Submitted:
23 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
(1) Background: Breast cancer (BC) is the second largest cause of mortality in female worldwide. Besides from basic risk factors, there are several hereditary variables that contribute to BC. Breast cancer has been linked to a variety of nuclear DNA changes as well as mitochondrial DNA alterations. The aim of this study was to analysis the association of mitochondrial tRNA leucine2 gene with BC. (2) Material and methods: In the current study, 24 samples have been collected from various families in Peshawar. DNA was extracted from Blood. PCR was used to amplify the mitochondrial tRNA MT-TL2 gene, and 22 samples were sequenced. The sequence was compared with accession #NC-012920.1 of the revised Cambridge Reference Sequence (rCRS). (3) Results: The results (Chromatograph, nucleotide sequence and rCRS alignment) shows mutations in mitochondrial tRNA MT-TL2 gene in our participants is not the cause of Breast cancer. (4) Conclusion: Yet, a significant number of BC patients must be studied, and their full mitochondrial DNA must be analyzed. This will provide an indication of the potential DNA marker that might be used to prevent BC deaths at the earliest stages.
Keywords:
breast cancer
; mitochondrial gene
; MT-TL2 gene
; mutation
; sequencing
1. Introduction
Although continued medical improvements, breast cancer (BC) represents the second most common and lethal disease in women [1]. BC incidence has increased dramatically during the last four decades [2]. There were around 2.3 million new instances of BC globally in 2020, as well as approximately 6,85,000 deaths from this condition, with significant regional variations across various nations and areas [3]. Notably, high-income countries had a higher proportion of breast cancer mortality. By 2040, more than 3 million new cases of breast cancer and more than 1 million deaths from the illness are expected [4]. Breast cancer are sporadic, with 5-10% being hereditary [5]. Environmental (e.g., hormone replacement treatment, menopausal age, obesity, and so on) and inherited factors all increase a woman’s risk of breast cancer [6].
Mitochondria are cytoplasmic organelles that produce energy and are inherited maternally. They are organelles that are both biosynthetic and bioenergetics. Through the consumption of cytoplasmic substrate, they power respiration, the electron transport chain, the tri-carboxylic acid cycle, and fatty acid oxidation. They produce lipids, heme, amino acids, iron-sulfur clusters, nucleotides, and NADPH for their own oxidative defense [7]. Mitochondria are semi-autonomous organelles with their own genetic material. However, it is not completely independent of nuclear DNA [8]. Mitochondrial DNA (mtDNA) is a 16,569 base pair circular, supercoiled molecule present in the mitochondrial matrix [9]. There are 37 genes in it without introns. They consist of 22 tRNA molecules, two rRNA molecules (12S and 16S rRNA), and 13 polypeptides that form protein respiratory chain complexes [10].
There have been more than 200 known mutations in mitochondrial DNA (mtDNA), including enormous mtDNA rearrangements and point mutations in ribosomal RNAs, protein-coding genes, and mitochondrial transfer RNAs (mt-tRNA) [11]. Mutations in the Mitochondrial tRNALeu(CUN) gene were discovered in MERRF-NARP syndrome patients for the first time [12]. The relationship of two mitochondrial genes, MT-TL2 and MT-ND3, with breast cancer is noteworthy [13]. Despite mtDNA mutations are usually passed down from mother to child, they can sometimes occur spontaneously. Furthermore, the correct maintenance of mtDNA depends on some nuclear genes; mutations in these genes can cause qualitative (mtDNA deletions) as well as quantitative (mtDNA depletion) mtDNA difficulties. We conducted the current investigation based on earlier research to seek for mutations in the MT-TL2 gene in BC patients and to compare our amplified sequences to previously published sequences.
2. Materials and Methods
2.1. Ethical Approval
The Hazara University (HU) Ethics Committee in Mansehra, Pakistan, approved the ethical form. In accordance with the Helsinki Declaration, all participants would be made aware of the purpose of the research and will sign informed consent forms.
2.2. Sample Collection
The hospital’s doctors verified that all of the patients had BC. A syringe was used to collect blood samples from 24 BC patients, and 5CC blood was extracted and put into an EDTA.K3 vacuum tube. The materials were taken to the HU molecular genetics lab and stored at -20°C.
2.3. DNA Extraction
Blood samples were collected from BC patients, and DNA was extracted using the Phenol-chloroform procedure, as previously reported [14].
2.4. Making Agarose Gell of DNA Samples
Agarose gel electrophoresis was utilised to assess the obtained DNA’s purity. 0.5g of agarose was dissolved in 29.4ml of double distal water in order to analyse the isolated DNA. Two millilitres of loading dye and five millilitres of extracted DNA were added to 600 microliters of 50X Tris-acetate elution Buffers containing 10 microliters of ethidium bromide (EB). After that, the gel was operated at 60 volts for 30 minutes, and an ultraviolet gel documentation system was used to take pictures of the gel.
2.5. Polymerase Chain Reaction (PCR)
The extracted DNA was then utilised in PCR to amplify the MT-TL2 gene. Leucine 2 gene was amplified using the polymerase chain reaction (PCR), which utilised the following chemicals: 1µl forwards and reverse primers, 0.3µl DNA polymerase, 11.7µl distilled water, 1µl dNTPs, 2µl Taq 10X buffer, and 2µl DNA template. The following primers were used for amplification of MT-TL2: F-primer 5-TTTACCACAACACAATGGGG-3, R-primer 5-GCTCAGTGTCAGTTCGAGATA-3.
2.6. PCR Optimal Conditions
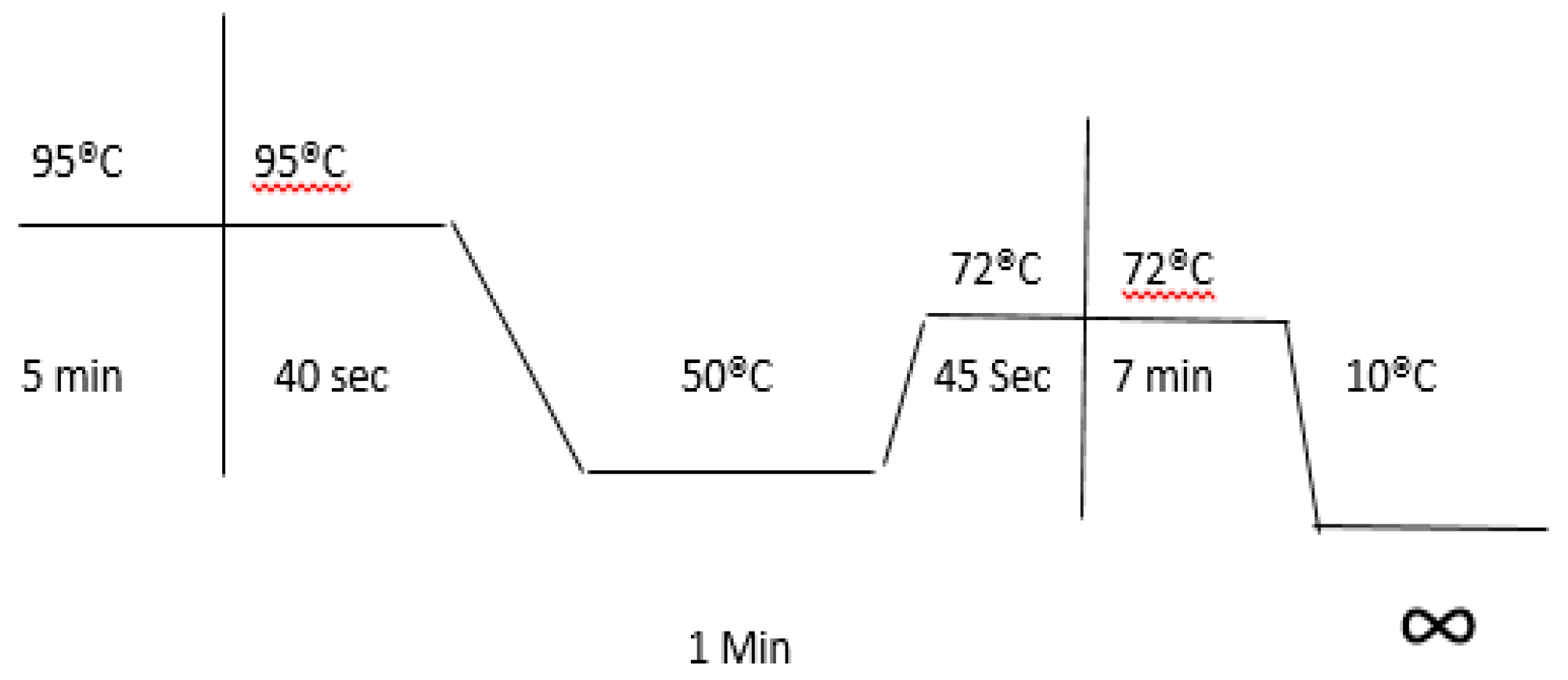
The PCR procedure is divided into three phases that are performed 40 times. The first step is 5 minutes of denaturation at 95°C, followed by 40 seconds of annealing at 50°C and lastly 7 minutes of extension at 72°C. There are two additional processes, the first of which is termed Pre PCR denaturation and is done for 5 minutes at 95°C. Another stage was a 7-minute post-PCR extension at 72 °C.
Figure 1.
Optimized conditions for Lucine2 gene PCR amplification.
2.7. Amplified Gene Fragment DNA Cleaning from Gel
To wash the PCR amplification, the TIAN gel Midi purification kit (Cat # DP20902) was applied. After being cut using a sterile medical blade, a PCR band containing tRNA MT-TL2 genes is kept in labelled Eppendorf tubes.
2.8. Sequencing and Data Analysis
For sequencing, 24 BC samples’ eluted DNA were transferred to Macrogen, Inc. in Korea. The whole mitochondrial sequence’s Revised Cambridge Reference Sequence (rCRS) Accession No. NC-012920.1 was aligned with the sequencing data that was obtained. A mutation in the MT-TL2 gene was examined in the alignment.
3. Results
3.1. Sample Collection
Samples was breast collected from several hospitals in Peshawar. Patients age range from 23 to 58 years old. The patients also had diabetes, hepatitis, chronic asthma, and hypertension in addition to their heart problems. For nucleotide sequence analysis, all 22 BC samples were transferred to Microgen Inc. Korea.
3.2. DNA Extraction
All of the samples collected have been examined for DNA extraction, and the findings of 24 samples of them are displayed in Figure 2.
3.3. Amplification of the MT-TL2 Gene
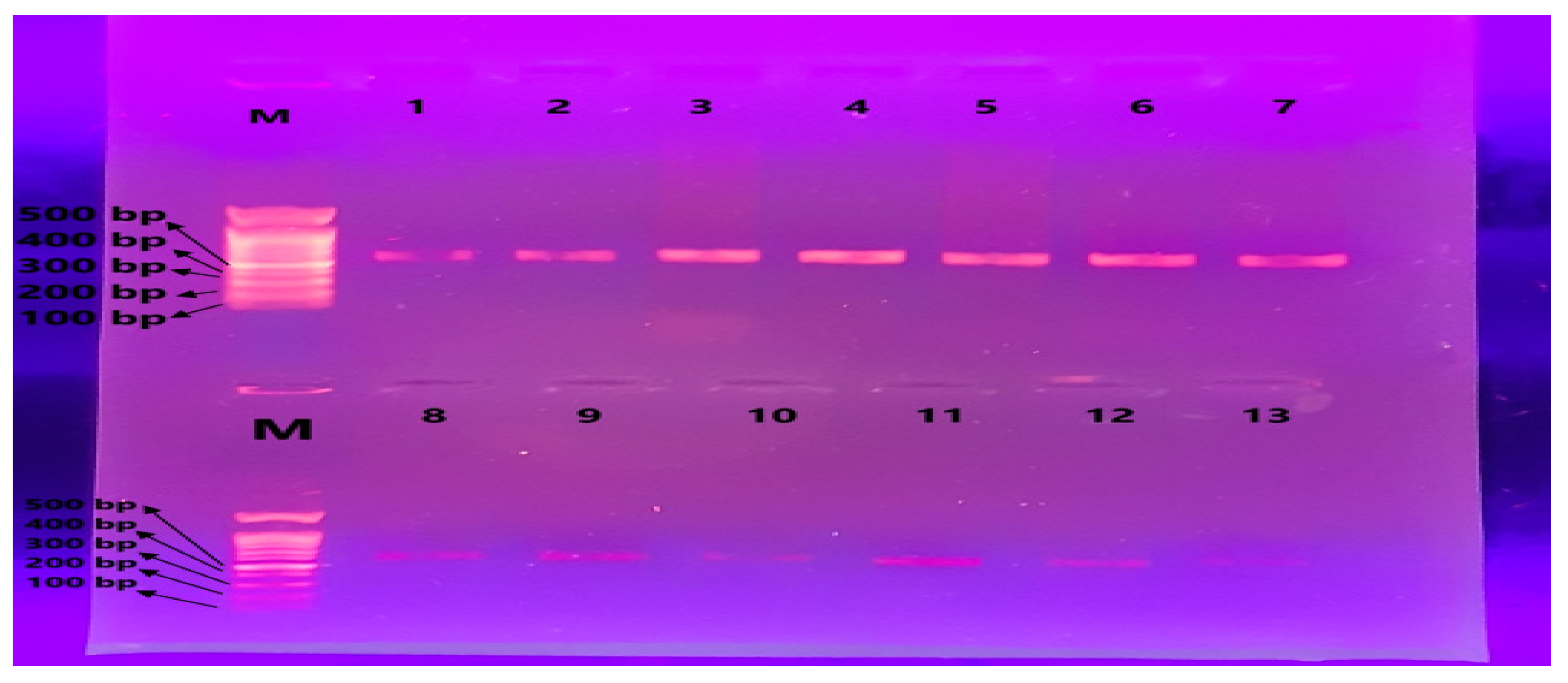
PCR was performed with forwards and reverse primers specific for a region encompassing the MT-TL2 gene, as indicated in Figure 3.
3.4. Sequencing Analysis
Macrogen, Inc. Korea received the cleaned DNA for sequencing. The resultant sequence was compared to the mitochondrial genome sequence (Accession NC-012920.1). We submitted 22 samples for sequencing and obtained results for 22 of them. Figure 4a, b, and c reveal the following information and analysis of these samples.
- Sample 1
The first subject on the list was 58 years old, had been diagnosed with severe asthma, and had a positive family history of breast cancer. She spent the previous four years receiving chemotherapy. The tRNA leucine2 gene was amplified using PCR, and the resulting sequence was compared to the mitochondria’s control DNA sequence. Using the revised Cambridge References Sequence (rCRS) accession NC_012920.1 as the control during the NCBI alignment procedure, two sequences were aligned. As seen in Figure 4a, the alignment findings revealed no alteration in this subject with tRNA leucine2 gene Figure 4c shows the chromatograph result.
- Sample 2
The second subject’s age was 52, and there was no family history of breast cancer. For the past year, she has been receiving chemotherapy. The tRNA leucine2 gene was amplified using PCR, and the resulting sequence was compared to the mitochondria’s control DNA sequence. Using the r rCRS accession NC_012920.1 as the control during the NCBI alignment procedure, two sequences were aligned. As seen in Figure 5a, the alignment findings revealed no alteration in this subject with tRNA leucine2 gene. Figure 5c shows the chromatograph.
- Sample 3
The third subject, who was 54 years old, was diagnosed with diabetes and had no family history of breast cancer. She spent the previous two years receiving chemotherapy. The tRNA leucine2 gene was amplified using PCR, and the resulting sequence was compared to the mitochondria’s control DNA sequence. Using the rCRS accession NC_012920.1 as the control during the NCBI alignment procedure, two sequences were aligned. As seen in Figure 6a, the alignment findings revealed no alteration in this subject with tRNA leucine2 gene. Figure 6c shows the chromatograph.
- Sample 4
At 42 years old, the fourth subject on the list had a positive family history of breast cancer. For the past year, she has been receiving chemotherapy. The tRNA leucine2 gene was amplified using PCR, and the resulting sequence was compared to the mitochondria’s control DNA sequence. Using the rCRS accession NC_012920.1 as the control during the NCBI alignment procedure, two sequences were aligned. As seen in Figure 7a, the alignment findings revealed no alteration in this subject with tRNA leucine2 gene. Figure 7c shows the chromatograph.
- Sample 5
49-year-old subject with positive family history of breast cancer. For the past year, she has been receiving chemotherapy. The tRNA leucine2 gene was amplified using PCR, and the resulting sequence was compared to the mitochondria’s control DNA sequence. Using the rCRS accession NC_012920.1 as the control during the NCBI alignment procedure, two sequences were aligned. As seen in Figure 8a, the alignment findings revealed no alteration in this subject with tRNA leucine2 gene. Figure 8c shows the resultant sequence’s chromatograph.
Figure 4a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 1.
Figure 4a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 1.
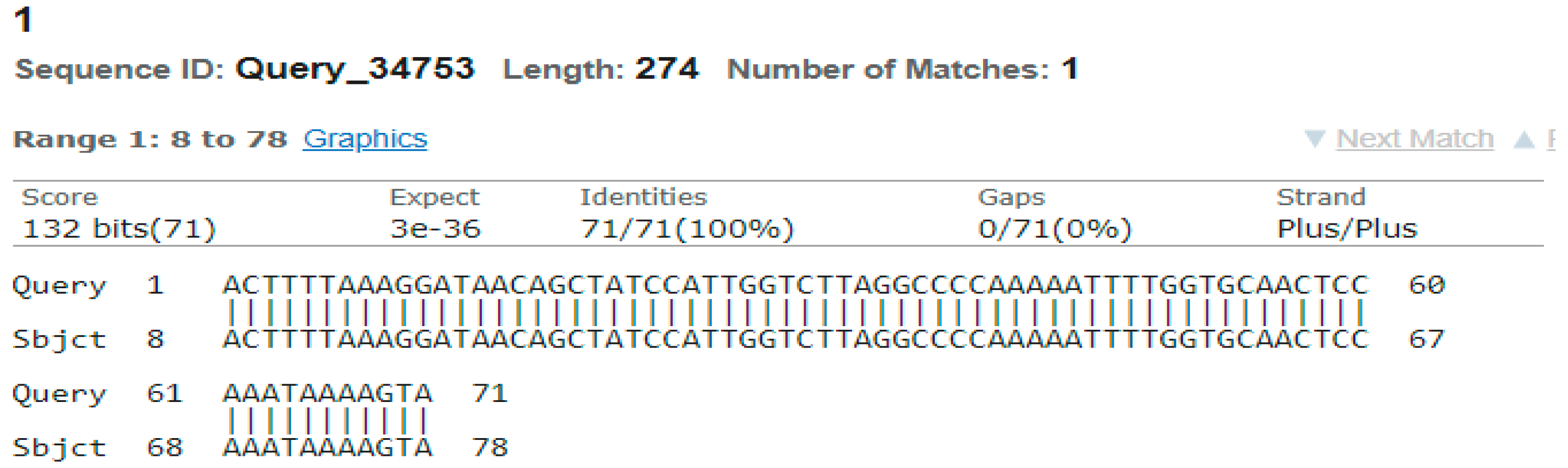
Figure 4b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.
Figure 4b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.

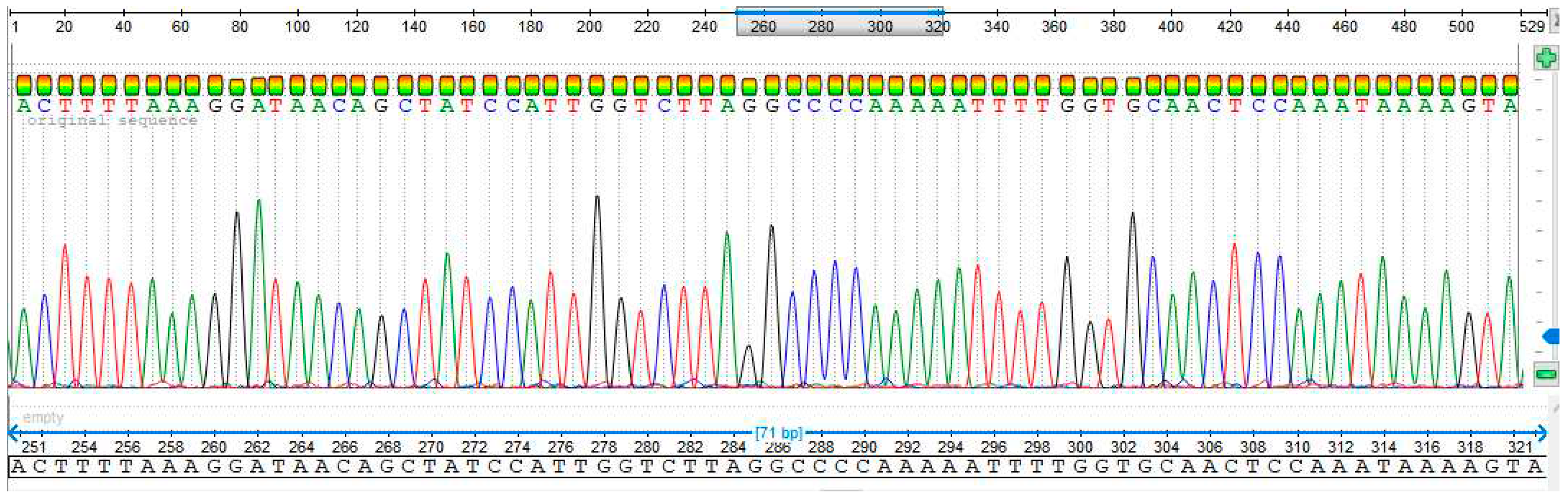
Figure 4c.
The Subject 1 has no changes in the MT-TL2 gene chromatograph.
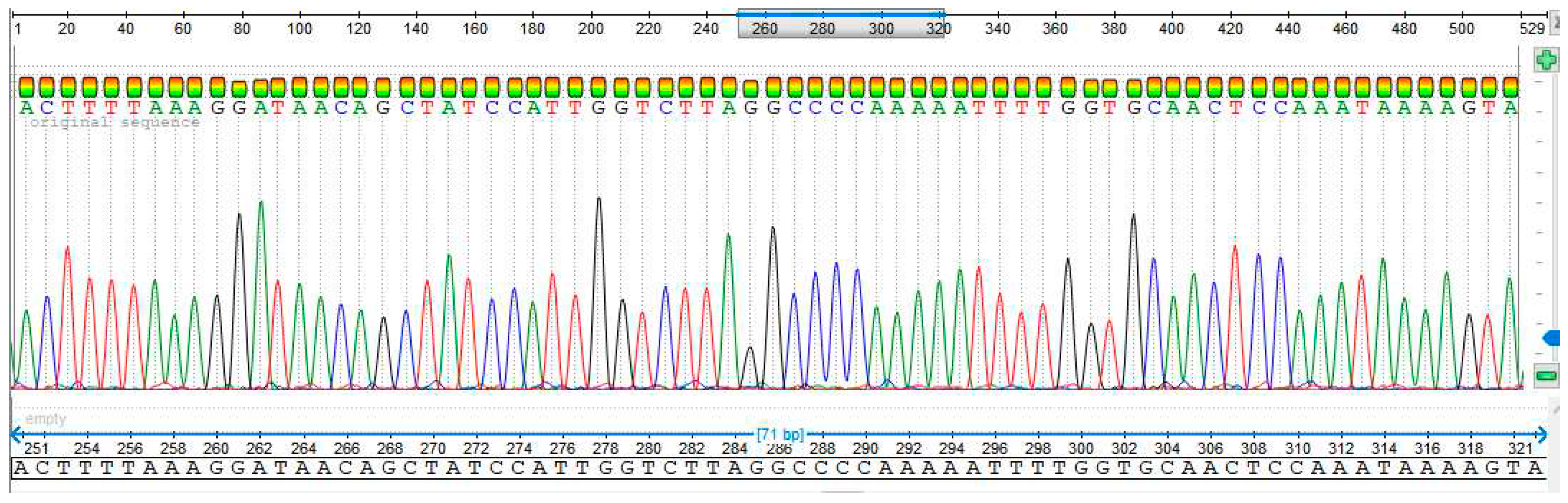
Figure 5a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 2.
Figure 5a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 2.
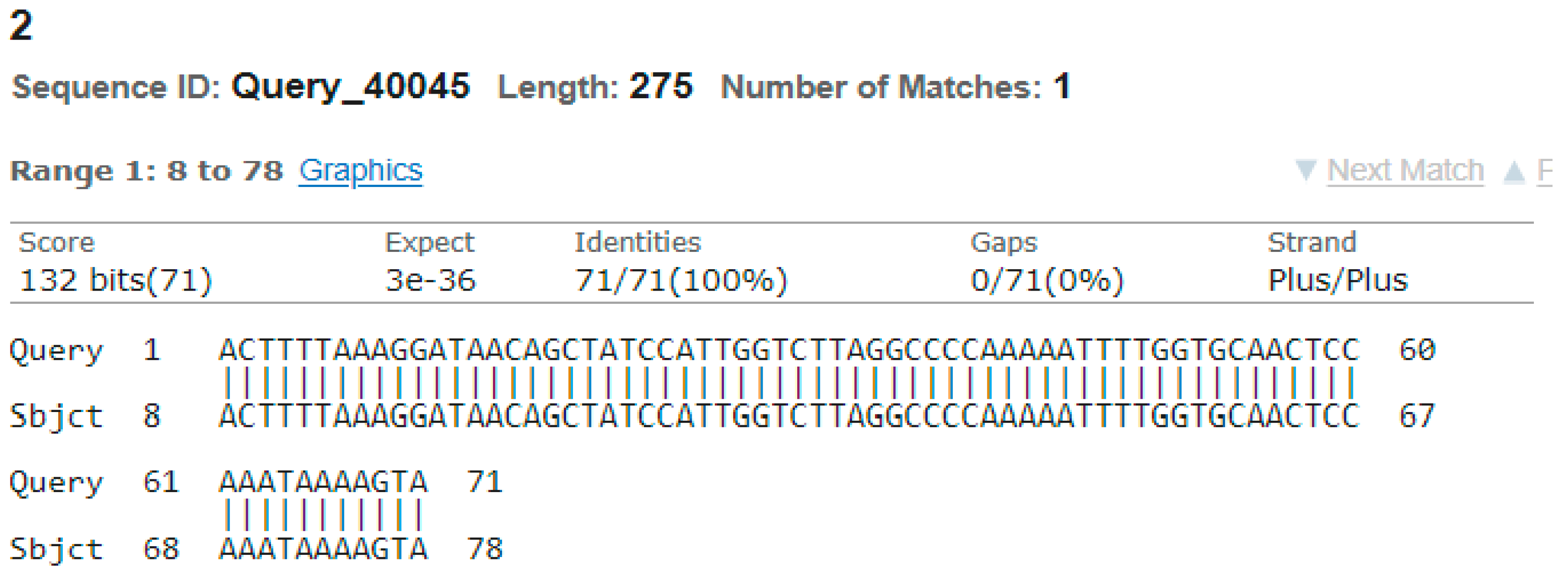
Figure 5b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.
Figure 5b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.

Figure 5c.
The Subject 2 has no changes in the MT-TL2 gene chromatograph.
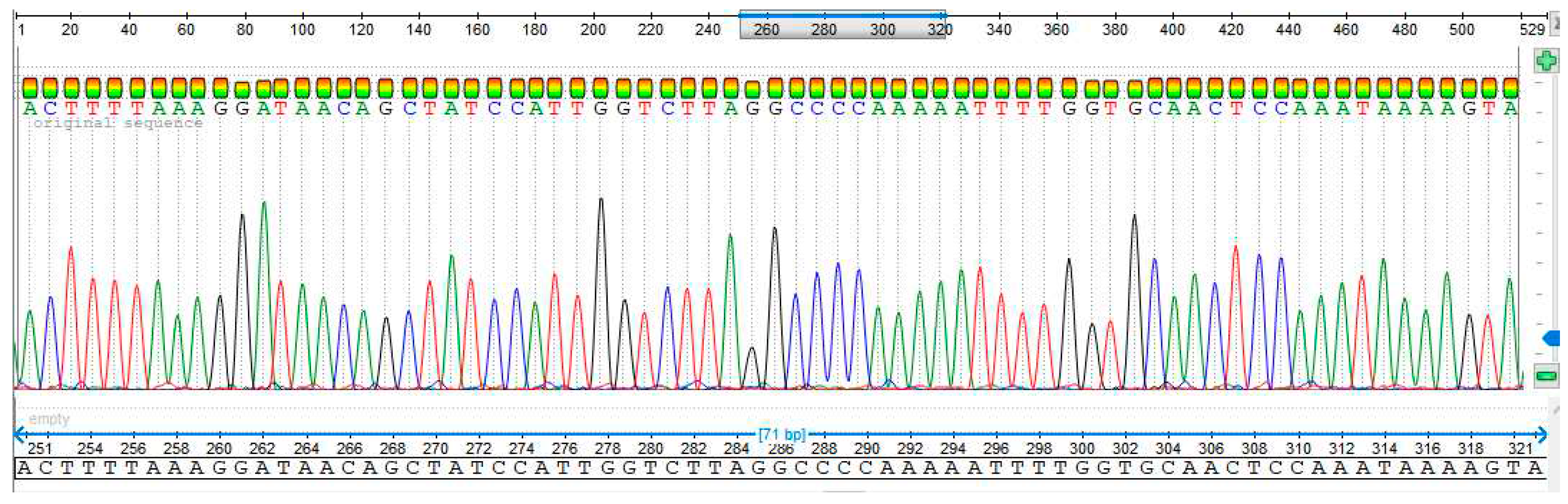
Figure 6a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 3.
Figure 6a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 3.
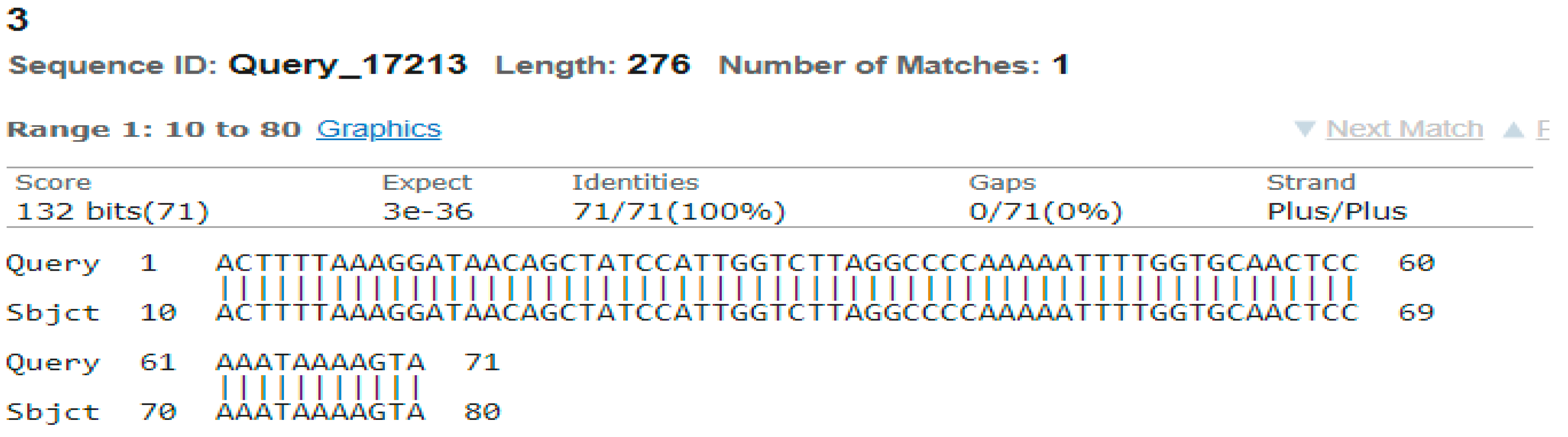
Figure 6b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.
Figure 6b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.

Figure 6c.
The Subject 3 has no changes in the MT-TL2 gene chromatograph.
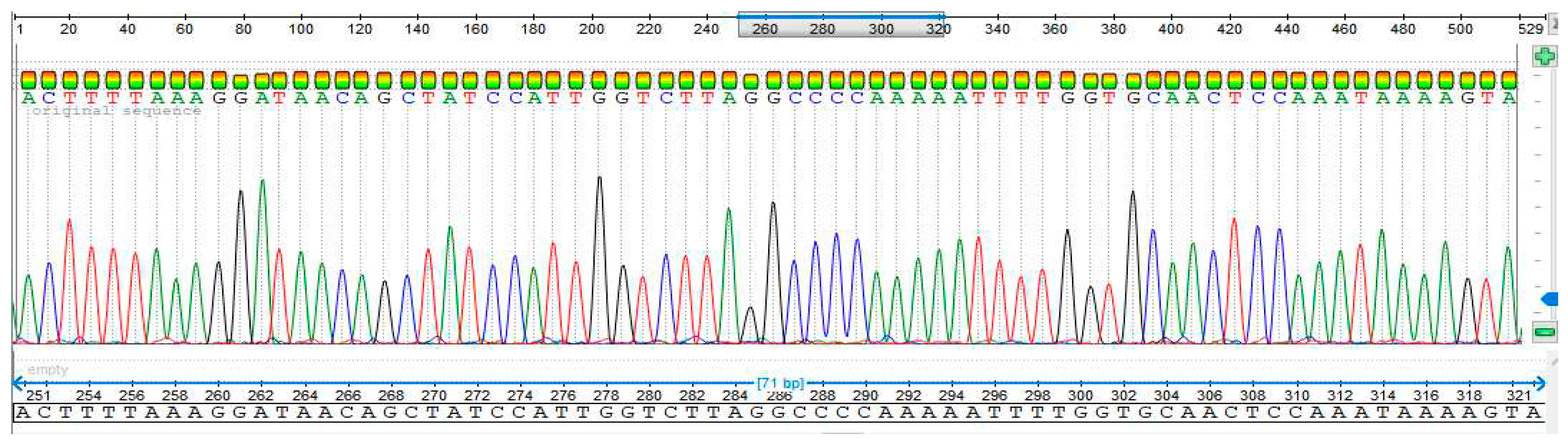
Figure 7a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 4.
Figure 7a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 4.
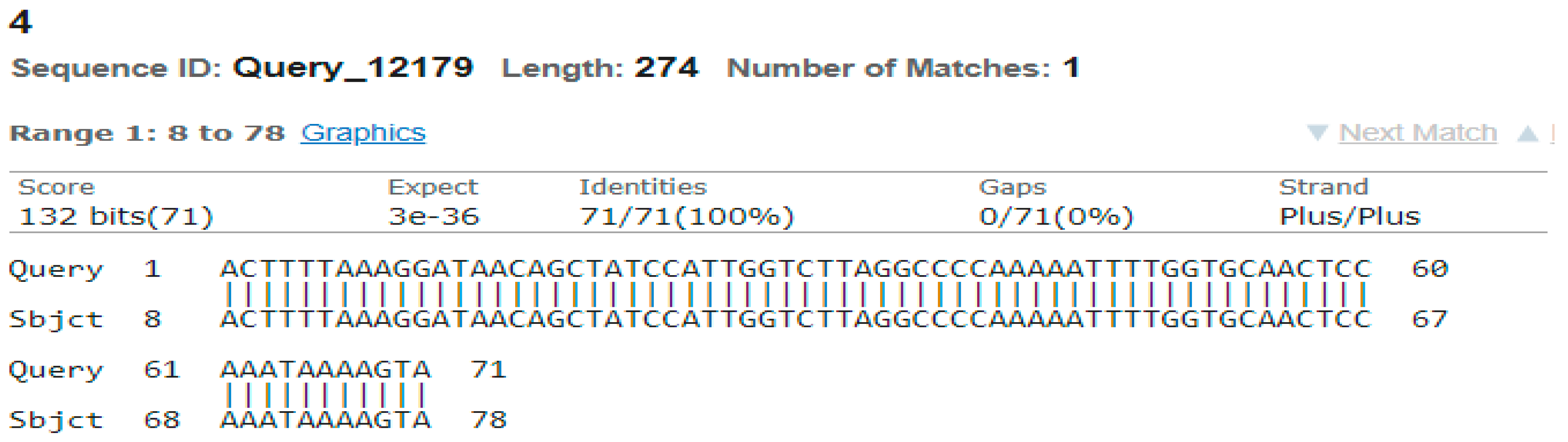
Figure 7b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.
Figure 7b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.

Figure 7c.
The Subject 4 has no changes in the MT-TL2 gene chromatograph.
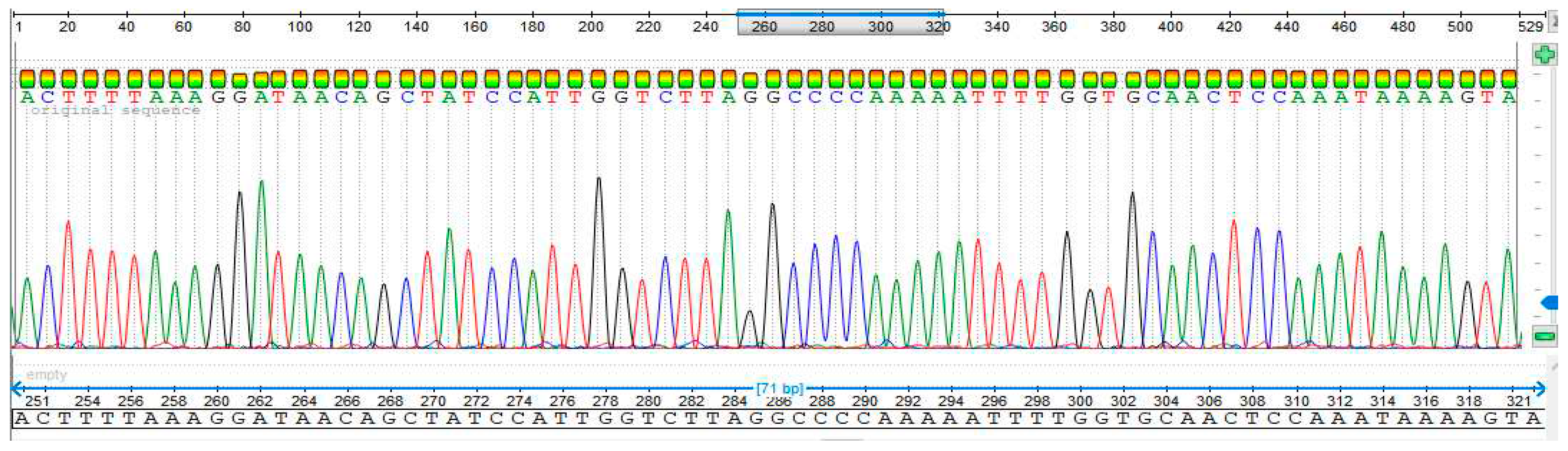
Figure 8a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 5.
Figure 8a.
No alteration in the patient’s MT-TL2 gene was found using rCRS Accession #NC_012920.1 nucleotide sequence alignment for Subject 5.
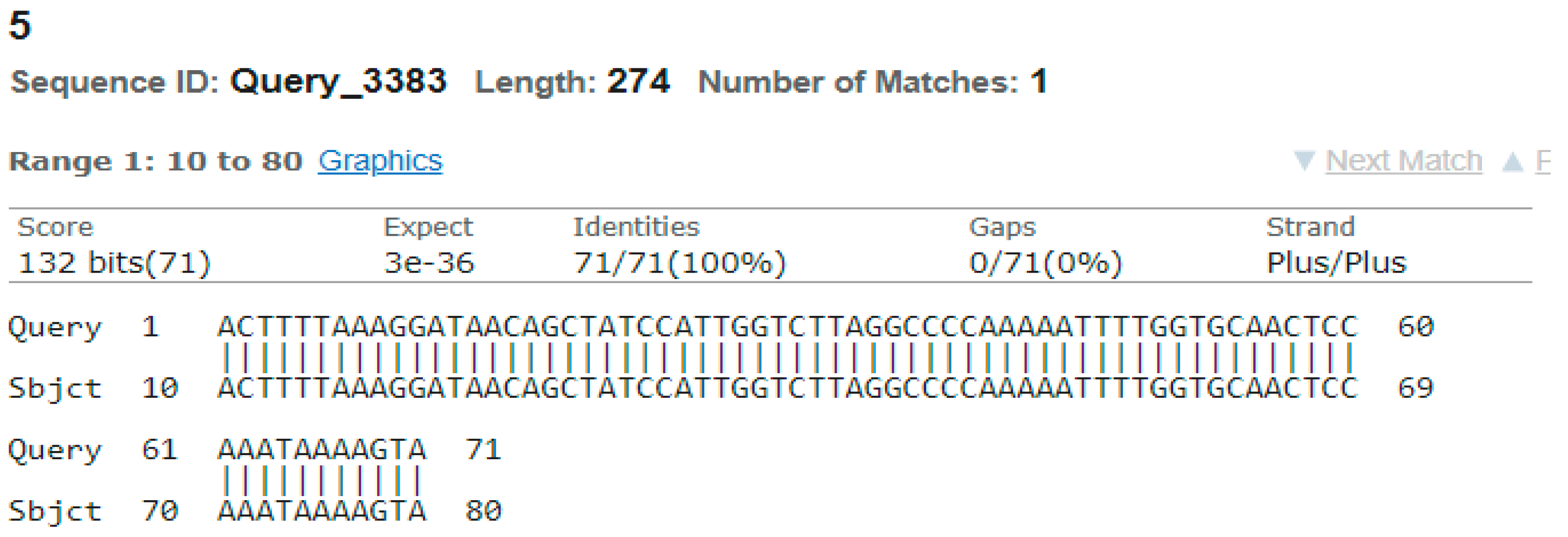
Figure 8b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.
Figure 8b.
Compression between MT-TL2 in normal human (Sequence obtained from NCBI) MT-TL2 gene with obtained results.

Figure 8c.
The Subject 5 has no changes in the MT-TL2 gene chromatograph.
4. Discussion
Pathological and clinical results indicate that breast cancer is a multidisciplinary disease. It is divided into two categories: invasive cancer and non-invasive cancer, depending on how the tumor cells spread [15]. In both industrialised and emerging nations, the prevalence of breast cancer is steadily rising. 1.7 million women worldwide were diagnosed with breast cancer in 2012, and out of 184 nations worldwide, 140 have recorded a case of the disease on a regular basis. Asian women are responsible for around 40% of all breast cancer cases globally. Among Asia’s nations, breast cancer ranks second in terms of cancer-related death and morbidity. With around 60% of all people on Earth, Asia is the largest continent in the globe. Compared to Western nations, Asia has a higher death rate from breast cancer incidence [16]. The continent of Asia has the highest rate of breast cancer malignancy. Breast cancer mortality is disturbingly higher in most Asian nations, especially in South-east Asia [17].
Numerous mitochondrial DNA alterations have been identified in a several human malignancies. Alterations in both the coding and non-coding regions of the mtDNA have been discovered, with the bulk of the mutations acting as homoplasmic in nature [18]. Variations in the mitochondrial genes of patients with diabetes mellitus may be the cause or have some connection. Three variations in diabetes individuals may be seen in the MT-TL2 gene variant examined in unrelated families. Every patient had their MT-TL2 gene sequenced, and every patient had a mutation found in [19]. There is a substantial correlation between breast cancer and the mitochondrial genes MT-TL2 and MT-ND3 [13].
Our research aimed to determine the relationship between BC and mutations in the mitochondrial encoded tRNA MT-TL2 gene in Peshawar. We took a move to determine how this disease is linked to several more mutations. A total of 24 subjects were included in this study suffering from BC. The tRNA leucine2 gene of 22 patients was amplified and sequenced in which five patients data show in the subjects 1, 2, 3, 4, 5 and the rest of 19 subjects data is available. There age ranged from 23 to 58 years old and had various problems such as diabetes, hepatitis, chronic asthama, and hypertension. However, we found no mutations in the tRNA MT-TL2 gene of our BC individuals. This might be owing to the small size of the people in which we studied the sequence of their tRNA MT-TL2 gene, or it could be related to the participation of other genes expressed by mitochondria.
5. Conclusions
The study reveals that no alteration was found in tRNA leucine2 gene in the samples taken from patients with BC. It is recommended that additional genes encoded by the mitochondrial genome be investigated in BC patients. To get an accurate conclusion, it is also advised that a large number of participants be included in future studies.
Acknowledgements
We express our gratitude to each participant and their families for their participation in this study.
Competing interest
The authors state that they do not have any conflicts of interest.
Abbreviations
Breast caner: BC
Revised Cambridge Reference Sequence: rCRS
References
- B. I. Bodai and P. Tuso, "Breast cancer survivorship: a comprehensive review of long-term medical issues and lifestyle recommendations," The Permanente Journal, vol. 19, no. 2, p. 48, 2015. [CrossRef]
- N. Giaquinto et al., "Breast cancer statistics, 2022," CA: a cancer journal for clinicians, vol. 72, no. 6, pp. 524-541, 2022. [CrossRef]
- Y. Li et al., "Global burden of female breast cancer: age-period-cohort analysis of incidence trends from 1990 to 2019 and forecasts for 2035," Frontiers in oncology, vol. 12, p. 891824, 2022. [CrossRef]
- M. Arnold et al., "Current and future burden of breast cancer: Global statistics for 2020 and 2040," The Breast, vol. 66, pp. 15-23, 2022. [CrossRef]
- E. B. Claus, J. M. Schildkraut, W. D. Thompson, and N. J. Risch, "The genetic attributable risk of breast and ovarian cancer," Cancer: Interdisciplinary International Journal of the American Cancer Society, vol. 77, no. 11, pp. 2318-2324, 1996. [CrossRef]
- C. Antoniou and D. Easton, "Models of genetic susceptibility to breast cancer," Oncogene, vol. 25, no. 43, pp. 5898-5905, 2006. [CrossRef]
- D. C. Wallace, "Mitochondria and cancer," Nature Reviews Cancer, vol. 12, no. 10, pp. 685-698, 2012. [CrossRef]
- N. Pfanner and A. Geissler, "Versatility of the mitochondrial protein import machinery," Nature reviews Molecular cell biology, vol. 2, no. 5, pp. 339-349, 2001. [CrossRef]
- F. Legros, F. Malka, P. Frachon, A. Lombès, and M. Rojo, "Organization and dynamics of human mitochondrial DNA," Journal of cell science, vol. 117, no. 13, pp. 2653-2662, 2004. [CrossRef]
- R. M. Andrews, I. Kubacka, P. F. Chinnery, R. N. Lightowlers, D. M. Turnbull, and N. Howell, "Reanalysis and revision of the Cambridge reference sequence for human mitochondrial DNA," Nature genetics, vol. 23, no. 2, pp. 147-147, 1999. [CrossRef]
- E. A. Schon, S. DiMauro, M. Hirano, and R. W. Gilkerson, "Therapeutic prospects for mitochondrial disease," Trends in molecular medicine, vol. 16, no. 6, pp. 268-276, 2010. [CrossRef]
- R. Martín-Jiménez, E. Martín-Hernández, A. Cabello, M. T. García-Silva, J. Arenas, and Y. Campos, "Clinical and cellular consequences of the mutation m. 12300G> A in the mitochondrial tRNALeu (CUN) gene," Mitochondrion, vol. 12, no. 2, pp. 288-293, 2012. [CrossRef]
- D. Covarrubias, R.-K. Bai, L.-J. C. Wong, and S. M. Leal, "Mitochondrial DNA variant interactions modify breast cancer risk," Journal of human genetics, vol. 53, no. 10, pp. 924-928, 2008. [CrossRef]
- M. Ghaheri, D. Kahrizi, K. Yari, A. Babaie, R. Suthar, and E. Kazemi, "A comparative evaluation of four DNA extraction protocols from whole blood sample," Cellular and Molecular Biology, vol. 62, no. 3, pp. 120-124, 2016.
- G. N. Sharma, R. Dave, J. Sanadya, P. Sharma, and K. Sharma, "Various types and management of breast cancer: an overview," Journal of advanced pharmaceutical technology & research, vol. 1, no. 2, p. 109, 2010.
- F. Bray, J. Ferlay, I. Soerjomataram, R. L. Siegel, L. A. Torre, and A. Jemal, "Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries," CA: a cancer journal for clinicians, vol. 68, no. 6, pp. 394-424, 2018. [CrossRef]
- J. Ferlay et al., "Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012," International journal of cancer, vol. 136, no. 5, pp. E359-E386, 2015. [CrossRef]
- Chatterjee, E. Mambo, and D. Sidransky, "Mitochondrial DNA mutations in human cancer," Oncogene, vol. 25, no. 34, pp. 4663-4674, 2006. [CrossRef]
- S. U. Haq et al., "Mutation in Mitochondrial MT-TL2 (CUN) Gene and Its Association with Diabetes mellitus in Pakistan," Available at SSRN 3473285, 2019. [CrossRef]
Figure 2.
Extracted whole genomic DNA from samples from.
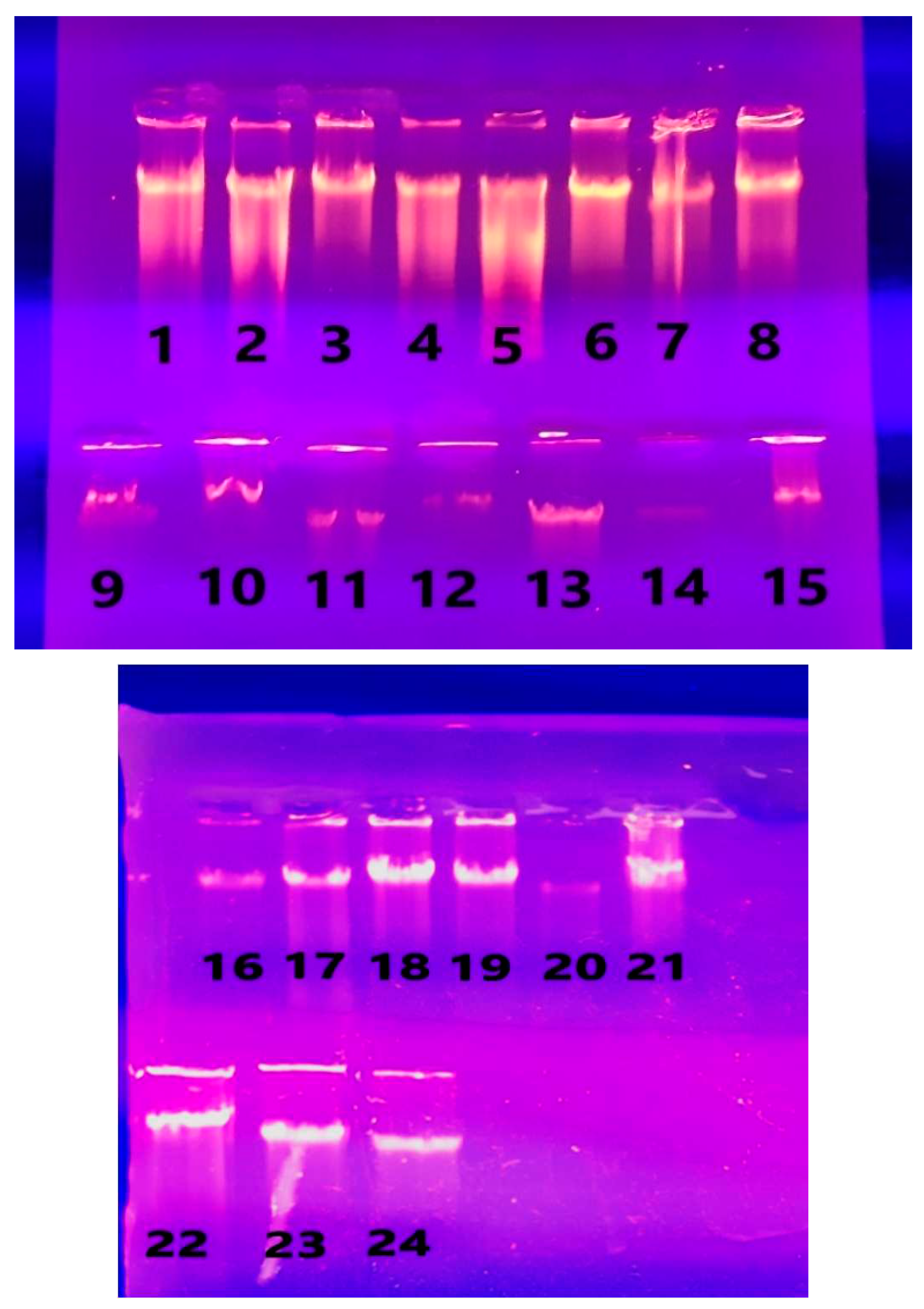
Figure 3.
PCR amplification of MT-TL2 gene with 13 BC samples.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



