
Submitted:
27 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
Infectious illnesses have always posed a threat to human health, with tuberculosis being a major concern. The use of various drugs in the fight against such TB has led to the emergence of drug-resistant tuberculosis, which has become increasingly difficult to manage. While there have been a few studies and proposed conceptual models on how to manage and prevent various drug-resistant TB mutations and lineages, a model aimed at limiting and controlling such mutations in rural areas burdened with tuberculosis is lacking. This study seeks to map a model that is to be used to bridge the gap by facilitating the exchange of knowledge among healthcare professionals in healthcare facilities, diagnostic laboratories, and research institutes, particularly for underprivileged communities in the Eastern Cape. The model information is based on three published manuscripts; therefore, this is a follow-up study. The model will also serve as a practical guide to monitor and evaluate epidemiological TB management plans.
Keywords:
model
; drug resistance tuberculosis
; collaboration
1. Introduction
Tuberculosis (TB) continues to be a significant public health concern worldwide, with drug-resistant tuberculosis (DR-TB) adding to the problem. The initial treatment for TB involves the use of two medications - Isoniazid (INH) and Rifampin (RIF) [1,2,3,4]. The most significant concern for TB control worldwide is now DR-TB, which is defined as TB that is resistant to the two most effective and commonly used first-line drugs, INH and RIF [5,6,7,8]. Resistance to first-line drugs for TB has been linked to various gene mutations, including rpoB, katG, and inhA [6]. Sharing knowledge between healthcare professionals (HCP) in healthcare facilities (HCF), diagnostic laboratories (DL), and research institutes (RI) might help to enhance a better understanding of the epidemiology of DR-TB and improve the approach on tackling this issue. As per various studies [9,10], healthcare organizations are increasingly recognizing the value of information sharing, with TB management being a critical area for knowledge transfer among health institutions. World Health Organization (WHO) and other sources define knowledge management as "a set of principles, tools, and practices that enable people to create, share, translate, and apply knowledge to create value and improve effectiveness [11,12].” Collaboration across a range of health stakeholders, including HCP, HCF, and DL, is characterized by knowledge exchange on improving management and the dissemination of up-to-date healthcare information to staff, patients, decision-makers, and other sectors. This approach has proven to be effective and efficient in TB management. It is crucial to provide health education and counseling to the communities. This will increase the awareness of healthcare providers who interact with patients, thereby improving the quality of medical treatment they provide [9,10]. Studies conducted in other countries have shown that a culture of information sharing is essential for the success of healthcare institutions, as it boosts intellectual capital, reduces costs, and enhances competitiveness [9,10,11,12]. To provide evidence-based healthcare and improve their expertise, health professionals need current health information from reliable sources. Unfortunately, medical personnel in resource-limited countries have a history of not sharing their experiences and information, leading to numerous medical errors. Therefore, it is essential to establish a model for these health stakeholders (HCF, HCP, and DL to share knowledge and collaborate, hence the formation of this model. According to the HCF, DL, and RI, it is a need to establish an information system to store data for building TB epidemiological information in rural areas of the Eastern Cape. Collaborative work by HCF, DL, and RI will ensure storage of information quality, which includes data completeness-a valuable aspect often overlooked. It is important to ensure complete data entry by all collaborating organizations in the information system. Otherwise, it becomes challenging to evaluate actions and develop disease control plans, ultimately affecting the epidemiological profile of affected areas. To gain a comprehensive understanding of TB transmission in rural parts of the Eastern Cape, a strategy that incorporates healthcare facilities, diagnostic services, and research services is required. Multi-sectoral cooperation between these parties will be economically advantageous in terms of resource allocation, staff motivation, and readily available information sources on interventions to enhance TB management in the research region. The study aims to map a model for collaboration of health care facilities, diagnostic laboratories, and research institutions in order to improve management of drug resistant tuberculosis in rural Eastern Cape.
2. Materials and Methods
Prototype information is based on three stages:
2.1. Stage 1
Our published study in the rural Eastern Cape Province identified gene mutations and DR-TB genotypes (mono DR-TB, MDR-TB, and XDR-TB) using different assays. We collected and analyzed 1157 sputum samples from patients suspected to have TB, and our study findings, presented in Table 1, Table 2, Figure 3, and Figure 4 [13], highlight the analytic methods used to identify regions of DR-TB mutations, heteroresistance, and genetic diversity, as presented in Table 3, Figure 5, and Figure 6 [13].
2.2. Stage 2
We conducted a study on the distribution of M. tuberculosis mutations and spoligotypes, which is presented in our published manuscript [14]. The aim of the study was to identify transmission hotspots of DR-TB and to analyze the Line Probe Assay (LPA) and spoligotype results of M. tuberculosis isolates using the QGIS 3.14 software. By doing so, we were able to identify geographical areas with a high incidence of the disease. To determine the type of DR-TB, gene mutations, and heteroresistance, we used the LPA score and banding patterns, which are further explained in Figure 7, Figure 8, and Figure 9 of our manuscript [14]. To conduct the analysis, we merged clinics within hospitals that had the same coordinates. This is shown in Table 1, Table 2, and Table 3, and Figure 2, Figure 3, Figure 4, Figure 5, and Figure 6 of our published manuscript [14]. Our investigation of the distribution of M. tuberculosis mutations and spoligotypes allowed us to identify transmission hotspots of DR-TB. This is shown in Table 1, Table 2, and Table 3, and Figure 2, Figure 3, Figure 4, Figure 5, and Figure 6 of our published manuscript [14]. All of this is further explained in our published manuscript [14], with detailed information provided in various tables and figures.
2.3. Stage 3
Our research on the treatment outcomes and related factors among tuberculosis patients involved examining the clinic records of 457 patients with DR-TB using the ambidirectional method. In addition, we followed up with 101 patients prospectively until the completion of their treatment, as detailed in our published manuscript [15]. The collected data included socio-demographics, clinical information, and treatment outcomes, which we analyzed using Stata version 17.0, as presented in Table 1, Table 2, Table 3, and Table 4, along with Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, and Figure 7 from our published manuscript [15]. We calculated the odds ratio and 95% confidence interval to assess the association between variables. A p-value of 0.05 or less was considered statistically significant [15].
3. HIV-TB Coinfection
The co-infection of TB and HIV is a major public health problem in many parts of the world, particularly in resource-limited countries like South Africa. According to Faye et al. [15], the rate of co-infection was high in rural areas of Eastern Cape, with men being mostly affected, leading to poor treatment outcomes. It has been established that the double burden of TB and HIV is a significant global health challenge [28,29,30]. TB is the leading immune-suppressing infection and the most common cause of death among HIV-infected patients [22,23,31]. The WHO estimates that patients living with HIV are 20 times more likely to acquire TB than those without HIV [1,2,3,30,31].
4. Treatment Outcomes
The success rate of TB treatment was lower than the WHO threshold standard at 65.8% due to a high number of patients being lost during follow-up. The co-infection of TB and HIV has resulted in poor treatment outcomes in rural areas of the Eastern Cape [15]. INH is one of the most efficient and targeted medications for treating the disease caused by M. tuberculosis. It is a key component of current short-course chemotherapy for TB and is commonly used to treat latent MTB infection (LTBI) to prevent the progression of the infection to active disease and the spread of TB. The development of INH resistance is a typical first stage in the transition to MDR [16]. Treatment success rate (TSR) is a critical factor in the global End TB strategy. South Africa has a national TSR of 76%, which still falls short of the standard set by the WHO, the global health body [30].
5. Validity and Reliability
Authenticity of an empirical measure refers to how accurately it reflects the intended concept. In order to establish the validity of this model, researchers tracked the intermediate results and compared them with observed outcomes. They validated the simulation model output by testing it with various input combinations. Additionally, the final simulation results were compared with analytic results. The research instruments were found to be substantially comparable and consistently produced the same or similar results when tested under the same conditions.
6. Definition of Operational Concepts
- Gene mutation is a change to a gene's DNA sequence to produce something different. It creates a permanent change to that gene's sequence. Genetic variations are important for humans to evolve, which is the process of change over generations [35]
- TB mutations are resistance originates in the course of treatment due to genomic mutations in M. tuberculosis. An increase in new cases of drug-resistant TB could be an indicator of high levels of circulating resistant strains [38]
- TB lineages are groups of related M. tuberculosis strains described variously as lineages, families, or clade [35]
- Model is an ideal guidance or imitation. The term "model" refers to something that is accepted or suggested as being admirable [40].
- Collaboration healthcare is defined as the sharing of responsibilities for problem-solving and making decisions to formulate and carry out plans for patient care [38].
- Health stakeholders are individuals or groups who have an interest in a sector, such as the health system. They can influence decisions, shape policy, and create an environment that best serves the needs of those involved in the sector [38].
- Spoligotype is a PCR-based method allowing analysis of strain-dependent polymorphisms observed in spacer sequences present within the direct repeat genomic region of M. tuberculosis complex strains [13].
3. Results
Here are some of the important discoveries from the initial investigations, which were conducted in three parts.
3.1. Gene mutation and Regions of Mutations.
The mutations associated with RIF resistance were analyzed, and it was found that the rpoB gene is the most common source of resistance in M. tuberculosis. The rpoB region S531L exhibited the highest prevalence of changes and is linked to major MDR-TB outbreaks in many parts of the world. Most of the samples studied had mutations in the rpoB codon 531, which is known to indicate RIF resistance [16]. Changes in codon 315 of the katG gene are primarily responsible for INH resistance. Numerous studies conducted worldwide have shown that the S315T mutation is closely related to high levels of INH resistance. The katG gene mutation is one of the main mechanisms of INH resistance in MTB [16].
3.2. Heteroresistance
It is a phenomenon that occurs when a patient is infected by both drug-resistant and susceptible strains of an infection simultaneously [17,18]. It is considered a precursor to full resistance or low levels of drug-resistant TB. According to studies conducted by Faye et al. [13], heteroresistance is increasing every year in rural areas of Eastern Cape. The results of treatment may be negatively affected by heteroresistance as it can develop when drug-resistant individuals spread susceptible and resistant M. tuberculosis strains to untreated cases or newly infected patients. It has been observed that MDR isolates are more likely to carry the katG S315T mutation than non-MDR strains [19,20]. It was discovered that the katG gene had more heteroresistant strains than rpoB and InhA genes, which can result from mixed infection or clonal heterogeneity. This is thought to be the first step toward total resistance, and it indicates that INH in this region is beginning to exhibit full resistance.
3.3. Type of Lineage
The Beijing family of tuberculosis is known to be associated with drug resistance in some parts of the world [27]. It is also recognized as being more transmissible than other families and is more prevalent in the Eastern and Western Cape regions [22,23]. Faye et al. have also confirmed this high prevalence in rural Eastern Cape [13,14]. Studies conducted in other provinces of South Africa such as Western Cape, Limpopo, and Mpumalanga have also reported a high prevalence of this family [35,36]. Several studies by Ameeruddin and Luke [34], Ano et al. [25], and Gagneux et al. [33] have reported that the katG-S315T mutation has a low-fitness cost, is spread to Beijing strains as well as other strains, and is more likely to be clustered. It has also been positively correlated with treatment failure [27].
3.4. Significance of the Model
Since 2020, there has been a slight increase in TB cases, which is believed to be due to the pandemic[38]. Unfortunately, this increase has set us back 12 years in our global progress towards tackling TB [38]. South Africa is currently one of the three countries in the world with the highest incidence of TB, drug-resistant TB, and HIV-associated TB. Shockingly, the WHO estimates that over 110,000 patients with TB died in South Africa between 2020 and 2021 [38]. However, South Africa is leading the way in TB research and development. The WHO's 2022 End TB strategy highlights the potential of multi-sectoral approaches to addressing TB determinants and achieving TB elimination [38]. This manuscript explores possible types of multi-sectoral collaboration and their potential in the context of innovative research, clinical management, and laboratory services. The goal of this manuscript is to be an enabler and policy advocate for the successful implementation and positive impact of the end TB policy in the Eastern Cape. Unfortunately, according to the studies by Pai and colleagues [39], the world is not on track to meet the End TB Strategy's goal of ending the global TB epidemic by 2030. Therefore, this manuscript emphasizes the importance of multi-sectoral collaboration and underlines the need for improved collaboration to confront drug-resistant MDR-TB and XDR-TB, which continue to pose a significant threat to the control of the disease on a global scale as a contribution to The end TB goals 2030 strategy. The WHO has indicated that communities and people affected by TB must be engaged, empowered, and supported. Additionally, it is acknowledged that multi-sectorial actions are necessary to address the social and economic determinants of the disease, including overall poverty reduction and achieving universal health coverage. The success of TB control depends largely on effective prevention strategies, early diagnosis, and adequate treatment, particularly for drug-resistant tuberculosis [38].
3.5. The Model's Aim to Enhance Capacity, Provide Improved Implementation Guidance, and Ensure Effective Monitoring and Evaluation.
A crucial part of the approach to managing TB is increasing the ability of healthcare providers, laboratory staff, and researchers to provide integrated services. Building capacity, providing guidance, monitoring, and evaluating the impact of the model will serve as the foundation for initiatives aimed at improving health systems and interventions intended to raise the quality of TB management and control services. Topics related to TB and its co-infection with HIV will be continuously discussed from the standpoint of collaboration among lab management, clinical management, and research methods. It is critical that training covers "systemic" topics including ways to improve referral systems and record keeping. Sessions will be held at the providers' sites to boost attendance, non-clinical personnel like clinic receptionists/clerks, data capturers, and even security guards who are interested but not mandatory will be included together with other community members. The capacity-building, implementation guide, including monitoring and evaluation, will be facilitated by the authors of this manuscript for the effective and efficient implementation of this model.
3.6. The Synthesised Model
The information from stage one, two, and three was used to manage TB. To manage TB, it is important to identify hotspots for gene mutations and lineages, especially those that contribute to DR-TB transmission and mixed infections in areas like rural Eastern Cape Province. Targeted interventions are required for rural populations as delivering DR-TB services in these regions is challenging due to obstacles such as co-infection with HIV and poverty. The Beijing family of M. tuberculosis and RIF resistance are both common in this region and are linked to the emergence of MDR. This study identified an increase in the rate of heteroresistance. Co-infection with HIV and inadequate treatment adherence are two variables that complicate the diagnosis and treatment of DR-TB, and thus, it is crucial that labs record them and treating clinicians are aware of the distribution of these spoligotypes of M. tuberculosis. There is a lack of information on the impact of antibiotic resistance on gene mutations, bacterial fitness, and other factors. Ongoing surveillance is recommended since genetic alterations are the main cause of the high frequency of treatment resistance seen in this TB study location. Early detection and management of drug-resistant tuberculosis is necessary to prevent its spread. Collaborating with health care facilities, diagnostic laboratories, and research institutions will improve and control tuberculosis, including HIV, especially in poor communities in the Eastern Cape Province Thus, the model's design is essential.
3.7. The Model's Origin
Faye et al.'s ecological research design stresses the importance of stopping the spread of DR-TB. Additionally, it draws attention to the gene mutations and lineages that are essential for the spread of DR-TB and mixed infections, especially in places with a high TB burden and little resources, like rural poverty areas. Since it is difficult to provide these services in these areas due to challenges in diagnosis and treatment, including co-infection with HIV and poverty, targeted interventions may be necessary for the rural population. As part of research, another study was conducted to assess the treatment outcomes of TB patients in the same rural of the eastern cape. The study involved reviewing medical records and following up with patients from the start of their TB treatment until the treatment outcome stage. Over a period of 36 months (January 2018 to December 2020), sputum samples were collected from 1,157 patients suspected of having TB from different healthcare facilities. The specimens were collected from patients who showed clinical signs of TB and were seeking medical assistance from 118 healthcare facilities located in five districts. The collection was performed by clinicians in various healthcare facilities as the last part of the study design for our last manuscript. The three manuscripts were then, the culmination of this model formulation.
3.8. Validation of the Model Value
In order to assess the effectiveness of this prototype, it was needed to be validated. This process helped to determine whether the model was suitable for achieving the study's objectives and provided a solution to the research question. In this investigation, it was verified to determine whether the study's aims were met. Researchers, laboratories, health professionals, and model development specialists at Walter Sisulu University received the questionnaires and structure to validate the prototype. The primary objective of the model during validation was to demonstrate that it could be used to manage drug-resistant TB in rural eastern cape communities. Through validation, the performance of the model, as well as its suitability for the study's objectives and research problem, were evaluated.
4. Discussion
The institutions presented in Figure 1 have been observed to have a weak connection, which negatively impacts the health programs aimed at strengthening TB control and reducing drug resistance. Effective sharing of TB information between DL, RI, and HCF through collaboration can enhance the information provided by HCPs to patients in a way that is easily understood. Similar studies have shown findings that are consistent with our study [39]. Many countries are currently facing high rates of TB and HIV co-infection, along with an increase in MDR and XDR infections. To combat this issue, the WHO has updated its policies with the aim of improving the diagnosis of this deadly disease in the countries that are most affected. The WHO's Strategic and Technical Advisory Group for TB has recommended that middle- and low-income countries use liquid culture and rapid species identification for culture and drug susceptibility testing (DST). The WHO has recognized that implementing these recommendations would require strengthening TB laboratory services, especially for clinicians, and improving research [41]. Another study conducted in Vietnam analyzed key stakeholders' model of collaboration in addressing barriers and facilitators when implementing active tuberculosis case-finding in six districts [42]. The increasing number of drug-resistant TB cases, heteroresistance, and treatment failures in the study area is a major concern. This is likely due to the lack of a collaborative approach to tackling TB among HCF, DL, and RI. Therefore, it is vital to establish cooperation between HCF, DL, and RI to address these issues as it requires multidisciplinary professionals to work together with the institutions depicted in Figure 1 to effectively analyze DR-TB mutations and strains for TB control. To achieve comprehensive TB control, all healthcare organizations (HCF, DL, and RI) must be included in the effort, as outlined by the WHO Global Report [30].
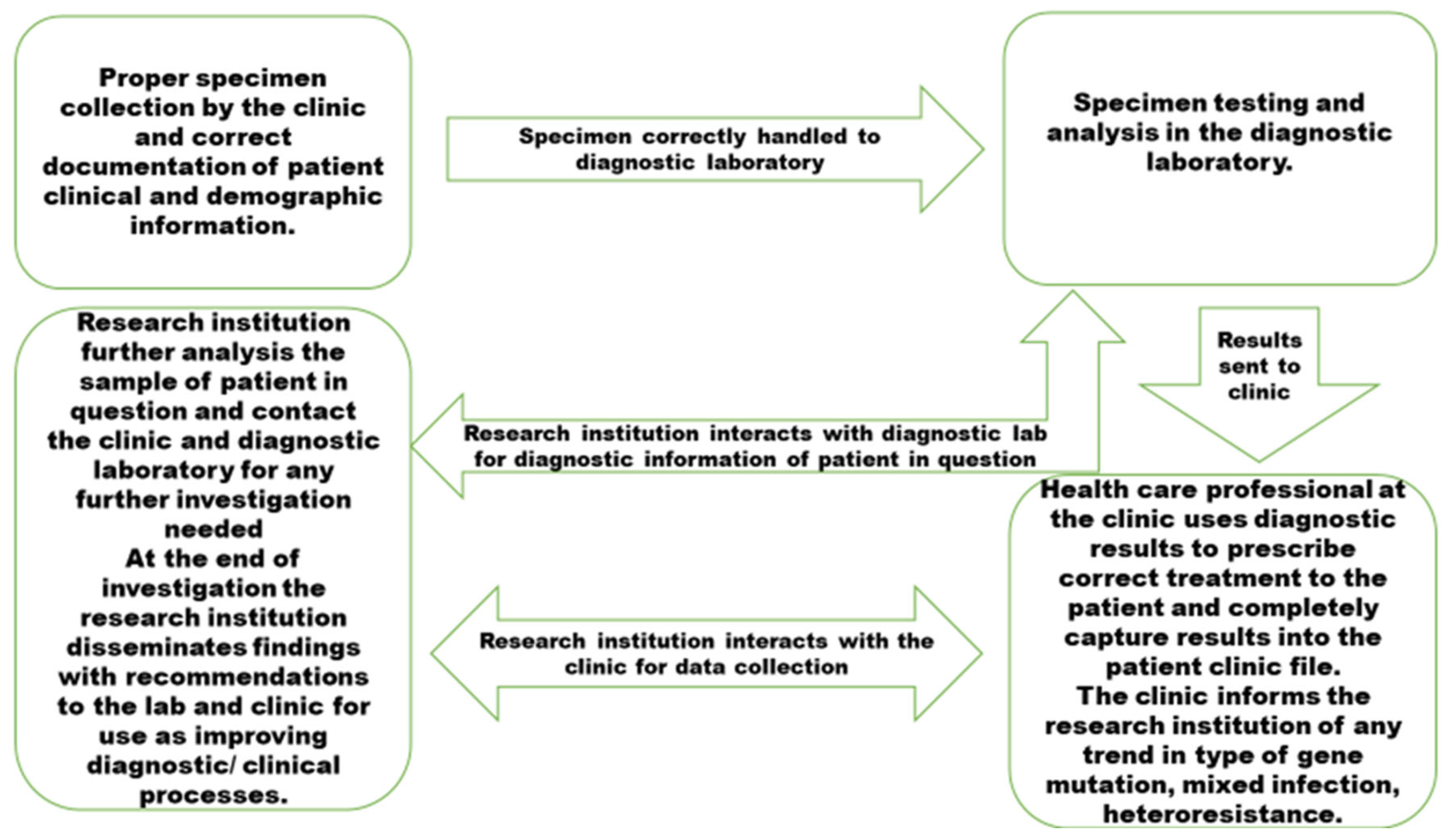
The accuracy of disease updates depends on the quality of data entered by the collaborators. It is vital to establish a strict system for entering complete and reliable data to accurately characterize the true epidemiological state of TB. Failure to provide quality data may lead to challenges in monitoring and managing the spread of DR-TB gene mutations and strains. It is recommended to perform spatial analysis at least every three months using data from the collaborators in the system to effectively monitor and manage the disease's spread. Incomplete disease notification instruments and follow-up procedures can lead to misinterpretation of the epidemiological situation and case follow-up. The COVID-19 pandemic has taught us the importance of collaborative TB management preparedness for any future pandemics. Before the emergence of SARS-CoV-2, TB was the biggest infectious killer of humans, causing an estimated 1.6 million deaths worldwide in 2021, with the majority of deaths occurring in low- and middle-income nations (LMICs). In 2019, an estimated 10 million people contracted TB, with only 7.1 million receiving diagnoses and notifications, leaving 2.9 million people undiagnosed. The pandemic has had a devastating effect on TB services, resulting in a diagnosis gap of 4.2 million cases. In 2021, only 6.4 million of the estimated 10.6 million TB cases were diagnosed and notified to national TB programs globally. Tackling the risks posed by DR-TB genetic mutations and strains in rural regions is the main focus. These areas have been identified as the primary sources of the TB epidemic in rural Eastern Cape [13,14,15]. To refine and adapt to the changing epidemiology of DR-TB and incorporate new advances in DR-TB control, it is essential to evaluate the existing systems regularly using key points, as shown in Figure 2. Though collaboration for enhancing DR-TB control is less emphasized in rural areas, this model illustrates how collaboration practices can influence the implementation of standardized TB control programs in different locations. Despite the availability of effective treatments since the 1980s, tuberculosis remains a significant global public health concern that requires proper management of information regarding DR-TB. Proper dissemination of information from laboratories and healthcare professionals will assist HCPs in gaining a better understanding of the disease's epidemiology through deep learning and data analysis, while patients will receive more comprehensive education. In Figure 3, there is a communication plan that emphasizes the importance of managing knowledge between three collaborators. Model mapping for the management and spread of DR-TB gene mutations and lineages in rural Eastern Cape needs quality pre-analytical and post-analytical processes that are well communicated among institutions responsible for TB management, as shown in Figure 4. Policymakers can use this model as a concept demonstrator to aid in making decisions based on analytical evidence when managing the spread of DR-TB, gene mutations, lineages, and treatment outcomes in rural areas of the province. It is important to create customized models to represent individual communities' unique factors that influence disease spread. This is especially crucial for the effective management of tuberculosis in rural areas of Eastern Cape. The HCF provides clinical care for a large number of tuberculosis patients, while research facilities continue to investigate the information on M. tuberculosis received from DL. Although all three collaborators will participate in the same intervention, their ability to exchange knowledge and implement improvements to integrate services will differ. Research conducted in various locations has shown that incorporating a collaborative knowledge translation framework, along with providing resources like facilitation and distributed leadership, within a transdisciplinary team consisting of research institutions, healthcare workers, and laboratories, can enhance collaboration and aid in achieving transdisciplinary research goals [35]. Tuberculosis is a significant disease that requires modeling to identify effective intervention strategies, especially in vulnerable communities such as rural areas of this province where the disease is prevalent [30]. It is crucial to note that TB transmission models are specific to certain geographic areas and should not be applied generally. Therefore, this model was developed specifically for this study setting, with the intention of allowing policymakers to determine which aspects to focus on to reduce the spread of TB in this area. Due to the unacceptable levels of M. tuberculosis spread in this study setting, it is essential to focus on reducing its spread. To provide healthcare services tailored to each community's needs, various service delivery models have been developed, including one that promotes ongoing collaboration among healthcare organizations to understand the epidemiology of TB in rural areas of the Eastern Cape. The objective of these efforts is to develop a robust model on drug-resistant TB.
5. Study Limitation
The outcomes of this study are dependent on the data published in manuscript parts one, two, and three, which limits its scope. Additionally, since the findings are based solely on data from rural areas of Eastern Cape research, their generalizability is limited. However, the study's ability to inform and improve intervention methods in the rural areas of the province and other similar contexts is a significant strength.
6. Conclusions
To improve patient management, there must be effective collaboration between clinicians, researchers, and laboratories. The model will strengthen health education programs that are custom-tailored to the unique needs of the community, taking into consideration the most recent updates on DR-TB gene mutations and strains, the partnership model will enhance health education initiatives that are specifically suited to the requirements of the community. Our primary goal is to diagnose and treat TB effectively, which necessitates early identification. The model for quality care in TB, including HIV management, will be implemented effectively and efficiently with continuous supervision, mentorship, and training. The designers of this model will lead the implementation process in collaboration with the programme managers of TB as well as the coordinators of the TB and HIV programs in the province. This approach will ensure that the model is strengthened and that quality care is provided to patients and the population of the Eastern Cape Province. If we cannot find TB, we cannot treat TB and if we cannot treat TB, we cannot end TB therefore that will hinder strategic vision of The End TB 2030.
Author Contributions
L.M.F.; Conceptualization, methodology, writing original draft; C.B., N.S., T.G; writing—review and editing, S.V. and T.A.; supervision, N.D.; writing—review, editing, methodology. All authors have read and agreed to the published version of the manuscript.
Funding
Financial support for this study was obtained from the South African Medical Research Council (SAMRC) Research development grant (Pilot grant).
Institutional Review Board Statement
This study was conducted by the Declaration of Helsinki. Approved granted Research Ethics and Biosafety Committee of the Faculty of Health Sciences of Walter Sisulu University (Ref. No. 026/2019) and Eastern Cape Department of Health (Reference Number EC_201904_011).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
The authors wish to sincerely acknowledge the clinicians and laboratory staff for support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Notoatmodjo, S. Promosi Kesehatan dan Ilmu Perilaku; Rineka Cipta: Jakarta, Indonesia, 2010. [Google Scholar]
- Bam, T.S.; Aditama, T.Y.; Chiang, C.Y.; Rubaeah, R.; Suhaemi, A. Smoking cessation and smoke-free environments for tuberculosis patients in Indonesia A cohort study. BMC Public Health 2015, 15, 604. [Google Scholar] [CrossRef] [PubMed]
- Vera Rahardjo, S.S.; Murti, B. Health Belief Model and Precede Proceed on the Risk Factors of Multidrug-Resistant Tuberculosis in Surakarta, Central Java. J. Epidemiol. Public Health 2017, 2, 241–254. [Google Scholar]
- Louwagie, G.M.; Ayo-Yusuf, O.A. Tobacco use patterns in tuberculosis patients with high rates of human immunodeficiency virus co-infection in South Africa. BMC Public Health 2013, 13, 1031. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.; Mahajan, S.; Lal, M.; Toor, A.K.; Deepti, S.S.; Chawla, N. Prevalence of tobacco consumption and smoking and its effect on outcome among microbiologically confirmed new pulmonary tuberculosis patients on daily regimen of DOTS in Amritsar city. J Family Med Prim Care 2022, 11, 2150–2154. [Google Scholar] [PubMed]
- Kant, S.; Maurya, A.K.; Kushwaha, R.A.S.; Nag, V.L. Multi Drug-resistant tuberculosis; an i6trogenic problem. Biosciences Trends 2010, 4, 48–53. [Google Scholar]
- Santha, T.; Garg, R.; Frieden, T.; Chandrasekaran, V.; Subramani, R.; Gopi, P.; Selvakumar, N.; Ganapathy, S.; Charles, N.; Rajamma, J. Risk Factors associated with default, failure, and death among tuberculosis patients treated in a DOTS program in Tiruvallur District, South India, 2000. Int J Tuberc Lung Dis. 2002, 6, 780–788. [Google Scholar] [PubMed]
- Lavigne, M.; Rocher, I.; Steensma, C.; Brassard, P. The impact of smoking on adherence to treatment for latent tuberculosis infection. BMC Public Health 2006, 6, 66. [Google Scholar] [CrossRef] [PubMed]
- WHO. Technical paper on regional strategy for knowledge management to support public health. WHO Regional Office Publisher, 2006; Available online: http://www.who.int/kms/about/en/.
- Veronique, L. Integrated knowledge translation for globally oriented public health practitioners and scientists: framing together sustainable transferontier knowledge translation vision. J Multidisciplinary Health care 2010, 3, 33–47. [Google Scholar]
- Ipe, M. Knowledge sharing in organizations: a conceptual framework. Human Resource Dev Rev 2003, 2, 337–359. [Google Scholar] [CrossRef]
- Pan, S.; Scarborough, H. A sociotechnical view of knowledge sharing at Buckman Laboratories’. J Knowl Manag 1998, 2, 55–66. [Google Scholar] [CrossRef]
- Faye, L.M.; Hosu, M.C.; Oostvogels, S.; Dippenaar, A.; Warren, R.M.; Sineke, N.; Vasaikar, S.; Apalata, T. The Detection of Mutations and Genotyping of Drug-Resistant Mycobacterium Tuberculosis Strains Isolated from Patients in the Rural Eastern Cape Province. Infect. Dis. Rep. 2023, 15, 403–416. [Google Scholar] [CrossRef]
- Faye, L.M.; Hosu, M.C.; Vasaikar, S.; Dippenaar, A.; Oostvogels, S.; Warren, R.M.; Apalata, T. Spatial Distribution of Drug-Resistant Mycobacterium tuberculosis Infections in Rural Eastern Cape Province of South Africa. Pathogens 2023, 12, 475. [Google Scholar] [CrossRef]
- Faye, L.M.; Hosu, M.C.; Iruedo, J.; Vasaikar, S.; Nokoyo, K.A.; Tsuro, U.; Apalata, T. Treatment Outcomes and Associated Factors among Tuberculosis Patients from Selected Rural Eastern Cape Hospitals: An Ambidirectional Study. Trop. Med. Infect. Dis. 2023, 8, 315. [Google Scholar] [CrossRef] [PubMed]
- Lipin, M.Y.; Stepanshina, V.N.; Shemyakin, I.G.; Shinnick, T.M. Association of specific mutations in katG, rpoB, rpsL, and rrs genes with spoligotypes of multidrug-resistant Mycobacterium tuberculosis isolates in Russia. Clin. Microbiol. Infect. 2007, 13, 620–626. [Google Scholar] [CrossRef]
- Andersson, D.I.; Nicoloff, H.; Hjort, K. Mechanisms and clinical relevance of bacterial heteroresistance. Nat Rev Microbiol. 2019, 17, 479–496. [Google Scholar] [CrossRef]
- Zheng, Y.; Xia, H.; Bao, X.; Zhao, B.; He, P.; Zhao, Y. Highly Sensitive Detection of Isoniazid Heteroresistance in Mycobacterium Tuberculosis by Droplet Digital PCR. Infection Drug Resistance. 2022, 6245. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; Sulaiman, S.A.S.; Hassali, M.A.; Khan, K.U.; Ming, L.C.; Mateen, O.; Ullah, M.O. Effect of smoking on treatment outcome among tuberculosis patients in Malaysia; a multicenter study. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hazbon, M.H. Population genetics study of isoniazid resistance mutations and evolution of multidrug-resistant Mycobacterium tuberculosis. Antimicrob. Agents Chemother 2006, 50, 2640–264. [Google Scholar] [CrossRef] [PubMed]
- van Doorn, H.R.; de Haas, P.E.W.; Kremer, K.; Vandenbroucke-Grauls, C.M.J.E.; Borgdorff, M.W.; van Soolingen, D. Public health impact of isoniazid-resistant Mycobacterium tuberculosis strains with a mutation at amino acid position 315 of katG: a decade of experience in The Netherlands. Clin Microbiol Infect 2006, 12, 769–775. [Google Scholar] [CrossRef]
- Karmakar, M.; Trauer, J.M.; Ascher, D.B.; Denholm, J.T. Hyper transmission of Beijing lineage Mycobacterium tuberculosis: Systematic review and meta-analysis. J. Infect. 2019, 79, 572–581. [Google Scholar] [CrossRef]
- Said, H.; Ratabane, J.; Erasmus, L.; Gardee, Y.; Omar, S.; Dreyer, A.; Ismail, F.; Bhyat, Z.; Lebaka, T.; van der Meulen, M.; et al. Distribution and Clonality of drug-resistant tuberculosis in South Africa. BMC Microbiol. 2021, 21, 157. [Google Scholar] [CrossRef] [PubMed]
- Shangase, Z.; Tsoka-Gwegweni, J.M.; Okem, A. Smoking prevalence among inpatients with drug-resistant tuberculosis in KwaZulu-Natal, South Africa. Tobacco-Induced Diseases. 2018, 16, 276. [Google Scholar] [CrossRef]
- Ano, H.; et al. Relationship between the isoniazid-resistant mutation katGS315T and the prevalence of MDR-/XDR-TB in Osaka, Japan. Int J Tuberc Lung Dis 2008, 12, 1300–1305.
- Swaminathan, S.; Narendran, G. HIV and tuberculosis in India. Journal of Biosciences. 2008, 33, 527. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Mathema, B.; Zhao, Q.; Zheng, X.; Li, D.; Jiang, W.; Wang, W.; Xu, B. Comparison of the sociodemographic and clinical features of pulmonary TB patients infected with sub-lineages within the W-Beijing and non-Beijing Mycobacterium tuberculosis. Tuberculosis 2016, 97, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kementerian Kesehatan, Republik Indonesia. Information Tuberculosis; Ministry of Health: Jakarta, Indonesia, 2018; Available online: https://pusdatin.kemkes.go.id/article/view/18101500001/infodatin-tuberkulosis-2018.html (accessed on 27 July 2023).
- Holmes, E.A.F.; Hughes, D.A.; Morrison, V.L. Predicting adherence to medications using health psychology theories: A systematic review of 20 years of empirical research. Value Health 2014, 17, 863–876. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global tuberculosis report. WHO/HTM/TB/2017.23, Geneva, 2017.
- van Doorn, H.R.; de Haas, P.E.W.; Kremer, K.; Vandenbroucke-Grauls, C.M.J.E.; Borgdorff, M.W.; van Soolingen, D. Public health impact of isoniazid-resistant Mycobacterium tuberculosis strains with a mutation at amino acid position 315 of katG: a decade of experience in The Netherlands. Clin Microbiol Infect 2006, 12, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Pillay, S.; Magula, N.P. Treatment outcomes of Gene Xpert positive tuberculosis patients in KwaMashu Community Health Centre, KwaZulu-Natal, South Africa: A retrospective review. S. Afr. J. Infect. Dis. 2019, 36, a217. [Google Scholar] [CrossRef] [PubMed]
- Gagneux, S. Impact of bacterial genetics on the transmission of isoniazid-resistant Mycobacterium tuberculosis. PLoSPathog 2006, 2, e61. [Google Scholar] [CrossRef]
- Ameeruddin, N.U.; Luke Elizabeth, H. Impact of isoniazid resistance on the virulence of global and south Indian clinical isolates of Mycobacterium tuberculosis. Tuberculosis (Edinb) 2014, 94, 557–563. [Google Scholar] [CrossRef]
- Ahmad, S.; Mokaddas, E.; Al-Mutairi, N.; Eldeen, H.S.; Mohammadi, S. Discordance across Phenotypic and Molecular Methods.
- for Drug Susceptibility Testing of Drug-Resistant Mycobacterium tuberculosis Isolates in a Low TB Incidence Country. PLoS ONE 2016, 11, e0153563. [CrossRef]
- Tolani, et al. BMC Infectious Diseases 2012, 12, 9. Available online: http://www.biomedcentral.com/1471-2334/12/9.
- Richardson, E.T.; Lin, S.Y.G.; Pinsky, B.A.; Desmond, E.; Banaei, N. The first documentation of isoniazid reversion in Mycobacterium tuberculosis. Int J Tuberc Lung Dis 2009, 13, 1347–1313. [Google Scholar] [PubMed]
- Global Tuberculosis Report 2022 (World Health Organization, 27 January 2023). Available online: https://go.nature.com/3FW2RVs.
- Pai, M.; Kasaeva, T.; Swaminathan, S.N. Eng. J. Med. 2022, 386, 1490–1493. [CrossRef] [PubMed]
- Dlatu, N.; Longo-Mbenza, B.; Oladimeji, K.E.; Apalata, T. Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa. Int J Environ Res Public Health. 2023, 20, 5977. [Google Scholar] [CrossRef]
- World Health Organization. The power of partnership. Geneva, WHO, 2000 (WHO/HTM/STB/2003.24).
- Biermann, O.; Tran, P.B.; Forse, R.J.; Vo, L.N.Q.; Codlin, A.J.; Viney, K.; Caws, M.; Lönnroth, K. Capitalizing on facilitators and addressing barriers when implementing active tuberculosis case-finding in six districts of Ho Chi Minh City, Vietnam: a qualitative study with key stakeholders. Implement Sci. 2021, 16, 54. [Google Scholar] [CrossRef]
Figure 1.
Collaboration and communication motivation model of patient care and disease monitoring institutions.
Figure 1.
Collaboration and communication motivation model of patient care and disease monitoring institutions.
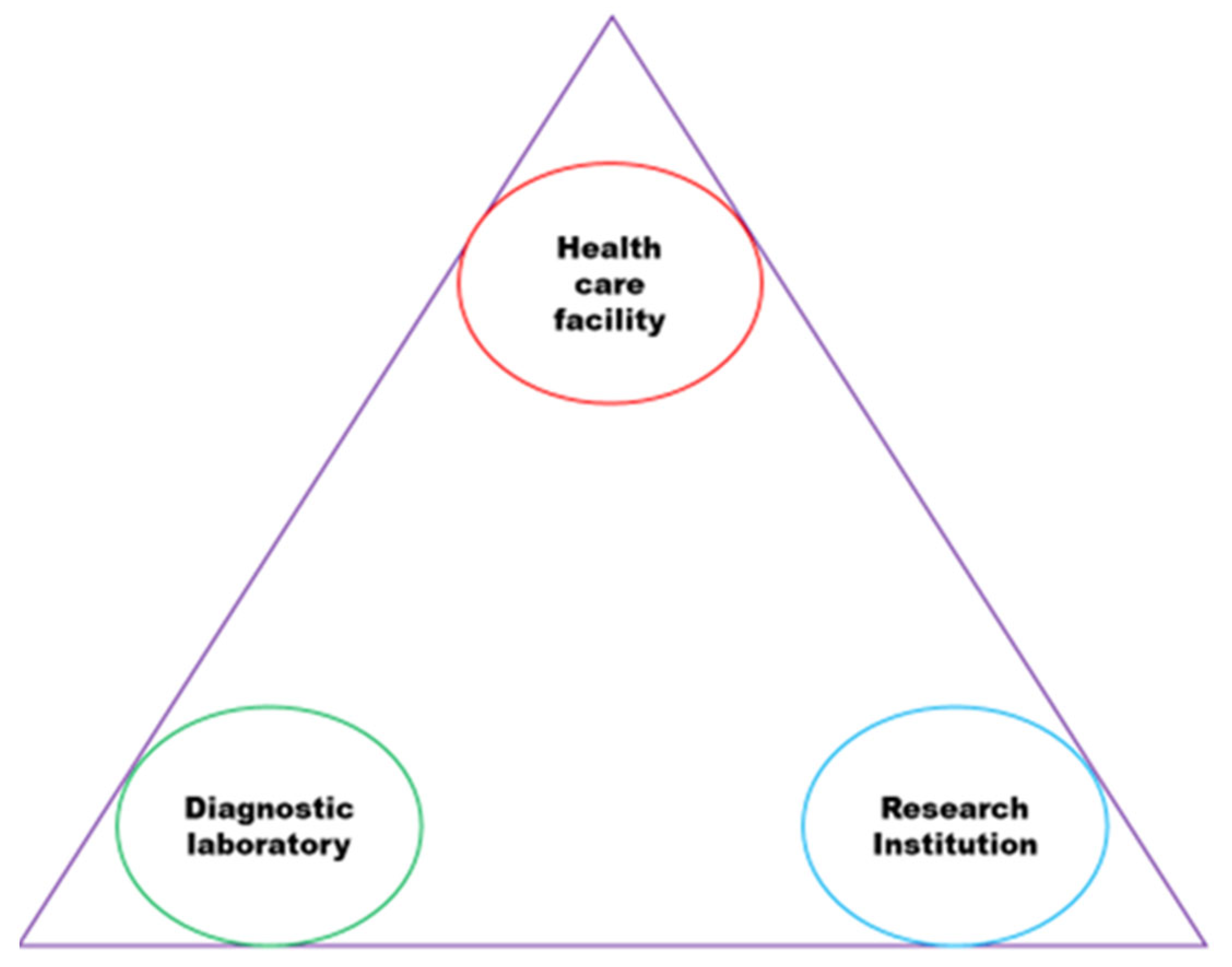
Figure 2.
Collaboration oversight.
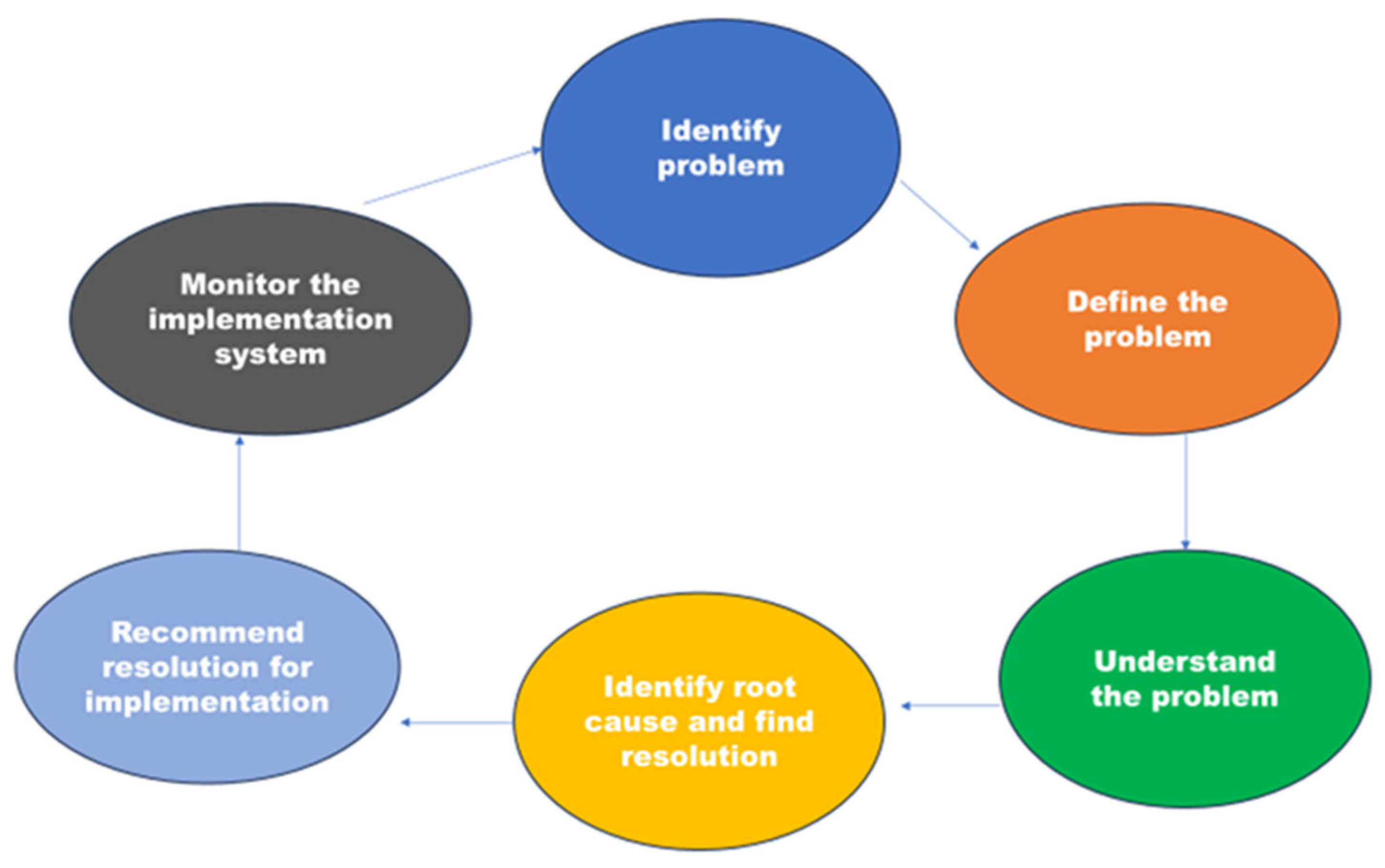
Figure 3.
Plan to manage information on DR-TB gene mutations and strains.
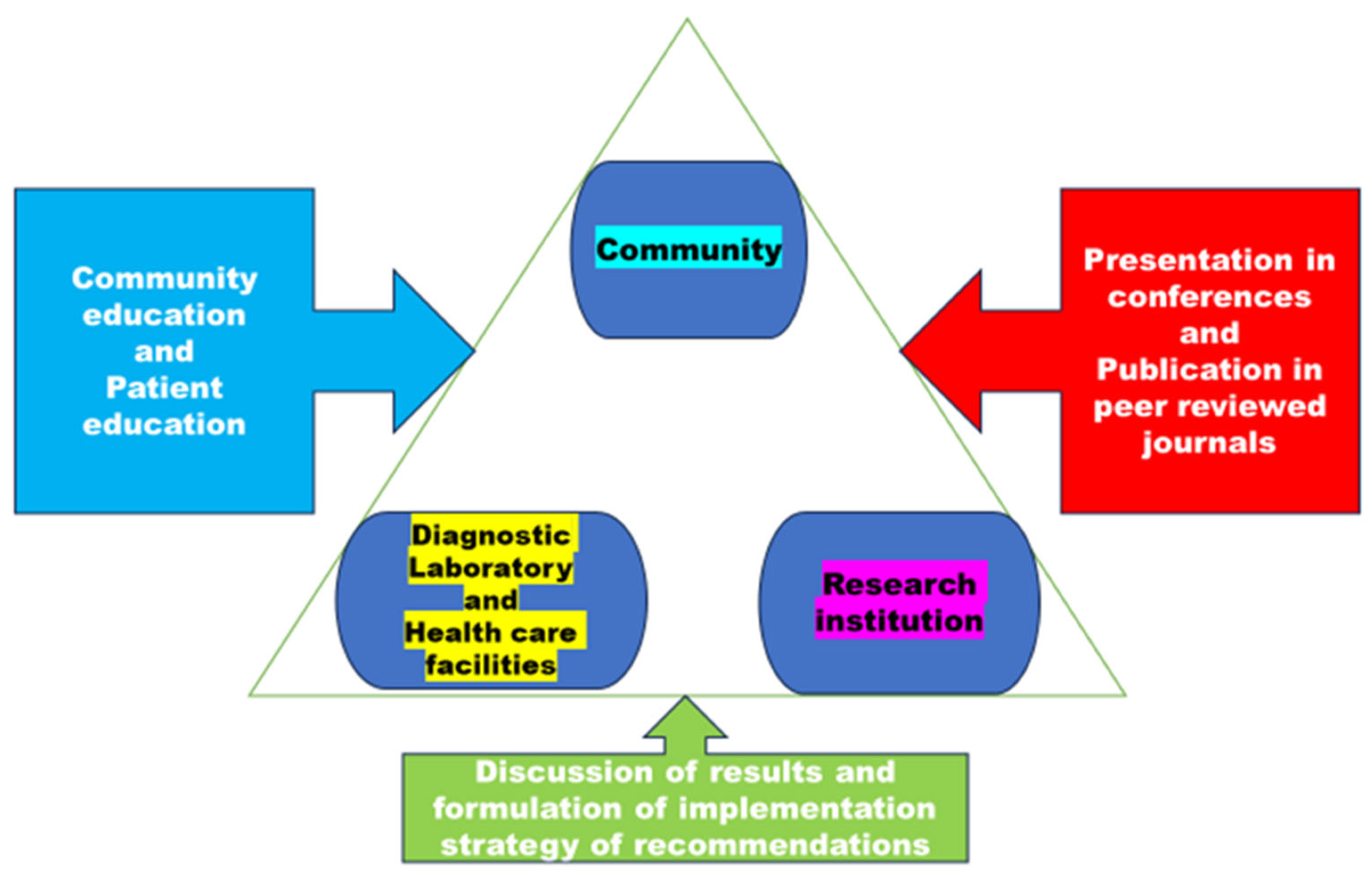
Figure 4.
Model mapping for management and spread of DR-TB gene mutations and lineages in rural Eastern Cape.
Figure 4.
Model mapping for management and spread of DR-TB gene mutations and lineages in rural Eastern Cape.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



