Submitted:
14 November 2023
Posted:
15 November 2023
You are already at the latest version
Abstract
To evaluate the effect of middle meningeal artery embolization (MMAE) on chronic subdural hematoma (CSDH). We enrolled consecutive patients with CSDH who underwent burr hole craniostomy (BHC) between January 2021 and February 2023. The primary outcome was recurrence rate, defined as an increase of hematoma width on imaging compared with the immediate postoperative imaging at a 3-month follow-up. Secondary outcomes included the rate of complications and adverse prognosis. Cohorts were balanced using 1:2 propensity score matching (PSM). A total of 271 patients were eligible for this study and divided into the MMAE group (n=23) and the BHC group (n=205). Compared with the BHC group, there was more use of anticoagulant or antiplatelet medication (47.8% vs 22.4%, P=0.008), bilateral hematoma (19.5% vs 19.5%, P=0.043) and hematoma with septations (47.8% vs 21.5%, P=0.005) in the MMAE group. After PSM, 64 cases were finally successfully matched. The logistic analysis result showed that MMAE was associated with the decreased recurrence rate of CSDH in the cohort after PSM (OR 0.072, 95%CI 0.322~0.746, P=0.028) but not with the improved clinical prognosis (OR 0.065, 95%CI 0.533~4.786, P=0.562). MAAE has a positive therapeutic effect on reducing the recurrence rate of CSDHs as an adjunct postoperative treatment after burr hole surgery.
Keywords:
chronic subdural hematoma
; middle meningeal artery embolization
; propensity score matching
; burr hole craniostomy
1. Introduction
Chronic subdural hematoma (CSDH) is a common neurosurgical disease characterized by blood collection in the space between the dura and arachnoid. The inciting event is often minor head trauma, followed by inflammation leading to the development of the disease [1]. CSDH generally develops over three or more weeks after trauma [2]. Latest estimates of the overall incidence of CSDH range from 1.7 to 20.6 per 100,000 persons-years, exceptionally high in the elderly population [3]. Owing to an aging population and widespread use of anticoagulants or antiplatelet drugs, the incidence of CSDH uprises steadily [4]. There is no doubt that CSDH will become an important public health issue in the future.
The mechanism underlying the formation and progression of CSDH is still controversial. The widely accepted hypothesis is that the appearance of membranes with permeable neo vessels secondary to hematoma formation is the main cause of CSDH progression or recurrence [5]. Most patients are asymptomatic in the early stages of the disease. As the hematoma expands, the intracranial pressure increases, compressing the adjacent brain parenchyma [6], which may lead to various clinical manifestations, including cognitive impairment, gait disturbance, limb weakness, or headache [7]. The diagnosis is made based on cranial imaging [8].
Surgical evacuation of the subdural collection remains the preferred treatment option for symptomatic patients [9]. A review of CSDH treatment suggested that burr hole craniostomy (BHC) had the best cure-to-complication ratio, which was still the first-line option for surgical treatment in clinical practice for symptomatic CSDH patients [10]. However, the hematoma recurs in 10 to 20% of surgically treated patients, especially in elderly patients with more risk factors for recurrence [11,12]. Moreover, preoperative withdrawal of anticoagulant and antiplatelet drugs, surgery with general anesthesia, and potentially longer postoperative hospitalizations carry higher perioperative risks. Therefore, current studies focus on exploring more safe and effective treatment options for CSDH.
Regrettably, although non-surgical treatment modalities such as steroids, antifibrinolytics, and statins may be effective, high-quality evidence is still lacking, limiting their routine use in the clinic [13]. With the in-depth understanding of the pathophysiology mechanism, the current studies indicate that the accumulation of blood between the dura and arachnoid initiates an inflammatory response [14], comprising dural border cell and fibroblast proliferation, granulation tissue formation, the release of angiogenic factors, and macrophage deposition [11]. This inflammatory response results in a hematoma membrane formation within several weeks after the primary injury. Repeated Micro-hemorrhage from fragile membrane capillaries is the putative contributor to the progression or recurrence of CSDH [15,16]. These neo-membrane capillaries are supposed to communicate with the middle meningeal artery (MMA) [17]. Based on this hypothesis, middle meningeal artery embolization (MMAE) emerges as a promising treatment option. Some studies have reported the therapeutic effect and safety of MMAE at present [18]. Most studies suggest that MMAE effectively reduces the recurrence rate, and the incidence of complications is lower than that of conventional management [19].
However, most studies on MMAE are single-center and retrospective with a small sample size [20]. More importantly, the heterogeneity in the presentation of data in many studies makes it difficult to make comparisons between studies and draw reliable conclusions. In addition, current studies generally adopt postoperative recurrence rates to evaluate the effectiveness of surgical approaches, which are disturbed by multiple risk factors that often statistically differ between the two cohorts. This study retrospectively compares the efficacy and safety of MMAE and BHC in patients with recurrent CSDH, using propensity score matching (PSM) to adjust for confounding factors in a screened population with similar baseline data.
2. Methods
2.1. Study design
This is a monocentric retrospective study. All patients with CSDH who underwent BHC between January 2021 and February 2023 were enrolled. Middle meningeal artery embolization (MMAE) was performed as an adjunct postsurgical treatment in patients with recurrent CSDH or high recurrence risk. MMAE was a concerted decision taken by the neurosurgery and interventional neuroradiology departments. Patients' clinical and pathological data were retrospectively retrieved from electronic medical systems. And we exclude patients with (1) other intracranial diseases that affected subdural hematoma, including vascular diseases, brain tumor, arachnoid cyst, spontaneous intracranial hypotension; (2) poor medical condition that presented in a moribund state or life expectancy of less than 3 months; (3) severe coagulation and hepatorenal dysfunction; (4) incomplete radiologic data or loss of follow-up. Patients were divided into the MAAE group and BHC group according to whether accepting MAAE. The institutional review board approved this study (CERAR IRB 00010254-2020-014). The need for signed patient consent was waived.
2.2. Embolization procedure
MMAE was performed with local anesthesia. Systemic heparinization was not used. The procedure was often performed as follows: A 5F or 6F guiding catheter was navigated into the common carotid artery through the femoral or radial sheath. And a microcatheter (Excelsior SL-10; Stryker Neurovascular, Fremont, Calif) was navigated into the MMA using a guidewire (Synchro-14; Stryker Neurovascular). Selective angiography through the microcatheter was performed to select target MMA branches and check for potentially dangerous collateral vessels. If no collaterals were observed, target branches were embolized with Onyx (18, Medtronic). The embolization procedure was considered successful when all target MMA branches were embolized without procedural complications. The specific MMAE strategy was at the discretion of the attending physician.
2.3. Follow-up and Data Collection
Demographic and clinical data were obtained retrospectively from the electronic medical record system, including age, sex, history of head trauma, use of anticoagulant or antiplatelet medication, atorvastatin, hypertension, diabetes mellitus, smoking, and chronic alcoholism. All patients underwent head CT for preoperative evaluation of subdural hematoma, including side, width, midline shifting, density, and hematoma of septation. For patients with bilateral hematoma or multiple operations, we recorded the maximum width of the hematoma. Brains with widely dilated sulci and subdural space were considered brain atrophy. Clinical and radiologic follow-up examinations with CT scans were performed 1 and 3 months after surgery. The mRS scores were collected by telephone discussions 90 days (±14) after surgery.
2.4. Study outcomes
The primary outcome was recurrence rate, defined as the reoperation rate to treat a recurrent CSDH or an increase of hematoma width on imaging during a 3-month follow-up compared with immediate postoperative imaging. One of the secondary outcomes was the rate of complications, defined as any adverse event related to the procedure, including all surgical and endovascular complications, for a safety measure. Adverse prognosis, another one of the secondary outcomes, is defined as the modified Rankin Scale (mRS) score >2 at least three months after treatment.
2.5. Statistical analysis
The Wilcoxon rank-sum test was used for continuous variables. And the x2 or Fisher exact test was used for nominal factors to compare baseline characteristics. Propensity score matching (PSM) analysis was used to minimize the potential confounders and selection bias, balancing the patient baseline characteristics between groups. The propensity score was estimated for each patient using a multivariate logistic regression model, and a 1:2 group matching was performed using the nearest-neighbor matching method without replacement. Variables including use of anticoagulant or antiplatelet medication, bilateral hematoma, and hematoma of septation were matched. A caliper width of 0.2 standard deviations was set to prevent poor matching. All statistical analyses were performed using the R program (version 4.2.0, R foundation for Statistical Computing, Vienna, Austria) with the Survival and Survminer packages. Then a comparison of outcomes between groups was performed using logistic regression analysis, and an adjusted odds ratio (OR) and 95% confidence interval (CI) were provided.
3. Results
3.1. Baseline characteristics
Two hundred seventy-one consecutive CSDH patients who underwent BHC between January 2021and February 2023 were enrolled in this research. The flowchart is presented in Figure 1. According to pre-set exclusion criteria, 43 patients were excluded because of poor general condition, other intracranial diseases, incomplete radiologic data and loss of follow-up.
Figure 1.
Flowchart of the study.
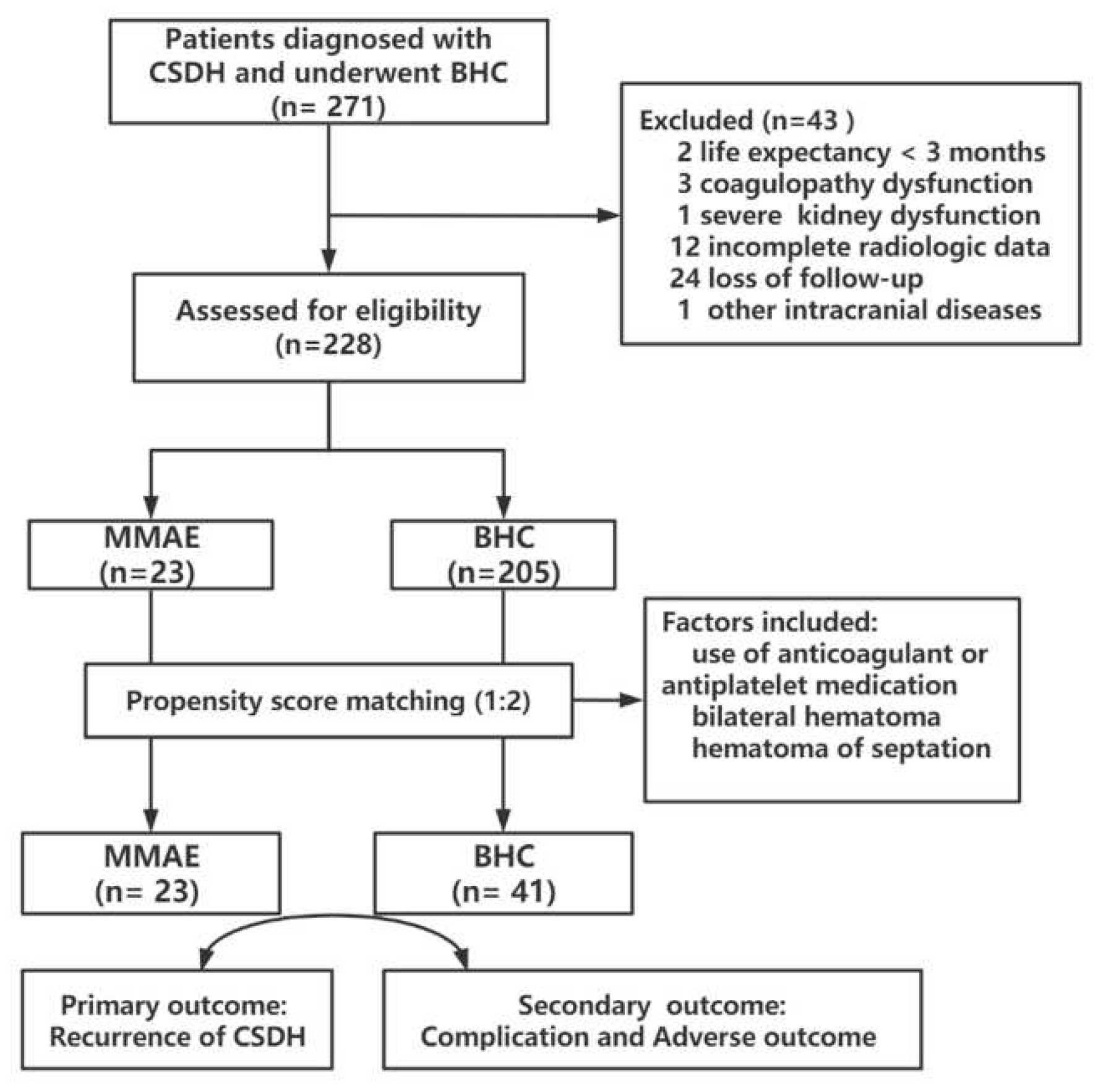
Twenty-three patients underwent the MMAE procedure as an adjuvant treatment after BHC and 205 patients underwent BHC alone. Baseline characteristics of the MMAE and BHC groups are summarized in Table 1. Compared with the BHC group, the use of anticoagulant or antiplatelet medication was more common in patients accepting MMAE (47.8% vs 22.4%, P=0.008). Through analysis of radiologic data, there are more bilateral hematoma (19.5% vs 19.5%, P=0.043) and hematoma with septations (47.8% vs 21.5%, P=0.005) in MMAE group. Although without statistically significant difference, the patients in the MMAE group tended to be older (71.7 ± 8.9 vs. 67.6 ± 11.2, P=0.064), with more hyper- or mixed-dense hematoma.

Table 1.
Baseline characteristics of the all patients.
| Factors | MMAE N=23 |
BHC N=205 |
P value |
|---|---|---|---|
| Age (y) | 71.7 ± 8.9 | 67.6 ± 11.2 | 0.064 |
| Male sex (%) | 15 (65.2) | 162 (79.0) | 0.132 |
| Trauma history (%) | 9 (39.1) | 82 (40.0) | 0.944 |
| Use of anticoagulant or antiplatelet medication (%) | 11 (47.8) | 46 (22.4) | 0.008 |
| Atorvastatin (%) | 20 (87.0) | 186 (90.7) | 0.564 |
| Hypertension (%) | 12 (52.2) | 86 (42.0) | 0.352 |
| Diabetes mellitus (%) | 3 (13.0) | 46 (22.4) | 0.305 |
| Smoking (%) | 2 (8.7) | 36 (17.6) | 0.277 |
| Chronic alcoholism (%) | 3 (13.0) | 18 (8.4) | 0.452 |
| Brain atrophy (%) | 4 (17.4) | 23 (11.2) | 0.384 |
| Hematoma width (mm) | 22.4 ± 4.6 | 19.8 ± 12.9 | 0.895 |
| Bilateral hematoma (%) | 9 (39.1) | 40 (19.5) | 0.043 |
| Midline shift >10 (%) | 7 (30.4) | 51 (24.9) | 0.566 |
| Hematoma density (%) | 0.087 | ||
| Hypodense/ isodense | 9 (39.1) | 119 (58.0) | |
| Hyperdense/ mixed density | 14 (60.9) | 86 (42.0) | |
| Hematoma of septation (%) | 11 (47.8) | 44 (21.5) | 0.005 |
Data are mean±SD, or n (%); MMAE: middle meningeal artery embolization; BHC: burr hole craniostomy; PSM propensity score matching.
3.2. Multivariate logistic regression
A multivariable logistic regression analysis was then performed to explore the factors related to the recurrence of CSDH in all participants. Variables with a P < 0.05 in univariable analysis were entered into a multivariable logistic regression model, including the use of anticoagulant or antiplatelet medication, bilateral hematoma, and hematoma of septation. Combined with clinical experience and previous studies, age, hematoma width and hematoma density were also included in the model.
The results demonstrated the use of anticoagulant or antiplatelet medication (aOR=6.821, 95% CI 1.416~13.549, P=0.024) and hematoma of septation (aOR=2.947, 95% CI 1.291~3.328, P=0.035) were independent risk factors for the recurrence of CSDH (Table 2). Other differences were not statistically significant.
Table 2.
Multivariate logistic regression analysis of factors related to the recurrence of CSDH.
| Factors | All patients N=228 |
aOR# | 95% CI | P value |
|---|---|---|---|---|
| Age | 68.1 ± 10.9 | 1.014 | 0.995~1.023 | 0.197 |
| Use of antiplatelet or anticoagulants medication | 57 (25.3) | 6.721 | 1.416~13.549 | 0.024 |
| Bilateral hematoma | 49 (21.5) | 1.357 | 0.758~2.237 | 0.234 |
| Hematoma of hyperdense or mixed density | 100 (48.9) | 2.432 | 0.942~1.455 | 0.062 |
| Hematoma of septation | 55 (24.1) | 2.947 | 1.291~3.328 | 0.035 |
Data are mean±SD, n (%) or median (IQR); aOR, adjusted odds ratio; # Variables included age, use of anticoagulant or antiplatelet medication, bilateral hematoma, hematoma of septation, hematoma width and hematoma density.
3.3. propensity score matching
We used propensity score matching to adjust confounders, ensuring an even distribution of baseline characteristics between the two groups. Variables in the PSM were determined based on previous univariate analysis and logistic analysis and combined with clinical experience, including the use of anticoagulant or antiplatelet medication, bilateral hematoma, and hematoma of septation. Finally, 64 cases were successfully matched (Table 3), and the absolute standardized mean difference (SMD) of all factors < 10% indicated that the matching effect was satisfactory. After PSM, all these baseline characteristics and clinical features became well balanced and comparable between the MMAE and BHC groups (all P>0.05). There was no significant difference in use of anticoagulant or antiplatelet medication (47.8% vs 29.3%, P=0.143), bilateral hematoma (39.1% vs 22.0%, P=0.277) and hematoma of septation (47.8% vs 36.6%, P=0.381)
Table 3.
Baseline characteristics of the patients after propensity score matching.
| Factors | MMAE N=23 |
BHC after PSM N=205 |
P value |
|---|---|---|---|
| Age (y) | 71.7 ± 8.9 | 69±7.9 | 0.741 |
| Male sex (%) | 15 (65.2) | 28 (68.2%) | 0.804 |
| Trauma history (%) | 9 (39.1) | 16 (39.0%) | 0.995 |
| Use of anticoagulant or antiplatelet medication (%) | 11 (47.8) | 12 (29.3%) | 0.143 |
| Atorvastatin (%) | 20 (87.0) | 38 (92.7%) | 0.215 |
| Hypertension (%) | 12 (52.2) | 16 (39.0%) | 0.316 |
| Diabetes mellitus (%) | 3 (13.0) | 6 (14.6%) | 0.918 |
| Smoking (%) | 2 (8.7) | 6 (14.6%) | 0.493 |
| Chronic alcoholism (%) | 3 (13.0) | 3 (7.3%) | 0.456 |
| Brain atrophy (%) | 4 (17.4) | 5 (12.2%) | 0.572 |
| Hematoma width (mm) | 22.4 ± 4.6 | 21.3 ± 7.3 | 0.657 |
| Bilateral hematoma (%) | 9 (39.1) | 9 (22.0%) | 0.277 |
| Midline shift >10 (%) | 7 (30.4) | 11 (26.8%) | 0.763 |
| Hematoma density (%) | 0.578 | ||
| Hypodense/ isodense | 9 (39.1) | 19 (46.3) | |
| Hyperdense/ mixed density | 14 (60.9) | 22 (53.7%%) | |
| Hematoma of septation (%) | 11 (47.8) | 15 (36.6%) | 0.381 |
Data are mean±SD, or n (%); MMAE: middle meningeal artery embolization; BHC: burr hole craniostomy; PSM propensity score matching;.
3.4. Comparison of Treatment Outcomes
The recurrence rate during the 3-month follow-up in the MMAE group was lower than the BHC group after PSM (1/23(4.3%) vs 5/41(12.1%)). Surgical complications occurred in 2 patients (1 cerebral infarction and 1 seizure) in the BHC group after PSM, while no complications occurred in the MMAE group (Figure 2). Of 41 patients in the BHC group, 11 (26.8%) had an adverse prognosis defined as mRS>2 at 3 months after the operation. Four (17.8%) patients had an adverse outcome in the MMAE group. The logistic analysis result showed that MMAE was associated with the decreased recurrence rate of CSDH (OR 0.072, 95%CI 0.322~0.746, P=0.028) but not with the improved clinical prognosis (OR 0.065, 95%CI 0.533~4.786, P=0.562) (Table 4).
4. Discussion
CSDH has been confirmed as a detrimental health event related to a reduction in long-term survival. This incidence is increasing with population age, posing a severe threat to the health of the elderly population [21]. BHC remains the recommended surgical approach in much literature if the patient has evidence of moderate to severe cognitive impairment or progressive neurological deterioration attributable to chronic SDH [22]. However, conventional surgical methods do not target the mechanism of occurrence and development of subdural hematoma with a recurrence rate of 10-20% [11]. It is reported that the complication rate of BHC is 9.3% [23]. For older patients, repeated experiences of this type of surgery undoubtedly increase the risk of death and disability [24]. Therefore, there is an urgent need for less invasive surgical options. Recent studies suggest that, in cases of traumatic etiology, the exact vascular source of hemorrhage is the bridging veins between the cerebral cortex and dural-venous sinuses, which are especially fragile in the elderly population with brain atrophy [25]. The collection of blood and its decomposition products incite the persistent inflammatory response, resulting in dural border cell and fibroblast proliferation, granulation tissue formation, the release of angiogenic factors, and macrophage deposition, ultimately forming the hematoma membrane [26]. Histopathology and angiography have shown that the hematoma membrane with neovascularization communicated with the peripheral end of the middle meningeal artery of the CSDH patient Histopathology and angiography have demonstrated that the hematoma membrane with neovascularization communicated with the peripheral end of the middle meningeal artery of the CSDH patient [27]. These findings indicate that the middle meningeal artery plays a key role in the occurrence and development of CSDH.
Some nonsurgical treatments target the underlying pathophysiology, including corticosteroids, antifibrinolytics, statins, and angiotensin-converting enzyme inhibitors [28,29,30]. However, there is currently a lack of high-quality clinical evidence, and drug therapies are still hard to replace the surgical treatment for CSDH, especially for patients with surgical indications. Middle meningeal artery embolization is prospected to be a therapeutic method targeting the mechanism of CSDH [31]. MMAE provides a minimally invasive surgical approach that targets the pathophysiological mechanisms underlying CSDH, as described above, hematoma membrane and fragile neovascularization communicated with MMA [15]. Moreover, patients are not requested to discontinue antiplatelet drugs or anticoagulation, avoiding complications such as cerebral infarction, coronary heart disease, and other vascular diseases caused by drug withdrawal [32]. Most clinical studies have proved that MAAE can effectively reduce the recurrence rate and has high safety [19,33].
In related studies, the timing of MMAE is mainly in three aspects: upfront treatment for untreated CSDH, prophylactic treatment after conventional surgery, and recurrent CSDH after conventional surgery [18]. Sam et al. designed a prospective study of prophylactic treatment after BHC. Twenty-one of 48 patients underwent additional MMAE after conventional surgery. They presented significantly more resorbed hematoma volume than the control group 3 months after surgery [34]. An earlier single-center study of MAA as an alternative to BHC showed that patients who received MAA alone had significantly lower treatment failure rates, recurrence rates, and treatment-related complication rates compared with conventional surgery [35]. Nevertheless, the patients in the MMA group with worse baseline characteristics include more history of hypertension, antiplatelet drugs or anticoagulant medication, and separated or trabecular-type hematoma. The presence of confounding factors differed between the two groups, which further illustrated the superiority of MMAE.
Previous studies demonstrated that factors that affect the recurrence of CSDH might include age, gender, anticoagulant or antiplatelet use, smoking, chronic alcoholism, and several imaging features (such as brain atrophy and characteristics of hematoma) [24]. Up to now, few studies investigate one of these aspects and most only include patients who received MMAE. The main reason is that there is currently no guideline specifying the indications or recommended population for MMAE. In our studies, there were differences in the use of anticoagulant or antiplatelet medication, bilateral hematoma, and hematoma with septations between the MAAE group and BHC group. Moreover, these mixed factors were found to affect the recurrence of CSDH through the multivariate logistic regression analysis. Therefore, PSM, a valuable alternative to reduce selection bias and increase the evidence level, was performed to select patients with matching baseline data for the cohort study. Considering the small sample size for the MAAE group and various confounding factors in the two groups, we chose the 1:2 match methods, with 64 cases successfully matched. The logistic analysis results in the cohort after PSM showed that MMAE was associated with the decreased recurrence rate of CSDH (OR 0.072, 95%CI 0.322~0.746, P=0.028). Furthermore, MMAE did not affect the clinical prognosis, and no complications occurred in the MMAE group.
The major limitations of this study are its retrospective, monocentric, and non-randomized design, with inherent risks of bias. In our center, MAA has not been used as a first-line treatment, so our patients preferred drilling and drainage, and there was no direct MAA without drilling. The selection bias remains objectively after PSM analysis. Although the current application population of MMAE often has a higher risk of recurrence than that of BHC, the results show lower recurrence rates in the MAAE group. From another point of view, it proves that MMAE significantly reduces the recurrence rate. However, to verify this conclusion, a large sample size and prospective studies comparing patients who received MAA or BHC alone are still needed in the future.
5. Conclusions
MMAE is an effective treatment for CSDH. Our research further confirms that, after PSM analysis excluding confounding factors as much as possible, the recurrence rate after MMAE is lower than that of BHC. In the future, MMAE deserves more large prospective trials.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Second Affiliated Hospital of Zhejiang University (Nos. 2021-0042).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Hutchinson, P.J., E. Edlmann, D. Bulters, A. Zolnourian, P. Holton, N. Suttner, K. Agyemang, S. Thomson, I.A. Anderson, Y.Z. Al-Tamimi, D. Henderson, P.C. Whitfield, M. Gherle, P.M. Brennan, A. Allison, E.P. Thelin, S. Tarantino, B. Pantaleo, K. Caldwell, C. Davis-Wilkie, H. Mee, E.A. Warburton, G. Barton, A. Chari, H.J. Marcus, A.T. King, A. Belli, P.K. Myint, I. Wilkinson, T. Santarius, C. Turner, S. Bond, and A.G. Kolias, Trial of Dexamethasone for Chronic Subdural Hematoma. N Engl J Med, 2020. 383(27): p. 2616-2627. [CrossRef]
- Feghali, J., W. Yang, and J. Huang, Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg, 2020. 141: p. 339-345. [CrossRef]
- Miranda, L.B., E. Braxton, J. Hobbs, and M.R. Quigley, Chronic subdural hematoma in the elderly: not a benign disease. J Neurosurg, 2011. 114(1): p. 72-6. [CrossRef]
- Kolias, A.G., A. Chari, T. Santarius, and P.J. Hutchinson, Chronic subdural haematoma: modern management and emerging therapies. Nat Rev Neurol, 2014. 10(10): p. 570-8. [CrossRef]
- Edlmann, E., P.C. Whitfield, A. Kolias, and P.J. Hutchinson, Pathogenesis of Chronic Subdural Hematoma: A Cohort Evidencing De Novo and Transformational Origins. J Neurotrauma, 2021. 38(18): p. 2580-2589. [CrossRef]
- Mehta, V., S.C. Harward, E.W. Sankey, G. Nayar, and P.J. Codd, Evidence based diagnosis and management of chronic subdural hematoma: A review of the literature. J Clin Neurosci, 2018. 50: p. 7-15. [CrossRef]
- Rauhala, M., P. Helén, H. Huhtala, P. Heikkilä, G.L. Iverson, T. Niskakangas, J. Öhman, and T.M. Luoto, Chronic subdural hematoma-incidence, complications, and financial impact. Acta Neurochir (Wien), 2020. 162(9): p. 2033-2043.
- Cecchini, G., Chronic subdural hematoma pathophysiology: a unifying theory for a dynamic process. J Neurosurg Sci, 2017. 61(5): p. 536-543. [CrossRef]
- Bounajem, M., R. Campbell, F. Denorme, and R. Grandhi, Paradigms in chronic subdural hematoma pathophysiology: Current treatments and new directions. The journal of trauma and acute care surgery, 2021. 91(6): p. e134-e141. [CrossRef]
- Smith, M., L. Kishikova, and J. Norris, Surgical management of chronic subdural haematoma: one hole or two? International journal of surgery (London, England), 2012. 10(9): p. 450-2.
- Tiwari, A., A.A. Dmytriw, R. Bo, N. Farkas, P. Ye, D.S. Gordon, K.M. Arcot, D. Turkel-Parrella, and J. Farkas, Recurrence and Coniglobus Volumetric Resolution of Subacute and Chronic Subdural Hematoma Post-Middle Meningeal Artery Embolization. Diagnostics (Basel), 2021. 11(2).
- Duerinck, J., J. Van Der Veken, S. Schuind, F. Van Calenbergh, J. van Loon, S. Du Four, S. Debacker, E. Costa, C. Raftopoulos, O. De Witte, W. Cools, R. Buyl, V. Van Velthoven, J. D'Haens, and M. Bruneau, Randomized Trial Comparing Burr Hole Craniostomy, Minicraniotomy, and Twist Drill Craniostomy for Treatment of Chronic Subdural Hematoma. Neurosurgery, 2022. [CrossRef]
- Berghauser Pont, L., R. Dammers, J. Schouten, H. Lingsma, and C. Dirven, Clinical factors associated with outcome in chronic subdural hematoma: a retrospective cohort study of patients on preoperative corticosteroid therapy. Neurosurgery, 2012. 70(4): p. 873-80; discussion 880.
- Quan, W., Z. Zhang, Q. Tian, X. Wen, P. Yu, D. Wang, W. Cui, L. Zhou, E. Park, A.J. Baker, J. Zhang, and R. Jiang, A rat model of chronic subdural hematoma: Insight into mechanisms of revascularization and inflammation. Brain Res, 2015. 1625: p. 84-96. [CrossRef]
- Edlmann, E., S. Giorgi-Coll, P.C. Whitfield, K.L.H. Carpenter, and P.J. Hutchinson, Pathophysiology of chronic subdural haematoma: inflammation, angiogenesis and implications for pharmacotherapy. J Neuroinflammation, 2017. 14(1): p. 108. [CrossRef]
- Holl, D.C., V. Volovici, C.M.F. Dirven, W.C. Peul, F. van Kooten, K. Jellema, N.A. van der Gaag, I.P. Miah, K.H. Kho, H.M. den Hertog, H.F. Lingsma, and R. Dammers, Pathophysiology and Nonsurgical Treatment of Chronic Subdural Hematoma: From Past to Present to Future. World Neurosurg, 2018. 116: p. 402-411.e2. [CrossRef]
- Hashimoto, T., T. Ohashi, D. Watanabe, S. Koyama, H. Namatame, H. Izawa, R. Haraoka, H. Okada, N. Ichimasu, J. Akimoto, and J. Haraoka, Usefulness of embolization of the middle meningeal artery for refractory chronic subdural hematomas. Surg Neurol Int, 2013. 4: p. 104. [CrossRef]
- Srivatsan, A., A. Mohanty, F.A. Nascimento, M.U. Hafeez, V.M. Srinivasan, A. Thomas, S.R. Chen, J.N. Johnson, and P. Kan, Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: Meta-Analysis and Systematic Review. World Neurosurg, 2019. 122: p. 613-619. [CrossRef]
- Haldrup, M., B. Ketharanathan, B. Debrabant, O.S. Schwartz, R. Mikkelsen, K. Fugleholm, F.R. Poulsen, T.S.R. Jensen, L.V. Thaarup, and B. Bergholt, Embolization of the middle meningeal artery in patients with chronic subdural hematoma-a systematic review and meta-analysis. Acta Neurochir (Wien), 2020. 162(4): p. 777-784. [CrossRef]
- Fiorella, D. and A. Arthur, Middle meningeal artery embolization for the management of chronic subdural hematoma. Journal of neurointerventional surgery, 2019. 11(9): p. 912-915. [CrossRef]
- Manickam, A., L.A. Marshman, and R. Johnston, Long-term survival after chronic subdural haematoma. J Clin Neurosci, 2016. 34: p. 100-104. [CrossRef]
- Santarius, T., P.J. Kirkpatrick, D. Ganesan, H.L. Chia, I. Jalloh, P. Smielewski, H.K. Richards, H. Marcus, R.A. Parker, S.J. Price, R.W. Kirollos, J.D. Pickard, and P.J. Hutchinson, Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet, 2009. 374(9695): p. 1067-73. [CrossRef]
- Ducruet, A.F., B.T. Grobelny, B.E. Zacharia, Z.L. Hickman, P.L. DeRosa, K.N. Andersen, E. Sussman, A. Carpenter, and E.S. Connolly, Jr., The surgical management of chronic subdural hematoma. Neurosurg Rev, 2012. 35(2): p. 155-69; discussion 169. [CrossRef]
- Shen, J., L. Yuan, R. Ge, Q. Wang, W. Zhou, X.C. Jiang, and X. Shao, Clinical and radiological factors predicting recurrence of chronic subdural hematoma: A retrospective cohort study. Injury, 2019. 50(10): p. 1634-1640. [CrossRef]
- Molnár, A., G.L. Nádasy, G. Dörnyei, B.B. Patai, J. Delfavero, G. Fülöp, A.C. Kirkpatrick, Z. Ungvári, and B. Merkely, The aging venous system: from varicosities to vascular cognitive impairment. Geroscience, 2021. 43(6): p. 2761-2784. [CrossRef]
- Zhang, X., D. Wang, Y. Tian, H. Wei, X. Liu, T. Xiang, Y. Fan, C. Gao, J. Huang, Z. Sha, W. Quan, J. Zhang, and R. Jiang, Risk Factors for Atorvastatin as a Monotherapy for Chronic Subdural Hematoma: A Retrospective Multifactor Analysis. Front Aging Neurosci, 2021. 13: p. 726592. [CrossRef]
- Chihara, H., H. Imamura, T. Ogura, H. Adachi, Y. Imai, and N. Sakai, Recurrence of a Refractory Chronic Subdural Hematoma after Middle Meningeal Artery Embolization That Required Craniotomy. NMC Case Rep J, 2014. 1(1): p. 1-5.
- Kwon, S., C. Jin, and K.H. Cho, Oreongsan, an herbal medicine prescription developed as a new alternative treatment in patients with chronic subdural hematoma: a narrative review. Integr Med Res, 2019. 8(1): p. 26-30.
- Wang, H., M. Zhang, H. Zheng, X. Xia, K. Luo, F. Guo, and C. Qian, The effects of antithrombotic drugs on the recurrence and mortality in patients with chronic subdural hematoma: A meta-analysis. Medicine (Baltimore), 2019. 98(1): p. e13972.
- Gong, Z., D. Zhan, M. Nie, X. Li, C. Gao, X. Liu, T. Xiang, J. Yuan, W. Jiang, J. Huang, W. Quan, D. Wang, Y. Tian, H. Yuan, J. Zhang, and R. Jiang, Dexamethasone enhances the efficacy of atorvastatin in inhibiting excessively inflammation-induced abnormal angiogenesis by regulating macrophages. J Neuroinflammation, 2021. 18(1): p. 203.
- Catapano, J.S., C.L. Nguyen, A.A. Wakim, F.C. Albuquerque, and A.F. Ducruet, Middle Meningeal Artery Embolization for Chronic Subdural Hematoma. Front Neurol, 2020. 11: p. 557233.
- Scerrati, A., A. Mangiola, F. Rigoni, S. Olei, M. Santantonio, G. Trevisi, C. Anile, M.A. Cavallo, and D.E.B. P, Do antiplatelet and anticoagulant drugs modify outcome of patients treated for chronic subdural hematoma? Still a controversial issue. J Neurosurg Sci, 2021. 65(6): p. 626-633. [CrossRef]
- Ironside, N., C. Nguyen, Q. Do, B. Ugiliweneza, C.J. Chen, E.P. Sieg, R.F. James, and D. Ding, Middle meningeal artery embolization for chronic subdural hematoma: a systematic review and meta-analysis. J Neurointerv Surg, 2021. 13(10): p. 951-957. [CrossRef]
- Ng, S., I. Derraz, J. Boetto, C. Dargazanli, G. Poulen, G. Gascou, P.H. Lefevre, N. Molinari, N. Lonjon, and V. Costalat, Middle meningeal artery embolization as an adjuvant treatment to surgery for symptomatic chronic subdural hematoma: a pilot study assessing hematoma volume resorption. J Neurointerv Surg, 2020. 12(7): p. 695-699. [CrossRef]
- Ban, S.P., G. Hwang, H.S. Byoun, T. Kim, S.U. Lee, J.S. Bang, J.H. Han, C.Y. Kim, O.K. Kwon, and C.W. Oh, Middle Meningeal Artery Embolization for Chronic Subdural Hematoma. Radiology, 2018. 286(3): p. 992-999.
Figure 2.
Example of a left-sided CSDH receiving middle meningeal artery (MMA) embolization as an adjunct postoperative treatment after burr hole craniostomy. A Preoperative CT showed left chronic hematomas with midline shift (maximum hematoma width, 23.8mm); B At the one-month follow-up, CT showed decrease in maximum width (12.4mm); C At the three-month follow-up, CT showed that the hematoma had been resolved; D Anterior cervical angiography before embolization; E Microcatheter angiography in frontal branch of MMA; F Microcatheter angiography in parietal parietal branch of MMA; G Anterior cervical angiography after embolization.
Figure 2.
Example of a left-sided CSDH receiving middle meningeal artery (MMA) embolization as an adjunct postoperative treatment after burr hole craniostomy. A Preoperative CT showed left chronic hematomas with midline shift (maximum hematoma width, 23.8mm); B At the one-month follow-up, CT showed decrease in maximum width (12.4mm); C At the three-month follow-up, CT showed that the hematoma had been resolved; D Anterior cervical angiography before embolization; E Microcatheter angiography in frontal branch of MMA; F Microcatheter angiography in parietal parietal branch of MMA; G Anterior cervical angiography after embolization.
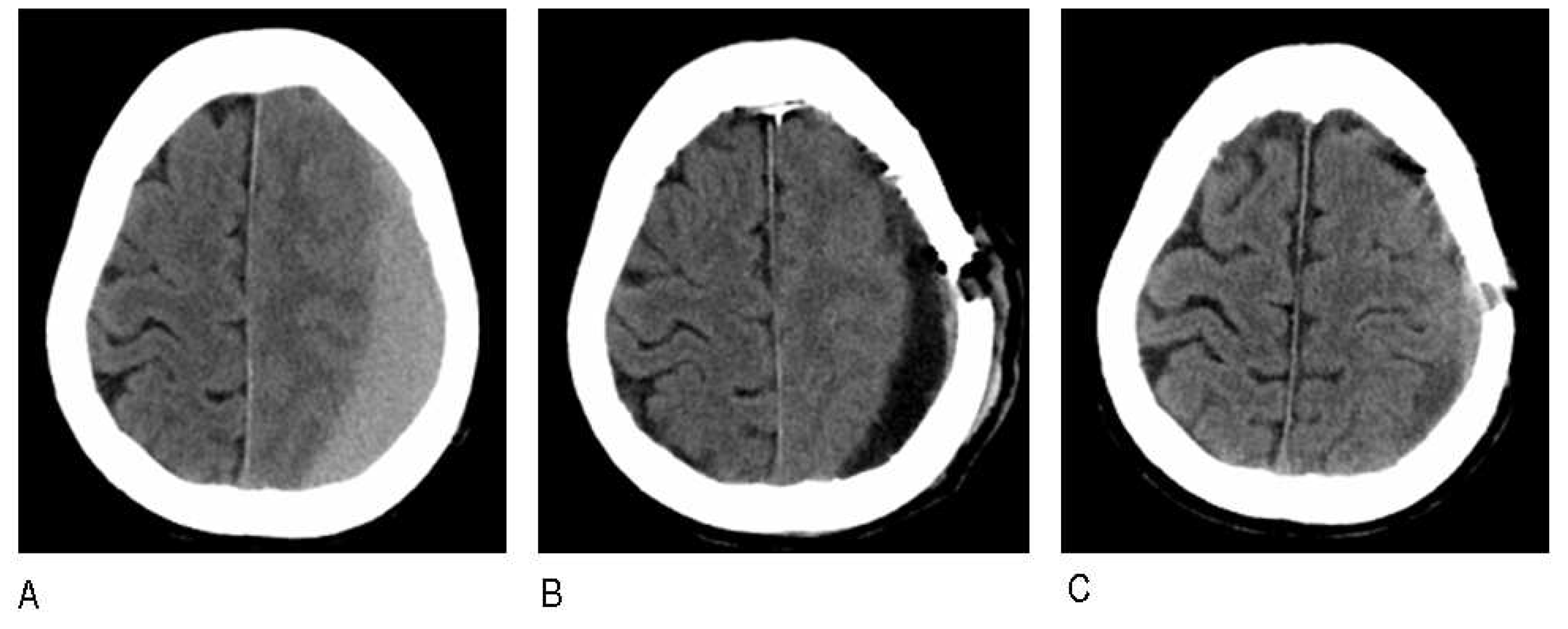
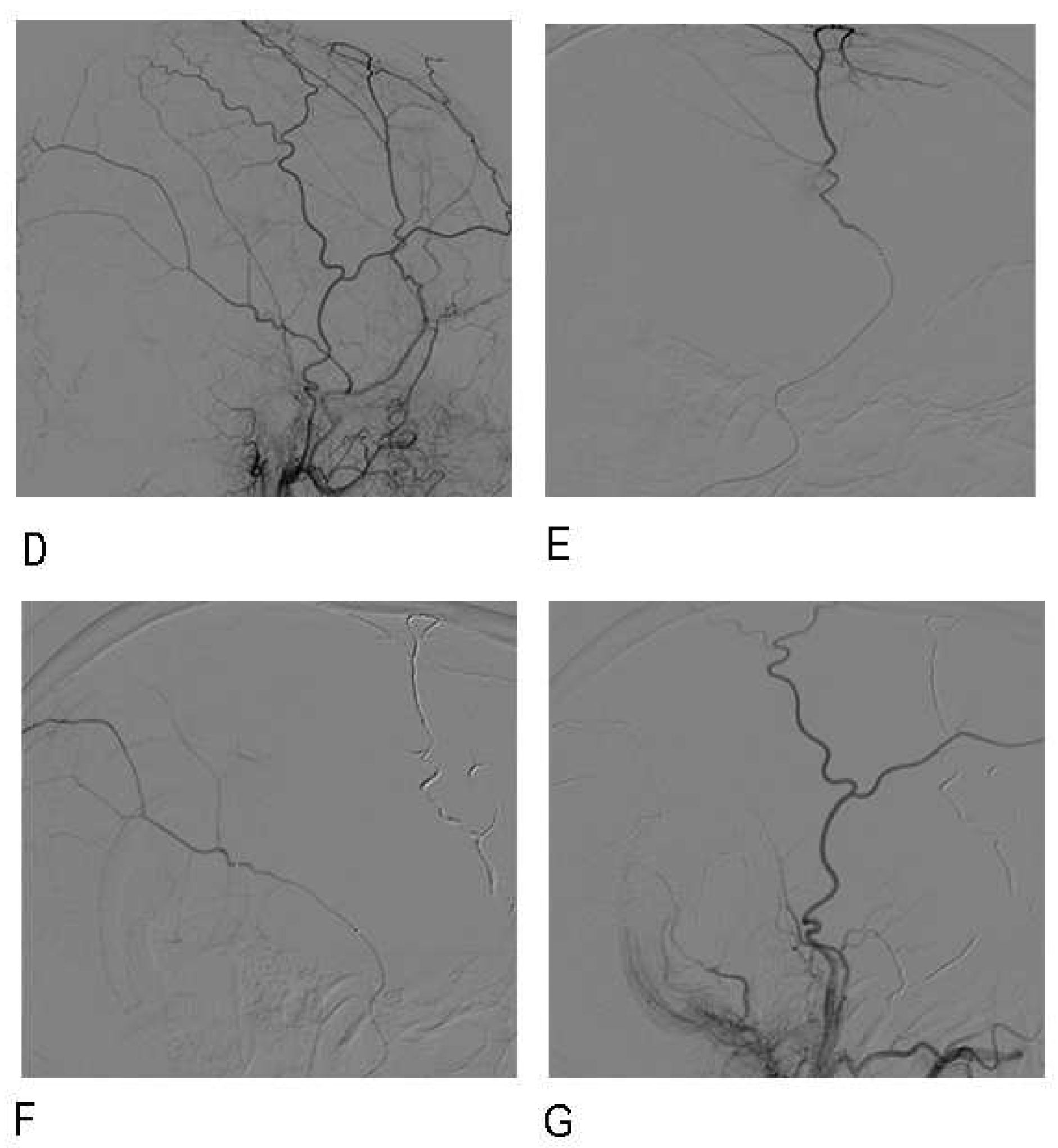
Table 4.
Primary and secondary outcomes in the cohort after PSM.
| Outcome | MMAE N=23 |
BHC after PSM N=41 |
OR (95%CI) | P value |
|---|---|---|---|---|
| Recurrence | 1 (4.3) | 5 (12.1) | 0.072 (0.322~0.746) | 0.028 |
| Complications | 0 (0) | 2 (4.8) | NA | NA |
| Adverse prognosis | 4 (17.8) | 11 (26.8) | 0.065 (0.533~4.786) | 0.562 |
Data are n (%); MMAE: middle meningeal artery embolization; BHC: burr hole craniostomy; PSM propensity score matching.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



