
Submitted:
17 November 2023
Posted:
20 November 2023
You are already at the latest version
Abstract
Background: Therapeutic climbing (TC) has emerged as a prospective rehabilitation approach for individuals with Multiple Sclerosis (MS). Existing literature primarily focuses on the physical and psychological benefits of TC across diverse populations but is limited concerning its application and efficacy for patients with MS. Objectives: This study aimed to delineate the experiences, effects, and perceptions of both individuals with MS and therapists regarding TC, highlighting the potential benefits and challenges of this therapeutic approach. Methods: Using a qualitative design, structured interviews were conducted with patients living with MS (N=5) and therapists (N=7) involved in TC sessions at a rehabilitation facility. The interviews were recorded, transcribed verbatim, and subjected to thematic qualitative text analysis. Results: Our analysis resulted in the identification of five main categories: (1) motivational factors, (2) training conditions, (3) training content, (4) observed effects, and (5) safety protocols. Findings primarily centred around the motivational aspects of TC. Participants consistently reported experiencing feelings of accomplishment, success, enjoyment, and increased self-confidence. Furthermore, TC was often perceived as a comprehensive intervention, addressing endurance, strength, flexibility, neuromotor functions, cognition, and mental health while having a low-risk profile. However, due to the demanding nature of TC, careful fatigue management is crucial. This entails personalized intensity adjustments during sessions and coordinating TC with other physically demanding therapies when implementing TC within a rehabilitation environment. Conclusions: TC shows promise within MS rehabilitation and can be considered safe under certain framework conditions. This research sheds light on its potential benefits, facilitators and barriers and provides insights for practical integration into rehabilitation programmes.
Keywords:
multiple sclerosis
; therapeutic climbing
; motivation
; training conditions
; neurorehabilitation
; qualitative research
1. Introduction
Multiple sclerosis (MS), also known as encephalomyelitis disseminata, is an inflammatory neurodegenerative disease affecting the central nervous system, which includes the brain and spinal cord [1,2]. This chronic autoimmune condition typically manifests early [3], frequently resulting in long-term disabilities and diminished social participation [4,5], as well as cognitive impairments and concentration problems [6,7]. The symptoms of MS can be managed through medications and non-drug therapies, such as physiotherapy, occupational therapy, speech therapy, psychotherapy, neuropsychological therapy, and psychosocial care [8]. Therapeutic climbing (TC) is one specific approach to treating patients with MS that involves non-cyclical whole-body movements, integrating elements of strength and endurance training [9,10]. Nonetheless, a standardized definition for TC remains elusive, as it can vary from bouldering without a safety rope to tailored exercise regimens and rope climbing [9,11,12,13]. While its initial use was in orthopaedics, TC has subsequently expanded to the fields of neurology, psychiatry, and psychology [12].
Numerous studies have highlighted the benefits of climbing on healthy individuals, citing improvements in balance, coordination, core stability, mobility, and muscle strength while carrying minimal risk of injury [14,15,16,17]. Further, a systematic [18] and a narrative review [12] underscored the potential of TC to alleviate MS symptoms, enhancing physical fitness, fatigue management, self-efficacy, and overall quality of life. Delving deeper into specific studies, a randomized controlled trial with 20 participants compared sport climbing, using a belt and a top rope system, to yoga [19]. After ten weeks, participants in the climbing group observed a 25% decrease in the severity of their reported disabilities and a 33% decline in fatigue levels. Another RCT (n=27) found a positive impact on fatigue after two hours of TC weekly over six months [13]. It is worth noting that no research on TC and its utilization for people with MS was identified in the rehabilitation setting. Therefore, there is a significant gap in comprehensive research addressing TC benefits and challenges for patients with MS in rehabilitation settings.
In response to this need, our study focused on gathering detailed experiences related to TC for patients with MS within a rehabilitation environment. We examined various facets, including motivational factors, necessary training conditions, observed effects, and safety protocols. Thus, barriers and facilitators towards the relatively novel intervention of TC should be uncovered. From the perspectives of both patients and therapists, we aimed to understand how and why certain elements hinder or promote the use of TC. This inclusion is crucial as it will provide insights into what is needed to optimize the therapeutic efficacy of TC.
2. Materials and methods
2.1. Study design
Adopting a qualitative research methodology, this manuscript is written according to the COREQ guidelines [20]. This study was performed at a rehabilitation facility in Vienna holding 147 inpatient and 30 outpatient therapy places specializing in neurological and neuropsychological rehabilitation [21]. The primary aim of this facility is to either restore or sustain patients' functional and performance abilities through maintaining an integrated multidisciplinary approach, with a team comprising physiotherapists, training therapists, dieticians, occupational therapists, speech therapists, neuropsychologists, orthoptists, nursing staff providing bedside therapeutic interventions, and neurologists. While TC is recognized as a standard intervention within the rehabilitation framework, its application is tailored to individual patients based on specific goal setting, indications, and contraindications. Sessions, typically lasting 25 minutes, are conducted 2 to 3 times weekly. During each session, two patients engage in climbing activities on two neighbouring boulder walls, each spanning a height of 2.5 meters. One therapist diligently oversees the activities throughout these sessions to ensure appropriate patient safety and guidance.
During this study, we used several techniques to meet the primary quality criteria regarding the trustworthiness of our qualitative data. In terms of credibility, we sought peer debriefing from colleagues experienced in qualitative research to provide us with their external perspectives to validate our interpretations. To enhance the dependability of the data, we maintained an audit trail in the form of a detailed record of our research process. We ensured consistency in our data collection methods through predetermined protocols. For confirmability, we strengthened our team's reflexivity through regular discussions to acknowledge and mitigate our biases. Finally, we contextualized our findings and interpretations in this work to allow transferability to other settings [22].
2.2. Participants
Two groups of participants were included, namely patients with MS and therapists working with them. To ensure representability, all potential participants at the rehabilitation facility were asked face-to-face if they wanted to take part in the study. From April 25th 2022, to July 21st 2022, all patients and therapists who met the eligibility criteria were invited to participate in qualitative interviews. The inclusion and exclusion criteria were established as follows. Patients had to be (1) diagnosed with MS according to ICD-10 (code: G35) [1], (2) aged ≥18 years, (3) undergoing rehabilitation at the facility where the research was conducted, (4) assigned to TC, and (5) providing informed consent. Patients who did not possess sufficient knowledge of the German language were excluded. Therapists were required to be (1) sports teachers or sports scientists working at the rehabilitation facility, (2) possessing a minimum of one year of practical experience in TC with patients with MS, and (3) providing informed consent.
2.3. Data collection
To gather individuals' subjective experiences, feelings, perspectives, and attitudes, two group-specific sets of semi-structured in-depth interview guidelines were employed for patients and therapists (see Appendix 1 for the full interview guidelines) [23]. For both groups, interview guidelines comprised training modalities, motivational aspects, subjective effects, safety considerations, and applicability of the therapeutic approach, with group-specific sub-questions. Additionally, therapists were asked about criteria that would lead to the exclusion of patients from TC. Both interview guidelines were pretested with a medical professional experienced in sport climbing and slightly adapted, subsequently. Furthermore, interview schedules were refined in comprehensive discussion rounds between researchers after each interview. Due to a lack of time and resources, we opted against a repeat-interview design.
All interviews were conducted individually and face-to-face at the premises of the rehabilitation facility by one physiotherapist (Eva Reiter). When this study was undertaken, she was an active physiotherapist at the rehabilitation facility, accumulating five years of professional experience. Before the study commenced, no previous relationship existed between her and the included patients. Participants were informed of the interviewer’s professional role within the rehabilitation facility and the research objectives before their interview. Patient interviews were scheduled at the earliest in the second week of their rehabilitation, ascertaining they had acquired sufficient experience with TC. Therapists were interviewed during their available working hours, ensuring they had a one-hour window without any patients. Interviews lasted between 24 and 36 minutes, and field notes were made during or after every interview. Interview transcripts were not returned to participants for further comments or corrections.
In addition to the interviews, patients’ age, sex, duration of illness, and the Expanded Disability Status Scale (EDSS) were collected. The EDSS is a scale ranging from 0 to 10 that provides information on the individual level of disability, with higher values indicating more severe impairments [24]. People scoring between 1.0 and 4.5 have a high degree of ambulatory ability, whereas those scoring between 5.0 and 9.5 experience a decline in their ambulatory ability. Additional information collected from therapists includes sex, years of work and TC experience.
2.4. Data analysis
The interviews were audio-recorded, manually transcribed and analysed using thematic qualitative text analysis following Kuckartz's methodology [25]. Initially, two researchers separately coded data collected from patients and therapists by assigning relevant text sequences to major codes derived from the two interview guidelines. This deductive approach yielded two group-specific code sets that were refined and expanded in the process. Iteratively comparing and contrasting the tentative codes with the original transcripts enhanced the precision and explanatory capacity of the subsequent inductive text analysis. Based on the collected interview material, the two researchers inductively adapted and synthesized the initial code sets, which resulted in six main categories with corresponding subcategories in a single code set (Figure 1). In order to reach a consensus during the process, the two coding researchers employed a systematic and iterative approach with regular in-person or online meetings to discuss their individual progress and coding decisions, resulting in a shared codebook. If a disagreement between coders occurred, triangulation was maintained by introducing a third independent researcher from the study team to review and mediate these discrepancies independently. Participants were not further involved in this stage. Both the transcription and coding were conducted software-aided utilizing MAXQDA 2022.
2.5. Ethical considerations
The Ethics Committee of the University for Continuing Education Krems granted ethical approval for this study (EK GZ 08/2021-2024). Participants provided informed consent both in verbal and written form prior to the initial interview session. The interview transcripts were pseudonymised to ensure data privacy by assigning consecutive numbers as codes to replace participants' names. While patients and therapists were allocated an individual number within their groups, patients' codes were designated with an additional letter "P", and therapists' codes were indicated with "T", respectively. Participants were given their codes after signing the informed consent form. Consequently, only the study authors could identify the individuals involved. Once the verbatim transcription was completed, all audio files were utterly deleted.
3. Results
At the rehabilitation facility, 30 patients with MS and 14 therapists were available during the study period. TC was not prescribed to 24 patients by their physicians in charge because the therapy did not align with their individual goals. In the group of therapists, six were not offering TC and were therefore excluded from participation. Furthermore, two eligible individuals, one patient and one therapist, chose not to take part in the study. Eventually, a total of 12 participants, comprising five patients and seven therapists, were interviewed (Figure 1). Three female and two male patients aged 35 to 59 participated in the study (Table 1). The duration of their disease varied between 1 and 24 years. The patients’ median EDSS score was 3.0, with a minimum of 2.0 and a maximum of 3.5. All patients engaged in TC sessions attended them between 3 and 11 times.
Among therapists, there were three women and four men. The therapists' experience with TC ranged from 2 to 15 years (Table 2).
The final code set consists of the five main categories: (1) Motivational factors, (2) Training conditions, (3) Training content, (4) Observed effects, and (5) Safety protocol, with subcategories indicated in Figure 2.
3.1. Motivational factors
All participating patients associated TC with a sense of challenge and fun, as they embraced the difficulties of the tasks, finding joy in overcoming them, and perceived these experiences as driving factors. Concurrently, all interviewed therapists emphasized the motivational aspect of fun emerging during TC sessions, recognizing its positive influence on patients' engagement in the entire therapeutic process:
And the big advantage is that the exercises are very short, and then you immediately have a success – and if you have no success, then you think to yourself that it also does not matter. […] But it is simple, uplifting. It is good for the mind. It raises your self-esteem again, and that's a fun factor, where you know: "Yes, if I make it, then it's good, and if not, it doesn't matter."(P2)
In addition, patients consistently reported their experience of achieving a profound level of concentration that seamlessly transitioned into a state often referred to as “flow”:
“You have quite a tunnel vision, then. For me, it is like this. I do not notice much around me. I am also quite sensitive to noise, but I am highly concentrated. I get into a flow and always want to do things right. So, I do not always want to do things halfway – I just want to do it right.”(P3)
Related to the desired outcome and among various motivational factors mentioned by both patients and therapists, the exhilaration of pushing one's physical limits and experiences of success and confidence stood out prominently. Several respondents emphasized the intense engagement and focus that climbing demanded, which contributed significantly to their motivation:
“The motivation is to get it done. So certain movements, whether the basic position or coming up [the wall], reach as high as I can. The nice thing is that you see the result immediately. If it works or does not work, that is just great. And if it does not work, I just do it again. So that is really special, and I really enjoy it.”(P5)
“I liked that although I am thin, I have quite a bit of strength in my hands, and I can use that. I have a good feeling because I know: "You can do that." And I am not at the mercy of the feeling that I am going to fail.”(P3)
Respondents enormously appreciated the training content, which they perceived as highly effective or remarkably diverse. As a means to further ends, the allure of trying out "something new" and the vast array of activities were seen as additional motivational factors. This sentiment was echoed by three professionals who highlighted TC’s capability to introduce patients with MS to novel experiences. They saw it as an opportunity to present patients with a potential new hobby. Two therapists valued TC's application versatility and capacity to provide patients valuable feedback through heightened body awareness during climbing.
3.2. Training conditions
The success of TC depends on several conditions, including intensity, frequency and duration, and setting (individual or group). All respondents unanimously described training intensity as ranging from intensive to very intensive:
“And that is simply what distinguishes it from physiotherapy, where it is quite clear what is happening, for instance, squatting down or with the heels on the floor – just as great. It is just that with climbing, there is also the aspect of fun, while at the same time, it is somehow very intense, but that is good.”(P5)
P5 further elaborated on the unique challenges posed by climbing:
"When you face challenges in climbing, you can't just take it lightly. In other forms of training, you can adjust the weight to your preference; for instance, I could choose to train with 5 kilos. But in climbing, you're contending with your own body weight. That's the weight you must manage."
Moreover, they perceived TC as demanding and strenuous due to the constant requirement of supporting one's body weight during exercises. However, this high training intensity was indicated as an inherent aspect of TC that is thus inevitable but can be modulated to fit patients’ needs:
“Because as a therapist, it starts relatively soon that I play with the intensities. If I see that the person is doing a great job and it is working great, I can think about doing a more difficult exercise for them. If I see that the exercise is already quite demanding, then I can make the next exercise easier.”(T2)
Therapists have highlighted challenges in therapy planning, emphasizing the need to coordinate TC sessions with other physically demanding therapies like strength training or physiotherapy. Moreover, they stressed that it is advisable not to schedule TC on two consecutive days. This particular condition was also echoed by the patients themselves, who often expressed the desire for a break immediately after a TC session:
“I just have to rest for a short while after the training. […] Half an hour or hour and then I feel very fit again.”(P4)
All patients expressed satisfaction with the frequency and duration of the therapy sessions, deeming them appropriate. They acknowledged that longer therapy sessions might lead to a potential loss of concentration and increased frustration:
“Longer [sessions] would avail to nothing because then you get into exhaustion, and then you are demotivated, because it does not work. So, because it is also a strength exercise, with this trunk stabilization, I think that is a good time interval. Just that long, not longer, not shorter.”(P2)
Patients and therapists responded in controversial ways regarding the TC group vs individual setting. However, several advantages of the group setting were highlighted by either group. Firstly, patients expressed their enjoyment of training in pairs, finding it a pleasurable experience. Secondly, the presence of fellow participants served as a motivating factor, providing the much-needed incentive to push themselves during the training sessions. Additionally, both groups appreciated the flexibility of taking necessary breaks when required, which the therapists emphasized. Nevertheless, a therapist, T5, highlighted the limitations of the group setting:
“It is a group, and group programs are usually just not so specific. Or let me put it this way: it is a clear extra effort if you give two patients completely different exercises.”(T5)
3.3. Training content
All respondents uniformly divided TC sessions into three main components: a warm-up phase, which can take place directly on the climbing wall or the floor, followed by the main phase encompassing specific exercises in the basic climbing position and dynamic climbing moves, and finally, an optional cool-down phase. All participants positively rated this training structure. The basic climbing position, where both hands and feet maintain contact with the climbing wall, was consistently regarded as a crucial element of TC. This position was seen as instrumental in promoting stability, ensuring safety, and enhancing body awareness during the sessions:
“So, what I find good is that the exercises always go out from a fixed basic position, where the basic position always recalls this stability again and again. That is – with the shoulders down and abdominal tension and a bit of squatting – heels up.”(T1)
Specific exercises, such as targeted grasping, were frequently highlighted for their role in improving coordination. Patients with MS particularly appreciated the activity of climbing from one side of the wall to the other while having to perform tasks. They described this experience as not only providing a pleasant somatic sensation but also fostering a sense of accomplishment by recognizing personal abilities:
“And today – I climbed today for the second time – I climbed from wall to wall. It was great, both with overhang, it was really cool. […] It is structured great. First, you learn to do the basics and climb that way. […] Then the arms relaxed, and I actually climbed from right to left and left to right today.”(P5)
3.4. Observed effects
In terms of the physical effects of TC, four participants reported significant gains in strength, particularly in the trunk, arms, and grip. Therapists also observed several positive physical effects, including improvements in strength, trunk stability, coordination, balance, body perception, mobility, and posture:
“Of course, [TC is] strengthening the muscles – be it upper arms or grip strength, lower extremities, or trunk stability, respectively. Another effect is, for example, torso stability, spinal stability, posture, but also coordination. And, of course, how to grasp things, how tightly you have to grip in order to be able to hold on. Balance is also trained for people to become a bit more mobile and secure in everyday life and minimize their risk of falling.”(T4)
“In the neck, shoulder, and upper back areas, I notice it already. And, of course, biceps, triceps, you feel very strongly. […] Anyways, you notice the strength, which then just increases a bit. The grip strength is what now just works properly.”(P3)
Both therapists and patients reported positive mental and psychological effects, including mood, executive functions, social skills, and self-confidence. Notably, self-confidence was highlighted as an area that was particularly empowered, according to the professionals:
“I think climbing also has a high motivational character, so the patients gain self-confidence and security. By climbing not only at standing height but also a little higher, I believe that patients gain self-confidence and thus appear more self-assured.”(T4)
Likewise, participants with MS mentioned TC’s positive effects on mental health and the benefits of combining physical and cognitive training:
“I already felt like I fit in. I think I have improved not only my athletic activity but also my cognitive capability because you just have to think ahead: Where do I step? Where do I reach? […] That is not so easy for me, and that is why I actually found it good that I can combine both in one unit, both physically and then mentally a bit.”(P3)
3.5. Safety protocol
Overall, all therapists unanimously described TC as an excellent whole-body workout. The indications for TC primarily revolved around patients’ desire to enhance trunk stability, strength, coordination, and concentration. However, using TC to increase leg muscle strength specifically sparked a controversy among therapists. While one respondent believed in its effectiveness, another therapist expressed reservations, suggesting that TC might not be the ideal method for targeting the legs. Therapists underscored a certain degree of body awareness and coordination as a prerequisite for engaging in TC.
Additionally, they pointed out that patients with MS should possess curiosity and a willingness to try out TC, as this attitude plays a significant role in the effectiveness of the therapeutic approach. Six therapists praised TC for its comprehensive, varied whole-body workout with abundant movement variations. Three of them even drew a comparison with traditional strength training, noting that TC outshined it in promoting body awareness, coordination, and variety:
“Well, it also has much to do with self-awareness, which is perhaps not the case with normal strength training, where I sit on the machine and simply move the leg press. There is just not as much body awareness as in climbing.”(T5)
Several contraindications for TC were identified during the therapist interviews, namely severe pain or sensory disorders, inability to hold onto the climbing wall due to reduced arm function, acute injuries or inflammations, epilepsy, inability to follow the tasks for 25 minutes due to limited attention and concentration, severe cardiovascular disease, and inability to stand safely for 25 minutes:
“First of all, they need to have a certain strength in the forefeet – so that they can stand on their forefeet at all – and then hold themselves up with the upper extremities with both hands.”(T2)
In addition, patients with MS named paresis, sensory disorders, and severe ataxia as potential contraindications. Three respondents emphasized assuming and maintaining the basic climbing position, necessitating toe stance, sufficient trunk stability, and grip function as essential TC requirements. As a result, patients severely affected by MS or those who have recently experienced a relapse should not be included in TC sessions. Notably, three patients expressed concern about the potential frustration that people with these contraindications might experience if they were assigned to TC despite their conditions:
“I mean – I have never had the case – but if any extremity would be paralyzed or that somebody has perhaps such feelings of numbness, I imagine that would be difficult. I would not know if that would not be rather frustrating if I felt that way.”(P3)
Safety was paramount for all patients during the TC sessions, and they unanimously expressed feeling secure throughout the training. The presence of fall mats and spotting (i.e., attentive therapists standing behind them) contributed to creating a protected and reassuring atmosphere:
“I felt safe because the therapist was always behind me, and I know she catches me when something happens.”(P1)
Moreover, therapists themselves rated TC as a very safe therapeutic approach. The low therapist-to-patient ratio, with one therapist attending to two patients, coupled with exercises tailored to the individual abilities of the patients, contributed significantly to ensuring safety during the sessions. Furthermore, using a low jump height, ranging from 30 to 40 cm, was deemed relevant in maintaining a safe environment. Five therapists mentioned spotting as an effective measure to prevent accidents and enhance overall safety:
“As a therapist, if you notice that it is unsafe, you can also stand directly behind the patients. That means that if they slip, it is safe so that they do not hurt themselves badly.”(T1)
Nevertheless, therapists stressed that while regular safety checks of the climbing wall are obligatory to ensure a secure environment, extra caution is necessary during both ascent and descent and when patients move horizontally across the climbing wall.
Participants also raised concerns about potential complications, including pain, exhaustion, and overheating. Specifically, four therapists noted that mild pain, particularly in the shoulder area, might occur as a possible side effect:
“Such [mild] pain may occur again and again, in the shoulders, in the knee joint – but nothing more serious.”(T4)
Remarkably, none of the patients reported experiencing pain during or after the climbing sessions. On the contrary, one of them even mentioned reducing their pre-existing back pain as a positive outcome of the TC training.
However, patients also highlighted exhaustion as a notable concern. Two respondents specifically mentioned experiencing motor fatigue either during or immediately after climbing. For one of these patients, recovery took a significant amount of time, while the other reported encountering eating restrictions resulting from the exhaustion:
“Once, it was too much for me. I think this morning was intense because I was training in half-hour intervals without a break – first climbing, then eating. And then, I had an intensity tremor in my hands, and then I noticed […] the trembling of the hands became significantly more, and it was difficult to eat.”(P3)
When specifically questioned about fatigue and fatigability, most therapists acknowledged having observed instances of fatigue among their patients with MS. However, they did not recognize it as a major issue of TC:
“I have to say that I cannot think of any MS patient who has stopped climbing with me because of fatigue. […] When patients stop, it is usually because of pain; those are more likely to be spine patients. […] Of course, what happens from time to time is that they say beforehand that they are totally exhausted. But then you try to arrange it so the MS patient takes longer breaks.”(T5)
Also, one therapist pointed out overheating as a potential complication. To address this concern, using cooling vests was suggested.
4. Discussion
The present investigation aims to gain a detailed understanding of the experiences and perceptions of therapists and patients with MS within the context of TC. The results provide important insights into various aspects of TC, including motivational factors, training conditions, training content, observed effects, and safety protocols.
- Motivational factors
In all interviews, the motivation, particularly challenge and fun, was strongly emphasized by both the participants and therapists. This high motivational factor of TC was also found in previous studies [10]. In contrast to our research, the mentioned study focused on TC in general, not specifically on MS. When looking at the mentioned motivational factors in detail, our findings are aligned with the pre-existing classification defined by Gabler [26]. Accordingly, the motivation to do sports activities can derive from the engagement in sports activities itself (relating to our subcategory “challenge and fun”), desired outcomes of sports activities (relating to our subcategory “experiences of success and confidence”), and sports activities as a means to further ends (relating to our subcategory “trying out ‘something new’”). This element appears to play a crucial role in maintaining engagement and adherence – an essential factor for the success of rehabilitative interventions. Considering this high motivational level, TC could potentially encourage long-term physical activity. This is especially important as studies indicate that patients with MS tend to be less physically active than individuals without health issues [27]. A promising pathway for long-term physical activity could involve integration with existing extramural climbing groups specifically tailored for individuals with disabilities. Organizations like the Austrian Alpine Club [28] could lead the way in accommodating patients with MS within their climbing activities. This approach not only ensures a structured and safe training environment but also capitalizes on the communal nature of climbing, potentially enriching the therapeutic experience. Another possibility would be to develop specialized apps [29,30].
- Training conditions
The training content mentioned in our study offers intriguing insights into rehabilitation practices. Our study delineated a structured division of TC sessions into a warm-up phase, a main phase, and an optional cool-down phase, aligning with literature identifying a well-organized structure as crucial for effective rehabilitation sessions [31]. This setup not only promotes safety but also ensures a challenging progression and efficient recovery. It is noteworthy that patients also perceive this structure as effective and appropriate. A fundamental aspect of TC is the emphasis on the basic climbing position. The "four-point contact" approach is particularly significant, as it trains core stability, a crucial factor for many patients with MS, given their frequent deficits in this area [32].
Concerning the intensity, the respondents highlighted the holistic approach of TC and often called it an excellent “whole-body workout”. The observed intensity, ranging from intensive to very intensive, aligns with the inherent nature of climbing, which demands a higher level of physical exertion [33]. Therefore, the challenge is to find the right balance between intensity and recovery [12,34], especially for patients undergoing a series of therapy sessions [35]. Generally, physical activity recommendations for MS call for an individualized program considering each person's needs and preferences [36,37].
One practical approach lies in scheduling. Research indicates that many patients with MS feel more energized in the mornings [38]. Thus, aligning intense activities with this period can optimize outcomes. Furthermore, gradually increasing intensity can also prevent sudden fatigue [39], the most commonly mentioned issue among interviewed patients with MS. Based on our results, recovery periods post-TC sessions are demanded. To effectively manage fatigue while maximising therapeutic benefits, customized therapy plans addressing individual reactions and requirements are essential.
- Observed effects
Looking at the observed effects, the therapeutic benefits of regular physical activity for individuals with MS are well documented, including reduced fatigue, pain, and depressive symptoms and increased functional capacity, balance, muscle strength, and aerobic capacity [40]. However, delving into the observed effects in our study, especially the improvements in strength, trunk stability, coordination, body perception, and psychological aspects, reflect a multifaceted reality of the individuals' therapeutic journey. Previous studies also found possible physiological and psychological benefits from TC [12,18]. Our current study adds to this discourse by emphasizing the combined physical and cognitive challenges posed by TC, especially considering the frequent cognitive challenges faced by patients with MS [10,41]. Additionally, the surge in self-confidence reported in our study aligns with previous findings [17]
Strengths and limitations
The study has clear strengths in its approach. First, the study was conducted in a precise environment, the rehabilitation setting. Especially in this setting, there is very little scientific literature on TC. Moreover, the inclusive participation of both patients with MS and therapists as key respondents enriches the depth and breadth of the data collected. By integrating insights from these two primary stakeholders, the research not only gains a multifaceted perspective but also bolsters the validity of its findings.
However, this study also has several limitations. Firstly, we cannot assess the effects of TC in this setting, as patients were simultaneously involved in other treatments (e.g. physiotherapy, treadmill training). Secondly, some patients had only a few TC sessions, which may have affected the depth of their feedback. Thirdly, the relatively small number of participants from only one institution could limit the breadth of perspectives and experiences captured, potentially affecting the degree of data saturation and transferability of our findings. Further, the potential for interviewer bias in relation to both patient and therapist interviews exists, given that the data collection was conducted by an active physiotherapist at the rehabilitation facility. Although no prior relationship existed between the interviewer and the included patients, the interviewer's professional role within the facility could have inadvertently influenced participants' responses. Lastly, the method of data collection, relying on semi-structured in-depth interviews, inherently carries a subjective element. Thus, the responses gathered are subject to the participants' perceptions and recall, which may not always provide an objective reflection of their experiences or the effects of TC.
5.Conclusions
Respondents viewed TC positively, appreciating its motivational factor, efficacy, and minimal risk profile. A standout feature of TC is its motivational component, which stems from individuals' first-hand experiences of enhanced physical capabilities and accomplishments. A finding emerging from this study is the impact of TC on managing and addressing fatigue, a prevalent concern for patients with MS. Feedback from participants indicates that while TC offers tangible physical improvements and boosts motivation, it is crucial to individualize sessions, especially considering the fatigue experienced by patients with MS. To gain a more transparent, more generalizable understanding, future studies should delve deeper, employing quantitative methodologies to evaluate TC's effectiveness rigorously. Given the intensive nature of TC, meticulous fatigue management and individualised intensity adjustments are essential.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgements
We would like to thank the Neurological Rehabilitation Centre Rosenhügel for making the research possible. A special thank you goes to the participating therapists and patients.
Competing interests
None to declare.
Disclosure statement
No potential conflict of interest was reported by the author(S).
References
- WHO. ICD-10: International Statistical Classification of Dis-eases and Related Health Problems 10th Revision 2019.
- Tafti, D.; Ehsan, M.; Xixis, K.L. Multiple Sclerosis. In StatPearls; StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL), 2022. [Google Scholar]
- Kesselring, J.; Beer, S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol 2005, 4, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, A.; Marissal, J.P.; Pouyfaucon, M.; Vermersch, P.; Hautecoeur, P.; Dervaux, B. Social participation in patients with multiple sclerosis: correlations between disability and economic burden. BMC Neurol 2014, 14, 115. [Google Scholar] [CrossRef] [PubMed]
- Salter, A.; Fox, R.J.; Tyry, T.; Cutter, G.; Marrie, R.A. The association of fatigue and social participation in multiple sclerosis as assessed using two different instruments. Mult Scler Relat Disord 2019, 31, 165–172. [Google Scholar] [CrossRef] [PubMed]
- DeSousa, E.A.; Albert, R.H.; Kalman, B. Cognitive impairments in multiple sclerosis: a review. Am J Alzheimers Dis Other Demen 2002, 17, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Petracca, M.; Pontillo, G.; Moccia, M.; Carotenuto, A.; Cocozza, S.; Lanzillo, R.; Brunetti, A.; Brescia Morra, V. Neuroimaging Correlates of Cognitive Dysfunction in Adults with Multiple Sclerosis. Brain Sci 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Iodice, R.; Aceto, G.; Ruggiero, L.; Cassano, E.; Manganelli, F.; Dubbioso, R. A review of current rehabilitation practices and their benefits in patients with multiple sclerosis. Multiple Sclerosis and Related Disorders 2023, 69. [Google Scholar] [CrossRef] [PubMed]
- Leichtfried, V. Therapeutisches Klettern – eine Extremsportart geht neue Wege. In Alpin und Höhenmedizin; Franz Berghold, H.B., Martin Burtscher, Wolfgang Domej, Bruno Durrer, Eds.; Springer, 2015; pp. 107–117. [Google Scholar]
- Frühauf, A.; Heußner, J.; Niedermeier, M.; Kopp, M. Expert Views on Therapeutic Climbing-A Multi-Perspective, Qualitative Study. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Buechter, R.B.; Fechtelpeter, D. Climbing for preventing and treating health problems: a systematic review of randomized controlled trials. Ger Med Sci 2011, 9, Doc19. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Gong, X.; Li, H.; Li, Y. The Origin, Application and Mechanism of Therapeutic Climbing: A Narrative Review. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Kern, C.; Elmenhorst, J.; Oberhoffer, R. [Effect of sport climbing on patients with multiple sclerosis – hints or evidence?]. Neurologie & Rehabilitation. 2013, 4, 247–256. [Google Scholar]
- Gallotta, M.C.; Emerenziani, G.P.; Monteiro, M.D.; Iasevoli, L.; Iazzoni, S.; Baldari, C.; Guidetti, L. PSYCHOPHYSICAL BENEFITS OF ROCK-CLIMBING ACTIVITY. Percept Mot Skills 2015, 121, 675–689. [Google Scholar] [CrossRef] [PubMed]
- Mermier, C.M.; Robergs, R.A.; McMinn, S.M.; Heyward, V.H. Energy expenditure and physiological responses during indoor rock climbing. Br J Sports Med 1997, 31, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Rodio, A.; Fattorini, L.; Rosponi, A.; Quattrini, F.M.; Marchetti, M. Physiological adaptation in noncompetitive rock climbers: good for aerobic fitness? J Strength Cond Res 2008, 22, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Fruhauf, A.; Sevecke, K.; Kopp, M. [Current state of the scientific literature on effects of therapeutic climbing on mental health - conclusion: a lot to do]. Neuropsychiatr 2019, 33, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Steimer, J.; Weissert, R. Effects of Sport Climbing on Multiple Sclerosis. Front Physiol 2017, 8, 1021. [Google Scholar] [CrossRef] [PubMed]
- Velikonja, O.; Curic, K.; Ozura, A.; Jazbec, S.S. Influence of sports climbing and yoga on spasticity, cognitive function, mood and fatigue in patients with multiple sclerosis. Clin Neurol Neurosurg 2010, 112, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International journal for quality in health care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- NRZ Rosenhügel. Available online: https://www.nrz.at/ (accessed on 22.03.2023).
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. International journal of qualitative methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Eppich, W.J.; Gormley, G.J.; Teunissen, P.W. In-Depth Interviews. In Healthcare Simulation Research: A Practical Guide, Nestel, D., Hui, J., Kunkler, K., Scerbo, M.W., Calhoun, A.W., Eds.; Springer International Publishing: Cham, 2019; pp. 85–91. [Google Scholar]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Kuckartz, U. Qualitative Text Analysis: A Guide to Methods, Practice & Using Software; SAGE Publications Ltd: New York City, 2014. [Google Scholar]
- Gabler, H. Motive im Sport: motivationspsychologische Analysen und empirische Studien. (No Title).
- Jeng, B.; DuBose, N.G.; Martin, T.B.; Silic, P.; Flores, V.A.; Zheng, P.; Motl, R.W. An updated systematic review and quantitative synthesis of physical activity levels in multiple sclerosis. Am J Phys Med Rehabil 2023. [Google Scholar] [CrossRef]
- Alpenverein, D.; Alpenverein, Ö.; Südtirol, A. Hoch hinaus!; B? ohlau Verlag: 2016.
- Gopal, A.; Bonanno, V.; Block, V.J.; Bove, R.M. Accessibility to Telerehabilitation Services for People With Multiple Sclerosis: Analysis of Barriers and Limitations. Int J MS Care 2022, 24, 260–265. [Google Scholar] [CrossRef]
- Morimoto, Y.; Takahashi, T.; Sawa, R.; Saitoh, M.; Morisawa, T.; Kagiyama, N.; Kasai, T.; Dinesen, B.; Hollingdal, M.; Refsgaard, J.; et al. Web Portals for Patients With Chronic Diseases: Scoping Review of the Functional Features and Theoretical Frameworks of Telerehabilitation Platforms. J Med Internet Res 2022, 24, e27759. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Watts, P.B. Physiology of difficult rock climbing. Eur J Appl Physiol 2004, 91, 361–372. [Google Scholar] [CrossRef]
- Gassner, L.; Dabnichki, P.; Langer, A.; Pokan, R.; Zach, H.; Ludwig, M.; Santer, A. The therapeutic effects of climbing: A systematic review and meta-analysis. PM&R.
- Gassner, L.; Dabnichki, P.; Langer, A.; Pokan, R.; Zach, H.; Ludwig, M.; Santer, A. The therapeutic effects of climbing: A systematic review and meta-analysis. Pm r 2023, 15, 1194–1209. [Google Scholar] [CrossRef] [PubMed]
- Rzepka, M.; Tos, M.; Boron, M.; Gibas, K.; Krzystanek, E. Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients. Medicina (Kaunas) 2020, 56. [Google Scholar] [CrossRef]
- Kalb, R.; Brown, T.R.; Coote, S.; Costello, K.; Dalgas, U.; Garmon, E.; Giesser, B.; Halper, J.; Karpatkin, H.; Keller, J.; et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult Scler 2020, 26, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Dalgas, U.; Langeskov-Christensen, M.; Stenager, E.; Riemenschneider, M.; Hvid, L.G. Exercise as Medicine in Multiple Sclerosis-Time for a Paradigm Shift: Preventive, Symptomatic, and Disease-Modifying Aspects and Perspectives. Curr Neurol Neurosci Rep 2019, 19, 88. [Google Scholar] [CrossRef]
- Learmonth, Y.C.; Motl, R.W. Exercise Training for Multiple Sclerosis: A Narrative Review of History, Benefits, Safety, Guidelines, and Promotion. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC neurology 2017, 17, 1–11. [Google Scholar] [CrossRef]
- Reina-Gutiérrez, S.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; de Arenas-Arroyo, S.N.; López-Muñoz, P.; Álvarez-Bueno, C.; Guzmán-Pavón, M.J.; Torres-Costoso, A. The type of exercise most beneficial for quality of life in people with multiple sclerosis: a network meta-analysis. Annals of Physical and Rehabilitation Medicine 2022, 65, 101578. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Motl, R.W.; Scudder, M.R.; DeLuca, J. Systematic, Evidence-Based Review of Exercise, Physical Activity, and Physical Fitness Effects on Cognition in Persons with Multiple Sclerosis. Neuropsychol Rev 2016, 26, 271–294. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of participants.
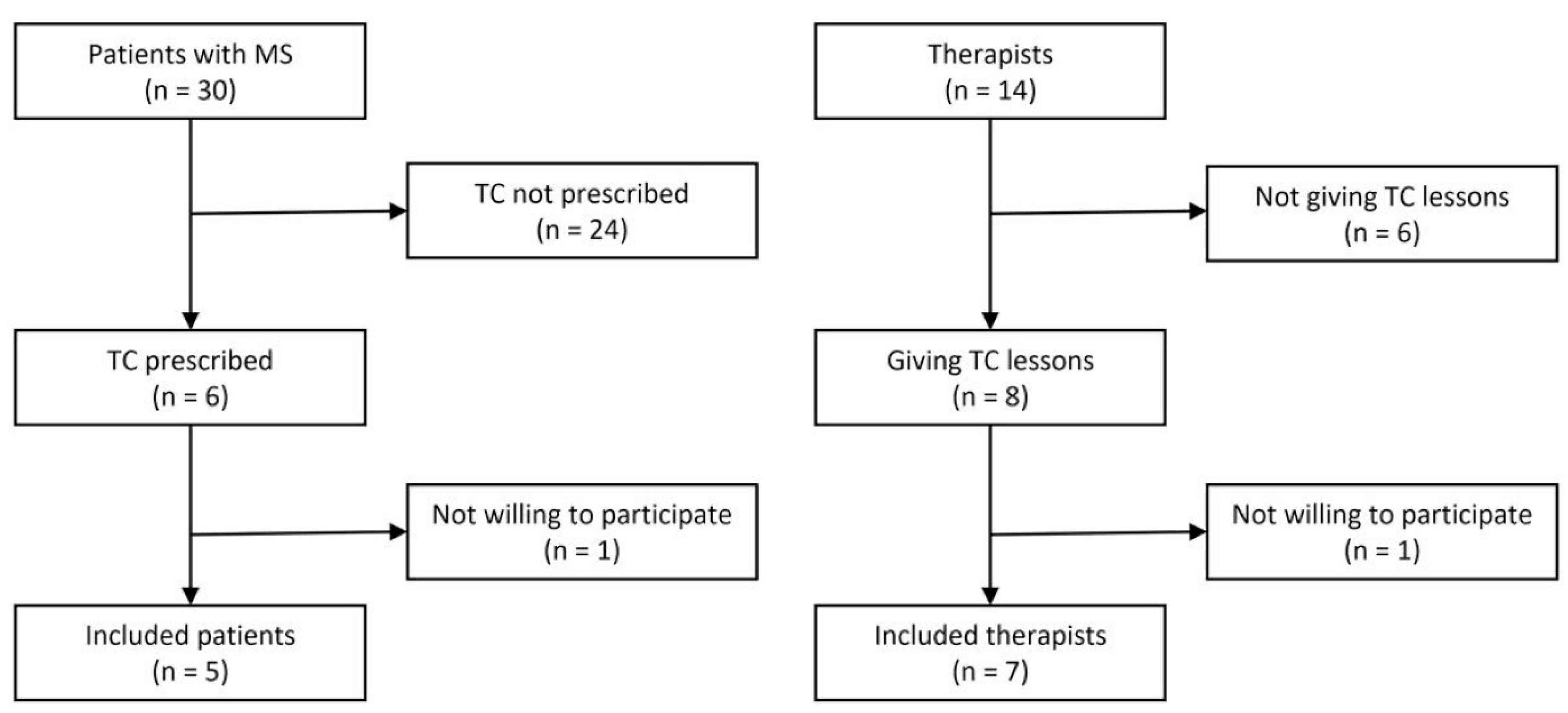
Figure 2.
Overview of Adapted Code Set Categories.
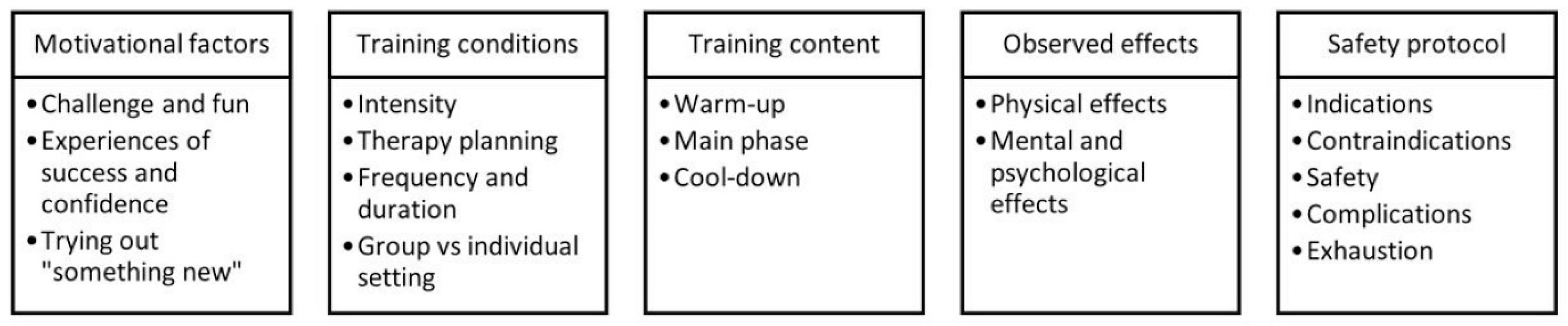

Table 1.
Participants’ characteristics – patients with MS.
| Code | Sex | Age | Duration of disease (years) |
EDSS score |
TC units attended |
|---|---|---|---|---|---|
| P1 | female | 59 | 22 | 3.0 | 3 |
| P2 | female | 54 | 24 | 3.5 | 6 |
| P3 | female | 35 | 11 | 3.5 | 11 |
| P4 | male | 37 | 5 | 2.0 | 7 |
| P5 | male | 35 | 1 | 2.5 | 6 |
EDSS = Expanded Disability Status Scale [24]; TC = Therapeutic climbing.
Table 2.
Participants’ characteristics – therapists.
| Code | Sex | Work experience (years) |
TC experience (years) |
|---|---|---|---|
| T1 | male | 16 | 4 |
| T2 | female | 6 | 3 |
| T3 | female | 20 | 15 |
| T4 | male | 2 | 2 |
| T5 | male | 9 | 9 |
| T6 | female | 12 | 2 |
| T7 | male | 20 | 15 |
TC = Therapeutic climbing.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



