
Submitted:
27 November 2023
Posted:
29 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has had a substantial impact on global health, notably the virus's association with autoimmune illnesses. Autoimmune illnesses occur when the immune system of the body targets healthy cells, causing damage and inflammation. The potential impact of COVID-19 on autoimmune disorders, the hazards of COVID-19 vaccinations for persons with autoimmune diseases, and the potential risks of COVID-19 vaccines are all discussed in this essay. COVID-19 can cause autoimmune illnesses by causing inflammation, organ and tissue damage, and molecular mimicry, in which the immune system mistakenly assaults healthy cells for the virus. However, not everyone infected with COVID-19 develops autoimmune disorders. While some research has found a link between COVID-19 and autoimmune illnesses, this does not always suggest causation. Other factors, such as genetics and environment, may also play a role in the emergence of autoimmune illnesses. COVID-19 can aggravate existing autoimmune disorders by causing the immune system to attack healthy cells, making management more difficult and increasing the risk of consequences. People with autoimmune disorders, on the other hand, may not be at a higher risk of severe COVID-19 than the general population. Some research has found that persons with autoimmune disorders are more likely to have severe COVID-19, whereas others have found no difference. COVID-19 vaccinations may represent dangers to persons with autoimmune illnesses since they contain antigens that can activate the immune system. Furthermore, due to their already overactive immune systems, some vaccines may not perform as well for people with autoimmune disorders, and some people with autoimmune diseases may have severe reactions to immunizations, producing inflammation and other symptoms. COVID-19 may not be any more hazardous to those with autoimmune illnesses than it is to the general population. The connection between COVID-19 and autoimmune disorders is complicated and under investigation. While some research implies that people with autoimmune disorders have a higher risk of severe COVID-19, others demonstrate no difference in death rates between them and the general population. There are also counterarguments that COVID-19 can induce and exacerbate autoimmune disorders, as well as worries about COVID-19 vaccine hazards for people who have autoimmune diseases. More research is required to completely understand the influence of COVID-19 on autoimmune illnesses, as well as the dangers and benefits of vaccinations for these people.
Keywords:
COVID-19
; SARS COV2
; coronavirus
; autoimmunity
; molecular mimicry
1. Introduction
The COVID-19 pandemic has significantly impacted individuals with autoimmune illnesses and overactive immune systems. As vaccines are rushed globally, it's crucial to examine the potential impact of COVID-19 immunization on those with autoimmune disorders. This paper reviews arguments on the potential worsening of symptoms and the benefits of immunization for these individuals.
The COVID-19 vaccine may worsen symptoms for individuals with autoimmune disorders due to the overactive immune system, which can trigger flares and exacerbate symptoms. For instance, individuals with rheumatoid arthritis may experience joint inflammation and pain after vaccination. Additionally, vaccination may increase the risk of autoimmune reactions and the development of new autoimmune disorders, as the immune system may mistakenly attack healthy cells.
The COVID-19 vaccination offers significant benefits for individuals with autoimmune disorders. It protects them from severe infection, reducing the risk of complications and hospitalizations. Additionally, vaccination achieves herd immunity, reducing the spread of COVID-19, thus protecting vulnerable populations, including those with autoimmune disorders. Therefore, vaccination is a crucial strategy for preventing severe illness.
Research suggests that individuals with autoimmune disorders are more susceptible to severe COVID-19 infection and higher fatality risks, making them more vulnerable to the virus and its complications. Therefore, the potential worsening of symptoms in these individuals is not a significant concern, as the benefits of vaccination outweigh the risks.
COVID-19 immunization can be customized to specific autoimmune illnesses, reducing potential risks. Pre-vaccination examinations can identify individuals at higher risk and implement appropriate precautions. Those with a history of severe autoimmune reactions should be cautious during vaccination. Most individuals with autoimmune disorders experience no adverse effects, indicating low risks. From the database, Peng et al. found 1,028,721 COVID-19 individuals and 3,168,467 non-COVID persons; the COVID-19 group had a higher crude incidence rate than the non-COVID group (Figure 1) [114].
The impact of COVID-19 vaccination on autoimmune patients is complex and controversial. While it may worsen symptoms and increase the risk of autoimmune reactions, it offers significant benefits by protecting against severe infection and reducing the risk of sequelae. The benefits outweigh the risks, especially when administered in a controlled environment. Individuals with autoimmune disorders should consult with healthcare providers for informed decisions.
2. Understanding Autoimmunity and Its Mechanisms
Autoimmunity is a condition where the immune system fails to differentiate between self and non-self, leading to immune responses directed against self [1]. This can be caused by T cells or antibodies against autoantigens in primary autoimmune diseases [3]. Autoimmune disorders result in inflammatory responses and the activation of previously inactive autoreactive T and B cells [4]. Defects in the immune system's mechanisms for controlling self-reactivity can lead to a breakdown of tolerance, causing autoimmune diseases [4]. Systemic autoimmune diseases involve the immune system reacting against various tissue antigens or self-components, but the mechanism behind their effects is poorly understood [2]. Multiple genetic factors are likely to interact to promote autoimmunity, with evidence for genetic underpinnings [1]. The female predominance in many autoimmune diseases suggests a role for the X-chromosome and its genes in self-reactivity development [1]. Autoimmune disorders are prevalent worldwide and can present with different clinical pictures depending on the T-cell subset involved [2] [3]. Understanding the molecular mechanism behind autoimmune disorders is crucial for developing novel treatment paradigms, including personalized medicine, to address skewed and dysfunctional diseases resulting from autoimmunity [1].
Autoimmunity is a widespread disorder of the immune system that is characterized by the immune system attacking the body's own tissues. There are several types of autoimmunity, including organ-specific autoimmune diseases and systemic autoimmune diseases. Organ-specific autoimmune diseases involve the immune system attacking specific organs or tissues, such as the skin or pancreas, while systemic autoimmune diseases affect multiple organs and tissues throughout the body. Our knowledge of autoimmune illnesses is currently limited, and research is being conducted to better understand the mechanisms that cause these disorders [5]. Although much progress has been made in understanding the underlying causes of autoimmunity, our current understanding is still incomplete. Nevertheless, model diseases such as pemphigus, dermatitis herpetiformis and psoriasis have contributed to our understanding of skin autoimmunity [3]. In addition, autoimmune diseases are known to be complex and multifactorial, with genetic and environmental factors playing a key role in their development [6]. Autoimmune diseases can also be triggered by infections, as microbes can promote autoimmunity by mimicking self-antigens or by inducing molecular mimicry [4]. To improve patient care, further research is needed to deepen our understanding of the fundamental mechanisms that drive autoimmune disease initiation and progression [1]. Ultimately, increased understanding of these mechanisms will enable better diagnosis and treatment of autoimmune diseases, thus improving patient outcomes [7].
Autoimmune illnesses are a diverse set of disorders that manifest differently depending on the site of pathology but share many basic processes [8]. Any molecule that enters the body via a parenteral route can be recognized by the immune system [8]. The host relies on particular mechanisms to avoid the detrimental effects of autoimmunity, including negative selection in the thymus and bone marrow and peripheral regulatory systems like anergy, ignorance, and suppression [8]. Despite these safeguards, autoimmune disorders are widespread in developed countries [8]. Self-reactive B and T lymphocytes are present in healthy people and have the potential to cause an autoimmune reaction [8]. The initiation of autoimmune disease in humans is still not well understood, although models that attempt to recapitulate this process with human tissue in vivo are actively being pursued. Understanding the mechanisms that lead to the clinical outcome of autoimmune disease is crucial for developing effective therapies, and increased understanding of these mechanisms will improve our knowledge of how autoimmune disease develops [8]. Efforts to understand autoimmunity have been pursued relentlessly for several decades, and the identification of new targets for intervention in the immune system has opened new avenues for therapeutic development. For example, ion channels have been identified as molecular targets in the development of new therapeutics against autoimmune disorders.
3. The Impact of COVID-19 Vaccination on Autoimmune Diseases: An Exploration of Possible Triggers and Exacerbations
The COVID-19 pandemic has raised questions about the autoimmune safety of COVID-19 vaccines, particularly among patients with systemic autoimmune illnesses. However, there is a dearth of accessible data on the balance of benefits and dangers of COVID-19 vaccinations in individuals with autoimmune disorders [9]. A study intends to describe the prevalence of autoimmune disorders following BNT162b2 and CoronaVac immunization [10]. Concerns about the autoimmune safety of COVID-19 vaccinations may have a negative influence on vaccine uptake, especially in patients with autoimmune illnesses [10]. Furthermore, there is no information in the text about how the COVID-19 vaccine affects autoimmune illnesses [9]. Patients with systemic autoimmune disorders are more susceptible to COVID-19 infection [9]. A study employed the Health Literacy about Vaccination in Adulthood in Italian (HLVa-IT) to assess vaccine literacy abilities in a cohort of patients with systemic autoimmune disorders [9]. According to the study, most autoimmune disease patients have favorable views and impressions of COVID-19 vaccines, and 96.7% intend to be immunized against COVID-19 [9]. Nonetheless, patients with systemic autoimmune illnesses may be more reluctant to get vaccinated against COVID-19 [9]. In general, further research is needed to determine the possible influence of COVID-19 vaccinations on autoimmune illnesses.
Although current evidence suggests that the benefits of COVID-19 vaccination outweigh the potential risk of adverse events (AEs) in patients with SAIDs [11], there is still limited information on the short- and long-term safety and efficacy of COVID-19 vaccines in this population. Two occurrences of serious adverse events (AEs) associated with the Moderna vaccination have been documented in SAIDs patients [11]. While the mRNA technology used in COVID-19 vaccinations may exacerbate inflammation and pre-existing autoimmune diseases, it is still unclear whether vaccination causes or worsens autoimmune diseases due to a lack of data and studies with a large sample size of both patients and controls [11]. Nonetheless, SAIDs patients have voiced concern about vaccination-induced flares, allergic responses, and other adverse events (AEs) potentially contributing to vaccine hesitancy [11]. Furthermore, the Oxford/AstraZeneca vaccine employs Adeno-associated virus (AAV) technology, which has been associated with uncommon side effects such as monophasic demyelinating events such as acute disseminated encephalomyelitis, optic neuritis, and transverse myelitis [11]. According to preliminary findings from the COVAD trial, patients with idiopathic inflammatory myopathies (IIM) are more likely to develop rashes after receiving COVID-19 immunization [11]. Furthermore, studies comparing the AEs associated with different vaccine types following COVID-19 inoculation are missing, and different vaccine types may be linked with varying frequencies and types of AEs [11]. As a result, more research is needed to assess the prevalence of vaccine-induced prothrombotic immune thrombocytopenia in patients with underlying SAIDs following COVID-19 immunization and to define an effective method for administering COVID-19 vaccines in the SAID population [11].
Currently, information on the impact of COVID-19 vaccination on autoimmune diseases is limited due to the exclusion of individuals with autoimmune diseases from the original vaccine trials [12]. Nevertheless, the protocol for the COVID-19 Vaccination in Autoimmune Diseases (COVAD) study has been developed to investigate the benefits and risks of COVID-19 vaccination in patients with autoimmune diseases [13]. Despite the benefits of vaccination, studies have shown that more than a third of patients with autoimmune diseases remain hesitant about receiving the vaccine [14]. Furthermore, there is a lack of empirical data on COVID-19 vaccines in rheumatic patients, leading to a hypothesis of possible modifiers of vaccine response [15]. One concern is that autoimmune conditions may develop following COVID-19 vaccination [10]. While there is a need for further research regarding the long-term safety of COVID-19 vaccination in individuals with autoimmune diseases, the current evidence suggests that the benefits of vaccination outweigh the risks of potential vaccine adverse effects [16,17]. At 7 days post-vaccination, research examining vaccine side effects based on vaccine type in individuals with systemic autoimmune disorders showed no significant differences between vaccine types and healthy controls [11]. It should be noted that vaccine literacy skills, attitudes, perceptions, and beliefs about current COVID-19 immunizations may be related to vaccine uptake in individuals with systemic autoimmune disorders [9].
4. Autoimmune Diseases Associated with COVID19 Vaccine
The pathophysiology of ITP and COVID-19
COVID-19 infection can cause severe thrombocytopenia, a condition characterized by a low platelet count, which can lead to potentially fatal bleeding [18]. Interestingly, COVID-19 can also lead to the development of immune thrombocytopenic purpura (ITP), a bleeding disorder caused by the abnormal destruction of platelets by the immune system [18]. While thrombocytopenia in COVID-19 patients does not necessarily require a history of ITP, the pathophysiology of ITP involves the abnormal destruction of platelets by the immune system, causing their numbers to decrease and increasing the risk of bleeding [18]. Platelets are responsible for helping blood clot and heal damaged blood vessel walls [18]. Therefore, having a diagnosis of ITP does not appear to increase someone’s chance of getting infected with COVID-19 [18]. However, research is ongoing about the relationship between ITP and COVID-19, and whether there is any correlation between their pathophysiology [18]. Importantly, having a diagnosis of ITP does not increase the risk for more severe infection with COVID-19 [18].
ITP has emerged as a significant COVID-19-associated complication, with COVID-19-mediated ITP being attributed to underlying immune dysregulation, susceptibility mutations, and other mechanisms [19,20]. However, evidence does not indicate that patients with ITP are more likely to contract COVID-19, nor do they appear to have more severe symptoms [18]. The COVID-19 vaccine series has also been linked to ITP as a rare adverse event, but the risks associated with COVID-19 disease appear to outweigh the risks associated with SARS-CoV-2 vaccination in ITP patients [21,22]. In fact, immune thrombocytopenia (ITP) should not be a reason to discourage vaccination [23]. The relationship between COVID-19 and ITP has not yet been established, but the pathogenesis of viral-induced ITP is thought to be like that of COVID-19-mediated ITP [24]. Despite the shared clinical manifestations between COVID-19 and ITP, it is important to note that people with ITP should take precautions to avoid contracting COVID-19, as it could potentially exacerbate their pre-existing condition.
Both COVID-19 and immune thrombocytopenia (ITP) share similar clinical manifestations [25,21]. Thrombocytopenia, or low platelet counts, is a common finding in COVID-19 patients, and ITP can develop because of an immune system reaction to the virus [25,26]. In fact, ITP has recently emerged as a significant COVID-19-associated complication [25,19]. A case report of thrombocytopenia associated with SARS-CoV-2 infection has been documented [27]. While there are similarities in the clinical manifestations between COVID-19 and ITP, it is important to note that they may have different clinical outcomes [19]. Furthermore, ITP can occur both after COVID-19 infection and because of COVID-19 [26]. The link between ITP and the COVID-19 vaccine series as a rare adverse event has also been reported [21]. Although the text does not provide specific information on how the clinical manifestations of ITP and COVID-19 differ, they share common clinical features such as thrombocytopenia [19,26].
The association between COVID-19 and Guillain-Barré Syndrome (GBS)
Guillain-Barré Syndrome (GBS) is a neurological disorder in which the body's immune system attacks part of the peripheral nervous system. GBS can cause muscle weakness, loss of reflexes, and tingling sensations in the hands and feet [28]. The disease progresses rapidly and can lead to paralysis of respiratory muscles, requiring mechanical ventilation [28]. Clinical evaluation, nerve conduction studies, and lumbar puncture can be used to diagnose GBS [28]. GBS can be triggered by infections, surgery, or vaccinations [28]. In around 71% of cases, cerebrospinal fluid (CSF) albuminocytological dissociation is present [28]. GBS is a disease spectrum with several subtypes, including Acute Inflammatory Demyelinating Polyneuropathy (AIDP) and AMSAN. More than 70% of GBS patients have a positive prognosis, mostly after receiving intravenous immunoglobulin [28]. While GBS can afflict people of all ages, with a male predominance [28], it is extremely rare. GBS, on the other hand, has been linked to the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) [28,29]. In fact, GBS can emerge following COVID-19; nevertheless, asymptomatic COVID-19 cases have also been recorded [28]. The lack of SARS-CoV-2 RNA in all analyzed CSF samples renders direct invasion of SARS-CoV-2 into nerve roots with intrathecal viral replication less likely [28]. GBS has been linked to SARS-Cov-2 infection [30]. Phosphorylated neurofilament heavy chain (pNfH) and serum neurofilament light chain (NfL) proteins can be utilized to diagnose nervous system affection in COVID-19-related disorders [28]. GBS is distinguished by increased CSF proteins and pleocytosis in approximately 50-80% of cases [28]. AIDP, AMSAN, and AMAN are electrophysiological variations of the illness [28]. MFS's immune-mediated mechanisms may differ from those of conventional GBS [28]. In the current pandemic, all newly diagnosed GBS cases should be screened for Covid-19 infection, even if they do not have respiratory symptoms [30]. GBS commonly develops neurological symptoms 14 days after COVID-19 and has a median latency period of 14 days [28]. When the condition is coupled with COVID-19, the severity of the symptoms increases [29]. GBS is treated with IVIG treatment [28].
COVID-19 is a fast-spreading epidemic that has sickened over 14,000,000 individuals worldwide [28]. Evidence suggests that SARS-CoV-2 infection may be linked to the development of Guillain-Barré Syndrome (GBS) [28]. GBS is a neurological condition in which the immune system of the body targets a portion of the peripheral nervous system. The virus that causes COVID-19, SARS-CoV-2, primarily affects the respiratory system but is increasingly linked to central and peripheral neurological symptoms [28]. Some patients with Guillain-Barre Syndrome (GBS) have a clinical history of COVID-19 pneumonia and/or a radiological image [28]. The frequency of COVID-19 pneumonia in GBS patients with poor outcome is slightly higher but not significant compared to those with a favorable prognosis [28]. Interestingly, there is no significant difference in the latency between COVID-19 and GBS and nadir between the two groups [28]. Furthermore, there is no significant difference in the distribution of sex and electrophysiological subtypes between the two groups [28]. However, age is a significant factor as patients with a poor outcome are significantly older than those with a favorable prognosis [28]. These findings suggest that COVID-19 may play a role in the development of GBS, and further research is necessary to fully understand this relationship.
Studies indicate a growing body of evidence pointing towards an association between COVID-19 and the development of Guillain–Barré Syndrome (GBS). A systematic review of 94 cases revealed that the clinical presentation of COVID-19-associated GBS has a few clinical characteristics that increase suspicion of the disease [31]. Further studies have explored the different subtypes of GBS in relation to COVID-19 infection. However, most reports referred to Acute Inflammatory Demyelinating Polyneuropathy (AIDP) [32]. In addition, a review of 37 published cases of GBS associated with COVID-19 found much remains unknown about the strength of the association and the features of GBS in this setting [33]. Nonetheless, all these cases argue that SARS-Cov-2 virus could be a triggering factor of GBS, and diagnosed Guillain-Barré cases should be tested for COVID-19 [30]. It is noteworthy that reports have also surfaced of GBS occurring soon after the first dose of Vaxzevria (previously known as COVID-19) [34]. Therefore, it is imperative to investigate whether a causal relationship could be determined between COVID-19 and GBS to help communicate the clinical implications and improve patient outcomes [35,29].
Miller Fisher Syndrome (MFS) and COVID-19
Miller Fisher Syndrome (MFS) is a rare neurological disorder that typically develops after exposure to various infectious agents such as viruses, bacteria, and fungi [36]. This acute peripheral neuropathy is characterized by a triad of external ophthalmoplegia, ataxia, and areflexia [36,37]. MFS is a variant of Guillain-Barre syndrome (GBS) [36]. MFS symptoms typically appear 1-4 weeks after the antecedent cause, which could be illnesses or vaccination [37]. MFS, despite being linked to COVID-19 in some cases, has not been linked to COVID-19 immunization [36,37]. MFS is characterized clinically by cranial polyradiculoneuritis involving the face and trigeminal nerves [38]. MFS is typically explained by the presence of anti-GQ1b antibodies, yet anti-GQ1b testing have yielded negative results [38]. Physical examination, brain magnetic resonance imaging (MRI), cerebrospinal fluid analysis (CSF), and positron emission tomography (PET) are used to diagnose MFS [37]. Treatment with intravenous immunoglobulins (IVIG) is efficacious and safe for MFS-related neurological symptoms [36,38]. Rapid MFS treatment can result in a favorable response [1]. Patients with a history of MFS or GBS should avoid revaccination following COVID-19 vaccination [37]. Although there have been instances of MFS following COVID-19 vaccination, more research is needed to confirm any link [37,36].
COVID-19 is a pandemic caused by the new coronavirus SARS-CoV-2, which has spread swiftly over the world and can produce severe respiratory symptoms that necessitate the use of assistive devices [37,38]. Vaccination is the most effective strategy to combat the pandemic, and the BNT162b2 mRNA COVID-19 vaccine has been developed and shown effective globally [37]. However, neurological problems associated with COVID-19 vaccination have been observed, including Guillain-Barré syndrome (GBS) and its subtypes, including Miller Fisher Syndrome (MFS) [37]. MFS is a variant of GBS, and it is characterized by the clinical trial of ophthalmoplegia, ataxia, and areflexia [38]. Approximately 60% of autoimmune syndromes, including those related to infections like MFS, can be infection-related [38]. COVID-19 is a respiratory infection, and there is a possibility that it can cause MFS due to its respiratory symptoms [38]. Infection-related autoimmune syndromes can be caused by humoral and cellular cross-reactivity [38]. It is necessary to monitor and report any adverse events related to the COVID-19 vaccination to understand the potential risks and benefits of the vaccine in the population.
Miller Fisher Syndrome (MFS) is a rare autoimmune disorder that affects the peripheral nerves. Recent studies have reported cases of MFS associated with COVID-19 [39]. To better understand the relationship between COVID-19 and MFS, a systematic review of case reports was conducted [40]. The review found that MFS following COVID-19 vaccination has been rare but has been observed. The phenotype of MFS varied among cases, with some manifesting with classic MFS and others with partial symptoms [41]. In addition, there is evidence that COVID-19-associated MFS patients may experience dysautonomia, which is an uncommon feature of MFS but well-reported in COVID-19 [42]. Previous studies also reported no evidence of intrathecal production of SARS-CoV-2 antibodies as the disease mechanism in COVID-19-associated MFS cases [43]. One study reported a case of MFS associated with inactivated COVID-19 vaccine, which to the best of our knowledge is the first reported case [44]. However, the temporal relationship between COVID-19 and MFS is not yet fully understood and requires further investigation [40]. Despite the limited number of reported cases, it is crucial to recognize the potential association between COVID-19 and MFS to facilitate early diagnosis and treatment of affected patients.
Antiphospholipid Antibodies and Thrombosis in COVID-19 Patients
Antiphospholipid antibodies (aPL Ab) are a type of antibody that can cause thrombosis. COVID-19 patients with elevated levels of aPL Ab may develop conditions like antiphospholipid syndrome (APS) [45,46]. However, the presence of aPL Ab alone does not diagnose APS unless other criteria are met [45]. Lupus anticoagulant is the most tested type of aPL Ab in COVID-19 patients, and a significant percentage of COVID-19 patients have at least one type of APLa in their blood [45,47]. It is not yet clear if aPL Ab plays a role in the pathogenesis of COVID-19 [45]. Although antiphospholipid syndrome and COVID-19 coagulopathy share certain similarities, such as the release of cytokines and endothelial damage leading to clot formation, they likely have different underlying causes and require different treatments [45,47]. Therefore, anticoagulation management may be changed based on aPL Ab testing, but the association between aPL Ab and thrombosis or clinical outcomes in COVID-19 patients is uncertain [45]. It is important to note that the presence of aPL Ab does not necessarily indicate a need for therapeutic anticoagulation, as other factors, such as the presence of clinical sequelae like thrombosis or pregnancy loss, may indicate APS [45]. Clinicians should be aware that antiphospholipid syndrome can cause misdiagnosis in COVID-19 patients, and lupus anticoagulant testing is a more common method for aPL Ab studies in these patients [46,45].
Antiphospholipid antibodies (aPL Ab), which are isotypes of antibodies, have been shown to contribute to thrombosis. In fact, these antibodies are being considered as a potential factor in the development of blood clots in COVID-19 patients. The presence of aPL Ab is considered during the differential diagnosis of antiphospholipid syndrome, and it has been suggested that they may be contributing to the thrombosis observed in patients [46]. Furthermore, a patient who exhibits an elevated level of aPL Ab has been shown to be at an increased risk of developing thrombosis [46]. These antibodies appear to play a role in the pathogenesis of the syndrome by targeting phospholipid-binding plasma proteins, causing endothelial dysfunction, and increasing the risk of thrombosis. The exact mechanism by which aPL Ab contributes to thrombosis is still not fully understood. However, it is believed that aPL Ab interferes with the coagulation cascade, leading to an increase in procoagulant activity and decreased fibrinolysis. This results in the formation of blood clots in veins and arteries, leading to thrombotic events such as deep vein thrombosis, pulmonary embolism, myocardial infarction, and stroke.
Emerging evidence suggests that COVID-19 is associated with an increased risk of thrombosis or blood clots, which can be dangerous for individuals who test positive for antiphospholipid antibodies (aPL) [48]. Antiphospholipid syndrome (APS) is an autoimmune disease characterized by the appearance of thrombosis and obstetric morbidity in patients with the clinical criteria [49]. COVID-19 patients with positive antiphospholipid antibodies may be at a higher risk for developing thrombosis recurrences, indicating that prophylactic treatment should be considered [50]. In fact, a recent large study documented that the risk of venous thromboembolism in COVID-19 patients was 16%, while the risk of arterial thrombosis was 11.1% [51]. In patients with specific clinical sequelae suggestive of APS, such as thrombosis or pregnancy loss, anticoagulation management is crucial [45]. Moreover, antiphospholipid antibody formation is believed to be one of the mechanisms behind COVID-19 associated thromboembolism [47]. Reports have also demonstrated an increased frequency of antiphospholipid antibodies in COVID-19 patients and evidence of thrombosis in vivo [52]. In primary APS cases, a patient on therapeutic anticoagulation developed adrenal hemorrhage and arterial thrombosis after contracting COVID-19 [53]. Therefore, it is important to closely monitor individuals with antiphospholipid antibodies who have contracted COVID-19 to prevent severe complications that may arise from thrombosis.
Kawasakilike Disease and its Association with COVID-19
Kawasaki-like disease is a condition that shares clinical features with Kawasaki disease and toxic shock syndrome [54]. Researchers have recently reported an association between COVID-19 and the occurrence of Kawasaki-like syndrome, especially in adult patients with COVID-19 [54]. A case report has even emerged of a young adult diagnosed with COVID-19 and subsequently developing Kawasaki-like syndrome [54]. The link between COVID-19 and Kawasaki-like syndrome is still being studied, and more research is needed to fully understand the relationship between these two conditions. It is vital to note that the presentation and severity of Kawasaki-like syndrome in COVID-19 patients may vary, and healthcare providers must remain vigilant in recognizing and treating this syndrome in patients with COVID-19. As the pandemic continues to evolve, it is essential to monitor and investigate any potential associations between COVID-19 and other medical conditions, such as Kawasaki-like syndrome.
As COVID-19 continues to spread globally, new concerns have surfaced regarding a severe Kawasaki-like disease in children who have contracted the virus [55]. The symptoms of Kawasaki-like disease associated with COVID-19 infection are like those of Kawasaki disease and toxic shock syndrome [56]. Recent reports have documented a large case series of patients with Kawasaki-like disease associated with COVID-19, which has led to more research on the clinical characteristics of this disease [57]. Specifically, an outbreak of Kawasaki-like multisystem inflammatory syndrome has been documented in children and adolescents in the Paris area, and it is associated with recent SARS-CoV-2 infection [58]. Furthermore, it has been suggested that children infected with SARS-CoV-2 and exhibiting Kawasaki-like disease may have a lower expression of ACE2 receptors, compared to their healthy counterparts [59]. Interestingly, reports have also emerged of adult patients with COVID-19 who develop a Kawasaki-like multisystem inflammatory condition [60]. This suggests that COVID-19-associated Kawasaki-like syndrome may affect individuals of all ages. In fact, some patients with COVID-19 present with symptoms and signs consistent with a Kawasaki-like syndrome [54]. While there has been some debate over what to call this syndrome, the focus should be on understanding its clinical features to provide effective treatment and management [61]. Overall, data so far suggests that SARS-CoV-2 may trigger a severe inflammatory syndrome in childhood, which warrants further investigation and attention from the medical community [62].
The prevalence of Kawasaki-like disease in COVID-19 patients has become a growing concern within the medical community. Reports of Kawasaki-like symptoms in COVID-19 patients have emerged, particularly in children, leading to speculation that the SARS-CoV-2 virus may trigger a severe inflammatory syndrome in childhood [55,54]. A study in the Paris area documented an outbreak of Kawasaki-like multisystem inflammatory syndrome in children and adolescents, which was associated with the recent SARS-CoV-2 infection [58]. The prevalence of Kawasaki-like disease in COVID-19 patients has been increasingly reported, with large case studies suggesting that the disease might be severe and require more attention [57]. Furthermore, it has been hypothesized that children infected with SARS-CoV-2 and exhibiting Kawasaki-like symptoms may have a lower expression of ACE2 receptors, compared to adults [59]. However, researchers suggest that regardless of the name given to this emerging condition, it is important to understand its implications and possible outcomes [61]. In addition to the pediatric population, cases of a COVID-19-associated Kawasaki-like multisystem inflammatory condition have also been reported in adults [60]. The ongoing emergence of this syndrome during the COVID-19 outbreak underscores the need for continued research to better understand its pathogenesis and clinical implications.
Impact of Preexisting Autoimmune Rheumatic Diseases on COVID19
Autoimmune rheumatic diseases are a group of disorders that affect the immune system and can lead to various comorbidities. Among these diseases, systematic lupus erythematosus (SLE) and rheumatoid arthritis (RA) are the most common ones [63]. These diseases appear to have a higher prevalence in women than in men [63]. Patients with autoimmune rheumatic diseases and comorbidities tend to have a higher risk of developing severe or critical illness [63]. Autoimmune rheumatic diseases can suppress immune defense function, making individuals more vulnerable to viral and bacterial infections [63]. Although the text does not provide information on how the most common autoimmune rheumatic diseases affect the immune system, it does offer a literature review on COVID-19 and autoimmune systemic diseases (ASD) [64]. The review found that immune suppression caused by autoimmune rheumatic diseases can increase the risk of SARS-CoV-2 infection [63]. However, even when b-DMARD medication is used, there is no higher frequency of COVID-19 in patients with rheumatic and musculoskeletal illnesses (RMDs) than in the general population [3]. Furthermore, individuals on DMARDs who were infected with COVID-19 did not experience life-threatening problems because of their underlying medication [65]. Although RMDs and immunosuppressive medications can make patients more susceptible to viral and bacterial infections, tailored treatment regimens can help patients manage their symptoms and enhance their quality of life [65]. In conclusion, SLE and RA are the most common autoimmune rheumatic illnesses that can impact the immune system and cause comorbidities.
Individuals with pre-existing autoimmune rheumatic disorders may be more susceptible to COVID-19 [64]. According to studies, the risks of severe COVID-19 in individuals with rheumatic conditions have gradually decreased over time. However, more research is needed to determine the long-term effects of COVID-19 in rheumatologic patients. While the influence of COVID-19 on patients with pre-existing autoimmune rheumatic disorders is still being explored [65], there have been indications suggesting hydroxychloroquine and methotrexate may play a protective role against COVID-19's most dangerous symptoms. Patients using anti-TNF-alpha medicines may be less likely to be hospitalized if they get COVID-19. Patients on greater glucocorticoid doses, on the other hand, are more likely to be hospitalized if they get COVID-19. Furthermore, patients who are not using any traditional synthetic disease-modifying anti-rheumatic medications are more vulnerable to COVID-19. According to a primary care data analysis, patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), or psoriasis were at a greater risk of death during the pandemic. As in the general population, the probability of severe outcomes in patients with rheumatic illnesses and COVID-19 is related to age and comorbidities [65]. Furthermore, comorbidities are more common in patients with rheumatic disease, either as a result of the underlying disease or as a result of treatment complications. Although Covid-19 disease manifestations in individuals with preexisting autoimmune rheumatic diseases are generally mild, the prevalence of Covid-19 in autoimmune systemic diseases may be underestimated [64]. Finally, the higher prevalence in the connective tissue diseases group may be due to immune system dysfunction [64]. Developing prevention/management strategies for COVID-19 in patients with autoimmune systemic diseases is important, and in-depth investigations are needed to verify the possible interactions between COVID-19 infection and impaired immune-system of autoimmune systemic diseases.
Studies have revealed that individuals with preexisting autoimmune rheumatic diseases face a higher risk of contracting COVID-19 and experiencing severe symptoms. These risks are even higher than those faced by the general population of each region [64]. In comparison, individuals with connective tissue diseases are at an even higher risk than those with inflammatory arthritis [64]. The prevalence of COVID-19 disease is significantly higher in individuals with preexisting autoimmune systemic diseases, including both definite diagnosis and highly suspected diagnosis of the disease [64]. Therefore, it is crucial that individuals with autoimmune rheumatic diseases take appropriate precautions to lower their risk of exposure to COVID-19. They must follow strict safety guidelines, such as wearing masks, washing their hands regularly, maintaining social distancing, and avoiding gatherings. Additionally, they should stay in close contact with their healthcare provider to monitor any changes in their health status, and to ensure they receive the necessary medical care if they do contract COVID-19. It is essential to gain a better understanding of the impact of COVID-19 on patients with rheumatic diseases to reduce the risks associated with this deadly virus.
The Relationship between Systemic Lupus Erythematosus and COVID-19
Patients with systemic lupus erythematosus (SLE) may be at an increased risk of developing COVID-19 due to the prevalence of pre-existing anti-IFNα autoantibodies [66]. In fact, individuals with SLE and pre-existing anti-IFNα autoantibodies may be at risk of developing COVID-19 [66]. Furthermore, SLE patients with COVID-19 have been found to have an increased prevalence of pre-existing anti-IFNα autoantibodies compared to the general population with severe COVID-19 [66]. COVID-19 has the potential to exacerbate the dysregulated immune response seen in SLE and could even trigger the development of autoimmune conditions in these patients [67]. It is important to note that the impact of COVID-19 on patients with SLE is not yet fully understood, and more research is needed to fully comprehend the relationship between the two conditions [67]. A study of ten SLE patients who developed COVID-19 between April 1st and October 1st, 2020, found that all ten patients had full recovery from COVID-19 [66]. Three of the ten patients had severe symptoms that necessitated hospitalization, oxygen therapy, steroids, and convalescent plasma infusion, whereas the remaining seven had mild to moderate COVID-19 symptoms that could be handled at home [66]. Notably, eight out of ten patients were using prednisone on a daily basis when they developed COVID-19 symptoms, and two were taking belimumab or rituximab [66]. Furthermore, seven individuals were taking hydroxychloroquine prior to COVID-19 and continued to take it during the infection [66]. Hospitalized SLE patients with COVID-19 were more likely to be admitted to the critical care unit and have severe consequences, especially if they had comorbidities such as hypertension, chronic kidney disease, being older, or being male [68]. Furthermore, 9.5% of COVID-19-infected hospitalized SLE patients died, and severe infection was linked to comorbidities such hypertension and chronic renal disease [68]. Pre-existing anti-IFN autoantibodies in SLE patients may possibly have a role in the greater severity of COVID-19 in this cohort [66]. However, it is important to note that the study cannot conclude if SLE patients are more likely to be admitted with COVID-19 than non-SLE individuals based on the mechanism of collection of the case information and the mix of rheumatic diseases in the cohort [68]. More research is needed to fully understand the relationship between COVID-19 and patients with SLE.
Due to immune system malfunction and immunosuppressive medication use, SLE patients are at an elevated risk for COVID-19 [68]. While some studies have discovered an increased incidence of COVID-19 hospitalization in SLE patients, the evidence is still limited [68]. A previous Danish study discovered a statistically non-significant 40% increased risk of hospitalization in SLE patients with COVID-19 [68]. This increased risk could be attributed to SLE patients' reduced immunological function [67]. COVID-19 elicits a strong immunological response, which can lead to inflammation in the lower lung airways. This could result in cytokine storms, which are thought to be important to the illness process that leads to ARF and multi-organ failure [67]. Due to COVID-19, SLE patients may undergo a change from Th1 to Th2 cells, resulting in autoimmune phenomena and possible illness [67]. In SLE patients, the adaptive immune system is often compromised, with increased autoreactivity of T and B cells and autoantibody production [67]. SLE patients have impaired production of interferon gamma, IL-1, IL-2, and TNF alpha, which may further damage their immunological response to COVID-19 [67]. Anti-IFN autoantibodies in SLE patients may predispose them to COVID-19 by inhibiting the function of an important antiviral cytokine [66]. Anti-IFN autoantibodies, on the other hand, are related with improved clinical and laboratory parameters as well as normalization of the type I IFN-induced gene signature in SLE, which should influence preventive approaches and management of this patient subset [66]. Overall, these characteristics may explain the severity of COVID-19 in SLE patients, and the existence of anti-IFN autoantibodies may be a useful prognostic marker for predicting which SLE patients will develop COVID-19 and informing preventive strategies and patient care [67,66].
COVID-19 infection puts patients with systemic lupus erythematosus (SLE) at risk of significant consequences. SLE and COVID-19, for example, can both cause myopericarditis, which may constitute a concern for people with SLE who get COVID-19 [67]. Furthermore, cardiac tamponade has been documented in both cases, which can result in significant morbidity and mortality [67]. It is crucial to highlight that in patients with both illnesses, there may be overlap in symptoms associated with SLE and COVID-19. As a result, distinguishing between the two in the setting of COVID-19 infection in SLE patients can be difficult [67]. Pericardial effusion is prevalent in SLE but uncommon in COVID-19 [67]. However, clinicians must stay watchful because COVID-19 can produce a variety of problems in SLE patients, particularly those with compromised immunological function who may be more susceptible to cytokine storms. More research is needed to better understand the dangers of COVID-19 infection in SLE patients.
The Relationship between Multiple Sclerosis and COVID-19
The COVID-19 pandemic has posed significant challenges to the medical community, particularly those treating patients with multiple sclerosis (MS). Given the potential impact of the virus on individuals with MS, there have been several studies and investigations conducted on this subject. One such study systematically reviewed literature on COVID-19 in MS patients and analyzed data on COVID-19 in patients with MS, which included a cross-sectional study of COVID-19 patients with MS [69]. In addition, there have been pressing needs to address patient concerns during the pandemic, as evidenced by the pilot phase of an investigation into COVID-19 among people with MS [70]. Moreover, educational programs have been established to provide updated medical information related to COVID-19 infection and safety concerns for MS patients [71]. There have also been reports on COVID-19 cases in MS patients in the Netherlands, which provide an extensive overview of reported cases between February and June 2020 [72]. Other studies have focused on how COVID-19 has challenged neurologists in counseling MS patients and guiding disease management [73]. Importantly, disease-modifying therapies (DMTs) are a mainstay of MS treatment, and studies have identified potential associations of certain DMT classes with COVID-19 [74]. Finally, a study was conducted to compare COVID-19-related outcomes in an Italian cohort of MS patients with those without MS, aiming to determine how MS affects the severity of COVID-19 [75]. There is a pressing need for further research into the impact of COVID-19 on individuals with MS and how best to manage their care during this pandemic.
Neurologists face difficulties in providing guidance to patients with multiple sclerosis (MS) due to the high risk posed by the COVID-19 pandemic. The cornerstone of MS treatment is disease-modifying medications (DMTs); nevertheless, certain DMT classes have been linked to COVID-19 in specific studies [74]. Biogen, Novartis, Roche, Sanofi/Genzyme, Teva, and Merck are the manufacturers of DMTs that were utilized in this investigation or that may be impacted by COVID-19 [76]. Following a thorough analysis of the literature, specific DMT classes were found to be associated with COVID-19 in MS patients [69,74]. The clinical characteristics of COVID-19 and the potential impact of MS on the severity of COVID-19 were followed by a thorough section on potential adjustments to immunomodulatory therapy in MS patients with COVID-19 [77,75]. An educational initiative was launched in the early stages of the pandemic with the goal of providing current medical knowledge on COVID-19 infection, safety issues, and the urgent needs of individuals with multiple sclerosis [71,70]. Additionally, a comprehensive summary of all COVID-19 instances that were reported in MS patients in the Netherlands between February and June 2020 was given, emphasizing the necessity for more research into the relationship between MS and COVID-19 outcomes [72]. Lastly, it's crucial to remember that while Ms. MD has nothing to reveal, she edits the Multiple Sclerosis Journal and is a network executive for International Women in Multiple Sclerosis (iWiMS) [78].
Many obstacles concerning the treatment of multiple sclerosis (MS) and the application of disease-modifying treatments (DMTs) have been brought about by the COVID-19 pandemic [73]. DMTs are used to treat MS, which may be impacted by COVID-19. Several pharmaceutical companies, including Biogen, Merck, Novartis, Roche, Sanofi/Genzyme, and Teva, produce these drugs [76]. Data analysis and a thorough literature review were conducted in a cross-sectional study of COVID-19 among MS patients [69]. Based on a core set of criteria, a pilot study of COVID-19 among MS patients was started to address the urgent needs of MS patients during the pandemic [70]. In addition, a program for education was created to offer current medical knowledge on COVID-19 infection and safety issues [71]. Certain DMT classes and COVID-19 have been linked in several studies [74]. Important information on the implications of COVID-19 for MS management was gleaned from a systematic overview of COVID-19 cases reported in MS patients in the Netherlands between February and June 2020 [72]. Furthermore, a study comparing COVID-19-related outcomes gathered in an Italian MS patient cohort discovered that MS did not seem to have a significant impact on the severity of COVID-19 [75]. All things considered, treating MS during the COVID-19 epidemic necessitates reevaluating treatment plans and taking into account any possible effects on DMTs.
5. The use of AntiIL-6 receptor antibodies Tocilizumab and Sarilumab for COVID-19 treatment
Tocilizumab and Sarilumab are both immunomodulatory therapies that have been found to improve survival rates and reduce the duration of organ support in patients with COVID-19 [79]. These drugs are anti-IL-6 monoclonal antibodies, which block the cytokine receptor and target both the soluble and membrane IL-6 receptor [80]. Although the specific mechanism of action of these drugs is not elaborated in the given text, they are known to be monoclonal antibodies targeting the IL-6 receptor [80]. Studies have shown that the administration of anti-IL-6 monoclonal antibodies, such as Tocilizumab and Sarilumab, is associated with lower mortality rates in COVID-19 patients after 28 days of treatment [80]. In fact, Tocilizumab was found to have the best results of associations among the three drugs evaluated in a meta-analysis [80]. Furthermore, the simultaneous administration of IL-6 pathway inhibitors and corticosteroids has been found to provide better results than each drug in monotherapy [80]. While Sarilumab is a recombinant humanized anti-IL-6 receptor mAb, no information about the mechanism of action of Tocilizumab is provided in the given text [79].
Tocilizumab and Sarilumab have been tested in COVID-19 patients in clinical trials. A international, double-blind, randomized trial comparing the effectiveness and safety of sarilumab in COVID-19 hospitalized patients was done [79]. In hospitalized patients getting supplementary oxygen, the trial found no therapeutic benefit for sarilumab. If other medications are not available or viable, IV sarilumab in conjunction with dexamethasone can be administered [79]. Sarilumab can be used to treat COVID-19 in hospitalized adults [79]. A placebo-controlled clinical trial with Sarilumab recipients who had serious COVID-19 pneumonia, required mechanical ventilation, and were given corticosteroids at the start indicated a reduction in mortality by Day 22, although the difference was not statistically significant due to the small sample size [79]. Sarilumab did not show any benefit in a clinical trial done in the United States with patients suffering with severe and critical COVID-19 [79]. The text contains no information about clinical trials on Sarilumab in COVID-19 patients [79]. The FDA has approved tocilizumab for the treatment of COVID-19 in hospitalized people taking systemic corticosteroids and requiring supplementary oxygen, NIV, mechanical ventilation, or ECMO [79]. Tocilizumab in combination with corticosteroids was granted an Emergency Use Authorization by the FDA for the treatment of COVID-19 in hospitalized children aged 2 years who require supplemental oxygen, NIV, mechanical ventilation, or ECMO [79]. Both Tocilizumab and Sarilumab are anti-IL-6 medications being tested in the trial [80]. The clinical trial NCT04486521 was done on COVID-19 individuals with CRS who received a combination of corticosteroids and anti-IL-6 medications. The trial compares combination therapy to both medications administered alone [80].
Tocilizumab and Sarilumab are two drugs found to be effective in treating COVID-19, as per clinical trial results. In fact, these are the first drugs found to be effective against COVID-19 since the WHO recommended the use of corticosteroids in September 2020 [81]. The clinical trials conducted on these drugs suggest that they are effective in treating COVID-19, particularly in severely or critically ill patients. These medications work to inhibit the immune system's response in these individuals, which is a primary cause of morbidity and mortality in COVID-19 [81]. Tocilizumab and Sarilumab are utilized in COVID-19 treatment, and their efficacy in patients with cytokine release syndrome (CRS) has been evaluated in combination with corticosteroids [81]. These clinical trials have yielded excellent findings, indicating that these medications have the potential to significantly improve the outcomes of COVID-19 patients. However, more research is needed to discover the best dosages, administration routes, and treatment duration for these medications in order to achieve maximal efficacy while avoiding side effects.
6. The Use of IL1 Inhibitors in COVID-19 Treatment
Inflammation has an important role in the pathophysiology of serious infections and acute respiratory distress syndrome (ARDS) [82]. Recent research has revealed that interleukin-1 (IL-1) plays a critical role in the immunological response to SARS-CoV-2 infection, which induces COVID-19. In individuals with symptomatic COVID-19 infection, evidence shows that IL-1 may be a potential target for host-directed treatments [82]. In individuals with severe COVID-19 illness, the IL-1/IL-6 pathway, which is predominantly involved in inflammation regulation, is substantially elevated [82]. Furthermore, inhibiting the IL-1 pathway is one potential immune modulatory treatment for severe COVID-19. However, the data for the benefit or harm of this intervention in COVID-19 is currently limited to small observational trials [82]. More research is required to assess the efficacy and safety of inhibiting the IL-1 pathway as a therapy for severe COVID-19 disease.
Anakinra is a bioengineered version of IL-1ra, a naturally occurring interleukin-1 receptor antagonist [82]. Anakinra, as an IL-1 inhibitor, suppresses IL-1 function by attaching to its receptor [83]. Dendritic cells and mononuclear macrophages triggered by PRRs generate IL-1 [83]. Anakinra binds to the IL-1 receptor and blocks IL-1 from attaching to its receptor, hence blocking the downstream actions of IL-1. The suppression of IL-1 occurs spontaneously as a self-regulation feedback mechanism [83]. Anakinra is commonly used in patients suffering from autoimmune and inflammatory illnesses, as well as MAS [82]. Because it is like its physiologic mechanism, Anakinra's activity is expected to be safe. It has only minor immunosuppressive effects and has no influence on the body's ability to eliminate bacterial or fungal infections [82]. Anakinra has been demonstrated to benefit COVID-19 patients by lowering the need for mechanical ventilation and death in severe COVID-19 pneumonia patients without causing serious side effects [83]. Nonetheless, RCT validation is required for additional proof of anakinra's efficacy in treating severe COVID-19 [83]. It is crucial to emphasize that inhibiting IL-1 may increase certain components of dysregulated host defense, so its usage should be used with caution [82]. Anakinra does not directly inhibit the crucial IFN-STAT1/STAT2 pathway [82]. Anakinra functions as an IL-1 inhibitor [83].
The potential benefits of using Anakinra in COVID-19 treatment have been explored by numerous researchers. Anakinra is known to have inhibitory effects on IL-1, and it has been hypothesized that this could be a significant factor in treating COVID-19. Specifically, Anakinra targets the cytokine storm syndrome that is driven by IL-1/IL-6 [82]. This is relevant because the cytokine storm syndrome is a common complication among COVID-19 patients, and it can be deadly. By inhibiting IL-1, Anakinra may be able to reduce the severity of the cytokine storm syndrome and improve patient outcomes. Anakinra is a recombinant IL-1 receptor antagonist that is a modified variant of the human IL-1 inhibitor. As a result, it has been used to treat a wide range of inflammatory disorders, such as rheumatoid arthritis and systemic juvenile idiopathic arthritis. While more research is required to determine Anakinra's efficacy in treating COVID-19, its potential as a therapy alternative is encouraging.
7. The Role of Molecular Mimicry in Covid-19 and Autoimmunity
Molecular mimicry is a phenomenon that has been studied in relation to autoimmunity. It is a potential mechanism by which viral infections can lead to autoimmunity [84]. In vitro studies of molecular mimicry have been conducted in relation to severe acute respiratory syndrome (SARS) caused by SARS-CoV [84]. In fact, molecular mimicry-based autoimmunity has been reported in SARS patients, highlighting the significance of this phenomenon in autoimmune disorders [84]. The core idea behind molecular mimicry is that pathogenic viral or bacterial proteins share sequence similarities with host proteins. Subsequently, the immune system starts attacking host proteins, mistaking them for the pathogen. This can lead to chronic inflammation and autoimmune diseases [84]. While there are no specific takeaways related to this topic, it is important to note that molecular mimicry plays a key role in the development of autoimmune disorders and requires further research to better understand its mechanisms and impact on human health.
A growing body of research has emerged because of the COVID-19 pandemic, suggesting that molecular mimicry actively contributes to the development of COVID-19 autoimmunity [85]. SARS-CoV-2 has the capacity to induce autoimmunity through viral proteins' molecular mimicry of human molecular chaperones. Certain human molecular chaperones, in particular heat shock proteins, can engage in molecular mimicry after contracting SARS-CoV-2 [85]. It has previously been documented that several chaperones that may participate in molecular mimicry after SARS-CoV-2 infection are localized in the plasma-cell membrane of endothelial cells [85]. Molecular chaperones may migrate to the plasma-cell membrane and exit the cell because of stress from diabetes and hypertension, which could lead the immune system to identify them as foreign antigens [85]. Moreover, shared peptides between chaperones and viral proteins comprise immunogenic epitopes expected for B or T cells; molecular chaperones make up 17 of these shared peptides [85]. The presence of DNAJ family proteins on the plasma membrane may be an indication of this since they are subject to the immune response [85]. According to the bioinformatics immunogenic epitope prediction tool, there is a high probability that the human immune system will identify shared peptides between 17 human chaperones and viral proteins, leading to an autoimmune reaction [85]. But more research is still needed to fully understand this theory [85]. The development of safe and effective vaccines can benefit from research on molecular mimicry phenomena in the design of experiments and clinical trials [85].
Recent studies have provided evidence of the influence of COVID-19 on subsequent autoimmunity through molecular mimicry. Molecular mimicry, a phenomenon that occurs when an exogenous agent shares structural similarity with self-antigens, has been proposed as a cause of the autoimmune phenomena observed in COVID-19 [86,87]. The progression of COVID-19 from step 2 to step 3 relies on molecular mimicry phenomena, further supporting the idea that SARS-CoV-2 triggers autoimmune diseases through molecular mimicry [88]. Several studies have focused on potential autoimmune diseases that may arise due to molecular mimicry triggered by COVID-19. For instance, it has been suggested that COVID-19 may trigger autoimmune diseases such as Guillain-Barre Syndrome and autoimmune hepatitis through molecular mimicry [89,84]. In addition, computational analysis has highlighted molecular mimicry hotspots in Spike protein, which may play a role in the development of autoimmune diseases [90]. While it has not yet been proved that molecular mimicry is the initiating factor in the development of autoimmune diseases, it is increasingly being recognized as a valid construct to explain the pathogenesis of such diseases [91]. Therefore, studying molecular mimicry phenomena will not only help in understanding the pathogenesis of COVID-19 but also in identifying potential autoimmune diseases that may arise due to molecular mimicry triggered by COVID-19 [85].
8. Histopathological Signs of Autoimmune Reactions in COVID-19
Various strains of viruses, including Epstein-Barr virus, herpes virus 6, cytomegalovirus, hepatitis A and C virus, parvovirus B19, rubella virus, and human T cell lymphotropic virus type 1, have been linked to the induction of autoimmunity [92]. Viral mimicry, epitope dissemination, and the loss of tolerance against self-antigens presented in the context of microbial infection are all proposed mechanisms for autoimmune induction [92]. The existence of autoantibodies has been observed in COVID-19 patients, but more tests are needed to assess their relevance to tissue damage [92]. COVID-19 has also been associated with autoimmune illnesses and disorders. Autoantibodies have not been adequately studied in patients with post-COVID-19 disorders or in the general healthy community. The formation of a harmful, self-sustaining autoimmune response against self-tissue antigens may be responsible for some people's post-COVID-19 symptoms [92]. Thus, understanding the likely histopathological indications of autoimmune reactions in COVID-19 is critical for improving clinical results and long-term patient treatment.
COVID-19 has been studied extensively, with a particular focus on its immune response and inflammatory reactions. The pathophysiology of the virus remains unclear, but it appears to share similarities with autoimmune diseases (ADs) in terms of its inflammatory immune response [93,94]. However, there is currently no evidence of coronavirus-induced pathological changes in organs or tissues other than the lungs [95]. Despite the respiratory and immune systems being the primary targets of COVID-19, acute kidney injury and proteinuria have also been observed [96]. In research studies, patients with diagnosed autoimmune diseases were excluded from analysis, indicating that COVID-19 may affect these individuals differently than those without a pre-existing autoimmune condition [97]. Infection with SARS-CoV-2 has also been associated to aberrant inflammatory and autoimmune responses, with one infected mink showing elevated autoimmune reactions [98]. There is even evidence that COVID-19 can cause autoimmune-mediated liver damage in children [99]. COVID-19 has been linked to autoimmune illnesses and disorders, prompting additional research into the relationship [92]. Even more troubling is research associating autoantibodies detected in COVID-19 patients to chronic autoimmune illnesses, even though the incidence of these autoantibodies in post-COVID-19 syndrome patients and healthy individuals is unknown [100]. Overall, there is still much to learn about how COVID-19 affects those with autoimmune conditions and the potential for autoimmunity following infection with the virus. Animal models have been developed to better understand these outcomes [101].
Histopathological signs in COVID-19 patients have significant implications for the treatment and management of the disease. Studies have identified various lung histopathological changes resulting from COVID-19 infection, including inflammatory responses and changes in lung tissue structure [102]. While COVID-19 shares similarities with autoimmune diseases in terms of immune response and inflammatory reactions [103,94], delayed immune responses to the virus may also play a role in pathological mechanisms [104]. Moreover, although COVID-19 primarily targets the respiratory and immune systems, other organs and tissues may also be affected, such as the kidneys and liver [95,96,99]. The development of autoimmune diseases and syndromes has also been associated with COVID-19 infection, making it an important consideration in disease management [92]. Furthermore, research has linked autoantibodies to chronic autoimmune diseases, indicating a potential connection between COVID-19 and the development of these diseases [100]. These histopathological signs should be considered when developing treatment plans and management strategies for COVID-19 patients. It is important to consider the potential development of autoimmune diseases and to monitor for signs of organ damage throughout the course of the disease. Further investigations into the mechanisms underlying these histopathological changes are necessary to develop more effective treatment strategies for COVID-19.
9. The Role of Autoimmunity in PASC (PostAcute Sequelae of SARS-CoV-2 Infection)
Post-acute sequelae of SARS-CoV-2 infection, or PASC for short, is a chronic illness that can afflict both adults and children. Tiredness, flu-like symptoms, autonomic dysfunction, memory or attention issues, and malaise after exercise are some of the symptoms of PASC [105]. Patients with PASC report symptoms that are either recurrent or intermittent [105,106]. Children can develop PASC; in earlier COVID-19 waves, the incidence reached up to 25%. Approximately 6% of children infected with SARS-CoV-2 met the criteria for PASC [105]. The worst post-COVID-19 sequelae in children are multisystem inflammatory syndrome (MIS-C), which has been classified as a component of the PASC spectrum [105]. Even though more than 200 PASC symptoms have been identified, each individual's symptom presentation is unique [105]. Numerous reports have surfaced of the Zika virus being spread sexually months after the patient has recovered from the acute illness, and people who have persistent Ebola have caused new outbreaks of the disease years after the patient has recovered from the acute illness. These precedents suggest that PASC could be caused by viral reservoirs. Replicating virus and/or viral RNA may remain in patients' tissues in a "reservoir" after acute infection, meaning that some PASC patients may not be able to fully eradicate the SARS-CoV-2 virus [105]. Changes in host signaling or epithelial barrier permeability brought on by microbiome/virome dysbiosis may make PASC symptoms worse [106]. Different therapy approaches might be needed in order to treat patients with a PASC diagnosis as effectively as possible [106].
Autoimmunity may be a factor in the post-acute sequelae of SARS-CoV-2 infection (PASC) [106]. When the immune system creates antibodies against its own cells and tissues, it causes tissue damage and inflammation [106].[107]. Autoantibodies may be formed in response to SARS-CoV-2 or other pathogens/organisms in the same niche in the instance of COVID-19 [106]. When evaluating data on autoantibody synthesis in COVID-19 patients, it is critical to evaluate the activities of these pathogens/organisms [106]. Autoantibodies can form as a result of molecular mimicry or sequence homology between peptides and proteins from the host and the organism, which can result in the creation of autoantibodies that target human proteins [106]. The makeup and virulence of patient microbiome/virome communities can lead to the generation of cross-reactive autoantibodies. Pathogens that can reactivate in COVID-19 tissue can also contribute to autoantibody synthesis [106]. COVID-19-induced autoantibody synthesis may persist following acute COVID-19 disease resolution, resulting in PASC symptoms [106]. Although COVID-19 "autoantibodies" are uncommon, their existence might induce collateral damage and inflammation, which could explain a considerable amount of patient clinical variance [106]. The trial will include tests for autoimmune diseases to rule out other diagnoses, and IVIG has been proposed as a therapy for certain autoimmune diseases, including those related to PASC, due to its ability to regulate innate and acquired immunity and inhibit immune cell and inflammatory pathway activation [107]. EBV infection has been linked to autoimmunity via the generation of immunoglobulins that react with human autoantigens [106].
There is growing evidence suggesting that autoimmunity plays a role in post-acute sequelae of SARS-CoV-2 infection (PASC). Several clinical entities associated with autoimmune mechanisms have been reported in patients with PASC [108]. In fact, some individuals with PASC may not fully clear SARS-CoV-2 after initial infection, leading to chronic post-viral complications like previous infections, such as ME/CFS, and can interfere with return to normal life [109,110]. One hypothesis is that the SARS-CoV-2 virus induces autoimmunity, leading to persistent symptoms [107]. The strongest evidence supporting a role for SARS-CoV-2-specific immunity in PASC lies in the presence of atypical memory B cells (atMBCs), which are also associated with the production of autoantibodies in several autoimmune diseases [111]. Autoantibodies can arise because of molecular mimicry between host and organism peptides and proteins. In an analysis of multiple sclerosis, for instance, it was suggested that molecular mimicry-based autoimmunity could be driven by persistent viral infection [105]. Moreover, a post-infectious autoimmune mechanism has been suggested in previous cases of Guillain-Barré syndrome (GBS) associated with GD1b antibodies [112]. Therefore, further research is needed to better understand the role of autoimmunity in PASC and identify appropriate therapies.
Conclusions and Future Research
Autoimmune diseases are chronic, debilitating illnesses that harm individuals, families, society, and the healthcare system. Aside from that, pandemics are always associated with several concomitant difficulties and obstacles, as well as potential sequelae that may emerge early or late after the pandemic. According to the findings of COVID-19-mediated autoimmunity, autoimmunity may be a significant COVID-19 complication. Understanding the pathophysiology of autoimmune manifestations in COVID-19 patients may aid in further elucidating the mechanism of viral injury to the host's body, whether direct viral injury or autoimmune reactivity, which may lead to the development of a better and more efficient treatment strategy. On the other hand, a time gap between the COVID-19 pandemic and autoimmune presentations is expected, assuming immune system reactivity due to COVID-19 infection and considering prior experience with the delay between the surge in the number of MIS-C or Kawasaki-like disease and the spread peaks of COVID-19 [113]. Therefore, keeping an eye on and preventing the onset or exacerbation of autoimmune symptoms may be made easier with a more precise comprehension of the pertinent pathways.
References
- Reynolds, J., Putterman, C. Progress and unmet needs in understanding fundamental mechanisms of autoimmunity. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0896841123000082.
- RamaKrishnan, A., Sankaranarayanan, K. Understanding autoimmunity: The ion channel perspective. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S1568997216300301.
- Gudjonsson, J., Kabashima, K., Eyerich, K. Mechanisms of skin autoimmunity: cellular and soluble immune components of the skin. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0091674920306862.
- Theofilopoulos, A., Kono, D., Baccala, R. The multiple pathways to autoimmunity. (n.d.) Retrieved November 25, 2023, from www.nature.com/articles/ni.3731.
- Jones, D., Diamond, A. The basis of autoimmunity: an overview. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0950351X9580787X.
- Sudres, M., Verdier, J., Truffault, F. Pathophysiological mechanisms of autoimmunity. (n.d.) Retrieved November 25, 2023, from nyaspubs.onlinelibrary.wiley.com/doi/abs/10.1111/nyas.13560.
- Simmonds, M., Gough, S. Genetic insights into disease mechanisms of autoimmunity. (n.d.) Retrieved November 25, 2023, from academic.oup.com/bmb/article-abstract/71/1/93/275997.
- Rose, N. Mechanisms of autoimmunity. (n.d.) Retrieved November 25, 2023, from www.thieme-connect.com.
- Correa-Rodríguez, M., Rueda-Medina, B. [HTML][HTML] COVID-19 vaccine literacy in patients with systemic autoimmune diseases. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s12144-022-02713-y.
- Li, X., Gao, L., Tong, X., Chan, V., Chui, C., Lai, F. Autoimmune conditions following mRNA (BNT162b2) and inactivated (CoronaVac) COVID-19 vaccination: a descriptive cohort study among 1.1 million vaccinated …. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0896841122000385.
- Sen, P., Ravichandran, N., Nune, A., Lilleker, J. COVID-19 vaccination-related adverse events among autoimmune disease patients: results from the COVAD study. (n.d.) Retrieved November 25, 2023, from academic.oup.com.
- Boekel, L., Steenhuis, M., Hooijberg, F. Antibody development after COVID-19 vaccination in patients with autoimmune diseases in the Netherlands: a substudy of data from two prospective cohort studies. (n.d.) Retrieved November 25, 2023, from www.thelancet.com.
- Sen, P., Gupta, L., Lilleker, J., Aggarwal, V. [HTML][HTML] COVID-19 vaccination in autoimmune disease (COVAD) survey protocol. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s00296-021-05046-4.
- Boekel, L., Kummer, L., van Dam, K. Adverse events after first COVID-19 vaccination in patients with autoimmune diseases. (n.d.) Retrieved November 25, 2023, from www.thelancet.com.
- Velikova, T., Georgiev, T. [HTML][HTML] SARS-CoV-2 vaccines and autoimmune diseases amidst the COVID-19 crisis. (n.d.) Retrieved November 25, 2023, from link.springer.com.
- Chen, Y., Xu, Z., Wang, P., Li, X., Shuai, Z., Ye, D. New-onset autoimmune phenomena post-COVID-19 vaccination. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/imm.13443.
- Gil-Vila, A., Ravichandran, N. COVID-19 vaccination in autoimmune diseases (COVAD) study: vaccine safety in idiopathic inflammatory myopathies. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1002/mus.27681.
- ITP and COVID-19: Risks, Complications, Considerations. (n.d.) Retrieved November 25, 2023, from www.verywellhealth.com/itp-and-covid-19-5190834.
- COVID-19 associated with immune thrombocytopenia. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC8862167/.
- A Case of COVID-19-Induced Immune Thrombocytopenia .... (n.d.) Retrieved November 25, 2023, from www.cureus.com.
- Immune Thrombocytopenic Purpura (ITP) Following .... (n.d.) Retrieved November 25, 2023, from www.cureus.com.
- COVID-19 and ITP: Frequently Asked Questions. (n.d.) Retrieved November 25, 2023, from www.hematology.org/covid-19/covid-19-and-itp.
- Secondary immune thrombocytopenia supposedly .... (n.d.) Retrieved November 25, 2023, from casereports.bmj.com/content/14/5/e242220.
- SARS-CoV-2 Infection Inducing Immune .... (n.d.) Retrieved November 25, 2023, from www.ochsnerjournal.org/content/21/2/187.
- Immune thrombocytopenia and COVID-19: Case report and .... (n.d.) Retrieved November 25, 2023, from journals.sagepub.com/doi/full/10.1177/09612033211021161.
- Immune Thrombocytopenic Purpura Following COVID-19 .... (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC10284310/.
- Idiopathic Thrombocytopenic Purpura Related to COVID-19. (n.d.) Retrieved November 25, 2023, from www.journalmc.org/index.php/JMC/article/view/3518/2819.
- Abu-Rumeileh, S., Abdelhak, A., Foschi, M., Tumani, H. [HTML][HTML] Guillain–Barré syndrome spectrum associated with COVID-19: an up-to-date systematic review of 73 cases. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s00415-020-10124-x.
- Gittermann, L., Feris, S. [HTML][HTML] Relation between COVID-19 and Guillain-Barré syndrome in adults: a systematic review. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S2173580820302145.
- El Otmani, H., El Moutawakil, B., Rafai, M. Covid-19 and Guillain-Barré syndrome: more than a coincidence!. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7180370/.
- Sheikh, A., Chourasia, P., Javed, N. Association of Guillain-Barre syndrome with COVID-19 infection: An updated systematic review. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0165572821001041.
- Rahimi, K. [HTML][HTML] Guillain-Barre syndrome during COVID-19 pandemic: an overview of the reports. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s10072-020-04693-y.
- Caress, J., Castoro, R., Simmons, Z., Scelsa, S. COVID-19–associated Guillain-Barré syndrome: The early pandemic experience. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1002/mus.27024.
- McKean, N., Chircop, C. Guillain-Barré syndrome after COVID-19 vaccination. (n.d.) Retrieved November 25, 2023, from casereports.bmj.com/content/14/7/e244125.abstract.
- Keddie, S., Pakpoor, J., Mousele, C., Pipis, M., Machado, P. Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barré syndrome. (n.d.) Retrieved November 25, 2023, from academic.oup.com/brain/article-abstract/144/2/682/6031905.
- Yaqoob, A., Dar, W., Khuja, Z., Bukhari, I. [HTML][HTML] Miller Fisher syndrome associated with COVID 19. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC9648327/.
- Nishiguchi, Y., Matsuyama, H., Maeda, K., Shindo, A. [HTML][HTML] Miller Fisher syndrome following BNT162b2 mRNA coronavirus 2019 vaccination. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1186/s12883-021-02489-x.
- Manganotti, P., Pesavento, V., Buoite Stella, A. [HTML][HTML] Miller Fisher syndrome diagnosis and treatment in a patient with SARS-CoV-2. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s13365-020-00858-9.
- Lantos, J., Strauss, S., Lin, E. COVID-19–associated miller fisher syndrome: MRI findings. (n.d.) Retrieved November 25, 2023, from http://www.ajnr.org/content/41/7/1184.abstract.
- Li, Z., Li, X., Shen, J., Chan, M., Wu, W. [HTML][HTML] Miller Fisher syndrome associated with COVID-19: an up-to-date systematic review. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s11356-021-13233-w.
- Kim, J., Yoon, B., Kim, Y., Kim, J. Miller Fisher syndrome following COVID-19 vaccines: A scoping review. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/ane.13687.
- Biswas, S., Ghosh, R., Mandal, A., Pandit, A. COVID-19 induced miller fisher syndrome presenting with autonomic dysfunction: a unique case report and review of literature. (n.d.) Retrieved November 25, 2023, from journals.sagepub.com/doi/abs/10.1177/19418744211016709.
- Senel, M., Abu-Rumeileh, S., Michel, D. Miller-Fisher syndrome after COVID-19: neurochemical markers as an early sign of nervous system involvement. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/ene.14473.
- Siddiqi, A., Khan, T., Tahir, M., Asghar, M., Islam, M. [HTML][HTML] Miller Fisher syndrome after COVID-19 vaccination: Case report and review of literature. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC9276158/.
- COVID-19 and aPL Antibodies: Frequently Asked Questions. (n.d.) Retrieved November 25, 2023, from www.hematology.org/covid-19/covid-19-and-apl-ab.
- Coronavirus-disease-2019-induced antiphospholipid-like .... (n.d.) Retrieved November 25, 2023, from jmedicalcasereports.biomedcentral.com.
- Antiphospholipid antibodies and vitamin D deficiency in .... (n.d.) Retrieved November 25, 2023, from journals.plos.org.
- Antiphospholipid Syndrome & COVID-19: What to Know. (n.d.) Retrieved November 25, 2023, from www.hss.edu.
- COVID-19 and the antiphospholipid syndrome - PMC. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC9527199/.
- Antiphospholipid antibodies and COVID-19 thrombotic .... (n.d.) Retrieved November 25, 2023, from ard.bmj.com/content/80/9/1105.
- Antiphospholipid antibodies in COVID-19: a meta-analysis .... (n.d.) Retrieved November 25, 2023, from rmdopen.bmj.com/content/7/2/e001580.
- Antiphospholipid antibodies and neurological ... - The Lancet. (n.d.) Retrieved November 25, 2023, from www.thelancet.com.
- COVID-19 and antiphospholipid antibodies - Sage Journals. (n.d.) Retrieved November 25, 2023, from http://journals.sagepub.com/doi/10.1177/09612033211062523.
- Lidder, A., Pandit, S., Lazzaro, D. [HTML][HTML] An adult with COVID-19 kawasaki-like syndrome and ocular manifestations. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S2451993620301900.
- Viner, R., Whittaker, E. Kawasaki-like disease: emerging complication during the COVID-19 pandemic. (n.d.) Retrieved November 25, 2023, from www.thelancet.com.
- Fang, Y., Aravamudan, V., Sridharan, G. Kawasaki like illness due to COVID-19: a review of the literature. (n.d.) Retrieved November 25, 2023, from jidc.org/index.php/journal/article/view/14185.
- Akca, U., Kesici, S., Ozsurekci, Y., Aykan, H. [HTML][HTML] Kawasaki-like disease in children with COVID-19. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s00296-020-04701-6.
- Toubiana, J., Poirault, C., Corsia, A., Bajolle, F. [HTML][HTML] Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. (n.d.) Retrieved November 25, 2023, from www.bmj.com/content/369/bmj.m2094.long.
- Amirfakhryan, H. Kawasaki-like disease in children with COVID-19: A hypothesis. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0306987720317278.
- Shaigany, S., Gnirke, M., Guttmann, A., Chong, H. An adult with Kawasaki-like multisystem inflammatory syndrome associated with COVID-19. (n.d.) Retrieved November 25, 2023, from www.thelancet.com.
- Koné-Paut, I., Cimaz, R. Is it Kawasaki shock syndrome, Kawasaki-like disease or pediatric inflammatory multisystem disease? The importance of semantic in the era of COVID-19 pandemic. (n.d.) Retrieved November 25, 2023, from rmdopen.bmj.com/content/6/2/e001333.abstract.
- Berardicurti, O., Conforti, A., Ruscitti, P. The wide spectrum of Kawasaki-like disease associated with SARS-CoV-2 infection. (n.d.) Retrieved November 25, 2023, from www.tandfonline.com/doi/abs/10.1080/1744666X.2021.1847643.
- Pang, R., Zhao, J., Gan, Z., Hu, Z., Xue, X., Wu, Y. Evolution of COVID-19 in patients with autoimmune rheumatic diseases. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7762508/.
- Antonelli, A. COVID-19 and rheumatic autoimmune systemic diseases: report of a large Italian patients series. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s10067-020-05334-7.
- Montero, F., Martínez-Barrio, J. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: clinical characteristics of poor outcomes. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s00296-020-04676-4.
- Gupta, S., Nakabo, S., Chu, J., Hasni, S., Kaplan, M. Association between anti-interferon-alpha autoantibodies and COVID-19 in systemic lupus erythematosus. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7658959/.
- Mantovani Cardoso, E., Hundal, J., Feterman, D. Concomitant new diagnosis of systemic lupus erythematosus and COVID-19 with possible antiphospholipid syndrome. Just a coincidence? A case report and review of intertwining pathophysiology. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s10067-020-05310-1.
- Cordtz, R., Kristensen, S., Dalgaard, L. JCM | Free Full-Text | Incidence of COVID-19 Hospitalisation in Patients with Systemic Lupus Erythematosus: A Nationwide Cohort Study from Denmark. (n.d.) Retrieved November 25, 2023, from www.mdpi.com/2077-0383/10/17/3842.
- Barzegar, M., Mirmosayyeb, O. COVID-19 among patients with multiple sclerosis: a systematic review. (n.d.) Retrieved November 25, 2023, from nn.neurology.org/content/8/4/e1001.abstract.
- Sormani, M. An Italian programme for COVID-19 infection in multiple sclerosis. (n.d.) Retrieved November 25, 2023, from www.thelancet.com/lancet/article/S1474-4422(20)30147-2.
- Achiron, A., Dolev, M., Menascu, S. COVID-19 vaccination in patients with multiple sclerosis: what we have learnt by February 2021. (n.d.) Retrieved November 25, 2023, from journals.sagepub.com/doi/abs/10.1177/13524585211003476.
- Loonstra, F., Hoitsma, E. COVID-19 in multiple sclerosis: the Dutch experience. (n.d.) Retrieved November 25, 2023, from journals.sagepub.com/doi/abs/10.1177/1352458520942198.
- Bsteh, G., Bitschnau, C., Hegen, H., Auer, M. Multiple sclerosis and COVID-19: how many are at risk?. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/ene.14555.
- Simpson-Yap, S., De Brouwer, E., Kalincik, T., Rijke, N. [HTML][HTML] Associations of disease-modifying therapies with COVID-19 severity in multiple sclerosis. (n.d.) Retrieved November 25, 2023, from n.neurology.org/content/97/19/e1870?ct=.
- Sormani, M., Schiavetti, I., Carmisciano, L. [HTML][HTML] COVID-19 severity in multiple sclerosis: putting data into context. (n.d.) Retrieved November 25, 2023, from nn.neurology.org/content/9/1/e1105.abstract.
- Tallantyre, E., Vickaryous, N., Anderson, V. COVID-19 vaccine response in people with multiple sclerosis. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1002/ana.26251.
- Maresa, J., Hartung, H. [PDF][PDF] Multiple sclerosis and COVID-19.. (n.d.) Retrieved November 25, 2023, from biomed.papers.upol.cz.
- Moss, B., Mahajan, K., Bermel, R. Multiple sclerosis management during the COVID-19 pandemic. (n.d.) Retrieved November 25, 2023, from journals.sagepub.com/doi/abs/10.1177/1352458520948231.
- Interleukin-6 Inhibitors. (n.d.) Retrieved November 25, 2023, from www.covid19treatmentguidelines.nih.gov.
- A New Approach to the Management of COVID-19. Antagonists of IL-6: Siltuximab. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s12325-022-02042-3.
- WHO recommends life-saving interleukin-6 receptor blockers for COVID-19 and urges producers to join efforts to rapidly increase access. (n.d.) Retrieved November 25, 2023, from www.who.int.
- Van de Veerdonk, F., Netea, M. Blocking IL-1 to prevent respiratory failure in COVID-19. (n.d.) Retrieved November 25, 2023, from ccforum.biomedcentral.com.
- Kim, J., Lee, J., Yang, J., Lee, K., Effenberger, M. Immunopathogenesis and treatment of cytokine storm in COVID-19. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7681075/.
- Salle, V. Coronavirus-induced autoimmunity. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S1521661621000310.
- Marino Gammazza, A., Légaré, S., Lo Bosco, G. [HTML][HTML] … with SARS-CoV-2 antigenic epitopes potentially capable of eliciting autoimmunity against endothelial cells: possible role of molecular mimicry in COVID-19. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s12192-020-01148-3.
- Rojas, M., Herrán, M., Ramírez-Santana, C. Molecular mimicry and autoimmunity in the time of COVID-19. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0896841123000793.
- Vahabi, M., Ghazanfari, T., Sepehrnia, S. Molecular mimicry, hyperactive immune system, and SARS-COV-2 are three prerequisites of the autoimmune disease triangle following COVID-19 infection. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S1567576922006671.
- Cappello, F., Marino Gammazza, A., Dieli, F. Does SARS-CoV-2 trigger stress-induced autoimmunity by molecular mimicry? A hypothesis. (n.d.) Retrieved November 25, 2023, from www.mdpi.com/2077-0383/9/7/2038.
- Ehrenfeld, M., Tincani, A., Andreoli, L., Cattalini, M. Covid-19 and autoimmunity. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S1568997220301610.
- Nunez-Castilla, J., Stebliankin, V., Baral, P., Balbin, C. [HTML][HTML] Potential autoimmunity resulting from molecular mimicry between SARS-CoV-2 spike and human proteins. (n.d.) Retrieved November 25, 2023, from www.mdpi.com/1999-4915/14/7/1415.
- Albert, L., Inman, R. Molecular mimicry and autoimmunity. (n.d.) Retrieved November 25, 2023, from www.nejm.org/doi/full/10.1056/NEJM199912303412707.
- Mehandru, S., Merad, M. [HTML][HTML] Pathological sequelae of long-haul COVID. (n.d.) Retrieved November 25, 2023, from www.nature.com/articles/s41590-021-01104-y.
- Kowalik, M., Trzonkowski, P. COVID-19—Toward a comprehensive understanding of the disease. (n.d.) Retrieved November 25, 2023, from journals.viamedica.pl/cardiology_journal/article/view/68719.
- Rodríguez, Y., Novelli, L., Rojas, M., De Santis, M. Autoinflammatory and autoimmune conditions at the crossroad of COVID-19. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0896841120301281.
- Yao, X., Li, T., He, Z., Ping, Y., Liu, H. A pathological report of three COVID-19 cases by minimal invasive autopsies. (n.d.) Retrieved November 25, 2023, from europepmc.org/article/med/32172546.
- Su, H., Yang, M., Wan, C., Yi, L., Tang, F., Zhu, H., Yi, F. [HTML][HTML] Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0085253820303690.
- El Hachem, M., Diociaiuti, A., Concato, C. … , histopathological and laboratory study of 19 consecutive Italian paediatric patients with chilblain-like lesions: lights and shadows on the relationship with COVID-19 …. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/jdv.16682.
- Song, Z., Bao, L., Deng, W., Liu, J., Ren, E., Lv, Q. [HTML][HTML] Integrated histopathological, lipidomic, and metabolomic profiles reveal mink is a useful animal model to mimic the pathogenicity of severe COVID-19 patients. (n.d.) Retrieved November 25, 2023, from www.nature.com/articles/s41392-022-00891-6.
- Cooper, S., Tobar, A., Konen, O., Orenstein, N. Long COVID-19 liver manifestation in children. (n.d.) Retrieved November 25, 2023, from journals.lww.com.
- Yong, S. Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. (n.d.) Retrieved November 25, 2023, from www.tandfonline.com/doi/abs/10.1080/23744235.2021.1924397.
- Gralinski, L., Baric, R. Molecular pathology of emerging coronavirus infections. (n.d.) Retrieved November 25, 2023, from pathsocjournals.onlinelibrary.wiley.com.
- Pannone, G., Caponio, V. [HTML][HTML] Lung histopathological findings in COVID-19 disease–a systematic review. (n.d.) Retrieved November 25, 2023, from infectagentscancer.biomedcentral.com.
- Li, H., Zhao, Y., Zhou, L., Hu, J. Cutaneous, skin histopathological manifestations and relationship to COVID-19 infection patients. (n.d.) Retrieved November 25, 2023, from onlinelibrary.wiley.com/doi/abs/10.1111/dth.14157.
- Rubio-Muniz, C., Puerta-Peña, M. [HTML][HTML] The broad spectrum of dermatological manifestations in COVID-19: clinical and histopathological features learned from a series of 34 cases. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7307079/.
- Proal, A., VanElzakker, M., Aleman, S., Bach, K. SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC). (n.d.) Retrieved November 25, 2023, from www.nature.com/articles/s41590-023-01601-2.
- Proal, A., VanElzakker, M. [HTML][HTML] Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. (n.d.) Retrieved November 25, 2023, from www.frontiersin.org.
- Reznik, S., Tiwari, A., Ashby Jr, C. [HTML][HTML] Intravenous immunoglobulin: A potential treatment for the post-acute sequelae of SARS-Cov-2 infection?. (n.d.) Retrieved November 25, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC9392972/.
- Peluso, M., Lu, S., Tang, A., Durstenfeld, M., Ho, H. Markers of immune activation and inflammation in individuals with post-acute sequelae of SARS-CoV-2 infection. (n.d.) Retrieved November 25, 2023, from www.medrxiv.org/content/10.1101/2021.07.09.21260287.abstract.
- Moghimi, N., Di Napoli, M., Biller, J., Siegler, J. [HTML][HTML] The neurological manifestations of post-acute sequelae of SARS-CoV-2 infection. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s11910-021-01130-1.
- Dreyer, N., Petruski-Ivleva, N., Albert, L. Identification of a vulnerable group for post-acute sequelae of SARS-CoV-2 (PASC): people with autoimmune diseases recover more slowly from COVID-19. (n.d.) Retrieved November 25, 2023, from www.tandfonline.com/doi/abs/10.2147/IJGM.S313486.
- Newell, K., Waickman, A. Inflammation, immunity, and antigen persistence in post-acute sequelae of SARS-CoV-2 infection. (n.d.) Retrieved November 25, 2023, from www.sciencedirect.com/science/article/pii/S0952791522000759.
- Younger, D. [HTML][HTML] Post-acute sequelae of SARS-CoV-2 infection (PASC): peripheral, autonomic, and central nervous system features in a child. (n.d.) Retrieved November 25, 2023, from link.springer.com/article/10.1007/s10072-021-05345-5.
- Bastard P, Rosen LB, Zhang Q, et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science. 2020; 370(6515): eabd4585.
- K. Peng et al., “Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study,” EClinicalMedicine, vol. 63, p. 102154, Sep. 2023. [CrossRef]
Figure 1.
Each autoimmune disease's crude incidence by COVID-19 and non-COVID categories [114].
Figure 1.
Each autoimmune disease's crude incidence by COVID-19 and non-COVID categories [114].
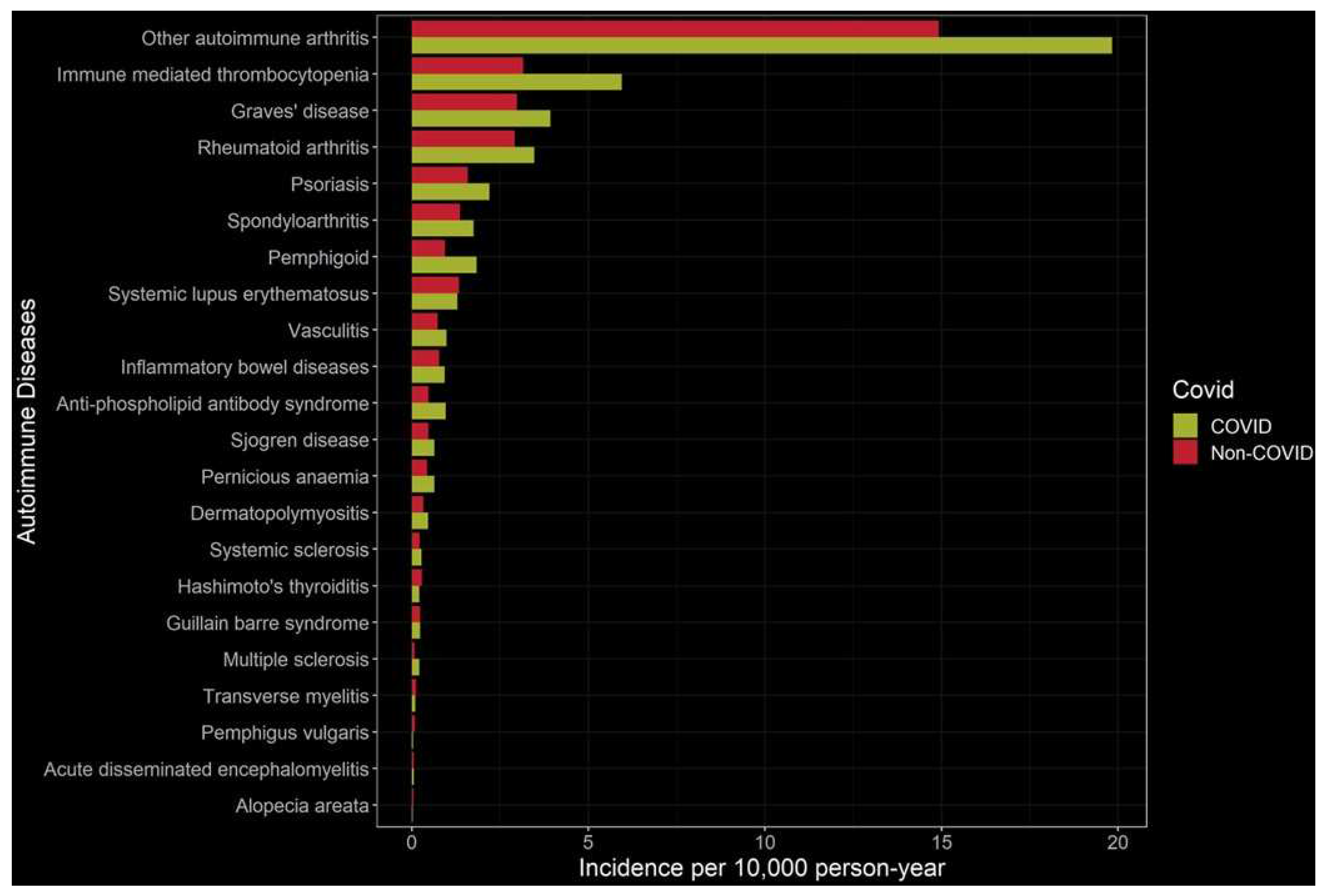
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



