Submitted:
22 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
Regular assessment of mood is used in Brazil for a wide variety of purposes, including screening athletes to provide an indicator of psychological wellbeing and risk of mental health issues. The present study tested the psychometric characteristics of the Brazil Mood Scale (BRAMS) using both “right now” and “past week” response time frames and investigated between-group differences in mood based on athlete sex, age, and social vulnerability. Participants were 898 athletes (511 male, 387 female, age range: 12–44 years) from eight sports. Structural equation modelling supported the BRAMS measurement model using both response time frames independently and in a multi-sample analysis. Subscale reliability was supported for both time frames. Fatigue, depression, and tension scores were higher using the past week time frame than the right now time frame. Males reported higher vigor scores than females, and younger participants (<18 years) reported lower scores for anger and depression than older participants (18+ years). No significant between-group differences emerged for social vulnerability. Findings supported the psychometric integrity of the BRAMS and its use as a screening measure for psychological wellbeing among youth and elite athletes in Brazil.
Keywords:
Brazil
; wellbeing
; mood
; emotion
; performance
; elite sport
; youth sport
1. Introduction
Elite sport organizations increasingly demonstrate a commitment to safeguarding the psychological wellbeing of athletes while also striving to maximize performance [1,2]. As part of this commitment, it is commonplace for sport organizations to use some form of psychological indicator to screen for wellbeing and risk of mental health issues. Regular mood assessments have been shown over several decades to have predictive utility for both psychological wellbeing [3,4] and performance outcome [5,6]. The mood construct has been defined as “a set of feelings, ephemeral in nature, varying in intensity and duration, and usually involving more than one emotion” (p.17) [7] with moods having both a valence dimension varying from positive (e.g., happy) to negative (e.g., depressed) and an arousal dimension varying from activation (e.g., alert) to deactivation (e.g., tired) [8]. Morgan’s mental health model [3] postulated that a mood profile referred to as the iceberg profile, which is characterized by above average scores for vigor combined with below average scores for tension, depression, anger, fatigue, and confusion, is indicative of positive mental health and is associated with superior sports performance. Subsequent meta-analytic reviews of the mood and sport performance literature have provided support for the benefits of the iceberg mood profile [5,6].
Several other mood profiles have been identified in the sport psychology literature [9]. For example, the inverse iceberg profile, characterized by above average scores for tension, depression, anger, fatigue, and confusion, coupled with below average scores for vigor, has been linked to overtraining syndrome [10,11], poor athletic performance [5,6] and a heightened risk of mental health issues [12]. Another mood profile that is indicative of poor performance and elevated risk of psychopathology, referred to as the inverse Everest profile, is characterized by low vigor scores, high scores for tension and fatigue, and very high scores for depression, anger, and confusion [9]. The surface profile is characterized by average scores on all mood dimensions, the submerged profile by below average scores on all mood dimensions, and the shark fin profile by below average scores for tension, depression, anger, vigor, and confusion, combined with very high fatigue scores [9].
Mood profiles are often used to compare individual scores to normative scores, to assess deviations from a typical mood, as a way of screening for psychological wellbeing and risk of mental health issues [12]. Mood profiles have been shown to be effective in identifying individual athletes experiencing significant emotional difficulties, particularly when used in combination with data gathered by other sports science professionals [13]. Most published measures in psychology were originally produced in the English language, presenting a challenge for researchers and practitioners who work in other languages. Until 2006, there was no validated version of the Brunel Mood Scale (BRUMS) [14,15], a derivative of the Profile of Mood States (POMS) [16], that was suitable for use in a Brazilian context. Rohlfs and colleagues [11] addressed this gap in the literature, validating the Brazil Mood Scale (BRAMS), which represented an important pre-cursor for further investigations in Brazil. Since its development, more than 400 published studies have used the BRAMS in, for example, several sports contexts related to athlete well-being [17-20] and performance [21-24], and in non-sport environments related to psychological responses to illness [25-27] and rehabilitation [28-29].
1.1. Influence of Response Time Frame on Mood Assessment
When conducting mood research or assessing mood for applied purposes, it is important to consider the influence of response time frame on mood assessments. It has been demonstrated that mood scores tend to vary according to whether respondents are asked to report how they feel “right now” or how they have felt “over the past week including today” [16,30]. As an example, mood scores of schoolchildren based on the past week time frame were significantly higher than the average scores derived from multiple right now assessments covering the same period; and recall of past week mood was highly correlated with mood at the time of recall [30]. Hence, it is likely that respondents who are, for example, angry at the time of assessment will more readily recall incidents of anger over the past week [31].
An important step in testing the impact of different response time frames on the psychometric properties of a measure, is to evaluate the degree of invariance of the measurement model across response time frames. Without that step, the mood scores of individuals or groups may not be supported by the underlying measurement structure. The BRAMS was validated for the Brazilian population to allow a quick assessment of mood state among populations of adults and adolescents, and all tables of normative data were based on right now data [11], meaning that normative scores may not apply to data collected using other response time frames. In this context, the BRAMS has still to be validated using the past week response time frame. The developers of the original POMS, McNair et al. [16], recommended use of the past week response time frame since they considered it was a long enough period to capture typical and persistent emotional reactions to daily life events, yet short enough to assess the acute effects of treatments of psychiatric outpatients, which was their primary population of interest. They also indicated the feasibility of using other response time frames, appropriate to the purpose of a study, or applied use of the mood scale.
1.2. Between-group Differences in Mood
When using standardized assessment tools such as the BRAMS, it is important to consider between-group differences because they may necessitate different tables of normative data for specific groups. Variations in mood responses have previously been identified among both athletes and the general population according to the sex and age of participants [32-34], which prompted consideration of these variables in the present study. Social vulnerability is another variable of particular interest within the current context. Youth athletes contending with poor housing, unstable family work conditions, and low incomes are considered as high-risk candidates for mental health issues [35,36]. A mental health survey of more than 1,200 residents of Rio de Janeiro’s slums, referred to as favelas, showed that over one third experienced anxiety, depression, post-traumatic stress, or suicidal ideation [37]. Economic disadvantage is pervasive and violence commonplace in the favelas, where many athletes in the present study live. Notably, the prevalence of mental health issues in the Cruz study [37] was highest among younger people and females. Therefore, investigation of social vulnerability as a situational variable that might influence mood scores was considered to be important.
1.3. Aims of the Study
The primary aim of the present study was to validate the measurement model of the BRAMS among youth and elite athletes using both past week and right now response time frames. A secondary aim was to assess between-group differences in BRAMS scores according to the sex, age, and social vulnerability of the athletes.
2. Materials and Methods
2.1. Participants
A total of 898 athletes from a prominent multisport club in Rio de Janeiro, Brazil participated in the study. Respondents were in two groups according to the response time frame used to assess mood (i.e., right now, or past week). The right now group comprised 481 athletes (male = 282, female = 199) from eight sports (artistic swimming, basketball, gymnastics, judo, rowing, swimming, volleyball, and water polo) aged from 12 to 44 years (M = 17.41 ± 4.36 years). The past week group comprised 417 athletes (male = 229, female = 188) from the same eight sports, also aged from 12 to 44 years (M = 17.72 ± 4.54 years). A full breakdown of the participant characteristics is shown in Table 1. All athletes were members of the Unified Center for the Identification and Development of Performance Athletes (CUIDAR, which is Portuguese for “care”), a program that provides training and multidisciplinary support, encompassing medicine, nursing, physiotherapy, strength and conditioning, massage therapy, nutrition, social service, and psychology, to more than 1000 youth and elite athletes.
2.2. Measurement of Mood
The Brazil Mood Scale (BRAMS) [11] was used to assess mood. The BRAMS is a 24-item measure to assess the mood subscales of tensão (tension), depressão (depression), raiva (anger), vigor (vigor), fadiga (fatigue), and confusão (confusion), each of four items. One group of participants indicated how they were feeling “right now” on a 5-point Likert-type scale, where 0 = nada (not at all), 1 = um pouco (a little), 2 = moderadamente (moderately), 3 = bastante (quite a bit), and 4 = extremamente (extremely). A second group of participants indicated how they had been feeling “over the past week including today” on the same 5-point scale. Possible subscale scores range from 0-16, with higher scores indicating higher levels of a mood dimension. The original BRUMS, of which the BRAMS is a direct translation, has demonstrated robust psychometric characteristics [14,15] and has been translated into at least 15 languages [38-52].
2.3. Procedure
Data collection occurred over a 5-month period from April to August 2023, which encompassed a period of preparation and specific training for national and international competitions in Brazil. The BRAMS measure was presented as an online questionnaire created in Google Forms. All participants were provided with a link and instructions for completion via mobile phone under the supevision of the team coach or strength and conditioning coach assigned to their sport, all of whom had received training in the correct completion of the BRAMS. Respondents completed the BRAMS in their normal training environment. Right now measures were taken before or after the first training session of the week. Past week measures were taken at the end of the week before or after the last training session. To assess the test–retest reliability of the right now BRAMS, a sub-sample of 304 participants completed the BRAMS for a second time, with an intervening period of 1–6 weeks. Similarly, to assess the test–retest reliability of the past week BRAMS, a sub-sample of 255 participants completed the BRAMS for a second time, with an intervening period of 1–6 weeks. All participants provided informed consent and were informed that their participation was voluntary and could be withdrawn at any time. The study was approved by the Human Research Ethics Committee of the University of Southern Queensland (#ETH2023-0046).
2.4. Data Analysis
Data were collated for analysis using SPSS version 29 [53] and duplicate entries from the same participants were removed except for those used for the purposes of assessing test-retest reliability. Descriptive statistics were calculated for all BRAMS subscale raw scores for both the right now and past week response time frames. Relationships among BRAMS subscale scores were quantified using Pearson correlation coefficients. To assist the interpretation of group comparisons using multivariate analysis of variance (MANOVA), BRAMS subscale scores were converted into standard scores (T-scores) by comparing raw scores to tables of normative data for adult athletes and adolescent athletes [12]. To avoid the potential for Type I errors in univariate F-tests, a Bonferroni adjustment was applied to the alpha level to account for the six dependent variables (anger, confusion, depression, fatigue, tension, vigor) by dividing p < 0.05 by 6, resulting in an alpha level of p < 0.008.
Confirmatory factor analysis using AMOS was used to test the BRAMS measurement model and several different indices were applied to assess the adequacy of the model. We first considered the chi-squared (χ2) to degrees of freedom (df) ratio (where ratios of < 5 and < 3 represent acceptable and good fitting models, respectively) [54]. However, the χ2 value tends to be significant with large samples (≥ 400 cases) and therefore we did not use this ratio as our primary indicator of model fit [54]. We instead prioritized two incremental fit indices, the comparative fit index (CFI) [55] and the Tucker-Lewis index (TLI) [56], which both adjust for sample size. Values ≥ .90 indicate an acceptable fit and values ≥ .95 indicate a good fit for both the TLI and CFI. Additionally, we applied the root mean square error of approximation (RMSEA) [57], indicating the mean discrepancy between the observed covariances and those implied by the model per degree of freedom, thereby avoiding issues related to larger samples. RMSEA values ≤ .05 and ≤ .08 indicate good and acceptable fit, respectively [57]. Finally, we used the root mean square residual (SRMR), a measure of the average of the standardized fitted residuals, where a value of ≤ .08 indicates an acceptable fitting model [54]. Our samples of 481 right now and 421 past week participants exceeded the recommended sample size for confirmatory factor analysis of 10 participants per model parameter [55].
3. Results
Univariate non-normality was apparent in the distributions of some negatively-valenced BRAMS subscales (i.e., anger, confusion, depression) in both the right now and past week datasets. Negative mood dimensions typically show a larger proportion of scores at the lower end, and fewer scores at the upper end [14,15]. High scores on negatively-valenced mood dimensions are of particular interest from an applied perspective because they suggest elevated risk of mental health issues. Similar non-normality was reported in past BRUMS validation studies [44,50,58], with adequate model fit being obtained without data transformation. Further, in line with the recommendation of Nevill and Lane [59] that self-report measures should not be transformed with measurement scales at the interval level, no data transformations occurred.
In the right now dataset, 46 multivariate outliers (p < 0.001) were identified using the Mahalanobis distances test, and another 37 multivariate outliers were identified in the past week dataset. All cases identified as multivariate outliers were scrutinized for response bias in the form of straight-line, acquiescent, or extreme responding [60,61], but none were found. Subsequently, all outliers were retained, and the final samples of 481 right now cases and 417 past week cases were included in the analyses.
Descriptive statistics, reliabilities (alpha coefficients) and intercorrelations among BRAMS subscales for both the right now and past week response time frames are shown in Table 2. Cronbach alpha coefficients for the six subscales ranged from 0.72 to 0.87 for the right now response time frame, and from 0.75 to 0.90 for the past week response time frame, exceeding the threshold of acceptability [62]. In both samples, BRAMS subscales with a negative orientation (i.e., tension, depression, anger, fatigue, confusion) were significantly intercorrelated and either correlated inversely with vigor scores or showed no relationship.
3.1. Confirmatory Factor Analysis
The six-factor BRAMS measurement model that was evaluated using AMOS Version 29 is shown in Figure 1. Mood items and latent factors are shown in both English and Brazilian Portuguese. Results of the CFA to test the adequacy of the measurement model using both the right now and past week response time frames are shown in Table 3. The six-factor measurement model showed acceptable fit with no modifications for both the right now (x2/df = 3.09, CFI = 0.916, TLI = 0.902, RMSEA = 0.066) and past week response time frames (x2/df = 2.65, CFI = 0.933, TLI = 0.921, RMSEA = 0.063) independently and also in a multi-sample CFA (x2/df = 2.87, CFI = 0.924, TLI = 0.912, RMSEA = 0.046). Factor loadings were adequate in both samples, with 17 of the 24 items (70.8%) loading onto the corresponding factor at > 0.70 and only three items (12.5%) loading at < 0.60.
3.2. Test–Retest Reliability.
For the right now time frame, test–retest coefficients for the six subscales ranged from 0.43 (anger) to 0.71 (vigor), which were almost identical to those reported previously [14,15] and judged to be appropriate for a measure of transient psychological states. For the past week time frame, test–retest coefficients for the six subscales ranged from 0.55 (depression) to 0.64 (fatigue), which were also judged to be appropriate for a measure of transient psychological states.
3.3. Right Now vs Past Week Mood Scores
Mood scores for the right now and past week response time frames were compared using MANOVA. Significant differences in mood responses between the two response time frames were identified [Hotelling’s T = 0.091, F (6, 891) = 13.48, p < 0.001, = 0.083], accounting for 8.3% of the common variance. As shown in Table 4, past week scores for fatigue were significantly higher than right now scores, with a moderate effect size. Depression and tension scores were also significantly higher when the past week time frame was used compared to the right now time frame, and in both instances effect sizes were small. Figure 2 shows the right now and past week scores plotted against athlete norms.
3.4. Between-Group Comparisons
MANOVA was used to test for differences in mood responses when participants were grouped by athlete sex, age group, and social vulnerability (see Table 5). Among the right now dataset, significant differences in mood responses were identified for sex [Hotelling’s T = 0.143, F (6, 474) = 11.31, p < 0.001, = 0.125], accounting for 12.5% of the variance. Males reported significantly higher vigor scores than females, with a moderate-to-large effect size. For age group [Hotelling’s T = 0.163, F (6, 474) = 12.88, p < 0.001, = 0.140], younger participants (<18 years) reported significantly lower scores for anger and depression than older participants (18+ years), both moderate effects, accounting for 14.0% of the variance. For social vulnerability [Hotelling’s T = 0.026, F (6, 457) = 1.94, p = 0.073, = 0.025], the multivariate statistic was not significant, and no significant univariate differences were identified.
Similarly, among the past week dataset, significant differences in mood responses were observed for sex [Hotelling’s T = 0.159, F (6, 410) = 10.84, p < 0.001, = 0.137], accounting for 13.7% of the variance. Males reported significantly higher vigor scores than females, with a moderate-to-large effect size. For age group [Hotelling’s T = 0.159, F (6, 410) = 10.86, p < 0.001, = 0.137], younger participants (<18 years) reported significantly lower scores for anger and depression than older participants (18+ years), both moderate effects, accounting for 13.7% of the variance. A marginally significant multivariate effect of social vulnerability was identified [Hotelling’s T = 0.033, F (6, 394) = 2.19, p = 0.044, = 0.032] accounting for 3.2% of variance in mood scores, although no significant univariate effects were found. Two-way MANOVAs conducted to test for interaction effects among the sex, age group, and social vulnerability of the athletes showed no significant interactions for any mood subscale on either response time frame.

Table 5.
MANOVA of BRAMS right now and past week T-scores by sex, age group, and social vulnerability.
Table 5.
MANOVA of BRAMS right now and past week T-scores by sex, age group, and social vulnerability.
| Right Now (N = 481) | ||||||
|---|---|---|---|---|---|---|
| Subscale | Male (n = 282) | Female (n = 199) | F | |||
| M | SD | M | SD | |||
| Anger | 51.22 | 13.43 | 52.95 | 15.04 | 1.75 | 0.12 |
| Confusion | 47.54 | 9.53 | 49.01 | 10.84 | 2.48 | 0.15 |
| Depression | 49.58 | 10.27 | 51.34 | 10.86 | 3.27 | 0.17 |
| Fatigue | 49.52 | 9.40 | 52.01 | 11.62 | 6.67 | 0.24 |
| Tension | 43.95 | 6.80 | 45.73 | 7.95 | 6.93 | 0.24 |
| Vigor | 49.45 | 8.02 | 43.88 | 8.39 | 54.09† | 0.65 |
|
Subscale |
U-18 yr. (n = 303) | 18+ yr. (n = 178) |
F |
|
||
| M | SD | M | SD | |||
| Anger | 49.33 | 8.90 | 56.38 | 0.12 | 29.59† | 0.50 |
| Confusion | 48.33 | 10.76 | 47.83 | 0.15 | 0.28 | 0.05 |
| Depression | 48.31 | 6.95 | 53.71 | 0.17 | 31.30† | 0.51 |
| Fatigue | 49.64 | 9.42 | 52.10 | 0.24 | 6.26 | 0.04 |
| Tension | 44.95 | 7.31 | 44.24 | 0.24 | 1.04 | 0.10 |
| Vigor | 47.32 | 8.56 | 46.85 | 0.65 | 0.33 | 0.05 |
|
Subscale |
Vulnerable (n = 258) | Not vulnerable (n = 206) |
F |
|
||
| M | SD | M | SD | |||
| Anger | 52.54 | 15.52 | 51.45 | 12.66 | 0.67 | 0.08 |
| Confusion | 48.39 | 11.73 | 47.88 | 7.84 | 0.29 | 0.05 |
| Depression | 51.00 | 12.01 | 49.43 | 8.13 | 2.60 | 0.15 |
| Fatigue | 50.73 | 11.53 | 50.59 | 9.21 | 0.02 | 0.01 |
| Tension | 44.31 | 7.52 | 45.32 | 7.26 | 2.11 | 0.14 |
| Vigor | 46.66 | 8.83 | 47.76 | 8.40 | 1.88 | 0.13 |
| Past Week (N = 417) | ||||||
|
Subscale |
Male (n = 229) | Female (n = 188) |
F |
|
||
| M | SD | M | SD | |||
| Anger | 52.66 | 15.11 | 56.56 | 17.88 | 5.83 | 0.24 |
| Confusion | 48.51 | 9.83 | 50.37 | 9.44 | 3.83 | 0.19 |
| Depression | 51.29 | 13.10 | 54.05 | 13.64 | 4.43 | 0.21 |
| Fatigue | 56.37 | 12.29 | 58.53 | 13.24 | 2.96 | 0.17 |
| Tension | 45.34 | 8.26 | 47.09 | 8.35 | 4.61 | 0.21 |
| Vigor | 48.35 | 8.62 | 42.92 | 7.34 | 46.81† | 0.64 |
|
Subscale |
U-18 yr. (n = 252) | 18+ yr. (n = 165) |
F |
|
||
| M | SD | M | SD | |||
| Anger | 51.04 | 10.98 | 59.58 | 21.50 | 28.43† | 0.52 |
| Confusion | 48.97 | 8.36 | 49.92 | 11.44 | 0.96 | 0.10 |
| Depression | 49.73 | 9.26 | 56.81 | 17.15 | 29.74† | 0.53 |
| Fatigue | 55.80 | 12.28 | 59.70 | 13.15 | 9.53* | 0.31 |
| Tension | 46.27 | 8.05 | 45.92 | 8.77 | 0.18 | 0.04 |
| Vigor | 46.26 | 8.52 | 45.36 | 8.47 | 1.13 | 0.11 |
|
Subscale |
Vulnerable (n = 232) | Not vulnerable (n = 169) |
F |
|
||
| M | SD | M | SD | |||
| Anger | 54.31 | 15.92 | 55.09 | 17.84 | 0.22 | 0.05 |
| Confusion | 49.00 | 9.80 | 49.89 | 9.80 | 0.80 | 0.09 |
| Depression | 52.94 | 12.86 | 52.40 | 14.57 | 0.15 | 0.04 |
| Fatigue | 56.97 | 12.84 | 58.47 | 12.53 | 1.36 | 0.12 |
| Tension | 45.24 | 7.76 | 47.46 | 9.15 | 6.86 | 0.26 |
| Vigor | 45.17 | 8.89 | 46.64 | 7.84 | 2.98 | 0.17 |
Note: †p < 0.001, *p < 0.008. Social vulnerability status was unknown for 33 participants.
4. Discussion
This paper reports on an investigation of youth and elite athletes from a prominent multisport club in Rio de Janeiro, Brazil, participating in a multidisciplinary support program known as CUIDAR, designed to safeguard physical and mental health. Mood profiling using the Brazil Mood Scale (BRAMS) occurs regularly with all CUIDAR athletes to help inform support staff about how athletes are coping with training demands and to monitor athletes for their wellbeing status and risk of mental health issues. Both the right now and past week response time frames are used. The primary focus of our investigation was to evaluate the psychometric characteristics of the BRAMS within the specific context of the CUIDAR environment, particularly with regard to the factorial validity of the measurement model, the internal consistency and test-retest reliability of the six mood factors. Our secondary aim was to evaluate between-group differences in mood scores according to the sex, age, and social vulnerability of athletes.
Our findings support the factorial validity of the BRAMS and the reliability of its six factors using both the right now and past week response time frames, confirming it as a psychometrically sound scale for use in Brazilian sporting contexts. The BRAMS has been used widely in Brazil and the current validation of the past week version of the scale extends research opportunities to situations where retrospective assessment of mood over a 7-day period is preferred to a more immediate assessment of present mood using the right now response time frame. Our comparison of mood scores derived from the right now and past week response time frames identified significant differences on three of the BRAMS subscales (fatigue, depression, tension), with higher scores reported for the past week time frame in each instance. Effect sizes were moderate for fatigue and very small for other subscales. These results are similar to a previous comparison of right now and past week mood scores among schoolchildren [30], which showed moderate effects for fatigue and small effects for other subscales, with the past week time frame producing higher scores on all subscales. Users of the BRAMS should be aware that use of the past week time frame may engender higher scores than the right now timeframe even if all else remains constant.
Significant differences in mood scores according to the sex of the athletes in the present study were restricted to the vigor subscale. Male athletes reported significantly higher scores than female athletes using both response timeframes, with moderate effect sizes in each instance. Female athletes reported higher scores than male athletes on all of the negative subscales for both response time frames, although the differences were non-significant and effect sizes were very small to small. These differences, although lesser in magnitude, are generally consistent with previous research, which often finds more positive moods reported by males than females among both athletes and nonathletes. Such differences are typically explained through a combination of biological [63], neurological [64], and psychosocial factors [65,66]. A previous study conducted in Brazil among 953 adolescent athletes similarly showed limited differences in mood responses between male and female athletes [67].
Regarding age group differences in mood responses, the adult (18+ years) group reported significantly higher scores than the youth (< 18 years) group for anger and depression using either response time frame, showing moderate effect sizes in each case. The adult group also reported significantly higher fatigue scores than the youth group using the past week response time frame. These results run counter to previous research, which has often shown reported mood to be more positive among older age groups [12,34,68], typically explained by the tendency of younger individuals to engage more in maladaptive coping strategies, such as rumination, avoidance, and suppression and for people to develop more effective mood regulation strategies as they get older [69]. A recent cross-national analysis of population surveys from 29 countries that included 156,331 respondents [70] identified that the first onset of mental health disorders peaks at approximately age 15 years, with a median age of onset of 19 years for males and 20 years for females. Hence, regular screening for risk of mental health issues among the cohort of participants involved in the present study is especially germane.
The present results showed no significant differences in mood scores using either response time frame between athletes identified as vulnerable due to low socio-economic status and those identified as not vulnerable. This result is counter intuitive, given the results of a prior mental health survey showing a high prevalence of mental health issues among residents of Rio de Janeiro’s favelas, where many of the athletes in our study lived [37]. Social support is regarded as a critical factor in building physical and psychological resilience [71-73], and the fact that mood scores did not differ between vulnerable and non-vulnerable athletes suggests a potential protective effect of the CUIDAR program. Not only were vulnerable athletes exposed to medical and health professional support when they joined the program, often for the first time in their lives, but they also received considerable emotional and psychological support from teammates, coaches, and health professionals.
We acknowledge some inherent limitations of our study. Firstly, we were unable to assess the convergent and divergent validity of the BRAMS due to participants not having completed any concurrent measures. This was because we conducted the study in a real-world setting, which precluded the opportunity to add additional concurrent measures. It should be noted, however, that the concurrent validity of the BRAMS was established previously in the original validation study [11]. Second, given the first author’s position as manager of CUIDAR and to avoid the potential for researcher bias, the responsibility for data collection was allocated to various members of the CUIDAR support team. Although all those responsible for data collection were trained in the use of the BRAMS, the impact of data being collected by different individuals is not known and may be seen as a limitation.
The present study is the first investigation to evaluate the measurement model of the Brunel Mood Scale in any language using the past week response time frame. As such, the results provide a valuable addition to the literature on the measurement of mood, particularly among sporting populations. The findings support use of the past week BRAMS from a psychometric perspective. Regarding future research, the BRAMS is a suitable measure to investigate the prevalence in Brazilian populations of the six mood profile clusters identified in the literature, namely, the iceberg, inverse iceberg, inverse Everest, surface, submerged, and shark-fin profiles [34,67,74]. Another future research direction would be to investigate how specific mood profile clusters are related to performance and risk of mental health issues among Brazilian athletes. It would be particularly worthwhile to test the predictive validity of mood profile clusters in Brazilian populations, for example, by assessing the proportion of individuals reporting the most negative mood profiles (i.e., inverse Everest, inverse iceberg, and shark fin profiles) who subsequently experience injury, overtraining, and/or mental and physical ill-health [75]. Almost the full range of possible scores (range = 0-16) was reported by participants for most BRAMS subscales, indicating that some athletes reported extremely negative moods, reflecting heightened risk of psychopathology. All such individuals would be candidates for follow-up assessment by a clinically trained health professional, and it is therefore encouraging to note such follow-up is an inherent feature of the CUIDAR program, which employs a mental health specialist. The relatively small mood differences between male and female athletes and between older and younger athletes within the current sample appears to obviate the need for separate tables of normative data, and users of the BRAMS should continue to use existing norms [11].
Author Contributions
Conceptualization: I.C.P.M.R., F.N., T.J.G., C.W., P.C.T.; methodology: I.C.P.M.R., F.N., T.J.G., C.W., P.C.T.; validation: I.C.P.M.R., V.R.T., P.C.T.; formal analysis: I.C.P.M.R., V.R.T., P.C.T.; investigation: I.C.P.M.R., C.W.; resources: M.V., P.C.T.; data curation: I.C.P.M.R., P.C.T.; writing—original draft preparation: I.C.P.M.R., V.R.T., P.C.T.; writing—review and editing: I.C.P.M.R., F.N., T.J.G., C.W., M.V., V.R.T., P.C.T.; visualization: I.C.P.M.R., V.R.T., P.C.T.; supervision: P.C.T., F.N., T.J.G., C.W.; project administration: I.C.P.M.R., M.V., V.R.T., P.C.T; funding acquisition: M.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding but was supported financially by Clube de Regatas do Flamengo, Rio de Janeiro, Brazil.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Human Research Ethics Committee of the University of Southern Queensland (#ETH2023-0046).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Acknowledgments
We acknowledge members of the CUIDAR support staff who assisted with data collection, in particular Carlos Alexandre Souto de Assis, Paula Moreira Magalhães, and Adriana de Lacerda Amaral Miranda. We also acknowledge the Executive Board of Olympic Sports, Clube de Regatas do Flamengo, Rio de Janeiro, Brazil for granting permission to conduct the research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Reardon, C.L.; Hainline, B.; Aron, C.M.; et al. Mental health in elite athletes: International Olympic Committee consensus statement. Br J Sports Med. 2019, 53, 667–699. [Google Scholar] [CrossRef] [PubMed]
- Purcell, R.; Pilkington, V.; Carberry, S.; et al. An evidence-informed framework to promote mental wellbeing in elite sport. Front Psychol. 2022, 13, e780359. [Google Scholar] [CrossRef] [PubMed]
- Morgan, W.P. Selected psychological factors limiting performance: A mental health model. In D.H. Clarke, H.M. Eckert (Eds.). Limits of Human Performance. Champaign, IL: Human Kinetics, 1985, 70-80.
- Morgan, W.P.; Brown, D.R.; Raglin, J.S.; O’Connor, P.J.; Ellickson, K. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Beedie, C.J.; Terry, P.C.; Lane, A.M. The Profile of Mood States and athletic performance: Two meta-analyses. J. Appl. Sport Psychol. 2000, 12, 49–68. [Google Scholar] [CrossRef]
- Lochbaum, M.; Zanatta, T.; Kirschling, D.; May, E. The Profile of Moods States and athletic performance: A meta-analysis of published studies. Eur. J. Investig. Health Psychol. Edu. 2021, 11, 50–70. [Google Scholar] [CrossRef] [PubMed]
- Lane, A.M.; Terry, P.C. The nature of mood: Development of a conceptual model with a focus on depression. J. Appl. Sport Psychol. 2000, 12, 16–33. [Google Scholar] [CrossRef]
- Feldman Barrett, L.; Russell, J.A. Independence and bipolarity in the structure of current affect. J. Personality Social Psychol. 1998, 74, 967–984. [Google Scholar] [CrossRef]
- Parsons-Smith, R.L.; Terry, P.C.; Machin, M.A. Identification and description of novel mood profile clusters. Front Psychol. 2017, 8, e1958. [Google Scholar] [CrossRef]
- Budgett, R. Fatigue and underperformance in athletes: The overtraining syndrome. Br. J. Sports Med. 1998, 32, 107–110. [Google Scholar] [CrossRef]
- Rohlfs, I.C.P.M.; Rotta, T.M.; Luft, C.D.B.; Andrade, A.; Krebs, R J.; Carvalho, T.D. Brunel Mood Scale (BRUMS): An instrument for early detection of overtraining syndrome. Rev. Bras. de Medicina do Esporte. 2008, 14, 176–181. [Google Scholar] [CrossRef]
- Terry, P.C.; Parsons-Smith, R.L. Mood profiling for sustainable mental health among athletes. Sustain. 2021, 13, e6116. [Google Scholar] [CrossRef]
- Rohlfs, I.C.P.M; Carvalho, T.; Rotta, T.M.; Krebs, R.J. Application of mood assessment instruments in the detection of overtraining syndrome. Rev. Bras. de Medicina do Esporte. 2004, 10, 111–116. [Google Scholar] [CrossRef]
- Terry, P.C.; Lane, A.M.; Lane, H.J.; Keohane, L. Development and validation of a mood measure for adolescents. J. Sport Sci. 1999, 17, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.C.; Lane, A.M.; Fogarty, G.J. Construct validity of the Profile of Mood States–Adolescents for use with adults. Psychol. Sport Exer. 2003, 4, 125–139. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing are Services, 1971.
- Andrade, A.; Bevilacqua, G.; Casagrande, P.; Brandt, R.; Coimbra, D. Sleep quality associated with mood in elite athletes. Phys. Sportsmed. 2019, 47, 312–317. [Google Scholar] [CrossRef]
- Marques, L.E.; Brandão, M.R.F. Training volume, perceived exertion, and mood states during a training macrocycle. Rev. Bras. Psicol. Esporte, 2010; 3, 63–78. [Google Scholar] [CrossRef]
- Wilke, C.F.; Wanner, S.P.; Santos, W.H.M.; Penna, E.M.; Ramos, G.P.; Nakamura, F.Y.; Duffield, R. Influence of faster and slower recovery-profile classifications, self-reported sleep, acute training load, and phase of the microcycle on perceived recovery in futsal players. Int. J. Sports Physiol. Perform. 2020, 15, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Wilke, C.F.; Wanner, S.P.; Penna, E.M.; Maia-Lima, A.; Santos, W.H.M.; Müller-Ribeiro, F.C.; Mendes, T.T.; Bruzzi, R.S.; Ramos, G.P.; Nakamura, F.Y.; et al. Preseason training improves perception of fatigue and recovery from a futsal training session. Int. J. Sports Physiol. Perform. 2021, 16, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Bevilacqua, G.G.; Coimbra, D.R.; Pereira, F.S.; Brandt, R. Sleep quality, mood and performance: A study of elite Brazilian volleyball athletes. J. Sports Sci. Med. 2016, 15, 601–605. [Google Scholar]
- Bevilacqua, G.G.; Viana, M.S.; Gutierres Filho, P.J.B.; da Silveira Borges, V.; Brandt, R. Estados de Humor e Resultado Esportivo de Uma Equipe ao Longo da Segunda Fase da Liga Nacional de Futsal. Psic. Teor. Pesq. 2019, 35. [Google Scholar] [CrossRef]
- Brandt, R.; Bevilacqua, G.G.; Andrade, A. Perceived sleep quality, mood states, and their relationship with performance among Brazilian elite athletes during a competitive period. J. Strength Cond. Res. 2017, 31, 1033–1039. [Google Scholar] [CrossRef]
- Brandt, R.; Viana, M.S.; Crocetta, T.B.; Andrade, A. Association between mood states and performance of Brazilian elite sailors: Winners vs. non-winners. Cult. Cienc. y Deporte 2016, 11, 119–125. [Google Scholar] [CrossRef]
- Andrade, A.; Steffens, R.D.A.K.; Sieczkowska, S.M.; Coimbra, D.R.; Vilarino, G.T. Acute effect of strength training on mood of patients with fibromyalgia syndrome. Reumatismo, 2019, 71, 141–147. [Google Scholar] [CrossRef]
- Andrade, A.; Steffens, R.; Vilarino, G.T.; Miranda, R.; Benetti, M.; Coimbra, D.R. Preferred exercise and mental health of the patients with fibromyalgia syndrome. Complement. Ther. Clin. Pract. 2020, 40, 101–195. [Google Scholar] [CrossRef]
- Noce, F.; de Castro, H.; Ferreira, T.S.; Guo, J.; de Andrade, A.G.P.; da Costa, V.T. A 6-month comparison of quality of life and mood states between physically active and sedentary college students. Medicina (Ribeirão Preto) 2016, 49, 9–16. [Google Scholar] [CrossRef]
- Brandt, R.; Viana, M.D.S.; Steffens, R.D.A.K.; Silva, R.B.; Sties, S.W.; Gonzáles, A.I.; Carvalho, T.D.; Andrade, A. Profile of mood and associated factors among participants of a program of cardiopulmonary and metabolic rehabilitation. J. Bra. Psiquiatr. 2012, 61, 72–77. [Google Scholar] [CrossRef]
- Sties, S.W.; Gonzáles, A.I.; Netto, A.S.; Wittkopf, P.G.; Lima, D.P.; Carvalho, T. Validation of the Brunel Mood Scale for cardiac rehabilitation program. Brazil J. Sports Med. 2014, 20, 281–284. [Google Scholar] [CrossRef]
- Terry, P.C.; Stevens, M.J.; Lane, A.M. Influence of response time frame on mood assessment. Anxiety Stress Coping. 2005, 18, 279–285. [Google Scholar] [CrossRef]
- Roberts, R.J.; Lane, A.M. Mood responses and regulation strategies used during COVID-19 among boxers and coaches. Front. Psychol. 2021, 12, e624119. [Google Scholar] [CrossRef] [PubMed]
- Masumoto, K.; Taishi, N.; Shiozaki, M. Age and gender differences in relationships among emotion regulation, mood, and mental health. Gerontol. Geriatr. Med. 2016, 2. [Google Scholar] [CrossRef]
- Sanchis-Sanchis, A.; Grau, M.D.; Moliner, A.R.; Morales-Murillo, C.P. Effects of age and gender in emotion regulation of children and adolescentes. Front. Psychol. 2020, 11, e946. [Google Scholar] [CrossRef]
- Terry, P.C.; Parsons-Smith, R.L.; King, R.; Terry, V.R. Influence of sex, age, and education on mood profile clusters. PLoS ONE, 2021; 16, e0245341. [Google Scholar] [CrossRef]
- Mezzina, R.; Gopikumar, V.; Jenkins, J.; Saraceno, B.; Sashidharan, S.P. Social vulnerability and mental health inequalities in the "Syndemic": Call for action. Front. Psychiatry 2022, 13, 894370. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Risks to mental health: An overview of vulnerabilities and risk factors. WHO: Geneva, 2012. [Google Scholar]
- Cruz, M.S.; Silva, E.S.; Jakaite, Z.; Krenzinger, M.; Valiati, L.; Gonçalves, D.; Ribeiro, E.; Heritage, P.; Priebe, S. Experience of neighbourhood violence and mental distress in Brazilian favelas: A cross-sectional household survey. Lancet Glob. Health. 2021, 4, e100067. [Google Scholar] [CrossRef]
- Çakiroğlu, A.A.; Demir, E.; Güçlü, M. The validity and reliability study of the Brunel Mood Scale with the adult athletes (Turkish adaptation). Int. J. Appl. Exerc. Physiol. 2020, 9, 126–140. Retrieved on 01 November 2023 from https://www.proquest.com/scholarly-journals/validity-reliablity-study-brunel-mood-scale-with/docview/2501930466/se-2.
- Cañadas, E.; Monleón, C.; Sanchis, C.; Fargueta, M.; Blasco, E. Spanish validation of BRUMS in sporting and non-sporting populations. Euro. J. Hum. Move. 2017, 38, 105–117. [Google Scholar]
- Hasan, M.M.; Mozibul, H.A.K. Bangla version of the Brunel Mood Scale (BRUMS): Validity, measurement invariance and normative data in non-clinical sample. Heliyon. 2022, 8, e09666. [Google Scholar] [CrossRef]
- Lane, A.M.; Soos, I.; Leibinger, E.; Karsai, I.; Hamar, P. Validity of the Brunel Mood Scale for use with UK, Italian and Hungarian athletes. In: Lane, A.M., editor. Mood and Human Performance: Conceptual, Measurement, and Applied Issues. Hauppauge, NY: Nova Science, 2007, 119–130.
- Lew, P.C.F.; Parsons-Smith, R.L.; Lamont-Mills, A.; Terry, P.C. Cross-cultural validation of the Malaysian Mood Scale and tests of between-group mood differences. Int. J. Environ. Res. Public Health. 2023, 20, e3348. [Google Scholar] [CrossRef]
- Kvĕton, P.; Jelínek, M.; Burešová, I.; Bartošová, K. Czech adaptation of the Brunel Mood States for adolescent athletes. Studia Sportiva. 2020, 14, e12758. [Google Scholar] [CrossRef]
- Quartiroli, A.; Terry, P.C.; Fogarty, G.J. Development and initial validation of the Italian Mood Scale (ITAMS) for use in sport and exercise contexts. Front. Psychol. 2017, 8, e1483. [Google Scholar] [CrossRef] [PubMed]
- Rajkovic, I. Translation and validation of the Brunel Mood Scale for a Serbian athlete population. Unpublished master thesis, University of Jyväskylä, Finland, 2014.
- Rouveix, M.; Duclos, M.; Gouarne, C.; Beauvieux, M.C.; Filaire, E. The 24h urinary cortisol/cortisone ratio and epinephrine/norepinephrine ratio for monitoring training in young female tennis players. Int. J. Sport Med. 2006, 27, 856–863. [Google Scholar] [CrossRef]
- Sahli, H.; Sahli, F.; Saidane, M.; Rebhi, M.; Guelmami, N.; Trabelsi, K.; Jahrami, H.; Ammar, A.; Terry, P.C.; Zghibi, M. Testing the psychometric properties of an Arabic version of the Brunel Mood Scale among physical education students. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1539–1552. [Google Scholar] [CrossRef]
- Terry, P.C.; Malekshahi, M.; Delva, H.A. Development and initial validation of the Farsi Mood Scale. Int. J. Sport Exer. Psychol. 2012, 10, 112–122. [Google Scholar] [CrossRef]
- Terry, P.C.; Potgieter, J.R.; Fogarty, G.J. The Stellenbosch Mood Scale: A dual-language measure of mood. Int. J. Sport Exer. Psychol. 2003, 1, 231–245. [Google Scholar] [CrossRef]
- Terry, P.C.; Skurvydas, A.; Lisinskiene, A.; Majauskiene, D.; Valanciene, D.; Cooper, S.; Lochbaum, M. Validation of a Lithuanian-language version of the Brunel Mood Scale: The BRUMS-LTU. Int. J. Environ. Res. Public Health. 2022, 19, e4867. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, K.; Oyama, T.; Fujiya, H.; Kato, H.; Seki, H.; Kohno, T. Development and validation of the preliminary Japanese version of the Profile of Mood States for adolescents. St. Marianna Med. J. 2006, 32, 539–547. Retrieved on 01 November 2023 from https://www.semanticscholar.org/paper/Development-and-Validation-of-the-Preliminary-of-of-Yatabe-Oyama/c2d17d970b896541a8c2d82fe3efa9452b378608.
- Zhang, C.Q.; Si, G.; Chung, P.K.; Du, M.; Terry, P.C. Psychometric properties of the Brunel Mood Scale in Chinese adolescents and adults. J. Sport Sci. 2014, 32, 1465–1476. [Google Scholar] [CrossRef]
- IBM, Corp. IBM SPSS Statistics for Windows, Version 29.0. Armonk, NY: IBM Corp, 2022.
- Kline, R.B. Principles and Practice of Structural Equation Modeling. New York: Guilford, 2015.
- Bentler, P.M. Comparative fit indexes in structural models. Psych. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychomet. 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Beh. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef]
- Han, C.; Parsons-Smith, R.L.; Fogarty, G.J.; Terry, P.C. Psychometric properties of the Brunel Mood Scale in a Singaporean sporting context. Int. J. Sport Exer. Psychol. 2021, 19, 1–17. [Google Scholar] [CrossRef]
- Nevill, A.; Lane, A.M. Why self-report “Likert” scale data should not be log-transformed. J. Sports Sci. 2007, 25, 1–2. [Google Scholar] [CrossRef]
- Leiner, D.J. Too fast, too straight, too weird: Non-reactive indicators for meaningless data in Internet surveys. Surv. Res. Meth. 2019, 13, e7403. [Google Scholar] [CrossRef]
- Meisenberg, G.; Williams, A. Are acquiescent and extreme response styles related to low intelligence and education? Pers. Indiv. Diff. 2008, 44, 1539–1550. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, USA, 1994. [Google Scholar]
- Amin, Z.; Canli, T.; Epperson, C.N. Effect of estrogen-serotonin interactions on mood and cognition. Behav. Cog. Neuro. Rev. 2005, 4, 43–58. [Google Scholar] [CrossRef]
- Ruigrok, A.N.V.; Salimi-Khorshidi, G.; Lai, M.C.; Baron-Cohen, S.; Lombardo, M.V.; Tait, R.J.; Suckling, J. A meta-analysis of sex differences in human brain structure. Neurosci. Biobehav. Rev. 2014, 39, 34–50. [Google Scholar] [CrossRef]
- Dorius, S.F.; Firebaugh, G. Trends in global gender inequality. Soc. Force. 2010, 88, 1941–1968. [Google Scholar] [CrossRef] [PubMed]
- Stamarski, C.S.; Son Hing, L.S. Gender inequalities in the workplace: The effects of organizational structures, processes, practices, and decision makers' sexism. Front. Psychol. 2015, 6, e1400. [Google Scholar] [CrossRef] [PubMed]
- Brandão, R. F.; Correa, M.; Sermarine, M.; Angelo, D L.; Parsons-Smith, R.L.; Terry, P.C. Psychometric re-evaluation of the Brazil Mood Scale and evidence of mood profile clusters among youth athletes in Brazil. Int. J. Sport Exerc. Psychol. 2021; 19, S183–S184. [Google Scholar] [CrossRef]
- Global Burden of Disease 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiat. 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.J.,; Al-Hamzawi, A., Alonso, J., Altwajiri, Y., Andrade, L.H., Bromet, E.J.; et al. Age of onset and cumulative risk of mental disorders: A cross-national analysis of population surveys from 29 countries. Lancet Psychiat. 2023; 10, 668–681. [CrossRef]
- Ozba, F.; Johnson, D.C.; Dimoulas, E.; Morgan, C.A.; Charney, D.; Southwick, S. Social support and resilience to stress: From neurobiology to clinical practice. Psychiatry (Edgmont). 2007, 4, 35–40. [Google Scholar]
- Ozbay, F.; Fitterling, H.; Charney, D.; Southwick, S. Social support and resilience to stress across the life span: A neurobiologic framework. Curr. Psychiatry Rep. 2008, 10, 304–310. [Google Scholar] [CrossRef]
- Løseth, G.E.; Eikemo, M.; Trøstheim, M.; Meier, I.M.; Bjørnstad, H.; Asratian, A.; Pazmandi, C.; Tangen, V.W.; Heilig, M.; Leknes, S. Stress recovery with social support: A dyadic stress and support task. Psychoneuroendocrinology 2022, 146, e105949. [Google Scholar] [CrossRef]
- Terry, P.C.; Parsons-Smith, R.L.; Skurvydas, A.; Lisinskienė, A.; Majauskienė, D.; Valančienė, D.; Cooper, S.; Lochbaum, M. Physical activity and healthy habits influence mood profile clusters in a Lithuanian population. Sustain. 2022, 14, e10006. [Google Scholar] [CrossRef]
- Noce, F.; da Costa, V.T.; Zanetti, M.C.; Brandão, M.R.F.; Winckler, C.; Rodrigues, F.V.; Wolff, A.A.; de Melo, C.C. Mental health in Brazilian sport: Olympic, Paralympic, and soccer athletes. In Mental Health in Elite Sport 2021, 45–56. London, UK: Routledge.
Figure 1.
Six-factor measurement model of the Brazil Mood Scale.
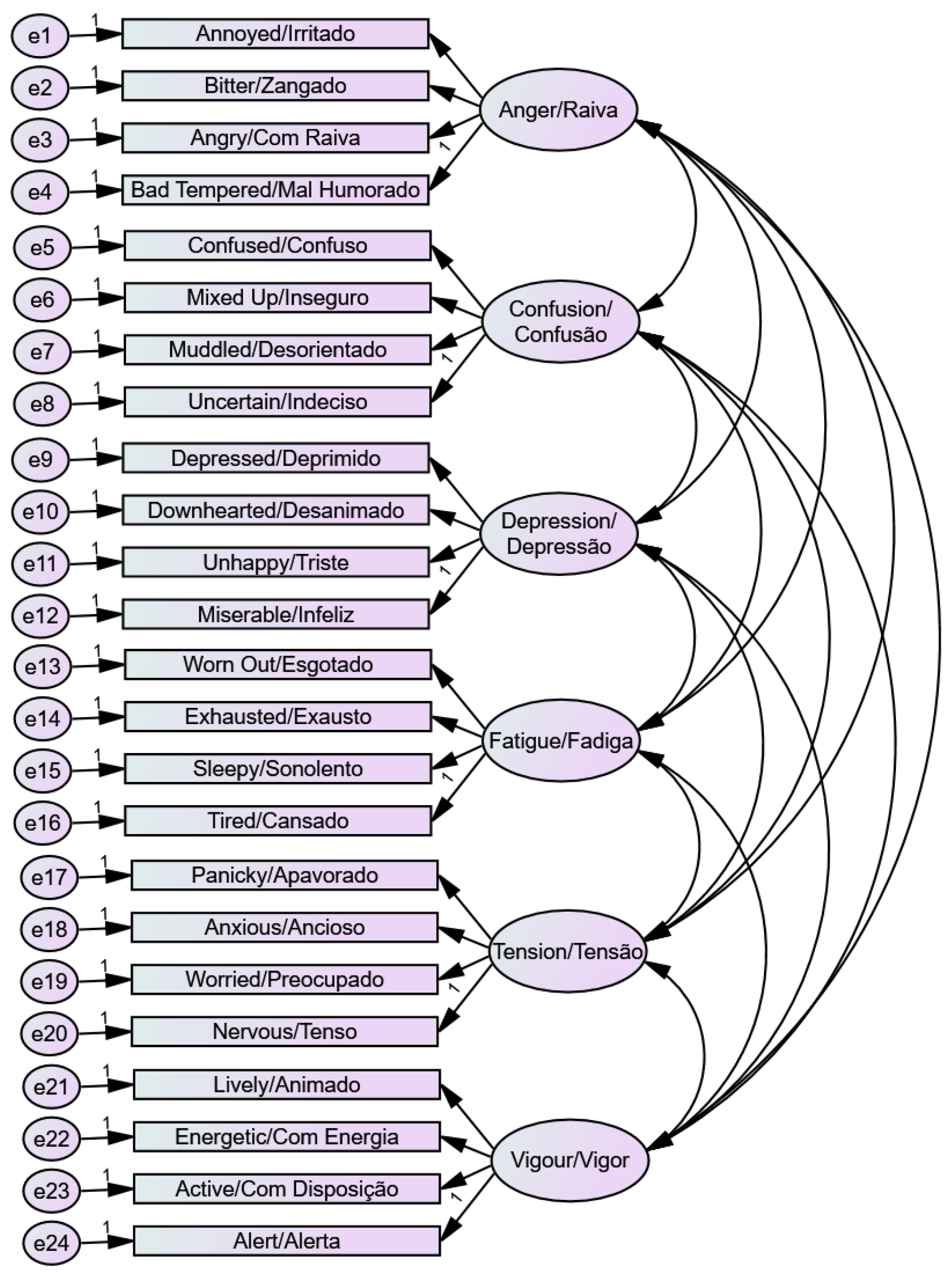
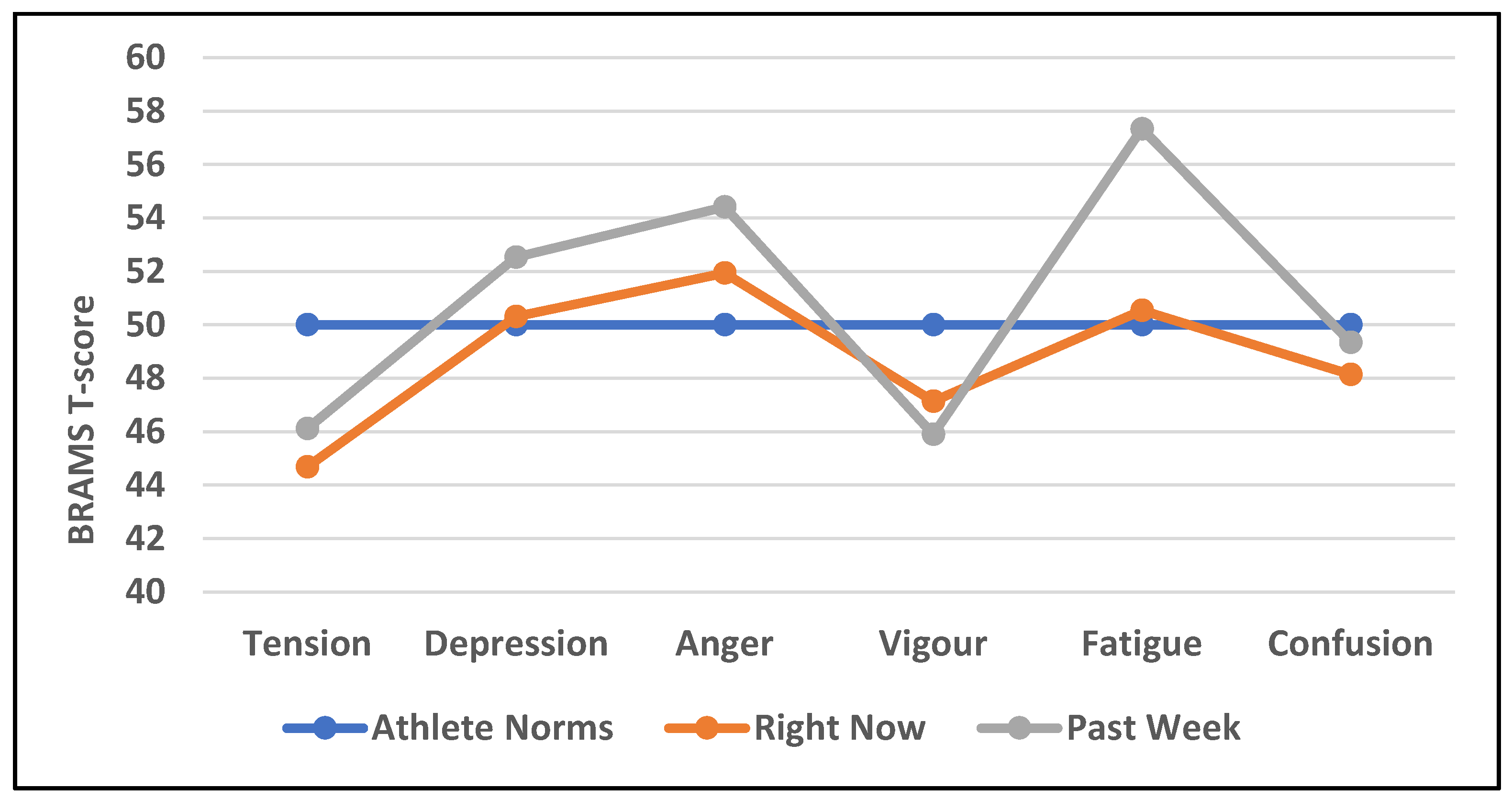
Table 1.
Demographic and situational distribution of the sample (N = 898).
| Source | Group | Right Now n % |
Past Week n % |
|---|---|---|---|
| Sex | Male | 282 58.6 | 229 54.9 |
| Female | 199 41.4 | 188 45.1 | |
| Age Group | 12-17 years | 303 63.0 | 252 60.4 |
| 18+ years | 178 37.0 | 165 39.6 | |
| Social Vulnerability | Vulnerable | 258 55.6 | 232 57.9 |
| Not vulnerable | 206 44.4 | 169 42.1 | |
| Sport | Artistic Swimming | 27 5.6 | 24 5.8 |
| Basketball | 55 11.4 | 22 5.3 | |
| Gymnastics | 10 2.1 | 10 2.4 | |
| Judo | 40 8.3 | 35 8.4 | |
| Rowing | 104 21.6 | 98 23.5 | |
| Swimming | 75 15.6 | 70 16.8 | |
| Volleyball | 93 19.3 | 83 19.9 | |
| Water Polo | 77 16.0 | 75 18.0 | |
| Total | All | 481 100.0 | 417 100.0 |
Note. Social vulnerability status was unknown for 33 participants.
Table 2.
Descriptives, reliabilities and intercorrelations for right now (n = 481) and past week (n = 417) response time frames.
Table 2.
Descriptives, reliabilities and intercorrelations for right now (n = 481) and past week (n = 417) response time frames.
| Time frame | Subscale | M | SD | Range | T-Score | α | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Right now | 1 Anger | 1.29 | 2.46 | 0–14 | 45–137 | 0.87 | 0.56* | 0.69* | 0.50* | 0.54* | -0.11 |
| 2 Confusion | 1.32 | 2.20 | 0–13 | 42–115 | 0.79 | 0.65* | 0.46* | 0.67* | -0.05 | ||
| 3 Depression | 1.05 | 2.00 | 0–14 | 45–120 | 0.80 | 0.51* | 0.58* | −0.22* | |||
| 4 Fatigue | 3.22 | 3.12 | 0–16 | 40–93 | 0.83 | 0.47* | −0.27* | ||||
| 5 Tension | 2.13 | 2.42 | 0–12 | 37–76 | 0.72 | 0.04 | |||||
| 6 Vigor | 7.39 | 3.52 | 0–16 | 29–70 | 0.80 | ||||||
| Past week | 1 Anger | 1.74 | 2.89 | 0–16 | 45–150 | 0.90 | 0.58* | 0.71* | 0.36* | 0.58* | −0.05 |
| 2 Confusion | 1.69 | 2.43 | 0–15 | 42–102 | 0.79 | 0.65* | 0.37* | 0.69* | 0.02 | ||
| 3 Depression | 1.49 | 2.57 | 0–15 | 45–139 | 0.87 | 0.37* | 0.54* | −0.20* | |||
| 4 Fatigue | 5.26 | 3.83 | 0–16 | 40–93 | 0.85 | 0.35* | −0.26* | ||||
| 5 Tension | 2.63 | 2.76 | 0–14 | 37–80 | 0.75 | 0.12 | |||||
| 6 Vigor | 6.89 | 3.48 | 0–16 | 29–67 | 0.78 |
Note: *p < 0.001.
Table 3.
Model testing of the BRAMS using right now and past week response time frames.
| Group | N | x2 | df | x2/df | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|---|---|---|
| Right now 6-factor model | 481 | 733.48* | 237 | 3.09 | 0.916 | 0.902 | 0.066 | 0.063 |
| Past week 6-factor model | 417 | 617.78* | 237 | 2.61 | 0.932 | 0.921 | 0.063 | 0.067 |
| Multisample (right now/past week) | 898 | 1360.47* | 474 | 2.87 | 0.924 | 0.912 | 0.046 | 0.052 |
Note: CFI = comparative fix index, TLI = Tucker–Lewis index, RMSEA = root mean square error of approximation, SRMR = standardized root mean square residual, *p < 0.001.
Table 4.
MANOVA of BRAMS T-scores by response time frame. .
| Subscale | Right Now (n = 481) | Past Week (n = 417) | F | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| Anger | 51.94 | 14.13 | 54.42 | 16.51 | 5.90 | 0.16 |
| Confusion | 48.15 | 10.11 | 49.35 | 9.69 | 3.26 | 0.12 |
| Depression | 50.31 | 10.54 | 52.53 | 13.40 | 7.74* | 0.19 |
| Fatigue | 50.55 | 10.43 | 57.34 | 12.76 | 76.97† | 0.56 |
| Tension | 44.69 | 7.34 | 46.13 | 8.34 | 7.59* | 0.18 |
| Vigor | 47.14 | 8.62 | 45.90 | 8.50 | 4.68 | 0.14 |
Note: †p < 0.001, *p < 0.008.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



