
Submitted:
28 November 2023
Posted:
30 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The present study aimed to investigate the effects of a 10-week online high-intensity interval training (HIIT) on body composition and aerobic performance in physically sedentary women. A parallel two-group, longitudinal (pre, post) design was used with physical tests performed before (preintervention) and after (postintervention) the 10-week intervention period. A total of for-ty-eight healthy and physically sedentary women were recruited to participate in this study. Par-ticipants were distributed in two groups: The experimental group (EG) with 24 women (n = 24, age 21.21 ± 2.15 years, weight 61.16 ± 8.94 kg, height 163.96 ± 4.87 cm, body mass index body weight 22.69 ± 2.49 kg/m2), and the control group (CG) with another 24 women (n = 24, age 20.50 ± 1.29 years, weight 62.0 ± 6.65 kg, height 163.92 ± 4 .89 cm, body mass index 23.04 ± 1.74 kg/m2). The EG performed an online HIIT program for 10 weeks, while CG continued with their daily life routines. The repeated measures ANCOVA indicated a significant effect in the within-group analysis for weight (p=0.001; d=-0.96), demonstrating a significant decrease in the Experimental Group (EG) while the Control Group (CG) did not show a significant decrease in body mass in-dex (p=0.15; d=-0.11). Regarding maximal oxygen uptake (VO2 max) values, the EG exhibited a significant improvement (p=0.001; d=-1.07), whereas the CG did not demonstrate a significant improvement (p=0.08; d=-0.37). A new within-group analysis with power output (W) revealed that EG significantly improved (p=0.01; d=-0.96), while CG did not show a significant improve-ment in power output (W/kg) (p=0.20; d=-0.11). Lastly, the within-group analysis with Load re-vealed that EG significantly improved (p=0.001; d=-0.50), while CG did not show a significant improvement in Load (p=0.10.; d=-0.10). The present study showed that 10 weeks of HIIT in an online environment during the Covid-19 lockdown significantly improved maximum oxygen consumption, and caused weight loss and a significant decrease in body mass index in physically sedentary women. These results suggest HIIT may be used as a time-efficient strategy to improve body composition and cardio-respiratory fitness in sedentary women.
Keywords:
performance
; sedentary
; women
; anthropometric
; interval training
1. Introduction
The COVID-19 pandemic has ushered in unprecedented challenges, significantly disrupting daily routines and prompting profound changes in lifestyle patterns worldwide [1]. Government-imposed lockdowns and restrictions on mobility have led to a surge in sedentary behaviors among individuals, exacerbating concerns about health and well-being [2]. Sedentary lifestyles are associated with various health issues, including increased risks of cardiovascular diseases, obesity, and mental health disorders [3]. The pandemic's impact on physical activity underscores the critical need for innovative and accessible exercise solutions that can be implemented under restrictive conditions.
High-intensity interval training (HIIT) is estimated to be one of the most popular trends in fitness, according to the American College of Sports Medicine (ACSM) Annual Fitness Trend Forecast [4]. Indeed, HIIT is characterized by repeated short-term explosive-intensity anaerobic activities (≥85-90% maximal oxygen uptake [VO2 max] for health subjects or ≥80% VO2 max for clinical populations), interspersed by periods of passive or low-intensity exercise recovery, and it typically takes less than 30 minutes per training session [5,6]. In recent years, HIIT versus traditional moderate-intensity continuous exercise has been recognized as an alternative and popular exercise approach to further improve waist circumference, body fat (%), resting heart rate, aerobic fitness, and cardio-metabolic health in a shorter time in sedentary individuals [7,8,9].
Likewise, due to its anaerobic condition, HIIT training also offers great improvements in VO2 max which benefits both aerobically and anaerobically in a very short time compared to other methods [10]. Therefore, previous studies suggested that HIIT could be the solution to improve health and reduce morbidity in the adult population [11,12]. This type of training is tolerable and acceptable with physically sedentary people, although at first, it generated a lot of controversy in people with little training due to the high intensity that this mode of training entails. However, in recent years it has been prescribed to the elderly, young people, and adolescents [13]. Therefore, it must be taken into account that these HIIT training programs can cause a greater feeling of fatigue due to a higher ratio of perceived exertion (RPE) in comparison with the classic continuous training of moderate intensity [14].
The context of the COVID-19 pandemic, which disrupted regular exercise routines, underscores the relevance of understanding the impact of online HIIT during periods of restricted mobility and social distancing. While previous literature has predominantly delivered HIIT in a presential approach [7], the present study explores the novel approach of online delivery, considering the unique challenges and opportunities it presents. Therefore, the present study may contribute valuable insights into promoting accessible and effective exercise strategies, particularly during times of restricted mobility and social isolation.
Understanding how an online HIIT approach can impact individuals during a period of restricted mobility and social distancing is highly relevant. For the above reasons, the purpose of this study was to investigate the effects of a 10-week online HIIT intervention on body composition and aerobic performance variables in healthy physically sedentary women.
2. Materials and Methods
2.1. Experimental Approach to the problem
A parallel two-group, longitudinal (pre, post) design was used with physical tests performed before (preintervention) and after (postintervention) the 10-week intervention period. The participants were assigned and matched into two groups, an experimental group (EG) and a control group (CG). The participants from the CG were asked to maintain their daily life routines, while those from the EG were introduced to a one-hour HIIT familiarization session before the start of the intervention. Regarding the day of training, it was preceded by 48 hours of absence of high effort. The study was conducted between January and March 2021. (See Table 1, for more information).
2.2. Participants
A total of forty-eight physically sedentary women were recruited to participate in this study. There were two groups. Thus, the EG with twenty-four women (n = 24, age 21.21 ± 2.15 years, weight 61.16 ± 8.94 kg, height 163.96 ± 4.87 cm, body mass index body weight 22.69 ± 2.49 kg/m2), and the CG with another twenty-four women (n = 24, age 20.50 ± 1.29 years, weight 62.0 ± 6.65 kg, height 163.92 ± 4.89 cm, body mass index 23.04 ± 1.74 kg/m2). The randomization sequence was generated electronically (https://www.randomizer.org) and was concealed until interventions were assigned.
Moreover, a priori sample size calculation was performed using a free online tool, G*Power (www.gpower.hhu.de), with a power level of 95% and an α level of 0.05 and based on previous and similar studies [15] revealed that a sample size of >36 would be sufficient for conducting a randomized controlled trial. The sample group for this study was selected using the criterion sampling method, which falls under the category of purposive sampling techniques [16]. The inclusion criteria of the participants in this study were: i) being physically sedentary (not engaging in 150 minutes per week or moderate intensity, or 75 minutes per week of vigorous intensity, or a combination equivalent to these two different intensities); ii) not presenting any injury; iii) giving their consent, and iv) participating in at least 90% of the training sessions during the intervention.
Finally, the participants obtained information on the main objectives of the research and signed the informed consent. All the participants in this research were treated according to the guidelines of the American Psychological Association (APA), therefore the anonymity of the participants' responses was guaranteed. The study was carried out in accordance with the ethical principles of the Declaration of Helsinki for research in humans and was approved by the Research Ethics Committee of the Pontifical University of Comillas (2021/85).
2.3. Procedures
The forty-eight physically sedentary women enrolled in this study visited the laboratory twice, both for pre-test and post-test assessments, consistently between 9:30 am and 5:00 pm. Heart rate (HR) was monitored throughout all sessions. During each session, participants underwent a sub-maximal incremental fitness test on a stationary ergometer. Adhering to the guidelines outlined by the American College of Sports Medicine (2018), measures were taken to ensure the safety of physically sedentary women. Body mass, measured without shoes, utilized a bioelectrical impedance analysis (BIA) device (Tanita BC-730) accurate to the nearest 0.1 kg. Height was measured using a stadiometer (Type SECA 225, Hamburg, Germany) accurate to the nearest 0.1 cm. Body mass index was computed as mass (in kilograms) divided by the square of height (in meters).
All participants performed a sub-maximal incremental fitness test on a cycle ergometer (Viasprint 150 P cycle-ergometer) connected Jaeger Master Screen gas analyzer. Determination of the ventilatory anaerobic threshold (VAT) was based on the respiratory gas exchange method (RER) (RER = CO2 production/O2 consumption), which detected the VAT at the point at which RER exceeds the cut-off value of 1.0 [17]. First, an RS800CX Polar monitor (Polar Electro, Finland) was used to monitor and record heart rate (HR) during both sessions. In this sense, the protocol consisted of a submaximal incremental test with a fixed cadence of 60 revolutions per minute (rpm). The warm-up started at 0 W and the workload was increased by 10 W every min until min 5. The participant began the exercise phase pedaling at 50 W, and the workload was increased to 25 W every two min. After each increase, the workload remained stable for the next 2 minutes. The submaximal test ended once the VAT was reached. The highest power output (W) reached during the cycle ergometer test was registered. Finally, the highest power output reached was relativized by each participant's body weight (W/kg).
2.4. Training program
Concerning the training regimen, the Experimental Group (EG) engaged in a 10-week online program, involving three sessions per week. The sessions comprised High-Intensity Interval Training (HIIT) following the Tabata method, involving 4-minute intervals with 8 intensive training blocks, each followed by 1 minute of recovery [18]. The exercises involved body weight and functional movements, aligning with a protocol that demonstrated favorable outcomes in female university students [8]. Notably, the last session of each week focused on continuous running, as outlined in Table 2.
In the first month, they exercised for 20 seconds of intense intervals with 10 seconds of recovery, repeating it for 4 minutes. In the second month, they increased the technical difficulty of the exercises and increased the volume of the sessions until they achieved 20 minutes of Tabata in the last week of the intervention.
The HIIT sessions were carried out twice a week and their intensity were monitored daily using both HR. Participants were instructed to perform the exercise at maximum intensity while maintaining the correct technique. The structure of the session consisted of a 10–15-minute warm-up, a 35-minute main part, and a 10-minute cooldown. On the third day of each training week, the participants completed a moderate-intensity session outdoors, combining continuous running with walking. In the initial weeks of the exercise program, the intensity was within the 65-75% HRmax range. As the weeks progressed, the intensity gradually increased, and in the final week, it was within the 80-90% HRmax range, and the intensity of the walking was always at 40-45% HRmax during the 10 weeks.
Moreover, the rate of perceived exertion (RPE) was measured using the Borg’s Scale (6-20) as a supplement of the HR during each training session. Each participant was individually asked: "How did you perceive exertion during the exercise execution?". The first four weeks had an RPE of 12-13, indicating a somewhat hard level. The following four weeks were at an RPE of 15-16, signifying a hard level. In the last two weeks, the RPE was 18-19, representing an extremely hard level.

Table 3.
Example of HIIT and running session and work set progression during the HIIT program.
| Example of weekly session | |||
|---|---|---|---|
| 1st session | 2nd session | 3rd session | |
| Exercises | HIIT. Example 1 | HIIT. Example 2 | Running |
| 1st | Push-ups | Jumping jacks | 5 minutes of running at 65-75% HRmax |
| 2nd | Mountain Climbers | Box squat | 5 minutes of walking at 40-45% HRm |
| 3rd | Forearm plank | Bench step-ups | 5 minutes of running at 65-75% HRmax |
| 4th | Dips using a bench or chair | Deadweight | 5 minutes of walking |
| Training progression during the HIIT program | |||
| Week | Set/session | Recovery between sets (s) | |
| 1st and 2nd | 2 | 60 | |
| 3rd to 5th | 3 | 60 | |
| 6th to 8th | 4 | 60 | |
| 9th and 10th | 4 | 45 | |
Technical progressions in exercise complexity were systematically implemented throughout the experimental period. The progression for push-ups involved starting with hands against the wall, followed by positioning knees on the floor, and advancing to performing the exercise without resting the knees. Planks transitioned from forearms on the floor to arms fully extended. Similarly, jumping jacks initially began as static and progressed to dynamic, while squats advanced from using a box to incorporating a jump. This systematic approach extended to all exercises. In the initial two weeks, participants engaged in 8 minutes of Tabata, gradually increasing the volume as their physical condition improved, ultimately reaching a 20-minute Tabata duration.
Due to the COVID-19 confinement regulations mandated by the Spanish government, the training program had to be conducted inside participants' homes, where the absence of equipment led to the selection of calisthenics exercises.
2.5. Statistical procedures
Data were analyzed using Statistica software (version 10.0; Statsoft, Inc., Tulsa, OK, USA). Finally, the significance level was set at p < 0.05. Normal distribution and homogeneity tests (Kolmogorov–Smirnov and Levene’s, respectively) were conducted on all metrics. A paired sample t-test was used for determining differences as a repeated measures analysis (pre and post). Cohen’s d was the effect size indicator. To interpret the magnitude of the effect size, we adopted the following criteria: d ≤ 0.20, small; d ≤ 0.50, medium; and d ≤ 0.80, large. To elucidate between-group differences, an ANCOVA test was performed using the pretest as a covariate and the times pre and post as factors. To interpret the magnitude of the effect size of ANCOVA we adopted the following criteria: ηp2 = 0.02, small; ηp2 = 0.06, medium; and ηp2 = 0.14, large.
Results
Descriptive statistics were calculated for each variable (Table 2). No significant baseline between-group differences were recorded for all measurements (p > 0.05, d = 0.04–0.31). Moreover, the adherence rate to the online HIIT program in the experimental group was 96.3% ± 2.2%, and no withdrawals were reported.
Table 2.
Performance variables before (pretest) and after (posttest) the intervention period (mean ± SD).
Table 2.
Performance variables before (pretest) and after (posttest) the intervention period (mean ± SD).
| Participants (n = 48) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control Group (n = 24) | Experimental Group (n = 24) | Differences between Groups (ANCOVA Test) | |||||||
| Pretest | Posttest | % | RM t-test (p) | Pretest | Posttest | % | RM t-test (p) | ||
| Anthropometric measures | |||||||||
| Age (yrs) | 20.50 ±1.29 | - | - | - | 21.21 ±2.15 | - | - | - | - |
| Height (cm) | 163.92 ±4.89 | - | - | - | 163.96 ±4.87 | - | - | - | - |
| Weight (kg) | 62.00 ±6.65 | 62.53 ±7.07 | 0.75± 2.89 | p = 0.15 d =-0.08 | 61.16 ±8.94 | 59.26 ±8.73 | -3.22± 1.98 |
p = 0.001** d = 0.41 |
F(1,47) = 1244.36; p=0.000; ηp2 = 0.97 |
| Body Mass Index (%) | 23.04 ±1.74 | 23.24 ±1.97 | 0.75± 2.89 | p = 0.15 d = -0.11 | 22.69± 2.49 | 22.10± 2.47 | -2.72± 1.98 |
p = 0.001** d = 0.24 |
F(1,47) = 685.01; p=0.000; ηp2 = 0.35 |
| Incremental test | |||||||||
| VO2 max (ml/kg/min) |
20.17 ±2.03 |
21.03 ±2.59 |
3.37 ±10.37 |
p = 0.08 d = -0.37 |
20.58 ±3.65 |
24.67 ±3.98 |
15.94 ±12.08 |
p = 0.001** d = -1.07 |
F(1,47) = 32.38; p=0.000; ηp2 = 0.42 |
| Power output (W/kg) | 1.52 ±0.16 |
1.54 ±0.12 |
1.18 ±3.84 |
p = 0.20 d = -0.11 |
1.48 ±0.26 |
1.73 ±0.26 |
13.50 ±11.72 |
p = 0.001** d = -0.96 |
F(1,47) = 43.21; p=0.000; ηp2 = 0.49 |
| Power output (W) | 94.71 ±17.32 | 96.48 ±15.04 |
1.90 ±5.21 |
p = 0.10 d = -0.10 |
91.26 ±23.11 |
102.92 ±23.86 | 10.67 ±12.57 |
p = 0.001** d = -0.50 |
F(1,47) = 148.58; p=0.000; ηp2 = 0.77 |
Note: %: Percentage of change. RM: Repeated Measures * Denotes significance at p<0.05. and ** denotes significance at p<0.01.
Significant group*time interactions were observed through repeated measures ANCOVA for weight (p=0.001; ηp2=0.97), body mass index (p=0.001; ηp2=0.35), VO2 max (p=0.001; ηp2=0.42), power output (W/kg) (p=0.001; ηp2=0.49), and power output (W) (p=0.001; ηp2=0.87). In the EG, weight significantly decreased (p=0.001; d=-0.96), while CG did not show a significant change (p=0.15; d=-0.11) in body mass index. In terms of VO2 max, EG demonstrated significant improvement (p=0.001; d=-1.07), while CG did not exhibit a significant change (p=0.08; d=-0.37). A separate analysis of power output (W) revealed a significant improvement in EG (p=0.01; d=-0.96), while CG did not show a significant change in power output (W/kg) (p=0.20; d=-0.11). Lastly, the analysis of power output (W) showed significant improvement in EG (p=0.001; d=-0.50), whereas CG did not show a significant change (p=0.10; d=-0.10). Refer to Figure 1 and Figure 2 for a graphical representation.
Discussion
The purpose of this study was to investigate the impact of a 10-week online high-intensity interval training (HIIT) on body composition and aerobic performance amid the COVID-19 lockdown. The main evidence of the present study revealed that significant reductions in body weight were observed after the 10-week HIIT program compared to the CG. Moreover, there were significant improvements in aerobic fitness after the HIIT program compared to the CG.
HIIT is a successful strategy to lose weight, and fat mass in sedentary normal weight and overweight/obese women [19,20]. In our study, the 10-week HIIT led to significant weight loss (effect size: 0.41, moderate, -3.22%), and a decrease in body mass index (effect size: 0.24, moderate, -2.72%) compared to CG in sedentary young women. Recent studies demonstrated that 8 weeks [8] and 15 weeks [19] of HIIT caused losses in body mass, body fat (%), and body mass index in sedentary young females. Another study showed that 8 weeks of HIIT protocol (4 min., 8x20 s intensive intervals, each followed by 10 s of rest, based on functional exercises with their weight), performed 2–3 times a week, significantly decreased body composition for adults in strict home confinement during COVID-19 [18].
The results of the present study showed that online HIIT can be an effective stimulus for weight loss and decreasing BMI. A possible explanation for such findings could be related to the increase in post-exercise energy expenditure. HIIT has been shown to induce an excess post-exercise oxygen consumption (EPOC) [21]. This phenomenon involves elevated oxygen consumption and calorie expenditure, which may contribute to a negative energy balance and, consequently, weight loss over time [22]. The heightened metabolic rate during the post-exercise period could play a role in the observed improvements in body composition [7]. Contrary to our results, there were no significant changes in body weight, body mass index, and body fat percentage above 80% HRmax after HIIT exercises performed 3 days a week for 6 weeks [23], and 12 weeks [24,25] in sedentary young females. The different results in the studies may stem from the participants' characteristics, and the exercise program's content (duration, frequency, intensity, volume, and progression).
VO2 max is directly linked to cardiovascular health, and an increase of 1.0 ml/kg/min in VO2 max, which is accepted as a clinically meaningful alteration, results in a decrease in the risk of death from cardiovascular disease and all-cause mortality [26]. The present study demonstrated that in comparison to the CG, a 10-week online HIIT yielded substantial enhancements in VO2 max, power output (W/kg), and power output (W) parameters among sedentary young women. In line with these findings, Lu et al. [8] reported a significant increase in VO2 max (+18.8%) following an 8-week HIIT (6 × 3-min running bouts at 80–90% VO2 max with 2-min active recovery at 30–40% VO2 max) conducted thrice weekly in sedentary young females. Similarly, another study demonstrated that a cycling HIIT (6–10 bouts of 1 min duration at 80–90% output max) performed for 18–30 minutes per week over 12 weeks resulted in substantial improvements in VO2 max (approximately 22%) in sedentary young women [24].
Furthermore, prior observations have indicated that both low volume of High-Intensity Interval Training (HIIT) (1x4-min treadmill running at 85%–95% HRmax, followed by 3 min of recovery by running at 70% HRmax) and high volume of HIIT (4x4-min treadmill running at 85%–95% HRmax, followed by 3 min of recovery by running at 70% HRmax), executed thrice weekly over 6 weeks, exhibit equal effectiveness in enhancing aerobic capacity (VO2 max) among sedentary young women [15]. Incorporating a cycling HIIT for 12 weeks, consisting of 18–30 minutes per week, resulted in noteworthy enhancements (approximately 22%) in VO2 max among sedentary young women [24]. Moreover, a systematic review and meta-analysis study on adults indicated that short-term HIIT (<12 weeks) and long-term HIIT (≥12 weeks) performed at least 3 times a week for 12 weeks resulted in an increase in VO2 max. Also, the increase in aerobic capacity was reported to be greater at longer training times [7]. Furthermore, a meta-analysis study demonstrated that HIIT ranging from 2 to 8 weeks led to a substantial increase in VO2 max by 4.2–13.4% in healthy sedentary/recreationally active adults. The weighted mean effect size (g = 0.63; 95% CI, 0.39; 0.87) indicated a significant positive impact on aerobic capacity [27]. Lastly, the available evidence from the recent systematic review and meta-analysis emphasized that HIIT with a minimum of 4 weeks of exercise training (3 times per week, 18-30 minutes per session, 85-95% HRR) was an effective training protocol for augmenting maximal aerobic capacity in women with a sedentary lifestyle [28].
Considering the above studies, it can be said that longer durations of HIIT are required for greater improvements in VO2 max. However, it was observed that HIIT exercises for 2-12 weeks improved cardiorespiratory fitness or aerobic performance. In addition, in our study, a 15.94% VO2 max increase was detected after 10 weeks of HIIT protocol. Our results were in agreement with previous studies, which indicated that improvements of 9% to 13% were found in VO2 max following the 8 weeks [29], and 12 weeks [30] of HIIT protocol in sedentary individuals. Moreover, the observed improvement was attributed to the training intensity, emphasizing that aerobic exercise intensity plays a pivotal role in enhancing VO2 max. These findings underscore the significance of HIIT conducted at higher training intensities, specifically within the range of 90-95% HRmax, for achieving optimal training-induced enhancements in VO2 max, especially concerning age-related considerations. [24,29]. The considerable enhancement in VO2 max observed can be ascribed to the exercise intensity implemented in the HIIT. Additionally, existing literature, aligning with our study, highlights that individuals with a more sedentary lifestyle exhibit the most substantial VO2 max response. [24,28].
Furthermore, previous studies have suggested several physiological mechanisms underlying the improvement in VO2 max after HIIT protocol. For instance; in one study, it was suggested that the improvement in VO2 max or cardiorespiratory fitness after HIIT could be associated with several central adaptations, such as increases in systolic volume and cardiac output due to the increased cardiac contractility and oxygen availability. Also, it was asserted that peripheral changes such as increased muscle oxidative potential, increased skeletal muscle diffusion capacity, increased number and size of mitochondria, increased mitochondrial enzyme activity, arterial vasodilation, increased nitric oxide bioavailability, and reduced oxidative stress might be responsible for the improvement in VO2 max following the HIIT intervention [24,26]. Moreover, in another study, it was stated that HIIT-induced increases in VO2 max and improved maximal aerobic performance could partly be explained by specific oxidative adaptations in type II fibers [27].
This study has some limitations to be considered. The first limitation of the study is related to the use of cycle ergometer evaluation, which may not precisely reflect the intensities prescribed for running and jumping exercises in the online high-intensity interval training program. Secondly, we did not control other influencing factors that could influence our results. As the 10-week HIIT intervention took place in online fashion during the Covid-19 lockdown, the participants may have encountered difficulties in adjusting the exercise intensity through the use of their HR monitors. Furthermore, given that the sample consisted of sedentary individuals, the outcomes may have been impacted by the duration of exercise progressions. Therefore, future studies employing similar training protocols in sedentary populations might benefit from extending the intervention period.
Conclusion
The present study aimed to analyze the effects of a 10-week online HIIT on body composition and aerobic performance during the COVID-19 lockdown. The main findings showed that the 10-week online HIIT intervention yielded significant improvements in maximum oxygen consumption, weight loss, and a noteworthy decrease in body mass index among sedentary young females. These findings underscore the efficacy of HIIT as a time-efficient strategy for enhancing both body composition and cardiorespiratory fitness in sedentary women, even under limited circumstances such as a confinement period.
Author Contributions
Conceptualization, L.R.G; methodology, A.F.S., and R.S..; formal analysis, A.F.S., and R.S..; writing—original draft preparation, A.F.S., R.S., H.I.C., A.G.G. and A.L.G. Writing—review and editing, A.G.G and H.I.C., supervision, L.R.G. All authors have read and agreed to the published version of the manuscript. All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Funding
No specific sources of funding were used to assist in the preparation of this article.
Data Availability Statement
The corresponding author will freely make the raw data used to support this article's conclusions available.
Acknowledgments
We thank the participants for their collaboration with and participation in the study.
Conflicts of Interest
The researchers affirm that there were no financial or commercial ties that might be seen as creating a conflict of interest during the research's conduct.
References
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.E.; Janiri, D.; Moccia, L.; Janiri, L.; Sani, G. Will nothing be the same again?: Changes in lifestyle during COVID-19 pandemic and consequences on mental health. Int. J. Environ. Res. Public Health 2021, 18, 8433. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Dergaa, I.; Bachiller, V.; Saad, B.H. Global Implications of COVID-19 Pandemic on Adults’ Lifestyle Behavior: The Invisible Pandemic of Noncommunicable Disease. Int. J. Prev. Med. 2023, 8, 1–9. [Google Scholar]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J. Fam. Med. 2020, 41, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.R. Worldwide survey of fitness trends for 2019. ACSM's Health Fit. J. 2018, 22, 10–17. [Google Scholar] [CrossRef]
- Gibala, M.J.; Jones, A.M. Physiological and performance adaptations to high-intensity interval training. Nestle Nutr. Inst. Workshop Ser. 2013, 76, 51–60. [Google Scholar] [PubMed]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Batacan, R.B.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Lu, M.; Li, M.; Yi, L.; Li, F.; Feng, L.; Ji, T.; Zang, Y.; Qiu, J. Effects of 8-week High-Intensity Interval Training and Moderate-Intensity Continuous Training on Bone Metabolism in Sedentary Young Females. J. Exerc. Sci. Fit. 2022, 20, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The Impact of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Vascular Function: A Systematic Review and Meta-Analysis. Sport. Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Bartlett, D.B.; Willis, L.H.; Slentz, C.A.; Hoselton, A.; Kelly, L.; Huebner, J.L.; Kraus, V.B.; Moss, J.; Muehlbauer, M.J.; Spielmann, G.; et al. Ten weeks of high-intensity interval walk training is associated with reduced disease activity and improved innate immune function in older adults with rheumatoid arthritis: A pilot study. Arthritis Res. Ther. 2018, 20, 1–16. [Google Scholar] [CrossRef]
- Dorneles, G.P.; da Silva, I.; Boeira, M.C.; Valentini, D.; Fonseca, S.G.; Dal Lago, P.; Peres, A.; Romão, P.R.T. Cardiorespiratory fitness modulates the proportions of monocytes and T helper subsets in lean and obese men. Scand. J. Med. Sci. Sport 2019, 29, 1755–1765. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Lampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scand. J. Med. Sci. Sport 2019, 29, 1288–1304. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Azuma, K.; Tabata, S.; Katsukawa, F.; Ishida, H.; Oguma, Y.; Kawai, T.; Itoh, H.; Okuda, S.; Matsumoto, H. Effects of 16-week high-intensity interval training using upper and lower body ergometers on aerobic fitness and morphological changes in healthy men : A preliminary study. Open Access J. Sport Med. 2014, 5, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.R.R.; Slama, F.A.; Deslandes, A.C.; Furtado, E.S.; Santos, T.M. Continuous and high-intensity interval training: Which promotes higher pleasure? PLoS ONE 2013, 8, e79965. [Google Scholar] [CrossRef] [PubMed]
- Bhati, P.; Bansal, V.; Moiz, J.A. Comparison of different volumes of high intensity interval training on cardiac autonomic function in sedentary young women. Int. J. Adolesc. Med. Health 2021, 31, 1–13. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.P.; Gardner, R.M.; Adams, T.D.; Yanowitz, F.G.; Crapo, R.O. Anaerobic threshold: Problems of determination and validation. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Fernández, D.; Fernández-Rodríguez, R.; Taboada-Iglesias, Y.; Gutiérrez-Sánchez, Á. Impact of High-Intensity Interval Training on Body Composition and Depressive Symptoms in Adults under Home Confinement. Int. J. Environ. Res. Public Health 2022, 19, 6145. [Google Scholar] [CrossRef]
- Dupuit, M.; Maillard, F.; Pereira, B.; Marquezi, M.L.; Lancha, A.H.; Boisseau, N. Effect of high intensity interval training on body composition in women before and after menopause: A meta-analysis. Exp. Physiol. 2020, 105, 1470–1490. [Google Scholar] [CrossRef]
- Nunes, P.R.P.; Martins, F.M.; Souza, A.P.; Carneiro, M.A.S.; Orsatti, C.L.; Michelin, M.A.; Murta, E.F.; de Oliveira, E.P.; Orsatti, F.L. Effect of high-intensity interval training on body composition and inflammatory markers in obese postmenopausal women: A randomized controlled trial. Menopause 2019, 26, 256–264. [Google Scholar] [CrossRef]
- Greer, B.K.; O’brien, J.; Hornbuckle, L.M.; Panton, L.B. EPOC Comparison Between Resistance Training and High-Intensity Interval Training in Aerobically Fit Women. Int. J. Exerc. Sci. 2021, 14, 1027–1035. [Google Scholar] [PubMed]
- Panissa, V.L.G.; Fukuda, D.H.; Staibano, V.; Marques, M.; Franchini, E. Magnitude and duration of excess of post-exercise oxygen consumption between high-intensity interval and moderate-intensity continuous exercise: A systematic review. Obes. Rev. 2021, 22, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Chidnok, W.; Wadthaisong, M.; Iamsongkham, P.; Mheonprayoon, W.; Wirajalarbha, W.; Thitiwuthikiat, P.; Siriwittayawan, D.; Vachirasrisirikul, S.; Nuamchit, T. Effects of high-intensity interval training on vascular function and maximum oxygen uptake in young sedentary females. Int. J. Health Sci. 2020, 14, 3–8. [Google Scholar]
- Astorino, T.A.; Schubert, M.M.; Palumbo, E.; Stirling, D.; McMillan, D.W.; Cooper, C.; Godinez, J.; Martinez, D.; Gallant, R. Magnitude and time course of changes in maximal oxygen uptake in response to distinct regimens of chronic interval training in sedentary women. Eur. J. Appl. Physiol. 2013, 113, 2361–2369. [Google Scholar] [CrossRef] [PubMed]
- Nybo, L.; Sundstrup, E.; Jakobsen, M.D.; Mohr, M.; Hornstrup, T.; Simonsen, L.; Bülow, J.; Randers, M.B.; Nielsen, J.J.; Aagaard, P.; et al. High-intensity training versus traditional exercise interventions for promoting health. Med. Sci. Sports Exerc. 2010, 42, 1951–1958. [Google Scholar] [CrossRef] [PubMed]
- Arboleda Serna, V.H.; Arango Vélez, E.F.; Gómez Arias, R.D.; Feito, Y. Effects of a high-intensity interval training program versus a moderate-intensity continuous training program on maximal oxygen uptake and blood pressure in healthy adults: Study protocol for a randomized controlled trial. Trials 2016, 17, 1–8. [Google Scholar] [CrossRef]
- Sloth, M.; Sloth, D.; Overgaard, K.; Dalgas, U. Effects of sprint interval training on VO2max and aerobic exercise performance: A systematic review and meta-analysis. Scand. J. Med. Sci. Sport 2013, 23, 341–352. [Google Scholar] [CrossRef]
- Syamsudin, F.; Wungu, C.D.K.; Qurnianingsih, E.; Herawati, L. High-intensity interval training for improving maximum aerobic capacity in women with sedentary lifestyle: A systematic review and meta-analysis. J. Phys. Educ. Sport 2021, 21, 1788–1797. [Google Scholar]
- StØren, Ø.; Helgerud, J.; SÆbØ, M.; StØa, E.M.; Bratland-Sanda, S.; Unhjem, R.J.; Hoff, J.; Wang, E. The Effect of Age on the V-O2max Response to High-Intensity Interval Training. Med. Sci. Sports Exerc. 2017, 49, 78–85. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-La-O, A.; Jurado-Fasoli, L.; Dote-Montero, M.; Gutiérrez, Á.; Ruiz, J.R.; Castillo, M.J. . Changes in physical fitness after 12 weeks of structured concurrent exercise training, high intensity interval training, or whole-body electromyostimulation training in sedentary middle-aged adults: A randomized controlled trial. Front. Physiol. 2019, 10, 451. [Google Scholar] [CrossRef]
Figure 1.
Pre- and post-tests in CG and EG of anthropometrical measures (Weight and Body Mass Index).
Figure 1.
Pre- and post-tests in CG and EG of anthropometrical measures (Weight and Body Mass Index).
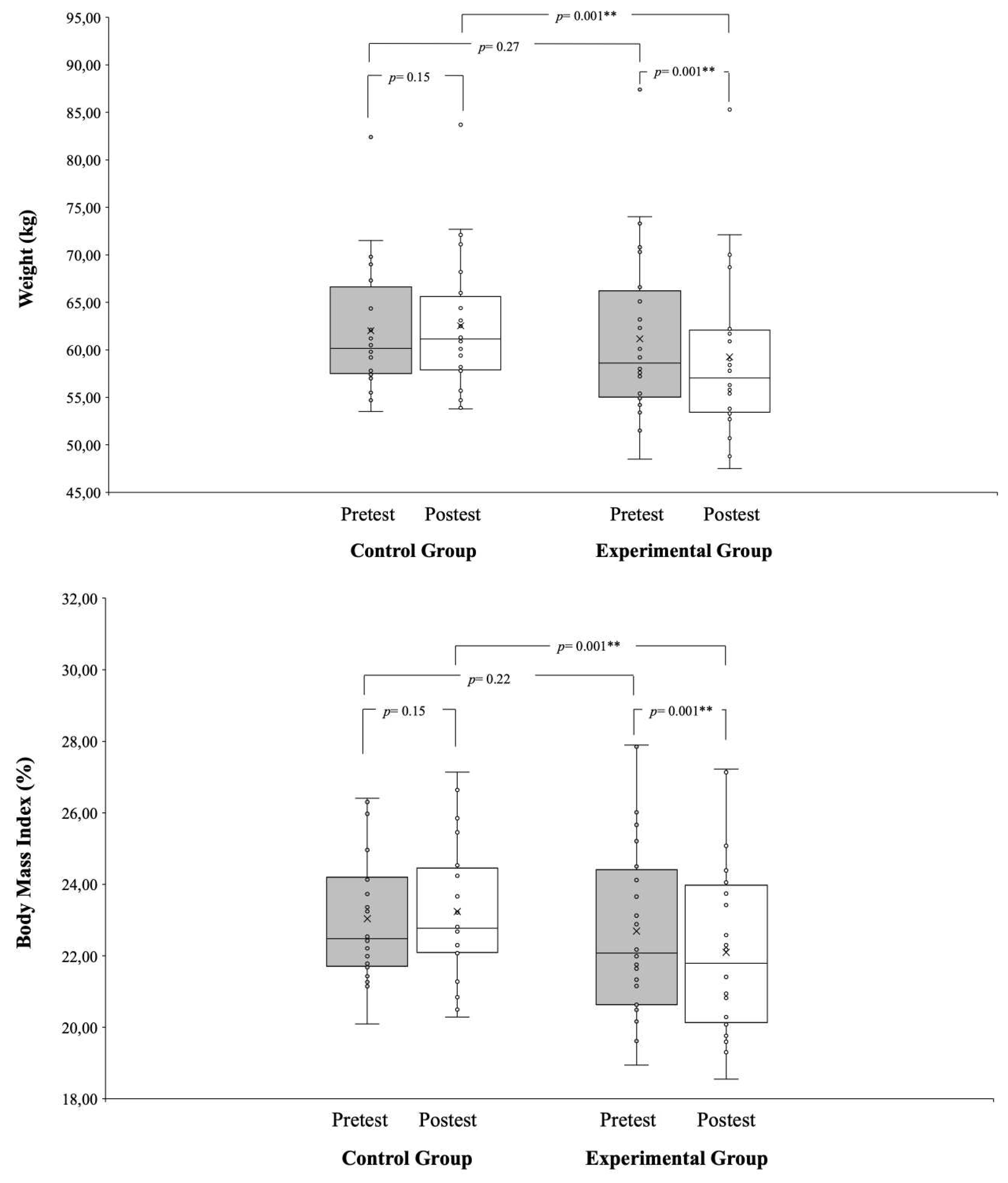
Figure 2.
Pre- and post-tests in CG and EG of performance variables (VO2 max, power output [W], and power output [W/kg]).
Figure 2.
Pre- and post-tests in CG and EG of performance variables (VO2 max, power output [W], and power output [W/kg]).
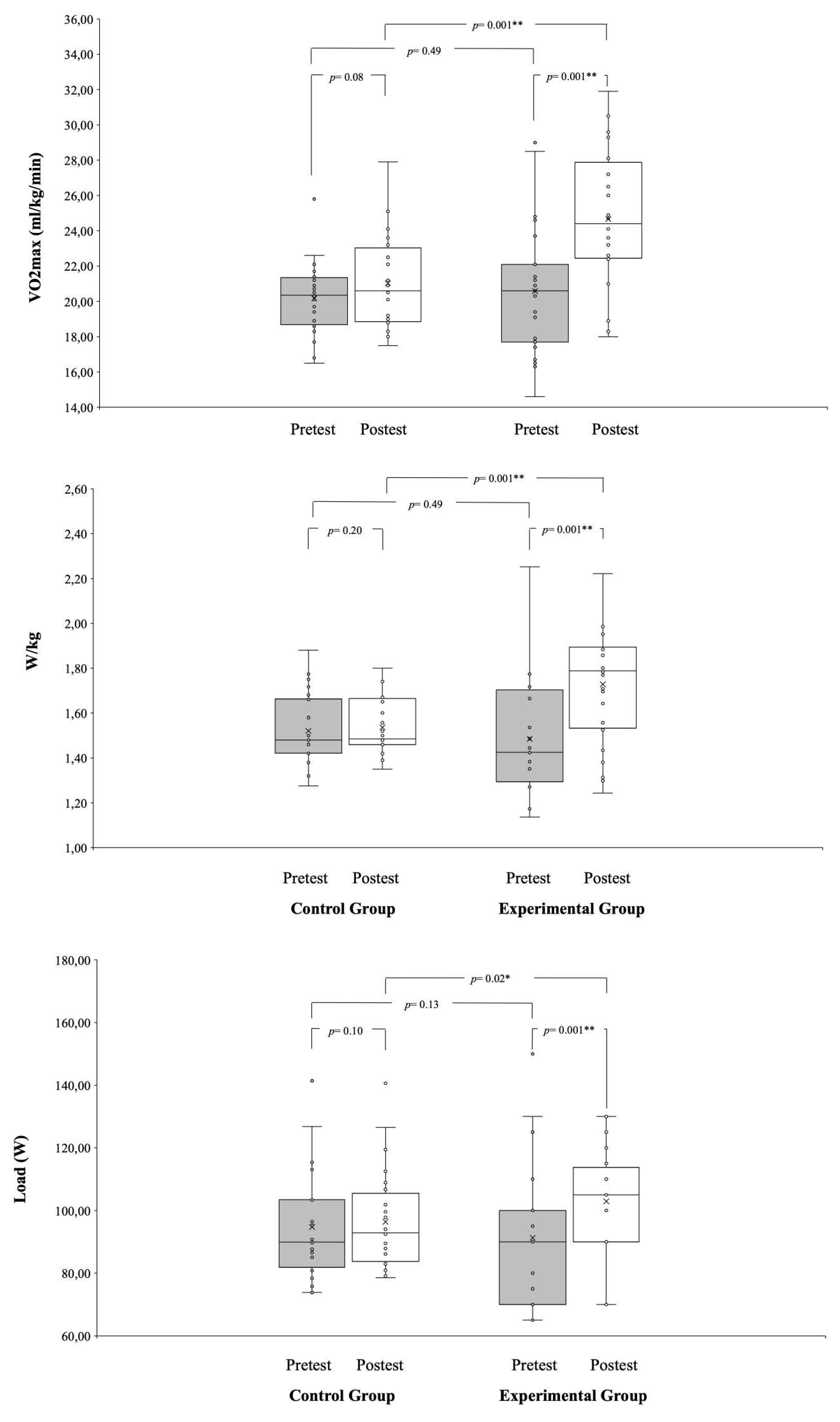
Table 1.
Timeline of this study.
| 2021 | ||||||||||||
| Months | January | February | March | |||||||||
| Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
| EG | Pre | High-intensity interval training | Post | |||||||||
| CG | Pre | Maintain routines | Post | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



