
Submitted:
24 November 2023
Posted:
27 November 2023
You are already at the latest version
Abstract
Dry eye syndrome (DES) has become increasingly prevalent due to the prolonged use of digital devices in modern society. Individual supplementation with lutein or docosahexaenoic acid (DHA) demonstrated potential benefits for eye health. This study aimed to investigate the effects of lutein plus DHA complex supplementation on DES, visual function, and memory in healthy individuals. Thirty-four participants, aged 40~60 years, received lutein/DHA complex supplements (containing 10 mg free-form lutein, 200 mg DHA, 30 mg red algae extract (astaxanthin), phosphatidylserine, and vitamin A) for 12 weeks. Ophthalmological examinations and memory tests were carried out, and a questionnaire was administered at weeks 0, 6, and 12 of the study. After 12 weeks of the intervention, the tear break-up time had significantly increased, and intraocular pressure (IOP) had significantly decreased. This suggests that lutein/DHA complex supplementation may reduce the IOP and offer potential benefits for DES, as indicated by improved tear stability.
Keywords:
lutein
; docosahexaenoic acid
; dry eye syndrome
; visual function
; memory function
1. Introduction
In modern society, people stare for long periods at digital devices, such as mobile phones, computers, and tablets, and stay in air-conditioned environments, which have led to an increase in the risk of dry eye syndrome (DES). DES is a common ophthalmological syndrome. According to the Asia Dry Eye Society, DES is a multifactorial disease characterized by an unstable tear film that causes a variety of symptoms and/or visual impairments, potentially accompanied by ocular surface damage[1]. DES is subdivided into two forms, aqueous-deficient (tear secretion deficiency) and hypervaporative (increased evaporation). However, mixed forms are also frequently observed. In addition, DES is usually accompanied by ocular symptoms, such as eye strain, heavy eyelids, itching eyes, thick eye discharges, a foreign-matter sensation in the eyes, and visual disturbances, resulting in a patient's decreased quality of life[2]. A previous study reported that the global prevalence of DES was 29.5%[3]. In Taiwan, a population-based cross-sectional survey showed that 33.7% of elderly were symptomatic, defined as frequently or always reporting one or more dry eye symptoms[4]. The incidence rate of DES in 2015 in Taiwan was 4.26%, and the incidence rates of DES generally increase with age[5]. Nowadays, a common method for treating DES is artificial tears, but this method can only temporarily relieve symptoms, and extended usage may lead to potential adverse effects such as elevated intraocular pressure (IOP), and the development of glaucoma and cataracts. Therefore, it is crucial to find effective alternative strategies to improve DES and prevent its worsening.
Lutein is one of the carotenoids which is present in the macula of the human retina. Many previous studies reported that lutein might have beneficial effects on visual performance, such as improving visual acuity or contrast sensitivity[6]. Moreover, lutein also protects the eyes against age-related macular degeneration, diabetic retinopathy, and cataracts due to its antioxidant and anti-inflammatory properties in the eye[7,8,9,10]. However, lutein supplementation alone appears to have little effect on improving DES. In addition, humans cannot synthesize lutein, and it must be obtained from the diet[11]. A previous study showed that the availability of lutein increased when consumed together with fat[12].
Docosahexaenoic acid (DHA) belongs to omega-3 long-chain polyunsaturated fatty acids (n-3 PUFAs) and is also an essential fatty acid. Humans cannot synthesize it, but it is very important for maintaining certain physiological functions and must be obtained from food. It is found in high amounts in the gray matter of the brain and in the outer rod segments of the retina[13]. Its main health benefits are anti-inflammation, increased cell membrane fluidity, and promotion of neuronal differentiation[14]. It is also one of the important nutrients associated with the development of the brain and eyes in infants[15]. Numerous studies demonstrated that supplementation with n-3 PUFAs enhances cognitive and memory functions[16,17]. Moreover, n-3 PUFAs are known to be effective in alleviating the signs and symptoms of DES[18,19].
Considering the evidence that lutein supplementation can protect the eyes and DHA can improve DES and memory function and to the best of our knowledge, the effects of lutein/DHA complex supplementation on DES, visual function, and memory function in healthy subjects are still unclear. Thus, in this study, we aimed to explore effects of the combination of lutein and DHA on dry eye-related indicators and symptoms, visual function, and memory function in healthy individuals.
2. Materials and Methods
2.1. Study Participants
In this single-arm clinical study, inclusion criteria were as follows: 40~60-year-old, healthy, male or female volunteers, who had subjective symptoms of dry eye or were frequent eye users. Exclusion criteria were defined as follows: pregnant, breastfeeding, having been treated or were taking medications, or had contingent infections, hypertension, diabetes, cerebrovascular disease, cardiovascular disease, liver disease, kidney disease, gastrointestinal disease, special ocular disease, or an allergy to products that contain the study components.
2.2. Trail Design
This study was conducted at Taipei Medical University Hospital (Taipei, Taiwan) and was approved by the Joint Institutional Review Board of Taipei Medical University (N202209063). In this study, all of the subjects provided written informed consent before participation. The study was conducted in accordance with principles of the Declaration of Helsinki. The duration of the study was 12 weeks. All subjects received two lutein/DHA complex supplements (soft gels) daily with water after dinner for 12 weeks. At the baseline, week 6, and week 12, ophthalmological examinations and a memory function test were performed, and a subjective symptom questionnaire was administered. In addition, participants were instructed to maintain their habitual diet, exercise routines, and sleep during the study. Compliance with lutein/DHA complex supplementation was assessed at the study visits by counting the soft gel supplements that were returned.
2.3. Test Supplement and Dosage
The lutein/DHA complex supplement was a product produced and supplied by Uni-President Enterprises (Tainan, Taiwan). Table 1 shows the composition of the lutein/DHA complex supplement, which included free-form lutein, DHA, astaxanthin, phosphatidylserine (PS), and vitamin A.
2.4. Dry Eye Syndrome (DES)
Several methods were used to assess DES, including the tear break-up time (TBUT) and a strip meniscometry test. The TBUT was used to assess the stability of the tears, and the strip meniscometry test was used to measure tear secretions. To determine whether lutein/DHA complex supplementation could attenuate DES, the TBUT and strip meniscometry test were conducted. All data associated with the eyes are presented as the average of both eyes.
2.4.1. Tear Break-Up Time (TBUT)
The TBUT was mainly used to observe the stability of the tear film. After fluorescein dye was instilled into the eyes of a subject, the subject was asked to blink a few times to ensure adequate mixing of the fluorescein dye and then to stop blinking. The time between the last blink and the appearance of the first black spot was measured with a slit lamp. A value of the TBUT below 10 seconds indicated tear instability.
2.4.2. Strip Meniscometry Test
The strip meniscometry test (Echo Electricity, Fukushima, Japan) was used to evaluate tear secretions. After topical anesthesia was applied, calibrated filter paper strips were placed in the lower eyelid for 5 seconds, and readings were measured in millimeters (mm) of the wet strip after 5 seconds. Values of less than 5 mm indicated insufficient tear secretion.
2.5. Visual Function
At each visit, subjects underwent a complete ophthalmologic examination to assess the visual function, including corrected visual acuity, contrast sensitivity, IOP, and central macular thickness. All data associated with the eyes are presented as the average of both eyes.
Corrected visual acuity and IOP were measured using an Auto Ref/Kerato/Tono/Pachymeter TONOREF™ III (Nidek, Gamagori, Japan). Contrast sensitivity (%) indicates an individual’s ability to distinguish an object’s lightness or darkness compared to the background in a picture with different levels of contrast changes (Figure 1). The central macular thickness was measured using optical coherence tomography (OCT) (Heidelberg Engineering, Heidelberg, Germany). OCT is a noninvasive imaging technique and was established to measure and assess structural parameters within the eye bulbus, such as the macular thickness.
2.7. Questionnaire of Subjective Symptoms associated with Ocular Comfort
Items of the subjective symptom questionnaire included eye strain, heavy eyelids, eye dryness, itching eyes, thick eye discharges, swollen eyes, sore eyes, foreign-matter sensation in the eyes, photophobia, blurred vision, blurred vision at night, and the eyes tearing involuntarily. The questionnaire consisted of 12 questions. Possible answers to the questions as to the frequency of symptoms within a 1-week recall period were “never", "rarely", "sometimes", "often", and "everyday”. Each frequency was assigned a score from 4 to 0. Possible answers to the questions as to the severity of symptoms within a 1-week recall period were “never", "mild", "moderate", and "severe”. Each severity level was assigned a score from 3 to 0. Scores for the frequency and severity of each symptom were summed to give a total score for that symptom. In addition, the total score of each subjective symptom represented the score of eye fatigue and dry eye-related symptoms. A higher summary score indicated less eye fatigue and fewer dry eye-related symptoms.
2.8. Memory Function
We used a paired association test to evaluate memory function, which included six black and white portraits. Each portrait was presented for 9 seconds in a random order, with a 2-second interval. Simultaneously, a test subject was provided with information about the name, occupation, and hobbies of the individuals depicted in the images. This information was repeated twice, and the participants were asked to remember the associations between the portraits and the provided details. Subsequently, the same images were presented in a different order, and the participants were required to immediately recall the names, occupations, and hobbies of the individuals in each portrait. A total of 30 seconds were allowed for each portrait's recall. Each correct name was worth 2 points, and each correct occupation or hobby was worth 1 point, with a total score calculated by summing these three categories (maximum score of 24 points).
2.9. Statisical Analysis
Data are presented as the mean ± standard deviation (SD) and were analyzed by GraphPad Prism vers. 8.0 software (GraphPad Software, San Diego, CA, USA). During the intervention period, differences among weeks 0, 4, and 8 were compared using a repeated-measures one-way analysis of variance (ANOVA), followed by Tukey's test. Statistical significance was accepted at p < 0.05.
3. Results
3.1. Subject Characteristics and Participation
A flow diagram is given in Figure 2, and baseline characteristics of participants in this study are shown in Table 2. In total, 34 participants were initially enrolled in the study at the baseline, including 17 males and 17 females. During the experimental period, five subjects dropped out without completing the experiment, and the remaining 29 participants completed the experiment (Figure 2). Compliance over the 12-week supplementation period was 98.6% ± 2.08% for the 29 participants who completed the study.
3.2. Effects of Lutein/DHA Complex Supplementation on DES in Healthy Subjects
As shown in Figure 3a, after 6 weeks of the intervention, no difference was found in the TBUT between weeks 0 and 6. However, after 12 weeks of the intervention, the TBUT had significantly increased by week 12, compared to weeks 0 and 6 (week 0: 4.66 ± 1.63 s; week 6: 4.84 ± 1.35 s; week 12: 5.26 ± 1.33 s). As shown in Figure 3b, after 6 and 12 weeks of the lutein/DHA complex supplementation intervention, there were no significant differences in the strip meniscometry test in healthy subjects (week 0: 2.52 ± 0.76 mm; week 6: 2.48 ± 0.69 mm; week 12: 2.38 ± 0.44 mm).
3.3. Effects of Lutein/DHA Complex Supplementation on Visual Function in Healthy Subjects
After 6 and 12 weeks of the intervention, no changes were seen in corrected visual acuity (week 0: 0.94 ± 0.12; week 6: 0.94 ± 0.08; week 12: 0.95 ± 0.07), contrast sensitivity (week 0: 2.76% ± 0.97%; week 6: 2.50% ± 0%; week 12: 2.59% ± 0.32%), or central macular thickness (week 0: 261.79 ± 14.89 µm; week 6: 265.07 ± 16.33 µm; week 12: 263.43 ± 14.82 µm) in healthy subjects between different time points (Figure 4a,b,d). However, compared to week 0, the IOP was significantly lower in both weeks 6 and 12 (week 0: 15.56 ± 2.10 mmHg; week 6: 14.78 ± 2.33 mmHg; week 12: 15.00 ± 2.29 mmHg) (Figure 4c).
3.4. Effects of Lutein/DHA Complex Supplementation on Subjective Symptoms Associated with Dry Eyes and Eye Fatigue in Healthy Subjects as Assessed by a Questionnaire
As shown in Table 3, after the intervention period, significant differences were not observed in any items of the subjective symptom questionnaire between different time points. In addition, there were no significant differences in summary scores of subjective symptoms associated dryness of the eyes or eye fatigue.
3.5. Effects of Lutein/DHA Complex Supplementation on Memory Function in Healthy Subjects
As shown in Figure 5, compared to week 0, scores of the memory function test had significantly increased by week 6 by 1.26-fold (126%). However, compared to week 0, only an increasing trend was shown in week 12, with an increase of 1.06-fold (106%).
4. Discussion
In this prospective, one-group, pretest-posttest clinical study, results indicated that after a 12-week intervention with lutein/DHA complex supplementation, there was a significant increase in the TBUT. However, there were no significant differences in the strip meniscometry test. These results suggested that while lutein/DHA complex supplementation might not increase tear secretion, it could enhance tear film stability and reduce tear film evaporation, thus improving DES. Taking lutein alone seemed to have little effect on improving DES, but previous studies found that some nutrients and antioxidants, including DHA and astaxanthin, were related to the alleviation of DES. Previous studies indicated that the pathogenesis of dry eye disease was associated with an imbalance in tear film stability which was accompanied by elevated levels of proinflammatory cytokines, such as interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)-α[20,21]. However, DHA is one of the n-3 PUFAs. Supplementation with n-3 PUFAs inhibits the production of the precursor to inflammatory mediators, arachidonic acid (AA). It also promotes the generation of anti-inflammatory substances like resolvins and protectins, and inhibits the production of IL-1 and TNF-α, thereby exerting an anti-inflammatory effect, including on the surface of the eye[22]. In addition to regulating the inflammatory response on the eye surface, n-3 PUFAs can also improve meibomian gland dysfunction. The meibomian glands are responsible for secreting the lipid components of tears, and the lipid content in tears is associated with tear stability, which can help prevent rapid tear evaporation. Li et al. found that the inflammatory response in the corneal stroma was reduced in a dry eye mouse model with the DHA-derived molecule, resolvin E1. Simultaneously, the density of surface epithelial cells returned to a level comparable to the control group, thereby improving corneal epithelial integrity[23]. Bhargava et al. showed that after supplementation with n-3 PUFA capsules (650 mg/day eicosapentaenoic acid (EPA) and 250 mg/day DHA) for 3 months, dry eye-related subjective symptom scores and the TBUT in DES patients significantly increased. In other words, n-3 PUFAs can improve subjective symptoms of DES and also improve objective clinical indicators of DES[24]. In addition, the supplement in our study contained red algae extract (containing astaxanthin), which is also a potential treatment for DES. Previous studies showed that astaxanthin can increase retinal capillary blood circulation, regulate ciliary muscle contractions, and improve eye comfort. Another study found that supplementation with 12 mg of astaxanthin for 30 days in mild to moderate DES patients caused the tear film break-up time to increase, the blink frequency to significantly decrease, and the ocular surface disease index (OSDI) questionnaire to improve. Therefore, we speculated that an intervention with supplements in this experiment could improve DES, which may have been related to DHA and astaxanthin [25].
In this experiment, participants were given 10 mg of free-form lutein and 200 mg of DHA for 12 weeks. Results indicated that there was no impact on the best-corrected visual acuity or contrast sensitivity in healthy individuals aged 40 to 60 years. In a previous study, compared to a placebo group, there was no significant difference in visual acuity or contrast sensitivity in healthy adults (18~40 years old) with 12 mg lutein and 1 mg zeaxanthin for 12 months[26]. Another study observed no changes in the best-corrected visual acuity in a healthy Mediterranean population supplemented with 6 mg of lutein plus 700 mg of DHA for 3 months[27]. A meta-analysis of supplementation with lutein and/or zeaxanthin in patients with age-related macular degeneration (AMD) for 6 months to 3 years showed improved visual acuity and contrast sensitivity after supplementation; that study mentioned that impacts of short-term experiments on improving visual function were not significant. It was observed that supplementation with lutein had a positive effect on visual function only after at least 6 months of an intervention [28]. While Liu et al.'s study did not focus on healthy individuals, further research can still explore longer intervention periods to verify the relationship between lutein/DHA and visual function. Furthermore, results of this experiment showed that most healthy participants had an optimal level of contrast sensitivity of 2.5%, and their vision was also normal. Therefore, the degree of improvement in contrast sensitivity and visual function was relatively minor.
IOP is crucial for eye health and function. Numerous factors can influence IOP, including systemic blood pressure and ischemia of the retinal nerve fiber layer, among others, which can lead to an increase in IOP. Ischemic tissue damage can result in a sudden decrease in IOP. Prolonged, chronically high IOP is associated with a higher probability of damaging retinal ganglion cells, causing structural abnormalities, chronic degeneration of the optic nerve, visual field loss, a reduction in the range of vision, and ultimately a significantly increased risk of developing glaucoma. Severe glaucoma can lead to irreversible and permanent blindness. High IOP is considered a modifiable risk factor for glaucoma, and early treatment was proven to have protective benefits for preserving vision. Therefore, reducing the IOP to prevent the onset of glaucoma is considered critically important[29,30]. In this study, the IOP was significantly decreased in healthy subjects with lutein/DHA complex supplementation for 12 weeks. Although IOP levels of participants in this study were within a normal range, lowering the IOP can prevent glaucoma. Currently, there is little research on the effect of lutein supplementation alone on IOP, but results show that it is less effective. However, previous studies suggested that DHA or astaxanthin might be associated with improvements in the IOP. Astaxanthin is a natural carotenoid. Previous studies suggested that astaxanthin might have the potential to reduce the IOP, which was attributed to its potent antioxidant capacity[31]. It can alleviate protein oxidation, lipid peroxidation, and apoptosis caused by elevated IOP, thereby inhibiting apoptosis of retinal ganglion cells and protecting the retinal integrity from damage due to high IOP[32]. DHA also appears to have potential protective effects. Another study indicated that DHA supplementation suppressed plasma malondialdehyde (MDA) and IL-6 levels, thus inhibiting oxidative and inflammatory responses, leading to a significant reduction in the IOP in patients with glaucoma[33]. However, the effects of DHA or astaxanthin on IOP in healthy individuals remain unclear, requiring further research to confirm their efficacy. Nevertheless, we speculated that the reduction in IOP observed in this experiment might have been related to the presence of DHA and astaxanthin in the formulation.
DHA accumulates in substantial amounts in both the retina and brain, playing crucial roles in cognitive abilities, which include neuronal cell growth, differentiation, signal transmission, and memory[34]. In our present study, we observed that after 6 weeks of the intervention, the memory function was significantly enhanced in healthy subjects. After 12 weeks of the intervention, the memory function showed an upward trend, although the differences did not reach statistical significance. These findings were inconsistent with the study by Stonehouse et al., in which a high-dose (1.16 g) DHA intervention for 6 months improved memory in healthy adults. A possible reason for our different results could be the use of a smaller dose or a relatively shorter intervention duration. It is possible that more than 6 months might be needed to achieve measurable effects on cognitive function in adults. [35]. As a result, by increasing the dosage of lutein/DHA complex supplementation or the intervention time, one might be able to observe more-significant effects of lutein/DHA complex supplementation on memory function.
This study had some limitations. It was a single-group, pre-post clinical experiment, which overlooked the placebo effect. However, as it remains unclear whether the combination of lutein and DHA justifies resource investment, this study opted for a simpler design to assess the efficacy of lutein/DHA complex supplementation. In the future, double-blind, randomized clinical trials with a placebo group, lutein supplementation group, DHA supplementation group, and lutein/DHA complex supplementation group are necessary to ascertain the effectiveness of lutein/DHA complex supplementation on DES, visual function, and memory function.
5. Conclusions
Lutein/DHA complex supplementation enhanced tear stability and reduced the IOP in healthy subjects with subjective dry eye symptoms. Consequently, lutein/DHA complex supplementation may be a beneficial strategy for alleviating eye dryness and increasing eye comfort in healthy individuals.
Author Contributions
Conceptualization, Y.-W.C.; Methodology, L.-W.H., E.J.-C.H., and Y.-W.C.; Formal analysis, L.-W.H.; Investigation, L.-W.H., E.J.-C.H., and Y.-W.C.; writing—original draft preparation, L.-W.H., and Y.-W.C.; writing—review and editing, L.-W.H. and Y.-W.C.; All authors read and agreed to the published version of the manuscript.
Funding
This research was supported by Uni-President Enterprises Corp. (Tainan, Taiwan).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Board of Taipei Medical University in Taiwan (protocol code N202209063 and date of approval: 2022 October 5).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Uni-President Enterprises Corp. (Tainan, Taiwan) for producing and supplying the products we used in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tsubota, K.; Yokoi, N.; Watanabe, H.; Dogru, M.; Kojima, T.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y., et al. A New Perspective on Dry Eye Classification: Proposal by the Asia Dry Eye Society. Eye Contact Lens 2020, 46 Suppl 1, S2-s13. [CrossRef]
- Messmer, E.M. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int 2015, 112, 71-81; quiz 82. [CrossRef]
- Papas, E.B. The global prevalence of dry eye disease: A Bayesian view. Ophthalmic Physiol Opt 2021, 41, 1254-1266. [CrossRef]
- Lin, P.Y.; Tsai, S.Y.; Cheng, C.Y.; Liu, J.H.; Chou, P.; Hsu, W.M. Prevalence of dry eye among an elderly Chinese population in Taiwan: the Shihpai Eye Study. Ophthalmology 2003, 110, 1096-1101. [CrossRef]
- Kuo, Y.K.; Lin, I.C.; Chien, L.N.; Lin, T.Y.; How, Y.T.; Chen, K.H.; Dusting, G.J.; Tseng, C.L. Dry Eye Disease: A Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits. J Clin Med 2019, 8. [CrossRef]
- Mares, J. Lutein and Zeaxanthin Isomers in Eye Health and Disease. Annu Rev Nutr 2016, 36, 571-602. [CrossRef]
- Mrowicka, M.; Mrowicki, J.; Kucharska, E.; Majsterek, I. Lutein and Zeaxanthin and Their Roles in Age-Related Macular Degeneration-Neurodegenerative Disease. Nutrients 2022, 14. [CrossRef]
- Eisenhauer, B.; Natoli, S.; Liew, G.; Flood, V.M. Lutein and Zeaxanthin-Food Sources, Bioavailability and Dietary Variety in Age-Related Macular Degeneration Protection. Nutrients 2017, 9. [CrossRef]
- Neelam, K.; Goenadi, C.J.; Lun, K.; Yip, C.C.; Au Eong, K.G. Putative protective role of lutein and zeaxanthin in diabetic retinopathy. Br J Ophthalmol 2017, 101, 551-558. [CrossRef]
- Manayi, A.; Abdollahi, M.; Raman, T.; Nabavi, S.F.; Habtemariam, S.; Daglia, M.; Nabavi, S.M. Lutein and cataract: from bench to bedside. Crit Rev Biotechnol 2016, 36, 829-839. [CrossRef]
- Al-Ahmary, K.M. The carotenoids of some food stuffs in Saudi Arabia. Int J Food Sci Nutr 2010, 61, 823-828. [CrossRef]
- Nagao, A. Absorption and metabolism of dietary carotenoids. Biofactors 2011, 37, 83-87. [CrossRef]
- Li, J.; Pora, B.L.R.; Dong, K.; Hasjim, J. Health benefits of docosahexaenoic acid and its bioavailability: A review. Food Sci Nutr 2021, 9, 5229-5243. [CrossRef]
- Swanson, D.; Block, R.; Mousa, S.A. Omega-3 fatty acids EPA and DHA: health benefits throughout life. Adv Nutr 2012, 3, 1-7. [CrossRef]
- Carver, J.D.; Benford, V.J.; Han, B.; Cantor, A.B. The relationship between age and the fatty acid composition of cerebral cortex and erythrocytes in human subjects. Brain Res Bull 2001, 56, 79-85. [CrossRef]
- Dighriri, I.M.; Alsubaie, A.M.; Hakami, F.M.; Hamithi, D.M.; Alshekh, M.M.; Khobrani, F.A.; Dalak, F.E.; Hakami, A.A.; Alsueaadi, E.H.; Alsaawi, L.S., et al. Effects of Omega-3 Polyunsaturated Fatty Acids on Brain Functions: A Systematic Review. Cureus 2022, 14, e30091. [CrossRef]
- Bauer, I.; Hughes, M.; Rowsell, R.; Cockerell, R.; Pipingas, A.; Crewther, S.; Crewther, D. Omega-3 supplementation improves cognition and modifies brain activation in young adults. Hum Psychopharmacol 2014, 29, 133-144. [CrossRef]
- Giannaccare, G.; Pellegrini, M.; Sebastiani, S.; Bernabei, F.; Roda, M.; Taroni, L.; Versura, P.; Campos, E.C. Efficacy of Omega-3 Fatty Acid Supplementation for Treatment of Dry Eye Disease: A Meta-Analysis of Randomized Clinical Trials. Cornea 2019, 38, 565-573. [CrossRef]
- Chi, S.C.; Tuan, H.I.; Kang, Y.N. Effects of Polyunsaturated Fatty Acids on Nonspecific Typical Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients 2019, 11. [CrossRef]
- Jackson, D.C.; Zeng, W.; Wong, C.Y.; Mifsud, E.J.; Williamson, N.A.; Ang, C.S.; Vingrys, A.J.; Downie, L.E. Tear Interferon-Gamma as a Biomarker for Evaporative Dry Eye Disease. Invest Ophthalmol Vis Sci 2016, 57, 4824-4830. [CrossRef]
- Massingale, M.L.; Li, X.; Vallabhajosyula, M.; Chen, D.; Wei, Y.; Asbell, P.A. Analysis of inflammatory cytokines in the tears of dry eye patients. Cornea 2009, 28, 1023-1027. [CrossRef]
- Simopoulos, A.P. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother 2002, 56, 365-379. [CrossRef]
- Li, N.; He, J.; Schwartz, C.E.; Gjorstrup, P.; Bazan, H.E. Resolvin E1 improves tear production and decreases inflammation in a dry eye mouse model. J Ocul Pharmacol Ther 2010, 26, 431-439. [CrossRef]
- Downie, L.E.; Ng, S.M.; Lindsley, K.B.; Akpek, E.K. Omega-3 and omega-6 polyunsaturated fatty acids for dry eye disease. Cochrane Database Syst Rev 2019, 12, Cd011016. [CrossRef]
- Tian, L.; Wen, Y.; Li, S.; Zhang, P.; Wang, Y.; Wang, J.; Cao, K.; Du, L.; Wang, N.; Jie, Y. Benefits and Safety of Astaxanthin in the Treatment of Mild-To-Moderate Dry Eye Disease. Front Nutr 2021, 8, 796951. [CrossRef]
- Nolan, J.M.; Loughman, J.; Akkali, M.C.; Stack, J.; Scanlon, G.; Davison, P.; Beatty, S. The impact of macular pigment augmentation on visual performance in normal subjects: COMPASS. Vision Res 2011, 51, 459-469. [CrossRef]
- Zanón-Moreno, V.; Domingo Pedrol, J.C.; Sanz-González, S.M.; Raga-Cervera, J.; Salazar-Corral, J.; Pinazo-Durán, M.D. Feasibility Study of a Docosahexaenoic Acid-Optimized Nutraceutical Formulation on the Macular Levels of Lutein in a Healthy Mediterranean Population. Ophthalmic Res 2021, 64, 1068-1076. [CrossRef]
- Liu, R.; Wang, T.; Zhang, B.; Qin, L.; Wu, C.; Li, Q.; Ma, L. Lutein and zeaxanthin supplementation and association with visual function in age-related macular degeneration. Invest Ophthalmol Vis Sci 2014, 56, 252-258. [CrossRef]
- Dietze, J.; Blair, K.; Havens, S.J. Glaucoma. In StatPearls, StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL), 2022.
- Machiele, R.; Motlagh, M.; Patel, B.C. Intraocular Pressure. In StatPearls, StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL), 2022.
- Yang, M.; Wang, Y. Recent Advances and the Mechanism of Astaxanthin in Ophthalmological Diseases. J Ophthalmol 2022, 2022, 8071406. [CrossRef]
- Cort, A.; Ozturk, N.; Akpinar, D.; Unal, M.; Yucel, G.; Ciftcioglu, A.; Yargicoglu, P.; Aslan, M. Suppressive effect of astaxanthin on retinal injury induced by elevated intraocular pressure. Regul Toxicol Pharmacol 2010, 58, 121-130. [CrossRef]
- Romeo Villadóniga, S.; Rodríguez García, E.; Sagastagoia Epelde, O.; Álvarez Díaz, M.D.; Domingo Pedrol, J.C. Effects of Oral Supplementation with Docosahexaenoic Acid (DHA) plus Antioxidants in Pseudoexfoliative Glaucoma: A 6-Month Open-Label Randomized Trial. J Ophthalmol 2018, 2018, 8259371. [CrossRef]
- Lauritzen, L.; Brambilla, P.; Mazzocchi, A.; Harsløf, L.B.; Ciappolino, V.; Agostoni, C. DHA Effects in Brain Development and Function. Nutrients 2016, 8. [CrossRef]
- Stonehouse, W.; Conlon, C.A.; Podd, J.; Hill, S.R.; Minihane, A.M.; Haskell, C.; Kennedy, D. DHA supplementation improved both memory and reaction time in healthy young adults: a randomized controlled trial. Am J Clin Nutr 2013, 97, 1134-1143. [CrossRef]
Figure 1.
Contrast sensitivity test picture.
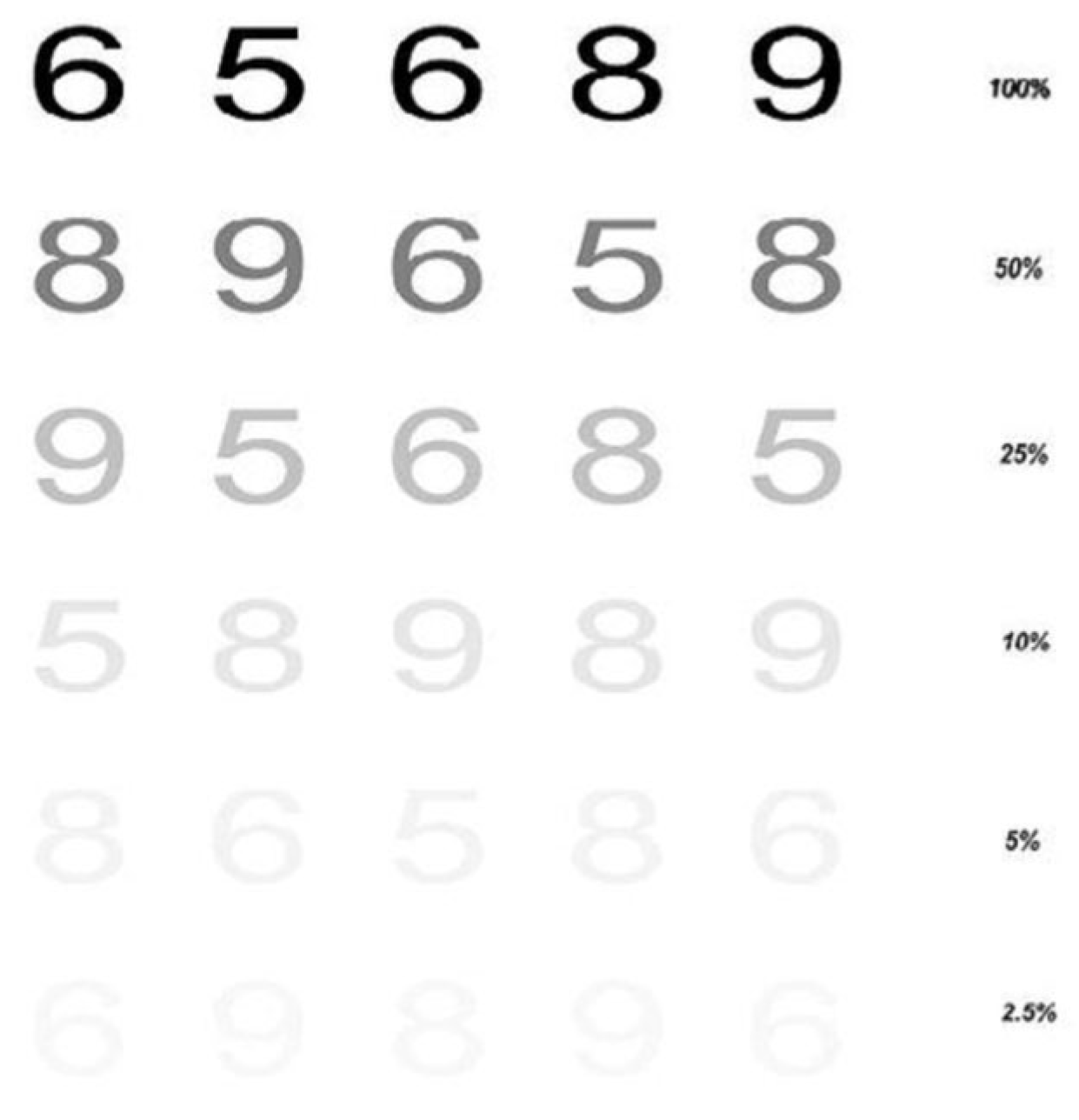
Figure 2.
Participant enrollment.
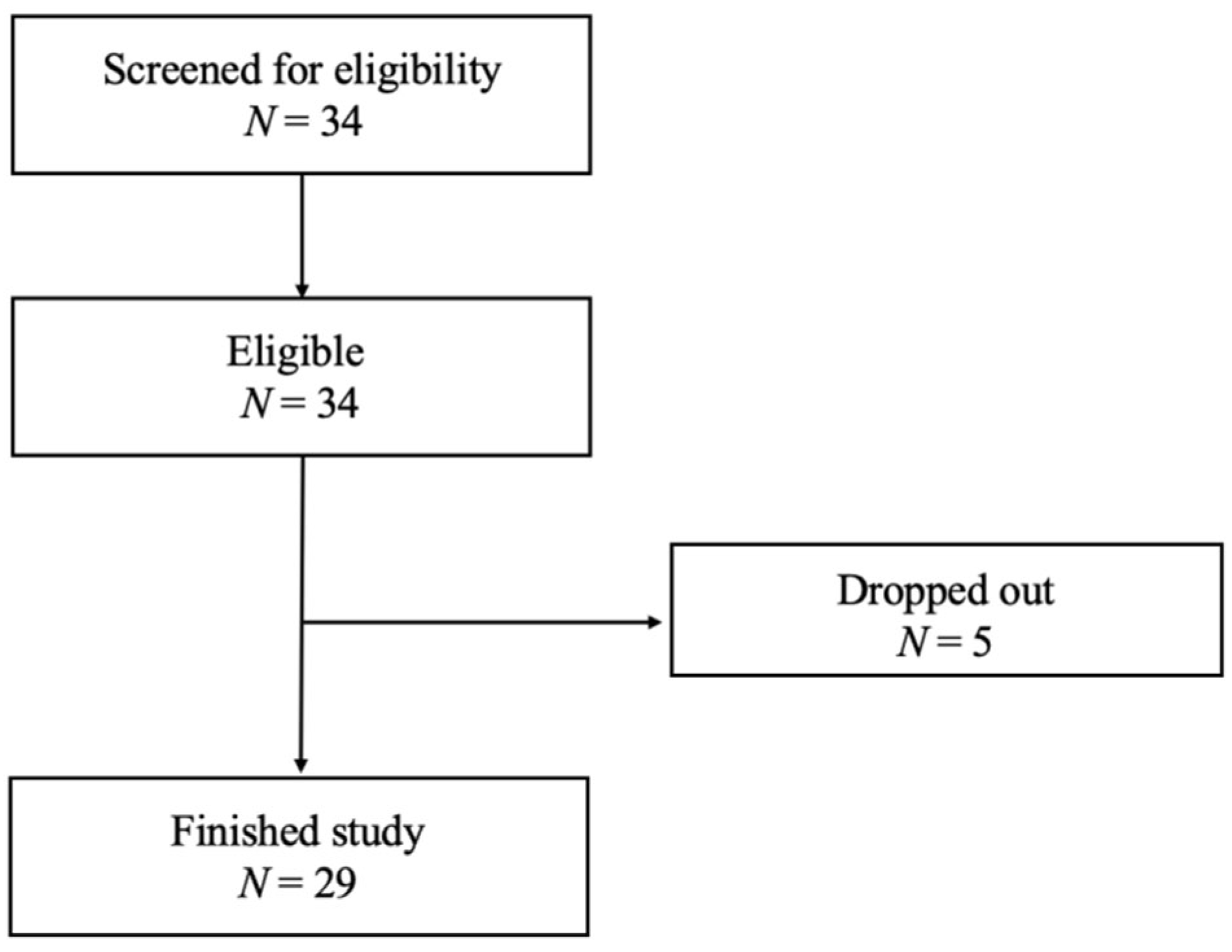
Figure 3.
Effects of lutein/DHA complex supplementation on (a) the tear break-up time (TBUT) and (b) strip meniscometry test in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
Figure 3.
Effects of lutein/DHA complex supplementation on (a) the tear break-up time (TBUT) and (b) strip meniscometry test in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
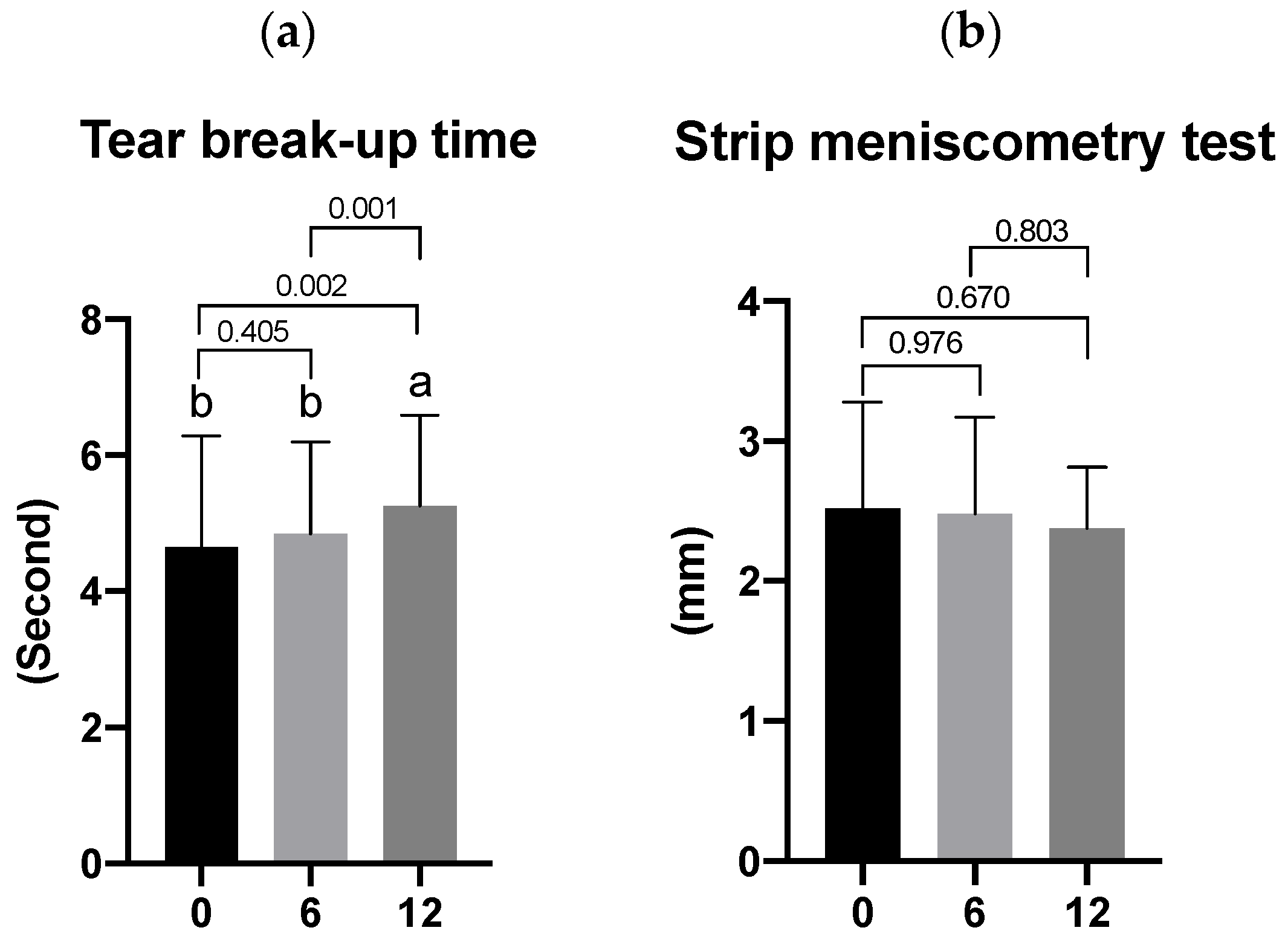
Figure 4.
Effects of lutein/DHA complex supplementation on (a) corrected visual acuity, (b) contrast sensitivity, (c) intraocular pressure (IOP), and (d) central macular thickness in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
Figure 4.
Effects of lutein/DHA complex supplementation on (a) corrected visual acuity, (b) contrast sensitivity, (c) intraocular pressure (IOP), and (d) central macular thickness in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
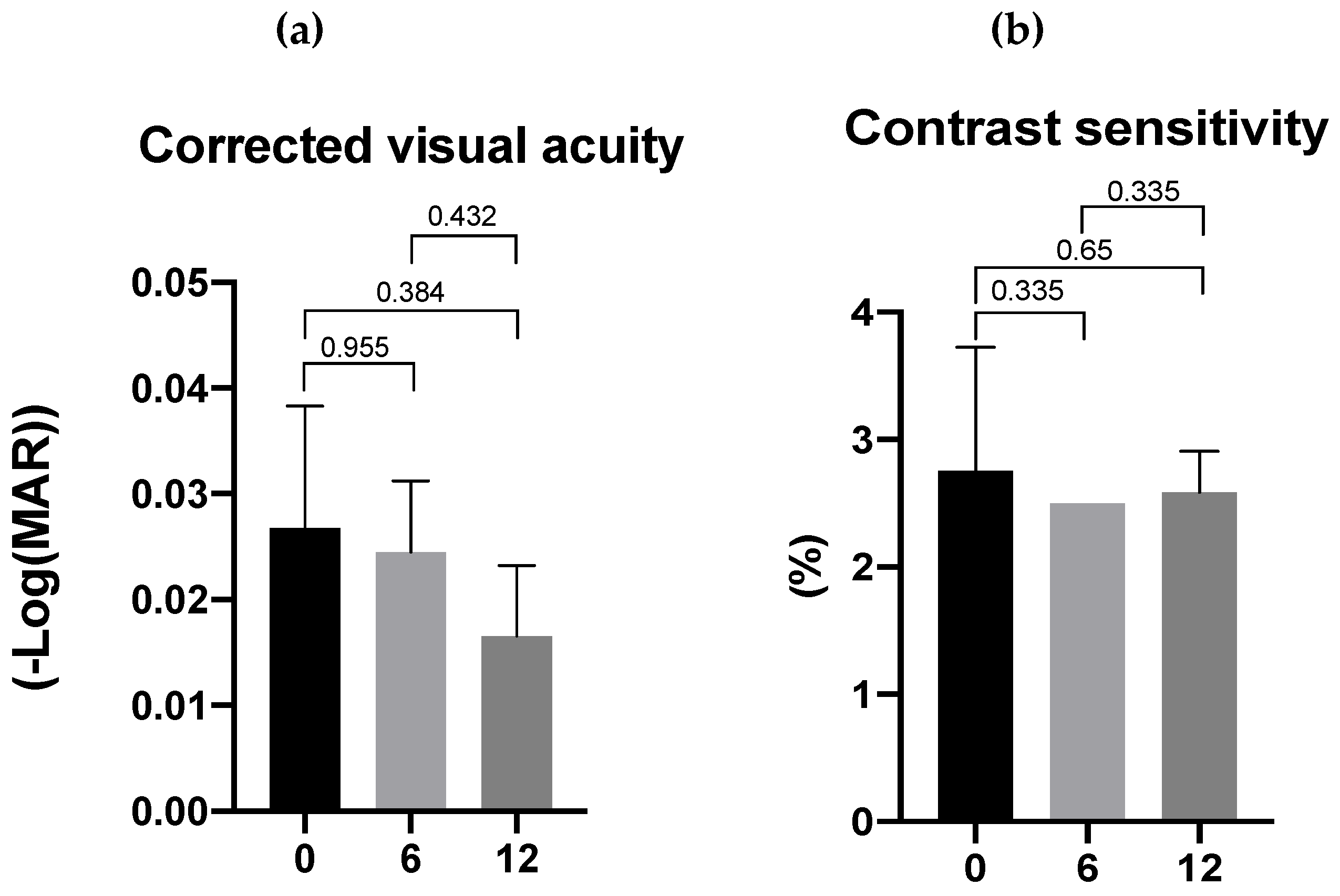
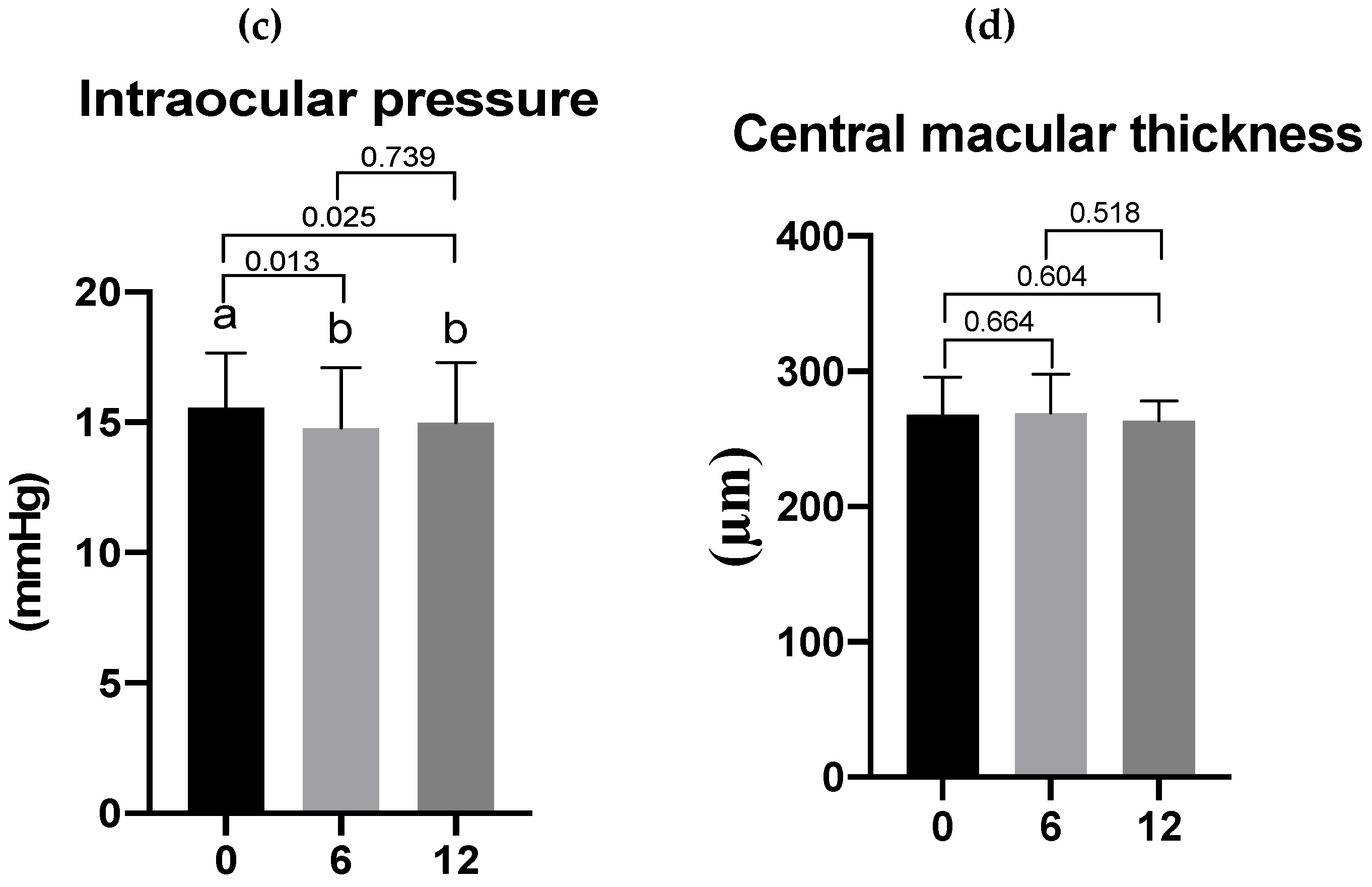
Figure 5.
Effects of lutein/DHA complex supplementation on memory function in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
Figure 5.
Effects of lutein/DHA complex supplementation on memory function in healthy subjects. All values are presented as the mean ± standard deviation (N=29). Different letters indicate a significant difference between different time points at p < 0.05 by a repeated-measures one-way ANOVA with Tukey's test.
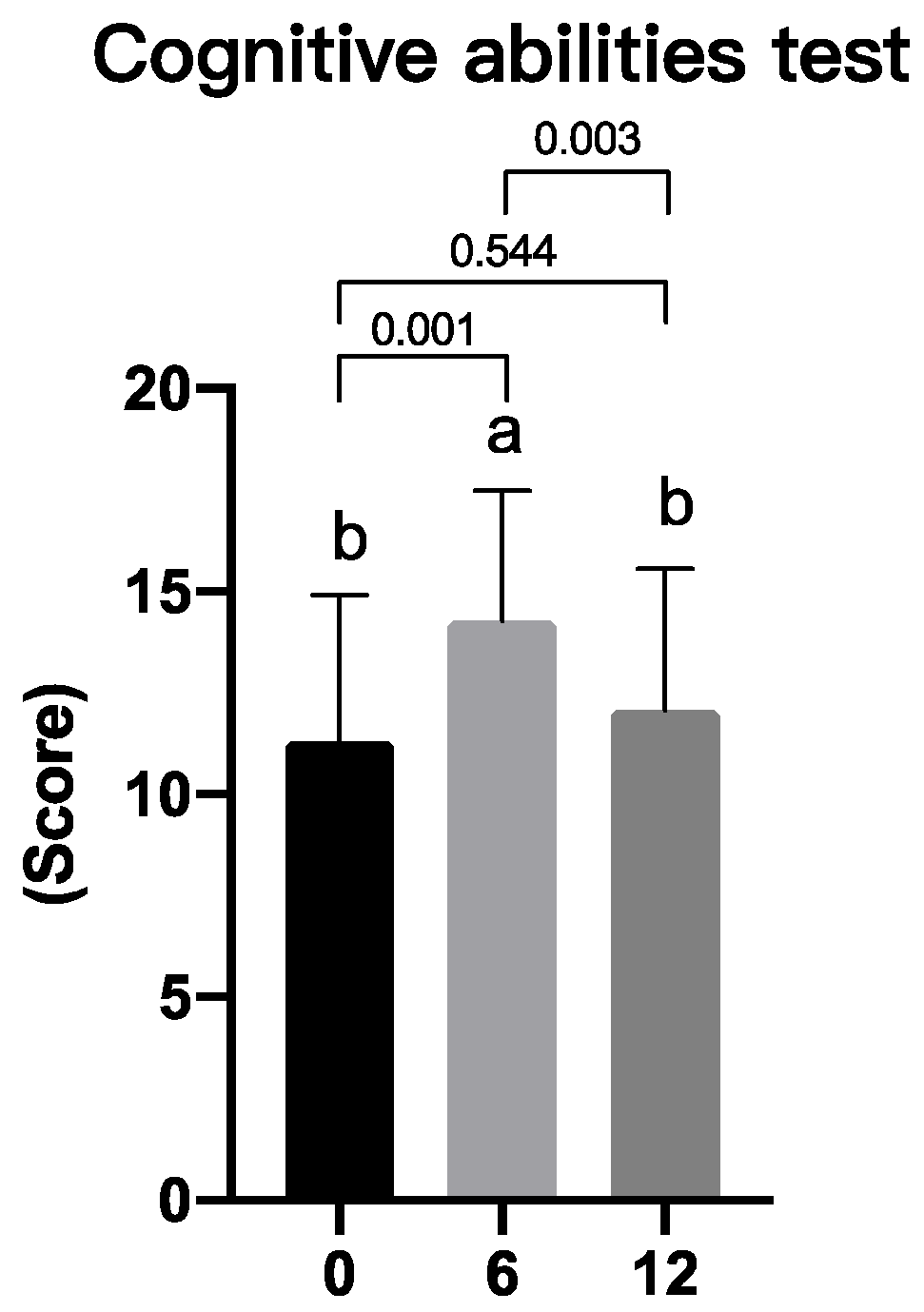

Table 1.
Ingredient list of the lutein/DHA complex supplement
| Ingredient | Amount per serving | Daily intake (2 servings) |
|---|---|---|
| Free-form lutein | 5 mg | 10 mg |
| Docosahexaenoic acid (DHA) | 100 mg | 200 mg |
| Red algae extract (astaxanthin) | 15 mg | 30 mg |
| Phosphatidylserine (PS) | 25 mg | 50 mg |
| Vitamin A | 70 μg RE | 140 μg RE |
RE, retinol equivalent.
Table 2.
Characteristics of enrolled subjects.
| All subjects (N=29) | |
|---|---|
| Male | 14 |
| Female | 15 |
| Age (years) | |
| 40~50 | 15 |
| 51~60 | 14 |
| Average age of subjects (years) | 50.03 ± 4.77 |
Average age is presented as the mean ± standard deviation (N = 29).
Table 3.
Effects of lutein/DHA complex supplementation on subjective symptoms associated with dryness of the eyes and eye fatigue in healthy subjects as assessed by a questionnaire.
Table 3.
Effects of lutein/DHA complex supplementation on subjective symptoms associated with dryness of the eyes and eye fatigue in healthy subjects as assessed by a questionnaire.
| Subjective symptoms associated with ocular comfort (score) | Week 0 | Week 6 | Week 12 |
|---|---|---|---|
| Eye strain | 4.59 ± 1.84 | 4.93 ± 1.65 | 5.14 ± 1.83 |
| Heavy eyelids | 6.17 ± 1.67 | 5.90 ± 1.47 | 6.07 ± 1.60 |
| Eye dryness | 5.28 ± 1.83 | 5.24 ± 2.05 | 5.34 ± 1.93 |
| Itching eyes | 5.59 ± 1.64 | 5.76 ± 1.38 | 5.97 ± 1.57 |
| Thick eye discharges | 5.97 ± 1.57 | 5.72 ± 1.69 | 5.86 ± 1.71 |
| Foreign-matter sensation in the eyes | 5.79 ± 1.72 | 5.76 ± 1.55 | 5.83± 2.00 |
| Photophobia | 6.17 ± 1.49 | 5.93 ± 1.58 | 5.86 ± 1.75 |
| Blurred vision | 4.45 ± 1.80 | 4.76 ± 1.77 | 4.86 ± 1.79 |
| Swollen eyes | 6.34 ± 1.56 | 6.21 ± 1.50 | 6.38 ± 1.50 |
| Sore eyes | 5.76 ± 1.48 | 6.00 ± 1.65 | 5.66 ± 1.91 |
| Eyes tearing involuntarily | 6.03 ± 1.43 | 6.17 ± 1.39 | 5.86 ± 1.57 |
| Blurred vision at night | 4.83 ± 2.00 | 5.17 ± 2.22 | 5.14 ± 1.81 |
| Summary score | 66.97± 14.27 | 67.55± 14.92 | 67.97± 16.33 |
All values are presented as the mean ± standard deviation (N=29). Differences between time points were determined by a repeated-measures one-way ANOVA with Tukey's test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



