
Submitted:
23 November 2023
Posted:
24 November 2023
You are already at the latest version
Abstract
Background: Alongside their long-term effects - post-concussion syndrome (PCS) - mild traumatic brain injuries (mTBI) are significant public health concerns. Currently, there is a lack of reliable biomarkers for diagnosing and monitoring mTBI and PCS. Exosomes are small extracellular vesicles secreted by cells that have recently emerged as a potential source of biomarkers for mTBI and PCS due to their ability to cross the blood-brain barrier and reflect the pathophysiology of brain injury. This study aimed to investigate the role of salivary exosomal biomarkers in mTBI and PCS. Methods: A systematic review using the PRISMA guidelines was conducted, and studies were selected based on their relevance to the topic. Results: Studies have shown that exosomal tau, phosphorylated tau (p-tau), amyloid beta (Aβ), and microRNAs (miRNAs) are potential biomarkers for mTBI and PCS. Specifically, elevated levels of exosomal tau and p-tau have been associated with mTBI and PCS, as well as with repetitive mTBI. Dysregulated exosomal miRNAs have also been observed in individuals with mTBI and PCS. Additionally, exosomal Prion cellular protein (PRPc), coagulation factor XIII (XIIIa), synaptogyrin-3, IL-6, and aquaporins have been identified as promising biomarkers for mTBI and PCS. Conclusion: Salivary exosomal biomarkers have the potential to serve as non-invasive and easily accessible diagnostic and prognostic tools for mTBI and PCS. Further studies are needed to validate these biomarkers and to develop standardized protocols for their use in clinical settings. Salivary exosomal biomarkers can improve the diagnosis, monitoring, and treatment of mTBI and PCS, leading to improved patient outcomes.
Keywords:
mild traumatic brain injury
; post-concussion syndrome
; exosomes
; salivary biomarkers
Introduction
Traumatic brain injury (TBI) is often caused by a blunt head trauma event significantly affecting the quality of life and the health of an individual. In some cases, TBI could even threaten the patient’s life, as it was showed that TBI has increased morbidity and mortality rates worldwide. Mild TBI (mTBI), also known as a concussion, accounts for approximately 80% of all TBI cases [1]. Despite the generally favorable outcomes for most mTBI patients, some individuals continue to experience chronic post-concussion (PC) symptoms, including cognitive impairment, headaches, sleep disturbances, and mood disorders, which can significantly impact their quality of life [2]. Early diagnosis and management of mTBI and its associated post-concussion syndrome (PCS) are crucial to prevent long-term complications. However, the current diagnostic methods for mTBI and PCS are limited and often rely on subjective clinical evaluations [2].
Exosomes are small extracellular vesicles released by almost all mammalian cell types, including neurons and glial cells [3]. Neuron-derived exosomes are extracellular vesicles released by neurons and are thought to be key mediators in the communication and waste management within the brain tissues [4]. The diameter of exosomes varies between 30 and 150 nm [5]. Exosomes were first described in the 1980s [6] and were thought to originate from the endomembrane system, while their membranous envelope is invaginated during the maturation process and forms the intraluminal vesicles (ILVs).
The ILVs are consisted in proteins, nucleic acids, and lipids. Mature endosomes which contain numerous ILVs are called multivesicular bodies (MVB) [7]. Multivesicular bodies will either be degraded by lysosomes or will be transported to cell membranes, will fuse with the cell membranes, and will release the inner vesicles into the extracellular space, forming exosomes loaded with proteins, non-coding RNAs, lipids and other active substances [8]. They contain particular and varied types of markers that contribute to identifying their origin. Once they are secreted, they can be internalized by recipient cells through different mechanisms, such as phagocytosis, micropinocytosis, endocytosis, and plasma membrane fusion [9,11]. Neuron and glial-derived exosomes carry and release multiple molecules related to neuronal function and neurotransmission in the brain. They are essential in neuronal development, neuroimmune communication, and synaptic spasticity [11].
The role of exosomes and the changes in the exosomal content in TBI have been extensively investigated in the past few years. Changes in the levels of exosomal content after a TBI can assist in the diagnosis and severity classification of the TBI [12]. The concentration of neuro-derived exosomes in the plasma of patients with a mTBI is reduced by 45% in the acute phase of the injury, while the alterations in the levels of neuropathological protein in these exosomes can depict phase and severity specificity [13]. Moreover, it was shown that a pattern in exosomal content dynamics can be seen during different periods after a mTBI [14]. In this way, several proteins could be qualitatively and quantitatively assessed in plasma of mTBI patients to prognose remote long-termed symptoms and recovery, as reported by Guedes et al for plasma exosomal neurofilament light chain peptide (NfL) levels [15]. The protective role of exosomes in TBI was also documented. More specifically, it was showed that exosomal miRNAs could improve the neurodegeneration following repetitive mTBI [16], suppress the inflammatory process, promote axonal growth, and improve neuroprognosis [17,18]. Recent studies have identified potential biomarkers, including microRNAs, as well as tau protein, cytokines, and other proteins, that could assist in mTBI and PCS diagnosis and management.
In this way, we aimed to describe the role of salivary exosomal biomarkers in mTBI and PCS and discuss their potential as diagnosis and prognosis tools based on a systematic review of recent literature.
Materials and Methods
Literature search
A comprehensive literature search was performed using PubMed, Embase, and Scopus databases to identify articles published until September 2022. The following search terms were used: "mild traumatic brain injury", "concussion", "post-concussion syndrome", "exosomes", "biomarkers", "proteomics", and “microRNAs”, "RNA-seq". The search was limited to studies conducted on human patients and published in English. PRISMA guidelines were used (PRISMA checklist attached as supplemental material). The systematic review was registered in PROSPERO platform under the ID 478729/1.11.2023.
Inclusion and exclusion criteria
Studies that investigated the role of exosomal biomarkers in mTBI and PCS were included. Studies that did not report data on salivary exosomes or biomarkers, case reports, or animal studies were excluded.
Data extraction
Data screening and selection was independently carried out according to PRISMA guideline by two authors. The eligibility criteria were then applied to the full text of the studies. Data were extracted from the included studies using a standardized data extraction form that included study design, participant characteristics, type of biomarkers measured, and main findings.
Quality assessment
The quality of the included studies was assessed using the Cochrane Risk of Bias Tool for randomized controlled trials and the Newcastle-Ottawa Scale for observational studies. The disagreements regarding the data selection and quality assessments, if any, found resolution by discussion until reaching consensus.
Data synthesis
A narrative synthesis approach was used to summarize the findings of the included studies. Data were organized by the type of the measured biomarkers and their potential role in diagnosis or prognosis.
Results
While the initial search resulted in 65 studies, duplicates elimination led to the inclusion of 37 studies in the screening process. After the initial screening process, 22 additional studies were removed. Then, the full text of the remaining 15 studies was screened. Seven studies were excluded, at this stage, and finally 8 studies were included in the present study (Figure 1). There were no concerns on the quality of the studies that were finally included (Figure 2a,b).
Narrative summary of the studies
Kenney et al. measured plasma and exosomal levels of tau protein, p-tau and amyloid beta peptide (Aβ) in Veterans with history of mTBI and chronic neuropsychological symptoms [19]. They reported that exosomal p-tau and tau peaks were associated with repetitive mTBI and were correlated with PC symptoms suggesting that blood-based exosomes could provide peripherally sourced information about mTBI effects on the brain tissues.
Wang et al. focused on developing a blood-based biomarker assay for mTBI using circulating exosomes and showed that the analysis of circulating exosomes via acoustofluidic exosome separation allows the detection of exosomal biomarkers in TBI [20]. Also, the study pointed out that these changes could pe depicted in the first 24 hours following head trauma which can be a considerable advantage. Thus, the acoustofluidic exosome separation could potentially improve early diagnosis and treatment decisions associated with TBI.
Devoto et al. conducted a study to investigate the potential role of exosomal microRNA expression in neurobehavioral outcomes among Veterans with mTBI from blunt or blast injuries [21]. The preliminary results originating from 152 participants described several dysregulated cellular pathways involved in neurodegeneration, inflammation, and central hormonal regulation that could be related to chronic neurobehavioral symptoms after blast TBI. The same group further investigated the role of exosomal micro-RNAs (miRNAs) by relation to the persistence of chronic TBI symptoms [22]. In this longitudinal study, dysregulated exosomal miRNAs were identified in participants with a history of mTBI, particularly those with repetitive mTBI correlating exosomal miRNAs with inflammatory regulation, neurological disease, and cell development. Thus, exosomal miRNAs analysis could also provide novel insights on the underlying pathobiology of chronic TBI symptom persistence.
Gill et al. also conducted a study to identify biomarkers in peripheral blood related to chronic post-concussive and behavioural symptoms following TBI [23]. The study investigated the concentrations of tau, amyloid β 42 peptides, and cytokines (TNF-α, IL-6, IL-10) in neuronal-derived exosomes from the peripheral blood of military personnel with or without mTBI concluding that increased exosomal tau, amyloid β 42, and IL-10 concentrations could be found in the plasma of mTBI patients, as compared to the controls. However, a relationship between PC symptoms exosomal tau concentrations increase was not reported, yet exosomal IL-10 concentrations correlated with post-traumatic stress disorder (PTSD) symptoms.
Goetzl et al. discussed the potential mechanisms and predictive biomarkers for chronic traumatic encephalopathy (CTE) after acute mTBI [24]. Their promising hypothesis explained a possible pathway for the progression of PCS to CTE that included the changes occurring in the physiological neuronal proteins, such as prion cellular protein (PRPc), coagulation factor XIII (XIIIa), synaptogyrin-3, IL-6, and aquaporins. They found that in patients with long term symptoms occurring after mTBI the levels of neuron-derived exosomes concentrations in some biological fluids could last as much as several months. This could suggest that neuron-derived exosomes could be significant contributors to CTE development, yet the pathological mechanisms in which they act was not clearly understood but thought to express direct actions or to interact with amyloid β peptides or p-tau proteins. To address this aspect, Goetzl et al. investigated the levels of neuron-derived exosomes and their plasma transporters in individuals with or without acute and chronic mTBI [14] and found that exosomal levels of brain functional proteins were significantly abnormal in acute mTBI. By contrast, chronic mTBI was characterized by normal levels of exosomal brain functional proteins, but exosomal brain pathogenic proteins were elevated. This could mean that some exosomal proteins could be promising biomarkers candidates for both acute and chronic mTBI and potentially predictive for long-term effects of mTBI as well as mTBI-induced neurodegeneration.
Further research on the potential of neuronal-derived exosomes and astrocytic-derived exosomes cargo proteins as biomarkers of chronic mTBI was conducted by Winston et al in military service members [25]. They found that plasma neuron-derived and astrocytic-derived exosomal amyloid β 42 peptide levels were significantly increased in patients affected by chronic mTBI. By contrast, plasma neuron-derived and astrocytic-derived exosomal neurogranin levels were found to be significantly decreased in mTBI patients, as compared to healthy controls. These findings could suggest that neuron-derived exosomes could be used to describe the pathomechanisms of TBI.
Regarding the potential of plasmatic exosomal content to predict PC symptoms chronicity, Guedes et al. investigated veterans with a history of mTBI and found that repetitive mTBIs as well as chronic PCS were characterized by increased plasma and exosomal levels of NfL. Furthermore, they reported that these molecules could be also associated with the presence of several symptoms of PTSD, such as depression [26]. Based on the molecular mechanisms underlying mTBI and the changes they reported in exosomal content, they proposed that the persistence of PCS could be tied to neuroinflammatory and disruptive impairments. Following a similar hypothesis, Meier et al. found that some extracellular vesicle-associated cytokines levels could be predictive for duration of PC symptoms [27]. In this way, IL-6 originating from extracellular vesicles was reported to follow this pattern and to significantly correlate the period that passed since the mTBI and the plasmatic profile dynamics leading to the conclusion that extracellular vesicle-associated IL-6 could be an important biomarker for concussion. Another study of Guedes and colleagues investigating the correlation between PTSD symptom severity and the peripheral levels of extracellular vesicles proteins and miRNAs in chronic mTBI reported that extracellular vesicles NfL levels was significantly increased in patients with positive history of mTBI and were corelated with more severe PTSD symptoms, as compared to healthy controls, and mTBI patients with less severe PTSD symptoms, respectively [28]. These could suggest that the levels of NfL could predict the severity of PTSD symptoms in individuals with a history of mTBI.
Tau protein
Exosomal tau protein was identified as a potential biomarker for mTBI and PCS. Increased levels of exosomal tau were observed in individuals with a history of repeated mTBIs, as compared to those with fewer or no mTBIs [25], whereas a significant correlation between exosomal tau levels and post-traumatic and PC symptoms that could include cognitive, affective, and somatic symptoms was reported. In this way, it was suggested that peripheral levels of exosomal tau could provide relevant information about the effects of mTBIs on the brain tissues due to its contribution to the mechanisms underlying the chronic feature of the specific neurophysiological symptoms.
On the other hand, phosphorylated tau protein levels were reported as significantly increased in the exosomes isolated from plasma samples of individuals with mTBI and correlated with repetitive head trauma events [19,25,27,28]. Furthermore, these changes were associated with the chronic neuropsychological symptoms of PCS. Therefore, exosomal phosphorylated tau could be considered a potential biomarker for mTBI and PCS and also being able to provide insights into the underlying pathobiology of these conditions.
Exosomal miRNAs
MiRNAs are small non-coding RNAs that play a role in post-transcriptional gene regulation. Two studies investigated miRNAs as potential biomarkers for mTBI and PCS, as well as for their potential involvement in the underlying pathobiology of these conditions [22,28]. Some specific miRNAs that are dysregulated in exosomes were identified to contribute to intercellular communication and to significantly associate with mTBI and PCS symptoms severity and duration. In this context, Devoto et al [22] reported more than 20 miRNAs as dysregulated when comparing mTBI patients with controls. They also pointed out that there could be significant differences in brain tissues response to the type of head injury, as they found that the expression of 23 miRNAs is significantly different in blast versus blunt mTBI. Furthermore, Guedes et al [28] reported that miR-139–5p, miR-204–5p, miR-372–3p, miR-509-3-5p, miR-615–5p, and miR-1277–3p expressions were different in mTBI patients versus healthy controls, and also that other 4 miRNAs have significantly different expression in mTBI patients that exhibit PTSD symptoms. Thus, the dysregulated miRNAs were analyzed in the context of their involvement in various pathways, including inflammation, neuronal repair, and cellular development.
Exosomal cytokines
The role of exosomal cytokines as biomarkers for mTBI and PCS was also investigated, and the levels of IL-6 and IL-10 were reported as significantly increased in neuronal-derived exosomes isolated from the peripheral blood of military personnel with mTBI [23]. Also, post-injury extracellular vesicles-associated IL-6 levels were significantly increased and positively associated with the number of days the injured athletes reported PC symptoms [27]. Similar findings were reported by Goetzl et al, but they further reported that impaired IL-6 levels could also be correlated to the chronic phase of mTBI and PCS and possibly contribute to the development of CTE [24].
Neuron-derived exosomes
The potential role of neuron-derived exosomes in transporting proteins and neurotoxic forms of amyloid β peptides or p-tau in the context of CTE was investigated by Goetzl et al. [24]. They described several pathways through which neuron-derived exosomal content (specifically IL-6 and aquaporins) could contribute to persistent PCS, neuroinflammation, and eventually to CTE development. The pathophysiological mechanisms of CTE were also described in the context neuron-derived exosomal content isolation from peripheral blood, as PRPc, XIIIa, and synaptogyrin-3 were found to interact with neurotoxic molecules within the brain tissues and act as transporters to peripheral regions.
Discussion
Mild TBI and PCS are complex disorders with a range of symptoms that can persist long after the initial injury [1,2]. Our previous studies described the persistent PCS symptoms and their implication in patients’ recovery following a mTBI event [29]. Also, we found that the persistent symptomatology could be associated with brain volumetric changes and long-term brain molecular imbalance [30]. However, there might be suggestive molecular changes that could be addressing a certain window in time following the traumatic event [31]. In this context, the lack of reliable biomarkers for mTBI and PCS has hindered these disorders diagnosis, understanding, and treatment [2]. Our studies have previously suggested the need of biomarkers that could be found in easily-obtainable biological fluids. In a recent review, we described the potential of saliva to contain several dozens of molecules with critical relevance to mTBI [31]. Not only that saliva is far easier to obtain, as compared to other biological fluids and preferred by the patients, but also a possible source of faster detection for biochemical changes after traumatic events [31]. Nevertheless, mTBI is not the sole pathological event that leads to changes within the exosomal content of the saliva, as also Zhang et al [32] and Hoffman et al [33] previously documented significant differences between healthy and cancer patients salivary exosomes profiles.
Recent studies have shown promising results in using salivary exosomal biomarkers as potential diagnosis and prognosis tools for mTBI and PCS. Also, the importance of exosomes was previously described in mTBI and PCS and studies have shown that their detection could be in significant correlation with the time passed from the traumatic event and with the extent of the subsequent damage [34]. Naturally, the role of exosomes within the brain tissues is to mediate intercellular communication [35]. However, in cases of crisis, exosomes were found to act as potent mediators of neuronal response to stress, inflammation, and regeneration [36,37]. Furthermore, exosomes are potent molecular complexes that could be successfully isolated or even synthetized in vitro and used as potential therapeutic agents [38]. They could moreover be efficient carriers of active therapeutic biomolecules [39]. In this context, various therapeutic applications have recently been described in regenerative medicine and have shown great potential in neurodegenerative diseases treatment [40].
One of the most studied salivary exosomal biomarkers for mTBI and PCS is tau protein, a microtubule-associated protein stabilizing neuronal axons. Tau protein is also implicated in the microtubule-mediated axonal transport making it a key player in neuronal development [41]. However, the active implication of tau aggregation in predisposing to tauopathies was previously demonstrated only for moderate to severe TBIs [42]. Despite this, it was shown that increased levels of tau protein within the biological fluids are mainly present within the first 24 hours post-TBI [43]. The balance between tau and its active phosphorylated form is a known biomarker for acute and chronic TBIs [44]. In several studies discussed here, increased levels of tau protein originating from exosomes were found in the saliva of individuals with mTBI and PCS, indicating axonal damage and neuronal degeneration [19,25,27,28]. Additionally, exosomal phosphorylated tau was found to be elevated in the saliva of individuals with repeated mTBI, suggesting a potential link between repetitive mTBI and chronic neurodegenerative disorders, such as CTE.
Exosomal miRNAs are another class of biomolecules that have shown promise as salivary biomarkers for mTBI and PCS as several studies currently discussed found dysregulated levels of exosomal miRNAs in the saliva of individuals with mTBI and PCS [22,28]. MiRNAs are short RNA molecules consisted of non-coding sequences that regulate gene expression. Some of the miRNAs that were isolated from post-mTBI patients were associated with dendritic differentiation, and synaptic function [34]. One study suggested that dysregulated exosomal miRNAs could be associated with inflammation and neuronal repair pathways in individuals with repeated mTBI [22]. Exosomal miRNAs were also associated with neurological disease, developmental injury and abnormalities, and neuropsychiatric disease, as well as with chronic mTBI [28]. While several miRNAs were shown to be implicated in mTBI, and PCS, as changes in biological fluids levels were previously documented, they were also described as potential therapeutic targets in both animal and patient studies [34].
Cytokines, such as IL-6 and IL-10, have also been investigated as potential salivary exosomal biomarkers for mTBI and PCS and exosomal TNF-α, IL-6, and IL-10 levels were significantly increased in individuals with mTBI, as compared to healthy controls [23,24,27]. The roles of cytokines are mainly tied to inflammatory response, however, in the brain, the activity of cytokines was also described as modulatory in pathways such as learning and memory, neuronal development and differentiation, synaptic plasticity, blood-brain barrier and sleep regulation [45]. Recent studies have investigated the role of salivary exosomal PRPc, XIIIa, synaptogyrin-3, IL-6, and aquaporins in mTBI and PCS and reported that the prolonged increased levels of aquaporins and IL-6 in neuron-derived exosomes might contribute to the persistent central nervous system oedema and inflammation observed in CTE [24]. In this context, the molecular dysregulations caused by mTBI target brain circulation and blood coagulation, brain water balance and edema formation, tau accumulation associated signaling pathway, and acute phase inflammatory response. On the other hand, counteracting measures have been described to aim for homeostasis and repair, as well as for replacement of the damaged cells [46,47]. A recent animal model study showed that Il-6 and TGF-β are implicated in macrophage infiltration and subsequent tissue repair [48]. In this context it would be interesting to study the potential of exosomal cytokines in regeneration after a mTBI event. Thus, future research could focus on describing the changes in exosomal miRNAs’ expressions by correlation to mTBI-affected brain molecular pathways to further understand the altered signaling pathways that lead to mTBI and PCS symptoms and outcomes, as well as possible means to overcome them and to prevent long term effects.
Overall, the discussed studies suggested that salivary exosomal biomarkers, including tau protein, miRNAs, and several cytokines, could be promising diagnosis and prognosis tools for mTBI and PCS. These biomarkers can provide insight into the underlying pathomechanisms of these disorders, as well as assist in the development of targeted therapies for mTBI and PCS. In this way, the importance of this study is given by the perspective we aimed to focus on regarding the potential of salivary mTBI biomarkers, by contrast to other recent studies that were mainly focused on blood biomarkers. However, further research is needed to fully understand the role of these salivary exosomal proteins in the context of mTBI and PCS and to validate these biomarkers according to their clinical utility.
Conclusions
In conclusion, using exosomal biomarkers in saliva has shown great promise in diagnosing and managing mTBI and PCS. There are several studies identifying several exosomal biomarkers for mTBI and PCS: tau protein, p-tau protein, miRNAs, IL-6, and IL-10. These salivary biomarkers could provide a non-invasive diagnostic tool and could assist in identifying individuals at risk for developing chronic symptoms and the progression to CTE. Further research could focus on the exosomal biomarkers as they may provide valuable insight into the underlying pathophysiology of mTBI and PCS that could lead to targeted therapies. Furthermore, future studies are needed to validate these biomarkers in larger cohorts and to determine their sensitivity and specificity in diagnosing mTBI and PCS, as well as finding reliable ways of separating salivary exosomes and quantifying exosomal content. Overall, exosomal biomarkers in saliva show great potential in the diagnosis and management of mTBI and PCS, and future research in this area can significantly improve patient outcomes.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Kazl C, Torres A. Definition, Classification, and Epidemiology of Concussion. Semin Pediatr Neurol. 2019 Jul;30:9-13. [CrossRef]
- Mavroudis I, Kazis D, Chowdhury R, Petridis F, Costa V, Balmus IM, Ciobica A, Luca AC, Radu I, Dobrin RP, Baloyannis S. Post-Concussion Syndrome and Chronic Traumatic Encephalopathy: Narrative Review on the Neuropathology, Neuroimaging and Fluid Biomarkers. Diagnostics (Basel). 2022 Mar 18;12(3):740. [CrossRef]
- Faure J, Lachenal G, Court M, Hirrlinger J, Chatellard-Causse C, Blot B, et al. Exosomes are released by cultured cortical neurones. Mol. Cell. Neurosci. 2006;31:642–648. [CrossRef]
- Song Z, Xu Y, Deng W, Zhang L, Zhu H, Yu P, Qu Y, Zhao W, Han Y, Qin C. Brain Derived Exosomes Are a Double-Edged Sword in Alzheimer's Disease. Front Mol Neurosci. 2020;13:79. [CrossRef]
- DeLeo AM, Ikezu T. Extracellular vesicle biology in Alzheimer’s disease and related tauopathy. J. Neuroimmune Pharmacol. 2018;13:292–308. [CrossRef]
- Johnstone RM, Adam M, Hammond JR, Orr L, Turbide C. Vesicle formation during reticulocyte maturation. Association of plasma membrane activities with released vesicles (exosomes). J Biol Chem. 1987;262:9412-9420.
- Zhang Y, Bi J, Huang J, Tang Y, Du S, Li P. Exosome: a review of its classification, isolation techniques, storage, diagnostic and targeted therapy applications. Int. J. Nanomed. 2020;15:6917–6934. [CrossRef]
- Ratajczak MZ, Ratajczak J. Extracellular microvesicles/exosomes: discovery, disbelief, acceptance, and the future? Leukemia 2020;34:3126–3135. [CrossRef]
- Lotvall J, Hill AF, Hochberg F, Buzas EI, Di Vizio D, Gardiner C, et al. Minimal experimental requirements for definition of extracellular vesicles and their functions: a position statement from the International Society for Extracellular Vesicles. J. Extracell Vesicles 2014;3:26913. [CrossRef]
- McKelvey KJ, Powell KL, Ashton AW, Morris JM, McCracken SA. Exosomes: mechanisms of uptake. J. Circ. Biomark 2015;4:7. [CrossRef]
- Fruhbeis C, Frohlich D, Kuo WP, Amphornrat J, Thilemann S, Saab AS, et al. Neurotransmitter-triggered transfer of exosomes mediates oligodendrocyte-neuron communication. PLoS Biol. 2013;11:e1001604. [CrossRef]
- Manek R, Moghieb A, Yang Z, Kumar D, Kobeissy F, Sarkis GA et al. Correction to: protein biomarkers and neuroproteomics characterization of microvesicles/exosomes from human cerebrospinal fluid following traumatic brain injury. Mol. Neurobiol. 2018;55:6129. [CrossRef]
- Peltz CB, Kenney K, Gill J, Diaz-Arrastia R, Gardner RC, Yaffe K. Blood biomarkers of traumatic brain injury and cognitive impairment in older veterans. Neurology 2020;95:e1126–e1133. [CrossRef]
- Goetzl EJ, Elahi FM, Mustapic M, Kapogiannis D, Pryhoda M, Gilmore A, et al. Altered levels of plasma neuron-derived exosomes and their cargo proteins characterize acute and chronic mild traumatic brain injury. FASEB J. 2019;33:5082–5088. [CrossRef]
- Guedes VA, Kenney K, Shahim P, Qu BX, Lai C, Devoto C et al. Exosomal neurofilament light: a prognostic biomarker for remote symptoms after mild traumatic brain injury? Neurology 2020;94: e2412–e2423. [CrossRef]
- Zhang ZG, Buller B, Chopp M. Exosomes - beyond stem cells for restorative therapy in stroke and neurological injury. Nat Rev Neurol. 2019;15(4):193-203. [CrossRef]
- Huang S, Ge X, Yu J, Han Z, Yin Z, Li Y, Chen F, Wang H, Zhang J, Lei P. Increased miR-124-3p in microglial exosomes following traumatic brain injury inhibits neuronal inflammation and contributes to neurite outgrowth via their transfer into neurons. FASEB J. 2018;32(1):512-528. Erratum in: FASEB J. 2018;32(4):2315. [CrossRef]
- Li D, Huang S, Yin Z, Zhu J, Ge X, Han Z, Tan J, Zhang S, Zhao J, Chen F, Wang H, Lei P. Increases in miR-124-3p in Microglial Exosomes Confer Neuroprotective Effects by Targeting FIP200-Mediated Neuronal Autophagy Following Traumatic Brain Injury. Neurochem Res. 2019;44(8):1903-1923. [CrossRef]
- Kenney K, Qu BX, Lai C, Devoto C, Motamedi V, Walker WC, Levin HS, Nolen T, Wilde EA, Diaz-Arrastia R, Gill J; CENC Multisite Observational Study Investigators. Higher exosomal phosphorylated tau and total tau among veterans with combat-related repetitive chronic mild traumatic brain injury. Brain Inj. 2018;32(10):1276-1284. [CrossRef]
- Wang Z, Wang H, Becker R, Rufo J, Yang S, Mace BE, Wu M, Zou J, Laskowitz DT, Huang TJ. Acoustofluidic separation enables early diagnosis of traumatic brain injury based on circulating exosomes. Microsyst Nanoeng. 2021;7:20. [CrossRef]
- Devoto C, Lai C, Qu BX, Guedes VA, Leete J, Wilde E, Walker WC, Diaz-Arrastia R, Kenney K, Gill J. Exosomal MicroRNAs in Military Personnel with Mild Traumatic Brain Injury: Preliminary Results from the Chronic Effects of Neurotrauma Consortium Biomarker Discovery Project. J Neurotrauma. 2020;37(23):2482-2492. [CrossRef]
- Devoto C, Guedes VA, Lai C, Leete JJ, Mithani S, Edwards K, Vorn R, Qu BX, Wilde EA, Walker WC, Diaz-Arrastia R, Werner JK, Kenney K, Gill JM. Remote blast-related mild traumatic brain injury is associated with differential expression of exosomal microRNAs identified in neurodegenerative and immunological processes. Brain Inj. 2022;36(5):652-661. [CrossRef]
- Gill J, Mustapic M, Diaz-Arrastia R, Lange R, Gulyani S, Diehl T, Motamedi V, Osier N, Stern RA, Kapogiannis D. Higher exosomal tau, amyloid-beta 42 and IL-10 are associated with mild TBIs and chronic symptoms in military personnel. Brain Inj. 2018;32(10):1277-1284. [CrossRef]
- Goetzl EJ, Ledreux A, Granholm AC, Elahi FM, Goetzl L, Hiramoto J, Kapogiannis D. Neuron-Derived Exosome Proteins May Contribute to Progression From Repetitive Mild Traumatic Brain Injuries to Chronic Traumatic Encephalopathy. Front Neurosci. 2019;13:452. [CrossRef]
- Winston CN, Romero HK, Ellisman M, Nauss S, Julovich DA, Conger T, Hall JR, Campana W, O'Bryant SE, Nievergelt CM, Baker DG, Risbrough VB, Rissman RA. Assessing Neuronal and Astrocyte Derived Exosomes From Individuals With Mild Traumatic Brain Injury for Markers of Neurodegeneration and Cytotoxic Activity. Front Neurosci. 2019;13:1005. [CrossRef]
- Guedes VA, Kenney K, Shahim P, Qu BX, Lai C, Devoto C, Walker WC, Nolen T, Diaz-Arrastia R, Gill JM; CENC Multisite Observational Study Investigators. Exosomal neurofilament light: A prognostic biomarker for remote symptoms after mild traumatic brain injury? Neurology. 2020;94(23):e2412-e2423. [CrossRef]
- Meier TB, Guedes VA, Smith EG, Sass D, Mithani S, Vorn R, Savitz J, Teague TK, McCrea MA, Gill JM. Extracellular vesicle-associated cytokines in sport-related concussion. Brain Behav Immun. 2022;100:83-87. [CrossRef]
- Guedes VA, Lai C, Devoto C, Edwards KA, Mithani S, Sass D, Vorn R, Qu BX, Rusch HL, Martin CA, Walker WC, Wilde EA, Diaz-Arrastia R, Gill JM, Kenney K. Extracellular Vesicle Proteins and MicroRNAs Are Linked to Chronic Post-Traumatic Stress Disorder Symptoms in Service Members and Veterans With Mild Traumatic Brain Injury. Front Pharmacol. 2021;12:745348. [CrossRef]
- Mavroudis, I.; Chatzikonstantinou, S.; Petridis, F.; Palade, O.D.; Ciobica, A.; Balmus, I.-M. Functional Overlay Model of Persistent Post-Concussion Syndrome. Brain Sci. 2023, 13, 1028. [CrossRef]
- Mavroudis, I.; Chatzikonstantinou, S.; Ciobica, A.; Balmus, I.-M.; Iordache, A.; Kazis, D.; Chowdhury, R.; Luca, A.-C. A Systematic Review and Meta-Analysis of the Grey Matter Volumetric Changes in Mild Traumatic Brain Injuries. Appl. Sci. 2022, 12, 9954. [Google Scholar] [CrossRef]
- Mavroudis, I.; Petridis, F.; Balmus, I.-M.; Ciobica, A.; Gorgan, D.L.; Luca, A.C. Review on the Role of Salivary Biomarkers in the Diagnosis of Mild Traumatic Brain Injury and Post-Concussion Syndrome. Diagnostics 2023, 13, 1367. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Bi, J.; Huang, J.; Tang, Y.; Du, S.; Li, P. Exosome: A Review of Its Classification, Isolation Techniques, Storage, Diagnostic and Targeted Therapy Applications. Int J Nanomedicine. 2020; 15, 6917-6934. [CrossRef]
- Hofmann, L.; Medyany, V.; Ezić, J.; Lotfi, R.; Niesler, B.; Röth, R.; Engelhardt, D.; Laban, S.; Schuler, P.J.; Hoffmann, T.K.; Brunner, C.; Jackson, E.K.; Theodoraki, M.N. Cargo and Functional Profile of Saliva-Derived Exosomes Reveal Biomarkers Specific for Head and Neck Cancer. Front Med (Lausanne). 2022, 9, 904295. [Google Scholar] [CrossRef] [PubMed]
- Mavroudis, I.; Balmus, I.-M.; Ciobica, A.; Nicoara, M.N.; Luca, A.C.; Palade, D.O. The Role of Microglial Exosomes and miR-124-3p in Neuroinflammation and Neuronal Repair after Traumatic Brain Injury. Life 2023, 13, 1924. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; He, F.; Li, T.; Chen, J.; Jiang, L.; Ouyang, X-P.; Zuo, L. Role of Exosomes in Brain Diseases. Front. Cell. Neurosci. 2021, 15, 743353. [CrossRef]
- Saeedi, S.; Israel, S.; Nagy, C.; Turecki, G. The emerging role of exosomes in mental disorders. Transl Psychiatry. 2019, 9, 122. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Chen, Z.; Zhang, M. Role of exosomes in the pathogenesis, diagnosis, and treatment of central nervous system diseases. J Transl Med, 2022, 20, 291. [CrossRef]
- Xu, X.; Xu, L.; Wen, C.; Xia, J.; Zhang, Y.; Liang, Y. Programming assembly of biomimetic exosomes: An emerging theranostic nanomedicine platform. Mater Today Bio. 2023, 22, 100760. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Cheng, K. Stem cell-derived exosome versus stem cell therapy. Nat Rev Bioeng. 2023, 1, 608–609. [Google Scholar] [CrossRef] [PubMed]
- Muthu, S.; Bapat, A.; Jain, R.; Jeyaraman, N.; Jeyaraman, M. Exosomal therapy-a new frontier in regenerative medicine. Stem Cell Investig. 2021, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Dehmelt, L.; Halpain, S. The MAP2/Tau family of microtubule-associated proteins. Genome Biol. 2004, 6 (1), 204. [Google Scholar] [CrossRef] [PubMed]
- Edwards, G.; Zhao, J.; Dash, P.K.; Soto, C.; Moreno-Gonzalez, I. Traumatic Brain Injury Induces Tau Aggregation and Spreading. J Neurotrauma. 2020, 37(1) ,80-92. [CrossRef]
- Hossain, I.; Blennow, K.; Posti, J.P.; Zetterberg, H. Tau as a fluid biomarker of concussion and neurodegeneration. Concussion. 2022, 7(2), CNC98. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau-Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74(9), 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Bourgognon, J-M.; Cavanagh, J. The role of cytokines in modulating learning and memory and brain plasticity. Brain and Neuroscience Advances. 2020, 4. [CrossRef]
- Alam, A.; Thelin, E.P.; Tajsic, T.; et al. Cellular infiltration in traumatic brain injury. J Neuroinflammation, 2020, 17, 328. [CrossRef]
- Bao, W.; Lin, Y.; Chen, Z. The Peripheral Immune System and Traumatic Brain Injury: Insight into the role of T-helper cells. Int J Med Sci 2021, 18(16), 3644–3651. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Xiao, J.; Xu, X.; Li, W.; Zhong, R.; Qi, L.; Chen, J.; Cui, G.; et al. M-CSF, IL-6, and TGF-β promote generation of a new subset of tissue repair macrophage for traumatic brain injury recovery. Sci Adv. 2021, 7(11), eabb6260. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flowchart of the study regarding the potential of exosomal biomarkers in mild traumatic brain injury and post-concussion syndrome.
Figure 1.
PRISMA flowchart of the study regarding the potential of exosomal biomarkers in mild traumatic brain injury and post-concussion syndrome.
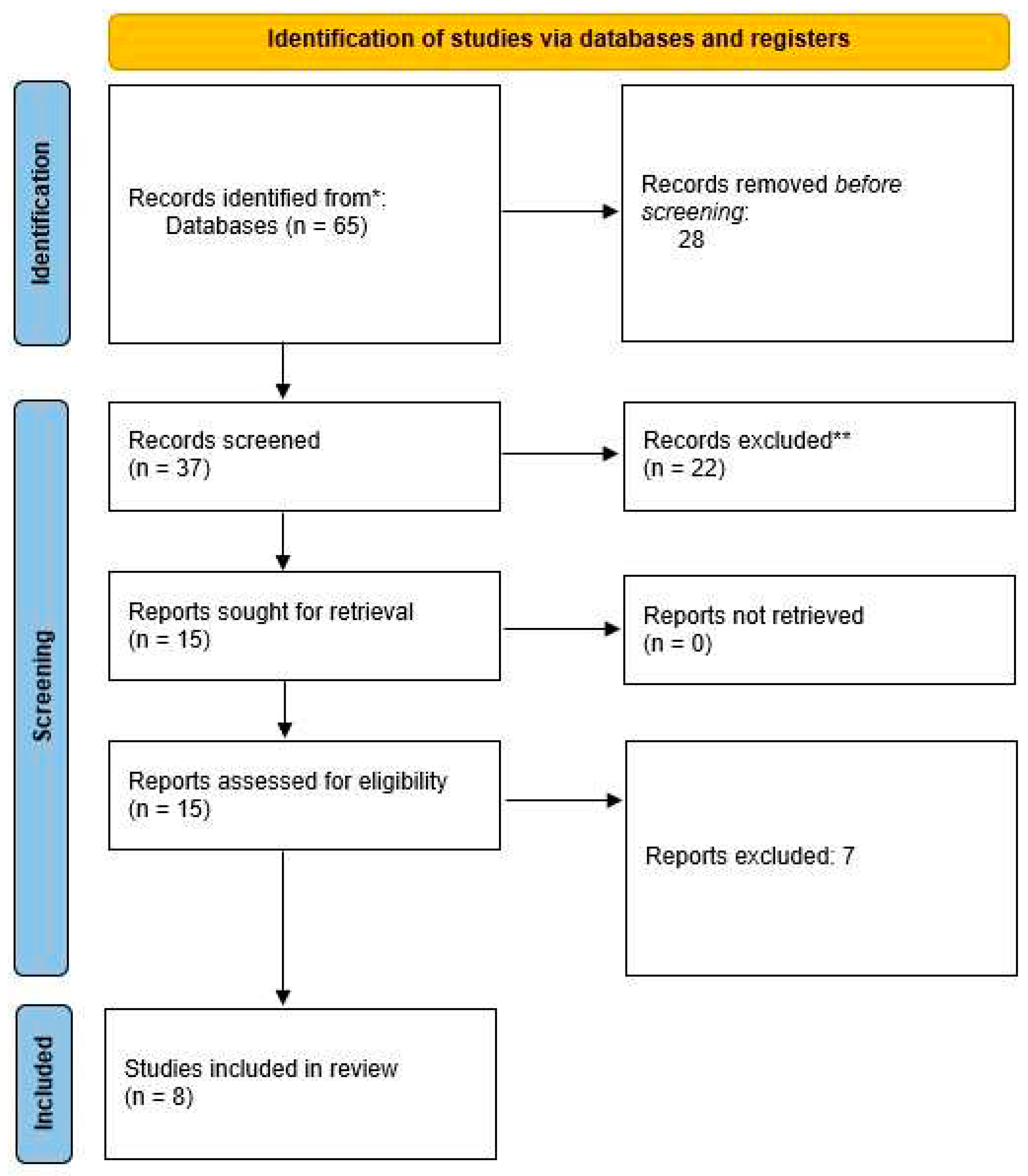
Figure 2.
Quality assessment for the studies included in this systematic review.
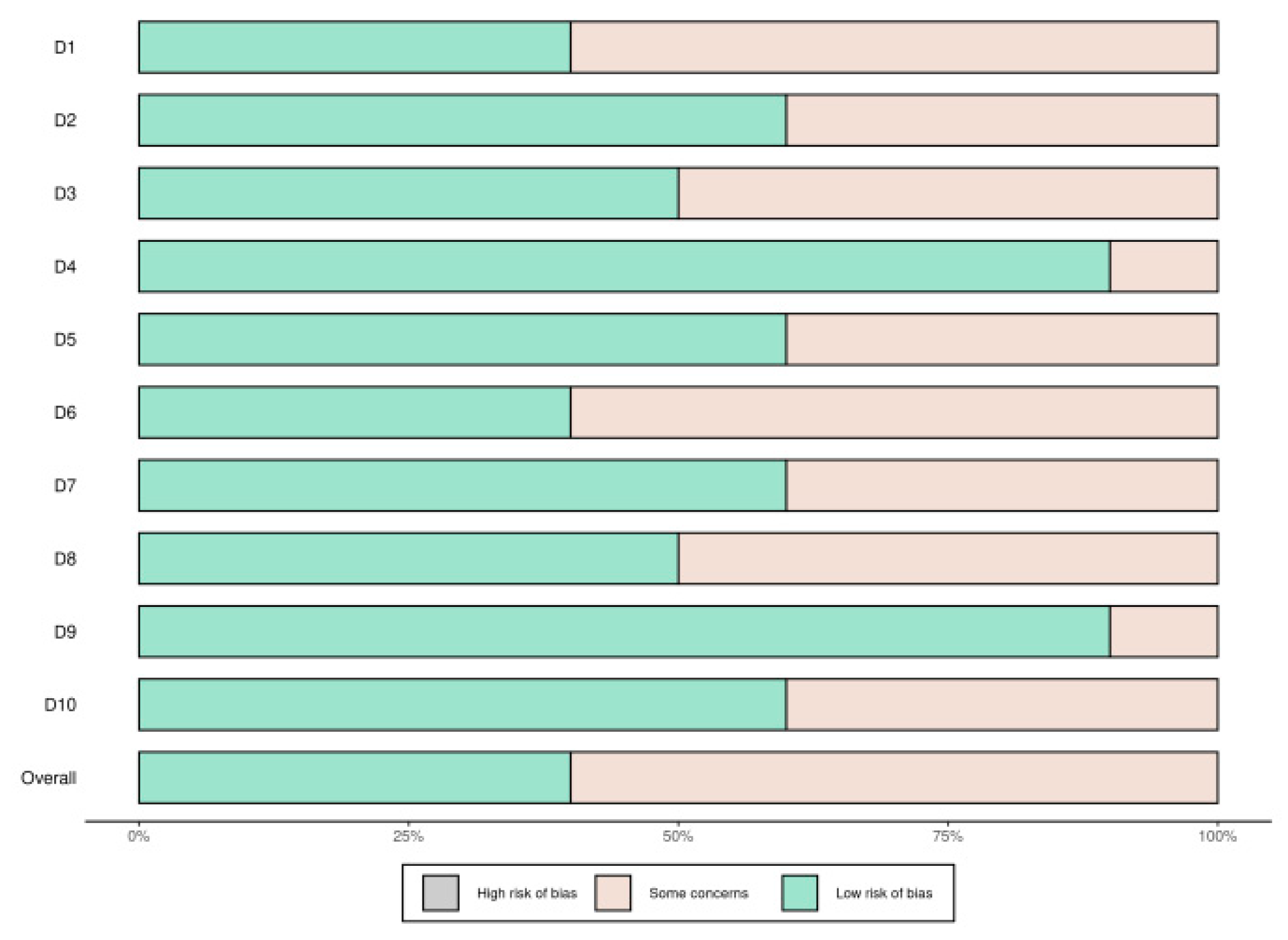
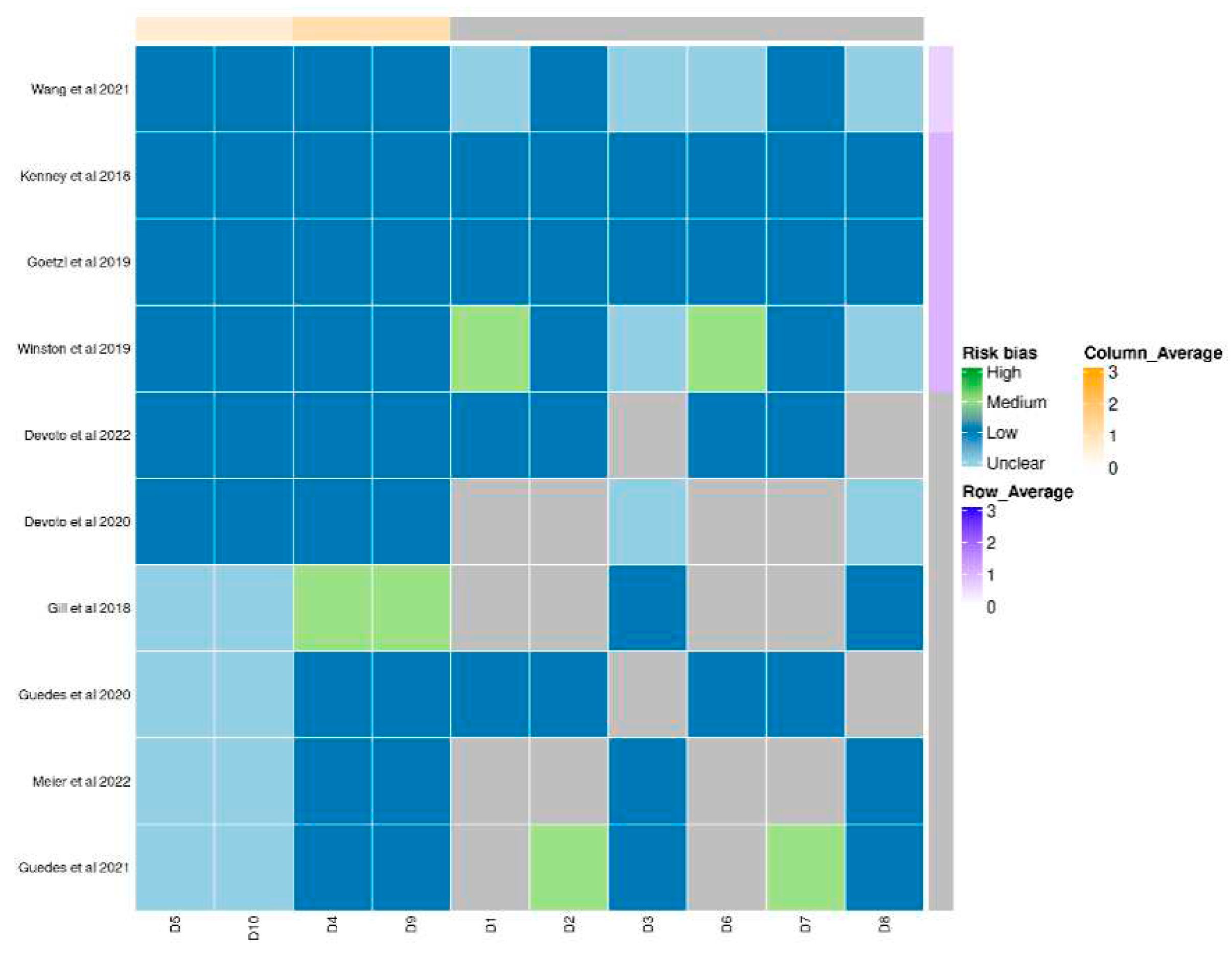

Table 1.
Recent highlights on the role of TBI biomarkers.
| Exosomal biomarkers | Recent findings | References |
|---|---|---|
| tau and p-tau | Both exosomal tau and p-tau level changes were reported in mTBI and repetitive mTBI; exosomal p-tau levels were correlated with chronic neurophychological symptoms of PCS | [19,25,27,28] |
| micro-RNAs | The miRNAs for which changes in expression were reported in mTBI and PCS are involved in cell proliferation, cerebral microcirculation, apoptosis, tau accumulation, and neuronal differentiation | [22,28] |
| cytokines | IL-6 and IL-10 could be correlated with acute phase response in mTBI; IL-6 was associated with chronic post-concussion symptoms and the number of days of their manifestation | [23,24,27] |
| neuron-derived exosomes | Potential in transporting signal molecules, proteins (inflammatory factors), and neurotoxic peptides | [24] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



