
Submitted:
30 November 2023
Posted:
01 December 2023
You are already at the latest version
Abstract
Abstract: The pursuit of youth and attractiveness is a fundamental desire in contemporary society. For many individuals, the appearance of visible signs of aging, such as skin laxity, gravitational changes in facial and neck soft tissues, and loss of harmonious proportions, can be psychologically distressing. The choice of effective methods for addressing these changes depends on their specific characteristics, the patient's anatomical features, and the type of facial aging. The introduction of 3D imaging to determine the hyoid bone level, the volume of soft tissue structures in the cervico-mental area, ptosis of subplatysmal structures, and the volume of submandibular glands, in addition to ultrasound study of the submental projection at the preoperative stage, are key for taking the best decision regarding preoperative planning. This case report aims to illustrate how modern imaging techniques are a fundamental part of the preoperative assessment of the mid and lower third of the face to ensure the most favorable aesthetic outcomes for each patient. Key message: To attain harmonious results in surgical correction of age-related facial and neck changes, it is crucial to consider the patient's anatomical features and the extent of age-related alterations. A comprehensive facial analysis, taking into account the type of facial aging and employing a CT scan and ultrasound examination of the soft tissues in the chin region, facilitates the development of an individualized plan tailored to achieve the patient's desired outcome.
Keywords:
platysmaplasty
; facial rejuvenation
; subplatysmal structures
; myotomy
; neck lift
; tomography
1. Introduction
Over the past decades, numerous techniques have emerged for correcting the contours of the lower third of the face [1]. Modern patients are well-informed about the capabilities of plastic surgery and demonstrate an increased interest in rejuvenation methods. According to statistics in our practice, approximately 400 patients seek facial rejuvenation at our clinic annually, including the cervico-mental area, with about 20% of them being over 60 years old.
The term "age-related changes in the lower third of the face" commonly refers to the deepening of perioral wrinkles, "marionette lines", sagging of the cervico-mental region, and the apparition of jowls, secondary to the redistribution of the fat in the neck, leading to the formation of an obtuse cervical-mandibular angle, that is very frequent in elderly [2]. The Aging manifests as ptosis, skin laxity in the anterior neck region, deformation of the "witch's chin," and weakness of the platysma muscle [3]. Anatomical studies have described not only supraplatysmal but also subplatysmal significant fat-increased volumes, which means that a superficial approach is not enough, multiplanar surgical intervention is usually required in older patients [4]. Also, controversial information about the correlation between age and body mass with hypertrophy and ptosis of submandibular salivary glands has been described, affecting the mandibular and cervical-mandibular angles, and requiring submandibular gland reduction to improve the contour of the neck [4,5,6,7,8].
A beautiful, youthful neckline also depends dramatically on the anatomy of the platysma muscle. Age-related changes in this muscle include shortening and thinning, with loss of anatomical architecture and, therefore, effacement of the cervical-mandibular angle [9].
This study aims to employ a comprehensive and individualized approach in addressing age-related changes in the lower third of the face using diagnostic imaging as a key part of the preoperative assessment
Methods of Evaluation for Cervico-mental Area Correction
The initial assessment of the face begins with a visual examination. The facial shape of an individual is primarily determined by the underlying bone structure, which is covered by soft tissues that possess distinct characteristics. Bone tissue generally undergoes minimal changes with age, such as a decrease in density and, in some cases, volume. Specifically in the face, the reduction in volume is significant in the maxilla and the mandible, with decreased projection of the soft tissue above [10]. These changes can be addressed through the use of implants or, to a certain extent, by augmenting the soft tissues [11,12]. However, facial aesthetic surgery primarily focuses on the manipulation of soft tissues.
Contemporary correction methods necessitate a comprehensive and individualized approach for each patient. Factors such as the size and shape of the lower jaw, neck fat distribution, the position of the hyoid bone, and the thickness and anatomical variations of the platysma muscle fibers change due to aging need to be assessed individually. To achieve optimal aesthetic results, a meticulous analysis of the patient's parameters is essential [13].
A notable advantage of selecting a correction method is that aesthetic surgery is not standardized. Similar to all forms of art, it is contingent upon the subjective judgments of both the patient and surgeon. Consequently, existing approaches for treating the aging neck, including neck liposuction, bilateral platysma plication, midline platysma plication with distal fiber crossing, neck lift with skin and soft tissue excision, and botulinum toxin injections for platysma relaxation, cater to specific patient categories. The surgeon must possess a thorough understanding of all the approaches mentioned above to ensure the most favorable aesthetic outcomes for each patient.
Modern Imaging Techniques in Plastic Surgery
Three-dimensional imaging has played a fundamental role in the evolution of plastic surgery. Computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) have improved the evaluation and preoperative planning by providing precise and detailed information about the tissues, to build a model in the surgeon’s head that will be useful during the intraoperative navigation [14,15].
This tool has been used for different goals in the field of reconstructive surgery including assessment of the microvascular anatomy for microsurgical reconstructions, diagnosis, preoperative evaluation, virtual planning, modeling of body parts, 3D printing, intraoperative evaluation, and postoperative follow-up [16,17,18,19,20,21,22].
In craniofacial reconstructive surgery, the use of 3-D imaging has proved to reduce operating room time, increase the accuracy of the reconstructions, facilitate preoperative planning, and even simulate the surgery before it is performed[21]. CT scan can also be employed in the preoperative planning of facial feminization in transgender patients, where the surgeon aims to address the osseous aspects of the whole anatomy of the face[23]. This approach has been fundamentally popular in the field of plastic reconstructive surgery and skeletal features but we believe that the role of 3D imaging can also be very valuable in aesthetic facial surgery of soft tissues.
Regarding rejuvenation of the lower third, a CT scan is performed to determine the hyoid bone elevation level, the volume of soft tissue structures in the cervico-mental area, ptosis of subplatysmal structures, and the volume of submandibular salivary glands [4,24]. MRI studies of the submandibular glands have reported a logarithmic increase in the fat component over the years to the ninth decade of life [25]. Ultrasound study of the submental projection at the preoperative stage can reveal insufficient projection in this area, while postoperative assessment can determine the degree of fat subplatysmal autograft survival, the use of which increased chin projection and harmonized the contours of the lower third[13].
3. Clinical Cases
3.1. Case 1
A 47-year-old woman, with no concomitant diseases, presented with slight gravitational changes in the lower third, violation of the cervico-mental angle, deep nasolabial folds and jaws. Along with this, she presented drooping of the eyebrow tails, overhanging skin in the upper eyelid area, bags in the lower eyelid area, and fine mimic wrinkles. When looking at the frontal view photos, the lack of proportions of the lower third is evident (Photo 1).

Photo 1. Patient before and 6 months after complete rejuvenation of the face.
In the lateral view, according to the Riedel-Rikkitz lines, the projection of the chin protrusion is missing[26] (Photo 2). This way, it highlights the lack of support for the midface.

Photo 2. Patient before and 6 months after complete rejuvenation of the face. Riedel plane and Rickett’s line show improvement in the chin projection.
On the CT scan, we assess the level of the hyoid bone so we can guarantee the formation of a beautiful line of the chin-neck angle. In this case, the hyoid bone was quite high. Also, determining the presence of submandibular gland ptosis/hypertrophy is key to achieving an optimal result. For the stability of the results, on the sagittal view of CT, we see the angle and plan a slight extension to harmonize the face (Photo 3 and 4).
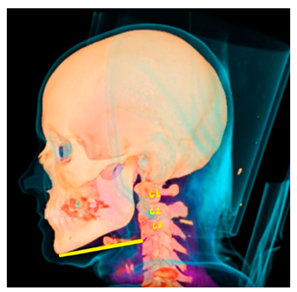
Photo 3. Computed Tomography, the Rocabado plane shows high hyoid bone, a favorable situation to achieve excellent results with platysmaplasty.
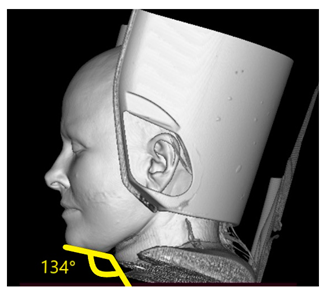
Photo 4. The soft tissues of the neck show an obtuse angle, far from the 90° that is considered aesthetically ideal.
Surgery plan: complex rejuvenation in the volume of DEEP SMAS, temporal lifting, upper + lower blepharoplasty, medial and lateral platysmaplasty with resection of the subplatysmal volume of adipose tissues and a slight extension of the chin with fat autografting, bullhorn lip lift.
3.2. Case 2
A female patient, 45 years old, normasthenic, height 165, weight 67 BMI: 24, smoker, presenting with a dysmorphic-edematous type of aging. The lower third is unsatisfactory, when analyzing the photos, a straight line is drawn showing the insufficiency of the lower third. In the lateral projection, it is evident that the chin protrusion is not enough, there is malocclusion, with microgenia and micrognathia (photo 5). From the anamnesis, chin liposuction + cryotherapy-cryolipolysis was performed twice with an unsatisfactory result. The patient’s main complaint was chin-neck contour.

Photo 5. Riedel plane and Rickett’s line show insufficiency in the lower third of the face, poor chin projection, and obtuse angle of the soft tissues. After surgery, there’s improvement in the lower third of the face.
According to the CT scan, the glands are lower than the level of the lower jaw and show how hypertrophied in volume are the anterior abdomens of the digastric muscles (Photo 6). The level of the hyoid bone is very low, the cervico-mental angle is 145 degrees, and the bone level can shift during the resection of the subplatysmal tissues.
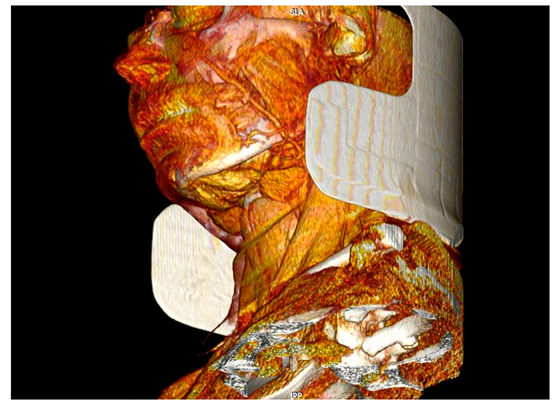
Photo 6. CT scan before surgery. In this projection, the ptosis of the submandibular glands and the hypertrophic digastric muscles are evident.
Surgery plan: Medial platysmaplasty with extended resection of subplatysmal tissues, resection of fat, bilateral digastric muscles by squamous resection, as well as submental glands, closure with medial platysmaplasty with suturing behind the hyoid bone, fixations to raise it to an aesthetically advantageous position and lateral platysmaplasty and vertical midface lifting with minimal access, upper lower blepharoplasty, bullhorn lip lift. Chin augmentation using subplatysmal fat autografting to strengthen the support of the middle zone. (Photo 7)

Photo 7. Before and after surgery, it is evident how the proportions of the face are now harmonized, the result was possible thanks to the integral management of soft tissues in the neck, identified in the CT scan.
4. Discussion
Facial and neck rejuvenation has been and continues to be, one of the most critical aspects of plastic surgery. Age-related changes in the cervical submental area are characterized by the development of an obtuse cervico-mental angle, the disappearance of well-defined lower jaw borders, the presence of jowls, the emergence of vertical platysmal bands, localized submental fat deposits, and excess skin [27]. An "ideal" surgical rejuvenation method for the face and neck should address all the aforementioned age-related changes with minimal risk of complications and a short recovery period [28]. A satisfactory result is considered to allow the patient to perceive a reduction in gravitational changes on the face, a biological age younger than their actual age, attractiveness, and a desire to radiate positive energy.
Attractiveness or the patient's biological (external) age is closely linked to various factors, such as skin quality, which is influenced by parameters like harmful habits, improper nutrition, sleep patterns, stress, and more [29]. Our comprehensive rehabilitation measures include promoting a healthy lifestyle and cosmetological skin care.
In our practice, we pay attention to the following significant criteria for age-related changes:
1. Decreased skin turgor and tone, the appearance of excess skin
2. Involutional changes in facial skeletal structures
3. Excess volume in the lower third of the face
4. Eyebrow ptosis of the eyebrow tail and displacement of soft tissues in the temporal area
5. Age-related changes in periocular soft tissues
6. Hypertonicity or hypotonicity of the chin area
7. Presence of jowls
8. Presence of an obtuse cervical-mental angle
9. Ptosis of the upper lip
10. Manifestation of deep facial wrinkles
These age-related changes must be approached individually, assessing their specific anatomic characteristics, therefore, we proposed the CT scan as a mandatory measure for the preoperative evaluation and surgical planning, especially in rejuvenation of the lower third of the face and neck. In one study, patients were divided by age, type of aging, and BMI. Depending on the individual characteristics of patients and the understanding of the mechanisms underlying the processes of tissue involution and age-related changes in the face, the choice of effective methods for their elimination was determined [12].
Concerns about radiation-induced malignancy can be mitigated by introducing Low-dose computed tomography in aesthetic preoperative evaluation, we believe it is an option that deserves further research [30]. Also, advanced CT techniques like dual-energy which is frequently used in the assessment of head and neck oncological pathologies, could have a role in aesthetic plastic surgery in the future [31].
Currently, there are various advanced non-invasive technological methods employed for the rejuvenation of the soft tissues in the face and neck, that can complement surgical results, to achieve an optimal aesthetic effect. For instance, the use of radiofrequency and ultrasound have shown very good results in terms of improvement of facial wrinkles and jaw sagging[32].
5. Conclusion
Thus, to obtain a harmonious result of surgical correction of age-related changes in the face and neck, it is necessary to take into account the anatomical features of the patient and the severity of age-related changes. In addition, a comprehensive analysis of the face, taking into account the type of facial aging and with the help of ultrasound examination of the soft tissues of the chin area, aids in drawing up an individual plan to obtain the ideal result that the patient imagines and can be implemented by the surgeon. The older the patient, the closer cosmetology and plastic surgery should cooperate, complementing each other, to obtain a rejuvenating effect on the skin both in terms of shape and volume and in terms of tissue quality. To achieve long-term results in the correction of an aging face and neck, it is necessary to master a whole arsenal of various techniques.
Type of aging, BMI, concomitant diseases, patient expectations, and anatomical characteristics are key for preoperative planning and achieving harmony and proportions, golden proportions, and not only prevent aging but enhance beauty.
Author Contributions
Conceptualization, A.B. and V.S.; methodology, A.B., S.A. and N.B. software 3D modeling and analysis, N.B. and A.A.; investigation, A.A. and F. O.; resources, V.S.; writing—original draft preparation, A.B.; writing—review and editing, V.S.; visualization, N.B. and A.A.; supervision, V.S.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sammy Sinno; Thorne, C. Cervical Branch of Facial Nerve: An Explanation for Recurrent Platysma Bands Following Necklift and Platysmaplasty | Aesthetic Surgery Journal | Oxford Academic. 2019, 39, 1–7. [CrossRef]
- Orra, S.; Tadisina, K.; Charafeddine, A.; Derakhshan, A.; Halliburton, S.; Hashem, A.; Doumit, G.; Zins, J. E. The Effect of Age on Fat Distribution in the Neck Using Volumetric Computed Tomography. Plast. Reconstr. Surg. 2021, 147, 49. [Google Scholar] [CrossRef]
- Frisenda, J. L.; Nassif, P. S. Correction of the Lower Face and Neck. Facial Plast. Surg. 2018, 34, 480–487. [Google Scholar] [CrossRef]
- Raveendran, S. S.; Anthony, D. J.; Ion, L. An Anatomic Basis for Volumetric Evaluation of the Neck. Aesthet. Surg. J. 2012, 32, 685–691. [Google Scholar] [CrossRef]
- Mendelson, B. C.; Tutino, R. Submandibular Gland Reduction in Aesthetic Surgery of the Neck: Review of 112 Consecutive Cases. Plast. Reconstr. Surg. 2015, 136, 463–471. [Google Scholar] [CrossRef]
- Mahne, A.; El-Haddad, G.; Alavi, A.; Houseni, M.; Moonis, G.; Mong, A.; Hernandez-Pampaloni, M.; Torigian, D. A. Assessment of Age-Related Morphological and Functional Changes of Selected Structures of the Head and Neck by Computed Tomography, Magnetic Resonance Imaging, and Positron Emission Tomography. Semin. Nucl. Med. 2007, 37, 88–102. [Google Scholar] [CrossRef]
- Lee, M.; Sepahdari, A.; Cohen, M. Radiologic Measurement of Submandibular Gland Ptosis. Facial Plast. Surg. 2013, 29, 316–320. [Google Scholar] [CrossRef]
- Heo, M.-S.; Lee, S.-C.; Lee, S.-S.; Choi, H.-M.; Choi, S.-C.; Park, T.-W. Quantitative Analysis of Normal Major Salivary Glands Using Computed Tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 240–244. [Google Scholar] [CrossRef]
- Hwang, K.; Kim, J. Y.; Lim, J. H. Anatomy of the Platysma Muscle. J. Craniofac. Surg. 2017, 28. [Google Scholar] [CrossRef]
- Shaw, R. B.; Katzel, E. B.; Koltz, P. F.; Kahn, D. M.; Puzas, E. J.; Langstein, H. N. Facial Bone Density: Effects of Aging and Impact on Facial Rejuvenation. Aesthet. Surg. J. 2012, 32, 937–942. [Google Scholar] [CrossRef]
- Mendelson, B.; Wong, C.-H. Changes in the Facial Skeleton With Aging: Implications and Clinical Applications in Facial Rejuvenation. Aesthetic Plast. Surg. 2012, 36, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Dikarev, A.; Mantardzhiev, D.; Tsinenko, D. Facial Skeleton Augmentation with Porous Implants for Long-Term Stability of Surgical Rejuvenation. Plastic Surgery and Aesthetic Medicine 2021, No. 1, 36–43. [Google Scholar] [CrossRef]
- Alimova, S. M.; Sharobaro, V. I.; Telnova, A. V.; Stepanyan, E. E. Planning of methods of surgical correction of soft tissues of the face and neck. Med. Vis. 2021, 25, 47–52. [Google Scholar] [CrossRef]
- Tarassoli, S. P.; Shield, M. E.; Allen, R. S.; Jessop, Z. M.; Dobbs, T. D.; Whitaker, I. S. Facial Reconstruction: A Systematic Review of Current Image Acquisition and Processing Techniques. Front. Surg. 2020, 7, 537616. [Google Scholar] [CrossRef] [PubMed]
- Shaye, D. A.; Tollefson, T. T.; Strong, E. B. Use of Intraoperative Computed Tomography for Maxillofacial Reconstructive Surgery. JAMA Facial Plast. Surg. 2015, 17, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Laungani, A.; Ritman, E.; Lachman, N.; Christner, J.; Vercnocke, A.; Jorgensen, S.; Anderson, J.; Regnier, T.; Saint-Cyr, M. The Use of Micro Computed Tomography in Plastic Surgery: Towards a Better Understanding of Flaps Microvascular Architecture. Plast. Reconstr. Surg. 2013, 132, (4S–1). [Google Scholar] [CrossRef]
- Kumar, T. S.; Vijai, A. 3D Reconstruction of Face from 2D CT Scan Images. Procedia Eng. 2012, 30, 970–977. [Google Scholar] [CrossRef]
- Krakowczyk, Ł.; Piotrowska-Seweryn, A.; Szymczyk, C.; Wierzgoń, J.; Oleś, K.; Ulczok, R.; Donocik, K.; Dowgierd, K.; Maciejewski, A. Virtual Surgical Planning and Cone Beamcomputed Tomography in Reconstruction Ofhead and Neck Tumors – Pilot Study. Otolaryngol. Pol. 2020, 75, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Yen, J.-H.; Chen, W.-H.; Chen, I.-C.; Lai, C.-S.; Lu, C.-T.; Song, D.-Y. Preoperative Computed Tomography Angiography for Evaluation of Feasibility of Free Flaps in Difficult Reconstruction of Head and Neck. Ann. Plast. Surg. 2016, 76, S19. [Google Scholar] [CrossRef]
- Xu, S.-Q.; Jia, X.-L.; Choi, Y.; Zhu, Z.-W.; Xu, Y.-B.; Velamuri, R.; Liu, X.-X. Three-Dimensional Scanning Technique in the Congenital Microtia Reconstruction with Tissue Expander. Chin. Med. J. (Engl.) 2021, 134, 842–844. [Google Scholar] [CrossRef]
- Markiewicz, M. R.; Bell, R. B. The Use of 3D Imaging Tools in Facial Plastic Surgery. Facial Plast. Surg. Clin. N. Am. 2011, 19, 655–682. [Google Scholar] [CrossRef] [PubMed]
- Lynn, A. Q.; Pflibsen, L. R.; Smith, A. A.; Rebecca, A. M.; Teven, C. M. Three-Dimensional Printing in Plastic Surgery: Current Applications, Future Directions, and Ethical Implications. Plast. Reconstr. Surg. Glob. Open 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Callen, A. L.; Badiee, R. K.; Phelps, A.; Potigailo, V.; Wang, E.; Lee, S.; Talbott, J.; Glastonbury, C.; Pomerantz, J. H.; Narvid, J. Facial Feminization Surgery: Key CT Findings for Preoperative Planning and Postoperative Evaluation. Am. J. Roentgenol. 2021, 217, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Alimova, S. M.; Sharobaro, V. I.; Avdeev, A. E.; Sidorenkov, D. A.; Guseva, T. S. Cone-Beam Computed Tomography for Objective Diagnosis of Age-Related Soft Tissue Changes in Lower Face and Neck. Aesthetic Plast. Surg. 2023. [Google Scholar] [CrossRef]
- Saito, N.; Sakai, O.; Bauer, C. M.; Norbash, A. M.; Jara, H. Age-Related Relaxo-Volumetric Quantitative Magnetic Resonance Imaging of the Major Salivary Glands. J. Comput. Assist. Tomogr. 2013, 37. [Google Scholar] [CrossRef] [PubMed]
- Naini, F. B.; Garagiola, U.; Wertheim, D. Analysing Chin Prominence in Relation to the Lower Lip: The Lower Lip-Chin Prominence Angle. J. Cranio-Maxillofac. Surg. 2019, 47, 1310–1316. [Google Scholar] [CrossRef]
- Langsdon, P. R.; Velargo, P. A.; Rodwell, D. W.; Douglas, D. Submental Muscular Medialization and Suspension. Aesthet. Surg. J. 2013, 33, 953–966. [Google Scholar] [CrossRef] [PubMed]
- Giampapa, V. C.; Mesa, J. M. Neck Rejuvenation With Suture Suspension Platysmaplasty Technique. Clin. Plast. Surg. 2014, 41, 109–124. [Google Scholar] [CrossRef]
- Sveikata, K.; Balciuniene, I.; Tutkuviene, J. Factors Influencing Face Aging. Literature Review. 2011, 13. [Google Scholar]
- Lala, B.; Shah, J.; Salvador, T. M.; Ricci, J. A. Expanding the Utilization of Low-Dose Computed Tomography in Plastic and Reconstructive Surgery Based on Validated Practices Among Surgical Specialties. Ann. Plast. Surg. 2021, 87. [Google Scholar] [CrossRef]
- Forghani, R.; Mukherji, S. K. Advanced Dual-Energy CT Applications for the Evaluation of the Soft Tissues of the Neck. Clin. Radiol. 2018, 73, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Hugul, H.; Cigdem, M.; Kirisci, M.; Kutlubay, Z. Focused Radiofrequency and Ultrasound for Face and Neck Rejuvenation: A Retrospective Evaluation of 158 Patients. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



