
Submitted:
13 November 2023
Posted:
14 November 2023
You are already at the latest version
Abstract
Study design : Technical note.
Objectives: To present a new spinal shortening technique for tethered cord syndrome.
Background : Tethered cord syndrome (TCS) is a debilitating condition of progressive neurological decline. Surgical detethering for TCS is a gold standard. However, symptomatic retethering of TCS has been reported in 5%–50% of patients after initial release. To solve this problem, posterior spinal shortening osteotomy has been reported. This technique has risks of massive blood loss and neurological deterioration. The authors hereby report a new safe spinal shortening technique for tethered cord syndrome.
Materials and Methods : A 31-year-old man with gait disturbance was referred to our hospital. After the delivery, he underwent surgical untethering of spinal cord in another hospital. He had hyperreflexia of Achilles tendon reflex and muscle weakness of bilateral legs (MMT 3-4). He also had urinary and bowel incontinence, and total sensory loss below L5.Anteroposterior lumbar radiogram indicates partial laminectomy of L3 and L4. Lumbar MRI showed retethering of spinal cord.
Results: He underwent new spinal shortening technique for tethered cord syndrome under the guidance of O-arm navigation. First, from anterior approach disectomy from T12 to L3 was performed. Second, from posterior Ponte osteotomy was done from T12 to L3, shorten the spinal column 15 mm. The patient was successfully treated surgically. Postoperative lumbar MRI showed the tension of spinal cord was released. Manual muscle testing results and sensory function of the left leg had recovered almost fully on final follow-up at one year.
Conclusions/Level of Evidence: Retethered spinal cord after initial untethering was difficult to treat. This new spinal shortening technique was effective and very safe technique to release the tension of spinal cord. Level V.
Keywords:
Tethered cord syndrome
; Navigation
; Spinal shortening osteotomy
1. Introduction
Tethered cord syndrome (TCS) is defined as the traction of the lower end of spinal cord by a thickened filum terminale or spinal lipoma [1,2]. The symptoms of TCS are low back pain, lower-extremity motor, and sensory deficits; and urinary and bowel incontinence; and sexual dysfunction [3]. If the symptoms are severe and progressive, the surgical intervention is indicated [4]. The aim of surgery is to release the spinal cord and neural elements from tension to restore neurological function and prevent further deterioration [5]. The gold standard for TCS surgery is untethering of spinal cord [6,7]. The result of detethering was relatively good; 40-60% improvement in urinary symptoms, 40-70% improvement in motor disturbance, and 80-90% pain improvement [5]. However, recurrent or retethering of spinal cord has been reported more than 25% [6,7,8].
Because of high complications such as retethering, arachnoid adhesion, cerebral fluid leakage, psuedomeningocele, and wound problem [9,10]. In 2009, Miyakoshi et al. reported spine-shortening vertebral osteotomy (SVO) for TCS to relieve the longitudinal tension placed on the tethered neural elements without violating the dura.[11]. After their reports, many authors reported excellent results of this technique [5,12]. However, disadvantage of SVO were massive blood loss and some risk of neurological deterioration [13]. The authors here by present a novel technique for shortening spinal column without such risks.
This study was approved by the ethics committee of our institute (No. 434). Necessary consents were obtained from the patient.
2. Case 1 31 years old male, tethered cord syndrome
2.1. Patient history
A 31-year-old man with gait disturbance was referred to our hospital. After the delivery, he underwent surgical untethering of spinal cord in another hospital.
2.2. Physical examination
The patient can walk without any support. In the examination, he had hyperreflexia of Achilles tendon reflex and muscle weakness of bilateral legs (MMT: tibialis anterior 4 4, extensor halluces longus 4 3, flexor halluces longus 4 2). He also had urinary and bowel incontinence, and total sensory loss below bilateral L5.
2.3. Preoperative imaging
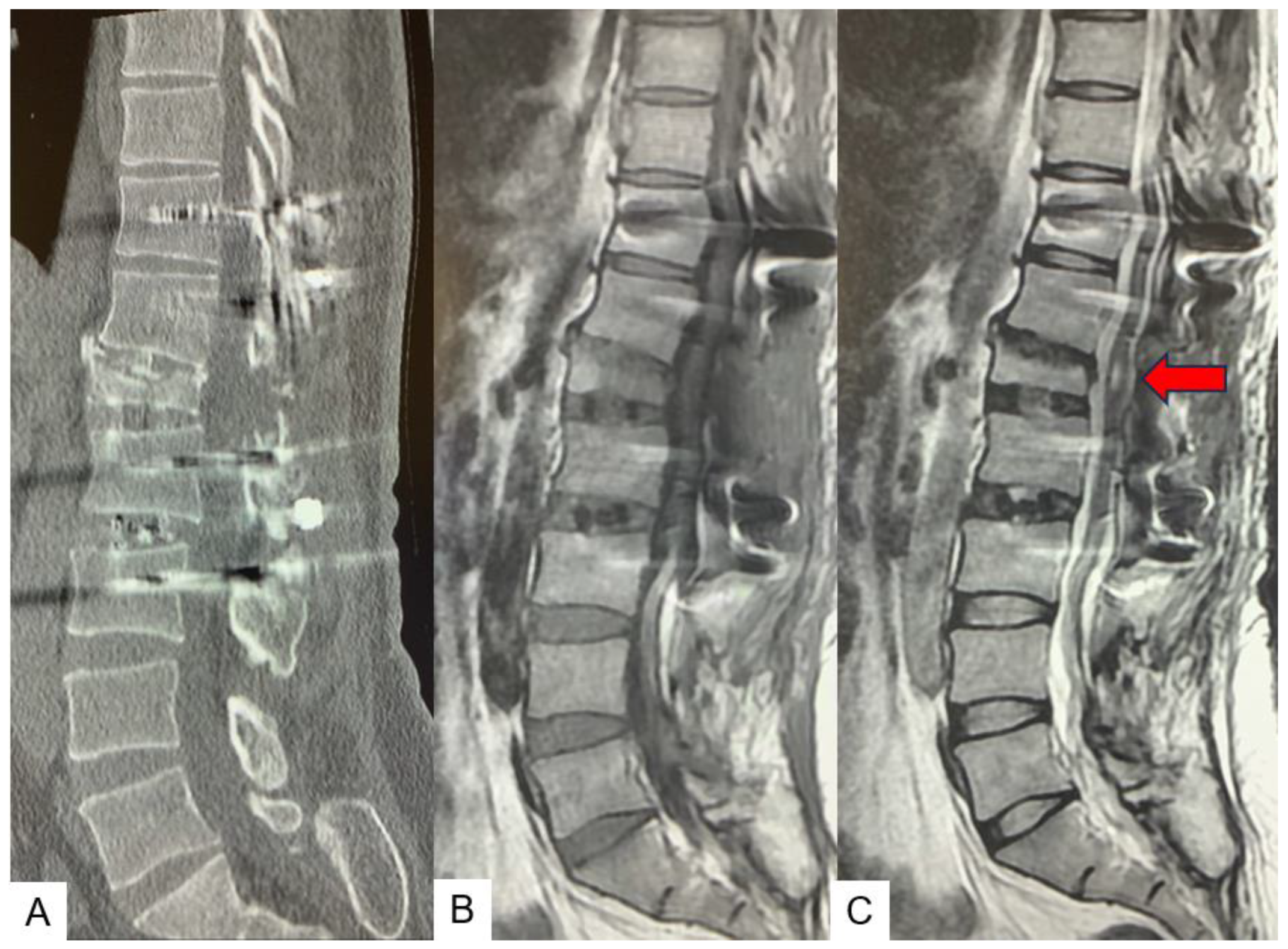
Preoperative anteroposterior lumbar radiogram indicates partial laminectomy of L3 and L4 (Figure 1). Preoperative lumbar CT showed small spinous process from L2 to S1. Preoperative MRI indicated retethering of spinal cord. In L4.5 spinal canal, a lipoma was attached with spinal cord and retethering was observed (Figure 2).
2.4. Surgery
2.4.1. Anterior disectomy
He underwent new spinal shortening technique for tethered cord syndrome under the guidance of O-arm navigation and neuromonitouring (Figure 3A). First step is anterior approach. The patient is placed in in right decbitus position on the full carbon table. The percutaneous reference frame is inserted into left sacroiliac joint. Then O-arm scan is performed and 3D images are transfered to the navigation. The left 11th rib is resected with 5cm oblique skin inscision (Figure 3B).
2.4.2. Posterior osteotomy
On the same day, the patient is on the prone position on a full carbon table. Another O-arm scan is performed. Then posterior elemnts are exposed with longitudinal incision. Pedicle screws from T11 to L3 are inserted under navigation guidance. The ponte osteotomy and posterior anulus are resected from T11/12 to L2/3 (Figure 7A). Finally, compression force is applied each disc level with compressor (Figure 7B), After the whole procedure is completed, the spinal column is shorted as 15 mm (Figure 8).
The patient was successfully treated surgically. Surgical time was 4 hours and 10 minutes and estimated blood loss was 775 ml. The patient experienced no postoperative complications such as dural tear, surgical site infection, or neurological compromise.
2.5. Postoperative imagings.
Postoperative radiograms showed a good alignment and the shortenig of the spinal column as 15 mm. The bony resection area was adequate (Figure 9).
2.6. One year follow-up
The patient recovered almost fully well (JOA 16/17) at six months follow-up. The syringomyelia showed decrease in morphology (Figure 10). Manual muscle testing became slightly recovered and sensory function of the left leg had recovered almost fully on final follow-up at one year.
3. Case 2 33 years old male, tethered cord syndrome, conventional technique
This patient underwent conventional shortening osteotomy. Preoperative radiograms (Figure 11), CT and MRI (Figure 12) are presented.
The conventional spinal column shortening osteotomy was performed (Figure 13 and Figure 14). The surgical time was 6 hours and 57 minutes and estimated blood loss was 2370 ml.
After the surgery, the patient neurological status was slightly deteriorated. Postoperative CT showed good spinal shortening was achieved, but spinal cord damage was observed in the osteotomy site (Figure 15). After two years follow up, the patient’s symptoms were almost recovered.
4. Discussion
Garceau first described ‘filum terminale syndrome’ in 1953 [14]. Hoffmann in 1976, first coined the term ‘tethered cord syndrome’ and described it to occur due to traction to spinal cord due to thick filum terminale [15]. Later, Yamada further included conditions like meningomyelocele, lipomeningomyelocele, diastematomyelia, intradural lipoma, dermoid sinus in tethered cord syndrome [16]. It has been postulated that disproportionate growth of vertebral column and spinal cord leads to nerve roots traction and metabolic changes.
The clinical presentation in Tethered cord syndrome varies according to the age and eatiology. Infants with this syndrome may show, lipomas, tufts of hair, nevi,hemangiomas, and dermal sinuses or, cutaneous manifestations of spina bifida occulta. Scoliosis or lower limb deformities may be present [17]. High suspicion of this syndrome should be kept in mind if anorectal malformations are present in child. Toddlers my present with pain, sensory motor deficit, scoliosis, bladder dysfunction, lower limb deformities, gait disturbance [18].
The trend of treatment for TCS has changed from wait and watch to early intervention in the form of surgical detethering as natural history of this disease is of gradual progression [19]. Warder et al reported sensory improvement in 100% cases, motor improvement in 67% cases, bladder and bowel symptoms improvement in 75% and 100% cases [20]. A systemic review by O’connor et al reported that after detethering sensory deficit improved in 45% cases, motor deficit improved in 61% cases, bladder and bowel dysfunction improved in 45% and 32% cases respectively [21]. But detethering surgery is associated with complications like CSF leak, surgical site infection, meningitis. Although major problem is of retethering which can be seen in about 5% to 50% case [22,23,24].
Because of these complications Kokubun et al [25] described alternative treatment in the form of spine vertebral shortening osteotomy for TCS and Miyakoshi [26] later presented their results with this technique. The aim of this procedure is to indirectly reduce traction of neural elements by spinal column shortening. However, complications in these procedures can be as high as 40% which include neurological injury and massive blood loss [27].
In our procedure, we are performing anterior O arm guided C arm free discectomy followed by posterior osteotomy and fixation. Anterior discectomy is muscle splitting approach with minimal blood loss and can be performed within short time with the help of O arm guidance [28]. Pontes osteotomy and pedicle screw fixation can be done with precision and in shorter time with O arm guidance, this reduces blood loss and risk of neurological injury [29].
Radiation exposure to surgeon and operating staff is major concern. Radiation exposure can lead to various health problems like early cataract, infertility can cancers [30]. With use of O arm there is no radiation exposure to operating staff and surgeon.
5. Conclusions
Retethered spinal cord after initial untethering was difficult to treat. This new spinal shortening technique was effective and very safe technique to release the tension of spinal cord.
Author Contributions
M.T.: conceptualisation, supervision; S.S: writing—review and editing; X.X.: writing—review and editing; S.A: writing—original draft preparation, methodology; Y.F.: data collection; T.T.: data collection.; K.U.: data collection, Y.O.: data collection, K.S.: data collection, All authors have read and agreed to the published version of the manuscript.
Funding
This study received funding from Japan Organization of Occupational Health and Safety.
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the institutional review boards at Okayama Rosai Hospital (approval No. xx, Aug 1, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in the article.
Acknowledgments
This study was supported by Okayama Spine Group.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Chapman PH: Congenital intraspinal lipomas: anatomic considerations and surgical treatment. Childs Brain 9:37–47, 1982. [CrossRef]
- Yamada S, Knerium DS, Mandybur GM, Schultz RL, Yamada BS: Pathophysiology of tethered cord syndrome and other complex factors. Neurol Res 26:722–726, 2004. [CrossRef]
- Pang D, Wilberger JE Jr: Tethered cord syndrome in adults. J Neurosurg 57:32–47, 1982. [CrossRef]
- Bui CJ, Tubbs RS, Oakes WJ: Tethered cord syndrome in children: a review. Neurosurg Focus 23(2):E2, 2007. [CrossRef]
- Hsieh PC, Stapleton CJ, Moldavskiy P, Koski TR, Ondra SL, Gokaslan ZL, Kuntz C. Posterior vertebral column subtraction osteotomy for the treatment of tethered cord syndrome: review of the literature and clinical outcomes of all cases reported to date. Neurosurg Focus. 2010 Jul;29(1):E6. [CrossRef]
- Archibeck MJ, Smith JT, Carroll KL, Davitt JS, Stevens PM: Surgical release of tethered spinal cord: survivorship analysis and orthopedic outcome. J Pediatr Orthop 17:773–776, 1997.
- Filler AG, Britton JA, Uttley D, Marsh HT: Adult postrepair myelomeningocoele and tethered cord syndrome: good surgical outcome after abrupt neurological decline. Br J Neurosurg 9:659–666, 1995. [CrossRef]
- Samuels R, McGirt MJ, Attenello FJ, Garcés Ambrossi GL, Singh N, Solakoglu C, et al: Incidence of symptomatic retethering after surgical management of pediatric tethered cord syndrome with or without duraplasty. Childs Nerv Syst 25:1085–1089, 2009. [CrossRef]
- Herman JM, McLone DG, Storrs BB, Dauser RC: Analysis of 153 patients with myelomeningocele or spinal lipoma reoperated upon for a tethered cord. Presentation, management and outcome. Pediatr Neurosurg 19:243–249, 1993. [CrossRef]
- Maher CO, Goumnerova L, Madsen JR, Proctor M, Scott RM: Outcome following multiple repeated spinal cord untethering operations. J Neurosurg 106 (6 Suppl):434–438, 2007. [CrossRef]
- Miyakoshi N, Abe E, Suzuki T, Kido T, Chiba M, Shimada Y. Spine-shortening vertebral osteotomy for tethered cord syndrome: report of three cases. Spine (Phila Pa 1976). 2009 Oct 15;34(22):E823-5. [CrossRef]
- Zhang C, Chang CC, Mummaneni PV, Yuan C, Dhall S, Jian F, Gupta N, Chou D. Spinal column shortening versus revision detethering for recurrent adult tethered cord syndrome: a preliminary comparison of perioperative and clinical outcomes. J Neurosurg Spine. 2020 Feb 7:1-7. [CrossRef]
- Auerbach JD, Lenke LG, Bridwell KH, Sehn JK, Milby AH, Bumpass D, Crawford CH 3rd, OʼShaughnessy BA, Buchowski JM, Chang MS, Zebala LP, Sides BA. Major complications and comparison between 3-column osteotomy techniques in 105 consecutive spinal deformity procedures. Spine (Phila Pa 1976). 2012 Jun 15;37(14):1198-210. [CrossRef]
- Garceau: George J. The filum terminale syndrome. The Journal of Bone & Joint Surgery 195335(3):p 711-716.
- Harold J Hoffman; E. Bruce Hendrick; Robin P Humphreys. The tethered spinal cord its protean manifestations, diagnosis and surgical correction. Child’s Brain 1976: 145-155. [CrossRef]
- Yamada S, Zinke DE, Sanders D. Pathophysiology of “tethered cord syndrome.” Vol. 54, J Neurosurg. 1981. [CrossRef]
- Yamada S, Knerium DS, Mandybur GM, Schultz RL, Yamada BS. Pathophysiology of tethered cord syndrome and other complex factors. Neurological Research. 2004, 722–726. [CrossRef]
- N. Muthukumar; B. Subramaniam; T. Gnanaseelan; R. Rathinam; A. Thiruthavadoss. Tethered cord syndrome in children with anorectal. J Neurosurg 2000, 92, 626–630. [CrossRef]
- J. Herman; D. McLone; B. Storrs; R. Dauser.Analysis of 153 patients with myelomeningocele or spinal lipoma reoperated upon for a tethered cord. Presentation, management and outcome. Pediatr Neurosurg 1993, 19, 243-249. [CrossRef]
- D E Warder; W J Oakes.Tethered cord syndrome and the conus in a normal position. Neurosurgery, 1993 Sep;33(3):374-378.
- O’Connor KP, Smitherman AD, Milton CK, Palejwala AH, Lu VM, Johnston SE, et al. Surgical Treatment of Tethered Cord Syndrome in Adults: A Systematic Review and Meta-Analysis. World Neurosurg. 2020, 1, 137, 221–241. [CrossRef]
- A G Filler ; J A Britton; D Uttley; H T Marsh. Adult postrepair myelomeningocoele and tethered cord syndrome good surgical outcome after abrupt neurological decline. Br J Neurosurg, 1995, 9(5), 659-666.
- Samuels R, McGirt MJ, Attenello FJ, Garcés Ambrossi GL, Singh N, Solakoglu C, et al. Incidence of symptomatic retethering after surgical management of pediatric tethered cord syndrome with or without duraplasty. Child’s Nervous System. 2009, 25(9), 1085–1089. [CrossRef]
- Morimoto K, Takemoto O, Wakayama A. Spinal lipomas in children - Surgical management and long-term follow-up. Pediatr Neurosurg. 2005, 41(2), 84–87. [CrossRef]
- Kokubun S, Ozawa H, Aizawa T, Ly NM, Tanaka Y. Spine-shortening osteotomy for patients with tethered cord syndrome caused by lipomyelomeningocele. J Neurosurg Spine. 2011, 15(1), 21–27. [CrossRef]
- Miyakoshi N, Abe E, Suzuki T, Kido T, Chiba M, Shimada Y. Spine-Shortening Vertebral Osteotomy for Tethered Cord Syndrome Report of Three Cases. SPINE , 34, 22, 823–825. [CrossRef]
- Auerbach JD, Lenke LG, Bridwell KH, Sehn JK, Milby AH, Bumpass D, et al. Major complications and comparison between 3-column osteotomy techniques in 105 consecutive spinal deformity procedures. Spine (Phila Pa 1976). 2012, 37(14),1198–210. [CrossRef]
- Masato Tanaka, Sameer Ruparel, Yoshiaki Oda, Yoshihiro Fujiwara, Sneha Shama, Koji Uotani, Shinya Arataki, Taro Yamauchi, Naveen Sake. C arm Free Simultaneous OLIF51 and Percutaneous Pedicle Screw Fixation in a Single Lateral Position. J Vis Exp, 2022, 16, 187-192. [CrossRef]
- Li B, Guo R, Jiang X, Wu J, Zhang D, Yang C, et al. Posterior wedge osteotomy assisted by O-arm navigation for treating ankylosing spondylitis with thoracolumbar fractures: An early clinical evaluation. Ann Palliat Med. 2021, 1, 10(6), 694–705. [CrossRef]
- D. Croci; S. Nguyen; S. Streitmatter; B. Sherrod; J. Hardy; K. Cole; A. Gamblin; E. Bisson; M Mazur; A. Dailey. O Arm Accuracy and Radiation Exposure in Adult Deformity Surgery. World Neurosurg. 2023, 171, 440-446. [CrossRef]
Figure 1.
Preoperative radiograms, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. L3.4 were partial laminectomy because of previous detethering surgery (red arrows).
Figure 1.
Preoperative radiograms, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. L3.4 were partial laminectomy because of previous detethering surgery (red arrows).
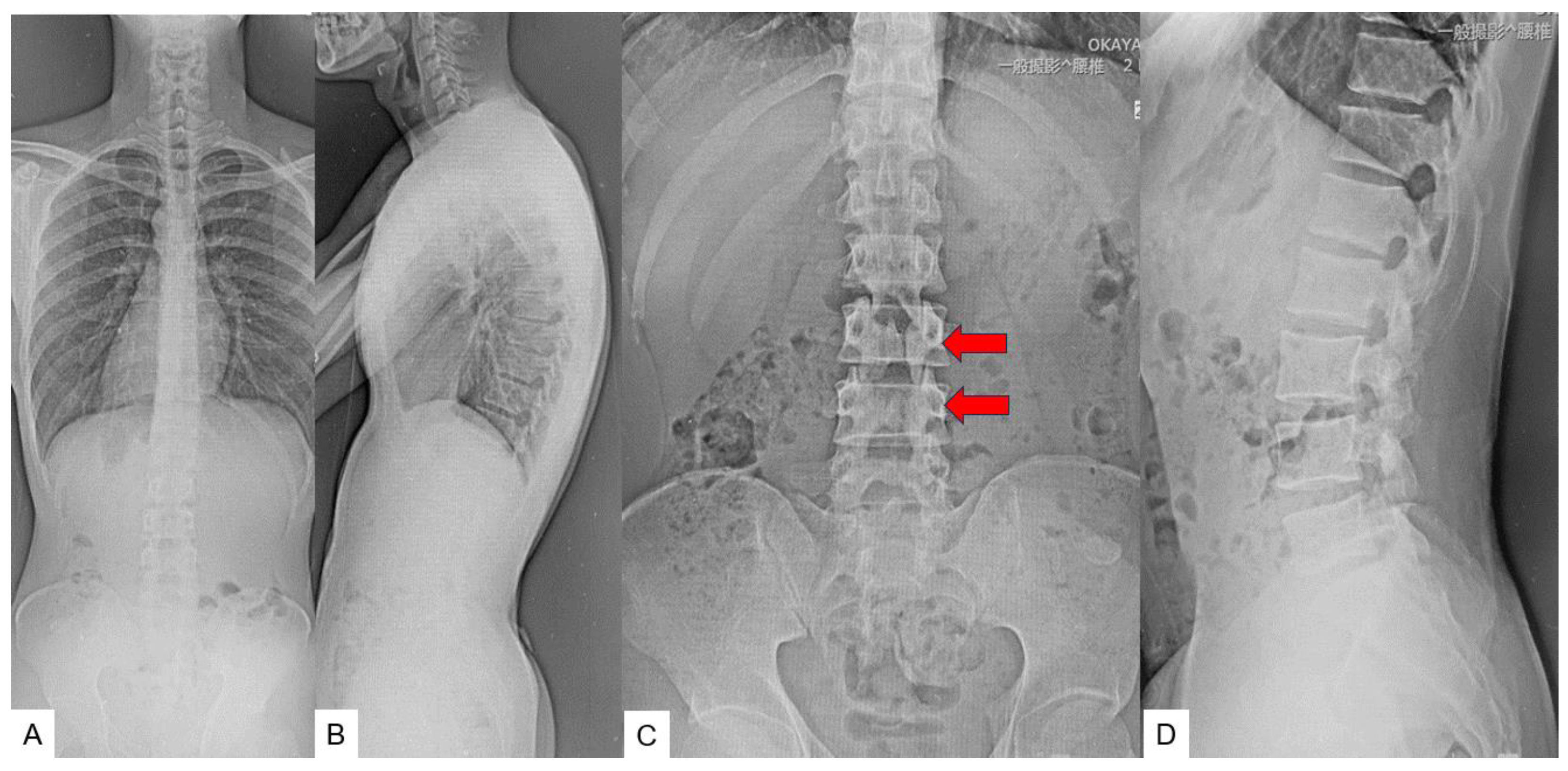
Figure 2.
Preoperative CT and MR imaging, A: Mid sagittal 3D reconstruction CT, B: T1 weighted mid-sagittal MR imaging, .C: T2 weighted mid-sagittal MR imaging, a lipoma was attached with spinal cord and retethering was observed (red arrows).
Figure 2.
Preoperative CT and MR imaging, A: Mid sagittal 3D reconstruction CT, B: T1 weighted mid-sagittal MR imaging, .C: T2 weighted mid-sagittal MR imaging, a lipoma was attached with spinal cord and retethering was observed (red arrows).
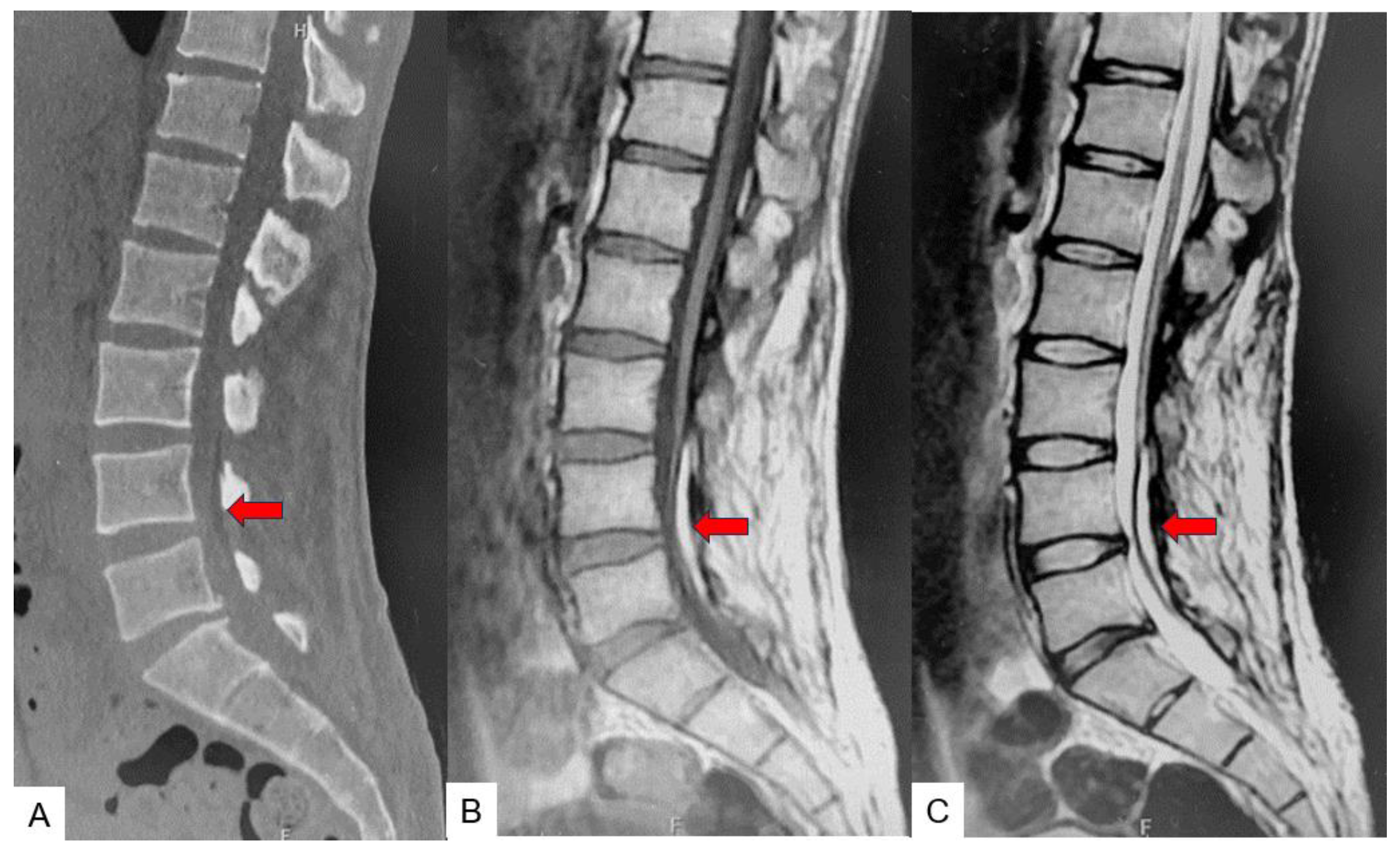
Figure 3.
Neuromonitouring and anterior approach, A: Neuromonitouring, B: The 11th rib resection.
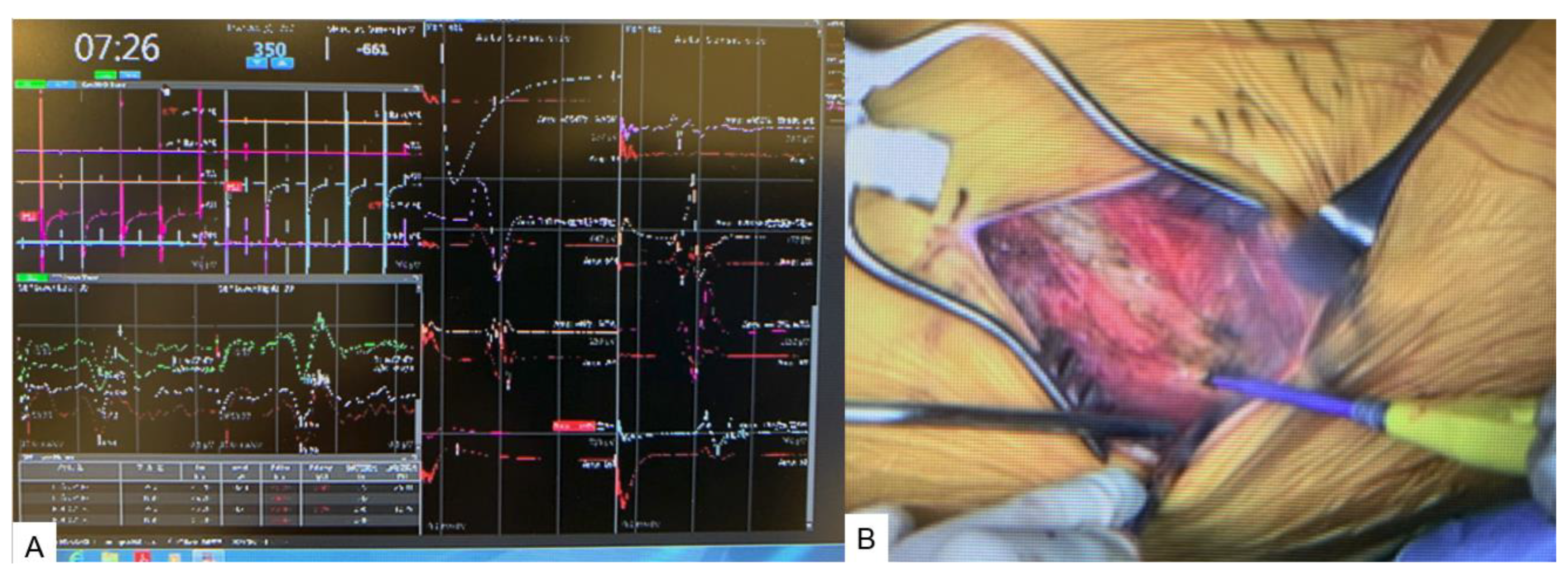
Figure 4.
Nagigated pointer, A: Intraoperative image, B: Navigation monitor (Coronal), C: Navigation monitor (Axial), D: Navigation monitor (3D).
Figure 4.
Nagigated pointer, A: Intraoperative image, B: Navigation monitor (Coronal), C: Navigation monitor (Axial), D: Navigation monitor (3D).
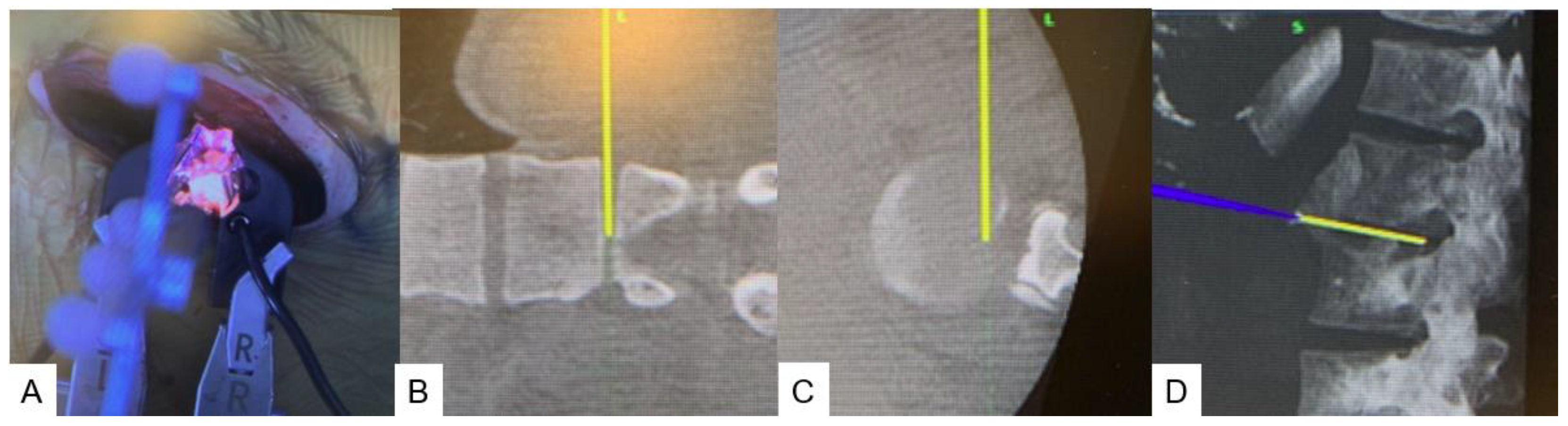
Figure 5.
navigated currte, A: Intraoperative image, B: Navigation monitor (Coronal), C: Navigation monitor (Axial), D: Navigation monitor (3D).
Figure 5.
navigated currte, A: Intraoperative image, B: Navigation monitor (Coronal), C: Navigation monitor (Axial), D: Navigation monitor (3D).
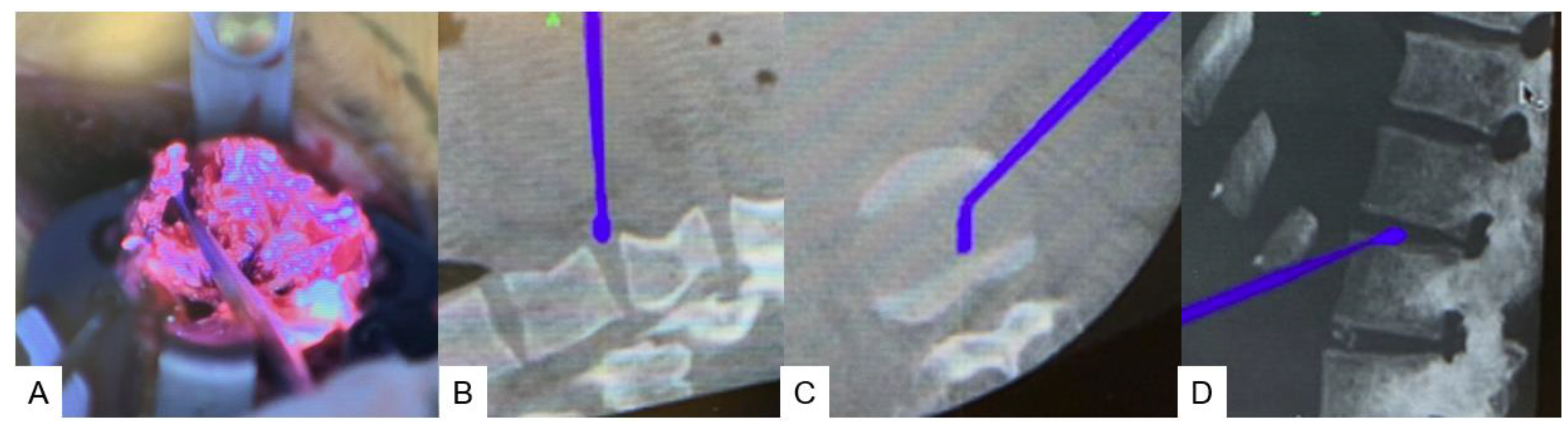
Figure 6.
navigated shaver and navigated Cobb, A: Navigated shaver (Coronal), B: Navigated shaver (Axial), C: Navigated Cobb (Coronal),, D: Navigated Cobb (Axial),.
Figure 6.
navigated shaver and navigated Cobb, A: Navigated shaver (Coronal), B: Navigated shaver (Axial), C: Navigated Cobb (Coronal),, D: Navigated Cobb (Axial),.
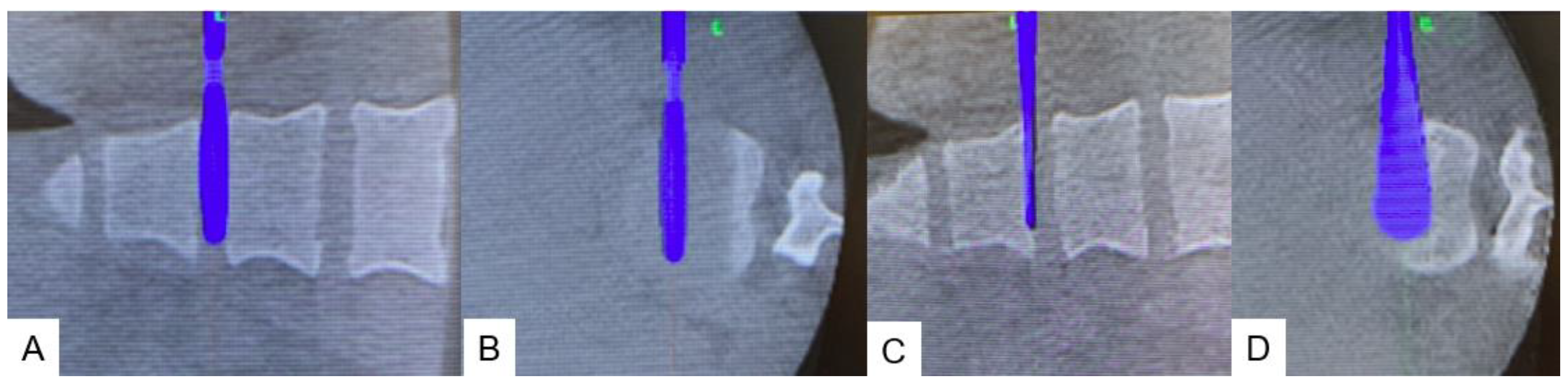
Figure 7.
Posterior surgery, A: Pone osteotomy, B: Spinal shortening with compressor.
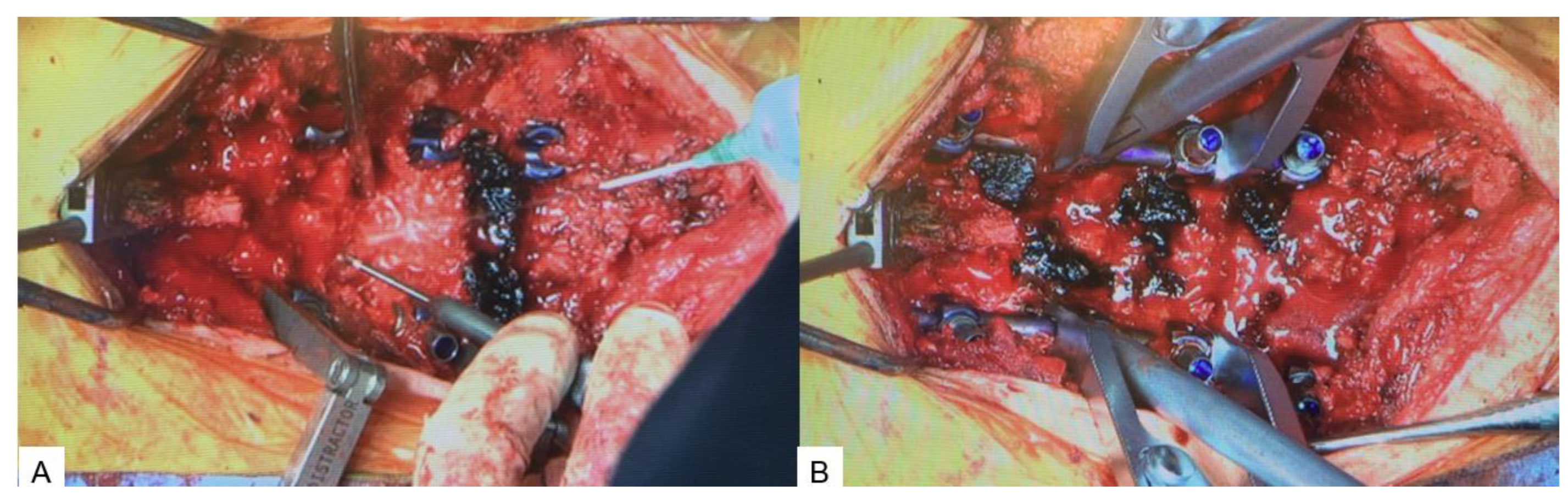
Figure 8.
Shema of new spinal shortening osteotomy.
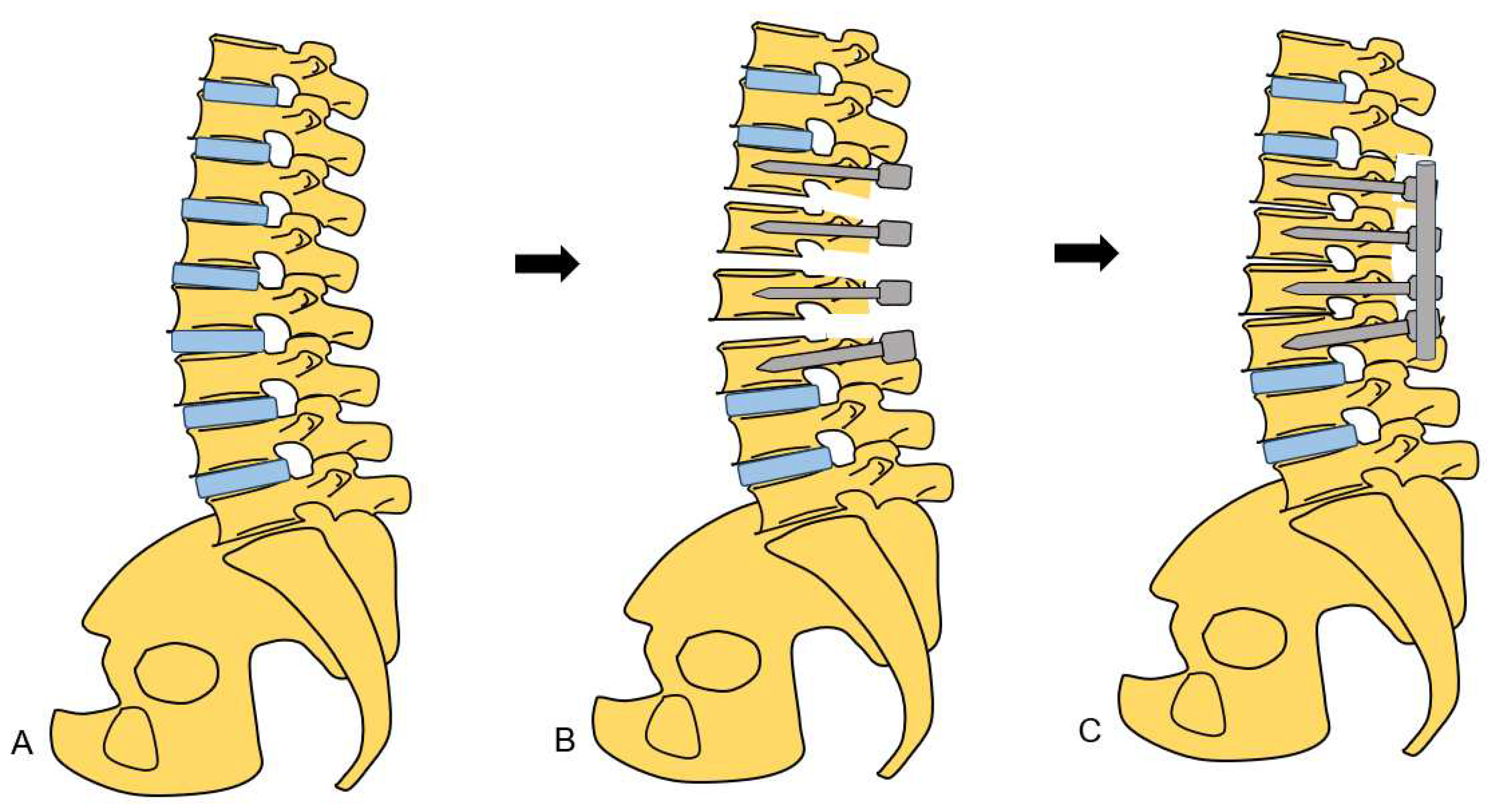
Figure 9.
Postoperative images, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. Spinal column was shortened 15 mm.
Figure 9.
Postoperative images, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. Spinal column was shortened 15 mm.
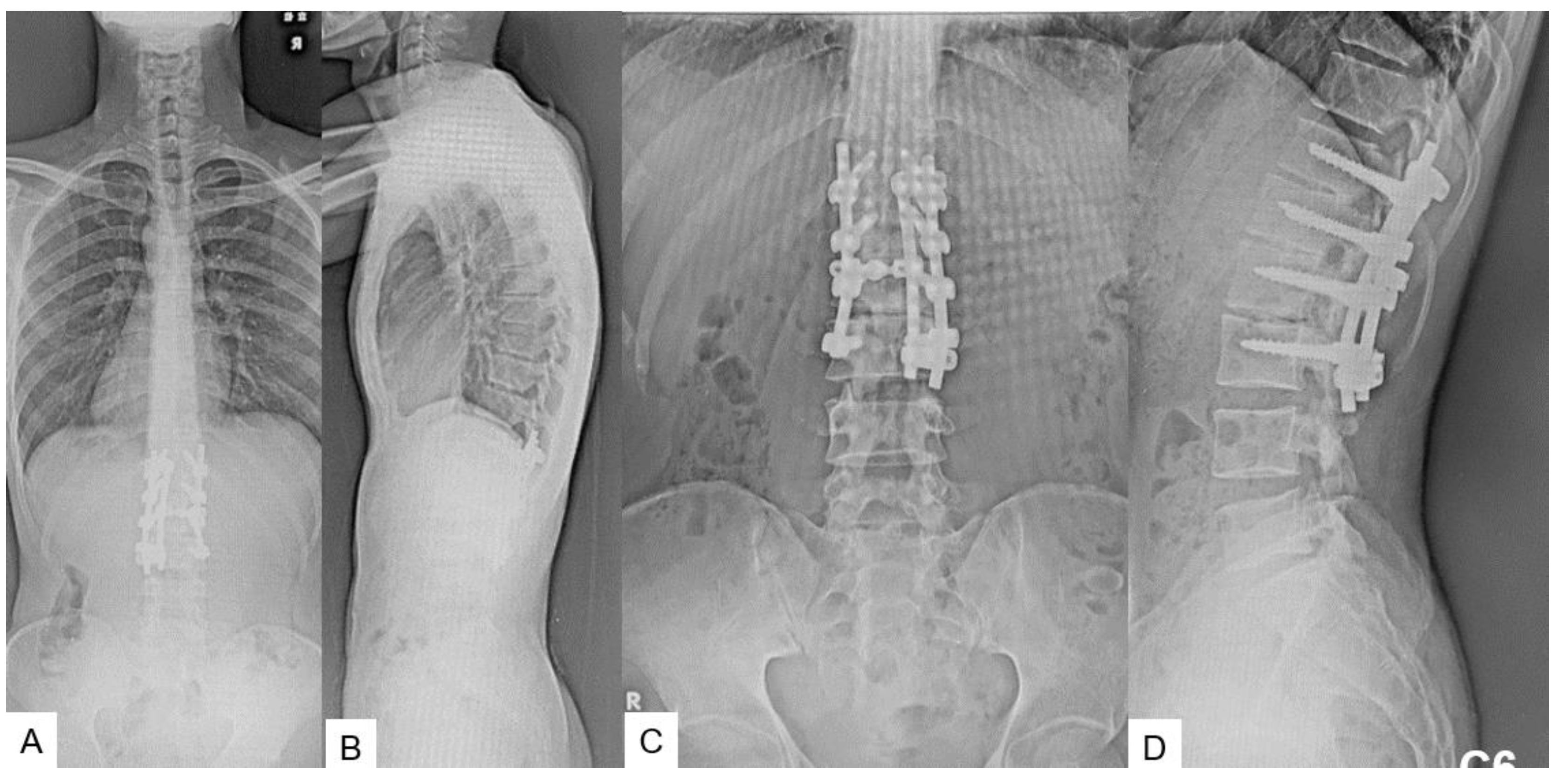
Figure 10.
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging.
Figure 10.
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging.

Figure 11.
Preoperative radiograms, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. L3.4 were partial laminectomy because of previous detethering surgery (red arrows).
Figure 11.
Preoperative radiograms, A: Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. L3.4 were partial laminectomy because of previous detethering surgery (red arrows).
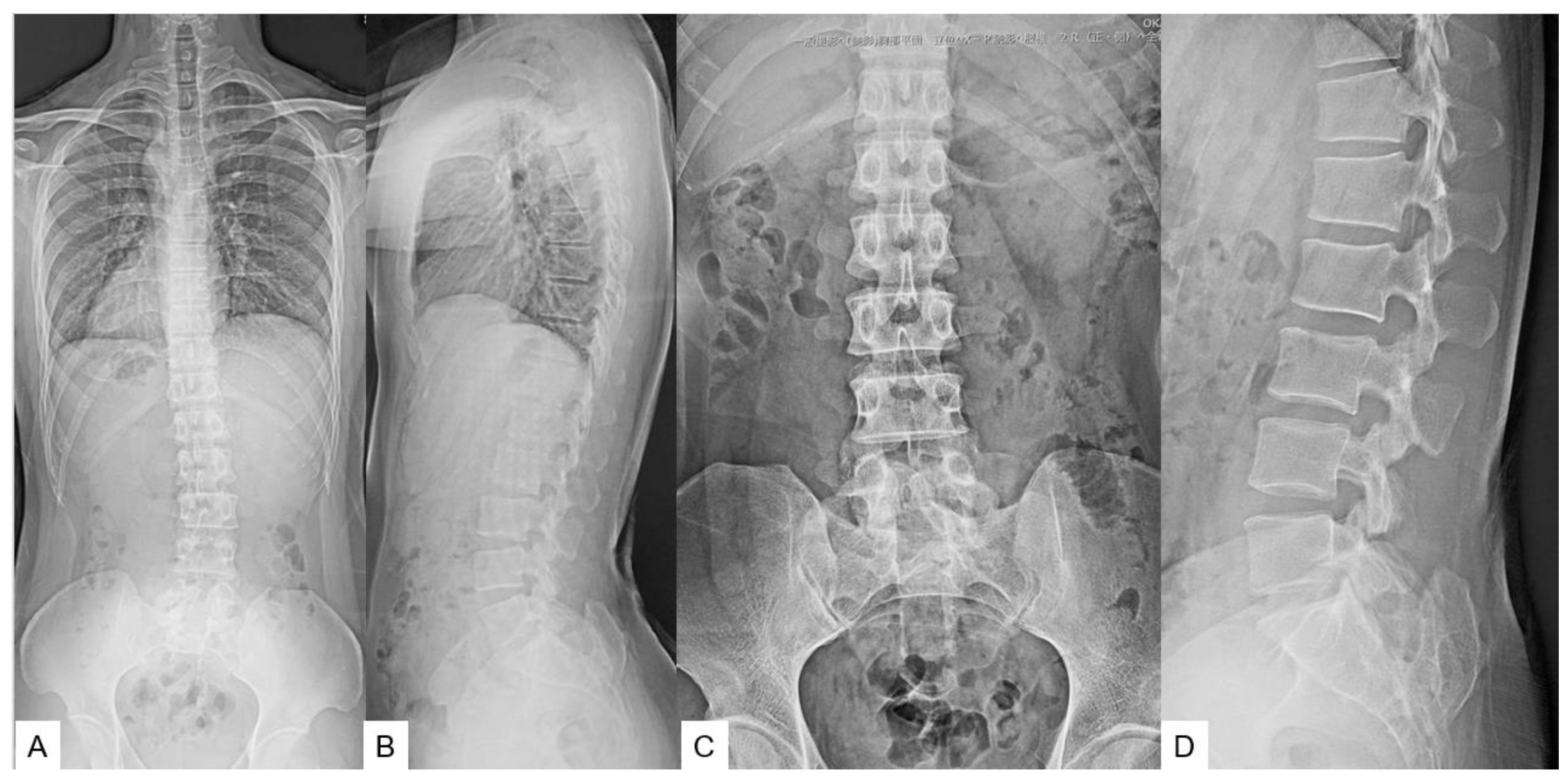
Figure 12.
Preoperative CT and MR imaging, A: Mid sagittal 3D reconstruction CT, B: T1 weighted mid-sagittal MR imaging, .C: T2 weighted mid-sagittal MR imaging, a lipoma was attached with spinal cord and retethering was observed (red arrows).
Figure 12.
Preoperative CT and MR imaging, A: Mid sagittal 3D reconstruction CT, B: T1 weighted mid-sagittal MR imaging, .C: T2 weighted mid-sagittal MR imaging, a lipoma was attached with spinal cord and retethering was observed (red arrows).
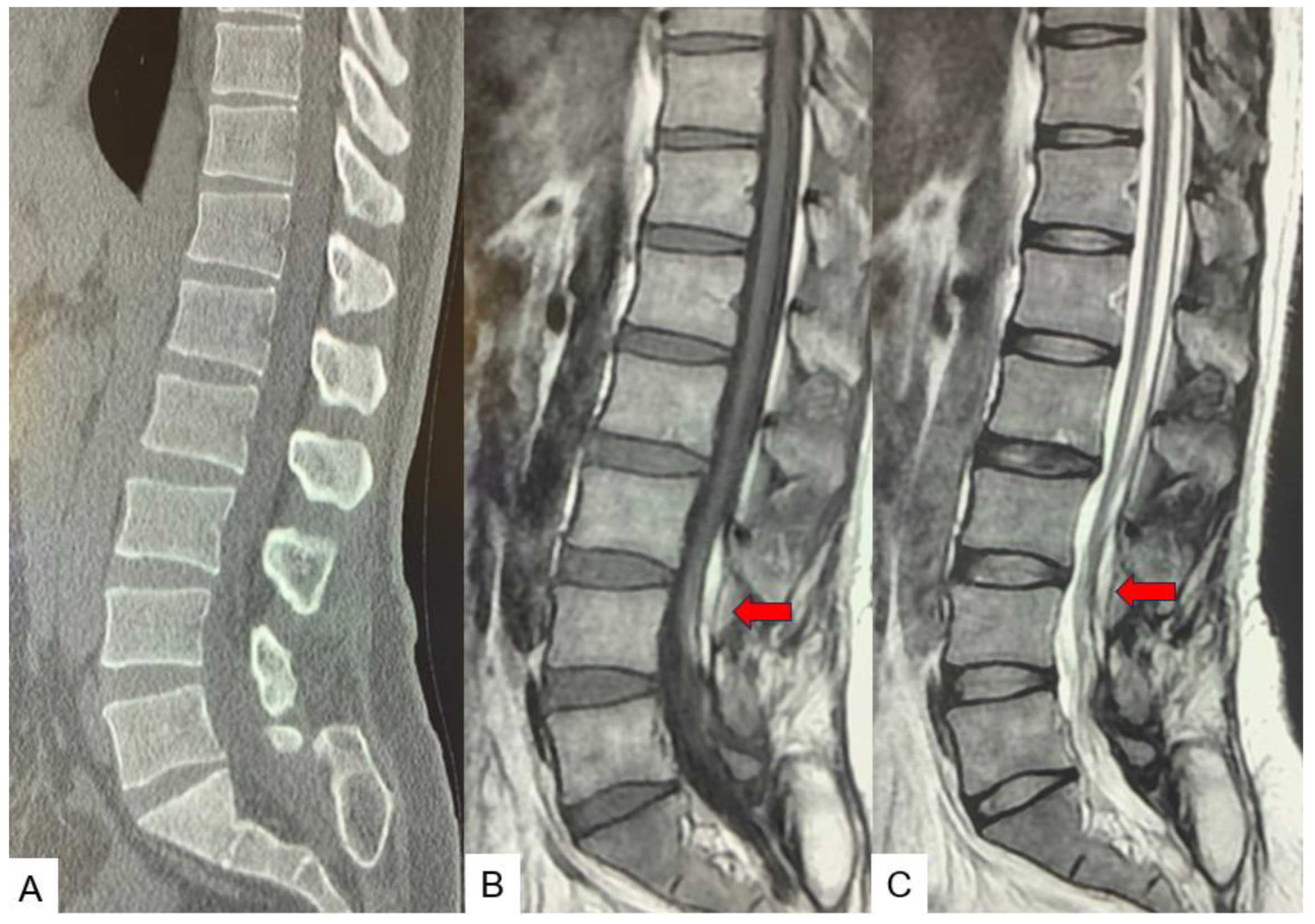
Figure 13.
Shema of conventional spinal shortening osteotomy.
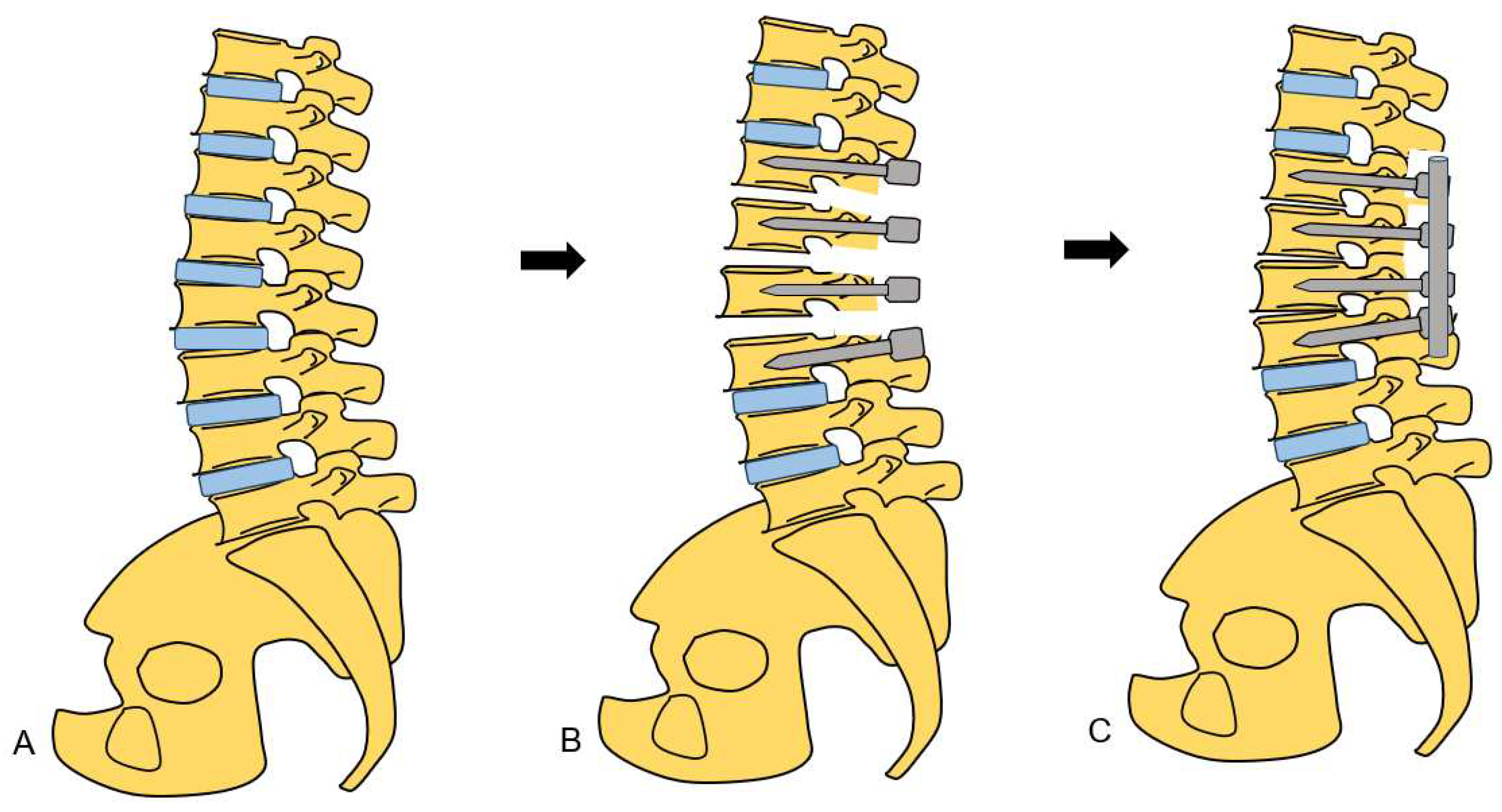
Figure 14.
Postoperative images, Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. Spinal column was shortened 20 mm.
Figure 14.
Postoperative images, Full spine standing postero-anterior radiogram, B: Full spine standing lateral radiogram, C: Lumar antero-posterior radiogram, D: Lumbar lateral radiogram. Spinal column was shortened 20 mm.
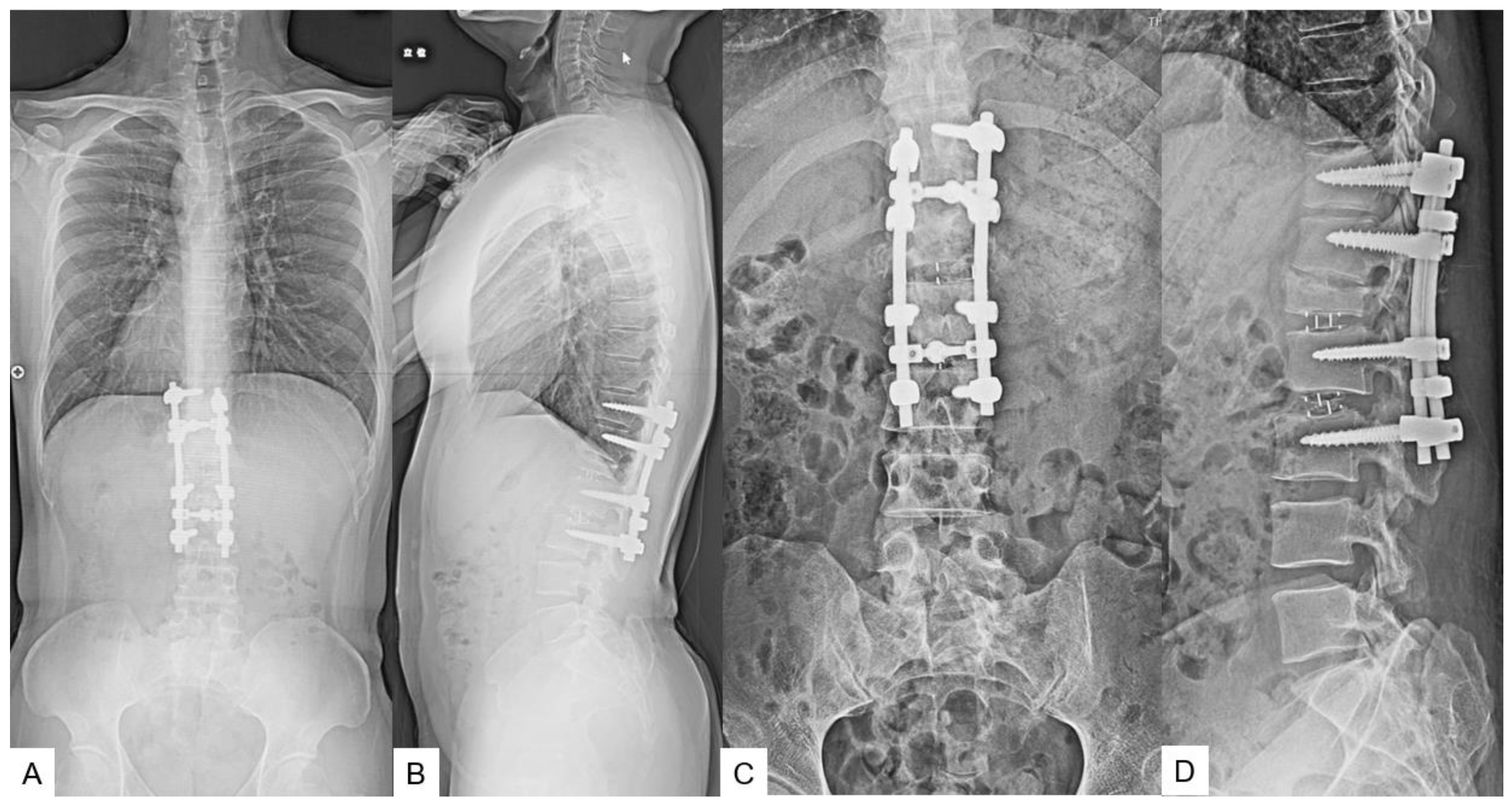
Figure 15.
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging. There was T2 high area in the spinal cord (red arrow).
Figure 15.
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging. There was T2 high area in the spinal cord (red arrow).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



