
Submitted:
20 November 2023
Posted:
21 November 2023
You are already at the latest version
Abstract
Study design: Creating and psychometric testing of a new QoL Questionnaire about Physiotherapeutic Specific Exercises of Scoliosis (Questionnaire of Physiotherapeutic Specific Exercises of Scoliosis -QPSSE).
Purpose: The purpose of this study is to create a reliable and valid questionnaire for patients suffering mild and moderate adolescent idiopathic scoliosis (AIS) who have been treated with Physiotherapeutic Specific Exercises of Scoliosis (PSSE) in order to evaluate their quality of life.
Materials and Methods: The developed questionnaire was based on a thorough literature review as well as on authors experience. It consists of 53 questions, of which 37 have a positive meaning, 15 have a negative meaning, and one is multiple choice question, additionally there are six “open” questions. Except for the multiple choice question, all other questions are answered on a Likert scale ranging from 1 to 5 scores. 5 represents a positive meaning or very much, whereas 1 stands for a negative meaning or not at all. Questions were developed by the authors who subsequently categorized the 53 questions into the following 8 domains: physical functioning, self-image, Physiotherapeutic Scoliosis-Specific Exercises (PSSEs), psychosocial functioning, cognitive functioning, compliance, motivation and pain. A pilot study was conducted so that we could calculate Cronbach’s Alpha based on the outcome. Due to the COVID-19 pandemic, the authors worked through the Zoom online platform to structure the questionnaire.
Results: Pearson's correlation coefficient was used for all correlations evaluated. P values of less than 0.05 were considered to be significant. Internal consistency was evaluated with Cronbach's alpha. Although there were very few missing values, accounting for 0.78% of the total values of the questionnaire, expectation maximization likelihood algorithm was used to impute data. IBM® SPSS® Statistics Software v.25 was used for the analysis. Cronbach's alpha coefficients for the overall score was 0.84.
Conclusion: This original QPSSE was found to be a reliable and valid tool for AIS treated conservatively with PSSE and for their clinicians.
Keywords:
adolescent idiopathic scoliosis
; physiotherapeutic specific exercises
; questionnaire
; quality of life
1. Introduction
Idiopathic scoliosis (IS) is the most common type of scoliosis in people aged 10-18 years [1,2]. IS, is usually characterized as a 3-D deformity, as it affects the body in all the transverse, sagittal and coronal planes [3,4], but in reality it is a 4-D deformity, as the parson having this condition suffers from this during the hole period of life, therefore the fourth dimension is time. It is reported that the incidence of adolescent idiopathic scoliosis (AIS) ranges from 0.93% to 12% [4].
Early diagnosis and regular monitoring of IS is therefore very important for the prevention and control of its progression. The first clinical diagnosis of the presence of scoliosis is made performing the forward bending test, called Adam's test, which examines for a height difference in one of the two hemithoraces i.e. the presence of a hump [5]. The radiological diagnosis of IS is made by measuring the Cobb angle, which according to the SRS must be equal to or greater than 10°, in the frontal plane and the presence of axial rotation in the horizontal plane. Also, distortion is observed in the oblique plane [6,7].
The term "idiopathic" means that the cause for the condition's development is unclear. Published research shows that IS may be associated with many genetic and epigenetic factors [4,8]. Although scoliosis is considered as a harmless condition, evidence suggests that people with scoliosis are more prone to experiencing back and low back pain [9,10]. Scoliosis causes multiple dysfunctions and appears to be a burden on healthcare, particularly when patients require extensive surgical treatment [11,12]. If scoliosis progresses to a form that is not amenable to conservative treatment, then surgical treatment is indicated. Surgical treatment of scoliosis places a significant burden on the healthcare system due to the relatively high cost and risk of complications involved. As the risks associated with mild and moderate scoliosis are not very high, conservative treatment is preferred to surgical treatment in order to stabilise the deformity, improve quality of life and significantly reduce rehabilitation costs.
The application of Physiotherapeutic Specific Exercises for Scoliosis (PSEE) alone or with bracing currently is one of the therapeutic modules for mild and moderate IS. SOSORT uses the term Physiotherapeutic Specific Exercises for Scoliosis (PSSE) for all approved schools and methods. Each method and school incorporate the SOSORT guidelines principles and shares a common goal, that of stabilization, arrest progression of IS and improving the quality of life of patients. The methodology of the PSSE must be based on scientific evidence and adjusted according to the type of the deformity of each patient [13,14]. Another protagonistic and high priority common goal during the implementation of PSSEs, as recommended by SOSORT, is "three-dimensional self-correction" [4,15]. Self-correction can be defined as the best possible trunk alignment that a patient with scoliosis can achieve in the three planes and axes [16].
- Schroth, Germany
- Lyon, France
- SEAS (Scientific Exercise Approach to Scoliosis), Italy
- BSPTS (Barcelona Scoliosis Physical Therapy School), Spain
- Side Shift, UK
- DoboMed, Poland
- FITS (Functional Individual Therapy of Scoliosis), Poland
In Greece, many of the above methods are applied for the rehabilitation of IS. To our knowledge a specific questionnaire for PSSEs was not yet published. In this report a questionnaire is presented which evaluates the quality of life of children and adolescents with diagnosed IS, who are undergoing treatment with one of the above PSSEs methods.
2. Materials and Methods
2.1. The questionnaire
For the development of the PSSEQ (Physiotherapeutic Scoliosis Specific Exercises Questionnaire) we followed the recommended guidelines [18] for designing a questionnaire. It is based on a thorough literature review of the field of scoliosis and Physiotherapeutic Scoliosis Specific Exercises (PSSEs), which are approved by the SOSORT organization [4], as well as on our experience regarding the needs of scoliotic children and adolescent patients in specialized physiotherapeutic centers, in our country. Permission and approval for conducting the research was requested and provided by the ethical committee of the Medical Association of Piraeus. In addition, because participants were minors, consent for using their children’ data who participated in the study was provided by their parents.
The total number of the questions was chosen and categorized accordingly to the SOSORT guidelines and scientific articles of IS. The development of questions was carried out by the authors who subsequently divided the questionnaire into the following 8 domains: 1) physical functioning (questions number 1,5, 6, 20, 21, 23, 24, 25, 26, 34, 35, 40), 2), self-image (questions number 2, 47, 49, 50), 3) Physiotherapeutic Scoliosis-Specific Exercises (PSSEs) (questions number 3, 19, 27, 28, 32, 37, 38, 39), 4) psychosocial functioning (questions number 4, 7, 22, 29, 36, 41, 42, 44, 45, 46, 48, 51), 5) cognitive functioning (questions number 11,18, 30, 52,53), 6) compliance (questions number 8, 9, 10, 12, 13, 14, 15, 16), 7) motivation 17, 33) and 8) pain (questions number 31, 43).
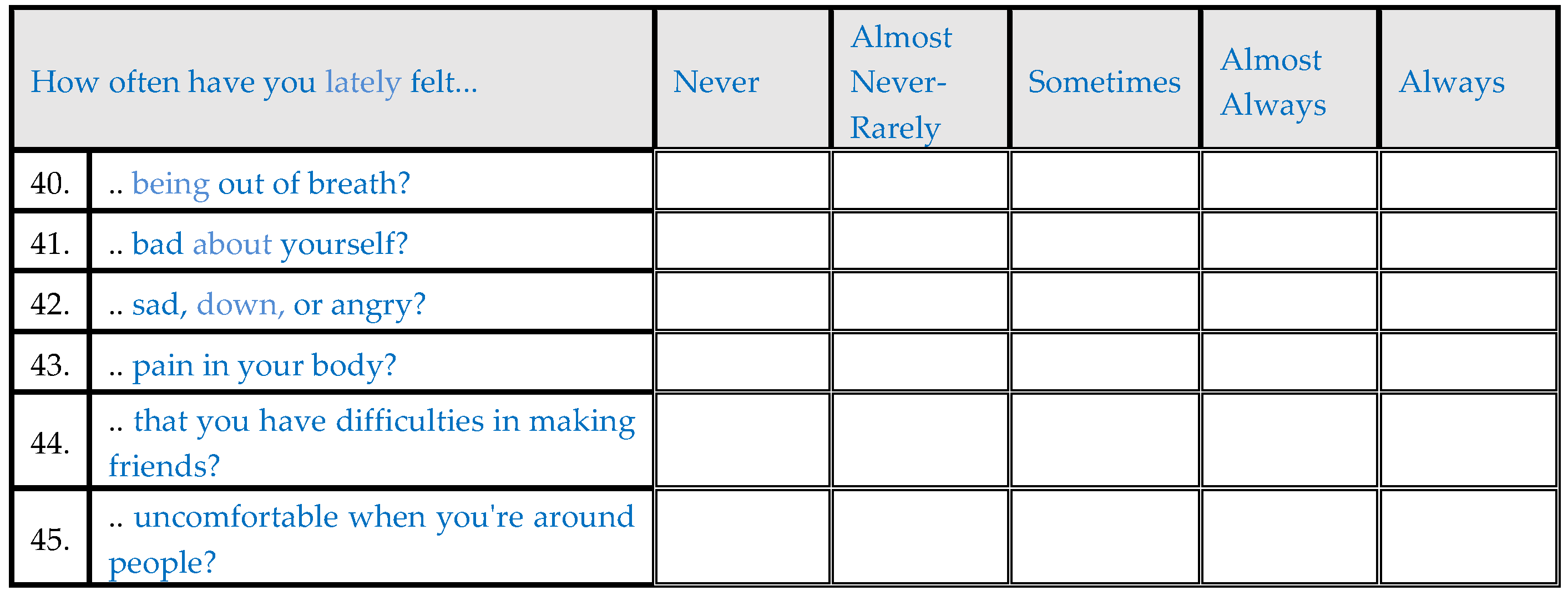
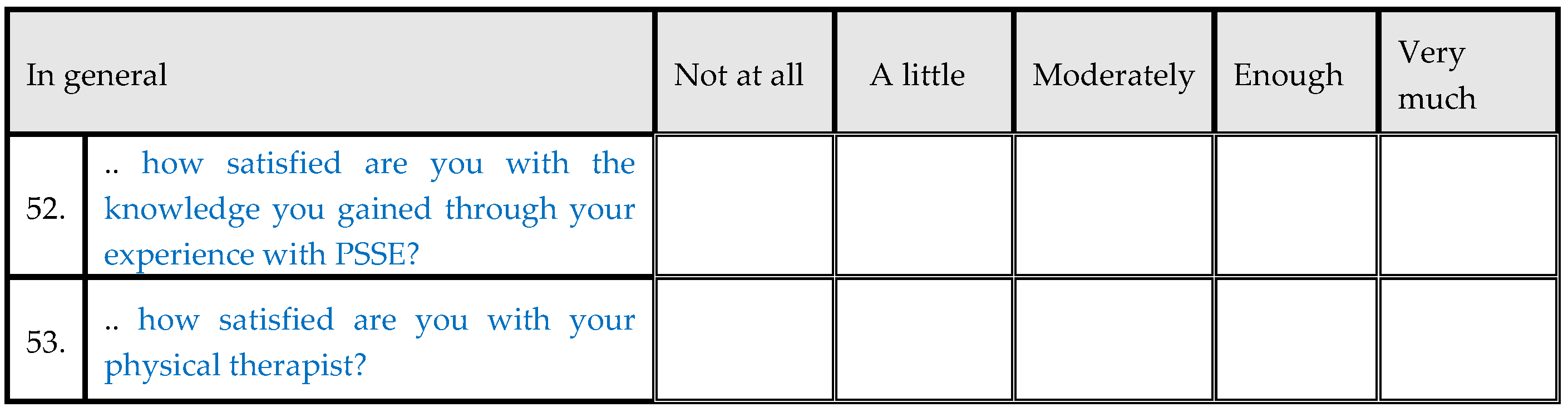
The questionnaire consists of 53 questions. There are 37 with positive meaning and 15 with negative meaning and one multiple choice question. Furthermore, 6 open-ended questions were included related to the PSSEs and the questionnaire. In the scored items, a Likert scale of 1 -5 was used. More specifically, responses 1-5 correspond to 5 = Strongly agree and 1 = Strongly disagree. An additional edit was made to the wording of the questions so that they could correspond meaningfully to these responses.
The first sheet of the questionnaire includes questions about: date of data collection, demographic characteristics, first name and surname, father’s and mother’s names, gender, date of birth, address, contact details, height and weight in kilos to calculate BMI, right or left handedness, date of menarche for females, hair and eye color and type of scoliosis. Data to be filled in by the researcher include Scoliometer angle, Cobb Angle, Risser sign, (Formetric - scoliosis angle), type of treatment (exercise or both exercise and bracing).
A pre-final PSSE questionnaire was developed and pilot study was conducted, which was completed by 16 participants with AIS. We asked the 16 participants to complete this questionnaire so that we could calculate Cronbach’s Alpha based on the results in their responses. The total sample responses to the questions were entered in SPSS and for each domain, the minimum and maximum effect (floor & ceiling effect), defined as the percentage of participants showing the minimum and maximum possible scores, respectively, were calculated. Results at the minimum and maximum effect exceeding 15% which were considered statistically significant. The floor effect was 53/265 and the ceiling effect was 265/265, respectively. Cronbach’s Alpha was calculated >0.7, which is considered a strong correlation-standard deviation result between responses. Internal consistency of the questionnaire was evaluated by calculating the Cronbach’s Alpha. The initial number of questions was 64, thus, 11 were excluded from the study or combined with the existing just to because more specific and easier for the objects to understand them. Thus the final PSSE questionnaire consists of 53 questions, and 6 “open” questions, see Appendix. The original questionnaire for PSSEs was developed in Greek language and were coined QPSSE.
2.2. Study Population
The inclusion criteria for participating in this study are the following: 1) Patients should be from 10 to 18 years old, 2) Patients should have been diagnosed with mild or moderate AIS, 3) Patients should be able to speak and read in Greek and 4) Patients should be undergoing or have undergone in the past Physiotherapeutic Scoliosis Specific Exercises (PSSE) for a period of at least 2 months.
The exclusion criteria were mental health problems, low level of communication, congenital, neurological or other type of scoliosis, and/or having had surgery for scoliosis.
2.3. Psychometric evaluation
The PSSE questionnaire was evaluated for the following psychometrics: reliability, validity, floor and ceiling effects. Reliability was assessed by analyzing internal consistency and test- retest reliability. Internal consistency was determined by the Cronbach’s Alpha. Intraclass Correlation Coefficient (ICC) was calculated to measure the test- retest reliability. The patients completed the questionnaire twice at an interval of 4-7 days for measuring of test- retest reliability. Convergent validity was compared against the critical value of Pearson’s correlation. Divergent validity was evaluated by analyzing the answers of the patients of the PSSEQ and their characteristics (e.g. Risser sign, Formetric, Cobb angle, gender etc.) using Pearson’s or Spearman correlation coefficient. The IBM SPSS software was used for the statistical analysis.
2.4. Materials
2.4.1. Scoliometer measurement (ATR)
Using a scoliometer the angle of trunk rotation (ATR) was assessed [15].
2.4.2. Formetric 4D-DIERS
The Formetric 4D DIERS is a scanning system with a light projector which scans the back of the patient. This system is connected with a computer that analyzes the data and provides information about the posture of the body, the spinal curves (frontal, lateral), pelvic position, vertebral rotation and muscle imbalance [16].
2.4.3. BMI
Body mass index (BMI) is a method that calculates body fat according to height and weight in females or males. A normal BMI range is between 18,5 to 24,9 [19].
2.4.4. Cobb angle
The Cobb angle measurement is used for calculating of spine curvatures in frontal plane. A radiograph is necessary in order for the Cobb angle to be measured. This method is used so as to determine the upper/lower end vertebras (UEV/LEV) on the radiograph, then, a vertical line respectively at the upper/lower end vertebra endplate lines is necessary (UEVEL/LEVEL), and the included angle of the two vertical lines is the Cobb angle [20].
2.4.5. Risser sign
Risser sign is used by clinicians in order to assess the skeletal maturity of a human. Risser sign is determined by the iliac apophysis from radiographs and is classified in 6 stages (0-5 Risser). It is often used for the evaluation of adolescent idiopathic scoliosis and for the selection of their treatment [21].
2.4.6. Demographics
Demographics are characteristics of a population and are often evaluated for statistical analysis. Some of them are age, gender, ethnicity, education, geographic location etc. In this study, age, gender and colour of hair and eyes were used in statistical analysis.
3. Results
Time needed to complete the PSSEQ was about 10-11 minutes.
80 patients were included in the study and 21 tests- retests were completed in a period of 14months.
3.1. Descriptive statistics
Descriptive statistics
| Mean | Standard Deviation | ||
| Age(yrs) | 16.5 | 7.1 | |
| BMI (Kg/m2) | 19.89 | 2.75 | |
| Cobb Angle (degrees) | 36.1 | 4.08 | |
| Risser sign | 4.6 | 1.6 | |
| Age at menarche | 12.1 | 1.1 | |
| Count | Column N % | ||
| Menarche | No | 12 | 18.2% |
| Yes | 54 | 81.8% | |
| Sex | Male | 11 | 13.8% |
| Female | 69 | 86.3% | |
| Brace | No | 19 | 25.0% |
| Yes | 57 | 75.0% | |
| Dominant hand | Right | 67 | 88.2% |
| Left | 9 | 11.8% | |
| In general how would you describe the state of your physical health? | Not good at all | 1 | 1.3% |
| Somewhatgood | 1 | 1.3% | |
| Moderately good | 20 | 25.0% | |
| Quite good | 41 | 51.3% | |
| Very good | 17 | 21.3% | |
| In general how would you rate your appearance? | Not good at all | 0 | 0.0% |
| Somewhatgood | 2 | 2.5% | |
| Moderately good | 17 | 21.3% | |
| Quite good | 39 | 48.8% | |
| Very good | 22 | 27.5% | |
| In general how would you describe your experience with PSSE? | Not good at all | 0 | 0.0% |
| Somewhatgood | 1 | 1.3% | |
| Moderately good | 11 | 13.8% | |
| Quite good | 42 | 52.5% | |
| Very good | 26 | 32.5% | |
| In general how would you describe your mental health? | Not good at all | 0 | 0.0% |
| Somewhatgood | 3 | 3.8% | |
| Moderately good | 11 | 13.8% | |
| Quite good | 40 | 50.0% | |
| Very good | 26 | 32.5% | |
| In general how would you rate your posture during the day? | Not good at all | 2 | 2.5% |
| Somewhatgood | 5 | 6.3% | |
| Moderately good | 29 | 36.3% | |
| Quite good | 36 | 45.0% | |
| Very good | 8 | 10.0% | |
| In general how would you rate your endurance? | Not good at all | 3 | 3.8% |
| Somewhatgood | 6 | 7.5% | |
| Moderately good | 13 | 16.3% | |
| Quite good | 26 | 32.5% | |
| Very good | 32 | 40.0% | |
| In general how would you describe your relationship with the people close to you? | Not good at all | 0 | 0.0% |
| Somewhatgood | 0 | 0.0% | |
| Moderately good | 5 | 6.3% | |
| Quite good | 17 | 21.3% | |
| Very good | 58 | 72.5% | |
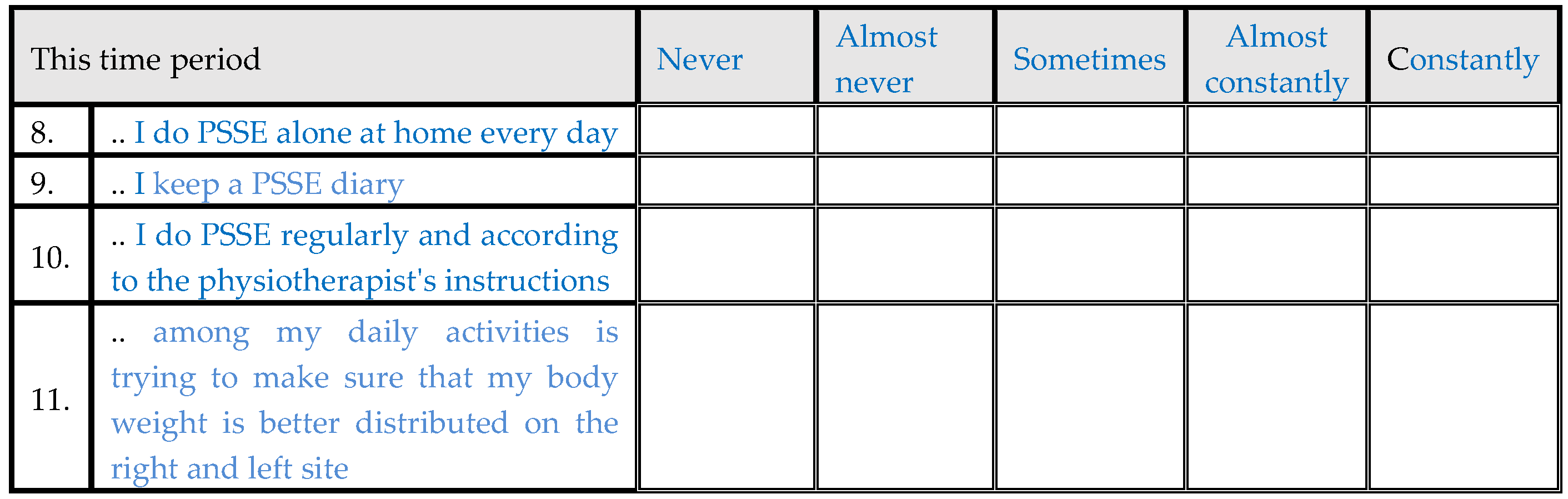
| This time period I do PSSE alone at home every day | Never | 1 | 1.3% |
| Almost never | 5 | 6.3% | |
| Sometimes | 28 | 35.0% | |
| Almost constantly | 32 | 40.0% | |
| Constantly | 14 | 17.5% | |
| This time period I keep a PSSE diary | Never | 51 | 63.8% |
| Almost never | 10 | 12.5% | |
| Sometimes | 7 | 8.8% | |
| Almost constantly | 5 | 6.3% | |
| Constantly | 7 | 8.8% | |
| This time period I do PSSE regularly and according to the physiotherapist's instructions | Never | 3 | 3.8% |
| Almost never | 1 | 1.3% | |
| Sometimes | 22 | 27.5% | |
| Almost constantly | 26 | 32.5% | |
| Constantly | 28 | 35.0% | |
| This time period among my daily activities is trying to make sure that my body weight is better distributed on the right and left site | Never | 2 | 2.5% |
| Almost never | 6 | 7.5% | |
| Sometimes | 29 | 36.3% | |
| Almost constantly | 39 | 48.8% | |
| Constantly | 4 | 5.0% | |
| I will do PSSE at home even if I’m tired | Not true at all | 6 | 7.5% |
| Somewhat true | 16 | 20.0% | |
| Almost true | 17 | 21.3% | |
| True enough | 31 | 38.8% | |
| Absolutely true | 10 | 12.5% | |
| I will do PSSE at home even if I’m in a bad mood | Not true at all | 10 | 12.5% |
| Somewhat true | 14 | 17.5% | |
| Almost true | 19 | 23.8% | |
| True enough | 22 | 27.5% | |
| Absolutely true | 15 | 18.8% | |
| I will do PSSE at home even if I don’t have time | Not true at all | 12 | 15.0% |
| Somewhat true | 26 | 32.5% | |
| Almost true | 23 | 28.8% | |
| True enough | 14 | 17.5% | |
| Absolutely true | 5 | 6.3% | |
| I will do PSSE at home even if I’m on vacation | Not true at all | 27 | 33.8% |
| Somewhat true | 19 | 23.8% | |
| Almost true | 16 | 20.0% | |
| True enough | 11 | 13.8% | |
| Absolutely true | 7 | 8.8% | |
| I will do PSSE at home even if the physiotherapist is not with me | Not true at all | 6 | 7.5% |
| Somewhat true | 8 | 10.0% | |
| Almost true | 15 | 18.8% | |
| True enough | 18 | 22.5% | |
| Absolutely true | 33 | 41.3% | |
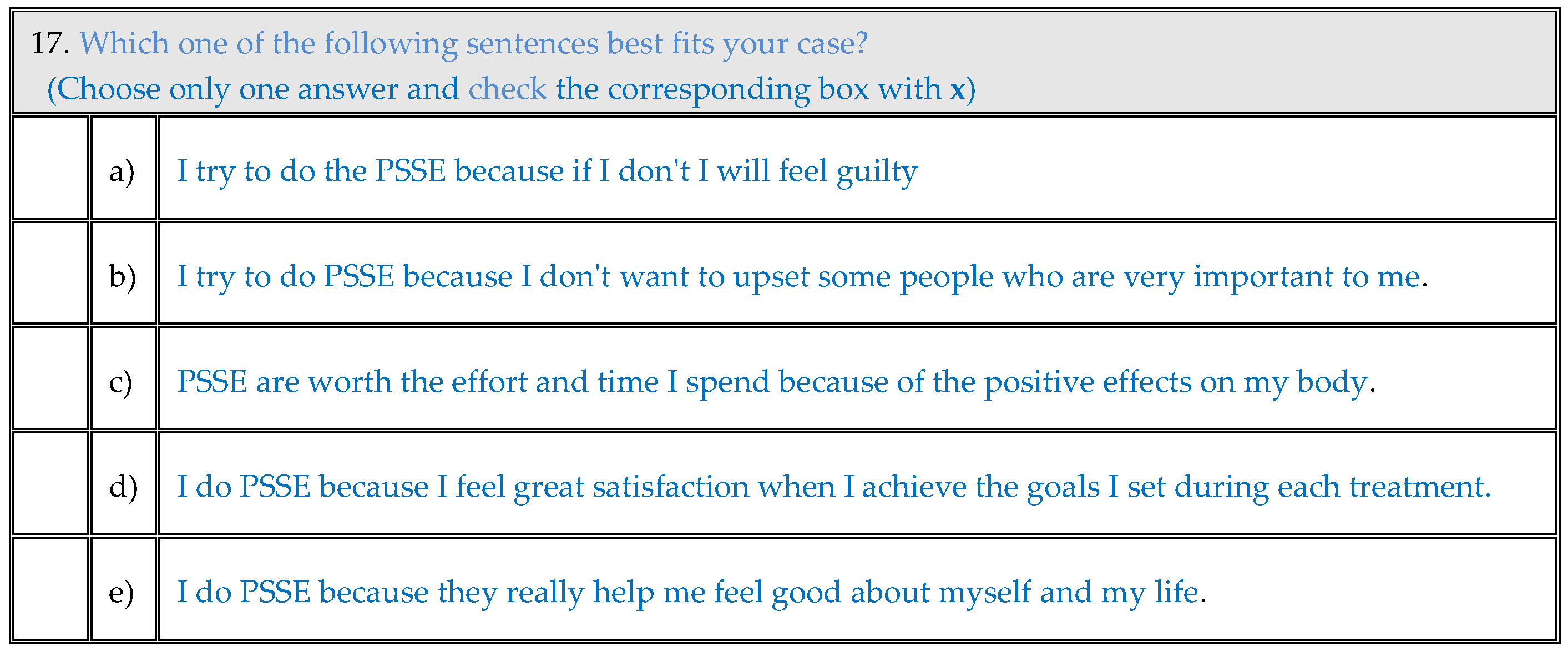
| Motivation | I try to do the PSSE because if I don't I will feel guilty | 4 | 5.0% |
| I try to do PSSE because I don't want to upset some people who are very important to me. | 16 | 20.0% | |
| PSSE are worth the effort and time I spend because of the positive effects on my body. | 37 | 46.3% | |
| I do PSSE because I feel great satisfaction when I achieve the goals I set during each treatment. | 14 | 17.5% | |
| I do PSSE because they really help me feel good about myself and my life. | 9 | 11.3% | |
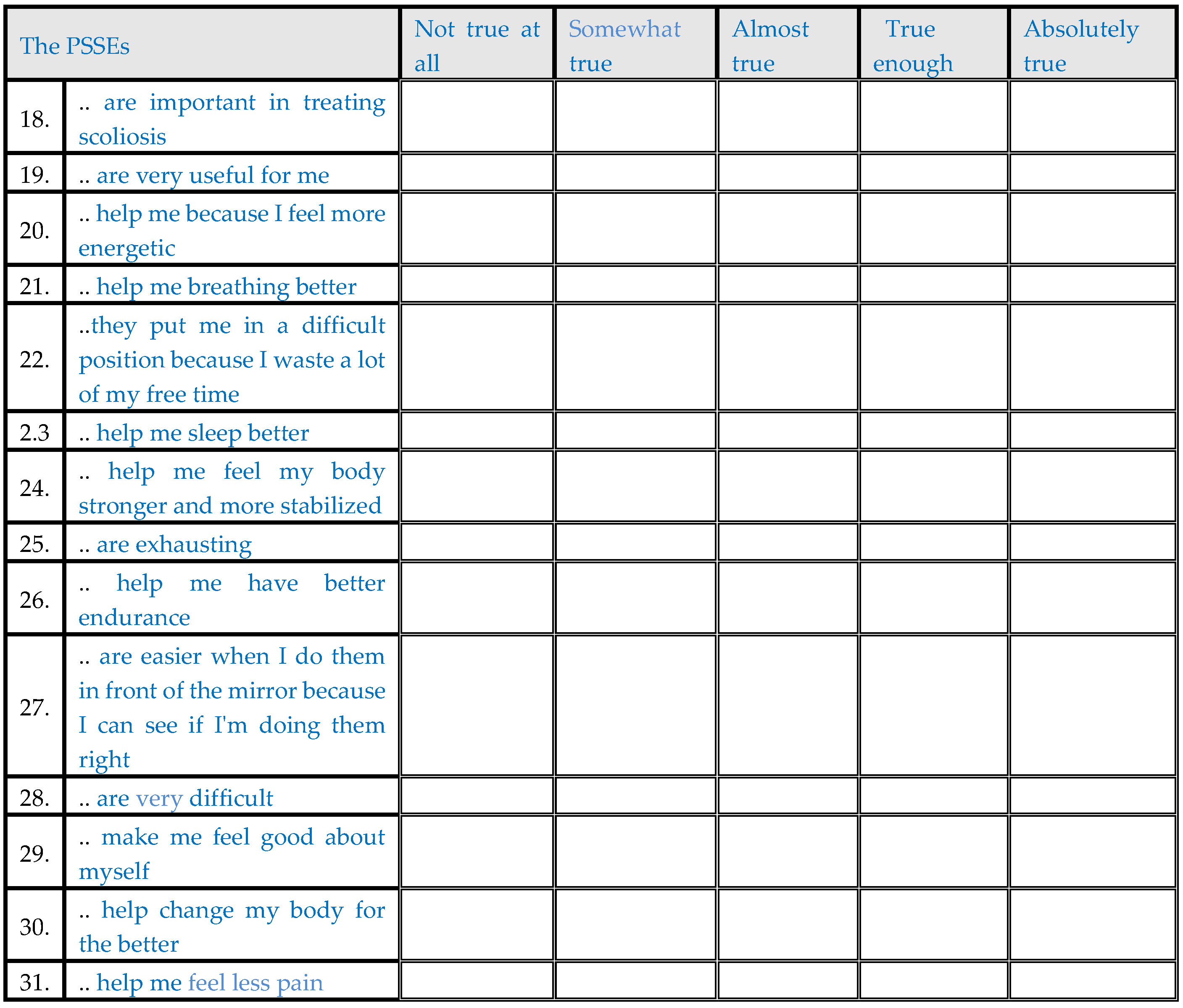
| The PSSEs are important in treating scoliosis | Not true at all | 0 | 0.0% |
| Somewhat true | 0 | 0.0% | |
| Almost true | 6 | 7.5% | |
| True enough | 29 | 36.3% | |
| Absolutely true | 45 | 56.3% | |
| The PSSEs are very useful for me | Not true at all | 0 | 0.0% |
| Somewhat true | 0 | 0.0% | |
| Almost true | 13 | 16.3% | |
| True enough | 33 | 41.3% | |
| Absolutely true | 34 | 42.5% | |
| The PSSEs help me because I feel more energetic | Not true at all | 10 | 12.5% |
| Somewhat true | 10 | 12.5% | |
| Almost true | 26 | 32.5% | |
| True enough | 21 | 26.3% | |
| Absolutely true | 13 | 16.3% | |
| The PSSEs help me breathing better | Not true at all | 10 | 12.5% |
| Somewhat true | 12 | 15.0% | |
| Almost true | 24 | 30.0% | |
| True enough | 23 | 28.8% | |
| Absolutely true | 11 | 13.8% | |
| The PSSEs put me in a difficult position because I waste a lot of my free time | Absolutely true | 12 | 15.0% |
| True enough | 27 | 33.8% | |
| Almost true | 12 | 15.0% | |
| Somewhat true | 16 | 20.0% | |
| Not true at all | 13 | 16.3% | |
| The PSSEs help me sleep better | Not true at all | 18 | 22.5% |
| Somewhat true | 23 | 28.8% | |
| Almost true | 29 | 36.3% | |
| True enough | 7 | 8.8% | |
| Absolutely true | 3 | 3.8% | |
| The PSSEs help me feel my body stronger and more stabilized | Not true at all | 5 | 6.3% |
| Somewhat true | 4 | 5.0% | |
| Almost true | 17 | 21.3% | |
| True enough | 36 | 45.0% | |
| Absolutely true | 18 | 22.5% | |
| The PSSEs are exhausting | Absolutely true | 10 | 12.5% |
| True enough | 9 | 11.3% | |
| Almost true | 21 | 26.3% | |
| Somewhat true | 25 | 31.3% | |
| Not true at all | 15 | 18.8% | |
| The PSSEs help me have better endurance | Not true at all | 5 | 6.3% |
| Somewhat true | 11 | 13.8% | |
| Almost true | 30 | 37.5% | |
| True enough | 26 | 32.5% | |
| Absolutely true | 8 | 10.0% | |
| The PSSEs are easier when I do them in front of the mirror because I can see if I'm doing them right | Not true at all | 0 | 0.0% |
| Somewhat true | 1 | 1.3% | |
| Almost true | 9 | 11.3% | |
| True enough | 29 | 36.3% | |
| Absolutely true | 41 | 51.3% | |
| The PSSEs are very difficult | Absolutely true | 10 | 12.5% |
| True enough | 9 | 11.3% | |
| Almost true | 28 | 35.0% | |
| Somewhat true | 16 | 20.0% | |
| Not true at all | 17 | 21.3% | |
| The PSSEs make me feel good about myself | Not true at all | 3 | 3.8% |
| Somewhat true | 6 | 7.5% | |
| Almost true | 22 | 27.5% | |
| True enough | 35 | 43.8% | |
| Absolutely true | 14 | 17.5% | |
| The PSSEs help change my body for the better | Not true at all | 0 | 0.0% |
| Somewhat true | 2 | 2.5% | |
| Almost true | 7 | 8.8% | |
| True enough | 29 | 36.3% | |
| Absolutely true | 42 | 52.5% | |
| The PSSEs help me feel less pain | Not true at all | 13 | 16.3% |
| Somewhat true | 19 | 23.8% | |
| Almost true | 15 | 18.8% | |
| True enough | 13 | 16.3% | |
| Absolutely true | 20 | 25.0% | |
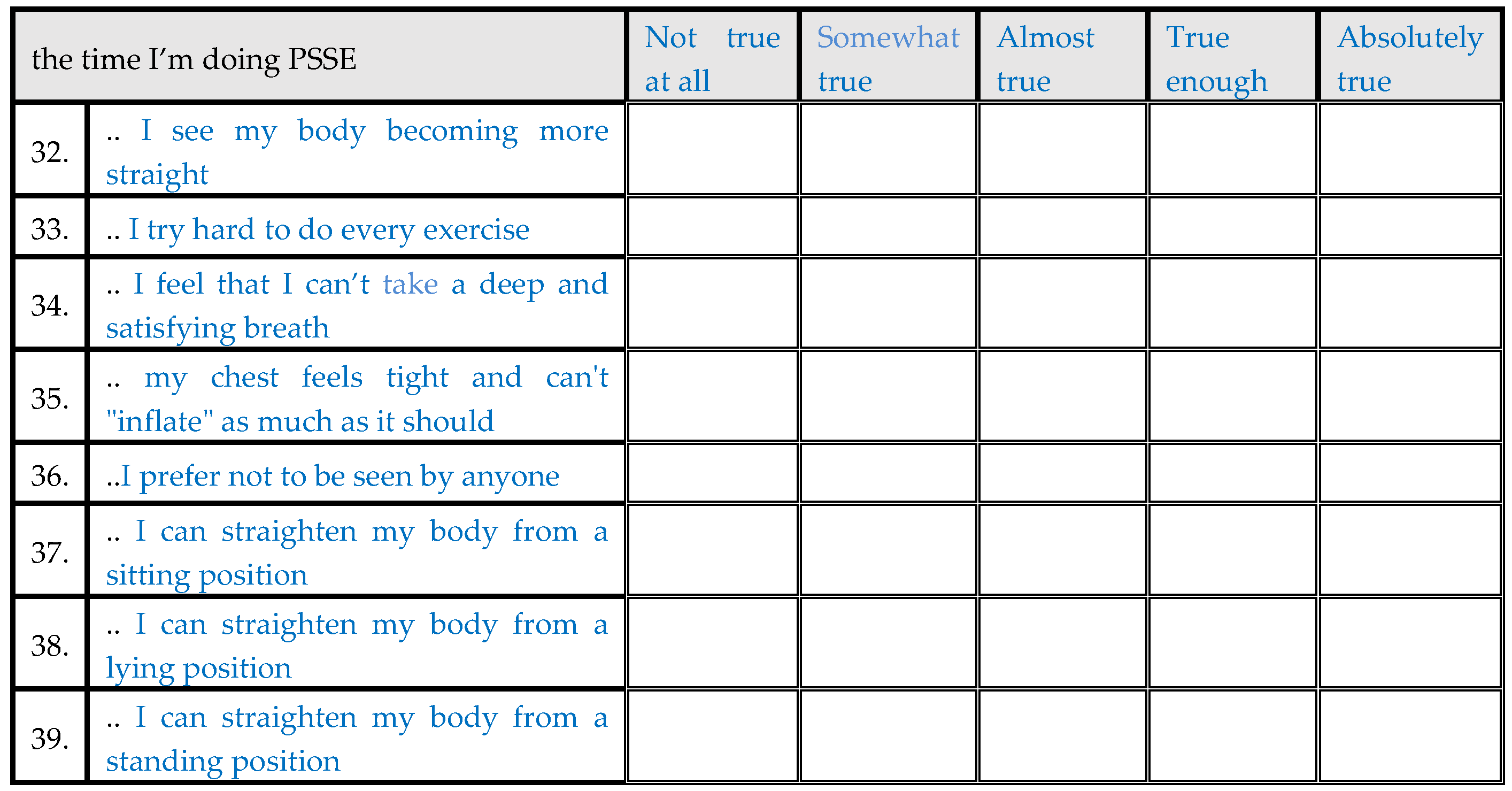
| The time I’m doing PSSEs I see my body becoming more straight | Not true at all | 0 | 0.0% |
| Somewhat true | 0 | 0.0% | |
| Almost true | 12 | 15.0% | |
| True enough | 37 | 46.3% | |
| Absolutely true | 31 | 38.8% | |
| The time I’m doing PSSEs I try hard to do every exercise | Not true at all | 2 | 2.5% |
| Somewhat true | 6 | 7.5% | |
| Almost true | 16 | 20.0% | |
| True enough | 31 | 38.8% | |
| Absolutely true | 25 | 31.3% | |
| The time I’m doing PSSEs I feel that I can’t take a deep and satisfying breath | Absolutely true | 19 | 23.8% |
| True enough | 22 | 27.5% | |
| Almost true | 11 | 13.8% | |
| Somewhat true | 11 | 13.8% | |
| Not true at all | 17 | 21.3% | |
| The time I’m doing PSSE my chest feels tight and can't "inflate" as much as it should | Absolutely true | 25 | 31.3% |
| True enough | 14 | 17.5% | |
| Almost true | 12 | 15.0% | |
| Somewhat true | 13 | 16.3% | |
| Not true at all | 16 | 20.0% | |
| The time I’m doing PSSE I prefer not to be seen by anyone | Absolutely true | 24 | 30.0% |
| True enough | 16 | 20.0% | |
| Almost true | 9 | 11.3% | |
| Somewhat true | 16 | 20.0% | |
| Not true at all | 15 | 18.8% | |
| The time I’m doing PSSE I can straighten my body from a sitting position | Not true at all | 0 | 0.0% |
| Somewhat true | 6 | 7.5% | |
| Almost true | 10 | 12.5% | |
| True enough | 26 | 32.5% | |
| Absolutely true | 38 | 47.5% | |
| The time I’m doing PSSE I can straighten my body from a lying position | Not true at all | 5 | 6.3% |
| Somewhat true | 8 | 10.0% | |
| Almost true | 9 | 11.3% | |
| True enough | 34 | 42.5% | |
| Absolutely true | 24 | 30.0% | |
| The time I’m doing PSSE I can straighten my body from a standing position | Not true at all | 2 | 2.5% |
| Somewhat true | 10 | 12.5% | |
| Almost true | 16 | 20.0% | |
| True enough | 22 | 27.5% | |
| Absolutely true | 30 | 37.5% | |
| How often have you felt being out of breath lately ? | Always | 26 | 32.5% |
| Almost always | 22 | 27.5% | |
| Sometimes | 12 | 15.0% | |
| Almost never | 6 | 7.5% | |
| Never | 14 | 17.5% | |
| How often have you lately felt bad about yourself? | Always | 15 | 18.8% |
| Almost always | 22 | 27.5% | |
| Sometimes | 26 | 32.5% | |
| Almost never | 4 | 5.0% | |
| Never | 13 | 16.3% | |
| How often have you lately felt sad, down, or angry? | Always | 5 | 6.3% |
| Almost always | 21 | 26.3% | |
| Sometimes | 41 | 51.3% | |
| Almost never | 7 | 8.8% | |
| Never | 6 | 7.5% | |
| How often have you lately felt pain in your body? | Always | 15 | 18.8% |
| Almost always | 20 | 25.0% | |
| Sometimes | 22 | 27.5% | |
| Almost never | 14 | 17.5% | |
| Never | 9 | 11.3% | |
| How often have you lately felt that you have difficulties in making friends? | Always | 25 | 31.3% |
| Almost always | 19 | 23.8% | |
| Sometimes | 12 | 15.0% | |
| Almost never | 5 | 6.3% | |
| Never | 19 | 23.8% | |
| How often have you lately felt uncomfortable when you're around people? | Always | 15 | 18.8% |
| Almost always | 28 | 35.0% | |
| Sometimes | 13 | 16.3% | |
| Almost never | 13 | 16.3% | |
| Never | 11 | 13.8% | |
| It is true for me that I find it hard to open up to someone, especially as long as I've been dealing with PSSEs | Strongly agree | 25 | 31.3% |
| Agree | 21 | 26.3% | |
| Neutral | 12 | 15.0% | |
| Disagree | 5 | 6.3% | |
| Strongly disagree | 17 | 21.3% | |
| It is true for me that I am not ashamed to do the PSSEs in front of people I consider close to me | Strongly disagree | 3 | 3.8% |
| Disagree | 8 | 10.0% | |
| Neutral | 9 | 11.3% | |
| Agree | 16 | 20.0% | |
| Strongly agree | 44 | 55.0% | |
| It is true for me that my physical therapist is very friendly and supportive | Strongly disagree | 0 | 0.0% |
| Disagree | 1 | 1.3% | |
| Neutral | 2 | 2.5% | |
| Agree | 17 | 21.3% | |
| Strongly agree | 60 | 75.0% | |
| It is true for me that my body’s curve is too obvious to others | Strongly agree | 12 | 15.0% |
| Agree | 9 | 11.3% | |
| Neutral | 27 | 33.8% | |
| Disagree | 20 | 25.0% | |
| Strongly disagree | 12 | 15.0% | |
| It is true that when I meet someone I worry about what they think about my appearance | Strongly agree | 16 | 20.0% |
| Agree | 8 | 10.0% | |
| Neutral | 27 | 33.8% | |
| Disagree | 18 | 22.5% | |
| Strongly disagree | 11 | 13.8% | |
| It is true for me that it doesn't matter how someone looks like | Strongly disagree | 5 | 6.3% |
| Disagree | 9 | 11.3% | |
| Neutral | 12 | 15.0% | |
| Agree | 32 | 40.0% | |
| Strongly agree | 22 | 27.5% | |
| In general how satisfied are you with the knowledge you gained through your experience with PSSE? | Not at all | 0 | 0.0% |
| A little | 0 | 0.0% | |
| Modarately | 10 | 12.5% | |
| Enough | 46 | 57.5% | |
| Very much | 24 | 30.0% | |
| In general how satisfied are you with your physical therapist? | Not at all | 1 | 1.3% |
| A little | 0 | 0.0% | |
| Modarately | 3 | 3.8% | |
| Enough | 16 | 20.0% | |
| Very much | 60 | 75.0% |
3.1. Statistical analysis
Based on Kolmogorov-Smirnov goodness-of-fit test and Shapiro-Wilk test for normality, data sis not follow the normal distribution; therefore, non-parametric tests were used for the statistical analysis. Pearson's correlation coefficient was used for all correlations evaluated. P values of less than 0.05 were considered to be significant. Internal consistency was evaluated by Cronbach's alpha method. Although there were very few missing values, accounting for 0.78% of the total values of the questionnaire, expectation maximization likelihood algorithm was used to impute data. IBM® SPSS® Statistics Software v.25 was used for the analysis.
3.2. Factor analysis
The results of the content validity analysis demonstrated excellent reliability and content validity for the questionnaire, as summarized in Table 1.
3.3. Internal consistency reliability
Cronbach's alpha coefficients for the overall score was 0.84, exceeding the minimum recommended standard of 0.70 and indicating satisfactory internal consistency.
3.4. Item convergent validity
The criterion for item convergent validity was the correlation coefficient of each item of each domain with the domain scale variable. This value was compared against the critical value of Pearson’s r equal to 0.219, taking into account 78 degrees of freedom for each comparison with a p<0.05.
3.5. Item divergent validity
The criterion for item divergent validity was the correlation coefficient of each domain scale variable and the clinical continuous variables (age, BMI, Cobb angle). Except for the pain domain variable that was positively correlated with age, there was no other significant correlation found between the aforementioned variables, indicating the lack of relationship of the 53 measurements of the questionnaire with the clinical data.
3.6. Test-Retest Reliability
Test-retest reliability was assessed using Pearson’s correlation coefficient r. 22 subjects were re-evaluated one week after the first interview. The results of the questionnaire were used for 53 discrete bivariate correlations, one for each variable of the questionnaire. The results showed that there was perfect test-retest reliability in terms of achieving r values equal to 1 in all correlations.
3.7. Floor and ceiling effects for the overall score
For the overall score, in the present study, 0 % of patients scored at floor and 0% scored at ceiling. Therefore, there were no floor or ceiling effects for the overall score. Floor and ceiling effects for each domain of the are shown in Table 1 Floor and ceiling effects for each item are shown in Table 2
4. Discussion
The aim of this study is to develop a questionnaire that evaluates the quality of life in Greek population with idiopathic scoliosis, who are undergoing Physiotherapeutic Specific Exercises for Scoliosis (PSSE) and the evaluation of its psychometrics. To our knowledge, no questionnaire evaluating patients undergone PSSEs has been developed to date. The QPSSE was created in order to determine how various aspects of conservative treatment, PSSEs, influence patients with AIS. A final 53-item questionnaire was developed with 8 domains. The 8 domains of the final questionnaire were as follows: 1) physical functioning, 2) self-image, 3) Physiotherapeutic scoliosis-specific exercises (PSSEs), 4) psychosocial functioning, 5) cognitive functioning, 6) compliance, 7) motivation and 8) pain.
Previous studies have developed other questionnaires that evaluate similar aspects of patients with AIS after other treatments, either conservative or surgical. One questionnaire that evaluates the quality of life in AIS is the 22 revised questionnaire of SRS (SRS-22R) that evaluates quality of life in AIS, especially after surgery treatment [22]. Another one is the Brace questionnaire (BrQ) that evaluates quality of life in populations with IS treated with brace [23]. Also, Short-Form Health Survey 36 (SF-36) or Short-form Health Survey (SF-12) that evaluate the Health-Related Quality of Life (HRQoL) [24,25] and Spinal appearance questionnaire (SAQ) aim to assess self-image in patients with AIS [26].
SRS-22-R is one of the most frequently used questionnaires in patients with scoliosis and includes 22 items that are divided in five domains: Pain, Self-Image, Function, Mental Health and Satisfaction with Management [27]. QPSSE was divided into eight domains. Some of them were, also, pain, self-image and psychosocial functioning. As it was mentioned before, SRS-22R was mainly intended for patients with AIS treated with surgery. However, to date, no questionnaires have been developed to evaluate the quality of life in AIS patients, so SRS-22R was often used for evaluating general quality of life in these patients regardless of their treatment.
BrQ is a self-administrated questionnaire that evaluates the quality of life in patients with AIS who are treated with brace. There is a 34-item Likert scale that consists of eight domains such as QPSSE: general health perception, physical functioning (physical functioning, also, in QPSSE), emotional functioning (psychosocial functioning in QPSSE), self-esteem and aesthetics (self-image in QPSSE), vitality (motivation QPSSE), school activity, bodily pain (pain in QPSSE) and social functioning (psychosocial functioning in QPSSE) [23].
SF-36 is a 36-item self-reported and one of the most widely used Health Related Quality of Life questionnaire. It is divided into eight sections: 1) vitality or energy (motivation in QPSSE), 2) physical functioning (also in QPSSE), 3) bodily pain (also in QPSSE), 4) general health perceptions, 5) physical role functioning, 6) emotional role functioning, 7) social role functioning (psychosocial functioning in QPSSE), 8) mental health or emotional wellbeing (cognitive functioning in QPSSE). SF-12 is a smaller version of SF-36. These questionnaires have also been used in patients with AIS in order to evaluate their general quality of life [24,25].
The 32-item SAQ is a questionnaire based on Walter Reed Visual Assessment Scale (WRVAS) and it evaluates AIS patients’ perception of spinal appearance. After validation, a 20- item SAQ was developed divided into 9 domains, and three textual items about the most distressing aspects of deformity. The items of SAQ are divided into the following domains: General (3 items), Curve (1), Prominence (2), Trunk shift (2), Waist (3), Shoulders (2), Kyphosis (1), Chest (2), Surgical Scar (1) and extra three textual questions as it was mentioned. The SAQ has been widely used and culturally adapted into many languages for the assessment of the appearance in patients with AIS. The original Greek- QPSSE (has) also includes a domain about AIS patients’ self-image (4 items) [28,28].
The PSSEQ results showed that there was perfect test-retest reliability in terms of achieving r values equal to 1 in all correlations and an overall score for internal consistency on 0.84, exceeding the minimum recommended standard of 0.70 and indicating satisfactory internal consistency. The Greek version of SRS-22 was shown to have three domains with very satisfactory Cronbach’s α (pain 0.85; mental health 0.87; self-image 0.83) and for two domains (function/activity 0.72 and satisfaction 0.67) were good. Intraclass correlation coefficient (ICC) was> 0.70, demonstrating very satisfactory or excellent test/retest reliability [27]. The initial Greek BrQ was shown to have satisfactory internal consistency with Cronbach’s alpha 0,82 [23]. The Greek version of SF-36 was found to have Cronbach’s α >0.70 [29]. The original English SAQ had good to excellent reliability (Spearman’s rho, 0.57–0.99) and high internal scale consistency (Cronbach’s alpha> 0.7) [26].
Divergent validity in QPSSE was found with no other significant correlation between the aforementioned variables, indicating the lack of relationship of the 53 measurements of the questionnaire with the clinical data. Concurrent validity of SRS-22 was evaluated by its correlation with SF-36 domains analyzing Pearson Correlation Coefficients and all correlations were found to be statistically significant [27]. Other cultural adaptations of SAQ evaluated convergent validity by correlating SAQ with appearance domain of SRS-22R and divergent validity by correlating patients’ answers in SAQ with their characteristics demonstrating good to excellent results [28,30,31,32,33] as in this study of the original Greek QPSSE.
The original Greek version of QPSSE showed similar results with the Greek versions or other studies of SRS-22, BrQ, SF-36 or SF-12 and SAQ. All these questionnaires evaluate the quality of life in AIS patients generally or after a treatment or assess in general Health Related Quality of Life. Our study assessed the intervention after Physiotherapeutic Scoliosis-Specific Exercises, BrQ after bracing and SRS-22 especially after surgery. However, further study of the QPSSE is needed in order to evaluate more psychometric properties, such as convergent validity or responsiveness. These tests would be necessary so as to develop if the PSSQ is responsive to changes. In order to assess convergent validity, it would be essential for other similar questionnaires or tools about the PSSEs and quality of life to be developed. Furthermore, a further study with a greater number of participants would potentially how better results in psychometrics in a questionnaire evaluating the quality of life in Greek population in AIS.
This questionnaire is a significant tool for the clinicians and physical therapists who work using PSSEs for adolescents with IS, in order to evaluate their patients’ quality of life and interventions after exercises. This tool will provide clinicians with information about AIS Greek patients so as to improve or change something in their treatment or intervention. It would be essential for this questionnaire to be translated in other languages too, so that other countries could have a tool available for evaluation of quality of life in patients who undergo PSSEs.
Conclusions
In conclusion, the PSSE questionnaire was found to be reliable and valid for clinical use in patients with AIS treated conservatively with PSSEs or both PSSEs and brace for Greek population.
Author Contributions
TBG conceptualization, literature search, editing the original draft preparation, DD review, literature search, SAF literature search, writing, AK data collection, KM review, writing, KM statistical analysis, writing, MO literature search, writing, ET data collection, AMG review, editing the original draft preparation. All authors have read and agreed to the published version of the manuscript.
Funding
This research waived no external funding.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Piraeus Medical Association, (June 2023).”
Informed Consent Statement
“Informed consent was obtained from all subjects of age involved in the study excepted for minors according to the Hellenic legislation- (children or Adolescents) for whom informed consent statement was obtained from their parents.
Data Availability Statement
Data are available on demand.
Conflicts of Interest
The authors TBG, DD, SAF, AK, KM, AMG declare that they have no conflicts of interest concerning this article. KM Physiotherapist & Complementary Therapist (Acupuncture), Athens, Greece, MO Aenaon- physio, 17342 Athens, ET Athens Scoliosis- Spine Rehabilitation Clinic
Abbreviations
AIS = Adolescent Idiopathic Scoliosis; IS idiopathic scoliosis, ATR = Angle of Trunk Rotation; lIS = Infantile Idiopathic Scoliosis; IS = Idiopathic Scoliosis; JIS = Juvenile Idiopathic Scoliosis; PSSEs = Physiotherapeutic Scoliosis-Specific Exercises, TA = Truncal Asymmetry
Appendix A
QUESTIONNAIRE FOR PHYSIOTHERAPEUTIC SPECIFIC SCOLIOSIS EXERCISES (QPSSE)
(ATTENTION: this page is to be completed by the physiotherapist/health promoter and not by the child being examined)
- Date of filling in the questionnaire: ….. / ….. /2022
- Name: ……………………………………………
- Surname: ………………………………………………………
- Father’s Name: ……………………………….…....
- Sex: ………………………………………………
- Date of Birth: ………………….………………………………………………
- Address:……………………………………………………………….……………………………
- Contact phone number: …………………………………………………….
- Email: ……………………………….……………………………………………………………
- Height in cm: …………………………………..
- Weight in kg: ……………..……..……… BMI: ………….…………..
- Left-handed/Right-handed? ………………………………………………………………
- For girls: Exact date the menstruation cycle started: ………………………………………
- Hair color: …………………………………………………………………………………
- Eye color: ……………………………………………………………….…….………………
- Type of scoliosis: ……………………….…………………………………………
- Standing forward bend test- Scoliometer in degrees- Hump :
- scoliometer right………thoracic…….… thoracolumbar………… lumbar…….…
- scoliometer left …… thoracic…….… thoracolumbar ….… lumbar…......…
- Seated forward bend test - Scoliometer in degrees- Hump :
- scoliometer right:thoracis……… thoracolumbar…………… lumbar …...…
- scoliometer left: thoracic……… thoracolumbar…………… lumbar ….…
- Cobb Angle: ………………………...............................
- Risser Sign : ………………………………………………………….
- Formetric: (if there is any please attach it)
- Treatment (wearing brace?) ………………………………………
- Which method of Physiotherapeutic Specific Scoliosis Exercises is being used:
- …………………………………………………………………………………………………
- TEST-VALIDITY: RETEST: RESPONSIVENESS
- Clinic:
QUESTIONNAIRE FOR PHYSIOTHERAPEUTIC SPECIFIC SCOLIOSIS EXERCISES (PSSE)
Thank you for completing this questionnaire. In doing so please respond to the questions freely and truly for there are no right or wrong answers in the case of Physiotherapeutic Specific Scoliosis Exercises (PSSE).



- 54.
- What would you like to have been different in the whole experience you have had so far with PSSE?
- 55.
- How would you feel if you been told that you must continue PSSE until you reach adulthood?
- 56.
- What changes do you think would improve this questionnaire?
- 57.
- Have you felt this questionnaire was tiresome? (Please explain)
- 58.
- Would you rather not answer some of the questions? which ones? (Please write down the numbers of the questions)
- 59.
- Would you like to comment on anything else?
Thank you very much for your participation!
References
- Kikanloo SR, Tarpada SP, Cho W. Etiology of Adolescent Idiopathic Scoliosis: A Literature Review. Asian Spine Journal [Internet]. 2019 Jun 1;13(3):519–26. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6547389/.
- Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of Bracing in Adolescents with Idiopathic Scoliosis. New England Journal of Medicine. 2013 Oct 17;369(16):1512–21.
- Hawes MC, O’Brien JP. The transformation of spinal curvature into spinal deformity: pathological processes and implications for treatment. Scoliosis. 2006 Mar 31;1(1).
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders. 2018 Jan 10;13(1).
- Grossman TW, Mazur JM, Cummings RJ. An Evaluation of the Adams Forward Bend Test and the Scoliometer in a Scoliosis School Screening Setting. Journal of Pediatric Orthopaedics. 1995 Jul;15(4):535–8.
- Fabio Galbusera, Bassani T, Panico M, Luca Maria Sconfienza, Cina A. A fresh look at spinal alignment and deformities: Automated analysis of a large database of 9832 biplanar radiographs. Frontiers in Bioengineering and Biotechnology [Internet]. 2022 Jul 15 [cited 2023 Nov 16];10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9335010/.
- Choudhry MN, Ahmad Z, Verma R. Adolescent Idiopathic Scoliosis. The Open Orthopaedics Journal. 2016 May 30;10(1):143–54.
- Peng Y, Wang SR, Qiu GX, Zhang JG, Zhuang QY. Research progress on the etiology and pathogenesis of adolescent idiopathic scoliosis. Chinese Medical Journal [Internet]. 2020 Feb 20;133(4):483–93. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9335010/. 7046.
- Balagué F, Pellisé F. Adolescent idiopathic scoliosis and back pain. Scoliosis and Spinal Disorders. 2016 Sep 9;11(1).
- Théroux J, Le May S, Hebert JJ, Labelle H. Back Pain Prevalence Is Associated With Curve-type and Severity in Adolescents With Idiopathic Scoliosis. SPINE. 2017 Aug;42(15):E914–9.
- Kobayashi K, Ando K, Machino M, Tanaka S, Morozumi M, Kanbara S, et al. Trends in Medical Costs for Adolescent Idiopathic Scoliosis Surgery in Japan. Global Spine Journal. 2019 Oct 29;10(8):1040–5.
- Boylan MR, Riesgo AM, Chu A, Paulino CB, Feldman DS. Costs and complications of increased length of stay following adolescent idiopathic scoliosis surgery. Journal of Pediatric Orthopaedics B. 2019 Jan;28(1):27–31.
- Bettany-Saltikov J, Parent E, Romano M, Villagrasa M, Negrini S. Physiotherapeutic scoliosis-specific exercises for adolescents with idiopathic scoliosis. European Journal of Physical and Rehabilitation Medicine [Internet]. 2014 Feb 1;50(1):111–21. Available from: https://pubmed.ncbi.nlm.nih.gov/24525556/. 2452.
- Berdishevsky H, Lebel VA, Bettany-Saltikov J, Rigo M, Lebel A, Hennes A, et al. Physiotherapy scoliosis-specific exercises – a comprehensive review of seven major schools. Scoliosis and Spinal Disorders. 2016 Aug 4;11(1).
- Côté P, Kreitz BG, Cassidy JD, Dzus AK, Martel J. A study of the diagnostic accuracy and reliability of the Scoliometer and Adam’s forward bend test. Spine [Internet]. 1998;23(7):796–802; discussion 803. Available from: https://pubmed.ncbi.nlm.nih.gov/24525556/. 9563.
- Diers H, Mooshake S, Heitmann K. Dynamic 3D (4D) in objective classification of severe back deformities. Scoliosis. 2009 Dec;4(S2).
- Seleviciene V, Cesnaviciute A, Strukcinskiene B, Marcinowicz L, Strazdiene N, Genowska A. Physiotherapeutic Scoliosis-Specific Exercise Methodologies Used for Conservative Treatment of Adolescent Idiopathic Scoliosis, and Their Effectiveness: An Extended Literature Review of Current Research and Practice. International Journal of Environmental Research and Public Health. 2022 Jul 28;19(15):9240.
- Jenn, NC. Designing A Questionnaire. Malaysian family physician: the official journal of the Academy of Family Physicians of Malaysia [Internet]. 2006 Apr 30;1(1):32–5. Available from: https://www.ncbi.nlm.nih. 4797. [Google Scholar]
- Weir CB, Jan A. BMI Classification Percentile And Cut Off Points [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://pubmed.ncbi.nlm.nih. 3108.
- Wang J, Zhang J, Xu R, Chen TG, Zhou KS, Zhang HH. Measurement of scoliosis Cobb angle by end vertebra tilt angle method. Journal of Orthopaedic Surgery and Research. 2018 Sep 4;13(1).
- Subramanian S, Viswanathan VK. Bone Age [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih. 5370.
- Asher M, Min Lai S, Burton D, Manna B. The Reliability and Concurrent Validity of the Scoliosis Research Society-22 Patient Questionnaire for Idiopathic Scoliosis. Spine. 2003 Jan;28(1):63–9.
- Vasiliadis E, Grivas TB, Gkoltsiou K. Development and preliminary validation of Brace Questionnaire (BrQ): a new instrument for measuring quality of life of brace treated scoliotics. Scoliosis. 2006 May 20 ;1(1).
- Ware JE, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. Journal of Clinical Epidemiology. 1998 Nov;51(11):903–12.
- Ware J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical care [Internet]. 1996;34(3):220–33. Available from: https://www.ncbi.nlm.nih.gov/pubmed/8628042. 8628.
- Sanders JO, Harrast JJ, Kuklo TR, Polly DW, Bridwell KH, Diab M, et al. The Spinal Appearance Questionnaire: Results of Reliability, Validity, and Responsiveness Testing in Patients With Idiopathic Scoliosis. Spine [Internet]. 2007 Nov 15 [cited 2021 May 2];32(24):2719–22. Available from: https://journals.lww.com/spinejournal/Abstract/2007/11150/The_Spinal_Appearance_Questionnaire__Results_of.15.aspx#:~:text=This%20study%20tested%20the%20instrument. 2 May.
- Antonarakos PD, Katranitsa L, Angelis L, Paganas A, Koen EM, Christodoulou EA, et al. Reliability and validity of the adapted Greek version of scoliosis research society – 22 (SRS-22) questionnaire. Scoliosis. 2009 Jul 16;4(1).
- Yapar A, Yapar D, Ergisi Y, Kaptan AY, Tokgoz MA, Senkoylu A. Reliability and validity of the adapted Turkish version of the Spinal Appearance Questionnaire. Spine Deformity. 2020 Aug 17;9(1):57–66.
- Pappa E, Kontodimopoulos N, Niakas D. Validating and norming of the Greek SF-36 Health Survey. Quality of Life Research. 2005 Jun;14(5):1433–8.
- Carreon LY, Sanders JO, Polly DW, Sucato DJ, Parent S, Roy-Beaudry M, et al. Spinal Appearance Questionnaire. Spine. 2011 Aug;36(18):E1240–4.
- Roy-Beaudry M, Beauséjour M, Joncas J, Forcier M, Bekhiche S, Labelle H, et al. Validation and Clinical Relevance of a French-Canadian Version of the Spinal Appearance Questionnaire in Adolescent Patients. Spine. 2011 Apr;36(9):746–51.
- Wei X, Zhu X, Bai Y, Wu D, Chen J, Wang C, et al. Development of the Simplified Chinese Version of the Spinal Appearance Questionnaire. Spine. 2012 Aug;37(17):1497–504.
- Guo J, Lau AHY, Chau J, Ng BKW, Lee KM, Qiu Y, et al. A validation study on the traditional Chinese version of Spinal Appearance Questionnaire for adolescent idiopathic scoliosis. European Spine Journal: Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society [Internet]. 2016 Oct 1 [cited 2023 Nov 16];25(10):3186–93. Available from: https://pubmed.ncbi.nlm.nih.gov/27167743/.

Table 1.
The questionnaire domains and the results of tests of item convergent validity, item consistency reliability and floor and ceiling effects.
Table 1.
The questionnaire domains and the results of tests of item convergent validity, item consistency reliability and floor and ceiling effects.
| Domain | Number of items | Cronbach's alpha | Item convergent validity* | Floor effects | Ceiling effects |
|---|---|---|---|---|---|
| Physical functioning | 12 | 0.452 | 75.0% | 0(0%) | 0(0%) |
| Self Image | 4 | 0.16 | 100.0% | 0(0%) | 0(0%) |
| PSSEs | 8 | 0.514 | 87.5% | 0(0%) | 0(0%) |
| Psychosocial Functioning | 12 | 0.75 | 75.0% | 0(0%) | 0(0%) |
| Cognitive functioning | 5 | 0.641 | 100.0% | 0(0%) | 0(0%) |
| Compliance | 8 | 0.822 | 100.0% | 0(0%) | 1(1.25%) |
| Motivation | 2 | 0.156 | 100.0% | 0(0%) | 3(3.8%) |
| Pain | 2 | 0.313 | 50.0% | 4(5%) | 2(2.5%) |
| Total | 53 | 0.836 | 79.2% | 0(0%) | 0(0%) |
* Percentage of item-scale correlations ≥ 0.219.
Table 2.
Floor and ceiling effects (percentage of respondents with minimum/maximum scale scores) for each item of the questionnaire.
Table 2.
Floor and ceiling effects (percentage of respondents with minimum/maximum scale scores) for each item of the questionnaire.
| No of Item | Floor effect | Ceiling effect |
|---|---|---|
| 1 | 1 (1.3%) | 17 (21.3%) |
| 2 | 0 (0%) | 22 (27.5%) |
| 3 | 0 (0%) | 26 (32.5%) |
| 4 | 0 (0%) | 26 (32.5%) |
| 5 | 2 (2.5%) | 8 (10%) |
| 6 | 3 (3.8%) | 32 (40%) |
| 7 | 0 (0%) | 58 (72.5%) |
| 8 | 1 (1.3%) | 14 (17.5%) |
| 9 | 51 (63.8%) | 7 (8.8%) |
| 10 | 3 (3.8%) | 28 (35%) |
| 11 | 2 (2.5%) | 4 (5%) |
| 12 | 6 (7.5%) | 10 (12.5%) |
| 13 | 10 (12.5%) | 15 (18.8%) |
| 14 | 12 (15%) | 5 (6.3%) |
| 15 | 27 (33.8%) | 7 (8.8%) |
| 16 | 6 (7.5%) | 33 (41.3%) |
| 17 | 4 (5%) | 9 (11.3%) |
| 18 | 0 (0%) | 45 (56.3%) |
| 19 | 0 (0%) | 34 (42.5%) |
| 20 | 10 (12.5%) | 13 (16.3%) |
| 21 | 10 (12.5%) | 11 (13.8%) |
| 22 | 12 (15%) | 13 (16.3%) |
| 23 | 18 (22.5%) | 3 (3.8%) |
| 24 | 5 (6.3%) | 18 (22.5%) |
| 25 | 10 (12.5%) | 15 (18.8%) |
| 26 | 5 (6.3%) | 8 (10%) |
| 27 | 0 (0%) | 41 (51.3%) |
| 28 | 10 (12.5%) | 17 (21.3%) |
| 29 | 3 (3.8%) | 14 (17.5%) |
| 30 | 0 (0%) | 42 (52.5%) |
| 31 | 13 (16.3%) | 20 (25%) |
| 32 | 0 (0%) | 31 (38.8%) |
| 33 | 2 (2.5%) | 25 (31.3%) |
| 34 | 19 (23.8%) | 17 (21.3%) |
| 35 | 25 (31.3%) | 16 (20%) |
| 36 | 24 (30%) | 15 (18.8%) |
| 37 | 0 (0%) | 38 (47.5%) |
| 38 | 5 (6.3%) | 24 (30%) |
| 39 | 2 (2.5%) | 30 (37.5%) |
| 40 | 26 (32.5%) | 14 (17.5%) |
| 41 | 15 (18.8%) | 13 (16.3%) |
| 42 | 5 (6.3%) | 6 (7.5%) |
| 43 | 15 (18.8%) | 9 (11.3%) |
| 44 | 25 (31.3%) | 19 (23.8%) |
| 45 | 15 (18.8%) | 11 (13.8%) |
| 46 | 25 (31.3%) | 17 (21.3%) |
| 47 | 3 (3.8%) | 44 (55%) |
| 48 | 0 (0%) | 60 (75%) |
| 49 | 12 (15%) | 12 (15%) |
| 50 | 16 (20%) | 11 (13.8%) |
| 51 | 5 (6.3%) | 22 (27.5%) |
| 52 | 0 (0%) | 24 (30%) |
| 53 | 1 (1.3%) | 60 (75%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



