
Submitted:
29 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
Hepatic Encephalopaty (HE) is a common complications of advanced liver disease and acute liver failure. It is a condition that features both neurological and psychiatric symptoms, that affects mortality, morbidity and quality of patients and caregivers’ life. HE diagnosis is generally an exclusion diagnosis. Once the patient is admitted to hospital, clinical examination, blood tests and eventually neuroimaging should be performed in order to rule out other causes of acute brain dysfunction. Moreover, HE recognizes various precipitants that can potentially promote its onset, alone or in combination, that must be identified. Once the diagnostic process is complete, a correct treatment should be started. The anti-HE treatment is based on a combination of correction of precipitants and non-absorbable disaccharides and non-absorbable antibiotic, such as rifaximin. Once the patient is discharged from the hospital, specific anti-HE therapy should be maintained in order to prevent other HE episodes.
Keywords:
overt hepatic encephalopathy
; minimal hepatic encephalopathy
; portosystemic shunts
; ammonia
; liver cirrhosis
1. Introduction
Hepatic encephalopathy (HE) is one of the major complications of advanced liver disease and acute liver failure (1). HE is characterized by a spectrum of neuropsychiatric symptoms ranging from mild cognitive impairment to severe manifestations such as coma (2). The most common is type C HE, associated to the presence of a chronic liver disease with portal hypertension or systemic shunting (3). According to West-Heaven criteria, overt HE could be classified in four grades, according to the severity of symptoms (3,4):
- -
- GRADE I: shortened attention span, lack of awareness, mood changes
- -
- GRADE II: disoriented to space (oriented to time), flapping tremor, inappropriate behavior
- -
- GRADE III: disoriented to time and space, somnolence but responding to verbal stimuli, confusion (Glasgow Coma Scale GCS > 8)
- -
- GRADE IV: coma (GCS < 8)
Based on time course and frequency of relapse (2,5), overt HE can be divided in:
- -
- Episodic: generally precipitated by one or more factors that must be identified and treated
- -
- Recurrent: if two or more episodes occur within 6 months
- -
- Persistent: if patient does not return to his baseline mental performance between bouts of HE
The prevalence of overt HE at the time of the first diagnosis of cirrhosis ranges between 10% and 20% (3, 6). However, the reported prevalence can vary widely in different studies and populations. It's important to note that hepatic encephalopathy can occur at any stage of cirrhosis, and its prevalence tends to increase as the severity of liver disease progresses (7).The overall incidence of HE after Transjugular Intrahepatic Portosystemic Shunt (TIPS) ranges between 18% and 45% (3, 6-8), and refractory HE post-TIPS can occur in 3% -8% of patients (9).
Minimal hepatic encephalopathy (MHE) is a subtle and early form of hepatic encephalopathy. Unlike overt hepatic encephalopathy, where symptoms are more pronounced, individuals with MHE may not display obvious clinical signs of cognitive impairment or altered mental status, making it challenging to diagnose based on traditional clinical assessments alone (5). MHE is characterized by subtle neurocognitive deficits, such as mild impairment in attention, psychomotor speed, and executive functions. These cognitive changes can be identified through specialized neuropsychological testing, but they may not be apparent in routine clinical examinations. Despite the lack of overt symptoms, MHE can still impact a person's daily functioning and quality of life (10-11).
The exact mechanisms leading to hepatic encephalopathy are not fully understood, but it is believed to be related to the accumulation of toxic substances, particularly ammonia, in the bloodstream (12). The primary factor contributing to hepatic encephalopathy is the liver's inability to metabolize and detoxify substances normally, leading to their accumulation in the body, particularly the brain. In a healthy liver, in fact, ammonia is converted into urea and excreted from the body. However, in liver disease, this process is impaired, leading to elevated levels of ammonia that can affect the brain. Ammonia is primarily generated in the gut as an end-product protein digestion, amino acid deamidation and bacterial urease activity. In addition to that, in muscles, brain and kidneys, ammonia is produced and used in numerous biochemical reactions, as the amination of glutamate and the deamidation of glutamine via glutamine synthetase and glutaminase (1, 12). In patients with altered liver function due to acute or chronic disease, the main detoxification pathway of ammonia is compromised, leading to high concentrations of ammonia in the blood (13). Other than that, in patients with spontaneous portosystemic shunts or TIPS, blood from the gut skips the liver because of the blood flow diversion due to the shunts, transporting higher levels of ammonia into the systemic circulation. Ammonia exerts its deleterious effects on brain functions through multiple pathways including astrocyte swelling and dysfunction, oxidative stress, mitochondrial dysfunction, and alterations in membrane potential (1). These abnormalities cause neuronal dysfunction and brain oedema (14), the basis for the development of neurological symptoms. Even if it is known that ammonia is crucial in the development of HE, a direct correlation between levels of ammonia and the grade of HE has not been confirmed by lot of studies (15). Recent works have highlighted the role of other mechanisms involved in HE pathophysiology, such as systemic inflammation and intestinal microbiota dysbiosis. These alterations lead to production of high levels of pro-inflammatory cytokines, that work synergistically with hyperammonemia crossing the blood-brain barrier and causing cellular swelling (15-18).
2. Management of Overt He in Hospitalized Patients
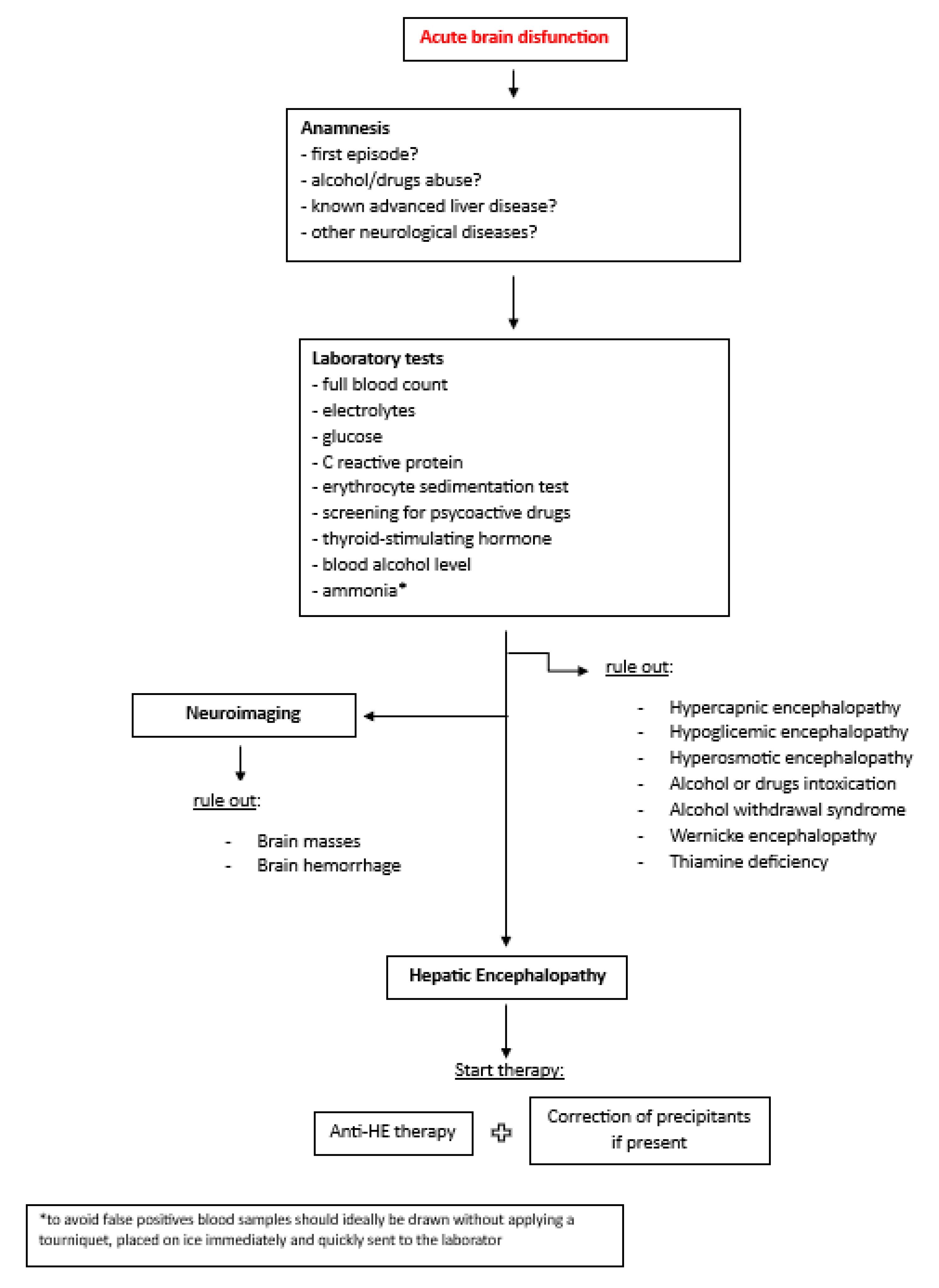
In a hospital setting, in front of a patient with advance liver disease or acute liver failure, it is important to promptly recognize HE, because it affects the prognosis, leading to a worsening of clinical outcomes and increasing mortality (19). The diagnosis of HE is not always immediate, because it can be overlapped with other medical, neurological, and psychiatric conditions that cause brain dysfunction (20). First, an accurate anamnesis should be done, also with the precious help of family members or caregivers, when possible, with the aim to identify previous episodes of HE or a known or possible liver disease. Clinical examination and features are crucial in HE diagnosis (flapping tremor, disorientation to time and space, changes of personality, somnolence, confusion, coma), as well as the exclusion of other neurological disorders that may simulate HE, such as electrolyte alterations, hypercapnia, dementia, meningoencephalitis, psychosis, drugs or alcohol intoxication, Wilson’s disease and brain masses (21). Akthar AJ et al demonstrated that 22% of patients with suspected HE and liver disease had other extrahepatic causes of acute brain dysfunction (22). So, in patients with suspected HE it is essential to identify alternative or additional causes of neurological impairment, to improve prognostic accuracy and the results of treatments (3). For this reason, patients with suspected HE should be undergone the same standardized diagnostic evaluation of all patients with altered consciousness (3). As shown in Figure 1, the diagnostic work-up might include the following tests: full blood count, electrolytes, glucose, inflammatory markers (for example C-reactive protein or erythrocyte sedimentation test), blood alcohol level and screening for psychoactive drugs and thyroid-stimulating hormone.
Since level of blood ammonia plays a key role in HE pathophysiology of HE, special reference needs to be made to the role of its blood determination. Measuring blood ammonia levels is a common diagnostic tool in the evaluation of patients with hepatic encephalopathy (HE). Elevated ammonia levels in the blood are associated with impaired liver function and are believed to contribute to the neurological symptoms of HE. However, it's important to note that blood ammonia levels alone do not provide a definitive diagnosis of hepatic encephalopathy, and clinical judgment, along with other diagnostic tests, is typically used to assess the severity and underlying cause of the condition. Moreover, it's important to consider that blood ammonia levels can fluctuate and may not always correlate directly with the severity of symptoms in hepatic encephalopathy. Other factors, such as dietary protein intake, medications, and the presence of gastrointestinal bleeding, can influence ammonia levels. Initially it has been thought that ammonia levels should be measured on arterial blood, but studies had demonstrated similar correlation between clinical severity of HE and arterial partial pressure of NH3 or ammoniemia and venous ammoniemia (23). The quality of ammoniemia measurements challenges the reliability of the results; in fact its measurement should be carefully performed in order to avoid a falsely elevated result (24). Blood samples should ideally be drawn without applying a tourniquet, placed on ice immediately and quickly sent to the laboratory, but a similar protocol is not as easy to apply in routine practice as it is in research protocols (23). Because of these difficulties, the utility of performing ammonia levels is debated and not systematically recommended (24). But, when properly performed, ammonia levels could help in differential diagnosis between HE and acute encephalopathy due to other causes, because a normal blood ammonia level has a negative predictive value in excluding HE (23-24). The prognostic role of ammonia remains unclear (15), but a recent multicenter study in acute-on-chronic liver failure suggested that plasma ammonia correlates not only with severity of HE but also with the failure of other organs and that the lack of amelioration in ammonia levels is associated with high risk of death (25).
There is no specific radiological sign of HE, but CT scan or MRI might be performed in case of diagnostic doubts and to exclude other causes of acute brain disfunctions.
The management of hepatic encephalopathy (HE) in a hospital setting involves addressing the underlying liver disease, managing precipitating factors, and providing supportive care to improve neurological symptoms. It is well known that HE is triggered by one or a combination of precipitating factors and then, once the diagnosis of HE is made, every effort should be made to identify single or multiple precipitants and implement appropriate corrective measures (21). Infections are one of the major causes of worsening of liver function in patients with acute or chronic liver disease. They increase mortality, morbidity, and rate of other complications (ascites, gastrointestinal variceal bleeding, kidney failure) (26). The prevalence of bacterial infections in patients hospitalized for decompensated cirrhosis is around 25–46% (21). A multicenter prospective study by Piano S. et al tried to better define infections epidemiology in cirrhotic patients. They found out that the prevalence of multidrug-resistant bacteria was 34%, and that it differed significantly among geographic areas, with the greatest prevalence in Asia (27). Another European prospective study by Fernandez et al. highlighted that infections caused by bacteria resistant to the main antibiotic families are prevalent in patients with cirrhosis, representing a growing and complex healthcare problem in patients with advanced liver disease (28). Higher Child-Pugh score or MELD score, ascites and gastrointestinal bleeding are directly related to susceptibility to develop infections (29) and for this reason, every patient with decompensated cirrhosis admitted to the hospital should be tested for potential infections (30). In the suspect of pneumonia, in addition to an accurate anamnesis of fever, dyspnea and other respiratory symptoms and classical blood test (leucocyte count and CPR), a chest X-ray or and high-definition CT scan must be performed to identify or exclude the presence of compatible parenchymal infiltrates. If a urinary tract infection is suspected, anamnesis for recent changes of urination and the execution of urine test and urinoculture is necessary. If patient has objective ascites, it is mandatory to perform a diagnostic paracentesis to exclude the presence of spontaneous bacterial peritonitis (SBP). If blood stream or systemic infection is suspected, blood cultures should be performed. To search for an acute infective gastroenteritis, an anamnesis of diarrhea with or without fever and presence of pathogen in stool should be performed. Gastrointestinal bleeding leads to an increase in blood ammonia, which is part of the reason that it is another major precipitant of HE (31). The incidence of HE after a GI bleeding is 10-39% in patient with Child-Pugh B or C cirrhosis (1). In a hospitalized patient with decompensated cirrhosis and HE, signs of recent GI bleeding (hematemesis, melena) should be investigated and an appropriate therapy must be promptly initiated. There are conflicting data on primary prophylaxis of HE in patients with acute gastrointestinal bleeding. Different RCTs showed that use of lactulose in cirrhotic patients admitted to hospital for acute gastrointestinal bleeding (variceal or non-variceal) is effective in preventing HE compared to placebo (32-33), while another recent RCT by Rattanasupar A. et al suggested the ineffectiveness of lactulose in preventing HE in these patients (34). These data suggest the need of more studies to assess the efficacy of a primary prophylaxis of HE in patient with decompensated cirrhosis and GI bleeding. Other precipitants that should be investigated and corrected if present are dehydration, constipation, electrolyte disorders, abuse of alcohol and use of benzodiazepines (BDZ) (21). Recent studies have highlighted the role of sarcopenia (loss of muscle mass) and myosteatosis (infiltration of muscle mass by intermuscular and intramuscular fat) in precipitate HE (35-37). It has been demonstrated that sarcopenia is a strong risk factor for the development of both MHE and overt HE (35-36). Because of this connection between HE and malnutrition, an early assessment of nutritional status should be performed in patients with advanced liver disease and a correct caloric intake should be given to patients (38-39). According to the latest EASL guidelines, in non-obese patients with advanced liver disease it is recommended a daily caloric intake of 30–40 kcal/Kg/day with a protein intake of 1–1.5 g/Kg/day and a diet that is rich in vegetable and dairy proteins (40). Lastly, also the presence of portosystemic shunts (spontaneous or TIPS) is strongly related to HE (41). Size, total cross-sectional area (TSA) and the morphology of spontaneous portosystemic shunts (SPSS) are associated with the development of HE, in fact, according to recent studies, it has been suggested that SPSS larger than 1 cm, TSA > 83 mm2 and splenorenal shunt are most associated than others with the development of recurrent or persistent HE (42-44). As far as TIPS, the incidence of new or worsening HE after TIPS placement is around 35–50% (45-46), depending on stent diameter used (47). A recent RCT by Wang Q. et al compared the incidence of post-TIPS overt HE in patients receiving 8 mm covered stent implantation vs patients receiving 10 mm covered stent implantation. They found out that TIPS with 8 mm covered stents showed similar shunt function to TIPS with 10 mm stents but halved the risk of spontaneous overt HE and reduced hepatic impairment (48). Also Schepis F. et al demonstrated that under dilation of stents during TIPS placement is associated with lower rates of HE (49).
According to latest EASL guidelines, patients with grade III or IV HE should be treated in Intensive Care Unit (ICU). These patients might have respiratory function altered and consequently they might be not able to protect their airways. For the high risk of aspiration, they need continuous monitoring in ICU. (3)
Hepatic encephalopathy poses a substantial economic burden to the healthcare system (50), which continued to increase during recent years (51). A large portion of the health care burden of HE is due to inpatient hospitalization. The burden on the healthcare system arises from several factors: hospitalization, diagnostic tests, treatment costs, follow-up care and impact on productivity; in fact patients with HE may experience a decline in cognitive function, which can impact their ability to work and perform daily activities. This can contribute to indirect costs related to lost productivity (52). Moreover, different studies that demonstrate that patients with cirrhosis and OHE have longer length of stay compared to patients with cirrhosis and without OHE (52-53). On the other hand, also hospital readmissions play a key role in increasing health care burden, in fact, HE is a primary risk factor for hospital readmissions among cirrhotic patients (54-55). The burden of hepatic encephalopathy extends beyond the direct economic aspect of health care use to include costs related to patients’ impaired health-related quality of life (51). In addition to that, HE has been associated with significant and psychological burdens to caregivers.
Figure 1.
Diagnostic-therapeutic algorithm of HE.
3. Therapeutical Management
3.1. Acute Episode of HE
Once OHE has been identified and diagnosed, a correct treatment should be started. Treatment of HE includes not only specific therapy aimed at reducing blood levels of ammonia, but also the correction of precipitating factors (21). In these settings, precipitants must be managed as follows:
- -
- Infections: empirical antibiotic therapy should be promptly started. The choose of the antibiotic is guided by local antibiotic resistances, type and severity of infection and local environment. Once the antibiogram is available, specific antibiotic should be used (56).
- -
- Variceal GI bleeding: according to latest Baveno VII guidelines, a combination of vasoactive drugs, antibiotic prophylaxis, and specific endoscopic treatment within 12 hours from the presentation of bleeding should be performed. In selected cases TIPS placement should be considered (57).
- -
- Non-variceal GI bleeding: high dosage of proton pump inhibitors should be started, and an upper endoscopy must be performed within 24 hours.
- -
- Electrolyte disorders: correction with infusion therapy.
- -
- Dehydration: use of fluid therapy and stop diuretics if used.
- -
- Constipation: use of oral laxatives or bowel enemas.
- -
- Malnutrition (muscle alterations): patients must follow dietary advice for a correct supply of nutrients (40).
- -
- SPSS: in case of recurrent or persistent HE, interventional radiology should be considered with the radiological retrograde shunt obliteration (balloon-occluded, plug-assisted or coil-assisted retrograde transvenous obliteration) (58-60).
- -
- TIPS: consider TIPS revision in case of persistent post-TIPS HE.
Correction of precipitants always precedes specific anti-HE treatment, and in most cases it can be expected the resolution of overt HE episode just with this primary intervention (3). After a first episode of HE secondary prophylaxis to prevent further HE episodes must be started, already when the patient is hospitalized.
3.2. Secondary Prophylaxis
To date, the best therapeutical strategy to prevent further episodes of HE is to maintain low the level of blood ammonia. This may involve interventions such as lactulose or lactitol, non-absorbable disaccharides that promote the excretion of ammonia in the feces, or rifaximin, an antibiotic that reduces the production of ammonia-producing bacteria in the gut (3). After first episode of HE, patient should start therapy with lactulose or lactitol. Lactulose is fermented and metabolized into lactic acid and acetic acid, increasing the acidity of the intestinal environment. In this environment ammonia (NH3) is converted to ammonium ions (NH4+) which cannot be absorbed through intestinal barrier. Lactulose is recommended as secondary prophylaxis following a first episode of overt HE, and should be titrated to obtain 2-3 bowel movements per day. If patients present with one or more new episodes of HE within six months from the first one, rifaximin should be added to lactulose therapy (3, 61-62). Rifaximin should be administered at a dosage of 550 mg twice daily (62). The action of rifaximin in hepatic encephalopathy is thought to be multifaceted: first it reduces the population of ammonia-producing bacteria in the gut, moreover rifaximin has anti-inflammatory properties mitigating the neuroinflammation observed in hepatic encephalopathy. A recent RCT by Vishal C. et al suggested that rifaximin exerts its action in leading to resolution and preventing new HE episodes by reducing the likelihood of infections and attenuating systemic inflammation. Rifaximin is minimally absorbed and is thought to act locally in the gut. According to their research, rifaximin plays a role on gut barrier repair, reducing the translocation of bacteria and endotoxins from the gut to the blood stream (63).
3.3. Primary Prophylaxis
To date, there is no recommendation for primary prophylaxis of HE in patients with advanced liver disease. Nevertheless, recent studies have suggested the importance of a primary prophylaxis for HE in selected cases:
Gastrointestinal bleeding: as already mentioned, GI bleedings are one of most common precipitants of HE and data of an effective primary prophylaxis on HE in these patients are conflicting. Sharma P. et al evaluated the role of lactulose for prophylaxis of HE after acute variceal bleeding (AVB). They compared two randomized groups of patients with AVB (lactulose vs placebo) and they found out that the majority of patients who developed HE was in the placebo group (64). Also Wen J. et al in another RCT suggested that lactulose is an effective prophylaxis agent of HE for cirrhotic patients who had developed GI bleeding (65). Another recent RCT demonstrated that lowering ammonia drugs (lactulose, rifaximin and L-ornithine L-aspartate) proved to be effective in preventing OHE in these patients (66). In opposite to that, Rattanasupar A. et al. conducted a randomized, double-blinded, placebo-controlled, multicenter study in which they compared lactulose group vs placebo group, showing no differences in HE incidence in the two groups, suggesting that unnecessary treatment with laxatives should be avoided in these patients (67). These conflicting data should stimulate new studies on the effectiveness of a pharmacological primary prophylaxis in patients with GI bleeding. To date, as the latest EASL guidelines suggest, the only effective prophylaxis is rapid removal of blood from the gastrointestinal tract with lactulose or mannitol by nasogastric tube or lactulose enemas (3).
TIPS: Post-TIPS HE is one of the major complication of TIPS (68). The first trial with the purpose of discover an effective pharmacological treatment to prevent HE after TIPS implantation was conducted by Riggio et al. in three different groups of patients submitted to TIPS (placebo vs lactitol vs rifaximin) and they found out that there was no difference in HE incidence in the first month after TIPS in the three groups (69). More recently, in a RCT by Bureau et al. it was demonstrated that rifaximin reduced the risk for OHE in patients with cirrhosis treated with TIPS (70). To date, based on the few available data, the most recent guidelines stated that rifaximin can be considered for prophylaxis of HE prior to non-urgent TIPS placement in patients with cirrhosis and previous episodes of OHE (3).
4. Domiciliary Care
Once the patient has been dismissed from the hospital after a new episode of HE, therapy with non-absorbable disaccharides with or without non absorbable antibiotic should be maintained. Discontinuation of therapy could be considered case-by-case only in selected patients, like those with an history of OHE and an amelioration of liver function and nutritional status and those in whom HE was triggered by a precipitating factor that is no more existing (for example patients with HE caused by acute variceal bleeding treated with endoscopic therapy and with no more evidence of esophageal or gastric varices) (3). More studies are needed to confirm this evidence.
In a domiciliary settings, a key role in the detection of first sign of HE in cirrhotic patients (especially in MHE, when the neuropsychological symptoms are shaded and subtle) is played by caregivers, people who may notice little changes in behavior, loss of attention, delayed time of reaction, sleep disorders, falls, reduced ability to work and driving skills and communicate these information to the physicians to actuate the best strategy in order to prevent a further episode of HE.
5. Minimal Hepatic Encephalopathy (Mhe)
MHE is associated with low quality of life (71-72), in addition to cirrhosis progression (73) and reduced survival rate (74). Its incidence in cirrhotic patients ranges from 20% to 80%, and it is associated to an increased risk to develop OHE (75). Because of these findings, in the latest EASL guidelines it is suggested to screen patients with cirrhosis and no history of HE for MHE in the ward and/or in clinic (3). MHE could be diagnosed with psychometric and/or electrophysiological tests. Electrophysiological tests are based on standard methodology, required sophisticated equipment and have lower sensitivity than psychometric tests (54). For this reason, in clinical practice psychometric tests are more performed. There is no gold standard for MHE diagnosis, which is often based on the execution of more test, chosen depending on available local norms or expertise (76). The Animal Naming Test (ANM) is the most used neuropsychological screening test; it consists in let the patient list the highest number of animals in 60 seconds (77). A result of < 15 animals is indicative of MHE. Psychometric Hepatic Encephalopathy Score (PHES) is another useful test; it includes a battery of “paper-pencil” tests for the assessment of psychomotor speed and skill, set shifting, attention, visuospatial orientation, concentration and memory. Others are Critical Flicker Frequency (CFR), Continuous Reaction Time Test (CRT), Inhibitory Control Test (ICT) (75), but they are not commonly practiced in clinical routine.
Therapy in MHE. Even if rifaximin improves cognition, quality of life, and driving capability (78), there are no RCTs to show that treatment of MHE prevents overt HE (79). The latest guidelines recommend to start therapy on a case-by-case basis (3, 80-81). Since MHE and OHE share the same pathophysiology, also the therapeutic strategies are supposed to be the same. In patients with MHE, treatment for HE could be considered also for the purposes of differential diagnosis (3).
6. Conclusion
HE is one on the main complication of advanced liver disease and it has to be promptly recognized because it affects prognosis and mortality. The diagnosis is based on the detection of symptoms and exclusion of other causes of acute brain dysfunction with the performance of an accurate anamnesis (even with the help of caregivers), blood tests and radiological imaging when indicated. The diagnostic algorithm also provides for the identification of precipitating factors. The treatment is based on correction of precipitant events and on the use of non-absorbable disaccharides and non-absorbable antibiotic. To date, there is no indication for primary prophylaxis of HE in patients with cirrhosis, except for selected cases where it could be suggested (post GI bleeding HE and post-TIPS HE).
References
- Rose, C.F.; Amodio, P.; Bajaj, J.S.; Dhiman, R.K.; Montagnese, S.; Taylor-Robinson, S.D.; Vilstrup, H.; Jalan, R. Hepatic encephalopathy: Novel insights into classification, pathophysiology and therapy. J Hepatol. 2020, 73, 1526–1547. [Google Scholar] [CrossRef] [PubMed]
- Häussinger, D.; Dhiman, R.K.; Felipo, V.; Görg, B.; Jalan, R.; Kircheis, G.; Merli, M.; Montagnese, S.; Romero-Gomez, M.; Schnitzler, A.; Taylor-Robinson, S.D.; Vilstrup, H. Hepatic encephalopathy. Nat Rev Dis Primers. 2022, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatic encephalopathy. J Hepatol. 2022, 77, 807–824. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; Russo, F.P.; Amodio, P.; Burra, P.; Gasbarrini, A.; Loguercio, C.; Marchesini, G.; Merli, M.; Ponziani, F.R.; Riggio, O.; Scarpignato, C. Hepatic encephalopathy 2018: A clinical practice guideline by the Italian Association for the Study of the Liver (AISF). Dig Liver Dis. 2019, 51, 190–205. [Google Scholar] [CrossRef]
- Ridola, L.; Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O. Hepatic Encephalopathy: Diagnosis and Management. J Transl Int Med. 2020, 8, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Elsaid, M.I.; Rustgi, V.K. Epidemiology of Hepatic Encephalopathy. Clin Liver Dis. 2020, 24, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Merli, M.; Pedretti, G.; Servi, R.; Meddi, P.; Lionetti, R.; Rossi, P.; Bezzi, M.; Salvatori, F.; Ugolotti, U.; Fiaccadori, F.; Capocaccia, L. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Incidence and risk factors. Dig Dis Sci. 1996, 41, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Rowley, M.W.; Choi, M.; Chen, S.; Hirsch, K.; Seetharam, A.B. Refractory Hepatic Encephalopathy After Elective Transjugular Intrahepatic Portosystemic Shunt: Risk Factors and Outcomes with Revision. Cardiovasc Intervent Radiol. 2018, 41, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Ridola, L.; Nardelli, S.; Gioia, S.; Riggio, O. Quality of life in patients with minimal hepatic encephalopathy. World J Gastroenterol. 2018, 24, 5446–5453. [Google Scholar] [CrossRef] [PubMed]
- Ridola, L.; Cardinale, V.; Riggio, O. The burden of minimal hepatic encephalopathy: from diagnosis to therapeutic strategies. Ann Gastroenterol. 2018, 31, 151–164. [Google Scholar] [CrossRef]
- Levitt, D.G.; Levitt, M.D. A model of blood-ammonia homeostasis based on a quantitative analysis of nitrogen metabolism in the multiple organs involved in the production, catabolism, and excretion of ammonia in humans. Clin Exp Gastroenterol. 2018, 11, 193–215. [Google Scholar] [CrossRef] [PubMed]
- Wright, G.; Noiret, L.; Olde Damink, S.W.; Jalan, R. Interorgan ammonia metabolism in liver failure: the basis of current and future therapies. Liver Int. 2011, 31, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Bosoi, C.R.; Rose, C.F. Identifying the direct effects of ammonia on the brain. Metab Brain Dis. 2009, 24, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Shawcross, D.L.; Sharifi, Y.; Canavan, J.B.; Yeoman, A.D.; Abeles, R.D.; Taylor, N.J.; Auzinger, G.; Bernal, W.; Wendon, J.A. Infection and systemic inflammation, not ammonia, are associated with Grade 3/4 hepatic encephalopathy, but not mortality in cirrhosis. J Hepatol. 2011, 54, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Shawcross, D.L.; Davies, N.A.; Williams, R.; Jalan, R. Systemic inflammatory response exacerbates the neuropsychological effects of induced hyperammonemia in cirrhosis. J Hepatol. 2004, 40, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K. Gut microbiota, inflammation and hepatic encephalopathy: a puzzle with a solution in sight. J Clin Exp Hepatol. 2012, 2, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Ridlon, J.M.; Hylemon, P.B.; Thacker, L.R.; Heuman, D.M.; Smith, S.; Sikaroodi, M.; Gillevet, P.M. Linkage of gut microbiome with cognition in hepatic encephalopathy. Am J Physiol Gastrointest Liver Physiol. 2012, 302, G168–G175. [Google Scholar] [CrossRef] [PubMed]
- Krishnarao, A.; Gordon, F.D. Prognosis of Hepatic Encephalopathy. Clin Liver Dis. 2020, 24, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Gioia, S.; Faccioli, J.; Riggio, O.; Ridola, L. Hepatic encephalopathy - recent advances in treatment and diagnosis. Expert Rev Gastroenterol Hepatol. 2023, 17, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Bellafante, D.; Gioia, S.; Faccioli, J.; Riggio, O.; Ridola, L.; Nardelli, S. Old and New Precipitants in Hepatic Encephalopathy: A New Look at a Field in Continuous Evolution. J Clin Med. 2023, 12, 1187. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, A.J.; Alamy, M.E.; Yoshikawa, T.T. Extrahepatic conditions and hepatic encephalopathy in elderly patients. Am J Med Sci. 2002, 324, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Nicolao, F.; Efrati, C.; Masini, A.; Merli, M.; Attili, A.F.; Riggio, O. Role of determination of partial pressure of ammonia in cirrhotic patients with and without hepatic encephalopathy. J Hepatol. 2003, 38, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Mallet, M.; Weiss, N.; Thabut, D.; Rudler, M. Why and when to measure ammonemia in cirrhosis? Clin Res Hepatol Gastroenterol. 2018, 42, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Shalimar Sheikh, M.F.; Mookerjee, R.P.; Agarwal, B.; Acharya, S.K.; Jalan, R. Prognostic Role of Ammonia in Patients With Cirrhosis. Hepatology. 2019, 70, 982–994. [Google Scholar] [CrossRef] [PubMed]
- Leber, B.; Spindelboeck, W.; Stadlbauer, V. Infectious complications of acute and chronic liver disease. Semin Respir Crit Care Med. 2012, 33, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Piano, S.; Singh, V.; Caraceni, P.; Maiwall, R.; Alessandria, C.; Fernandez, J.; Soares, E.C.; Kim, D.J.; Kim, S.E.; Marino, M.; Vorobioff, J.; Barea, R.C.R.; Merli, M.; Elkrief, L.; Vargas, V.; Krag, A.; Singh, S.P.; Lesmana, L.A.; Toledo, C.; Marciano, S.; Verhelst, X.; Wong, F.; Intagliata, N.; Rabinowich, L.; Colombato, L.; Kim, S.G.; Gerbes, A.; Durand, F.; Roblero, J.P.; Bhamidimarri, K.R.; Boyer, T.D.; Maevskaya, M.; Fassio, E.; Kim, H.S.; Hwang, J.S.; Gines, P.; Gadano, A.; Sarin, S.K.; Angeli, P.; International Club of Ascites Global Study Group. Epidemiology and Effects of Bacterial Infections in Patients With Cirrhosis Worldwide. Gastroenterology. 2019, 156, 1368–1380. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Prado, V.; Trebicka, J.; Amoros, A.; Gustot, T.; Wiest, R.; Deulofeu, C.; Garcia, E.; Acevedo, J.; Fuhrmann, V.; Durand, F.; Sánchez, C.; Papp, M.; Caraceni, P.; Vargas, V.; Bañares, R.; Piano, S.; Janicko, M.; Albillos, A.; Alessandria, C.; Soriano, G.; Welzel, T.M.; Laleman, W.; Gerbes, A.; De Gottardi, A.; Merli, M.; Coenraad, M.; Saliba, F.; Pavesi, M.; Jalan, R.; Ginès, P.; Angeli, P.; Arroyo, V.; European Foundation for the Study of Chronic Liver Failure (EF-Clif). Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe. J Hepatol. 2019, 70, 398–411. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; Fernandez, J.; Wiest, R.; Schnabl, B.; Moreau, R.; Angeli, P.; Stadlbauer, V.; Gustot, T.; Bernardi, M.; Canton, R.; Albillos, A.; Lammert, F.; Wilmer, A.; Mookerjee, R.; Vila, J.; Garcia-Martinez, R.; Wendon, J.; Such, J.; Cordoba, J.; Sanyal, A.; Garcia-Tsao, G.; Arroyo, V.; Burroughs, A.; Ginès, P. Bacterial infections in cirrhosis: a position statement based on the EASL Special Conference 2013. J Hepatol. 2014, 60, 1310–1324. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Nardelli, S.; Gioia, S.; Lucidi, C.; Merli, M. Management of hepatic encephalopathy as an inpatient. Clin Liver Dis (Hoboken). 2015, 5, 79–82. [Google Scholar] [CrossRef]
- Rattanasupar, A.; Tiawijit, N.; Rachatapantanakorn, B. Predictive factor for hepatic encephalopathy in cirrhotic patients who presented with acute variceal bleeding. J Med Assoc Thai. 2014, 97, 567–573. [Google Scholar] [PubMed]
- Higuera-de-la-Tijera, F.; Servín-Caamaño, A.I.; Salas-Gordillo, F.; Pérez-Hernández, J.L.; Abdo-Francis, J.M.; Camacho-Aguilera, J.; Alla, S.N.; Jiménez-Ponce, F. Primary Prophylaxis to Prevent the Development of Hepatic Encephalopathy in Cirrhotic Patients with Acute Variceal Bleeding. Can J Gastroenterol Hepatol. 2018, 2018, 3015891. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Liu, Q.; Song, J.; Tong, M.; Peng, L.; Liang, H. Lactulose is highly potential in prophylaxis of hepatic encephalopathy in patients with cirrhosis and upper gastrointestinal bleeding: results of a controlled randomized trial. Digestion. 2013, 87, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Rattanasupar, A.; Chang, A.; Akarapatima, K.; Chaojin, T.; Piratvisuth, T. Role of lactulose for prophylaxis against hepatic encephalopathy in cirrhotic patients with upper gastrointestinal bleeding: A randomized trial. Indian J Gastroenterol. 2021, 40, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Merli, M.; Farcomeni, A.; Gioia, S.; Ridola, L.; Riggio, O. Muscle Alterations Are Associated With Minimal and Overt Hepatic Encephalopathy in Patients With Liver Cirrhosis. Hepatology. 2019, 70, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Giusto, M.; Lucidi, C.; Giannelli, V.; Pentassuglio, I.; Di Gregorio, V.; Lattanzi, B.; Riggio, O. Muscle depletion increases the risk of overt and minimal hepatic encephalopathy: results of a prospective study. Metab Brain Dis. 2013, 28, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, B.; Nardelli, S.; Pigliacelli, A.; Di Cola, S.; Farcomeni, A.; D'Ambrosio, D.; Gioia, S.; Ginanni Corradini, S.; Lucidi, C.; Mennini, G.; Rossi, M.; Merli, M.; Riggio, O. The additive value of sarcopenia, myosteatosis and hepatic encephalopathy in the predictivity of model for end-stage liver disease. Dig Liver Dis. 2019, 51, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Romeiro, F.G.; Augusti, L. Nutritional assessment in cirrhotic patients with hepatic encephalopathy. World J Hepatol. 2015, 7, 2940–2954. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O.; Ridola, L. Nutrition Assessment and Management in Patients with Cirrhosis and Cognitive Impairment: A Comprehensive Review of Literature. J Clin Med. 2022, 11, 2842. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef]
- Simón-Talero, M.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Llop, E.; Praktiknjo, M.; Maurer, M.H.; Zipprich, A.; Triolo, M.; Vangrinsven, G.; Garcia-Martinez, R.; Dam, A.; Majumdar, A.; Picón, C.; Toth, D.; Darnell, A.; Abraldes, J.G.; Lopez, M.; Kukuk, G.; Krag, A.; Bañares, R.; Laleman, W.; La Mura, V.; Ripoll, C.; Berzigotti, A.; Trebicka, J.; Calleja, J.L.; Tandon, P.; Hernandez-Gea, V.; Reiberger, T.; Albillos, A.; Tsochatzis, E.A.; Augustin, S.; Genescà, J.; Baveno VI-SPSS group from the Baveno Cooperation. Association Between Portosystemic Shunts and Increased Complications and Mortality in Patients With Cirrhosis. Gastroenterology. 2018, 154, 1694–1705. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Riggio, O.; Gioia, S.; Puzzono, M.; Pelle, G.; Ridola, L. Spontaneous porto-systemic shunts in liver cirrhosis: Clinical and therapeutical aspects. World J Gastroenterol. 2020, 26, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Praktiknjo, M.; Simón-Talero, M.; Römer, J.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Llop, E.; Maurer, M.H.; Zipprich, A.; Triolo, M.; Maleux, G.; Fialla, A.D.; Dam, C.; Vidal-González, J.; Majumdar, A.; Picón, C.; Toth, D.; Darnell, A.; Abraldes, J.G.; López, M.; Jansen, C.; Chang, J.; Schierwagen, R.; Uschner, F.; Kukuk, G.; Meyer, C.; Thomas, D.; Wolter, K.; Strassburg, C.P.; Laleman, W.; La Mura, V.; Ripoll, C.; Berzigotti, A.; Calleja, J.L.; Tandon, P.; Hernandez-Gea, V.; Reiberger, T.; Albillos, A.; Tsochatzis, E.A.; Krag, A.; Genescà, J.; Trebicka, J.; Baveno VI-SPSS group of the Baveno Cooperation. Total area of spontaneous portosystemic shunts independently predicts hepatic encephalopathy and mortality in liver cirrhosis. J Hepatol. 2020, 72, 1140–1150. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Riggio, O.; Turco, L.; Gioia, S.; Puzzono, M.; Bianchini, M.; Ridola, L.; Aprile, F.; Gitto, S.; Pelle, G.; Di Martino, M.; Marzocchi, G.; Caporali, C.; Spagnoli, A.; Di Rocco, A.; Schepis, F. Relevance of Spontaneous Portosystemic Shunts Detected with CT in Patients with Cirrhosis. Radiology. 2021, 299, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Bellafante, D.; Ridola, L.; Faccioli, J.; Riggio, O.; Gioia, S. Prevention of post-tips hepatic encephalopathy: The search of the ideal candidate. Metab Brain Dis. 2023, 38, 1729–1736. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Qi, X.S.; Yang, Z.P.; Yang, M.; Fan, D.M.; Han, G.H. TIPS improves liver transplantation-free survival in cirrhotic patients with refractory ascites: an updated meta-analysis. World J Gastroenterol. 2014, 20, 2704–2714. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Angeloni, S.; Salvatori, F.M.; De Santis, A.; Cerini, F.; Farcomeni, A.; Attili, A.F.; Merli, M. Incidence, natural history, and risk factors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stent grafts. Am J Gastroenterol. 2008, 103, 2738–2746. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Lv, Y.; Bai, M.; Wang, Z.; Liu, H.; He, C.; Niu, J.; Guo, W.; Luo, B.; Yin, Z.; Bai, W.; Chen, H.; Wang, E.; Xia, D.; Li, X.; Yuan, J.; Han, N.; Cai, H.; Li, T.; Xie, H.; Xia, J.; Wang, J.; Zhang, H.; Wu, K.; Fan, D.; Han, G. Eight millimetre covered TIPS does not compromise shunt function but reduces hepatic encephalopathy in preventing variceal rebleeding. J Hepatol. 2017, 67, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Schepis, F.; Vizzutti, F.; Garcia-Tsao, G.; Marzocchi, G.; Rega, L.; De Maria, N.; Di Maira, T.; Gitto, S.; Caporali, C.; Colopi, S.; De Santis, M.; Arena, U.; Rampoldi, A.; Airoldi, A.; Cannavale, A.; Fanelli, F.; Mosconi, C.; Renzulli, M.; Agazzi, R.; Nani, R.; Quaretti, P.; Fiorina, I.; Moramarco, L.; Miraglia, R.; Luca, A.; Bruno, R.; Fagiuoli, S.; Golfieri, R.; Torricelli, P.; Di Benedetto, F.; Belli, L.S.; Banchelli, F.; Laffi, G.; Marra, F.; Villa, E. Under-dilated TIPS Associate With Efficacy and Reduced Encephalopathy in a Prospective, Non-randomized Study of Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2018, 16, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Elsaid, M.I.; John, T.; Li, Y.; Pentakota, S.R.; Rustgi, V.K. The Health Care Burden of Hepatic Encephalopathy. Clin Liver Dis. 2020, 24, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Neff, G.; Zachry, W., III. Systematic Review of the Economic Burden of Overt Hepatic Encephalopathy and Pharmacoeconomic Impact of Rifaximin. Pharmacoeconomics. 2018, 36, 809–822. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Riggio, O.; Allampati, S.; Prakash, R.; Gioia, S.; Onori, E.; Piazza, N.; Noble, N.A.; White, M.B.; Mullen, K.D. Cognitive dysfunction is associated with poor socioeconomic status in patients with cirrhosis: an international multicenter study. Clin Gastroenterol Hepatol. 2013, 11, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Hirode, G.; Vittinghoff, E.; Wong, R.J. Increasing Burden of Hepatic Encephalopathy Among Hospitalized Adults: An Analysis of the 2010-2014 National Inpatient Sample. Dig Dis Sci. 2019, 64, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, M.; Mishra, A.; Venkatesan, C.; Younossi, Z.M. In-hospital mortality and economic burden associated with hepatic encephalopathy in the United States from 2005 to 2009. Clin Gastroenterol Hepatol. 2012, 10, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Orman, E.S.; Ghabril, M.; Emmett, T.W.; Chalasani, N. Hospital Readmissions in Patients with Cirrhosis: A Systematic Review. J Hosp Med. 2018, 13, 490–495. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Baveno VII Faculty. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef]
- Laleman, W.; Simon-Talero, M.; Maleux, G.; Perez, M.; Ameloot, K.; Soriano, G.; Villalba, J.; Garcia-Pagan, J.C.; Barrufet, M.; Jalan, R.; Brookes, J.; Thalassinos, E.; Burroughs, A.K.; Cordoba, J.; Nevens, F.; EASL-CLIF-Consortium. Embolization of large spontaneous portosystemic shunts for refractory hepatic encephalopathy: a multicenter survey on safety and efficacy. Hepatology. 2013, 57, 2448–2457. [Google Scholar] [CrossRef] [PubMed]
- Gwon, D.I.; Kim, Y.H.; Ko, G.Y.; Kim, J.W.; Ko, H.K.; Kim, J.H.; Shin, J.H.; Yoon, H.K.; Sung, K.B. Vascular Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices and Hepatic Encephalopathy: A Prospective Multicenter Study. J Vasc Interv Radiol. 2015, 26, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Mukund, A.; Anandpara, K.M.; Ramalingam, R.; Choudhury, A.; Sarin, S.K. Plug-Assisted Retrograde Transvenous Obliteration (PARTO): Anatomical Factors Determining Procedure Outcome. Cardiovasc Intervent Radiol. 2020, 43, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K.; Thumburu, K.K.; Verma, N.; Chopra, M.; Rathi, S.; Dutta, U.; Singal, A.K.; Taneja, S.; Duseja, A.; Singh, M. Comparative Efficacy of Treatment Options for Minimal Hepatic Encephalopathy: A Systematic Review and Network Meta-Analysis. Clin Gastroenterol Hepatol. 2020, 18, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Bass, N.M.; Mullen, K.D.; Sanyal, A.; Poordad, F.; Neff, G.; Leevy, C.B.; Sigal, S.; Sheikh, M.Y.; Beavers, K.; Frederick, T.; Teperman, L.; Hillebrand, D.; Huang, S.; Merchant, K.; Shaw, A.; Bortey, E.; Forbes, W.P. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010, 362, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.C.; Lee, S.; McPhail, M.J.W.; Da Silva, K.; Guilly, S.; Zamalloa, A.; Witherden, E.; Støy, S.; Manakkat Vijay, G.K.; Pons, N.; Galleron, N.; Huang, X.; Gencer, S.; Coen, M.; Tranah, T.H.; Wendon, J.A.; Bruce, K.D.; Le Chatelier, E.; Ehrlich, S.D.; Edwards, L.A.; Shoaie, S.; Shawcross, D.L. Rifaximin-α reduces gut-derived inflammation and mucin degradation in cirrhosis and encephalopathy: RIFSYS randomised controlled trial. J Hepatol. 2022, 76, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Agrawal, A.; Sharma, B.C.; Sarin, S.K. Prophylaxis of hepatic encephalopathy in acute variceal bleed: a randomized controlled trial of lactulose versus no lactulose. J Gastroenterol Hepatol. 2011, 26, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Liu, Q.; Song, J.; Tong, M.; Peng, L.; Liang, H. Lactulose is highly potential in prophylaxis of hepatic encephalopathy in patients with cirrhosis and upper gastrointestinal bleeding: results of a controlled randomized trial. Digestion. 2013, 87, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Higuera-de-la-Tijera, F.; Servín-Caamaño, A.I.; Salas-Gordillo, F.; Pérez-Hernández, J.L.; Abdo-Francis, J.M.; Camacho-Aguilera, J.; Alla, S.N.; Jiménez-Ponce, F. Primary Prophylaxis to Prevent the Development of Hepatic Encephalopathy in Cirrhotic Patients with Acute Variceal Bleeding. Can J Gastroenterol Hepatol. 2018, 2018, 3015891. [Google Scholar] [CrossRef] [PubMed]
- Rattanasupar, A.; Chang, A.; Akarapatima, K.; Chaojin, T.; Piratvisuth, T. Role of lactulose for prophylaxis against hepatic encephalopathy in cirrhotic patients with upper gastrointestinal bleeding: A randomized trial. Indian J Gastroenterol. 2021, 40, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Nardelli, S.; Moscucci, F.; Pasquale, C.; Ridola, L.; Merli, M. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Clin Liver Dis. 2012, 16, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Masini, A.; Efrati, C.; Nicolao, F.; Angeloni, S.; Salvatori, F.M.; Bezzi, M.; Attili, A.F.; MerliM. Pharmacological prophylaxis of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt: a randomized controlled study. J Hepatol. 2005, 42, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Bureau, C.; Thabut, D.; Jezequel, C.; Archambeaud, I.; D'Alteroche, L.; Dharancy, S.; Borentain, P.; Oberti, F.; Plessier, A.; De Ledinghen, V.; Ganne-Carrié, N.; Carbonell, N.; Rousseau, V.; Sommet, A.; Péron, J.M.; Vinel, J.P. The Use of Rifaximin in the Prevention of Overt Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt: A Randomized Controlled Trial. Ann Intern Med. 2021, 174, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Schomerus, H.; Hamster, W. Quality of life in cirrhotics with minimal hepatic encephalopathy. Metab Brain Dis. 2001, 16, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Umapathy, S.; Dhiman, R.K. Minimal hepatic encephalopathy impairs quality of life. J Clin Exp Hepatol. 2015, 5 (Suppl. S1), S42–S48. [Google Scholar] [CrossRef]
- Ampuero, J.; Montoliú, C.; Simón-Talero, M.; Aguilera, V.; Millán, R.; Márquez, C.; Jover, R.; Rico, M.C.; Sendra, C.; Serra, M.Á.; Romero-Gómez, M. Minimal hepatic encephalopathy identifies patients at risk of faster cirrhosis progression. J Gastroenterol Hepatol. 2018, 33, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Ampuero, J.; Simón, M.; Montoliú, C.; Jover, R.; Serra, M.Á.; Córdoba, J.; Romero-Gómez, M. Minimal hepatic encephalopathy and critical flicker frequency are associated with survival of patients with cirrhosis. Gastroenterology. 2015, 149, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O.; Ridola, L. Minimal Hepatic Encephalopathy Affects Daily Life of Cirrhotic Patients: A Viewpoint on Clinical Consequences and Therapeutic Opportunities. J Clin Med. 2022, 11, 7246. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Riggio, O.; Allampati, S.; Prakash, R.; Gioia, S.; Onori, E.; Piazza, N.; Noble, N.A.; White, M.B.; Mullen, K.D. Cognitive dysfunction is associated with poor socioeconomic status in patients with cirrhosis: an international multicenter study. Clin Gastroenterol Hepatol. 2013, 11, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Campagna, F.; Montagnese, S.; Ridola, L.; Senzolo, M.; Schiff, S.; De Rui, M.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Merkel, C.; Angeli, P.; Riggio, O.; Amodio, P. The animal naming test: An easy tool for the assessment of hepatic encephalopathy. Hepatology. 2017, 66, 198–208. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Wade, J.B.; Gibson, D.P.; Saeian, K.; Wegelin, J.A.; Hafeezullah, M.; Bell, D.E.; Sterling, R.K.; Stravitz, R.T.; Fuchs, M.; Luketic, V.; Sanyal, A.J. Rifaximin improves driving simulator performance in a randomized trial of patients with minimal hepatic encephalopathy. Gastroenterology. 2011, 140, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.S.; Goyal, O.; Mishra, B.P.; Sood, A.; Chhina, R.S.; Soni, R.K. Rifaximin improves psychometric performance and health-related quality of life in patients with minimal hepatic encephalopathy (the RIME Trial). Am J Gastroenterol. 2011, 106, 307–316. [Google Scholar] [CrossRef]
- Caraceni, P.; Vargas, V.; Solà, E.; Alessandria, C.; de Wit, K.; Trebicka, J.; Angeli, P.; Mookerjee, R.P.; Durand, F.; Pose, E.; Krag, A.; Bajaj, J.S.; Beuers, U.; Ginès, P.; Liverhope Consortium. The Use of Rifaximin in Patients With Cirrhosis. Hepatology. 2021, 74, 1660–1673. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Suzuki, F.; Imamura, M.; Murashima, N.; Yanase, M.; Mine, T.; Fujisawa, M.; Sato, I.; Yoshiji, H.; Okita, K.; Suzuki, K. Rifaximin-altered gut microbiota components associated with liver/neuropsychological functions in patients with hepatic encephalopathy: An exploratory data analysis of phase II/III clinical trials. Hepatol Res. 2019, 49, 404–418. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



