholar] [CrossRef]
- Gibby, R.; Hartwell, B.K.; Wright, S. Dyslexia, literacy difficulties and the self-perceptions of children and young people: A systematic review. Curr Psychol 2021, 40, 5595–5612. [Google Scholar] [CrossRef]
- Korlat, S.; Reiter, J.; Kollmayer, M.; Holzer, J.; Pelikan, E.; Schober, B.; Spiel, C.; Lüftenegger, M. Basic psychological needs and agency and communion during the COVID-19 pandemic: Gender differentials and the role of well-being in adolescence and early adulthood. J Individ Differ 2023, 44, 18–35. [Google Scholar] [CrossRef]
- Losada, L. Reflexión y construcción del conocimiento en torno a las habilidades sociales y la competencia social. Rev Carib Investig Educ 2018, 2, 7–22. [Google Scholar] [CrossRef]
- Huber, L.; Plötner, M.; Schmitz, J. Social competence and psychopathology in early childhood: A systematic review. Eur Child Adolesc Psychiatry 2019, 28, 443–459. [Google Scholar] [CrossRef]
- Aguilar EFR. Variables psicológicas y educativas para la intervención en el ámbito escolar. En M.M. Molero, A. Martos, A.B. Barragán, M.M Simón, M. sisto, R.M. Pino, B.M. Tortosa, & J.J. Gázquez (Eds.) Variables psicológicas y educativas para la intervención en el ámbito escolar: nuevas realidades de análisis. Dykinson 2020, 9-102.
- Portela, P.I.; Alvariñas, V.M.; Pino, J. M. Socio-Emotional Skills in Adolescence. Influence of Personal and Extracurricular Variables. Int J Environ Res Public Health 2021, 18, 4811. [Google Scholar] [CrossRef]
- Fernández-Pinto I, Santamaría P, Sánchez-Sánchez F, Carrasco MA, Del Barrio V. Sistema de Evaluación de Niños y Adolescentes (SENA). TEA Ediciones. 2015.
- Schoeps, K.; Tamarit, A.; González, R.; Montoya, C.I. Competencias emocionales y autoestima en la adolescencia: Impacto sobre el ajuste psicológico. Rev Psicol Clín Niños Adolesc 2019, 6, 51–56. [Google Scholar] [CrossRef]
- Reynolds C, Kamphaus R. Sistema de evaluación de la conducta de niños y adolescentes (BASC). Pearson. 2004.
- Morey LC. Inventario de evaluación de la personalidad para adolescentes (PAI-A). TEA Ediciones. 2015.
- Consejería de Educación de la Junta de Andalucía. La educación en Andalucía. Datos y cifras. Gobierno Andaluz: Sevilla, ESP. 2021.
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical power analysis. Curr Dir Psychol Sci 1992, 1, 98–101. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows (Version 25), [Computer software]. IBM Corp. 2021.
- González, R.M.; Delgadillo, R.G.; Valles, M.A.M.; Caloca, L.H.; de la Mora, S. Internalizing and externalizing behaviors in high school adolescents in a northern border city of Mexico and their type of family. Aten primaria 2023, 55, 102743. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.J.; Kim, B.N.; Song, D.H. Gender differences in the relationships between internet gaming disorder and aggression among South Korean teenagers. J Psychiatr Res 2018, 98, 7–14. [Google Scholar]
- Carre, J.M.; Archer, J. Testosterone and human aggression: An evaluation of the challenge hypothesis. Neurosci Biobehav Rev 2020, 116, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Bettencourt, A.; Farrell, A.; Liu, W. Gender differences in aggression: The mediating role of social information processing. J Youth Adolesc 2020, 49, 858–874. [Google Scholar]
- Stegge, H.; Terwogt, M. M. Emotional intelligence, self-esteem, and externalizing problems in early adolescence. J Early Adolesc 2017, 37, 681–696. [Google Scholar]
- Barry, C.M.; Nelson, L.J.; Dulin, R. Associations between adolescent externalizing behaviors, mental health, and social competence: A longitudinal study. J Child Fam Stud 2019, 28, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Harachi, T.W. The mediating role of social integration in the relationship between aggression and substance use in early adolescence. J Youth Adolesc 2020, 49, 707–722. [Google Scholar] [CrossRef]
- Canals, J.; Voltas, N.; Hernández-Martínez, C.; Cosi, S.; Arija, V. Prevalence of DSM-5 anxiety disorders, comorbidity, and persistence of symptoms in Spanish early adolescents. Eur Child Adolesc Psychiatry 2019, 28, 131–143. [Google Scholar] [CrossRef]
- Resa, J. A. Z. Gestión Emocional durante la cuarentena: orientaciones desde la práctica de la Atención Plena. Rev Orient Educ AOSMA 2020, 28, 134-1. [Google Scholar]

Table 1.
Distribution of students by gender and school year.
| Academic Year | n | female | male | f |
|---|---|---|---|---|
| 1st year of Compulsory Secondary Education | 109 | 60 | 49 | 24.5 |
| 2nd year of Compulsory Secondary Education | 210 | 115 | 95 | 47.2 |
| 3rd year of Compulsory Secondary Education | 66 | 33 | 33 | 14.8 |
| 4th year of Compulsory Secondary Education | 60 | 22 | 38 | 13.5 |
| Total | 445 | 215 | 230 | 100 |
Note. n (number of students), f (percentage of sample).
Table 2.
Reliability of the Evaluation of Children and Adolescents Questionnaire, SENA.
| Variables | N | Pmín | Pmáx | αt | αe |
|---|---|---|---|---|---|
| ANX | 10 | 10 | 50 | .87 | .89 |
| DEP | 14 | 14 | 70 | .91 | .94 |
| ANG | 8 | 8 | 40 | .89 | .88 |
| AGR | 7 | 7 | 35 | .91 | .81 |
| SEL | 7 | 7 | 35 | .93 | .95 |
| SOC | 7 | 7 | 35 | .93 | .88 |
| AWE | 9 | 9 | 45 | .93 | .88 |
Note: N (Number of items), Pmin (Minimum Score), Pmax (Maximum Score), αt (Theoretical Reliability), αe (Study Reliability), ANX (Anxiety), DEP (Depression), ANG (Anger), AGR (Aggression), SEL (Self-esteem), SOC (Social competence and integration) and AWE (Awareness of problems).
Table 3.
Descriptive statistics.
| Variables | Female | Male | ||
|---|---|---|---|---|
| M (SD) | Range | M (SD) | Range | |
| ANX | 3.07 (0.96) | 1.00-5.00 | 2.25 (0.82) | 1.00-5.00 |
| DEP | 2.35 (0.99) | 1.00-4.57 | 1.76 (0.75) | 1.00-5.00 |
| ANG | 2.30 (0.92) | 1.00-4.88 | 1.96 (0.86) | 1.00-5.00 |
| AGR | 1.35 (0.45) | 1.00-3.57 | 1.40 (0.53) | 1.00-3.86 |
| SEL | 3.18 (1.07) | 1.00-5.00 | 3.91 (0.87) | 1.00-5.00 |
| SOC | 3.55 (0.79) | 1.44-5.00 | 3.85 (0.76) | 1.44-5.00 |
| AWE | 2.60 (0.89) | 1.00-4.29 | 2.18 (0.78) | 1.00-5.00 |
Note: M (mean), DT (standard deviation), ANX (anxiety), DEP (depression), ANG (Anger), AGR (Aggression), SEL (Self-Esteem), SOC (Social Competence and Integration), AWE (Awareness of problems).
Table 4.
Correlations between variables (Male participants in the upper right and Female participants in the lower left).
Table 4.
Correlations between variables (Male participants in the upper right and Female participants in the lower left).
| Variables | ANX | DEP | ANG | AGR | SEL | SOC | AWE |
|---|---|---|---|---|---|---|---|
| ANX | .724** | .456** | .366** | -.528** | -.247*** | .598** | |
| DEP | .815** | .553** | .427** | -.664** | -.422*** | .673** | |
| ANG | .445** | .471** | .626** | -.277** | -.093** | .440** | |
| AGR | .255** | .309** | .635** | -.271** | -.078** | .422** | |
| SEL | -.687** | -.798** | -.388** | -.257** | .613** | -.442** | |
| SOC | -.349** | -.488** | -.160** | .020** | .537** | -.231** | |
| AWE | .750** | .775** | .440** | .318** | -.676** | -.410** |
Note: * p < .05; ** p < .01; ANX (anxiety), DEP (depression), ANG (Anger), AGR (Aggression), SEL (Self-Esteem), SOC (Social Competence and Integration), AWE (Awareness of problems).
Table 5.
Differences in internalising, externalising and personal resources variables according to gender.
Table 5.
Differences in internalising, externalising and personal resources variables according to gender.
| Male | Female | U | p | d | |
|---|---|---|---|---|---|
| M (SD) | M (SD) | ||||
| ANX | 3.07 (0.96) | 2.25 (0.82) | 12582 | .001 | 0.49 |
| DEP | 2.35 (0.99) | 1.76 (0.75) | 15680 | .001 | 0.36 |
| ANG | 2.30 (0.92) | 1.96 (0.86) | 18971 | .001 | 0.23 |
| AGR | 1.35 (0.45) | 1.40 (0.53) | 24553 | .897 | - |
| SEL | 3.18 (1.07) | 3.91 (0.87) | 14897 | .001 | 0.39 |
| SOC | 3.55 (0.79) | 3.85 (0.76) | 19201 | .001 | 0.22 |
| AWE | 2.60 (0.89) | 2.18 (0.78) | 17983 | .001 | 0.27 |
Note: M (mean), SD (Standard Deviation), ANX (Anxiety), DEP (Depression), ANG (Anger), AGR (Aggression), SEL (Self-Esteem), SOC (Social Competence and Integration), AWE (Awareness of problems) F (Welch’s F), p Significance), d (Cohen’s d).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



