
Submitted:
21 December 2023
Posted:
22 December 2023
You are already at the latest version
Abstract
Manual handling tasks, both in daily activities and at work, require high dexterity and the ability to move objects of different shapes and sizes. However, musculoskeletal disorders that can arise due to aging, disabilities, overloading, or strenuous work can impact the natural capabilities of the hand with serious repercussions both in working and daily activities. To address this, researchers have been developing and proving the benefits of wrist exoskeleton., This paper, which is the part II of a study on wrist exoskeletons, presents and summarizes wearable wrist exoskeleton devices conceived for use in rehabilitation, assistance, and occupational fields. Exoskeletons considered within the study are those available either in a prototyping phase or on the market. They can support the human wrist by relieving pain or mitigating fatigue while allowing at least one movement. According to the requirements to be met, the majority have been designed active (80%) for higher force/torque transmission, and soft for better kinematic compliance, ergonomics, and safety (13 devices out of 24, more than 50%). Electric motors (11 devices out of 24, almost 50%) and cable transmission (9 devices out of 24, almost 40%) are the most common due to their simplicity, controllability, safety, power-to-weight ratio, and the possibility of remote actuation. As sensing technologies, position and force sensors are widely used in all devices (almost 90%). The control strategy depends mainly on the application domain: for rehabilitation, CPM (Control Passive Motion) is preferred (35% of the devices), while for assistance and occupational purposes AAN (Assistance-As-Needed) is more suitable (38% of the devices). What emerges from this analysis is that while rehabilitation and training are fields in which exoskeletons have been grown more easily and gained some user acceptance (almost 18 devices of which 4 are available on the market), relatively few devices have been designed for occupational aims (6 of which only 2 are available on the market) due to difficulties in meeting the acceptance and needs of users. In this perspective, as a result of the state-of-the-art analysis, the authors propose a conceptual idea of a portable soft wrist exoskeleton for occupational assistance.
Keywords:
wrist exoskeletons
; wearable devices
; occupational sector
; rehabilitation field
; industrialization issues
1. Introduction
Manual handling tasks such as opening a jar, lifting a weight, and manipulating objects of different shapes and sizes, both in daily activities and at work, require high hand/wrist dexterity and the appliance of forces. These actions performed for a prolonged time, or where they are violent, irregular, repetitive, and/or involve awkward postures, play a role in the growth and aggravation of musculoskeletal discomforts of arms, wrists, and hands [1]. Musculoskeletal Disorders (MSD) affect joints, bones, muscles, tendons, or ligaments. They can progress from mild to severe and can lead to episodic or chronic diseases that alter the quality of life of people by reducing mobility and dexterity in activities of daily living (ADL). They can also arise as a result of aging, disabilities, and injuries.
Work-Related Musculoskeletal Disorders (WRMSD) have been known for a long time with early literature dating back to the work of Bernardino Ramazzini, an 18th Italian physician and scientist, who is considered the father of occupational medicine [2]. His studies on workers in Padova (Italy) identified more than 50 methods for preventing harm at work and pointed out that "workers’ diseases" were attributable to the working environment, and prolonged, violent, irregular movements and postures [3,4,5].
Nowadays, as reported by the World Health Organization (WHO), approximately 1.71 billion people have MSD worldwide, most of which involve pain in the lower back and upper limbs [6]. In Italy, a report from the Italian Workers’ Compensatory Authority (INAIL) [7] confirms this noting that 51.6 % of all Italian workers suffer from back pain problems, while 46.7 % have upper limb-related problems [8].
Fortunately, exoskeletons are increasingly being shown to provide benefits to the human body by transferring loads from the most vulnerable areas, and through the effective transfer of energy between the human and the robotic system. The number of projects involving these devices has increased dramatically since the 2000s and has involved different sectors such as military, medical, and industrial [9], although many of the very first examples were for military programs such as DARPA’s “Exoskeleton for human performance augmentation”. The key early developments were also focused on static devices for rehabilitation in clinical settings to help recover functionalities of the limb or reduce pain after injuries [10,11]. However, today the growing impact of WRMSD is placing more emphasis on Occupational Exoskeletons (OEs). Crea et al. in [12] produced a roadmap for the large-scale adoption of OEs that highlights the costs and benefits of these technologies in real-world scenarios, but only in the past 12 years commercial wearable solutions have entered the market to assist workers in burdensome and repetitive tasks [11]. Although this growth has been substantial, few have focused on the wrist, despite this being considered the fourth most common site for musculoskeletal pain in the upper limb [10,11,12,13,14]. This is due to design difficulties in the one-to-one correspondence with the human body. As presented and explained in the Part I of this work [15], these devices have to meet a variety of often requirements including: the bio-mechanics and pain factors of the human joint; the application field; the kinematic compliance with the human limbs and joints; the dynamic compliance according to the forces/torques required to perform certain tasks; the stiffness of the mechanism; the ergonomics and safety of the device, all of which must combine to ensure the system’s adoption in real scenarios and its overall acceptance.
Different design structures have been explored by researchers and are still under development in the areas of rehabilitation and assistance [13,14,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33], and occupational [11,34,35,36] exoskeletons. Those structures, as shown in the part I [15], can be classified according to the stiffness, actuation type, power source, power transmission methods, sensing and control strategy. Rigid devices [13,16,17,18,31,32], mostly made of hard and stiff materials (e.g. stiff linkages and gears), are preferred for better reliability in motion control and force/torque transmission. But soft or compliant structures are also seen to have benefits when there is a demand for more comfortable, lighter, safer devices that can overcome axis mismatches [11,14,19,20,21,22,23,24,25,26,27,28,29,30,33,34,35,36,37,38]. Soft are composed of materials such as textiles, foam, rubber, or silicon, and have the advantage of being more comfortable and ergonomic, not hindering the natural movement of human joints. While compliant devices are increasingly seen as a good compromise between totally rigid or soft, as they are a system of compliant structures, cables, and springs, which are partly stiff and soft [15]. With respect to actuation type, a first and very critical distinction can be made between passive and active exoskeletons. Passive devices (which are by far the most common) are often driven by springs that store potential energy typically extracted from motion of the user [18,28,31,33,36]; while active units can use a variety of different sources of power: electrical [11,13,14,16,17,18,19,23,29,30,32,35], pneumatic [20,21,22,34,37], and thermal [24,25,26,27,38]. Electrical motors are the most preferred due to their robust controllability, good power-to-weight ratio, and price. The type of power transmission influences the rigidity of the system. Various methods have been explored involving rigid structures (such as direct drive, rigid links, or gears) [13,16,17,18,27,31,32], tendons or Bowden cables [11,14,19,23,26,29,35,38], or compliant elements (such as springs, artificial muscles, or flexible joint-less structures) [20,21,22,24,25,26,28,30,33,34,36,37]. To function correctly, providing feedback for and to the human body, all wearable devices need sensing and control paradigms, and usually adopt more than one type of sensor and control strategy. In wrist exoskeletons, the key sensing parameters are position detected by encoders, potentiometers, IMU or flex sensors, force/torque measured using load cells, pressure sensors, or force resistive sensors (FSR), and bio-signals recorded using electromyography (EMG). Controllers can be designed to exert predefined trajectories and forces/torques based on a Control Passive Motion (CPM) strategy. This is mainly used in rehabilitation protocols for passive users. Or to provide Assistance-As-Needed (AAN) control, that guarantees a higher adaptability to the user needs. Furthermore, controllers can work in an active resistance mode by adjusting the stiffness of some springs to impose forces/torques that resist the motion of the subject and improve rehabilitation training.
Although Part I has already focused on the human wrist anatomy and bio-mechanics, relevant musculoskeletal disorders, and the requirements and issues to guide the design of wrist exoskeletons. However, it does not include how these aspects can be implemented into effective robotic devices. Thus, as a continuation of Part I, this Part II is motivated by the intention to describe how different technologies and different requirements were put together to create effective wrist exoskeletons. This article reiterates that there is a very clear distinction between hand and wrist, especially from a clinical point of view [39]. Frequently diagnosed wrist injuries include carpal tunnel syndrome (CTS), ganglion cysts, sprains, tendinitis, and tenosynovitis as a result of repetitiveness and speed of the task, awkward postures, and the use of force while lifting and transporting loads, holding objects or using different working tools [15]. Thus, all the devices discussed in this article are designed to support the wrist by facilitating the execution of certain movements following the human wrist kinematics, and reduce the pressure on the bones, ligaments, and tendons of the wrist by providing assistance force. This helps lower the strain on the forearm muscles, thereby decreasing the risk of injury due to the aforementioned problems.
This Part II paper review differs from the available literature [10,12,40,41,42,43,44,45,46] through its focus on wearable and portable wrist exoskeletons designed since the 2000s and available both as prototypes and as commercial devices. With respect to the previous work (Part I), it highlights the features of each device more clearly, by analysing their mechanical design, control, and functionalities, highlighting pros and cons, and providing general suggestions on industrialising effective devices. The reported devices are grouped on the basis of the structural stiffness (rigid, soft and compliant) and field of application (rehabilitation, assistance, and occupational). The criteria for categorizing exoskeletons into rehabilitation, assistance, and occupational are mainly associated with required force/torque values depending on the aim to be addressed, as can be deduced from Part I. In rehabilitation, because of impairments, muscular spasticity, or bone weaknesses, the limb does not function properly. Therefore, the forces and torques must be low to avoid worsening of medical conditions, and movements are slow and gently controlled to restore natural functions. In the occupational field, mid-high forces and torques are usually required. The limb is fully and correctly functioning, so the device should provide additional force to support the user by reducing workload. The assistance domain may be considered as somewhat in between the rehabilitation and occupational fields. The user may come from a post-rehabilitation phase and still have a weak limb that is not fully functional as it should be. Thus, mid-low forces/torques are usually required to help the user in daily activities.
This paper seeks to identify the disparity between marketed and prototype products by examining the technical distinctions and peculiarities, determining the most suitable features for creating effective devices that meet user needs, and exploring the obstacles that can prevent their commercialization. It is organized as follows: in Section 2 there is the explanation and schematization of the materials and data selection protocol adopted. In Section 3 and Section 4 there are detailed descriptions of wearable and portable wrist devices available, respectively, in a prototyping phase and in the market, and conceived for rehabilitation, assistance, or occupational purposes. As a result of the state-of-the-art analysis, in Section 5 the authors propose a conceptual idea of a novel portable soft wrist exoskeleton for occupational assistance. Finally, Section 6 summarises the most significant findings of the review paper and future trends of wrist exoskeletons. To simplify the gathering of information by the reader, a summary table is proposed in Appendix 7 (Table 1) reporting all devices took into account and their characteristics. All acronyms are listed and defined after Appendix in Abbreviations.
2. Materials and Methods
The methodological approach behind this review paper consists in searching on the market and in several databases (i.e. Google Scholar, MDPI, Scopus, Frontiers, Elsevier, ResearchGate, IEEE/ASME, ScienceDirect, Sage, Wiley and Taylor&Francis), looking for all technologies explored and implemented since 2000’s about wrist exoskeletons.
The main keywords for conducting the research were “Wrist exoskeletons”, designed to be “Wearable” and “Portable”, for “Rehabilitation”, "Assistance", or "Occupational" purposes. To ensure the results best reflects the goals of the study a set of specific inclusion and exclusion criteria were implemented to refine the search domain.
Inclusion criteria consist of:
- Upper limb exoskeletons which include the wrist in their design;
- Devices able to relieve pain or mitigate fatigue by supporting at least one wrist movement;
- Devices intended for rehabilitation, assistance and occupational purposes;
- Portable devices;
- All studies must be accessible by the authors in English.
Exclusion criteria consist of:
- Prosthesis or exoskeletons which do not allow free wrist movements;
- Military devices;
- Fixed/grounded devices;
- Studies in other languages or with insufficient information, which made the analysis unclear.
3. Research and Pre-commercial Devices
As with all developmental cycles, there is with exoskeletons an early phase of prototype design for research and pre-commercial testing. While the end goals for these devices may fully align with eventual commercial systems, they are often more complex in terms of hardware and software, may have unrealistic costs or may not fully conform to strict commercial mandatory regulations. Nonetheless these devices often form the basis for designs that will eventually become industry standards, and a full and comprehensive study and analysis of these systems is vital in any detailed review. The section provides a detailed study of wearable and portable wrist exoskeleton prototypes with, where appropriate, an assessment of the integrated actuation, electronics, control system and batteries, the ease of donning and doffing and the potential application scenarios. All devices are shown in Figure 2 and grouped according to structural rigidity criteria.
Based on the requirements proposed in [15], the schematic shown in Figure 3 provides relevant information about research and pre-commercial wrist exoskeletons.
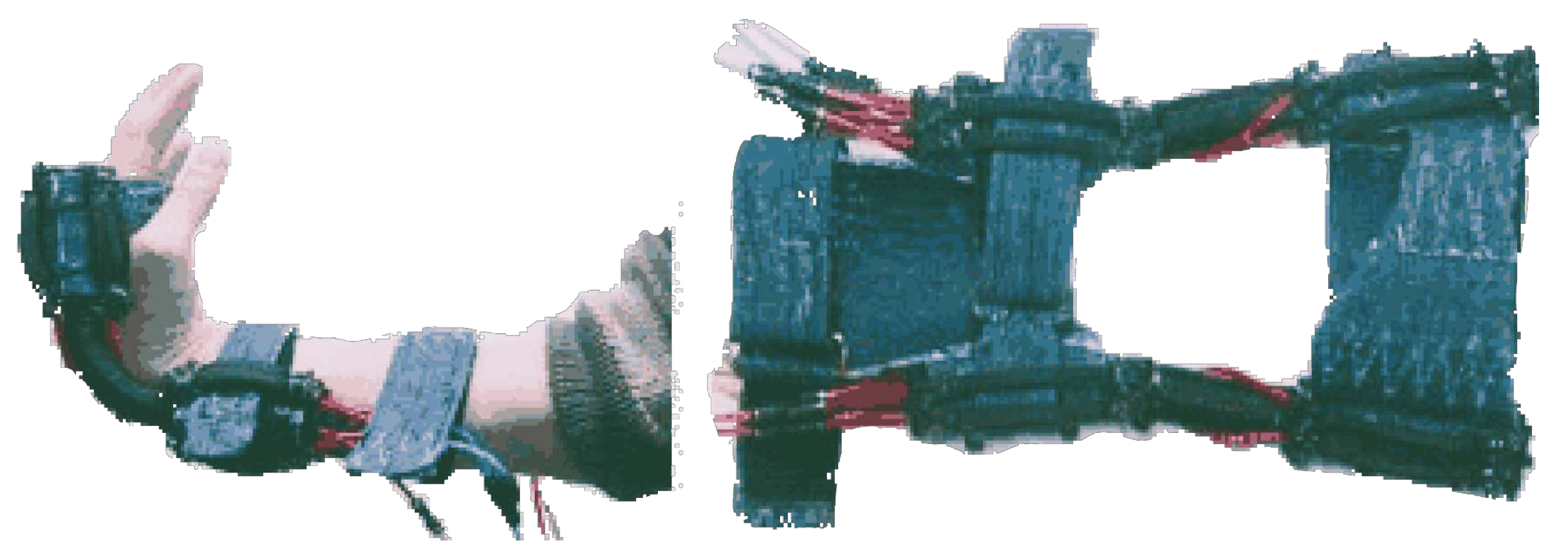
Figure 2.
All wearable exoskeleton prototypes for wrist assistance. Devices are grouped by stiffness criteria in: rigid (a-c), soft (d-p) and compliant (q-t). From from top left to bottom right it is possible to find: a) Portable Wrist Exoskeleton (PWE) designed by [47]; b) eWrist designed by [13,17]; c) wrist exoskeleton designed by [18]; d) exosuit designed by [11] and already reported in [15]; e) Exo-Wrist designed by [19]; f) soft orthosis designed by [20]; g) Active Support Splint for the wrist (ASSIST) designed by [21]; h) Soft Origami-patterned Actuator (SOA)-based wrist exoskeleton designed by [22]; i) a soft wrist exoskeleton designed by [23]; l) a pneumatic soft wrist exoskeleton (EXOWRIST) designed by [37]; m) a soft robotic device designed by [34]; n) Soft Wrist Assist (SWA) designed by [24,25]; o) Wearable wrist and forearm exoskeleton developed by [26]; p) Advanced Service Robot (ASR) a Shape Memory Alloy (SMA)-based hand exoskeleton designed by [38]; q) SMA-based wrist exoskeleton designed by [27]; r) SCRIPT Passive wirst Orthosis (SCRIPT-SPO) designed by [28] already reported in [15]; s) a hand and wrist exoskeleton designed by [14,29]; t) a low profile wrist exoskeleton designed by [30].
Figure 2.
All wearable exoskeleton prototypes for wrist assistance. Devices are grouped by stiffness criteria in: rigid (a-c), soft (d-p) and compliant (q-t). From from top left to bottom right it is possible to find: a) Portable Wrist Exoskeleton (PWE) designed by [47]; b) eWrist designed by [13,17]; c) wrist exoskeleton designed by [18]; d) exosuit designed by [11] and already reported in [15]; e) Exo-Wrist designed by [19]; f) soft orthosis designed by [20]; g) Active Support Splint for the wrist (ASSIST) designed by [21]; h) Soft Origami-patterned Actuator (SOA)-based wrist exoskeleton designed by [22]; i) a soft wrist exoskeleton designed by [23]; l) a pneumatic soft wrist exoskeleton (EXOWRIST) designed by [37]; m) a soft robotic device designed by [34]; n) Soft Wrist Assist (SWA) designed by [24,25]; o) Wearable wrist and forearm exoskeleton developed by [26]; p) Advanced Service Robot (ASR) a Shape Memory Alloy (SMA)-based hand exoskeleton designed by [38]; q) SMA-based wrist exoskeleton designed by [27]; r) SCRIPT Passive wirst Orthosis (SCRIPT-SPO) designed by [28] already reported in [15]; s) a hand and wrist exoskeleton designed by [14,29]; t) a low profile wrist exoskeleton designed by [30].
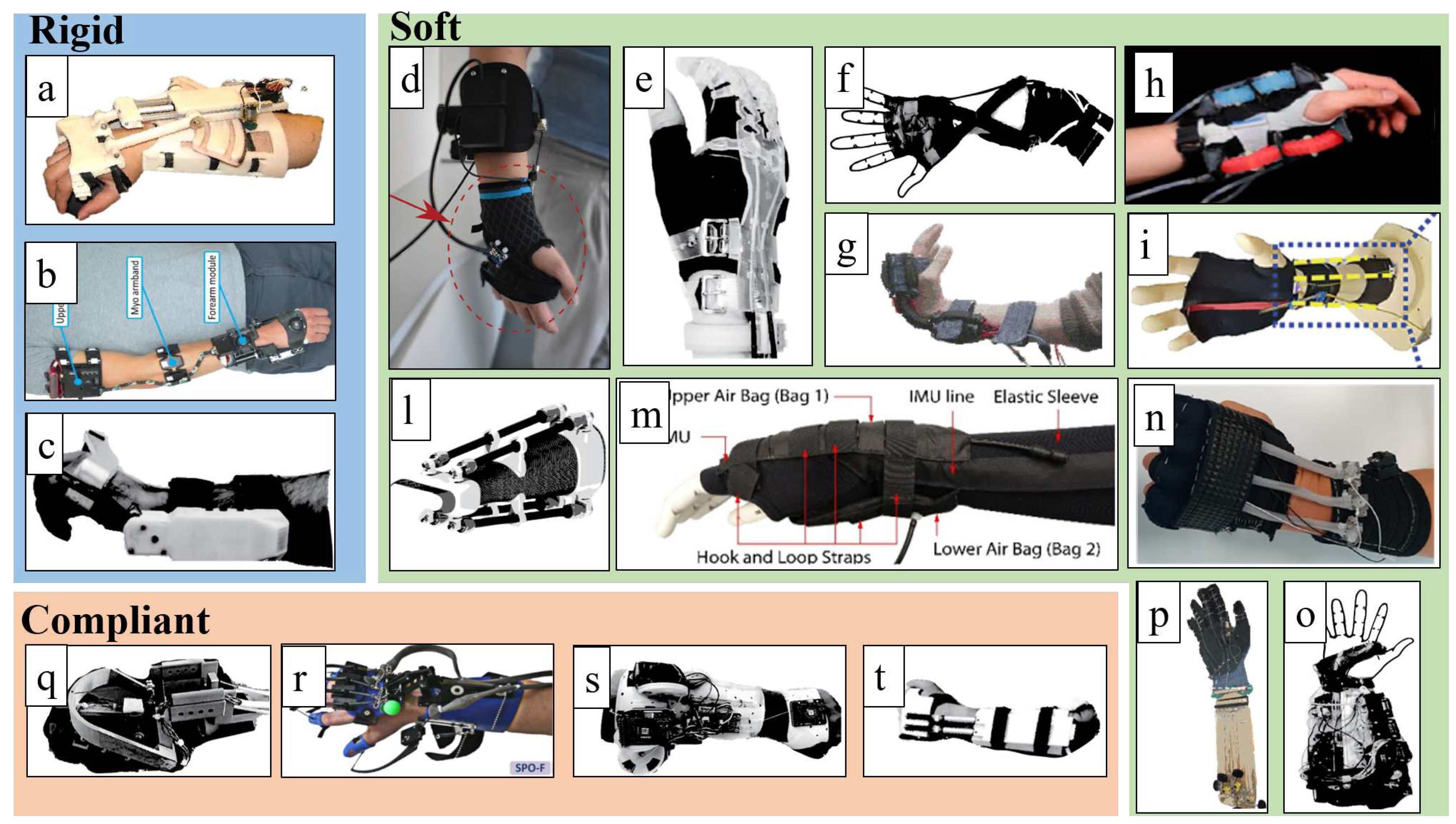
3.1. Rigid devices
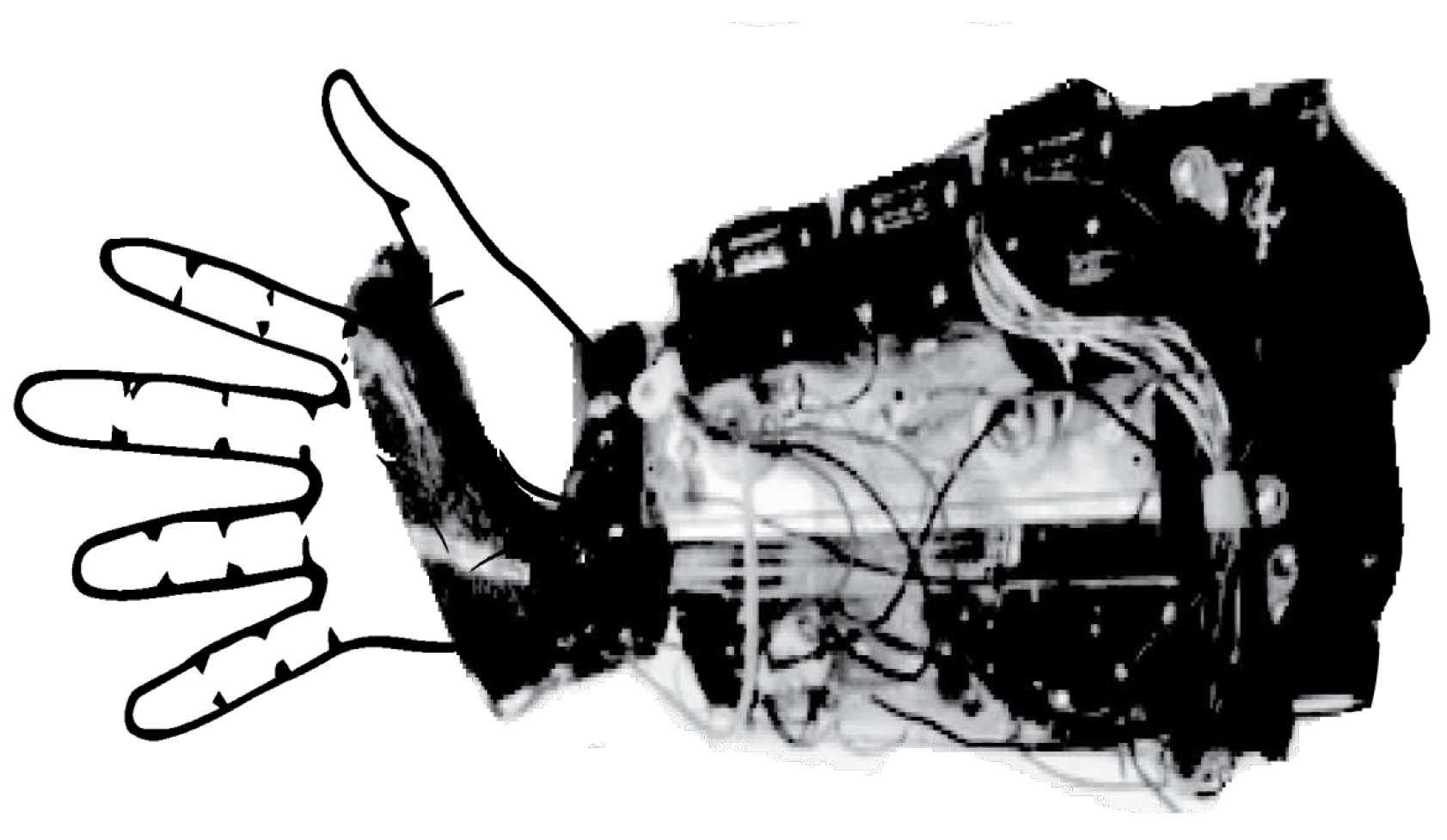
3.1.1. Development of a Portable Wrist Exoskeleton (PWE)
Xiao et al. in [16,47] investigated the design and control of a 2 DoF (flexion/extension and radial/ulnar deviation) portable, active and rigid wrist exoskeleton conceived for post-stroke rehabilitation at home, or used by workers to provide assistance in industrial settings.
Figure 4.
An older version of the Portable Wrist Exoskeleton (PWE) [47].
Figure 4.
An older version of the Portable Wrist Exoskeleton (PWE) [47].
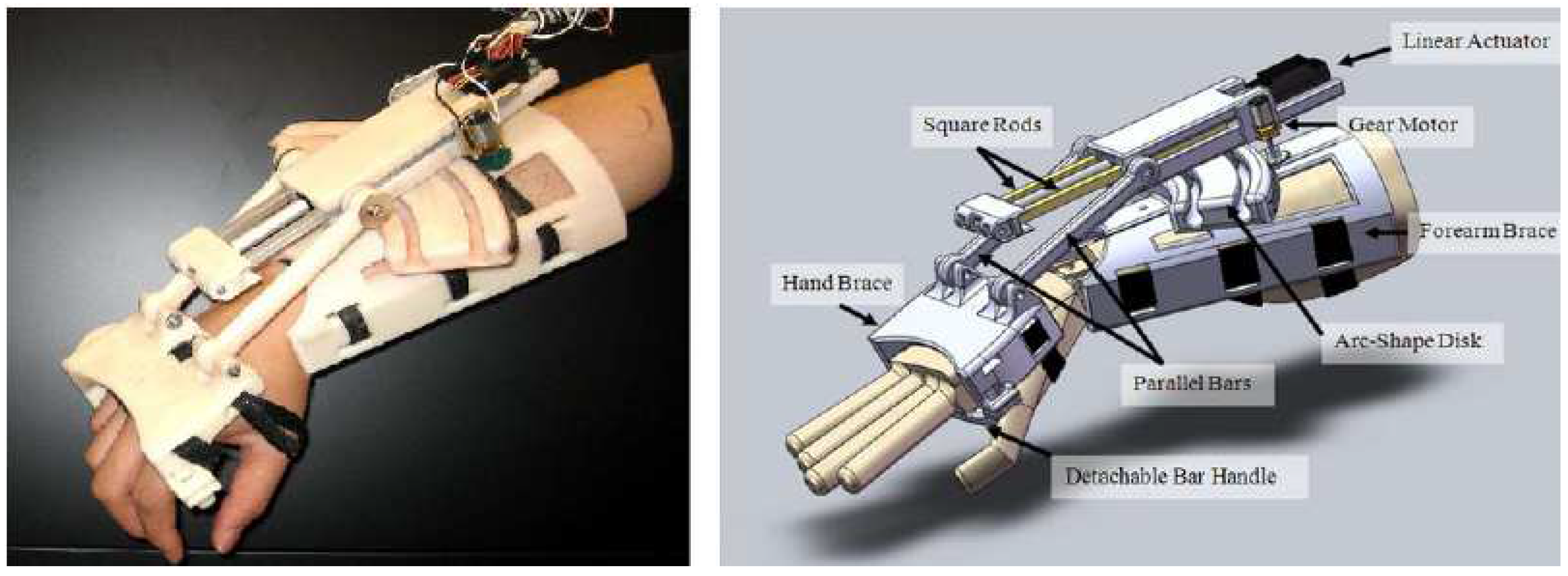
The Portable Wrist Exoskeleton (PWE) has a rigid kinematic chain made of ABS plastic and weighs 360 g. To avoid harm to the user, foam pads are inserted between the rigid parts and skin. To increase safety and prevent possible injuries, mechanical stoppers limit the RoM to ° flexion/extension, and ° radial/ulnar deviation. The power is transferred from the actuator (Pololu 298:1 micro DC geared motor), placed on the forearm brace, to the hand brace through gears and links. The maximum torque generated are 2.3 Nm for flexion/extension, and 2.5 Nm for ulnar/radial deviation, which are enough for rehabilitation application, yet it may not be adequate for industrial use.
Two different control modalities have been implemented: position control for passive repetitive pre-programmed movements, suitable for rehabilitation application; and a torque control designed for torque amplification applications such as for workers’ assistance. As control strategy, they investigated the feasibility of surface electromyography (sEMG) signal classification through neural network (NN) and support vector machine (SVM). The experiment consisted of measuring the sEMG amplitude and torque exerted by the main wrist muscles of a healthy subject, who gradually applied maximum voluntary contraction in all wrist directions with the forearm and hand placed on a rig. The SVM predicted and followed the wrist movement in real time with the greatest accuracy (up to 80.44%), exerting different levels of torque depending on the wrist position. This study suggests that machine learning techniques for motion prediction could be beneficial when performing highly dynamic tasks. However, the requirement for sEMG signals makes it hard to apply in industrial settings, where workers must wear them in contact with the skin.
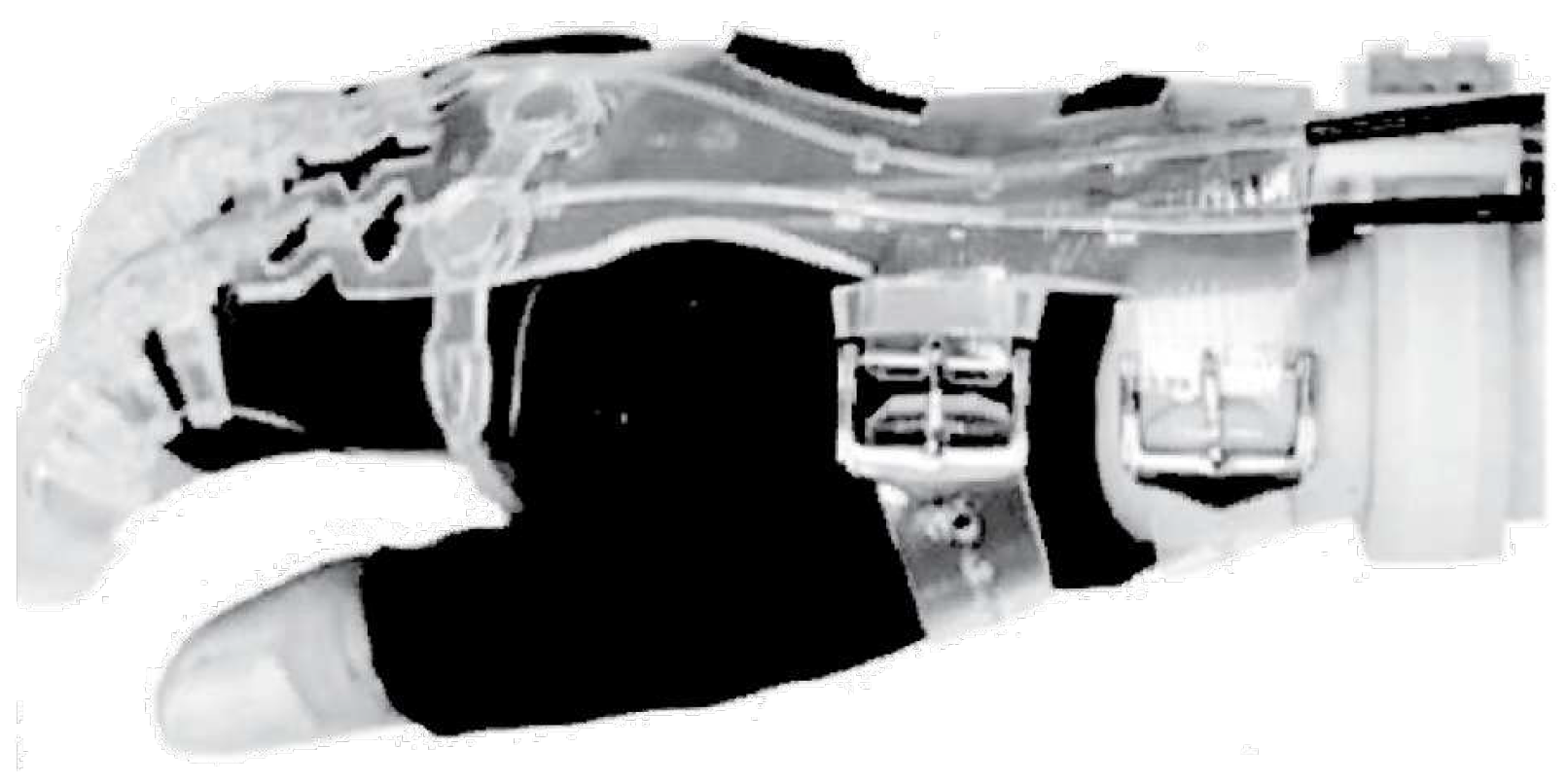
3.1.2. The eWrist - A Wearable Wrist Exoskeleton
Lambelet et al. in [13,17] have presented eWrist, a portable and rigid 1-DoF wrist exoskeleton to support flexion/extension in rehabilitation and training. The device, shown in Figure 5, aims at enhancing wrist muscles activity in ADLs by measuring residual sEMG amplitude of stroke patients through a Myo armband: a commercially available sEMG device. The whole device consists of a kinematic chain made of rigid and soft 3D printed parts, and weighs 556 g, including the battery (80 g) and the Myo armband [17]. A Boa Closure is used as tightening system and allows quick and easy one-handed placement. The actuation system incorporates a 12V DC brushless rotary motor (Maxon EC 16) with a total reduction ratio of 475:1, making it difficult to back-drive. Therefore, mechanical transparency is obtained through active control. A two-channel Hall effect sensor, integrated within the motor, determines joint angular velocity and position. A load cell, mounted between the bevel gear and the hand fixation, determines the torque. The battery can power the device for about 125 min in normal use.
A real-time PD-controller, integrated in a Raspberry Pi Zero, implements an Assistance-As-Needed (AAN) support strategy. This adjusts position and torque output based on several inputs: raw sEMG data from the Myo, force from the load cell, and the angular velocity. Two different dynamic behaviours, for different rehabilitation settings, are available: transparent or resistive. In transparency mode users can move freely and rapidly with low interaction torques (up to 0.34 Nm); in resistive modality, movements are constrained by higher torque values (up to 1.59 Nm).
The device has been characterized based on standardized metrics for rehabilitation devices and, subsequently, tested with healthy and stroke participants. Fifteen healthy subjects (7 females and 8 males, mean age: 26 ±3.4) and two stroke survivors were recruited (both males, age: 68 and 52 years). Tests performed on healthy subjects showed that it can provide: a RoM of 154°, a maximum output torque of 3.7 Nm, a maximum output velocity close to 520°/s, and an average set-up time of 37.3 s. Observations from questionnaires showed that the eWrist was positively received: it helped impaired subjects achieve a RoM comparable to that of healthy subjects; all participants were able to use it independently; the fixation systems were evaluated as being efficient, secure, and easy to handle. However, some limitations still remain in terms of aesthetics, physical proportions and weight distribution: some subjects felt discomfort due to a wrong size, alignment mismatch between mechanical and biological joints, and skin pain caused by fixations.
3.1.3. Robotic Orthosis for Wrist Assistance
Sangha et al. in [18] have presented a wearable 1 DoF robotic orthosis to assist wrist flexion and extension in rehabilitation.
The device, shown in Figure 6, weighs 330 g and consists of a rigid aluminium kinematic chain, secured at the palm and forearm by C-shaped clamps and Velcro straps, and 3D printed ABS plastics which cover all the electronics. The actuator is a DC rotary motor with a custom gearbox with a high reduction ratio (1700:1). It provides a nominal torque of 1.12 Nm, and a stall torque of 8 Nm.
The device can operate in three different modes according to the patient’s impairment: passive, active resistive, and active assistive. Passive mode assists the wrist movements based on predefined parameters and the patient’s RoM. It is useful for those with muscle weaknesses. Active modes assist wrist movements to augment brain plasticity and decrease muscles spasticity. Assistance is provided after detecting muscular effort with 8 force sensitive resistors (FSR) to record force-myography (FMG) signals from the forearm. A neural network (NN) is implemented in Arduino software to process the FMG signals and send the control command to the motor.
Tested on a healthy volunteer, it has: a RoM from 0° (full flexion) to 120° (full extension), a nominal torque of 1.12 Nm, and a battery life of 150 min. Despite its interesting performances and features such as working modalities, compactness, lightweight, and cost, further investigations are required to test its efficacy in real scenarios with more subjects (both healthy and impaired).
3.2. Soft devices
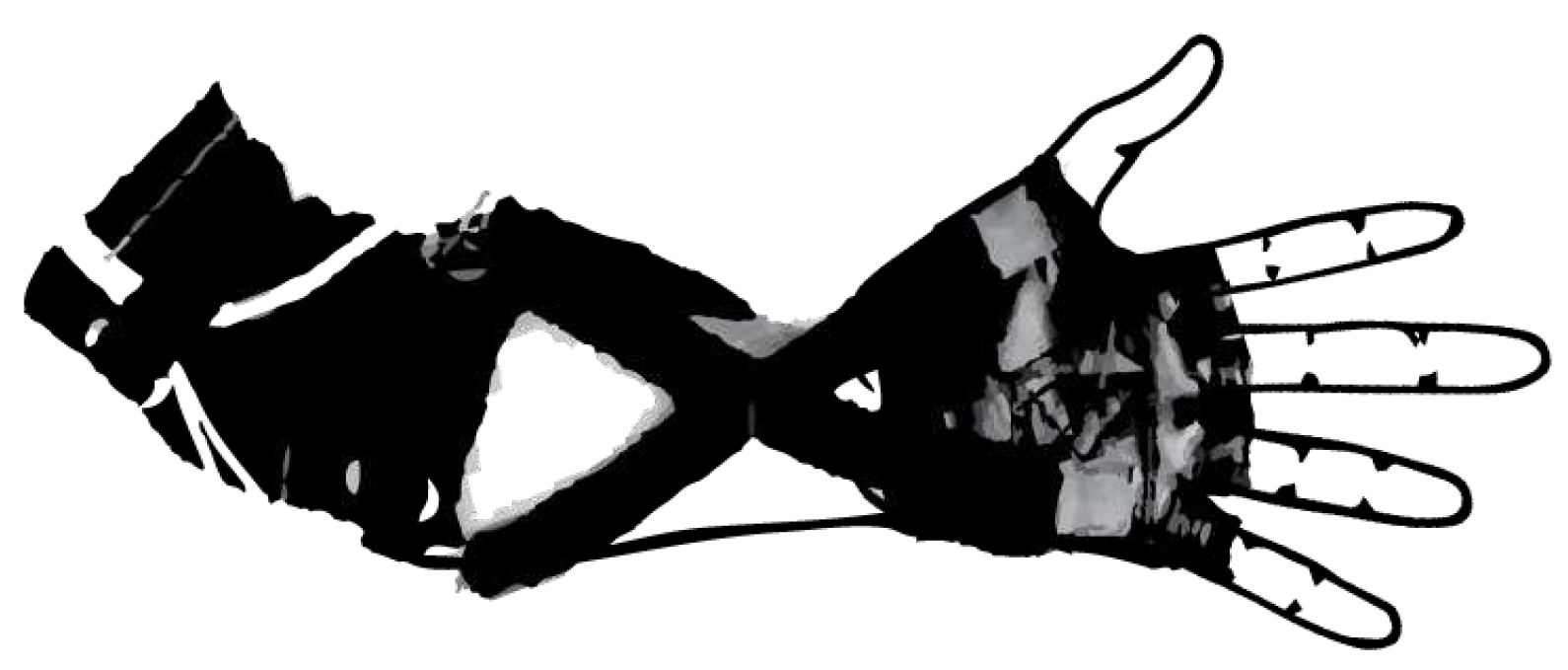
3.2.1. Soft Wrist Exosuit
Chiaradia et al. [11] have developed a novel 1-DoF wrist exosuit for assistance at work. It is made up of a soft wrist orthosis and two 3D printed ABS supports (one for the back and one for the palm), which help to distribute pressure on large areas, bear cable tension and sensors. The wearable parts, shown in Figure 7, weigh 300 g.
The system is actuated remotely using a bowden cable transmission and a Kollmorgen motor (AKM23F) with an Apex Dynamics planetary gear drive (PG II 040), and a gear ratio of 10:1. This helps reduce the weight on the human joint and the metabolic impact. A load cell measures cable tension, and 9 DoF inertial measurement units (IMUs) estimate wrist flexion: one on the back of the hand and one on the forearm. The control strategy is based on admittance control for transparency and gravity compensation. The torque exerted on the wrist is compensated by evaluating an estimated torque, knowing the wrist angle and the cable force. The addition of a PID controller on the angular velocity gives the assistance faster by capturing the user motion intention.
The device was tested on four healthy participants (all males, aged 28.0 ±4.0) under both isometric and dynamic conditions. In the isometric test, the participants were asked to keep their forearm and hand parallel to the ground for 3 min holding 1.5 kg weight. While, dynamic test required participant to track a Minimum Jerk Trajectory (MJT) that involves a wrist flexion, from 0° to 60° at two different speeds (35 and 70°/s), with and without exosuit assistance, while performing 15 repetitions with a 1.5 kg of weight. Overall, the device enhances the wrist movement in a range of 150° (70° for flexion and 80° for extension) and can provide 3 Nm torque, sufficient to hold 3.0 kg. However, it adopts an external heavy DC motor which makes it difficult to wear, and the reduction in muscle activation seems lower than with other devices.
Despite its limitations, this prototype is worth attention due to its characteristics such as: industrial applications, softness because of the tendon-driven actuation, comfort and customization as the rigid parts are designed following a 3D scan of a human hand. Future developments may include full wearable actuation and control systems, improving the transmission efficiency with a control strategy for friction management and the comfort.
3.2.2. ExoWrist - a soft tendon-driven wrist wearable robot for dart-throwing motion
Choi et al. in [19] presented a new soft wearable wrist robot called ExoWrist. The device is active and conceived to restore wrist functionalities of weakened upper limbs after injuries by focusing on the Dart Throwing Motion (DTM), the most natural wrist movement [48,49,50,51]. It is expected to be used both in or out-of-clinics. The ExoWrist consists of a golf glove, a forearm active anchor and a wrist armlet. On the back of the glove, tendons are placed to transmit forces. The forearm anchoring consists of a truncated cone shape made of soft and flexible materials. This compresses the forearm only when assistance is needed to reduce force losses through friction. The wrist armlet is a silicon-based 3D printed part and is customisable based on: wrist width, wrist height, and the DTM orientation plane. The use of soft materials and cables makes the whole device comfortable with an overall weight of 1 kg. The DTM plane and wrist kinematics of each individual have been measured by using 3D motion-capture sensors (Vicon) to define the tendons path to correctly apply assistive force.
Figure 8.
Soft tendon driven wearable wrist robot for dart-throwing motion designed and developed by [19]. Image adapted from [19].
The robot has been assessed on three healthy subjects through three experiments, evaluating respectively: the efficacy of the anchoring system, the motion tracking performance, and the ability not to hinder other movements. Participants sat on chairs with their elbows extended, forearms pronated, and wrists in a neutral position. For the first experiment each participant was asked to wear the anchor and place their forearm on the setup, which restricts forearm movement. Then the maximum displacement of the forearm anchor was measured at different anchoring wire tensions. For the motion tracking control, the were instructed not to exert any volitional effort on their wrists, while the robot pulled them. The last experiment was the comparison of the average maximum ROM of the finger joints (by using a goniometer) and the grasp force before and after the actuation of the robot. The results showed that without the active anchor the robot could not provide proper assistance. When the anchoring point is activated and properly tightened, the robot can assist more than 0.5 Nm, otherwise it cannot generate more than 0.2 Nm, less than required for ADLs (0.35 Nm). The robot can extend the wrist along the DTM plane for more than 50°, more than is needed for constraint-induced movement therapy (CIMT, 0°-20°), and it does not also affect movements at elbow, shoulder and fingers.
3.2.3. A soft robotic orthosis for wrist rehabilitation
Bartlett et al. in [20] have proposed a home wrist rehabilitation soft device designed for patients suffering from hemiparesis after stroke. It is pneumatically actuated, portable, and soft, and weighs 2.26 kg. It consists of a glove, an elbow sleeve and a Boa ratchet tensioning mechanism, which facilitates donning and doffing with one hand and adaptation to different arm lengths. The actuation mechanism consists of pneumatic artificial muscles (McKibben actuators) anchored on both the palm and back of the hand. Their size is crucial: a tube diameter of 1/2 in. (approx. 12.5 mm) can exert a contractile force close to 120 N, at a pressure of 30 PSI (approx. 200 kPa), which is enough for rehabilitation. Their anchoring points determine the initial actuator length and thus affect contraction length, RoM and force direction.
The device works on agonist-antagonist principle: a single movement can be generated by activating a pair of actuators (e.g. the two in the palm for flexion, the two in the back for extension, etc.). The air pressure of each actuator is constantly monitored and modulated by a controller, which reads the status of pressure sensors and gives the input signal to a pump and relevant valves. The device is tested on a mannequin hand and on a healthy subject for assessment. The user was instructed to fully relax his wrist while the robot is actuated. Results show, it can support all wrist DoFs by providing assistance over a range of 91° in flexion/extension, 78° in pronation/supination, and 32° in radial/ulnar deviation. Presented to a group of stroke patients, the participants gave positive feedback for its use in therapy.
3.2.4. Active Support Splint driven by Pneumatic Soft Actuator (ASSIST)
Sasaki et al. [21] have developed ASSIST, an active soft wrist splint to assist elderly or people in need of care, making them more independent.
Two different types of ASSIST have been created: one for assistance in the whole RoM (type I), and the other for increasing muscular endurance (type II). They differ in the McKibben structure of artificial muscle actuators. Both devices consist of plastic interfaces, on the palm and back, to which two rotary soft pneumatic actuators are attached. Reinforcements at the ends allow the actuators to bend circumferentially, providing enough bending angle and torque for wrist assistance. The devices weigh almost 390 g. ASSIST is controlled by measuring the wrist angle with flex sensors and keeping the inner pressure constant. At 400 kPa pressure, type II provides almost 80° rotation and 1 Nm of torque; while type I allows the same bending angle with a lower torque (0.25 Nm). In contrast, the torque of type II decreases faster as the bending angle increases.
These devices were assessed on 5 male subjects by measuring. In these experiment, human wrist was bended by ASSIST without any human muscular effort. For evaluating the assist effectiveness, the bending angle at human wrist, and the amplitude of sEMG signals at the flexor carpi ulnaris were measured. Results showed their suitability in correctly bending the wrist, and reducing muscular effort while lifting 3 kg. Although the results are not statistically significant, these devices have promising capabilities also for industrial applications. However, there are drawbacks and further analysis and more data are needed to verify the benefits of prolonged use, make it fully wearable with a pressure tank and compressor above 400 kPa, assess reliability and control of the actuators’ behaviour.
3.2.5. A soft robotic wrist brace with origami actuators
Liu S. et al. in [22] designed a low-profile, active and soft robotic (SR) wrist brace, that is pneumatically driven and has 2 DoF (flexion/extension and radial/ulnar deviation). It consists of eight modular soft origami-patterned actuators (SOAs), a commercial wrist brace, and rigid anchors made of fabric to fix the actuators and transmit forces, as shown in Figure 11. Due to the inherent compliance of its materials, the SR brace enables safe interaction, has light-weight, compactness, comfort and adapts to various wrist sizes. The parts worn on the wrist weighs 214 g (each SOA weighs approximately 1.9 g), but the overall device weighs almost 1.76 kg, including the actuation system and batteries.
The actuation system includes four identical two-SOAs units and two diaphragm air pumps. The device works by alternately contracting and expanding the actuators (e.g. during flexion actuators on the dorsal side of the wrist elongate while those on the palmar contract). Their axial deformation exhibited when pressurized is converted into large bending due to anchoring constrain. The control architecture consists of a high-level and a low-level control. The high-level controller estimates the wrist position depending on the pressure feedback from each actuator, and compares it with the desired motion. Thus, a pressure command is sent to the low-level controller to regulate the SOA pressure and elongation.
The device assessment was based on the RoM, output force, wearing position adaptivity, and performance. The RoM was measured without and with external loads (100, 200, 300 g). The maximum values, at pressure, were 30° in extension, 31° in flexion, 33° in radial deviation, and 22° in ulnar deviation. They decrease as the load increases. The force exerted achieved up to 7.5 N in flexion/extension, and 6 N in radial/ulnar deviation. The torque reached up to 0.76 Nm and met the functional requirement for rehabilitation therapy. The performance, assessed with IMU sensor, showed that the device consistently followed the planned flexion/extension, while it had less stability in ulnar/radial direction. Although the results are promising and comparable with existing devices, future work will aim to optimize the design, improve compactness and portability, validate the effectiveness and side effects of specific rehabilitation therapies.
3.2.6. Bioinspired Musculoskeletal Model-based Soft Wrist Exoskeleton
Ning Li et al. in [23] describe a novel soft wrist exoskeleton for stroke rehabilitation and ADLs, shown in Figure 12. They used commercially available components (motors, commercial body protectors, sensors, power supply) and investigated the distribution of muscle tension lines to identify the most efficacy path along which artificial tendons should be placed to correctly move the wrist. They analysed the kinematics of wrist muscles and simplified this to four main muscles: Extensor Carpi Radialis Longus (ECRL), Extensor Carpi Ulnaris (ECU), Flexor Carpi Radialis (FCR), and Flexor Carpi Ulnaris (FCU), which were arranged as to form a quadrilateral around the wrist. This design guarantees a more natural interaction with the user. To compare the exoskeleton movements with a real wrist, a VICON tracking system was used to capture wrist trajectories of healthy subjects and those produced by the exoskeleton mounted on a hand mannequin.
The assessment was done in simulation (OpenSim software), and on healthy and impaired subjects. One healthy volunteer and three stroke (hemorrhagic) survivors (3 males, age range 32-57 years) were enrolled for clinical trials. First of all, tests were done on a healthy subject as to have a baseline. The wrist motions were captured by VICON, and sEMG signals at forearm were measured when lifting 5 kg weight during wrist flexion with and without exoskeleton assistance. Then, tests on stroke patients were carried out to verify the clinical assistance effects. Overall, the device was able to cover the daily RoM requirements with a flexion/extension range of 115°, and a radial/ulnar deviation range of 70°. When tested on stroke patients, the device demonstrated an average 90.3% ability to recover healthy wrist motion in ADLs (e.g. drinking action was selected to evaluate the assistance effect of the exoskeleton). Moreover, by measuring the forearm sEMG signals from a healthy subject during 5 kg lift, the exo exhibited more than 40% reduction in muscle activation. The overall results are consistent both in simulation and real scenarios, and pave the way for new and even better performing soft wrist exoskeletons. Although it is designed for rehabilitation and daily life assistance, the halving of muscle effort in lifting 5 kg is a great achievement and similar solutions could also be adopted in industry.
3.2.7. EXOWRIST: a wrist exoskeleton actuated by pneumatic muscle actuators
Andrikopoulos et al. in [37] developed a novel soft 2-DoF robotic wrist exoskeleton for rehabilitation, powered by pneumatic muscle actuators (Mckibben actuators). The device, shown in Figure 13, consists of wearable elastic neoprene-based glove. It adopts four Pneumatic Muscle Actuators (PMAs), symmetrically distributed around the forearm, to function antagonistically and generate wrist flexion/extension and radial/ulnar deviation. PMA is like a tube, fixed to the glove with plastic supports, and it is characterized by a decrease in length when pressurized. The design uses few hard materials and enhances lightness, comfort and safety, with a total weight of approximately 430 g.
EXOWRIST’s performance have been evaluated on a healthy, passive male volunteer, with no medical history of hand and arm, to prove its motion capabilities and its safety. The motion test consists on the execution of wrist flexion-extension and ulnar-radial deviation movements, with the patient’s arm lying parallel to the floor. To achieve the maximum RoM, PMA should first be inflated to half its maximum stroke. Measured with an IMU placed on the back of the hand, the device can reach ° in both flexion/extension and radial/ulnar deviation in less than 1 s. The pressure range is 0 to 8 bar, with a maximum operating pressure reaching 630 N of delivered force. The control strategy adopts an Advanced Nonlinear PID (ANPID) algorithm which allows tracking of pre-defined sinusoidal motions with smooth, fast and accurate PMA responses. The safety was assessed by placing FSR force sensors between PMA connections and the human’s skin to measure the contact forces, as they are the main sources of torque. The shear forces generated remain low, not exceeding 2.2 N, and the respective generated torques remains under 0.055 Nm. The results prove that the EXOWRIST has potential in rehabilitation scenarios. However, there is a need for further improvements especially in the actuation system to make the device fully wearable, portable and safe, since high levels of pressure are required and must be supplied from a compressor or high pressure tank.
3.2.8. Carpal Tunnel Syndrome Soft Relief Device
Zhu et al. in [34] have proposed a novel device to alleviate Carpal Tunnel Syndrome (CTS) strains and pain by actively adjusting the wrist angle when operating in awkward postures for prolonged time, e.g. while typing on a keyboard. The device, shown in Figure 14, consists of an elastic fabric sleeve that can be worn like a glove, and two thermoplastic (TPU) airbag actuators (eight-flanged bladders) sewn onto it. They are located at the lower and top part of the sleeve to extend and flex the wrist respectively by dynamically pressurizing and depressurizing them.
The performances were assessed on a hand mannequin by lifting the hand, with an external load of 200 g, to a height similar to that of a keyboard (1.9 cm). The device was able to lift the hand above 2 cm under a pressure of 31 kPa and from 0° to around 65° in 9 s under a maximum pressure of 62 kPa. Although this device has interesting characteristics such as soft actuation, breathable materials, safety, easy and compact design, it needs further development to the design, control and experimental evaluation with subjects. CTS problems are highly topical and need special attention for the well-being of workers.
3.2.9. Wrist Assisting Soft Wearable Robot with integrated SMA Muscle
Jeong et al. in [24,25] proposed a novel shape memory alloy (SMA)-based wearable robot that assists 2-DoF (flexion/extension and radial/ulnar deviation) wrist motions in performing ADLs. SMA actuators are metallic alloy that deform when heated above their transformation temperature and reduce their length between 3-5%, depending on the type and shape of the alloy chosen. SMA has potential properties as artificial muscles since it can produce high forces and can be fairly rapidly actuated via Joule heating. Furthermore, if shaped as a coil spring, it can produce forces up to 10 N, a contraction ratio of 40% and strains over 200%, achieving performances higher that than of SMA shaped as wires [27].
The device, shown in Figure 15, named Soft Wrist Assist (SWA), consists of: a finger-less glove, a forearm Velcro strap, and an elbow anchoring Velcro strap to adapt to different users’ sizes, prevent and improve dislocation and slip [24]. Moreover, to transmit forces properly actuators are fixed on the glove with non-stretchable fabric. Five muscle-like actuators are attached at various positions: three to the back of the hand, and two on the palm. They are designed as coil springs, integrated into an active and stretchable coolant vessel, filled with mineral oil, for improved heating and cooling response. The wearable parts weigh 300 g, while the total mass, including the pump and radiator, is around 1.92 kg.
The device can produce combined wrist movements such as radial-extension and ulnar-flexion by selectively activating the actuators. First, the overall RoM, torque, mechanical performances, wearability and set-up time have been assessed on a hand mannequinn, and then on five healthy subjects (three males and two females). The ROM was measured through absolute magnetic encoders were attached to the wrist joint. The average RoM was 38°, 50°, 34°, and 35° respectively for flexion, extension, radial, and ulnar deviation. The maximum torques, measured on a 3D-printed arm mannequin, were 1.32 Nm during extension, while greater than 0.5 Nm for the other motions. Tests with external loads (1.5 kg and 3 kg) have shown that the torque assistance increased, on average, support by 62.81 %, 101.65 %, 58.11 %, and 44.23 % in flexion, extension, radial and ulnar deviation, respectively. The average wearing time was 87 s (if self-worn), and 75 s (if assisted by another person).
These performances are in line with rehabilitation targets. However,some issues have still to be solved: the anchoring system (Velcro straps) could not perfectly prevent dislocation and should be modified to ensure stronger fixation and faster locking. The robot size and shape should be optimized for all users, reducing discomfort due to actuator misalignments. Full wearability can be guaranteed by reducing weights and keeping working temperatures as low as possible to prevent burning of the user’s skin.
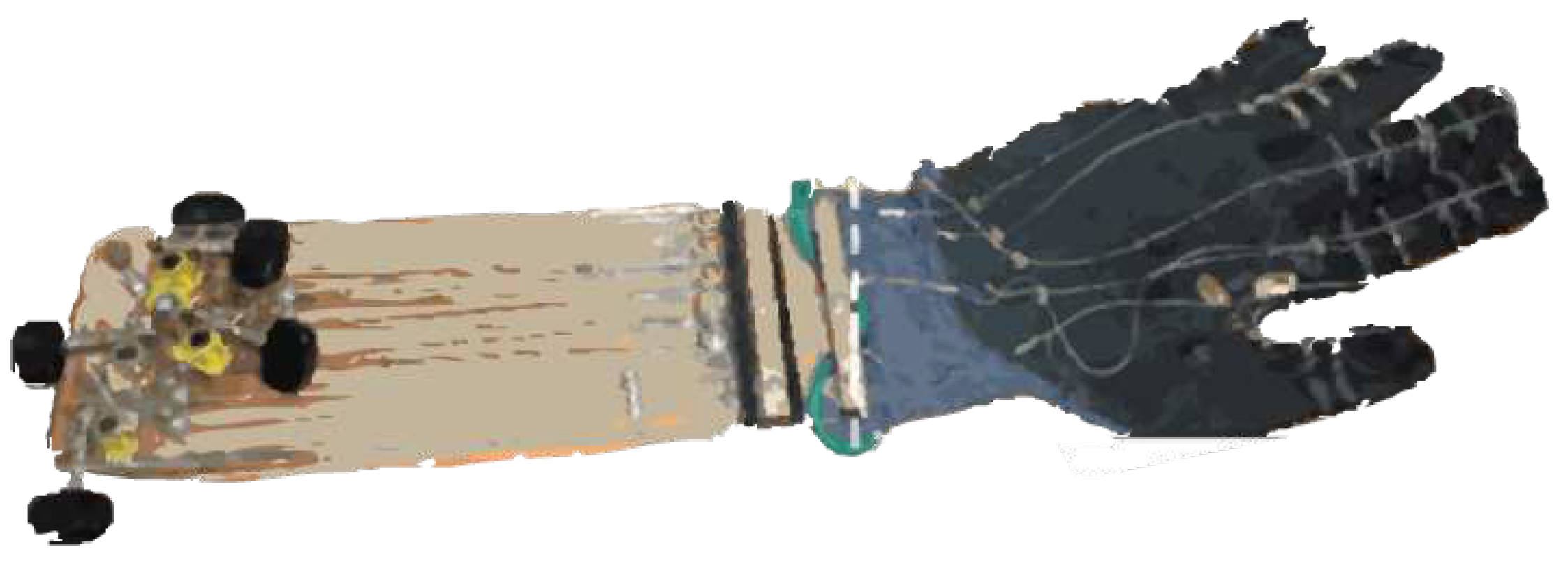
3.2.10. Wearable SMA-based Wrist and Forearm Exoskeleton
Hope and McDaid in [26] proposed a novel 3-DoF (flexion/extension, radial/ulnar deviation, pronation/supination) wearable and portable wrist-forearm SMA-actuated exoskeleton, for rehabilitation at home, or helping people perform ADLs. The exoskeleton is active, soft, compact, low profile, lightweight (950 g) and low noise. It is attached to the user at three points: hand, wrist and forearm. Forces/torques are transferred from SMA actuators to the limb by tendon-pulley mechanisms which adopt wheels of different radii for force amplification, arranged around the forearm. Each DoF is controlled independently through a tendon module and a SMA actuator, for a total of six tendons and related mechanisms. This arrangement allows complex combinations of movements (e.g. DTM) based on agonist-antagonist principles by varying SMA length through Joule heating. The wire tension is released after cooling through conduction and forced convection heat transfer with fans. Tendon length is chosen to allow free movements covering the maximum RoM, and a potentiometer, fitted into the amplification wheel, measures SMA wire linear displacement. Six force sensors, arranged around the hand, provide information on flexion/extension and radial/ulnar deviation. A variable stiffness model and active stiffness control of SMA actuators have been implemented. Stress and position of SMA wires are determined by potentiometer and force sensors. A closed loop PID controller modulates the duty cycle of the voltage applied to each actuator according to a target strain/position.
Figure 16.
SMA wrist-forearm exoskeleton for home rehabilitation developed by [26]. Image adapted from [26].
Two prototypes have been tested: one using a SMA actuator and a compensation spring, and another using SMA actuators in differential configuration. The assessment has been done by measuring tendon displacement on a test-bench while lifting a variable load and tracking different trajectories (step, sinusoidal and triangle waves). The expected displacement of the actuators in the spring-bias configuration covers 40 % of the expected RoM, while in the differential module covers the 65 %. In both cases the major issues are related to friction (especially at lower strain rates and duty cycle), tolerances in the mechanical components, and the uncontrolled pre-stress on the SMA wires. Further potential improvements could include: a quantitative analysis of system friction to generate better and smoother control; a more effective cooling system rather than miniature fans, integration of sEMG sensors on the forearm cover as additional sensing method; redesign of each module to reduce the overall weight and fit different sizes.
3.2.11. ASR: a wearable glove for hand grasping
Hadi et al. in [38] have presented the ASR (Advanced Service Robots), a 5-fingered SMA-based hand exoskeleton for grasping rehabilitation and assistance, for use both in clinics and at home. ASR is active, portable, light (300 g without electronics and batteries), compact, and noiseless. Its actuation system consists of: two fishing wires for each finger (attached to the proximal and distal phalanges), a SMA actuator for each fishing wire (for a total of 10 SMA), and guides for connecting wires and transferring the force. The SMAs are fastened to a rigid platform on the forearm, and use 1 m FLEXINOL of 0.38 mm diameter, that can produce 22.5 N force. When the actuators are heated up with a current of 2.2 A, their tension force and length variation are transformed into phalanges motion and hand grasping.
A theoretical model which correlates tendon tension and grasping force have been developed and experimentally assessed by using two load cells to measure fingertip and tendon forces, a signal amplifier and Arduino Uno micro-controller to record data. Results show good agreement between theoretical and experimental values. The device was assessed on a volunteer. The force exerted on the fingertip is 35% of the force produced by the SMA actuator. The total grasping force is more than 40 N, which is sufficient for typical ADLs (18 N). The overall speed of hand closure is 3 s, while it takes about 4 s to open by cooling down the actuators using air fans. Although not directly conceived for wrist assistance, due to motion synergies between hand and wrist, problems at the wrist level reduce grasping ability, therefore this device could be considered a valuable wrist support. Current drawbacks include: a lack of full wearability as integration of sensing and control systems is not yet implemented; no user trials; the high currents (2.2 A) needed which might be dangerous for real applications.
3.3. Compliant devices
3.3.1. SMA based wrist exoskeleton
Serrano et al. [27] have proposed a rehabilitation wearable wrist exoskeleton with 2-DoF (flexion/extension and radial/ulnar deviation) based on SMA actuators. The device, shown in Figure 18, is a hybrid because of a rigid kinematic chain around the joint actuated by flexible materials remotely placed. Flexinol® is used as SMA actuator (0.51 mm of diameter), which can exert 35.6 N of force and more than 0.5 Nm of torque. One SMA wire is used for each movement, except flexion which is left under gravity. The exoskeleton is made of simple and low cost parts through 3D-sintering polyamide with aluminum powder. The rigid interfaces are sewn on a glove to ease wearability. The device is symmetrical and can be worn both on right and left hands. The overall weight, considering the actuators, is less than 1 kg and the price is approximatively 1060 $.
The feasibility of the system has been tested first on a simulator and then in real cases. Biomechanics of Bodies (BoB) software was used to select the proper actuation systems, evaluate human body biomechanics, mechanical designs and control algorithms. Then a pilot study was conducted on 3 healthy subjects. Results showed the device allows a RoM between + 40° and -10° in flexion/extension; while between + 30° and -10° in radial/ulnar deviation. In both cases, the exoskeleton can follow a reference movement with small error. For a proper displacement of the wrist, 2.2 m long SMA wires are needed for extension, and 1.7 m for radial/ulnar deviation.
The main difficulty when controlling SMA actuators is their hysteresis which introduces non-linearity in the system. Thus, a BPID controller (a combination of a standard linear PID controller with a bi-linear compensator) has been used for a single SMA wire. This device could be an alternative noiseless and low cost solution to current rehabilitation robots. Despite the inherent flexibility allows it to adapt easily to the body, the wearability is still an issue due to the encumbrance of long cables and the high temperature needed to activate the actuators.
3.3.2. SCRIPT: a passive orthosis
Ates et al. in [28] have developed a hand and wrist exoskeleton for post-stroke rehabilitation at home, which provides compliant and adaptable extension assistance during ADLs.
SCRIPT has been designed with either passive and active actuation. However, even if the active ones provide more benefits, their architecture results more complex, heavy (1.5 kg) and bulky. Thus, the authors focused on improving the passive mechanisms with dynamic interaction. The device in Figure 19 is called SPO-F, and represents the final achievement after 4 design architectures described in [28]. It is an hybrid solution involving a rigid kinematic chain with a soft actuation system (springs and cables). It provides assistance along 1-DoF: wrist and fingers extension to overcome the hyper-flexion problems and restore a more functional position. The finger mechanisms consist of 3D-printed stiff levers connected with digit caps via a Dyneema cable, and actuated via extension spring. The wrist mechanism is a 3D-printed double parallelogram which transfers torque to the hand plate thanks to an extension spring. Each spring force can be adjusted by individual ball-chains. As rigid interfaces, off-the-shelf ergonomic components from SaeboFlex [33] are used and available in different sizes (S, M, L, XL) to better fit on each subject.
The device RoM has been assessed by using rotary position sensors (potentiometers), an Arduino Nano micro-controller and a visual marker on the hand plate for motion tracking. Results show the device can rotate up to 45° in flexion and 30° in extension. Assistance is proportional to hand flexion, spring stiffness (k), levers length, and their placement. The forces and torques are measured, via force sensors, for different stiffness values and different pre-tensioning forces at fixed k = 0.5 N/mm. In all cases, the minimum torque is higher than 0.5 Nm, while the maximum is 2 Nm at 60° of extension.
The first SPO orthosis was tested by 33 stroke patients in 3 different EU-countries. This has helped address the final design of SPO-F, which looks lighter (650 g), safer, more professional, comfortable, compliant, simple, easy to wear and able to satisfy rehabilitation requirements according to a stroke patient. Despite the great achievements obtained over the years, the design should be further improved in compactness due to its vertical profile. Furthermore, the extension force applied on the digits should be assessed with more patients because the compression applied might cause some fingers pain.
3.3.3. Hand and Wrist actuated Exoskeleton for Rehabilitation and Training
Dragusanu et al. [14,29] have developed a 2-DoF (flexion/extension and radial/ulnar deviation) active and hybrid exoskeleton to allow people with disabilities regain autonomy.
The device, shown in Figure 20, consists of a tendon-actuated mechanism with thermoplastic interfaces, which allows remote actuation and user’s adaptation. All actuation and electronic components are placed on the forearm, and data are transmitted via Bluetooth. It is composed of two independent rigid parts tailored on the user: one on the hand and the other one on the forearm. Three tendons, wrapped around three pulleys, connect the motors on the forearm to the hand plate. Dynamixe XL-320 DC rotary motors are selected, with a stall torque up to 0.39 Nm at 7.4V, that is suitable for rehabilitation applications. The whole system weighs almost 300 g, and costs about 150 $. The control consists in tracking wrist movements by measuring the orientation of the hand with respect to the forearm using IMUs (on the hand and forearm). A Matlab GUI interface has been developed to guide the users during rehabilitation making the whole process easier to set and less boring.
This wrist exoskeleton has become a module of a full hand/wrist exoskeleton developed by the same authors [14], which can also actuate fingers flexion/extension, works for about 3 h, and has an overall weight of 500 g. The updated version of the wrist comes from users’ feedback on wearability and anatomical adaptability. Subsequently, all rigid interfaces and the actuation module have been re-designed with a parametric approach: pulleys connected to the motor shafts are reduced in dimensions; an external support is added to wrap the excess wire; an automatic closure for the forearm module is designed to ease and halve the wearing time. The structure and control are developed to guarantee the use of hand and wrist modulus independently.
The device’s performance has been assessed involving a patient in the execution of three exercises: flexion/extension, radial/ulnar deviation, and recording and reproducing a movement performed by a physiotherapist. Predefined set of movements are generated. Among 60 trials, the average root-mean-square (RMS) errors in following flexion/extension and radial/ulnar deviation movements are not normally distributed, and have statistically significant differences for different motor speeds (). This device has interesting features and great potential for use in rehabilitation. It can assist all wrist movements, it is portable, wearable, cheap, lightweight, easy to control and manage autonomously, and has a TRL of 4. However, some improvements could be made to reduce the overall encumbrance, weight and improve the torque provided.
3.3.4. Low-Profile Two-DoF Wrist Exoskeleton
Higuma et al. in [30] have developed a 2-DoF rigid wrist exoskeleton for rehabilitation, which allows flexion/extension and radial/ulnar deviation movements.
Figure 21.
Low profile 2-DoF wrist exoskeleton for rehabilitation developed by [30]. Image adapted from [30].
The mechanism consists of a hand back support, a forearm base where two linear actuators are placed, and two steel spring blades which connect the motors to the hand. The device is inherently flexible thanks to elastic elements which can deform during motion and adapt to the wrist center of rotation while transmitting forces. Each linear actuator moves a spring blade independently, back and forth, allowing bi-directional force transmission.The device is made of 3D-printed resin, it is 310 mm in length and weighs 509.5 g.
Performances measured on a test bench showed a RoM in good agreement with Finite Element Analysis (FEA) results, which covers most of that of healthy subjects: 56.7° in flexion, 68.1° in extension, 39.5° in radial deviation and 13.8° in ulnar deviation. The constrains are mainly due to the limited stroke of the actuators. The torque varies from 0.26 Nm (max flexion) to 2.47 Nm (max extension), with an average of almost 0.65 Nm for radial and ulnar deviation. The maximum load applied perpendicular to the wrist is 10.24 N for flexion/extension, with a shear force of 7.98 N; while for radial and ulnar deviation is 4.26 N, with a shear force of 4.14 N. Despite small interaction forces, a human evaluation is required to verify whether it harms the user.
Overall, it is a simple mechanism with a fairly soft structure which allows the wrist moving less overloaded. However, since linear actuators are not manually backdrivable, when turned off the fixed position of the blades may apply some shear force on user’s skin. Moreover, the absence of a defined center of rotation could make the springs deform in unwanted manners, increasing discomfort.
4. Commercial Devices
Searching online it is possible to notice how difficult is to find in the market devices conceived for workers’ wrist assistance. Most of them are designed for rehabilitation and training, or are still prototypes unable to jump out from research labs and hit the market. In 2020 Forbes published an article titled "The Number Of Companies Making Industrial Exoskeletons Has Been Quietly Increasing For The Past Five Years" [52]. One of the main contributors was Borislav Marinov, a founder of ExR-ExoskeletonReport website [53]. Borislav pointed out that still a comprehensive definition of what constitutes an "industrial exoskeleton" has to be defined [52]. The Wearable Robotics Association (WearRA) has estimated that the total number of businesses engaged with producing or distributing industrial exoskeletons has increased by 350% between 2015 and 2020, tallying an increase from 16 to 56 companies (as shown in Figure 22), and more than 700% up to now with almost 120 companies around the World [52,53]. A reason behind this increase may depend on a recent shift in the perception of the exoskeleton not as something which makes people either "superhuman" or "better", but rather as a specific tool, that could be worn and help workers complete physically repetitive tasks safer and more efficiently.
To get an idea of which are the exoskeletons that have been introduced onto the market over the last decade, the website ExR-ExoskeletonReport has taken on relevance. It could be considered the widest repository/catalog of exoskeleton devices for all application domains [53]. Looking into the body area section, it is possible to notice that there is a lack of devices conceived for wrist assistance. These deficiencies make the research and development phases more difficult since there is very little information. Hereafter, we propose a list of devices, already available on the market, which involve the wrist in their assisted segments. All devices taken into account, which will be described in the following sub-sections, are shown in Figure 23 and grouped according to structural stiffness criteria. Moreover, based on the wrist exoskeleton requirements proposed in [15], the schematic shown in Figure 24 provides relevant information about commercial wrist exoskeletons.
4.1. Rigid devices
4.1.1. JAS Wrists
These products are developed by Joint Active Systems Inc. (JAS), a leading company in the US for range-of-motion therapy for patients with motion losses. They provide a wide range of options, for assisting different limbs and joints, to meet the needs of each patient, and some open-source data/analyses demonstrating the effectiveness of these devices. The company proposes a well-structured protocol for starting ROM therapy after an injury or surgery.Their pioneering device for the wrist is JAS Static Progressive Stretch (SPS) Wrist. It utilizes proven principles of SPS to achieve permanent restoration of joint ROM. It is conceived for injuries such as distal radius/ulnar fractures, carpal fractures, ligament/tendon repairs. Clinical studies carried out in more than 60 patients with deficits in wrist flexion or extension ROM, or healed distal radius fractures, have shown an increase in ROM, and grip strength already after six months of therapy [57,58].
However, among all their products oriented to the wrist joint, we would like to focus more on the devices called Advanced Dynamic Wrist Flexion and Extension [31], shown in Figure 25 since they seem more practical and comfortable for use outside clinics, at home to enhance therapy, while sleeping and resting to achieve permanent RoM gains. These devices are a ready-to-fit, low profile, and lightweight passive rehabilitation orthoses. They include integrated tension control, allowing patients to optimize spring tension by simply rotating a lever by hand. Actually, there are not many studies reporting on the application Advanced Dynamic JAS Wrists. In [59] the concept of dynamic splints was tested with 133 patients (78 women, 55 men; mean age 53 ± 17.6) on wrist extension, in both surgical and non-surgical patients (respectively 42 and 91 subjects) following distal radius fractures. The results showed a 62% recovery in active range of motion within 3 to 20 weeks of treatment, with no significant differences between genders, or among patients who received previous surgical intervention. Based on clinical and published evidence, some articles described their safety, usefulness in the effective RoM increase and restoration for all levels of joint stiffness (e.g. wrist arthrofibrosis), and patient satisfaction [60,61].
4.1.2. MyoPro Orthosis
MyoPro Orthosis was born in 2006 thanks to the work done at MIT and Harvard Medical School, and then commercialized by the company Myomo Inc, Figure 26. The product is a wearable active powered arm orthosis (including elbow-wrist-hand) designed to restore the function of paralysed or weakened arm for patients suffering from neuromuscular and neurological diseases or injuries (e.g. stroke arm paralysis, brachial plexus injury, cerebral palsy, multiple sclerosis). The MyoPro weighs approximately 1.8 kg, provides almost 0° to 130° of motion and 7 Nm of torque at the elbow, and 1 - 2.7 Nm torque for the fingers, ensuring the lifting of approximately 2.3 - 3.6 kg [62]. The device works by reading the faint nerve signals from the skin through sEMG, then amplifies them and activates motors to move the limb as the user intends, as shown in Figure 26. The wrist joint is conceived for improving dexterity and recovery muscle tones and functionalities.
Since 2017 several experiments have been done to evaluate its effects on in-clinic and at-home rehabilitation in patients with arm weakness following neurological disease. Over fifty individuals who have been diagnosed with upper limb paralysis caused by spinal cord injury (SCI), chronic stroke, or traumatic brain injury (TBI) have taken part in clinical trials. In [62] a 62-year-old US Army veteran with upper extremity paresis and chronic stroke was involved. He was monitored for 3 years. During the first year, he mainly received traditional occupational therapy (OT) without orthosis, such as electrical stimulation, mirror therapy, massage wand, active assisted and passive ROM, and task-oriented interventions. Starting from the second year it was included in his therapy the use of a functional grasp MyoPro Arm, either in clinics and at home. At the end he was able to independently open his hand (75%), which indicates a substantial improvements in ADLs using his paretic left arm, and in his level of independence. In [63,64] 2 adult males (respectively 75 and 31 years old) with SCI were involved. Experimental protocol consists in evaluating active hand-grip angular position, hand-grip force and sEMG from the finger flexor and extensor muscles, by squeezing and opening the hand through 18-training sessions in a rehabilitation research center, three times per week (almost 60 min/session). In [65] 18 stroke subjects were selected (11 males, 7 females; average age 55.5 (±21.5) years old) in a single-day-session study to evaluate the device usability, functionality and efficacy. Most participants were able to don/doff, use the device without any assistance, and hold up to 1 kg weights for 2 minutes. In [66] 13 volunteers (5 males, 8 females; average age 50.9 (±19.9) years old), 7 of whom suffered a stroke and another 6 TBI, were involved in a pilot study of about 18 weeks of both in-clinic sessions and home exercise therapy with the use of MyoPro arm. In-clinic therapy consisted of 2 weekly sessions each lasting 1.5 h under the direction of a physical therapist. In [67] 18 stroke patients participated in a 3 months home rehabilitation trial (13 males and 5 females; average age 52.5 (±14.7) years old). Before receiving their MyoPro, a baseline session evaluated their performance on a battery of functional tasks (e.g. move object to mouth, hold object in space,stabilize object) with their paretic side.
Overall, participants involved showed a high level of satisfaction using the device, and significant improvement in overall task completion (time and correctness in execution); furthermore, compared to baseline (without the device), they were able to perform bi-manual tasks for prolonged periods, increase their independence in ADLs, improve forces while grasping, lateral pinch strength, wrist RoM, and avoid emerging wrist ulnar and radial deviations. Moreover no serious adverse events, such as hyperextension of the joints, pain caused by the device, or skin breakdown were recorded [62,63,64,65,66,67,68].
4.2. Soft devices
4.2.1. Carbonhand®
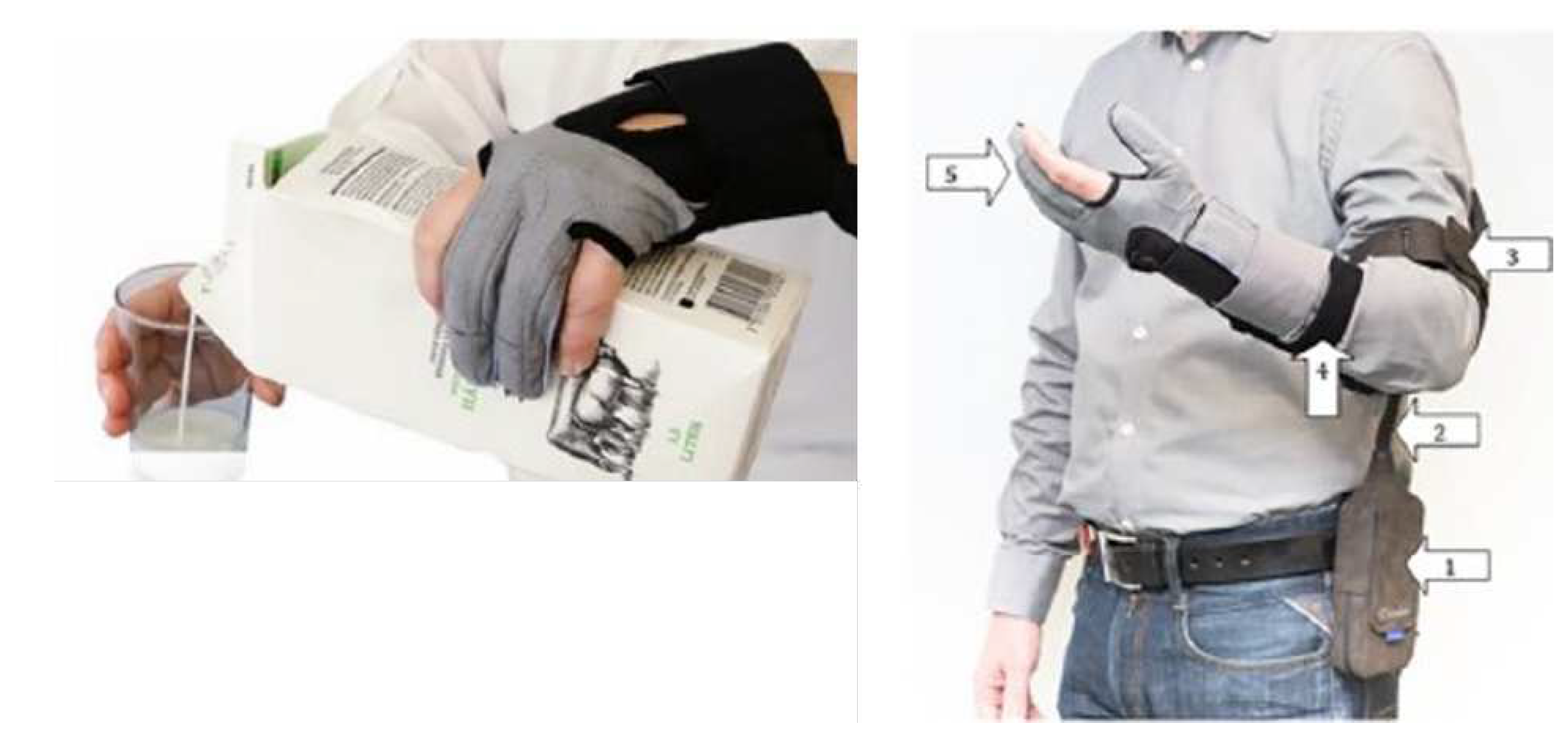
Carbon-Hand is an assistive soft robotic glove for use outside of clinical settings, built on the Soft Extra Muscle (SEMTM) technology [35,69]. It is sold by Bioservo for almost $7000. It is designed on a glove with pressure sensors in the fingertips to measure contact forces when interacting with objects or tools. Thus, power will be applied when the user initiates gripping to ensure a firm grip. So, it activates 1 DoF: the gripping (or finger flexion). It augments human capabilities by applying a force of up to 20 N per finger (involving only 3 fingers). The overall device weighs 685 g (glove + control unit), but since the control unit and the battery could be placed wherever preferred to the user’s body, weight should not be an issue. Batteries are designed to last approximately 8 hours and the device is available in different sizes (XS, S, M, L, XL) for both right and left hands. The device is conceived for rehabilitation and assistance-at-home by helping people with reduced hand functions perform ADLs independently [35,69]. This device goes under our attention because, due to motion synergies, hand dexterity is related to wrist motion and resistance capabilities: problems at the wrist level reduce grasping ability. Therefore, this device could be considered a valuable wrist support.
Figure 27.
Bioservo Carbonhand ® device and examples of related application [54]. Legend: 1) SEM unit; 2) Cord; 3) Arm strap; 4) Slap wrap: 5) Glove, three finger version.
Figure 27.
Bioservo Carbonhand ® device and examples of related application [54]. Legend: 1) SEM unit; 2) Cord; 3) Arm strap; 4) Slap wrap: 5) Glove, three finger version.
A first pilot study in [70] involved 15 participants (18 - 65 years old) with a chronic SCI and impaired hand function. They were given instructions on how to use the device at home for 12 weeks for at least 4 h a day during regular ADLs, and executing task-specific activities such as squeezing and releasing a soft ball, simulated drinking, eating a meal and writing. Participants were asked to record their activities in a diary. They returned for reassessment after week 6 and week 12 to evaluate grip strength and hand function. Most participants reported that they used the glove 0.3–6 h daily, and the average grip strength across subjects improved from initial (9.9 ± 2.9 kg), to week 6 (14.0 ± 3.0 kg), and week 12 (14.0 ± 3.2 kg). Moreover, it has recently been assessed for six weeks in 63 participants (between 18 and 90 years old) with impaired hand functions [71]. The protocol consists of 5 assessments for each participant: 3 pre-assessments across three weeks as baselines prior to the intervention; a post-assessment Within 1 week of the end of the intervention; and a follow-up assessment 4 weeks later to measure the retention of effects. Participants are patients who experience limitations in hand function, and who will therefore be asked to use the glove, at least 180 minutes per week, during ADLs at home (such as lifting and carrying items, performing hobbies, cleaning, cooking). The outcome measures are handgrip strength, arm and hand functional abilities, amount of glove use, and quality of life. Preliminary results have shown promising improvements in grip strength (+27%), pinch strength (+15%) and hand functionality (+12%). Since 2022, it has also been approved as a medical device according to the European Medical Device Regulation (EU-MDR).
4.2.2. Ironhand®
IronHand® is a soft active exoskeleton for grasping assistance and augmentation also built on the Soft Extra Muscle (SEMTM). Initially, the development of the SEMTM technology was intended to rehabilitate patients with impaired hand function (e.g. CarbonHand®). Today, Bioservo Technologies is also focusing on prevention of injuries at work. The product has undergone long-term testing with various industrial partners, which have become key factors for its quick development since its first release in 2019 for almost $6,500 [35,55]. IronHand 2.0, shown in Figure 28, consists of a sensorised glove, a back-pack (with control and battery) and a hip-carry, everything designed in different sizes (S, M, L, XL) to better fit user’s body. The whole system weighs almost 2,75 kg, of which 50 g the glove. The lithium battery in the back-pack is the sore point for the weight with a full-charge duration of almost 6-8 hours. The glove has force sensors (FSR) on the finger tips and the palm, and it is innervated by artificial tendons (e.g. bowden cables) which enhance fingers flexion and gripping thanks to the push-pull action of linear DC motors. Enabled when force sensors detect certain pressure levels, the tendon-driven system can generate a maximum force of 16 N per finger (80 N in total) [35,55], adjustable to adapt to different needs and applications, as shown in Figure 29. The device can collect and share data through Bluetooth, 4G and Wi-Fi among different devices (e.g. tablet, control equipment), and save them in a local storage or in cloud (BioCloudTM), Figure 29. The collected data also allow to assess the wearer’s risk of developing injuries. Several clinical trials have been done on the SEM technology over months [54,55,70,71]. First preliminary study on the effect of IronHand in working tasks (automotive assembly) has been published in [72]. Eight participants (4 males and 4 females) were identified by a General Motors (GM) ergonomist based on the task which required the hand to be active for most of the work cycle, gripping efforts to manipulate parts/tools, and willingness to use the device for 2 weeks. Muscle activity was recorded using sEMG from main forearm muscles. For each participant, sEMG was collected on the first day without IronHand, and on the second day with it. Once all electrodes were properly placed, participants performed muscle specific isometric maximum voluntary contractions (MVCs) for 3 seconds. Controlling task, repetition and cycle variables across participants was not possible, since each one performed different tasks within a work cycle (almost 120 sec) on the assembly line for one 8-hour shift (e.g. curtain airbag installation and secure, floor-pan secure, overhead fastener secures, carry and installation of engine splash guard). Overall results have reported a significant reductions in forearm muscle activity, improvement in gross hand grip strength, pinch strength and all hand functions (e.g. grip, grasp, precise movements, writing, etc). Further evaluation demonstrated that 59% of the recorded cycles resulted in a reduction in at least one muscle’s activity and 41% in an increase in activity. Thus, when compared to no exoskeleton, the IronHand produced both increases and decreases in forearm muscle activity, depending on the individual and the specific tasks. Therefore, specific use cases need to be carefully determined and the device optimized for each individual to ensure benefits.
Even if it is a hand exoskeleton for grasping augmentation, again due to motion synergies, it is safe to assume that grip force and wrist fatigue are in a sense correlated. The strong the grasping the more compression will be transmitted to hand ligaments and wrist. However, in spite of these promising results, in our opinion, this does not mean that reducing grasping fatigue it will guarantee the same reduction in wrist workload. Rather, it will reduce the probability to get injured, inflammations (such as CTS) and pain in the wrist joint.
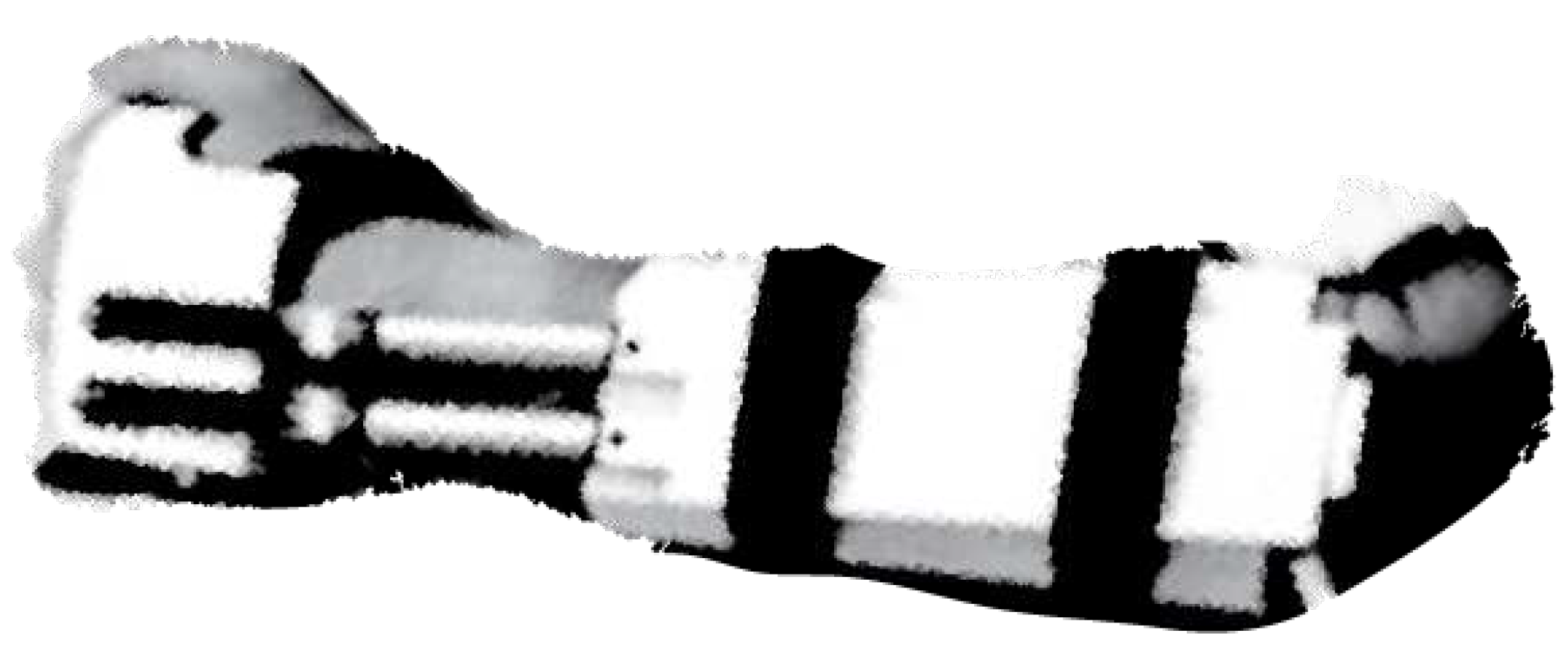
4.2.3. Paexo Wrist®
Paexo Wrist is a commercial passive wrist exoskeleton developed and sold by Ottobock for almost 160$. In practice, it is an orthosis which aims at supporting the wrist while moving loads, and preventing injuries and inflammations. It can be used when holding a screwdriver, riveting tool or welding equipment, and carrying loads. By looking on the website Paexo.com and the user manual, the device adopts innovative solutions: materials for thermal regulation tested in space (provided by Outlast Material), a Pull-2-Lock mechanism for quick one-handed donning in few seconds, a metal splint inside the garment which fulfills the function of a flexible beam to absorb and transfer loads away from the wrist. For a better versatility, the device can fit both left and right hands and is available in different sizes (S, M, L) to satisfy different users. No sensors and control strategies have been implemented. The device and its application are shown in Figure 30. The company mentions that Paexo Wrist has been thought for relieving muscles and tendons when working for long periods with tools and in assembly, by stabilizing the wrist and ensuring an optimal distribution of the workload. Unfortunately we have found no more technical aspects or analyses about its positive effects on workers’ health. So that, we cannot quantify its usefulness compared to other devices.
4.3. Compliant devices
4.3.1. SaeboFlex
SaeboFlex, shown in Figure 31, is a custom-fabricated wrist, hand, finger orthosis [73], developed and sold by Saebo Inc. for almost $600 [33]. It is designed to improve mobility in individuals with hand/wrist weakness or spasticity due to neurological or orthopedic conditions. It is a passive device made of resistive springs and conceived for therapy both in clinics and at home. No sensors and control strategies have been implemented. The major goal is to position the impaired wrist and fingers into extension for proper functional grip and release training [73]. Optimum wrist angle is measured at 35° of extension, which is considered the position where maximum grip effort onset. This value can be modified according to the patient impairment.
Pilot studies [74,75,76] were conducted to explore the feasibility, patients and therapists experience of SaeboFlex training. In [74] ten stroke patients were recruited from a rehabilitation hospital (five for the experimental group, of which 3 males and 2 females; and five for the control group, of which 4 males and 1 female). Subjects in the experimental group participated in 4 weeks of training using SaeboFlex for 1 hour per day, 5 times per week. Each session consisted of 9 task-oriented practice sessions involving the hemiparetic arm, such as moving a soft ball side-by-side, diagonally, reaching a target, grasping and releasing a soft ball. Each subject in the control group wore the same orthosis for 1 hour per day without participating in upper extremity training. In [75] eight stroke participants (4 males and 4 females; 70 ± 15 years old) with upper limb extremities weaknesses were recruited for 12 weeks of rehabilitation. A battery of measurements were taken at baseline, 4, 8, and 12 weeks. Participants were trained once or twice a day with sessions lasting between 5 and 105 minutes per day. The number of grasp and release repetitions ranged between 12 and 500 per day. In [76] authors focused more on the patients and therapists’ experiences by using SaeboFlex with both quantitative and qualitative data coming from previous clinical trials. Eleven stroke participants (7 males and 5 females; mean age was 60.2 ± 7.89) were recruited to answer questionnaires after their training program with the device. The questions relate to the Psychosocial Impacts of Assistive Devices Scales, and how the SaeboFlex supported their ability to do, be, become, and belong. Furthermore, five therapist were enrolled and asked to complete reflective responses for their work with clients. In [56] a 43-year-old woman with left upper extremity spasticity after stroke was involved in a treatment which combines botulinum toxin injection and SaeboFlex training. A 16-week program consisted of three 50-min sessions daily and focused on grasping and releasing with and without the splint. The patient was evaluated before botulinum toxin injection and after 6, 12 and 16 weeks. After completing the program, the treatment reduces disability and improves quality of life. However, further investigation is needed.
Overall results from clinical trials and questionnaires, conducted over months on patients who suffered from stroke [56,74,75,76,77,78], have proven that the device is safe, improves hand grip strength and dexterity moving objects, increases wrist extension RoM by 5-6 degrees, facilitates clinically significant improvements in upper limb function, coordination and velocity, participation and independence in ADLs, and reduces carer burden and associated costs.
5. Design proposal for a portable wrist exoskeleton
Based on the literature and our experience, in this section, we propose a conceptual idea (TRL 1-2) of a technological device to assist all wrist movements, provide sufficient force support, and guarantee good user acceptance in industrial settings. Softness, lightness, and customization are a must. Although obvious, these are factors that often emerge from user evaluation questionnaires [13,14,19,68]. Therefore, we will design a wrist exoskeleton on a glove to meet comfort requirements. We will customize the device to the user by taking anatomical measurements and utilizing 3D scanning technologies for the hand/wrist shape [11].
The device should allow the main movements of the wrist (flexion/extension and radial/ulnar deviation) and a combination of them in a controlled way. This would help during activities such as screwing, holding, hammering, and lifting. However, the RoM must be limited to avoid overstretching the human joint causing pain. This is in line with the safety requirements of a wearable device [15].
Gripping is also important, as the more the grasping, the more compression between the wrist ligaments, and the higher the probability of getting carpal tunnel inflammation.
To allow these movements, the idea is to use cable transmissions. Soft plastic supports/saddles (thick purple shapes in Figure 32 and Figure 33) would be sewn on a glove to hold steel or fiber cables (tiny light blue lines in Figure 32 and Figure 33) on the back, palm, lateral sides of the hand and fingers, as shown in Figure 32 and Figure 33, where forces would be applied. The shape of cable supports would be designed starting from the 3D hand/wrist profile. The cables from the actuators should be routed around the hand, passing through Teflon sleeves (black in Figure 32 and Figure 33) along the forearm to reduce friction. Care should be taken to avoid sharp edges or bending angles (e.g. 90° or more), as these cause friction losses along the cable’s path. One cable would be used to actuate a single wrist movement, except for grasping, where all cables around the fingers would be actuated simultaneously.
A rotary actuator, with a proper reduction transmission, would allow agonist and antagonist movements by pulling two cables (flexion/extension and radial/ulnar deviation), and would guarantee backdrivability. While for grasping a linear motor would be used to pull and close all fingers simultaneously. Forces (green arrow in Figure 32) would be applied through cables attached to actuators placed remotely, e.g. on a back-pack. This would help redistribute localized weights on the hand/wrist.
In terms of dynamic requirements [15], ideally, the device should guarantee to hold objects of 5 kg with almost no muscular effort. This could be beneficial both in rehabilitation and industrial sectors while handling loads. Actuators and transmissions have to be sized according to the weight to be handled. Consider a weight of 5 kg held on the palm, 10 cm from the wrist joint. It produces a force of almost 50 N and a torque of 5 Nm, which has to be compensated by the exoskeleton. Considering that standard normal-sized men’s wrists have a 16-18 cm circumference, the wrist radius is between 2.5 - 2.8 cm. Therefore, the cable force to produce 5 Nm torque around the wrist should be almost 180 N. This can be improved with special supports by raising the cable and increasing the radius with respect to the wrist. These supports (orange in Figure 32 and Figure 33) would also avoid cables unwinding, prevent the force vector from passing through the wrist CoR without producing effective torque, as shown in Figure 34, and reduce compression forces on the wrist. In fact, without these supports, the cable may become loose during pulling, causing the force to be closer to the wrist’s center of rotation, thus reducing the momentum and augmenting wrist compression (in Figure 34 the distances d, d’, and d” represent the pulling force arm in the neutral, flexion, and extension positions, respectively). With cable supports the cable unwinding is limited, and there is always a minimum distance, similar to that in the neutral position, which ensures a minimum effective momentum even when the wrist is flexed (the worst position).
We would implement sEMG sensors (red in Figure 33) to detect electrical muscle spikes and muscle fatigue when the user moves the wrist. And FSR sensors (yellow in Figure 33) in the palm to detect when an object is grasped and measure the gripping pressure. A control system would rely on state-of-the-art controllers based on machine learning strategies to anticipate hand/wrist movements according to muscle activation, and on a PID controller to generate the required pulling forces on cables [16,79,80,81,82]. The control scheme will be structured on two levels, as depicted in Figure 35, to guarantee the user is free to move as intended and experiences assistive forces with appropriate timing and extent. The high-level strategy establishes wrist movement based on muscular activation, the necessary amount of assistive force/torque and generates reference signals accordingly. While, at the low-level, a closed-loop force/torque controller tracks the reference signals at each actuator. EMG signals would be recorder from the high level controller, segmented and classified (e.g. by adopting neural networks or support vector machines classifiers) to establish the intensity of muscular activity, recognize which muscles are working and predict hand/wrist movement. FSR sensors in the palm would help assess the applied grasp force, which would be correlated with the amplitude of the EMG to determine the amount of support to be provided. As a result, force/torque and pulling direction reference signals would be generated by the high-level control and sent to the low-level controller. There a PID controller determines which motor to switch on based on the expected movement of the wrist, and regulates the output force/torque at each motor by tracking the reference force/torque signal.
The objective is to design a device that supports user handling at least 5 kg without effort, as soft and light as possible (less than 1 kg), comfortable, portable, with a 6-8 hours battery, and an affordable and user-friendly command interface (UCI). We are inspired by existing commercial and research products with the most promising characteristics and well received by patients and workers. We aim to enrich research by creating a new wrist exoskeleton for occupational purposes, helping to support all wrist movements during activities that can be detrimental to its health.
Figure 35.
Control scheme articulated in two levels. The high-level is responsible for the assistance to be given within appropriate timing. The low-level determines which actuators to switch on and regulates the force/torque output references at the actuators.
Figure 35.
Control scheme articulated in two levels. The high-level is responsible for the assistance to be given within appropriate timing. The low-level determines which actuators to switch on and regulates the force/torque output references at the actuators.
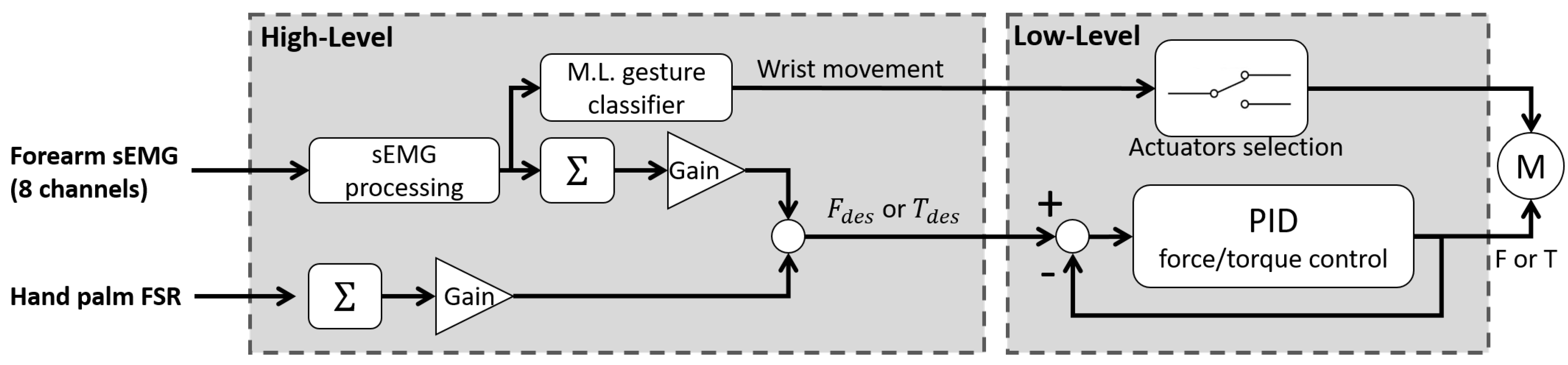
6. Discussion and conclusions
During the past few decades researchers have been working towards the development of exoskeletons with improved capabilities and "intelligence" levels to solve problems due to aging, disabilities, overload, strenuous works, which can prevent people from living a normal life, leading to marginalisation both on work and private life. These devices are expected to play an important role in human health in the areas of rehabilitation, assistive technologies, and human power augmentation by transferring loads away from the human body while assisting in certain tasks. Some positive results and approvals have already been achieved in rehabilitation, while others need to be further investigated,such as for the occupational sector. The recent increase in disabilities caused by musculoskeletal disorders (with more than 1.7 billion cases worldwide) has frightened the European Commission and the WHO which have been leading awareness campaigns on this issue. Only in the last decade wearable commercial solutions have entered the market to assist workers in burdensome and repetitive tasks. However, has reported by Tiboni et al. in [44], relatively a few focus on the wrist despite being considered the fourth most common site of musculoskeletal pain in the upper limbs.
This paper review provides a comprehensive summary of several types of wearable and portable wrist exoskeletons, available in both the market and research, as shown in Table 1 (see Section 7 Appendix 1), and aims to gather sufficient information to develop critical thinking on what distinguishing features can determine the design of effective exoskeletons depending on the field of application and the requirements to be met. We have described and compared devices conceived for different applications (rehabilitation, assistance and occupational), by focusing on their technologies (hardware and control), their functions, their potential and limitations. Macroscopic classifications of the wrist exoskeleton can be based on several aspects, as described in [15], including: purpose (rehabilitation, assistance or occupational), stiffness (rigid, soft, compliant), type of actuation, power source, power transmission, sensing, control strategies and technology readiness level (TRL), as shown in Figure 36 and Figure 37. A total of 24 wearable and portable wrist exoskeletons have been designed: almost 18 devices for rehabilitation and assistance, while 6 for occupational tasks, as shown in Figure 36 and Figure 38.
Looking at those data and Table 1, a strong prevalence of active devices emerged as they can provide greater forces/torques ensuring a wider range of applications. The most widespread actuation systems are electrical motors due to their robust controllability, great power-to-weight ratio, reliability, and price. For the power transmission, cables and tendons are preferred because of high force transmission, and remote actuation with a better redistribution of weight along the human body. However, they suffer from friction losses with non-linear behaviour, which make their control difficult. To ensure a better control of the device, lot of sensors are implemented. Position (encoder, potentiometer, IMU, flexible sensors) and force sensors (FSR, load cell, pressure gauge) are the most used. Position sensors improve device performance by estimating wrist motion parameters (angle position, velocity, and acceleration). Thus, it allows to determine which movement has been performed, and apply the drive parameters to provide assistance as fast as possible. Clearly, those solutions may suffer from time delay, discretization-related effects if the speed is obtained from position differentiation, or drift problems. Therefore, they usually require additional sensors for a more accurate evaluation of the kinematics. Force sensors are useful for the proper functioning of a device as they estimate the external loads applied to the wrist, thus establishing the torque/force to be applied to compensate for them, providing the required level of assistance at a specific time. However, limitations still occur. Although load cells are robust, very accurate and already calibrated, they are not easy to integrate into wearables because they are bulky, rigid, heavy, and require expensive signal conditioning. In contrast, FSRs are a good solution because they are easy to integrate, inexpensive and lightweight; however, they are not very accurate, must be calibrated, have great variability to environmental conditions, ageing and can be easily damaged.
Nowadays, new control methods based on bio-feedback signals (e.g. sEMG), directly related to the user motion intention, have also been tested. These sensors still have limitations in unstructured environments, as they must be attached directly to human skin and suffer from external noises. The main control strategies adopted are Control Passive Motion (CPM) and Assistance-As-Needed (AAN). The former consists in control the movement of the exoskeleton according to predefined trajectories; the latter evaluates the actual external load or muscle effort to modulate the assistance provided by the robotic device. AAN is strongly recommended in unstructured environments where the user could perform different activities. Moreover, new control techniques are being developed based on Machine Learning (ML) algorithms to predict user motion intention, and reduce the number of sensors adopted.
In terms of ergonomics and safety, the design features sought are kinematic compliance with human joints (choice of an appropriate number of both active and passive DoF), covering and protection systems for electronics and moving parts, wearability, customisation, and lightness. Wearability and comfort are obtained by using soft materials, textiles, and foams, especially on human-robot interfaces, as shock-absorbent or as a coating for rigid parts. 3D scanning technologies have been considered a reliable and increasingly common approach to customised design, gathering information on the shape, dimensions and metrics of a real object. To achieve lightness, the focus is on the choice of design materials and low-profile shapes for the parts that wrap around the limb. Moreover, in active devices, remote actuation helps to locally lowering and better distributing the weights and pressure points on the human body by moving the actuators far from the actuated joints/limbs. Safety is usually guaranteed by introducing mechanical limit stops to avoid excessive joint excursions and cause harm to the user, covering open or forbidden spaces of the robot, avoiding floating cables, implementing emergency shutoff switches, and multiple control routines in the software to monitor sensor status, joint angles and joint torques to prevent sudden and unexpected movements and limit maximum torque.
It is not easy to design wrist exoskeletons because of the complex anatomy of the joint: it can move in a 3D space while supporting high forces in a very compact size. This creates difficulties in reproducing and assisting such kinematics and dynamics, without hindering human movement. Moreover, the requirements and specifications needed in certain applications lead to different design approaches. The majority of the devices reviewed are still under development with promising practical outcomes, tested and used only in a laboratory setting. By looking at these, as presented in Section 5, the authors are working on the development of a novel portable wrist exoskeleton for occupational purposes. To facilitate user acceptance and accelerate the industrialisation phase, a soft device made on a glove would be the starting point. Tendon mechanisms, remotely actuated via DC motors, would first be tested as more reliable, robust, light, safe and cheap solutions. As sensing, position and force sensors would be distributed throughout the glove to detect wrist movements and forces/torques applied. As control strategies, advanced machine learning algorithms for the AAN would be adopted. They would detect motion intentions and provide assistance according to the position and overload of the wrist.
The main limitations of this study, which may affect the generalisability of the findings, are as follows: a small number of trials conducted on subjects and in real conditions in both rehabilitation and occupational settings, especially for non-commercial devices; a small number of commercial devices that can be compared, especially designed for workers; a limited amount of accessible information on clinical data and experimentation on subjects especially for commercial devices. All this makes it difficult to quantitatively evaluate the benefits of devices and their technologies, without showing real limits. Rather, it only allows one to speculate on what the most effective solutions might be.
Like all products, technological and economic barriers, as well as communication biases, are open issues opposed to acceptance and industrialisation. The main obstacles could be identified in: the high costs and long-term research and development times, which are often incompatible with the views of stakeholders and consumers; lack of interest from stakeholders that makes it more difficult to justify the development; lack of market competitors makes it difficult to identify their pros and cons, and find more advanced solutions; need for CE or FDA or similar certifications. Furthermore, for occupational aims challenges, specific user needs and acceptance issues may concern: physiological (e.g. personal history of physical complaints, wearing comfort), psycho-social (e.g. perceived usefulness, openness to innovation, being in control, safety), work related (e.g. compatibility with tasks, storage, durability, reliability), policy-related and implementation-related factors (e.g. WRMDs prevention, costs, ease of use, training). Moreover, if the development of a device is driven by specific end-user needs and collaborations, the results greatly improve acceptability. This makes it more likely that exoskeletons are adopted rather than deserted after an initial period of testing. Although various frameworks have been suggested on existing technology acceptance models for industrial exoskeletons with potential end-users [83], a grounded framework is still lacking.
Even though it is difficult to justify exoskeletons effectiveness, due to the lack of long-term experimental tests (more than 3 months), the need for standardized products, evaluation protocols and regulations, these devices bring both benefits and limitations [83,84]. Some studies claimed their potential and effectiveness at reducing muscle demand to the pathophysiological mechanisms underlying MSDs during load handling tasks, static bending postures, and elevating postures. However, using exoskeletons could lead to antagonist muscle compensations and/or spinal imbalance, changes in postural strategies and muscle coordination (i.e. inertia, force, speed trajectory), which could, counter-productively, increase tendinopathies and the risk of injuries [84]. The current state of knowledge does not allow unreserved endorsement of the use of these devices as preventive technologies because many questions still need to be investigated and clarified, in particular the occurrence of muscle fatigue and chronic adaptations, skin pain, the impact of movement assistance on neuromuscular coordination and joints kinematics. In view of emerging health and industrial needs, and thanks to the latest research findings, the authors expect an increase in demand for progress and development in the field of portable wrist exoskeletons in the coming decades, hoping for the same positive results as other devices to improve working conditions and people’s health.
7. Appendix 1

Table 1.
Comparison of all wearable and portable wrist exoskeletons highlighting their characteristics.
Table 1.
Comparison of all wearable and portable wrist exoskeletons highlighting their characteristics.
| Reference | Device Name | Application Field | Actuation Type | Power Source | Power transmission | Force/Torque output [N][Nm] | Active DoF | Assisted motion | RoM | Sensing | Control | TRL | Weight | Price($) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Research prototypes | ||||||||||||||
| [16] | PWE | Rehab/Assistance | Active | DC motor | Links, gears | 2.3 Nm | 2 | Flex/Extension | ± 60° | Potentiometer | CPM | **4 | 0.36 kg | - |
| Occupational | 2.5 Nm | Rad/Ulnar dev. | ± 25° | sEMG | M.L. | |||||||||
| [13,17] | eWrist | Rehab/Assistance | Active | DC motor | Links, gears | up to 3.7 Nm | 1 | Flex/Extension | range 154° | sEMG, load cell, | AAN | **4 | 0.56 kg | - |
| encoder | ||||||||||||||
| [18] | *- | Rehabilitation | Passive | DC motor | Links, gears | up to 1.12 Nm | 1 | Flex/Extension | range 120° | Triggered | CPM | **4 | 0.33 kg | *- |
| Active | Force (FSR) | M.L. | ||||||||||||
| [11] | Wrist exosuit | Occupational | Active | Brushless motor | Bowden cables | 3 Nm | 1 | Flex/Extension | 70°/80° | Load cell,IMU | AAN | **4 | 0.3 kg (hand) | - |
| [19] | Exo-Wrist | Rehabilitation | Active | DC motor | Bowden cables | ≥ 0.5 Nm | 1 | Extension | ≥ 50° | sEMG | AAN | **4 | 1 kg | - |
| [20] | *- | Rehabilitation | Active | Pneumatic | Artificial muscles | 120 N | 3 | Flex/Extension | 91° | Pressure | Triggered | **4 | 2.26 kg | - |
| Rad/Ulnar dev. | 32° | |||||||||||||
| Pron/supination | 78° | |||||||||||||
| [21] | ASSIST | Rehabilitation | Active | Pneumatic | Artificial muscles | up to 1 Nm | 1 | Flex/Extension | 80° | Flex sensor | AAN | **4 | 0.39 kg | - |
| Pressure | ||||||||||||||
| [22] | SOA-wrist | Rehab/Assistance | Active | Pneumatic | Flexible joint-less | up to 0.76 Nm | 2 | Flex/Extension | 31°/30° | Pressure, | AAN | **4 | 1.76 kg | - |
| structures | Rad/Ulnar dev. | 33°/22° | IMU | |||||||||||
| [23] | *- | Rehab/Assistance | Active | Brushless motors | Bowden cables | **≥ 5 Nm | 2 | Flex/Extension | range 115° | IMU | CPM | **4 | 0.65 kg | - |
| Rad/Ulnar dev. | range 70° | |||||||||||||
| [37] | EXOWRIST | Rehabilitation | Active | Pneumatic | Artificial muscles | 630 N | 2 | Flex/Extension | ±30° | IMU | CPM | **4 | 0.43 kg | - |
| Rad/Ulnar dev. | ±30° | |||||||||||||
| [34] | *- | Occupational | Active | Pneumatic | Flexible joint-less | *- | 1 | Flex/Extension | ± 65° | IMU | AAN | **3 | *- | - |
| structure | Pressure | |||||||||||||
| [24,25] | SWA | Rehab/Assistance | Active | Thermal SMA | Compliant | up to 1.32 Nm | 2 | Flex/Extension | 38°/50° | Encoder | AAN | **4 | 1.9 kg | - |
| ≥ 0.6 Nm | Rad/Ulnar dev. | 34°/35° | Load cell | |||||||||||
| [26] | *- | Rehabilitation | Active | Thermal SMA | Pulley-tendons | *- | 3 | Flex/Extension | **up to 50°/48° | Potentiometer | CPM | **3 | 0.95 kg | *- |
| Rad/Ulnar dev. | **up to 16°/29° | Load cell | ||||||||||||
| Pron/Supination | **up to 52° | |||||||||||||
| [38] | ASR | Rehab/Assistance | Active | Thermal SMA | Tendons | 40 N | 1 | Gripping | - | Load cell | Triggered | **3 | 300 g | - |
| [27] | SMA-wrist exo | Rehabilitation | Active | Thermal SMA | Linkages | ≥ 0.5 Nm | 2 | Flex/Extension | range 50° | Potentiometer | CPM | **4 | 1 kg | 1060 |
| Rad/Ulnar dev. | range 40° | |||||||||||||
| [28] | SCRIPT | Rehabilitation | Passive | Springs | Links, tendons | 0.5-2 Nm | 1 | Flex/Extension | 45°/30° | Potentiometer | - | **4 | 0.65 kg | - |
| [14,29] | *- | Rehabilitation | Active | DC motor | Tendons | 0.4 Nm | 2 | Flex/Extension | All | IMU | CPM | 4 | 0.3 kg | 160 |
| Rad/Ulnar dev. | ||||||||||||||
| [30] | *- | Rehabilitation | Active | Linear DC motor | Leaf springs | 0.26 to 2.47 Nm | 2 | Flex/Extension | 57°/68 | Potentiometer | CPM | **4 | 0.51 kg | - |
| 0.65 Nm | Rad/Ulnar dev. | 40°/14° | ||||||||||||
| Commercial devices | ||||||||||||||
| [31] | JAS wrist | Rehabilitation | Passive | **Springs | Links | - | 1 | Flex/Extension | up to 95° | - | - | 9 | *- | *- |
| [32] | MyoPro orthosis | Rehab/Assistance | Active | DC motor | Likages | 10 to 20 N | 2 | Flex/Extension | improve up to 35° | sEMG | AAN | 9 | 1.8 kg | 10000 |
| Rad/Ulnar dev. | ||||||||||||||
| [35] | Carbonhand | Assistance | Active | DC motor | Bowden cables | **60 N | 1 | Gripping | All | Force (FSR) | AAN | 9 | 0.7 kg | 7000 |
| [35] | Ironhand | Occupational | Active | DC motor | Bowden cables | 80 N | 1 | Gripping | All | Force (FSR) | AAN | 9 | 2.5 kg | 6500 |
| [36] | Paexo wrist | Occupational | Passive | Leaf spring | Elastic | - | *1 | Holding | All | - | - | 9 | *- | 160 |
| [33] | SaeboFlex | Rehabilitation | Passive | Springs | Links, elastics | - | 1 | Flex/Extension | improve up to 6° | - | - | 9 | 1.6 kg | 600 |
Note: * no information; ** hypotised according to its characteristics.
Table 2.
Number of clinical trials, number of subjects involved, age, gender, setting and testing period for each device. The authors wish to emphasise that the information below may not be exhaustive, as it refers only to documentation accessible online, and does not include confidential data held by companies, especially for commercial devices.
Table 2.
Number of clinical trials, number of subjects involved, age, gender, setting and testing period for each device. The authors wish to emphasise that the information below may not be exhaustive, as it refers only to documentation accessible online, and does not include confidential data held by companies, especially for commercial devices.
| Experimental tests conducted on the device in a real environment or laboratory | ||||||
| Reference | Subjects | Age | Gender | Clinical Condition | Setting | Testing Period |
| Research prototypes | ||||||
| [16] | 1 | n.d. | n.d. | Healthy | Lab. | n.d. |
| [13,17] | 15 | 26±3.4 | 7 M, 8 F | Healthy | Lab. | n.d. |
| 2 | 60±8 | M | Stroke | Lab. | n.d. | |
| [18] | 1 | n.d. | n.d. | Healthy | Lab. | n.d. |
| [11] | 4 | 28±4.0 | M | Healthy | Lab. | n.d. |
| [19] | 3 | n.d. | n.d. | Healthy | Lab. | n.d. |
| [20] | 1 | n.d. | n.d. | Healthy | Lab. | n.d. |
| [21] | 5 | n.d. | M | Healthy | Lab. | n.d. |
| [22] | - | n.d. | n.d. | n.d. | Lab. | n.d. |
| [23] | 1 | n.d. | n.d. | Healthy | Lab. | n.d. |
| 3 | 47±10.0 | M | Stroke | Lab. | ||
| [37] | 1 | n.d. | M | Healthy | Lab. | n.d. |
| [34] | - | n.d. | n.d. | n.d. | Lab. | n.d. |
| [24,25] | 5 | n.d. | 3 M, 2 F | Healthy | Lab. | n.d. |
| [26] | - | n.d. | n.d. | n.d. | Lab. | n.d. |
| [38] | 1 | n.d. | M | Healthy | Lab. | n.d. |
| [27] | 3 | n.d. | M | Healthy | Lab. | n.d. |
| [28] | 33 | n.d. | n.d. | Stroke | Lab. | n.d. |
| [14,29] | 1 | n.d. | M | Impaired Hand | Lab. | 60 trials |
| [30] | - | n.d. | n.d. | n.d. | Lab. | n.d. |
| Commercial devices | ||||||
| [31,59,60,61] | 133 | 53±17.6 | 55 M, 78 F | Radius fractures | Clinic | 3-20 weeks |
| [32,62,63,64,65,66,67,68] | 1 | 62 | M | Stroke | Clinic/Home | 3 years |
| 2 | 53±22 | M | SCI | Clinic | 6 weeks | |
| 18 | 55.5±21.5 | 11 M, 7 F | Stroke | Clinic | 1 x day | |
| 13 | 51±19.9 | 5 M, 8 F | 7 Stroke, 6 TBI | Clinic/Home | 18 weeks | |
| 18 | 52.5±14.7 | 13 M, 5 F | Stroke | Home | 3 months | |
| [35,70,71] | 15 | 41.5±23.5 | n.d. | SCI | Home | 12 weeks |
| 63 | 54±36 | n.d. | Impaired Hand | Home | 6 weeks | |
| [35,72] | 8 | n.d. | 4 M, 4 F | Healthy | Industry | 2 weeks |
| [36] | - | n.d. | n.d. | n.d. | Industry | n.d. |
| [33,56,74,75,76,77,78] | 10 | n.d. | 7 M, 3 F | Stroke | Clinic | 4 weeks |
| 8 | 70±15 | 4 M, 4 F | Stroke | Clinic | 12 weeks | |
| 11 | 60.2±7.89 | 7 M, 5 F | Stroke | Clinic | n.d. | |
| 1 | 43 | F | Stroke | Clinic | 16 weeks | |
| n.d. = Not Defined | ||||||
| M = Male | ||||||
| F = Female | ||||||
Author Contributions
Conceptualization, R.F.P., D.P., G.B., J.O.; methodology, R.F.P., D.P., G.B., J.O.; formal analysis, R.F.P., D.P.; investigation, R.F.P.; resources, R.F.P.; writing—original draft preparation, R.F.P.; writing—review and editing, R.F.P., D.P., D.C., G.B., J.O.; visualization, D.P., D.C., G.B., J.O.; supervision, D.P., D.C., G.B., J.O.; project administration, D.C., J.O.; funding acquisition, D.C., J.O. All authors have read and agreed to the published version of the manuscript.
Funding
This work is funded by the Italian Workers’ Compensation Authority (INAIL).
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to the pure use of literature to obtain the results.
Informed Consent Statement
Not applicable since this study did not involve humans.
Data Availability Statement
Data sharing is not applicable to this review paper. No new data were created in this study.
Acknowledgments
Our thanks go to INAIL (Italian Worker’s Compensation Authority) for its ongoing support, collaboration and funding in the development of novel types of industrial exoskeletons, under the project Collaborative Exoskeletons-EC-2 in collaboration with Istituto Italiano di Tecnologia (IIT) and the University of Genoa.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MSD | Musculoskeletal Disorder |
| WRMSD | Work-Related Musculoskeletal Disorder |
| WHO | World Health Organization |
| INAIL | Italian’s Workers Compensatory Authority |
| DARPA | Defense Advanced Research Projects Agency |
| OE | Occupational Exoskeletons |
| CTS | Carpal Tunnel Syndrome |
| DoF | Degree of Freedom |
| RoM | Range of Motion |
| CoR | Centre of Rotation |
| ADL | Activities of Daily Living |
| DTM | Dart Throwing Motion |
| TRL | Technology Readiness Level |
| ICR | Instantaneous Centre of Rotation |
| OA | Hand Osteoarthritis |
| HAL | Hand Activity Level |
| IMU | Inertial Magnetic Unit |
| FSR | Force Resistive Sensor |
| sEMG | Surface Electromyography signals |
| CPM | Continuous Passive Motion |
| AAN | Assistance-As-Needed |
| ML | Machine Learning |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| WearRA | Wearable Robotics Association |
| SEM | Soft Extra Muscle |
| SCI | Spinal Cord Injury |
| JAS | Joint Active Systems Inc. |
| PWE | Portable Wrist Exoskeleton |
| NN | Neural Network |
| SVM | Support Vector Machine |
| FMG | Force-myography signal |
| CIMT | Constraint-Induced Movement Therapy |
| MVC | Maximum Voluntary Contraction |
| SOA | Soft Origami Actuator |
| PMA | Pneumatic Muscle Actuator |
| SMA | Shape Memory Alloy |
| SWA | Soft Wrist Assist |
| RMSE | Root Means Squared Error |
| SPS | Static Progressive Stretch |
| TBI | Traumatic Brain Injury |
| OT | Occupational Therapy |
References
- Gonçalves, H.; Cardoso, A.; Mattos, D.; Deola Borges, G.; Anacleto, P.; Colim, A.; Carneiro, P.; Arezes, P.M. Assessment of Work-Related Musculoskeletal Disorders by Observational Methods in Repetitive Tasks—A Systematic Review. Occupational and Environmental Safety and Health III 2022, 455–463. [Google Scholar] [CrossRef]
- Ramazzini, B. De morbis artificum diatriba [diseases of workers]. American journal of public health 2001, 91, 1380–1382. [Google Scholar] [CrossRef]
- Armstrong, T.J.; Fine, L.J.; Goldstein, S.A.; Lifshitz, Y.R.; Silverstein, B.A. Ergonomics considerations in hand and wrist tendinitis. The Journal of hand surgery 1987, 12, 830–837. [Google Scholar] [CrossRef]
- Sluiter, J.K.; Rest, K.M.; Frings-Dresen, M.H. Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorders. Scandinavian journal of work, environment & health 2001, pp. 1–102. http://www.jstor.org/stable/40967163.
- Franco, G.; Franco, F. Bernardino Ramazzini: The father of occupational medicine. American Journal of Public Health 2001, 91, 1382–1382. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Musculoskeletal conditions, Key facts. https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions, 2021.
- INAIL-Italian Workers’ Compensatory Authority). OCCUPATIONAL EXOSKELETONS:WEARABLE ROBOTIC DEVICES TO PREVENT WORK RELATED MUSCULOSKELETAL DISORDERS IN THE WORKPLACE OF THE FUTURE, 2020. Available online:http://www.osha.europa.eu.
- European Agency for Safety and Health at Work (EU-OSHA). Work-related musculoskeletal disorders – Facts and figures. Standard, European Agency for Safety and Health at Work (EU-OSHA), Publications Office of the European Union, Luxembourg, 2020. [CrossRef]
- Pons, J.L. Wearable robots: biomechatronic exoskeletons; John Wiley & Sons, 2008; pp. 4,11,219,332. ISBN:9780470512944.
- Du Plesis, T.; et al. Review of Active Hand Exoskeletons for Rehabilitation and Assistance. Robotics 2021, 10, 1–42. [Google Scholar] [CrossRef]
- Chiaradia, D.; Tiseni, L.; Xiloyannis, M.; Solazzi, M.; Masia, L.; Frisoli, A. An assistive soft wrist exosuit for flexion movements with an ergonomic reinforced glove. Frontiers in Robotics and AI 2021, 7, 595862. [Google Scholar] [CrossRef]
- Crea, S.; Beckerle, P.; De Looze, M.; De Pauw, K.; Grazi, L.; Kermavnar, T.; Masood, J.; O’Sullivan, L.W.; Pacifico, I.; Rodriguez-Guerrero, C.; et al. Occupational exoskeletons: A roadmap toward large-scale adoption. Methodology and challenges of bringing exoskeletons to workplaces. Wearable Technologies 2021, 2. [Google Scholar] [CrossRef]
- Lambelet, C.; Temiraliuly, D.; Siegenthaler, M.; Wirth, M.; Woolley, D.G.; Lambercy, O.; Gassert, R.; Wenderoth, N. Characterization and wearability evaluation of a fully portable wrist exoskeleton for unsupervised training after stroke. Journal of NeuroEngineering and Rehabilitation 2020, 17, 1–16. [Google Scholar] [CrossRef]
- Dragusanu, M.; Iqbal, M.Z.; Baldi, T.L.; Prattichizzo, D.; Malvezzi, M. Design, Development, and Control of a Hand/Wrist Exoskeleton for Rehabilitation and Training. IEEE Transactions on Robotics 2022. [Google Scholar] [CrossRef]
- Pitzalis, R.F.; Park, D.; Caldwell, D.G.; Berselli, G.; Ortiz, J. State of the Art in Wearable Wrist Exoskeletons Part I: Background Needs and Design Requirements. Machines 2023, 11, 458. [Google Scholar] [CrossRef]
- Xiao, Z.G.; Menon, C. Towards the development of a portable wrist exoskeleton. 2011 IEEE International Conference on Robotics and Biomimetics. IEEE, 2011, pp. 1884–1889. [CrossRef]
- Lambelet, C.; Lyu, M.; Woolley, D.; Gassert, R.; Wenderoth, N. The eWrist—A wearable wrist exoskeleton with sEMG-based force control for stroke rehabilitation. 2017 International Conference on Rehabilitation Robotics (ICORR). IEEE, 2017, pp. 726–733. [CrossRef]
- Sangha, S.; Elnady, A.M.; Menon, C. A compact robotic orthosis for wrist assistance. 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob). IEEE, 2016, pp. 1080–1085. [CrossRef]
- Choi, H.; Kang, B.B.; Jung, B.K.; Cho, K.J. Exo-wrist: A soft tendon-driven wrist-wearable robot with active anchor for dart-throwing motion in hemiplegic patients. IEEE Robotics and Automation Letters 2019, 4, 4499–4506. [Google Scholar] [CrossRef]
- Bartlett, N.W.; Lyau, V.; Raiford, W.A.; Holland, D.; Gafford, J.B.; Ellis, T.D.; Walsh, C.J. A soft robotic orthosis for wrist rehabilitation. Journal of Medical Devices 2015, 9. [Google Scholar] [CrossRef]
- Sasaki, D.; Noritsugu, T.; Takaiwa, M. Development of active support splint driven by pneumatic soft actuator (ASSIST). Proceedings of the 2005 IEEE international conference on robotics and automation. IEEE, 2005, pp. 520–525. [CrossRef]
- Liu, S.; Fang, Z.; Liu, J.; Tang, K.; Luo, J.; Yi, J.; Hu, X.; Wang, Z. A compact soft robotic wrist brace with origami actuators. Frontiers in Robotics and AI 2021, 34. [Google Scholar] [CrossRef]
- Li, N.; Yang, T.; Yang, Y.; Yu, P.; Xue, X.; Zhao, X.; Song, G.; Elhajj, I.H.; Wang, W.; Xi, N.; et al. Bioinspired musculoskeletal model-based soft wrist exoskeleton for stroke rehabilitation. Journal of Bionic Engineering 2020, 17, 1163–1174. [Google Scholar] [CrossRef]
- Jeong, J.; Yasir, I.B.; Han, J.; Park, C.H.; Bok, S.K.; Kyung, K.U. Design of shape memory alloy-based soft wearable robot for assisting wrist motion. Applied Sciences 2019, 9, 4025. [Google Scholar] [CrossRef]
- Jeong, J.; Hyeon, K.; Han, J.; Park, C.H.; Ahn, S.Y.; Bok, S.K.; Kyung, K.U. Wrist assisting soft wearable robot with stretchable coolant vessel integrated SMA muscle. IEEE/ASME Transactions on Mechatronics 2021, 27, 1046–1058. [Google Scholar] [CrossRef]
- Hope, J.; McDaid, A. Development of wearable wrist and forearm exoskeleton with shape memory alloy actuators. Journal of Intelligent & Robotic Systems 2017, 86, 397. [Google Scholar] [CrossRef]
- Serrano, D.; Copaci, D.S.; Moreno, L.; Blanco, D. SMA based wrist exoskeleton for rehabilitation therapy. 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS). IEEE, 2018, pp. 2318–2323. [CrossRef]
- Ates, S.; Haarman, C.J.; Stienen, A.H. SCRIPT passive orthosis: design of interactive hand and wrist exoskeleton for rehabilitation at home after stroke. Autonomous Robots 2017, 41, 711–723. [Google Scholar] [CrossRef]
- Dragusanu, M.; Baldi, T.L.; Iqbal, Z.; Prattichizzo, D.; Malvezzi, M. Design, development, and control of a tendon-actuated exoskeleton for wrist rehabilitation and training. 2020 IEEE International Conference on Robotics and Automation (ICRA). IEEE, 2020, pp. 1749–1754. [CrossRef]
- Higuma, T.; Kiguchi, K.; Arata, J. Low-profile two-degree-of-freedom wrist exoskeleton device using multiple spring blades. IEEE Robotics and Automation Letters 2017, 3, 305–311. [Google Scholar] [CrossRef]
- JAS-Joint Active Systems. JAS Wrist. https://www.jointactivesystems.com/products/areas/wrist, 2017. Online; accessed 5th of August 2022.
- Myomo Inc.. MyoPro Orthosis. https://myomo.com/what-is-a-myopro-orthosis/, 2006. Online; accessed 8th of August 2022.
- Saebo Inc.. SaeboFlex. https://www.saebo.com/shop/saeboflex/. Last accessed 30th of November 2022.
- Zhu, M.; Adams, W.; Polygerinos, P. Carpal tunnel syndrome soft relief device for typing applications. Frontiers in Biomedical Devices. American Society of Mechanical Engineers, 2017, Vol. 40672, p. V001T03A003. [CrossRef]
- Bioservo Technologies. Bioservo Strength for life - Professional and Healthcare. https://www.bioservo.com/. Last accessed 7th of September 2022.
- Ottobock. Paexo Wrist Exoskeleton. https://paexo.com/paexo-wrist/?lang=it. Last accessed 5th of August 2022.
- Andrikopoulos, G.; Nikolakopoulos, G.; Manesis, S. Motion control of a novel robotic wrist exoskeleton via pneumatic muscle actuators. 2015 IEEE 20th Conference on Emerging Technologies & Factory Automation (ETFA). IEEE, 2015, pp. 1–8. [CrossRef]
- Hadi, A.; Alipour, K.; Kazeminasab, S.; Elahinia, M. ASR glove: A wearable glove for hand assistance and rehabilitation using shape memory alloys. Journal of Intelligent Material Systems and Structures 2018, 29, 1575–1585. [Google Scholar] [CrossRef]
- Ferguson, R.; et al. Wrist pain: a systematic review of prevalence and risk factors–what is the role of occupation and activity? BMC Musculoskeletal Disorders 2019, 20. [Google Scholar] [CrossRef]
- Noronha, B.; Accoto, D. Exoskeletal devices for hand assistance and rehabilitation: A comprehensive analysis of state-of-the-art technologies. IEEE Transactions on Medical Robotics and Bionics 2021, 3, 525–538. [Google Scholar] [CrossRef]
- Gopura, R.; Kiguchi, K. Mechanical designs of active upper-limb exoskeleton robots: State-of-the-art and design difficulties. 2009 IEEE International Conference on Rehabilitation Robotics. IEEE, 2009, pp. 178–187. [CrossRef]
- Gopura, R.; Bandara, D.; Kiguchi, K.; Mann, G.K. Developments in hardware systems of active upper-limb exoskeleton robots: A review. Robotics and Autonomous Systems 2016, 75, 203–220. [Google Scholar] [CrossRef]
- Nikhil, G.; Yedukondalu, G.; Rao, S. Robotic exoskeletons: a review on development. International Journal of Mechanical and Production Engineering Research and Development 2019, 9, 529–542, https://archive.org/details/52.ijmperdaug201952. [Google Scholar]
- Tiboni, M.; Borboni, A.; Vérité, F.; Bregoli, C.; Amici, C. Sensors and actuation technologies in exoskeletons: A review. Sensors 2022, 22, 884. [Google Scholar] [CrossRef]
- Hussain, S.; Jamwal, P.K.; Van Vliet, P.; Ghayesh, M.H. State-of-the-art robotic devices for wrist rehabilitation: Design and control aspects. IEEE Transactions on Human-Machine Systems 2020, 50, 361–372. [Google Scholar] [CrossRef]
- Cornejo, J.; Huamanchahua, D.; Huamán-Vizconde, S.; Terrazas-Rodas, D.; Sierra-Huertas, J.; Janampa-Espinoza, A.; Gonzáles, J.; Cardona, M. Mechatronic exoskeleton systems for supporting the biomechanics of shoulder-elbow-wrist: An innovative review. 2021 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS). IEEE, 2021, pp. 1–9. [CrossRef]
- Khokhar, Z.O.; Xiao, Z.G.; Menon, C. Surface EMG pattern recognition for real-time control of a wrist exoskeleton. Biomedical engineering online 2010, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Vardakastani, V.; Bell, H.; Mee, S.; Brigstocke, G.; Kedgley, A.E. Clinical measurement of the dart throwing motion of the wrist: variability, accuracy and correction. Journal of Hand Surgery (European Volume) 2018, 43, 723–731. [Google Scholar]
- Braidotti, F.; Atzei, A.; Fairplay, T. Dart-Splint: an innovative orthosis that can be integrated into a scapho-lunate and palmar midcarpal instability re-education protocol. Journal of Hand Therapy 2015, 28, 329–335. [Google Scholar] [CrossRef]
- Kaufman-Cohen, Y.; Friedman, J.; Levanon, Y.; Jacobi, G.; Doron, N.; Portnoy, S. Wrist plane of motion and range during daily activities. The American Journal of Occupational Therapy 2018, 72, 7206205080p1–7206205080p10. [Google Scholar] [CrossRef]
- Brigstocke, G.; Hearnden, A.; Holt, C.; Whatling, G. In-vivo confirmation of the use of the dart thrower’s motion during activities of daily living. Journal of Hand Surgery (European Volume) 2014, 39, 373–378. [Google Scholar]
- Borislav, M. The Number Of Companies Making Industrial Exoskeletons Has Been Quietly Increasing For The Past Five Years. https://www.forbes.com/sites/borislavmarinov/2020/09/24/the-number-of-companies-making-industrial-exoskeletons-has-been-quietly-increasing-for-the-past-five-years/?sh=231b1c067bf4, 2020. Last accessed 5th of August 2022.
- Borislav, M. Updated Directory of Exoskeleton Companies and Industry Statistics. https://exoskeletonreport.com/2021/12/updated-directory-of-exoskeleton-companies-and-industry-statistics/, 2021. Last accessed 5th of August 2022.
- Radder, B.; Prange-Lasonder, G.B.; Kottink, A.I.; Holmberg, J.; Sletta, K.; van Dijk, M.; Meyer, T.; Melendez-Calderon, A.; Buurke, J.H.; Rietman, J.S. Home rehabilitation supported by a wearable soft-robotic device for improving hand function in older adults: A pilot randomized controlled trial. PloS one 2019, 14, e0220544. [Google Scholar] [CrossRef]
- Hyttinge, M.; Einarsson, F. Bioservo Technologies. Technical report, Redeye, Equity Research and Investment Banking Company, 2021.
- Moskiewicz, D.; Mraz, M.; Chamela-Bilińska, D. Botulinum Toxin and Dynamic Splint Restore Grasping Function after Stroke: A Case Report. International Journal of Environmental Research and Public Health 2023, 20, 4873. [Google Scholar] [CrossRef] [PubMed]
- Lucado, A.M.; Li, Z.; Russell, G.B.; Papadonikolakis, A.; Ruch, D.S. Changes in impairment and function after static progressive splinting for stiffness after distal radius fracture. Journal of Hand Therapy 2008, 21, 319–325. [Google Scholar] [CrossRef]
- Lucado, A.M.; Li, Z. Static progressive splinting to improve wrist stiffness after distal radius fracture: a prospective, case series study. Physiotherapy theory and practice 2009, 25, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Berner, S.H.; Willis, F.B. Dynamic splinting in wrist extension following distal radius fractures. Journal of orthopaedic surgery and research 2010, 5, 1–4. [Google Scholar] [CrossRef]
- Schwartz, D.A. Static progressive orthoses for the upper extremity: a comprehensive literature review. Hand 2012, 7, 10–17. [Google Scholar] [CrossRef]
- Sodhi, N.; Yao, B.; Anis, H.K.; Khlopas, A.; Sultan, A.A.; Newman, J.M.; Mont, M.A. Patient satisfaction and outcomes of static progressive stretch bracing: a 10-year prospective analysis. Annals of Translational Medicine 2019, 7. [Google Scholar] [CrossRef]
- Dunaway, S.; Dezsi, D.B.; Perkins, J.; Tran, D.; Naft, J. Case report on the use of a custom myoelectric elbow–wrist–hand orthosis for the remediation of upper extremity paresis and loss of function in chronic stroke. Military medicine 2017, 182, e1963–e1968. [Google Scholar] [CrossRef]
- Androwis, G.J.; Engler, A.; Rana, S.; Kirshblum, S.; Yue, G.H. The Rehabilitation Effects of Myoelectric Powered Wearable Orthotics on Improving Upper Extremity Function in Persons with SCI. 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). IEEE, 2021, pp. 4944–4948.
- Androwis, G.J.; Engler, A.; Rana, S.; Kirshblum, S.; Yue, G. Upper Extremity Functional Improvements in Persons with SCI Resulted from Daily Utilization of Myoelectric Powered Wearable Orthotics. 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). IEEE, 2021, pp. 4949–4952.
- Hoppe-Ludwig, S.; Armitage, J.; Turner, K.L.; O’Brien, M.K.; Mummidisetty, C.K.; Koch, L.M.; Kocherginsky, M.; Jayaraman, A. Usability, functionality, and efficacy of a custom myoelectric elbow-wrist-hand orthosis to assist elbow function in individuals with stroke. Journal of Rehabilitation and Assistive Technologies Engineering 2021, 8, 20556683211035057. [Google Scholar] [CrossRef] [PubMed]
- Pundik, S.; McCabe, J.; Skelly, M.; Salameh, A.; Naft, J.; Chen, Z.; Tatsuoka, C.; Fatone, S. Myoelectric Arm Orthosis in Motor Learning-Based Therapy for Chronic Deficits After Stroke and Traumatic Brain Injury. Frontiers in Neurology 2022, 13, 19. [Google Scholar] [CrossRef]
- Chang, S.R.; Hofland, N.; Chen, Z.; Tatsuoka, C.; Richards, L.G.; Bruestle, M.; Kovelman, H.; Naft, J. Myoelectric Arm Orthosis Assists Functional Activities: A 3-Month Home Use Outcome Report. Archives of Rehabilitation Research and Clinical Translation 2023, 5, 100279. [Google Scholar] [CrossRef]
- McCabe, J.P.; Henniger, D.; Perkins, J.; Skelly, M.; Tatsuoka, C.; Pundik, S. Feasibility and clinical experience of implementing a myoelectric upper limb orthosis in the rehabilitation of chronic stroke patients: a clinical case series report. PloS one 2019, 14, e0215311. [Google Scholar] [CrossRef]
- Nilsson, M.; Ingvast, J.; Wikander, J.; von Holst, H. The Soft Extra Muscle system for improving the grasping capability in neurological rehabilitation. 2012 IEEE-EMBS conference on biomedical engineering and sciences. IEEE, 2012, pp. 412–417. [CrossRef]
- Osuagwu, B.A.; Timms, S.; Peachment, R.; Dowie, S.; Thrussell, H.; Cross, S.; Heywood, T.; Shirley, R.; Taylor, J. Clinical Trial of the Soft Extra Muscle Glove to Assess Orthotic and Long-Term Functional Gain Following Chronic Incomplete Tetraplegia: Preliminary Functional Results. International Conference on NeuroRehabilitation. Springer, 2018, pp. 385–389. [CrossRef]
- Kottink, A.I.R.; Nikamp, C.D.; Bos, F.P.; van der Sluis, C.K.; van den Broek, M.; Onneweer, B.; Stolwijk-Swüste, J.M.; Brink, S.M.; Voet, N.B.; Buurke, J.B.; et al. Therapeutic Effect of a Soft Robotic Glove for Activities of Daily Living In People With Impaired Hand Strength: Protocol for a Multicenter Clinical Trial (iHand). JMIR research protocols 2022, 11, e34200. [Google Scholar] [CrossRef]
- Cousins, D.; Porto, R.; Bigelo, A.; Fox, R.; Libs, B.; Holmes, M.; Cort, J. Effects of the Ironhand® Soft Exoskeleton on Forearm Muscle Activity During in Field Automotive Assembly Tasks. Available at SSRN 4559929.
- Hoffman, H.B.; Blakey, G.L. New design of dynamic orthoses for neurological conditions. NeuroRehabilitation 2011, 28, 55–61. [Google Scholar] [CrossRef]
- Jeon, H.s.; Woo, Y.K.; Yi, C.h.; Kwon, O.y.; Jung, M.y.; Lee, Y.h.; Hwang, S.; Choi, B.r. Effect of intensive training with a pring-assisted hand orthosis on movement smoothness in upper extremity following stroke: A pilot clinical trial. Topics in stroke rehabilitation 2012, 19, 320–328. [Google Scholar] [CrossRef]
- Stuck, R.A.; Marshall, L.M.; Sivakumar, R. Feasibility of SaeboFlex upper-limb training in acute stroke rehabilitation: a clinical case series. Occupational therapy international 2014, 21, 108–114. [Google Scholar] [CrossRef]
- Andriske, L.; Verikios, D.; Hitch, D.; et al. Patient and therapist experiences of the SaeboFlex: A pilot study. Occupational therapy international 2017, 2017. [Google Scholar] [CrossRef]
- Barry, J.; Saabye, S.; Baker, D.; Fogarty, J.; Beck, K. Effects of the saeboflex® orthosis and a home exercise program on upper extremity recovery in individuals with chronic. Journal of Neurologic Physical Therapy 2006, 30, 207. [Google Scholar] [CrossRef]
- Lannin, N.A.; Cusick, A.; Hills, C.; Kinnear, B.; Vogel, K.; Matthews, K.; Bowring, G. Upper limb motor training using a Saebo™ orthosis is feasible for increasing task-specific practice in hospital after stroke. Australian occupational therapy journal 2016, 63, 364–372. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, J.; Li, Z.; Su, C.Y. Adaptive impedance control of robotic exoskeletons using reinforcement learning. 2016 International Conference on Advanced Robotics and Mechatronics (ICARM). IEEE, 2016, pp. 243–248. [CrossRef]
- Ren, J.L.; Chien, Y.H.; Chia, E.Y.; Fu, L.C.; Lai, J.S. Deep learning based motion prediction for exoskeleton robot control in upper limb rehabilitation. 2019 International Conference on Robotics and Automation (ICRA). IEEE, 2019, pp. 5076–5082. [CrossRef]
- Rose, L.; Bazzocchi, M.C.; Nejat, G. A model-free deep reinforcement learning approach for control of exoskeleton gait patterns. Robotica 2022, 40, 2189–2214. [Google Scholar] [CrossRef]
- Côté-Allard, U.; Fall, C.L.; Drouin, A.; Campeau-Lecours, A.; Gosselin, C.; Glette, K.; Laviolette, F.; Gosselin, B. Deep learning for electromyographic hand gesture signal classification using transfer learning. IEEE transactions on neural systems and rehabilitation engineering 2019, 27, 760–771. [Google Scholar] [CrossRef]
- Theurel, J.; Desbrosses, K. Occupational exoskeletons: overview of their benefits and limitations in preventing work-related musculoskeletal disorders. IISE Transactions on Occupational Ergonomics and Human Factors 2019, 7, 264–280. [Google Scholar] [CrossRef]
- Elprama, S.A.; Vanderborght, B.; Jacobs, A. An industrial exoskeleton user acceptance framework based on a literature review of empirical studies. Applied Ergonomics 2022, 100, 103615. [Google Scholar] [CrossRef]
Figure 1.
The flow chart methodology adopted to identify and screen all information available from online database and conduct our review. This is in line with Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart.
Figure 1.
The flow chart methodology adopted to identify and screen all information available from online database and conduct our review. This is in line with Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart.
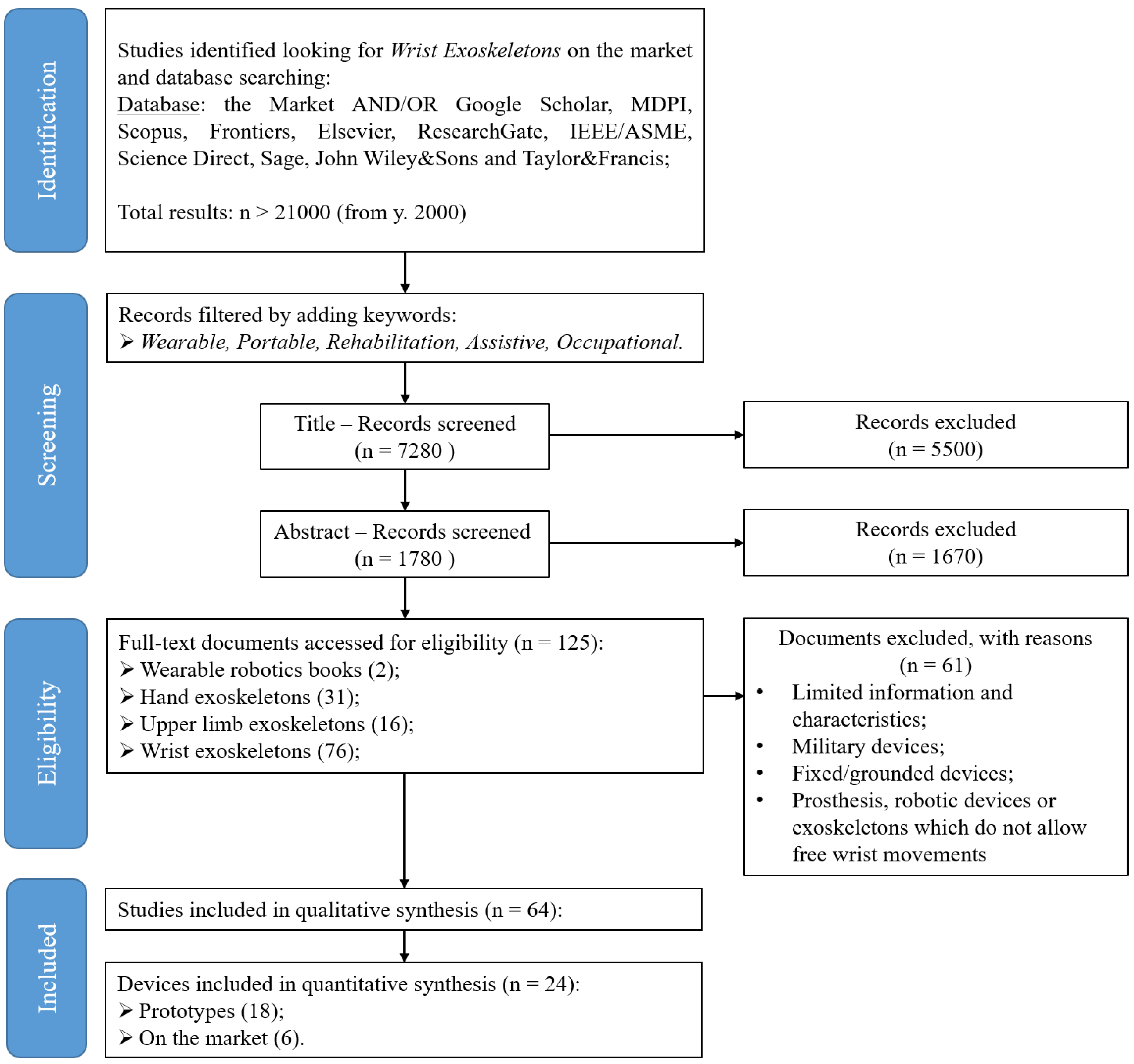
Figure 3.
Schematic of research-wrist exoskeletons grouped by design requirements. Devices, named from a) to s), are the same as reported in Figure 2.
Figure 3.
Schematic of research-wrist exoskeletons grouped by design requirements. Devices, named from a) to s), are the same as reported in Figure 2.
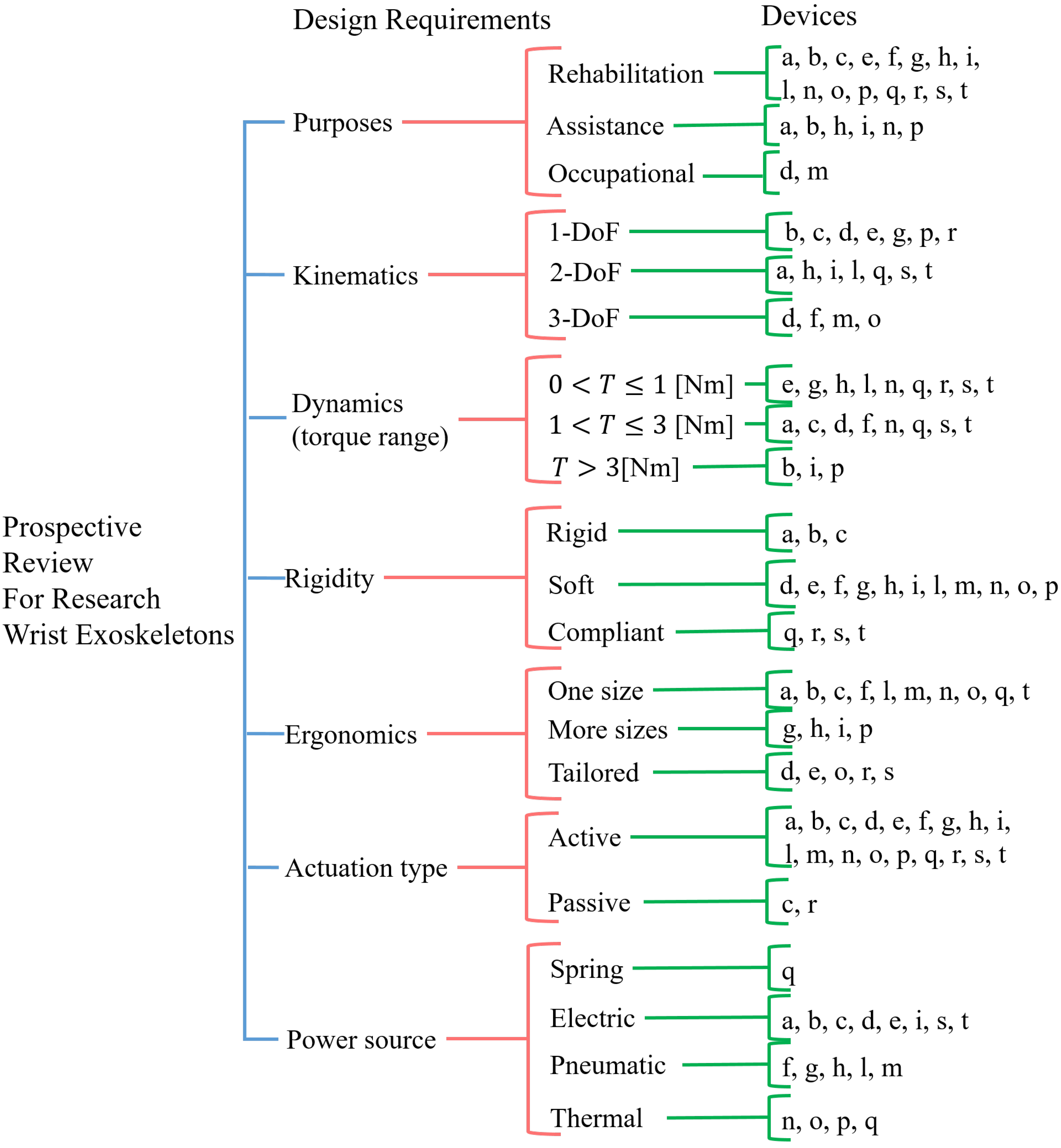
Figure 5.
the eWrist: first attempt prototype of a wrist exoskeleton for rehabilitation and training designed by [13,17]. It is made of a rigid mechanism and powered by a rotary motor placed on a side of the forearm. It is conceived for wrist flexion/extension.
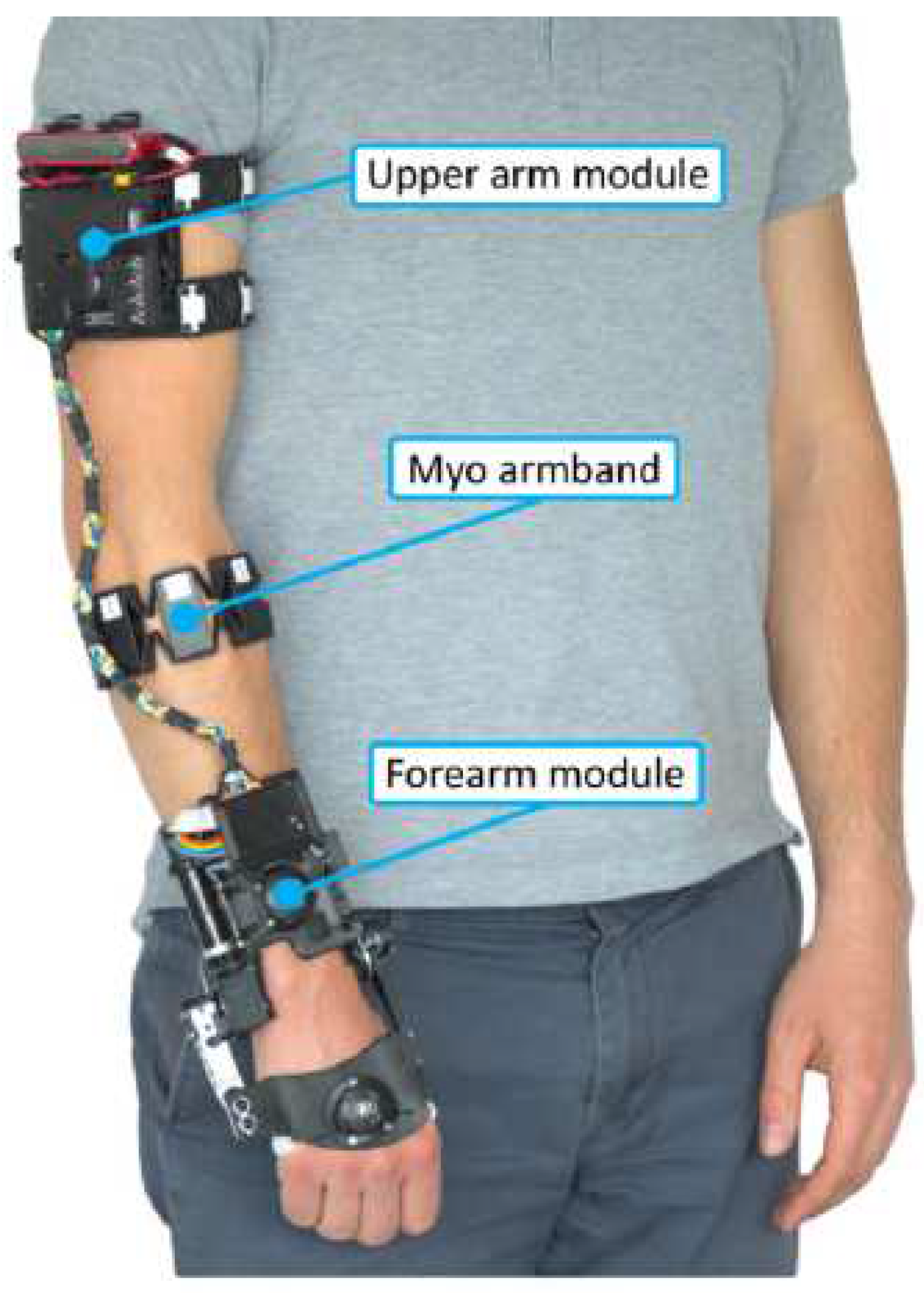
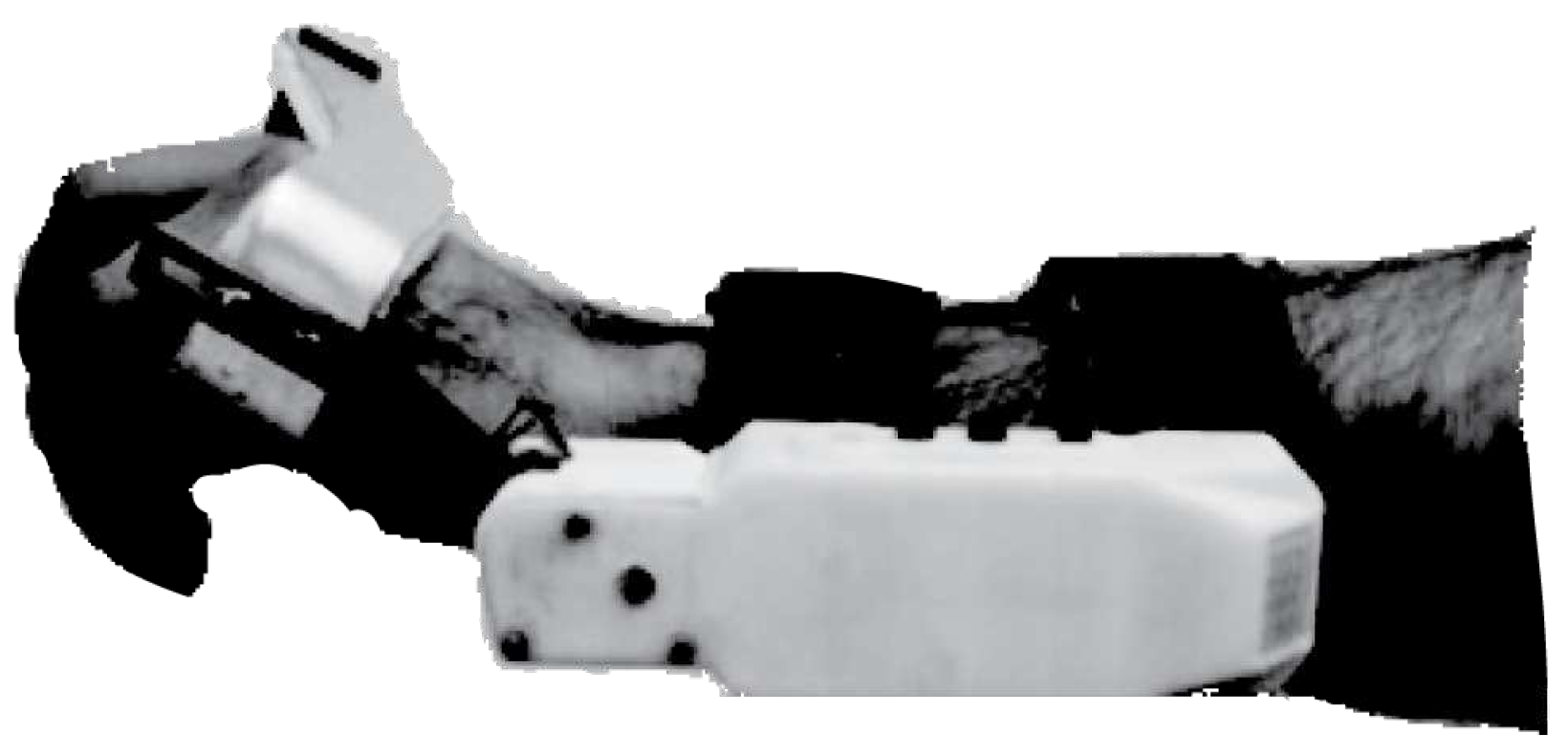
Figure 7.
Soft wrist exosuit designed and developed by [11].
Figure 7.
Soft wrist exosuit designed and developed by [11].
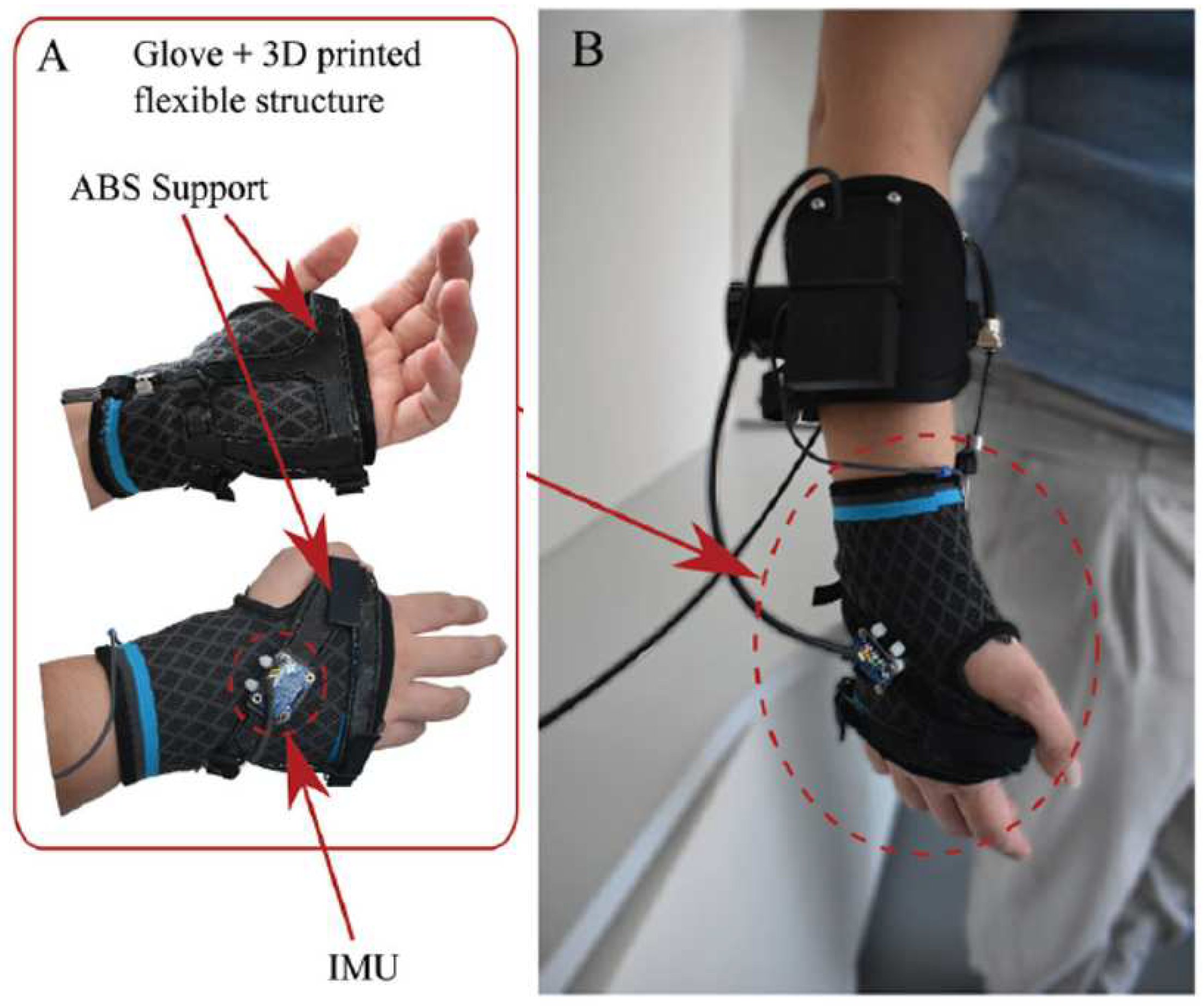
Figure 11.
A robotic wrist brace with origami actuators developed by [22]. The actuators are placed on both the dorsal and palmar hand sides. Their elongation and contraction state are marked respectively as red and blue.
Figure 11.
A robotic wrist brace with origami actuators developed by [22]. The actuators are placed on both the dorsal and palmar hand sides. Their elongation and contraction state are marked respectively as red and blue.
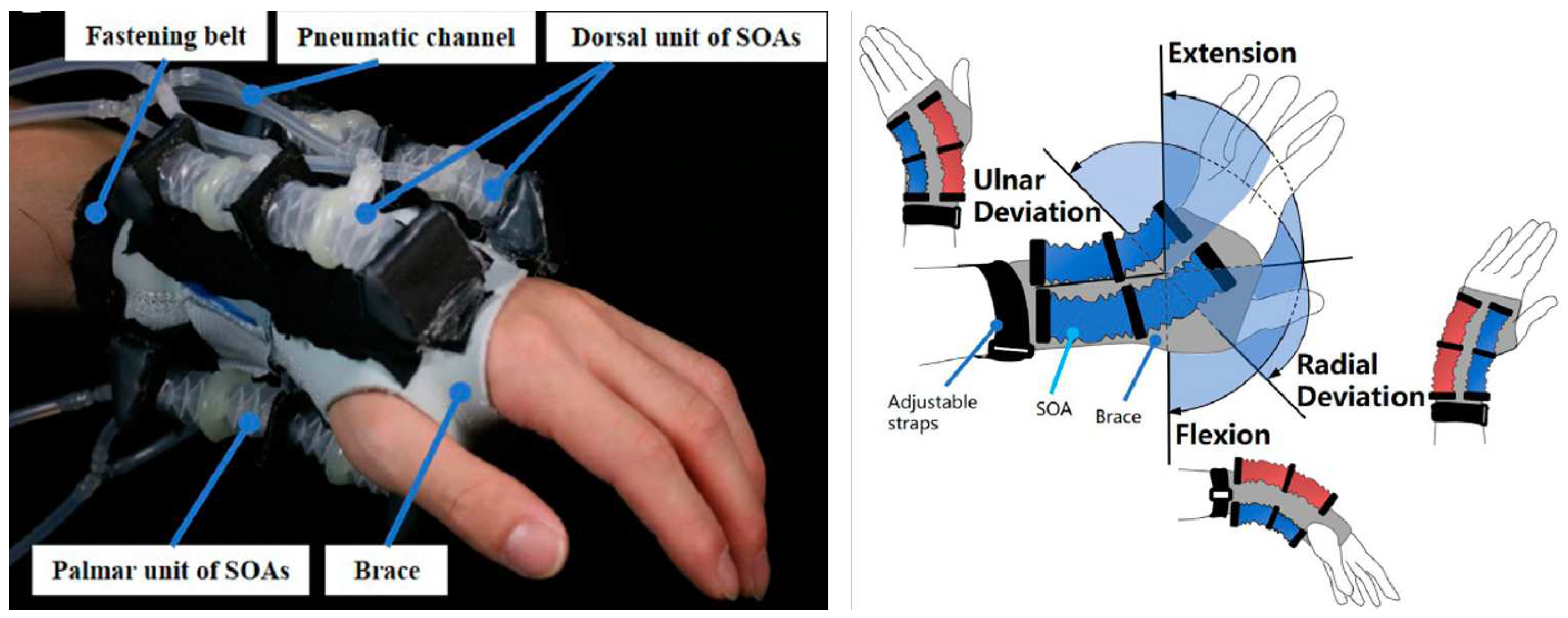
Figure 12.
A soft wrist exoskeleton developed by [23]. The model shown comes from OpenSim simulation software.
Figure 12.
A soft wrist exoskeleton developed by [23]. The model shown comes from OpenSim simulation software.
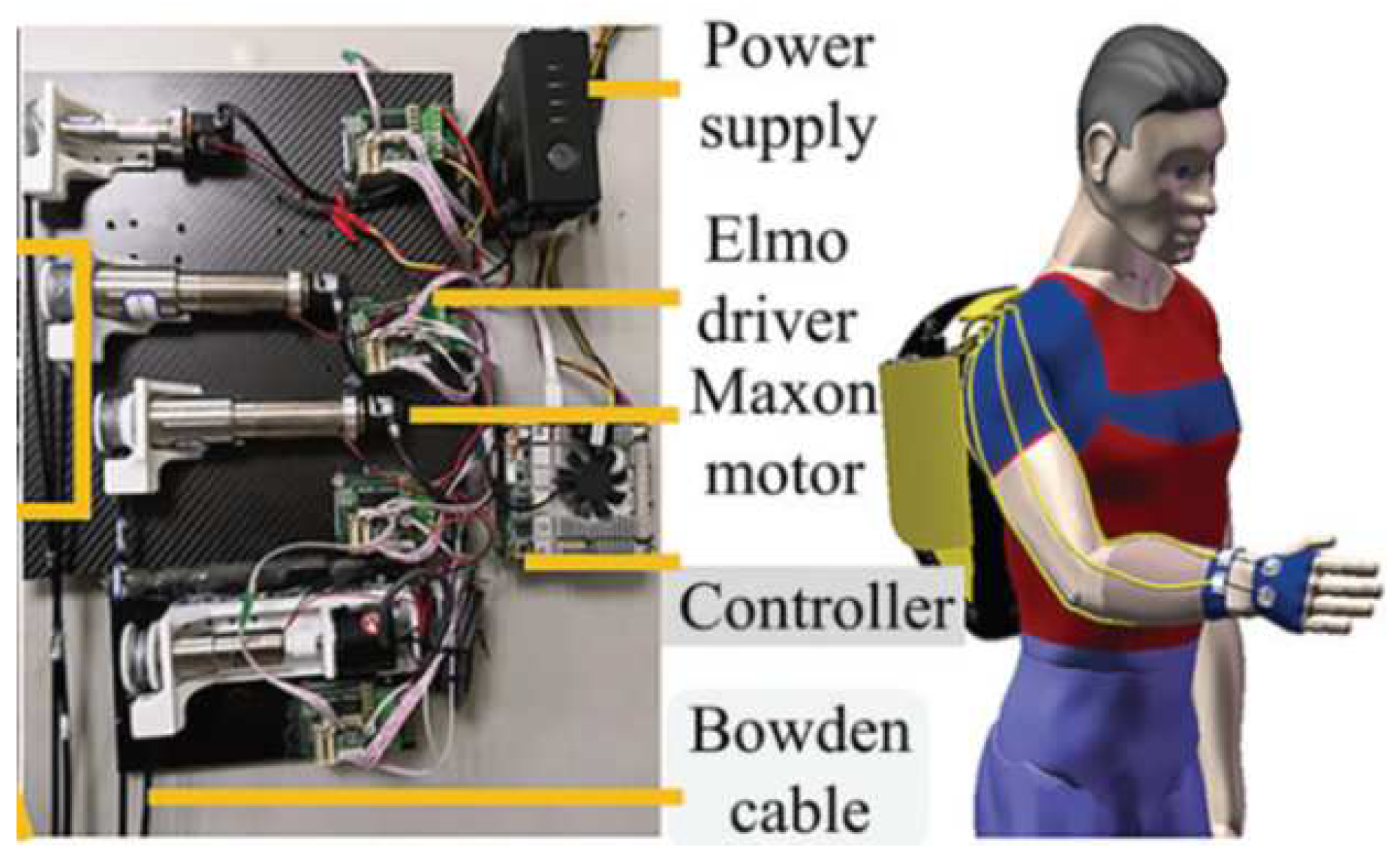
Figure 13.
Soft wrist exoskeleton driven by pneumatic actuators and developed by [37]. Image adapted from [37].
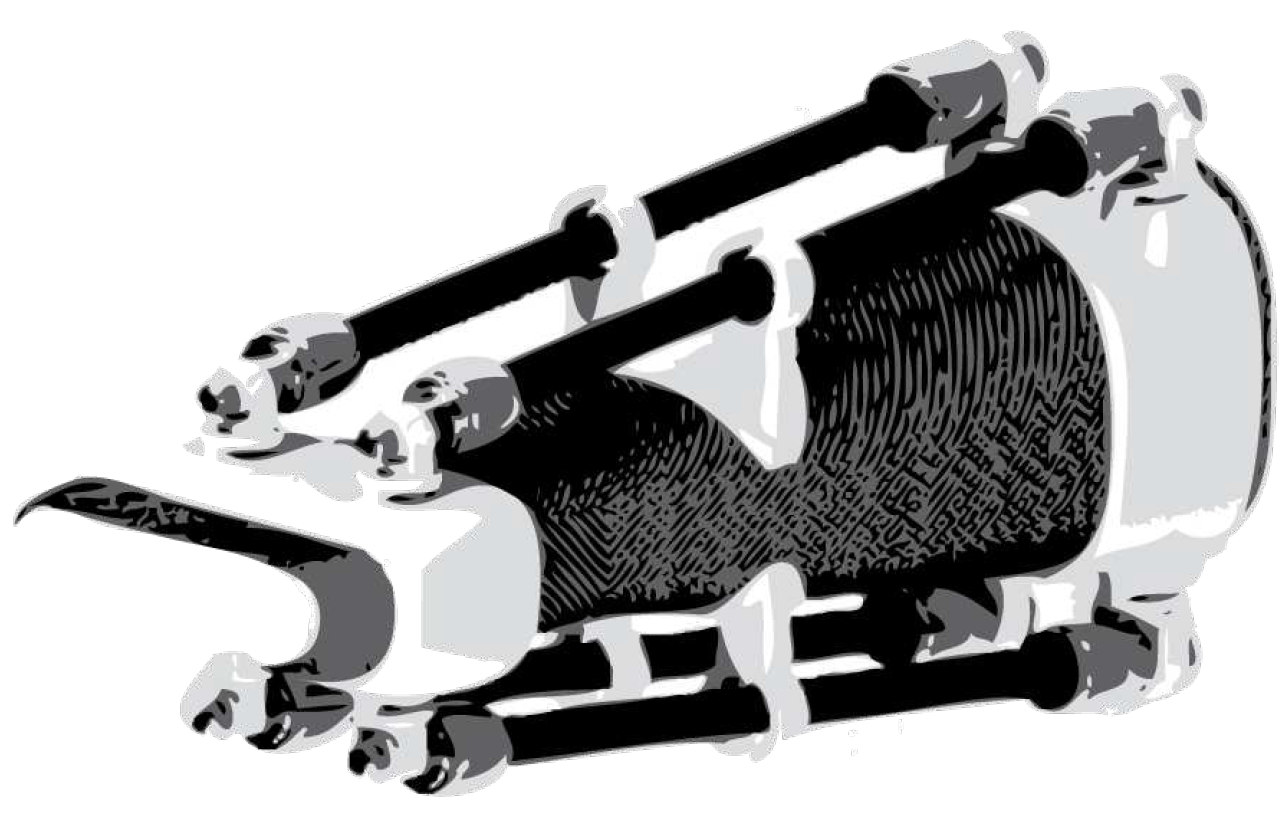
Figure 14.
Soft wrist exoskeleton designed by [34] to alleviate CTS: a) the whole device; b) the airbag actuators.
Figure 14.
Soft wrist exoskeleton designed by [34] to alleviate CTS: a) the whole device; b) the airbag actuators.

Figure 15.
SMA-based wrist wearable robot developed by [24]: a) the real device; b) the SMA actuator design.
Figure 15.
SMA-based wrist wearable robot developed by [24]: a) the real device; b) the SMA actuator design.
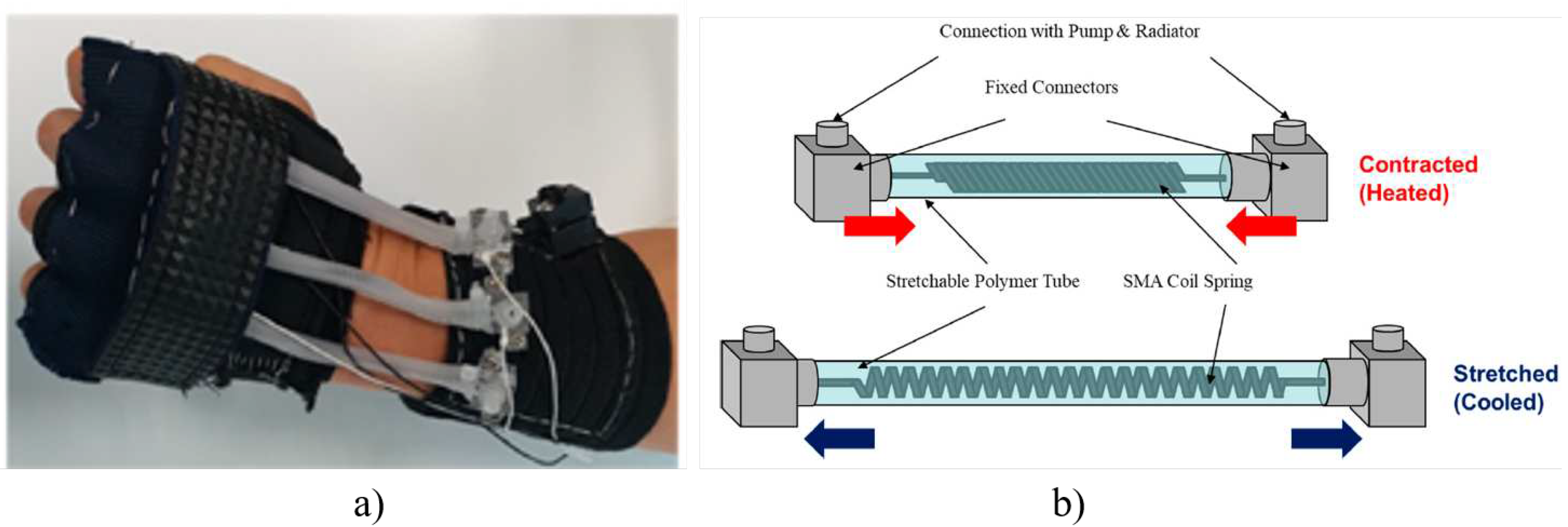
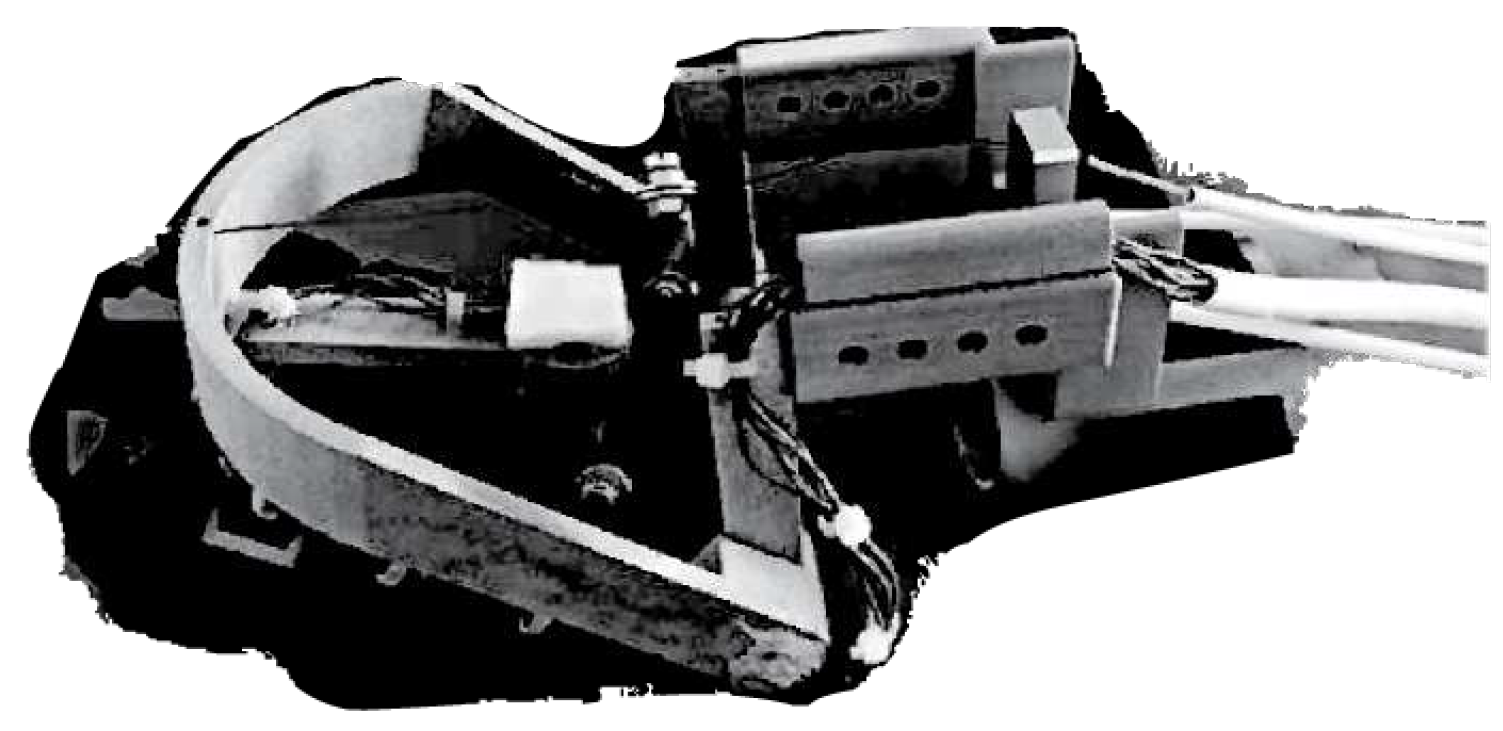
Figure 19.
SCRIPT passive orthosis. The SPO-F design developed by [28].
Figure 19.
SCRIPT passive orthosis. The SPO-F design developed by [28].

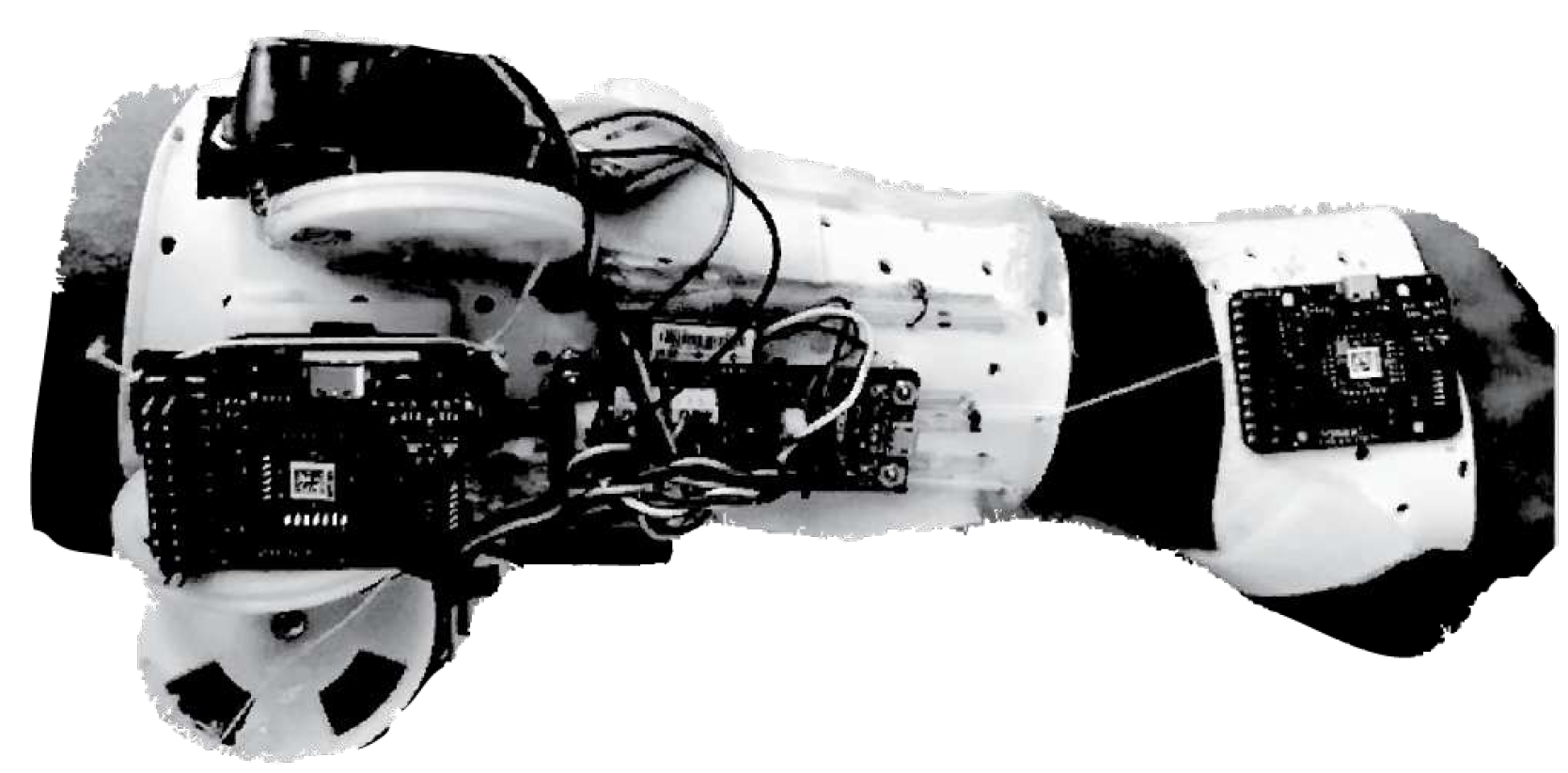
Figure 22.
Statistics from resources available on ExR-ExoskeletonReport website [53].
Figure 22.
Statistics from resources available on ExR-ExoskeletonReport website [53].
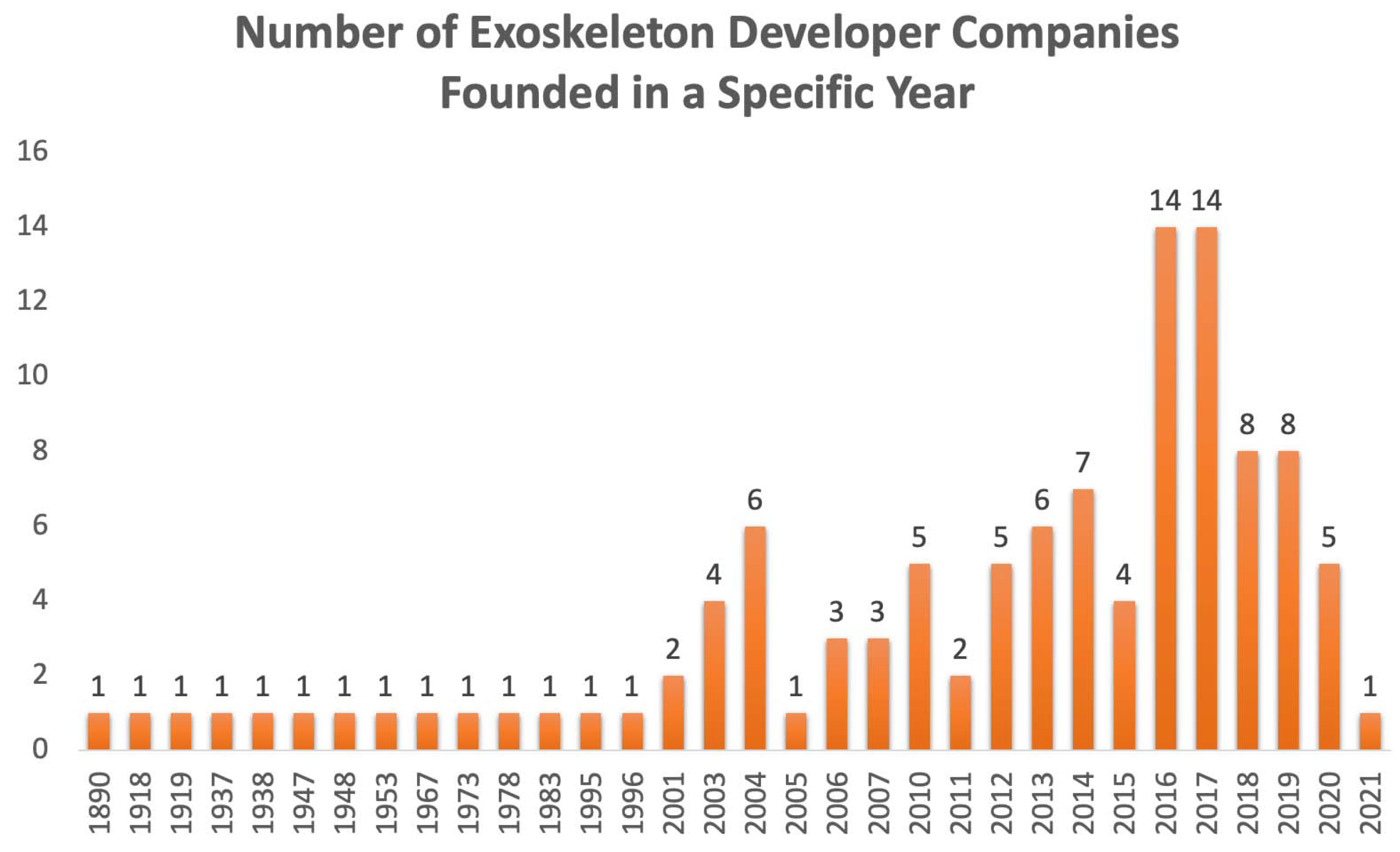
Figure 23.
All commercial wearable exoskeleton for wrist assistance. Devices are grouped by stiffness criteria in: rigid (a,b), soft (c-e) and compliant (f). From top left to bottom right it is possible to find: a) JAS wrists from Joint Active Systems [31]. Re-edited images; b) Myopro designed by Myomo [32]. Image used with the permission of Myomo company;c) CarbonHand designed by Bioservo [54]; d) IronHand designed by Bioservo [55]. Re-edited image; e) Paexo wrist designed by Ottobock [36]. Re-edited image; f) soft orthosis designed by Saebo [56].
Figure 23.
All commercial wearable exoskeleton for wrist assistance. Devices are grouped by stiffness criteria in: rigid (a,b), soft (c-e) and compliant (f). From top left to bottom right it is possible to find: a) JAS wrists from Joint Active Systems [31]. Re-edited images; b) Myopro designed by Myomo [32]. Image used with the permission of Myomo company;c) CarbonHand designed by Bioservo [54]; d) IronHand designed by Bioservo [55]. Re-edited image; e) Paexo wrist designed by Ottobock [36]. Re-edited image; f) soft orthosis designed by Saebo [56].

Figure 24.
Schematic of commercial wrist exoskeletons grouped by design requirements. The devices, named from a) to f), are the same reported in Figure 23.
Figure 24.
Schematic of commercial wrist exoskeletons grouped by design requirements. The devices, named from a) to f), are the same reported in Figure 23.
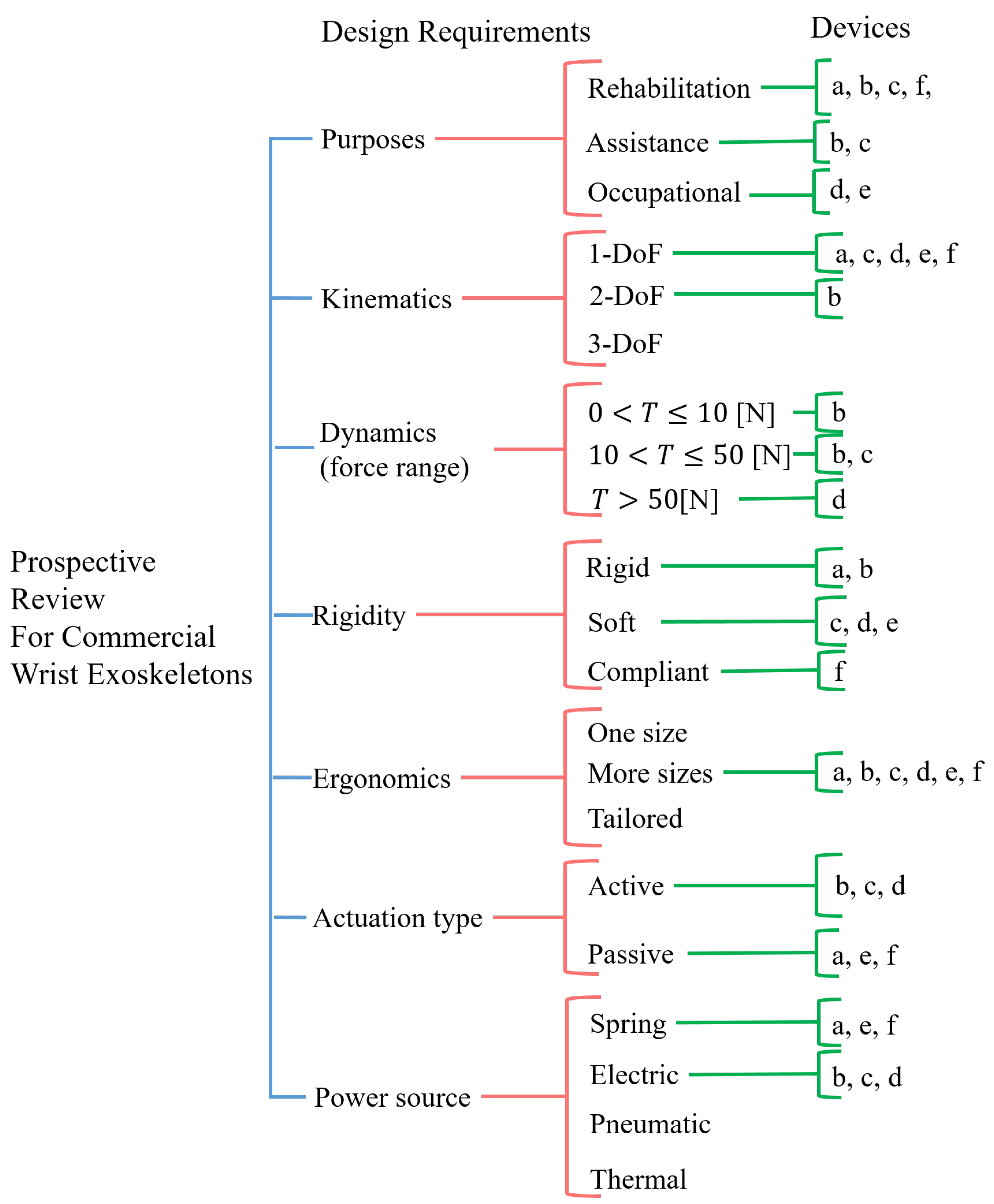
Figure 25.
Dynamic Wrist orthosis for wrist flexion and extension recovery by JAS Inc. [31]. Re-edited image.
Figure 25.
Dynamic Wrist orthosis for wrist flexion and extension recovery by JAS Inc. [31]. Re-edited image.

Figure 26.
MyoPro device by Myomo Inc. [32]. Images reproduced by permission of the company.
Figure 26.
MyoPro device by Myomo Inc. [32]. Images reproduced by permission of the company.
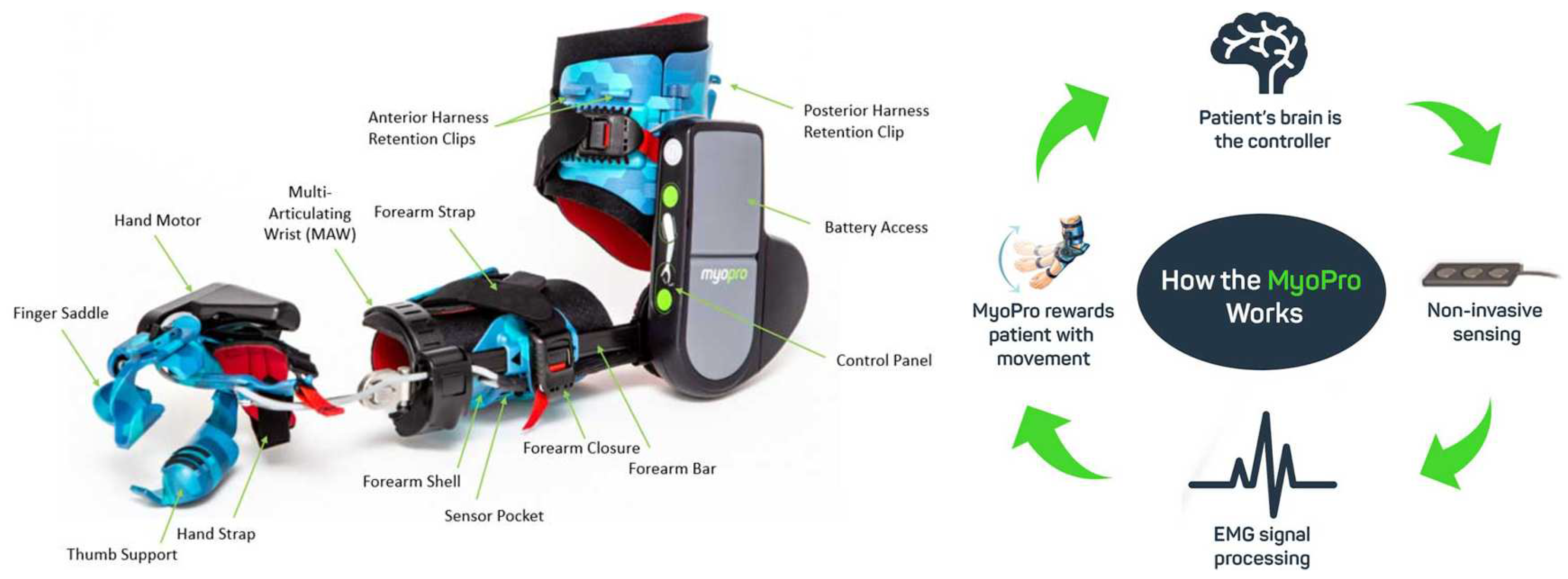
Figure 28.
Bioservo IronHand® system and application. Image revised from [35].
Figure 28.
Bioservo IronHand® system and application. Image revised from [35].
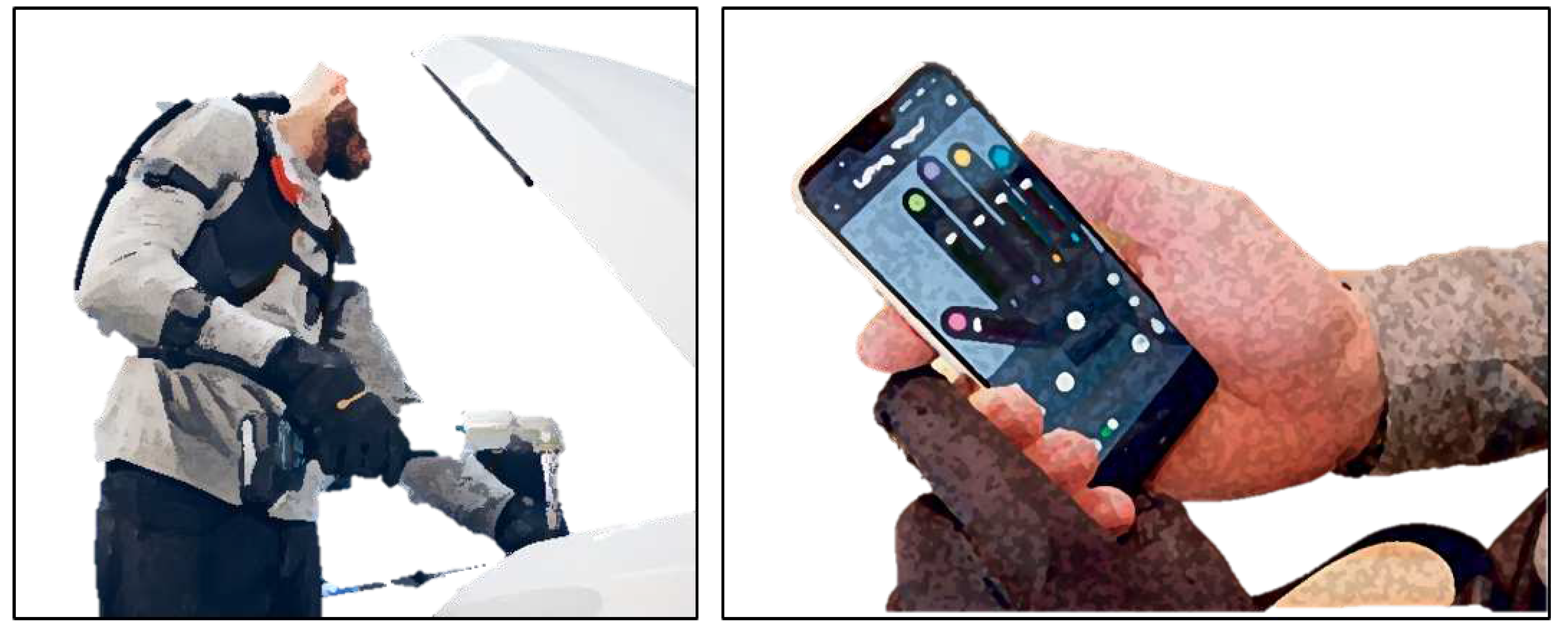
Figure 29.
Bioservo IronHand® system control and connectivity. Image revised from [55].
Figure 29.
Bioservo IronHand® system control and connectivity. Image revised from [55].
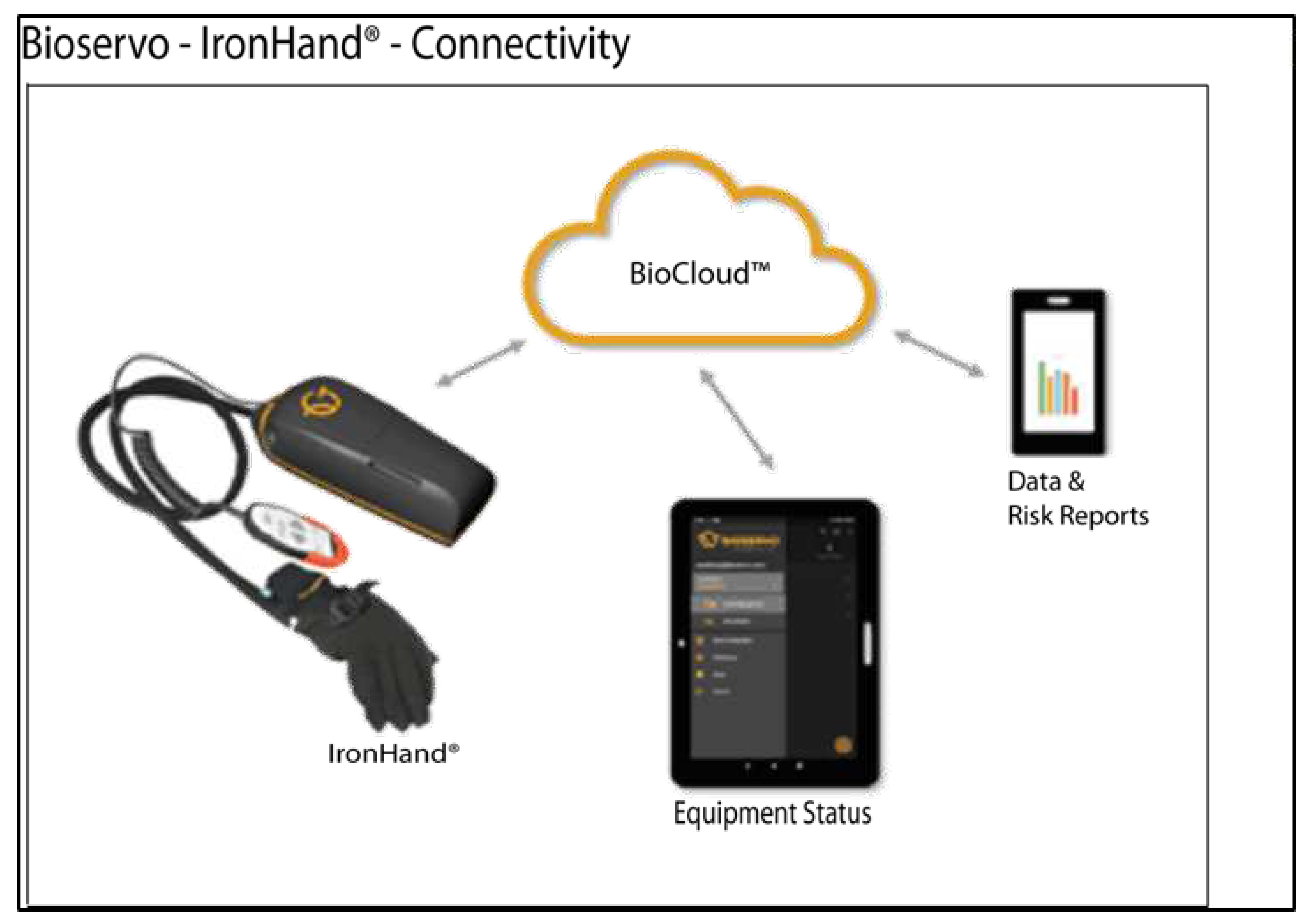
Figure 30.
Paexo Wrist device [36]. Images taken and revised from Ottobock official website.
Figure 30.
Paexo Wrist device [36]. Images taken and revised from Ottobock official website.

Figure 31.
SaeboFlex device [56].
Figure 31.
SaeboFlex device [56].
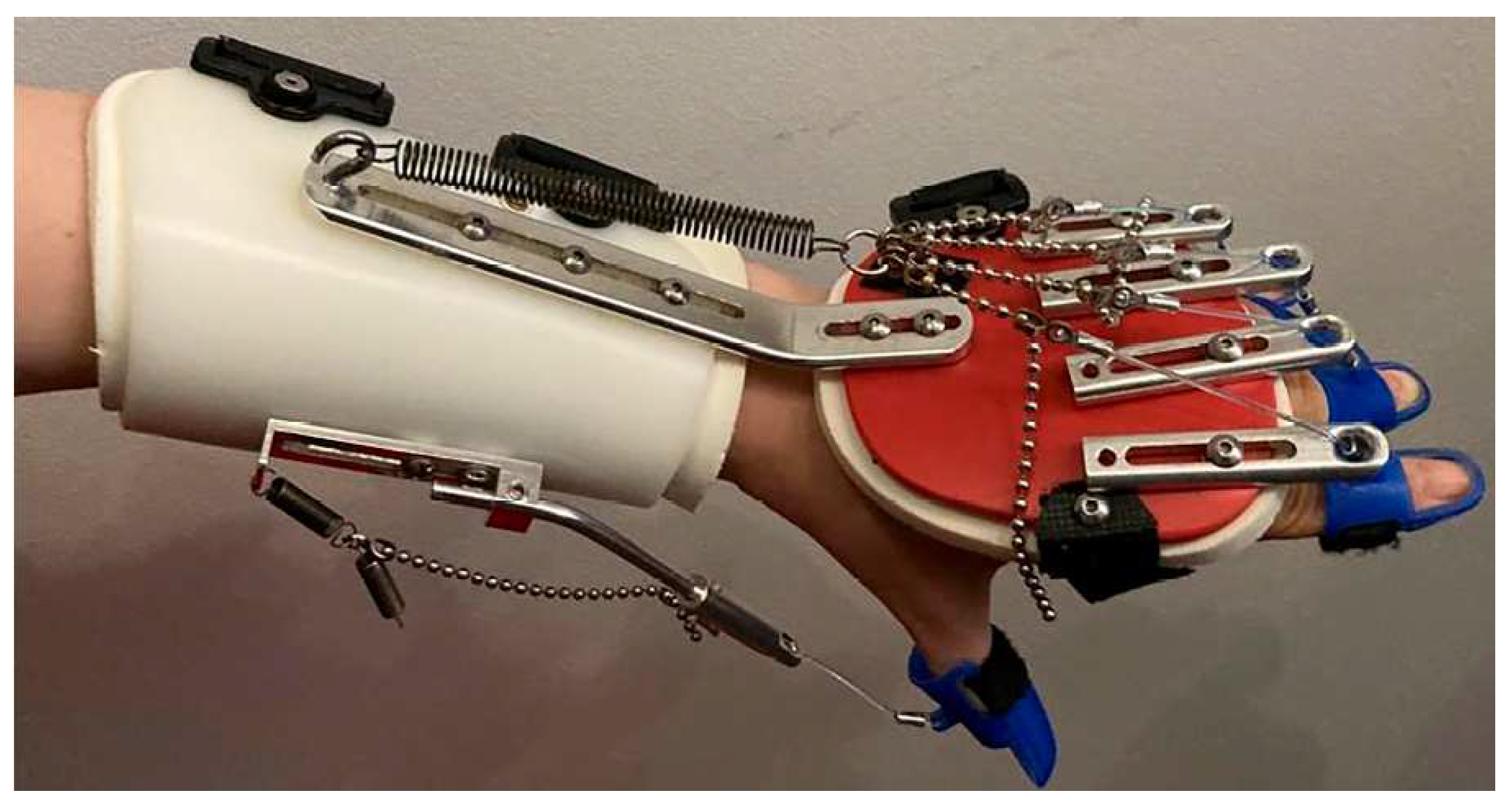
Figure 32.
Hand and wrist movements to be assisted.
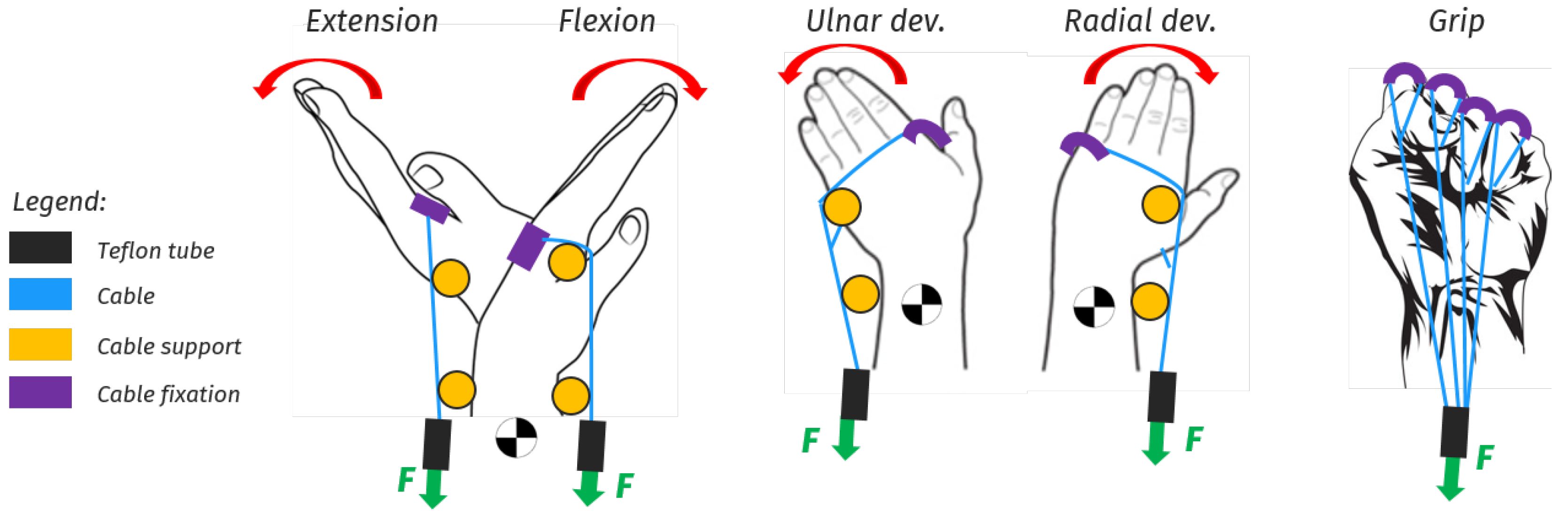
Figure 33.
Conceptual idea of a portable wrist exoskeleton. Grey: backpack containing actuators and electronics; Green: webbings; Red: sEMG sensors; Black lines: Teflon tubes; Light blue lines: steel or fiber cables; Orange: rigid cable supports; Yellow: FSR sensors; Black: glove; Purple: soft plastic cable holders.
Figure 33.
Conceptual idea of a portable wrist exoskeleton. Grey: backpack containing actuators and electronics; Green: webbings; Red: sEMG sensors; Black lines: Teflon tubes; Light blue lines: steel or fiber cables; Orange: rigid cable supports; Yellow: FSR sensors; Black: glove; Purple: soft plastic cable holders.
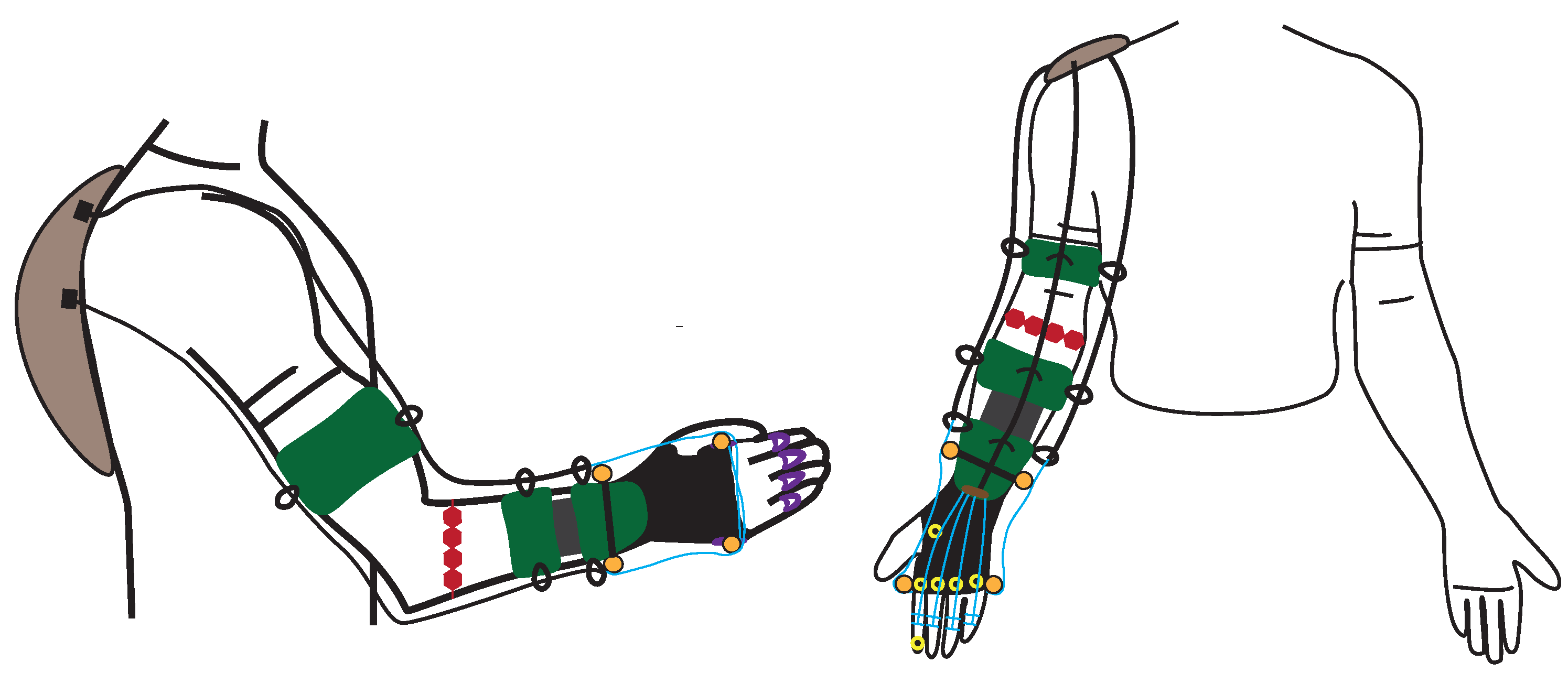
Figure 34.
Description of the modality according to which the direction of the force changes when cable supports (orange in picture) are either present or absent. On the left, the wrist goes from neutral to flexion, while on the right it goes from neutral to extension.
Figure 34.
Description of the modality according to which the direction of the force changes when cable supports (orange in picture) are either present or absent. On the left, the wrist goes from neutral to flexion, while on the right it goes from neutral to extension.
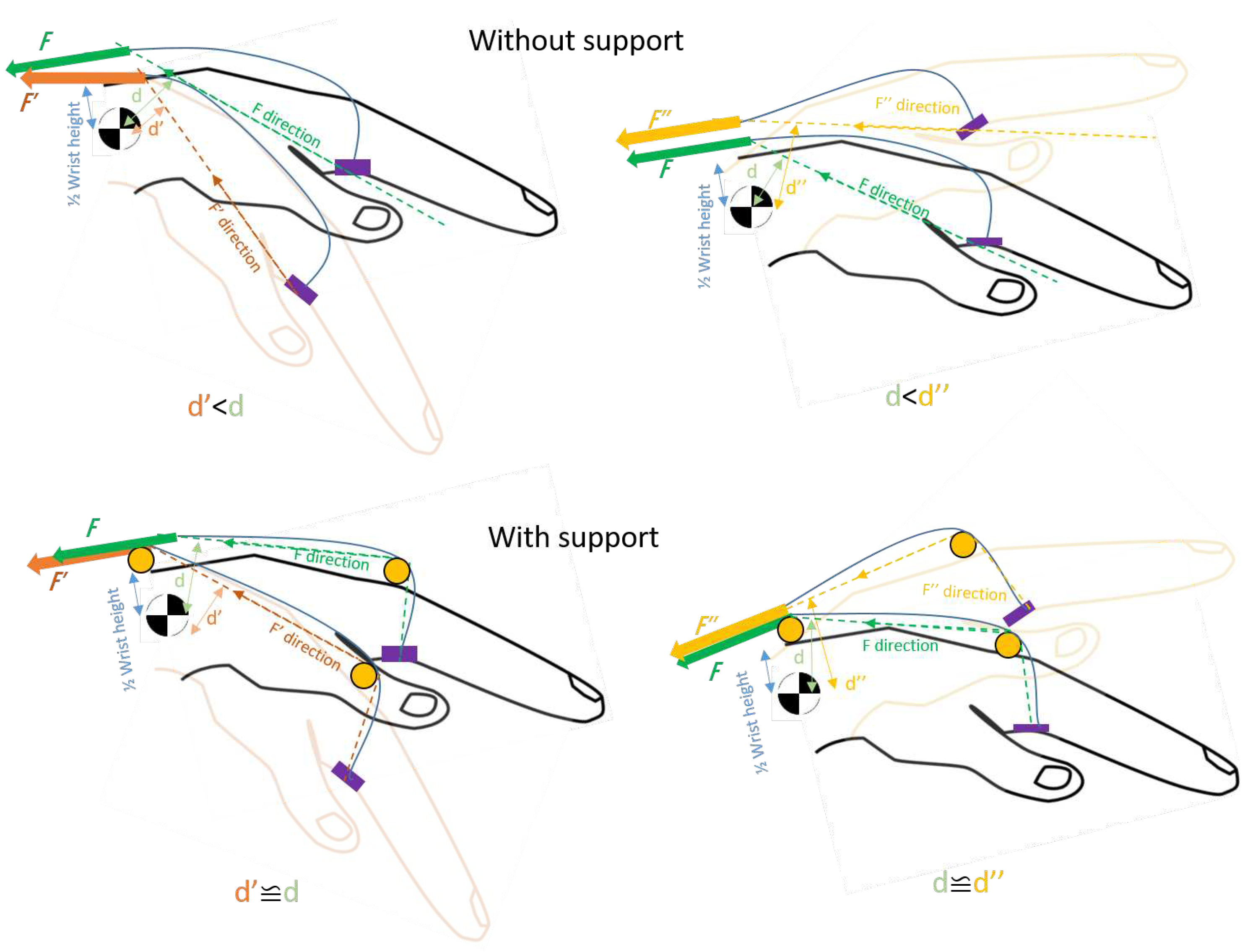
Figure 36.
Different classifications by purpose (a), actuation type (b), number of active DoF (c), stiffness (d) and TRL (e), of wearable wrist exoskeleton took into consideration. The amount of devices considered is 24. In some graphs, the percentage is preferred because some devices have been designed for more than one application or can be used both as passive or active. Only 6 devices out of 24 have passed conformity tests and entered the market.
Figure 36.
Different classifications by purpose (a), actuation type (b), number of active DoF (c), stiffness (d) and TRL (e), of wearable wrist exoskeleton took into consideration. The amount of devices considered is 24. In some graphs, the percentage is preferred because some devices have been designed for more than one application or can be used both as passive or active. Only 6 devices out of 24 have passed conformity tests and entered the market.
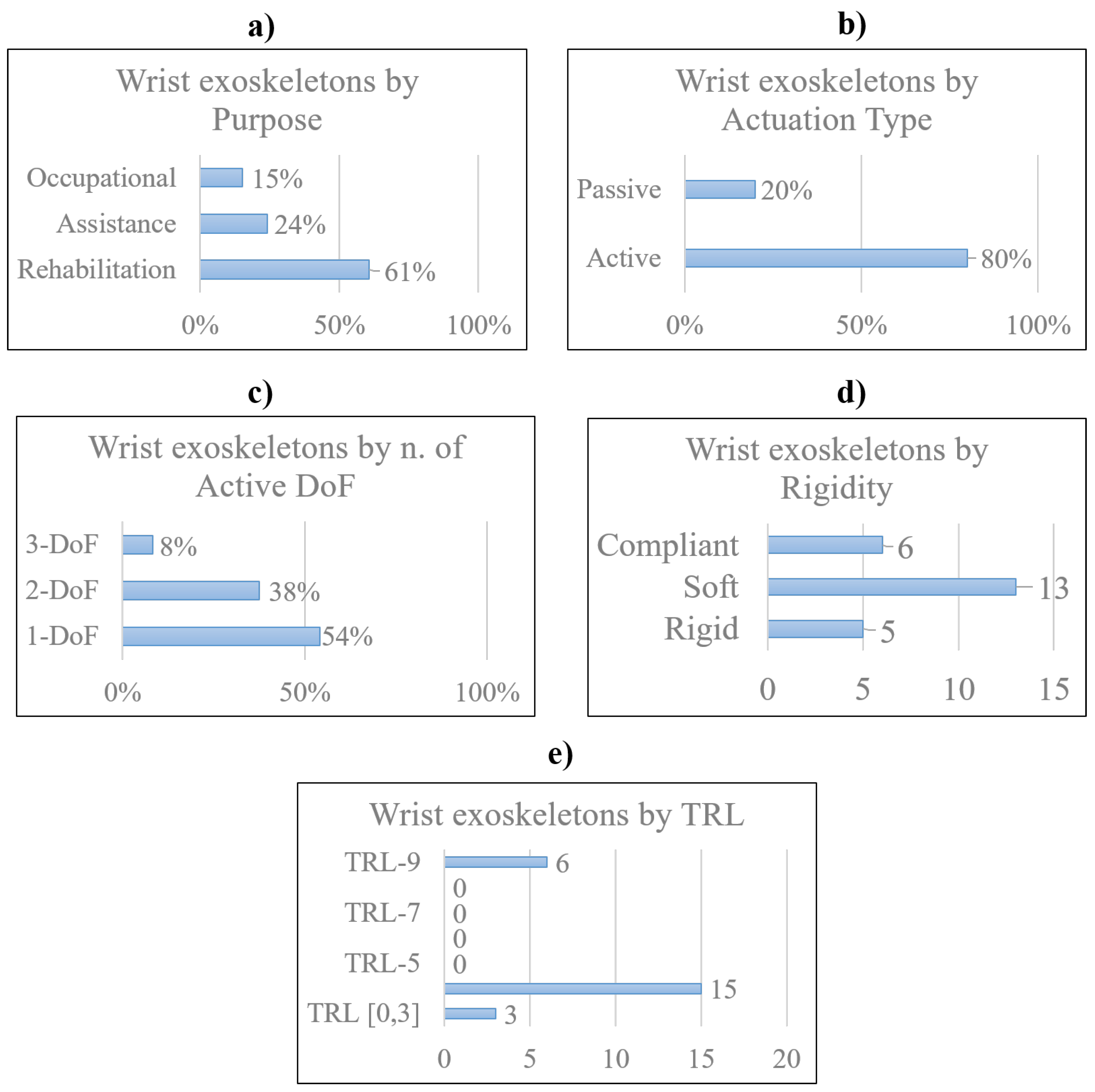
Figure 37.
Different classifications by power source (f), power transmission (g), sensing technologies (h) and control strategies (i), of wearable wrist exoskeleton took into consideration. The total amount of devices considered is 24. In some graphs, the percentage is preferred because some devices adopts more than one sensing technology and control strategy.
Figure 37.
Different classifications by power source (f), power transmission (g), sensing technologies (h) and control strategies (i), of wearable wrist exoskeleton took into consideration. The total amount of devices considered is 24. In some graphs, the percentage is preferred because some devices adopts more than one sensing technology and control strategy.
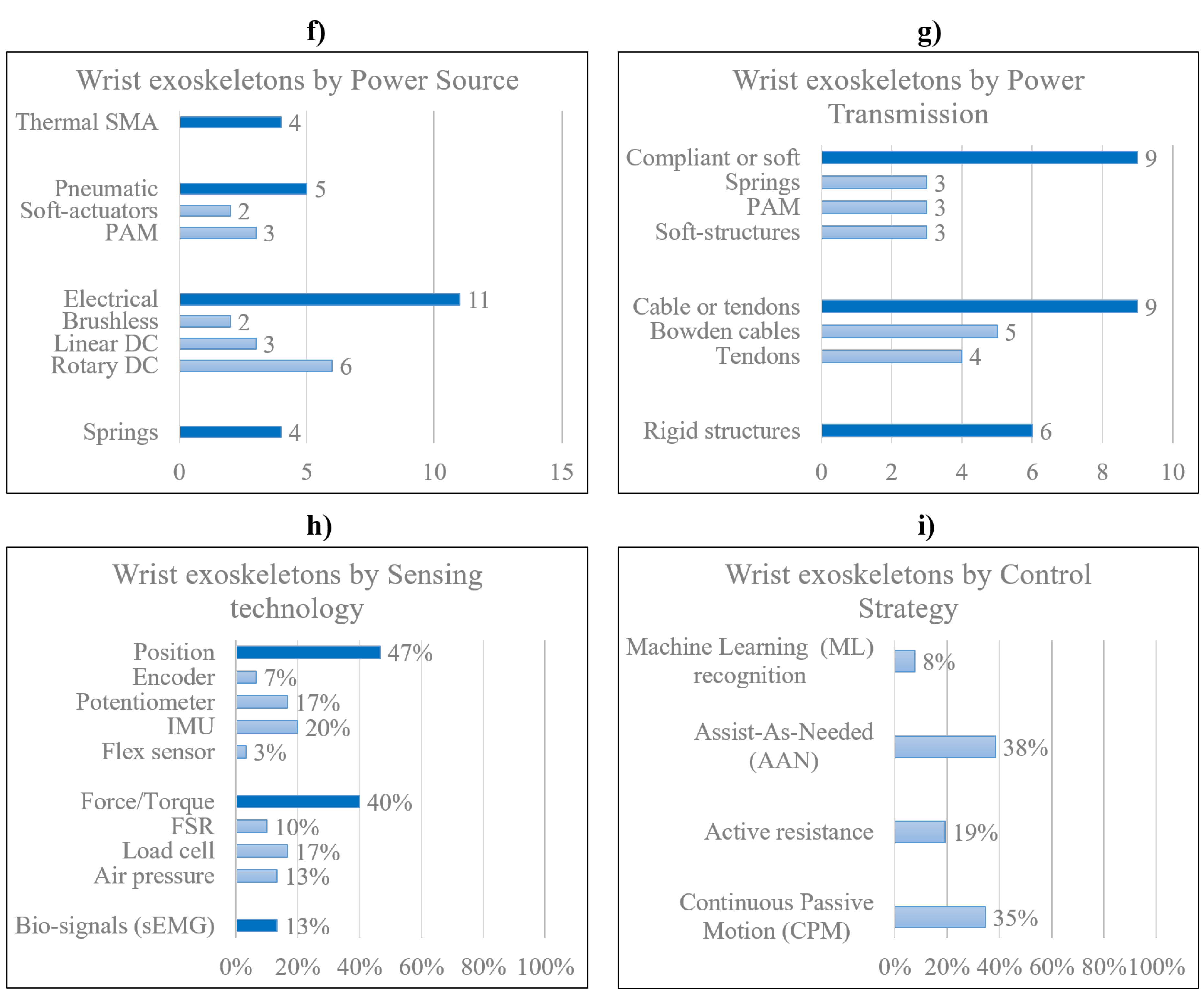
Figure 38.
Classification by TRL of wearable wrist exoskeleton conceived for occupational purposes. Only two devices are available in the market: IronHand designed by Bioservo (active device), and Paexo wrist designed by Ottobock (passive device).
Figure 38.
Classification by TRL of wearable wrist exoskeleton conceived for occupational purposes. Only two devices are available in the market: IronHand designed by Bioservo (active device), and Paexo wrist designed by Ottobock (passive device).
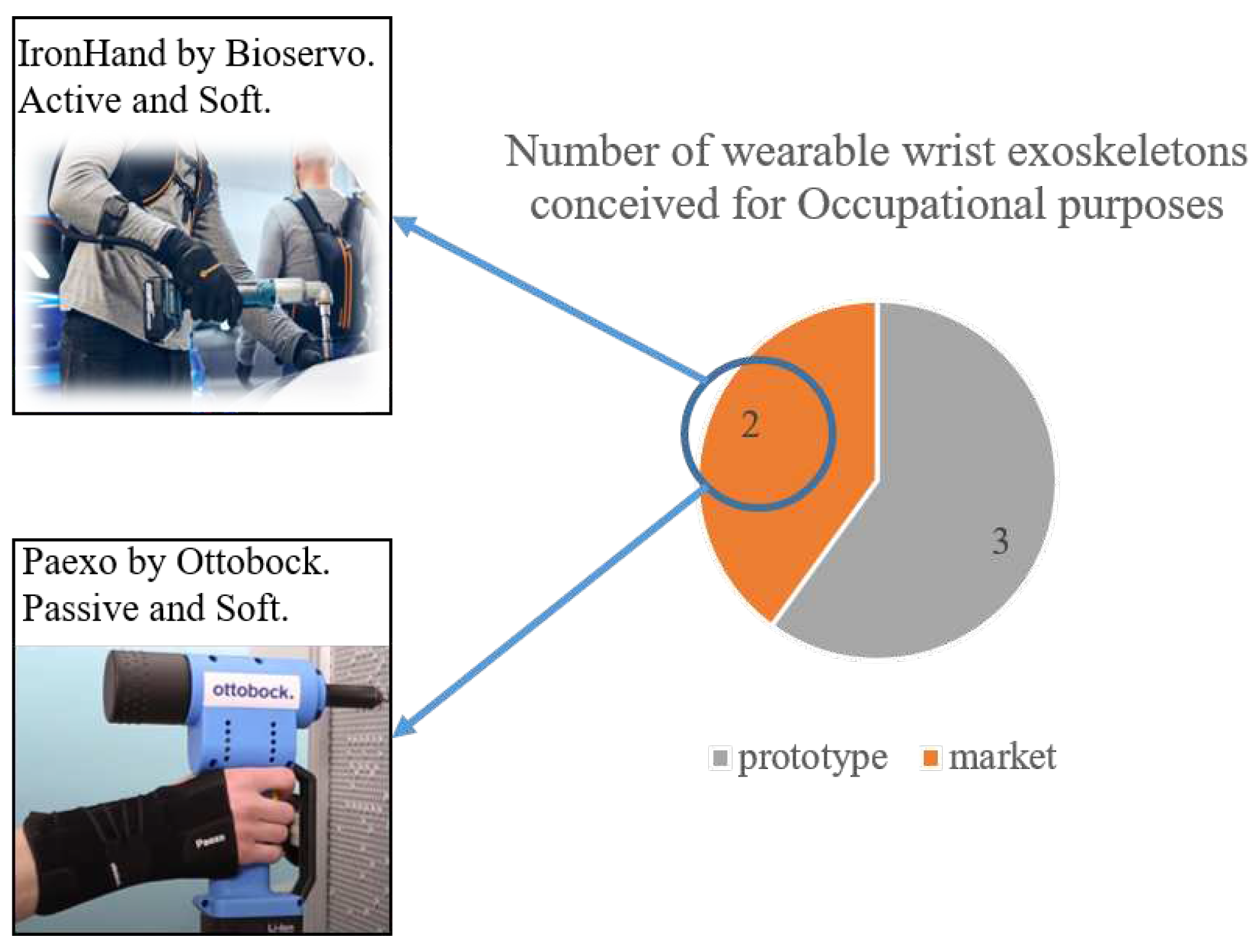
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



