
Submitted:
22 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
(1) Background: China holds the highest esophageal squamous cell carcinoma (ESCC) incidence areas in the world, with some areas of incidence over 100 per 100,000. Despite extensive public health efforts, its etiology is still poorly understood. This study aims to review and summarize past research into potential etiologic factors for ESCC in China. (2) Methods: Relevant observational and intervention studies were systematically extracted from four databases using key terms, reviewed using Rayyan software, and summarized into Excel tables. (3) Results: Among the 207 studies included in this review, 130 studies were focused on genetic etiologic factors, followed by 22 studies focused on dietary-related factors, 18 studies focused on HPV-related factors, and 37 studies focused on other factors. (4) Conclusions: ESCC in China involves a variety of factors including genetic variations, gene-environment interactions, dietary factors like alcohol, tobacco use, pickled vegetables, and salted meat, dietary behavior such as hot food/drink consumption, infections like HPV, poor oral health, gastric atrophy, and socioeconomic factors. Public health measures should prioritize genetic screening for relevant polymorphisms, conduct comprehensive investigations into environmental, dietary, and HPV influences, enhance oral health education, and consider socioeconomic factors overall as integral strategies to reduce ESCC in high-risk areas of China.
Keywords:
esophageal squamous cell carcinoma
; esophageal cancer
; cancer etiology
1. Introduction
The 6th highest mortality from cancer worldwide comes from esophageal cancer, with 544,000 esophageal cancer-related deaths reported in 2020 [1]. Esophageal cancer prognosis is poor; during 2010-2014, the age-standardized 5-year net survival was observed to be 10-30% in most countries [2]. In 2018, newly reported esophageal cancers represented 3.2% of all diagnosed malignancies and 5.3% of all cancer-related mortalities, worldwide [1]. There are two primary types of esophageal cancer: squamous cell carcinoma and adenocarcinoma. Adenocarcinoma is recognized to be the dominant type in the Western world [3], whereas squamous cell carcinoma represents 90% of esophageal carcinomas in Asia, Eastern Europe, and Africa [4]. Over 50% of the world’s esophageal cancer cases were identified in China in 2020, with esophageal squamous cell carcinoma (ESCC) as the dominant histological type [5]. China holds the highest ESCC incidence areas in the world, with some areas of incidence over 100 per 100,000 [6]. The survival rate in China has been estimated to have increased from 20.9% to 30.3% in the past ten years, however, most cases were found in late stages and the prognosis remains quite poor [7]. Despite the extensive public health efforts to investigate ESCC risk factors in China, its etiology is still poorly understood and merits review. To better focus further research, this study aims to systematically review and summarize past research into potential risk factors for ESCC in China.
2. Materials and Methods
A systematic literature search was conducted in the databases PubMed, Web of Science, Cochrane, and EMBASE using combinations of the keywords “risk factor”, “risk factors”, “esophageal squamous cell carcinoma”, “oesophageal squamous cell carcinoma”, “China”, and “Chinese” (Table 1). One reviewer used Rayyan [8] to conduct a study title and abstract review, followed by a full-text review. Included were population studies in English, in humans, in populations in China mainland or Hong Kong, and qualitative or quantitative data on ESCC etiology. Exclusion criteria were studies not in English, populations outside of China mainland or Hong Kong, studies focusing on ESCC diagnosis, screening, treatment, or prognosis, studies focusing on dysplasia or precancerous lesions, animal or cell studies, reviews, case reports, studies without qualitative or quantitative risk factor data on ESCC etiology, and irrelevant studies. The study’s PRISMA diagram is shown in Figure 1. Following a full-text review, each study’s main findings were extracted into Excel at the reviewer’s discretion. Data from multivariate analyses was always reported first; if no multivariate data was available, data from univariate analyses was reported. ArcGIS was used to visualize the study population region according to the Chinese province. A meta-analysis was not conducted due to the incomparability of the studies.
3. Results
3.1. Study characteristics
From 1890 studies identified, following duplicate study removal, title, abstract, and full-text review, a total of 202 studies met the inclusion criteria (Figure 1). By manual search, 5 studies were added following full-text review, resulting in a total of 207 studies included in this review. An overview of included study aim, ethnicity, and study count per province is shown in Table 2 and Table 3, and Figure 2, respectively.
3.2. Study type
According to the risk factors identified in the reviewed studies, risk factors were divided into 15 groups including genetic, gene-environment interactions, family history, HPV, H. pylori., alcohol and smoking, pickled vegetable consumption, salted meat consumption, tea type consumption, fresh fruit and vegetable consumption, other dietary factors, dietary behavior, oral health, environmental factors, and socioeconomic status.
Genetic
An extensive amount of literature reports genetic mechanisms related to ESCC risk. Among the 207 studies included in this review, 141 studies investigated genetically related risk to ESCC (Supplementary materials, Tables S1 and S2). SNPs in more than 151 unique genes and their association with ESCC were investigated (Supplementary materials, Table S1). Among the genetic variants investigated, eight studies found that various TP53 SNPs increased ESCC risk, however with varying statistical significance [9,10,11,12,13,14,15,16]; notably p53 rs1042522 Arg/Arg genotype was reported to increase risk by more than 5 times [9]. Five studies reported significant associations between various SNPs in alcohol metabolism genes ALDH1, ALDH2, or ALDH7 and ESCC risk [17,18,19,20,21]. Notably, Guo et al. reported that among moderate to heavy drinkers, those carrying ADH1B *1/*1 had increased risk by more than 27 times [20]. Four studies showed various SNPs in the XRCC1 DNA repair gene significantly associated with ESCC [19,22,23,24]; a fifth study found no association between the XRCC1 SNP but found an association between SNP haplotype [25]. Additionally, 10 unique miRNA associations were investigated. Other genetically related factors investigated in terms of association with ESCC risk include spectra and frequency of certain gene mutations, short telomere length, gene deletions, loss of heterozygosity, short tandem repeat polymorphisms, and gene-environment interactions (Supplementary materials, Tables S1 and S2).
Gene-environment interactions
Twelve studies investigated gene-environment interactions among their primary aims (Supplementary materials, Table S2). Notably, Pan et al. found an interaction between short leukocyte telomere length, smoking, and alcohol that increased ESCC risk by almost 17 times [26]. Yang et al. showed that carrying XRCC1 G28152A GA + AA vs. GG and consuming long-term stored rice increased ESCC risk by more than 7 times [24]. Additionally, Tan et al. found an interaction between Thymidylate synthase low expression genotype 3Rc/3Rc þ 3Rc/2R þ 2R/2R and low serum folate concentration that increased risk by more than 22 times [27]. Shi et al. found an increased risk of more than 8 times among CYP2C19*3 A Allele carriers who drink [28].
Family history
Three studies aimed at investigating family history of ESCC as a risk factor, and a total of about 7% of studies adjusted for family history in their analyses (Supplementary materials, Table S3). Chen et al. found an increased risk of ESCC of almost two times among individuals having a first-degree relative with ESCC history, compared to those without a first-degree relative with ESCC history [29]. The same study also reported that having two or more first-degree relatives with a history of ESCC increased ESCC risk by almost 3 times, and having both parents with a history of ESCC increased ESCC risk by almost 8 times [29]. Yang et al. showed a 45% increased risk of ESCC among those with a family history of UGI cancer (including gastric and esophageal cancers) and an additional 20% increase among those who had both parents with a history of UGI cancer [30]. Interestingly, the same study reported that having a spouse with UGI cancer did not increase the risk of ESCC [30]. Nan et al. found that those with a positive family history of ESCC had an earlier age of onset by almost two years compared to those with a negative ESCC family history (51.83 vs. 53.59 years) [31].
HPV
HPV as a risk factor for ESCC has been heavily investigated (Supplementary materials, Table S4). Eleven studies across multiple provinces in China measured overall HPV positivity and detected HPV positivity of 0-80% in samples of cases with ESCC [32,33,34,35,36,37,38,39,40,41,42]. Five of these studies also measured HPV-positive controls or healthy distal mucosa samples as comparison groups; no significant trends were found between studies [34,36,38,40,42]. Shuyama et al. compared HPV prevalence in high versus low-risk ESCC risk areas and they detected HPV in 65% and 6% of cases in high and low-risk areas, respectively [41]. Multiple studies reported on high-risk HPV prevalence in ESCC cases, with emphasis on HPV-16 and/or 18. Five studies assessed the association between HPV (including studies that looked at HPV overall, HPV high-risk types, or HPV serum antibodies) and ESCC [34,36,42,43,44]. Among the studies that looked at HPV overall, two studies reported an increased risk of ESCC of 1.56 and 6.4 times [34,42]; one study found no significant association among non-smokers or drinkers but showed an increased risk of two times among smokers and an increased risk of more than ten times among individuals who smoke and drank [36]. Two studies from neighboring provinces studied HPV-16 and the risk associated with ESCC; Guo et al. reported an increased risk of ESCC by nearly thirteen times; Kamangar et al. found no significant association [34,44]. Lastly, Yang et al. investigated the interaction between p53 polymorphisms and HPV-16 seropositivity. They found that among individuals carrying p53 rs1042522 Arg/Arg or Arg/Pro and HPV-16 seropositivity, ESCC risk increased more than 9 times, compared to individuals HPV-16 seronegative and carrying the Pro/Pro genotype, and that risk increased to 27 and 13 times among smokers and drinkers, respectively [9].
Helicobacter pylori
Three studies investigated Helicobacter pylori (H. pylori) as a potential risk factor (Supplementary materials, Table S6). Li et al. investigated H. pylori infection rate in ESCC samples from the three high-risk regions of Linzhou, Shantou, and Shaanxi and reported no differences, but noted that the infection rate was very high overall (estimated ≥70%) [45]. They used PCR to investigate H. pylori 16S rRNA in ESCC and healthy tissues and found 63% and 27% of H. pylori among cases and controls, respectively. Xue et al. investigated the association between H. pylori and ESCC in Hebei province and found no significant association, however, the ESCC sample size was small [46]. In contrast, Wang et al. conducted a multivariate analysis in Jiangsu and showed that H. pylori infection increases ESCC by more than three times [47]. Gastric atrophy, which in most cases is caused by chronic H. pylori, was reported as an etiological factor in three studies. A recent study in 2020 reported a 61% increased risk of ESCC associated with gastric atrophy, signified by having a serum pepsinogen level I of <55ug/L [48]. Similarly, Ren et al. reported a 56% increased risk of ESCC associated with gastric atrophy, defined as PG I/II ratio ≤ 4ng/ml, however, quartile models and continuous models reported no association [49]. In contrast, Xue et al. looked at PG I ≤70 ng/ml, PG I/II ratio ≤3, or 70 ng/ml and PG I/II ratios and ESCC and found no significant associations [46]. In terms of interactions, as mentioned earlier, Ekheden et al. reported an additive interaction between poor oral health and gastric atrophy that increased ESCC risk by 28%, although this finding was not statistically significant [48].
Alcohol and smoking
Multiple studies reported associations between alcohol consumption and ESCC (Supplementary materials, Table S7). Xu et al. reported that alcohol increased ESCC risk almost 1.7 times among men and women [50]. Two studies reported that alcohol consumption increased ESCC risk by more than 2 times among men [24,51]. Guo et al. found that alcohol consumption increased ESCC risk by more than 3 times among heavy drinkers, and by more than 1.5 times among those who consumed alcohol for more than 30 drink-years [20]. Similar to alcohol, multiple studies reported smoking increased ESCC risk by 1.5-2.6 times [50,52,53,54]. Chen et al. found that smoking tobacco for 30 or more years increased ESCC risk by more than 4.5 times [55]. Kumagai et al. reported that smoking 20 or fewer cigarettes a day for more than 20 years was associated with an increased risk of ESCC by more than 1.5 times, however, smoking more than 20 cigarettes a day for 20 years or less, or smoking 20 cigarettes a day for more than 20 years, did not find a significant association, so there may be an issue in this study [56]. The interaction of smoking and alcohol was also reported to affect ESCC risk. Wu et al. found that the joint effect of 40 or more cigarettes per day and 500ml of alcohol/week increased ESCC risk by more than 7 times, compared to those who never smoked or drank [52]. Chen et al. reported that consuming alcohol and smoking tobacco interaction increases the risk of ESCC by almost 44 times [55]. When factoring in duration and dose intensity of alcohol consumption, the same study found that consuming alcohol for 20 years or more and consuming 60 or more grams, was associated with an astounding increase of 183 times ESCC risk.
Pickled vegetable consumption
Among the studies included in this review, three studies found significant independent associations between pickled vegetable consumption and increased ESCC risk, and one study reported no association (Supplementary materials, Table S9). Yu et al. compared the lifestyle of immigrants from the high-risk area of Henan who immigrated to Caihu, Hubei, a lower-risk region, and host residents of Hubei, and found that immigrant residents had a higher consumption of pickled vegetables than host residents [57]. Additionally, Peng et al. conducted a study in Fujian province, also a high-risk region, and showed a significant positive association between consumption of pickled vegetables and ESCC among ESCC cases and healthy controls, as well as an additive interaction between CYP219 polymorphism and pickled vegetable consumption [58]. Wang et al. reported that in their study conducted in Huai’an, Hebei Province, also a high-risk region, a univariate significant association was found between consumption of pickled vegetables and ESCC, however, this association was not present in the multivariate analysis [47]. In contrast, in Tran et al.’s study looking prospectively at the Linxian Intervention Trial, among which almost 2000 individuals developed esophageal cancer during the follow-up period, they reported no significant associations between pickled vegetable consumption and ESCC [59].
Salted meat consumption
Two studies reported on salted meat consumption (Supplementary materials, Table S5). In terms of salted meat consumption amount, Lin et al. reported a slightly increased risk of 18% associated with consuming 50g/week of salted meat in Sichuan province [60]. The same study reported that the interaction of high salted meat intake, defined by more than 90.8g/week, with alcohol and smoking, increased ESCC risk by more than 12 times. In terms of salted meat intake frequency, the same study reported high salted meat intake, defined as intake of 4 or more times per week, was associated with a seven-times increased ESCC risk. Zhao et al., who also investigated high salted meat consumption frequency in Sichuan province, but defined high salted meat consumption as consuming salted meat 1 or more times per week, reported that this frequency of salted meat consumption increased the risk to ESCC by more than two times [61].
Tea type consumption
Four studies reported on green tea consumption among ESCC cases and controls (Supplementary materials, Table S5 and S9). Two studies reported green tea as a protective effect against ESCC. Z. Wang et al. reported an 87% decreased risk of ESCC associated with green tea drinking [47], and J.M. Wang et al. reported a 74% decreased risk of ESCC associated with green tea drinking in women [51]. In contrast, Yang et al. reported green tea drinking as increasing the risk to ESCC by more than 1.5 times, among men [62], and Lin et al. found no significant association between green tea drinking alone and ESCC [63]. The same study showed that black tea, on the other hand, increased the risk for ESCC by almost two times among individuals who consumed >300g/month of black tea [63]. One study investigated jasmine tea consumption and reported no significant association between jasmine tea consumption among males and females combined, however, they did report that high consumption of jasmine tea among males was associated with a 1.68 increased ESCC risk [64].
Fresh fruit and vegetable consumption
Four studies investigated associations between fresh fruit and vegetable intake and ESCC risk (Supplementary materials, Tables S5 and S9). Gao et al. reported ESCC risk reductions of 47% and 54% associated with the consumption of 189 times or more of fresh fruit consumption, and 1230 times or more of fresh vegetable consumption per year, respectively [65]. Peng et al. reported that consuming fresh fruit and vegetables of 400g or more per day decreased ESCC risk by 80%, although this was not statistically significant [58]. Additionally, Liu et al. reported having a dietary food pattern containing higher pattern weight from vegetables and fruits was associated with a 30% reduction in ESCC risk [66]. Tran et al. found a reduced risk of 20% associated with fresh fruit intake of more than 13 times per year but did not find any significant association with fresh vegetable consumption in any amount of intake [59].
Other dietary factors
Other factors related to dietary consumption were also widely investigated (Supplementary materials, Table S5 and S9). Significant inverse associations reported between nutritional factors and ESCC risk include dietary selenium [15], dietary n-3 long-chain polyunsaturated fatty acid pattern consumption [67], dietary monounsaturated and polyunsaturated fatty acids [68], high vitamin D-3 and beta-carotene levels [69], higher intake of certain flavonoids (isoflavones, daidzein, genistein, and glycitein, specifically), moderate anthocyanidin consumption [70], as well as “prudent” food patterns (higher tofu and bean-curd, dry beans, seeds, wheat, rice, etc.) [66], and peanut consumption of 1 or more times per week (also a dose-response relationship) [71]. Significant positive associations reported between nutritional factors and ESCC risk include dietary even-chain unsaturated fatty acid pattern consumption [67], dietary inflammatory nutrients [72], consumption of processed food or alcohol drinking patterns [66], high mycotoxin exposure [73], consumption of pork braised in brown sauce, old stocked rice, high amounts of chili (among men) [51], or milk or dairy products [65]. One study assessed the daily consumption of scalding hot food, fried food, moldy food, or pickled vegetables, compared to a diet excluding those factors, and found an associated increased risk of ESCC of four times [74]. One study found moldy food consumption increased ESCC risk [65], whereas Tran et al. found consumption of moldy bread or moldy vegetables had no significant association with ESCC [59].
Dietary behavior
In this review, five studies reported hot food or drink consumption was associated with more than two times increased risk for ESCC (Supplementary materials, Tables S5 and S9) [51,58,65,75,76]. Among these studies, Peng et al. also found an additive interaction between CYP2C19 GA/AA genotype polymorphism and hot beverage and food consumption [58]. Additionally, three studies reported that drinking very hot tea was associated with more than 1.5 times increased risk (odds ratios ranging from 1.67 to 2.48) [62,63,76]. Among these eight studies, Tai et al. specifically investigated the consumption of high-temperature versus low-temperature water and found an increased risk of ESCC of more than two times [76]. Also among these studies, Zhao et al. reported that waiting 10 or more minutes between water boiling and drinking decreased cancer risk by more than 80% [75]. One study by Tran et al. found no association with the consumption of hot liquids [59]. The behavior associated with alcohol consumption has also been previously investigated. Sun et al. found that drinking alcohol before a meal at mealtime compared to drinking alcohol and eating at the same time, increased ESCC risk by 1.76 times and that drinking alcohol outside of mealtime compared to drinking alcohol at mealtime increased ESCC risk by more than 6 times (Supplementary materials, Table S7) [77]. Additionally, they showed that drinking before mealtime increased the risk by more than 3.5 times among heavy drinkers [77]. Additional dietary behavior investigated includes fast eating, as well as the period between food consumption and bedtime. Wang et al. reported fast eating increased the risk of ESCC by more than three times (Supplementary materials, Table S9) [47]. Similarly, Zhao et al. additionally reported that a more than 50% decrease in ESCC is associated with taking 15 minutes or more to finish a meal (Supplementary materials, Table S5) [75].
Oral Health
Several studies reported an associated risk of ESCC with poor oral health (Supplementary materials, Table S8). Abnet et al. reported a relative risk of 1.3 associated with tooth loss and ESCC in Linzhou, Henan Province [59]. Similarly, Chen et al. reported nearly a 1.5 increase in the risk of ESCC, associated with the loss of 6 or more teeth after age 20 compared to losing no teeth after age 20, but in Jiangsu Province [78]. The same study showed that brushing teeth less than or equal to one time per day was associated with a 1.8 increased risk for ESCC, compared to brushing teeth 2 or more times per day. In another study conducted in Jiangsu Province, Chen et al. reported finding individuals with ESCC had less diversity of oral bacteria compared to healthy individuals [79]. Zhao et al. reported an association of ESCC with poor oral hygiene in combination with genetic interactions in Jiangsu Province [80]. They reported nearly five times an increase in risk for ESCC from a synergistic interaction between the PLCE1 gene SNP rs3765524 TT and tooth brushing less than two times per day [80]. In addition, they reported two times increased ESCC risk from an interaction between ADH1B rs1159918TT and tooth loss. One study by Ekheden et al., also in Jiangsu Province, reported additive interactions between gastric atrophy and poor oral health. They reported nearly 1.3 times increased risk from gastric atrophy combined with once-a-day or no tooth brushing; however, this result was not statistically significant [48].
Environmental factors
Three studies reported etiological factors related to environmental exposures (Supplementary materials, Tables S2 and S10). In two studies, Lian et al. found phytoliths resembling prickle hair from wheat bract in ESCC tumor tissue samples [81,82]. Additionally, Yu et al reported drinking river water increased risk by more than 4 times in men and more than 8 times in women [24]. Lastly, Zhao et al. showed an increased risk of ESCC among urinary exposures to N-nitrosamines [83].
Socioeconomic status
Other etiological factors of ESCC identified in multiple studies in this review include socioeconomic factors (Supplementary materials, Tables S9 and S10). Three studies looked at education level as a risk factor. Tran et al. found having 1-5 years, having completed primary school, or having completed middle school reduced ESCC risk by 13%, 22%, and 43%, respectively [59]. P. Gao reported having completed primary school, primary high school, or secondary high school or more was associated with a 26%, 40%, and 40% reduction in ESCC risk, respectively [84]. Y. Gao et al. found that having 6-9 years of education was associated with a 25% reduction in ESCC risk [65]. Y. Gao et al. also found that having a higher education (secondary high school or above) was associated with a reduced risk of ESCC by 40%, but this association was not statistically significant. Household size as a socioeconomic variable was investigated in two studies. Y. Gao et al. found that having 4 or more people in each household was associated with a 29% increased risk [65]. P. Gao et al. found that having 6 or more people in the household increased risk by 63% [84]. In addition, performing high amounts of physical labor was shown to increase ESCC risk [84]. Having water piped in the home,[59] having a larger house area per person [84], having a higher wealth score [84], and owning certain appliances including owning a refrigerator for >5 [84] or ≥8 years [65], were included among the socioeconomic factors found to reduce ESCC risk.
4. Discussion
This review highlights the extensive amount of research that has been conducted to investigate multiple mechanisms related to ESCC etiology in China. The most investigated risk factors were genetically related, followed by diet and dietary habits, HPV, gene-environment interactions, oral health, family history, H. pylori, and socioeconomic factors.
Almost 70% (68.11%) of included studies investigated genetically related etiologies of ESCC, among which most investigated genetic polymorphisms. The most investigated polymorphism was that on the TP53 gene. The TP53 gene encodes p53, which primarily functions as a tumor suppressor protein, which plays a critical role in cancer development [85,86]. TP53 mutation is the most occurring mutation found in human cancer, with over 50% of cancers holding mutations in the TP53 gene [87]. TP53 mutation leads to p53 loss of functions that are needed to prevent tumor growth, which can lead to cell multiplication and cancer development [88,89]. Because of TP53’s role in cancer development, much research has been conducted looking at TP53 mutations and associations with ESCC. In addition to TP53 polymorphisms, the genetic variations included in this review include SNPs of over 151 unique genes, gene deletions, loss of heterozygosity, missense point mutations, and other genetic variations. Based on the extensive evidence of genetically related risk to ESCC shown in Supplementary materials, Table S1, it is clear that there is a genetic influence on ESCC risk. However, due to the heterogeneity of studies, it was challenging to compare the influence of many different genetic variations measured across studies in a variety of regions, and a meta-analysis was not performed. A meta-analysis may be merited, however, in the future, if more evidence of the same genetic variations becomes available in comparable populations.
The significant portion of studies identified in this review that focused on genetically related etiologies underscores the importance of genetic susceptibility in advising public health prevention and intervention measures. These measures include genetic screening, early detection, personalized prevention strategies, targeted intervention, and public education and awareness. Genetic screening of polymorphisms in high-risk populations could identify genetic mutations associated with increased ESCC risk, could encourage individuals at high risk to be more proactive about endoscopic screening for early cancer detection when treatment outcomes are more favorable, and could provide eligibility information for potential gene therapy interventions. Because most cases are identified in late stages [90], more emphasis on early screening, both genetic and endoscopic, prevention, and public education and awareness is imperative. Guidelines for practitioners for advising individuals carrying high-risk mutations, e.g. TP53 mutations, should be developed and readily/widely available. Guidelines might include younger, more frequent, and more aggressive cancer screening for individuals at higher risk. Policies should be implemented to fund genetic screening in high-risk populations. This review highlights the need for genetic susceptibility screening and the potential for more targeted intervention based on genetic risk factors of ESCC to be prioritized, especially in Chinese communities with significantly higher mortality rates of ESCC such as in Linzhou. Although genetic susceptibility was the most frequently researched etiologic factor identified in this review, its influence relative to and interaction with other factors is still unknown. Therefore, a comprehensive approach that measures genetic as well as other factors is crucial for effective public health ESCC intervention and prevention.
In addition to the extensive investigation of genetically related risk factors, this review also delved into other critical aspects contributing to ESCC risk, encompassing gene-environment interactions, family history, diet, dietary behavior, environmental-related risk factors, H. pylori, HPV, oral health, and socioeconomic factors. Many of these studies relied on retrospective qualitative data gathered through interviews, which carries the potential for recall bias. Despite these limitations, many studies identified significant associations.
The twelve studies that focused on gene-environment interactions highlighted in this review (Supplementary materials, Table S2), particularly the studies that found associations that increased ESCC risk by almost 17 [26] and more than 22 [27] times, emphasize the significance of gene-environment interactions in ESCC development. Genetic polymorphisms or genetic changes can affect one’s susceptibility to environmental exposures and vice versa. For example, the increased risk from the positive multiplicative interaction between an XRCC1 polymorphism and consuming long-term stored rice, found by Yang et al., may suggest that the dietary habit of consuming long-term stored rice may worsen the effects of an XRCC1 polymorphism affecting DNA damage repair. This may lead to a synergistic effect on the development of ESCC, meaning that the combined effects of both factors are greater than the sum of each of their individual effects. Another example is the cumulative interaction between short leukocyte telomere length, smoking, and alcohol consumption found by Pan et al. This finding may suggest that smoking and alcohol consumption could cause oxidative stress, which would further impact individuals with shorter telomeres, further exacerbating the risk of all individual effects when combined. Additionally, the interaction between the Thymidylate synthase low expression genotype and low serum folate concentration reported by Tan et al. [27] may suggest that consuming low amounts of folate may make DNA damage from the Thymidylate synthase polymorphism worse, leading to increased ESCC risk. This presence of a complex interplay between environmental exposures and genetic susceptibility in ESCC development suggests that a comprehensive approach to cancer prevention that includes genetic susceptibility, gene-environment interactions, and other etiologic factors is needed for effective ESCC mitigation. By incorporating information about gene-environment interactions into public health education programs, public health authorities can raise awareness about the complexity of cancer development and encourage individuals to be more proactive about reducing their risk to ESCC.
Three studies in this review reported family history as a potential ESCC etiologic factor, but because of the complexity of family history, concluding family history alone is challenging. Family history as an etiology of any disease can mean one’s risk might be affected by inherited genetic variations, similar living environments or lifestyles as family members, or both, and therefore contains many different factors. Only 7% of the studies included in this review adjusted for family history in their study; the lack of higher adjustments or considerations for family history makes sense as family history can mean a range of influencing factors, which makes it challenging to adjust for. Additionally, because most studies do not have exposure information of relatives, it’s challenging to distinguish the influence of environmental factors from genetic influence. Instead of family history as an etiologic factor, considering genetic, environmental, and the interaction between them may provide more insight into ESCC development.
Multiple studies identified alcohol and tobacco as potential risk factors in Jiangsu, Shandong, Hebei, and Gansu, among other provinces, and many studies acknowledged alcohol and tobacco consumption as well-established risk factors and adjusted for them in their analyses. Despite this evidence, a study conducted in Linzhou (formally known as Linxian), in 1989, which at the time had ten times higher rates of esophageal cancer mortality than China’s average, and still has one of the highest ESCC mortality rates in the world today, reported close to zero tobacco and alcohol consumption among females, little alcohol consumption in males, and only slightly higher tobacco usage among male ESCC cases compared to controls [91] (study was not included in this review because it did not report ESCC-specific data). This review identified multiple studies that found alcohol and tobacco, and interactions with them, as contributing to ESCC development. However, this may vary by region, lifestyle, and culture. Further research including community dietary studies and risk factor comparisons by region may help address the role of alcohol and tobacco relative to other potential etiologies. Public health efforts should prioritize recognizing esophageal cancer as a heightened risk associated with tobacco and alcohol use, especially in high-incidence ESCC regions. Promoting greater public awareness of the link between alcohol and tobacco use and esophageal cancer is advisable, as well as the implementation of stricter tobacco and alcohol control measures, alongside the provision of well-funded, accessible programs for tobacco and alcohol use reduction.
Frequently consumed in high-risk areas of China, pickled vegetables and salted meat were reported by multiple studies in this review to be associated with ESCC etiology. The pickling of vegetables via fermentation and curing meats via the addition of nitrite or nitrate salts can produce N-nitroso compounds [60] or mycotoxins,[58] both considered carcinogens.[92,93,94] It’s also possible that consuming high amounts of salt could lead to esophageal tissue injury, which could increase esophageal cancer risk through repeated esophageal injury, and that consuming high amounts of pickled vegetables could contribute to gastric atrophy, another risk factor identified in this review, through mucosa inflammation from repeated high-acid pickled vegetable consumption. Not all studies identified in this review identified pickled vegetables and salted meat as risk factors. As with many dietary studies, this inconsistency between studies could stem from dietary questionnaire recall bias, poor questionnaire design, or little reported variation between individuals’ dietary habits. The evidence suggests further exploration into diet culture in high-risk areas is imperative, particularly by comparing them with drastically lower ESCC incidence, such as the contrast between the high-incidence areas of Linzhou and adjacent lower-incidence areas. Furthermore, considering the possibility of contamination of various origins such as water, air, soil, and sharp micro contaminants e.g. silica or microplastics, adds further complexity to dietary-related risk factors. Accordingly, environmental health assessments should be conducted to further assess food contamination and safety. Through exploring dietary culture as well as environmental health factors, public health authorities can implement tailored interventions that promote healthier dietary choices to reduce ESCC risk. These interventions might include educational campaigns on higher-risk foods and policies to reduce consumption of pickled and salted foods. Such holistic efforts hold the potential to improve food safety and reduce ESCC risk.
Consumption of hot food or drink was identified in eight studies as a potential ESCC etiologic factor. Very hot beverages are designated as Group 2A carcinogens for ESCC by the IARC monographs, although they mention that the evidence in humans is limited [93]. A few potential mechanisms of hot food or drink increasing ESCC risk are through physical esophageal damage leading to chronic inflammation of the esophageal mucosa, or the reduced ability of the mucosa to prevent exposure to carcinogenic substances, and the carcinogens themselves increasing risk to ESCC. Also identified in this review were multiple studies investigating tea consumption as a potential etiologic factor, with a range of outcomes. Among the studies that identified tea consumption as a risk factor, a potential mechanism could be a thermal injury. Other potential mechanisms include exposure to contaminants (e.g. mold) from fermented tea (black tea) old tea (some tea is intentionally consumed after prolonged storage) or water contamination. Current evidence suggests a further review of hot food and beverage consumption, as well as tea consumption, as risk factors of ESCC, as well as a comprehensive exam of potential mechanisms involved, such as thermal injury, change of salivary gland action, or exposure to contaminants. Additionally, it is critical to further develop targeted public health interventions, such as reducing high-temperature food and drink consumption.
HPV has been heavily investigated as a potential ESCC etiologic factor because of the extensive evidence of HPV’s association with cervical cancer [95,96]. In terms of ESCC etiology, it has been proposed that some proteins made by HPV, especially E6, are oncoproteins that can inactivate host proteins, namely p53, and may cause mutations in host cell DNA and lead to ESCC [97]. Across eleven studies in this review, there was a wide range of HPV-positive prevalence rates reported among various provinces in China. Among the studies that looked at the association between HPV and ESCC risk, some studies found increased risk to ESCC, and others did not. This mixed level of detection, and lack of trends among associations, may point to a true lack of HPV prevalence in ESCC tissue and its limited evidence as an etiologic factor, but could also be due to the varying methods in sample processing or detection (e.g. PCR-based assays or serological tests), varying viral loads in ESCC samples and controls, regional differences, and other confounding factors that include alcohol or tobacco use. The presence of HPV in ESCC tissues, and the significant associations found in some studies, though limited, underscores HPV as a potential ESCC etiologic factor. More research is needed to further understand HPV's impact on ESCC risk and its mechanisms, as well as to inform early ESCC detection efforts e.g. HPV vaccination strategies, and any related regional disparities.
Additional environmental factors were explored in four studies. Two of the studies identified siliceous prickles resembling prickle hair from wheat bracts, in ESCC tissues [81,82]. Sharp micro-silica could potentially physically damage esophageal tissue and even provide a physical attachment point for cancer cell proliferation. Silica fibers could come from prickle hairs in wheat flour or wheat products as proposed in the two mentioned studies or could come from other sources entirely as silica is found in many foods and naturally in the environment. Additional environmentally related evidence identified in this review includes river water consumption as a risk factor [24], and urinary exposure to N-nitrosamines [83]. The available research on environmental factors associated with ESCC in China is limited but suggests that further investigation is warranted due to the potential impact of environmental exposures on the development of ESCC.
Several studies in this review reported that poor oral health, such as tooth loss, teeth brushing frequency, and oral bacteria diversity, may increase ESCC risk. Poor oral health could also play a role in ESCC development by increasing one’s risk for gastric atrophy, changing oral bacteria that affect how orally exposed carcinogens are digested, and increasing local and systemic body inflammation, leading to increased ESCC risk. These studies, four of which were conducted in Jiangsu, used questionnaires as some or part of their method of assessing oral health, which comes with recall bias. Additionally, the identified associations could also be confounded by diet or socioeconomic hardship (e.g. lack of access to dental care, or overall healthcare access as a whole), amongst other factors. For example, Abnet et al.’s study [98] reported an increased risk of ESCC associated with tooth loss but did not address the potential reasons behind the tooth loss, which makes it hard to differentiate whether tooth loss itself increased ESCC risk, or if other factors increased ESCC risk and also contributed to tooth loss. Given these limitations, studies identified in this review suggest there is a link between poor oral health and ESCC. Public health education around improving oral health should be prioritized in high-risk communities to reduce ESCC risk.
Socioeconomic status (SES) factors, such as education level, household size, or appliance ownership, were also highlighted in multiple studies as potentially affecting ESCC risk. This makes sense, as SES indicators together may contribute to disease risk. For example, individuals who have received more formal education may have higher income opportunities, which may come with access to more frequent medical care, and earlier cancer detection. Individuals with more formal education may also have selectively higher access to endoscopic screening for ESCC and may therefore more frequently get screened. Many of the diet and lifestyle factors may be influenced by SES. As addressed in multiple studies, the importance of SES factors in disease development, including ESCC, is significant. Further efforts should be made to prioritize research into finding more SES factors that may influence ESCC development and allocating resources to mitigate those.
This review has several limitations. Only studies published in English were included in this review, which could underestimate or inaccurately represent the past or current research in China. Additionally, search terms used for the literature search were chosen to broadly encompass most research in the field, however, the search terms chosen could have also limited the studies included. Some studies included in this review did not account for the cancer history of all their study participants, or the history of cancer in study participants’ families, which could confound some of the study outcomes. Furthermore, the reported findings from each reviewed study do not include all results reported by each study, but instead include the most relevant and statistically significant results (p < 0.05) as decided by the reviewer; therefore, there are additional factors reported in these studies that may contribute to or be associated with ESCC risk. Also, there was one reviewer for this study which comes with inherent bias. Lastly, as this was a qualitative review of studies based on inclusion and exclusion criteria, this comes with some inherent selection bias of studies to some extent.
5. Conclusion
In summary, this review underscores the variety of factors that may contribute to ESCC development in China, including genetic variations, gene-environment interactions, dietary factors such as alcohol and tobacco use, pickled vegetables and salted meat, hot food or drink consumption, infections such as HPV, poor oral health, gastric atrophy, environmentally-related factors, and socioeconomic factors. While further study is essential to better understand the interactions and contributions of these potential etiologic factors, public health measures should prioritize genetic screening for relevant polymorphisms, comprehensive investigations into environmental and dietary influences, enhanced oral health education, implement enhanced HPV screening in high-risk ESCC areas, and pursue initiatives aimed at improving socioeconomic status overall. These comprehensive measures are critical to effectively reduce ESCC risk and improve public health outcomes in high-risk ESCC areas of China.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Genetic ; Table S2: GxE inter.; Table S3: Family hx; Table S4: HPV; Table S5: Diet; Table S6: H. pylori; Table S7: Alc. & Smoking; Table S8: Oral Health; Table S9: Multiple; Table S10: Other.
Author Contributions
Conceptualization, E.C.; methodology, E.C.; software, E.C.; validation, E.C; formal analysis, E.C..; investigation, E.C.; resources, E.C.; data curation, E.C.; writing—original draft preparation, E.C.; writing—review, E.C. and LW.T.; writing—editing, E.C.; visualization, H.W. and E.C.; supervision, LW.T.; project administration, LW.T.; funding acquisition, LW.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Health and Medical Research Fund (HMRF) from the Food and Health Bureau (FHB) of The Government of the Hong Kong Special Administrative Region (Ref. No.: 18192061; 20211551), the General Research Fund (GRF) scheme from the Research Grants Council of the Hong Kong Special Administrative Region (Ref. No.: 17613819; 17115122, and 17109723), the Theme-based Research Scheme (TRS) of the Hong Kong Research Grants Council (Ref. No.: T24-508/22-N), the General Program of National Natural Science Foundation of China (Ref. No.: 82173469), the Guangdong Natural Science Fund (GD-NSF) of China (Ref. No.: 2022A1515011151), and Seed Funding for Strategic Interdisciplinary Research Scheme from the University Research Committee at the University of Hong Kong (Ref. No.: 102010191).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global Surveillance of Trends in Cancer Survival 2000-14 (CONCORD-3): Analysis of Individual Records for 37 513 025 Patients Diagnosed with One of 18 Cancers from 322 Population-Based Registries in 71 Countries. Lancet Lond. Engl. 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Zaidi, N.; Kelly, R.J. The Management of Localized Esophageal Squamous Cell Carcinoma: Western Approach. Chin. Clin. Oncol. 2017, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Ferlay, J.; Curado, M.-P.; Bray, F.; Edwards, B.; Shin, H.-R.; Forman, D. Fifty Years of Cancer Incidence: CI5 I-IX. Int. J. Cancer 2010, 127, 2918–2927. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, Morbidity, and Risk Factors in China and Its Provinces, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Lond. Engl. 2019, 394, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Totsuka, Y.; Shan, B.; Wang, C.; Wei, W.; Qiao, Y.; Kikuchi, S.; Inoue, M.; Tanaka, H.; He, Y. Esophageal Cancer in High-Risk Areas of China: Research Progress and Challenges. Ann. Epidemiol. 2017, 27, 215–221. [Google Scholar] [CrossRef]
- Chen, R.; Zheng, R.; Zhang, S.; Wang, S.; Sun, K.; Zeng, H.; Li, L.; Wei, W.; He, J. Patterns and Trends in Esophageal Cancer Incidence and Mortality in China: An Analysis Based on Cancer Registry Data. J. Natl. Cancer Cent. 2023, 3, 21–27. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan — a Web and Mobile App for Systematic Reviews. 2016, 5. 5. [CrossRef]
- Yang, J.; Liu, B.; Li, W.; Xiong, H.; Qiu, H.; Fu, Q.; Chen, B.; Hu, G.; Yuan, X. Association of P53 and MDM2 Polymorphisms with Risk of Human Papillomavirus (HPV)-Related Esophageal Squamous Cell Carcinoma (ESCC). Cancer Epidemiol. 2013, 37, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Zhang, Y.; Tian, X.; Ning, T.; Ke, Y. P53 Codon 72 Polymorphism and the Risk of Esophageal Squamous Cell Carcinoma. Mol. Carcinog. 2008, 47, 100–104. [Google Scholar] [CrossRef]
- Li, W.Q.; Hu, N.; Hyland, P.L.; Gao, Y.; Wang, Z.M.; Yu, K.; Su, H.; Wang, C.Y.; Wang, L.M.; Chanock, S.J.; et al. Genetic Variants in DNA Repair Pathway Genes and Risk of Esophageal Squamous Cell Carcinoma and Gastric Adenocarcinoma in a Chinese Population. Carcinogenesis 2013, 34, 1536–1542. [Google Scholar] [CrossRef]
- Shao, Y.; Tan, W.; Zhang, S. P53 Gene Codon 72 Polymorphism and Risk of Esophageal Squamous Cell Carcinoma: A Case/Control Study in a Chinese Population. Esophagus 2008, 21, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Yang, J.; Liu, B.; Li, W.; Hu, G.; Qiu, H.; Huang, L.; Xiong, H.; Yuan, X. Combined Effects of Leukocyte Telomere Length, P53 Polymorphism and Human Papillomavirus Infection on Esophageal Squamous Cell Carcinoma in a Han Chinese Population. Cancer Epidemiol. 2014, 38, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, D.; Wang, Y.; Sun, G.; Song, W.; Zhang, B.; Borjigin, B. Association of TP53 Codon 72 Genotype Polymorphism and Environmental Factors with Esophageal Squamous Cell Carcinoma in the Mongolian Population of the Chinese Region of Inner Mongolia. Oncol. Lett. 2017, 14, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Mu, L.N.; Lu, H.; Lu, Q.Y.; You, N.C.Y.; Yu, S.Z.; Le, A.D.; Zhao, J.; Zhou, X.F.; Marshall, J.; et al. Dietary Selenium Intake and Genetic Polymorphisms of the GSTP1 and P53 Genes on the Risk of Esophageal Squamous Cell Carcinoma. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhang, J.; Ning, T.; Chen, Z.; Xu, C. Association of Genetic Polymorphisms in MDM2, PTEN and P53 with Risk of Esophageal Squamous Cell Carcinoma. J Hum Genet 2012, 57, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tong, L.; Wei, J.; Pan, W.; Li, L.; Ge, Y.; Zhou, L.; Yuan, Q.; Zhou, C.; Yang, M. The ALDH7A1 Genetic Polymorphisms Contribute to Development of Esophageal Squamous Cell Carcinoma. Tumor Biol. 2014, 35, 12665–12670. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Runli, J.; Wei, X.; Lili, G.; Linyan, C.; Yamei, R.; Ruitao, W.; Zhengyun, Z.; Baiqing, L.; Xia, S. Esophageal Squamous Cell Carcinoma and ALDH2 and ADH1B Polymorphisms in Chinese Females. Asian Pac. J. Cancer Prev. 2011, 12, 2065–2068. [Google Scholar] [PubMed]
- Cai, L.; You, N.C.; Lu, H.; Mu, L.N.; Lu, Q.Y.; Yu, S.Z.; Le, A.D.; Marshall, J.; Heber, D.; Zhang, Z.F. Dietary Selenium Intake, Aldehyde Dehydrogenase-2 and X-Ray Repair Cross-Complementing 1 Genetic Polymorphisms, and the Risk of Esophageal Squamous Cell Carcinoma. Cancer 2006, 106, 2345–2354. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.M.; Wang, Q.; Liu, Y.Z.; Chen, H.M.; Qi, Z.; Guo, Q.H. Genetic Polymorphisms in Cytochrome P4502E1, Alcohol and Aldehyde Dehydrogenases and the Risk of Esophageal Squamous Cell Carcinoma in Gansu Chinese Males. World J. Gastroenterol. 2008, 14, 1444–1449. [Google Scholar] [CrossRef]
- Suo, C.; Yang, Y.; Yuan, Z.; Zhang, T.; Yang, X.; Qing, T.; Gao, P.; Shi, L.; Fan, M.; Cheng, H.; et al. Alcohol Intake Interacts with Functional Genetic Polymorphisms of Aldehyde Dehydrogenase (ALDH2) and Alcohol Dehydrogenase (ADH) to Increase Esophageal Squamous Cell Cancer Risk. J. Thorac. Oncol. 2019, 14, 712–725. [Google Scholar] [CrossRef]
- Hao, B.; Wang, H.; Zhou, K.; Li, Y.; Chen, X.; Zhou, G.; Zhu, Y.; Miao, X.; Tan, W.; Wei, Q.; et al. Identification of Genetic Variants in Base Excision Repair Pathway and Their Associations with Risk of Esophageal Squamous Cell Carcinoma. Cancer Res. 2004, 64, 4378–4384. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Zhou, R.M.; Wan, L.L.; Wang, N.; Li, Y.; Zhang, X.J.; Dong, X.J. Polymorphisms of the DNA Repair Gene Xeroderma Pigmentosum Groups A and C and Risk of Esophageal Squamous Cell Carcinoma in a Population of High Incidence Region of North China. J Cancer Res Clin Oncol 2008, 134, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Fu, C.; Wang, J.; Xue, H.; Xu, B. Interaction between XRCC1 Polymorphisms and Intake of Long-Term Stored Rice in the Risk of Esophageal Squamous Cell Carcinoma: A Case-Control Study. Biomed. Environ. Sci. 2011, 24, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.X.; Dai, L.P.; Wang, P.; Wang, K.J.; Zhang, J.Y.; Xie, W. Association of Polymorphisms in X-Ray Repair Cross Complementing 1 Gene and Risk of Esophageal Squamous Cell Carcinoma in a Chinese Population. Biomed Res Int 2015, 2015, 509215. [Google Scholar] [CrossRef]
- Pan, W.; Du, J.; Shi, M.; Jin, G.; Yang, M. Short Leukocyte Telomere Length, Alone and in Combination with Smoking, Contributes to Increased Risk of Gastric Cancer or Esophageal Squamous Cell Carcinoma. Carcinogenesis 2017, 38, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Miao, X.; Wang, L.; Yu, C.; Xiong, P.; Liang, G.; Sun, T.; Zhou, Y.; Zhang, X.; Li, H.; et al. Significant Increase in Risk of Gastroesophageal Cancer Is Associated with Interaction between Promoter Polymorphisms in Thymidylate Synthase and Serum Folate Status. Carcinogenesis 2005, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Luo, G. j; Zhang, L.; Shi, J.; Zhang, D. q; Chen, J. m; Chen, X. b; Li, Z. d; Zhao, Q. Interaction between Alcohol Consumption and CYP 2C19 Gene Polymorphism in Relation to Oesophageal Squamous Cell Carcinoma. PLoS ONE 2012, 7, e43412. [Google Scholar] [CrossRef]
- Chen, T.; Cheng, H.; Chen, X.; Yuan, Z.; Yang, X.; Zhuang, M.; Lu, M.; Jin, L.; Ye, W. Family History of Esophageal Cancer Increases the Risk of Esophageal Squamous Cell Carcinoma. Sci. Rep. 2015, 5, 16038. [Google Scholar] [CrossRef]
- Yang, H.; Wang, J.B.; Zhang, J.Y.; Fan, J.H.; Qiao, Y.L.; Taylor, P.R. Family History and Risk of Upper Gastrointestinal Cancer in the Linxian General Population. Front. Oncol. 2021, 11, 605106. [Google Scholar] [CrossRef]
- Jia, N.; Wen, X.D.; Zhang, N.; Yang, Y.; Zhang, L.W.; Wang, X.L.; Wang, N.; Wen, D.G. Younger Age of Onset and Multiple Primary Lesions Associated with Esophageal Squamous Cell Carcinoma Cases with a Positive Family History of the Cancer Suggests Genetic Predisposition. Chin. Med. J. (Engl.) 2014, 127, 2779–2783. [Google Scholar] [CrossRef]
- Teng, H.; Li, X.; Liu, X.; Wu, J.; Zhang, J. The Absence of Human Papillomavirus in Esophageal Squamous Cell Carcinoma in East China. Int. J. Clin. Exp. Pathol. 2014, 7, 4184–4193. [Google Scholar] [PubMed]
- Liu, T.; Liu, Q.; Liang, M.; Zheng, S.; Li, X.L.; Lu, X.; Sheyhidin, I. Viral Load of HPV 16/18 in Esophageal Squamous Cell Carcinoma in Three Ethnic Groups Living in Xinjiang Autonomous Region, China. Mol. Biol. Rep. 2013, 40, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Liu, Y.; Wang, X.; He, Z.; Weiss, N.S.; Madeleine, M.M.; Liu, F.; Tian, X.; Song, Y.; Pan, Y.; et al. Human Papillomavirus Infection and Esophageal Squamous Cell Carcinoma: A Case-Control Study. Cancer Epidemiol. Biomarkers Prev. 2012, 21, 780–785. [Google Scholar] [CrossRef]
- He, D.; Zhang, D.K.; Lam, K.Y.; Ma, L.; Ngan, H.Y.; Liu, S.S.; Tsao, S.W. Prevalence of HPV Infection in Esophageal Squamous Cell Carcinoma in Chinese Patients and Its Relationship to the P53 Gene Mutation. Int J Cancer 1997, 72, 959–964. [Google Scholar] [CrossRef]
- Qi, Z.; Jiang, Q.; Yang, J.; Chen, X.; Wu, H.; Huang, L.; Hu, G.; Yuan, X. Human Papillomavirus (HPV) Infection and the Risk of Esophageal Squamous Cell Carcinoma. Dis. Esophagus 2013, 26, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Mehryar, M.M.; Li, S.Y.; Liu, H.W.; Li, F.; Zhang, F.; Zhou, Y.B.; Zeng, Y.; Li, J.T. Prevalence of Human Papillomavirus in Esophageal Carcinoma in Tangshan, China. World J Gastroenterol 2015, 21, 2905–2911. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.Y.; Hu, S.P.; Lu, L.C.; Tang, C.Z.; Kuang, Z.S.; Zhong, S.P.; Zeng, Y. Detection of Human Papillomavirus in Esophageal Carcinoma. J. Med. Virol. 2002, 68, 412–416. [Google Scholar] [CrossRef]
- Si, H.X.; Tsao, S.W.; Poon, C.S.P.; Wang, L.D.; Wong, Y.C.; Cheung, A.L.M. Viral Load of HPV in Esophageal Squamous Cell Carcinoma. Int. J. Cancer 2003, 103, 496–500. [Google Scholar] [CrossRef]
- Gao, G.F.; Roth, M.J.; Wei, W.Q.; Abnet, C.C.; Chen, F.; Lu, N.; Zhao, F.H.; Li, X.Q.; Wang, G.Q.; Taylor, P.R.; et al. No Association between HPV Infection and the Neoplastic Progression of Esophageal Squamous Cell Carcinoma: Result from a Cross-Sectional Study in a High-Risk Region of China. Int. J. Cancer 2006, 119, 1354–1359. [Google Scholar] [CrossRef]
- Shuyama, K.; Castillo, A.; Aguayo, F.; Sun, Q.; Khan, N.; Koriyama, C.; Akiba, S. Human Papillomavirus in High- and Low-Risk Areas of Oesophageal Squamous Cell Carcinoma in China. Br J Cancer 2007, 96, 1554–1559. [Google Scholar] [CrossRef]
- Yang, J.; Wu, H.; Wei, S.; Xiong, H.; Fu, X.; Qi, Z.; Jiang, Q.; Li, W.; Hu, G.; Yuan, X.; et al. HPV Seropositivity Joints with Susceptibility Loci Identified in GWASs at Apoptosis Associated Genes to Increase the Risk of Esophageal Squamous Cell Carcinoma (ESCC). BMC Cancer 2014, 14, 501. [Google Scholar] [CrossRef]
- He, Z.; Xu, Z.; Hang, D.; Guo, F.; Abliz, A.; Weiss, N.S.; Xi, L.; Liu, F.; Ning, T.; Pan, Y.; et al. Anti-HPV-E7 Seropositivity and Risk of Esophageal Squamous Cell Carcinoma in a High-Risk Population in China. Carcinogenesis 2014, 35, 816–821. [Google Scholar] [CrossRef]
- Kamangar, F.; Qiao, Y.L.; Schiller, J.T.; Dawsey, S.M.; Fears, T.; Sun, X.D.; Abnet, C.C.; Zhao, P.; Taylor, P.R.; Mark, S.D. Human Papillomavirus Serology and the Risk of Esophageal and Gastric Cancers: Results from a Cohort in a High-Risk Region in China. Int J Cancer 2006, 119, 579–584. [Google Scholar] [CrossRef]
- Li, W.S.; Tian, D.P.; Guan, X.Y.; Yun, H.; Wang, H.T.; Xiao, Y.; Bi, C.; Ying, S.; Su, M. Esophageal Intraepithelial Invasion of Helicobacter Pylori Correlates with Atypical Hyperplasia. Int J Cancer 2014, 134, 2626–2632. [Google Scholar] [CrossRef]
- Xue, L.; Xing, L.; Shen, H.; Cui, J.; Mi, J.; Wang, J.; Misumi, J.; Hang, X. Serum Pepsinogens and Helicobacter Pylori Are Not Associated with Esophageal Squamous Cell Carcinoma in a High-Risk Area in China. Tumori 2013, 99, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tang, L.; Sun, G.; Tang, Y.; Xie, Y.; Wang, S.; Hu, X.; Gao, W.; Cox, S.B.; Wang, J.S. Etiological Study of Esophageal Squamous Cell Carcinoma in an Endemic Region: A Population-Based Case Control Study in Huaian, China. BMC Cancer 2006, 6, 287. [Google Scholar] [CrossRef] [PubMed]
- Ekheden, I.; Yang, X.; Chen, H.; Chen, X.; Yuan, Z.; Jin, L.; Lu, M.; Ye, W. Gastric Atrophy and Its Interaction with Poor Oral Health Elevate the Risk for Esophageal Squamous Cell Carcinoma in a High-Risk Region of China: A Population-Based Case-Control Study. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Ren, J.S.; Kamangar, F.; Qiao, Y.L.; Taylor, P.R.; Liang, H.; Dawsey, S.M.; Liu, B.; Fan, J.H.; Abnet, C.C. Serum Pepsinogens and Risk of Gastric and Oesophageal Cancers in the General Population Nutrition Intervention Trial Cohort. Gut 2009, 58, 636–642. [Google Scholar] [CrossRef]
- Xu, X.; Mao, B.; Wu, L.; Liu, L.; Rui, J.; Chen, G. A118G Polymorphism in μ-Opioid Receptor Gene and Interactions with Smoking and Drinking on Risk of Oesophageal Squamous Cell Carcinoma. J Clin Lab Anal 2017, 31. [Google Scholar] [CrossRef]
- Wang, J.M.; Xu, B.; Rao, J.Y.; Shen, H.B.; Xue, H.C.; Jiang, Q.W. Diet Habits, Alcohol Drinking, Tobacco Smoking, Green Tea Drinking, and the Risk of Esophageal Squamous Cell Carcinoma in the Chinese Population. Eur J Gastroenterol Hepatol 2007, 19, 171–176. [Google Scholar] [CrossRef]
- M, W.; JK, Z.; ZF, Z.; RQ, H.; J, Y.; JY, Z.; XS, W.; XF, Z.; AM, L.; P, van’ t V. ; et al. Smoking and Alcohol Drinking Increased the Risk of Esophageal Cancer among Chinese Men but Not Women in a High-Risk Population. Cancer Causes Control CCC 2011, 22, 649–657. [Google Scholar] [CrossRef]
- Xing, D.Y.; Tan, W.; Song, N.; Lin, D.X. Ser326Cys Polymorphism in hOGG1 Gene and Risk of Esophageal Cancer in a Chinese Population. Int J Cancer 2001, 95, 140–143. [Google Scholar] [CrossRef]
- Ye, B.; Feng, J.; Pan, X.; Yang, Y.; Ji, C.; Cheng, M.; Cheng, Y.; Shi, J.; Zhao, H. Genetic Variant of Single-Nucleotide Polymorphism Is Associated with Risk of Esophageal Squamous Cell Carcinoma. Genet. Test. Mol. Biomark. 2014, 18, 45–49. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, N.; Wakai, T.; Wei, L.; He, Y.; Kumagai, N.; Kitsu, K.; Wang, S.; Akazawa, K. Effect of the Interaction between the Amount and Duration of Alcohol Consumption and Tobacco Smoking on the Risk of Esophageal Cancer: A Case-Control Study. Exp. Ther. Med. 2010, 1, 991–997. [Google Scholar] [CrossRef]
- Kumagai, N.; Wakai, T.; Akazawa, K.; Ling, Y.; Wang, S.; Shan, B.; Okuhara, Y.; Hatakeyama, Y.; Kataoka, H. Heavy Alcohol Intake Is a Risk Factor for Esophageal Squamous Cell Carcinoma among Middle-Aged Men: A Case-Control and Simulation Study. Mol. Clin. Oncol. 2013, 1, 811–816. [Google Scholar] [CrossRef]
- Yu, X.; Zhang, T.; Zhang, H.; Hu, A.; Hu, Y.; Guo, W.; Wang, Y. Comparison of Lifestyle and Living Environment among High Risk Immigrant and Low Risk Host Residents: Implications for Esophageal Cancer Etiology. Asian Pac. J. Cancer Prev. 2010, 11, 1827–1831. [Google Scholar]
- Peng, X.E.; Chen, H.F.; Hu, Z.J.; Shi, X.S. Independent and Combined Effects of Environmental Factors and CYP2C19 Polymorphisms on the Risk of Esophageal Squamous Cell Carcinoma in Fujian Province of China. BMC Med. Genet. 2015, 16, 15. [Google Scholar] [CrossRef]
- Tran, G.D.; Sun, X.D.; Abnet, C.C.; Fan, J.H.; Dawsey, S.M.; Dong, Z.W.; Mark, S.D.; Qiao, Y.L.; Taylor, P.R. Prospective Study of Risk Factors for Esophageal and Gastric Cancers in the Linxian General Population Trial Cohort in China. Int. J. Cancer 2005, 113, 456–463. [Google Scholar] [CrossRef]
- Lin, S.; Wang, X.; Huang, C.; Liu, X.; Zhao, J.; Yu, I.T.S.; Christiani, D.C. Consumption of Salted Meat and Its Interactions with Alcohol Drinking and Tobacco Smoking on Esophageal Squamous-Cell Carcinoma. Int. J. Cancer 2015, 137, 582–589. [Google Scholar] [CrossRef]
- Zhao, L.; Li, Y.C.; Wu, J.P.; Zhao, Y.J.; Wang, R.B.; Jiang, M.; Song, Q.K. Increased Risk of Esophageal Squamous Cell Carcinoma Associated with Frequent and Long-Term Consumption of Salted Meat and Salted Fat. J Int Med Res 2019, 47, 3841–3849. [Google Scholar] [CrossRef]
- Yang, X.; Ni, Y.; Yuan, Z.; Chen, H.; Plymoth, A.; Jin, L.; Chen, X.; Lu, M.; Ye, W. Very Hot Tea Drinking Increases Esophageal Squamous Cell Carcinoma Risk in a High-Risk Area of China: A Population-Based Case-Control Study. Clin. Epidemiol. 2018, 10, 1307–1320. [Google Scholar] [CrossRef]
- Lin, S.; Xu, G.; Chen, Z.; Liu, X.; Li, J.; Ma, L.; Wang, X. Tea Drinking and the Risk of Esophageal Cancer: Focus on Tea Type and Drinking Temperature. Eur. J. Cancer Prev. 2020, 29, 382–387. [Google Scholar] [CrossRef]
- Gao, Y.; Hu, N.; Han, X.; Giffen, C.; Ding, T.; Goldstein, A.M.; Taylor, P.R. Jasmine Tea Consumption and Upper Gastrointestinal Cancer in China. Cancer Causes Control 2009, 20, 1997–2007. [Google Scholar] [CrossRef]
- Gao, Y.; Hu, N.; Han, X.Y.; Ding, T.; Giffen, C.; Goldstein, A.M.; Taylor, P.R. Risk Factors for Esophageal and Gastric Cancers in Shanxi Province, China: A Case-Control Study. Cancer Epidemiol. 2011, 35, e91–e99. [Google Scholar] [CrossRef]
- Liu, X.; Wang, X.; Lin, S.; Lao, X.; Zhao, J.; Song, Q.; Su, X.; Tak-Sun Yu, I. Dietary Patterns and the Risk of Esophageal Squamous Cell Carcinoma: A Population-Based Case-Control Study in a Rural Population. Clin Nutr 2017, 36, 260–266. [Google Scholar] [CrossRef]
- Hu, C.; Lin, Z.; Liu, Z.; Tang, X.; Song, J.; Lin, J.; Chen, Y.; Hu, Z. Dietary Fatty Acid Patterns and Risk of Oesophageal Squamous Cell Carcinoma. PeerJ 2022, 10, e13036. [Google Scholar] [CrossRef]
- Tang, Y.X.; Zhao, W.; Li, J.; Xie, P.; Wang, S.; Yan, L.; Xing, X.; Lu, J.; Tse, L.A.; Wang, H.H.X.; et al. Dietary Intake of Monounsaturated and Polyunsaturated Fatty Acids Is Related to the Reduced Risk of Esophageal Squamous Cell Carcinoma. Lipids Health Dis. 2022, 21, 25. [Google Scholar] [CrossRef]
- Huang, G.L.; Yang, L.; Su, M.; Wang, S.K.; Yin, H.; Wang, J.S.; Sun, G.J. Vitamin D3 and Beta-Carotene Deficiency Is Associated with Risk of Esophageal Squamous Cell Carcinoma - Results of a Case-Control Study in China. Asian Pac. J. Cancer Prev. 2014, 15, 819–823. [Google Scholar] [CrossRef]
- Sun, L.; Zhao, W.; Li, J.; Tse, L.A.; Xing, X.; Lin, S.; Zhao, J.; Ren, Z.; Zhang, C.X.; Liu, X. Dietary Flavonoid Intake and Risk of Esophageal Squamous Cell Carcinoma: A Population-Based Case-Control Study. Nutrition 2021, 89, 111235. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, L.; Hu, Z.; Wu, J.; Li, J.; Qu, C.; He, Y.; Song, Q. Peanut Consumption Associated with a Reduced Risk of Esophageal Squamous Cell Carcinoma: A Case-Control Study in a High-Risk Area in China. Thorac Cancer 2018, 9, 30–36. [Google Scholar] [CrossRef]
- Li, S.; Ye, J.; Lin, Z.; Lin, Z.; Tang, X.; Rao, W.; Hu, Z. Dietary Inflammatory Nutrients and Esophageal Squamous Cell Carcinoma Risk: A Case-Control Study. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Xue, K.S.; Tang, L.; Sun, G.; Wang, S.; Hu, X.; Wang, J.S. Mycotoxin Exposure Is Associated with Increased Risk of Esophageal Squamous Cell Carcinoma in Huaian Area, China. BMC Cancer 2019, 19, 1218. [Google Scholar] [CrossRef]
- Song, Q.; Liu, H.; Wang, J.; Jia, Y.; Liu, Y.; Wang, N.; Tan, B.; Guan, S.; An, D.; Cheng, Y. Dinner-to-Bed Time and Post-Dinner Walk: New Potential Independent Factors in Esophageal Cancer Development. J. Cancer Res. Clin. Oncol. 2014, 140, 817–821. [Google Scholar] [CrossRef]
- Zhao, L.; Liu, C.L.; Song, Q.K.; Deng, Y.M.; Qu, C.X.; Li, J. Association between Dietary Behavior and Esophageal Squamous Cell Carcinoma in Yanting. Asian Pac. J. Cancer Prev. APJCP 2014, 15, 8657–8660. [Google Scholar] [CrossRef]
- Tai, W.P.; Nie, G.J.; Chen, M.J.; Yaz, T.Y.; Guli, A.; Wuxur, A.; Huang, Q.Q.; Lin, Z.G.; Wu, J. Hot Food and Beverage Consumption and the Risk of Esophageal Squamous Cell Carcinoma: A Case-Control Study in a Northwest Area in China. Med. Baltim. 2017, 96, e9325. [Google Scholar] [CrossRef]
- Sun, M.; Yang, A.; Xing, J.; Yu, J.; Wang, K.; Lu, H.; Han, J. Association of Alcohol Consumption before a Meal with the Risk of Gastric Adenocarcinoma and Esophageal Squamous Cell Carcinoma: A Case-Control Study. Int. J. Clin. Exp. Med. 2019, 12, 1914–1921. [Google Scholar]
- Chen, X.; Yuan, Z.; Lu, M.; Zhang, Y.; Jin, L.; Ye, W. Poor Oral Health Is Associated with an Increased Risk of Esophageal Squamous Cell Carcinoma - a Population-Based Case-Control Study in China. Int. J. Cancer 2017, 140, 626–635. [Google Scholar] [CrossRef]
- Chen, X.; Winckler, B.; Lu, M.; Cheng, H.; Yuan, Z.; Yang, Y.; Jin, L.; Ye, W. Oral Microbiota and Risk for Esophageal Squamous Cell Carcinoma in a High-Risk Area of China. PLoS One 2015, 10, e0143603. [Google Scholar] [CrossRef]
- Zhao, R.; Li, X.; Yang, X.; Zhang, T.; Lu, M.; Ye, W.; Jin, L.; Suo, C.; Chen, X. Association of Esophageal Squamous Cell Carcinoma With the Interaction Between Poor Oral Health and Single Nucleotide Polymorphisms in Regulating Cell Cycles and Angiogenesis: A Case-Control Study in High-Incidence Chinese. Cancer Control 2022, 29. [Google Scholar] [CrossRef]
- Lian, C.; Xie, S.; Li, W.; Ran, J.; Zhang, J.; Han, Z.; Zuo, X.; Tian, L. Association of Wheat Chaff Derived Silica Fiber and Esophageal Cancer in North China. Ecotoxicol. Environ. Saf. 2019, 178, 79–85. [Google Scholar] [CrossRef]
- Lian, C.; Zuo, X.; Tian, L. A Possible Role of Biogenic Silica in Esophageal Cancer in North China? Environ. Sci. Pollut. Res. Int. 2019, 26, 8340–8343. [Google Scholar] [CrossRef]
- Zhao, C.; Zhou, J.; Gu, Y.; Pan, E.; Sun, Z.; Zhang, H.; Lu, Q.; Zhang, Y.; Yu, X.; Liu, R.; et al. Urinary Exposure of N-Nitrosamines and Associated Risk of Esophageal Cancer in a High Incidence Area in China. Sci. Total Environ. 2020, 738, 139713. [Google Scholar] [CrossRef]
- Gao, P.; Yang, X.; Suo, C.; Yuan, Z.; Cheng, H.; Zhang, Y.; Jin, L.; Lu, M.; Chen, X.; Ye, W. Socioeconomic Status Is Inversely Associated with Esophageal Squamous Cell Carcinoma Risk: Results from a Population-Based Case-Control Study in China. Oncotarget 2018, 9, 6911–6923. [Google Scholar] [CrossRef]
- Aubrey, B.J.; Strasser, A.; Kelly, G.L. Tumor-Suppressor Functions of the TP53 Pathway. Cold Spring Harb. Perspect. Med. 2016, 6, a026062. [Google Scholar] [CrossRef]
- Olivier, M.; Hollstein, M.; Hainaut, P. TP53 Mutations in Human Cancers: Origins, Consequences, and Clinical Use. Cold Spring Harb. Perspect. Biol. 2010, 2, a001008. [Google Scholar] [CrossRef]
- Ozaki, T.; Nakagawara, A. Role of P53 in Cell Death and Human Cancers. Cancers 2011, 3, 994–1013. [Google Scholar] [CrossRef]
- Hu, J.; Cao, J.; Topatana, W.; Juengpanich, S.; Li, S.; Zhang, B.; Shen, J.; Cai, L.; Cai, X.; Chen, M. Targeting Mutant P53 for Cancer Therapy: Direct and Indirect Strategies. J. Hematol. Oncol.J Hematol Oncol 2021, 14, 157. [Google Scholar] [CrossRef]
- Marei, H.E.; Althani, A.; Afifi, N.; Hasan, A.; Caceci, T.; Pozzoli, G.; Morrione, A.; Giordano, A.; Cenciarelli, C. P53 Signaling in Cancer Progression and Therapy. Cancer Cell Int. 2021, 21, 703. [Google Scholar] [CrossRef]
- He, Z.; Ke, Y. Precision Screening for Esophageal Squamous Cell Carcinoma in China. Chin. J. Cancer Res. 2020, 32, 673–682. [Google Scholar] [CrossRef]
- Li, J.Y.; Ershow, A.G.; Chen, Z.J.; Wacholder, S.; Li, G.Y.; Guo, W.; Li, B.; Blot, W.J. A Case-Control Study of Cancer of the Esophagus and Gastric Cardia in Linxian. Int. J. Cancer 1989, 43, 755–761. [Google Scholar] [CrossRef]
- Tricker, A.R.; Preussmann, R. Carcinogenic N-Nitrosamines in the Diet: Occurrence, Formation, Mechanisms and Carcinogenic Potential. Mutat. Res. 1991, 259, 277–289. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer List of Classifications by Cancer Sites with Sufficient or Limited Evidence in Humans, IARC Monographs Volumes 1–134.
- Claeys, L.; Romano, C.; De Ruyck, K.; Wilson, H.; Fervers, B.; Korenjak, M.; Zavadil, J.; Gunter, M.J.; De Saeger, S.; De Boevre, M.; et al. Mycotoxin Exposure and Human Cancer Risk: A Systematic Review of Epidemiological Studies. Compr. Rev. Food Sci. Food Saf. 2020, 19, 1449–1464. [Google Scholar] [CrossRef] [PubMed]
- Burd, E.M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef]
- Cervical Cancer Available online:. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 9 August 2023).
- Farhadi, M.; Tahmasebi, Z.; Merat, S.; Kamangar, F.; Nasrollahzadeh, D.; Malekzadeh, R. Human Papillomavirus in Squamous Cell Carcinoma of Esophagus in a High-Risk Population. World J. Gastroenterol. 2005, 11, 1200–1203. [Google Scholar] [CrossRef]
- Abnet, C.C.; Qiao, Y.L.; Mark, S.D.; Dong, Z.W.; Taylor, P.R.; Dawsey, S.M. Prospective Study of Tooth Loss and Incident Esophageal and Gastric Cancers in China. Cancer Causes Control 2001, 12, 847–854. [Google Scholar] [CrossRef]
Figure 1.
Study PRISMA diagram.
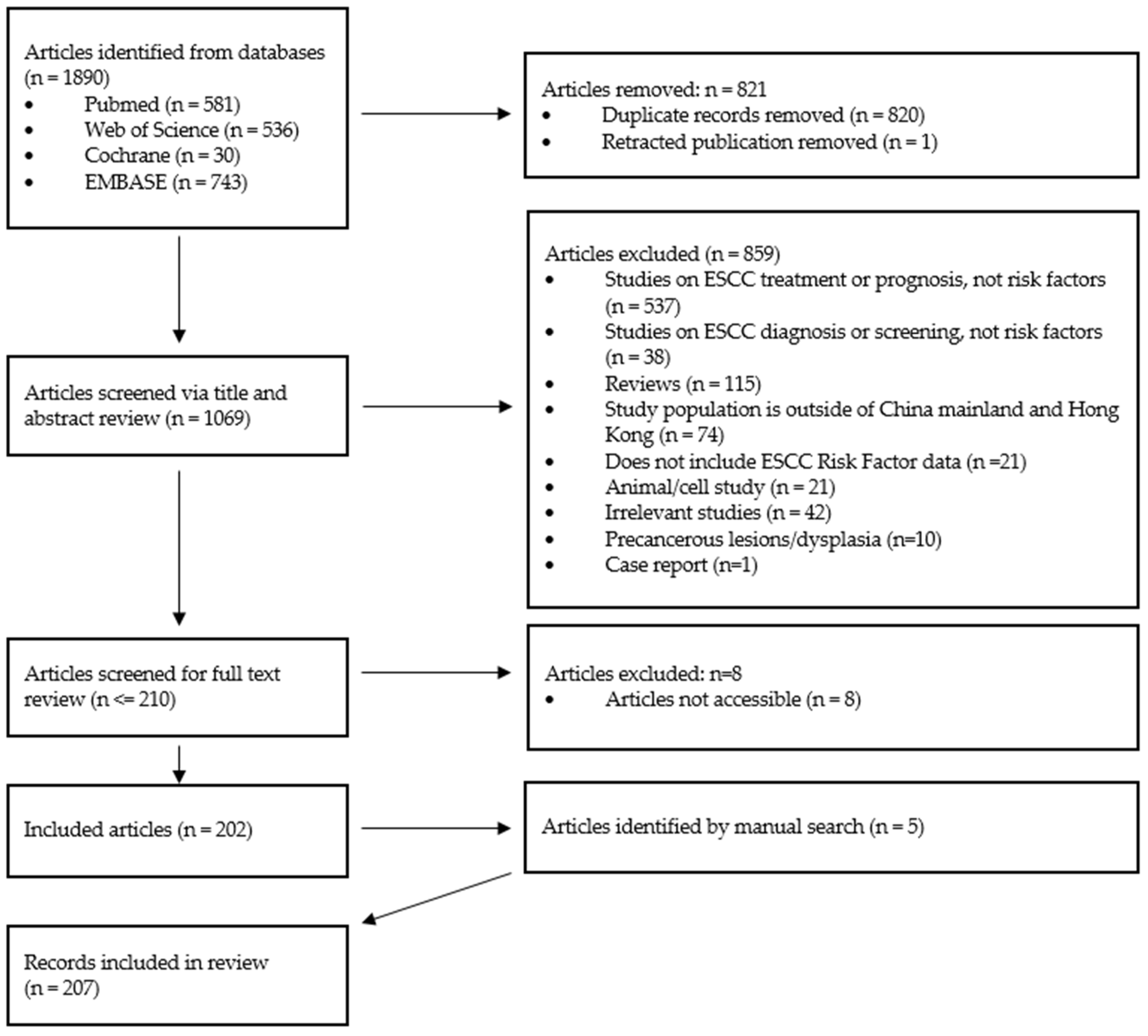
Figure 2.
Estimated study count per Chinese province.
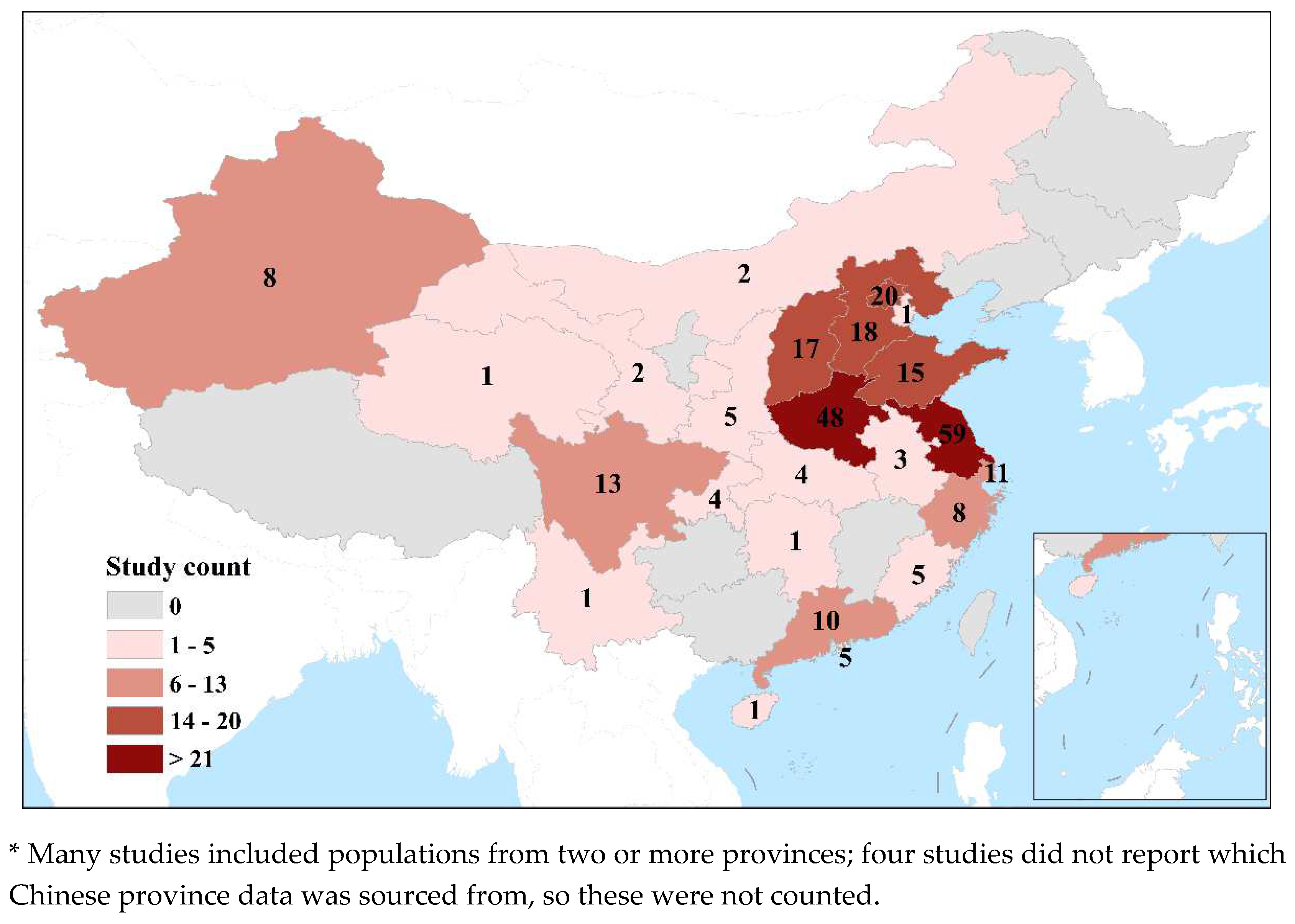

Table 1.
Database search terms used for each online database.
| Database | Search terms |
|---|---|
| Pubmed | ("risk factor" OR "risk factors") AND ("esophageal squamous cell carcinoma" OR "oesophageal squamous cell carcinoma" OR "esophageal squamous-cell carcinoma" OR "oesophageal squamous-cell carcinoma") AND ("China" or "Chinese") Filters: Human, English |
| Web of Science | ("risk factor" OR "risk factors") AND ("esophageal squamous cell carcinoma" OR "oesophageal squamous cell carcinoma" OR "esophageal squamous-cell carcinoma" OR "oesophageal squamous-cell carcinoma") AND ("China" or "Chinese") |
| Cochrane trials | All text: (risk factor OR risk factors) AND (China OR Chinese) AND (esophageal squamous cell carcinoma OR oesophageal squamous cell carcinoma OR oesophageal squamous-cell carcinoma OR esophageal squamous-cell carcinoma) Filters: English, Human |
| Embase | All text: (risk factor OR risk factors) AND (China OR Chinese) AND (esophageal squamous cell carcinoma OR oesophageal squamous cell carcinoma OR oesophageal squamous-cell carcinoma OR esophageal squamous-cell carcinoma) Filters: English, Human, has an abstract, and exported only articles. Selected exclusions: conference abstracts, reviews, articles in press, preprints |
Table 2.
Studies divided into groups based on potential intervening risk factors.
| Study Group | Count (n = 207) |
|---|---|
| Genetic | 129 (62.3%) |
| Diet/dietary habits | 22 (10.6%) |
| HPV | 19 (9.2%) |
| Other | 11 (5.3%) |
| Gene-environ. interaction | 10* (4.8%) |
| Multiple risk factors | 6 (2.9%) |
| Oral Health | 5 (2.4%) |
| Family history | 3 (1.4%) |
| H. pylori | 2** (1.0%) |
* 2 additional studies investigated risk associated with Gene-environment interactions but were counted under the Oral Health category in this list. ** 1 additional study investigated risk associated with H. pylori but was counted under the Multiple risk factors category in this list.
Table 3.
Study population ethnicity
| Study population ethnicity | Count (n = 207) |
| Not reported | 138 (66.7%) |
| Han | 66 (31.9%) |
| Kazakh | 2 (1%) |
| Uyghur, Kazakh, or Han | 1 (0.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



