
Submitted:
22 November 2023
Posted:
26 November 2023
You are already at the latest version
Abstract
Background: First-line biological diagnosis of malaria in Mali is based on the use of rapid diagnostic tests (RDT), which detect in the blood the Histidin Rich Protein 2 antigen, specific to Plasmodium falciparum. Our study, based on a real-time polymerase chain reaction (qPCR) gold-standard diagnosis, aims to evaluate the performance of RDTs used in Mali and to describe the distribution of Plasmodium species in each administrative regions of Mali; Methods: We collected RDT cassettes in 47 sites of the nine regions of Mali. We randomly selected 150 malaria-negative and up to 30 malaria-positive RDTs from each regions. DNA was extracted from the RDTs’ nitrocellulose strip and then assayed with a pan-Plasmodium qPCR. Positive samples were then analyzed with qPCRs specific for P. falciparum, P. malariae, P. vivax, and P. ovale; Results: Of the 1,389 tested by qPCR RDTs, 258 (18.6%) were positive for Plasmodium spp. P.falciparum was the most predominant (97.3%). However, the prevalence of P.vivax reach 21.1% in the Ménaka region in the north; Conclusion: Overall, RDT diagnostic indices are adequate for the biological diagnosis of malaria in Mali. Our finding support the adjustment of RDTs to the local epidemiology.
Keywords:
Diagnostic
; Paludisme
; TDR
; Sensibilité
; Spécificité
; RAP
; Mali
1. Introduction
Despite numerous efforts, malaria remains a major public health problem in the world [1]. According to the latest estimates of the World Health Organization published in December 2022, there were 247 million cases of malaria in 2021 vs 245 million in 2020 [2]. About 619,000 deaths were attributed to this disease in 2021 vs 625,000 deaths in 2020[1]. Four of the African countries account for nearly half of all malaria cases worldwide - Nigeria (26.6 %), the Democratic Republic of Congo 12.3 %, Uganda 5.1 %, and Mozambique 4.1 % [1].
The 5.9% increase in malaria incidence in 2020 is mainly explained, on the one hand, by the of the health system dysfunctions secondary to the Covid-19 world crisis in countries already burdened by extreme poverty and, on the other hand, an increased rainfall in some countries [2]. Notably, the incidence of malaria has decreased by 229 cases per 1000 inhabitants in 2021, which is quite encouraging [1]. The WHO African Region alone will account for more than 95 % of all malaria cases and 96% of all deaths attributable to malaria in 2021. Children under five years of age are the most vulnerable targets affected by malaria with 80% of all malaria cases and 96 % of all malaria deaths in 2021 [1].
According to the local health information system (LHIS) data in 2021, Mali recorded 3,204,275 confirmed cases of malaria. The number of deaths reported by health facilities was 1,480 deaths, for a hospital case fatality rate of 1.41 ‰ [3]. The Demographic and Health Survey (DHS 2018) showed a 19 % national prevalence of malaria among children under 59 months. Malaria prevalence vary by region: 13 % in Kayes; 22% in Koulikoro; 30 % in Sikasso; 26 % in Segou; 15 % in Gao; 3 % in Timbuktu; 2 % in Kidal; and 1 % in Bamako [4]. The same report stated that infant and child mortality was 101 per 1,000 children aged 6-59 months in 2018[4]. The Malaria Indicator Survey in Mali (MIS 2021), reported a 19.4% national RDT test-based malaria prevalence among children aged 6-59 months [5]. Overall, the figures mentioned above imply that, despite numerous efforts made by the State with its partners, the 125 ‰ (DHIS2 2020) malaria incidence has not decreased to the desired 81 ‰ target level in Mali [6].
After its participating to the Amsterdam Ministerial Conference [7] and joining the Roll-Back Malaria (RBM) initiative in 1999, Mali has edited a national malaria control policy document aiming to enhance malaria control coordination [8]. This document is regularly updated following the WHO recommendations for malaria control. Malaria control is based on prevention and case management. Prevention is achieved with long-lasting insecticidal nets and indoor residual spraying. For malaria case-management, early diagnosis and effective treatment of cases with artemisinin-based combination therapies (ACT) and injectable forms significantly curbed malaria burden [9]. To promote the use of these services, adaptive actions have been taken by the highest Malian authorities, namely the free delivery of ACT, malaria Rapid Diagnostic Tests (RDTs), and malaria treatment kits for pregnant women and children under 5 years of age [10].
For the diagnosis of suspected malaria cases, Mali uses microscopic examination (thick drop and thin smears) and/or lateral flow immunochromatography assays (malaria RDT) [10]. The RDT is based on the detection in the blood of the antigen Histidin Rich Protein 2 (HRP2) specific to Plasmodium falciparum, which is the most prevalent species in Mali [11]. It is most frequently used in primary health care facilities and at the community level by community health workers (CHWs) because of its easy handling [12,13]. It is advantageous in providing results within 15 minutes and discriminating malaria from non-malaria fevers through the detection of at least one specific antigen. The most used antibodies react to HRP2, aldolase, and/or plasmodial lactate dehydrogenase (pLDH). Proper use of RDTs should optimize malaria diagnosis and avoid the negative drug selection pressure due to inappropriate malaria chemotherapy; however, the increase in false-negatives RDTs results poses a new challenge to malaria control [14,15]. Among others, malaria RDTs false-negative results can be explained by asymptomatic malaria with a low, below the RDTs’ limit of detection, parasite density [16,17], and the increasingly reported deletion of the parasites’ PfHRP2/3 genes. Whatever the cause, false-negative RDT results in untreated patients who carry parasites, which maintain malaria transmission [18]. All of these issues pose a serious threat to NMCPs, especially when only RDT results are used for malaria prevalence monitoring, with no other reference technique [19]. PCR-based diagnostic tests display an improved sensitivity, specificity for Plasmodium species detection and identification and they more accurately detect mixed infections than traditional methods [20,21]. Although PCR is not currently optimized for routine diagnostics, its use in epidemiological studies remains unquestionable [9].
P. falciparum is the dominant species in Mali. It causes severe and complicated forms of malaria and is burdened by a high fatality [22]. However, studies conducted in northern and central Mali have documented other species of Plasmodium such as P. malariae, P. vivax, and P. ovale with a prevalence ranging from 1 to 20%.[23,24,25]. In the context of scaling up malaria control measures, and in the perspective of the emergence of other Plasmodium species, this study aimed to provide useful information on i) the performance of rapid diagnostic tests compared to qPCR for the biological diagnosis of malaria and ii) the distribution of the different Plasmodium species in Mali.
2. Methods
2.1. Study sites and period of sample collection
Mali is a landlocked country in West Africa located between the 10- and 25-degrees north latitudes and between the 4- and 12-degrees west longitudes. It covers a 1,241,238 km2 area, which extends from North to South for 1,500 km, and from East to West for 1,800 km. It shares 7,200 km of borders with Algeria and Mauritania to the north, Niger to the east, Burkina Faso and Côte d’Ivoire to the south, the Republic of Guinea to the southwest and Senegal to the west. Two major rivers, namely the Niger and the Senegal rivers, serve Mali, especially the south and part of the north of the country. The climate is tropical with very high temperature variations. There is a dry season and a rainy season, the latter lasts on average 5 months in the south and less than 3 months in the north. There are 3 climatic zones in Mali that extend from south to north. The Sudano-Guinean zone, which covers 25% of the territory and has a rainfall of approximately 1,300 to 1,500 mm per year, the Sahelian zone, which covers 50 % of the territory and receives rainfall of 200 to 800 mm per year and the Saharan desert zone which represents 25 % of the territory. This zone is marked by irregular rainfall, often less than 200 mm per year.
Mali’s population is characterized by its extreme youth. Since 2012, the country has been going through an unprecedented political and security crisis that has led to numerous internally displaced persons and refugees in neighbouring countries. The level of malaria endemicity in Mali varies from one eco-climatic region to the other. Factors responsible for variations in endemicity include rainfall, altitude, temperature, hydro-agricultural development and urbanization.
TDR cassette samples were collected as part of a national malaria control program (NMCP) survey between June and December 2021 in 47 study sites located in the regions of Kayes, Koulikoro, Sikasso, Ségou, Mopti, Timbuktu, Gao, Kidal and Menaka. The region of Taoudenit was not surveyed because it is not endemic for malaria due to its Saharan climate.
2.2. Rapid diagnostic test (RDT):
In Mali, the purchase and distribution of rapid diagnostic tests (whether paid for by patients or free of charge) is an essential part of the master plan for the supply and distribution of essential medicines (SDADME). To control consumption needs and guarantee their availability and quality, they are managed in the same way as other medicines, using the same management tools. Decision No. 2011-774/MS-SG of 11 July 2011 made their application mandatory.
Its objective is to ensure the correct supply of health products to the population by the Popular Pharmacy of Mali (PPM), which is the State’s preferred tool for the supply, storage and distribution of health products through a State-PPM contract-plan. This system is supplemented by the private sector through the Private Import and Wholesale Establishments (EPIWG) of approved pharmaceutical products or private “wholesalers”. As part of humanitarian actions, non-governmental organizations (NGOs) can donate TDRs to the regions without the NMCP being informed of the model (manufacturer, type of tape, etc.).
The RDTs that were used in our study sites were: the SD Bioline Pf Ag (Standard Diagnostics, Inc, 05FK50), Adv Dx Malaria Pf Ag HRP2 (J. Mitra & Co. Pvt. Ltd., IR016025), which both detect the P. falciparum specific Histidin-rich Protein 2; and First Response Malaria Ag pLDH/HRP2 (Premier Medical Corporation Ltd., I16FRC25) that detect the protein Lactate Dehydrogenase (pLDH) of P. falciparum and screen for other Plasmodium species (Pan). RDT were used for malaria diagnosis on from febrile persons presenting at the health centres in our study sites (Figure 1). They were selected proportionally to the different collection sites in the region before including positive and negative RDTs in the study. Invalid RDTs only were excluded.
2.3. DNA extraction technique:
The selected RDT cassettes were opened under a Type 2 Microbiological Safety Station (MSS) using the dissecting needle (LANCEOLEE Models LT2304, Pakistan), dissecting forceps and a pair of scissors. The nitrocellulose tape was removed from the plastic cassette and then cut into small 3x3 mm pieces using scissors for each sample. The scissors were decontaminated between each sample with 70° ethanol [26].The cut nitrocellulose samples were then introduced into 1.5mL collection tubes for incubation at room temperature in 400 µL of Nuclisens EasyMag Lysis Buffer (bioMérieux, Craponne, France). The tubes were then centrifuged for two minutes at 13000 rpm using Lyse & spin basket tubes (Qiagen, Courtaboeuf, France) to retain the nitrocellulose pieces and to perform an extraction of the filtrate.
The extraction was performed from 200 µL of the filtrate according to the DNA Blood EZI Advanced XL protocol (QIAGEN Instruments Hombrechtikon, Switzerland), with a final elution volume of 50 µL to concentrate the DNA sample as much as possible. To control the quality of DNA extraction, some samples were assayed by the Qubit technique (QUBIT2.0, Life Technologies Villebon sur Yvette, France). The extracted DNA was then stored at -20 °C.
2.4. Plasmodium species detection by qPCR
DNA extracted from the nitrocellulose strip of malaria-positive and malaria-negative RDT cassettes were first subjected to pan-Plasmodium qPCR. In a second step only the samples that were positive were tested with primers and probes specific for P. falciparum, P. malariae, P. vivax, and P. ovale for identification of the Plasmodium species [27].
For the amplification reactions we used:100μl of Roche Mix (Roche diagnostics GmbH, Mannheim, Germany), 18 μl of each primer (sense and antisense), 12 μl of probe (Var ATS Probe) and 2μl of distilled water then were distributed 20 μl of this Mix plus 2 μl of added DNA. Several negative controls were plated on each PCR plate. A positive control for each species was also deposited as a reaction control. The PCR conditions are summarized in (Table 1). The analyses were performed by real-time PCR technique on CFX96 (BIO-RAD, Marnes-la-Coquette, France) and LightCycler480 II, 384, (Roche Diagnostic International Ltd., Rotkreuz, Switzerland).
For the first (pan-Plasmodium) qPCR, the samples were deposited in duplicate with 3 negative controls and one positive control. The qPCR results were considered positive when the amplification threshold (Ct) value obtained for the sample was less than 39. The amplification reaction program for the detection of plasmodial species was performed as follows: 2 minutes at 50 °C, 5 minutes at 95 °C, 45 cycles (10 seconds at 95 °C, 30 seconds at 54 °C, 1 minute at 60 °C), and 30 seconds at 40 °C [25].
Hybridisation temperature were 60 °C for each, and the probes were TaqmanTM hydrolysis probes [25].
2.5. Case definition
We considered the Plasmodium-specific PCR assay as the malaria diagnosis gold-standard. Irrespective of the TDR result, a malaria case had to display a positive Plasmodium-specific PCR result.
2.6. Data analyses
Data were processed in Excel (version 2013) and analysed using 2 way contingency table analysis [28]. Diagnostic performance of malaria RDTs were determined via sensitivity (Se), specificity (Sp), and Youden and Kappa indices, each with their 95% confidence intervals (CI95%). Sensitivity was as the proportion of malaria cases who had a positive RDT. Specificity was the proportion of non-malaria cases (PCR negative) who had a negative RDT. The agreement between the two diagnostic methods was estimated by the Kappa coefficient [29]. The Kappa coefficient indicates a strong agreement when greater than 0.8 and a poor agreement when less than 0.53. The Youden index (Y= Se+Sp-1) considers both sensitivity and specificity to assess the validity of a diagnostic test.
3. Results
During the study period, 3098 malaria RDT cassettes were collected from 47 sites in the 9 regions of Mali, of which 1002 (32%) were positive (Table 2). We then randomly selected 30 positive and 150 negative RDTs in each administrative region; except in two regions, namely Menaka and Kidal, where all positive tests (21 and 29 for Menaka and Kidal, respectively) and all negative test (n=36) in Menaka were included. Of the 1397 selected malaria RDT cassettes, 260 were positive and 1131 negative for malaria, and all were further analysed by Plasmodium spp qPCR. Among the 1389 RDTs assayed, 258 had a positive Plasmodium spp. qPCR. Among these 258, 251 (97.3 %) were positive for P. falciparum, 5 (1.9 %) for P. vivax and 2 (0.8 %) for P. malariae. We detected two cases of mixed infections, where P. falciparum was combined either with P. vivax or P. malariae, in Kidal or Koulikoro, respectively (Table 3).
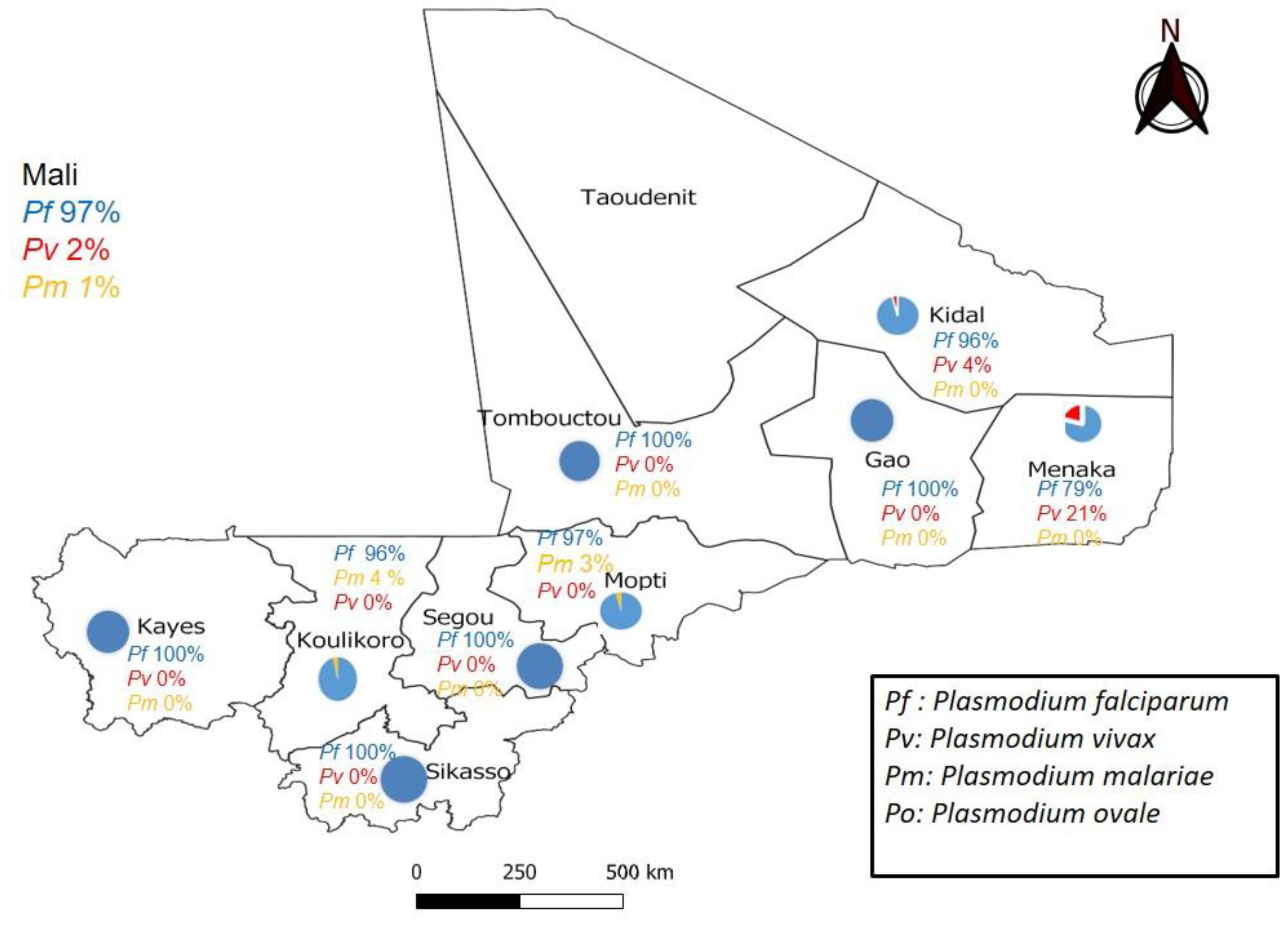
Figure 2.
Plasmodium species distribution in the nine administrative regions of Mali where malaria is endemic.
Figure 2.
Plasmodium species distribution in the nine administrative regions of Mali where malaria is endemic.
P. falciparum distribution was ubiquitous species with a prevalence ranging from 79 % to 100 % of the positive PCRs, depending on the region. P. vivax was identified in 21.5 % (4/19) and 4.3 % (1/23) of the positive PCRs in Menaka and Kidal, respectively. P. malariae was identified in 2.90 % (1/34) and 3.57% (1/28) of the positive PCRs in Mopti and Koulikoro, respectively. P. ovale was detected in none of our samples. Remarkably, we identified two cases of P. vivax for example in Menaka (4) (Figure 3) and Kidal (1) on negative RDTs, which only detected the HPR2 antigen specific to P. falciparum.
We observed 81 discordant RDT results, namely 15.6 % (39/250) false-positive and 3.7 % (42/1131) false-negative results (Table 4) had discordant cases. We found a particularly high false-negative rate (12/100) in Segou.
We observed both a high (96.4%) sensitivity (Se) and high (98 %) specificity (Sp) of the RDTs in the Koulikoro region. In contrast, the Kidal region displayed the lowest Se (65.2) and Sp (91.8 %). The Youden and Cohen’s Kappa indices of RDTs compared to PCR for the different regions are detailed in the (Table 4). The RDT displayed acceptable diagnostic indices. The lower bounds of the 95% confidence intervals (CI95%) of Cohen’s Youden and Kappa indices were all ≥ 0.50 except in the Kidal region where Youden and Kappa indices were 0.57 (95%CI [0.35-0.75]) and 0.53 (95%CI [0.32-0.70], respectively.
4. Discussion:
This study’s main findings are that, although P. falciparum is the most prevalent species overall, non-Plasmodium species are also observed notably P. vivax in the Northern part of Mali. Remarkably, the RDT display lower diagnostic indices in these regions.
Regarding the predominance of P. falciparum, we report a prevalence ranging from 79 % to 100 % of the positive malaria tests according to the regions of Mali. Our results are consistent with those of Doumbo et al., who reported that P. falciparum accounted for 98.2% of the positive Plasmodium spp. tests since 1988 [23]. In 2011, an increase in the prevalence of P. falciparum from 74.13 % during the dry season to 63.72 % during the cold season was observed in the study by O. Koita et al. [24]. The results obtained in the Mopti region (97 %) are in line with those of Konate et al. who reported a 98% prevalence of P. falciparum in Badiangara in 2020.[25]. This high prevalence could be explained by the highly seasonal nature of the climate, meso- to hyper-endemic which is characterised by a short rainy season running from June/July to August/September, with rainfall of 400 to 700 mm per year, and a longer dry season. The region is irrigated by the river niger and a tributary, the Yamé, which provides numerous breeding sites for Anopheles gambiae and Anopheles funestus during the 5 months of transmission each year [30].
Remarkably, we found a 21 % or 4 % prevalence of P. vivax in the Menaka or Kidal regions, respectively. Our results are in line with those of Bernabeu et al. in five cities (Goundam, Timbuktu, Gao, Bourem, and Kidal) located in Northern Mali who reported a 30 % prevalence of P. vivax [31]. Briefly, P. vivax was on the rise in the northern part of the country, especially in Menaka where we observed a higher prevalence than Koïta et al. who reported in 2011.
In 2016, a study conducted in four West African countries Burkina Faso, the Gambia, Ghana and Mali verified that the prevalence of non-falciparum infections was higher in Mali (3.81 %, 95% CI [2.22-5.68]) than in The Gambia (0.17 %) [32]. To support this assertion, P. vivax and P. malariae have been found in black African women living in the Bamako area [32]. We also observed P. malariae infections in two regions of Southern Mali, namely 3.7 % in Koulikoro and 2.9 % in Mopti. These findings are comparable with those of a study carried out in the same locality (Koulikoro region), which reported a 2.69 % prevalence rate [33]. P. malariae infection is an established cause of nephrotic syndrome, which can lead to progressive renal failure, particularly in adolescents or young adults [34,35],and it has been associated with a high burden of anaemia [36,37] or death[38]. It is therefore important now for the NMCP to control all non-P. falciparum human infections in order to achieve the malaria elimination goal.
We did not find P. ovale in our samples. However, this less dangerous than P. falciparum parasite species reamin a major public health burden, which needs to be included in the malaria elimination programs [39,40,41]. P. ovale has been reported with a prevalence of around 2% in Mali. [42]. Conventional PCR followed by DNA sequence analysis is commonly used to differentiate these two subspecies, P. ovale curtisi and P. ovale wallikeri, which have been documented in Mali and other West African countries [40,43,44].
The rapid detection and identification of Plasmodium parasite species with improved diagnostic tools are key for operative NMCPs [32]. In our study, the sensitivity of RDTs was higher than 80 % in each region except in Kidal and Segou where it was moderate. The relatively lower performance of RDTs observed in these regions could be explained by the presence of false-negative results in our sites where species other than P. falciparum are detected. Another explanation of an increase in false-negative RDTs results is the emergence of HRP-2/3 gene deletion in P. falciparum populations [15,45]. Other causes might also be the low parasite densities in the blood sample tested [46], the non-compliance with the RDT manufacturer standards, the presence of rheumatoid factors ,the persistence of HRP2 antigen in the patient’s blood several weeks after a well-conducted antimalarial treatment, all of which might cause false-positive RDT results [47]. This relative emergence of non-P. falciparum Plasmodium species could be explained by the incapacity of RDTs only based on the detection of the Pf HRP-2 that is specific to P. falciparum and cannot detect other Plasmodium species. Therefore adapting the diagnostic tools to the regional epidemiology is likely to strengthen malaria control in Mali[48,49] . The use of RDTs that are capable to detect pan-Plasmodium antigens, such as lactate dehydrogenase (pLDH) or aldolase, may improve malaria diagnosis in region where non-P. falciparum Plasmodium species are endemic [13,50].
5. Conclusions
This study confirms that malaria rapid diagnostic tests (RDTs) contribute to a significant improvement in the quality of malaria management in Mali. The performance for malaria diagnosis was excellent in some regions with relatively good sensitivity and specificity. Some false-negative results are linked to the presence of non-P. falciparum species such as P. vivax and P. malariae. Hence, we advocate for adapting RDTs’ specificity to the local epidemiology in order to improve the diagnosis of malaria in Mali.
Authors Contributions
Pascal DEMBELE, Mady Cissoko, Mahamadou A THERA and Stéphane RANQUE designed the study and wrote the first version of the manuscript. Pascal DEMBELE, Mady Cissoko, Adama Z DIARRA, Lassana DOUMBIA, and Maissane Mehadji performed the analysis and interpretation of the results. Mahamadou H MAGASSA and Assaïta KONE contributed to the collection and transport of samples. Mady Cissoko, Mahamadou A THERA and Stéphane RANQUE contributed to the critical revision of the manuscript. All authors have read and approved the final draft of the manuscript.
Acknowledgments
This study was made possible thanks to the academic and financial support of Mediterranee Infection foundation in Marseille, France, and the effective collaboration of each collection sites supervisors. We thank each of you.
Ethical considerations
Our study was authorized by the National Malaria Control Program (number 042/MSDS-SG/NMCP, February 4, 2023), in accordance with Malian regulations on ethics and medical research.
Competing of Interest
The authors declare no competing interest.
References
- Global messaging: World malaria report 2022 https://www.who.int/publications/m/item/WHO-UCN-GMP-2022.07. Available online: https://www.who.int/publications/m/item/WHO-UCN-GMP-2022.07 (accessed on 5 March 2023).
- OMS World Health Organization World Malaria Report 2020; World Health Organization: Geneva, 2021; ISBN 978-92-4-004049-6.; 2021; p. 322;
- CPS/SS-DS-PF-Annuaire SNIS 2021.
- Institut National de La Statistique (INSTAT) Enquête Demographique et de Santé:Http://Www.Sante.Gov.Ml/Docs/EDSM VI.Pdf.
- Enquête Sur Les Indicateurs Du Paludisme Au Mali En 2021.
- PNLP PSE-MALI 2018-2022 2018.
- Conférence ministérielle sur le paludisme (1992 ; Amsterdam).
- WHO_CDS_RBM_2000.25.Pdf.
- OMS Stratégie Technique Mondiale de lutte contre le Paludisme 2016–2030. 2016, 91, 9–10. 91.
- Ministère de La Santé et Du Développement Social, Programme National de Lutte Contre Le Paludisme. Directives Nationales Pour La Prise En Charge de Cas de Paludisme Au Mali. Bamako: Ministère de La Santé et Du Développement Social; 2020.
- Bell, D.; Wongsrichanalai, C.; Barnwell, J.W. Ensuring Quality and Access for Malaria Diagnosis: How Can It Be Achieved? Nat Rev Microbiol 2006, 4, S7–20. [Google Scholar] [CrossRef] [PubMed]
- Lohfeld, L.; Kangombe-Ngwenya, T.; Winters, A.M.; Chisha, Z.; Hamainza, B.; Kamuliwo, M.; Miller, J.M.; Burns, M.; Bridges, D.J. A Qualitative Review of Implementer Perceptions of the National Community-Level Malaria Surveillance System in Southern Province, Zambia. Malar J 2016, 15, 400. [Google Scholar] [CrossRef]
- Randriatsarafara, F.M.; Mandrosovololona, V.; Andrianirinarison, J.C.; Rakotondrandriana, A.N.; Randrianarivo-Solofoniaina, A.E.; Ratsimbasoa, A.; Rakotomanga, J.; de, D.M. [Adherence of private sector providers to uncomplicated malaria management policy in Madagascar]. Pan Afr Med J 2019, 32, 79. [Google Scholar] [CrossRef] [PubMed]
- Mouatcho, J.C.; Goldring, J.P.D. Malaria Rapid Diagnostic Tests: Challenges and Prospects. Journal of Medical Microbiology 2013, 62, 1491–1505. [Google Scholar] [CrossRef]
- Kozycki, C.T.; Umulisa, N.; Rulisa, S.; Mwikarago, E.I.; Musabyimana, J.P.; Habimana, J.P.; Karema, C.; Krogstad, D.J. False-Negative Malaria Rapid Diagnostic Tests in Rwanda: Impact of Plasmodium Falciparum Isolates Lacking Hrp2 and Declining Malaria Transmission. Malar J 2017, 16, 123. [Google Scholar] [CrossRef] [PubMed]
- McMorrow, M.L.; Aidoo, M.; Kachur, S.P. Malaria Rapid Diagnostic Tests in Elimination Settings—Can They Find the Last Parasite? Clinical Microbiology and Infection 2011, 17, 1624–1631. [Google Scholar] [CrossRef]
- Motshoge, T.; Ababio, G.K.; Aleksenko, L.; Read, J.; Peloewetse, E.; Loeto, M.; Mosweunyane, T.; Moakofhi, K.; Ntebele, D.S.; Chihanga, S.; et al. Molecular Evidence of High Rates of Asymptomatic P. Vivax Infection and Very Low P. Falciparum Malaria in Botswana. BMC Infect Dis 2016, 16, 520. [Google Scholar] [CrossRef] [PubMed]
- Feleke, S.M.; Gidey, B.; Mohammed, H.; Nega, D.; Dillu, D.; Haile, M.; Solomon, H.; Parr, J.B.; Tollera, G.; Tasew, G.; et al. Field Performance of Plasmodium Falciparum Lactate Dehydrogenase Rapid Diagnostic Tests during a Large Histidine-Rich Protein 2 Deletion Survey in Ethiopia. Malar J 2022, 21, 236. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Choi, L.; Johnson, S.; Takwoingi, Y. Rapid Diagnostic Tests for Plasmodium Vivax Malaria in Endemic Countries. Cochrane Database of Systematic Reviews 2020, 2020. [Google Scholar] [CrossRef]
- Mens, P.F.; Schoone, G.J.; Kager, P.A.; Schallig, H.D. Detection and Identification of Human Plasmodium Species with Real-Time Quantitative Nucleic Acid Sequence-Based Amplification. Malar J 2006, 5, 80. [Google Scholar] [CrossRef]
- Snounou, G.; Viriyakosol, S.; Zhu, X.P.; Jarra, W.; Pinheiro, L.; do Rosario, V.E.; Thaithong, S.; Brown, K.N. High Sensitivity of Detection of Human Malaria Parasites by the Use of Nested Polymerase Chain Reaction. Mol Biochem Parasitol 1993, 61, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Doumbo, O.; Koita, O.; Traore, S.F.; Sangare, O.; Coulibaly, A.; Robert, V.; Soula, G.; Quilici, M.; Toure, Y.T. Les Aspects Parasitologiques de l’épidémiologie Du Paludisme Dans Le Sahara Malien.
- Doumbo, O.; Koita, O.; Traore, S.F.; Sangare, O.; Coulibaly, A.; Robert, V.; Soula, G.; Quilici, M.; Toure, Y.T. LES ASPECTS PARASITOLOGIQUES DE L’EPIDEMIOLOGIE DU PALUDISME. Médecine d’Afrique Noire, 1991; 5. [Google Scholar]
- Koita, O.A.; Sangaré, L.; Sango, H.A.; Dao, S.; Keita, N.; Maiga, M.; Mounkoro, M.; Fané, Z.; Maiga, A.S.; Traoré, K.; et al. Effect of Seasonality and Ecological Factors on the Prevalence of the Four Malaria Parasite Species in Northern Mali. Journal of Tropical Medicine 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Konaté, A.M. Dynamique de l’infection palustre dans une étude de cohorte d’enfant à Bandiagara. Mali. Thesis, 2020. [Google Scholar]
- DNA Extraction: Preparing Rapid Diagnostic Tests. Available online: https://www.wwarn.org/tools-resources/procedures/dna-extraction-preparing-rapid-diagnostic-tests (accessed on 20 March 2022).
- Sazed, S.A.; Kibria, M.G.; Alam, M.S. An Optimized Real-Time QPCR Method for the Effective Detection of Human Malaria Infections. Diagnostics 2021, 11, 736. [Google Scholar] [CrossRef]
- JavaStat -- 2-Way Contingency Table Analysis. Available online: https://statpages.info/ctab2x2.html (accessed on 8 February 2023).
- Un Coefficient d’accord Pour Les Échelles Nominales - Jacob Cohen, 1960. Available online: https://journals.sagepub.com/doi/abs/10.1177/001316446002000104?journalCode=epma (accessed on 19 February 2023).
- Coulibaly, D.; Rebaudet, S.; Travassos, M.; Tolo, Y.; Laurens, M.; Kone, A.K.; Traore, K.; Guindo, A.; Diarra, I.; Niangaly, A.; et al. Spatio-Temporal Analysis of Malaria within a Transmission Season in Bandiagara, Mali. Malar J 2013, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu, M.; Gomez-Perez, G.P.; Sissoko, S.; Niambélé, M.B.; Haibala, A.A.; Sanz, A.; Théra, M.A.; Fernandez-Becerra, C.; Traoré, K.; Alonso, P.L.; et al. Plasmodium Vivax Malaria in Mali: A Study from Three Different Regions. Malar J 2012, 11, 405. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Njie, F.; Cairns, M.; Bojang, K.; Coulibaly, S.O.; Kayentao, K.; Abubakar, I.; Akor, F.; Mohammed, K.; Bationo, R.; et al. Non-Falciparum Malaria Infections in Pregnant Women in West Africa. Malar J 2016, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Dao, F.; Dembele, L.; Diarra, B.; Sogore, F.; Marin-Menendez, A.; Goita, S.; Haidara, A.S.; Barre, Y.N.; Sangare, C.P.O.; Kone, A.; et al. The Prevalence of Human Plasmodium Species during Peak Transmission Seasons from 2016 to 2021 in the Rural Commune of Ntjiba, Mali. Trop Med Infect Dis 2023, 8, 438. [Google Scholar] [CrossRef] [PubMed]
- Eiam-Ong, S. Malarial Nephropathy. Semin Nephrol 2003, 23, 21–33. [Google Scholar] [CrossRef]
- Hendrickse, R.G.; Adeniyi, A.; Edington, G.M.; Glasgow, E.F.; White, R.H.; Houba, V. Quartan Malarial Nephrotic Syndrome. Collaborative Clinicopathological Study in Nigerian Children. Lancet 1972, 1, 1143–1149. [Google Scholar] [CrossRef]
- Langford, S.; Douglas, N.M.; Lampah, D.A.; Simpson, J.A.; Kenangalem, E.; Sugiarto, P.; Anstey, N.M.; Poespoprodjo, J.R.; Price, R.N. Plasmodium malariae Infection Associated with a High Burden of Anemia: A Hospital-Based Surveillance Study. PLOS Neglected Tropical Diseases 2015, 9, e0004195. [Google Scholar] [CrossRef]
- Dao, F.; Djonor, S.K.; Ayin, C.T.-M.; Adu, G.A.; Sarfo, B.; Nortey, P.; Akuffo, K.O.; Danso-Appiah, A. Burden of Malaria in Children under Five and Caregivers’ Health-Seeking Behaviour for Malaria-Related Symptoms in Artisanal Mining Communities in Ghana. Parasit Vectors 2021, 14, 418. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Cullen, K.A.; Kachur, S.P.; Arguin, P.M.; Baird, J.K. Severe Morbidity and Mortality Risk From Malaria in the United States, 1985–2011. Open Forum Infect Dis 2014, 1, ofu034. [Google Scholar] [CrossRef] [PubMed]
- Collins, W.E.; Jeffery, G.M. Plasmodium Malariae: Parasite and Disease. Clin Microbiol Rev 2007, 20, 579–592. [Google Scholar] [CrossRef]
- Milner, D.A. Malaria Pathogenesis. Cold Spring Harb Perspect Med 2018, 8, a025569. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, G.G.; Böhme, U.; Sanders, M.; Reid, A.J.; Cotton, J.A.; Maiga-Ascofare, O.; Djimdé, A.A.; Apinjoh, T.O.; Amenga-Etego, L.; Manske, M.; et al. Plasmodium Malariae and P. Ovale Genomes Provide Insights into Malaria Parasite Evolution. Nature 2017, 542, 101–104. [Google Scholar] [CrossRef]
- Tebben, K.; Yirampo, S.; Coulibaly, D.; Koné, A.K.; Laurens, M.B.; Stucke, E.M.; Dembélé, A.; Tolo, Y.; Traoré, K.; Niangaly, A.; et al. Malian Children Infected with Plasmodium Ovale and Plasmodium Falciparum Display Very Similar Gene Expression Profiles. PLoS Negl Trop Dis 2023, 17, e0010802. [Google Scholar] [CrossRef]
- Oguike, M.C.; Betson, M.; Burke, M.; Nolder, D.; Stothard, J.R.; Kleinschmidt, I.; Proietti, C.; Bousema, T.; Ndounga, M.; Tanabe, K.; et al. Plasmodium Ovale Curtisi and Plasmodium Ovale Wallikeri Circulate Simultaneously in African Communities. Int J Parasitol 2011, 41, 677–683. [Google Scholar] [CrossRef]
- Phillips, M.A.; Burrows, J.N.; Manyando, C.; van Huijsduijnen, R.H.; Van Voorhis, W.C.; Wells, T.N.C. Malaria. Nat Rev Dis Primers 2017, 3, 17050. [Google Scholar] [CrossRef]
- Martiáñez-Vendrell, X.; Skjefte, M.; Sikka, R.; Gupta, H. Factors Affecting the Performance of HRP2-Based Malaria Rapid Diagnostic Tests. Tropical Medicine and Infectious Disease 2022, 7. [Google Scholar] [CrossRef]
- Harris, I.; Sharrock, W.W.; Bain, L.M.; Gray, K.-A.; Bobogare, A.; Boaz, L.; Lilley, K.; Krause, D.; Vallely, A.; Johnson, M.-L.; et al. A Large Proportion of Asymptomatic Plasmodium Infections with Low and Sub-Microscopic Parasite Densities in the Low Transmission Setting of Temotu Province, Solomon Islands: Challenges for Malaria Diagnostics in an Elimination Setting. Malar J 2010, 9, 254. [Google Scholar] [CrossRef]
- Maltha, J.; Gillet, P.; Cnops, L.; van den Ende, J.; van Esbroeck, M.; Jacobs, J. Malaria Rapid Diagnostic Tests: Plasmodium Falciparum Infections with High Parasite Densities May Generate False Positive Plasmodium Vivax PLDH Lines. Malar J 2010, 9, 198. [Google Scholar] [CrossRef] [PubMed]
- Dembele, P.; Cissoko, M.; Kone, A.; Diarra, A.; Doumbia, L.; Magassa, M.; Mehadji, M.; Thera, M.; Ranque, S. Performance Des Tests de Diagnostic Rapide Pour Le Diagnostic Du Paludisme Au Mali. Revue d’Épidémiologie et de Santé Publique 2023, 71, 101795. [Google Scholar] [CrossRef]
- Agarwal, R.; Choi, L.; Johnson, S.; Takwoingi, Y. Rapid Diagnostic Tests for Plasmodium Vivax Malaria in Endemic Countries. Cochrane Database Syst Rev 2020, 11, CD013218. [Google Scholar] [CrossRef] [PubMed]
- Briolant, S.; Pradines, B.; Basco, L.K. Place de la primaquine dans la lutte contre le paludisme en Afrique francophone. Bull. Soc. Pathol. Exot. 2017, 110, 198–206. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Location of the study sites, in the nine administrative regions of Mali where malaria is endemic.
Figure 1.
Location of the study sites, in the nine administrative regions of Mali where malaria is endemic.
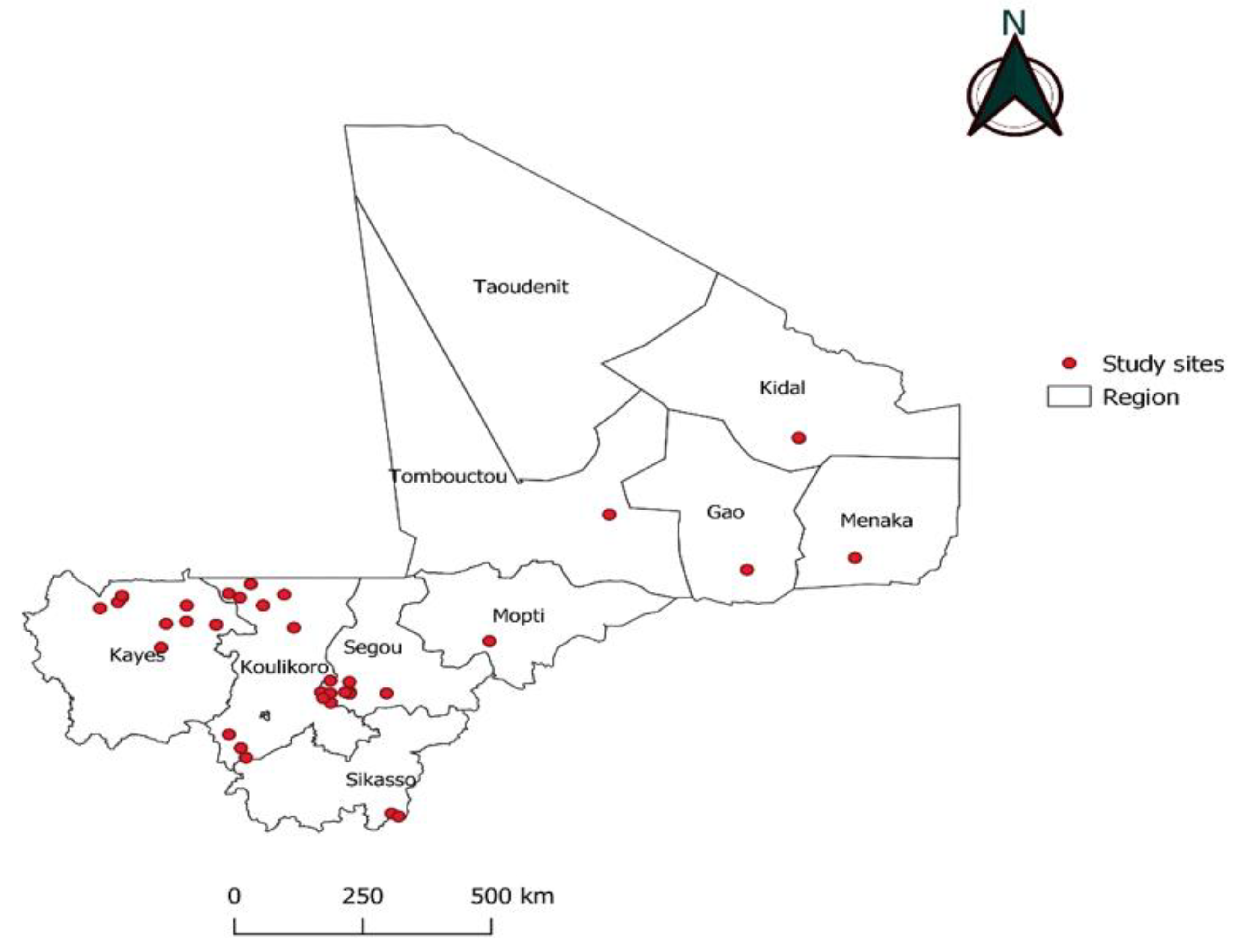
Figure 3.
Amplification curves for real-time PCR targeting 18S rRNA of Plasmodium vivax species in Menaka (positive control in red and positive samples in green).
Figure 3.
Amplification curves for real-time PCR targeting 18S rRNA of Plasmodium vivax species in Menaka (positive control in red and positive samples in green).
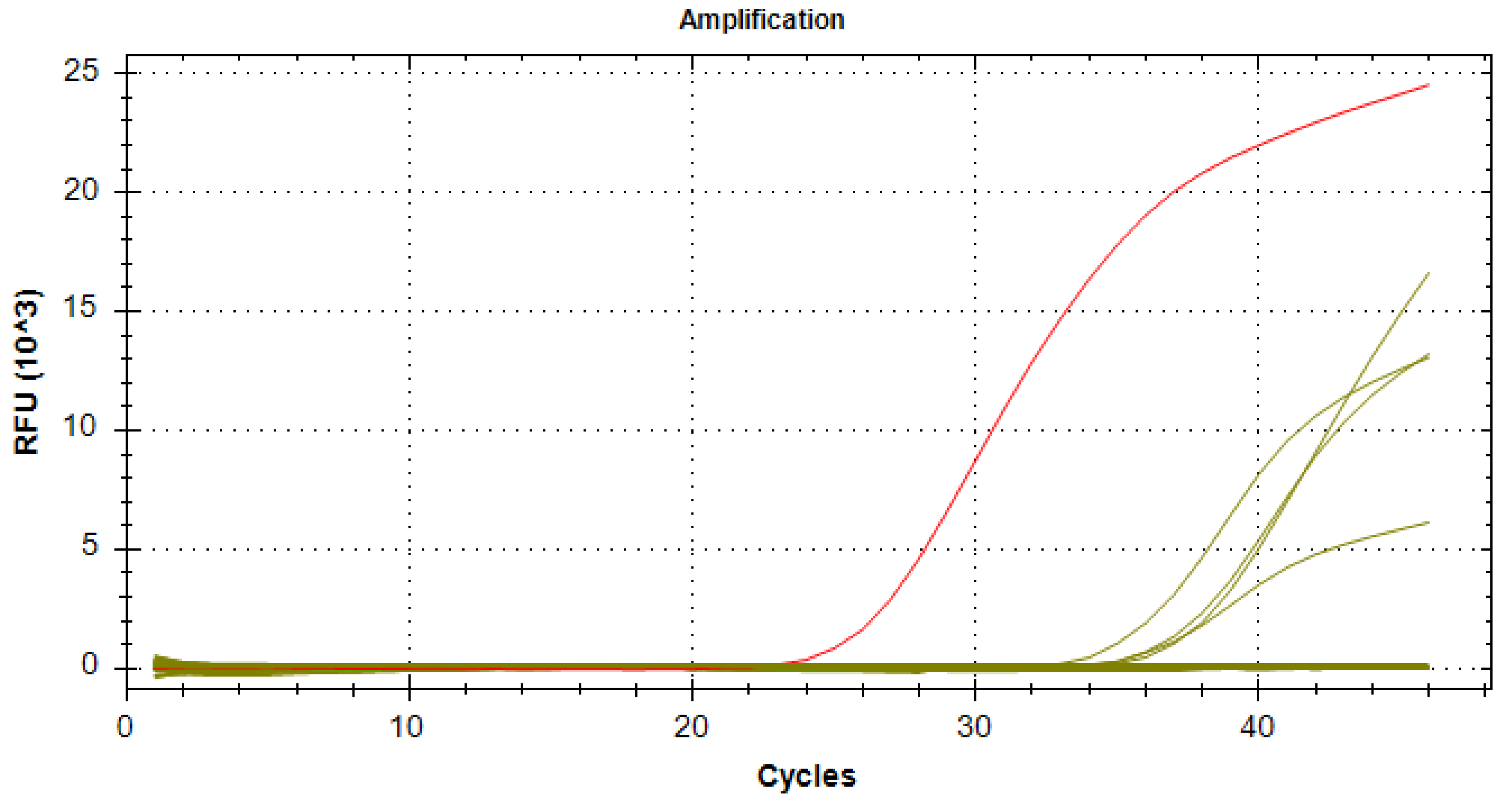

Table 1.
List of the primers and probes, which targeting the Plasmodium spp. 18s rRNA genes, used in our study.
Table 1.
List of the primers and probes, which targeting the Plasmodium spp. 18s rRNA genes, used in our study.
| Target Species | Primers and Probes | Sequences |
|---|---|---|
| Plasmodium spp | VAR ATS-F | CCCATACACAACCAAYTGGA |
| VAR ATS-R | TTCGCACATATCTCTATGTCTATCT | |
| Var ATS-Probe | FAM-TRTTCCATAAATGGT | |
| Plasmodium falciparum | Pf-F | TAGCATATATTAAAATTGTTGCAG |
| Pf-R | GTTATTCCATGCTGTAGTATTCA | |
| Pf-probe | 6FAM-CGGGTAGTCATGATTGAGTTCATTC | |
| Plasmodium malariae | Pm-F | TAGCATATATTAAAATTGTTGCAG |
| Pm-R | GTTATTCCATGCTGTAGTATTCA | |
| Pm-probe | 6FAM- TGCATGGGAATTTTGTTACTTTGAGT | |
| Plasmodium ovale | Po-F | TAGCATATATTAAAATTGTTGCAG |
| Po-F R | GTTATTCCATGCTGTAGTATTCA | |
| Po-probe | 6VIC- TGCATTCCTTATGCAAAATGTGTTC | |
| Plasmodium vivax | Pv-F | AGCATATATTAAAATTGTTGCAG |
| Pv-R | GTTATTCCATGCTGTAGTATTCA | |
| Pv-probe | 6VIC- CGACTTTGTGCGCATTTTGC |
Table 2.
Detail of the total number and the prevalence of positive and negative Malaria Rapid Diagnostic Tests in each health center.
Table 2.
Detail of the total number and the prevalence of positive and negative Malaria Rapid Diagnostic Tests in each health center.
| Area | Health district | RDT collection site | Result | Total | ||
|---|---|---|---|---|---|---|
| Positive N (%) | Negative N (%) | |||||
| Kayes | Diéma | Torodo | 6 (2.2) | 272(97.8) | 278 | |
| Lakamané | 0 (0.0) | 89 (100) | 89 | |||
| Lattakaf | 0 (0.0) | 47 (100) | 47 | |||
| Débomassassi | 0 (0.0) | 48 (100) | 48 | |||
| Koungo | 3 (75.0) | 1 (25.0) | 4 | |||
| Lambidou | 0 (0.0) | 13 (100) | 13 | |||
| Yélimané | kodié | 12 (19.0) | 51(81.0) | 63 | ||
| Csréf | 6 (4,1) | 139 (95.9) | 145 | |||
| Dogofry | 0 (0.0) | 23 (100.0) | 23 | |||
| Bandiougoula | 0 (0.0) | 11 (100.0) | 11 | |||
| sub total | 27 (3.7) | 694 (96.3) | 721 | |||
| Koulikoro | Nara | Bagoini | 0 (0.0) | 50 (100.0) | 50 | |
| Mourdiah | 0 (0.0) | 68 (100.0) | 68 | |||
| Kassakaré | 4 (12.1) | 29 (87.9) | 33 | |||
| Alasso | 1 (3.4) | 28 (96.6) | 29 | |||
| Tiapato | 3 (14.3) | 18 (85.7) | 21 | |||
| Waourou | 0 (0.0) | 13 (100.0) | 13 | |||
| Kangaba | Naréna | 2 (1.6) | 126 (98.4) | 128 | ||
| Cscom Central | 14 (28.0) | 36 (72.0) | 50 | |||
| Séléfougou | 0 (0.0) | 30 (100.0) | 30 | |||
| sub total | 24 (5.7) | 398 (94.3) | 422 | |||
| Sikasso | Kadiolo | cscom central | 110 (59.5) | 75 (40.5) | 185 | |
| Zégoua | 28 (38.89) | 44 (61.1) | 72 | |||
| sub total | 138 (53.7) | 119 (46.3) | 257 | |||
| Segou | Barouéli | Cscom Central | 5 (41.7) | 7 (58.3) | 12 | |
| Dioforogo | 13 (65.0) | 7 (35.0) | 20 | |||
| Tamani | 7 (35.0) | 13 (65.0) | 20 | |||
| NGara | 16 (80.0) | 4 (20.0) | 20 | |||
| Tigui | 20 (100.0) | 0 (0.0) | 20 | |||
| bananido | 7 (50.0) | 7 (50.0) | 14 | |||
| N’Gossola | 5 (31.3) | 11(68.75) | 16 | |||
| Nianzana | 20 (66.7) | 10 (33.3) | 30 | |||
| yerebougou | 16 (80.0) | 4 (20.0) | 20 | |||
| Csréf | 8 (40.0) | 12 (60.0) | 20 | |||
| Ndjila | 10 (50.0) | 10 (50.0) | 20 | |||
| sub total | 127 (59.9) | 85 (40.1) | 212 | |||
| Mopti | Mopti | Soufouroulaye | 79 (34.3) | 151 (65.7) | 230 | |
| Fatoma | 0 (0.0) | 35 (100.0) | 35 | |||
| Sévaré II | 136 (91.9) | 12 (8.1) | 148 | |||
| sub total | 215 (52.1) | 198 (47.9) | 413 | |||
| Tombouctou | Gourma Rharous | 400 (66.9) | 198 (33.1) | 598 | ||
| Gao | Gao | Csref d’Ansongo | 30 (13.4) | 194 (86.6) | 224 | |
| Menaka | Ménaka | Menaka | 21 (36.8) | 36 (63.2) | 57 | |
| Kidal | Kidal | Cscom d’Aliou | 0 (0.0) | 54 (100.0) | 54 | |
| CSRéf de Kidal | 20 (10.3) | 120 (85.7) | 140 | |||
| sub total | 20 (10.3) | 174 (89.7) | 194 | |||
| Total | 1002 (32.3) | 2096 (67.7) | 3098 | |||
3098 RDT cassettes were collected at the various study sites, of which 67.7 were malaria-negatives.
Table 3.
Distribution of plasmodial species as identified by qPCR according to research sites.
| Regions | P.f | P.v | P.m | P.o | Mixed Pf+P.m | Mixed Pf+P.v | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Kayes | 33 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 33 |
| Koulikoro | 28 | 100 | 0 | 0 | 1 | 3.57 | 0 | 0 | 1 | 3.57 | 0 | 0 | 28 |
| Sikasso | 30 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 30 |
| Ségou | 42 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 42 |
| Mopti | 33 | 97.05 | 0 | 0 | 1 | 2.90 | 0 | 0 | 0 | 0 | 0 | 0 | 34 |
| Tombouctou | 30 | 96.77 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 31 |
| Gao | 18 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 18 |
| Kidal | 22 | 95.65 | 1 | 4.34 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 4.34 | 23 |
| Ménaka | 15 | 79 | 4 | 21.05 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 19 |
| Total | 251 | 97.29 | 5 | 1.94 | 2 | 0.78 | 0 | 0 | 1 | 0.39 | 1 | 0.39 | 258 |
Table 4.
Diagnostic indices [95% confidence intervals], when compared to the qPCR gold standard, of the rapid diagnostic tests (RDT) used for the biological diagnosis of malaria in each administrative in region of Mali.
Table 4.
Diagnostic indices [95% confidence intervals], when compared to the qPCR gold standard, of the rapid diagnostic tests (RDT) used for the biological diagnosis of malaria in each administrative in region of Mali.
| Regions | Sensitivity (Se) | Specificity (Sp) | Youden Index | Kappa |
|---|---|---|---|---|
| Kayes | 87.9 % [76.9 - 90.7] | 99.3 % [96.9 - 100] | 0.87 [0.74 - 0.91] | 0.90 [0.77 - 0.94] |
| Koulikoro | 96.4 % [83.9- 99.8] | 98 % [95.7 - 98.6] | 0.95 [0.80 - 0.99] | 0.92 [0.77 - 0.96] |
| Sikasso | 83.3 % [69.2 - 92] | 95.1 % [90.9 -97.6] | 0.78 [0.60 - 0.90] | 0.78 [0.60 - 0.90] |
| Segou | 71.4 % [61.9- 73.7] | 98.9 % [94.4 - 99.9] | 0.70 [0.56 - 0.74] | 0.76 [0.60 - 0.79] |
| Mopti | 88.2 % [79 - 88] | 100 % [0.98 - 100] | 0.88 [0.76 - 0.88] | 0.92 [0.80 - 0.92] |
| Tombouctou | 85.3 % [74.4 - 88.1] | 99.3 % [96.8 - 100] | 0.85 [0.71 - 0.88] | 0.89 [0.75 - 0.92] |
| Gao | 94.7 % [74.6 - 99.7 | 92.5 % [90.2 - 93.1] | 0.87 [0.65 - 0.93] | 0.70 [0.52 - 0.74] |
| Kidal | 65.2 % [45.8 - 808] | 91.8 % [88.7 - 94] | 0.57 [0.35 - 0.75] | 0.53 [0.32 - 0.70] |
| Ménaka | 89.5 % [70.9 - 98] | 89.5 % [80.2 - 93.7] | 0.79 [0.51 - 0.92] | 0.77 [0.50 - 89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



