
Submitted:
28 November 2023
Posted:
29 November 2023
You are already at the latest version
Abstract
3D Printing (3DP) technology has revolutionized the field of the use of bioceramics for maxillofacial and periodontal applications, offering unprecedented control over the shape, size, and structure of bioceramic implants. In addition, bioceramics have become attractive materials for these applications due to their biocompatibility, biostability, and favorable mechanical properties. However, despite their advantages, bioceramic implants are still associated with inferior biological performance issues after implantation, such as slow osseointegration, inadequate tissue response, and increased risk of implant failure. To address these challenges, researchers have been developing strategies to improve the biological performance of 3D printed bioceramic implants. The purpose of this review is to provide an overview of 3DP techniques and strategies for bioceramic materials designed for bone regeneration. The review also addresses the use and incorporation of active biomolecules in 3D printed bioceramic constructs to stimulate bone regeneration. By controlling the surface roughness, and chemical composition of the implant, the construct can be tailored to promote osseointegration and reduce the risk of adverse tissue reactions. Additionally, growth factors, such as bone morphogenic proteins (rhBMP-2) and pharmacologic agent (dipyridamole), can be incorporated to promote the growth of new bone tissue. Incorporating porosity into bioceramic constructs can improve bone tissue formation and the overall biological response of the implant. As such, by employing surface modification, combining with other materials, and incorporation of 3DP workflow can lead to better patient healing outcomes.
Keywords:
Bioceramics
; 3Dprinting
; Bone tissue engineering
; Scaffold fabrication
1. Introduction
Autogenous bone grafts (autografts) are widely recognized as the preeminent standard for addressing bony defects [1]. These grafts, sourced from the patient, are acknowledged for their non-immunogenic nature and possession of osteoinductive and osteoconductive properties [2,3]. Nevertheless, the use of autografts is hampered by limited availability, necessitating a secondary surgical site for harvesting, thereby heightening risk associated with inflammation, infection, and donor site morbidity [1,2]. Conversely, allografts consist of transplanted bone tissue obtained from the same species, typically harvested from cadaveric bone sources [2]. As a result, the utilization of allografts is constrained by the requirements for sterilization, processing, and the inherent potential risk of viral disease transmission, bacterial infection, or the prospect of host rejection [4]. Moreover, due to the requisite processing for sterilization, allografts exhibit diminished biocompatibility in comparison to autografts, resulting in an unpredictable osteoinductive potential [2,3,6].
A range of synthetic scaffolds has emerged as viable alternatives to autografts and allografts [2,5]. These porous constructs have a pivotal role within Bone Tissue Engineering (BTE) strategies, aiming to restore damaged or missing tissue. Optimal scaffolds are structures compatible with biological systems, acting as extracellular matrices (ECM), supporting cellular activity, and facilitating the growth of recently formed tissue [4]. The interconnected pores within scaffold structures facilitate nutrition, oxygen transport, cell migration, and tissue formation [6,7,8].
Among the material options available for scaffold fabrication, bioceramics have been explored for their biocompatibility and osteoconductivity. Certain bioceramics are sourced from biological origins, such as demineralized bone matrix [5], while others are artificially manufactured, including hydroxyapatite (HA), bioactive glasses, and β-tricalcium phosphate (β-TCP) [4]. Traditional methods for crafting bioceramic scaffolds involve techniques like salt leaching, freeze-drying, gas foaming, and the polymer template method [9]. However, these methods present inherent challenges, including a lack of reproducibility and the absence of a structured, engineered internal pore network. This structural randomness resulting from these techniques has demonstrated implications on biological function, causing heterogeneity in the distribution of cells in vitro and non-uniform tissue ingrowth in vivo [10,11,12].
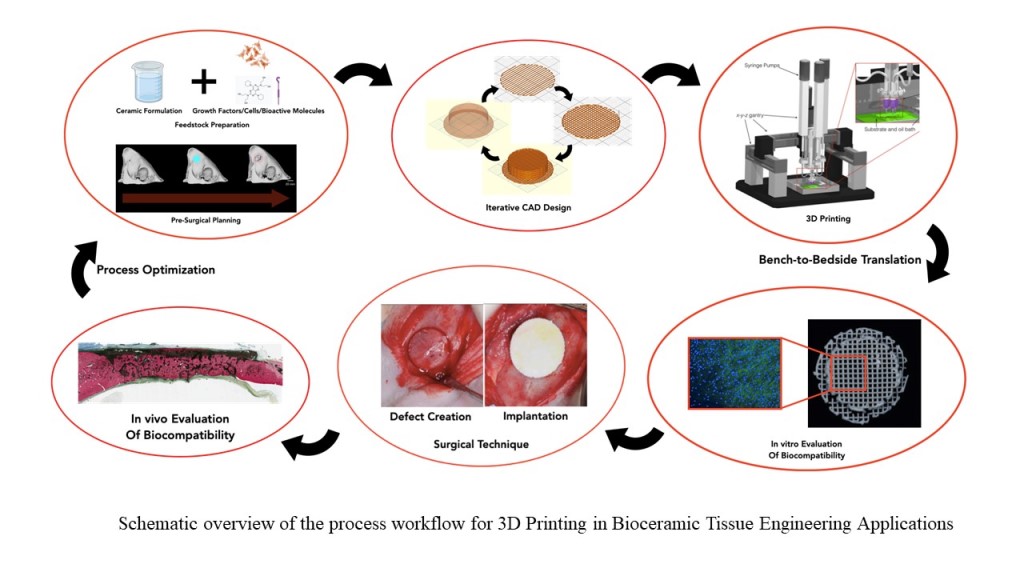
Three-dimensional printing (3DP) technology in BTE (workflow schematic presented in Figure 1) is expected to play a crucial role in offering improved bone reconstruction, rehabilitation and regeneration [13,14]. 3DP as a technique was initially introduced in 1986 by Charles W. Hull, known then as stereolithography [15]. Since then, various techniques have emerged with the aim of creating 3D constructions that replicate both the external and internal structure of the bone at the implanted site [16], seeking to provide a vital framework for cell migration and adhesion, thereby initiating and strengthening the tissue regeneration process [17]. The use of 3DP in the craniofacial region has focused on rehabilitation of the defect site and restoration of facial and intraoral form and function, with an aim of preserving the existing bone and stimulating osteogenesis [14,18].
3DP technology in BTE has emerged with strong potential for fabricating patient-specific scaffolds for bone repair and regeneration applications. Over recent years, there has been an exponential growth in research and application of 3DP techniques for BTE [22]. For instance, enhanced bone tissue regeneration using printed scaffolds has been achieved by tailoring with surface modifications or incorporating bioactive factors, creating a favorable environment for tissue formation [23]. Moreover, incorporating growth factors has shown positive outcomes by promoting cell adhesion, proliferation, osteogenic differentiation, and bone formation [24].
The selection of bioceramic materials for creating scaffolds plays an extremely important part, as each material carries its own set of advantages and disadvantages. To achieve an optimal scaffold, it is imperative that it possesses the ability to promote cell migration and proliferation, thereby stimulating the formation of bone tissue in the desired region. Furthermore, several other parameters related to the material can influence the quality of the printed structure. These factors encompass aspects such as the concentration, viscosity, and volume of the binding agent employed, the density and size of powder particles, the wettability between the powder and the binding agent, as well as the post-processing methods [25]. Furthermore, the scaffolds must also possess satisfactory mechanical properties. Therefore, detailed knowledge of each technique and material to be used is essential for proper planning and execution of the 3DP process. This review concentrates on the principal steps involved in producing 3DP scaffolds, various 3DP techniques, major bioceramic materials, and vital biological molecules used in BTE.
2. Bioceramics
Ceramics constitute a class of materials comprising inorganic and non-metallic solid components [24]. Upon exposure to high temperatures, these materials undergo a structural transition, resulting in bone-like arrangements due to the development of ionic and covalent bonds. Bioceramics, a subclass within this category, have gained significant attention for their potential in fabricating resorbable and implantable devices [26]. This increased interest is attributable to their ready availability, biocompatibility, bioactivity, hydrophilicity, stoichiometric similarity to natural bone, and osteoconductivity [27].
Bioceramics intended for BTE applications can be categorized as natural or synthetic. Natural bioceramics are sourced from human, bovine, porcine and piscine origins [24]. Conversely, synthetic alloplastic ceramics have been developed in laboratory settings through advancements in materials science research for BTE purposes. Synthetic bioceramics exhibit promising biological responses and offer a microenvironment comparable to natural bone [28]. For instance, the stoichiometry of tricalcium phosphate (TCP) and HA ceramics closely resembles that of amorphous bone precursors and bone minerals [29].
Despite the numerous favorable attributes associated with bioceramics, their inherent stiffness and low flexibility render them brittle, posing a challenge when shaping them into constructs [30]. Consequently, they exhibit inferior mechanical strength [31] and fracture toughness [32] compared to metallic materials, which limits their applications to anatomic areas that are non-load-bearing. A detailed overview of bioceramics utilized in BTE is presented in Table 1.
2.1. Commonly Used Bioceramics
Hydroxyapatite (HA; Ca10(PO4)6(OH)2) is a calcium phosphate-based bioceramic with calcium to phosphorus ratio between 1.50 and 1.67 [45]. HA is a major component of natural bone and constitutes ~ 65% of bone mass and bulk of the inorganic components in bone tissue [46,47]. HA in bulk form demonstrates slow resorption in vivo, with a rate of <1% per year, is weak under tensile and shear forces, but has good compressive strength [48]. HA can be prepared using different methods depending on whether it is naturally harvested and synthesized in the laboratory. Naturally sourced hydroxyapatite can come from porcine [49], bovine [50], and piscine (scales) [51] sources, and be converted osteoconductive scaffolds, facilitating bone cell growth [52]. Synthetic HA transforms to a highly crystalline calcium phosphate when subjected to high temperatures (>1000°C). The mechanical properties of HA scaffolds have been optimized by heat treatment and by varying the amount of ceramic material used for fabricating both load bearing, and non-load bearing scaffolds for bone repair and regeneration [53].
Tricalcium phosphate (TCP; Ca3(PO4)2) is another such bioceramic that has been extensively investigated for use as a bone substitute, as it is known to induce osteoblastic development of progenitor cells [54]. TCP is well known for its biocompatibility, bioactivity, osteoconductivity, and resorbability [48,65]. TCP is produced in situ by dissolution precipitation process at 37°C [64,66], and has two primary crystallographic forms, namely α-TCP and β-TCP [16] with the later exhibiting more favorable biological response and osteoconductivity [54,56]. To elaborate, β-TCP is a porous, osteoconductive ceramic which is slow to resorb [57]. However, studies have demonstrated β-TCP to have a more rapid resorption rate when compared to HA, maintaining osteoconductive properties - features that are desirable for achieving rapid replacement of scaffold with bone [57,58]. In addition, β-TCP has shown promise for use in BTE due to its mechanical strength and chemical stability. Its main mechanism of bioactivity is the partial dissolution and release of calcium and phosphate ion products forming a biological apatite precipitate on the scaffold surface [59]. β-TCP constructs are usually sintered to high temperatures (~1100°C) to facilitate densification and to render adequate mechanical strength (compressive strength: 2.5–16 MPa), making it an appropriate choice for low or medium load-bearing applications [54].
2.2. Other Ceramic Materials
Silicon carbide (SiC) bioceramics have been investigated for use as biomedical implants due to their bio inertness, biocompatibility, ease of handling, capacity to be molded into any desired shape and physicochemical stability [60]. Research has shown that SiC has been used extensively for hip implants and load-bearing anatomical locations as it demonstrates high compressive strength, slow degradation and high biocompatibility [61,62]. SiC-based bioceramics constructs are typically sintered at high temperatures (between 1860–1950°C) that yields high elastic modulus, lower frictional coefficient, increased hardness, and renders chemical inertness [63]. Furthermore, SiC also demonstrates high wear and chemical resistance, and low thermal expansion [62,64]. However, there are some notable disadvantages associated with SiC for bone tissue regeneration. First, silicon carbide is not naturally bioactive, and lacks the inherent ability to promote osteogenesis, or bone tissue growth. This could potentially hinder the speed and efficiency of the bone regeneration process compared to other bioceramics. Additionally, the cost of producing SiC can be relatively high, potentially limiting its accessibility to certain patients and healthcare institutions. Overcoming these challenges through ongoing research and development efforts is crucial to fully unlock the potential of SiC in the field of regenerative medicine. Zirconium oxide (ZrO2) has been extensively studied for biomedical applications due to its biocompatibility, chemical stability, and excellent mechanical properties [42] . Zirconia can exist in three different crystallographic phases which are dependent on the temperature, namely monoclinic (up to 1,170°C), tetragonal (up to 2,370°C), and cubic (above 2,370°C) [66]. In its tetragonal phase, it offers the most advantageous mechanical properties, and therefore, dopants can be employed to stabilize this phase at room temperature. Among the dopants used, yttrium oxide (Y2O3) is the most common, resulting in the material known as yttria-stabilized tetragonal zirconia polycrystals (Y-TZP) [67]. Previous research indicates that the flexural strength of Y-TZP can surpass 1000 MPa, while its fracture toughness can achieve levels of up to 10 MPa [68,69]. This outstanding mechanical performance can be attributed to a transformation toughening mechanism, in which tetragonal grains undergo a conversion to monoclinic (t-m) when the material experiences tensile stresses. This t-m transformation leads to a 4% volumetric expansion, hampering crack propagation and thereby enhancing the ceramic’s resistance to damage [66,67,68,69].
Furthermore, ZrO2 exhibits an elastic modulus compatible with human bone tissue and demonstrates excellent osseointegration capabilities [70]. These characteristics render zirconia a promising choice for applications in bone reconstructions. With a high melting point (2715°C) and a sintering temperature range spanning from 1000 to 1450°C, ZrO2 has been explored in the literature as a material of choice for 3DP of scaffolds for bone tissue [67,70,71,72,73,74]. Nevertheless, the utilization of ZrO2 as BTE scaffolds can present some challenges including, but not limited to its non-resorbable characteristics [75].
Barium titanate (BaTiO3) is another bioceramic used in BTE. It induces piezoelectric effect, which is important for bone formation by maintaining a charged surface, thereby improving cell adhesion and proliferation [76,77]. Scaffolds fabricated using BaTiO3 are effective for BTE due to their cytocompatibility and osteogenic differentiation, with high compressive strength and Young’s modulus [78,79,80]. Blending of BaTiO3 with other bioactive materials like HA has further allowed for enhancement of bioactivity and implant stability by integrating with host bone tissues [81]. Despite its potential, there are some notable disadvantages such as ensuring its long-term biocompatibility and safety for implantation in the human body and is an ongoing area of research. Moreover, the technology for synthesizing BaTiO3 is still in its early stages, requiring further development and refinement to optimize its use for BTE.
2.3. Polymer-Ceramic Composite Materials
Scaffolds made of inorganic materials like HA, β-TCP, or other bioceramics display remarkable biocompatibility but suffer from brittleness. One explored strategy to enhance the mechanical properties of these brittle scaffolds involves the application of polymer coatings [82]. This ensures filling of existing cracks within the bioceramic structure with a polymer phase. It is hypothesized that this polymer phase not only fills the cracks but also acts to bridge them during fractures, thus increasing the toughness of the bioceramic scaffold. In addition, the polymer phase could be utilized as carriers for drugs and other biomolecules such as growth factors, which enhance the functionality and bioactivity of the scaffolds.
As mentioned in previous sections, calcium phosphates including HA and β-TCP play an important role in the development of scaffolds for BTE. Polymers such as those derived from lactic acid (LABPs) offer mechanisms for promoting healing and minimizing infections while including controlled delivery of growth factors, antibiotics, and surface/chemical modifications [83,84]. These properties are similar to those present in calcium phosphate based ceramic materials. Due to this, LABPs have been used in combination with ceramics yielding mixtures such as in Polycaprolactone/TCP, and Polylactic Acid/HA yielding enhanced biocompatibility and mechanical properties relative to their individual constituent materials [85,86].
Considering the compositional organization of the polymer-ceramic composites, polymers matrices and ceramic reinforcement particles would be ideal as the low mechanical strength of the polymer phase would be compensated by the ceramic phase. Additionally, ceramic particles would promote self-healing in the polymer matrices [87,88]. Hence, where the nature of the purely ceramic or polymeric scaffolds may not completely satisfy all dimensional, mechanical, and biological requirements, composites have been utilized and proven to be effective alternatives [89]. The fundamental procedure for creating polymer-ceramic scaffolds with interconnected microstructures involves the infusion of a sintered or partially sintered bioceramic scaffold with a polymer. Typically, a biodegradable synthetic polymer is employed, taking inspiration from the composition of bone, which comprises approximately 60% inorganic material (hydroxyapatite) and the remainder as organic material (collagen). As such, a defining characteristic of such materials affecting their improved mechanical and biological properties are the interfaces between their various phases.
As in the case of any composite material, binders enhance interface properties. Shuai et al. described such interfaces as small regions in which the chemical composition of the two phases in the composite material has a significant change, forms a bond (Vanderwaal’s forces, chemical bonds, mechanical interlocks or electrostatic attraction) with each other, and can play a role in transferring load [90,91,92]. Considering polymer-ceramic composites, literature also indicates self-healing due to the interface formed between the various phases. Techniques to achieve better interface bonding comprise of polymer-ceramic composites include coupling agent modification that is described in detail further in this section; surface treatment such as polymer grafting [93,94] that can initiate polymerization of the monomer on the surface of the ceramic particles; and esterification whereby ester bonds can be formed through a reaction between an acid and a hydroxyl group leading to the formation of an active group that can react with a biopolymer on the bioceramic surface [94,95]. Presently, coupling agent modification is the most frequently utilized method to improve the interface bonding [90]. This operates by improving the degree of interface bonding between the two phases, imparting higher strength and superior-properties when compared to the other techniques described above for use in load bearing BTE applications [96].
3. 3DP Methods for Fabrication of BTE Scaffolds
Investigations into granular bioceramic materials reveal that their random nucleation sites and the absence of spatial coordination pose obstacles to the organized directional growth of bone. This challenge is pivotal, as it impedes the complete restoration of both the form and function of recently regenerated bone tissue [97]. In addition, while conventional natural and synthetic bone grafting materials offer favorable healing outcomes and serve the role of as supporting structures during bone formation, they have several disadvantages including poor mechanical properties, and poor resorption capabilities [5,98]. As such, the fabrication of complex geometries and interconnecting porous framework using bioceramics poses significant difficulties. Drawbacks associated with granular ceramics have spurred investigations into the creation of geometrically robust devices through 3D printing. 3DP, alternatively referred to as additive manufacturing (AM), facilitates the incremental assembly of scaffolds based on bioceramics, forming elaborate and accurate constructs. The physical characteristics of the structures, encompassing factors like pore dimensions and configuration, the linkage between pores, and the overall geometry of the scaffold, can be specified through a three-dimensional model and produced by the machine [99,100]. The engineered 3D architectures achievable through 3DP facilitate enhanced cell proliferation, adhesion, differentiation, and overall bone tissue formation [101].
Consequently, the field of craniomaxillofacial (CMF) surgery has undergone a recent transformation, embracing individualized treatment approaches. The emergence of 3DP technology has been instrumental in the field of regenerative medicine, opening new avenues for creating customized scaffolds designed for site-specific defects while conserving space. These scaffolds exhibit osteogenic, osteoinductive, and osteoconductive properties, promote angiogenesis, and showcase mechanical stability upon implantation, preventing immediate failure [102,103,104,105,106]. Advancements in Computer-Aided Design (CAD), Magnetic Resonance Imaging (MRI), and computed tomography (CT) have facilitated the reconstruction of regions of interest (ROIs). CT and MRI imaging enable the acquisition of series of high-resolution images of the ROI, which can then be segmented for digital reconstruction. Subsequently, scaffold macro geometric features are delineated to ensure adequate stabilization of the defect site and confer the necessary mechanical integrity at the site [107,108,109]. In subsequent stages, the reconstruction process involves converting the isolated ROI into a stereolithography (STL) file format to generate high-fidelity templates of the defect through discretization [110]. Upon determining the scaffold’s macro geometric parameters, suitable slicing software is employed to slice objects, generating a multilayered three-dimensional (3D) object composed of a sequence of parallel surfaces or planes with a specific interplanar spacing. Slicing converts the STL file into machine-level .gcode, containing essential coordinate-related instructions and auxiliary commands. These commands play a crucial role in customizing scaffold lattice parameters, such as pore spacing, layer height, and rod size, both prior and during the printing process. The .gcode further details the scaffold’s printing orientation, offers virtual representations of the scaffold for ease of visualization, and allows print time optimization during rapid prototyping. Following this, scaffolds of varying sizes, shapes, and pore structures are manufactured to address the identified defect site through diverse 3DP methodologies. These techniques encompass laser-assisted methods like selective laser sintering (SLS) and stereolithography (SLA), micro-extrusion techniques such as fused deposition modeling (FDM) and direct inkjet writing (DIW), as well as light-assisted methods like digital light processing (DLP) (Table 2) [58,107,111,112].
3.1. Laser/Light Assisted 3DP Techniques
3.1.1. Selective Laser Sintering (SLS)
Introduced by Deckard and Beaman in 1986, SLS is a technique extensively utilized for the printing of custom implants, surgical planning guides, and constructs applied in orthopedics and dental tissue engineering [126,127]. In this method, a high-powered CO2 laser selectively and continuously fuses the surface of the powders, forming layers and resulting in the creation of the 3D construct [128]. Loose particles surrounding the sintered particles provide support, and with each layer scan, the powder bed descends as a roller spreads the subsequent layer of powder over the prior one. The application of SLS to ceramic-based materials can be achieved through either a direct or indirect method (Figure 2) [129,130].
The direct SLS approach can be either slurry-based or powder-based. Thus, to ensure the dimensional accuracy of the structure, the powder or slurry is heated and sintered in-situ [131]. However, the use of ceramics in the direct SLS method becomes challenging due to the need for high melting temperatures. Although the laser has the potential to reach the sintering temperature, achieving ideal densification of the ceramic powder within the brief laser exposure time is impractical. Moreover, extending the exposure time may lead to significant dimensional changes [132]. Additionally, factors such as laser energy consumption, extended cooling times, and laser scattering among ceramic particles can make this technique inefficient and costly to produce large and complex bioceramic scaffolds [133]. However, it is possible to enhance print quality by optimizing various factors, including particle size, particle shape, binder content, scanning speed, and laser energy [134]. On the other hand, the indirect SLS technique involves coating the chosen powder with a sacrificial organic polymer, which melts upon exposure to the laser, binding the ceramic particles together [100,129]. Subsequent high-temperature sintering of the green constructs is then carried out to produce the final scaffold [130].
3.1.2. Stereolithography Apparatus (SLA)
SLA, depicted in Figure 3, is a 3DP technique which allows the creation of highly precise and complex constructs with control over fine internal architectures (at the micrometer scale) and offering a high-quality surface topography [135,136]. Chuck Hull developed SLA in 1986 for manufacturing polymeric structures [137]. SLA involves a UV-curable photopolymer, a laser unit, galvanometric mirrors, support structures, an elevator, and a recoater blade [138,139]. The ultraviolet (UV) laser in SLA selectively crosslinks a photosensitive liquid resin in a layer-by-layer manner to construct a 3D object. Once a layer is completed, the resin bed moves upward and then descends back into the vat. This process continues until the final print is completed, achieving the intended scaffold [140]. The same principle can be applied to use SLA for printing ceramic materials. However, in this case, ceramic particles suspended in a slurry system replace the resin-based system with micro/nanometer size, light-sensitive monomers, and a photo initiator which solidifies by via photo-polymerization mechanism once exposed to UV laser [141,142]. To obtain a smooth flow for printing and homogeneity of the print, the ceramic resin is required to have long shelf life, and appropriate rheological behavior [143].
SLA is used to fabricate scaffolds for bone regenerative applications using materials such as HA, β-TCP, alumina, ZrO2, and bioactive glasses [142]. A primary difference between traditional SLA and ceramic SLA method is the contribution of scattering phenomena due to the addition of ceramic particles relative to the light-sensitive monomer [141]. To elaborate, the ceramic particles scatter UV light, which reduces curing depth, resolution, and increases the printing time [102]. Hence, smaller particle sizes lower the occurrence of scattering and are hence preferable for SLA technique, coupled with the fact that the cure depth can be controlled by adjusting the power of the laser, exposure time and scan speed [103,104]. Organic components have to be calcined to be removed and eventually sintered at high temperatures to fuse/densify the ceramic particles [105].
3.1.3. Digital Light Processing
Digital light processing (DLP) employs resins made of photopolymers to create three-dimensional structures under an illumination source [106,144]. The key components of this 3DP technique are a projector screen made up of pixels with digital light, digital mirror device made of numerous micro-mirrors that navigates light from the projector, conveyor and a resin tank that contains the feedstock (Figure 4) [145]. Speed, printing efficiency with great dimensional accuracy are the main advantages of using the digital light processing method [146]. Digital Light Processing (DLP) is an advanced AM technology that is increasingly being explored and adapted for use in BTE, with a focus on the fabrication of ceramic-based scaffolds [147,148,149,150]. This innovative process leverages a digital micromirror device (DMD) or a liquid crystal display (LCD) to precisely control and modulate light exposure patterns in a layer-by-layer fashion. In the context of BTE, DLP employs photosensitive ceramic resins as the starting material. These resins are formulated to include ceramic particles or precursors, which respond to photopolymerization upon exposure to ultraviolet (UV) light or other suitable light sources [146]. The DLP apparatus projects digital images, dictated by a computer-aided design (CAD) model, onto the ceramic resin. As the light interacts with the resin, it triggers the photopolymerization reaction, leading to the solidification of the material in the desired pattern. This highly controlled, layer-by-layer process enables the creation of intricate and precise ceramic scaffolds that closely mimic the structure and properties required for effective BTE [149].
The advantages of DLP for ceramic based BTE are manifold. Foremost, it offers the capability for patient-specific customization, allowing the creation of implants that match an individual’s anatomical characteristics [151]. This personalization enhances the likelihood of implant integration, minimizing the risk of rejection and promoting optimal bone healing. Moreover, DLP allows for meticulous control over the architecture of the scaffold, including the size, shape, and distribution of pores, which are critical factors influencing cell infiltration, nutrient diffusion, and vascularization within the scaffold. These parameters are vital for supporting bone tissue regeneration. Furthermore, DLP-printed ceramic structures typically demonstrate excellent mechanical properties, making them suitable for load-bearing applications in bone reconstruction [152]. However, post-processing steps like sintering may be required to enhance the mechanical strength and biocompatibility of the printed ceramic structures. As the field of DLP for ceramic BTE continues to advance, it holds immense potential for revolutionizing the field by delivering customized, high-quality ceramic scaffolds that foster efficient bone regeneration, leading to improved patient outcomes.
3.2. Micro Extrusion Based Techniques
3.2.1. Direct Inkjet Writing (DIW)
The DIW technique, showcased in Figure 5, originated with Cesarano in 1997 and is also commonly referred to as micro-robotic deposition or robocasting. This approach involves the layer-by-layer creation of objects by extruding and depositing a water-based colloidal suspension (referred to as ink) which comprises a substantial amount of ceramic powder (usually exceeding 40%), employing a movable nozzle managed by a robotic deposition arm or gantry [153,154,155]. In contrast to alternative methods, DIW presents superior speed and cost-efficiency, enabling the entire procedure, encompassing production, drying, and sintering, to conclude within a relatively short period, typically between 24 to 48 hours. Compared to other techniques, DIW offers greater speed and cost-effectiveness, enabling the entire process, including fabrication, drying, and sintering, to be completed within a relatively short timeframe, typically ranging from 24 to 48 hours [156].
A DIW printer achieves three-axis motion by inputting a tool path (.gcode) to a computer numerical controller. These printers generally include a fixed platform equipped with a mobile gantry. The controller governs the gantry’s movements, and manages the downward motion of syringe pumps containing the colloidal gels [21]. Multiple extrusion nozzles permit the simultaneous deposition of diverse colloidal gels, , comprising the primary printing material (such as β-TCP) and fugitive support material (like Carbon Black). This support material is typically introduced during the printing process and subsequently eliminated through dissolution or melting once the printing operation is finalized [57]. The use of fugitive support material facilitates the creation of elements with internal voids or overhangs that would otherwise be challenging to produce without such support.
During the DIW procedure, the printer’s extruders adhere to the Cartesian coordinate pathway specified in the .gcode file while placing the gel or slurry onto a substrate [157]. The time required to build periodic structures, such as lattices or scaffolds, depends on various factors, including the nozzle diameter, extrusion rate from the nozzle, overall scaffold volume, and printing speed. Challenges linked with the DIW method involve recurrent nozzle clogging, sensitivity of ink to processing parameters, requirements for optimizing colloidal ink, and ‘filter pressing’ caused by constant ink extrusion pressure and particle separation from the liquid phase [158]. In addition, developing a colloidal gel (or ceramic ink), that is suitable for the deposition process with a shear-thinning property and yet be able to retain its shape after extrusion is a major challenge with DIW technique [159,160]. As such, there is usually a high solid content which prevents crack formation during the drying process and enables the deposited ink to retain it shape or volume after drying [161].
3.2.2. Fused Deposition Modeling (FDM)
Thermoplastic polymer filaments are used to fabricate 3D constructs by fusion deposition modeling, an extrusion-based 3DP technique. FDM functions on the principle of AM, systematically depositing material in a layered manner onto the surface [163]. The essential components of the FDM process include material feeding, gantry, print head, and the forming surface [162]. In this printing method, thermoplastic filaments undergo a melting process between rollers and are subsequently extruded through a nozzle onto the construction surface (Figure 6). FDM offers the advantage of enabling multi-material printing, ensuring high design quality, and enhanced mechanical properties [164]. Although this method is conventionally linked with thermoplastic materials [114], its application has extended to ceramics, presenting new opportunities for crafting ceramic components with intricate geometries [165,166]. In FDM for ceramics, a ceramic-filled filament is extruded layer-by-layer, following a computer-aided design (CAD) model. Once the ceramic filament is deposited, it is heated to fuse the particles together, creating a solid structure [167]. This process enables the production of ceramic parts with intricate shapes that would be challenging to achieve through traditional ceramic forming methods.
Despite its advantages, FDM for ceramics comes with some challenges and limitations. The high-temperature requirements for sintering or post-processing ceramic FDM parts can pose difficulties in terms of energy consumption and equipment costs [168]. Moreover, achieving high levels of detail and surface finish in ceramic FDM parts can be challenging, as the process may result in a rougher texture compared to conventionally manufactured ceramics. Furthermore, the choice of ceramic materials available for FDM is limited compared to traditional ceramic processing techniques or DIW. As research and development in the field of ceramic FDM continue to advance, it is likely that many of these challenges will be addressed, further expanding the utility of this technology in various industries.
3.3. Process Optimization and Post Processing
The effective and precise application of 3D printing processes relies on an extensive optimization of various parameters. These parameters include the size of the powder, the density of the powder bed, surface characteristics, and properties of the binder, especially in micro-extrusion techniques. In resin-based printing, parameters involve laser power source attributes, resin optical characteristics, and the size of ceramic particles within the resin [106,169,170].
Some of the advantages of 3DP is scalability to large sizes, relative low-cost, control over the pore geometry, pore size, and interconnectivity of constructs [99,171,172]. Nevertheless, a significant challenge of this technique lies in the extensive optimization required to create a construct with a precisely porous structure [133]. Optimizing the powder size plays a crucial role in enabling the smooth flow of particles in DIW and in achieving a tightly packed powder bed using the laser-assisted 3DP method. This optimization facilitates the creation of intricate details within the printed scaffold [173]. Generally, the use of finer powder particles enables more accurate and delicate microscale features, leading to a smoother surface finish in the printed constructs. In contrast, larger-sized particles spread more easily over the powder bed and allow for efficient binder penetration. However, utilizing excessively large particles with high flowability results in reduced stability and powder density in the printing bed. The roundness of particles significantly enhances powder flowability during printing [174].
In the post-processing of bioceramic scaffolds, sintering is a critical step in various 3D printing techniques detailed in this review. It serves to enhance the mechanical properties and eliminate the organic binder, burn off fugitive support material, or remove undesirable polymeric impurities (employed in the ink formulation step in DIW), and/or fuse the individual ceramic particles together. Sintering results in both physical and chemical changes in the printed constructs, whereby high interconnectivity between particles is achieved, making the printed constructs stronger and more resilient to fracture by mechanical loading [133]. Although sintering is an essential step, it results in volumetric shrinkage [99], which can lead to dimensional inaccuracy. In addition, the shrinkage may not be uniform leading to the incorporation of residual stresses, and crack formation in the printed construct, which requires a good understanding of feedstock preparation, geometric dimensioning and tolerancing prior to ink, filament or slurry (feedstock) preparation. To replace sintering, acid-based binders are now being utilized and explored and could serve as a viable option in some cases where sintering is not possible [169,175].
Sterilizing 3D printed (3DP) devices forms a critical aspect of their medical applicability. The primary sterilization methods include steam, ethylene oxide (EtO) or by γ-radiation. Steam sterilization employs high temperatures (up to 135°C, but generally between 121-135°C) and is cost-effective and non-toxic. It exposes the devices to high-temperature steam under pressure for a calculated duration to eliminate microorganisms [176]. EtO operates at lower temperatures within the range of 37–63°C. Ethylene oxide functions by alkylation of proteins and DNA in microorganisms [177]. EtO sterilization is a lengthier process than steam sterilization and requires aeration to eliminate residue. However, as EtO sterilization is performed at lower operating temperatures, it is compatible with a wider range of materials, especially those sensitive to heat or moisture. γ-radiation sterilizes through irradiation, typically at levels exceeding 25 kGy, and does not necessitate an extended aeration process [178]. When considering devices meant for implantation versus those used as intraoperative models for reference, distinct factors come into play. For 3DP devices designed for implantation, it is crucial that the sterilization process doesn’t compromise the device’s structural and mechanical integrity. Consequently, it’s essential to consider the ability of the material to withstand these different sterilization methods, while also considering factors such as the availability of aforementioned techniques.
4. Biological Factors and Bioactive Molecules
With the emergence of tissue engineering methodologies, such as the utilization of 3D scaffolds that provide conducive environments for cell migration and proliferation, there has been a focus on enhancing the rate of bone formation and regeneration by incorporating exogenous osteogenic cells, especially through the application of stem cells (SCs) [109,179,180,181]. Therefore, a clear understanding of the selection of cell sources and the strategies employed to enhance osteogenic differentiation is essential. Osteoblasts possess strong osteogenic potential and can synthesize and secrete bone matrix, thereby promoting mineralization and bone formation. However, their main disadvantages include low availability of donor sites, low proliferative capacity, and longer incubation time [109]. Consequently, stem cells (SCs) have been extensively investigated in BTE [109,182,183,184]. SCs are undifferentiated cells with the capacity for self-renew, proliferation, and, with appropriate signaling, differentiation into different lineages of specialized cells. This cells can be categorized as embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs), and postnatal adult stem cells based on their source [109]. Considerable efforts have been made towards ESC differentiation into osteogenic lineage for BTE, however, there is currently no consensus regarding their tumorigenicity, immunogenicity, and ethical and safety issues [109,184]. Similarly, with the use of iPSCs, although some attempts have been made towards their differentiation in osteogenic lineage, further study and improvements are needed for the optimization of induction approaches and control of cellular differentiation [109]. On the other hand, adult stem cells have been the most investigated in BTE research, including bone marrow mesenchymal stem cells (BMSCs), dental pulp stem cells (DPSCs), adipose derived stem cells (ASCs), among others.
Adult stem cells have demonstrated a potential to differentiate into osteoblasts, with BMSCs specifically recognized for their ability to differentiate into osteoblasts, chondrocytes, or adipocytes [109,184]. Using autologous BMSCs has yielded optimal outcomes in repairing mandible defects, showcasing promising potential for bone regeneration in the CMF [185]. Clinical data has also shown an enhanced rate of bone formation with BMSCs [29,30,31,32,33]. However, the procedure for aspirating BMSCs is invasive and painful for patients. Moreover, their retrieval is challenging due to the low frequency of BMSCs in human bone marrow (0.001%–0.01%) [186]. This scarcity worsens with age, further limiting the attainment of a significant osteogenic effect [187]. Therefore, the proposal for in vitro culture expansion aims to acquire an adequate quantity of cells for clinical application. Nevertheless, cell expansion needs to be carried out in facilities that follow good laboratory practices, which are laborious, expensive, and time-consuming. Moreover, issues such as loss of proliferative and differentiation capability during cell expansion, along with heightened risks of pathogen contamination and genetic transformation, are associated with these expansion procedures [184].
Considering this, numerous strategies and methods have been developed to enable clinicians to utilize growth factors, such as platelet concentrates (platelet-rich plasma – PRP and platelet-rich fibrin – PRF), fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF), bone morphogenetic protein (BMP), platelet-derived growth factor (PDGF), and dipyridamole (DIPY) for regenerative purposes [180,188,189]. Growth factors transmit signals to target cells through receptor binding, leading to the activation of specific genes. Therefore, a site-specific dosage relationship and sequence of biomolecules determine the cellular response, as well as the quality and quantity of tissue regeneration [190]. However, the multiplicity of applied factors, carriers, and methods utilized in the literature makes it challenging to evaluate the most predictable therapy [191].
The most widely used osseoinductive growth factor is BMP, which is a member of the transforming growth factor superfamily - β, isolated and purified from bone extracts [182]. BMP displays chemoattraction toward osteoprogenitor and SCs, promoting their proliferation and differentiation into mature osteoblasts. It also up-regulates VEGF to enhance angiogenesis [192]. In large bone defects, BMP-2 delivered locally via scaffolds has shown to result in increased osteogenesis compared to BTE devices (scaffolds) alone [193,194,195]. BMP-2 application has resulted in increase in both quantity of bone formation and its quality, with an increase rate of bone forming markers, such as osteocalcin [191]. Reported side effects of using BMPs include severe inflammation, ectopic bone formation, and premature suture fusion [196]. An additional biological side effect pertains to the development of antibodies against these growth factors, which not only poses risks for future BMP use but may also lead to cross reactions against naturally occurring growth factors [196,197]. Moreover, the short biological half-lives and localized action of BMP-2 contribute to the associated drawbacks [191]. Thus, the responsible clinical use of BMPs will necessitate further research in developing more sophisticated carriers with biologically suitable release characteristics for growth factors, enabling dose reduction and a more controlled bone formation process [190].
Recently, a promising alternative growth factor has emerged, displaying favorable potential for bone regeneration, while avoiding the adverse side effects commonly associated with BMP-2 [111,198,199,200,201]. Adenosine, known as protective metabolite, has attracted attention for its osteogenic properties. Traditionally recognized as a cellular-level metabolic marker, adenosine attenuates activity across various cell types as a protective mechanism [201]. However, alterations in bone homeostasis via adenosine receptor activity occur at concentrations above normal physiological levels [198]. In non-stressed cellular conditions, achieving sufficient extracellular adenosine concentrations to trigger receptor activation remains challenging, even with continuous inhibition of the adenosine deaminase enzyme [202]. Consequently, alternative approaches exploring pharmacological manipulation to activate adenosine receptors have been investigated. This manipulation has demonstrated the potential to attain the requisite adenosine concentrations to influence its receptors without inducing stressful cellular conditions. Consequently, alternative approaches exploring pharmacological manipulation to activate adenosine receptors have been investigated. This manipulation has demonstrated the potential to attain the requisite adenosine concentrations to influence its receptors without inducing stressful cellular conditions.
The primary pharmacological agent of note is Dipyridamole (DIPY), an indirect agonist of adenosine A2A receptor. DIPY operates through the Type 1 equilibrative nucleoside transporter, ENT1, hindering adenosine reuptake into the cell, leading to its extracellular accumulation [203,204,205]. Recent studies have indicated that DIPY not only enhances osteoblast function but also curtails osteoclast formation [206]. Meanwhile, the safety profile of DIPY has been well established after decades-long clinical use in cardiac stress testing and anti-platelet therapy and has been shown to preserve suture patency without indications of ectopic bone formation [203,204,205]. 3D-printed bioceramic (β-TCP) scaffolds coated with DIPY (3DPBC-DIPY) in various animal models have previously been shown to be effective in bone regeneration for a range of clinical scenarios including defects induced in the calvaria, ramus, mandible and alveolus suggesting adenosine as a promising therapeutic target for rapid bone formation, as described in following sections.
5. Future Considerations and Requirements for 3DP of Bioceramics
To fulfill the functional prerequisites of the 3DP technique for bone scaffolds, each step of the process plays a crucial role. The pre-processing stage begins with the acquisition of images of the defect site, which can be done through scanning the region via computerized tomography, and magnetic resonance imaging [207]. The obtained data is then transferred to computer-aided design (CAD) software for the planning phase and design of the scaffold. Subsequently, the information is exported to the 3D printer. In this phase, parameters such as printing speed, layer thickness, alignment, printing temperature, and filling density are defined, depending on the chosen technique and material [208]. Considering this, emerging technologies such as machine learning and artificial intelligence (AI) are being applied to assist in the quality control of AM processes. Studies have highlighted the benefits of machine learning for optimizing 3DP techniques [209,210,211,212]. ML, a subfield of AI, primarily focuses on creating analytical models capable of identifying patterns in data and making predictions of future outcomes based on prior information [211]. ML has been shown to assists in determining ideal printing methods that result in faster printing of structures with higher shape fidelity and superior mechanical properties, while also providing insights into the impact of different parameters on the printing process [212].
On the other hand, biomaterials, and equipment employed in 3DP of scaffolds are continuously evolving, becoming increasingly specialized to meet the demands of regenerative medicine, yielding more promising results. However, as discussed in previous sections, there is room for significant improvement. To achieve even more refined outcomes, it is essential to foster collaboration among professionals from diverse fields, including engineers, healthcare practitioners, experts in artificial intelligence, and biomaterial specialists, among others. Teamwork and knowledge sharing facilitate the identification of existing gaps in techniques and promote discussions on potential solutions. With the advancement of various AM technologies, it becomes imperative to establish clear guidelines and standards for the development of 3D-printed scaffolds and their clinical applications. The results of studies already conducted and those currently in progress will play a crucial role in defining these guidelines and will contribute towards more predictable and personalized medical and dental care.
References
- Wang, W.; Yeung, K. W. J. B. m., Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact Mater. 2017, 2, (4), 224-247. [CrossRef]
- Damien, C. J.; Parsons, J. R. J. J. o. A. B., Bone graft and bone graft substitutes: a review of current technology and applications. J Appl Biomater. 1991, 2, (3), 187-208. [CrossRef]
- Haugen, H. J.; Lyngstadaas, S. P.; Rossi, F.; Perale, G. J. J. o. c. p., Bone grafts: which is the ideal biomaterial? J Clin Periodontol. 2019, 46, 92-102.
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. J. B. r., Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: a review. Biomater Res. 2017, 21, (1), 9. [CrossRef]
- Sheikh, Z.; Sima, C.; Glogauer, M., Bone Replacement Materials and Techniques Used for Achieving Vertical Alveolar Bone Augmentation. Materials 2015, 8, (6), 2953-2993. [CrossRef]
- Ribas, R. G.; Schatkoski, V. M.; do Amaral Montanheiro, T. L.; de Menezes, B. R. C.; Stegemann, C.; Leite, D. M. G.; Thim, G. P. J. C. I., Current advances in bone tissue engineering concerning ceramic and bioglass scaffolds: A review. Ceramics International 2019, 45, (17), 21051-21061. [CrossRef]
- Gokyer, S.; Yilgor, E.; Yilgor, I.; Berber, E.; Vrana, E.; Orhan, K.; Monsef, Y. A.; Guvener, O.; Zinnuroglu, M.; Oto, C. J. A. B. S.; Engineering, 3D printed biodegradable polyurethaneurea elastomer recapitulates skeletal muscle structure and function. ACS Biomater Sci Eng. 2021, 7, (11), 5189-5205. [CrossRef]
- Zadpoor, A. A. J. B. s., Bone tissue regeneration: the role of scaffold geometry. Biomater Sci. 2015, 3, (2), 231-245. [CrossRef]
- Sheikh, Z.; Zhang, Y. L.; Tamimi, F.; Barralet, J., Effect of processing conditions of dicalcium phosphate cements on graft resorption and bone formation. Acta Biomaterialia 2017. [CrossRef]
- Tamimi, F.; Sheikh, Z.; Barralet, J., Dicalcium phosphate cements: brushite and monetite. Acta Biomater 2012, 8, (2), 474-87. [CrossRef]
- Tamimi, F.; Le Nihouannen, D.; Eimar, H.; Sheikh, Z.; Komarova, S.; Barralet, J., The effect of autoclaving on the physical and biological properties of dicalcium phosphate dihydrate bioceramics: brushite vs. monetite. Acta Biomater 2012, 8, (8), 3161-9. [CrossRef]
- Peltola, S. M.; Melchels, F. P.; Grijpma, D. W.; Kellomäki, M. J. A. o. m., A review of rapid prototyping techniques for tissue engineering purposes. Annals of Medicine 2008, 40, (4), 268-280. [CrossRef]
- Fahmy, M. D.; Jazayeri, H. E.; Razavi, M.; Masri, R.; Tayebi, L., Three-dimensional bioprinting materials with potential application in preprosthetic surgery. Journal of Prosthodontics 2016, 25, (4), 310-318. [CrossRef]
- Nyberg, E. L.; Farris, A. L.; Hung, B. P.; Dias, M.; Garcia, J. R.; Dorafshar, A. H.; Grayson, W. L., 3D-printing technologies for craniofacial rehabilitation, reconstruction, and regeneration. Annals of biomedical engineering 2017, 45, 45-57. [CrossRef]
- Hull, C. W., Apparatus for production of three-dimensional objects by stereolithography. United States Patent, Appl., No. 638905, Filed 1984.
- Kruth, J.-P., Material incress manufacturing by rapid prototyping techniques. CIRP annals 1991, 40, (2), 603-614. [CrossRef]
- Yan, Q.; Dong, H.; Su, J.; Han, J.; Song, B.; Wei, Q.; Shi, Y., A review of 3D printing technology for medical applications. Engineering 2018, 4, (5), 729-742. [CrossRef]
- Obregon, F.; Vaquette, C.; Ivanovski, S.; Hutmacher, D.; Bertassoni, L., Three-dimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. Journal of dental research 2015, 94, (9_suppl), 143S-152S. [CrossRef]
- Witek, L.; Alifarag, A. M.; Tovar, N.; Lopez, C. D.; Cronstein, B. N.; Rodriguez, E. D.; Coelho, P. G., Repair of critical-sized long bone defects using dipyridamole-augmented 3D-printed bioactive ceramic scaffolds. Journal of Orthopaedic Research® 2019, 37, (12), 2499-2507.
- DeMitchell-Rodriguez, E. M.; Shen, C.; Nayak, V. V.; Tovar, N.; Witek, L.; Torroni, A.; Yarholar, L. M.; Cronstein, B. N.; Flores, R. L.; Coelho, P. G., Bone Tissue Engineering in the Growing Calvaria: A 3D Printed Bioceramic Scaffold to Reconstruct Critical-Sized Defects in a Skeletally Immature Pig Model. Plastic and Reconstructive Surgery 2023, 10.1097.
- Nayak, V. V.; Slavin, B.; Bergamo, E. T.; Boczar, D.; Slavin, B. R.; Runyan, C. M.; Tovar, N.; Witek, L.; Coelho, P. G., Bone Tissue Engineering (BTE) of the Craniofacial Skeleton, Part I: Evolution and Optimization of 3D-Printed Scaffolds for Repair of Defects. The Journal of craniofacial surgery. [CrossRef]
- Trombetta, R.; Inzana, J. A.; Schwarz, E. M.; Kates, S. L.; Awad, H. A. J. A. o. b. e., 3D printing of calcium phosphate ceramics for bone tissue engineering and drug delivery. Ann Biomed Eng. 2017, 45, 23-44. [CrossRef]
- Budharaju, H.; Zennifer, A.; Sethuraman, S.; Paul, A.; Sundaramurthi, D. J. M. H., Designer DNA biomolecules as a defined biomaterial for 3D bioprinting applications. Mater Horiz. 2022, 9, (4), 1141-1166. [CrossRef]
- Budharaju, H.; Suresh, S.; Sekar, M. P.; De Vega, B.; Sethuraman, S.; Sundaramurthi, D.; Kalaskar, D. M. J. M.; Design, Ceramic Materials for 3D Printing of Biomimetic Bone Scaffolds–Current state–of–the–art & Future Perspectives. Materials & Design 2023, 112064.
- Lin, K.; Sheikh, R.; Romanazzo, S.; Roohani, I., 3D Printing of Bioceramic Scaffolds—Barriers to the Clinical Translation: From Promise to Reality, and Future Perspectives. Materials 2019, 12, (17), 2660. [CrossRef]
- Sarkar, R.; Banerjee, G., Ceramic based bio-medical implants. Interceram 2010, 59, (2), 98-102.
- Woodard, J. R.; Hilldore, A. J.; Lan, S. K.; Park, C.; Morgan, A. W.; Eurell, J. A. C.; Clark, S. G.; Wheeler, M. B.; Jamison, R. D.; Johnson, A. J. W., The mechanical properties and osteoconductivity of hydroxyapatite bone scaffolds with multi-scale porosity. Biomaterials 2007, 28, (1), 45-54. [CrossRef]
- Roberts, T. T.; Rosenbaum, A. J. J. O., Bone grafts, bone substitutes and orthobiologics: the bridge between basic science and clinical advancements in fracture healing. Organogenesis 2012, 8, (4), 114-124.
- Eliaz, N.; Metoki, N. J. M., Calcium phosphate bioceramics: a review of their history, structure, properties, coating technologies and biomedical applications. Materials (Basel). 2017, 10, (4), 334. [CrossRef]
- Kim, H. W.; Lee, E. J.; Jun, I. K.; Kim, H. E.; Knowles, J. C., Degradation and drug release of phosphate glass/polycaprolactone biological composites for hard-tissue regeneration. J Biomed Mater Res B Appl Biomater. 2005, 75, (1), 34-41. [CrossRef]
- Hench, L. L., Bioceramics: from concept to clinic. Journal of the american ceramic society 1991, 74, (7), 1487-1510.
- Tevlin, R.; McArdle, A.; Atashroo, D.; Walmsley, G.; Senarath-Yapa, K.; Zielins, E.; Paik, K.; Longaker, M.; Wan, D., Biomaterials for craniofacial bone engineering. Journal of dental research 2014, 93, (12), 1187-1195. [CrossRef]
- Polley, C.; Distler, T.; Detsch, R.; Lund, H.; Springer, A.; Boccaccini, A. R.; Seitz, H., 3D printing of piezoelectric barium titanate-hydroxyapatite scaffolds with interconnected porosity for bone tissue engineering. Materials 2020, 13, (7), 1773. [CrossRef]
- Aboushelib, M. N.; Shawky, R., Osteogenesis ability of CAD/CAM porous zirconia scaffolds enriched with nano-hydroxyapatite particles. International Journal of Implant Dentistry 2017, 3, (1), 1-6. [CrossRef]
- Muralithran, G.; Ramesh, S., The effects of sintering temperature on the properties of hydroxyapatite. Ceramics International 2000, 26, (2), 221-230. [CrossRef]
- Lee, D. K.; Ki, M.-R.; Kim, E. H.; Park, C.-J.; Ryu, J. J.; Jang, H. S.; Pack, S. P.; Jo, Y. K.; Jun, S. H., Biosilicated collagen/β-tricalcium phosphate composites as a BMP-2-delivering bone-graft substitute for accelerated craniofacial bone regeneration. Biomaterials Research 2021, 25, 1-11. [CrossRef]
- Khiri, M. Z. A.; Matori, K. A.; Zaid, M. H. M.; Abdullah, C. A. C.; Zainuddin, N.; Alibe, I. M.; Rahman, N. A. A.; Wahab, S. A. A.; Azman, A. Z. K.; Effendy, N., Crystallization behavior of low-cost biphasic hydroxyapatite/β-tricalcium phosphate ceramic at high sintering temperatures derived from high potential calcium waste sources. Results in Physics 2019, 12, 638-644. [CrossRef]
- Bohner, M.; Santoni, B. L. G.; Döbelin, N., β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta biomaterialia 2020, 113, 23-41. [CrossRef]
- Li, H.; Xue, K.; Kong, N.; Liu, K.; Chang, J., Silicate bioceramics enhanced vascularization and osteogenesis through stimulating interactions between endothelia cells and bone marrow stromal cells. Biomaterials 2014, 35, (12), 3803-3818. [CrossRef]
- Mei, H.; Yin, X.; Zhang, J.; Zhao, W., Compressive properties of 3D printed polylactic acid matrix composites reinforced by short fibers and SiC nanowires. Advanced Engineering Materials 2019, 21, (5), 1800539. [CrossRef]
- Petousis, M.; Vidakis, N.; Mountakis, N.; Grammatikos, S.; Papadakis, V.; David, C. N.; Moutsopoulou, A.; Das, S. C., Silicon carbide nanoparticles as a mechanical boosting agent in material extrusion 3D-printed polycarbonate. Polymers 2022, 14, (17), 3492. [CrossRef]
- Sailer, I.; Balmer, M.; Hüsler, J.; Hämmerle, C. H. F.; Känel, S.; Thoma, D. S., 10-year randomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dental prostheses. Journal of Dentistry 2018, 76, 32-39. [CrossRef]
- Guess, P. C.; Bonfante, E. A.; Silva, N. R.; Coelho, P. G.; Thompson, V. P., Effect of core design and veneering technique on damage and reliability of Y-TZP-supported crowns. Dental materials : official publication of the Academy of Dental Materials 2013, 29, (3), 307-16. [CrossRef]
- Naghib-zadeh, H.; Glitzky, C.; Dörfel, I.; Rabe, T., Low temperature sintering of barium titanate ceramics assisted by addition of lithium fluoride-containing sintering additives. Journal of the European Ceramic Society 2010, 30, (1), 81-86. [CrossRef]
- Ulfa, U.; Kusumandari, K.; Iriani, Y. In The effect of temperature and holding time sintering process on microstructure and dielectric properties of barium titanate by co-precipitation method, AIP Conference Proceedings, 2019; AIP Publishing.
- Klein, C. P.; Driessen, A. A.; de Groot, K.; van den Hooff, A., Biodegradation behavior of various calcium phosphate materials in bone tissue. J Biomed Mater Res 1983, 17, (5), 769-84. [CrossRef]
- Lowe, B.; Hardy, J. G.; Walsh, L. J. J. A. o., Optimizing nanohydroxyapatite nanocomposites for bone tissue engineering. ACS Omega 2019, 5, (1), 1-9. [CrossRef]
- Roopavath, U. K.; Malferrari, S.; Van Haver, A.; Verstreken, F.; Rath, S. N.; Kalaskar, D. M. J. M.; Design, Optimization of extrusion based ceramic 3D printing process for complex bony designs. Materials & Design 2019, 162, 263-270. [CrossRef]
- Moore, W. R.; Graves, S. E.; Bain, G. I., Synthetic bone graft substitutes. ANZ journal of surgery 2001, 71, (6), 354-61.
- Janus, A. M.; Faryna, M.; Haberko, K.; Rakowska, A.; Panz, T. J. M. A., Chemical and microstructural characterization of natural hydroxyapatite derived from pig bones. Microchimica Acta 2008, 161, 349-353. [CrossRef]
- Ooi, C.; Hamdi, M.; Ramesh, S. J. C. i., Properties of hydroxyapatite produced by annealing of bovine bone. Ceramics International 2007, 33, (7), 1171-1177. [CrossRef]
- Pon-On, W.; Suntornsaratoon, P.; Charoenphandhu, N.; Thongbunchoo, J.; Krishnamra, N.; Tang, I. M. J. M. S.; C, E., Hydroxyapatite from fish scale for potential use as bone scaffold or regenerative material. Mater Sci Eng C Mater Biol Appl. 2016, 62, 183-189. [CrossRef]
- Mondal, S.; Pal, U.; Dey, A. J. C. I., Natural origin hydroxyapatite scaffold as potential bone tissue engineering substitute. Ceramics International 2016, 42, (16), 18338-18346. [CrossRef]
- Chen, W.; Nichols, L.; Brinkley, F.; Bohna, K.; Tian, W.; Priddy, M. W.; Priddy, L. B. J. M. S.; C, E., Alkali treatment facilitates functional nano-hydroxyapatite coating of 3D printed polylactic acid scaffolds. Mater Sci Eng C Mater Biol Appl. 2021, 120, 111686. [CrossRef]
- Bohner, M.; Santoni, B. L. G.; Döbelin, N. J. A. b., β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23-41. [CrossRef]
- Sulaiman, S. B.; Keong, T. K.; Cheng, C. H.; Saim, A. B.; Idrus, R. B. H. J. T. I. j. o. m. r., Tricalcium phosphate/hydroxyapatite (TCP-HA) bone scaffold as potential candidate for the formation of tissue engineered bone. Indian J Med Res. 2013, 137, (6), 1093.
- Metsger, D. S.; Driskell, T.; Paulsrud, J. J. J. o. t. A. D. A., Tricalcium phosphate ceramic--a resorbable bone implant: review and current status. J Am Dent Assoc. 1982, 105, (6), 1035-1038. [CrossRef]
- Shen, C.; Witek, L.; Flores, R. L.; Tovar, N.; Torroni, A.; Coelho, P. G.; Kasper, F. K.; Wong, M.; Young, S., Three-Dimensional Printing for Craniofacial Bone Tissue Engineering. Tissue engineering. Part A 2020, 26, (23-24), 1303-1311. [CrossRef]
- Lopez, C. D.; Diaz-Siso, J. R.; Witek, L.; Bekisz, J. M.; Cronstein, B. N.; Torroni, A.; Flores, R. L.; Rodriguez, E. D.; Coelho, P. G., Three dimensionally printed bioactive ceramic scaffold osseoconduction across critical-sized mandibular defects. J Surg Res 2018, 223, 115-122. [CrossRef]
- Ma, H.; Feng, C.; Chang, J.; Wu, C., 3D-printed bioceramic scaffolds: From bone tissue engineering to tumor therapy. Acta biomaterialia 2018, 79, 37-59. [CrossRef]
- González, P.; Borrajo, J. P.; Serra, J.; Liste, S.; Chiussi, S.; León, B.; Semmelmann, K.; de Carlos, A.; Varela-Feria, F. M.; Martínez-Fernández, J. J. K. E. M., Extensive studies on biomorphic SiC ceramics properties for medical applications. Bioceramics 2004, 254, 1029-1032. [CrossRef]
- Visbal, S.; Lira-Olivares, J.; Sekino, T.; Niihara, K.; Moon, B. K.; Lee, S. W. In Mechanical properties of Al2O3-TiO2-SiC nanocomposites for the femoral head of hip joint replacement, Materials Science Forum, 2005; Trans Tech Publ: pp 197-200. [CrossRef]
- Li, H.; Xue, K.; Kong, N.; Liu, K.; Chang, J. J. B., Silicate bioceramics enhanced vascularization and osteogenesis through stimulating interactions between endothelia cells and bone marrow stromal cells. Biomaterials 2014, 35, (12), 3803-3818. [CrossRef]
- Liu, W.; Li, Q.; Yang, X.; Chen, X.; Xu, X. J. C., Synthesis and characterization of N-doped SiC powder with enhanced photocatalytic and photoelectrochemical performance. Catalysts 2020, 10, (7), 769. [CrossRef]
- Ma, Z.; Li, J.; Cao, F.; Yang, J.; Liu, R.; Zhao, D. J. R. B., Porous silicon carbide coated with tantalum as potential material for bone implants. Regen Biomater. 2020, 7, (5), 453-459. [CrossRef]
- Abderrazak, H.; Hmida, E. J. P.; Carbide, a. o. S., Silicon carbide: synthesis and properties. 2011, 361-388.
- Garvie, R. C.; Hannink, R. H.; Pascoe, R. T., Ceramic steel? Nature 1975, 258, (5537), 703-704.
- Zhang, Y.; Lawn, B. R., Novel Zirconia Materials in Dentistry. Journal of dental research 2018, 97, (2), 140-147. [CrossRef]
- Gupta, T. K.; Lange, F. F.; Bechtold, J. H., Effect of stress-induced phase transformation on the properties of polycrystalline zirconia containing metastable tetragonal phase. Journal of Materials Science 1978, 13, (7), 1464-1470. [CrossRef]
- Chevalier, J.; Calès, B.; Drouin, J. M. J. J. o. t. A. C. S., Low-Temperature Aging of Y-TZP Ceramics. Journal of the American Ceramic Society 2004, 82, 2150-2154.
- Wang, Q.; Ma, Z.; Wang, Y.; Zhong, L.; Xie, W., Fabrication and characterization of 3D printed biocomposite scaffolds based on PCL and zirconia nanoparticles. Bio-Design and Manufacturing 2021, 4, (1), 60-71. [CrossRef]
- Fu, S.; Liu, W.; Liu, S.; Zhao, S.; Zhu, Y., 3D printed porous β-Ca(2)SiO(4) scaffolds derived from preceramic resin and their physicochemical and biological properties. Science and technology of advanced materials 2018, 19, (1), 495-506.
- Sakthiabirami, K.; Kang, J.-H.; Jang, J.-G.; Soundharrajan, V.; Lim, H.-P.; Yun, K.-D.; Park, C.; Lee, B.-N.; Yang, Y. P.; Park, S.-W., Hybrid porous zirconia scaffolds fabricated using additive manufacturing for bone tissue engineering applications. Materials Science and Engineering: C 2021, 123, 111950. [CrossRef]
- Zhang, X.; Wu, X.; Shi, J., Additive manufacturing of zirconia ceramics: a state-of-the-art review. Journal of Materials Research and Technology 2020, 9, (4), 9029-9048. [CrossRef]
- Li, Y.-y.; Li, L.-t.; Li, B., Direct write printing of three-dimensional ZrO2 biological scaffolds. Materials & Design 2015, 72, 16-20. [CrossRef]
- Al-Radha, A. S. D.; Dymock, D.; Younes, C.; O’Sullivan, D., Surface properties of titanium and zirconia dental implant materials and their effect on bacterial adhesion. Journal of dentistry 2012, 40, (2), 146-153. [CrossRef]
- Cerrolaza, M.; Duarte, V.; Garzón-Alvarado, D. J. J. o. B. E., Analysis of bone remodeling under piezoelectricity effects using boundary elements. Journal of Bionic Engineering 2017, 14, (4), 659-671. [CrossRef]
- Jacob, J.; More, N.; Kalia, K.; Kapusetti, G. J. I.; regeneration, Piezoelectric smart biomaterials for bone and cartilage tissue engineering. Inflamm Regen 2018, 38, (1), 2. [CrossRef]
- Ismail, F. A.; Osman, R. A. M.; Idris, M. S.; Taking, S.; Jamal, Z. A. Z. In Dielectric and microstructural properties of BaTiO3 and Ba0. 9925Er0. 0075TiO3 ceramics, EPJ Web of Conferences, 2017; EDP Sciences: p 01051.
- Rocca, A.; Marino, A.; Rocca, V.; Moscato, S.; de Vito, G.; Piazza, V.; Mazzolai, B.; Mattoli, V.; Ngo-Anh, T. J.; Ciofani, G. J. I. J. o. N., Barium titanate nanoparticles and hypergravity stimulation improve differentiation of mesenchymal stem cells into osteoblasts. Int J Nanomedicine. 2015, 433-445. [CrossRef]
- Zhou, Z.-j.; Yang, Z.-f.; Yuan, Q.-m. J. T. o. N. M. S. o. C., Barium titanate ceramic inks for continuous ink-jet printing synthesized by mechanical mixing and sol-gel methods. Trans. Nonferrous Met. Soc. China 2008, 18, (1), 150-154. [CrossRef]
- Zarkoob, H.; Ziaei-Rad, S.; Fathi, M.; Dadkhah, H. J. A. e. m., Synthesis, characterization and bioactivity evaluation of porous barium titanate with nanostructured hydroxyapatite coating for biomedical application. Advanced Engineering Materials 2012, 14, (6), B322-B329. [CrossRef]
- Vella, J. B., Trombetta, R. P., Hoffman, M. D., Inzana, J., Awad, H., & Benoit, D. S. W. (2018). Three dimensional printed calcium phosphate and poly(caprolactone) composites with improved mechanical properties and preserved microstructure. Journal of biomedical materials research. Part A, 106(3), 663–672. [CrossRef]
- Baker, R. M.; Tseng, L. F.; Iannolo, M. T.; Oest, M. E.; Henderson, J. H., Self-deploying shape memory polymer scaffolds for grafting and stabilizing complex bone defects: A mouse femoral segmental defect study. Biomaterials 2016, 76, 388-98. [CrossRef]
- Shah, S. R.; Kasper, F. K.; Mikos, A. G., Perspectives on the prevention and treatment of infection for orthopedic tissue engineering applications. Chinese Science Bulletin 2013, 58, (35), 4342-4348. [CrossRef]
- Shim, J.-H.; Won, J.-Y.; Sung, S.-J.; Lim, D.-H.; Yun, W.-S.; Jeon, Y.-C.; Huh, J.-B., Comparative efficacies of a 3D-printed PCL/PLGA/β-TCP membrane and a titanium membrane for guided bone regeneration in beagle dogs. Polymers 2015, 7, (10), 2061-2077. [CrossRef]
- Won, J. Y.; Park, C. Y.; Bae, J. H.; Ahn, G.; Kim, C.; Lim, D. H.; Cho, D. W.; Yun, W. S.; Shim, J. H.; Huh, J. B., Evaluation of 3D printed PCL/PLGA/beta-TCP versus collagen membranes for guided bone regeneration in a beagle implant model. Biomed Mater 2016, 11, (5), 055013.
- Senatov, F. S.; Niaza, K. V.; Zadorozhnyy, M. Y.; Maksimkin, A. V.; Kaloshkin, S. D.; Estrin, Y. Z., Mechanical properties and shape memory effect of 3D-printed PLA-based porous scaffolds. J Mech Behav Biomed Mater 2016, 57, 139-48. [CrossRef]
- Senatov, F. S.; Zadorozhnyy, M. Y.; Niaza, K. V.; Medvedev, V. V.; Kaloshkin, S. D.; Anisimova, N. Y.; Kiselevskiy, M. V.; Yang, K.-C., Shape memory effect in 3D-printed scaffolds for self-fitting implants. European Polymer Journal 2017, 93, 222-231. [CrossRef]
- Zhang, D.; George, O. J.; Petersen, K. M.; Jimenez-Vergara, A. C.; Hahn, M. S.; Grunlan, M. A., A bioactive “self-fitting” shape memory polymer scaffold with potential to treat cranio-maxillo facial bone defects. Acta Biomater 2014, 10, (11), 4597-4605. [CrossRef]
- Shuai, C.; Yu, L.; Feng, P.; Gao, C.; Peng, S., Interfacial reinforcement in bioceramic/biopolymer composite bone scaffold: The role of coupling agent. Colloids Surf B Biointerfaces 2020, 193, 111083. [CrossRef]
- Hou, S.; Bao, C.; Zhang, Z.; Bai, Y., Microstructure and Wear Behavior of High-Cr WCI Matrix Surface Composite Reinforced with Cemented Carbide Rods. Journal of Materials Engineering and Performance 2013, 22, (7), 2064-2072. [CrossRef]
- Johnson, A. C.; Hayes, S. A.; Jones, F. R., An improved model including plasticity for the prediction of the stress in fibres with an interface/interphase region. Composites Part A: Applied Science and Manufacturing 2005, 36, (2), 263-271.
- Zhang, P.; Hong, Z.; Yu, T.; Chen, X.; Jing, X., In vivo mineralization and osteogenesis of nanocomposite scaffold of poly(lactide-co-glycolide) and hydroxyapatite surface-grafted with poly(l-lactide). Biomaterials 2009, 30, (1), 58-70. [CrossRef]
- Cui, Y.; Liu, Y.; Cui, Y.; Jing, X.; Zhang, P.; Chen, X., The nanocomposite scaffold of poly(lactide-co-glycolide) and hydroxyapatite surface-grafted with l-lactic acid oligomer for bone repair. Acta Biomaterialia 2009, 5, (7), 2680-2692. [CrossRef]
- Kharaziha, M.; Fathi, M. H.; Edris, H., Effects of surface modification on the mechanical and structural properties of nanofibrous poly(ε-caprolactone)/forsterite scaffold for tissue engineering applications. Materials Science and Engineering: C 2013, 33, (8), 4512-4519.
- Tham, W. L.; Chow, W. S.; Mohd Ishak, Z. A., Effects of titanate coupling agent on the mechanical, thermal, and morphological properties of poly(methyl methacrylate)/hydroxyapatite denture base composites. Journal of Composite Materials 2011, 45, (22), 2335-2345.
- Lopez, C. D.; Witek, L.; Torroni, A.; Flores, R. L.; Demissie, D. B.; Young, S.; Cronstein, B. N.; Coelho, P. G., The role of 3D printing in treating craniomaxillofacial congenital anomalies. Birth Defects Research 2018, 110, (13), 1055-1064. [CrossRef]
- Kamboj, N.; Ressler, A.; Hussainova, I. J. M., Bioactive ceramic scaffolds for bone tissue engineering by powder bed selective laser processing: A review. Materials (Basel) 2021, 14, (18), 5338. [CrossRef]
- Bose, S.; Vahabzadeh, S.; Bandyopadhyay, A. J. M. t., Bone tissue engineering using 3D printing. Materials Today 2013, 16, (12), 496-504. [CrossRef]
- Gmeiner, R.; Deisinger, U.; Schönherr, J.; Lechner, B.; Detsch, R.; Boccaccini, A.; Stampfl, J. J. J. C. S. T., Additive manufacturing of bioactive glasses and silicate bioceramics. Journal of Ceramic Science and Technology 2015, 6, (2), 75-86.
- Seunarine, K.; Gadegaard, N.; Tormen, M.; Meredith, D.; Riehle, M.; Wilkinson, C., 3D polymer scaffolds for tissue engineering. Nanomedicine 2006. [CrossRef]
- de Hazan, Y.; Penner, D. J. J. o. t. E. C. S., SiC and SiOC ceramic articles produced by stereolithography of acrylate modified polycarbosilane systems. Journal of the European Ceramic Society 2017, 37, (16), 5205-5212. [CrossRef]
- Gentry, S. P.; Halloran, J. W. J. J. o. t. E. C. S., Depth and width of cured lines in photopolymerizable ceramic suspensions. Journal of the European Ceramic Society 2013, 33, (10), 1981-1988. [CrossRef]
- Mitteramskogler, G.; Gmeiner, R.; Felzmann, R.; Gruber, S.; Hofstetter, C.; Stampfl, J.; Ebert, J.; Wachter, W.; Laubersheimer, J. J. A. M., Light curing strategies for lithography-based additive manufacturing of customized ceramics. Additive Manufacturing 2014, 1, 110-118. [CrossRef]
- Pfaffinger, M.; Mitteramskogler, G.; Gmeiner, R.; Stampfl, J. In Thermal debinding of ceramic-filled photopolymers, Materials Science Forum 2015; Trans Tech Publ: pp 75-81.
- Chaudhary, R.; Fabbri, P.; Leoni, E.; Mazzanti, F.; Akbari, R.; Antonini, C. J. P. i. A. M., Additive manufacturing by digital light processing: a review. Progress in Additive Manufacturing 2023, 8, (2), 331-351. [CrossRef]
- Maroulakos, M.; Kamperos, G.; Tayebi, L.; Halazonetis, D.; Ren, Y., Applications of 3D printing on craniofacial bone repair: A systematic review. Journal of Dentistry 2019, 80, 1-14. [CrossRef]
- Kinoshita, Y.; Maeda, H. J. T. S. W. J., Recent developments of functional scaffolds for craniomaxillofacial bone tissue engineering applications. Scientific World Journal 2013, 2013. [CrossRef]
- Zhang, Z., Bone regeneration by stem cell and tissue engineering in oral and maxillofacial region. Frontiers of medicine 2011, 5, (4), 401-413. [CrossRef]
- Silva, N. R.; Witek, L.; Coelho, P. G.; Thompson, V. P.; Rekow, E. D.; Smay, J., Additive CAD/CAM process for dental prostheses. J Prosthodont 2011, 20, (2), 93-6. [CrossRef]
- Witek, L.; Colon, R. R.; Wang, M. M.; Torroni, A.; Young, S.; Melville, J.; Lopez, C. D.; Flores, R. L.; Cronstein, B. N.; Coelho, P. G., Tissue-engineered alloplastic scaffolds for reconstruction of alveolar defects. In Handbook of Tissue Engineering Scaffolds: Volume One, Elsevier: 2019; pp 505-520.
- Bauermeister, A. J.; Zuriarrain, A.; Newman, M. I., Three-Dimensional Printing inPlastic and Reconstructive Surgery: A Systematic Review. Ann Plast Surg 2016, 77, (5), 569-576.
- Zhang, B.; Wang, L.; Song, P.; Pei, X.; Sun, H.; Wu, L.; Zhou, C.; Wang, K.; Fan, Y.; Zhang, X., 3D printed bone tissue regenerative PLA/HA scaffolds with comprehensive performance optimizations. Materials & Design 2021, 201, 109490. [CrossRef]
- Rahim, T. N. A. T.; Abdullah, A. M.; Md Akil, H., Recent developments in fused deposition modeling-based 3D printing of polymers and their composites. Polymer Reviews 2019, 59, (4), 589-624. [CrossRef]
- Yao, Y.; Qin, W.; Xing, B.; Sha, N.; Jiao, T.; Zhao, Z., High performance hydroxyapatite ceramics and a triply periodic minimum surface structure fabricated by digital light processing 3D printing. Journal of Advanced Ceramics 2021, 10, 39-48. [CrossRef]
- Ding, G.; He, R.; Zhang, K.; Zhou, N.; Xu, H., Stereolithography 3D printing of SiC ceramic with potential for lightweight optical mirror. Ceramics International 2020, 46, (11), 18785-18790. [CrossRef]
- Wu, H.; Cheng, Y.; Liu, W.; He, R.; Zhou, M.; Wu, S.; Song, X.; Chen, Y., Effect of the particle size and the debinding process on the density of alumina ceramics fabricated by 3D printing based on stereolithography. Ceramics International 2016, 42, (15), 17290-17294. [CrossRef]
- Chioibasu, D.; Achim, A.; Popescu, C.; Stan, G. E.; Pasuk, I.; Enculescu, M.; Iosub, S.; Duta, L.; Popescu, A., Prototype orthopedic bone plates 3D printed by laser melting deposition. Materials 2019, 12, (6), 906. [CrossRef]
- Lupone, F.; Padovano, E.; Pietroluongo, M.; Giudice, S.; Ostrovskaya, O.; Badini, C., Optimization of selective laser sintering process conditions using stable sintering region approach. Express Polymer Letters 2021, 15, (2). [CrossRef]
- Lee, H.; Yoo, J. M.; Nam, S. Y., Additive fabrication and characterization of biomimetic composite bone scaffolds with high hydroxyapatite content. Gels 2021, 7, (3), 100. [CrossRef]
- He, J.; Shao, H.; Lin, T., Effect of magnesium silicate on 3D gel-printing of hydroxyapatite ceramic composite scaffold. International Journal of Applied Ceramic Technology 2019, 16, (2), 494-502. [CrossRef]
- Ren, X.; Shao, H.; Lin, T.; Zheng, H., 3D gel-printing—An additive manufacturing method for producing complex shape parts. Materials & Design 2016, 101, 80-87. [CrossRef]
- Chen, Y.; Huang, J.; Liu, J.; Wei, Y.; Yang, X.; Lei, L.; Chen, L.; Wu, Y.; Gou, Z., Tuning filament composition and microstructure of 3D-printed bioceramic scaffolds facilitate bone defect regeneration and repair. Regenerative Biomaterials 2021, 8, (2), rbab007. [CrossRef]
- Li, F.; Ji, X.; Wu, Z.; Qi, C.; Xian, Q.; Sun, B., Digital light processing 3D printing of ceramic shell for precision casting. Materials Letters 2020, 276, 128037. [CrossRef]
- Reid, A.; Jackson, J. C.; Windmill, J., Voxel based method for predictive modelling of solidification and stress in digital light processing based additive manufacture. Soft Matter 2021, 17, (7), 1881-1887. [CrossRef]
- Wubneh, A.; Tsekoura, E. K.; Ayranci, C.; Uludağ, H. J. A. B., Current state of fabrication technologies and materials for bone tissue engineering. Acta Biomater. 2018, 80, 1-30. [CrossRef]
- Shivalkar, S.; Singh, S. J. T. e.; medicine, r., Solid freeform techniques application in bone tissue engineering for scaffold fabrication. Tissue Eng Regen Med. 2017, 14, 187-200. [CrossRef]
- Shirazi, S. F. S.; Gharehkhani, S.; Mehrali, M.; Yarmand, H.; Metselaar, H. S. C.; Kadri, N. A.; Osman, N. A. A. J. S.; materials, t. o. a., A review on powder-based additive manufacturing for tissue engineering: selective laser sintering and inkjet 3D printing. Sci Technol Adv Mater. 2015. [CrossRef]
- Drummer, D.; Rietzel, D.; Kühnlein, F. J. P. P., Development of a characterization approach for the sintering behavior of new thermoplastics for selective laser sintering. Physics Procedia 2010, 5, 533-542. [CrossRef]
- Shahzad, K.; Deckers, J.; Zhang, Z.; Kruth, J.-P.; Vleugels, J. J. J. o. t. E. C. S., Additive manufacturing of zirconia parts by indirect selective laser sintering. ournal of The European Ceramic Society 2014, 34, (1), 81-89. [CrossRef]
- Bakshi, K.; Mulay, A. J. I. J. M. C. E., A review on selective laser sintering: A rapid prototyping technology. IOSR Journal of Mechanical and Civil Engineering 2016, 4, (4), 53-57.
- Kolan, K. C.; Leu, M. C.; Hilmas, G. E.; Velez, M. J. J. o. t. m. b. o. b. m., Effect of material, process parameters, and simulated body fluids on mechanical properties of 13-93 bioactive glass porous constructs made by selective laser sintering. J Mech Behav Biomed Mater. 2012, 13, 14-24. [CrossRef]
- Lin, K.; Sheikh, R.; Romanazzo, S.; Roohani, I. J. M., 3D printing of bioceramic scaffolds—Barriers to the clinical translation: From promise to reality, and future perspectives. Materials (Basel). 2019, 12, (17), 2660. [CrossRef]
- Yves-Christian, H.; Jan, W.; Wilhelm, M.; Konrad, W.; Reinhart, P. J. P. P., Net shaped high performance oxide ceramic parts by selective laser melting. Physics Procedia 2010, 5, 587-594. [CrossRef]
- López-Álvarez, M.; Rodríguez-Valencia, C.; Serra, J.; González, P. J. P. E., Bio-inspired ceramics: promising scaffolds for bone tissue engineering. Procedia Engineering 2013, 59, 51-58. [CrossRef]
- Sarment, D. P.; Sukovic, P.; Clinthorne, N. J. I. J. o. O.; Implants, M., Accuracy of implant placement with a stereolithographic surgical guide. Int J Oral Maxillofac Implants. 2003, 18, (4).
- Hull, C. W. J. U. S. P., Appl., No. 638905, Filed, Apparatus for production of three-dimensional objects by stereolithography. 1984.
- Schmidleithner, C.; Kalaskar, D. M., Stereolithography. IntechOpen: 2018.
- Bártolo, P. J., Stereolithography: materials, processes and applications. Springer Science & Business Media: 2011.
- Allen Brady, G.; Halloran, J. W. J. R. P. J., Stereolithography of ceramic suspensions. Rapid Prototyping Journal 1997, 3, (2), 61-65. [CrossRef]
- Hinczewski, C.; Corbel, S.; Chartier, T. J. J. o. t. E. C. S., Ceramic suspensions suitable for stereolithography. Journal of the European Ceramic Society 1998, 18, (6), 583-590. [CrossRef]
- Skoog, S. A.; Goering, P. L.; Narayan, R. J. J. J. o. M. S. M. i. M., Stereolithography in tissue engineering. J Mater Sci Mater Med. 2014, 25, 845-856. [CrossRef]
- Chen, Z.; Li, D.; Zhou, W. J. P. o. t. I. o. M. E., Part B: Journal of Engineering Manufacture, Process parameters appraisal of fabricating ceramic parts based on stereolithography using the Taguchi method. Journal of Advanced Ceramics 2012, 226, (7), 1249-1258. [CrossRef]
- Schmidleithner, C.; Malferrari, S.; Palgrave, R.; Bomze, D.; Schwentenwein, M.; Kalaskar, D. M. J. B. M., Application of high resolution DLP stereolithography for fabrication of tricalcium phosphate scaffolds for bone regeneration. Biomed Mater. 2019, 14, (4), 045018. [CrossRef]
- Li, F.; Ji, X.; Wu, Z.; Qi, C.; Xian, Q.; Sun, B. J. M. L., Digital light processing 3D printing of ceramic shell for precision casting. Materials Letters 2020, 276, 128037. [CrossRef]
- Mu, Q.; Wang, L.; Dunn, C. K.; Kuang, X.; Duan, F.; Zhang, Z.; Qi, H. J.; Wang, T., Digital light processing 3D printing of conductive complex structures. Additive Manufacturing 2017, 18, 74-83. [CrossRef]
- Wang, Y.; Chen, S.; Liang, H.; Liu, Y.; Bai, J.; Wang, M. J. C. I., Digital light processing (DLP) of nano biphasic calcium phosphate bioceramic for making bone tissue engineering scaffolds. Ceramics International 2022, 48, (19), 27681-27692. [CrossRef]
- Feng, C.; Zhang, K.; He, R.; Ding, G.; Xia, M.; Jin, X.; Xie, C. J. J. o. A. C., Additive manufacturing of hydroxyapatite bioceramic scaffolds: Dispersion, digital light processing, sintering, mechanical properties, and biocompatibility. Journal of Advanced Ceramics 2020, 9, 360-373. [CrossRef]
- Liu, Z.; Liang, H.; Shi, T.; Xie, D.; Chen, R.; Han, X.; Shen, L.; Wang, C.; Tian, Z. J. C. I., Additive manufacturing of hydroxyapatite bone scaffolds via digital light processing and in vitro compatibility. Ceramics International 2019, 45, (8), 11079-11086. [CrossRef]
- Zeng, Y.; Yan, Y.; Yan, H.; Liu, C.; Li, P.; Dong, P.; Zhao, Y.; Chen, J. J. J. o. m. s., 3D printing of hydroxyapatite scaffolds with good mechanical and biocompatible properties by digital light processing. Journal of Materials Science 2018, 53, (9), 6291-6301. [CrossRef]
- Kim, J.-W.; Lee, J.-B.; Koh, Y.-H.; Kim, H.-E., Digital Light Processing of Freeze-cast Ceramic Layers for Macroporous Calcium Phosphate Scaffolds with Tailored Microporous Frameworks. Materials 2019, 12, (18), 2893. [CrossRef]
- Schmidleithner, C.; Malferrari, S.; Palgrave, R.; Bomze, D.; Schwentenwein, M.; Kalaskar, D. M., Application of high resolution DLP stereolithography for fabrication of tricalcium phosphate scaffolds for bone regeneration. Biomedical Materials 2019, 14, (4), 045018. [CrossRef]
- Elsayed, H.; Colombo, P.; Bernardo, E., Direct ink writing of wollastonite-diopside glass-ceramic scaffolds from a silicone resin and engineered fillers. Journal of the European Ceramic Society 2017, 37, (13), 4187-4195. [CrossRef]
- Cesarano, J.; Segalman, R.; Calvert, P., Robocasting provides MOULDLESS fabrication from slurry deposition. Ceramic industry 1998, 148, (4), 94-96.
- Lewis, J. A., Direct ink writing of 3D functional materials. Advanced Functional Materials 2006, 16, (17), 2193-2204.
- Feilden, E.; Blanca, E. G.-T.; Giuliani, F.; Saiz, E.; Vandeperre, L., Robocasting of structural ceramic parts with hydrogel inks. Journal of the European Ceramic Society 2016, 36, (10), 2525-2533. [CrossRef]
- Three-Dimensional Printing Bioceramic Scaffolds Using Direct-Ink-Writing for Craniomaxillofacial Bone Regeneration. Tissue Eng Part C Methods .2023, 29, (7), 332-345.
- Lewis, J. A.; Smay, J. E.; Stuecker, J.; Cesarano, J., Direct Ink Writing of Three-Dimensional Ceramic Structures. Journal of the American Ceramic Society 2006, 89, (12), 3599-3609. [CrossRef]
- Miranda, P.; Saiz, E.; Gryn, K.; Tomsia, A. P., Sintering and robocasting of β-tricalcium phosphate scaffolds for orthopaedic applications. Acta biomaterialia 2006, 2, (4), 457-466. [CrossRef]
- Michna, S.; Wu, W.; Lewis, J. A., Concentrated hydroxyapatite inks for direct-write assembly of 3-D periodic scaffolds. Biomaterials 2005, 26, (28), 5632-5639. [CrossRef]
- Lewis, J. A., Colloidal processing of ceramics. Journal of the American Ceramic Society 2000, 83, (10), 2341-2359.
- Ashammakhi, N.; Hasan, A.; Kaarela, O.; Byambaa, B.; Sheikhi, A.; Gaharwar, A. K.; Khademhosseini, A. J. A. h. m., Advancing frontiers in bone bioprinting. Adv. Healthcare Mater. 2019, 8, (7), 1801048.
- Vikram Singh, A.; Gharat, T.; Batuwangala, M.; Park, B. W.; Endlein, T.; Sitti, M. J. J. o. B. M. R. P. B. A. B., Three-dimensional patterning in biomedicine: Importance and applications in neuropharmacology. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2018, 106, (3), 1369-1382. [CrossRef]
- Li, Q.; Lewis, J. A. J. A. M., Nanoparticle inks for directed assembly of three-dimensional periodic structures. Adv. Mater. 2003, 15, (19), 1639-1643. [CrossRef]
- Corcione, C. E.; Gervaso, F.; Scalera, F.; Padmanabhan, S. K.; Madaghiele, M.; Montagna, F.; Sannino, A.; Licciulli, A.; Maffezzoli, A. J. C. I., Highly loaded hydroxyapatite microsphere/PLA porous scaffolds obtained by fused deposition modelling. Ceramics International 2019, 45, (2), 2803-2810. [CrossRef]
- Kalita, S. J.; Bose, S.; Hosick, H. L.; Bandyopadhyay, A. J. M. S.; C, E., Development of controlled porosity polymer-ceramic composite scaffolds via fused deposition modeling. Materials Science and Engineering: C 2003, 23, (5), 611-620. [CrossRef]
- Janek, M.; Žilinská, V.; Kovár, V.; Hajdúchová, Z.; Tomanová, K.; Peciar, P.; Veteška, P.; Gabošová, T.; Fialka, R.; Feranc, J.; Omaníková, L.; Plavec, R.; Bača, Ľ., Mechanical testing of hydroxyapatite filaments for tissue scaffolds preparation by fused deposition of ceramics. Journal of the European Ceramic Society 2020, 40, (14), 4932-4938. [CrossRef]
- Chen, Z.; Li, Z.; Li, J.; Liu, C.; Lao, C.; Fu, Y.; Liu, C.; Li, Y.; Wang, P.; He, Y., 3D printing of ceramics: A review. Journal of the European Ceramic Society 2019, 39, (4), 661-687.
- Butscher, A.; Bohner, M.; Roth, C.; Ernstberger, A.; Heuberger, R.; Doebelin, N.; Von Rohr, P. R.; Müller, R. J. A. b., Printability of calcium phosphate powders for three-dimensional printing of tissue engineering scaffolds. Acta Biomater. 2012, 8, (1), 373-385. [CrossRef]
- Griffith, M. L.; Halloran, J. W. J. J. o. t. A. C. S., Freeform fabrication of ceramics via stereolithography. Journal of the American Ceramic Society 1996, 79, (10), 2601-2608. [CrossRef]
- Uhland, S. A.; Holman, R. K.; Morissette, S.; Cima, M. J.; Sachs, E. M. J. J. o. t. A. C. S., Strength of green ceramics with low binder content. Journal of the American Ceramic Society 2001, 84, (12), 2809-2818. [CrossRef]
- Leukers, B.; Gülkan, H.; Irsen, S.; Milz, S.; Tille, C.; Seitz, H.; Schieker, M. J. M. u. W. E., Fertigung, Prüfung, Eigenschaften und Anwendungen technischer Werkstoffe, Biocompatibility of ceramic scaffolds for bone replacement made by 3D printing. Mat.-wiss. u. Werkstofftech. 2005, 36, (12), 781-787. [CrossRef]
- Vaezi, M.; Seitz, H.; Yang, S. J. T. I. J. o. A. M. T., A review on 3D micro-additive manufacturing technologies. Int J Adv Manuf Technol. 2013, 67, 1721-1754. [CrossRef]
- Hwa, L. C.; Rajoo, S.; Noor, A. M.; Ahmad, N.; Uday, M. J. C. O. i. S. S.; Science, M., Recent advances in 3D printing of porous ceramics: A review. Current Opinion in Solid State & Materials Science 2017, 21, (6), 323-347. [CrossRef]
- Gbureck, U.; Hölzel, T.; Klammert, U.; Wuerzler, K.; Mueller, F. A.; Barralet, J. E. J. A. F. M., Resorbable dicalcium phosphate bone substitutes prepared by 3D powder printing. Adv. Funct. Mater. 2007, 17, (18), 3940-3945. [CrossRef]
- Agalloco, J. P.; Akers, J. E.; Madsen, R. E. J. P. J. o. P. S.; Technology, Moist heat sterilization—myths and realities. PDA J Pharm Sci Technol. 1998, 52, (6), 346-350.
- Rutala, W. A.; Weber, D. J., Infection control: the role of disinfection and sterilization. The Journal of hospital infection 1999, 43 Suppl, S43-55. [CrossRef]
- Rodriguez Colon, R.; Nayak, V. V.; Parente, P. E. L.; Leucht, P.; Tovar, N.; Lin, C. C.; Rezzadeh, K.; Hacquebord, J. H.; Coelho, P. G.; Witek, L., The presence of 3D printing in orthopedics: A clinical and material review. J Orthop Res. 2023, 41, (3), 601-613. [CrossRef]
- Melville, J. C.; Nassari, N. N.; Hanna, I. A.; Shum, J. W.; Wong, M. E.; Young, S., Immediate transoral allogeneic bone grafting for large mandibular defects. Less morbidity, more bone. A paradigm in benign tumor mandibular reconstruction? Journal of Oral and Maxillofacial Surgery 2017, 75, (4), 828-838.
- Melville, J. C.; Shum, J. W.; Young, S.; Wong, M. E., Regenerative strategies for maxillary and mandibular reconstruction: a practical guide. Springer: 2019.
- Jäger, M.; Herten, M.; Fochtmann, U.; Fischer, J.; Hernigou, P.; Zilkens, C.; Hendrich, C.; Krauspe, R., Bridging the gap: bone marrow aspiration concentrate reduces autologous bone grafting in osseous defects. Journal of Orthopaedic Research 2011, 29, (2), 173-180. [CrossRef]
- Aghaloo, T. L.; Hadaya, D., Basic principles of bioengineering and regeneration. Oral and Maxillofacial Surgery Clinics 2017, 29, (1), 1-7. [CrossRef]
- Chang, C.; Yan, J.; Yao, Z.; Zhang, C.; Li, X.; Mao, H. Q., Effects of Mesenchymal Stem Cell-Derived Paracrine Signals and Their Delivery Strategies. Advanced Healthcare Materials 2021, 10, (7), 2001689. [CrossRef]
- Wu, V.; Helder, M. N.; Bravenboer, N.; Ten Bruggenkate, C. M.; Jin, J.; Klein-Nulend, J.; Schulten, E. A., Bone tissue regeneration in the oral and maxillofacial region: a review on the application of stem cells and new strategies to improve vascularization. Stem Cells International 2019, 2019. [CrossRef]
- Jakobsen, C.; Sørensen, J.; Kassem, M.; Thygesen, T. J. J. o. O. R., Mesenchymal stem cells in oral reconstructive surgery: a systematic review of the literature. Journal of Oral Rehabilitation 2013, 40, (9), 693-706. [CrossRef]
- Pittenger, M. F.; Mackay, A. M.; Beck, S. C.; Jaiswal, R. K.; Douglas, R.; Mosca, J. D.; Moorman, M. A.; Simonetti, D. W.; Craig, S.; Marshak, D. R., Multilineage potential of adult human mesenchymal stem cells. Science (New York, N.Y.) 1999, 284, (5411), 143-7. [CrossRef]
- Wu, V.; Helder, M. N.; Bravenboer, N.; Ten Bruggenkate, C. M.; Jin, J.; Klein-Nulend, J.; Schulten, E. A. J. S. C. I., Bone tissue regeneration in the oral and maxillofacial region: a review on the application of stem cells and new strategies to improve vascularization. Stem Cells Int. 2019 Dec 30;2019:6279721. [CrossRef]
- Melville, J. C.; Nassari, N. N.; Hanna, I. A.; Shum, J. W.; Wong, M. E.; Young, S., Immediate Transoral Allogeneic Bone Grafting for Large Mandibular Defects. Less Morbidity, More Bone. A Paradigm in Benign Tumor Mandibular Reconstruction? J Oral Maxillofac Surg 2017, 75, (4), 828-838.
- Talaat, W. M.; Ghoneim, M. M.; Salah, O.; Adly, O. A., Autologous bone marrow concentrates and concentrated growth factors accelerate bone regeneration after enucleation of mandibular pathologic lesions. Journal of Craniofacial Surgery 2018, 29, (4), 992-997. [CrossRef]
- Schliephake, H., Clinical efficacy of growth factors to enhance tissue repair in oral and maxillofacial reconstruction: a systematic review. Clinical implant dentistry and related research 2015, 17, (2), 247-273. [CrossRef]
- Khojasteh, A.; Behnia, H.; Naghdi, N.; Esmaeelinejad, M.; Alikhassy, Z.; Stevens, M., Effects of different growth factors and carriers on bone regeneration: a systematic review. Oral surgery, oral medicine, oral pathology and oral radiology 2013, 116, (6), e405-e423. [CrossRef]
- Gomes-Ferreira, P. H. S.; Okamoto, R.; Ferreira, S.; De Oliveira, D.; Momesso, G. A. C.; Faverani, L. P., Scientific evidence on the use of recombinant human bone morphogenetic protein-2 (rhBMP-2) in oral and maxillofacial surgery. Oral and maxillofacial surgery 2016, 20, (3), 223-232. [CrossRef]
- Hidalgo, D. A.; Rekow, A., A review of 60 consecutive fibula free flap mandible reconstructions. Plastic and reconstructive surgery 1995, 96, (3), 585-596. [CrossRef]
- Hidalgo, D. A., Condyle transplantation in free flap mandible reconstruction. Plastic and reconstructive surgery 1994, 93, (4), 770-781.
- Teven, C. M.; Fisher, S.; Ameer, G. A.; He, T. C.; Reid, R. R., Biomimetic approaches to complex craniofacial defects. Ann Maxillofac Surg 2015, 5, (1), 4-13. [CrossRef]
- Kinoshita, Y.; Maeda, H., Recent developments of functional scaffolds for craniomaxillofacial bone tissue engineering applications. The Scientific World Journal 2013, 2013. [CrossRef]
- Ramly, E. P.; Alfonso, A. R.; Kantar, R. S.; Wang, M. M.; Siso, J. R. D.; Ibrahim, A.; Coelho, P. G.; Flores, R. L. J. P.; Open, R. S. G., Safety and efficacy of recombinant human bone morphogenetic protein-2 (rhBMP-2) in craniofacial surgery. Plast Reconstr Surg Glob Open. 2019, 7, (8). [CrossRef]
- Costa, A. M.; Barbosa, A.; Neto, E.; Sousa, S. A.; Freitas, R.; Neves, J. M.; Cardoso, M. T.; Ferreirinha, F.; Sá, C. P., On the role of subtype selective adenosine receptor agonists during proliferation and osteogenic differentiation of human primary bone marrow stromal cells. Journal of cellular physiology 2011, 226, (5), 1353-1366.
- Mediero, A.; Wilder, T.; Perez-Aso, M.; Cronstein, B. N., Direct or indirect stimulation of adenosine A2A receptors enhances bone regeneration as well as bone morphogenetic protein-2. The FASEB Journal 2015, 29, (4), 1577-1590. [CrossRef]
- Mediero, A.; Frenkel, S. R.; Wilder, T.; He, W.; Mazumder, A.; Cronstein, B. N., Adenosine A2A receptor activation prevents wear particle-induced osteolysis. Sci Transl Med 2012, 4, (135), 135ra65.
- Mediero, A.; Cronstein, B. N., Adenosine and bone metabolism. Trends in Endocrinology & Metabolism 2013, 24, (6), 290-300.
- Lopez, C. D.; Witek, L.; Flores, R. L.; Torroni, A.; Rodriguez, E. D.; Cronstein, B. N.; Coelho, P. G. J. R. S. f. M.; Guide, M. R. A. P., 3D Printing and Adenosine Receptor Activation for Craniomaxillofacial Regeneration. 2019, 255-267.
- FitzGerald, G. A., Dipyridamole. The New England journal of medicine 1987, 316, (20), 1247-1257.
- Patrono, C.; Coller, B.; Dalen, J. E.; Fuster, V.; Gent, M.; Harker, L. A.; Hirsh, J.; Roth, G., Platelet-active drugs: the relationships among dose, effectiveness, and side effects. Chest 1998, 114, (5 Suppl).
- Monagle, P.; Chan, A. K. C. K. C.; Goldenberg, N. A.; Ichord, R. N.; Journeycake, J. M.; Nowak-Göttl, U.; Vesely, S. K., Antithrombotic therapy in neonates and children: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, (2 Suppl). [CrossRef]
- Lopez, C. D.; Diaz-Siso, J. R.; Witek, L.; Bekisz, J. M.; Gil, L. F.; Cronstein, B. N.; Flores, R. L.; Torroni, A.; Rodriguez, E. D.; Coelho, P. G. J. P.; surgery, r., Dipyridamole augments 3D printed bioactive ceramic scaffolds to regenerate craniofacial bone. Plast Reconstr Surg. 2019, 143, (5), 1408.
- Budharaju, H.; Suresh, S.; Sekar, M. P.; De Vega, B.; Sethuraman, S.; Sundaramurthi, D.; Kalaskar, D. M., Ceramic materials for 3D printing of biomimetic bone scaffolds – Current state-of-the-art & future perspectives. Materials & Design 2023, 231, 112064.
- Sakthiabirami, K.; Soundharrajan, V.; Jin-Ho, K.; Nileshkumar, D.; Geetha, M.; Kwi-Dug, Y.; Sang-Won, P., Perspective Chapter: Additive Manufactured Zirconia-Based Bio-Ceramics for Biomedical Applications. In Advanced Additive Manufacturing, Igor, V. S., Ed. IntechOpen: Rijeka 2022; p Ch. 1.
- Yanamandra, K.; Chen, G. L.; Xu, X.; Mac, G.; Gupta, N., Reverse engineering of additive manufactured composite part by toolpath reconstruction using imaging and machine learning. Composites Science and Technology 2020, 198, 108318. [CrossRef]
- Delli, U.; Chang, S., Automated Process Monitoring in 3D Printing Using Supervised Machine Learning. Procedia Manufacturing 2018, 26, 865-870. [CrossRef]
- Guo, J. L.; Januszyk, M.; Longaker, M. T., Machine Learning in Tissue Engineering. Tissue engineering. Part A 2023, 29, (1-2), 2-19. [CrossRef]
- Conev, A.; Litsa, E. E.; Perez, M. R.; Diba, M.; Mikos, A. G.; Kavraki, L. E., Machine Learning-Guided Three-Dimensional Printing of Tissue Engineering Scaffolds. Tissue engineering. Part A 2020, 26, (23-24), 1359-1368. [CrossRef]
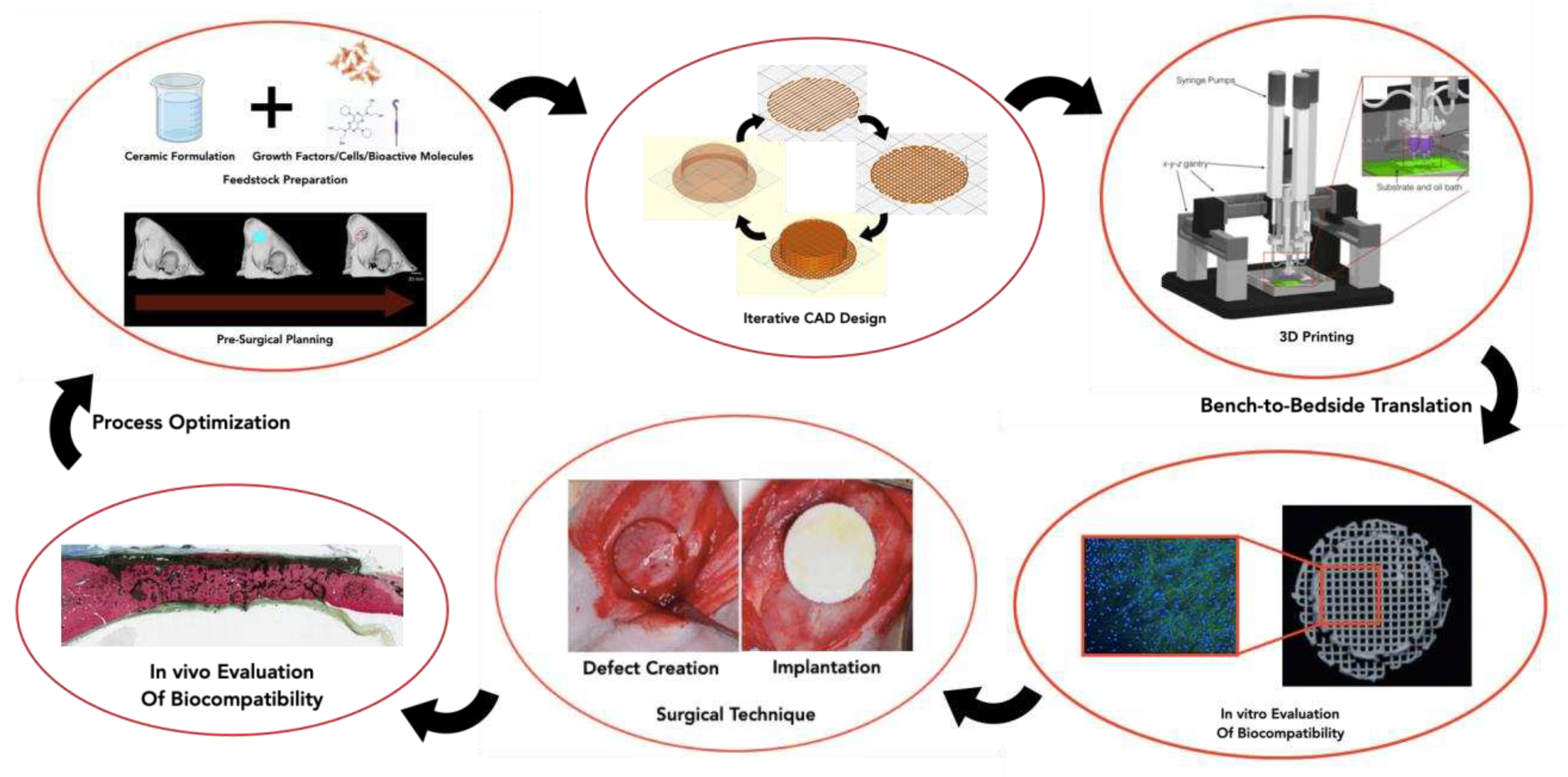
Figure 2.
Schematic overview of the SLS methodology.
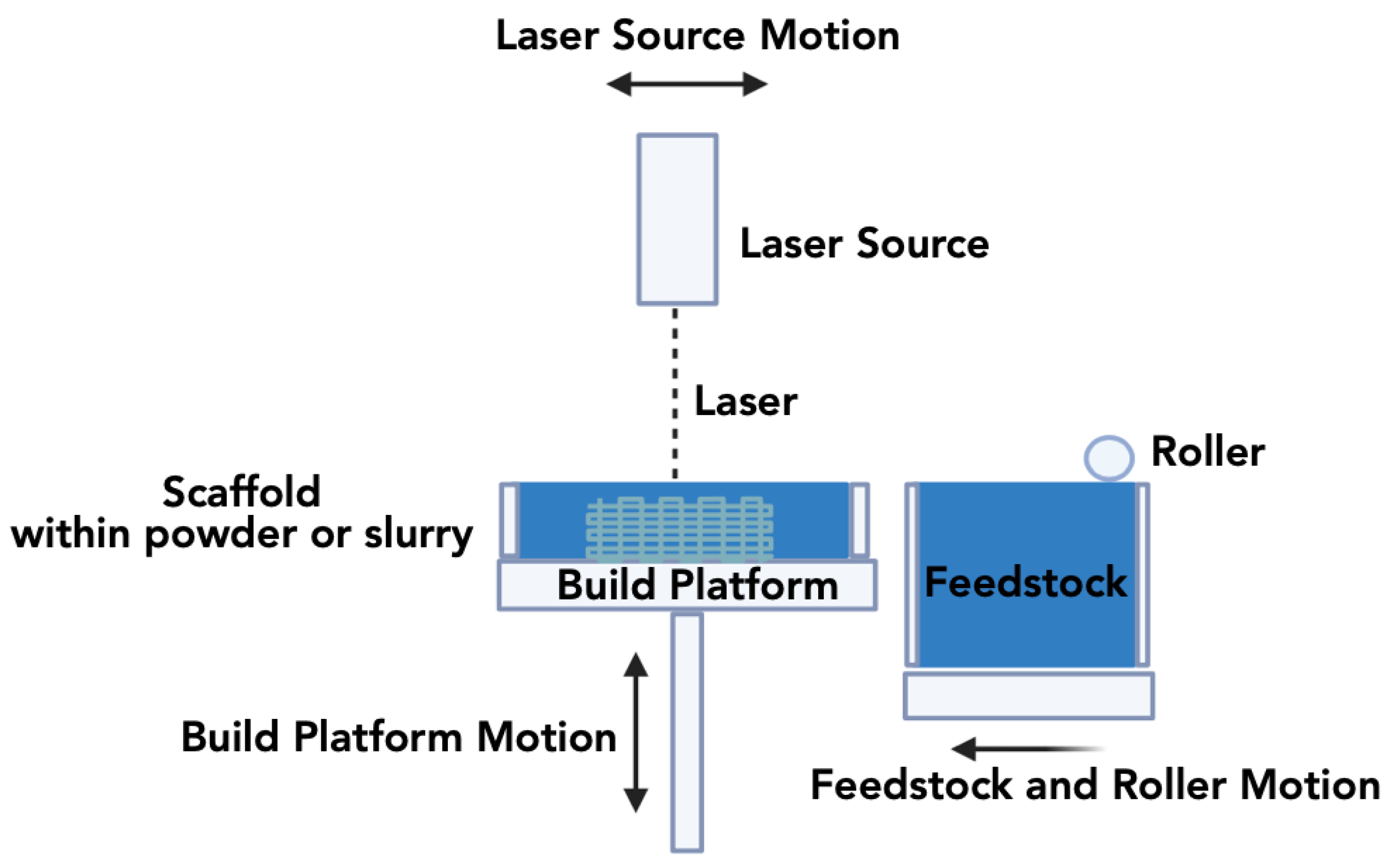
Figure 3.
Schematic overview of the SLA methodology.
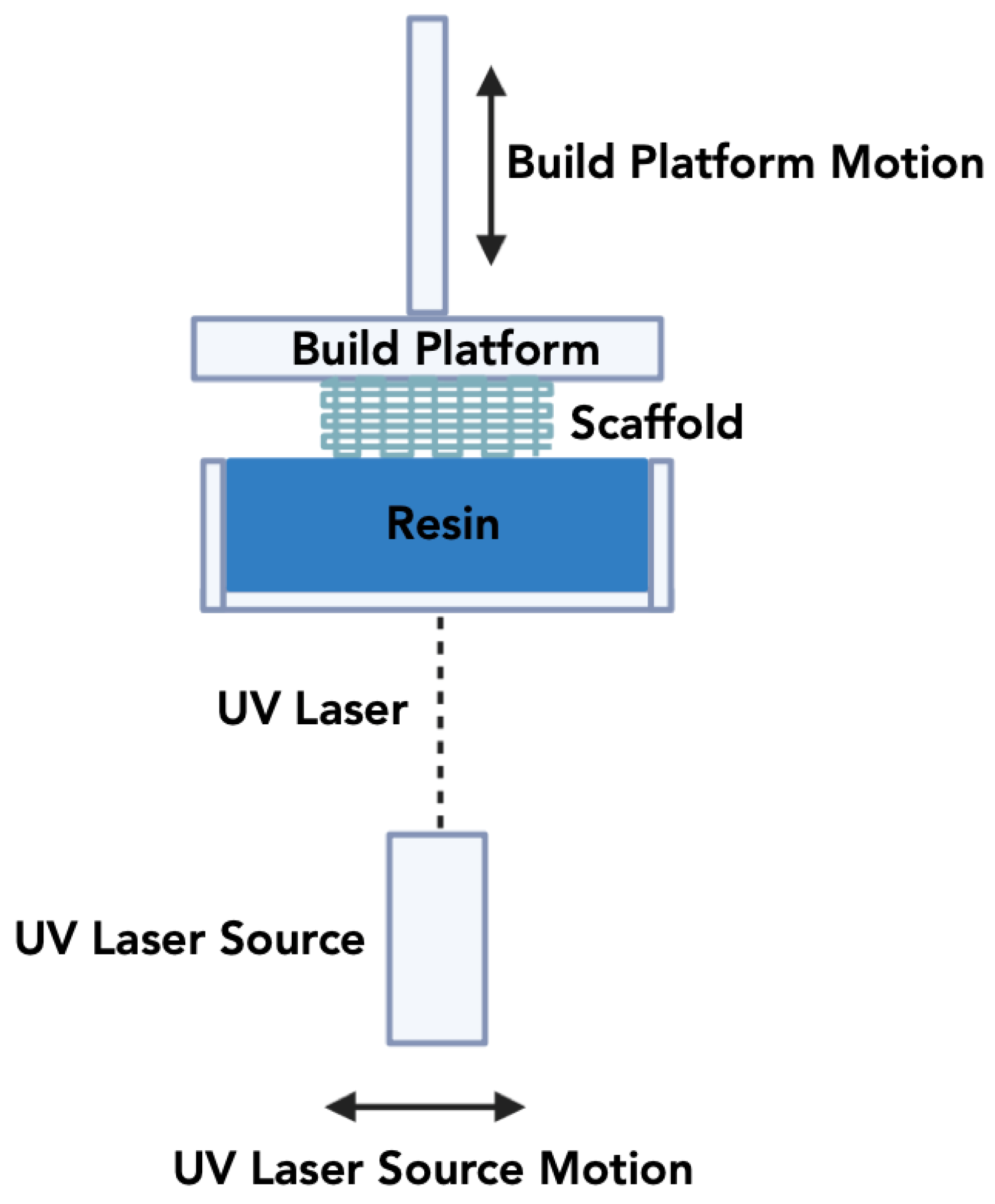
Figure 4.
Schematic overview of the Digital Light Processing methodology.
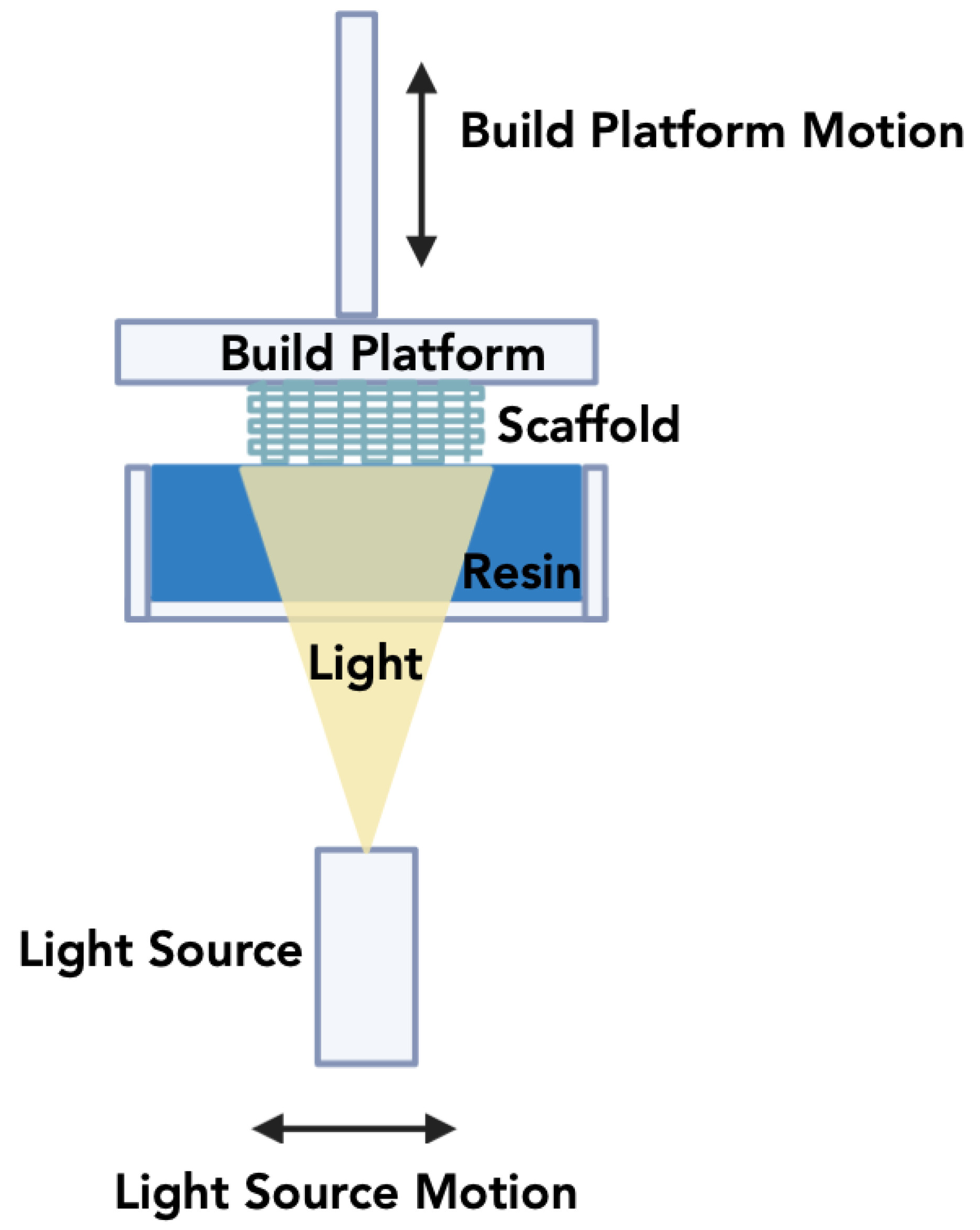
Figure 5.
Schematic overview of the Direct Ink Writing methodology.
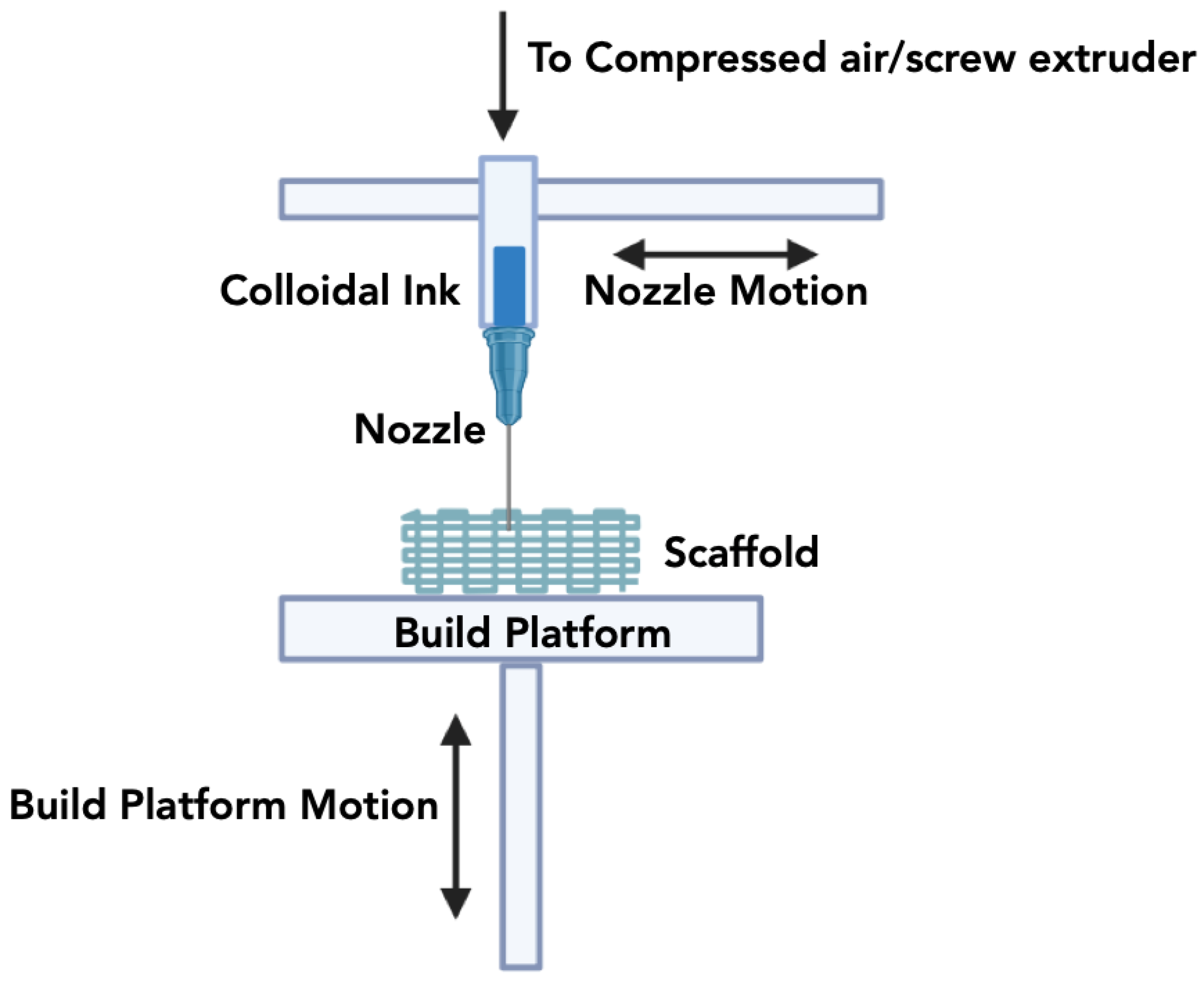
Figure 6.
Schematic overview of the Fused Deposition Modeling methodology.
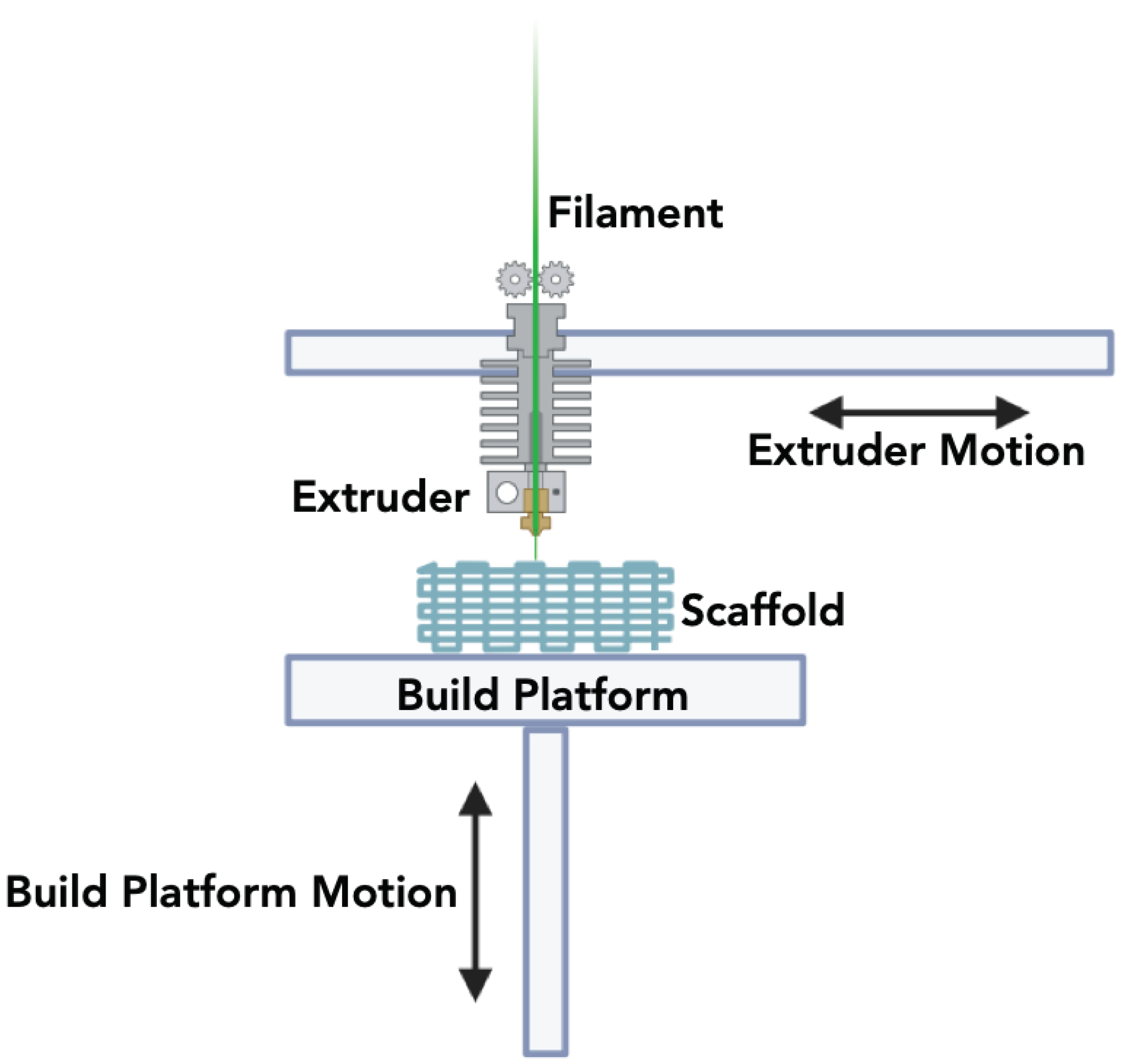

Table 1.
Bioceramic materials used in BTE and their applications.
| Ceramic | Sintering Temperature | Characteristic | Applications | Ref. | |
| Hydroxyapatite Ca10(PO4)6(OH)2 |
1000–1250°C | Capable of fostering cell growth, possessing excellent biocompatibility and good compression strength | Repair of bone defects | [33,34,35] | |
| β-Tricalcium phosphate β-Ca3(PO4)2 |
200–1400°C | Minimal shrinkage, biodegradability, appropriate porosity reduced cracking and deformation | Hard tissue repair of defects | [36,37,38] | |
| Silicon carbide SiC |
1860–1950°C | High strength and good compressive strength | Light weight structural ceramics | [39,40,41] | |
| Zirconium oxide ZrO2 |
1000–1450°C | Biocompatibility, chemical stability, and excellent mechanical properties | Bone repair and tissue engineering | [42] | |
| Barium titanate BaTiO3 |
900–1200°C | Biocompatible and good tensile strength | Repair of extensive bone defects | [43,44] | |
Table 2.
Summary of commonly used AM methods for the production of ceramic based bone replacement scaffolds, and constructs.
Table 2.
Summary of commonly used AM methods for the production of ceramic based bone replacement scaffolds, and constructs.
| AM Method | Ceramic slurry/filament/ink/ preparation |
Printing Resolution | Advantages | Disadvantages | Reference |
| Fused Deposition Modelling (FDM) |
Filaments are produced through a blend of ceramic powders and thermoplastic polymers for 3D printing of structures. | 100µm– 1mm |
Compatible with other materials, reproducibility, low-cost and ease of operation. | Limited resolution and uneven adhesion between layers. | [113,114] |
| Stereolithography (SLA) | The printing process involves combining ceramics with a photopolymerizable resin. | 20 µm –100µm | Low wastage of ceramic materials, high resolution, and printing speed. |
Requirement for photopolymers, and the need for subsequent post-processing steps. | [115,116,117] |
| Selective laser sintering (SLS) |
The powder bed is prepared with ceramic particles of equal size to withstand laser power and temperature, ensuring a defect-free construct. | 20 µm –100µm | High resolution, fabrication of complex structures using powder as support, and high mechanical strength of printed constructs. | Demand of materials capable of enduring laser heat, managing scaffold shrinkage, and pre- and post-heating treatments. | [118,119] |
| Direct Inkjet Writing (DIW) | A homogeneous ceramic slurry is created by blending ceramic materials with polymer binders and viscosifiers into the solutions. | 100µm– 1mm |
Low cost, scalability, capability for fabrication of complex and larger structures. | High pressure, low resolution, needle clogging. | [120,121,122,123] |
| Digital light processing (DLP) |
Ceramic powder with liquid photopolymer is exposed to digital light arrays. | 25 µm –100µm | High resolution, cost-effectiveness, and accuracy of print. | Limited availability of materials, requirement for photo reactivity, and restricted build volume. | [115,124,125] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



