
Submitted:
22 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
Hallux valgus deformity (HVD) involves subluxation of the first metatarsophalangeal joint. While HVD is primarily considered a forefoot condition, midfoot instability may play a significant role in its development and severity. Therefore, this review had a particular focus on understanding midfoot instability based upon weightbearing imaging assessments of the TMT joint. This review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and searched five databases for studies on midfoot instability in HVD patients. Severity of HVD was defined by hallux valgus angle (HVA) and distal metatarsal articular angle (DMAA). Data was extracted, and articles were graded using the Methodological Index for Non-Randomized Studies (MINORS). Of 547 initially retrieved articles, 23 met inclusion criteria. Patients with HVD showed higher HVA and DMAA on weight-bearing radiographs (WBRG) and weight-bearing computed tomography (WBCT) compared to healthy individuals. Midfoot instability was assessed through intermetatarsal angle (IMA) and tarsometatarsal angle (TMT angle). Patients with HVD exhibited greater IMA and TMT angles on both WBRG and WBCT. This review highlights the importance of weight-bearing imaging assessments for midfoot instability in HVD. IMA and TMT angles can differentiate between healthy individuals and HVD patients, emphasizing the significance of midfoot assessment in understanding HVD pathology.
Keywords:
Hallux Valgus Deformity
; Midfoot Instability
; WBCT
; Systematic Review
; Imaging
1. Introduction
Hallux valgus deformity (HVD), a common foot and ankle condition, [1,2] relates to a medial shift of the first metatarsal head followed by a lateral shift of the proximal phalanx. [3] As HVD progresses, subluxation of the first metatarsophalangeal (MTP) joint is observed. [1] HVD is predominantly described as a forefoot condition, but biomechanical failure or hereditary conditions at any point along the first ray can lead to hallux valgus. [3] Therefore, measurements that assess the entire first ray, such as intermetatarsal angle, [4,5,6,7,8,9] may describe the condition more comprehensively. Studies have eluded that hypermobility of the first tarsometatarsal (TMT) is related to HVD severity, [4,10,11,12,13] but the number of studies analyzing solely midfoot instability in HVD patients is slim. However, midfoot assessments of HVD have allowed for a more comprehensive assessment of HVD as various TMT measurements may directly lead to changes in corresponding MTP measurements. [14] Furthermore, reliability of forefoot measurements associated with HVD have shown greater variability than midfoot related measurements. [15] Therefore, it’s of great interest to study HVD from the midfoot, as the entirety of the first ray mobility can be more completely assessed.
While there are previous systematic reviews pertaining to HVD, topics are limited to demographic, [16] treatment, [17] and outcome-based studies. [18] Furthermore, no review dedicated solely to analyzing HVD imaging-based studies has been performed, particularly in weightbearing. As a proper imaging assessment may lead to a more complete pre-operative assessment, a review focused on radiographic assessment of HVD is of high interest. Therefore, the primary aim of this systematic review was to summarize all studies pertaining to HVD, with a particular focus on understanding midfoot instability based upon weightbearing imaging assessments of the TMT joint.
2. Materials and Methods
2.1. Study Creation
This study is a systematic review examining midfoot instability in patients with confirmed HVD assessed via weight-bearing imaging modalities to further explore the understanding of how HVD impacts the midfoot, potentially guiding treatment in the future. This systematic review was performed in line with the most recent Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for optimal clarity. [19] Five databases – PubMed, SPORTDiscus, CINAHL, MEDLINE, and Web of Science – were searched from database creation until July 6th, 2023. The search algorithm used in each of the five databases to address our study objective was (hallux valgus OR bunion) AND (medial column OR midfoot OR tarsometatarsal OR “tarsal-metatarsal” OR “metatarsal-cuneiform” OR Lisfranc) AND (mobility OR instability OR stability OR rotation).
2.2. Inclusion and Exclusion Criteria
Inclusion criteria was articles that examined the midfoot region, articles that had patients with a diagnosis of HVD, articles that were full-text, articles that were in English, and randomized controlled trials or observational studies with at least ten patients. Exclusion criteria was articles not examining the TMT joint/midfoot, articles that only had healthy patients or patients without a diagnosis of HVD, articles not having full-text, abstract, articles not in English, systematic reviews, meta-analyses, books, case reports, case series with nine patients or less, and clinical commentaries. Articles that involved surgical correction to HV were included if they reported preoperative (i.e. non-surgical) values that could be used to assess for the impact of the HV on the midfoot region.
2.3. Study Definitions
As several studies reported both healthy patients as well as patients with HVD, it was necessary to use measurements to define the severity of HVD in this study. Severity of HVD was defined in this study via hallux valgus angle (HVA) and distal metatarsal articular angle (DMAA). Furthermore, the main objective of this study was to examine the severity of midfoot instability and pathology. For the purposes of this study, severity of midfoot instability was primarily defined via measurements such as intermetatarsal angle (IMT angle), tarsometatarsal angle (TMT angle) in various imaging views. Weight-bearing imaging was defined as weight-bearing radiograph (WBRG) or computed tomography (WBCT).
2.4. Article Screening Process
After all the five databases were searched with the aforementioned algorithm, all of the retrieved articles were downloaded into Rayyan, an online public software commonly utilized in the literature to allow for efficient article screening. [20] Duplicate articles were first removed manually and then all remaining articles were screened by title and abstract via the inclusion and exclusion criteria. Article screening was performed by multiple authors. After screening by title and abstract, articles were screened by full-text for final article inclusion.
2.5. Data Extraction
Data extraction was performed by a single author. Data extracted from the included articles include first author, year of publication, type of study, number of patients, number of feet, average patient age, type of imaging modality (weight-bearing radiograph or weight-bearing CT), HVA (degrees), IMT angle (degrees), TMT angle (degrees), sagittal lift (mm), and Meary’s angle (degrees).
2.6. Article Quality Grading
All observational studies were graded via the Methodological Index for Non-Randomized Studies (MINORS) as previously used in the literature for systematic reviews and meta-analyses. [21] The MINORS scale differentiates between comparative and non-comparative studies, with comparative studies being out of 0–24 points and non-comparative studies being out of 16 points. Each item on the MINORS scale assesses the quality of the article and is worth 0–2 points. All grading was completed by one author.
2.7. Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 29.0 (Armonk, NY: IBM Corp) was used for analysis in this systematic review. Descriptive statistics (means, frequencies) and frequency weighted means were utilized to report the data. Due to the heterogeneity of the data, a narrative approach to systematic review with qualitative statistics was used as meta-analysis could not be performed.
3. Results
3.1. Initial Study Results
A total of 23 articles met the inclusion criteria from 547 articles initially retrieved from the five databases utilized in this systematic review. [14,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44] Refer to Figure 1 for the PRISMA diagram outlining the search process for this systematic review.
3.2. Article Quality Results
All 23 included articles were graded via the MINORS scale due to the observational nature of the included studies. The mean MINORS score for all included articles (n=23 articles) was 10.4 ± 4.0 points (range: 5.0–20.0 points). Based on study type, the mean MINORS score was 8.4 ± 1.9 points (range: 5.0–12.0 points) for non-comparative studies and 16.2 ± 2.0 points (range: 14.0–20.0 points) for comparative studies. Refer to Table 1 for more specific information on the MINORS grading for each individual article included in this study.
3.3. General Patient Demographics
Total patients (n=962) had a frequency weighted mean age of 45.5 ± 6.4 years (n=962; 100% of patients reported). However, three studies did not report the number of patients, but reported the number of feet investigated in their study. Furthermore, 20 out of 23 articles reported on the number of feet investigated with a total of 1,232 feet included in this systematic review. Based on patient subgroup, there were 851 patients with HV and 111 healthy patients without HV used as comparison groups in some of the included studies. The frequency weighted mean age of patients with HV (n=851) was 45.6 ± 6.4 years and the frequency weighted mean age of healthy patients without HV (n=111) was 44.2 ± 6.3 years. Of the 1,232 feet included in this study, 1,057 feet belonged to patients with HV and 175 feet belonged to healthy patients without HV. In terms of imaging modality, 196 patients (20.4%) were evaluated via WBCT and 766 patients (79.6%) were evaluated using WBRG. Refer to Table 2 for more specific information on the demographics and patient information for each individual included article.
3.4. Severity of Hallux Valgus by Imaging
For severity of HV as defined by HVA and/or DMAA, patients with HV evaluated with WBCT (n=185 feet) had a frequency weighted mean HVA (axial view) of 31.2 ± 1.4 degrees (n=112; 60.5% of feet reported), a mean HVA (coronal view) of 28.6 degrees (n=10 feet; 5.4% of feet reported) and a frequency weighted mean HVA (sagittal view) of 33.1 ± 5.8 degrees (n=41; 22.2% of feet reported). Healthy patients without HV evaluated with WBCT (n=175 feet) had a frequency weighted mean HVA (axial view) of 10.5 ± 1.8 degrees (n=109; 62.2% of feet reported), a mean HVA (coronal view) of 11.0 degrees (n=36 feet; 20.6% of feet reported) or a mean HVA (sagittal view) of 14.1 degrees (n=10; 5.7% of feet reported). For severity of HV as defined by HVA and/or DMAA, patients with HV evaluated by WBRG (n=872 feet) had a frequency weighted mean HVA (anterior-posterior) of 28.9 ± 6.7 degrees (n=673; 77.2% of feet reported). The frequency weighted mean DMAA on WBRG (n=263 feet) was 14.7 ± 4.5 degrees for patients with HV. Refer to Table 2 for more specific information on the demographics and patient information for each individual included article.
3.5. Midfoot Instability via Intermetatarsal Angle
Kimura et al. (2017) reported a significantly greater TMT angle (sagittal) on WBCT in patients with HV as compared to healthy patients without HV (22.1 versus 9.3 degrees; p<0.01). [38] Similarly, Randich et al. (2021) reported a significantly greater TMT angle (frontal) on WBCT in patients with HV as compared to healthy patients without HV (16.5 versus 8.7 degrees; p<0.001). [42] Both Lee et al. (2022) and Ji et al. (2023) reported significantly greater IMT angles (axial view) on WBCT in patients with HV as compared to healthy patients without HV (p<0.001 and p<0.01, respectively). [14,28] The frequency weighted mean TMT angle (axial) on WBCT was 15.4 ± 1.0 degrees for patients with HV (n=112 feet) and 8.6 ± 0.5 degrees for healthy patients without HV (n=109 feet). The frequency weighted mean IMT angle (anterior-posterior) on WBRG for patients with HV (n=763 feet) was 15.2 ± 2.7 degrees. Refer to Table 3 for more information on IMT angles from individual articles included in this systematic review.
3.6. Midfoot Instability via Tarsometatarsal angle
The frequency weighted mean TMT angle (sagittal view) on WBCT was 1.9 ± 1.4 degrees for patients with HV (n=122 feet) as compared to 0.9 ± 0.7 degrees in healthy patients without HV (n=119 feet). From individual articles, both Kimura et al. (2017) and Lee et al. (2022) found significantly larger TMT angles (sagittal view) on WBCT in patients with HV compared to healthy patients without HV (p<0.01 and p<0.001, respectively). [14,38] Likewise, Ji et al. (2023) reported a significantly larger TMT angle (sagittal view) in patients with HV as compared to healthy patients without HV on WBCT (1.6 versus 0.9 degrees; p<0.01). [28] From a different view, Randich et al. (2021) reported a TMT angle (frontal view) on WBCT of -5.36 ± 6.28 degrees in patients with HV as compared to -1.28 ± 6.33 degrees in healthy patients without HV (p=0.08). [42] On WBRG, King et al. (2004) reported higher absolute TMT angles (anterior-posterior and lateral view) of 11.0 ± 7.0 degrees and 13.0 ± 8.0 degrees in patients with HV as compared to TMT angles (anterior-posterior and lateral view) of 8.0 ± 4.0 degrees and 4.0 ± 8.0 degrees in healthy patients without HV. [30] Refer to Table 3 for more information on TMT angles from individual articles included in this study.
4. Discussion
In this systematic review, analysis of the midfoot region of the foot was performed for patients of confirmed HVD. To the authors’ knowledge, this is the first review to study HVD from an image-based perspective, as all previous reviews have been centered around prevalence and outcome-based topics. While these topics are of high interest, a review focused strictly on pre-operative imaging is of great interest, as proper pre-operative radiographic assessment is essential for surgical planning. [45] While a review focused on the MTP joint would be insightful, a midfoot assessment was chosen for this review for two reasons. (1) Increased TMT instability and first ray hypermobility has been linked to increased HVD severity, [14,26,46] and (2) the recent emergence of weightbearing computed topography (WBCT) allows for three-dimensional assessment of the entire first ray, [47,48,49] allowing for measurements that are difficult on pain radiographs. Furthermore, MTP joint measurements of HVD indicate the severity of the resulting deformity, not necessarily revealing the cause of deformity. As instability at any point along the first ray can cause HVD, [3] understanding the impact that the midfoot has on the pathology of HVD was of high interest for this review. As no direct comparison of measurements across studies was possible, this review’s purpose remains in summarizing the importance of weightbearing and midfoot assessment when planning for HVD correction.
The most common midfoot measurements to analyze HVD were intermetatarsal angle (IMA) and tarsometatarsal angle (TMT angle). Each included study was able to differentiate healthy and HVD using these measurements, regardless of image modality. As WBCT has yet to become universal care for foot and ankle clinics, this conclusion was encouraging for WBRG. However, while WBRG manual measurements have demonstrated reliability, [50] two-dimensional analysis of HVD may lead to less detailed pre-operative planning due to HVD often including a rotational aspect of the first ray. [51] As improper correction of first ray/medial column rotation is tied to poor HVD post-operative outcomes, accurate measurement of midfoot parameters is of high priority. [52] Fortunately, studies that compare the rotational measurement sensitivity of WBRG and WBCT have found agreement between the two image modalities. [53,54] However, WBCT has shown increased sensitivity when assessing rotation, likely due to its inherent three-dimensional advantage. [54] One concern still surrounds the reliability and consistency of WBRG scan protocol when assessing these measurements. [15] While no study has found significant differences for TMT angles in lateral views, dorsoplantar view has shown to differ significantly with varying scan protocol. [15] It is interesting to note that differences in scan protocol led to greater variability for traditional WBRG forefoot measurements than WBRG midfoot measurements, suggesting that midfoot analysis is not only potentially more comprehensive, but also more reliable regardless of scan protocol. [15] While some may suggest that WBCT scan protocol may also vary significantly due to WB being painful for severe deformities, there is little to no evidence suggesting that HVD causes significant pain in static stance.
While this review described the severity of injury based upon a forefoot measurement (HV angle), evidence exists suggesting that forefoot measurements are a direct result of medial column/first ray alignment. [14] Even though HVD is most evident at the metatarsal head, [3] data suggests patient-specific anatomy and biomechanics of the TMT joint may have an impact on the emergence of HVD. [14] This is due to the TMT joint being the apex of the metatarsal, as well as being the center of rotation of angulation (CORA). [55] Numerous studies point to this joint being the true center of HVD, and indicate that correction of the TMT joint addresses the primary deformity while also preventing the development of secondary deformities that may form in part due to MTP arthrodesis to correct HVD. [56,57,58,59,60,61] While this review was unable to directly statistically assess the sensitivity of TMT measurements, one take-away revolved around the lack of standard TMT measurements. Two measurements to assess an entire three-dimensional deformity are unlikely to provide a complete pre-operative assessment. Furthermore, the method of measurement collection was primarily manual measurement. With the recent advancements in semi-automatic and automatic measurement capabilities, the possibility to not only limit variability, but also provide more standardized, comprehensive pre-operative assessment is possible. [47] Future research and standardization of TMT-related measurements to assess HVD may lead to a more detailed pre-operative plan.
One crucial aspect of this review was its focus on weightbearing. In included studies that directly compared NWB and WB, significant differences were found between patients with HVD and healthy controls. [37] While it may seem obvious to assess HVD with WB imaging, comprehensive WB assessment is not standard. Many physicians rely on intra-operative assessment of first ray rotation when correcting HVD. [53] As only simulated WB can be obtained within the operating room, and WB changes first ray metrics, [62] there should be an emphasis on consistent, standard WB pre-operative assessment.
Regarding the limitations of this study, the lack of direct comparison between studies is of primary concern. Only two common midfoot measurements were collected across all studies, suggesting that future research should work towards additional standard midfoot measurements. This improvement could allow for meta-analysis of midfoot measurements, providing significant guidance for physicians when deciding which metrics to rely on for pre-operative planning. While this was mentioned previously, the lack of scan protocol standardization across studies is nearly impossible to account for. As changes in WB causes changes in midfoot measurements, [62] it is importance that future research also works to account for differences in scan acquisition. As pain may prevent patients from standing with exact 50/50 load distribution, comparison across studies requires a consistent scan protocol. Furthermore, the studies included in this systematic review were of an observational nature, indicating that bias likely impacted the results of this manuscript. Future research should focus on higher level-of-evidence studies to further solidify the impact of WB imaging on assessment of midfoot instability in patients with HVD.
5. Conclusions
In conclusion, this systematic review focused on WB imaging assessments of midfoot instability in patients with HVD. To the authors’ knowledge, this is the first comprehensive review of HVD from a pre-operative, image-based perspective, emphasizing the importance of midfoot assessment in understanding the pathology of HVD. The review highlighted the significance of measurements such as intermetatarsal angle (IMA) and tarsometatarsal angle (TMT angle) in differentiating between healthy individuals and those with HVD, regardless of the imaging modality used. While weight-bearing radiographs (WBRG) have shown promise in assessing midfoot instability, weight-bearing computed tomography (WBCT) offers a three-dimensional advantage, particularly when evaluating rotational aspects of the first ray. The review also underscored the potential for more standardized and comprehensive pre-operative assessments with the development of semi-automatic and automatic measurement capabilities for TMT-related measurements. Furthermore, the importance of consistent weight-bearing assessment in pre-operative planning was emphasized.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization, G.M.T., A.B., A.A. and S.A; methodology, G.M.T. and A.B.; software, G.M.T., A.B. and B.S.; validation, G.M.T., A.B., K.C.W. and C.N.O.; formal analysis, A.B.; investigation, G.M.T.; data curation, A.B. and B.S.; writing—original draft preparation, G.M.T. and A.B.; writing—review and editing, G.M.T., A.B., A.A., K.C.W., C.N.O. and S.A.; supervision, G.M.T., A.A. and S.A; project administration, G.M.T. and S.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
A.A. receives consulting fees from QPIX and S.A receives consulting fees Stryker Corporation, EXACTECH Inc., Trilliant Surgical LLC, and MedShape Inc.. S.A receives royalties from Flower Orthopedics Corporation, MedShape Inc., and In2Bones LLC.
References
- MANN, R.A. and M.J. COUGHLIN, Hallux valgus—etiology, anatomy, treatment and surgical considerations. Clinical Orthopaedics and Related Research®, 1981. 157: p. 31-41.
- Coughlin, M., Juvenile hallux valgus. Surgery of the Foot and Ankle, 1999.
- Perera, A., L. Mason, and M. Stephens, The pathogenesis of hallux valgus. JBJS, 2011. 93(17): p. 1650-1661. [CrossRef]
- Coughlin, M.J., Instructional course lectures, The American academy of orthopaedic surgeons-hallux valgus. JBJS, 1996. 78(6): p. 932-66.
- Coughlin, M.J., Hallux valgus: causes, evaluation, and treatment. Postgraduate medicine, 1984. 75(5): p. 174-187.
- Hardy, R. and J. Clapham, Hallux valgus predisposing anatomical causes. The Lancet, 1952. 259(6720): p. 1180-1183. [CrossRef]
- Hardy, R. and J. Clapham, Observations on hallux valgus. The Journal of Bone & Joint Surgery British Volume, 1951. 33(3): p. 376-391.
- Hawkins, F., C.L. Mitchell, and D.W. Hedrick, Correction of hallux valgus by metatarsal osteotomy. JBJS, 1945. 27(3): p. 387-394.
- Jones, C.P., et al., The validity and reliability of the Klaue device. Foot & ankle international, 2005. 26(11): p. 951-956. [CrossRef]
- Hansen Jr, S., Hallux valgus surgery. Morton and Lapidus were right! Clinics in podiatric medicine and surgery, 1996. 13(3): p. 347-354.
- Hofbauer, M. and J. Grossman, The Lapidus procedure. Clinics in podiatric medicine and surgery, 1996. 13(3): p. 485-496.
- Johnson, K. and T. Kile, Hallux valgus due to cuneiform-metatarsal instability. Journal of the Southern Orthopaedic Association, 1994. 3(4): p. 273-282.
- Myerson, M., Metatarsocuneiform arthrodesis for treatment of hallux valgus and metatarsus primus varus. 1990, SLACK Incorporated Thorofare, NJ. p. 1025-1031. [CrossRef]
- Lee, H.Y., et al., Multiplanar instability of the first tarsometatarsal joint in hallux valgus and hallux rigidus patients: a case–control study. International Orthopaedics, 2022. 46(2): p. 255-263. [CrossRef]
- Brage, M.E., J.R. Holmes, and B.J. Sangeorzan, The influence of x-ray orientation on the first metatarsocuneiform joint angle. Foot & ankle international, 1994. 15(9): p. 495-497. [CrossRef]
- Nix, S., M. Smith, and B. Vicenzino, Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. Journal of foot and ankle research, 2010. 3: p. 1-9. [CrossRef]
- MANN, R.A., M.J. COUGHLIN, and H.L. DUVRIES, Hallux rigidus: a review of the literature and a method of treatment. Clinical Orthopaedics and Related Research®, 1979(142): p. 57-63.
- Barg, A., et al., Unfavorable outcomes following surgical treatment of hallux valgus deformity: a systematic literature review. The Journal of Bone and Joint surgery. American Volume, 2018. 100(18): p. 1563.
- Page, M.J., et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International journal of surgery, 2021. 88: p. 105906.
- Ouzzani, M., et al., Rayyan—a web and mobile app for systematic reviews. Systematic reviews, 2016. 5: p. 1-10. [CrossRef]
- Slim, K., et al., Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ journal of surgery, 2003. 73(9): p. 712-716. [CrossRef]
- Javed, A., et al., PREVALENCE OF HALLUX VALGUX DEFORMITY IN ADULTS.
- Conti, M.S., et al., Association of first metatarsal pronation correction with patient-reported outcomes and recurrence rates in hallux valgus. Foot & Ankle International, 2022. 43(3): p. 309-320. [CrossRef]
- Conti, M.S., et al., Effect of the modified Lapidus procedure on pronation of the first ray in hallux valgus. Foot & Ankle International, 2020. 41(2): p. 125-132. [CrossRef]
- Coughlin, M.J. and C.P. Jones, Hallux valgus: demographics, etiology, and radiographic assessment. Foot & ankle international, 2007. 28(7): p. 759-777. [CrossRef]
- Faber, F.W., et al., Mobility of the first tarsometatarsal joint in hallux valgus patients: a radiographic analysis. Foot & ankle international, 2001. 22(12): p. 965-969. [CrossRef]
- Greeff, W., et al., Radiographic assessment of relative first metatarsal length following modified lapidus procedure. Foot & Ankle International, 2020. 41(8): p. 972-977. [CrossRef]
- Ji, L., et al., The role of first tarsometatarsal joint morphology and instability in the etiology of hallux valgus: a case-control study. Foot & Ankle International, 2023. 44(8): p. 778-787. [CrossRef]
- Kernozek, T.W. and S.A. Sterriker, Chevron (Austin) distal metatarsal osteotomy for hallux valgus: comparison of pre-and post-surgical characteristics. Foot & ankle international, 2002. 23(6): p. 503-508. [CrossRef]
- King, D.M. and B.C. Toolan, Associated deformities and hypermobility in hallux valgus: an investigation with weightbearing radiographs. Foot & ankle international, 2004. 25(4): p. 251-255. [CrossRef]
- Kopp, F.J., et al., The modified Lapidus procedure for hallux valgus: a clinical and radiographic analysis. Foot & ankle international, 2005. 26(11): p. 913-917. [CrossRef]
- Lalevée, M., et al., Coronal Plane Rotation of the Medial Column in Hallux Valgus: A Retrospective Case-Control Study. Foot & Ankle International, 2022. 43(8): p. 1041-1048. [CrossRef]
- Ahuero, J.S., J.S. Kirchner, and P.M. Ryan, Medial Cuneiform Opening-Wedge Osteotomy for the Treatment of Hallux Valgus. Foot & Ankle Orthopaedics, 2019. 4(1): p. 2473011418813318. [CrossRef]
- Shelton, T.J., et al., The influence of percentage weight-bearing on foot radiographs. Foot & Ankle Specialist, 2019. 12(4): p. 363-369. [CrossRef]
- Ferreyra, M., et al., Can we correct first metatarsal rotation and sesamoid position with the 3D Lapidus procedure? Foot and Ankle Surgery, 2022. 28(3): p. 313-318.
- Ozturk, A.M., et al., Three-dimensional printed anatomical models help in correcting foot alignment in hallux valgus deformities. Indian Journal of Orthopaedics, 2020. 54: p. 199-209. [CrossRef]
- Manceron, A., et al., Correlation between first tarsometatarsal joint mobility and hallux valgus severity. International Orthopaedics, 2022. 46(4): p. 855-859. [CrossRef]
- Kimura, T., et al., Evaluation of first-ray mobility in patients with hallux valgus using weight-bearing CT and a 3-D analysis system: a comparison with normal feet. JBJS, 2017. 99(3): p. 247-255.
- Dayton, P., et al., Comparison of radiographic measurements before and after triplane tarsometatarsal arthrodesis for hallux valgus. The Journal of Foot and Ankle Surgery, 2020. 59(2): p. 291-297. [CrossRef]
- Naguib, S., B. Derner, and A.J. Meyr, Evaluation of the mechanical axis of the first ray before and after first metatarsal-phalangeal joint reconstructive surgery. The Journal of Foot and Ankle Surgery, 2018. 57(6): p. 1140-1142. [CrossRef]
- Oravakangas, R., et al., Proximal opening wedge osteotomy provides satisfactory midterm results with a low complication rate. The Journal of Foot and Ankle Surgery, 2016. 55(3): p. 456-460. [CrossRef]
- Randich, J.R., et al., Frontal plane rotation of the first Ray in hallux valgus using standing computerized tomography (CT). The Journal of Foot and Ankle Surgery, 2021. 60(3): p. 489-493. [CrossRef]
- Thompson, J.M. and C.F. Hyer, Maintenance of Correction of the Modified Lapidus Procedure With a First Metatarsal to Second Metatarsal Screw With “Spot Weld” Technique: A Retrospective and Radiographic Analysis. The Journal of Foot and Ankle Surgery, 2023. [CrossRef]
- Klemola, T., et al., First Tarsometatarsal Joint Derotational Arthrodesis for Flexible Hallux Valgus: Results from Follow-Up of 3–8 Years. Scandinavian Journal of Surgery, 2017. 106(4): p. 325-331. [CrossRef]
- Karasick, D. and K.L. Wapner, Hallux valgus deformity: preoperative radiologic assessment. AJR Am j Roentgenol, 1990. 155(1): p. 119-23. [CrossRef]
- Faber, F.W., et al., Mobility of the first tarsometatarsal joint in relation to hallux valgus deformity: anatomical and biomechanical aspects. Foot & ankle international, 1999. 20(10): p. 651-656. [CrossRef]
- de Carvalho, K.A.M., et al., Comparison between Weightbearing-CT semiautomatic and manual measurements in Hallux Valgus. Foot and Ankle Surgery, 2022. 28(4): p. 518-525.
- Mahmoud, K., et al., The role of weightbearing computed tomography scan in hallux valgus. Foot & Ankle International, 2021. 42(3): p. 287-293. [CrossRef]
- Najefi, A.-A., et al., Imaging findings and first metatarsal rotation in hallux valgus. Foot & Ankle International, 2022. 43(5): p. 665-675. [CrossRef]
- Coughlin, M.J. and E. Freund, The reliability of angular measurements in hallux valgus deformities. Foot & ankle international, 2001. 22(5): p. 369-379. [CrossRef]
- Kim, Y., et al., A new measure of tibial sesamoid position in hallux valgus in relation to the coronal rotation of the first metatarsal in CT scans. Foot & ankle international, 2015. 36(8): p. 944-952. [CrossRef]
- Shibuya, N., et al., Factors associated with early loss of hallux valgus correction. The Journal of Foot and Ankle Surgery, 2018. 57(2): p. 236-240. [CrossRef]
- Wagner, P., et al., Validity and reliability of a new radiological method to estimate medial column internal rotation in hallux valgus using foot weight-bearing x-ray. Foot & Ankle Specialist, 2021: p. 19386400211029162. [CrossRef]
- Lintz, F., et al., Three-Dimensional Weightbearing Assessment of the First Ray in Hallux Valgus: A Case-Control Study. Foot & Ankle Orthopaedics, 2019. 4(4): p. 2473011419S00050. [CrossRef]
- Ray, J.J., et al., Multicenter early radiographic outcomes of triplanar tarsometatarsal arthrodesis with early weightbearing. Foot & ankle international, 2019. 40(8): p. 955-960. [CrossRef]
- Dayton, P., M. Kauwe, and M. Feilmeier, Is our current paradigm for evaluation and management of the bunion deformity flawed? A discussion of procedure philosophy relative to anatomy. The Journal of Foot and Ankle Surgery, 2015. 54(1): p. 102-111. [CrossRef]
- Mashima, N., et al., Correction of hallux valgus deformity using the center of rotation of angulation method. Journal of Orthopaedic Science, 2009. 14(4): p. 377-384. [CrossRef]
- Mortier, J.-P., J.-L. Bernard, and M. Maestro, Axial rotation of the first metatarsal head in a normal population and hallux valgus patients. Orthopaedics & Traumatology: Surgery & Research, 2012. 98(6): p. 677-683. [CrossRef]
- Paley, D., et al., Deformity planning for frontal and sagittal plane corrective osteotomies. Orthopedic Clinics of North America, 1994. 25(3): p. 425-466. [CrossRef]
- Tanaka, Y., et al., Radiographic analysis of hallux valgus. A two-dimensional coordinate system. JBJS, 1995. 77(2): p. 205-213. [CrossRef]
- Wagner, E., C. Ortiz, and P. Wagner, Using the center of rotation of angulation concept in hallux valgus correction: why do we choose the proximal oblique sliding closing wedge osteotomy? Foot and Ankle Clinics, 2018. 23(2): p. 247-256.
- Watanabe, K., et al., Three-dimensional analysis of tarsal bone response to axial loading in patients with hallux valgus and normal feet. Clinical Biomechanics, 2017. 42: p. 65-69. [CrossRef]
Figure 1.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram for this systematic review depicting the search process.
Figure 1.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram for this systematic review depicting the search process.
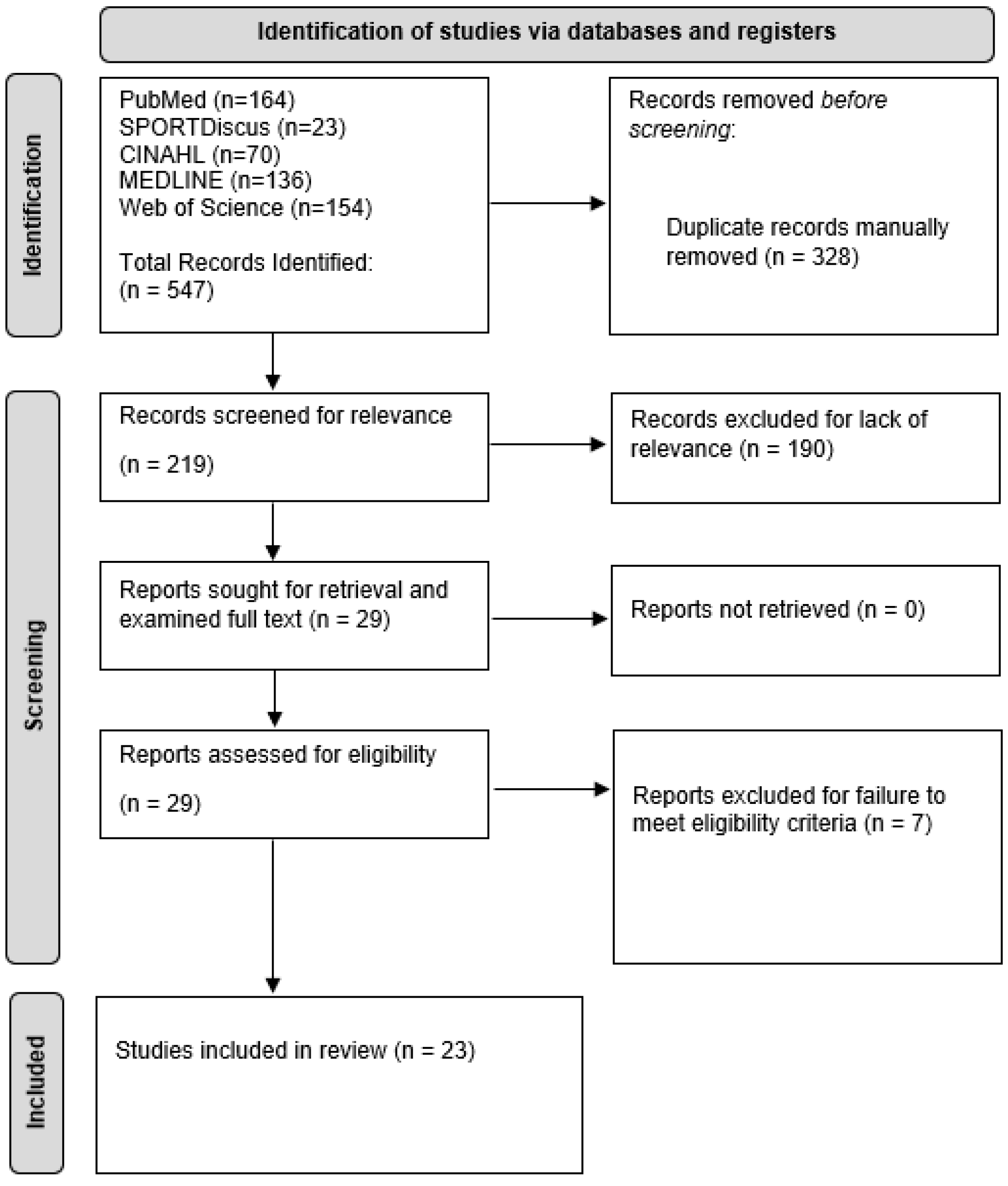

Table 1.
The Methodological Index for Non-Randomized Studies (MINORS) grading results for the included articles in this systematic review. Each item is worth 0–2 points for a total possible 16 points for non-comparative studies and 24 points for comparative studies.
Table 1.
The Methodological Index for Non-Randomized Studies (MINORS) grading results for the included articles in this systematic review. Each item is worth 0–2 points for a total possible 16 points for non-comparative studies and 24 points for comparative studies.
| Author (Year) | Study Type | Total MINORS Score | Clearly stated aim | Inclusion of consecutive patients | Prospective collection of data | End points appropriate to study aim | Unbiased assessment of study end point | Follow-up period appropriate to study aim | Less than 5% lost to follow up | Prospective calculation of the study size | Adequate control group | Contemporary groups | Baseline equivalence of groups | Adequate statistical analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Conti (2020) | Non-comparative | 10 | 2 | 2 | 0 | 2 | 1 | 1 | 2 | 0 | - | - | - | - |
| King (2004) | Comparative | 15 | 2 | 2 | 1 | 1 | 0 | 0 | 2 | 0 | 2 | 2 | 1 | 2 |
| Ferreyra (2022) | Non-comparative | 8 | 2 | 2 | 0 | 2 | 0 | 0 | 2 | 0 | - | - | - | - |
| Kernozek (2002) | Non-comparative | 6 | 1 | 1 | 0 | 1 | 0 | 1 | 2 | 0 | - | - | - | - |
| Dayton (2020) | Non-comparative | 9 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 0 | - | - | - | - |
| Lalevée (2022) | Comparative | 16 | 2 | 1 | 1 | 2 | 0 | 0 | 2 | 0 | 2 | 2 | 2 | 2 |
| Manceron (2022) | Non-comparative | 8 | 2 | 2 | 0 | 2 | 0 | 0 | 2 | 0 | - | - | - | - |
| Conti (2022) | Non-comparative | 12 | 2 | 2 | 1 | 2 | 0 | 1 | 2 | 2 | - | - | - | - |
| Kimura (2017) | Comparative | 20 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 |
| Naguib (2018) | Non-comparative | 7 | 2 | 1 | 0 | 2 | 0 | 0 | 2 | 0 | - | - | - | - |
| Klemola (2017) | Non-comparative | 7 | 2 | 1 | 0 | 1 | 0 | 2 | 1 | 0 | - | - | - | - |
| Randich (2021) | Comparative | 16 | 2 | 2 | 0 | 2 | 0 | 0 | 2 | 2 | 1 | 2 | 1 | 2 |
| Coughlin (2007) | Non-comparative | 10 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 0 | - | - | - | - |
| Thompson (2023) | Non-comparative | 9 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 0 | - | - | - | - |
| Ahuero (2019) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Faber (2001) | Non-comparative | 6 | 1 | 1 | 0 | 2 | 0 | 0 | 2 | 0 | - | - | - | - |
| Lee (2022) | Comparative | 14 | 2 | 2 | 0 | 2 | 0 | 0 | 2 | 0 | 1 | 2 | 1 | 2 |
| Oravakangas (2016) | Non-comparative | 8 | 2 | 2 | 0 | 2 | 0 | 2 | 0 | 0 | - | - | - | - |
| Greeff (2020) | Non-comparative | 5 | 2 | 1 | 0 | 2 | 0 | 0 | 0 | 0 | - | - | - | - |
| Almaawi (2021) | Non-comparative | 9 | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | - | - | - | - |
| Kopp (2005) | Non-comparative | 8 | 2 | 2 | 0 | 1 | 0 | 1 | 2 | 0 | - | - | - | - |
| Ji (2023) | Comparative | 16 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 |
| Ozturk (2020) | Non-comparative | 8 | 2 | 1 | 0 | 2 | 0 | 1 | 2 | 0 | - | - | - | - |
Table 2.
Patient demographics for the included articles in this systematic review and meta-analysis. Data recorded included first author, year of publication, type of study, type of patient by group (healthy or patient with hallux valgus (HV)), number of patients, number of feet (due to possible bilateral HV), average patient age (standard deviation and range), imaging modality (weight bearing radiographs (WBRG) or weight bearing computed tomography (WBCT)), and measures of HV severity (hallux valgus angle (HVA) by imaging view and dorsal metatarsal articular angle (DMAA)).
Table 2.
Patient demographics for the included articles in this systematic review and meta-analysis. Data recorded included first author, year of publication, type of study, type of patient by group (healthy or patient with hallux valgus (HV)), number of patients, number of feet (due to possible bilateral HV), average patient age (standard deviation and range), imaging modality (weight bearing radiographs (WBRG) or weight bearing computed tomography (WBCT)), and measures of HV severity (hallux valgus angle (HVA) by imaging view and dorsal metatarsal articular angle (DMAA)).
| Author (year) | Study type | Treatment group | Patients (n) | Feet (n) | Mean age (standard deviation) (range) | Imaging Modality | HVA (AP) | HVA (lateral) | HVA (axial) | HVA (sagittal) | HVA (frontal) | DMAA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Conti (2020) | Retrospective | HV | 31 | 31 | 51.2 (29–67) | WBCT | - | - | - | 29.9 (17–47) | - | - |
| Lalevée (2022) | Retrospective | Healthy | 20 | 20 | 37.3 (16.5) | WBCT | - | - | - | - | - | - |
| HV | 22 | 22 | 40.1 (17.4) | - | - | - | - | - | - | |||
| Kimura (2017) | Retrospective | Healthy | 10 | 10 | 56 (5) (50–66) | WBCT | - | - | - | 14.1 (2.8) | - | - |
| HV | 10 | 10 | 58 (14.2) (33–74) | - | - | - | 43.2 (10.1) | - | - | |||
| Randich (2021) | Retrospective | Healthy | 36 | 36 | 49.31 (12.71) | WBCT | - | - | - | - | 11.03 (6.56) | - |
| HV | 10 | 10 | 53.00 (19.35) | - | - | - | - | 28.66 (10.99) | - | |||
| Lee (2022) | Retrospective | Healthy | 30 | 30 | 42.97 (17.52) | WBCT | - | - | 7.52 (4.49) | - | - | - |
| HV | 27 | 30 | 54.20 (14.01) | - | - | 33.50 (9.47) | - | - | - | |||
| Ji (2023) | Retrospective | Healthy | - | 79 | 42 (32–51) | WBCT | - | - | 11.6 (10.1–14.0) | - | - | - |
| HV | - | 82 | 46 (37–55) | - | - | 30.4 (22.4–38.6) | - | - | - | |||
| Conti (2022) | Retrospective | HV | 39 | - | 51.5 (24.1–64.3) | WBRG | 33.2 (10.7) | - | - | - | - | - |
| WBCT | - | - | - | - | - | - | ||||||
| King (2004) | Prospective | Healthy | 15 | - | 36 (15) (18–62) | WBRG | 5 (3) | - | - | - | - | - |
| HV | 25 | - | 48 (17) (14–81) | 13 (7) | - | - | - | - | - | |||
| Ferreyra (2022) | Retrospective | HV | 30 | 37 | 45.68 (15–76) | WBRG | 32.12 | - | - | - | - | - |
| Kernozek (2002) | Retrospective | HV | 25 | - | 43 (40–60) | WBRG | 31.7 (4.7) | - | - | - | - | - |
| Naguib (2018) | Retrospective | HV | - | 59 | - | WBRG | 11.59 (3.79) | - | - | - | - | - |
| Klemola (2017) | Retrospective | HV | 66 | 84 | 47.9 (10.2) | WBRG | 30.1 (7.0) | - | - | - | - | - |
| Coughlin (2007) | Retrospective | HV | 103 | 122 | 50 (22–78) | WBRG | 30 (20–53) | - | - | - | - | 10 (0–20) |
| Thompson (2023) | Retrospective | HV | 77 | 90 | 48.8 (16.2) | WBRG | - | - | - | - | - | - |
| Ahuero (2019) | Retrospective | HV | 13 | 14 | 56 (22–75) | WBRG | 32 (26.5–41) | - | - | - | - | - |
| Faber (2001) | Prospective | HV | 94 | 109 | 41.4 (15–63) | WBRG | - | - | - | - | - | - |
| Oravakangas (2016) | Retrospective | HV | 20 | 23 | 50 (22–69) | WBRG | 38 (5) | - | - | - | - | - |
| Greeff (2020) | Retrospective | HV | 23 | 32 | 43 (20–68) | WBRG | 33 (16–46) | - | - | - | - | 16 (4–26) |
| Almaawi (2021) | Retrospective | HV | 89 | 100 | 40.7 | WBRG | 33.2 (8.0) | - | - | - | - | - |
| Kopp (2005) | Retrospective | HV | 29 | 34 | 54.2 (27–84) | WBRG | 33.6 (17–61) | - | - | - | - | - |
| Ozturk (2020) | Prospective | HV | 10 | 10 | 59.3 (15.8)(25–72) | WBRG | 38.4 (6.5) | - | - | - | - | - |
| Manceron (2022) | Retrospective | HV | - | 20 | - | WBRG | 32 | - | - | - | - | - |
| HV | - | 20 | - | 34.2 | - | - | - | - | - | |||
| HV | - | 9 | - | 37.9 | - | - | - | - | - | |||
| Dayton (2020) | Retrospective | HV | 108 | 109 | 33.9 (14.1) | WBRG | 22.9 (7.6) | - | - | - | - | 19.6 (9.2) |
Table 3.
Imaging assessments of midfoot instability in patients with HV and healthy patients without HV in the individual articles included in this study. Data recorded includes first author, year of publication, patient group (patients with hallux valgus (HV) or healthy patients), number of patients, number of feet, intermetatarsal angle (IMT angle), tarsometatarsal angle (TMT angle) by view, sagittal lift (in millimeters), and Meary’s angle.
Table 3.
Imaging assessments of midfoot instability in patients with HV and healthy patients without HV in the individual articles included in this study. Data recorded includes first author, year of publication, patient group (patients with hallux valgus (HV) or healthy patients), number of patients, number of feet, intermetatarsal angle (IMT angle), tarsometatarsal angle (TMT angle) by view, sagittal lift (in millimeters), and Meary’s angle.
| Author (Year) | Treatment Group | Patients | # Feet | IMT Angle (AP) | IMT Angle (Lateral) | IMT Angle (Axial) | IMT Angle (Sagittal) | IMT Angle (Frontal) | TMTAngle (AP) | TMTAngle (Lateral) | TMTAngle (Axial) | TMTAngle(Sagittal) | TMTAngle (Frontal) | Sagittal Lift (mm) | Meary’s Angle |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Conti (2020) | HV | 31 | 31 | - | - | - | 16.7 (10–25) | - | - | - | - | - | - | - | - |
| Lalevée (2022) | Healthy | 20 | 20 | - | - | - | - | - | - | - | - | - | - | - | - |
| HV | 22 | 22 | - | - | - | - | - | - | - | - | - | - | - | - | |
| Kimura (2017) | Healthy | 10 | 10 | - | - | - | 9.3 (1.3) | - | - | - | - | 3.2 (1.3) | - | - | - |
| HV | 10 | 10 | - | - | - | 22.1 (4.1) | - | - | - | - | 6.5 (2.6) | - | - | - | |
| Randich (2021) | Healthy | 36 | 36 | - | - | - | - | 8.77 (2.45) | - | - | - | - | -1.28 (6.33) | - | - |
| HV | 10 | 10 | - | - | - | - | 16.45 (4.47) | - | - | - | - | -5.36 (6.28) | - | - | |
| Lee (2022) | Healthy | 30 | 30 | - | - | 9.46 (2.58) | - | - | - | - | - | 0.23 (0.42) | - | - | - |
| HV | 27 | 30 | - | - | 16.98 (5.27) | - | - | - | - | - | 1.15 (1.23) | - | - | - | |
| Ji (2023) | Healthy | - | 79 | - | - | 8.3 (7.8–8.7) | - | - | - | - | - | 0.9 (0.8–1.0) | - | - | - |
| HV | - | 82 | - | - | 14.8 (11.8–16.7) | - | - | - | - | - | 1.6 (1.6–2.1) | - | - | - | |
| Conti (2022) | HV | 39 | - | 15.6 (3.2) | - | - | - | - | - | - | - | - | - | - | - |
| - | - | - | - | - | - | - | - | - | - | - | - | ||||
| King (2004) | Healthy | 15 | - | 8 (2) | - | 0.0001 | - | - | 8 (4) | 4 (8) | - | - | - | 0.3 (0.5) | - |
| HV | 25 | - | 15 (3) | - | - | - | 11 (7) | 13 (8) | - | - | - | 2 (2) | - | ||
| Ferreyra (2022) | HV | 30 | 37 | 16.42 | - | - | - | - | 27.2 (7.3) | - | - | - | - | - | - |
| Kernozek (2002) | HV | 25 | - | 14.5 (1.7) | - | - | - | - | - | - | - | - | - | - | - |
| Naguib (2018) | HV | - | 59 | 23.86 (7.76) | - | - | - | - | - | - | - | - | - | - | - |
| Klemola (2017) | HV | 66 | 84 | 13.3 (2.7) | - | - | - | - | - | - | - | - | - | - | -3.7 (6.8) |
| Coughlin (2007) | HV | 103 | 122 | 14.5 (7–23) | - | - | - | - | - | - | - | - | - | - | - |
| Thompson (2023) | HV | 77 | 90 | 14.9 (3.1) | - | - | - | - | - | - | - | - | - | - | - |
| Ahuero (2019) | HV | 13 | 14 | 16 (9.5–21) | - | - | - | - | - | - | - | - | - | - | - |
| Faber (2001) | HV | 94 | 109 | - | - | - | - | - | - | 12.9 (4.8) | - | - | - | - | - |
| Oravakangas (2016) | HV | 20 | 23 | 17 (2) | - | - | - | - | - | - | - | - | - | - | -5 (8) |
| Greeff (2020) | HV | 23 | 32 | 15 (11–20) | - | - | - | - | - | - | - | - | - | - | - |
| Almaawi (2021) | HV | 89 | 100 | 14.4 (3.3) | - | - | - | - | - | - | - | - | - | - | 5.5 (4.1) |
| Kopp (2005) | HV | 29 | 34 | 15.9 (10–22) | - | - | - | - | - | - | - | - | - | - | - |
| Ozturk (2020) | HV | 10 | 10 | 13.8 (0.5) | - | - | - | - | - | - | - | - | - | - | - |
| Manceron (2022) | HV | - | 20 | 13.3 | - | - | - | - | - | - | - | - | - | - | - |
| HV | - | 20 | 14.8 | - | - | - | - | - | - | - | - | - | - | - | |
| HV | - | 9 | 16.9 | - | - | - | - | - | - | - | - | - | - | - | |
| Dayton (2020) | HV | 108 | 109 | 13.3 (2.4) | - | - | - | - | - | - | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



