
Submitted:
13 November 2023
Posted:
13 November 2023
You are already at the latest version
Abstract
Osteopontin (OPN)-CD44 signaling plays an important role in promoting tumor progression and metastasis. In cancer, OPN and CD44 overexpression is a marker of aggressive disease and poor prognosis, and correlates with therapy resistance. In this study, we aimed to evaluate the association of single nucleotide polymorphisms (SNPs) in the OPN and CD44 genes with clinical outcomes in 307 non-small cell lung cancer (NSCLC) patients treated with radiotherapy or chemoradiotherapy. The potential impact of the variants on plasma OPN levels was also inves-tigated. Multivariate analysis showed that OPN rs11730582 CC carriers had a significantly in-creased risk of death (p = 0.029), while the CD44 rs187116 A allele correlated with reduced risk of locoregional recurrence (p = 0.016) in the curative treatment subset. The rs11730582/rs187116 combination was associated with an elevated risk of metastasis in these patients (p = 0.016). Fur-thermore, the OPN rs1126772 G variant alone (p = 0.018) and in combination with rs11730582 CC (p = 7x10-5) was associated with poor OS in the squamous cell carcinoma subgroup. The rs11730582 CC, rs187116 GG and rs1126772 G, as well as their respective combinations, were in-dependent risk factors for unfavorable treatment outcomes. The impact of rs11730582-rs1126772 haplotypes on OS was also observed. These data suggest that OPN and CD44 germline variants may predict treatment effects in NSCLC.
Keywords:
osteopontin
; OPN
; SPP1
; CD44
; lung cancer
; polymorphism
; cancer progression
; metastasis
; prognosis
; radiotherapy
; curative treatment
1. Introduction
Lung cancer continues to be the leading cause of cancer deaths worldwide [1]. Despite the introduction of targeted therapies and immunotherapy, radiotherapy and platinum-based chemoradiotherapy are still the mainstay of treatment in locally advanced and inoperable non-small cell lung cancer (NSCLC). However, common drug and radiation resistance impact the effectiveness of these treatments and contribute to progression and poor prognosis [2]. At the same time, conventional clinical factors used to guide therapeutic decisions are not able to predict precisely the patients’ outcome. Hence, it is necessary to search for factors that may help in the assessment of treatment effects and prognosis in NSCLC in order to identify risk groups and select an optimized therapeutic strategy.
Osteopontin (OPN), also known as secreted phosphoprotein 1 (SPP1), is a multifunctional glycoprotein and extracellular matrix (ECM) component, that mediates a variety of physiological and pathological processes. It is involved in tumorigenesis and metastasis, including cell proliferation, adhesion, invasion, migration, angiogenesis, apoptosis, autophagy and immune response [3]. In many solid tumors, including lung cancer, OPN overexpression in the tumor and increased circulating levels are markers of an aggressive phenotype and/or unfavorable prognosis [3,4]. For example, high OPN levels correlated with tumor growth and lymphatic metastasis in several lung cancer studies [5,6], while OPN knockdown inhibited invasion and metastasis of NSCLC cells [7]. OPN expression was also associated with reduced apoptotic activity in lung adenocarcinoma [8]. In NSCLC patients, a relationship was found between increased levels of OPN in the tumor and serum/plasma and advanced disease, poor treatment response and survival outcomes [9,10,11,12]. In our previous study, high pretreatment plasma OPN levels were significantly associated with unfavorable survival in inoperable NSCLC, especially in patients with squamous cell carcinoma [13]. Moreover, OPN expression may correlate with hypoxia and mediate resistance to radiotherapy and cytotoxic drugs [14]. High pretreatment OPN levels were related to poor oxygenation status of NSCLC patients treated with curative-intent radiotherapy [12]. Blocking the OPN gene in combination with irradiation led to decreased viability of breast cancer cells and induction of apoptosis, which highlights the role of OPN in the response to ionizing radiation [15]. In glioblastoma, OPN inhibition resulted in increased radiosensitivity and tumor size reduction in vivo [16]. It was found that autophagy-induced OPN suppression abrogated radioresistance of NSCLC cells [17]. OPN has also been shown to promote cisplatin resistance in small cell lung cancer cells, mainly by inhibiting apoptosis [18]. In NSCLC, OPN expression significantly correlated with distant metastasis and response to platinum-based chemotherapy [19].
OPN promotes tumor progression through binding to CD44 and integrin cell receptors. CD44 is a transmembrane cell surface glycoprotein and a marker for cancer stem cells in many solid tumors [20]. Data show that OPN-CD44 signaling is an important factor influencing cancer aggressiveness [3,21,22]. In addition to OPN, CD44 ligands also include hyaluronic acid, matrix metalloproteinases (MMPs) and growth factors. CD44 regulates proliferation, invasion, migration and stemness, and its overexpression is associated with cancer recurrence and metastasis [23]. In NSCLC, high CD44 levels promoted cell proliferation and colony formation [24]. Primary lung tumors with highly expressed CD44 demonstrated increased metastasis to the regional lymph nodes, and CD44 enhanced the ability of lung cancer cells to migrate and invade [25]. CD44 overexpression may also contribute to drug and radiation resistance, as well as poor prognosis in various malignancies [22,26]. For example, CD44 knockdown was associated with enhanced chemo- and radiosensitivity and reduced epithelial-mesenchymal transition in prostate cancer cells [27]. The CD44(+) gastric cancer cells exhibited increased resistance to chemotherapy- or radiation-induced cell death [28]. In glioma model in vivo, CD44 promoted cancer stem cell phenotype and radiation resistance, while CD44 expression correlated with hypoxia-induced gene signatures and poor survival in glioblastoma patients [21]. In lung cancer, CD44 downregulation was involved in sensitization to cisplatin and gefitinib, whereas lower CD44 expression in tumor was associated with better recurrence-free survival [29]. It was also demonstrated that CD44 was upregulated in radiation-survived NSCLC cells which could suggest its role as a marker of radiotherapy response in NSCLC [30].
Common germline genetic variants, such as single nucleotide polymorphisms (SNPs), especially in the promoter and regulatory regions, may modulate protein levels and activity, consequently affecting therapy results and disease progression in lung cancer. Most research on the prognostic role of OPN and CD44 in cancer focuses on protein expression levels. The literature data on the OPN and CD44 SNPs and clinical outcomes in solid tumors usually refer to Asian populations and the results are inconclusive [31]. Moreover, there are very few such studies in lung cancer. Therefore, in this report we aimed to evaluate the association between common SNPs in the OPN (also known as SPP1) and CD44 genes and three survival endpoints, as well as the potential relationship with circulating OPN levels before treatment, in patients with inoperable NSCLC receiving radiotherapy (RT) alone or in combination with chemotherapy (CTRT). To our knowledge, this is the first study of this type conducted in Caucasian NSCLC patients. Some of the analyzed variants (e.g., OPN rs1126772 or CD44 rs187116) have never been investigated in lung cancer before.
2. Materials and Methods
2.1. Study population
The study group consisted of 307 Caucasian patients with inoperable NSCLC. Patient characteristics are shown in Table 1. The mean age at diagnosis was 64.0 years (median, 64; range 33–84 years). Most of the cases were at advanced clinical stage III or IV (90%), had a Zubrod performance status (PS) of 0–1 (91%) and had a history of cigarette smoking (94%). Squamous cell carcinoma (SCC) was diagnosed in 181 (59%) patients, adenocarcinoma (AC) was diagnosed in 51 (17%) patients and 75 (24%) patients had NSCLC not otherwise specified (NOS). All patients received RT with a total dose ≥ 20 Gy, and 216 (70%) patients were given platinum-based CT. Out of all patients, 145 (47%) individuals were qualified to treatment with curative intent, i.e. thoracic RT at a total dose ≥ 60 Gy (range 60–72 Gy). Induction CT (i.e. 2–4 courses) was administered to 92% of these patients. The treatment details have been described in our previous study [13].
2.2. SNP identification
Five common SNPs were examined in this study, including OPN rs1126772, OPN rs11730582, OPN rs4754, CD44 rs187116 and CD44 rs13347. The following selection criteria were used: variants had a minor allele frequency (MAF) in the European Caucasian population ≥ 20% [32], were associated with cancer and located in regulatory or coding regions or in domains relevant to protein activity, and/or had potential or documented functional significance (Table S1) [33,34,35,36,37].
Genomic DNA was extracted from frozen peripheral blood collected during routine diagnostic tests prior to treatment. The rs1126772, rs4754 and rs187116 SNPs were identified with polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. The primers used for PCR are shown in Table S2. The reaction was performed in 25 µl of total volume containing 50 ng of genomic DNA, 0.2 mM of each dNTP, 12.5 pmol of each primer (Genomed, Warszawa, Poland), 1x PCR buffer, 1.5 mM MgCl2, 0.5 U of Perpetual Taq DNA polymerase (Eurx, Gdańsk, Poland). The initial denaturation at 95°C for 5 min was followed by 35 cycles of denaturation at 95°C for 30 s, annealing at 57°C (for rs1126772) or 55°C (rs4754 and rs187116) for 30 s and elongation at 72°C for 30 s, ending with 72°C for 5 min. Then, PCR products were digested overnight with 5U BfaI (for rs1126772), or BbsI (for rs4754) or MspI (for rs187116) restriction enzymes (New England Biolabs, Ipswich, MA, USA), and the fragments were separated on 3–4% ethidium bromide-stained agarose gels. The rs11730582 and rs13347 genotypes were determined using C_1840808_20 and C_7619022_10 TaqMan SNP Genotyping Assays (Applied Biosystems, Foster City, CA, USA), respectively, according to the manufacturer’s standard protocol. Genotyping was repeated in 30 randomly selected samples and 100% concordance was found.
2.3. Measurement of plasma OPN
Blood samples were collected before treatment and processed as previously described [13]. Plasma samples were stored at -80°C until analysis. Circulating OPN levels were measured by enzyme-linked immunosorbent assay (ELISA) using Human OPN Quantikine ELISA kit, DOST00 (R&D Systems Inc., Minneapolis, MN, USA) according to the manufacturer’s instructions.
2.4. Statistical analysis
Clinical endpoints of the study included overall survival (OS), locoregional recurrence-free survival (LRFS) and metastasis-free survival (MFS). OS was calculated from diagnosis until the date of death or last known date alive, while LRFS and MFS were calculated from the date of treatment initiation to the date of documented locoregional progression (for LRFS) or the date of distant relapse (for MFS), or last follow-up evaluation. Survival curves were determined with Kaplan-Meier method and compared with log-rank test. The SNPs were tested under dominant, recessive and additive genetic models, and the model with the most significant p value was selected for further analysis. The hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using univariate and multivariate Cox proportional hazards regression models. Multivariate models were adjusted for median age at diagnosis (< 64 versus ≥ 64 years), sex (male versus female), histology (SCC versus non-SCC), clinical stage (I-II versus III versus IV), Zubrod PS (0–1 versus 2), smoking (ever versus never), CT use (yes versus no) and RT dose (< 60 versus ≥ 60 Gy). A backward stepwise multiple regression was performed to identify independent risk factors. Haplotypes and their frequencies were estimated using PHASE v2.1.1 [38]. Haplotype blocks with D’ and r2 parameters used to estimate the degree of linkage disequilibrium (LD) between SNPs were determined in the Haploview v4.2 software [39,40] according to Garbiel et al. [41]. The Kruskall-Wallis H test and the Mann-Whitney U test were used to compare OPN levels between groups. The Spearman’s correlation and Pearson’s chi-square test were applied to evaluate the associations between variables. All tests were two-tailed and the p value was considered significant at 0.05. Statistical analyses were performed using Statistica 13.3 (TIBCO Software Inc., Palo Alto, CA, USA) and R v3.6.1 software (The R Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org, accessed on 4 December 2022).
3. Results
The median OS in the group was 18.3 months, the median LRFS was 18.6 months, and the median MFS was 28.7 months. The median follow-up time was 40.9 months. During observation time 218 (71%) deaths occurred, while 102 (33%) patients experienced locoregional recurrence, and 78 (25%) patients developed distant metastasis. The analysis showed that age ≥ 64 years (p = 0.011), male sex (p = 0.032), SCC histology (p = 0.013), clinical stage IV (p = 0.024), PS 2 (p = 0.016), smoking (p = 0.001), lack of CT (p = 1x10-6), and RT dose < 60 Gy (p < 1x10-6) correlated with poor OS, whereas SCC histology (p = 0.017), clinical stage IV (p = 0.052), PS 2 (p = 0.005), smoking (p = 0.041), lack of CT (p = 4x10-5), and RT dose < 60 Gy (p = 2x10-5), as well as clinical stage IV (p < 1x10-6) and RT dose < 60 Gy (p < 1x10-6), were associated with unfavorable LRFS and MFS, respectively. There was no statistically significant relationship between the genotypes and clinico-demographic parameters, except that rs13347 correlated with use of CT (p = 0.035). The MAFs in the group were consistent with those found in the European Caucasian population [32], and the genotype distribution was in accordance with Hardy-Weinberg law (Table S1).
3.1. OPN and CD44 SNPs and survival outcomes
There was no statistically significant effect of the studied SNPs on the outcome observed in the whole group. Only patients with CD44 rs187116 A variant had better LRFS than GG homozygotes (p = 0.083) in univariate models, and the OPN rs11730582 CC carriers showed elevated risk of distant relapse in the multivariate analysis (HR 1.63, p = 0.064), but the associations were not significant (Table 2).
However, when a more homogeneous subgroup of patients treated with curative RT doses (i.e. ≥ 60 Gy) was analyzed separately, two SNPs were found to be significantly associated with the studied clinical endpoints. Patients with at least one CD44 rs187116 A allele had significantly better LRFS than GG homozygotes (median LRFS 30.4 versus 22.0 months, p = 0.039). The rs187116 A variant carriers also demonstrated better MFS compared to GG homozygotes, but the difference was not statistically significant (median MFS not reached versus 24.8 months, p = 0.063). In multivariate analysis adjusted for clinical and demographic parameters, the OPN rs11730582 CC carriers had a significantly increased risk of death compared to T variant carriers (HR 1.74, p = 0.029) (Table 2). The rs11730582 C variant was also associated with an over two-fold increase in the risk of metastasis in multivariate model, but this was not statistically significant (p = 0.068). The CD44 rs187116 A allele had a significant protective effect with respect to risk of locoregional recurrence in univariate and multivariate Cox models (HR 0.55, p = 0.033 and HR 0.48, p = 0.016, respectively). The rs187116 A variant carriers also showed a reduced risk of metastasis as compared to GG homozygotes in univariate and multivariate models, however the association was not statistically significant (p = 0.054 and 0.076, respectively). The final model demonstrated that the OPN rs11730582 CC genotype (p = 0.042) together with SCC histological subtype and smoking were independent predictors of poor OS in the curative treatment subgroup (Table 3). In contrast, the CD44 rs187116 A allele was an independent protective factor against locoregional recurrence (p = 0.016), whereas the SCC histology and advanced clinical stage were independent indicators of unfavorable LRFS.
Furthermore, as hypoxia is a much greater clinical problem in SCC than in AC and the OPN levels had strong prognostic value among SCC patients in our previous study [13], we assessed the effect of the studied SNPs in this subgroup. The rs11730582 CC homozygotes with SCC had shorter OS than T variant carriers (median OS 10.0 versus 19.3 months, p = 0.027). The CC genotype was also significantly associated with increased risk of death in the univariate model (HR 1.60, p = 0.015), but not in the multivariate model (p = 0.093) (Table 2). Patients with the OPN rs1126772 G allele demonstrated unfavorable OS compared to AA homozygotes (median OS 12.5 versus 17.8 months, p = 0.034). The G variant carriers were at significantly increased risk of death in both univariate and multivariate analyses (HR 1.54, p = 0.020 and HR 1.59, p = 0.018, respectively). The rs11730582 CC and rs1126772 G were also non-significantly associated with an increased risk of recurrence in univariate models (p = 0.096 and 0.095, respectively). In the final model, only the rs1126772 G variant was an independent risk factor for poor OS, together with smoking and RT dose lower than 60 Gy (Table 3).
3.2. Cumulative analysis
In order to examine whether the co-occurrence of SNPs had a stronger effect on clinical outcomes than single variants, we constructed for each endpoint the genotype combinations for SNPs with p ≤ 0.100 in the multivariate analysis (Table 2). Thus, there were two combinations meeting this criterion. One of them was possible for MFS in the curative treatment subgroup and involved OPN rs11730582 and CD44 rs187116. The unfavorable genotypes were TC/CC and GG, respectively. MFS was significantly shorter in carriers of both adverse genotypes compared to TT + GA/AA carriers (median MFS 24.8 months versus median not reached, p = 0.036; Figure 1A), however no interaction was observed (likelihood ratio test p = 0.123). Patients carrying the unfavorable rs11730582 TC/CC + rs187116 GG combination had a 3.6-fold and more than four-fold higher risk of developing metastasis compared to TT + GA/AA carriers in univariate (HR 3.59, p = 0.028) and multivariate models (HR 4.19, p = 0.016; Table 2), respectively. In the final model, this SNP combination was the only independent risk factor for metastasis in patients treated with curative intent (HR 2.05, p = 0.043) (Table 3). The second combination was possible for OS in the SCC subgroup and involved OPN rs11730582 and rs1126772. The adverse genotypes were CC and AG/GG, respectively. Patients with two risk genotypes showed significantly reduced OS compared to non-carriers (median OS 9.1 versus 18.0 months, p = 0.0029; Figure 1B) and an interaction was found between these SNPs (rs11730582 versus rs11730582/rs1126772, p = 0.013 and rs1126772 versus rs11730582/rs1126772, p = 0.003; likelihood ratio test p = 0.0024). The presence of the rs11730582 CC + rs1126772 AG/GG combination conferred nearly a three-fold increase in risk of death in univariate (HR 2.82, p = 3.3x10-5) and multivariate analyses (HR 2.74, p = 7x10-5; Table 2). The final model showed that CC + AG/GG combination was strongly and independently associated with unfavorable OS in the SCC subgroup, together with smoking and RT dose below 60 Gy (Table 3).
3.3. OPN haplotypes and clinical outcome
The influence of haplotypes on survival outcomes was assessed only for SNPs exhibiting strong LD, i.e. for OPN rs11730582-rs1126772 (D’ = 1.0, 95% CI 0.96–1.0) and rs4754-rs1126772 (D’ = 0.96, 95% CI 0.86–0.99) (Figure S1). The rs11730582-rs1126772 haplotype frequencies in the group were: 52.5% for T-A, 28.8% for C-A, 18.2% for C-G and 0.5% for T-G. The rs4754-rs1126772 haplotype frequencies were: 75.1% for T-A, 18.7% for C-G, 6.2% for C-A and 0% for T-G. The analysis was conducted only for haplotypes more frequent than 1%. There was no statistically significant relationship between haplotypes and clinical outcome in the whole patient group. In the curative treatment subset, patients carrying at least one rs4754-rs1126772 C-A copy had better OS (median OS 37.5 versus 21.6 months, p = 0.045) and non-significantly longer LRFS (median LRFS 38.0 versus 20.3 months, p = 0.070) compared to non-carriers (Figure S2A,B), however this was not confirmed in the multivariate analysis (p = 0.123 and 0.312, respectively). The presence of at least one rs11730582-rs1126772 C-A copy was significantly associated with increased risk of death in the multivariate model (HR 1.81, p = 0.007) (Table 4). Moreover, the C-A haplotype carriers showed non-significantly reduced MFS (p = 0.077, Figure S2 C) as well as an elevated risk of metastasis in univariate (HR 1.81, p = 0.082) and multivariate models (HR 2.02, p = 0.053) when compared to non-carriers. In the final model, the rs11730582-rs1126772 C-A haplotype was an independent indicator of poor OS (HR 1.70, 95% CI 1.11–2.59, p = 0.014), together with age ≥ 64 years, SCC histology and smoking. In the SCC subgroup, carriers of the rs4754-rs1126772 C-A haplotype had longer LRFS compared to non-carriers (median LRFS 31.5 and 15.2 months, p = 0.011; Figure S3 A) and significantly lower risk of recurrence in univariate model (HR 0.35, 95% CI 0.13–0.97, p = 0.044) but not in multivariate model (p = 0.110). The rs11730582-rs1126772 T-A haplotype was associated with better OS (p = 0.027; Figure S3 B) and significantly lower risk of death in univariate model (HR 0.62, p = 0.014) but not in multivariate analysis (p = 0.098) (Table 4). The SCC patients with rs11730582-rs1126772 C-G demonstrated shorter OS than non-carriers (median OS 12.1 versus 18.0 months, p = 0.033; Figure S3 C). The C-G haplotype was also associated with significantly increased risk of death in both the univariate (HR 1.55, p = 0.019) and multivariate models (HR 1.61, p = 0.016; Table 4). The final model showed that the C-G haplotype was an independent indicator of unfavorable OS (HR 1.60, 95% 1.10–2.24, p = 0.018) in the SCC subgroup, together with smoking and RT dose < 60 Gy.
3.4. OPN levels and SNPs
The mean ± standard deviation (SD) OPN levels were 119.5 ± 66.1 ng/ml (median 104.0, range 6.5–674.3) in the entire group, 106.1 ± 68.3 ng/ml (median 90.2, range 6.5–674.3) in the curative treatment subset and 124.0 ± 72.0 (median 106.9, range 6.5–674.3) in the SCC subset. The prognostic value of plasma OPN concentration in relation to clinical parameters in this NSCLC cohort has been investigated in our previous report [13]. In the current study, there was no statistically significant association between OPN genotypes or haplotypes, as well as tested SNP combinations, and circulating OPN levels before treatment neither in all patients nor in both patient subsets examined (Table S3).
4. Discussion
In this report, using multivariate models, we demonstrated a statistically significant effect of the OPN rs11730582 and CD44 rs187116 SNPs, as well as OPN rs11730582-rs1126772 haplotype on survival outcomes in inoperable NSCLC patients treated with curative intent. Our observation that the rs11730582 CC genotype was independently associated with decreased OS confirmed the results of two previous lung cancer studies in the Chinese population, in which Hao et al. [42] showed a correlation of the C variant with a worse response to platinum-based CT and poor prognosis in patients with inoperable stage IIIB-IV NSCLC, while Chen et al. [43] reported shorter survival and an increased incidence of bone metastases in CC homozygotes. In the only published study involving Caucasian patients, the authors found no association with prognosis, local recurrence and metastasis in stage I-III NSCLC [9]. Similar to our data, CC homozygotes had significantly lower survival rates and higher susceptibility to gastric cancer [35,44], as well as increased invasiveness and risk of thyroid cancer [45]. However, in the case of other solid tumors, such as e.g. glioma or oral, nasopharyngeal, hepatocellular and breast cancers, variant C was protective in terms of cancer risk or prognosis [36,46,47,48,49]. The results of a meta-analysis based on 11 studies in the Chinese population, including the NSCLC study, suggested in turn that rs11730582 had no effect on cancer risk [50].
Consistent with the above-mentioned data, we also identified the C-A haplotype of the rs11730582 and rs1126772 as an independent indicator of poor OS in the curative treatment subset. Moreover, in our dataset, the OPN rs1126772 GG genotype and the rs11730582-rs1126772 C-G haplotype were independently associated with unfavorable OS in patients with SCC. In addition, we observed a strong independent effect of the rs11730582 CC and rs1126772 G combination on prognosis in this subgroup. The rs1126772 A>G SNP in the 3’ untranslated region (3’UTR) may deregulate the OPN gene expression and protein production. Although, to our knowledge, it has not been functionally tested, it was predicted to be within the miR-23a, miR-23b and miR-371-5p binding sites [51] what might suggest its potential phenotypic effect. This SNP has been very rarely studied in cancer disease, with the only finding that the G variant was associated with an increased risk of gastric cancer [52]. In turn, the rs11730582 -443T>C functional polymorphism located within the gene promoter is one of the most frequently investigated OPN gene variants. It was found to cause a differential binding of unknown nuclear factor, which may be the MYT1 transcription factor [33]. The study by Schultz et al. in melanoma cells showed enhanced transcription for the -443C variant associated with allele-specific binding of c-Myb to the promoter region [34]. In gastric cancer, the C variant resulted in significantly higher promoter activity [35]. Elevated OPN protein levels were also observed in melanoma cell lines homozygous for C allele, as well as in tumor tissue from thyroid cancer patients with CC genotype [34,45]. However, in a single study, Dong et al. demonstrated the opposite relationship using a hepatocellular carcinoma model, namely the T allele caused higher transcriptional activity and protein expression leading to significant increase of tumor growth and metastasis [36]. These data suggest that rs11730582 T>C promoter SNP may be one of the factors modulating the OPN gene and protein expression levels. OPN overexpression is known to correlate with the aggressiveness and poor outcome in lung cancer [5,9,10,13,53]. Functional studies mostly indicate that variant C may confer a higher level of OPN, which is in line with the results of our study and other reports regarding lung, gastric and thyroid cancers. However, it is likely that the effect direction of this SNP may be context-dependent. Based on the existing data, it can therefore be speculated that both rs11730582 and rs1126772 contribute to unfavorable prognosis in NSCLC as OPN upregulation promotes tumor progression and metastasis, as well as plays a role in resistance to anticancer drugs, including platinum agents, and ionizing radiation [14].
Another interesting finding in our study was the protective effect of the CD44 rs187116 A variant with respect to the risk of locoregional recurrence after curative treatment. Although the functional significance of this SNP is unknown, the rs187116 G>A substitution is located in intron 1 and this may affect the transcriptional activity of the gene and splicing regulation. In lung cancer, data on the role of various CD44 SNPs are very limited, while the rs187116 has not been studied at all. Nevertheless, an effect of this SNP consistent with our observations has been previously reported for gastric cancer. For example, both Winder et al. [54] as well as Bitaraf et al. [55] showed that the unfavorable G allele was associated with poor OS and higher risk of tumor recurrence in these patients. In a Japanese study, the G variant carriers had shorter disease-free survival compared to AA homozygotes [56]. Increased CD44 expression has also been demonstrated in gastric tissue in patients with G variant [57]. Moreover, the G allele was found to correlate with a higher susceptibility to this type of cancer [55]. However, the opposite relationship has been reported for the risk of breast and colorectal cancer [58,59], whereas no association with prognosis and recurrence was found in a single study on colon carcinoma [60]. Interestingly, in our NSCLC group treated with curative intent, a joint effect of OPN rs11730582 and CD44 rs187116 on the risk of developing metastases was also observed, while each of them individually showed no significant influence on MFS, what indicates the need to take multiple SNPs into account for risk stratification. This finding also highlights the possible usefulness of these variants in predicting lung cancer dissemination after radical therapy, especially since the OPN-CD44 axis is known to play a role in progression of several solid tumors [21,22]. Both our results in NSCLC and those of other authors show that the OPN and CD44 polymorphisms may be important modulators of the disease course and therapeutic response.
Finally, we found no association between the rs1126772, rs11730582 and rs4754 SNPs, as well as their haplotypes, and pretreatment circulating OPN levels in our NSCLC cohort. Similar results were previously obtained by several other authors in lung cancer and melanoma patients [9,10,61]. However, rs11730582 in the promoter region was shown to be linked to serum/plasma OPN levels in nasopharyngeal and breast cancers [48,49]. These inconsistencies may reflect the complexity of the mechanisms influencing circulating OPN levels, thus further research is required to elucidate the role of particular SNPs in OPN regulation.
In conclusion, this study identified for the first time three germline variants in the OPN and CD44 genes that individually, or jointly, influenced clinical outcome and prognosis in inoperable NSCLC patients treated with curative RT doses and in patients with SCC. We demonstrated that rs187116, rs11730582 and rs1126772 were predictors of recurrence, metastasis and poor survival independently of strong clinical and lifestyle factors. These findings may be of particular importance since SNPs can be easily detected in DNA from readily available peripheral blood samples prior to treatment. Our study, however, is subject to certain limitations, the largest of which include relatively small sample size and number of examined SNPs, as well as so far poorly understood molecular mechanisms underlying the associations found. Therefore, our initial results should be verified in larger populations of cancer patients. If these observations were confirmed, certain OPN and CD44 SNPs could become valuable additional information in predicting response to RT and CTRT in NSCLC patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, D.B., B.M. and R.S.; Methodology, A.G.-K., D.B., S.G. and B.M.; Formal analysis, D.B. and S.G.; Investigation, S.G., R.D. and B.M.; Validation, A.G.-K., B.M. and D.B.; Resources, D.B., B.M., M.G. and R.S.; Data curation, D.B., M.G., B.M. and R.S.; Writing—original draft preparation, D.B., A.G.-K. and S.G.; Writing—review and editing, D.B., R.S. and A.G.-K.; Visualization, D.B. and S.G.; Supervision and project administration, D.B.; Funding acquisition, D.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Science Centre (NCN), Poland, grant number 2012/05/B/NZ5/01905 to D.B. S.G. was supported in part by the NCN grant number 2020/37/B/ST6/01959.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Maria Skłodowska-Curie National Research Institute of Oncology, Gliwice Branch, Poland (protocol code KB/493-43/07, 10 May 2007, and KB/493-9/08, 17 March 2008).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
The authors thank Iwona Matuszczyk and Zofia Kołosza for their technical help and assistance in epidemiological data acquisition. The contribution of Małgorzata Marszałek-Zeńczak and Aleksander Sochanik is also appreciated. Some of the calculations were carried out using the Ziemowit computer cluster funded by the Silesian BIO-FARMA project number POIG.02.01.00-00-166/08 in the Computational Biology and Bioinformatics Laboratory of the Biotechnology Centre in the Silesian University of Technology.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Willers, H.; Azzoli, C.G.; Santivasi, W.L.; Xia, F. Basic mechanisms of therapeutic resistance to radiation and chemotherapy in lung cancer. Cancer J. 2013, 19, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Moorman, H.R.; Poschel, D.; Klement, J.D.; Lu, C.; Redd, P.S.; Liu, K. Osteopontin: A Key Regulator of Tumor Progression and Immunomodulation. Cancers (Basel) 2020, 12, 3379. [Google Scholar] [CrossRef] [PubMed]
- Weber, G.F.; Lett, G.S.; Haubein, N.C. Osteopontin is a marker for cancer aggressiveness and patient survival. Br. J. Cancer 2010, 103, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Lin, D.; Yuan, J.; Xiao, T.; Zhang, H.; Sun, W.; Han, N.; Ma, Y.; Di, X.; Gao, M.; Ma, J.; Zhang, J.; Cheng, S.; Gao, Y. Overexpression of osteopontin is associated with more aggressive phenotypes in human non-small cell lung cancer. Clin. Cancer Res. 2005, 11, 4646–4652. [Google Scholar] [CrossRef]
- Wang, X.M.; Li, J.; Yan, M.X.; Liu, L.; Jia, D.S.; Geng, Q.; Lin, H.C.; He, X.H.; Li, J.J.; Yao, M. Integrative analyses identify osteopontin, LAMB3 and ITGB1 as critical pro-metastatic genes for lung cancer. PLoS One 2013, 8, e55714. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.S.; You, J.; Li, Y.; Zhang, Z.F.; Wang, C.L. Osteopontin knockdown suppresses non–small cell lung cancer cell invasion and metastasis. Chin. Med. J. (Engl) 2013, 126, 1683–1688. [Google Scholar] [CrossRef]
- Štemberger, C.; Matušan-Ilijaš, K.; Avirović, M.; Bulat-Kardum, L.; Ivančić, A.; Jonjić, N.; Lučin, K. Osteopontin is associated with decreased apoptosis and αv integrin expression in lung adenocarcinoma. Acta Histochem. 2014, 116, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Rud, A.K.; Boye, K.; Oijordsbakken, M.; Lund-Iversen, M.; Halvorsen, A.R.; Solberg, S.K.; Berge, G.; Helland, A.; Brustugun, O.T.; Mælandsmo, G.M. Osteopontin is a prognostic biomarker in non-small cell lung cancer. BMC Cancer 2013, 13, 540. [Google Scholar] [CrossRef]
- Chang, Y.S.; Kim, H.J.; Chang, J.; Ahn, C.M.; Kim, S.K. Elevated circulating level of osteopontin is associated with advanced disease state of non-small cell lung cancer. Lung Cancer 2007, 57, 373–380. [Google Scholar] [CrossRef]
- Mack, P.C.; Redman, M.W.; Chansky, K.; Williamson, S.K.; Farneth, N.C.; Lara, P.N. Jr.; Franklin, W.A.; Le, Q.T.; Crowley, J.J.; Gandara, D.R.; SWOG. Lower osteopontin plasma levels are associated with superior outcomes in advanced non-small-cell lung cancer patients receiving platinum-based chemotherapy: SWOG Study S0003. J. Clin. Oncol. 2008, 26, 4771–4776. [Google Scholar] [CrossRef] [PubMed]
- Ostheimer, C.; Bache, M.; Güttler, A.; Reese, T.; Vordermark, D. Prognostic information of serial plasma osteopontin measurement in radiotherapy of non-small-cell lung cancer. BMC Cancer 2014, 14, 858. [Google Scholar] [CrossRef] [PubMed]
- Suwinski, R.; Giglok, M.; Galwas-Kliber, K.; Idasiak, A.; Jochymek, B.; Deja, R.; Maslyk, B.; Mrochem-Kwarciak, J.; Butkiewicz, D. Blood serum proteins as biomarkers for prediction of survival, locoregional control and distant metastasis rate in radiotherapy and radio-chemotherapy for non-small cell lung cancer. BMC Cancer 2019, 19, 427. [Google Scholar] [CrossRef]
- Gimba, E.R.P.; Brum, M.C.M.; Nestal De Moraes, G. Full-length osteopontin and its splice variants as modulators of chemoresistance and radioresistance (Review). Int. J. Oncol. 2019, 54, 420–430. [Google Scholar] [CrossRef]
- Behbahani, R.G.; Danyaei, A.; Teimoori, A.; Neisi, N.; Tahmasbi, M.J. Breast cancer radioresistance may be overcome by osteopontin gene knocking out with CRISPR/Cas9 technique. Cancer Radiother. 2021, 25, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Henry, A.; Nokin, M.J.; Leroi, N.; Lallemand, F.; Lambert, J.; Goffart, N.; Roncarati, P.; Bianchi, E.; Peixoto, P.; Blomme, A.; Turtoi, A.; Peulen, O.; Habraken, Y.; Scholtes, F.; Martinive, P.; Delvenne, P.; Rogister, B.; Castronovo, V.; Bellahcène, A. New role of osteopontin in DNA repair and impact on human glioblastoma radiosensitivity. Oncotarget 2016, 7, 63708–63721. [Google Scholar] [CrossRef]
- Chang, S.H.; Minai-Tehrani, A.; Shin, J.Y.; Park, S.; Kim, J.E.; Yu, K.N.; Hong, S.H.; Hong,, C.M.; Lee, K.H.; Beck, G.R. Jr.; Cho, M.H. Beclin1-induced autophagy abrogates radioresistance of lung cancer cells by suppressing osteopontin. J. Radiat. Res. 2012, 53, 422–432. [CrossRef] [PubMed]
- Gu, T.; Ohashi, R.; Cui, R.; Tajima, K.; Yoshioka, M.; Iwakami, S.; Sasaki, S.; Shinohara, A.; Matsukawa, T.; Kobayashi, J.; Inaba, Y.; Takahashi, K. Osteopontin is involved in the development of acquired chemo-resistance of cisplatin in small cell lung cancer. Lung Cancer 2009, 66, 176–183. [Google Scholar] [CrossRef]
- Ouyang, X.; Huang, Y.; Jin, X.; Zhao, W.; Hu, T.; Wu, F.; Huang, J. Osteopontin promotes cancer cell drug resistance, invasion, and lactate production and is associated with poor outcome of patients with advanced non-small-cell lung cancer. Onco. Targets Ther. 2018, 11, 5933–5941. [Google Scholar] [CrossRef]
- Morath, I.; Hartmann, T.N.; Orian-Rousseau, V. CD44: More than a mere stem cell marker. Int. J. Biochem. Cell Biol. 2016, 81, 166–173. [Google Scholar] [CrossRef]
- Pietras, A.; Katz, A.M.; Ekström, E.J.; Wee, B.; Halliday, J.J.; Pitter, K.L.; Werbeck, J.L.; Amankulor, N.M.; Huse, J.T.; Holland, E.C. Osteopontin-CD44 signaling in the glioma perivascular niche enhances cancer stem cell phenotypes and promotes aggressive tumor growth. Cell Stem Cell. 2014, 14, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Hassn Mesrati, M.; Syafruddin, S.E.; Mohtar, M.A.; Syahir, A. CD44: A Multifunctional Mediator of Cancer Progression. Biomolecules 2021, 11, 1850. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhao, S.; Karnad, A.; Freeman, J.W. The biology and role of CD44 in cancer progression: therapeutic implications. J. Hematol. Oncol. 2018, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Ma, Y.; Yang, Y.; Zhang, L.; Han, H.; Chen, J. CD44 promotes cell proliferation in non-small cell lung cancer. Oncol. Lett. 2018, 15, 5627–5633. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Vadhan, A.; Chen, P.H.; Lee, Y.L.; Chao, C.Y.; Cheng, K.H.; Chang, Y.C.; Hu, S.C.; Yuan, S.F. CD44 Promotes Lung Cancer Cell Metastasis through ERK-ZEB1 Signaling. Cancers (Basel) 2021, 13, 4057. [Google Scholar] [CrossRef] [PubMed]
- Yaghobi, Z.; Movassaghpour, A.; Talebi, M.; Abdoli Shadbad, M.; Hajiasgharzadeh, K.; Pourvahdani, S.; Baradaran, B. The role of CD44 in cancer chemoresistance: A concise review. Eur. J. Pharmacol. 2021, 903, 174147. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Cozzi, P.J.; Hao, J.L.; Beretov, J.; Chang, L.; Duan, W.; Shigdar, S.; Delprado, W.J.; Graham, P.H.; Bucci, J.; Kearsley, J.H.; Li, Y. CD44 variant 6 is associated with prostate cancer metastasis and chemo-/radioresistance. Prostate 2014, 74, 602–617. [Google Scholar] [CrossRef] [PubMed]
- Takaishi, S.; Okumura, T.; Tu, S.; Wang, S.S.; Shibata, W.; Vigneshwaran, R.; Gordon, S.A.; Shimada, Y.; Wang, T.C. Identification of gastric cancer stem cells using the cell surface marker CD44. Stem Cells 2009, 27, 1006–1020. [Google Scholar] [CrossRef]
- Liu, J.; Xiao, Z.; Wong, S.K.; Tin, V.P.; Ho, K.Y.; Wang, J.; Sham, M.H.; Wong, M.P. Lung cancer tumorigenicity and drug resistance are maintained through ALDH(hi)CD44(hi) tumor initiating cells. Oncotarget 2013, 4, 1698–1711. [Google Scholar] [CrossRef]
- Gomez-Casal, R.; Bhattacharya, C.; Ganesh, N.; Bailey, L.; Basse, P.; Gibson, M.; Epperly, M.; Levina, V. Non-small cell lung cancer cells survived ionizing radiation treatment display cancer stem cell and epithelial-mesenchymal transition phenotypes. Mol. Cancer 2013, 12, 94. [Google Scholar] [CrossRef]
- Briones-Orta, M.A.; Avendaño-Vázquez, S.E.; Aparicio-Bautista, D.I.; Coombes, J.D.; Weber, G.F.; Syn, W.K. Osteopontin splice variants and polymorphisms in cancer progression and prognosis. Biochim. Biophys. Acta Rev. Cancer 2017, 1868, 93–108. [Google Scholar] [CrossRef]
- Ensembl Database 103. Available online: http://www.ensembl.org/ (accessed on 28 February 2022).
- Giacopelli, F.; Marciano, R.; Pistorio, A.; Catarsi, P.; Canini, S.; Karsenty, G.; Ravazzolo, R. Polymorphisms in the osteopontin promoter affect its transcriptional activity. Physiol. Genomics 2004, 20, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.; Lorenz, P.; Ibrahim, S.M.; Kundt, G.; Gross, G.; Kunz, M. The functional -443T/C osteopontin promoter polymorphism influences osteopontin gene expression in melanoma cells via binding of c-Myb transcription factor. Mol. Carcinog. 2009, 48, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Chen, X.; Meng, T.; Hao, B.; Zhang, Z.; Zhang, G. Genetic polymorphisms in the osteopontin promoter increases the risk of distance metastasis and death in Chinese patients with gastric cancer. BMC Cancer 2012, 12, 477. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.Z.; Zhang, X.F.; Zhao, Y.; Jia, H.L.; Zhou, H.J.; Dai, C.; Sun, H.J.; Qin, Y.; Zhang, W.D.; Ren, N.; Ye, Q.H.; Qin, L.X. Osteopontin promoter polymorphisms at locus -443 significantly affect the metastasis and prognosis of human hepatocellular carcinoma. Hepatology 2013, 57, 1024–1034. [Google Scholar] [CrossRef]
- Jiang, L.; Deng, J.; Zhu, X.; Zheng, J.; You, Y.; Li, N.; Wu, H.; Lu, J.; Zhou, Y. CD44 rs13347 C>T polymorphism predicts breast cancer risk and prognosis in Chinese populations. Breast Cancer Res. 2012, 14, R105. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.; Smith, N.J.; Donnelly, P. A new statistical method for haplotype reconstruction from population data. Am. J. Hum. Genet. 2001, 68, 978–989. [Google Scholar] [CrossRef]
- Broad Institute of Harvard and Massachusetts Institute of Technology, Cambridge, MA, USA. Available online: https://www.broadinstitute.org/haploview/haploview (accessed on 17 October 2022).
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; Liu-Cordero, S.N.; Rotimi, C.; Adeyemo, A.; Cooper, R.; Ward, R.; Lander, E.S.; Daly, M. J.; Altshuler, D. The structure of haplotype blocks in the human genome. Science 2002, 296, 2225–2229. [Google Scholar] [CrossRef]
- Hao, Y.; Liu, J.; Wang, P.; Wang, F.; Yu, Z.; Li, M.; Chen, S.; Ning, F. OPN Polymorphism Is Related to the Chemotherapy Response and Prognosis in Advanced NSCLC. Int. J. Genomics 2014, 2014, 846142. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, H.; Wu, W.; Li, Y.; Li, J. Osteopontin genetic variants are associated with overall survival in advanced non-small-cell lung cancer patients and bone metastasis. J. Exp. Clin. Cancer Res. 2013, 32, 45. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.Y.; Lin, J.T.; Wu, C.C.; Yu, C.C.; Wu, M.S.; Lee, T.C.; Chen, H.P.; Wu, C.Y. Osteopontin promoter polymorphisms are associated with susceptibility to gastric cancer. J. Clin. Gastroenterol. 2013, 47, e55–e59. [Google Scholar] [CrossRef]
- Mu, G.; Wang, H.; Cai, Z.; Ji, H. OPN -443C>T genetic polymorphism and tumor OPN expression are associated with the risk and clinical features of papillary thyroid cancer in a Chinese cohort. Cell Physiol. Biochem. 2013, 32, 171–179. [Google Scholar] [CrossRef]
- Chen, J.; Wu, Q.; Lu, Y.; Xu, T.; Huang, Y.; Ribas, J.; Ni, X.; Hu, G.; Huang, F.; Zhou, L.; Lu, D. SPP1 promoter polymorphisms and glioma risk in a Chinese Han population. J. Hum. Genet. 2010, 55, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.W.; Tu, H.F.; Wang, I.K.; Wu, C.H.; Chang, K.W.; Liu, T.Y.; Kao, S.Y. The implication of osteopontin (OPN) expression and genetic polymorphisms of OPN promoter in oral carcinogenesis. Oral Oncol. 2010, 46, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Nong, L.; Wei, Y.; Qin, S.; Zhou, Y.; Tang, Y. Association of osteopontin polymorphisms with nasopharyngeal carcinoma risk. Hum. Immunol. 2014, 75, 76–80. [Google Scholar] [CrossRef]
- Liang, L.; Lu, G.; Pan, G.; Deng, Y.; Liang, J.; Liang, L.; Liu, J.; Tang, Y.; Wei, G. A Case-Control Study of the Association Between the SPP1 Gene SNPs and the Susceptibility to Breast Cancer in Guangxi, China. Front. Oncol. 2019, 9, 1415. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lei, H.; Zhang, J.; Wang, J.; Li, K.; Dong, W. Associations between the Genetic Polymorphisms of Osteopontin Promoter and Susceptibility to Cancer in Chinese Population: A Meta-Analysis. PLoS One 2015, 10, e0135318. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, H.; Ou, S.; Chen, H. Von Hippel-Lindau gene single nucleotide polymorphism (rs1642742) may be related to the occurrence and metastasis of HBV-related hepatocellular carcinoma. Medicine 2021, 100, e27187. [Google Scholar] [CrossRef]
- Qiu, Y.; Hu, Y.; Zhang, Z.Y.; Ye, L.; Xu, F.H.; Schneider, M.E.; Ma, X.L.; Du, Y.X.; Zuo, X.B.; Zhou, F.S.; Chen, G.; Xie, X.S.; Zhang, Y.; Xia, H.Z.; Wu, J.F.; Du, W.D. Genetic association of osteopontin (OPN) and its receptor CD44 genes with susceptibility to Chinese gastric cancer patients. J. Cancer Res. Clin. Oncol. 2014, 140, 2143–2156. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, J.; Liu, H.; Bi, J.; Liu, Y.; Chen, Y.; Cao, J.; Lu, Y. The association between osteopontin and survival in non-small-cell lung cancer patients: a meta-analysis of 13 cohorts. Onco. Targets Ther. 2015, 8, 3513–3521. [Google Scholar] [CrossRef] [PubMed]
- Winder, T.; Ning, Y.; Yang, D.; Zhang, W.; Power, D.G.; Bohanes, P.; Gerger, A.; Wilson, P.M.; Lurje, G.; Tang, L.H.; Shah, M.; Lenz, H.J. Germline polymorphisms in genes involved in the CD44 signaling pathway are associated with clinical outcome in localized gastric adenocarcinoma. Int. J. Cancer 2011, 129, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Bitaraf, S.M.; Mahmoudian, R.A.; Abbaszadegan, M.; Mohseni Meybodi, A.; Taghehchian, N.; Mansouri, A.; Forghanifard, M.M.; Memar, B.; Gholamin, M. Association of Two CD44 Polymorphisms with Clinical Outcomes of Gastric Cancer Patients. Asian Pac. J. Cancer Prev. 2018, 19, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Suenaga, M.; Yamada, S.; Fuchs, B.C.; Fujii, T.; Kanda, M.; Tanaka, C.; Kobayashi, D.; Fujiwara, M.; Tanabe, K.K.; Kodera, Y. CD44 single nucleotide polymorphism and isoform switching may predict gastric cancer recurrence. J. Surg. Oncol. 2015, 112, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Tongtawee, T.; Wattanawongdon, W.; Simawaranon, T.; Kaewpitoon, S.; Kaengpenkae, S.; Jintabanditwong, N.; Tangjanyatham, P.; Ratchapol, W.; Kangwantas, K.; Dechsukhum, C.; Leeanansaksiri, W.; Kaewpitoon, N.; Matrakool, L.; Panpimanmas, S. Expression of Cancer Stem Cell Marker CD44 and Its Polymorphisms in Patients with Chronic Gastritis, Precancerous Gastric Lesion, and Gastric Cancer: A Cross-Sectional Multicenter Study in Thailand. Biomed. Res. Int. 2017, 2017, 4384823. [Google Scholar] [CrossRef] [PubMed]
- Sapcharoen, K.; Sanguansermsri, P.; Yasothornsrikul, S.; Muisuk, K.; Srikummool, M. Gene Combination of CD44 rs187116, CD133 rs2240688, NF-κB1 rs28362491 and GSTM1 Deletion as a Potential Biomarker in Risk Prediction of Breast Cancer in Lower Northern Thailand. Asian Pac. J. Cancer Prev. 2019, 20, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Márquez-González, R.M.; Saucedo-Sariñana, A.M.; Barros-Núñez, P.; Gallegos-Arreola, M.P.; Pineda-Razo, T.D.; Marin-Contreras, M.E.; Flores-Martínez, S.E.; Sánchez-Corona, J.; Rosales-Reynoso, M.A. CD44 Genotypes Are Associated with Susceptibility and Tumor Characteristics in Colorectal Cancer Patients. Tohoku J. Exp. Med. 2020, 250, 109–119. [Google Scholar] [CrossRef]
- Stotz, M.; Herzog, S.A.; Pichler, M.; Smolle, M.; Riedl, J.; Rossmann, C.; Bezan, A.; Stöger, H.; Renner, W.; Berghold, A.; Gerger, A. Cancer Stem Cell Gene Variants in CD44 Predict Outcome in Stage II and Stage III Colon Cancer Patients. Anticancer Res. 2017, 37, 2011–2018. [Google Scholar] [CrossRef]
- Prasmickaite, L.; Berge, G.; Bettum, I.J.; Aamdal, S.; Hansson, J.; Bastholt, L.; Øijordsbakken, M.; Boye, K.; Mælandsmo, G.M. Evaluation of serum osteopontin level and gene polymorphism as biomarkers: analyses from the Nordic Adjuvant Interferon alpha Melanoma trial. Cancer Immunol. Immunother. 2015, 64, 769–776. [Google Scholar] [CrossRef]
Figure 1.
The Kaplan-Meier plots for (A) metastasis-free survival (MFS) with respect to the OPN rs11730582 and CD44 rs187116 SNP combination in the curative treatment subgroup and for (B) overall survival (OS) with respect to the OPN rs11730582 and rs1126772 SNP combination in the squamous cell carcinoma (SCC) subgroup. Number of events and n are shown in the brackets.
Figure 1.
The Kaplan-Meier plots for (A) metastasis-free survival (MFS) with respect to the OPN rs11730582 and CD44 rs187116 SNP combination in the curative treatment subgroup and for (B) overall survival (OS) with respect to the OPN rs11730582 and rs1126772 SNP combination in the squamous cell carcinoma (SCC) subgroup. Number of events and n are shown in the brackets.
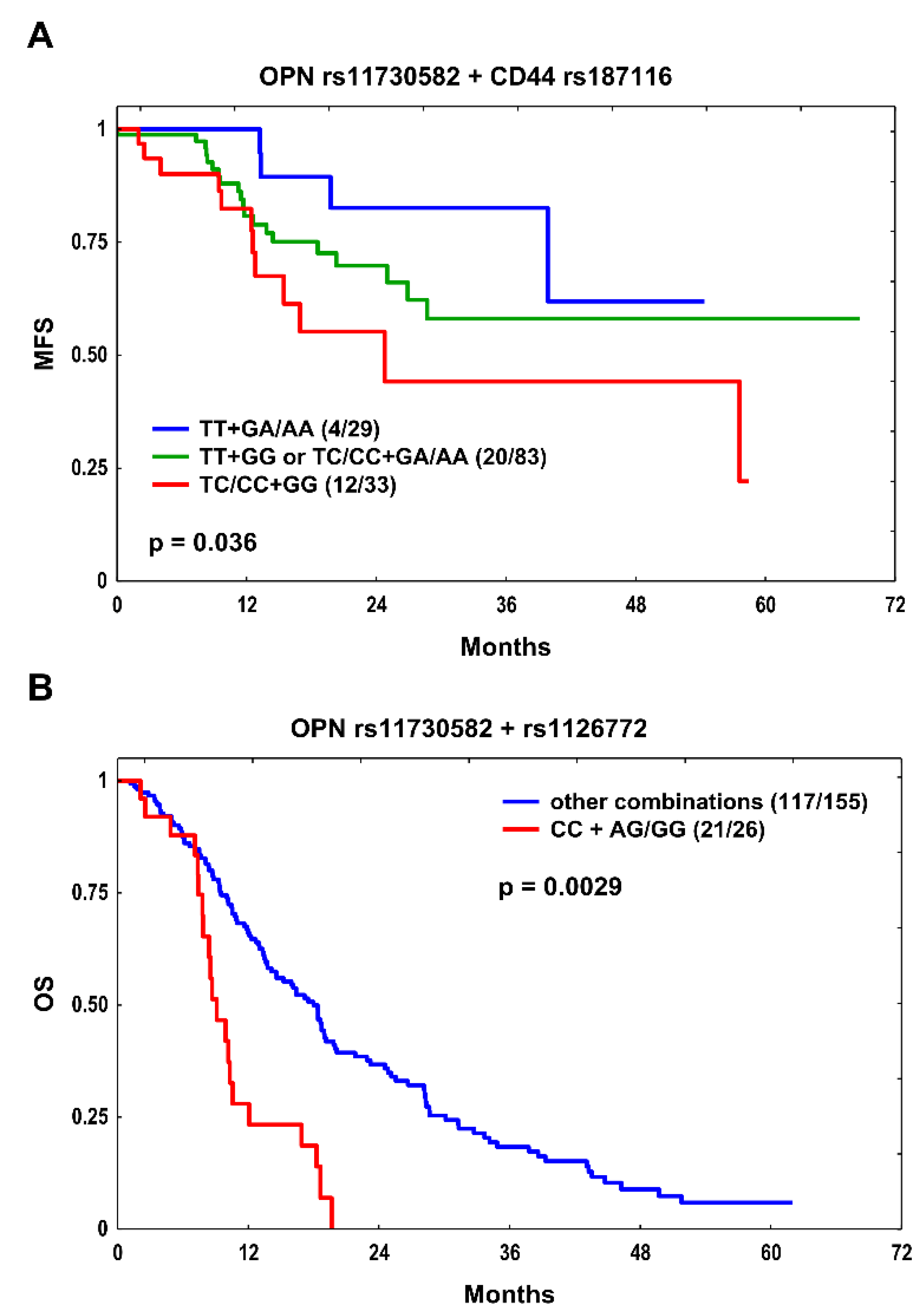

Table 1.
Characteristics of the patients.
| Feature |
All patients n (%) |
Curative treatment n (%) |
|
| Total | 307 (100) | 145 (100) | |
| Age at diagnosis (median) | < 64 years ≥ 64 years |
146 (48) 161 (52) |
84 (58) 61 (42) |
| Sex | Male Female |
239 (78) 68 (22) |
108 (74) 37 (26) |
| Histology NSCLC | SCC AC NOS |
181 (59) 51 (17) 75 (24) |
86 (59) 23 (16) 36 (25) |
| Clinical stage | I–II III–IV |
30 (10) 277 (90) |
20 (14) 125 (86) |
| Performance status | 0 1 2 |
81 (26) 199 (65) 27 (9) |
57 (39) 88 (61) 0 (0) |
| Smoking status | Never smokers Ever smokers |
19 (6) 288 (94) |
13 (9) 132 (91) |
| Chemotherapy use | No Yes |
91 (30) 216 (70) |
12 (8) 133 (92) |
| Radiation dose | < 60 Gy ≥ 60 Gy |
162 (53) 145 (47) |
- 145 (100) |
NSCLC, non-small cell lung cancer; SCC, squamous cell carcinoma; AC, adenocarcinoma; NOS, not otherwise specified.
Table 2.
Cox regression analysis in the whole group, in the curative treatment subset and in patients with SCC (SNPs with p < 0.100 in uni- or multivariate models shown only).
Table 2.
Cox regression analysis in the whole group, in the curative treatment subset and in patients with SCC (SNPs with p < 0.100 in uni- or multivariate models shown only).
| Endpoint | SNP | Genotype | Events/n | p log-rank | HR (95% CI) | p | HR (95% CI) a | p | |
|---|---|---|---|---|---|---|---|---|---|
| All patients | |||||||||
| LRFS |
CD44 rs187116 |
GG GA/AA |
42/105 60/202 |
0.084 |
1.0 0.70 (0.47–1.05) |
0.083 |
1.0 0.73 (0.48–1.11) |
0.139 |
|
| MFS |
OPN rs11730582 |
TT/TC CC |
57/231 21/76 |
0.199 |
1.0 1.42 (0.86–2.34) |
0.174 |
1.0 1.63 (0.97–2.74) |
0.064 |
|
| Curative treatment subgroup | |||||||||
| OS |
OPN rs11730582 |
TT/TC CC |
72/112 23/33 |
0.274 |
1.0 1.32 (0.82–2.11) |
0.251 |
1.0 1.74 (1.06–2.86) |
0.029 |
|
| LRFS |
CD44 rs187116 |
GG GA/AA |
22/48 32/97 |
0.039 |
1.0 0.55 (0.32–0.95) |
0.033 |
1.0 0.48 (0.27–0.87) |
0.016 |
|
| MFS |
OPN rs11730582 |
TT TC/CC |
7/44 29/101 |
0.139 |
1.0 1.84 (0.80–4.21) |
0.148 |
1.0 2.21 (0.94–5.16) |
0.068 |
|
|
CD44 rs187116 |
GG GA/AA |
15/48 21/97 |
0.063 |
1.0 0.52 (0.27–1.01) |
0.054 |
1.0 0.53 (0.27–1.07) |
0.076 |
||
| MFS |
OPN rs11730582 + CD44 rs187116 |
TT + GA/AA TT + GG or TC/CC + GA/AA TC/CC + GG |
4/29 20/83 12/33 |
0.036 |
1.0 2.04 (0.70–5.99) 3.59 (1.15–11.18) |
0.193 0.028 |
1.0 2.36 (0.78–7.12) 4.19 (1.30–13.48) |
0.126 0.016 |
|
| SCC subgroup | |||||||||
|
OS |
OPN rs11730582 |
TT/TC CC |
101/136 37/45 |
0.027 |
1.0 1.60 (1.09–2.34) |
0.015 |
1.0 1.41 (0.94–2.11) |
0.093 |
|
| OPN rs1126772 | AA AG/GG |
92/120 46/61 |
0.034 |
1.0 1.54 (1.07–2.22) |
0.020 |
1.0 1.59 (1.08–2.33) |
0.018 |
||
| OS |
OPN rs11730582 + rs1126772 |
Other combinations CC + AG/GG |
117/155 21/26 |
0.0029 |
1.0 2.82 (1.73–4.60) |
3.3x10-5 |
1.0 2.74 (1.67–4.51 |
7x10-5 |
|
| LRFS |
OPN rs11730582 |
TT/TC CC |
48/136 17/45 |
0.131 |
1.0 1.61 (0.92–2.80) |
0.096 |
1.0 1.48 (0.82–2.66) |
0.192 |
|
| OPN rs1126772 | AA AG/GG |
44/120 21/61 |
0.133 |
1.0 1.57 (0.92–2.67) |
0.095 |
1.0 1.35 (0.75–2.42) |
0.318 |
||
SNP, single nucleotide polymorphism; OS, overall survival; LRFS, locoregional recurrence–free survival; MFS, metastasis–free survival; HR, hazard ratio; CI, confidence interval; SCC, squamous cell carcinoma; a Adjusted for age at diagnosis, sex, smoking, clinical stage, histology type (for the whole group and the curative treatment subset only), performance status, chemotherapy use and radiation dose (for the whole group and the SCC subgroup only); p ≤ 0.05 shown in bold.
Table 3.
The final models for OS, LRFS and MFS considering single SNPs, rs11730582 + rs187116 or rs11730582 + rs1126772 SNP combinations in the curative treatment and SCC subgroups.
Table 3.
The final models for OS, LRFS and MFS considering single SNPs, rs11730582 + rs187116 or rs11730582 + rs1126772 SNP combinations in the curative treatment and SCC subgroups.
| Variable | HR (95% CI) | p |
| Curative treatment subgroup | ||
| OS | ||
|
OPN rs11730582 CC Histology: SCC Ever smoking |
1.66 (1.02–2.70) 2.09 (1.33–3.28) 3.11 (1.13–8.51) |
0.042 0.001 0.027 |
| LRFS | ||
|
CD44 rs187116 GA/AA Histology: SCC Clinical stage III-IV |
0.50 (0.29–0.88) 2.48 (1.40–4.40) 3.34 (1.03–10.84) |
0.016 0.002 0.044 |
| MFS | ||
| OPN rs11730582 + CD44 rs187116 combination: TC/CC + GG | 2.05 (1.02–4.12) | 0.043 |
| SCC subgroup | ||
| OS | ||
|
OPN rs1126772 AG/GG Ever smoking RT dose ≥ 60 Gy |
1.54 (1.06–2.22) 3.42 (1.07–10.86) 0.50 (0.36–0.71) |
0.022 0.037 7.7x10-5 |
|
OPN rs11730582 + rs1126772 combination: CC + AG/GG Ever smoking RT dose ≥ 60 Gy |
2.85 (1.74–4.67) 3.53 (1.11–11.17) 0.50 (0.36–0.72) |
3x10-5 0.032 8.2x10-5 |
OS, overall survival; LRFS, locoregional recurrence-free survival; MFS, metastasis-free survival; HR, hazard ratio; CI, confidence interval; SCC, squamous cell carcinoma; RT, radiotherapy.
Table 4.
Analysis for OS and MFS according to the OPN rs11730582–rs1126772 haplotypes in the curative treatment and SCC subgroups (haplotypes with p < 0.100 in multivariate models shown only).
Table 4.
Analysis for OS and MFS according to the OPN rs11730582–rs1126772 haplotypes in the curative treatment and SCC subgroups (haplotypes with p < 0.100 in multivariate models shown only).
| SNP | Haplotype | Number of copies | plog-rank | HR (95%CI) | p | HR (95% CI)a | p |
| Curative treatment subgroup | |||||||
| rs11730582–rs1126772 | C-A | OS | |||||
| 01–2 | 0.227 | 1.01.28 (0.86–1.92) | 0.229 | 1.01.81 (1.18–2.78) | 0.007 | ||
| MFS | |||||||
| 01–2 | 0.077 | 1.01.81 (0.93–3.54) | 0.082 | 1.02.02 (0.99–4.13) | 0.053 | ||
| SCC subgroup | |||||||
| rs11730582–rs1126772 | T-A | OS | |||||
| 01–2 | 0.026 | 1.00.62 (0.43–0.91) | 0.014 | 1.00.71 (0.47–1.06) | 0.098 | ||
| C-G | OS | ||||||
| 01–2 | 0.033 | 1.01.55 (1.08–2.24) | 0.019 | 1.01.61 (1.10–2.38) | 0.016 | ||
SNP, single nucleotide polymorphism; OS, overall survival; MFS, metastasis–free survival; HR, hazard ratio; CI, confidence interval; a Adjusted for age at diagnosis, sex, smoking, clinical stage, histology type (for the curative treatment subset only), performance status, chemotherapy use and radiation dose (for the SCC subgroup only); p ≤ 0.05 shown in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



