
Submitted:
20 November 2023
Posted:
22 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Laboratory analyses reveal significant differences between vaccinated and unvaccinated patients in parameters like C-reactive protein, ferritin, and white blood cell counts. Univariate and multivariate Cox proportional hazards regression analyses identify several factors influencing mortality, including comorbidities, pneumonia development, and various inflammatory markers.
Keywords:
Covid-19
; vaccines
; chronic kidney disease
; hemodialysis
; lymphocytopenia
1. Introduction
The global outbreak of coronavirus disease 2019 (COVID-19) signifies a widespread pandemic resulting from the infectious severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1,2,3]. This viral agent is responsible for causing the respiratory illness that has affected populations worldwide [4,5]. Because of the gravity of the situation, World Health Organization declared COVID-19 a public health emergency of international concern in January 2020 [6], and announced the pandemic in March 2020 [7].
The incidence of COVID-19 is notably elevated among the elderly and those with comorbidities [8,9,10]. Pre-existing conditions such as cardiovascular disease, diabetes mellitus (DM), hypertension (HT), and chronic kidney disease (CKD) have been identified as significant risk factors for severe disease and mortality [11,12,13,14,15,16]. The emergence of the COVID-19 pandemic has brought forth unprecedented challenges for individuals on a global level, but for those undergoing hemodialysis, the impact has been particularly pronounced [17,18,19,20].
Considering that most individuals with chronic kidney disease (CKD) experience compromised immune systems due to uremia, requiring regular dialysis sessions at hemodialysis centers two to three times a week, this group is more vulnerable to SARS-CoV-2, exhibiting a higher mortality rate compared to the general population [14,21].
Additionally, various laboratory indicators, including lymphocytopenia, leukocytosis, elevated C-reactive protein (CRP), D-dimer, procalcitonin, and troponin I, have been linked to increased mortality, especially among hemodialyzed patients [22,23,24]. Moreover, a connection has been observed between the use of mechanical ventilation and admission to intensive care units (ICUs) with elevated mortality rates [25].
A crucial element in safeguarding CKD patients is implementing a successful vaccination strategy against SARS-CoV-2.This is especially vital due to the observed correlation between the severity of COVID-19 and the stage of CKD in these individuals. Those with kidney failure tend to exhibit the most severe symptoms of COVID-19 [26]. Interestingly, patients with kidney failure appear to mount a sufficient cellular and humoral response to a natural SARS-CoV-2 infection. The magnitude and functionality of SARS-CoV-2-specific immunity, including T cell and neutralizing antibody responses, were found to be comparable between these patients and individuals with normal kidney function [27,28]. In general, individuals with chronic kidney disease tend to have diminished immune responses to vaccinations when compared to those who are in good health [29].
Our objective was to investigate whether there is a correlation between the vaccination status of hemodialysis patients and their laboratory findings during COVID-19, aiming to identify predictive factors for mortality.
2. Materials and Methods
This study included 442 patients on a chronic hemodialysis treatment program affected by COVID-19 infection, conducted at the COVID hospital in Batajnica, University Clinical Center of Serbia, from December 2020 to June 2022. Consecutive inclusion in the study involved patients over 18 years old who have been on a chronic hemodialysis treatment program for more than 3 months and had confirmed infection with the SARS-CoV-2 virus. The Ethic Committee of the Faculty of Medicine University of Belgrade, Serbia granted approval to collect the medical data, and carry out the study (ref. number 17/I-10). The study presented here was conducted following all ethical standards laid down in the 1964 Declaration of Helsinki.
2.1. Study Protocol
Patients undergoing chronic hemodialysis treatment, in the case of a confirmed infection with the SARS-CoV-2 virus, are referred to the COVID hospital in Batajnica for further treatment. Throughout the study duration, all facilities implemented a protocol involving temperature and symptom screening at each dialysis session. Additionally, all patients underwent SARS-CoV-2 PCR testing, with extra PCR testing conducted for individuals who had been in contact with confirmed cases. Cases were also identified through testing prompted by contact with a confirmed case or the presence of symptoms, such as seeking emergency services. The date of SARS-CoV-2 infection was determined based on the date of the initial positive PCR result within the observation period.
The patient monitoring period in the study encompasses the time from the registration of the presence of the SARS-CoV-2 virus in patients with either a) positive epidemiological risk, involving direct contact with a person infected with the SARS-CoV-2 virus, or b) the onset of symptoms of COVID-19 infection, until the outcome.
The outcome was defined as 1) discharge from the COVID hospital in Batajnica in the event of the cessation of the need for oxygen therapy with a negative test for the presence of the SARS-CoV-2 virus, or 2) occurrence of a fatal outcome.
Demographic data, data on the length of dialysis vintage, and anamnestic data on the onset of COVID-19 symptoms were collected upon the patient's admission to the COVID hospital in Batajnica, supplemented from accompanying medical documentation. Data on the course of the disease, laboratory analyses, chest X-ray findings, modes of oxygen supplementation, administered drug therapy, as well as the treatment outcome, were extracted from the medical history. Information about the vaccination of patients against the SARS-CoV-2 virus were retrieved from the official database of the Ministry of Health of the Republic of Serbia, accessible through the internet portal.
2.2. Measurement Instruments
The presence of pneumonia foci will be analyzed using tele-radiography of the lungs in the postero-anterior position. Based on the findings, patients were categorized into groups: 1) those without pneumonia, 2) with unilateral pneumonia, or 3) with bilateral pneumonia. Monitoring of inflammatory parameters and blood counts were conducted through standard laboratory analyses. The adequacy of pulmonary function will be assessed by arterial blood oxygen saturation using a gas analyzer.
2.3. Statistical Analysis
The normal distribution of continuous variables was tested using the Kolmogorov-Smirnov test. Continuous variables with a normal distribution are presented as mean ± standard deviation (SD), and continuous variables that did not show a normal distribution are presented as the median value and interquartile range (IQR). They were compared using one-way ANOVA, or its non-parametric equivalent Kruskal–Wallis test. Leven’s test for homogeneity of variance was used to test for equality of variances. Tokey test was performed for post hock multiple comparisons or Mann-Whitney U test for non-normal distributed variables. Categorical variables are presented as counts and percentages and were compared with the Chi square or Fisher’s exact test, as appropriate. Survival curves for different vaccination status groups of patients were constructed using the Kaplan–Meier method and further compared with the log-rank test. The identification of independent predictors for death was determined using a Cox proportional hazards regression model. Initially, all variables underwent univariate analysis. Those variables demonstrating an association with the outcome at a significance level below 0.1 were subsequently incorporated into the multivariate Cox model. The C statistic, a measure of the area under the receiver operating characteristic curve (AUC), quantified the predictive validity form mortality of CRP on admission, maximal value of CRP and minimal lymphocyte counts during hospitalization.
Statistical analyses were performed using the statistical package for social sciences, version 17 (SPSS, Chicago, Ill). Statistical significance was defined as p < 0.05.
3. Results
This research included 442 patients on maintenance hemodialysis, who received treatment at the COVID hospital in Batajnica, University Clinical Center of Serbia, between December 2020 and June 2022 due to SARS-CoV-2 infection. Demographic characteristics and vaccination status details are presented in Table 1. Among the 442 patients, 173 were unvaccinated against Covid-19, 19 had received a single dose, 112 had received two doses, and 138 had received three doses. After analyzing gender, age, primary kidney disease diagnosis, and comorbidities, no statistically significant differences were identified.
All patients admitted to the hospital undergo a chest X-ray (Table 2). Among the 442 patients, 189 showed no signs of pneumonia, while 227 exhibited bilateral pneumonia. Notably, 107 of these were unvaccinated, and 47 received three vaccine doses (p<0.001). Also, a difference was shown only among patients who received three doses of the vaccine in comparison to the others. A difference was shown between patients who received three doses compared to the unvaccinated and those who received one or two doses, while no difference was observed among the other cohorts. Out of the total 442 patients, 154 required additional oxygen support, with 66 patients on invasive mechanical ventilation (IMV). Of those on IMV, 34 were unvaccinated, and eight received three vaccine doses (p<0.001). On post hock analysis, a difference was observed exclusively among patients who received three doses compared to the others. According to our data, the use of antiviral drugs and monoclonal antibody - RegenCov (casirivimab and imdevimab) did not demonstrate statistical significance between unvaccinated and vaccinated patients. Upon hospital admission, there were significant differences in oxygen saturation between vaccinated and unvaccinated patients (p=0.017). Notably, patients who received two or three doses of the vaccine demonstrated higher oxygen saturation compared to those with a single dose or no vaccination. Regarding the systolic blood pressure on admission no differences were observed between vaccinated and unvaccinated patients (Table 2).
During the hospital stay, complications such as hemorrhage and thrombosis exhibited significant differences between vaccinated and unvaccinated patients (p=0.022), whereas 20 patients of total 34 with hemorrhage were unvaccinated and five of them received all three doses. Thrombosis gained 12 unvaccinated patients out of 21 and four were fully vaccinated patients. In post-hoc analysis, it has been demonstrated that this distinction is associated with both the unvaccinated individuals and those who have received three doses (p=0.020).
A total of 119 patients experienced a fatal outcome, with 60 being unvaccinated and 17 having received the full vaccination series (p<0.001). Post hoc analysis revealed that the distinction is applicable to patients who have received 3 doses, with no discernible difference observed between the unvaccinated individuals and those who received one or two doses (Table 2).
During the admission of patients to the hospital, biochemical analyzes were performed, with a specific emphasis on inflammatory markers (Table 3). A significant and statistically notable difference in C-reactive protein (CRP) levels in serum was observed between unvaccinated and vaccinated patients (p<0.001). Significantly lower CRP levels were observed in individuals who received all three vaccine doses when compared to both unvaccinated individuals and those who received two doses.
A significant difference in the concentrations of serum ferritin was established among patients based on vaccination status (p<0.001). Patients who received three doses exhibited significantly lower serum ferritin values compared to the unvaccinated and those who received a single dose. Additionally, patients vaccinated with two doses had lower ferritin values upon admission compared to the unvaccinated.
Furthermore, there were significant differences in blood albumin levels among the groups (p<0.001).
Throughout the hospitalization period, patients underwent daily monitoring for biochemical analysis (Table 4). Significant differences were observed in the maximum levels of white blood cells (WBC) between unvaccinated and vaccinated individuals (p=0.001). The detected lymphocytopenia, representing minimal lymphocyte values during hospitalization. It was least pronounced in patients who received three vaccine doses.
Significant differences in the maximum values of CRP were observed between unvaccinated and vaccinated patients (p<0.001). Significantly lower values were observed in patients who were vaccinated with three doses compared to the others.
When comparing maximum ferritin levels between unvaccinated and vaccinated patients, a substantial difference was noted (p<0.001). The median values in unvaccinated patients were 1976.2 µg/L (IQR 3853.70), whereas in patients who received all three doses of the vaccine, the median was 766.3 µg/L (IQR 1893.4) (p=0.002), Table 4.
Furthermore, variations in the highest fibrinogen levels were noted between unvaccinated and vaccinated individuals (p=0.001). Unvaccinated patients exhibited a maximal mean fibrinogen value of 5.7 ± 1.89 g/L, whereas fully vaccinated patients showed a lower maximal mean fibrinogen value of 5.1 ± 1.69 g/L, as detailed in Table 4.
Through Univariate Cox proportional hazards regression analysis, our findings indicate that elderly patients have an increased risk of a lethal outcome (HR: 1.025, 95% CI 1.010-1.040). While patients with comorbidities generally did not exhibit a heightened risk, those with CMP (HR: 2.400, 95% CI 1.666-3.458) showed a statistically significant difference (p<0.001). Also, only bilateral pneumonia was a predictor of a lethal outcome in the examined patients (HR: 19.888, 95% CI 6.312-62.664). Mortality was nearly 2.5 times higher in patients who had complications in the form of bleeding compared to patients without vascular complications and those who developed thrombosis (HR 2.401, 95% CI 1.539-3.745), Table 5.
Additionally, Univariate Cox proportional hazards regression analysis demonstrated that only patients vaccinated with three doses had significantly lower mortality compared to the unvaccinated (HR 0.397, 95% CI 0.231-0.683).
Various inflammatory parameters, including WBC on admission (HR: 1.077, 95% CI 1.038-1.118), lymphocyte count on admission (HR: 0.425, 95% CI 0.274-0.660), CRP on admission, and maximal values during hospitalization (HR: 1.006, 95% CI 1.004-1.007, HR: 1.007, 95% CI 1.005-1.009), IL-6 on admission and maximal values during hospitalization (HR: 1.001, 95% CI 1.000-1.002, HR: 1.001, 95% CI 1.000-1.002), ferritin on admission and maximal values during hospitalization (HR: 1.001, 95% CI 1.000-1.002, HR: 1.001, 95% CI 1.001-1.002), D-dimer on admission and maximal values during hospitalization (HR: 1.054, 95% CI 1.033-1.076, HR: 1.022, 95% CI 1.012-1.033), as well as minimal and maximal counts of lymphocytes (HR: 0.062, 95% CI 0.027-0.143, HR: 0.690, 95% CI 0.500-0.952), exhibited significant influence as predictive factors for a lethal outcome, Table 5.
In the Multivariate Cox proportional hazards regression analysis, our findings indicate a significant increase in the mortality of patients with CM (HR: 3.364, 95% CI 1.874-6.040). Additionally, CRP on admission (HR: 1.004, 95% CI 1.001-1.008), maximal values of CRP (HR: 1.006, 95% CI 1.002-1.010), and maximal values of IL-6 (HR: 1.001, 95% CI 1.0001-1.002) emerged as independent risk factors for a lethal outcome, as presented in Table 6.
In Figure 1, the Kaplan-Meier survival analysis curve is presented according to the number of received vaccine doses. Survival was significantly higher only in patients vaccinated with three doses (p=0.007).
The significance of lymphocytopenia in predicting a lethal outcome has been established in dialysis patients, both across the entire examined population and within patient subgroups based on their vaccination status. A cutoff of 0.395 for the minimal amount of lymphocytes during hospitalization shows a sensitivity of 84.2% and specificity of 81.5% for mortality prediction in the study population, Figure 2.
The C-statistic revealed a high level of discriminatory ability for the maximum CRP values in predicting mortality among dialysis patients, thought all subgroups based on the number of received doses of the vaccines (Figure 3). The cut-off value for CRP upon admission set at 56.5 mg/dL, demonstrates a sensitivity of 69.7% and specificity of 67.5% for mortality prediction. On the other hand, the cut-off value for the maximal CRP during hospitalization, set at 108.15 mg/dL, exhibits a sensitivity of 82.4% and specificity of 76.2% for mortality prediction.
4. Discussion
Patients with chronic kidney disease (CKD) are a particularly vulnerable group to infectious diseases, and morbidity and mortality increase with the progression of CKD [30,31]. Considering that patients undergoing chronic hemodialysis treatment often have one or more comorbidities, this makes them an even more vulnerable group. One of the reasons for such outcomes is the immunocompromised state of these patients. On the other hand, immunodeficiency leads to a weaker immune response to active immunization with vaccines.
Our findings indicate that factors such as gender, primary kidney disease diagnosis, and comorbidities did not exhibit statistical significance in hemodialyzed patients when considering vaccination status and mortality, except for age and cardiomyopathy. In the study by Rista et al., higher mortality rates were observed in patients undergoing dialysis for diabetic nephropathy (p<0.04) and peripheral vascular disease (p<0.01) [32], in contrast to Selvaskandan et al., who found no association between obesity, diabetes status, ethnicity, or CCI with COVID-19 severity [33]. Kikuchi et al., in their study, used multivariate analysis to showed a significant increase in mortality with prolonged duration of dialysis, without a difference in gender or primary disease [34]. Some multicenter studies indicated that advanced age, diabetes, and immune suppression in patients on hemodialysis with SARS-CoV-2 infection correlated with more severe illness [35], and in another study, age and pneumonia were independent risk factors for death using multivariable analysis [36]. These differences can be explained by the inherent heterogeneity in the design of studies encompassing these patients.
In our results, a significant difference was observed in the presence of bilateral pneumonia according to vaccination status. The lowest incidence of bilateral pneumonia was observed in patients who received a three-dose vaccination. However, univariate Cox analysis showed a higher risk for a lethal outcome of bilateral pneumonia (HR: 19.888). Upon hospital admission, there were notable differences in oxygen saturation between vaccinated and unvaccinated patients (p=0.017). Among the total 442 patients, 154 required additional oxygen support, with 66 undergoing invasive mechanical ventilation (IMV). Among those on IMV, 34 were unvaccinated, and eight had received three vaccine doses (p<0.001). This finding supports the fact that severe impairment of respiratory function has a poor prognostic significance, especially in such a vulnerable category of patients [36].
To the best of our knowledge, there is no literature data regarding the influence of vaccination status (unvaccinated/vaccinated) on complications such as hemorrhage in hemodialyzed patients with Covid-19 infection, particularly. Giot et al. demonstrated only the safety of vaccine application against COVID-19 during the dialysis session in patients under oral anticoagulants therapy [37]. Our results revealed a significantly higher incidence of hemorrhage as a complication due to Covid-19 infection within unvaccinated patients than in fully vaccinated patients (p < 0.001, HR: 2.401, 95%CI 1.539-3.745), which therefore represents a potential predictive factor for a lethal outcome.
Laboratory findings played a significant role in determining the survival rate. Our results indicated that various inflammatory parameters, including WBC on admission lymphocyte count on admission CRP on admission, and maximal values during hospitalization IL-6 on admission and maximal values during hospitalization, ferritin on admission and maximal values during hospitalization, D-dimer on admission and maximal values during hospitalization as well as minimal and maximal counts of lymphocytes, significantly influenced the predictive factors for a lethal outcome.
Zaidi et al., in their meta-analysis, suggested that lymphocytopenia serves as a crucial hematological indicator of severe COVID-19, with lymphocytopenia <1500/mm3 being a practical parameter for predicting severe outcomes [38]. Niu et al. demonstrated the predictive efficacy of lymphocytopenia, with areas under the receiver operating characteristic curves (AUC) of 0.68, 0.69, 0.78, and 0.79 for the corresponding adverse outcomes when age, gender, race, and comorbidities were taken into account. Among the patients analyzed, 2409 (57.3%) exhibited lymphocytopenia (absolute lymphocyte count < 1.1 × 109/L) upon admission, experiencing higher rates of ICU admission (17.9% versus 9.5%, p < 0.001), invasive mechanical ventilation (14.4% versus 6.5%, p < 0.001), dialysis (3.4% versus 1.8%, p < 0.001), and in-hospital mortality (16.6% versus 6.6%, p < 0.001). Multivariable-adjusted odds ratios for these outcomes were 1.86 (95% CI, 1.55–2.25), 2.09 (95% CI, 1.69–2.59), 1.77 (95% CI, 1.19–2.68), and 2.19 (95% CI 1.76–2.72), respectively, compared to those without lymphocytopenia. These findings were not compared with vaccination status [39]. Hartantri et al., based on laboratory parameters, identified high procalcitonin and C-reactive protein levels, along with a neutrophil-to-lymphocyte ratio >3.53, as associated with mortality. In our study, CRP on admission as well as maximal values during hospitalization were found to be independent predictive factors for a lethal outcome, respectively [40]. Rista et al., using ROC analysis, identified lymphocytopenia and eosinopenia as robust predictors of mortality. Post-vaccination, the mortality rate in the vaccinated population was 8%, a significant contrast to the 66.7% mortality rate observed in the unvaccinated group (p < 0.001), [32]. Similar results were observed in our study. We also found a significant predictive ability of lymphocytopenia for mortality in dialysis patients. Additionally, the AUC was 0.886 and a cutoff of 0.395 for the minimal amount of lymphocytes during hospitalization shows a sensitivity of 84.2% and specificity of 81.5% for mortality prediction in the study population. The C-statistic indicated a robust discriminatory ability in predicting mortality among dialysis patients using the maximum CRP values, across all subgroups based on the number of vaccine doses received. A threshold value for CRP upon admission, established at 56.5 mg/dL, shows a sensitivity of 69.7% and specificity of 67.5% for mortality prediction. Conversely, the threshold value for maximum CRP during hospitalization, set at 108.15 mg/dL, demonstrates a sensitivity of 82.4% and specificity of 76.2% for predicting mortality.
Although many studies showed the influence of the usage of antiviral drugs in contrary to the duration of hospitalization [34,41], our results showed that antiviral drugs and monoclonal antibodies did not show any statistical significance in mortality prevention nor duration of hospitalization (p=0.196). Possible explanation lies in the fact that these medications were administered only to the most severe patients, and therefore, there is a selection bias.
Numerous studies have highlighted the impact of vaccination status on survival rates in hemodialyzed patients with COVID-19, presenting real-world effectiveness and immunogenicity data for vaccines [42]. Espi et al. conducted a prospective observational study, emphasizing the safety and efficacy of a third dose of mRNA vaccine in maintenance hemodialysis patients [43]. In a study by Ashby et al., the analysis demonstrated that, factoring in age, comorbidities, and the time period, a two-dose vaccination history was associated with a 75% lower risk of admission and an 88% reduction in deaths compared to unvaccinated patients. Even after the first dose, there were noticeable differences, with a 45% lower risk of admission. Notably, the protection from severe illness associated with vaccination was most evident in patients over 65 years. Third doses provided additional protection, with a 51% further reduction in admissions [44]. Furthermore, a US study involving over 12,000 hemodialysis patients receiving vaccine indicated a significantly lower subsequent risk of symptomatic COVID-19 compared to a matched unvaccinated cohort dialyzing at the same facilities [42]. However, an analysis of linked Scottish registry data, encompassing patients on dialysis and those with kidney transplants, estimated vaccine effectiveness in preventing infection at only 33% [45]. The results of our study indicated that patients who received three doses of the vaccine against SARS-CoV-2 had a 60.3% lower probability for lethal outcome in comparison to unvaccinated patients. Additionally, patients vaccinated with one or two doses did not show a significantly lower mortality compared to the unvaccinated group.
5. Conclusions
Among hemodialysis patients affected by Covid-19 infection, vaccination with at least three doses emerges as a protective factor against fatal outcomes and bilateral pneumonia. Predictors of mortality in this cohort include CRP levels upon admission, especially the maximum CRP values during the illness. Additionally, individuals with cardiovascular comorbidities face a heightened risk of adverse consequences. Noteworthy is the observation that the most pronounced lymphocytopenia during infection exhibits a notable level of specificity and sensitivity (84.2% and 81.5%, respectively) in predicting mortality, with a lymphocyte count cutoff of 0.395×10^9/L.
Author Contributions
Conceptualization: V.B.; methodology. V.B.; formal analysis. V.B., M.B; investigation V.B., M.K.; data curation. V.B., M.M., J.P. writing—original draft preparation. V.B., G.N.; writing—review and editing. M.L., M.R.; visualization. M.R; supervision. M.R.; funding acquisition. M.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by The Ethic Committee of the Faculty of Medicine University of Belgrade, Serbia, which granted approval to collect the medical data, and carry out the study (ref. number 17/I-10).
Informed Consent Statement
Patient consent was waived due to pandemic situation and current situation worldwide.
Acknowledgments
This research is part of doctoral dissertation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abd El-Aziz T.M; Stockand J.D. Recent progress and challenges in drug development against COVID-19 coronavirus (SARS-CoV-2) - an update on the status. Infect Genet Evol. 2020; 83:104327. [CrossRef]
- Sharma A.; Tiwari S.; Deb M.K.; Marty J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): a global pandemic and treatment strategies. Int J Antimicrob Agents. 2020, 56(2):106054. [CrossRef]
- Mohanty S.K.; Satapathy A.; Naidu M.M.; Mukhopadhyay S.; Sharma S.; Barton L.M.; Stroberg E.; Duval E.J.; Pradhan D.; Tzankov A.; Parwani A.V. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19) - anatomic pathology perspective on current knowledge. Diagn Pathol. 2020, 15(1):103.
- Chatterjee P.; Nagi N.; Agarwal A.; Das B.; Banerjee S.; Sarkar S.; Gupta N.; Gangakhedkar R.R. The 2019 novel coronavirus disease (COVID-19) pandemic: A review of the current evidence. Indian J Med Res. 2020, 151(2&3):147-159. [CrossRef]
- Arshad Ali S.; Baloch M.; Ahmed N.; Arshad Ali A.; Iqbal A. The outbreak of Coronavirus Disease 2019 (COVID-19)-An emerging global health threat. J Infect Public Health. 2020, 13(4):644-646. [CrossRef]
- Sohrabi C.; Alsafi Z.; O'Neill N.; Khan M.; Kerwan A.; Al-Jabir A.; Iosifidis C.; Agha R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020, 76:71-76. [CrossRef]
- Cucinotta D.; Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91(1):157-160. [CrossRef]
- Sanyaolu A.; Okorie C.; Marinkovic A.; Patidar R.; Younis K.; Desai P.; Hosein Z.; Padda I.; Mangat J.; Altaf M. Comorbidity and its Impact on Patients with COVID-19. SN Compr Clin Med. 2020, 2(8):1069-1076. [CrossRef]
- Bajgain K.T.; Badal S.; Bajgain B.B.; Santana M.J.; Prevalence of comorbidities among individuals with COVID-19: A rapid review of current literature. Am J Infect Control. 2021, 49(2):238-246. [CrossRef]
- Mi J.; Zhong W.; Huang C.; Zhang W.; Tan L.; Ding L. Gender, age and comorbidities as the main prognostic factors in patients with COVID-19 pneumonia. Am J Transl Res. 2020, 12(10):6537-6548.
- Varikasuvu S.R.; Dutt N.; Thangappazham B.; Varshney S. Diabetes and COVID-19: A pooled analysis related to disease severity and mortality. Prim Care Diabetes. 2021, 15(1):24-27. [CrossRef]
- Lippi G.; Wong J.; Henry B.M. Hypertension in patients with coronavirus disease 2019 (COVID-19): a pooled analysis. Pol Arch Intern Med. 2020, 130(4):304-309.
- Cai R.; Zhang J.; Zhu Y.; Liu L.; Liu Y.; He Q. Mortality in chronic kidney disease patients with COVID-19: a systematic review and meta-analysis. Int Urol Nephrol. 2021, 53(8):1623-1629. [CrossRef]
- Menon T.; Gandhi S.A.Q.; Tariq W.; Sharma R.; Sardar S.; Arshad A.M.; Adhikari R.; Ata F.; Kataria S.; Singh R. Impact of Chronic Kidney Disease on Severity and Mortality in COVID-19 Patients: A Systematic Review and Meta-analysis. Cureus. 2021, 13(4):e14279. [CrossRef]
- Wu Z.H.; Tang Y.; Cheng Q. Diabetes increases the mortality of patients with COVID-19: a meta-analysis. Acta Diabetol. 2021, 58(2):139-144. [CrossRef]
- Pranata R.; Lim M.A.; Huang I.; Raharjo S.B., Lukito A.A. Hypertension is associated with increased mortality and severity of disease in COVID-19 pneumonia: A systematic review, meta-analysis and meta-regression. J Renin Angiotensin Aldosterone Syst. 2020, 21(2):1470320320926899. [CrossRef]
- Jager K.J.; Kramer A.; Chesnaye N.C.; Couchoud C.; Sánchez-Álvarez J.E.; Garneata L.; Collart F.; Hemmelder M.H.; Ambühl P.; Kerschbaum J.; Legeai C.; Del Pino Y Pino M.D.; Mircescu G.; Mazzoleni L.; Hoekstra T.; Winzeler R.; Mayer G.; Stel V.S.; Wanner C.; Zoccali C.; Massy Z.A. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98(6):1540-1548. [CrossRef]
- Wang F.; Ao G.; Wang Y.; Liu F.; Bao M.; Gao M.; Zhou S.; Qi X. Risk factors for mortality in hemodialysis patients with COVID-19: a systematic review and meta-analysis. Ren Fail. 2021, 43(1):1394-1407. [CrossRef]
- Li J.; Li S.X.; Zhao L.F.; Kong D.L.; Guo Z.Y. Management recommendations for patients with chronic kidney disease during the novel coronavirus disease 2019 (COVID-19) epidemic. Chronic Dis Transl Med. 2020, 6(2), 119-123. [CrossRef]
- Nogueira G.M.; Oliveira M.S.; Moura A.F.; Cruz C.M.S.; Moura-Neto J.A. COVID-19 in dialysis units: A comprehensive review. World J Virol. 2021,10(5):264-274. [CrossRef]
- Ng W.H.; Tipih T.; Makoah N.A.; Vermeulen J.G.; Goedhals D.; Sempa J.B.; Burt F.J.; Taylor A.; Mahalingam S. Comorbidities in SARS-CoV-2 Patients: a Systematic Review and Meta-Analysis. mBio. 2021, 9;12(1):e03647-20. [CrossRef]
- Ali E.T.; Sajid Jabbar A.; Al Ali H.S.; Shaheen Hamadi S.; Jabir M.S.; Albukhaty S. Extensive Study on Hematological, Immunological, Inflammatory Markers, and Biochemical Profile to Identify the Risk Factors in COVID-19 Patients. Int J Inflam. 2022, 2022:5735546. [CrossRef]
- Gao Y.D.; Ding M.; Dong X.; Zhang J.J.; Kursat Azkur A.; Azkur D.; Gan H.; Sun Y.L.; Fu W.; Li W., Liang H.L., Cao Y.Y., Yan Q., Cao C., Gao H.Y., Brüggen M.C., van de Veen W., Sokolowska M., Akdis M., Akdis C.A. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy. 202.1, 76(2):428-455. [CrossRef]
- Mudatsir M.; Fajar J.K.; Wulandari L.; Soegiarto G.; Ilmawan M.; Purnamasari Y.; Mahdi B.A.; Jayanto G.D.; Suhendra S.; Setianingsih Y.A.; Hamdani R.; Suseno D.A.; Agustina K.; Naim H.Y.; Muchlas M.; Alluza H.H.D.; Rosida N.A.; Mayasari M.; Mustofa M.; Hartono A.; Aditya R.; Prastiwi F.; Meku F.X.; Sitio M.; Azmy A.; Santoso A.S.; Nugroho R.A. .; Gersom C.; Rabaan A.A.; Masyeni S.; Nainu F., Wagner A.L.; Dhama K.; Harapan H. Predictors of COVID-19 severity: a systematic review and meta-analysis. F1000Res. 2020, 9:1107.
- Roedl K.; Jarczak D.; Thasler L.; Bachmann M.; Schulte F.; Bein B.; Weber C.F.; Schäfer U.; Veit C.; Hauber H.P.; Kopp S.; Sydow K.; de Weerth A.; Bota M.; Schreiber R.; Detsch O.; Rogmann J.P.; Frings D.; Sensen B.; Burdelski C.; Boenisch O.; Nierhaus A.; de Heer G.; Kluge S. Mechanical ventilation and mortality among 223 critically ill patients with coronavirus disease 2019: A multicentric study in Germany. Aust Crit Care. 2021, 2:167-175. [CrossRef]
- Hou Y.C.; Lu K.C.; Kuo K.L. The Efficacy of COVID-19 Vaccines in Chronic Kidney Disease and Kidney Transplantation Patients: A Narrative Review. Vaccines 2021, 9, 885. [CrossRef]
- Hartzell S.; Bin S.; Benedetti C.; Haverly M.; Gallon L.; Zaza G.; Riella L.V.; Menon M.C.; Florman S.; Rahman A.H.; Leech J.M.; Heeger P.S.; Cravedi P. Evidence of potent humoral immune activity in COVID-19-infected kidney transplant recipients. Am J Transplant. 2020, 20(11):3149-3161. [CrossRef]
- Candon S.; Guerrot D.; Drouot L.; Lemoine M.; Lebourg L.; Hanoy M.; Boyer O.; Bertrand D. T cell and antibody responses to SARS-CoV-2: Experience from a French transplantation and hemodialysis center during the COVID-19 pandemic. Am J Transplant. 2021, 2, 854-863. [CrossRef]
- Kato S.; Chmielewski M.; Honda H.; Pecoits-Filho R.; Matsuo S.; Yuzawa Y.; Tranaeus A.; Stenvinkel P.; Lindholm B. Aspects of immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol. 2008, 5,1526-33. [CrossRef]
- Allon M.; Depner T.A.; Radeva M.; Bailey J.; Beddhu S.; Butterly D.; Coyne D.W.; Gassman J.J.; Kaufman A.M.; Kaysen G.A.; Lewis J.A.; Schwab S.J.; HEMO Study Group. Impact of dialysis dose and membrane on infection-related hospitalization and death: results of the HEMO Study. J Am Soc Nephrol. 2003, 7, 1863-70. [CrossRef]
- James M.T.; Quan H.; Tonelli M.; Manns B.J.; Faris P.; Laupland K.B.; Hemmelgarn BR.; Alberta Kidney Disease Network. CKD and risk of hospitalization and death with pneumonia. Am J Kidney Dis. 2009,1,24-32. [CrossRef]
- Rista E.; Dervishi D.; Cadri V.; Akshija I.; Saliaj K.; Bino S.; Puca E.; Harxhi A. Predictors of mortality in hemodialysis patients with COVID-19: A single-center experience. J Infect Dev Ctries. 2023, 17(4):454-460. [CrossRef]
- Selvaskandan H.; Hull K.L.; Adenwalla S.; Ahmed S.; Cusu M.C.; Graham-Brown M.; Gray L.; Hall M.; Hamer R.; Kanbar A.; Kanji H.; Lambie M.; Lee H.S.; Mahdi K.; Major R.; Medcalf J.F.; Natarajan S.; Oseya B.; Stringer S.; Tabinor M.; Burton J. Risk factors associated with COVID-19 severity among patients on maintenance haemodialysis: a retrospective multicentre cross-sectional study in the UK. BMJ Open. 2022, 5:e054869. [CrossRef]
- Kikuchi K.;, Nangaku M.; Ryuzaki M.; Yamakawa T.; Yoshihiro O.; Hanafusa N.; Sakai K.; Kanno Y.; Ando R.; Shinoda T.; Nakamoto H.; Akizawa T.; COVID-19 Task Force Committee of the Japanese Association of Dialysis Physicians, the Japanese Society for Dialysis Therapy, and the Japanese Society of Nephrology. Survival and predictive factors in dialysis patients with COVID-19 in Japan: a nationwide cohort study. Ren Replace Ther. 2021, 7(1):59. [CrossRef]
- Ashby D.R.; Caplin B.; Corbett R.W.; Asgari E.; Kumar N.; Sarnowski A.; Hull R.; Makanjuola D.; Cole N.; Chen J.; Nyberg S.; McCafferty K.; Zaman F.; Cairns H.; Sharpe C.; Bramham K.; Motallebzadeh R.; Anwari K.J.; Salama A.D.; Banerjee D; Pan-London COVID-19 Renal Audit Group. Severity of COVID-19 after Vaccination among Hemodialysis Patients: An Observational Cohort Study. Clin J Am Soc Nephrol. 2022, 17(6):843-850. [CrossRef]
- Turgutalp K.; Ozturk S.; Arici M.; Eren N.; Gorgulu N.; Islam M.; Uzun S.; Sakaci T.; Aydin Z.; Sengul E.; Demirelli B.; Ayar Y.; Altiparmak M.R.; Sipahi S.; Mentes I.B.; Ozler TE.; Oguz EG.; Huddam B.; Hur E.; Kazancioglu R.; Gungor O.; Tokgoz B.; Tonbul H.Z.; Yildiz A.; Sezer S.; Odabas A.R.; Ates K. Determinants of mortality in a large group of hemodialysis patients hospitalized for COVID-19. BMC Nephrol. 2021, 22(1):29. [CrossRef]
- Giot M.; Robert T.; Brunet P.; Resseguier N.; Lano G. Vaccination against COVID-19 in a haemodialysis centre: what is the risk of bleeding complications? Clin Kidney J. 2021, 14(6):1701-1703.
- Ziadi A.; Hachimi A.; Admou B.; Hazime R.; Brahim I.; Douirek F.; Zarrouki Y.; El Adib A.R, Younous S.; Samkaoui A.M. Lymphopenia in critically ill COVID-19 patients: A predictor factor of severity and mortality. Int J Lab Hematol. 2021, 43(1):e38-e40. [CrossRef]
- Niu J.; Sareli C.; Mayer D.; Visbal A.; Sareli A. Lymphopenia as a Predictor for Adverse Clinical Outcomes in Hospitalized Patients with COVID-19: A Single Center Retrospective Study of 4485 Cases. J Clin Med. 2022, 11(3):700. [CrossRef]
- Hartantri Y.; Debora J.; Widyatmoko L.; Giwangkancana G.; Suryadinata H.; Susandi E.; Hutajulu E.; Hakiman A.P.A.; Pusparini Y.; Alisjahbana B. Clinical and treatment factors associated with the mortality of COVID-19 patients admitted to a referral hospital in Indonesia. Lancet Reg Health Southeast Asia. 2023,100167. [CrossRef]
- Zeng B.; Zhou J.; Peng D.; Dong C.; Qin Q. The prevention and treatment of COVID-19 in patients treated with hemodialysis. Eur J Med Res. 2023, 28(1):410. [CrossRef]
- Sibbel S.; McKeon K.; Luo J.; Wendt K.; Walker A.G.; Kelley T.; Lazar R.; Zywno M.L.; Connaire J.J.; Tentori F.; Young A.; Brunelli S.M. Real-World Effectiveness and Immunogenicity of BNT162b2 and mRNA-1273 SARS-CoV-2 Vaccines in Patients on Hemodialysis. J Am Soc Nephrol. 2022, 49-57. [CrossRef]
- Espi M.; Charmetant X.; Barba T.; Mathieu C.; Pelletier C.; Koppe L.; Chalencon E.; Kalbacher E.; Mathias V.; Ovize A.; Cart-Tanneur E.; Bouz C.; Pellegrina L.; Morelon E.; Juillard L.; Fouque D.; Couchoud C.; Thaunat O.; REIN Registry. A prospective observational study for justification, safety, and efficacy of a third dose of mRNA vaccine in patients receiving maintenance hemodialysis. Kidney Int. 2022, 390-402. [CrossRef]
- Ashby D.R.; Caplin B.; Corbett RW.; Asgari E.; Kumar N.; Sarnowski A.; Hull R.; Makanjuola D.; Cole N.; Chen J.; Nyberg S.; Forbes S.; McCafferty K.; Zaman F.; Cairns H.; Sharpe C.; Bramham K.; Motallebzadeh R.; Anwari K.; Roper T.; Salama A.D.; Banerjee D.; pan-London Covid-19 renal audit groups. Outcome and effect of vaccination in SARS-CoV-2 Omicron infection in hemodialysis patients: a cohort study. Nephrol Dial Transplant. 2022, 37(10), 1944-1950. [CrossRef]
- Bell S.; Campbell J.; Lambourg E.; Watters C.; O’Neil M.; Almond A.; Buck K.; Carr EJ.; Clark L.; Cousland Z.; Findlay M.; Joss N.; Metcalfe W.; Petrie M.; Spalding E.; Traynor J.P.; Sanu V.; Thomson P.; Methven S.; Mark P.B: The impact of vaccination on incidence and outcomes of SARS-CoV-2 infection in patients with kidney failure in Scotland. J Am Soc Nephrol, 2022, 33: 677–686. [CrossRef]
Figure 1.
Kaplan Meier curve survival analysis according to the number of received vaccine doses whereas unvaccinated vs. 3 doses p=0.001, 2 doses vs. 3 doses p=0.009. The lack of a notable distinction when compared to individuals who received a single vaccine dose is probably attributable to the limited number of participants in that particular group.
Figure 1.
Kaplan Meier curve survival analysis according to the number of received vaccine doses whereas unvaccinated vs. 3 doses p=0.001, 2 doses vs. 3 doses p=0.009. The lack of a notable distinction when compared to individuals who received a single vaccine dose is probably attributable to the limited number of participants in that particular group.
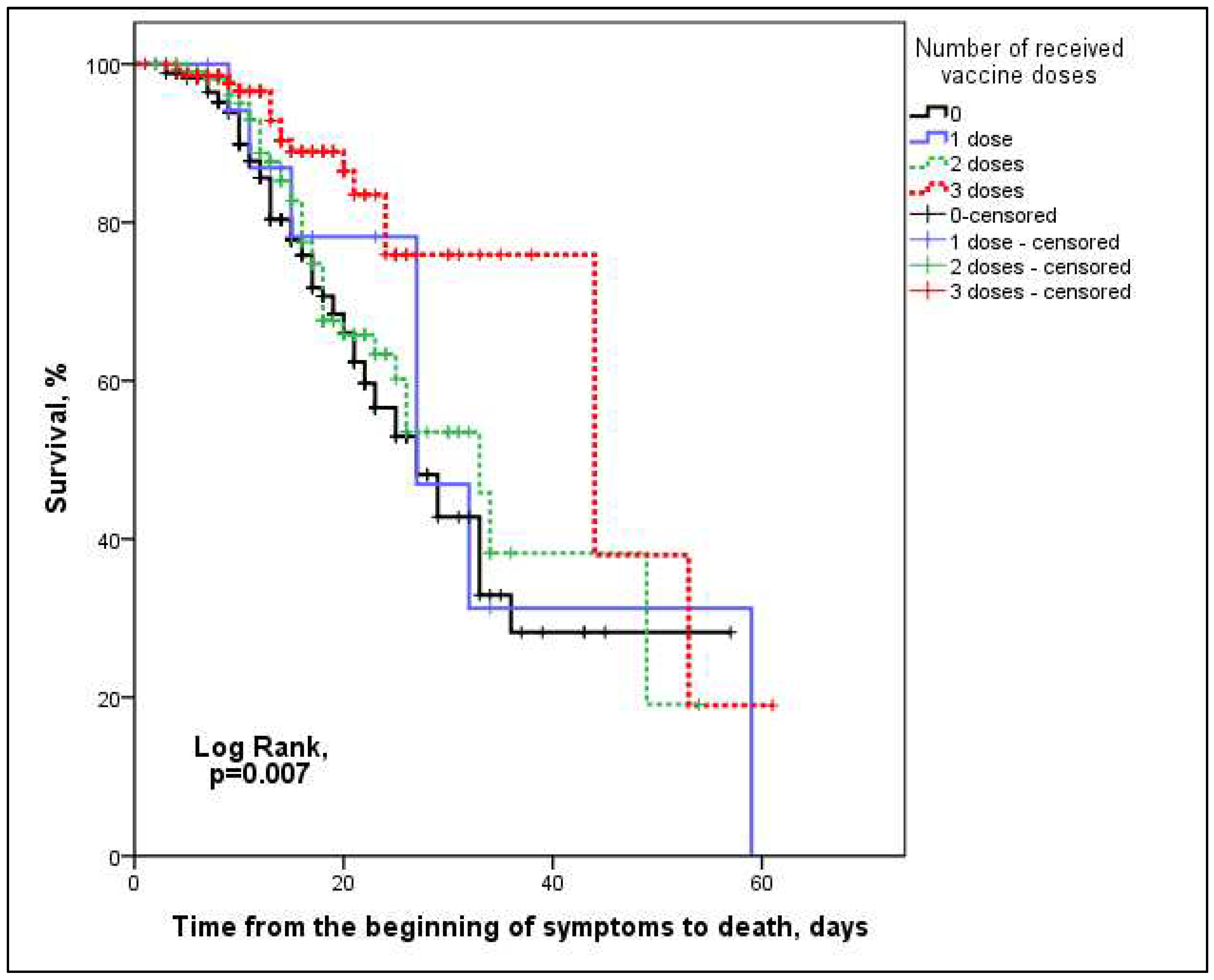
Figure 2.
The ROC curve of the discriminative ability of the minimum number of lymphocytes during hospitalization in predicting mortality: A- represent all admission patients to the hospital (n=442), B- represent unvaccinated patients (n=173), C- represent patients who received only one dose of the vaccine (n=19), D- represent patients who received two doses of the vaccine (n=112) and E- represent fully vaccinated patients with three doses of the vaccine (n=138).
Figure 2.
The ROC curve of the discriminative ability of the minimum number of lymphocytes during hospitalization in predicting mortality: A- represent all admission patients to the hospital (n=442), B- represent unvaccinated patients (n=173), C- represent patients who received only one dose of the vaccine (n=19), D- represent patients who received two doses of the vaccine (n=112) and E- represent fully vaccinated patients with three doses of the vaccine (n=138).
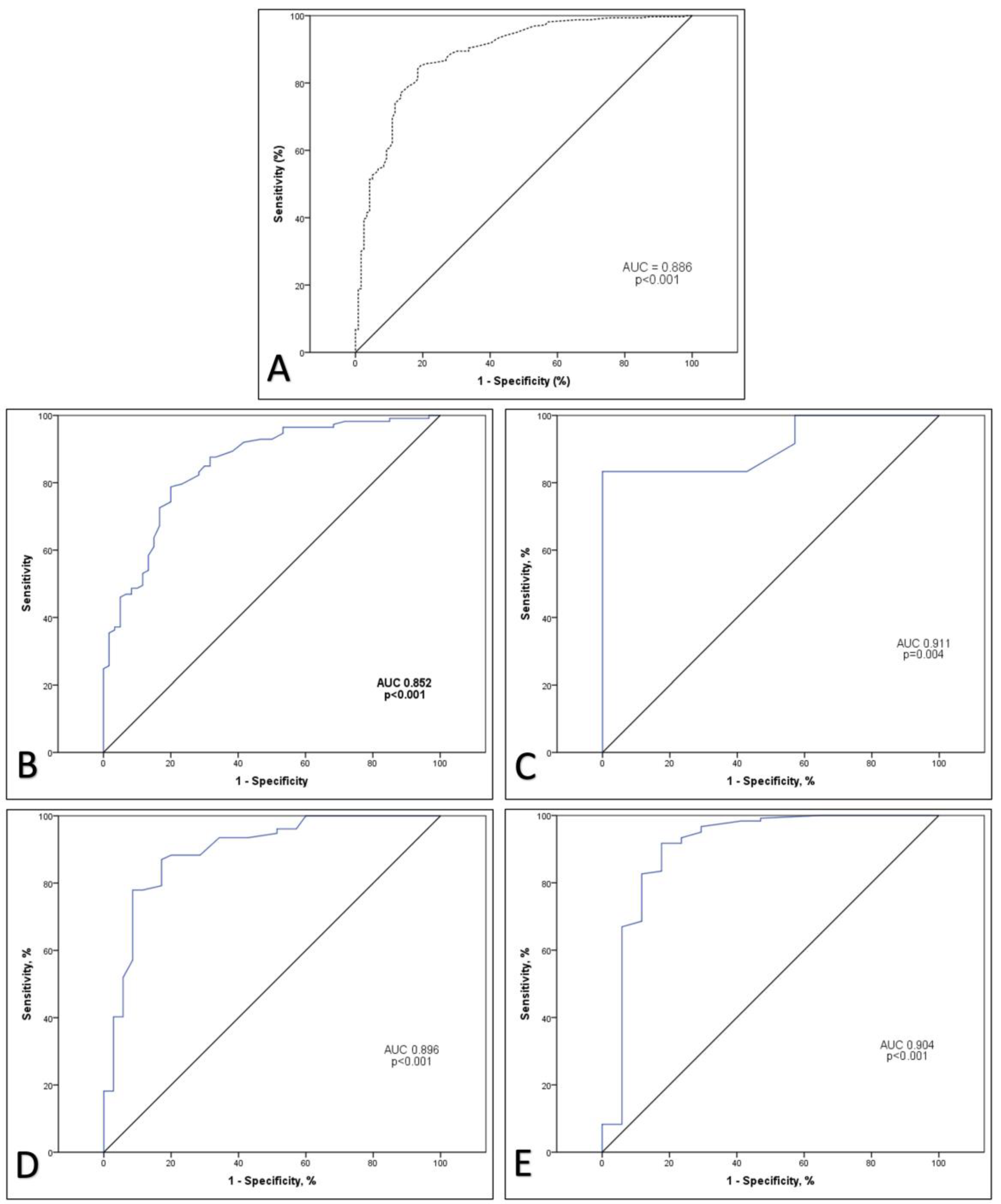
Figure 3.
ROC curve of the discriminative ability of CRP values in predicting mortality: A- represent all admission patients to the hospital (n=442), B- represent unvaccinated patients (n=173), C- represent patients who received only one dose of the vaccine (n=19), D- represent patients who received two doses of the vaccine (n=112) and E- represent fully vaccinated patients with three doses of the vaccine (n=138).
Figure 3.
ROC curve of the discriminative ability of CRP values in predicting mortality: A- represent all admission patients to the hospital (n=442), B- represent unvaccinated patients (n=173), C- represent patients who received only one dose of the vaccine (n=19), D- represent patients who received two doses of the vaccine (n=112) and E- represent fully vaccinated patients with three doses of the vaccine (n=138).
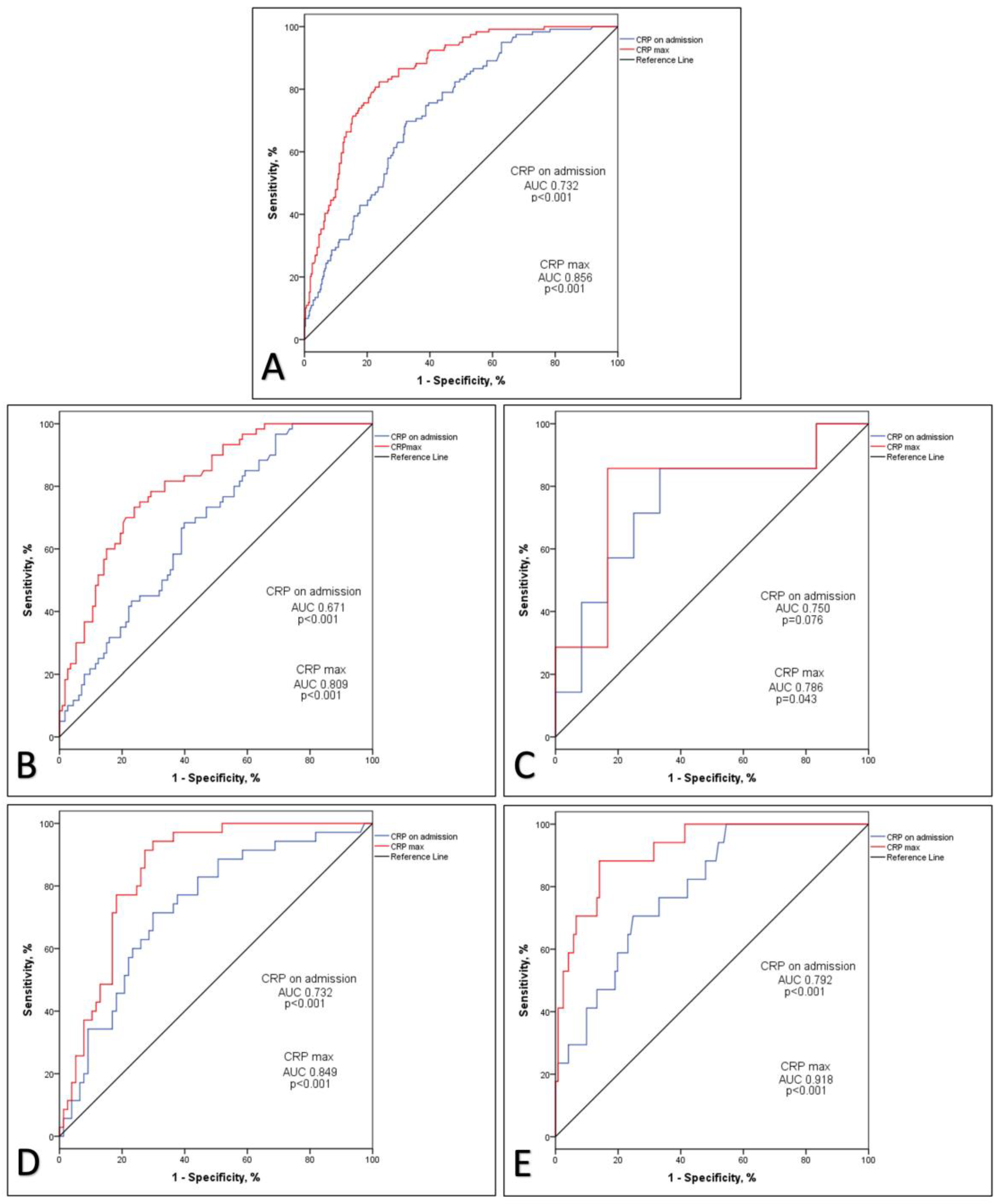

Table 1.
Demographic and clinical characteristics of the studied population according to vaccination status.
Table 1.
Demographic and clinical characteristics of the studied population according to vaccination status.
| Overall, N=442 |
Unvaccinated, n=173 |
1 dose, n=19 |
2 doses, n=112 | 3 doses, n=138 | p | |
|---|---|---|---|---|---|---|
| Male sex, n (%) | 285 (64.5%) | 118 (68.2) | 9 (47.7) | 68 (60.7) | 90 (65.2) | 0.240 |
| Age, years ± SD | 63 ± 13.7 | 62 ± 14.3 | 63 ± 15.9 | 64 ± 13.9 | 65 ± 12.3 | 0.162 |
| Primary kidney disease, n (%) Hypertension Diabetes Glomerulonephritis Lupus nephritis and vasculitis Polycystic kidney disease Others |
169 (38.2) 115 (26.0) 36 (8.1) 21 (4.8) 27 (6.1) 74 (16.7) |
62 (35.8) 42 (24.3) 17 (9.8) 9 (5.2) 9 (5.2) 34 (19.7) |
9 (47.4) 3 (15.8) 2 (10.5) 3 (15.8) 1 (5.3) 1 (5.3) |
43 (38.4) 33 (29.5) 5 (4.5) 4 (3.6) 7 (6.3) 20 (17.9) |
55 (39.9) 37 (26.8) 12 (8.7) 5 (3.6) 10 (7.2) 19 (13.8) |
0.502 |
| Comorbidity, n (%) Hypertension Diabetes Cardiomyopathy Cerebrovascular disease Malignancy COPD |
374 (84.6) 125 (28.3) 155 (35.1) 32 (7.2) 45 (10.2) 17 (3.8) |
144 (83.2) 47 (27.2) 64 (37.0) 14 (8.1) 15 (8.7) 7 (4.0) |
16 (84.2) 3 (15.8) 9 (47.4) 2 (10.5) 2 (10.5) 0 (0) |
94 (83.9) 35 (31.3) 32 (28.6) 9 (8.0) 12 (10.7) 5 (4.5) |
120 (87.0) 40 (29.0) 50 (36.2) 7 (5.1) 16 (11.6) 5 (3.6) |
0.831 0.554 0.295 0.668 0.857 0.822 |
| Duration of dialysis, years, median (IQR) | 4 (7) | 4.73 (8) | 3.75 (9) | 4 (7) | 4 (7) | 0.920 |
*COPD, chronic obstructive pulmonary disease.
Table 2.
Clinical characteristics and therapeutic approaches of patients infected with the SARS-CoV-2 virus based on vaccination status.
Table 2.
Clinical characteristics and therapeutic approaches of patients infected with the SARS-CoV-2 virus based on vaccination status.
| Overall, N=442 |
Unvaccinated, n=173 |
1 dose, n=19 |
2 doses, n=112 | 3 doses, n=138 | p | |
|---|---|---|---|---|---|---|
| The X-ray signs of pneumonia, n (%) Withut pneumona Unilateral pneumonia Bilateral pneumonia |
189 (42.8) 26 (5.9) 227 (51.3) |
50 (28.9) 16 (9.2) 107 (61.8) |
5 (26.3) 2 (10.5) 12 (63.2) |
46 (41.1) 5 (4.5) 61 (54.5) |
88 (63.8) 3 (2.2) 47 (34.1) |
<0.001 |
| Oxigenation, n (%) Ambient air Low flow nasal cannula High Flow face mask Noninvasive ventilation Invasive mechanical ventilation |
268 (60.6) 83 (18.8) 10 (2.3) 15 (3.4) 66 (14.9) |
83 (48.0) 40 (23.1) 5 (2.9) 11 (6.4) 34 (19.7) |
10 (52.6) 7 (36.8) 0 (0) 0 (0) 2 (10.5) |
64 (57.1) 22 (19.6) 3 (2.7) 1 (0.9) 22 (19.6) |
111 (80.4) 14 (10.1) 2 (1.4) 3 (2.2) 8 (5.8) |
<0.001 |
| Antivirotic, n (%) | 59 (13.3) | 19 (11.0) | 1 (5.3) | 14 (12.5) | 25 (18.1) | 0.196 |
| Regen Cov, n (%) | 22 (5.0) | 6 (3.5) | 1 (5.3) | 6 (5.4) | 9 (6.5) | 0.667 |
| Time from the last vaccine dose to the onset of illness, day, median (IQR) | 141 (170) | - | 14 (225) | 168 (120) | 122.5 (171) | <0.001 |
| Time from illness onset to outcome, day, median (IQR) | 15 (11) min-max 1-61 | 15 (12) | 15 (18) | 17 (10) | 14 (11) | 0.137 |
| Oxygen saturation on admission, % ± SD | 96 ± 5.3 | 95 ± 6.6 | 95 ± 4.1 | 96 ± 4.9 | 96 ± 4.1 | 0.017 |
| Systolic blood pressure on admission, mm/Hg, mean ± SD | 130 ± 22.9 | 134 ± 25.4 | 130 ± 24.3 | 133 ± 17.7 | 130 ± 23.4 | 0.401 |
| Complication, n (%) Without complication Major bleeding Thrombosis Bleeding + thrombosis |
383 (86.7) 34 (7.7) 21 (4.8) 4 (0.9) |
140 (80.9) 20 (11.6) 12 (6.9) 1 (0.6) |
16 (84.2) 3 (15.8) 0 (0) 0 (0) |
98 (87.5) 6 (5.4) 5 (4.5) 3 (2.7) |
129 (93.5) 5 (3.6) 4 (2.9) 0 (0) |
0.022 |
| Death, n (%) | 119 (26.9) | 60 (34.7) | 7 (36.8) | 35 (31.3) | 17 (12.3) | <0.001 |
Table 3.
Inflammatory parameters on admission according to vaccination status.
| Overall, N=442 |
Unvaccinated, n=173 |
1 dose, n=19 |
2 doses, n=112 | 3 doses, n=138 | p | |
|---|---|---|---|---|---|---|
| WBC count*, mean ± SD | 7.1 ± 3.77 | 7.3 ± 4.39 | 5.8 ± 1.82 | 7.1 ± 3.51 | 7.0 ± 3.30 | 0.371 |
| Ly count*, median (IQR) | 0.93 (0.70) | 0.84 (0.67) | 0.95 (0.54) | 0.91 (0.73) | 1.0 (0.66) | 0.207 |
| Hgb, g/L, mean ± SD | 104 ± 17.3 | 103 ± 19.6 | 99 ± 16.4 | 106 ± 16.0 | 104 ± 15.0 | 0.213 |
| D-dimer, mg/L, median (IQR) | 1.4 (1.72) | 1.89 (2.30) | 1.64 (1.59) | 1.30 (1.77) | 1.22 (1.05) | 0.073 |
| CRP, mg/L, median (IQR) | 43.1 (82.98) | 57.1 (98.05) | 45.9 (85.5) | 45.5 (72.5) | 25.9 (63.45) | <0.001 |
| Ferritin, µg/L, median (IQR) | 923.3 (1806.48) | 1108.0 (1801.80) | 1557.3 (1748.3) | 753.0 (1678.1) | 624.8 (1287.0) | <0.001 |
| Fibrinogen, g/L, mean ± SD | 4.9 ± 1.61 | 5.1 ± 1.76 | 5.5 ± 1.52 | 5.1 ± 1.5 | 4.8 ± 1.48 | 0.127 |
| Albumin, g/L, mean ± SD | 36 ± 5.8 | 34 ± 6.0* | 36 ± 6.7 | 36 ± 6.0 | 37 ± 4.6 | <0.001 |
*WBC - white blood cells, Ly – Lymphocyte, * multiply by 1 ×109/L, CRP – C reactive protein IL-6 - interleukin-6; **Post hock analysis: CRP: unvaccinated vs. 3 doses p<0.001, 2 doses vs. 3 doses p=0.001; Feritin: unvaccinated vs. 2 doses p<0.001, unvaccinated vs. 3 doses p<0.001, 1 doses vs. 3 doses p=0.027; Albumini: unvaccinated vs. 2 doses p=0.046, unvaccinated vs. 3 doses p<0.001.
Table 4.
Maximum values of inflammatory factors depending on vaccination status.
| Overall, N=442 |
Unvaccinated, n=173 |
1 dose, n=19 |
2 doses, n=112 | 3 doses, n=138 | p | |
|---|---|---|---|---|---|---|
| WBC max* count, mean ± SD | 12.4 ± 8.05 | 13.5±7.95 | 12.8±6.36 | 13.4±9.06 | 10.2±7.06 | 0.001 |
| Ly min** counts, median (IQR) | 0.6 (0.69) | 0.49 (0.65) | 0.47 (0.59) | 0.56 (0.67) | 0.80 (0.62) | <0.001 |
| Ly max counts, median (IQR) | 1.25 (4.47) | 1.27 (1.05) | 1.18 (0.71) | 1.20 (0.83) | 1.25 (0.80) | 0.701 |
| D-dimer max, mg/L, median (IQR) | 2.16 (3.88) | 2.9 (4.81) | 2.19 (1.98) | 2.20 (3.80) | 1.42 (2.54) | 0.002 |
| CRP max, mg/L, median (IQR) | 78.6 (153.3) | 109.3 (149.30) | 100.3 (153.3) | 77.85 (181.88) | 37.8 (94.78) | <0.001 |
| Ferritin max, µg/L, median (IQR) | 1277.8 (3322.1) | 1976.2 (3853.70) | 2309.8 (3011.8) | 1104.4 (3448.8) | 766.3 (1893.4) | <0.001 |
| Fibrinogen max, g/L, mean ± SD | 5.6 ± 1.82 | 5.7 ± 1.89 | 6.4 ± 1.69 | 5.8 ± 1.78 | 5.1 ± 1.69 | 0.001 |
| IL6 max, pg/ml, median (IQR) | 49.1 (164.25) | 49.1 (231.25) | 51.75 (71.82) | 64.9 (186.84) | 36.2 (190.61) | 0.808 |
WBC white blood cells, Ly – Lymphocyte counts, *max – maximum values during hospitalization, **minimal values during hospitalization. Post hock analysis: Le max.: unvaccinated. vs. 3 doses p=0.002, 2 doses vs. 3 doses p=0.008. Ly min.: unvaccinated vs. 3 doses p<0.001, 1 doses vs. 3 doses p=0.013, 2 doses vs. 3 doses p=0.001. D-dimer max.: unvaccinated vs. 3 doses p<0.001, 2 doses vs. 3 doses p=0.019. CRP max.: unvaccinated vs. 3 doses p<0.001, 1 doses vs. 3 doses p=0.029, 2 doses vs. 3 doses p<0.001. Ferritin max.: unvaccinated vs. 2 doses p=0.004, 0 doses vs. 3 doses p<0.001, 1 doses vs. 3 doses p=0.002. Fibrinogen max.: unvaccinated vs. 3 doses p=0.016, 1 doses vs. 3 doses p=0.024, 2 doses vs. 3 doses p=0.010.
Table 5.
Univariate Cox proportional hazards regression analysis of predictors of lethal outcome.
| B | p | HR | CI 95% | |
|---|---|---|---|---|
| Age | 0.025 | 0.001 | 1.025 | 1.010-1.040 |
| Male | -0.047 | 0.808 | 0.954 | 0.653-1.394 |
| Hypertension | 0.303 | 0.288 | 1.354 | 0.774-2.371 |
| Diabetes | 0.202 | 0.300 | 1.224 | 0.835-1.794 |
| Cardiomyopathy | 0.876 | <0.001 | 2.400 | 1.666-3.458 |
| Cerebrovascular disease | 0.471 | 0.115 | 1.604 | 0.892-2.874 |
| Malignancy | -0.044 | 0.877 | 0.957 | 0.546-1.676 |
| COPD | 0.021 | 0.968 | 1.021 | 0.375-2.776 |
| The X-ray signs of pneumonia, n (%) Withut pneumona Unilateral pneumonia Bilateral pneumonia |
- 0.913 0.586 |
- 0.191 <0.001 |
- 3.299 19.888 |
- 0.551-19.761 6.312-62.664 |
| Vaccination: Unvaccinated 1 dose 2 doses 3 doses |
- -0.216 -0.180 -0.923 |
- 0.603 0.399 0.001 |
- 0.806 0.836 0.397 |
- 0.357-1.817 0.550-1.268 0.231-0.683 |
| Antivirotic | -0.365 | 0.253 | 0.694 | 0.372-1.298 |
| RegenCov | -0.805 | 0.176 | 0.447 | 0.139-1.435 |
| Duration of dialysis | 0.015 | 0.323 | 1.015 | 0.968-1.044 |
| Complication Without complication Hemorrhage Thrombosis Hemorrhage + thrombosis |
- 0.876 0.515 0.392 |
- <0.001 0.108 0.508 |
- 2.401 1.674 1.480 |
- 1.539-3.745 0.893-3.140 0.463-4.729 |
| WBC od admission | 0.075 | <0.001 | 1.077 | 1.038-1.118 |
| Ly on admission | -0.856 | <0.001 | 0.425 | 0.274-0.660 |
| CRP on admission | 0.006 | <0.001 | 1.006 | 1.004-1.007 |
| IL-6 on admission | 0.001 | 0.024 | 1.001 | 1.000-1.002 |
| Ferritin on admission | 0.001 | <0.001 | 1.001 | 1.001-1.002 |
| Fibrinogen on admission | 0.063 | 0.279 | 1.065 | 0.950-1.193 |
| D dimer on admission | 0.053 | <0.001 | 1.054 | 10.33-1.076 |
| Le max | 0.053 | <0.001 | 1.055 | 1.038-1.071 |
| Ly min | -2.781 | <0.001 | 0.062 | 0.027-0.143 |
| Ly max | -0.371 | 0.024 | 0.690 | 0.500-0.952 |
| D-dimer max | 0.022 | <0.001 | 1.022 | 1.012-1.033 |
| CRP max | 0.007 | <0.001 | 1.007 | 1.005-1.009 |
| Ferritin max | 0.001 | <0.001 | 1.001 | 1.001-1.002 |
| IL6 max | 0.001 | <0.001 | 1.001 | 1.001-1.002 |
*COPD, chronic obstructive pulmonary disease.
Table 6.
Multivariate Cox proportional hazards regression analysis of predictors of lethal outcome.
| B | p | HR | CI 95% | |
|---|---|---|---|---|
| Cardiomyopathy | 1.213 | <0.001 | 3.364 | 1.874-6.040 |
| CRP on admission | 0.004 | 0.005 | 1.004 | 1.001-1.008 |
| CRP max | 0.006 | 0.003 | 1.006 | 1.002-1.010 |
| IL6 max | 0.001 | <0.001 | 1.001 | 1.001-1.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



