
Submitted:
16 November 2023
Posted:
17 November 2023
You are already at the latest version
Abstract
Handwriting is a complex perceptual-motor task that requires years of training and practice before complete mastering. Its acquisition is crucial since handwriting is the basis, together with reading, for the acquisition of higher-level skills such as spelling, grammar, syntax, and text composition. Despite correct learning and practice of handwriting, some children never master this skill to a sufficient level. These handwriting deficits, referred to as developmental dysgraphia, can seriously impact the acquisition of other skills and thus the academic success of the child if they are not diagnosed and handled early. In this review, we present a non-exhaustive listing of the tools which are the most reported in the literature for the analysis of handwriting and the diagnosis of dysgraphia. Tools focusing on both the final handwriting product and the handwriting process will be considered. We will then discuss the pros and cons of the existing tools, and the perspectives for the development of future tools.
Keywords:
handwriting
; developmental dysgraphia
; product
; process
; diagnosis
1. Handwriting: acquisition and role
Handwriting, considered as language by hand [1], is a complex perceptual-motor task involving attentional, perceptual, linguistic, and fine motor skills. Handwriting occupies a large proportion of children’s daily activities at school [2,3] and is the basis, together with reading, for the acquisition of higher-level skills such as spelling, grammar, syntax, and text composition. A relationship between the mastery of handwriting movement and the quality of writing content has been established, both at the semantic level in text production [4] and at the orthographic level, in word formation [5]. If children pay too much attention to handwriting movements, they may have difficulties in the allocation of cognitive resources to higher-level processes [6].
From a developmental perspective, handwriting originates from drawing, from which it slowly differentiates as the child grows. In younger children, the quality of drawings is correlated to the quality of handwriting [7]. Then, with the acquisition of handwriting, this relationship between drawing and writing quality decreases to eventually disappear [8]. The formal acquisition of handwriting begins around the age of 5 at preschool, and its mastering requires about 10 years of practice and training. The automation of handwriting is partial at the age of 10 (5th-grade) and is considered almost complete around the age of 14 (9th-grade) (for a review, see [9]). During acquisition, handwriting evolves first in terms of quality (primarily between 1st- and 5th-grade), then in terms of speed (from 4th-grade essentially). Efficient, fully automated handwriting relies on a balance between speed and quality: it should be fast enough to allow the retranscription of a course or the transcription of ideas, and of sufficient quality to be readable by the writer and by others.
2. Handwriting deficits
Despite correct learning and practice of handwriting, some children never master this skill to a sufficient level of automation (reviewed in [10,11,12]. These handwriting deficits, referred to as developmental dysgraphia in children, have been defined as a written-language disorder that concerns mechanical writing skills in children of average intelligence and with no distinct neurological or perceptual-motor deficits [13]. Currently, dysgraphia is not recognised as a disorder per se by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) [14] or the International Classification of Diseases 11th edition (ICD-11). The DSM-5 only mentions « deficits in the fine motricity required for handwriting », in the chapter dedicated to the development and evolution of learning disorders. Due to the diversity of methodological approaches and the absence of a consensual definition, the exact prevalence of dysgraphia is not known, and probably differs between countries and writing systems.
Dygraphia is generally found in association with neurodevelopmental disorders, namely dyslexia (DL), Developmental Coordination Disorder (DCD) and Attention Deficit Disorder/Hyperactivity Disorder (ADHD) [15,16,17,18,19,20]. Dysgraphia preferentially affects boys (3:1 ratio), most likely because of the prevalence of the associated disorders in boys [10,21]. Many studies have shown differences handwriting deficits depending on the associated disorder [22,23,24,25,26,27,28]. DCD primarily affects handwriting quality [24,29,30] while DL affects both speed and, to a lesser extent, handwriting quality [28,31]. Children with comorbid DL and DCD present nearly the same profile of difficulties as children with DL, although with a much higher within-group variability. Comorbidity seems to lead to the addition of DCD and DL writing difficulties but without aggravation of the deficits in each of the two dimensions [26]
Given the central role of handwriting in the acquisition of other skills, these deficits can seriously hamper the acquisition of other skills [32,33,34]. It has been shown that, at equal content, worst quotes are attributed to less legible school works [35], resulting in a decrease in the child’s self-esteem. Dysgraphia may thus impact the academic success of the child if it is not diagnosed and handled early [36,37]. To this end, different tools are available to allow researchers and clinicians to analyze the two dimensions of handwriting: the final product of handwriting and the dynamic process of handwriting that generates the trace [38].
Evaluating the handwriting product refers to the static, spatial features of the written trace. This kind of analysis is performed afterwards. This is the principle of many tests used in different countries (for a review see [10]). The quality of the trace is evaluated based on different features such as letter size and form, spatial organization of handwriting on the paper sheet, margin, etc.
Evaluating the handwriting process refers to the analysis of dynamic, kinematic and temporal features of handwriting. Several type of variables can be analyzed, depending on the tools used for the evaluation: posture, finger and arm movements, pen grip and finger pressure on the pen, in-air and on-paper durations, pen velocity, pen pressure, etc. The increasing number of publications on the analysis of the handwriting process over the past years attests for the growing interest of researchers for this field (e.g., [39,40,41,42].
The objective of this quasi-systematic review is to make a concise listing of the tools and methods which are the most reported in the literature for the analysis of handwriting and the diagnosis of dysgraphia. Tools focusing on both the final handwriting product and the handwriting process will be considered. We will then discuss the pros and cons of the existing tools, and the perspectives for the development of future tools.
3. Handwriting tools based on the product
In order to list the diagnosis tools based on the analysis of the handwriting product, we searched in the two scientific browsers PubMed and Google Scholar using the following keywords: Handwriting, Assessment, Test, Tool, Quality, Evaluation, Battery, Children, Students, and Questionnaire.
The tools meeting our search criteria are listed in Table 1. We included only tools for which the following data were available: norms or age class, type of task, subdomain analyzed, criteria evaluated.
Although mainly designed for a developmental population (from the age of 5), some diagnosis tools can also be used in adults up to the age of 80 (QNST-3; [57]). The test duration is variable, from a few minutes up to 30 minutes. This parameter is interesting because deficits may not be visible during the first few minutes of handwriting, but may appear during a continuous handwriting task, as it is the case in the classroom. The tasks used in the tests are of three main types: copying a text or a sentence, writing under dictation (letters, digits, words, or text), and spontaneous writing. These complementary tasks explore different aspects of handwriting. The copy task is the easiest, and can be used with beginner writers. Moreover, it resembles the condition of the classroom, where children are often asked to copy texts. However, the reading component can pose problems for children with dyslexia, introducing a possible bias in the interpretation of the test results. The dictation task is ecologic too, without the reading component, but the spelling processes and the orthographic components may again pose problems for children with dyslexia. Finally, the spontaneous writing task is likely to be the most relevant task. The difficulty here is the establishment of norms, since the texts produced are all unique. General criteria of legibility and quality are thus used in this case, which may provide a less fine-grained analysis of handwriting.
It should be noted that one test includes an analysis of texts produced at school, the TOLH (Test Of Legible Handwriting, [59]). Two others include writing from memory: the ETCH-M (Evaluation Tool of Children’s Handwriting – Manuscript, [50]) and the MMHAP (Mac Master Handwriting Assessment Protocol, [54]). Two tests also add another level of analysis, thanks to two conditions in the copy task: normal speed and maximum speed (the DASH, [48]). This approach is particularly interesting since it mimicks certain classroom conditions, and it is well known that adding constraints (temporal or spatial) during handwriting helps revealing handwriting deficits [63,64]. Combining different tasks and/or conditions can provide a fine and detailed analysis of handwriting. It is worth noting that although these tasks are complementary, only three tests involve all three types: the BVSCO-3 [45], the ETCH-M [50], and the MMHAP [54].
The majority of the tests listed in Table 1 analyze handwriting quality using different criteria such as legibility, letter form, spatial organization of letters or words, alignment, etc. Some tests also measure handwriting speed by evaluating the number of characters or letters (BHK, [43]; French adaptation, [65]; BHK-ado, [44]; BVSCO-3, [45] ; CHES-M, [47]; ETCH-M, [50]; EVEDP, [51]; MMHAP, [54]; MHA, [55,56]) or the number of words (DASH, [48]; EVEDP, [51]) produced in a fixed period of time. Since a universal, gold standard test for the diagnosis of dysgraphia is not available, it is sometimes necessary to combine several tests to perform an optimal clinical assessment. The DASH test appears to be the most complete one, since it includes various types of tasks, different constraints of writing and it requires about 15 minutes of writing. Its weakness is that it only evaluates handwriting speed.
Finally, we also mention in Table 1 a couple of questionnaires, which can be interesting to use in complement to the other tests (HPSQ, [61]; « questionnaire for children », [62]). Indeed, these questionnaires provide information about the evaluation of handwriting quality by the teacher or the child himself, which can be useful in the perspective of a rehabilitation program.
Another important point to consider when choosing which test to use is the existence of standards. The Table 2 presents the psychometric properties of the main tests used both in research and in clinical practice. A number of tests have relatively inter-rater and test-retest reliabilities (the French adaptation of the BHK for example, [65]), while others reach high validity-related standards (the MHA, [55], and the TOLH [59] for example).
More recently, a few computerized diagnostic tools based on the analysis of the final product of handwriting have also been developed. They are listed in Table 3.
These algorithms are all based on pattern recognition methods using images of letters, digits, words or sentences. They use a large database of images, from which characteristic features of « poor writing » are extracted and analyzed using machine learning approaches. The performances of computer tools are evaluated using a series of criteria. The precision, also called positive predictive value, is defined as the number of correct classifications of dysgraphic children divided by the total number of classifications. The sensitivity represents the true-positive detection rate (correct classification of children with dysgraphia). The specificity represents the true-negative detection rate (correct classification of typically developing children).
As shown in Table 3, the performance of these classification tools is below that of the paper-and-pen tools listed above (73% for [69], 79.7% for [70]). The only exception is TestGraphia, the algorithm developed by Dimauro et al. [68], with good performances very closed to that of the original BHK test. It analyses the same criteria as the original BHK test [66], but using scanned images of the BHK texts. The sensitivity of TestGraphia is 83%, and its specificity is 98%. This algorithm seems thus very promising for the future development of computerized diagnostic tools.
4. Handwriting tools based on the process
Collecting the spatio-temporal characteristics of a written trace has become possible thanks to the development of digital tablets. The principle is simple: the tablet records the x, y and sometimes z (up to 2 cm) positions of the pen with a high frequency (every 5 or 10 milliseconds), as well as the time, the pen pressure, and the angle of the pen with the tablet. From these data, a large variety of static (size, alignment…), kinematic (speed, acceleration, jerk…) and dynamic (pen pressure, pen tilt…) features can be calculated. To avoid the undesirable effects of loss of surface roughness (e.g., [40]), a sheet of paper must be attached to the digital tablet and an ink pen compatible with the tablet must be used.
Over the last decades, a growing number of studies have focused on the development of tools for the diagnosis of dysgraphia using digital tablets. In this review, we present a non-exhaustive overview of these tools, which are not yet available to clinicians (Table 4).
The different digital tools for the diagnosis of dysgraphia presented in Table 4 combine dynamic, kinematic, and static features extracted from the handwritten tracks. These features are then analyzed mainly using machine learning approaches to classify the data (i.e. classifiers). These tools differ by the nature of the tasks analyzed (handwriting or graphomotor tasks), the size of the dataset, and the computational approach used to analyze the data.
Of the 22 studies reported here, four use graphomotor tasks, the others use handwriting alone or a combination of handwriting and drawings. It is interesting to mention that several studies use tasks that have been validated in clinical practice, such as the BHK [39,71,74,80], the BVSCO2 [76], or the Minnesota Handwriting Assessment (MHA, [78]).
The size of the dataset used varies between 35 and 580 participants, and the children included in the different studies are between 5 and 15 years of age.
Nine studies use classical statistical comparisons to identify discriminative features between groups (in blue in Table 4; [39,75,76,78,79,80,81,86,89]. The others (in black in Table 4) use different algorithms of machine learning (Random Forest, Support Vector Machine, Convolutional Neuron Network, etc.) to classify the children into different groups. These methods are called « supervised learning approaches » since the algorithm is trained to identify groups which were previously labeled. Most of the studies reported here present a simplistic classification of children in two groups: with or without dysgraphia. Only one study classifies the children into four groups: typically developing, with mild dysgraphia, with mean dysgraphia, and with severe dysgraphia [87]. This approach is interesting since it considers dysgraphia as a continuum of severity. This is probably closer to the reality than a dichotomic classification, as recently suggested by Lopez & Vaivre-Douret [90], who described 3 levels of handwriting disorders in children from 1st- to 5th-grade: mild disorder, moderate disorder, and dysgraphia.
The tools based on the analysis of handwriting samples obtained the best classification performance. For example, Asselborn et al. [71] reached a sensitivity of 96.6% and a specificity of 99%, and Mekyska et al. [84] reached a sensitivity of 96%. It is worth noting, however, that the excellent performances obtained in [71] must be considered with caution since they may be biased by the fact that the authors only included participants with severe dysgraphia [91]. The most discriminative features between children with and without dysgraphia vary among the studies, but generally include a larger size in dysgraphic handwriting, numerous velocity variations, a lower mean speed, increased lift and stop duration, and variations in the pen angle with the tablet.
The tools based on the analysis of drawing samples appear promising too, although their performances are slightly lower than those based on handwriting. For instance, the algorithm developed by Mekyska et al. [85] obtained a sensitivity of 90%. The idea that a dysgraphia can be identified based on graphomotor tasks suggests that dysgraphia can be independent from higher order processes, namely linguistic ones. Developing diagnostic tools based on drawings is interesting for two reasons: these tools would be more universal since they are independent of the language and the alphabet, and they can be used with younger children to identify « at-risk » children, which could be handled earlier.
Developing a computer tool for the diagnosis of dysgraphia is not trivial, as attested by the variability in the performance of the tools presented in Table 4. Several reasons can explain these differences. First, the variety of the tasks used and the number of participants leads to large differences in the size of the databases, which is a critical determinant in a classifier’s performances. Second, a large panel of machine learning approaches were used, with a different number of features analyzed among studies. Although certain classification methods appear better than others (Random Forest for example), none reached excellent performances nowadays. Since the interest of researchers for these tools is growing, it seems obvious that their efficiency will rapidly be improved. To do so, however, a number of key elements will be important to consider. First, it will require the constitution of large databases of handwriting and drawing samples from children which are perfectly characterized from a clinical point of view. It will also be necessary to estimate the severity of dysgraphia, and not only provide a dichotomic classification of children with or without dysgraphia, as proposed by Sihwi et al. [87]. Moreover, other processes involved in handwriting, such as visuomotor aspects, which are currently investigated [92], would be interesting to include in future diagnostic tools. Finally, it is also worth noting that diagnostic tools fully integrated into the pen and using machine learning approaches are also under investigation [93,94,95].
5. Perspectives: Towards a universal, standardized test of dysgraphia?
Although very promising, none of the computer and paper-and-pen tools presented above is fully satisfactory and sufficient to provide a completely reliable diagnosis of dysgraphia. In addition, most of the tools available to clinicians today do not give precise information about the specific handwriting difficulties of each child.
In this context, it appears interesting to think about developing a reliable, comprehensive and universal diagnostic tool for dysgraphia. Several important points need to be considered for the development of such an instrument. First, an “ideal” diagnostic tool will probably combine computer and paper-and-pen approaches, since they are complementary and provide distinct information on the writing process and product, respectively. A fully computerized tool could also be envisaged, provided that it is complemented by the assessment of the clinician, who must remain the reference assessor. Indeed, the spreading of tablets and the rapidity of computerized analyses could allow the collection of written samples in school or at the children’s house, which could then be sent to a clinician. Standard pen-and-paper tools could subsequently be used in case the computer tools detected a risk for dysgraphia in the child’s handwritten productions, in order to firmly confirm the diagnosis. In this perspective, the goal of the computer tools is thus not to replace the clinician and the existing, validated tests, but to help in screening larger populations of children and in facilitating the clinician diagnosis (Figure 1). In addition, these tools provide valuable information on the process of handwriting himself, by identifying dynamic or kinematic features which may be altered in each particular child. This information would be very relevant for the clinician, since it would offer cues for an individualized rehabilitation of handwriting.
Second, using a combination of tasks targeting different skills seems crucial to provide more information about handwriting difficulties. Indeed, some children with dysgraphia may succeed certain tasks and thus be undiagnosed if only a single one is used. Combining different tasks in a unique test would thus greatly increase its efficacy, as previously suggested by Safarova et al. [96]. Namely, the test should include spontaneous handwriting, copying of words and/or sentences, writing to dictation, digits writing, writing under speed and accuracy constraints, and drawing and/or graphomotor tasks. Temporal (i.e. speed) or spatial (i.e. size) constraints add a cognitive load and are known to increase handwriting difficulties [18,63,64]. With regards to the spontaneous production task, we could, for example, ask to write a 7-sentence text corresponding to the writer’s ideal weekly schedule. This would enable a specific analysis to me made of the days of the week, which would be common to all texts produced. As mentioned above, the addition of graphomotor and/or drawings tasks, which are language-independent, will enable to target younger children than with the existing tests and thus detect and handle earlier children “at-risk” of dysgraphia. In addition, it would provide a universal test, allowing comparisons between countries and alphabetic systems. In addition, the test needs to last at least 20 minutes in order to enhance the difficulty of the task and induce fatigue. Finally, completing the test by a self-questionnaire will enable the clinician to better characterize the difficulties experienced by the writer.
Thirdly, the choice of the cohort of participants will be crucial. A large developmental window ranging from 5 to at least 15 years old should be included, and the content of the test should be adapted depending on the age and/or class of the child, and the level of handwriting automation. The number of participants should be important enough to allow machine learning approaches. It would also be important to include children presenting a dysgraphia in various clinical contexts and precisely characterized from a clinical perspective. This would enable to evaluate the severity of dysgraphia, which could eventually be an additional evaluation criterion provided by the diagnostic tool. Finally, participants should be recruited in multiple sites representative of different socio-economic and educational statuses.
Developing such a complete diagnostic tool implies to collect large databases of handwriting and drawing samples in different places around the world. This would be possible by the implication of a consortium of laboratories and clinicians. Besides the diagnostic tool itself, the benefits of these developments would be twice: (i) from a clinical perspective, it would allow to estimate the prevalence of dysgraphia in different countries and it would further tailor rehabilitation programs to the characteristics of handwriting difficulties, and (ii) from a research perspective, it would provide large annotated databases that could be freely available to researchers working in the fields graphonomics, whether in educational, clinical, or human movement sciences.
Author Contributions
Writing—original draft preparation, C.J.; writing—review and editing, C.J., F.P., J.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Berninger, V. W.; Abbott, R. D.; Abbott, S. P.; Graham, S.; Richards, T. Writing and reading: Connections between language by hand and language by eye. J. Learn. Disab. 2002, 35(1), 39-56. [CrossRef]
- McHale, K.; Cermak, S. A. Fine motor activities in elementary school: Preliminary findings and provisional implications for children with fine motor problems. Am. J. Occup. Ther. 1992, 46(10), 898-903. [CrossRef]
- Mc Master, E.; Roberts, T. Handwriting in 2015: A main occupation for primary school–aged children in the classroom? J. Occup. Ther. Schools Early Interv. 2016, 9(1), 38. [CrossRef]
- Jones, D.; Christensen, C. A. Relationship between automaticity in handwriting and students' ability to generate written text. J. Educ. Psychol. 1999, 91(1), 44. [CrossRef]
- Danna, J.; Longcamp, M.; Nalborczyk, L.; Velay, J.-L.; Commengé, C.; Jover, M. Interaction between orthographic and graphomotor constraints in learning to write. Learn. Instruct. 2022, 80, 101622. [CrossRef]
- Olive, T.; Kellogg, R. T. Concurrent activation of high- and low-level production processes in written composition. Memory Cogn. 2002, 30, 594–600. [CrossRef]
- Marr, D.; Windsor, M. M.; Cermak, S. Handwriting readiness: Locatives and visuomotor skills in the kindergarten year. The Cambridge handbook of multimedia learning (2nd ed.). University Press: Cambridge, UK, 2001.
- Karlsdottir, R.; Stefansson, T. Problems in developing functional handwriting. Percept. Mot. Skills 2002, 94(2), 623-662. [CrossRef]
- Palmis, S.; Danna, J.; Velay, J.-L.; Longcamp, M. Motor control of handwriting in the developing brain: A review. Cogn. Neuropsychol. 2017, 34(3-4), 187-204. [CrossRef]
- Chung, P.J.; Patel, D.R.; Nizami, I. Disorder of written expression and dysgraphia: definition, diagnosis, and management. Transl. Pediatr. 2020, 9(Suppl.1), S46-S54. [CrossRef]
- Kalenjuk, E.; Laletas, S.; Subban, P.; Wilson, S. A scoping review to map research on children with dysgraphia, their carers, and educators. Austral. J. Learn. Difficult. 2022, 27(1), 19-63. [CrossRef]
- Aiswarya, G.S.; Ponniah, R.J. The modularity of dysgraphia. J. Psycholinguist. Res. 2023, in press. [CrossRef]
- Hamstra-Bletz, L.; Blöte, A.W. A longitudinal study on dysgraphic handwriting in primary school. J. Learn. Disab. 1993, 26, 689-699. [CrossRef]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®); American Psychiatric Pub: Washington DC, USA, 2013.
- Adi-Japha, E.; Landau, Y. E.; Frenkel, L.; Teicher, M.; Gross-Tsur, V.; Shalev, R. S. ADHD and dysgraphia: underlying mechanisms. Cortex 2007, 43, 700-709. [CrossRef]
- Barnett, A.L.; Prunty, M. Handwriting Difficulties in Developmental Coordination Disorder (DCD). Curr. Dev. Disord. Rep. 2020, 8, 1-9. [CrossRef]
- Biotteau, M.; Danna, J.; Baudou, E.; Puyjarinet, F.; Velay, J.-L.; Albaret, J.-M.; Chaix, Y. Developmental coordination disorder and dysgraphia: signs and symptoms, diagnosis, and rehabilitation. Neuropsy. Dis. Treat. 2019, 15, 1873-1885. [CrossRef]
- Capodieci, A.; Lachina, S.; Cornoldi, C. Handwriting difficulties in children with attention deficit hyperactivity disorder (ADHD). Res. Dev. Disab. 2018, 74, 41-49. [CrossRef]
- Cohen, R.; Cohen-Kroitoru B.; Halevy, A.; Aharoni, S.; Aizenberg, I.; Shuper, A. Handwriting in children with Attention Deficient Hyperactive Disorder: role of graphology. BMC Pediatr. 2019, 19(1), 1-6. [CrossRef]
- Di Brina, C.; Caravale, B.; Mirante, N. Handwriting in children with developmental coordination disorder: Is legibility the only indicator of a poor performance? Occup. Ther. Health Care 2021, 36(4), 353-367. [CrossRef]
- Berninger, V.W.; May, M.O. Evidence-based diagnosis and treatment for specific learning disabilities involving impairments in written and/or oral language. J. Learn. Disab. 2011, 44, 167-183. [CrossRef]
- Afonso, O.; Suárez-Coalla, P.; Cuetos, F. Writing impairments in Spanish children with developmental dyslexia. J. Learn. Disab. 2020, 53, 109-119. [CrossRef]
- Alamargot, D.; Morin, M.-F.; Simard-Dupuis, E. Handwriting delay in dyslexia: children at the end of primary school still make numerous short pauses when producing letters. J. Learn. Disab., 2020, 53, 163-175. [CrossRef]
- Huau, A.; Velay, J.-L.; Jover, M. Graphomotor skills in children with developmental coordination disorder (DCD): Handwriting and learning a new letter. Hum. Mov. Sci. 2015, 42, 318-332. [CrossRef]
- Johnson, B. P.; Papadopoulos, N.; Fielding, J.; Tonge, B.; Phillips, J. G.; Rinehart, N. J. Aquantitative comparison of handwriting in children with high-functioning autism andattention deficit hyperactivity disorder. Res. Autism Spectr. Dis. 2013, 7(12),1638–1646. [CrossRef]
- Jolly, C.; Jover, M.; Danna J. Dysgraphia differs between children with developmental coordination disorder and/or reading disorder. J. Learn. Disab. 2023 (in press).
- Sandler, A. D.; Watson, T. E.; Footo, M.; Levine, M. D.; Coleman, W. L.; Hooper, S. R. Neurodevelopmental study of writing disorders in middle childhood. J. Dev. Behav. Pediatr. 1992, 13(1), 17–23. [CrossRef]
- Sumner, E.; Connelly, V.; Barnett, A.L. Children with dyslexia are slow writers because they pause more often and not because they are slow at handwriting execution. Read. Writ. 2013, 26(6), 991-1008. [CrossRef]
- Prunty, M.; Barnett, A.L. Accuracy and consistency of letter formation in children with developmental coordination disorder. J. Learn. Disab. 2020, 53(2), 120-130. [CrossRef]
- Richards, T.L.; Grabowski, T.J.; Boord, P.; Yagle, K.; Askren, M.; Mestre, Z.; Robinson, P.; Welker, O.; Gulliford, D.; Nagy, W.; Berninger, V. Contrasting brain patterns of writing-relatedDTI parameters, fMRI connectivity, and DTI–fMRI connectivity correlations in children with and without dysgraphia or dyslexia. NeuroImage: Clinical 2015, 8, 408–421. [CrossRef]
- Gosse, C.; Van Reybroeck, M. Do children with dyslexia present a handwriting deficit? Impact of word orthographic and graphic complexity on handwriting and spelling performance. Res. Dev. Disab. 2020, 97, 103553. [CrossRef]
- Berninger, V.; Abbott, R; Cook, C. R.; Nagy, W. Relationships of attention and executive functions to oral language, reading, and writing skills and systems in middle childhood and early adolescence. J. Learn. Disab. 2017, 50(4), 434-449. [CrossRef]
- Graham, S.; Harris, K. R. The role of self-regulation and transcription skills in writing and writing development. Educ. Psychol. 2000, 35(1), 3–12. [CrossRef]
- Nielsen, S. K.; Kelsch, K.; Miller, K. Occupational therapy interventions for children with attention deficit hyperactivity disorder: A systematic review. Occup. Ther. Mental Health 2017, 33(1), 70–80. [CrossRef]
- Markham, L. R. Influences of handwriting quality on teacher evaluation of written work. Am. Educ. Res. J. 1976, 13(4), 277-283. [CrossRef]
- Engel-Yeger, B.; Nagauker-Yanuv, L.; Rosenblum, S. Handwriting performance, selfreports, and perceived self-efficacy among children with dysgraphia. Am. J. Occup. Ther. 2009, 63(2), 182–192. [CrossRef]
- Graham, S.; Fishman, E. J.; Reid, R.; Hebert, M. Writing characteristics of students with attention deficit hyperactive disorder: A meta-analysis. Learn. Disab. Res. Pract. 2016 31(2), 75–89. [CrossRef]
- Rosenblum, S.; Weiss, P. L.; Parush, S. Product and process evaluation of handwriting difficulties. Educ. Psychol. Rev. 2003, 15, 41-81. [CrossRef]
- Asselborn, T.; Chapatte, M.; Dillenbourg, P. (2020). Extending the spectrum of dysgraphia: A data driven strategy to estimate handwriting quality. Sci. Rep. 2020, 10, 3140. [CrossRef]
- Drotár, P.; Dobeš, M. Dysgraphia detection through machine learning. Sci. Rep. 2020, 10, 21541. [CrossRef]
- Guilbert, J.; Alamargot, D.; Morin, M. F. Handwriting on a tablet screen: Role of visual and proprioceptive feedback in the control of movement by children and adults. Hum. Mov. Sci. 2019, 65, 30-41. [CrossRef]
- Rosenblum, S.; Dror, G. Identifying developmental dysgraphia characteristics utilizing handwriting classification methods. IEEE Trans. Hum. Mach. Syst. 2017, 47(2), 293-298. [CrossRef]
- Hamstra-Bletz, E.; de Bie, J.; den Brinker, B.P.L.M. Beknopte beoordelingsmethode voor kinderhandschriften/ Concise evaluation scale for children’s handwriting. Swets & Zeitlinger: Lisse, Netherlands, 1987.
- Soppelsa, R.; Albaret, J.-M. BHK Ado. Editions du Centre de Psychologie Appliquée: Paris, France, 2013.
- Cornoldi, C.; Ferrara, R.; Re, A. M. BVSCO-3 Batteria per la Valutazione clinica della Scrittura e della Competenza Ortografica–3 [BVSCO-3, Battery for the assessment of writing and spelling accuracy]. Giunti Psychometrics: Italy, 2022.
- Phelps, J.; Stempel, L.; Speck, G. The Children’s Handwriting Scale: a new diagnostic tool. J. Educ. Res. 1985, 79, 46-50. [CrossRef]
- Phelps, J.; Stempel, L. The Children’s Handwriting Evaluation Scale for manuscript writing. Read. Improv. 1988, 25(4), 247-254.
- Barnett, A.; Henderson, S.; Scheib, B.; Schulz, J. Development and standardization of a new handwriting speed test: The Detailed Assessment of Speed of Handwriting. Teach. Learn. Writ. 2009, 1, 137-157.
- Scott, D.H.; Moyes, F.A.; Henderson, S.E. Diagnosis and remediation of handwriting problems. DRAKE Educational Associate: Fairwater, UK, 1985.
- Amundson, S.J. Evaluation Tool of Children’s Handwriting; OT KIDS: Homer, USA, 1995.
- Pouhet, A. L’évaluation de la vitesse d’écriture manuelle à l’aide d’une dictée de niveau progressif: l’EVEDP. A.N.A.E. 2005, 136-137, 354-363.
- Erez, N.; Parush, S. The Hebrew handwriting evaluation. School of Occupational Therapy. Faculty of Medicine. Hebrew University of Jerusalem, Israel; 1999.
- Barnett, A. L.; Prunty, M.; Rosenblum, S. Development of the handwriting legibility scale (HLS): A preliminary examination of reliability and validity. Res. Dev. Disab. 2018, 72, 240-247. [CrossRef]
- Pollock, N.; Lockhart, J.; Blowes, B.; Semple, K.; Webster, M.; Farhat, L.; Jacbson, J.; Bradley, J.; Brunetti, S. The McMAster Handwriting Assessment Protocol – 2nd ed. Hamilton: McMaster University, Canada, 2009.
- Reisman, J.E. Development and reliability of the research version of the Minnesota Handwriting Test. Phys. Occup. Ther. Pediatr. 1993, 13(2), 41-55. [CrossRef]
- Reisman, J.E. Minnesota Handwriting Assessment. Harcourt Assessment: San Antonio, USA, 1999.
- Mutti, M.; Martin, N.; Sterling, H.; Spalding, N. QNST-3R: Quick Neurological Screening Test (3rd ed.). Academic Therapy Publications: Novato, USA, 2017.
- Weil, M. J.; Cunningham Amundson, S. J. Relationship between visuomotor and handwriting skills of children in kindergarten. Am. J. Occup. Ther. 1994, 48(11), 982-988. [CrossRef]
- Larsen, S.C.; Hammill, D.D. Test of legible handwriting: An ecological approach to holistic assessment. Pro-Ed: Austin, USA, 1989.
- Milone, M. THS-R: Test of Handwriting skills. Revised. Academic Therapy Publications: Novato, USA, 2007.
- Rosenblum, S. Development, reliability, and validity of the Handwriting Proficiency Screening Questionnaire (HPSQ). Am. J. Occup. Ther. 2008, 62(3), 298-307. [CrossRef]
- Santamaria, M.; Albaret, J.-M. Troubles graphomoteurs chez les enfants d’intelligence supérieure. Evolutions Psychomotrices 1996, 33(8), 113-120.
- Chartrel, E.; Vinter, A. The impact of spatio-temporal constraints on cursive letter handwriting in children. Learn. Instruct. 2008, 18(6), 537-547. [CrossRef]
- Fitzpatrick, P.; Vander Hart, N.; Cortesa, C. The influence of instructional variables and task constraints on handwriting performance. J. Educ. Res. 2013, 106(3), 216-234. [CrossRef]
- Charles, M.; Soppelsa, R.; Albaret, J.-M. BHK – Echelle d’évaluation rapide de l’écriture chez l’enfant; Editions du Centre de Psychologie Appliquée: Paris, France, 2003.
- Di Brina, C.; Rossini, G. Test BHK-Scala sintetica per la valutazione della scrittura in età evolutiva. Erickson: Portland, USA, 2011; 242.
- Loizzo, A.; Zaccaria, V.; Caravale, B.; Di Brina, C. Validation of the concise assessment scale for children’s handwriting (BHK) in an Italian population. Children 2023, 10, 223. [CrossRef]
- Dimauro, G.; Bevilacqua, V.; Colizzi, L.; Di Pierro, D. TestGraphia, a software system for the early diagnosis of dysgraphia. IEEE Access 2020, 8, 1-12. [CrossRef]
- Isa, I. S.; Rahimi, W. N. S.; Ramlan, S. A.; Sulaiman, S. N. Automated detection of dyslexia symptom based on handwriting image for primary school children. Proced. Comp. Sci. 2019, 163, 440-449. [CrossRef]
- Skunda, J.; Nerusil, B.; Polec, J. Method for Dysgraphia Disorder Detection using Convolutional Neural Network. 30th Intl. Conf. Central Europe Comput. Graphics Visual Comput. Vision 2022.
- Asselborn, T.; Gargot, T.; Kidziński, Ł.; Johal, W.; Cohen, D.; Jolly, C.; Dillenbourg, P. Automated Human-Level Diagnosis of Dysgraphia Using a Consumer Tablet. Npj Dig. Med. 2018, 1, 1–9. [CrossRef]
- Dankovičová, Z.; Hurtuk, J.; Feciľak, P. Evaluation of Digitalized Handwriting for Dysgraphia Detection Using Random Forest Classification Method. In 2019 IEEE 17th Intl. Symp. Intell. Systems Inform. (SISY) 2019; pp. 000149-000154. [CrossRef]
- Devillaine, L.; Lambert, R.; Boutet, J.; Aloui, S.; Brault, V.; Jolly, C.; Labyt, E. Analysis of Graphomotor Tests with Machine learning Algorithms for an Early and Universal Pre-Diagnosis of Dysgraphia. Sensors 2021, 21(21), 7026. [CrossRef]
- Deschamps, L.; Devillaine, L.; Gaffet, C.; Lambert, R.; Aloui, S.; Boutet, J.; Brault, V.; Labyt, E.; Jolly, C. Development of a pre-diagnosis tool based on machine learning Algorithms on the BHK test to improve the diagnosis of dysgraphia. Adv. Artif. Intell. Mach. Learn. 2021, 1(2), 109-128. [CrossRef]
- Dui, L. G.; Lunardini, F.; Termine, C.; Matteucci, M.; Stucchi, N. A.; Borghese, N. A.; Ferrante, S. A tablet app for handwriting skill screening at the preliteracy stage: Instrument validation study. JMIR Serious Games 2020, 8(4), e20126. [CrossRef]
- Dui, L. G.; Calogero, E.; Malavolti, M.; Termine, C.; Matteucci, M.; Ferrante, S. Digital tools for handwriting proficiency evaluation in children. In 2021 IEEE EMBS Intl. Conf. Biomed. Health Inform. (BHI) 2021; pp. 1-4. [CrossRef]
- Dui, L. G.; Lomurno, E.; Lunardini, F.; Termine, C.; Campi, A.; Matteucci, M.; Ferrante, S. Identification and characterization of learning weakness from drawing analysis at the pre-literacy stage. Sci. Rep. 2022, 12(1), 21624. [CrossRef]
- Falk, T. H.; Tam, C.; Schellnus, H.; Chau, T. On the development of a computer-based handwriting assessment tool to objectively quantify handwriting proficiency in children. Comp. Meth. Progr. Biomed. 2011, 104(3), e102-e111. [CrossRef]
- Galaz, Z.; Mucha, J.; Zvoncak, V.; Mekyska, J.; Smekal, Z.; Safarova, K.; Ondrackova ; A.; Urbanke, T.; Havigerova, J. M.; Bednarova, J.; Faundez-Zanuy, M. Advanced parametrization of graphomotor difficulties in school-aged children. IEEE Access 2020, 8, 112883-112897. [CrossRef]
- Gargot, T.; Asselborn, T.; Pellerin, H.; Zammouri, I.; Anzalone, S.M.; Casteran, L.; Johal, W.; Dillenbourg, P.; Cohen, D.; Jolly, C. Acquisition of handwriting in children with and without dysgraphia: A computational approach, PLOS ONE 2020, 15(9), e0237575. [CrossRef]
- Herstic, A.Y.; Bansil, S.; Plotkin, M.; Zabel, T.A.; Mostofsky, S.H. Validity of an automated handwriting assessment in occupational therapy settings. J. Occup. Ther. Schools Early Interv. 2022, 16, 28-38. [CrossRef]
- Kedar, S. V. Identifying Learning Disability Through Digital Handwriting Analysis. Turk. J. Comp. Math. Educ. (TURCOMAT) 2021, 12(1S), 46-56. [CrossRef]
- Kunhoth, J.; Al Maadeed, S.; Saleh, M.; Akbari, Y. Exploration and analysis of On-Surface and In-Air handwriting attributes to improve dysgraphia disorder diagnosis in children based on machine learning methods. Biomed. Sign. Process. Control 2023, 83, 104715. [CrossRef]
- Mekyska, J.; Faundez-Zanuy, M.; Mzourek, Z.; Galaz, Z.; Smekal, Z.; Rosenblum, S. Identification and rating of developmental dysgraphia by handwriting analysis. IEEE Trans. Hum. Mach. Syst. 2016, 47(2), 235-248. [CrossRef]
- Mekyska, J.; Galaz, Z.; Safarova, K.; Zvoncak, V.; Mucha, J; Smekal, Z.; Ondrackova, A.; Urbanek, T.; Havigerova, J. M.; Bednarova, J.; Faundez-Zanuy, M. Computerised assessment of graphomotor difficulties in a cohort of school-aged children. In 2019 11th International Congress on Ultra Modern Telecommunications and Control Systems and Workshops (ICUMT) 2019 (pp. 1-6). [CrossRef]
- Rosenblum, S.; Dvorkin, A.Y.; Weiss, P.L. Automatic segmentation as a tool for examining the handwriting process of children with dysgraphic and proficient handwriting. Hum. Mov. Sci. 2006, 25, 608-621. [CrossRef]
- Sihwi, S.W.; Fikri, K.; Aziz, A. Dysgraphia identification from handwriting with Support Vector Machine method. J. Physics Conf. Series 2019, 1201. [CrossRef]
- Zvoncak, V.; Mekyska, J.; Safarova, K.; Smekal, Z.; Brezany, P. New approach of dysgraphic handwriting analysis based on the tunable Q-factor wavelet transform. 42nd International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), 2019a, pp. 289-294.
- Zvoncak, V.; Mucha, J.; Galaz, Z.; Mekyska, J.; Safarova, K.; Faundez-Zanuy, M. Fractional order derivatives evaluation in computerized assessment of handwriting difficulties in school-aged children. 11th International Congress on Ultra Modern Telecommunications and Control Systems and Workshops (ICUMT), 2019b, pp. 1-6.
- Lopez, C.; Vaivre-Douret, L. Exploratory investigation of handwriting disorders in school-aged children from first to fifth grade. Children 2023a, 10, 1512. [CrossRef]
- Deschamps, L.; Gaffet, C.; Aloui, S.; Boutet, J.; Brault, V.; Labyt, E. Methodological issues in the creation of a diagnosis tool for dysgraphia. NPJ Dig. Med. 2019, 2(1), 36. [CrossRef]
- Lambert, R.; Boutet, J.; Labyt, E.; Jolly, C. Analysis of Eye Movements in Children with Developmental Coordination Disorder During a Handwriting Copy Task. In International Graphonomics Conference, Evora, Portugal, October 2023. Cham: Springer Nature, Switzerland; (pp. 36-44).
- Lopez, C.; Cannafarina, A.; Vaivre-Douret, L. Validity of kinematics measures to assess handwriting development and disorders with a graphomotor task. Eur. Psych. 2021, 64.
- Bublin, M.; Werner, F.; Kerschbaumer, A.; Korak, G.; Geyer, S.; Rettinger, L.; Schönthaler, E.; Schmid-Kietreiber, M. Handwriting evaluation using deep-leraning with SensoGrip. Sensors 2023, 23¸ 5215. [CrossRef]
- Lopez, C.; Vaivre-Douret, L. Concurrent and predictive validity of a cycloid loops copy task to assess handwriting disorders in children. Children 2023b, 10, 305. [CrossRef]
- Safarova, K.; Mekyska, J.; Zvoncak, V. Developmental dysgraphia: A new approach to diagnosis. Int. J. Assess. Eval. 2021, 28,143-160. [CrossRef]
Figure 1.
Examples of the complementary use of paper-and-pen tests and computerized tools for the diagnosis and rehabilitation of handwriting deficits.
Figure 1.
Examples of the complementary use of paper-and-pen tests and computerized tools for the diagnosis and rehabilitation of handwriting deficits.
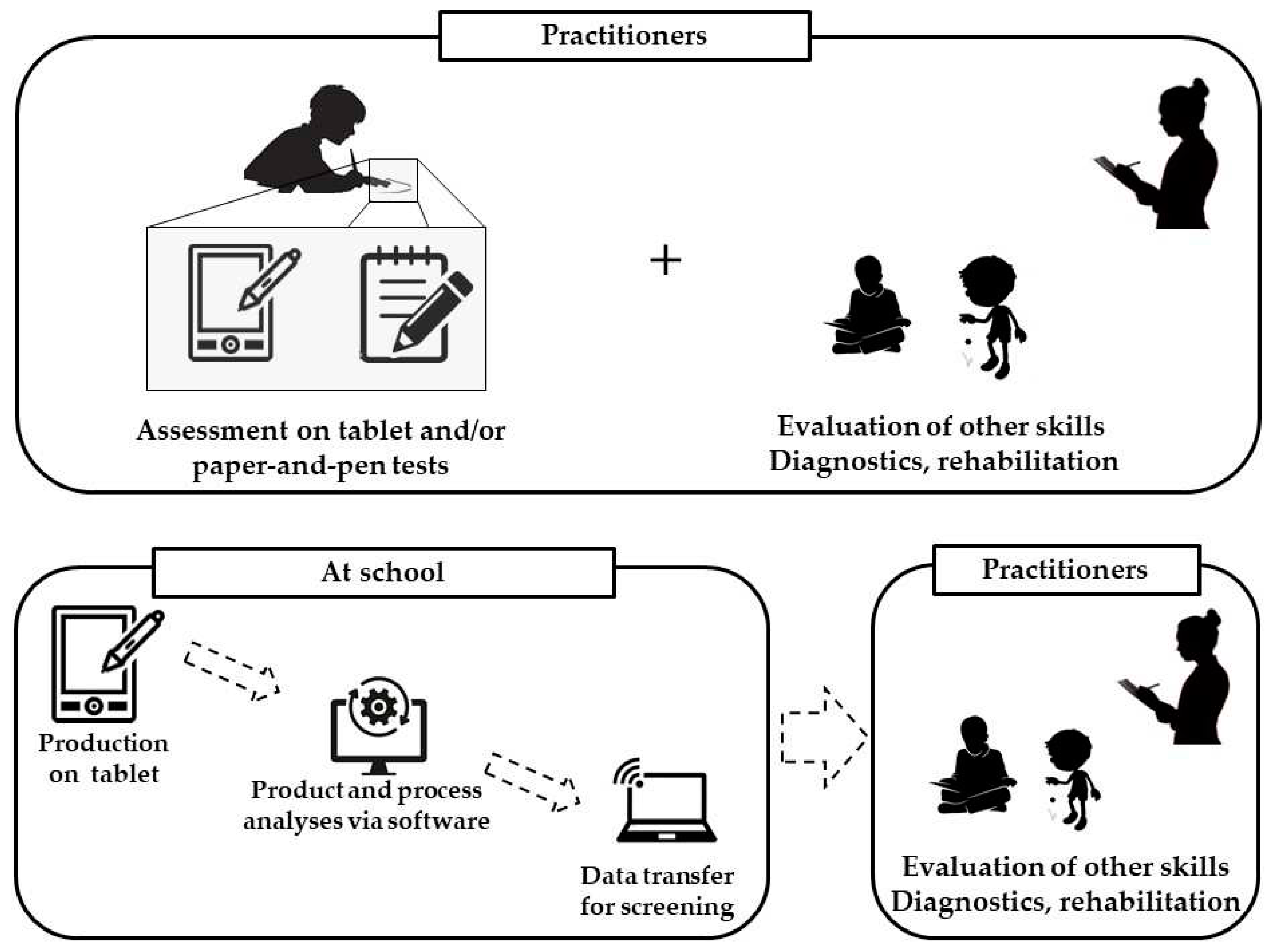

Table 1.
List of the most commonly used tools for the diagnosis of dysgraphia in children based on the analysis of the handwriting product (presented in alphabetical order). N.A.: not available.
Table 1.
List of the most commonly used tools for the diagnosis of dysgraphia in children based on the analysis of the handwriting product (presented in alphabetical order). N.A.: not available.
| Test name | Reference | Ages / Classes | Duration of test | Language | Task(s) | Subdomains |
|---|---|---|---|---|---|---|
| BHK: Brave Handwriting Kinder | [43] | 1st- to 5th-grade | 5 mn | Multi-language | Copy | Quality Speed |
| BHK Ado: Rapid writing evaluation scale for adolescents [Echelle d’évaluation rapide de l’écriture chez l’adolescent] | [44] | 6th- to 9th-grade | 5 mn | French | Copy | Quality Speed |
| BVSCO-3 – Test for the Evaluation of Writing and Orthographic Ability, 3rd ed. |
[45] | 6-14 y | Variable | Multi-language | Copy Dictation Spontaneous production |
Speed % of errors |
| CHES – Children's Handwriting Evaluation Scale | [46] | 3rd- to 8th-grade | 2 mn | English | Copy | Quality Fluency |
| CHES-M – Children's Handwriting Evaluation Scale - Manuscript Writing |
[47] | 1st- to 2nd-grade | 2 mn | English | Copy | Quality Fluency |
| DASH – Detailed Assessment of Speed of Handwriting | [48] | 9-16 y | 14 mn | English | Alphabet copy at normal and high speed Spontaneous production |
Speed |
| DRHP – Diagnosis and Remediation of Handwriting Problems | [49] | From 3rd-grade | Variable | English | Spontaneous production from images observation | Quality |
| ETCH-M – Evaluation Tool of Children's Handwriting - Manuscript |
[50] | 1st- to 2nd-grade | 15-20 mn | English | Copy Dictation Spontaneous production Handwriting from memory |
Quality Speed |
| EVEDP – Evaluation de la Vitesse d’Ecriture – Dictée Progressive | [51] | 2nd- to 5th-grade | Variable | French | Dictation | Speed |
| HHE - Hebrew Handwriting Evaluation | [52] | 6-18 y | 5 min | Hebrew | Alphabet Copy of a text |
Quality Speed |
| HLS – Handwriting Legibility Scale | [53] | 9-14 y | 10 mn | English | Spontaneous production | Quality |
| MMHAP – Mac Master Handwriting Assessment Protocol | [54] | Preschool to 6th-grade | Variable | English | Copy Dictation Spontaneous production Handwriting from memory |
Quality Speed |
| MHA – Minnesota Handwriting Assessment | [55,56] | 1st- to 2nd-grade | 2 mn ½ | English | Alphabet Copy |
Quality Speed |
| QNST-3 Revised – Quick Neurological Screening Test, 3rd ed. Revised | [57] | 5-80 y | 30 mn | English | Copy | Quality |
| SCRIPT– Scale of Children’s Readiness in PrinTing | [58] | N.A. | 3-8 mn | English | Copy | Quality |
| TOLH – Test Of Legible Handwriting | [59] | 2nd- to 12th-grade | Variable | English | Spontaneous production Text composition at school |
Quality |
| THS-R | [60] | 6-18 y | N.A. | English | Alphabet Copy |
Quality |
| HPSQ – Handwriting Proficiency Screening Questionnaire | [61] | 7-14 y | N.A. | Multi-language | Questionnaire | Quality |
| Questionnaire for children | [62] | 1st- to 5th-grade | 2-3 mn | French | Auto-questionnaire | Self-report on handwriting quality and difficulties |
Table 2.
Psychometric properties of the main diagnosis tools for handwriting assessment. BHK: Brave Handwriting Kinder; CHES-M: Children’s Handwriting Evaluation Scale for Manuscript writing; DASH: Detailed Assessment of Speed of Handwriting; DRHP: Diagnosis and Remediation of Handwriting problems; ETCH-M: Evaluation Tool for Children’s Handwriting-Manuscript; HHE: Hebrew Handwriting Evaluation; HPSQ: Handwriting Proficiency Screening Questionnaire; THS-R: Test of Handwriting; TOLH: Test Of Legible Handwriting; N.A.: not available.
Table 2.
Psychometric properties of the main diagnosis tools for handwriting assessment. BHK: Brave Handwriting Kinder; CHES-M: Children’s Handwriting Evaluation Scale for Manuscript writing; DASH: Detailed Assessment of Speed of Handwriting; DRHP: Diagnosis and Remediation of Handwriting problems; ETCH-M: Evaluation Tool for Children’s Handwriting-Manuscript; HHE: Hebrew Handwriting Evaluation; HPSQ: Handwriting Proficiency Screening Questionnaire; THS-R: Test of Handwriting; TOLH: Test Of Legible Handwriting; N.A.: not available.
| Test name [ref] | Number of participants | Country of validation | Inter-rater validity | Test-retest validity | Internal consistancy |
|---|---|---|---|---|---|
| BHK [13,43] | 121 | Netherlands | .71 to .89 | .74 to .86 | N.A. |
| BHK - French adaptation [65] | 837 | France | .68 to .90 | .80 to .92 | N.A. |
| BHK Ado [44] | 471 | France | .24 to .66 | N.A. | N.A. |
| BHK - Italian adaptation [66,67] | 562 | Italy | .82 to .93 for speed .42 to .63 for quality |
N.A. | N.A. |
| CHES-M [47] | 643 | USA | .85 to .93 | N.A. | N.A. |
| DASH [48] | 1163 | Netherlands | .85 to .99 | .50 to .92 .81 | .88 to .94 |
| DRHP [49] | 300 | UK | .61 to .65 | N.A. | N.A. |
| ETCH-M [50] | N.A. | N.A. | .75 to .92 | .63 to .77 | N.A. |
| HHE [52] | N.A. | Israël | .75 to .79 | N.A. | N.A. |
| HPSQ [61] | 230 | Israël | .92 | .84 | .90 |
| MHA [55,56] | N.A. | USA | .87 to .98 | .58 to .94 | N.A. |
| THS-R [60] | N.A. | USA | N.A. | .82 | N.A. |
| TOLH [59] | 1723 | USA | .95 | .90 | .86 |
Table 3.
List of the computerized diagnosis tools in children based on the analysis of the handwriting product. CNN: Convolutional Neural Network; RF: Random Forest; SVM: Support Vecotr Machine; ANN: Artificial Neural Network.
Table 3.
List of the computerized diagnosis tools in children based on the analysis of the handwriting product. CNN: Convolutional Neural Network; RF: Random Forest; SVM: Support Vecotr Machine; ANN: Artificial Neural Network.
| Ref | Ages / Classes | Characteristics of participants | Task(s) | Language | Approach | Performances |
|---|---|---|---|---|---|---|
| [68] | 7-10 y | Dysgraphic | BHK (5 lines) | Italian | Algorithms for document analysis | Sensitivity: 83 % Specificity: 98 % Precision: 96 % |
| [69] | 7-12 y | Dyslexic | Letters and digits writing | Malaysian | Machine Learning (ANN) | Sensitivity: 73 % |
| [70] | 8-15 y | Typically Developing and Dysgraphic |
Letters, syllables, words, pseudowords, and sentences |
Slovak | Machine Learning (CNN, RF, SVM, AdaBoost) | Precision: 79.7 % |
Table 4.
List of the algorithms and computer tools for the diagnosis of handwriting deficits. In blue: tools based on statistical approaches, in black: tools based on machine learning approaches. ADHD: Attention-Deficit/Hyperactivity Disorder. BEM: Beta-elliptic Model; BVSCO-2 – Test for the Evaluation of Writing and Orthographic Ability, 2nd ed.; CNN: Convolutional Neural Network; DG: dysgraphic children; FDM: Fourier Descriptor Model; FOD: Fractional Order Derivatives; KNN: K-nearest Neighbors; MHA: Minnesota Handwriting Assessment; MLP: Mumti Layers Perceptron; P: precision; RBF: Radial Basis Function; RF: Random forest; SE: sensitivity; SP: specificity; TD: Typically Developing children.
Table 4.
List of the algorithms and computer tools for the diagnosis of handwriting deficits. In blue: tools based on statistical approaches, in black: tools based on machine learning approaches. ADHD: Attention-Deficit/Hyperactivity Disorder. BEM: Beta-elliptic Model; BVSCO-2 – Test for the Evaluation of Writing and Orthographic Ability, 2nd ed.; CNN: Convolutional Neural Network; DG: dysgraphic children; FDM: Fourier Descriptor Model; FOD: Fractional Order Derivatives; KNN: K-nearest Neighbors; MHA: Minnesota Handwriting Assessment; MLP: Mumti Layers Perceptron; P: precision; RBF: Radial Basis Function; RF: Random forest; SE: sensitivity; SP: specificity; TD: Typically Developing children.
| Reference | Ages / Classes | n | Tasks | Langage / alphabet | Approach | Criteria analysed | Performances |
|---|---|---|---|---|---|---|---|
| [71] | 6-10 y | 242 TD 56 DG |
Copy of a (BHK) | French | RF | Static Kinematic Pressure Pen tilt |
SE: 96,6 % SP: 99,2 % P: 97,98 % |
| [39] | 5-12 y |
390 TD 58 DG |
Letters, words, sentences | French | PCA + K-means clustering |
Static Kinematic |
SE: 91 % SP: 90 % |
| [72] | 10-13 y | 39 TD 39 DG |
Letters, words, sentences | Slovak | SVM | Kinematic | SE: 75,5 % |
| [73] | 7-11 y | 262 TD 63 DG |
Copy of graphic shapes | N.A. | SVM, RF, MLP, extra trees, AdaBoost, Gaussian Naive Bayes | Kinematic | SE: 75,1 % (RF) SP: 72,1 % (MLP) P: 73 % (extra trees), 73,4 % (RF) |
| [74] | 7-11 y | 458 TD 122 DG |
Copy of a text (BHK) | French | SVM | Kinematic Spatial | SE: 91 % SP: 81 % P: 86 % |
| [40] | 8-15 y | 63 TD 57 DG |
Letters, syllables, words, pseudowords, sentences with speed constraints | Slovak | AdaBoost, RF, SVM | Kinematic | SE: 79,7 % SP: 76,7 % P: 80 % |
| [75] | 5-8 y |
76 TD 28 DG |
Copy of words (8y), graphic shapes (5 and 8y) |
Italian | Statistical comparison between groups |
Kinematic Pressure |
N.A. |
| [76] | 7-8 y | 52 TD | Subtest of the BVSCO-2 (digits, sequence of small and large loops, words) | Italian | Statistical comparisons | Kinematic | N.A. |
| [77] | 5 y | 241 «at-risk of DG» | Copy of graphic shapes | N.A. | 1 dimension CNN | Kinematic | SE: 75 % SP: 77 % P: 76 % |
| [78] | 6-7 y |
26 TD 9 DG |
MHA | English | Statistical comparisons |
Static Kinematic |
N.A. |
| [79] | 8-12 y | 26 TD | Copy of graphic shapes | Czech | Q factor wavelet transform + statistical comparisons |
Static Kinematic |
P: 84 % |
| 27 DG | |||||||
| [80] | 7-10 y |
218 TD 62 DG |
Copy of a text (BHK) | French | Statistical comparisons between groups (linear regression), clustering |
Static Kinematic Pressure Pen tilt |
N.A. |
| [81] | 6-11 y |
5 TD 9 ADHD |
Dictation of letters and digits MHA |
English | Statistical correlations between manual and digital data |
Static Kinematic |
N.A. |
| [82] | 7-12 y | 60 | Copy of words, sentences and graphic shapes | Latin | RF, Decision tree, SVM | Kinematic | SE: 92,8 % P: 92,6 % |
| [83] | 8-15 y | 63 TD 57 DG |
Letters, words, sentences | Slovak | KNN, SVM, RF, AdaBoost | Kinematic (on-surface and in-air) | SE: 78,5 % P: 80,8 % |
| [84] | 8 y | 27 TD | Letters | Hebrew | RF, linear discriminant analysis | Kinematic | SE: 96 % |
| 27 DG | |||||||
| [85] | 8-9 y | 61 TD 15 DG |
Copy of patterns and figures | Czech | XG-Boost | Kinematic | SE: 90 % |
| [86] | 8-9 y |
14 TD 14 DG |
Copy of a text | Hebrew | Statistical comparisons between groups |
Static Kinematic |
N.A. |
| [42] | 8-9 y | 50 TD 49 DG |
Copy of letters and sentences | Hebrew | SVM | Static Kinematic |
SE: 90 % SP: 90 % P : 89,9 % |
| [87] | 8-11 y | 32 TD | Spontaneous writing (sentences), drawings | Indonesian | SVM & RBF Kernel | Kinematic | P : 82,5 % |
| [88] | 8-9 y | 33 TD 32 DG |
Copy of a text | Czech | Tunable Q-factor wavelet transfom, RF and SVM classifiers | Kinematic | SE: 88,7 % SP: 83 % P: 84,7 % |
| [89] | 8-9 y |
30 TD 25 DG |
Spontaneous writing of letters | Czech | Correlation between the kinematic features and the HPSQ-C | Kinematic | N.A. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



