Submitted:
13 November 2023
Posted:
14 November 2023
You are already at the latest version
Abstract
Background: Hospital-acquired infections (HAI) pose a significant danger to global public health, mainly because their numbers are growing exponentially each year. Additionally, the rise of bacterial strains resistant to current treatment options further exacerbates this threat. The study aimed to examine the occurrences of HAIs identified in public hospitals at the county level. Methods: We conducted a cross-sectional study utilizing data provided to the Mures Public Health Directorate from all the public hospitals within this county. We examined HAIs reported during the period spanning from 2017 to 2021, which amounted to a total of 4603 cases. Results: The medical departments reported the highest prevalence of HAIs at 48.25%. The most common infections in-cluded enterocolitis with Clostridioides difficile (32.61%), COVID-19 (19.83%), bronchopneumonia (16.90%), sepsis, surgical wound infections, and urinary tract infections. The five most frequently identified pathogens were Clostridioides difficile (32.61%), SARS-CoV-2 (19.83%), Acinetobacter baumannii (11.82%), Klebsiella pneumoniae (9.58%), and Pseudomonas aeruginosa (7.95%). Acinetobacter baumannii was the predominant agent causing bronchopneumonia, while Klebsiella pneumoniae was the leading cause of sepsis cases. Escherichia coli was the primary agent behind urinary tract infec-tions, and Staphylococcus aureus MRSA was identified as the main etiology for wound infections and central catheter infections. Throughout the study period, there was a significant rise in Clostridioides difficile cases, accounting for 40.36% of all reported HAIs in 2021. Conclusions: The study identifies Clostridioides difficile increase in HAI cases during COVID-19, highlighting the need for careful antibiotic use, and emphasizing the growing challenge of multi-resistant strains in post-pandemic state hospitals.
Keywords:
Hospital-acquired infections
; colonization
; infection
; risk factors
; antibiotics
1. Introduction
HAI, also known as “nosocomial infections” occur in patients receiving medical care in hospitals or other healthcare facilities, including chronic care units and retirement homes. In recent years, these infections have posed a significant threat to public health, leading to increased mortality and morbidity. Additionally, there are challenges in limiting and treating these infections effectively [1].
In Europe, the most recent data from the World Health Organization indicates an annual occurrence of 8.9 million HAIs in acute and long-term care facilities. The majority of these cases are reported in intensive care units (ICU), affecting up to 30% of patients in high-income countries and 2-3 times more in low-income nations. The statistics also reveal that 23.6% of all hospital-treated sepsis cases are healthcare-associated, with a mortality rate of 24.4% among patients affected, rising to 52.3% for those treated in intensive care units. Moreover, there has been an emergence of multidrug-resistant bacteria, including Vancomycin-resistant Enterococci (VRE), Staphylococcus aureus MRSA among Gram-positive agents, and Pseudomonas aeruginosa, Klebsiella pneumoniae, and Enterobacter spp. as significant concerns among resistant Gram-negative pathogens [2].
In Romania, HAI remains underreported, with an official prevalence of 0.2-0.3%, contrasting with the 7.1% prevalence across Europe. A 2018 study on HAI prevalence in Europe, based on two prevalence surveys, indicated a rate of 2.6% in Romania (95% Confidence Interval: 1.7-4.0) [3,4]. The primary issue contributing to these discrepancies in prevalence comparisons is the lack of proper reporting of these infections. Although the implementation of Order No. 1101 in 2016 [5], approving the norms for surveillance, prevention, and limitation of HAI in health units, led to an increase in reporting rates, the prevalence rate still falls significantly below the European average. Common pathologies associated with HAI include mechanical ventilation-associated pneumonia and urinary tract infections in ICUs, wound infections in surgical units, and intestinal tract infections involving Clostridioides difficile, which can compound other HAIs due to prolonged antibiotic treatment [6,7].
The aim of this study was to analyze the cases of HAIs identified from the public hospitals from Mures county level, through the case reports sheets as they are reported according to Romanian legislation.
2. Results
The patients diagnosed with HAI had an average age of 60.27±21.67 years (mean ± standard deviation), ranging from a minimum of 3 weeks to a maximum of 99 years. Out of the total 4603 cases, 2454 (53.31%) were males, and 46.69% were females. In terms of residence, 54.16% were from urban areas, and the remaining 45.84% were from rural regions.
HAIs were most prevalent in medical sections (48.25%), followed by ICU wards (32.28%), surgical units (17.18%), neonatology (1.39%), and the ED with the fewest cases (0.90%). Regarding the type of HAI reported, enterocolitis with Clostridioides difficile was the most common at 32.61%, followed by Covid-19 (19.83%), bronchopneumonia (16.90%), sepsis (9.04%), urinary tract infections (9.04%), surgical wound/tissue infections (8.30%), central catheter infections (2.04%), and other types of infections (2.24%). Other infections included meningitis, external ventricular drainage infections, otitis, phlebitis, and influenza-type A/B infections. Among the cases reported, 92.48% originated from the reporting hospital, and HAI was considered a possible cause of death in only 7.06% of 1176 fatal cases (Table 1).
Among all reported cases, Clostridioides difficile was the most common etiological agent isolated, accounting for 32.61%. SARS-CoV-2, identified as HAI in 2020, emerged as the second most frequent agent in the study group, comprising 19.83%, while Escherichia coli had the lowest incidence as an HAI etiology, with only 153 cases (Figure 1).
The majority of reported HAIs were observed in medical sections (2221 cases) primarily due to Clostridioides difficile (42.05%), followed by SARS-CoV-2 (26.97%). In ICU units, Clostridioides difficile infections were predominant (27.79%), followed by Acinetobacter baumannii (15.34%), Pseudomonas aeruginosa (13.53%), and Klebsiella pneumoniae (9.96%), with Escherichia coli being the least frequent at 3.57%. Surgical wards reported 791 HAI cases, with Acinetobacter baumannii being the most common pathogen (22.76%), succeeded by Clostridioides difficile (18.33%) and Staphylococcus aureus MRSA (13.65%) among all nosocomial surgical cases. Neonatology departments identified Escherichia coli as the primary etiological agent (25%), closely followed by Staphylococcus aureus MRSA (20.31%). The ED reported the fewest HAI cases (0.9%), mainly attributed to SARS-CoV-2 (26.83%) and Staphylococcus aureus MRSA (21.95%) (Figure 2).
In terms of infection types, enterocolitis was the most common, exclusively caused by Clostridioides difficile in 100% of cases. Among the 778 cases of bronchopneumonia, Acinetobacter baumannii was the predominant etiological agent, accounting for 40.36%, followed by Pseudomonas aeruginosa (19.67%) and Klebsiella pneumoniae (19.54%). Escherichia coli was the primary cause of urinary tract infections in 22.12% of cases, with this infection type being most frequently reported in medical wards and ICU units. Staphylococcus aureus MRSA was predominantly isolated in central catheter infections (27.66%) and surgical wound infections (27.49%). The main sources of infection for sepsis were Klebsiella pneumoniae (29.33%), Acinetobacter baumannii (21.88%), and Pseudomonas aeruginosa (17.07%) (Figure 3).
In 1176 cases, death was reported as an outcome, with Clostridioides difficile and Acinetobacter baumannii identified as the etiological agents in nearly half of them. The majority of patients were discharged with improved status, accounting for 36.98%. Among these cases, Clostridioides difficile was also the most frequently isolated agent (571). A total of 481 patients were successfully treated and discharged as cured, with Clostridioides difficile responsible for almost half of these cases (41.08%). Data on the discharge status of patients were unavailable in 1002 cases (Figure 4).
Isolation conditions were implemented in 2301 reported cases, predominantly for patients infected with Clostridioides difficile. Contacts were documented in 2536 cases, with the majority infected by SARS-CoV-2 and other pathogens (Figure 5).
In 2017, HAIs attributed to Clostridioides difficile accounted for 27.15% of cases. During the study period, a significant increase was observed, reaching 43.60% in 2021. In contrast, nosocomial infections involving Klebsiella pneumoniae declined from 15.55% in 2017 to 6.69% in 2021. The peak number of HAI cases linked to Acinetobacter baumannii was recorded in 2018, comprising 18.89% of all 593 reported nosocomial infections. Monitoring HAIs related to SARS-CoV-2 from the pandemic's onset in 2020 until the end of 2021 revealed a decrease in incidence from 43.15% to 24.13%.
In the initial three years analyzed, Pseudomonas aeruginosa was found in more than 10% of cases each year, followed by a decrease to 5.81% in 2020 and 5.79% in 2021, Escherichia coli showed a relatively steady incidence during the first three years (4.41%, 4.89%, and 4.42%), with a slight decrease to 3.02% in 2021.
3. Discussion
This research monitored HAI cases over a span of 5 years, during which 4603 cases were documented. The average age of the participants ranged from 60 to 65 years, with ages spanning from 3 weeks to 99 years. Older individuals constituted the majority of patients requiring medical services. They form a vulnerable demographic due to their diminished immune system, influenced by both age-related factors and underlying chronic illnesses [8]. Typically, patients diagnosed with HAIs exhibit multiple concurrent health conditions, making them susceptible to a general decline in immune competence. Prolonged or repeated hospital stays increase the likelihood of HAI, occurring not only in ICUs but also in various medical and surgical services.[9].
All instances were documented from seven public hospitals, establishments inherently more susceptible to the proliferation of pathogens causing HAIs when compared to private institutions. Firstly, state-run hospitals accommodate a significantly larger number of patients than private medical facilities. They have a higher quantity of medical departments and limited space, making it challenging to create isolation rooms [10]. Secondly, financially, public hospitals lack the resources of their private counterparts. Consequently, ensuring an equivalent level of cutting-edge equipment or a continuous supply of cleaning agents and disinfectants remains unfeasible. [11]. Conversely, private hospitals might report fewer HAI cases due to potential underreporting. This omission could stem from their desire to avoid negative publicity, subsequently reducing patient attendance [12].
In this study, it was noted that the majority of HAI cases occurred in medical departments. Before 2020, the studied hospitals primarily reported nosocomial infections in the ICU. However, during the onset of the COVID-19 pandemic, a significant shift was observed, with most HAIs being recorded in medical wards, followed closely by the ICU. In 2020, due to the surge in SARS-CoV-2 cases and the rise in critical cases, Romanian hospitals faced limited space in their ICUs. Consequently, medical departments, particularly those specializing in infectious diseases and pneumology, had to accommodate a substantial number of patients. The overcrowding in these departments, coupled with the prolonged hospital stays of COVID-19 patients, increased the risk of nosocomial infections in these areas.
Additionally, there was a shift in the predominant type of HAI infection. While bronchopneumonia caused by Acinetobacter baumannii was the most common type between 2017 and 2019, starting from 2020, enterocolitis associated with Clostridioides difficile became the most frequently reported infection. Consequently, over the five-year period, enterocolitis stood out as the most prevalent infection, documented in a total of 1,501 cases, with 62.23% of them within medical wards.
Clostridioides difficile emerged as the most frequently detected pathogen responsible for HAIs, constituting 1501 out of 4603 cases. Notably, compared to the pre-pandemic years when Acinetobacter baumannii was predominant, Clostridioides difficile exhibited a significant surge in its incidence rate. Particularly striking was the rise coinciding with the emergence of the SARS-CoV-2 virus, accounting for nearly half of all HAI cases in 2021. Indeed, the occurrences of Clostridioides difficile infections in the period 2020-2021 surpassed those reported between 2017-2019. Several factors could explain this trend. Firstly, during the pandemic, healthcare facilities faced overcrowding, making it challenging to isolate potential community cases effectively. Consequently, bacterial transmission among patients became inevitable. Similar limitations in isolation protocols were observed concerning HAI with Clostridioides difficile, where strict isolation measures would have been necessary. Secondly, recent research indicates that SARS-CoV-2 can persist and replicate in the intestinal environment for extended periods. Moreover, the findings from Lin et al. study [13] revealed that a portion of patients (27.3%) exhibited no lung imaging characteristics of COVID-19. Instead, they presented gastrointestinal symptoms, underscoring the susceptibility of gastrointestinal tissues to SARS-CoV-2. The interaction between SARS-CoV-2 and the renin-angiotensin-aldosterone system leads to reduced local anti-inflammatory responses. This viral cycle triggers an excessive imbalance in immune responses and cytokine release. Post-viral infection, the downregulation of angiotensin-converting enzyme 2 causes gastrointestinal dysfunctions. Consequently, SARS-CoV-2 infection might heighten susceptibility to Clostridioides difficile infections, given the opportunistic nature of this bacterium. [14].
Furthermore, managing antibiotic treatment for COVID-19 patients presents challenges due to similarities between bacterial pneumonia and moderate to severe COVID-19 cases. Although current guidelines suggest using empiric antibiotics only when bacterial infections are suspected in moderate COVID-19, they are routinely recommended for severe COVID-19 cases. Distinguishing between advancing COVID-19 illness and bacterial co-infection or superinfection is challenging. The decision for empiric antibiotic treatment might be influenced by experiences from Influenza cases, where bacterial co-infection rates range from 11% to 35%. [15]. Despite this, hospitals commonly utilize prophylactic antibiotic therapy. Studies indicate that antibiotic treatment for bacterial infections in hospitalized COVID-19 patients leads to the depletion of beneficial commensals and the proliferation of opportunistic pathogens, including Clostridioides difficile [16].
A crucial issue to address concerning Clostridioides difficile infections is the management and treatment of this condition. Clostridioides difficile, being a widespread organism, has developed unique survival mechanisms that enable its successful proliferation in the competitive gut environment. This pathogen's remarkable adaptability is largely attributed to the diversity of its genome. When Clostridioides difficile encounters cellular stress, it employs two survival strategies: producing a toxin and forming a protective coat through sporulation. Sporulation aids its persistence in the gut or facilitates an escape. Considering the rising number of cases and the bacterium's exposure to various treatments, there has been an increase in its resistance to antibiotics. Metronidazole exhibits low bioavailability in the colon, leading to fecal concentrations ranging from 0.8 to 24.2 µg/g stool [17]. This phenomenon may account for metronidazole nonsusceptibility, as exposure to subinhibitory concentrations might have played a role in the selection of resistance. Oral vancomycin is increasingly being utilized as the primary treatment option, driven by recent updates in treatment guidelines as well as concerns related to costs and availability. A study conducted by Darkoh and colleagues [18] identified Clostridioides difficile isolates with reduced susceptibility to vancomycin in patient populations from two distinct geographic locations on different continents – Houston and Nairobi. The results revealed that 26% of patients in Houston and 67% of patients in Nairobi, suffering from enterocolitis with Clostridioides difficile, carried bacterium isolates that were not susceptible to vancomycin. Fidaxomicin has demonstrated superiority over vancomycin in preventing recurrent enterocolitis with Clostridioides difficile. This superiority might be attributed to its narrow spectrum of activity, which allows the gut to restore a normal microbiome. Additionally, fidaxomicin inhibits Clostridioides difficile sporulation and the production of toxins. The inhibition of sporulation by fidaxomicin could potentially reduce the transmission of the infection to others by decreasing the shedding of spores and subsequent environmental contamination [19]. While some studies indicate that fidaxomicin, as opposed to vancomycin, decreases the risk of recurrent enterocolitis caused by Clostridioides difficile [20], the use of fidaxomicin comes with substantial costs that surpass the financial constraints of state hospitals. Consequently, Fidaxomicin remains an impractical treatment option for most state-funded medical facilities. Modern medicine requires further research to explore innovative solutions for managing this infection, focusing on both prevention and treatment of the infection and its recurrence.
Apart from enterocolitis, the leading types of nosocomial infections included COVID-19, bronchopneumonia, urinary tract infections, sepsis, and surgical wound infections. Bronchopneumonia was notably frequent in ICU cases, with Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Staphylococcus aureus MRSA being the primary causative agents, especially prevalent in ICU sections. The extensive use of tracheal intubation and mechanical ventilation for critically ill patients further heightens the risk for this condition among patients already susceptible [21]. In line with our findings, a cohort study conducted by Trivedi et al. [22] revealed that the most common isolates in ICU nosocomial pneumonia were Pseudomonas aeruginosa (55%), Acinetobacter baumannii (20%), Staphylococcus aureus (14.5%), and Klebsiella pneumoniae (7.5%). A limited number of nosocomial lower respiratory tract infections were linked to Escherichia coli. Aspiration and mechanical ventilation were identified as risk factors for this condition. In recent years, Escherichia coli with extraintestinal pathogenicity has attracted attention and is believed to cause a range of infections, including bacteremia, urinary tract infections, prostate infections, pneumonia, liver abscesses, meningitis, and brain abscesses [23].
Urinary tract infections accounted for 416 cases, predominantly caused by Escherichia coli. More than half of these cases were reported in the ICU and medical departments. In a comprehensive retrospective study, Machado et al. [24] analyzed the prevalence of HAIs caused by extended-spectrum beta-lactamase - or carbapenemase-producing Escherichia coli. Their findings indicated alarming prevalence rates, possibly underestimated due to clinically diagnosed HAIs, highlighting the persistence and spread of these bacteria in healthcare institutions in Portugal. Similar epidemiological trends have been reported in other countries as well.
We discovered that among the HAIs, 416 were identified as sepsis, with Klebsiella pneumoniae infections being the most common culprit, accounting for 122 cases. The majority of systemic infections were detected in ICU wards. Klebsiella pneumoniae was also isolated in 62 cases of surgical wound infections and 16 cases of urinary tract infections. The significant challenge in dealing with Klebsiella pneumoniae infections lies in limited treatment options due to extensive antibiotic resistance, leading to heightened morbidity and mortality rates. The widespread and inappropriate use of carbapenems can result in challenging-to-control epidemics, particularly in intensive care units, owing to the acquired resistance to this group of antibiotics. Outbreaks and isolated cases caused by carbapenem-resistant Klebsiella pneumoniae species have been increasingly reported worldwide in recent years [25].
Surgical wound infections and central catheter infections are frequently identified in both ICU and surgical wards. It's essential to consider that some ICU patients were initially in surgical wards. Additionally, patients reported with HAIs in surgical wards might have had ICU exposure during postoperative care, indicating potential infections originating from the ICU.
In the case of neonates, although they accounted for only 1.39% of reported HAI cases, it's crucial to highlight the prevalence of Escherichia coli and Staphylococcus aureus MRSA infections in this group. Newborns in neonatal ICUs, especially preterm infants, face elevated infection risks due to factors such as immature immune systems, extended hospital stays, and frequent use of invasive devices and antibiotics. Staphylococcus aureus MRSA infections are particularly common in neonatal ICUs, leading to severe conditions like pneumonia, osteomyelitis, and bacteremia. [26]. Neonatal bloodstream infections often result in Staphylococcus aureus MRSA-related sepsis, associated with high mortality rates. Studies have revealed the endemic presence of Staphylococcus aureus MRSA in numerous neonatal ICUs, causing invasive diseases and death [27,28]. Escherichia coli stands out as a major pathogen causing neonatal infections, particularly meningitis and sepsis in developing countries. Recent increases in its incidence and drug resistance pose significant threats to neonatal health. Plasmid-borne extended-spectrum beta-lactamase (ESBL) genes lead to Escherichia coli resistance against β-lactam antibiotics like cephalosporin, resulting in treatment challenges worldwide. A study published by Xiao et al. [29] found that some Escherichia coli strains were resistant to carbapenem antibiotics, including ertapenem, doripenem, meropenem, and imipenem. Carbapenem resistance can occur through various mechanisms, severely limiting treatment options for multidrug-resistant Escherichia coli, particularly ESBL and carbapenem-resistant Enterobacterales (CRE) infections in neonates. Consequently, there is an urgent need to focus on surveillance, prevention, and management of ESBL and CRE to enhance the accuracy of neonatal infection diagnosis and the rational use of antibiotics.
Considering our study, which highlighted a gradual decrease in reported cases of HAIs caused by Acinetobacter baumanii, Pseudomonas aeruginosa, and Klebsiella pneumoniae strains, particularly in the last two years, 2020 and 2021, we attribute this trend to potential underreporting. Numerous recent scientific articles have demonstrated a significant rise in HAIs with these strains since the onset of the COVID-19 pandemic [30,31]. A review study published in June 2023 has shown an overall increase in drug-resistant bacterial infections involving Streptococcus pneumoniae, Klebsiella pneumoniae, Haemophilus influenzae, Escherichia coli, Staphylococcus aureus, Pseudomonas aeruginosa, and Acinetobacter baumannii, correlating with the heightened use of antibiotics in COVID-19 admissions [32]. Contrary to the literature findings, the lower incidence of infections with these agents observed in our study during the pandemic period (2020-2021) could be attributed to underreporting. The medical staff's exclusive focus on diagnosing and treating SARS-CoV-2 infections, along with laboratories being burdened by COVID-19 testing, likely resulted in a partial interruption in detecting these bacteria.
In the post-pandemic era, it becomes crucial to resume accurate reporting of HAI cases in hospitals.
Additional comprehensive studies are essential to assess the current antibiotic resistance of reported germs causing HAIs. Implementing preventive measures to safeguard patients against these infections and adopting appropriate therapeutic interventions for confirmed nosocomial infections is imperative.
Limitations of the study
The research was conducted solely at the county level, making it insufficient to draw valid comparisons with other regions in Romania. The data utilized were incomplete regarding patients' risk factors and comorbidities. Additionally, the discharge status of a significant number of cases remained unknown.
4. Materials and Methods
We conducted a cross-sectional study analyzing cases reported by public hospitals in Mures County (Romania) to the Mures Public Health Directorate. This included county clinical hospitals, a cardiovascular disease institute, municipal hospitals, and a city hospital. No cases were reported from private hospitals. The study focused on HAIs reported between 2017-2021, totaling 4603 cases. Data analysis considered patient demographics, hospital departments, diagnoses, surgical procedures, HAI diagnoses, isolation protocols, pathogens involved, antibiotic resistance, treatment details, patient status upon discharge, and potential links between HAI and patient deaths. The study encompassed various medical and surgical departments, which were later categorized into ICU, surgical units (general surgery, plastic surgery, obstetrics and gynecology, orthopedics, neurosurgery, urology), medical units (infectious diseases, cardiology, diabetes, hematology, gastroenterology, palliative care, internal medicine, neurology, nephrology, oncology, pediatrics), neonatology units, and emergency departments (ED) for statistical analysis. For processing the data, we received the consent of the Mures Public Health Directorate, and confidentiality and anonymity were maintained.
HAI identification and diagnosis in Romania
On September 30, 2016, the Romanian Minister of Health issued Order No. 1101/2016 [5], approving the regulations for the supervision, prevention, and containment of infections associated with medical care in healthcare facilities. According to this document, an HAI is defined as an infection acquired in healthcare settings (both public and private) and encompasses any infectious disease identifiable clinically and/or microbiologically. It must have epidemiological evidence indicating contraction during hospitalization or medical/surgical procedures. The incubation period of these infections is linked to the duration of medical care received by the patient in these facilities, regardless of whether symptoms appear during the hospitalization period. To diagnose HAIs, it is crucial to establish that the infection resulted from hospitalization or medical care in healthcare settings and was not present during the incubation/initial phase of the disease at the time of hospitalization or medical procedure.
When a physician suspects an HAI, they promptly notify the hospital's HAI prevention department, following the European Union's specified case definitions. The microbiology lab investigates suspected cases within 24 hours. Upon germ identification, bacteriology notifies the Public Health Directorate and relevant medical departments, especially when multidrug-resistant germs are isolated. The attending physician collaborates with an epidemiologist to assess the case clinically and classify it as confirmed, denied, or colonization based on definitions. The attending physician completes signs and files the HAI case statement, including the diagnosis in clinical records. The HAI diagnosis (coded Y95) is recorded in the general clinical observation sheet and computer system at the patient's discharge or transfer. The responsible physician ensures data accuracy. Suspected cases trigger daily electronic reports, while confirmed cases are reported weekly to the HAI prevention department. At the hospital level, the department maintains centralized records and prepares epidemiological investigations, implementing measures to prevent pathogen transmission. Monthly, quarterly, and annual reports on HAI incidence, categorized by sections and infection types, are submitted to the hospital's Steering Committee and the county's Public Health Directorate.
Statistical analysis
We utilized Statistical Package for Social Sciences (SPSS) for statistical analysis. Normally distributed quantitative data, such as age, were expressed as mean and standard deviation. Qualitative data were represented as counts and percentages.
5. Conclusions
This study conducted a statistical analysis of HAI cases in Mures County. It identified Clostridioides difficile as the predominant pathogen reported as a nosocomial infection over a 5-year period, encompassing both pre-pandemic and pandemic times. Notably, a correspondence was observed between SARS-CoV-2 infection and the rise in enterocolitis cases caused by Clostridioides difficile. This underlines existing research indicating immunological changes induced by SARS-CoV-2 in the gastrointestinal tract, heightening susceptibility to this opportunistic agent. It also emphasizes the importance of cautious antibiotic treatment administration for COVID-19 patients to reduce cases of enterocolitis caused by Clostridioides difficile due to antibiotic therapy. Particularly in state hospitals, HAIs pose a continuous threat due to limitations in treating multi-resistant strains. Current studies highlight a worsening of this situation in the post-pandemic period.
6. Patents
Author Contributions
Conceptualization, methodology, software, and formal analysis, SV.; validation, all authors; investigation, resources, data curation, DI, IM, BT, SV.; writing—original draft preparation, writing—review and editing, visualization, supervision, project administration, DI. and SV All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cassini, A.; Plachouras, D.; Eckmanns, T.; Abu Sin, M.; Blank, H.-P.; Ducomble. T.; Haller. S.; Harder, M.; Velasco, E.; Edward, W.; et al. Burden of Six Healthcare-Associated Infections on European Population Health: Estimating Incidence-Based Disability-Adjusted Life Years through a Population Prevalence-Based Modelling Study. PLoS Med. 2016, 13, e1002150. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, Matteo et al. Management of Infections Caused by Multidrug-resistant Gram-negative Pathogens: Recent Advances and Future Directions. Archives of medical research 2021, 52, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Suetens, C.; Latour, K.; Karki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikainen, O.; et al. Healthcare-Associated Infections Prevalence Study Group, Prevalence of health care associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Eurosurveillance 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Voidazan, S.; Albu, S.; Toth, R.; Grigorescu, B.; Rachita, A.; Moldovan, I. Healthcare Associated Infections—A New Pathology in Medical Practice? Int. J. Environ. Res. Public Health 2020, 17, 760. [Google Scholar] [CrossRef] [PubMed]
- Order, no. 1101/2016 Regarding the Approval of the Norms of Surveillance, Prevention and Limitation of the Healthcare-Associated Infections in the Health Units. Available online: https://lege5.ro/Gratuit/geztanjsgmzq/ordinul-nr-1101-2016-privind-aprobarea-normelor-de-supraveghere prevenire-si-limitare-a-infectiilor-asociate-asistentei-medicale-in-unitatile-sanitare (accessed on 16 October 2023).
- Salmanov, A.; Vozianov, S.; Kryzhevsky, V.; Litus, O.; Drozdova, A.; Vlasenko, I. Prevalence of healthcareassociated infections and antimicrobial resistance in acute care hospitals in Kyiv, Ukraine. J. Hosp. Infect. 2019, 102, 431–437. [Google Scholar] [CrossRef]
- Mullish, B.H.; Williams, H.R. Clostridium difficile infection and antibiotic-associated diarrhoea. Clinical medicine 2018, 18, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Kariya, N. , Sakon, N., Komano, J., Tomono, K.; Iso, H. Current prevention and control of health care-associated infections in long-term care facilities for the elderly in Japan. Journal of infection and chemotherapy : Official journal of the Japan Society of Chemotherapy 2018, 24, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Moro, M.L.; Ricchizzi, E.; Morsillo, F.; Marchi, M.; Puro, V.; Zotti, C.M.; Prato, R.; Privitera, G.; Poli, A.; Mura, I.; et al. Infections and antimicrobial resistance in long term care facilities: A national prevalence study. Ann. Ig. 2013, 25, 109–118. [Google Scholar]
- Al-Omari, A. , Al Mutair, A., Alhumaid, S., Salih, S., Alanazi, A., Albarsan, H., Abourayan, M.; Al Subaie, M. The impact of antimicrobial stewardship program implementation at four tertiary private hospitals: Results of a five-years pre-post analysis. Antimicrobial resistance and infection control 2020, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Revelas, A. Healthcare - associated infections: A public health problem. Nigerian medical journal : Journal of the Nigeria Medical Association 2012, 53, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Deryabina, A. , Aiypkhanova, A., Juvashev, A., Alimbetov, K., Tekebayev, K., Kassa, G.; Howard, A.A. Core components of infection prevention and control programs at the facility level in Kazakhstan: Key challenges and opportunities. Antimicrobial resistance and infection control 2023, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Lin L, Jiang X, Zhang Z, Huang S, Zhang Z, Fang Z; et al. . Gastrointestinal Symptoms of 95 Cases With SARS-CoV-2 Infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H. , Shao, B., Dang, Q., Chen, Z., Zhou, Q., Luo, H., Yuan, W.; Sun, Z. Pathogenesis and Mechanism of Gastrointestinal Infection With COVID-19. Frontiers in immunology 2021, 12, 674074. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses.
- Azimirad, M. , Noori, M., Raeisi, H., Yadegar, A., Shahrokh, S., Asadzadeh Aghdaei, H., Bentivegna, E., Martelletti, P., Petrosillo, N.; Zali, M.R. How Does COVID-19 Pandemic Impact on Incidence of Clostridioides difficile Infection and Exacerbation of Its Gastrointestinal Symptoms? Frontiers in medicine 2021, 8, 775063. [Google Scholar] [PubMed]
- Bolton, R.P.; Culshaw, M.A. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986, 27, 1169–1172. [Google Scholar] [CrossRef] [PubMed]
- Darkoh C, Keita K, Odo C; et al. Emergence of Clinical Clostridioides difficile Isolates With Decreased Susceptibility to Vancomycin. Clin Infect Dis. 2022, 74, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Mullane, K. Fidaxomicin in Clostridium difficile infection: Latest evidence and clinical guidance. Ther Adv Chronic Dis. 2014, 5, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Patel D, Senecal J, Spellberg, B. ; et al. Fidaxomicin to prevent recurrent Clostridioides difficile: What will it cost in the USA and Canada? JAC Antimicrob Resist. 2023, 5, dlac138. [Google Scholar]
- Dandagi, G.L. Nosocomial pneumonia in critically ill patients. Lung India : Official organ of Indian Chest Society 2010, 27, 149–153. [Google Scholar] [CrossRef]
- Trivedi, T.H.; Shejale, S.B.; Yeolekar, M.E. Nosocomial pneumonia in medical intensive care unit. J Assoc Physicians India 2000, 48, 1070–1073. [Google Scholar] [PubMed]
- Ehman, D. , Mugarab Samedi, V., Kalaniti, K.; Daspal, S. Neonatal Escherichia coli infection in twins: Clinical spectrum and management dilemma. BMJ case reports 2021, 14, e238470. [Google Scholar] [CrossRef] [PubMed]
- Machado, E. , Costa, P., Carvalho, A.; On Behalf Of The Sarel Investigators. Occurrence of Healthcare-Associated Infections (HAIs) by Escherichia coli and Klebsiella spp. Producing Extended-Spectrum β-lactamases (ESBL) and/or Carbapenemases in Portuguese Long-Term Care Facilities. Pathogens 2022, 11, 1019. [Google Scholar] [PubMed]
- Büyüktuna, S.A. , Hasbek, M., Çelik, C., Ünlüsavuran, M., Avcı, O., Baltacı, S., Fırtına Topcu, K.; Elaldı, N. Yoğun Bakım Ünitesinde Gelişen Klebsiella pneumoniae Enfeksiyonları: Karbapenem Direnci ve Hasta Mortalitesi ile İlgili Risk Faktörleri [Klebsiella pneumoniae Infections in the Intensive Care Unit: Risk Factors Related to Carbapenem Resistance and Patient Mortality]. Mikrobiyoloji bulteni 2020, 54, 378–391. [Google Scholar] [PubMed]
- Couvé-Deacon, E. , Mons, F., Garnier, F., Leduc, P., Ponthier, L., Domelier, M., Tristan, A., Ploy, M.C.; Pestourie, N. Neonatal Outbreak of Methicillin-Resistant Staphylococcus aureus Clone Geraldine: A Bundle of Measures to Halt Transmission. Infection control and hospital epidemiology 2017, 38, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Huang, H. , Ran, J., Yang, J., Li, P.; Zhuang, G. Impact of MRSA Transmission and Infection in a Neonatal Intensive Care Unit in China: A Bundle Intervention Study during 2014-2017. BioMed research international 2019, 2019, 5490413. [Google Scholar] [CrossRef] [PubMed]
- Semple, A.; O’Curráin, E.; O’Donovan, D.; Ní Riain, U.; Moylett, E. Neonatal methicillin-resistant Staphylococcus aureus surveillance and management practice: Results of a National Irish Survey. Infection Control & Hospital Epidemiology 2014, 35, 1438–1439. [Google Scholar]
- Xiao, R. , Li, Y., Liu, X., Ding, Y., Lai, J., Li, Y., Kang, W., Zou, P., Wang, J., Du, Y., Zhang, J.; Wang, Y. Antibiotic susceptibility of Escherichia coli isolated from neonates admitted to neonatal intensive care units across China from 2015 to 2020. Frontiers in cellular and infection microbiology 2023, 13, 1183736. [Google Scholar] [CrossRef] [PubMed]
- Khaznadar, O.; Khaznadar, F.; Petrovic, A.; Kuna, L.; Loncar, A.; Omanovic Kolaric, T.; Mihaljevic, V.; Tabll, A.A.; Smolic, R.; Smolic, M. Antimicrobial Resistance and Antimicrobial Stewardship: Before, during and after the COVID-19 Pandemic. Microbiology Research 2023, 14, 727–740. [Google Scholar] [CrossRef]
- Ronan, F. O'Toole, The interface between COVID-19 and bacterial healthcare-associated infections. Clinical Microbiology and Infection 2021, 27, 1772–1776. [Google Scholar]
- Biondo, C. , Ponzo, E., Midiri, A., Ostone, G.B.; Mancuso, G. The Dark Side of Nosocomial Infections in Critically Ill COVID-19 Patients. Life 2023, 13, 1408. [Google Scholar] [CrossRef]
Figure 1.
Prevalence of the etiological agents reported as HAI.
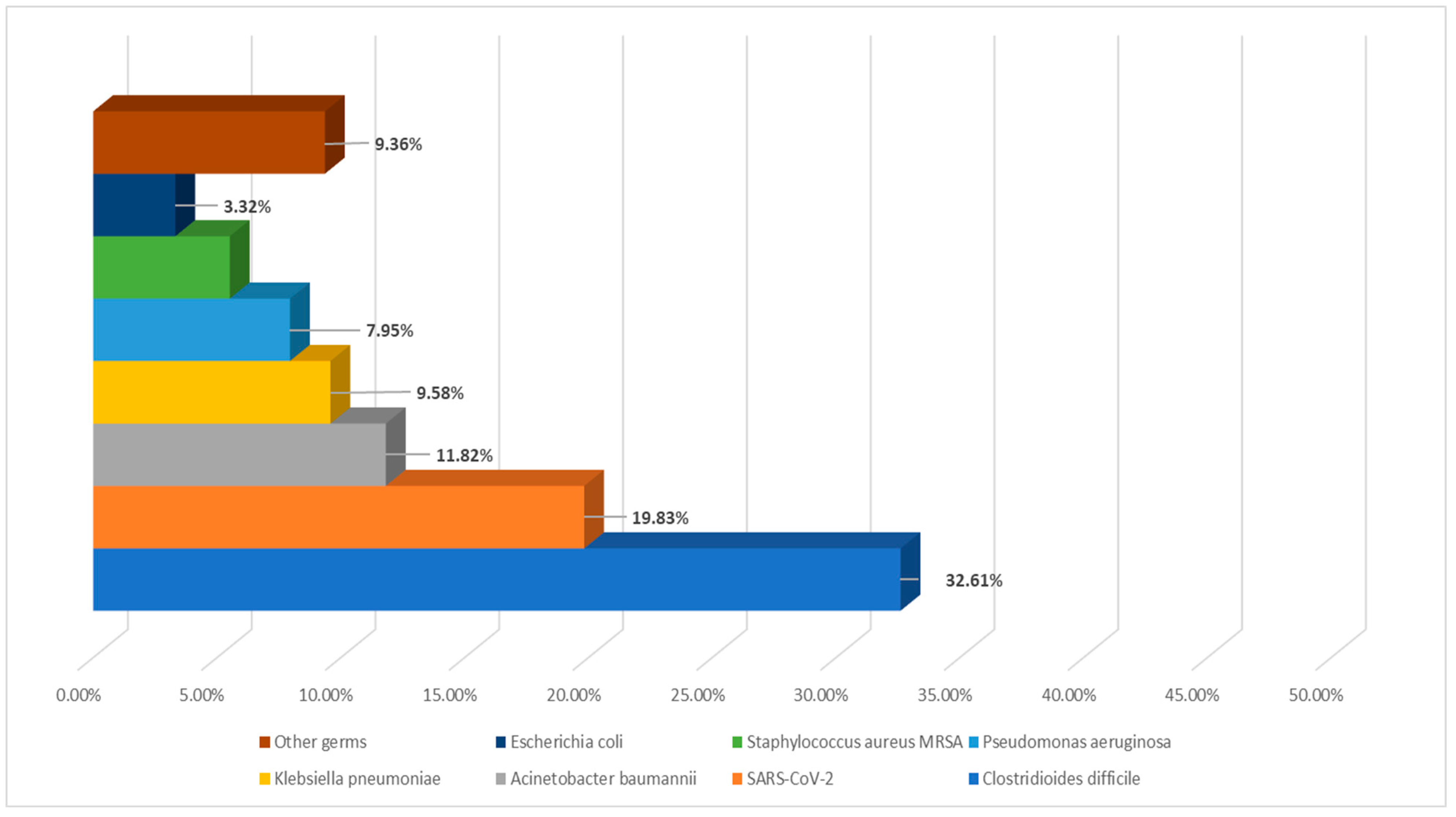
Figure 2.
The identification of the pathogen based on the specific department examined.
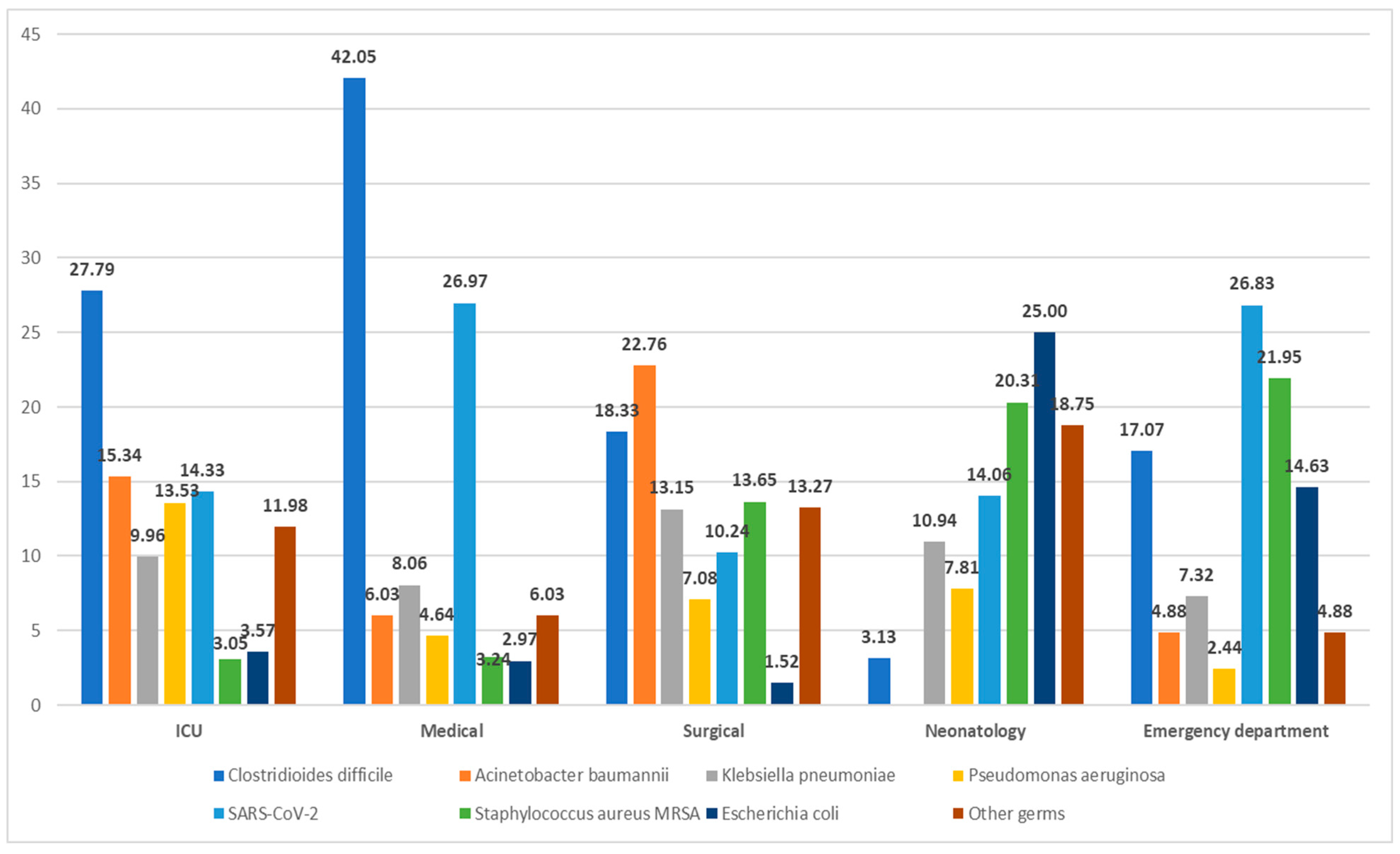
Figure 3.
The prevalence of etiological agents according to the type of HAI infection.
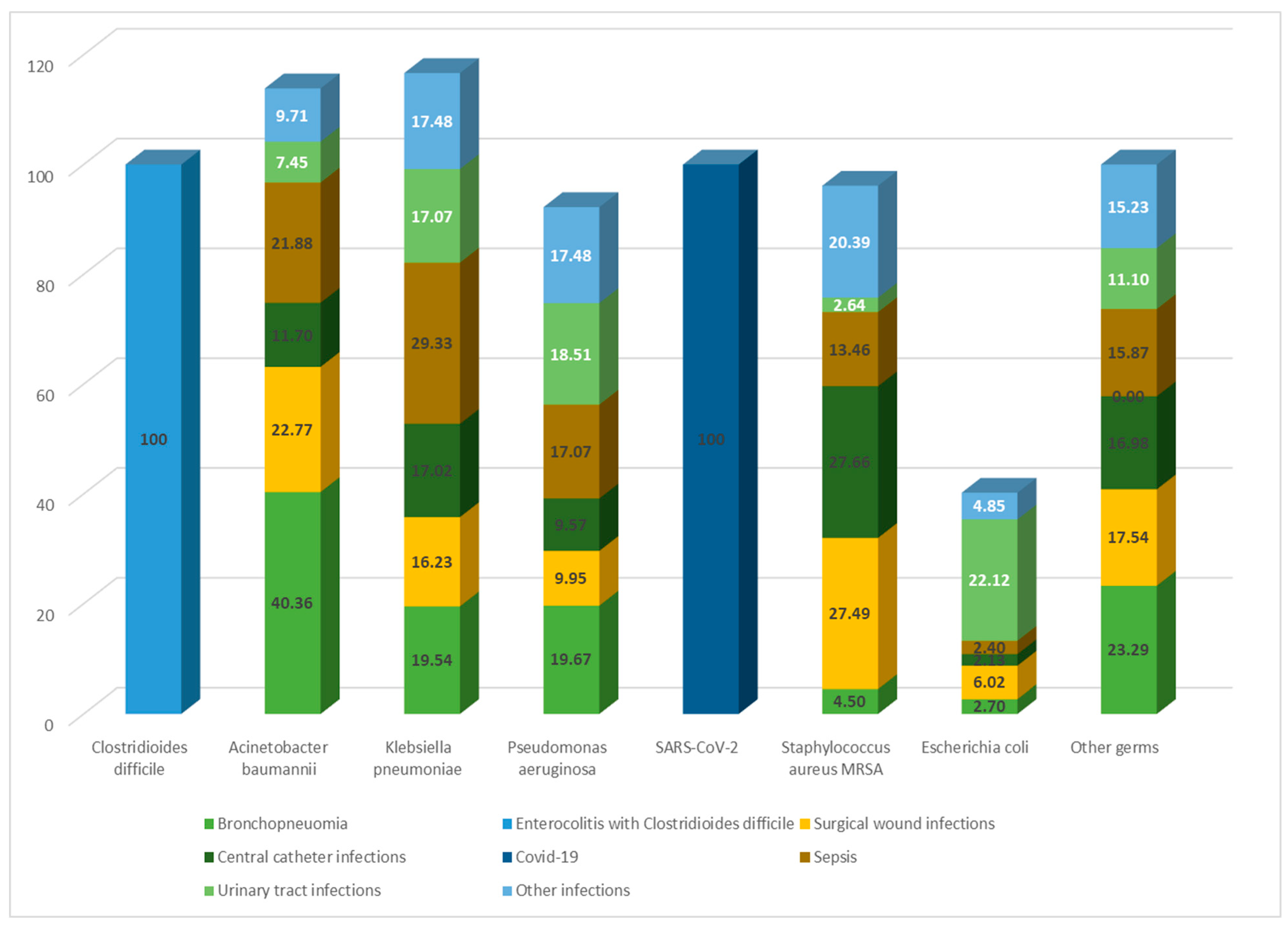
Figure 4.
The distribution of the pathogen according to the patient’s status upon discharge.
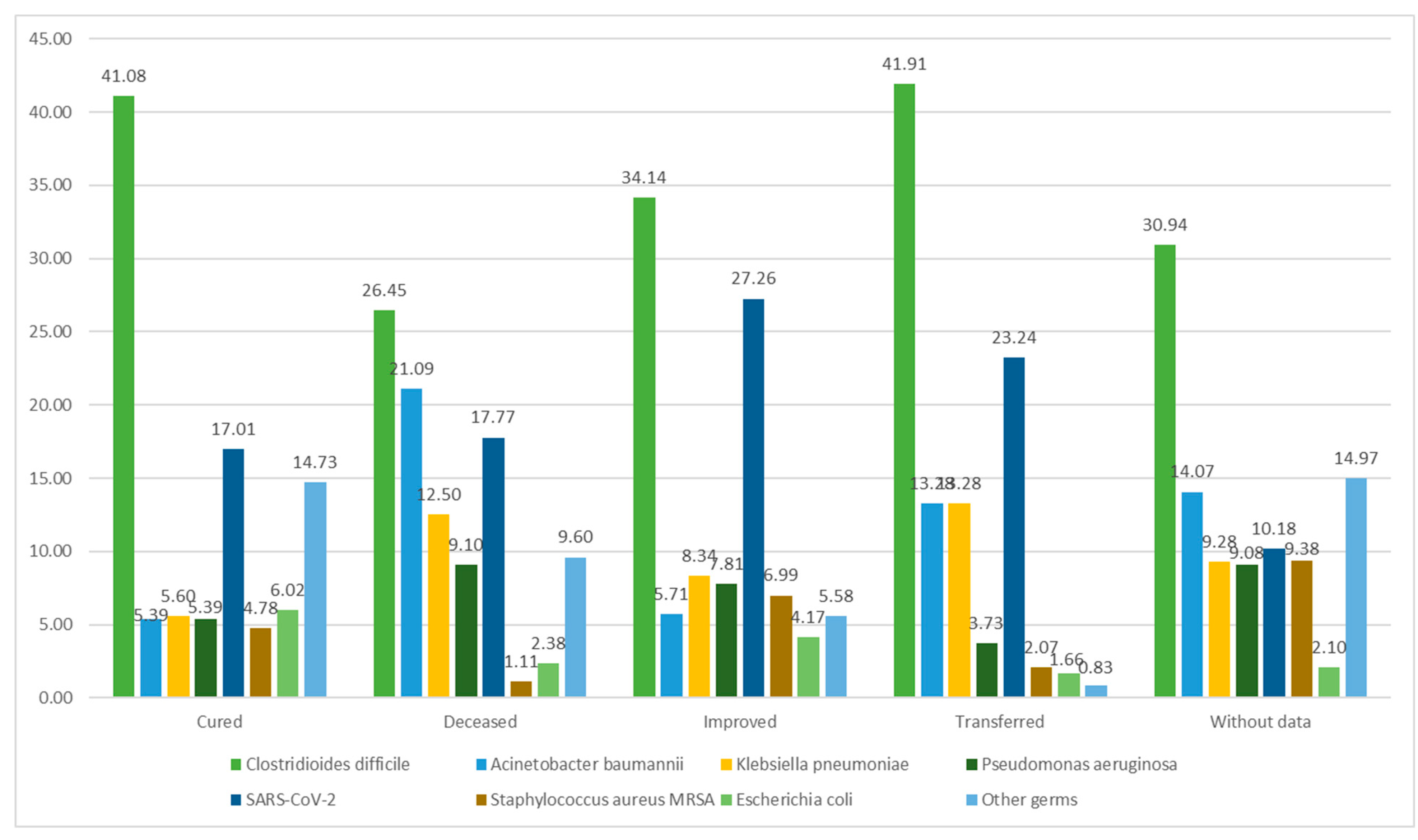
Figure 5.
The identification of the pathogen in relation to the patient's isolation and contact history.
Figure 5.
The identification of the pathogen in relation to the patient's isolation and contact history.
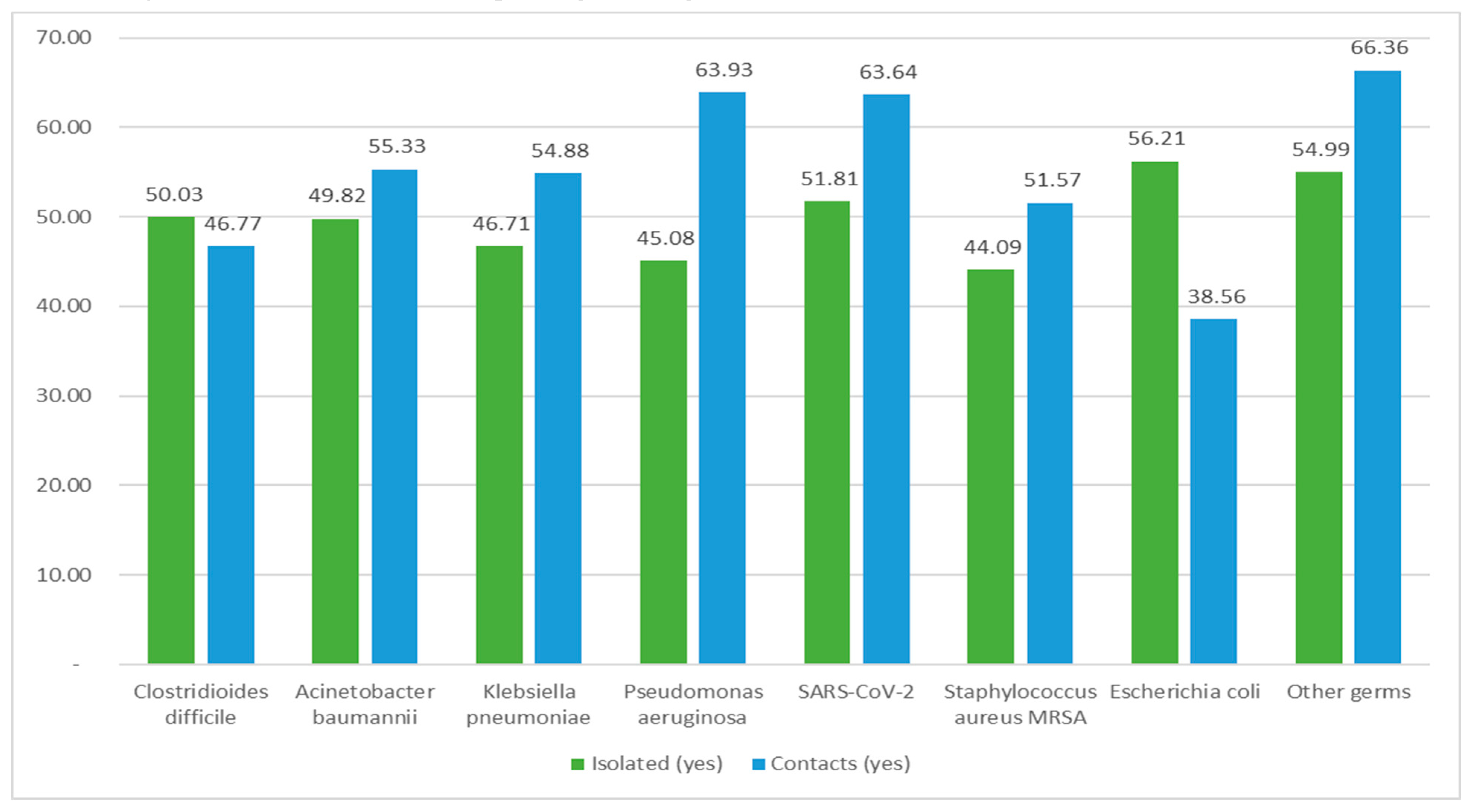
Figure 6.
The occurrence of the causative agents throughout the studied timeframe.
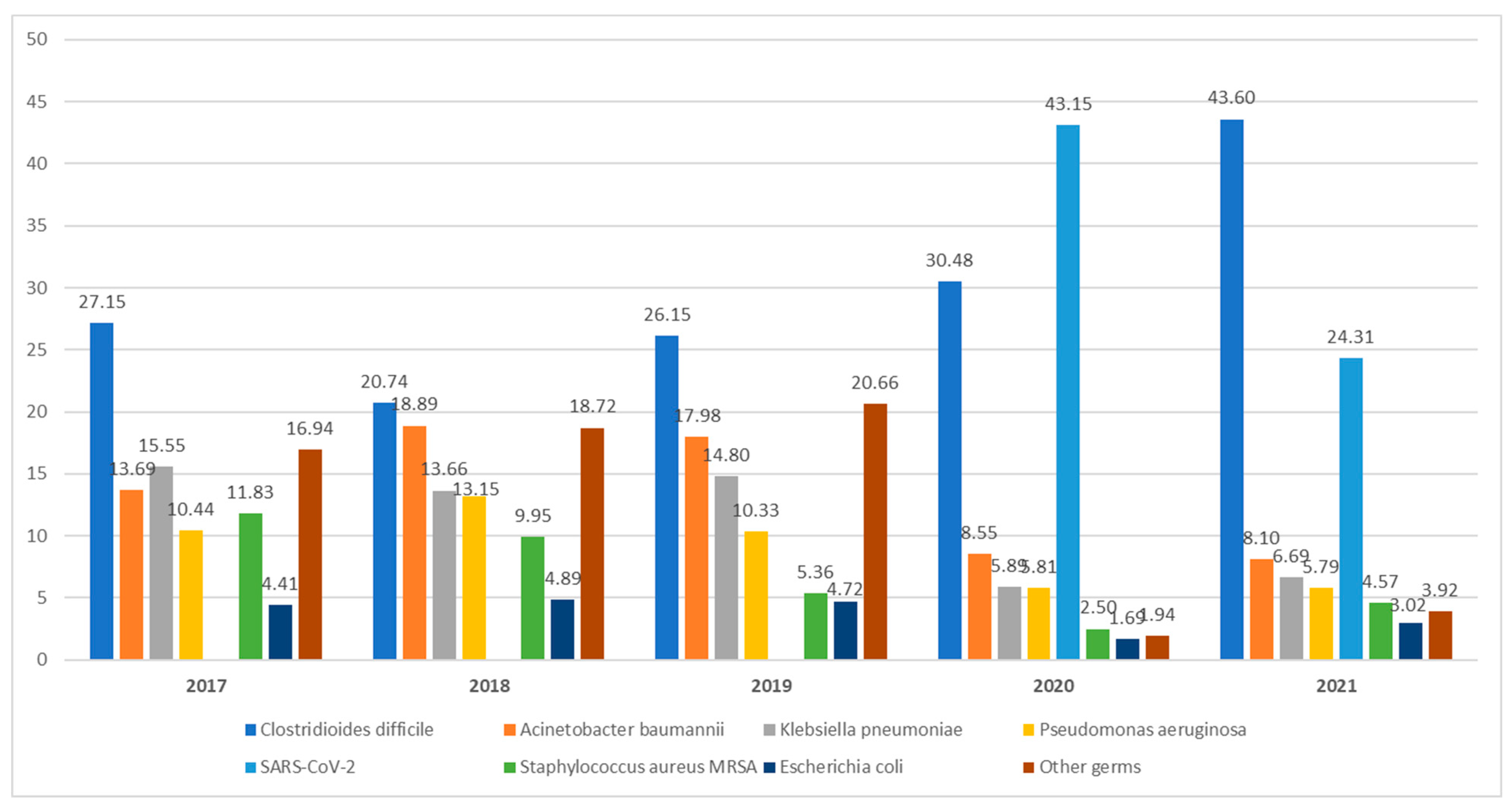

Table 1.
Characteristics of the study group.
| Caption | Number (4603) | Percentage (%) |
| Age (mean ± SD) | 60.27±21.67 | 0-99 years |
| Gender (males) | 2454 | 53.31 |
| Residence (urban) | 2493 | 54.16 |
| Isolated (yes) | 2301 | 49.99 |
| Contacts (yes) | 2536 | 55.09 |
| Section type | ||
| Intensive care unit | 1486 | 32.28 |
| Surgical | 791 | 17.18 |
| Medical | 2221 | 48.25 |
| Neonatology | 64 | 1.39 |
| Emergency department | 41 | 0.90 |
| Types of infections | ||
| Bronchopneumonia | 778 | 16.90 |
| Enterocolitis with Cl. diff. | 1501 | 32.61 |
| Surgical wound infections/tissue infection | 382 | 8.30 |
| Systemic infections (sepsis) | 416 | 9.04 |
| Central catheter infections | 94 | 2.04 |
| Urinary tract infections | 416 | 9.04 |
| Covid 19 | 913 | 19.83 |
| Others | 103 | 2.24 |
| Origin of the case | ||
| From the reported hospital | 4257 | 92.48 |
| From another hospital | 234 | 5.08 |
| Chronic/elderly care units | 27 | 0.59 |
| Other types of medical care | 85 | 1.85 |
| Status on discharge | ||
| Cured | 482 | 10.47 |
| Improved | 1702 | 36.98 |
| Deceased | 1176 | 25.55 |
| Transferred to another unit | 241 | 5.24 |
| No data | 1002 | 21.77 |
| Cause of death | ||
| Possibly caused by the HAI | 325 | 7.06 |
| Not related to HAI | 935 | 20.31 |
| Unknown | 153 | 3.32 |
| No data | 3190 | 69.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



