
Submitted:
22 November 2023
Posted:
22 November 2023
You are already at the latest version
Abstract
The targeting-Her-2/neu therapy by passive application with trastuzumab is associated with acquired resistance and subsequent metastasis development, attributed to upregulation of tumoral PD-L1 expression and downregulation of Her-2/neu. We aimed to investigate this association, following active immunization with our recently constructed B cell–peptide based Her-2/neu vaccines in both preclinical and clinical settings. Immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and combined positive score (CPS), were applied to evaluate Her-2/neu and PD-L1 expression using a murine syngeneic tumor model for Her-2/neu lung metastases, and tumor biopsies from a gastric cancer patient with disease progression. A significant and concomitant reduction of Her-2/neu and upregulation of PD-L1 expression was observed in the vaccinated mice, after 7 but not after 4 weeks of metastases development. A significant increase of tumor-infiltrating B lymphocytes was observed at both time points. Downregulation of Her-2/neu and upregulation of PD-L1 were observed in a patient’s primary tumor at the disease progression time point but not prior to vaccination (Her-2/neu IHC: 3 to 0, FISH: 4.98 to 1.63; PD-L1 CPS: 0% to 5%). Our results further underline the need for combination therapy by targeting PD-L1 to prevent metastasis formation and immune evasion of Her-2/neu positive and PD-L1 negative tumor cells.
Keywords:
PD-L1
; Her-2/neu
; Expression
; Preclinical and clinical settings
; Immune evasion
; Combination therapy
1. Introduction
Her-2/neu, a member of the epidermal growth factor receptor (EGFR) family, is an attractive tumor-associated target antigen for cancer therapy because of its overexpression and association with aggressive biological cancer phenotypes, reduced survival, poor response to traditional chemotherapy, and consequently unfavorable prognosis [1]. The use of trastuzumab (Herceptin®), a monoclonal antibody (mAb) blocking Her-2/neu downstream signaling and inducing antibody-dependent cellular cytotoxicity (ADCC), has significantly improved the survival rate of patients with Her-2/neu positive carcinomas [2].
Based on the results of the phase III ToGA (trastuzumab for Gastric Cancer) trial [3], cisplatin/fluoropyrimidine plus trastuzumab, with the latter binding to the extracellular domain IV of Her-2/neu, blocking Her-2/neu signaling, and mediating ADCC, has become a standard first-line treatment for patients with Her-2/neu-positive advanced gastric cancers. However, resistance to trastuzumab restricts its therapeutic efficacy in patients with both breast and gastric cancers [4]. PD-L1 is an immune checkpoint expressed on various tumor cells [5], and its binding to its receptor PD-1, which is expressed in various immune cells, including tumor-infiltrating T cells [6], results in immune evasion [4]. Upregulation of PD-L1 in Her-2/neu-expressing tumors is considered a mechanism of acquired resistance to trastuzumab [4].
The success of passive immunotherapy with trastuzumab has paved the way for the identification of B cell peptides/binding epitopes of mAbs for use in active immunization [7]. Using a computer algorithm, we identified and used three single peptides (P4, P6, and P7) and formulated Her2 vaccine (HER-Vaxx), comprising B-cell peptides from the trastuzumab binding site, conjugated to the carrier protein CRM197 and used together with the adjuvant Montanide [8]. By employing a Her-2/neu lung metastasis mouse model [9], the antitumor effect of the vaccine, alone or together with the mimotope of pertuzumab, as a multi-peptide vaccine, was recently shown [9]. In a phase 1b dose-escalation study (NCT02795988), HER-Vaxx was shown to be safe and to prolong progression-free survival in patients with Her2-overexpressing gastric/gastro-esophageal junction (GEJ) cancer (GC) [10]. Based on the success of this evaluation, the highest dose (50 µg) of the vaccine was selected and being evaluated in a phase II randomized controlled trial to compare the effects of the vaccine plus chemotherapy versus chemotherapy alone. The vaccination has shown a robust anti-HER-2/neu IgG antibody response and a statistically significant overall survival benefit in the vaccinated patients compared to the chemotherapy alone-treated patients [11]. In a Phase 2 expansion trial, we could now show that Her-2/neu antibodies correlate with the reduction of tumor size in patients with GEJ adenocarcinoma [12]. Considering the fact that pertuzumab, an additional therapeutic mAb against Her-2/neu, is used simultaneously together with trastuzumab for the treatment of patients with metastatic Her-2/neu-overexpressing breast cancer, we have formulated a multi B cell-peptide vaccine comprising HER-Vaxx and the mimotope/binding epitope of pertuzumab. This vaccine showed a significant prevention of Her-2/neu-expressing lung metastases formation in a mouse model, in association with upregulation of PD-L1 and downregulation of Her-2/neu expression in the tumors of the treated mice [9,13].
Here, we aimed to further investigate the association observed in the preclinical setting. Additionally, we took this aim one step further to examine the occurrence of such observations in a clinical setting, by examining the primary tumor of a patient from the phase 1b trial of HER-Vaxx (NCT02795988), who had disease progression after prolonged treatment with the HER-Vaxx. The comparison of Her-2/neu-targeted vaccination in both clinical and preclinical settings further shed light on the potential immune evasion after targeting the receptor, further emphasizing the effective tumor elimination and prevention of tumor immune evasion by combination therapy.
2. Results
Her-2/neu-targeted therapy upregulates PD-L1 expression in association with loss of Her-2/meu expression - preclinical observation
We formulated a multi-peptide vaccine for targeting the binding sites of trastuzumab and Pertuzumab, by HER-Vaxx and a B cell epitope (mimotope; JTMP), respectively [8]. Applying a mouse model of Her-2/neu lung metastasis, we previously demonstrated that 4 weeks after vaccination with a multi-peptide vaccine, a significant decrease in the size of metastasized lungs was observed [9]. We further showed that the antitumor effect was associated with upregulation of PD-L1 and downregulation of Her-2/neu expression, reflected by a significant ratio of PD-L1 positive to Her-2/neu positive tumors in the lungs [9].
In this study, we aimed to further investigate the observed upregulation of PD-L1 associated with the loss of Her-2/neu expression at the cellular level. Mice were either only tail-vein injected with 5 × 104 of BALB/c-derived mammary carcinoma cells expressing human Her-2/neu, that is, control mice, or actively immunized with the multi-peptide vaccine (HER-Vaxx plus JTMP, 50 µg/dose) [9] prior to tail vein injection of the tumor cells. To examine the kinetic of the previously observed upregulation of PD-L1 and downregulation of Her-2/neu expression, the control and treated mice were sacrificed 30 and 45 days after the injection and their lungs were excised for evaluation of PD-L1 and Her-2/neu expression levels. RT-PCR was performed to evaluate the level of transcribed mRNA of both proteins in metastasized lungs. As shown in Figure 1, at 30 days post-injection, similar ratios of PD-L1 to Her-2/neu RNA were observed in control mice and in mice actively immunized with the multi-peptide vaccine. However, 45 days after tumor cell injection, the ratio of PD-L1 to Her-2/neu RNA was significantly higher in vaccinated mice than in control mice, indicating a significant upregulation of PD-L1 and/or downregulation of Her-2/neu at this time point. The significantly increased ratio of PD-L1 to Her-2/neu RNA, 45 but not 30 days after tumor cell injection, is in line with our previous observation showing a delayed immunological response to vaccination [9].
To examine the surface expression of PD-L1 and Her-2/neu as a result of their transcriptional upregulation and downregulation, respectively, tumor cells from the lungs of the control and vaccinated mice from the 45-day post-injection time point (Figure 1) were evaluated by IHC staining of PD-L1 and Her-2/neu. As shown in Figure 2, the vaccination resulted in the upregulation of PD-L1 protein expression (Figure 2b, e) concomitant with the downregulation of Her-2/neu protein expression (Figure 2c, f) in the same tumors. The regions of the same tumor with increased levels of PD-L1 expression showed a loss of Her-2/neu expression.
To further evaluate the metastasized lungs, they were stained for macrophages (F4/80) and B cells (CD79b). As shown in the Figure 3A, no significant difference in the F4/80 positive areas was observed in the metastasized lungs of the control and vaccinated mice, at both time points, suggesting no increased infiltration of the lungs with macrophages at the evaluated time points.
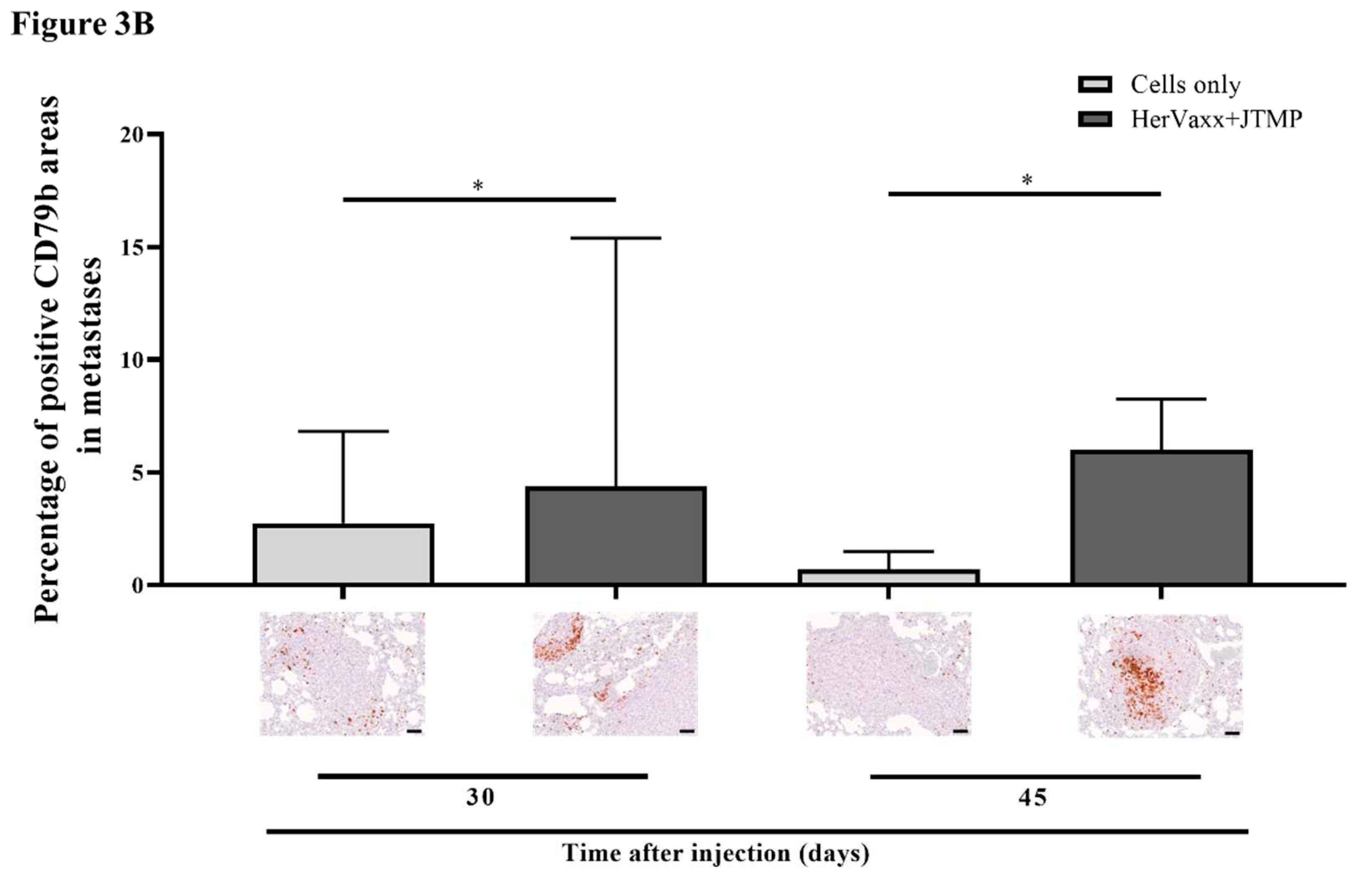
We next also stained the lungs for CD79b+ cells. Compared to the control mice, significantly more area stained positive for B cells at both time points were observed in the vaccinated mice lungs (Figure 3B), indicating recruitment of B cells in the metastasized lungs following vaccination.
These results suggest an associated upregulation of PD-L1 expression in conjunction with downregulation of Her-2/neu expression following Her-2/neu therapy with the examined multipeptide vaccine in the employed preclinical setting. Furthermore, the association does not seem to be linked to infiltrating F4/80+ macrophages and CD79b+ B cells.
The above observation tempted us to evaluate the occurrence of the same phenomenon in the primary tumor of a patient enrolled in the Her-Vaxx phase Ib trial [10], who had disease progression at the end of the treatment and had developed a new Her-2/neu negative metastatic lesion concomitant with the loss of Her-2/neu expression in the primary tumor [10].
Treatment with HER-Vaxx is associated with upregulation of PD-L1 expression in concomitance with downregulation of Her-2/meu expression – clinical observation
The dose-escalation trial NCT02795988 for the evaluation of HER-Vaxx included an adult patient who was diagnosed with T4N3M1 stage IV Her-2/neu +++ adenocarcinoma of the stomach with four target lesions (2x liver and 2x lymph) and five non-target lesions and received, in addition to cisplatin-5FU chemotherapy, a total of seven vaccinations (50µg dose). During the course of the vaccination, the patient responded to the vaccine and generated high levels of vaccine-induced antibodies against Her-2/neu, with antibody levels rising from 30 ng/ml on day 0 to 2000 ng/ml, after three vaccinations [10]. The strong antibody response in this patient, together with cellular responses, reflected by high Th1 cytokine (IFNγ/IL-10, and TNFα/IL-10) ratios, correlated with the patient’s increase of progression-free survival and tumor reduction [10]. After 182 days of treatment, the patient had a partial response (PR) for target lesions with a 71% reduction in the sum of diameters (SOD) from 177 mm to 52 mm, and a complete response (CR) for four of five non-target lesions. By day 266, the target lesion SOD (nadir) was reduced by 79% (from 177 to 37 mm). However, 350 days after treatment, the patient showed disease progression, and the primary tumor size increased by 16% to 43 mm, according to RECIST 1.1. The patient also developed a newly identified metastatic lesion in the stomach, which was Her-2/neu negative [10], suggesting immune evasion of the metastatic tumor during Her-2/neu therapy. The patient’s primary tumor at the pre- and post-treatment time points was retrospectively assessed for PD-L1 and Her-2/neu expression.
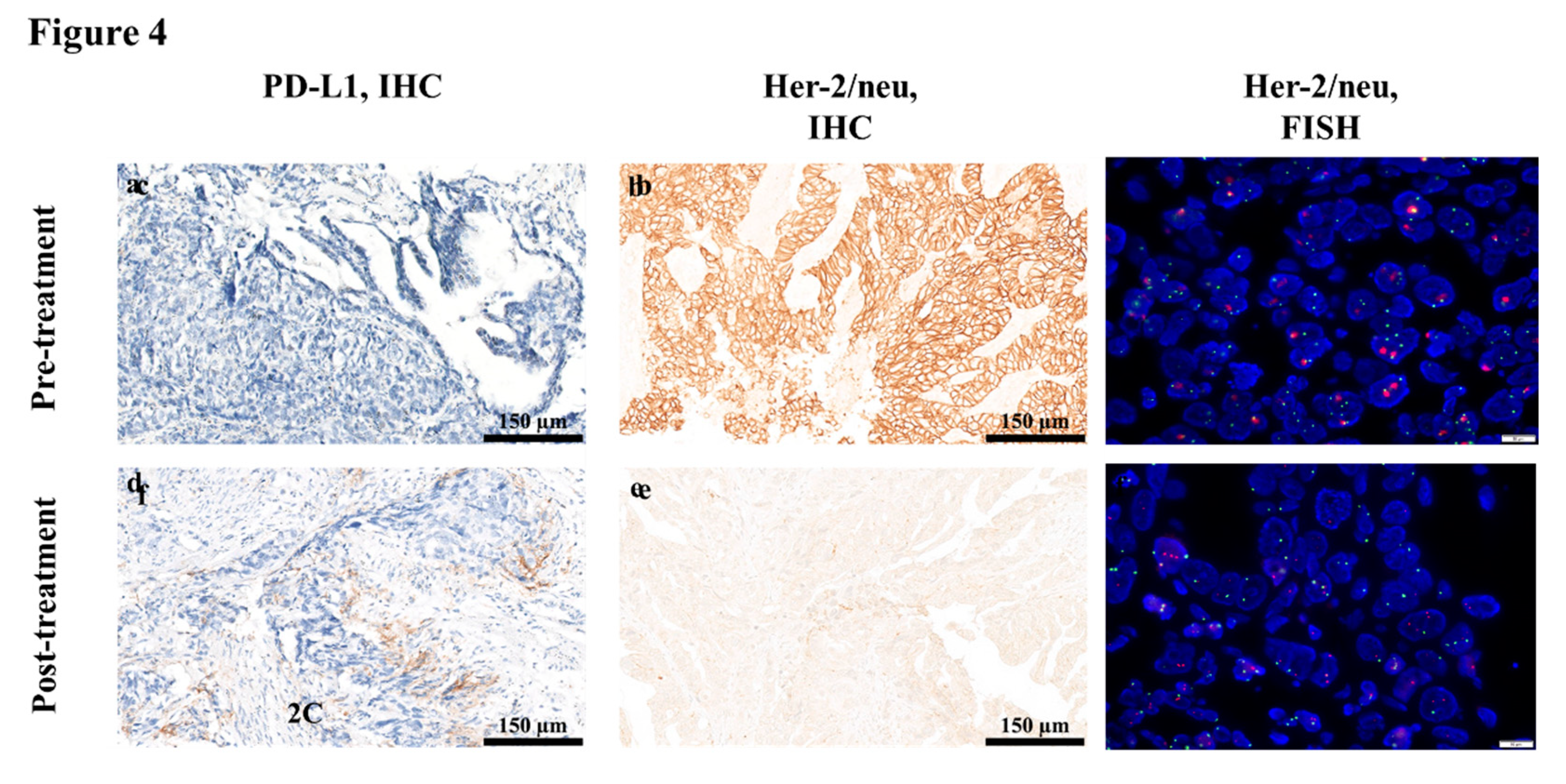
The assessment of pre-treatment (baseline) level of PD-L1 expression in the patient was negative (0%; CPS) (Figure 3a), whereas the Her-2/neu status was 3+ overexpression (IHC) (Figure 3b) with a Her-2/neu / CEP17 (FISH) ratio of 4.98 (Figure 3c). In contrast, post-treatment evaluation of PD-L1 and Her-2/neu expression in the patient’s primary tumor showed 5% PD-L1 expression (CPS) (Figure 3d), and Her-2/neu status of 0 (IHC) (Figure 3e) with a Her-2/neu / CEP17 ratio of 1.63 (FISH; Figure 3f).
Figure 4.
PD-L1 and Her-2/neu status in the primary tumor of the referenced patient. The levels of PD-L1 protein surface expression were assessed by IHC staining of the patient's primary tumor, before (a) and after treatment (d). The levels of Her-2/neu protein surface expression were assessed by immunohistochemistry (IHC) staining and by fluorescent in situ hybridization (FISH) of the patient's formalin-fixed paraffin-embedded gastric primary tumor, before (b, c) and after treatment (e, f). .
Figure 4.
PD-L1 and Her-2/neu status in the primary tumor of the referenced patient. The levels of PD-L1 protein surface expression were assessed by IHC staining of the patient's primary tumor, before (a) and after treatment (d). The levels of Her-2/neu protein surface expression were assessed by immunohistochemistry (IHC) staining and by fluorescent in situ hybridization (FISH) of the patient's formalin-fixed paraffin-embedded gastric primary tumor, before (b, c) and after treatment (e, f). .
These results indicated upregulation of PD-L1 and downregulation of Her-2/neu in the reference patient, who had disease progression, following Her-2/neu-targeting vaccination with HER-Vaxx.
3. Discussion
Upregulation of PD-L1 following treatment with trastuzumab and recruitment of immune effector cells, mediating antibody-dependent cell cytotoxicity (ADCC), and stimulation of IFNγ secretion [14], as a potential mechanism of resistance to the mAb [14], has been reported in gastric malignancies [15]. In parallel, the loss of Her-2/neu expression following treatment with trastuzumab has been reported among breast cancer patients [16] and patients with gastric or gastroesophageal cancers [17], resulting in the escape of tumor cells from treatment and survival advantage of Her-2/neu negative cancer cells. Here, we demonstrated that vaccination-based Her-2/neu-targeting therapy results in upregulation of PD-L1 and downregulation of Her-2/neu expression in both preclinical and clinical settings.
It has been reported that overexpression of Her-2/neu is associated with downregulation of MHC-I molecules in tumor cells [18], with the latter being essential for tumor recognition by cytotoxic T-lymphocytes (CTLs). The role of IFNγ produced by CTLs and the induction of PD-L1 overexpression has also been demonstrated [19]. Currently, it is unknown whether the upregulation of PD-L1 in the patient’s tumor referenced in this study is associated with upregulation of MHC-I; however, we demonstrated increased levels of Her-2/neu-specific IFNγ production in the patient in the phase 1b trial [10]. Thus, we speculate that the increased levels of IFNγ in the tumor microenvironment may have led to the upregulation of PD-L1 in association with the loss of Her-2/neu expression in the patient’s tumor.
In recent studies, the effect of Her-2/neu targeting by trastuzumab, inhibition of the Akt signaling pathway, and the consequent upregulation of PD-L1 expression have been speculated [14]. In our Phase 1b trial, we reported that vaccination with HER-Vaxx resulted in the induction of polyclonal Her-2/neu-specific antibodies in patients [10]. The induced antibodies, including those in the patient referenced in this study, had the capacity to inhibit intracellular Her-2/neu phosphorylation and the downstream phosphorylation of the Akt (Thr 308) signaling pathway in gastric cancer cells NCI-N87 [10]. Thus, these observations suggest that the upregulation of PD-L1, shown here in preclinical and clinical evaluations, is the direct result of the Her-2/neu-targeting therapy in combination with the effects of the tumor microenvironment. The preclinical setting in our study was based on the evaluation of Her-2/neu lung metastases originated from the mammary carcinoma cells D2F2/E2 transfected for expression of Her-2/neu (transgene) [20]. The loss of Her-2/neu and upregulation of PD-L1 expression were observed in the clinical setting, and the relative increase in tumors expressing PD-L1 compared to those expressing Her-2/neu, as well as the relative increase of the respective RNA in the mouse model, point in the same direction.
Pertuzumab, which binds to the dimerization loop in the extracellular domain II of Her-2/neu, has shown a synergistic effect in combination with trastuzumab on the clinical outcome of patients with Her-2/neu-overexpressing breast cancers [21]. Since both trastuzumab and pertuzumab inhibit intracellular Her-2/neu phosphorylation, as well as the phosphorylation of the downstream Akt signaling pathway [22], the upregulation of PD-L1 that was observed following treatment with our multi-peptide vaccine might be the result of a broader binding spectrum of the induced antibodies, thus leading to stronger therapeutic pressure on the receptors expressed on tumor cells [9].
Upregulation of PD-L1 expression upon cellular activation has been reported in lymphocytes, dendritic cells, and myeloid cells including macrophages [23]. In our study, IHC indicated moderate to strong expression of PD-L1 in the metastases of the vaccinated animals. Staining of the metastatic tumor in the animals for Her-2/neu and PD-L1, suggested the increased expression of PD-L1 and the loss of Her-2/neu expression in the same region of the tumor cells (Figure 2e, f), suggesting a direct link between the detected PD-L1 expression in the tumor cells. This is further supported based on the staining of the metastasized mouse lungs showing no increased levels of macrophages.
The role of infiltrating vaccine-induced B cells and T cells in tertiary lymphoid structures and better prognosis has been demonstrated repeatedly [24,25]. In addition to the important role of B cells in humoral immunity, the prognostic role of B cell infiltration of tumors in different cancers has been shown [26,27]. HER-Vaxx is based on B cell epitopes peptides activating naïve B cells which mature toward the production of Her-2/neu-specific antibodies [10,28]. The formulated vaccine also includes the carrier protein CRM197, comprising T cell epitopes, which activate T cells and subsequently enhance production of the peptide-specific antibodies by CD4 T helper cells. Based on our previous preclinical and clinical observations, vaccination with HER-Vaxx induces production of IFNγ [28,29]. Here, the staining of the mice lungs for B cells indicated a significant increase of vaccine-induced infiltration of B cells. While we speculate that the detected B cells are vaccine-induced with the capacity in reducing the tumors size , further evaluations are ongoing to examined whether the detected B cells are PD-L1 positive, i.e. regulatory B cells, which have been reported in various cancers [30,31,32].
Gastric cancer is a highly heterogeneous malignancy, and Her-2/neu overexpression can range from 26% to 79% [33] thus, a more adapted strategy for combination therapy based on the level of Her-2/neu expression might be required. An adapted strategy might also be required in cases of tumors that already have a low expression level of PD-L1 at baseline. The observation from the clinical setting reported in this study is based on the primary tumor of one patient, which is the main limitation of this study, and inclusion of additional cases would further support the proposed combination immunotherapy by vaccination against Her-2 and targeting PD-L1. However, firstly, this indicates a relatively low percentage of vaccinated patients who may progress with the disease and develop new metastatic lesions. Secondly, the similar observations reported based on the preclinical setting further emphasize the potential role of the Her-2/neu-targeted vaccination in promoting tumoral upregulation of PD-L1 and downregulation of Her-2/neu expression, and stress a targeted combination therapy.
4. Materials and Methods
Cell line and culture conditions
D2F2/E2 cells, a BALB/c mouse cell line derived from a mammary carcinoma line that was transfected with the human Her-2/neu gene (transgene) for stable expression of the receptor [20], were kindly provided by Prof. Wei-Zen Wei (Karmanos Cancer Institute, Wayne State University School of Medicine, Detroit, Michigan, USA). The cells were maintained in high-glucose DMEM (supplemented with FBS (10%), NCTC 109 (10%) medium, L-glutamine (200 mM), PenStrep (100 units/ml penicillin, 100 μg/ml streptomycin), Sodium Bicarbonate (5%), 2-mercaptoethanol (10mM) and Sodium bicarbonate (2%).
Preclinical setting
Animals and immunization settings
Female BALB/c mice aged 6–8 weeks at the time of delivery were purchased from Charles River (Germany), maintained under conventional housing conditions, and used in the experiments detailed below. The experiments were approved by the Animal Experimentation Committee of the Medical University of Vienna and the University of Veterinary Medicine and by the Austrian Federal Ministry of Science and Research (BMWF-66.009/0136-WF/V/3b/2017).
Experimental setting: Two groups of mice (n=8/group) were subcutaneously injected (actively immunized) with the multi-peptide vaccine HER-Vaxx and the mimotope of pertuzumab JTMP (conjugated to CRM197 and administered Montanide ISA-51-VG (Seppic, France). The multipeptide vaccine was prepared as described previously [9]. One week after the third subcutaneous injection/immunization, 5x104 of the tumor cells D2F2/E2 were injected into the tail vein of the mice. Control setting: Two additional groups of mice (n=8/group) received PBS by subcutaneous injection and then tail vein injected with 5x104 D2F2/E2 cells. One group of mice from each setting was sacrificed at a 30-day post-injection time point and similarly at a 45-day post-injection time point. Mouse lungs were excised and evaluated for PD-L1 and Her-2/neu expression by Real-Time Polymerase Chain Reaction (RT-PCR) (days 30 and 45) and IHC staining (day 45).
Pathohistological Assessment
For histological examination, the right lung lobes were excised, fixed in a 4% buffered formaldehyde solution, and embedded in paraffin wax. Sections of 2-3µm thickness, covering the entire lung were cut on a sliding microtome and stained with H/E. IHC staining was performed using primary antibodies against Her-2/neu, PD-L1, F4-80, and CD79b using an autostainer (Lab Vision AS 360, Thermo Scientific, Fremont, USA). Details regarding primary antibodies, dilution, antigen retrieval, secondary antibodies, chromogen, and counterstain are presented in the supplementary Table S1.
An experienced pathologist blinded to the treatment regimens evaluated the HE-stained lungs in a descriptive manner using an Olympus BX-53 microscope (Olympus). Images of Her-2/neu- and PD-L1-stained lung sections were taken with an Olympus DP26 camera (10x objective lens) and evaluated using the open-source software FIJI in ImageJ (RRID: SCR_003070) [34]. Adobe Photoshop (RRID: SCR_014199) 2021 was used for white balance and arrangement of representative images. To quantify CD79b and F4/80 expression, slides were scanned using a PANNORAMIC Scan II from 3DHISTECH and saved as MRXS files. Analysis of IHC staining was performed with QuPath (version 0.4.3) by a pathologist blinded to the treatment regimens. For each lung all metastases were annotated and the area above a defined DAB threshold was measured. Representative pictures for figures were exported using the snapshot function of CaseViewer (Build, version 2.4.0.119028).
Assessment of PD-L1 and Her-2/neu expression by RT-PCR
A portion of the lungs from the control and immunized mice was homogenized and used for isolation of total RNA, using the RNeasy kit (QIAGEN, Germany) according to the manufacturer’s instructions. Isolated RNA was quantified using an ND-1000 Spectrophotometer (Nanodrop Technologies Inc., Wilmington, USA). One microgram of total RNA was used for the preparation of cDNA using the iScript™ cDNA Synthesis Kit (Bio-Rad, USA) as specified by the manufacturer.
RT-PCR was performed to measure the relative mRNA expression of PD-L1 and Her-2/neu. The mouse housekeeping gene β-actin was used as an internal control to measure the relative expression of the examined genes, using the 2-ΔCt method. Briefly, SsoAdvanced™ Universal SYBR Green Supermix kit (Bio-Rad, USA) was used for the RT-PCR reactions, using the following primers: mouse PD-L1 (Accession #NM_021893.1; Forward: 5’-TGCGGACTACAAGCGAATCACG-3,’ reverse: 5’-CTCAGCTTCTGGATAACCCTCG-3’), human Her-2/neu (Accession #NM_001382796.1; Forward:5’-GCACAGACATGAAGCTGCG-3,’ Reverse:5’- GTGGGCAGGTAGGTGAGTTC-3’), and mouse β-actin (Accession #XM_021163894.2; Forward:5’- GATCAAGATCATTGCTCCTCCTGA-3,’ Reverse:5’- CAGCTCAGTAACAGTCCGCC-3’). PCR reactions, in total volume of 10µl, included 5µl SsoAdvanced SYBR Green reaction mix (Bio-Rad, Hercules, CA), 0.25µl of each primer at a concentration of 20µM, 3µl of nuclease-free water and 1.5µl of the prepared cDNA. RT-PCR reactions were carried out on a CFX Connect Real-Time System (Bio-Rad) under the following conditions: one cycle at 95⁰C for 2 min, 40 cycles at 95⁰C for 15s and 60⁰C for 30s. This was followed by a dissociation stage (melting curve) at 65⁰C for 30s and cycles of 5s starting at 65⁰C, raising 0.5⁰C per cycle. Following amplification, Ct values were obtained using CFX Manager software 3.1 (Bio-Rad).
Clinical setting
The phase 1b dose-escalation trial (IMU.ACS.001, NCT02795988)
The completed trial NCT02795988 evaluated different doses of HER-Vaxx (10 µg, 30 µg, and 50 µg of the vaccine peptide P467) and enrolled 14 patients with Her-2/neu-overexpressing metastatic or advanced adenocarcinoma of the stomach or GEJ. Among the enrolled patients, 11 (10 µg, n=3; 30 µg, n=5; 50 µg, n=3) were evaluated for the assessment of tumor responses [10]. The trial was a multicenter study conducted in Georgia, Moldova, Taiwan and Thailand [10]. Pre- and post-treatment biopsies from the primary tumor sites of the patient referenced in this study were assessed for PD-L1 and Her-2/neu expression by immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and combined positive score (CPS).
Biopsies from the vaccinated patient
In a clinical study, one patient showed disease progression. Four-micrometer-thick slides were cut from the formalin-fixed paraffin-embedded (FFPE) blocks with the patient’s biopsies before treatment on day 0 and at the end of the treatment on day 350 (following three single-dose vaccine injections and four booster vaccinations for long-term maintenance). PD-L1 immunohistochemical (IHC) staining was carried out using the Dako PD-L1 immunohistochemistry 22C3 pharmDx assay (Dako, Carpinteria, CA), including appropriate controls, according to the manufacturer’s instructions. PD-L1 assessment was based on CPS, which had been similarly applied in two recent phase III trials evaluating the effect of nivolumab [35] and pembrolizumab [36] in patients with advanced GC and esophageal adenocarcinoma, respectively. IHC staining for Her-2/neu was performed using the 4B5 mAb (Ventana, Tucson, AZ, USA) for the BenchMarkULTRA system (Ventana). Images of Her-2/neu- and PD-L1-stained lung sections were obtained using a Philips IntelliSite Pathology Solution with an Ultra-Fast Scanner. Fluorescence in situ hybridization (FISH) for the evaluation of Her-2/neu gene amplification was performed as described previously [10].
Statistical analysis
In the animal experiment, subgroups of control animals and vaccinated animals, both injected with 5 × 104 tumor cells, were sacrificed on days 30 and 45 after injection. RNA levels of PD-L1 and Her-2/neu were measured relative to β-actin expression. The ratio of the relative RNA expression of PD-L1 to that of Her-2/neu was calculated. These values were statistically evaluated using a generalized linear model with group (controls/vaccinated) and days (30 and 45) as between factors, together with their interaction, assuming a log-normal distribution. Comparisons of the ratios of PD-L1 to Her-2/neu between the groups at the two time points were obtained from linear contrasts by applying Sidak correction. Similarly, the ratio of PD-L1 to Her-2/neu positive tumors in the lungs was statistically compared to control animals by applying a generalized linear model and linear contrasts. Statistical significance was set at p < 0.05. The analysis was performed using Stata 17 (StataCorp, College Station, Tulsa, USA).
5. Conclusions
Overall, the observed tumoral upregulation of PD-L1 and downregulation of Her-2/neu expression, based on the comparison of the same vaccine in both preclinical and clinical settings is clinically relevant for the elimination of tumor cells with a PD-L1 positive/Her-2/neu negative status, preventing new metastasis and immune evasion. Accordingly, two clinical trials have been planned (Imugene Limited, Sydney, Australia) to assess: first, HER-Vaxx in combination with chemotherapy or the anti-PD-1 antibody pembrolizumab in patients with Her-2/neu-overexpressing gastric cancer who have failed treatment with trastuzumab, and, second, HER-Vaxx in combination with chemotherapy +/- the anti-PD-L1 antibody avelumab in patients with Her-2/neu-overexpressing gastric cancer.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Details regarding primary antibodies, dilution, antigen retrieval, secondary antibodies, chromogen, and counterstain, used for the pathohistological assessments.
Author Contributions
Conceptualization, J.T., U.W.; Validation, J.T., S.H., D.S-C.L., A.J.G., M.K., U.W.; Formal analysis, J.T., S.H., D.S-C.L., M.K.; Methodology, J.T., S.H., D.S-C.L.; Investigation, J.T., S.H., A.J.G., U.W.; Resources, Y.C., A.J.G., U.W.; Data curation, J.T., S.H., D.S-C.L., M.K.; Writing-original draft preparation, J.T., U.W.; Reviewing and/or editing, J.T., S.H., E.G.S., N.J.E., C.C.Z., A.J.G, M.K., U.W.; Visualization, J.T., S.H., A.J.G; Supervision, J.T., Y.C., A.J.G., U.W.; Project administration, J.T., A.J.G., U.W. Finalization of the manuscript, J.T., M.K., U.W.
Funding
1) The preclinical studies shown in the submitted manuscript were supported until 31.10.2020 by a research grant from Imugene Ltd. and thereafter by the Medical University of Vienna. 2) The clinical study (NCT02795988) and the evaluations shown in the submitted manuscript were sponsored by Imugene Ltd.
Institutional Review Board Statement/Statement of Ethics
The trial NCT02795988 was registered at ClinicalTrials.gov, and conducted in accordance with the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences 2002), the Guidelines for GCP (ICH 1996), and the Declaration of Helsinki (World Medical Association 1996, 2008).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding authors.
Acknowledgments
The authors cordially thank, 1) Dr. Anthony J. Good for coordinating the availability of the FISH and IHC data relating to the referenced patient reported here, and 2) Mrs. Petra Kodajova for the preparation and IHC staining of sections with the mouse lungs.
Conflicts of Interest
J.T., S.H, M.R., D.S-C.L.,Y.C., E.G-S., L.K., M.K., A.J.G.: declare no potential conflicts of interest; N.J.E., S.Y.: Imugene Limited (Employment); C.C.Z.: Consultation (Athenex, MSD, Imugene Limited (until Sept 2018), AstraZeneca, Servier, Eli Lilly); Institutional (Eli Lilly, BMS, MSD, Pfizer, AstraZeneca, Merck Amgen, Servier, Takeda, Daiichi Roche, Boehringer, Celgene, Halozyme); U.W.: Imugene Limited (Consultation, until Sept 2018); GSK, Pfizer, Themis (Funding to the Institute).
References
- Arienti, C.; Pignatta, S.; Tesei, A. Epidermal Growth Factor Receptor Family and its Role in Gastric Cancer. Front Oncol 2019, 9, 1308. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Lv, M.; Jiang, H.; Wang, Y.; Yu, S.; Li, W.; Yu, Y.; Liu, T. A prospective observational study on the optimal maintenance strategy in HER2-positive advanced gastric cancer treated with trastuzumab-based therapy. J Cancer Res Clin Oncol 2020, 146, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Vivekanandhan, S.; Knutson, K.L. Resistance to Trastuzumab. Cancers 2022, 14, 5115. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Teng, F.; Kong, L.; Yu, J. PD-L1 expression in human cancers and its association with clinical outcomes. Onco Targets Ther 2016, 9, 5023–5039. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 pathway: current researches in cancer. Am J Cancer Res 2020, 10, 727–742. [Google Scholar] [PubMed]
- Ladjemi, M.Z.; Jacot, W.; Chardes, T.; Pelegrin, A.; Navarro-Teulon, I. Anti-HER2 vaccines: new prospects for breast cancer therapy. Cancer Immunol Immunother 2010, 59, 1295–1312. [Google Scholar] [CrossRef] [PubMed]
- Tobias, J.; Garner-Spitzer, E.; Drinic, M.; Wiedermann, U. Vaccination against Her-2/neu, with focus on peptide-based vaccines. ESMO Open 2022, 7, 100361. [Google Scholar] [CrossRef] [PubMed]
- Tobias, J.; Drinic, M.; Hogler, S.; Ambroz, K.; Baier, K.; Kodajova, P.; Tomasich, E.; Berghoff, A.S.; Schmid, A.; Garner-Spitzer, E.; et al. Active immunization with a Her-2/neu-targeting Multi-peptide B cell vaccine prevents lung metastases formation from Her-2/neu breast cancer in a mouse model. Transl Oncol 2022, 19, 101378. [Google Scholar] [CrossRef]
- Wiedermann, U.; Garner-Spitzer, E.; Chao, Y.; Maglakelidze, M.; Bulat, I.; Dechaphunkul, A.; Arpornwirat, W.; Charoentum, C.; Yen, C.J.; Yau, T.C.; et al. Clinical and Immunologic Responses to a B-Cell Epitope Vaccine in Patients with HER2/neu-Overexpressing Advanced Gastric Cancer-Results from Phase Ib Trial IMU.ACS.001. Clin Cancer Res 2021, 27, 3649–3660. [Google Scholar] [CrossRef]
- Maglakelidze, M.; Ryspayeva, D.; Bulat, I.; Andric, Z.; Nikolic, I.; Chawla, T.; Nagarkar, R.; Chourdhary, V.; Venkata, G.; Singh, R.K.; et al. A phase 1b/2 open-label study with randomization in phase 2 of Imu-131 Her2/neu peptide vaccine plus standard of care chemotherapy in patients with Her2/neu overexpressing metastatic or advanced adenocarcinoma of the stomach or gastroesophageal junction. Cancer Res 2021, 81, CT107–CT107. [Google Scholar] [CrossRef]
- Tobias, J.; Kundi, M.; Garner-Spitzer, E.; Zielinski, C.; Maglakelidze, M.; Andric, Z.; Petrovic, Z.; Nagarkar, R.; Chawla, T.; Chong, L.; et al. PD-8 HERIZON: A phase 2 study of HER-Vaxx (IMU-131), a HER2-targeting peptide vaccine plus SOC chemotherapy in patients with HER2+ advanced stomach cancer – correlation of the antibody responses and clinical outcome. Ann Oncol 2023, 34, S4. [Google Scholar] [CrossRef]
- Tobias, J.; Drinic, M.; Högler, S.; Schmid, A.; Garner-Spitzer, E.; Kenner, L.; Kundi, M.; Zieleinski, C.; Wiedermann, U. 1676P Active immunization with a multi-peptide B cell vaccine, targeting trastuzumab and pertuzumab binding sites, prevents the formation of HER-2/neu expressing lung metastases. Ann Oncol 2022, 33, S1309. [Google Scholar] [CrossRef]
- Chaganty, B.K.R.; Qiu, S.; Gest, A.; Lu, Y.; Ivan, C.; Calin, G.A.; Weiner, L.M.; Fan, Z. Trastuzumab upregulates PD-L1 as a potential mechanism of trastuzumab resistance through engagement of immune effector cells and stimulation of IFNgamma secretion. Cancer Lett 2018, 430, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Iwatsuki, M.; Yasuda-Yoshihara, N.; Morinaga, T.; Nakao, Y.; Harada, K.; Eto, K.; Kurashige, J.; Hiyoshi, Y.; Ishimoto, T.; et al. Trastuzumab upregulates programmed death ligand-1 expression through interaction with NK cells in gastric cancer. Br J Cancer 2021, 124, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Ignatov, T.; Gorbunow, F.; Eggemann, H.; Ortmann, O.; Ignatov, A. Loss of HER2 after HER2-targeted treatment. Breast Cancer Res Treat 2019, 175, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.; Ryu, M.H.; Park, Y.S.; Ahn, J.Y.; Park, Y.; Park, S.R.; Ryoo, B.Y.; Lee, G.H.; Jung, H.Y.; Kang, Y.K. Loss of HER2 positivity after anti-HER2 chemotherapy in HER2-positive gastric cancer patients: results of the GASTric cancer HER2 reassessment study 3 (GASTHER3). Gastric Cancer 2019, 22, 527–535. [Google Scholar] [CrossRef]
- Maruyama, T.; Mimura, K.; Sato, E.; Watanabe, M.; Mizukami, Y.; Kawaguchi, Y.; Ando, T.; Kinouchi, H.; Fujii, H.; Kono, K. Inverse correlation of HER2 with MHC class I expression on oesophageal squamous cell carcinoma. Br J Cancer 2010, 103, 552–559. [Google Scholar] [CrossRef]
- Garcia-Diaz, A.; Shin, D.S.; Moreno, B.H.; Saco, J.; Escuin-Ordinas, H.; Rodriguez, G.A.; Zaretsky, J.M.; Sun, L.; Hugo, W.; Wang, X.; et al. Interferon Receptor Signaling Pathways Regulating PD-L1 and PD-L2 Expression. Cell Rep 2019, 29, 3766. [Google Scholar] [CrossRef]
- Wei, W.Z.; Shi, W.P.; Galy, A.; Lichlyter, D.; Hernandez, S.; Groner, B.; Heilbrun, L.; Jones, R.F. Protection against mammary tumor growth by vaccination with full-length, modified human ErbB-2 DNA. Int J Cancer 1999, 81, 748–754. [Google Scholar] [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.B.; Im, Y.H.; Im, S.A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol 2020, 21, 519–530. [Google Scholar] [CrossRef]
- Nami, B.; Maadi, H.; Wang, Z. The Effects of Pertuzumab and Its Combination with Trastuzumab on HER2 Homodimerization and Phosphorylation. Cancers 2019, 11, 375. [Google Scholar] [CrossRef] [PubMed]
- Peranzoni, E.; Ingangi, V.; Masetto, E.; Pinton, L.; Marigo, I. Myeloid Cells as Clinical Biomarkers for Immune Checkpoint Blockade. Front Immunol 2020, 11, 1590. [Google Scholar] [CrossRef]
- Qin, M.; Jin, Y.; Pan, L.Y. Tertiary lymphoid structure and B-cell-related pathways: A potential target in tumor immunotherapy. Oncol Lett 2021, 22, 836. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, S. Tertiary lymphoid structures are critical for cancer prognosis and therapeutic response. Front Immunol 2022, 13, 1063711. [Google Scholar] [CrossRef]
- Schaafsma, E.; Jiang, C.; Cheng, C. B cell infiltration is highly associated with prognosis and an immune-infiltrated tumor microenvironment in neuroblastoma. J Cancer Metastasis Treat 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Wouters, M.C.A.; Nelson, B.H. Prognostic Significance of Tumor-Infiltrating B Cells and Plasma Cells in Human Cancer. Clin Cancer Res 2018, 24, 6125–6135. [Google Scholar] [CrossRef]
- Tobias, J.; Jasinska, J.; Baier, K.; Kundi, M.; Ede, N.; Zielinski, C.; Wiedermann, U. Enhanced and long term immunogenicity of a Her-2/neu multi-epitope vaccine conjugated to the carrier CRM197 in conjunction with the adjuvant Montanide. BMC Cancer 2017, 17, 118. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, U.; Garner-Spitzer, E.; Chao, Y.; Bulat, I.; Dechaphunkul, A.; Arpornwirat, W.; Charoentum, C.; Yen, C.J.; Yau, T.; Maglakelidzde, M.; et al. Comprehensive results of a phase Ib study with a HER2/neu B-cell peptide vaccine administered with cisplatin and 5-fluorouracil or capecitabine chemotherapy show safety, immunogenicity and clinical response in patients with HER2/Neu overexpressing advanced gastric cancer. Ann Oncol 2019, 30, v495–v496. [Google Scholar] [CrossRef]
- Michaud, D.; Steward, C.R.; Mirlekar, B.; Pylayeva-Gupta, Y. Regulatory B cells in cancer. Immunol Rev 2021, 299, 74–92. [Google Scholar] [CrossRef]
- Wu, H.; Xia, L.; Jia, D.; Zou, H.; Jin, G.; Qian, W.; Xu, H.; Li, T. PD-L1(+) regulatory B cells act as a T cell suppressor in a PD-L1-dependent manner in melanoma patients with bone metastasis. Mol Immunol 2020, 119, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Mao, Y.; Lv, Y.; Tang, W.; Xu, J. B cells in tumor metastasis: friend or foe? Int J Biol Sci 2023, 19, 2382–2393. [Google Scholar] [CrossRef] [PubMed]
- Palle, J.; Rochand, A.; Pernot, S.; Gallois, C.; Taieb, J.; Zaanan, A. Human Epidermal Growth Factor Receptor 2 (HER2) in Advanced Gastric Cancer: Current Knowledge and Future Perspectives. Drugs 2020, 80, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: an open-source platform for biological-image analysis. Nat Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Campos Bragagnoli, A.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Chao, J.; Fuchs, C.S.; Shitara, K.; Tabernero, J.; Muro, K.; Van Cutsem, E.; Bang, Y.J.; De Vita, F.; Landers, G.; Yen, C.J.; et al. Assessment of Pembrolizumab Therapy for the Treatment of Microsatellite Instability-High Gastric or Gastroesophageal Junction Cancer Among Patients in the KEYNOTE-059, KEYNOTE-061, and KEYNOTE-062 Clinical Trials. JAMA Oncol 2021, 7, 895–902. [Google Scholar] [CrossRef]
Figure 1.
The ratio of PD-L1 to Her-2/neu RNA in metastasized lungs of mice. Mice (n=8/group), either administered with PBS (controls) by injection or actively immunized three times with the multi-peptide vaccine (HER-Vaxx plus the mimotope (JTMP) of pertuzumab), followed by tail-vein injection with tumor cells expressing human Her-2/neu [8,9] and sacrificed on days 30 and 45 following the tumor cells injection. Means and 95% confidence intervals are shown estimated by a generalized linear model with all the time points and both mRNA levels evaluated simultaneously. The ratio of PD-L1 to Her-2/neu RNA from vaccinated and control (tumor cells only) mice were calculated based on the RT-PCR Ct values relative to β-actin, using the formula 2–∆Ct. Comparisons were by linear contrasts (Sidak corrected). (**, p<0.01).
Figure 1.
The ratio of PD-L1 to Her-2/neu RNA in metastasized lungs of mice. Mice (n=8/group), either administered with PBS (controls) by injection or actively immunized three times with the multi-peptide vaccine (HER-Vaxx plus the mimotope (JTMP) of pertuzumab), followed by tail-vein injection with tumor cells expressing human Her-2/neu [8,9] and sacrificed on days 30 and 45 following the tumor cells injection. Means and 95% confidence intervals are shown estimated by a generalized linear model with all the time points and both mRNA levels evaluated simultaneously. The ratio of PD-L1 to Her-2/neu RNA from vaccinated and control (tumor cells only) mice were calculated based on the RT-PCR Ct values relative to β-actin, using the formula 2–∆Ct. Comparisons were by linear contrasts (Sidak corrected). (**, p<0.01).
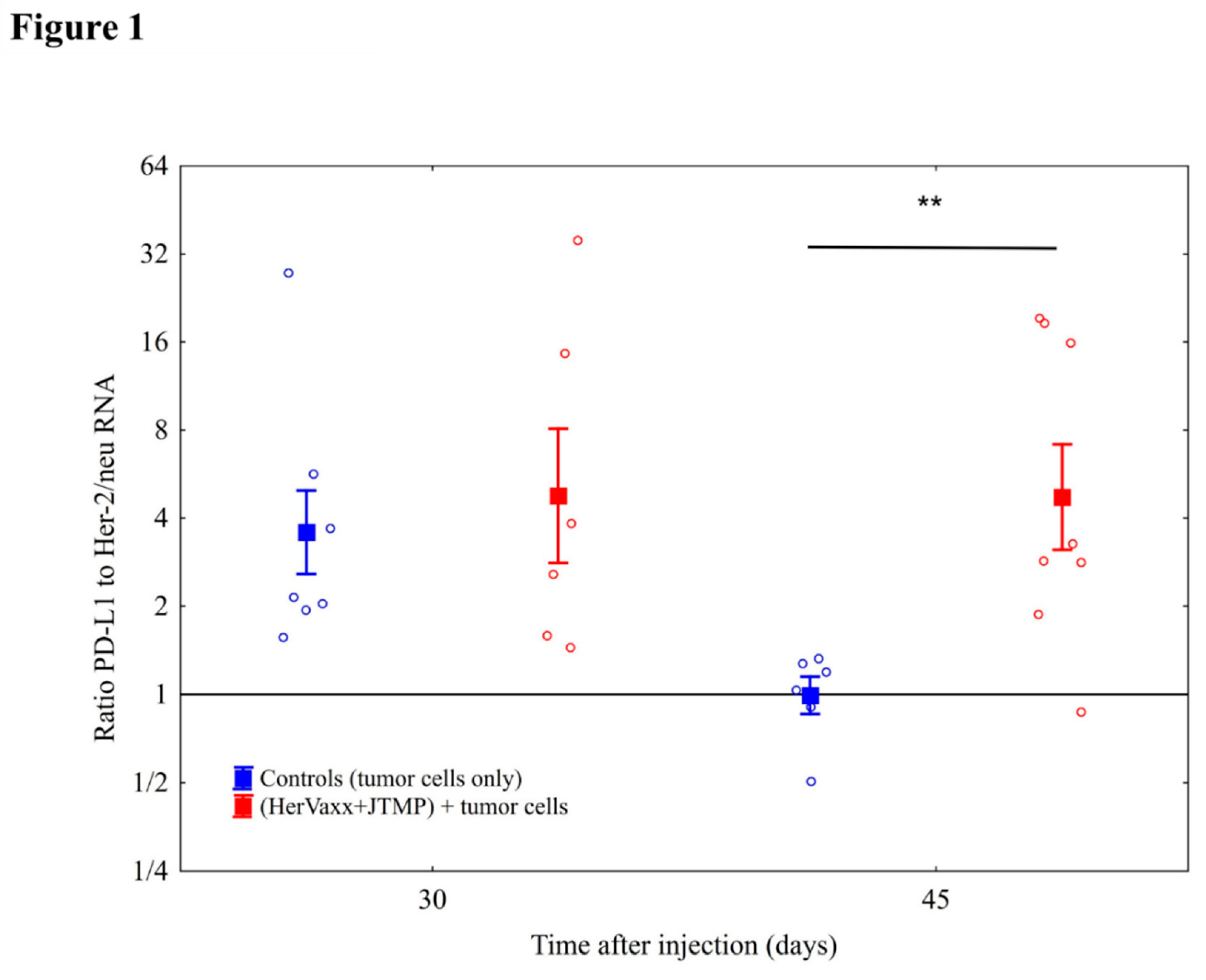
Figure 2.
The protein expression status of PD-L1 and Her-2/neu in metastasized lungs of mice sacrificed at the 45-days post-injection time point. Representative images of a tumor from the metastasized lungs of the mice sacrificed at the 45-days post-injection time point, after H/E staining (a, d), PD-L1 (b, e) and Her-2/neu (c, f) single staining by IHC, are shown for the respective treatments; Control (tumor cells only) and with the multi-peptide vaccine (HER-Vaxx+JTMP).
Figure 2.
The protein expression status of PD-L1 and Her-2/neu in metastasized lungs of mice sacrificed at the 45-days post-injection time point. Representative images of a tumor from the metastasized lungs of the mice sacrificed at the 45-days post-injection time point, after H/E staining (a, d), PD-L1 (b, e) and Her-2/neu (c, f) single staining by IHC, are shown for the respective treatments; Control (tumor cells only) and with the multi-peptide vaccine (HER-Vaxx+JTMP).
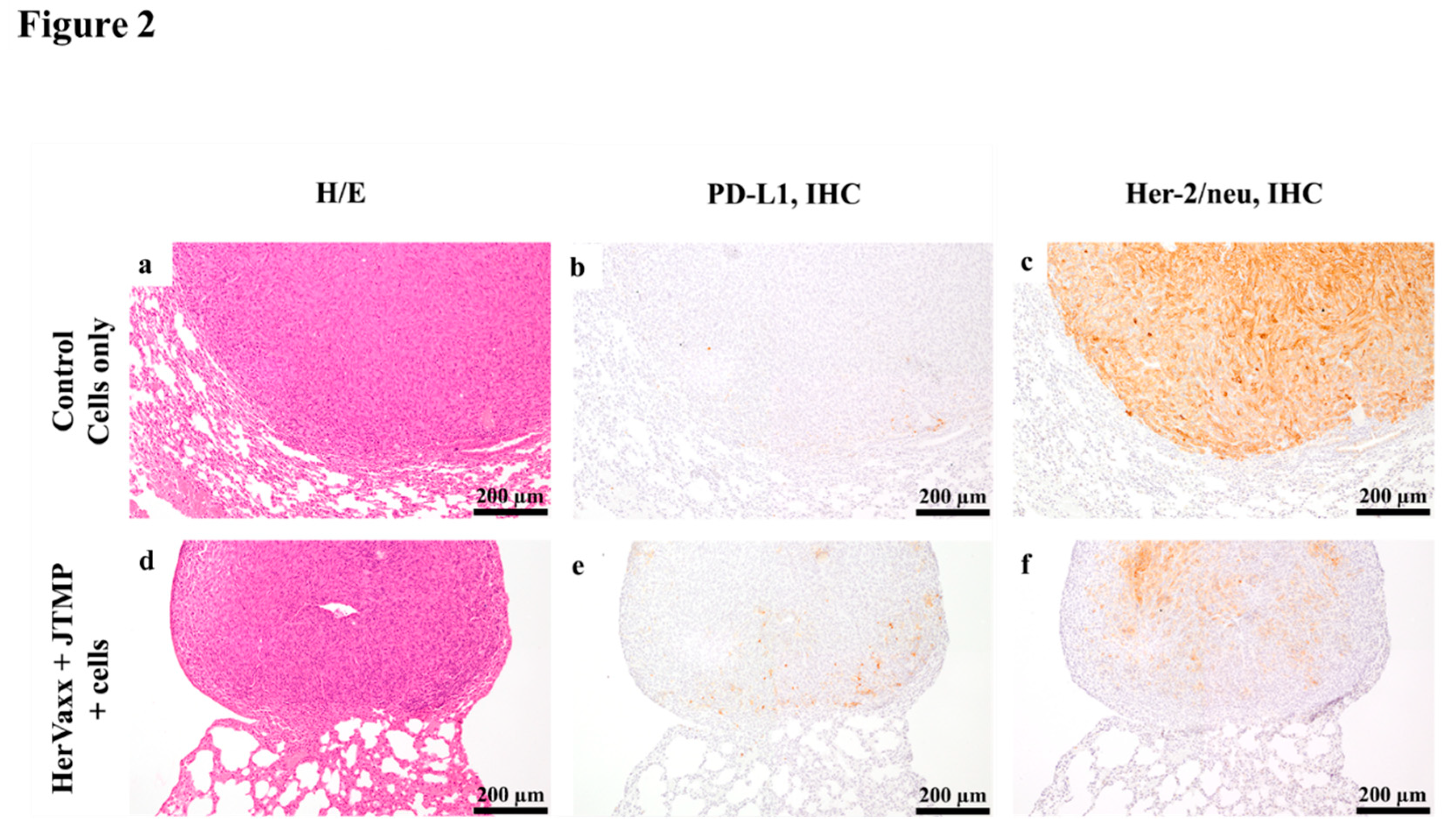
Figure 3A.
Percentage of positive F4/80 (macrophages) areas in the metastasized lungs of mice. Mice were immunized with a multi-peptide vaccine combining both HER-Vaxx and the mimotope of Pertuzumab, followed by tail-vein injection with tumor cells expressing human Her-2/neu and sacrificed at 30 and 45 days following the tumor cells injection [8,9]. Based on F4/80 single staining by IHC, the stained positive areas were assessed and presented as percentages of tumor tissue in the graph’s bars. A representative IHC image, showing the staining levels, is shown under each bar, scale bar = 60µm.
Figure 3A.
Percentage of positive F4/80 (macrophages) areas in the metastasized lungs of mice. Mice were immunized with a multi-peptide vaccine combining both HER-Vaxx and the mimotope of Pertuzumab, followed by tail-vein injection with tumor cells expressing human Her-2/neu and sacrificed at 30 and 45 days following the tumor cells injection [8,9]. Based on F4/80 single staining by IHC, the stained positive areas were assessed and presented as percentages of tumor tissue in the graph’s bars. A representative IHC image, showing the staining levels, is shown under each bar, scale bar = 60µm.
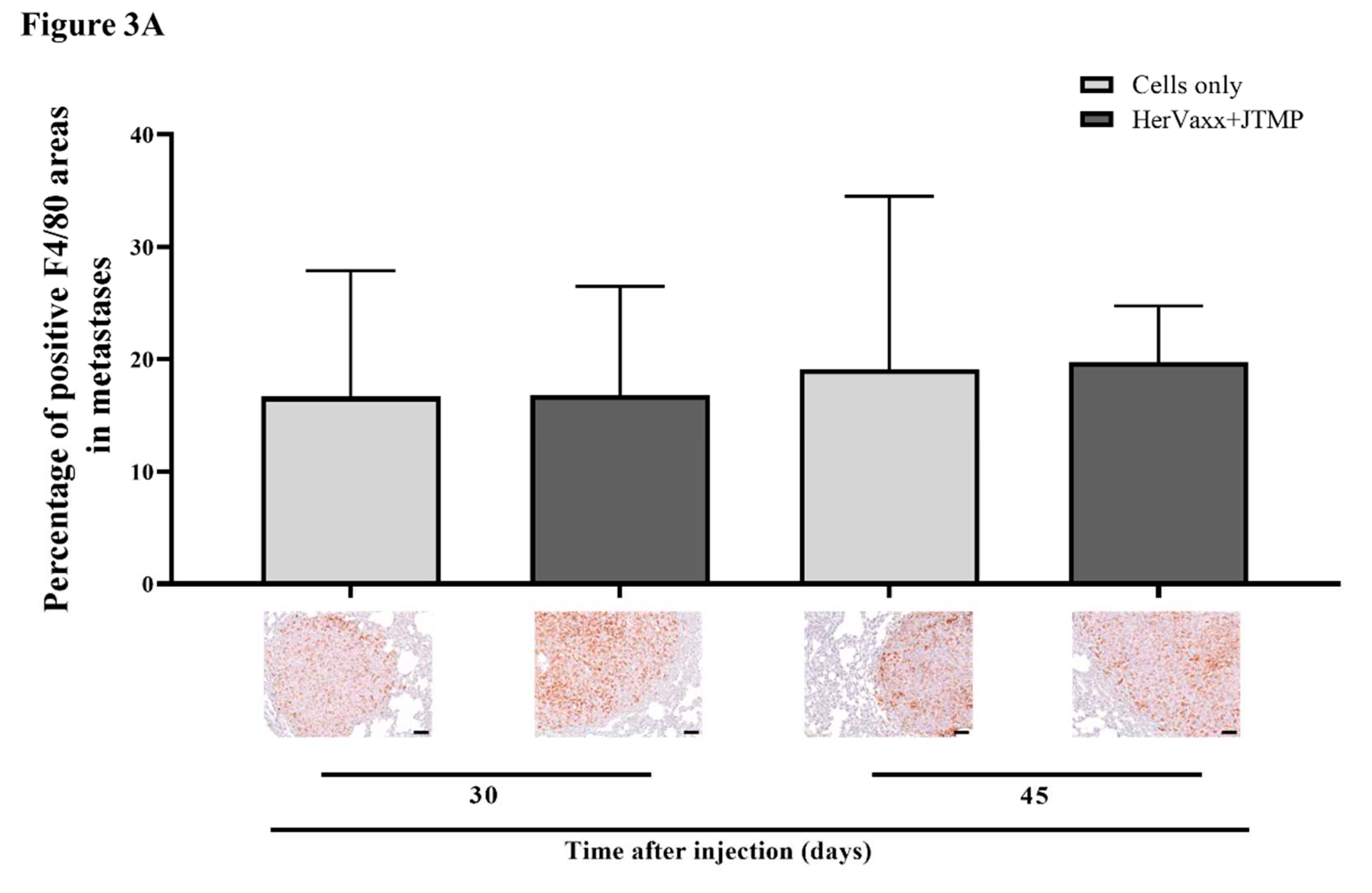
Figure 3B.
Percentage of positive CD79b (B cells) areas in the metastasized lungs of mice. Mice were immunized with a multi-peptide vaccine combining both HER-Vaxx and the mimotope of Pertuzumab, followed by tail-vein injection with tumor cells expressing human Her-2/neu and sacrificed at 30 and 45 days following the tumor cells injection [8,9]. Based on CD79b single staining by IHC, the stained positive areas were assessed and presented as percentages of tumor tissue in the graph’s bars. A representative IHC image, showing the staining levels, is shown under each bar, scale bar = 60µm. .
Figure 3B.
Percentage of positive CD79b (B cells) areas in the metastasized lungs of mice. Mice were immunized with a multi-peptide vaccine combining both HER-Vaxx and the mimotope of Pertuzumab, followed by tail-vein injection with tumor cells expressing human Her-2/neu and sacrificed at 30 and 45 days following the tumor cells injection [8,9]. Based on CD79b single staining by IHC, the stained positive areas were assessed and presented as percentages of tumor tissue in the graph’s bars. A representative IHC image, showing the staining levels, is shown under each bar, scale bar = 60µm. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



