
Submitted:
01 December 2023
Posted:
04 December 2023
You are already at the latest version
Abstract
(1) Background: Neonatal early-onset sepsis (EOS) is associated with important mortality and morbidity. The aims of this study were to evaluate the association between serum biomarkers with early onset neonatal sepsis in a cohort of patients with prolonged rupture of membranes (PROM), and to calculate their diagnostic accuracy. (2) Methods: A retrospective cohort study was conducted on 1355 newborns with PROM admitted between January 2017 and March 2020, who were divided in two groups: group A, with PROM ≥ 18 hours and group B, with PROM < 18 hours. Both groups were further split into subgroups: proven sepsis, probable sepsis and no sepsis. Descriptive statistics, ANOVA analysis, and a Random Effects Generalized Least Squares (GLS) regression were used to evaluate the data. (3) Results: The statistically significant predictors of neonatal sepsis were the high white blood cells count from the first (p = 0.005) and third day (p = 0.028), and high CRP values from the first day (p = 0.004). Procalcitonin (area under the curve - AUC = 0.78) and CRP (AUC = 0.76) measured on the first day had the best predictive performance for early onset neonatal sepsis. (4) Conclusions: Further studies are needed to explore other bi-omarkers of sepsis in both pregnant women and newborns to better predict EOS.
Keywords:
Early-onset sepsis
; Biomarker
; C-reactive protein
; Procalcitonin
; White blood count
; Antibiotics
1. Introduction
Prolonged rupture of membranes (PROM) occurs in 8-10% of pregnancies [1,2] and may be complicated by microbial invasion of the amniotic cavity, inducing histological chorioamnionitis, intraamniotic inflammation, premature birth and neonatal infection [3]. Approximately one third of spontaneous preterm births are associated with premature prolonged rupture of membranes (PPROM) [4]. Other causes of preterm birth include multiple pregnancies, congenital abnormalities, chronic maternal conditions (diabetes, hypertension, autoimmune disorders, abdominal or uterine tumors, etc), in vitro fertilization (IVF), extremes of ages or weight, maternal use of illicit drugs or alcohol, psychiatric comorbidities or current pregnancy complications that require an iatrogenic preterm birth [5,6,7,8,9,10,11,12,13,14,15]. Previous studies have proven that the lower the gestational age (GA) at which the membranes rupture, the greater the probability of infection [16,17].
Obstetricians need to choose between conservative management, that could lead to chorioamnionitis and neonatal early-onset sepsis (EOS), and premature delivery, that is associated with prematurity complications. EOS was defined as an infection due to organisms acquired before and during delivery, occurring in the first 72 hours of life [18]. However, there are studies which extend the definition of EOS determined by group B Streptococcus (GBS) up to 7 days of life [19,20,21].
EOS is a challenge for neonatologists, being an invasive infection often suspected, but rarely diagnosed, with a proven diagnosis of 0.8 in 1000 births [22]. Due to significant mortality and severe complications associated with neonatal sepsis, early initiation of broad-spectrum antibiotics is the first step to decrease the morbidity and mortality [23,24]. Positive blood culture is the only certain diagnostic tool, but its results are confirmed within a 36-48 h time frame. Even in the presence of specific signs and symptoms, less than 1% of newborns with suspected sepsis have a positive blood culture [25].
In order to aid in the prompt detection and precise diagnosis of neonatal sepsis, more modern molecular approaches and nonculture-based techniques are required. Although the white blood cells (WBC), the immature/total neutrophils ratio (I/T), and the number of platelets (PLT) do not show high sensitivity and specificity to diagnose infections, these markers are the most used in neonatal units [26].
Leucopenia (WBC count 5000/mm3) has a high specificity (91%), but a low sensitivity (29%) for the diagnosis of newborn sepsis according to a literature review by Sharma et al [27]. I/T ratio may be the most accurate predictor of neonatal sepsis when compared to other hematological indicators, with a value greater than 0.27 in term newborns, and greater than 0.22 in preterm newborns being indicative of neonatal sepsis, but the serum level of this biomarker fluctuates with gestational age and postnatal age [28].
It has been shown that serial C-reactive protein (CRP) measurements increase its sensitivity and negative predictive value for neonatal sepsis, and may be beneficial for assessing the treatment response of affected neonates under antibiotic therapy [29]. Procalcitonin (PCT) could also be considered as a promising biomarker for neonatal sepsis due to high sensitivity (81%; 95% CI: 74–87%) and specificity (79%; 95% CI: 69–87%) values, as reported in a meta-analysis [30].
Other literature data indicated that currently determined markers in the newborns’ serum may be elevated due to other factors unrelated to infection, such as: hypertension or maternal fever, prolonged labor, perinatal asphyxia, meconium aspiration syndrome, respiratory distress syndrome, intracranial hemorrhage or pneumothorax [31,32].
The aims of this study were to evaluate the association between specific serum biomarkers with early onset neonatal sepsis in a cohort of patients with PROM, and to calculate their diagnostic accuracy.
2. Materials and Methods
2.1. Study design
An observational retrospective cohort study was conducted using the database of patients admitted to a level III neonatal center ” Cuza voda” Obstetrics- Gynecology Clinic Hospital between January 2017 and March 2020. The medical charts of the neonates were retrospectively reviewed. Information on the gestational age, weight, gender, mode of delivery, need for resuscitation, Apgar score, risk factors for infection and clinical signs of sepsis were extracted.
Access to patient’s medical records and the study protocol was approved by the Institutional Ethics Committee of the regional hospital (No 5332/21.05.2020). Newborns’ personal data were anonymized prior to analysis.
2.2. Definitions and study population
A total of 1355 medical records of neonates were analyzed. Newborns with PROM and postnatal age < 24 hours were included in the study. The gestational age (GA) ranged from 23 to 43 weeks. Exclusion criteria were: infants born at less than 23 weeks of gestation, infants with congenital anomalies, the absence/incomplete sepsis screening according to the unit protocol.
The population was divided in 2 groups. Group A (n=826 patients) included neonates with PROM longer than 18 hours before birth, while the infants with PROM less than 18 hours were assigned to group B (n=529 patients). The cut-off of 18 hours was chosen in accordance to our local protocols.
For the secondary analysis, we further stratified the neonates into 3 subgroups: proven EOS (subgroups A1 and B1), probable EOS (subgroups A2 and B2) and absence of EOS–control group (subgroups A3 and B3). Assignation of patients in one of the subgroups was performed according to the criteria proposed by the European Medicines Agency (EMA) [33].
The suspicion of infection was assessed on admission in all newborns with clinical signs suggesting infection: 1. respiratory signs: apnea, tachypnea, retractions, need for supplemental oxygen/respiratory support; 2. cardio-circulatory signs: tachycardia/bradycardia, hypotension, or impaired peripheral perfusion (mottled skin, cold extremities); 3. oliguria (urine output < 1 ml/kg/h); 4. temperature instability, hypothermia or hyperthermia; 5. gastrointestinal signs: vomiting, abdominal distension, bilious/bloody gastric aspirates; 6. skin and subcutaneous signs: petechial rash or scleroderma; 7. neurological signs: irritability, lethargy, hypotonia, weak sucking.
The sepsis panel included: complete blood count (CBC), C-reactive protein (CRP), procalcitonin (PCT), fibrinogen and blood culture, that was performed at admission, at 72 hours of life and on the 5th day of life, except for the blood culture and procalcitonin levels that were determined on a single occasion, at admission. Serum parameters were flagged as abnormal as follows: leukopenia (< 4 x109 cells/L) or leukocytosis (> 20 x 109 cells/L), immature to total neutrophils ratio (I/T) > 0.2, thrombocytopenia (< 100 x 109 cells/L) and inflammatory syndrome (CRP > 10 mg/L or PCT ≥ 10 ng/mL). According to the local protocol, antibiotic therapy was started in all neonates with clinical suspicion of infection and/or risk factors for sepsis (including rupture of membranes).
An amniotic fluid culture was performed for all pregnant patients with ruptured membranes before delivery. Clinical chorioamnionitis was diagnosed in the presence of maternal fever with two of the following: maternal tachycardia, fetal tachycardia, uterine tenderness, foul odor of amniotic fluid, or maternal leukocytosis [34]. Leukocytosis (> 10.000/mm3) and high CRP values (> 6 mg/dL) were considered as signs of maternal inflammatory syndrome according to the local laboratory thresholds. Maternal fever was considered when the core body temperature was higher than 38o Celsius.
2.3. Statistical analysis
The paired sample t-test and independent-sample t-test were used for continuous variables. Continuous variables were presented as the mean +/- standard deviation (SD). Categorical variables were presented as frequencies with corresponding percentages.
ANOVA analysis with the Bonferroni post-hoc test was used to determine whether or not there is a statistically significant difference between the means of serum biomarkers (WBC, CRP, and fibrinogen) between subgroups, and boxplots were used for graphical representations of these differences.
A Random Effects Generalized Least Squares (GLS) regression was used to measure the association between predictor variables, such as serum biomarkers levels (WBC, CRP, and fibrinogen) measured on three different occasions, and an outcome variable, proven neonatal sepsis. The performance of laboratory biomarkers in the diagnosis of EOS was calculated by using area under the curve-receiver operating curve (AUC–ROC). These analyses were performed using STATA SE (version 15, StataCorp LLC). A p-value of less than 0.05 was considered statistically significant.
3. Results
According to the criteria mentioned, 826 newborns were assigned to the group with PROM ≥ 18 hours, out of which 10 were included in the proven EOS group (0.7%), 414 neonates in the probable EOS category (30.6%), and 402 in the control group, without sepsis (29.7%). Another 549 neonates with PROM < 18 hours were segregated into proven EOS category (n= 11 patients, 0.8%), 266 in the probable EOS category (19.6%), and 252 in the control group, without sepsis (18.6%) (Figure 1).
A significant difference was found among the groups and each of the subgroups regarding the GA, birth weight (BW), as shown in Table 2 and Table 3.
Antibiotics were more frequently administered to neonates in the group with PROM ≥ 18 hours (p < 0.001). Duration of hospital stay was significantly longer for patients in group A compared to group B (15.37 ± 21.54 days vs. 7.67 ± 12.98 days, p < 0.001).

Table 1.
Clinical and demographic characteristics of the study group.
| PROM ≥18 hours (group A) N=826 |
PROM <18 HOURS (GROUP B) n=529 |
P value | |
|---|---|---|---|
| GA mean ± SD | 36.15 ± 3.9 | 37.83 ± 2.528 | <0.001 |
| Preterm* | 332 | 86 | <0.001 |
| BW mean ± SD | 2730.3 ± 857.7 | 3146.3 ± 636.2 | <0.001 |
| CS | 371 | 245 | 0.615 |
| VB | 455 | 284 | 0.614 |
| Male | 419 | 307 | 0.009 |
| Female | 407 | 222 | 0.009 |
| Apgar 1 min - median | 7 | 8 | <0.001 |
| Apgar 5 min - median | 8 | 9 | <0.001 |
| Apgar 10 min - median | 8 | 9 | <0.001 |
* Table 1 legend: GA: Gestational Age; BW: Birth Weight; CS: C-section; VB: vaginal birth; *GA < 37 weeks.
The Apgar scores were lower in neonates with proven sepsis (Subgroups A1 and B1) compared to those with probable sepsis or without sepsis, irrespective of duration of ruptured membranes (Table 2).
Moreover, a statistically significant difference was found when comparing the Apgar scores of group A with group B (p < 0.001). The proportion of preterm newborns was higher in the proven EOS group. Prolonged rupture of membranes ≥ 18 hours was associated with longer hospital stay in all subgroups (Table 2).
Table 2.
Clinical and demographic characteristics of the newborns in the subgroups.
| Proven EOS (A1) N=10 |
Proven EOS (B1) N=11 |
P value | Probable EOS (A2) N=414 |
Probable EOS (B2) N=266 |
P value | No sepsis (A3) N=402 |
No sepsis (B3) N=252 |
P value | |
|---|---|---|---|---|---|---|---|---|---|
| GA (mean ± SD) | 29.5 ± 4.3 | 35.3 ± 3.1 | 0.002 | 35.6 ± 4.3 | 37.6 ± 3.1 | <0.001 | 36.8 ± 3.1 | 38.1 ± 1.6 | <0.001 |
| Preterm* | 9 | 7 | 0.157 | 185 | 46 | <0.001 | 138 | 32 | <0.001 |
| BW (median) | 1484 | 2636 | 0.005 | 2605 | 3109 | <0.001 | 2889 | 3250 | <0.001 |
| CS | 4 | 8 | 0.130 | 188 | 123 | 0.519 | 179 | 114 | 0.969 |
| VB | 6 | 3 | 0.130 | 226 | 143 | 0.832 | 223 | 138 | 0.859 |
| Male | 6 | 8 | 0.014 | 204 | 152 | 0.045 | 213 | 147 | 0.181 |
| Female | 4 | 3 | 0.016 | 210 | 114 | 0.045 | 189 | 105 | 0.181 |
| Apgar 1 min (median) | 6 | 7 | 0.475 | 8 | 8 | <0.001 | 8 | 9 | <0.001 |
|
Apgar 5 min (median) |
7 | 8 | 0.453 | 8 | 9 | 0.004 | 9 | 9 |
<0.001 |
|
Apgar 10 min (median) |
7 | 8 | 0.413 | 8 | 9 | 0.006 | 9 | 9 | <0.001 |
| Duration of stay (mean ± SD) | 52.10 ± 40.5 | 22.73 ± 12.1 | <0.005 | 18.80 ± 24.6 | 9.75 ± 17.1 | <0.001 | 10.92 ± 15.1 | 4.81 ± 3.8 | <0.001 |
*Table 2 legend: GA: Gestational Age; BW: Birth Weight; CS: C-section; VB: vaginal birth; *GA < 37 weeks.
Analysis of perinatal risk factors for EOS revealed that the number of positive amniotic fluid cultures was significantly higher in group A (p = 0.001) compared to group B. Subgroup analysis revealed that positive amniotic fluid culture was associated only with probable EOS (p = 0.001), but no statistical significance was found between subgroups A1/B1 or A3/B3.
Furthermore, 12 of the mothers in subgroup A2 had chorioamnionitis, compared to none in B2 subgroup (p = 0.005). Also, there were no statistically significant differences concerning other analyzed risk factors such as foul-smelling amniotic fluid, maternal fever or maternal inflammatory syndrome between neonates in either subgroup (Table 3).
Table 3.
Perinatal risk factors for infection.
| Proven EOS (A1) N=10 |
Proven EOS (B1) N=11 |
P value | Probable EOS (A2) N=414 |
Probable EOS (B2) N=266 |
P value | No sepsis (A3) N=402 |
No sepsis (B3) N=252 |
P value | |
|---|---|---|---|---|---|---|---|---|---|
| Positive amniotic fluid culture | 5 | 0 | 0.007 | 58 | 15 | 0.001 | 19 | 8 | 0.83 |
| Foul smelling amniotic fluid | 2 | 3 | 0.28 | 41 | 27 | 0.41 | 16 | 16 | 0.739 |
| Maternal fever | 1 | 1 | 0.94 | 6 | 3 | 0.72 | 1 | 0 | 0.428 |
| Maternal inflammatory markers | 0 | 0 | - | 5 | 6 | 0.29 | 1 | 0 | 0.428 |
*Table 3 legend: EOS- early onset sepsis.
Regarding neonatal complications, respiratory distress syndrome (RDS) and retinopathy of prematurity (ROP) were significantly more frequent in group A than in group B (p < 0.001). Pneumothorax and pulmonary hemorrhage were statistically significant in subgroup A2 compared to group B2 (p = 0.002). Complications including mortality and patients included in the study are shown in Table 5. One neonate in subgroup A1 died due to EOS with Staphylococcus capitis (p = 0.28).
When comparing subgroup A1 with B1 more infants required mechanical ventilation (50% vs 27%; p = 0.806), for a longer period (13.8 vs 3.6 days; p = 0.322). However, no statistical significance was found. Inotropic support was necessary for 3 infants (30%) of subgroup A1, and 2 infants (18.2%) of subgroup B1 (p = 0.525).
Table 4.
Neonatal mortality and complications in the studied subgroups.
| Proven EOS (A1) N=10 |
Proven EOS (B1) N=11 |
P value | Probable EOS (A2) N=414 |
Probable EOS (B2) N=266 |
P value | No sepsis (A3) N=402 |
No sepsis (B3) N=252 |
P value | |
|---|---|---|---|---|---|---|---|---|---|
| Short term complications | |||||||||
| RDS | 9 | 7 | 0.157 | 134 | 57 | 0.002 | 68 | 5 | <0.001 |
| PPHN | 1 | 0 | 0.28 | 7 | 7 | 0.399 | 2 | 0 | 0.262 |
| Pulmonary hemorrhage | 0 | 1 | 0.329 | 1 | 1 | 0.002 | 1 | 0 | 0.428 |
| Pneumothorax | 1 | 0 | 0.366 | 8 | 4 | 0.002 | 2 | 2 | 0.636 |
| Severe ivH* | 0 | 1 | 0.32 | 8 | 6 | 0.772 | 0 | 0 | - |
| Long term complications | |||||||||
| nec | 1 | 0 | 0.28 | 4 | 0 | 0.049 | 0 | 0 | 0.428 |
| rop | 2 | 0 | <0.001 | 24 | 4 | 0.006 | 4 | 0 | 0.112 |
| BPD | 0 | 1 | 0.329 | 6 | 4 | 0.954 | 4 | 0 | 0.428 |
| Antibiotherapy | 9.2 | 10.7 | 0.801 | 4.6 | 8 | 0.501 | 8 | 5.8 | 0.562 |
| Duration of stay mean ± SD | 52.10 ± 40.5 | 22.73 ± 12.1 | <0.005 | 18.80 ± 24.6 | 9.75 ± 17.1 | <0.001 | 10.92 ± 15.1 | 4.81 ± 3.8 | <0.001 |
| Mortality | 1 | 0 | 0.28 | 8 | 7 | 0.54 | 7 | 0 | 0.428 |
* Table 4 legend: RDS: Respiratory distress syndrome; PPHN: persistent pulmonary hypertension of the newborn; IVH: intraventricular hemorrhage; NEC: necrotizing enterocolitis; ROP: retinopathy of prematurity; BPD: bronchopulmonary dysplasia; severe IVH* > grade III; EOS- early onset sepsis; SD- standard deviation.
Of the total 1355 patients, microorganisms were identified in the blood samples of 21 neonates (subgroup A1: 10 infants, and subgroup B1: 11 infants). The most common pathogen responsible for EOS was Staphylococcus spp. (n= 6; 28%; p = 0.89). Among neonates with EOS and PROM ≥18 hours, Escherichia coli was the most frequently detected pathogen (n=5; 50%), whereas in group B, the most prevalent pathogen was Klebsiella pneumoniae (n=4; 36.3%) (Table 5).
Table 5.
Comparison of blood culture results from the neonates with PPROM.
| Microorganism | PROM ≥18 hours % | PROM <18 HOURS % | Total (%) |
|---|---|---|---|
| Staphylococcus spp. | 3 (30) | 3 (27.3) | 6 (28.5) |
| Klebsiella pneumoniae | 1 (10) | 4 (36.4) | 5 (23.8) |
| Escherichia coli | 5 (50) | 0 | 5 (23.8) |
| Streptococcus spp. | 1 (10) | 3 (27.3) | 4 (19.2) |
| Listeria monocytogenes | 0 | 1 (9) | 1 (4.7) |
* Table 5 legend: PROM- prolonged rupture of membranes.
A comparison of hematological parameters between groups is summarized in Table 6. Significant leukocytosis and high CRP values measured in day 1 were encountered in group B, with PROM <18 hours (p < 0.001).
Table 7 summarizes the descriptive statistics and t-tests for the main serum biomarkers with repeated measurements among subgroups with proven EOS. However, none of the evaluated parameters were significantly different between A1 and B1 subgroups.
Table 8 summarizes the descriptive statistics and t-tests for the main serum biomarkers with repeated measurements among subgroups with suspected EOS, and without neonatal sepsis. Leukocytosis and CRP serum values recorded in the first day were significantly higher in the B2 subgroup compared to A2 subgroup (p < 0.05). Also, when taking into consideration the subgroups without neonatal sepsis, our results showed that leukocytosis on day 1, CRP on day 3, and fibrinogen levels on day 2 were significantly higher in the B3 subgroup compared to A3 subgroup (p < 0.05). The procalcitonin serum levels were significantly higher (cut-off 10 ng/ml) in the B2 subgroup compared to A2 subgroup (p < 0.05), while for other subgroups it did not differ significantly.
ANOVA analysis of variance along with the Bonferroni post-hoc multiple comparisons (Table 9) and boxplots (Figure 2, Figure 3 and Figure 4) were used for explanatory analysis of the differences in serum biomarkers concentrations (CRP, WBC, and fibrinogen) between subgroups. While ANOVA analysis revealed in the majority of cases a statistically significant difference in mean serum biomarkers concentrations between at least two groups (p < 0.05), the Bonferroni post-hoc test found that a statistically significant mean difference in: white blood cells count from the first day between A2-B2 (p= 0.010; 95% CI: -16.24- -1.17), and A3-B3 subgroups (p= 0.022; 95% CI: -15.53- -0.64), serum CRP concentration from the first day between A2-B2 subgroups (p = 0.003; 95% CI: -5.47- -0.64), serum CRP concentration from the fifth day between A3-B3 subgroups (p = 0.04; 95% CI: 10.27-39.14), and serum fibrinogen concentration from the third day between A2-B2 subgroups (p = 0.008; 95% CI: 0.86-10.36), respectively.
A Random Effects GLS regression was used to measure the association between predictor variables, such as serum biomarkers levels (WBC, CRP, and fibrinogen) measured on three different occasions, and an outcome variable, proven neonatal sepsis (Table 10). Our model had a p value < 0.001, a R-squared value within groups of 0.47, and between groups of 0.82, while rho was 0.42. The statistically significant predictors of neonatal sepsis were the white blood cells count from the first (p = 0.005) and third day (p = 0.028), and CRP values from the first day (p = 0.004).
Table 11 summarizes the AUC for proven sepsis of the WBC, CRP, and fibrinogen serum levels measured on three different occasions, as well as for I/T and procalcitonin measured on one occasion. Moreover, it summarizes the AUC values corresponding to various combinations of these biomarkers. Our results showed that procalcitonin (AUC - 0.78) and CRP measured on the first day (AUC - 0.76) had the best predictive performance for early onset neonatal sepsis. The best predictive performance for this type of sepsis was obtained by the combinations of biomarkers: WBC, CRP, and fibrinogen recorded on the first day (AUC: 0.83), and WBC, CRP, and fibrinogen recorded on the third day (AUC: 0.90), respectively. The corresponding plots of AUC are presented as supplementary materials (Figure S1- S15).
4. Discussion
In order to prevent the morbidity and mortality related to EOS, identifying the main risk factors along with early diagnosis and therapy are crucial. Along with PROM, GA <30 weeks, male sex, birth weight <1500 g, inadequate prenatal care, low socio-economic status of the mother, poor maternal nutrition, maternal substance abuse, clinical chorioamnionitis and lack of intrapartum antibiotics were cited as risk factors for neonatal sepsis [18,35].
Our study revealed that prematurity was significantly more frequent in the EOS group (p<0.001). We found that out of 16 (76%) preterm neonates who developed EOS, 9 patients (90%) had PROM ≥ 18 hours, and 7 patients (63.7%) had PROM < 18 hours. Consistent with the data reported in the literature, the present study also showed that in the subgroup with proven sepsis male infants were predominant (subgroup A1: n=6, 60%; subgroup B1: n=8, 72%, EOS subgroups: n=14, 66%), although this parameter did not present statistical significance [36,37,38,39]. Male neonates were reported to be at higher risk for EOS, according to the study on the largest population (n=56 261, 50.8%) and the one extended over the longest period (18 years) [39,40]. However, there are studies whose results have identified an equal gender ratio or a predominance of females [41,42,43].
Marks et al. reviewed the literature over a period of 40 years in order to estimate the time until obtaining positive blood cultures in EOS [44]. On a total of 6188 blood cultures (5848 neonates), 250 positive cultures were identified, of which 146 were contaminants. The majority of blood cultures (54%) were positive for Group B Streptococcus (GBS). Moreover, in their study, 7 out of 8 (20%) neonates positive to Escherichia coli died from EOS. Recent studies, identified a change in the distribution of organism causing EOS, with a predominance of Gram-negative rods, especially Escherichia coli [45]. National Institute of Child Health and Human birth (NICHD), identified an increase from 3.2 to 5.09/1000 in Escherichia coli EOS and a decrease in GBS sepsis from 5.9 to 2.08/1000 on a cohort of VLBW infants [46].
Our results were consistent with these changes, Escherichia coli (n= 5/10; 50%) being the agent most isolated in group A, followed by Staphylococcus spp. (n= 3/10; 30%), Klebsiella pneumoniae (n= 1/10; 10%) and Streptococcus spp. (n= 1/10; 10%). In contradiction to group A, the pathogens inducing sepsis in group B were Klebsiella pneumoniae (n=4/11; 36.3%), Staphylococcus spp. (n= 3/11; 27.2%), Streptococcus spp. (n= 3/11; 27.2%) and Listeria monocytogenes (n=1/11; 9%). Sabry et al., identified Klebsiella pneumoniae as the leading cause of EOS in term infants [47]. In another study on term infants EOS was most frequently caused by Group B Streptococcus, Escherichia coli and Enterococcus spp. [48]. By comparison, the present study showed the following bacteria on term infants: group A (Staphylococcus epidermidis: n=1, 10%), whereas in group B there were 2 neonates with Klebsiella pneumoniae (27%), 1 with Staphylococcus epidermidis (18%), and 1 was positive for both of them. The rate of gram-negative infection was higher in term than in preterm infants (60% vs 45%). In contrast, the rate of gram-positive sepsis was higher in preterm than in term infants (76% vs 24%). Overall, gram-positive organisms were isolated in 12 patients (57%), and gram-negative pathogens were identified in the probes of 9 infants (42%).
However, there are still numerous studies which reported Group B Streptococcus to be the most prevalent cause of EOS, especially in term infants [49,50]. These also include studies conducted in Southern Europe [51]. In the Greek study, this happens after the exclusion of Coagulase-negative staphylococci (CoNS) which were predominant (28.6%) [51].
Our region ranked first in the European colonization rate (6–32%), followed by Eastern Europe (19–29%) and Western Europe (11–21%) [52]. In contradiction, the literature cites Coagulase-negative staphylococci as a characteristic complication of LOS [53]. Of the total of 21 infants with EOS, the one who died had the blood culture positive for Staphylococcus capitis. Interesting, this pathogen has been isolated in the intensive care units of seventeen countries. Given the increased drug resistance, the unfavorable prognosis was not surprising.
As both CRP and PCT are influenced by gestational age and birth weight, it is also important to take into consideration the optimal time of determination [54]. It was demonstrated that term infants have higher CRP than preterm [55]. Eschborn et al., reviewed the kinetics of PCT and CRP, and concluded that in order to rule out EOS, it is more conclusive to determine CRP and PCT at 12 hours of life rather than immediately after birth [56]. They also emphasized that serial determinations of these markers and their correlation with clinical findings were needed to support the decision of antibiotic therapy.
Neonatal complications (asphyxia, meconium aspiration, shock and intraventricular hemorrhage) and maternal risk factors (prolonged labor, PROM) may also cause increase values of CRP [57]. In this context, there has been a constant quest for other markers that could be included in the laboratory panels used for evaluation of newborns suspected of EOS. Newer studied markers like endocan, have elevated levels in newborns with sepsis (both early-onset and late-onset) and it is not influenced by gestational age, sex, fetal distress (meconium-stained amniotic fluid), delivery method or minor birth trauma [58,59,60].
According to recent studies, presepsin may be a better marker than CRP and PCT for the diagnosis of EOS and for monitoring the response to therapy. Its value rise early in the umbilical cord blood of the newborns with PPROM, does not vary with GA, postnatal age or with perinatal factors and decreases progressively with the administration of antibiotics [61,62]. However, these biomarkers were not available for evaluation in our cohort of patients.
Another study which investigated WBC, PLT and CRP in the diagnosis of EOS, reported normal values for WBC and PLT in both day 1 and day 3, but high values of CRP in both days, with an even elevated value in day 3 [41]. In our study, 7 (70%) patients with EOS (subgroup A1) showed high levels of CRP in day 1 and 3, while 6 (60%) of them had elevated CRP in day 5. The majority of neonates (n=8; 72%) with EOS and PROM <18 hours showed high CRP levels in day 3. Furthermore, the results from our random Effects GLS regression indicated as statistically significant predictors of neonatal sepsis were the white blood cells count from the first (p= 0.005) and third day (p= 0.028), and CRP values from the first day (p= 0.004).
A biomarker is considered good if the AUC is higher than 0.75 or excellent if greater than 0.9, respectively. Hence, in our study, out of all the researched biomarkers, procalcitonin (AUC - 0.78) and CRP measured on the first day (AUC - 0.76) had the best predictive performance for early onset neonatal sepsis. Even if we obtained good results, and procalcitonin is known as an early biomarker for neonatal sepsis, there are studies which state that it may also be increased in healthy newborns, and could be more accurate in diagnosing late onset neonatal sepsis [63]. Moreover, our results showed that a combination of biomarkers (WBC, CRP, and fibrinogen), evaluated on the first and third day of life, had superior accuracy in detecting early onset neonatal sepsis (AUC: 0.83, AND 0.90, respectively).
Stocker et al., studied the relationship between simultaneous determination of CRP, PCT and WBC in no sepsis, sepsis uncertain, sepsis probable and sepsis proven patients [43]. When comparing the proven sepsis group with the no sepsis one, they reported an AUC of 0.986 for CRP, and an AUC of 0,921 for PCT, and those values increased with extended time frames up to 36 hours, whereas there was no difference between start to 36 hours vs start to 48 hours. In our study, although the AUC for CRP and PCT were lower, they did decrease between the first, second, and third determination. This change in the biomarker ‘s dynamic could be the result of antibiotherapy.
This study has the following limitations: retrospective design, unbalanced data for the proven sepsis subgroups, limited number of biomarkers included. Further studies, on larger cohorts of neonates with early onset sepsis, that would include multiple panels of biomarkers could offer a more consistent perspective over the topic.
Supplementary Materials
Figure S1. AUC WBC day 1; Figure S2. AUC WBC day 3; Figure S3. AUC WBC day 5; Figure S4. AUC CRP day 1; Figure S5. AUC CRP day 3; Figure S6. AUC CRP day 5; Figure S7. AUC FIB day 1; Figure S8. AUC FIB day 3; Figure S9. AUC FIB day 5; Figure S10. AUC I/T; Figure S11. AUC PCT; Figure S12. AUC I/T+PCT; Figure S13. AUC parameters day 1; Figure S14. AUC parameters day 3; Figure S15. AUC parameters day 5.
Author Contributions
This paper was written as part of a doctoral program of M.A.H. at UMF “Grigore T. Popa”. Conceptualization, M.A.H, G.I.Z., P.V., V.H., A.H., A-S.M-P., A.C., and L.P.; methodology, M.M-P., E.M.,I.A.V., and D.N.; software, I.A.V; validation, M.M-P., E.M.,I.A.V., and D.N.; formal analysis, M.M-P., E.M.,I.A.V., and D.N.; investigation, I M.A.H, G.I.Z., P.V., V.H., A.H., A-S.M-P., A.C., and L.P.; resources, I.A.V.; data curation M.M-P., E.M.,I.A.V., and D.N.; writing—original draft preparation, M.A.H, G.I.Z., P.V., V.H., A.H., A-S.M-P., A.C., and L.P.; writing—review and editing, M.A.H, G.I.Z., P.V., V.H., A.H., A-S.M-P., A.C., and L.P.; visualization, I.A.V; supervision, D.N.; project administration, L.P; All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the regional hospital (No. 5332/21.05.2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank our patients for participating in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Al-Lawama M, AlZaatreh A, Elrajabi R, Abdelhamid S, Badran E. Prolonged Rupture of Membranes, Neonatal Outcomes and Management Guidelines. J Clin Med Res. 2019; 11: 360-366. [CrossRef]
- Musilova I, Bestvina T, Hudeckova M, Michalec I, Cobo T, Jacobsson B, Kacerovsky M. Vaginal fluid interleukin-6 concentrations as a point-of-care test is of value in women with preterm prelabor rupture of membranes. American Journal of Obstetrics and Gynecology. 2016; 215: 619. [CrossRef]
- Toprak E, Bozkurt M, Dinçgez Çakmak B, Özçimen EE, Silahlı M, Ender Yumru A, Çalışkan E. Platelet-to-lymphocyte ratio: A new inflammatory marker for the diagnosis of preterm premature rupture of membranes. J Turk Ger Gynecol Assoc. 2017; 18: 122-6. [CrossRef]
- Caloone J, Rabilloud M, Boutitie F, Traverse-Glehen A, Allias-Montmayeur F, Denis L, Boisson-Gaudin C, Hot IJ, Guerre P, Cortet M, Huissoud C; ICAMs Study Group. Accuracy of several maternal seric markers for predicting histological chorioamnionitis after preterm premature rupture of membranes: a prospective and multicentric study. Eur J Obstet Gynecol Reprod Biol. 2016; 205:133-140. [CrossRef]
- Văduva CC, Constantinescu C, Radu MM, Văduva AR, Pănuş A, Ţenovici M, DiŢescu D, Albu DF. Pregnancy resulting from IMSI after testicular biopsy in a patient with obstructive azoospermia. Rom J Morphol Embryol. 2016; 57: 879-883.
- Albu DF, Albu CC, Văduva C-C, Niculescu M, Edu A. Diagnosis problems in a case of ovarian tumor-case presentation. Romanian Journal of Morphology and Embryology= Revue Roumaine de Morphologie et Embryologie. 2016; 57: 1437-1442.
- Enătescu I, Craina M, Gluhovschi A, Giurgi-Oncu C, Hogea L, Nussbaum LA, Bernad E, Simu M, Cosman D, Iacob D, Marinescu I, Enătescu VR. The role of personality dimensions and trait anxiety in increasing the likelihood of suicide ideation in women during the perinatal period. J Psychosom Obstet Gynaecol. 2021; 42: 242-252. [CrossRef]
- Enatescu VR, Bernad E, Gluhovschi A, Papava I, Romosan R, Palicsak A, Munteanu R, Craina M, Enatescu I. Perinatal characteristics and mother's personality profile associated with increased likelihood of postpartum depression occurrence in a Romanian outpatient sample. J Ment Health. 2017; 26: 212-219. [CrossRef]
- Covali R, Socolov D, Socolov R. Coagulation tests and blood glucose before vaginal delivery in healthy teenage pregnant women compared with healthy adult pregnant women. Medicine (Baltimore). 2019; 98: e14360. [CrossRef]
- Covali R, Socolov D, Socolov R, Pavaleanu I, Carauleanu A, Akad M, Boiculese VL, Adam AM. Complete Blood Count Peculiarities in Pregnant SARS-CoV-2-Infected Patients at Term: A Cohort Study. Diagnostics (Basel). 2021; 12. [CrossRef]
- Vicoveanu P, Vasilache IA, Nemescu D, Carauleanu A, Scripcariu IS, Rudisteanu D, Burlui A, Rezus E, Socolov D. Predictors Associated with Adverse Pregnancy Outcomes in a Cohort of Women with Systematic Lupus Erythematosus from Romania-An Observational Study (Stage 2). J Clin Med. 2022; 11. [CrossRef]
- Nemescu D, Constantinescu D, Gorduza V, Carauleanu A, Caba L, Navolan DB. Comparison between paramagnetic and CD71 magnetic activated cell sorting of fetal nucleated red blood cells from the maternal blood. J Clin Lab Anal. 2020; 34: e23420. [CrossRef]
- Iliescu M, Cărăuleanu A. The Portrait of a Good Doctor: Conclusions from a Patients and Medical Students Survey. Revista de Cercetare si Interventie Sociala. 2014; 47: 261-271.
- Cucu A, Costea C, Cărăuleanu A, Dumitrescu G, Sava, A, Scripcariu I, Costan, V-V, Turliuc, S, Poeata, I, Turliuc, D. Meningiomas Related to the Chernobyl Irradiation Disaster in North-Eastern Romania Between 1990 and 2015. Revista de Chimie -Bucharest- Original Edition. 2018; 69. [CrossRef]
- Turliuc, D, Turliuc, S, Cucu, S, Dumitrescu G, Cărăuleanu, A, Buzdugă, C, Camelia, Tamas, Sava, A, Costea, C. A review of analogies between some neuroanatomical terms and roman household objects. Annals of anatomy = Anatomischer Anzeiger: official organ of the Anatomische Gesellschaft. 10.1016/j.aanat.2015.07.001. 2015. [CrossRef]
- Dorfeuille N, Morin V, Tétu A, Demers S, Laforest G, Gouin K, Piedboeuf B, Bujold E. Vaginal Fluid Inflammatory Biomarkers and the Risk of Adverse Neonatal Outcomes in Women with PPROM. Am J Perinatol. 2016; 33: 1003-7. [CrossRef]
- Zhuang L, Li ZK, Zhu YF, Ju R, Hua SD, Yu CZ, Li X, Zhang YP, Li L, Yu Y, Zeng W, Cui J, Chen XY, Peng JY, Li T, Feng ZC. The correlation between prelabour rupture of the membranes and neonatal infectious diseases, and the evaluation of guideline implementation in China: a multi-centre prospective cohort study. Lancet Reg Health West Pac. 2020; 3: 100029. [CrossRef]
- Mukhopadhyay S, Puopolo KM, editors. Risk assessment in neonatal early onset sepsis. Seminars in perinatology; 2012: Elsevier. [CrossRef]
- Sgro M, Yudin MH, Lee S, Sankaran K, Tran D, Campbell D. Early-onset neonatal sepsis: It is not only group B streptococcus. Paediatr Child Health. 2011; 16: 269. [CrossRef]
- Shim GH, Kim SD, Kim HS, Kim ES, Lee HJ, Lee JA, et al. Trends in epidemiology of neonatal sepsis in a tertiary center in Korea: a 26-year longitudinal analysis, 1980-2005. J Korean Med Sci. 2011; 26: 284-289. [CrossRef]
- Shah BA, Padbury JF. Neonatal sepsis: an old problem with new insights. Virulence. 2014; 5: 170-178. [CrossRef]
- Ganesan P, Shanmugam P, Sattar SB, Shankar SL. Evaluation of IL-6, CRP and hs-CRP as Early Markers of Neonatal Sepsis. J Clin Diagn Res. 2016; 10: Dc13-17. [CrossRef]
- Ovayolu A, Ovayolu G, Karaman E, Yuce T, Turgut A, Bostancıeri N. Maternal serum endocan concentrations are elevated in patients with preterm premature rupture of membranes. J Perinat Med. 2019; 47: 510-515. [CrossRef]
- Benitz WE. Adjunct laboratory tests in the diagnosis of early-onset neonatal sepsis. Clin Perinatol. 2010; 37: 421-438. [CrossRef]
- Helmbrecht AR, Marfurt S, Chaaban H. Systematic Review of the Effectiveness of the Neonatal Early-Onset Sepsis Calculator. J Perinat Neonatal Nurs. 2019; 33: 82-88. [CrossRef]
- Hornik CP, Benjamin DK, Becker KC, Benjamin DK Jr, Li J, Clark RH, Cohen-Wolkowiez M, Smith PB. Use of the complete blood cell count in early-onset neonatal sepsis. Pediatr Infect Dis J. 2012; 31: 799-802. [CrossRef]
- Sharma D, Farahbakhsh N, Shastri S, Sharma P. Biomarkers for diagnosis of neonatal sepsis: a literature review. J Matern Fetal Neonatal Med. 2018; 31: 1646-1659. [CrossRef]
- Gandhi P, Kondekar S. A Review of the Different Haematological Parameters and Biomarkers Used for Diagnosis of Neonatal Sepsis. EMJ Hematology. 2019: 85-92. [CrossRef]
- Hedegaard SS, Wisborg K, Hvas AM. Diagnostic utility of biomarkers for neonatal sepsis--a systematic review. Infect Dis (Lond). 2015; 47: 117-124. [CrossRef]
- Vouloumanou EK, Plessa E, Karageorgopoulos DE, Mantadakis E, Falagas ME. Serum procalcitonin as a diagnostic marker for neonatal sepsis: a systematic review and meta-analysis. Intensive Care Med. 2011; 37: 747-762. [CrossRef]
- Hincu MA, Zonda GI, Stanciu GD, Nemescu D, Paduraru L. Relevance of Biomarkers Currently in Use or Research for Practical Diagnosis Approach of Neonatal Early-Onset Sepsis. Children (Basel). 2020; 7. [CrossRef]
- Odabasi IO, Bulbul A. Neonatal Sepsis. Sisli Etfal Hastan Tip Bul. 2020; 54: 142-158. [CrossRef]
- Tuzun F, Ozkan H, Cetinkaya M, Yucesoy E, Kurum O, Cebeci B, Cakmak E, Ozkutuk A, Keskinoglu P, Baysal B, Kumral A, Duman N. Is European Medicines Agency (EMA) sepsis criteria accurate for neonatal sepsis diagnosis or do we need new criteria? Plos one. 2019; 14: e0218002. [CrossRef]
- Gibbs RS, Blanco JE, St. Clair PJ, Castaneda YS. Quantitative bacteriology of amniotic fluid from women with clinical intraamniotic infection at term. Journal of Infectious Diseases. 1982; 145: 1-8. [CrossRef]
- Simonsen KA, Anderson-Berry AL, Delair SF, Davies HD. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27: 21-47. [CrossRef]
- Achten NB, Dorigo-Zetsma JW, van Rossum AMC, Oostenbrink R, Plötz FB. Risk-based maternal group B Streptococcus screening strategy is compatible with the implementation of neonatal early-onset sepsis calculator. Clin Exp Pediatr. 2020; 63: 406-410. [CrossRef]
- Polcwiartek LB, Smith PB, Benjamin DK, Zimmerman K, Love A, Tiu L, Murray S, Kang P, Ebbesen F, Hagstrøm S, Clark RH, Greenberg RG. Early-onset sepsis in term infants admitted to neonatal intensive care units (2011-2016). J Perinatol. 2021; 41: 157-163. [CrossRef]
- Karabulut B, Alatas SO. Diagnostic Value of Neutrophil to Lymphocyte Ratio and Mean Platelet Volume on Early Onset Neonatal Sepsis on Term Neonate. J Pediatr Intensive Care. 2021; 10: 143-147. [CrossRef]
- Kuzniewicz MW, Puopolo KM, Fischer A, Walsh EM, Li S, Newman TB, Kipnis P, Escobar GJ. A Quantitative, Risk-Based Approach to the Management of Neonatal Early-Onset Sepsis. JAMA Pediatr. 2017; 171: 365-371. [CrossRef]
- Ko MH, Chang HY, Li ST, Jim WT, Chi H, Hsu CH, Peng CC, Lin CY, Chen CH, Chang JH. An 18-year retrospective study on the epidemiology of early-onset neonatal sepsis - emergence of uncommon pathogens. Pediatr Neonatol. 2021; 62: 491-498. [CrossRef]
- Shaaban HA, Safwat N. Mean platelet volume in preterm: a predictor of early onset neonatal sepsis. J Matern Fetal Neonatal Med. 2020; 33: 206-211. [CrossRef]
- Arcagok BC, Karabulut B. Platelet to Lymphocyte Ratio in Neonates: A Predictor of Early onset Neonatal Sepsis. Mediterr J Hematol Infect Dis. 2019; 11: e2019055. [CrossRef]
- Stocker M, van Herk W, El Helou S, Dutta S, Schuerman FABA, van den Tooren-de Groot RK, Wieringa JW, Janota J, van der Meer-Kappelle LH, Moonen R, Sie SD, de Vries E, Donker AE, Zimmerman U, Schlapbach LJ, de Mol AC, Hoffman-Haringsma A, Roy M, Tomaske M, F Kornelisse R, van Gijsel J, Visser EG, Plötz FB, Heath P, Achten NB, Lehnick D, van Rossum AMC. C-Reactive Protein, Procalcitonin, and White Blood Count to Rule Out Neonatal Early-onset Sepsis Within 36 Hours: A Secondary Analysis of the Neonatal Procalcitonin Intervention Study. Clin Infect Dis. 2021; 73: 383-390. [CrossRef]
- Marks L, de Waal K, Ferguson JK. Time to positive blood culture in early onset neonatal sepsis: A retrospective clinical study and review of the literature. J Paediatr Child Health. 2020; 56: 1371-1375. [CrossRef]
- Koenig JM, Keenan WJ. Group B streptococcus and early-onset sepsis in the era of maternal prophylaxis. Pediatr Clin North Am. 2009; 56: 689-708. [CrossRef]
- Stoll BJ, Hansen NI, Sánchez PJ, Faix RG, Poindexter BB, Van Meurs KP, Bizzarro MJ, Goldberg RN, Frantz ID 3rd, Hale EC, Shankaran S, Kennedy K, Carlo WA, Watterberg KL, Bell EF, Walsh MC, Schibler K, Laptook AR, Shane AL, Schrag SJ, Das A, Higgins RD; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011; 127: 817-826. [CrossRef]
- Sabry N, Abdelhakeem M, Mohamed H, Baheeg G. Validity of Platelet to Lymphocyte Ratio and Neutrophil to Lymphocyte Ratio in Diagnosing Early-onset Neonatal Sepsis in Full-term Newborns. Journal of Comprehensive Pediatrics. 2022. [CrossRef]
- Al-Matary A, Heena H, AlSarheed AS, Ouda W, AlShahrani DA, Wani TA, Qaraqei M, Abu-Shaheen A. Characteristics of neonatal Sepsis at a tertiary care hospital in Saudi Arabia. J Infect Public Health. 2019; 12: 666-672. [CrossRef]
- Kim SJ, Kim GE, Park JH, Lee SL, Kim CS. Clinical features and prognostic factors of early-onset sepsis: a 7.5-year experience in one neonatal intensive care unit. Korean J Pediatr. 2019; 62: 36-41. [CrossRef]
- Dong Y, Basmaci R, Titomanlio L, Sun B, Mercier JC. Neonatal sepsis: within and beyond China. Chin Med J (Engl). 2020; 133: 2219-2228. [CrossRef]
- Gkentzi D, Kortsalioudaki C, Cailes BC, Zaoutis T, Kopsidas J, Tsolia M, Spyridis N, Siahanidou S, Sarafidis K, Heath PT, Dimitriou G. Epidemiology of infections and antimicrobial use in Greek Neonatal Units. Arch Dis Child Fetal Neonatal Ed. 2019; 104: 293-297. [CrossRef]
- Barcaite E, Bartusevicius A, Tameliene R, Kliucinskas M, Maleckiene L, Nadisauskiene R. Prevalence of maternal group B streptococcal colonisation in European countries. Acta Obstet Gynecol Scand. 2008; 87: 260-271. [CrossRef]
- Wirth T, Bergot M, Rasigade JP, Pichon B, Barbier M, Martins-Simoes P, Jacob L, Pike R, Tissieres P, Picaud JC, Kearns A, Supply P, Butin M, Laurent F. Niche specialization and spread of Staphylococcus capitis involved in neonatal sepsis. Nat Microbiol. 2020; 5: 735-745. [CrossRef]
- Chiesa C, Natale F, Pascone R, Osborn JF, Pacifico L, Bonci E, De Curtis M. C reactive protein and procalcitonin: reference intervals for preterm and term newborns during the early neonatal period. Clin Chim Acta. 2011; 412: 1053-1059. [CrossRef]
- Eichberger J, Resch E, Resch B. Diagnosis of Neonatal Sepsis: The Role of Inflammatory Markers. Front Pediatr. 2022; 10: 840288. [CrossRef]
- Eschborn S, Weitkamp JH. Procalcitonin versus C-reactive protein: review of kinetics and performance for diagnosis of neonatal sepsis. J Perinatol. 2019; 39: 893-903. [CrossRef]
- Mjelle AB, Guthe HJT, Reigstad H, Bjørke-Monsen AL, Markestad T. Serum concentrations of C-reactive protein in healthy term-born Norwegian infants 48-72 hours after birth. Acta Paediatr. 2019; 108: 849-854. [CrossRef]
- Saldir M, Tunc T, Cekmez F, Cetinkaya M, Kalayci T, Fidanci K, Babacan O, Erdem G, Kocak N, Sari E, Akgul EO, Kul M. Endocan and Soluble Triggering Receptor Expressed on Myeloid Cells-1 as Novel Markers for Neonatal Sepsis. Pediatr Neonatol. 2015; 56: 415-421. [CrossRef]
- Zonda GI, Zonda R, Cernomaz AT, Paduraru L, Grigoriu BD. Endocan serum concentration in uninfected newborn infants. J Infect Dev Ctries. 2019; 13: 817-822. [CrossRef]
- Zonda GI, Zonda R, Cernomaz AT, Paduraru L, Avasiloaiei AL, Grigoriu BD. Endocan - a potential diagnostic marker for early onset sepsis in neonates. J Infect Dev Ctries. 2019; 13: 311-317. [CrossRef]
- Seliem W, Sultan AM. Presepsin as a predictor of early onset neonatal sepsis in the umbilical cord blood of premature infants with premature rupture of membranes. Pediatr Int. 2018; 60: 428-432. [CrossRef]
- Ruan L, Chen GY, Liu Z, Zhao Y, Xu GY, Li SF, Li CN, Chen LS, Tao Z. The combination of procalcitonin and C-reactive protein or presepsin alone improves the accuracy of diagnosis of neonatal sepsis: a meta-analysis and systematic review. Crit Care. 2018; 22: 316. [CrossRef]
- Liu C, Fang C, Xie L. Diagnostic utility of procalcitonin as a biomarker for late-onset neonatal sepsis. Transl Pediatr. 2020; 9: 237-242. [CrossRef]
Figure 1.
Flowchart of the study group distribution.
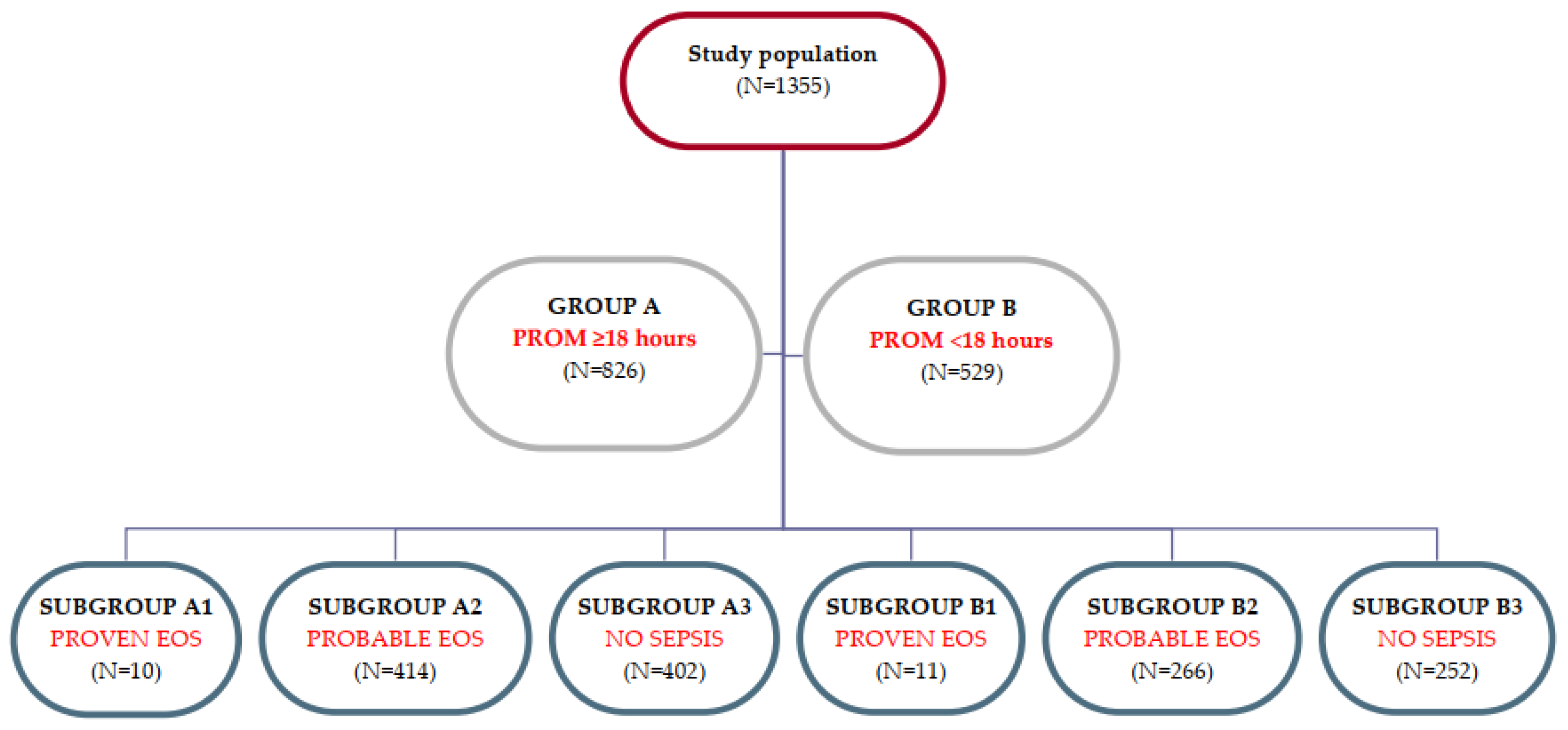
Figure 2.
Boxplot representing the white blood cells count from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
Figure 2.
Boxplot representing the white blood cells count from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
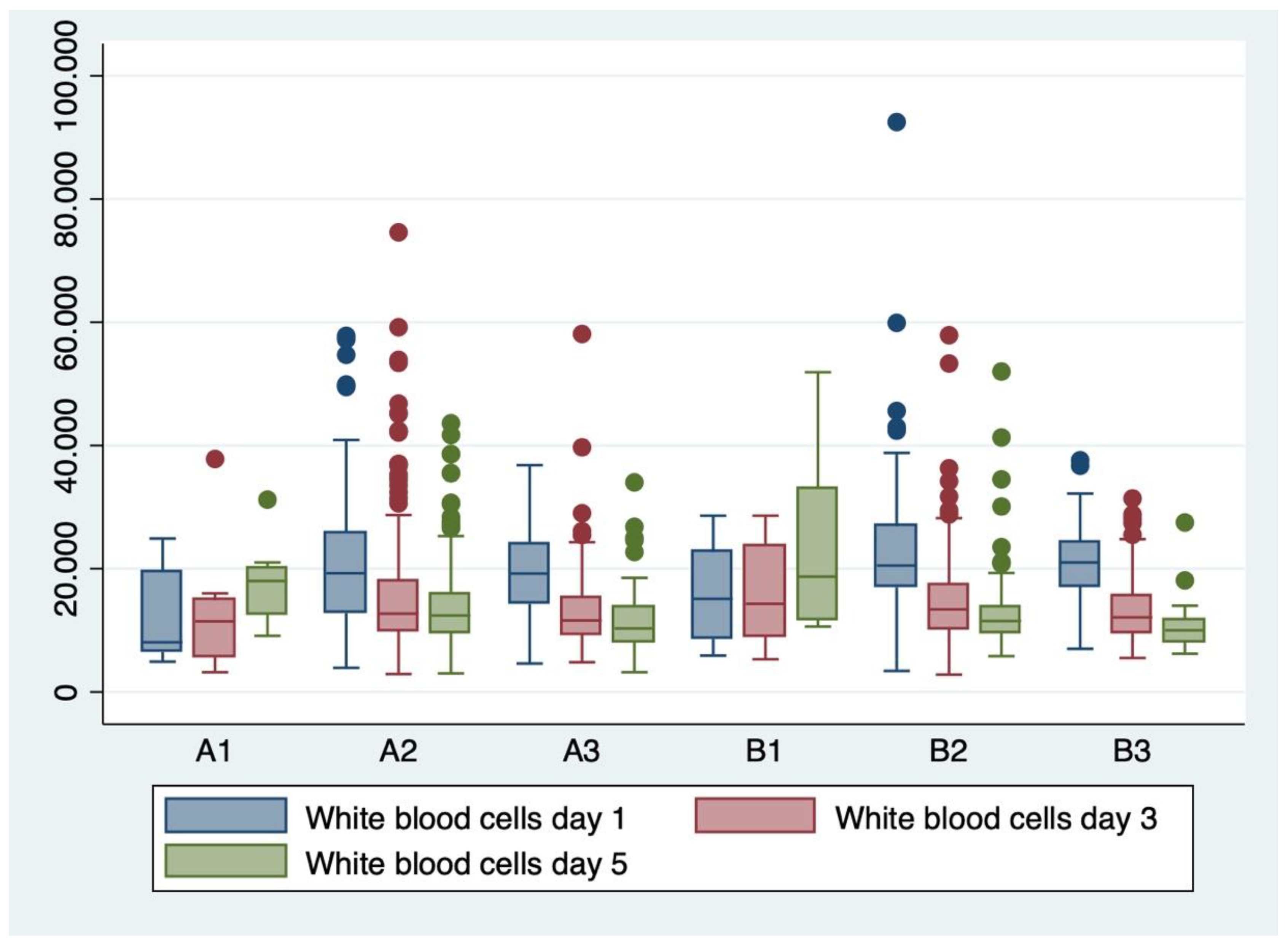
Figure 3.
Boxplot representing the C-reactive protein (CRP) serum concentrations from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
Figure 3.
Boxplot representing the C-reactive protein (CRP) serum concentrations from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
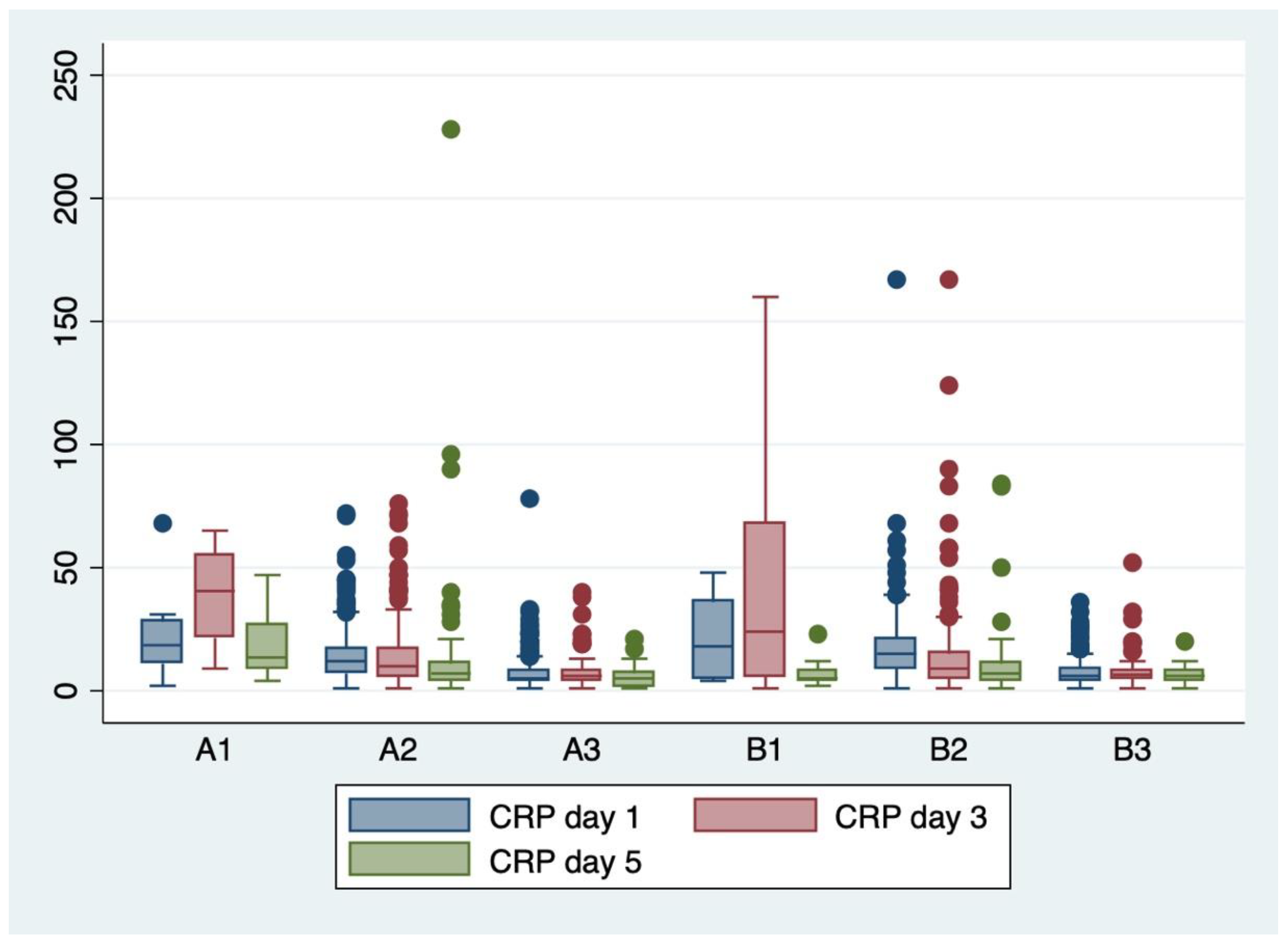
Figure 4.
Boxplot representing the fibrinogen serum concentrations from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
Figure 4.
Boxplot representing the fibrinogen serum concentrations from days 1, 3, and 5 in the evaluated subgroups (A1-A3, B1-B3).
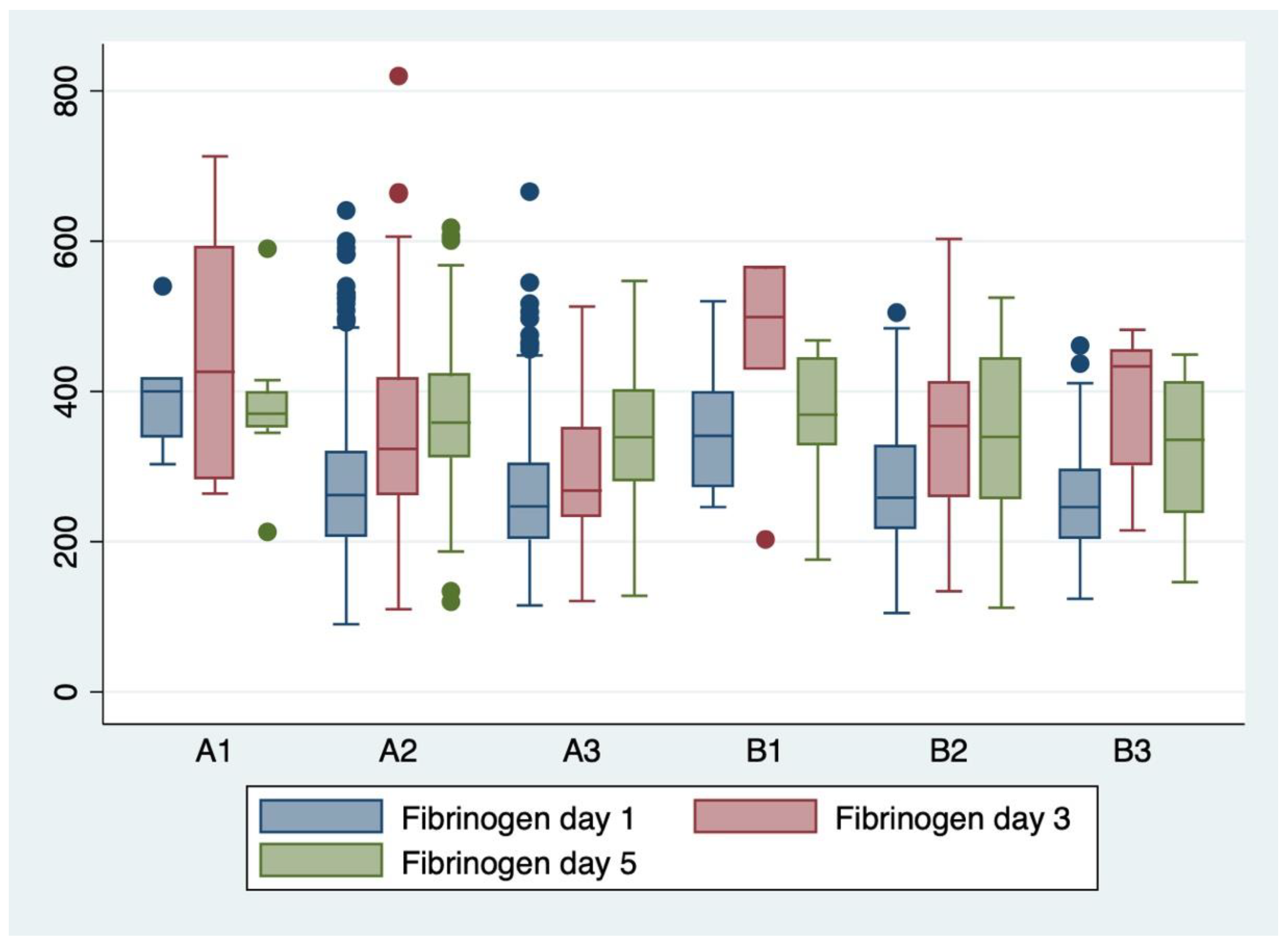
Table 6.
Comparison of the hematological parameters of the groups.
| Parameters | PROM >18 hours GROUP A |
PROM <18 hours GROUP B |
Independent t-Test | |||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | T | P value | |||||
|
WBC x 103 /mm3 D1/D3/D5 |
19.54 ± 8.02 |
14.45 ± 8.21 |
13.1 ± 6.34 |
21.2 ± 7.87 |
14.34 ± 6.54 |
13.19 ± 7.61 |
-3.7 0.2 0.0 |
<0.001 >0.05 >0.05 |
| I/T ratio | 0.14 ± 0.11 |
0.15 ± 0.08 |
-0.53 | >0.05 | ||||
|
CRP mg/L D1/D3/D5 |
10.83 ± 9.56 |
11.86 ± 11.26 |
8.58 ± 15.06 |
13.02 ± 12.4 |
12.97 ± 18.35 |
8.51 ± 9.40 |
-3.3 -1.0 0.0 |
<0.001 >0.05 >0.05 |
|
Fibrinogen D1/D3/D5 |
270 ± 98.3 |
332 ± 118.6 |
362 ± 88.3 |
268 ± 79.8 |
362± 114.2 |
340 ± 108.9 |
0.16 -1.7 1.4 |
>0.05 >0.05 >0.05 |
* Table 6 legend: PROM- prolonged rupture of membranes; WBC- white blood cells; CRP- c- reactive protein; I/T- immature/total neutrophils ratio; D- day; SD- standard deviation.
Table 7.
Comparison of the serum biomarkers measurements for the proven sepsis subgroups.
|
PROVEN SEPSIS Subgroup A1 Subgroup B1 |
Day 1 | Day 3 | Day 5 | Independent t-test |
|
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | t | P value | |
| WBC x 103 /mm3 | 12.05 ± 7.74 | 13.15 ± 10.89 | 17.71 ± 6.98 | -0.8 -0.5 -1.0 |
>0.05 >0.05 >0.05 |
| 15.1 ± 8.03 | 15.49 ± 8.13 | 23.67 ± 15 | |||
| I/T ratio | 0.20 ± 0.08 | 2.0 | >0.05 | ||
| 0.12 ± 0.04 | |||||
| CRP mg/L | 21.5 ± 19.10 | 38.5 ± 18.75 | 20.64 ± 14.25 | 0.4 0.0 2.1 |
>0.05 >0.05 >0.05 |
| 19.57 ± 16.93 | 38.36 ± 7.56 | 47.88 ± 6.48 | |||
| Fibrinogen | 399 ± 81.4 | 450 ± 191 | 380 ± 103 | 0.7 -0.0 0.3 |
>0.05 >0.05 >0.05 |
| 355 ± 109.4 | 457 ± 125 | 358 ± 104 | |||
* Table 7 legend: WBC- white blood cells; CRP- c- reactive protein; I/T- immature/total neutrophils ratio; SD- standard deviation.
Table 8.
Comparison of the serum biomarkers measurements for the subgroups with suspected sepsis or without proven sepsis.
Table 8.
Comparison of the serum biomarkers measurements for the subgroups with suspected sepsis or without proven sepsis.
|
Suspected EOS Subgroup A2 Subgroup B2 |
Day 1 | Day 3 | Day 5 | Independent t-test |
|
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | t | P value | |
| WBC x 103 /mm3 | 20.13 ± 9.15 | 13.92 ± 9.15 | 15.31 ± 9.05 | -2.4 0.6 0.7 |
<0.05 >0.05 >0.05 |
| 21.9 ± 9.18 | 13.23 ± 6.9 | 14.83 ± 7.09 | |||
| I/T ratio | 0.14 ± 0.12 | -0.4 | >0.05 | ||
| 0.15 ± 0.09 | |||||
| CRP mg/L | 13.96 ± 10.17 | 13.4 ± 6.7 | 17.6 ± 9.78 | -3.0 -0.3 0.2 |
<0.05 >0.05 >0.05 |
| 17 ± 4.37 | 13.8 ± 9.32 | 18 ± 10.7 | |||
| Fibrinogen | 277 ± 104 | 343 ± 120 | 364 ± 87.6 | 0.1 -0.0 1.3 |
>0.05 >0.05 >0.05 |
| 275 ± 84.7 | 344 ± 109 | 342 ± 110 | |||
|
No sepsis Subgroup A3 Subgroup B3 |
Day 1 Mean ± SD |
Day 3 Mean ± SD |
Day 5 Mean ± SD |
t | P value |
| WBC x 103 /mm3 | 19.09 ± 6.44 | 13.02 ± 6.13 | 11.42 ± 4.80 | -3.0 -0.5 0.9 |
<0.05 >0.05 >0.05 |
| 20.76 ± 5.57 | 13.39 ± 5.19 | 10.55 ± 3.99 | |||
| I/T ratio | 0.104 ± 0.09 | -3.5 | >0.05 | ||
| 0.14 | |||||
| CRP mg/L | 7.03 ± 6.5 | 7.18 ± 5.77 | 4.99 ± 3.38 | -0.9 -0.7 -2.0 |
>0.05 >0.05 <0.05 |
| 7.57 ± 5.6 | 7.80 ± 6.93 | 6.22 ± 3.42 | |||
| Fibrinogen | 257 ± 86 | 293 ± 92.67 | 350 ± 88 | 0.1 -2.5 0.8 |
>0.05 <0.05 >0.05 |
| 255 ± 68.11 | 383 ± 99.59 | 320 ± 115 | |||
* Table 8 legend: EOS- early onset sepsis; WBC- white blood cells; CRP- c- reactive protein; I/T- immature/total neutrophils ratio; SD- standard deviation.
Table 9.
ANOVA analysis of variance and Bonferroni post-hoc test for the serum biomarkers for neonatal sepsis.
Table 9.
ANOVA analysis of variance and Bonferroni post-hoc test for the serum biomarkers for neonatal sepsis.
| Serum biomarkers | Groups | ANOVA results | Bonferroni test | |||||
|---|---|---|---|---|---|---|---|---|
| F score | P value | Mean difference | Standard error | P value | 95% confidence interval lower limit | 95% confidence interval upper limit | ||
|
WBC day 1 |
A1-B1 | 7.13 | <0.001 | -3.05 | 3.45 | 1.000 | - 13.21 | 7.11 |
| A2-B2 | -8.71 | 2.56 | 0.010 | -16.24 | -1.17 | |||
| A3-B3 | -8.08 | 2.53 | 0.022 | -15.53 | -0.64 | |||
| WBC day 3 | A1-B1 | 2.79 | 0.016 | -2.34 | 3.59 | 1.000 | -12.92 | 8.24 |
| A2-B2 | 0.48 | 0.68 | 1.000 | -1.53 | 2.50 | |||
| A3-B3 | -0.037 | 0.90 | 1.000 | -3.03 | 2.28 | |||
| WBC day 5 | A1-B1 | 8.27 | <0.001 | -5.96 | 3.23 | 0.98 | -15.49 | 3.57 |
| A2-B2 | 0.68 | 0.82 | 1.000 | -1.73 | 3.10 | |||
| A3-B3 | 0.87 | 1.28 | 1.000 | -2.91 | 4.66 | |||
| CRP day 1 | A1-B1 | 41.43 | <0.001 | 1.92 | 4.92 | 1.000 | -12.55 | 16.40 |
| A2-B2 | -3.05 | 0.82 | 0.003 | -5.47 | -0.64 | |||
| A3-B3 | -0.54 | 0.91 | 1.000 | -3.22 | 2.13 | |||
| CRP day 3 | A1-B1 | 21.4 | <0.001 | 0.13 | 6.33 | 1.000 | -18.50 | 18.78 |
| A2-B2 | -0.39 | 1.16 | 1.000 | -3.84 | 3.05 | |||
| A3-B3 | -0.61 | 1.79 | 1.000 | -5.91 | 4.68 | |||
| CRP day 5 | A1-B1 | 3.2 | 0.007 | 11.19 | 6.37 | 1.000 | -7.59 | 29.98 |
| A2-B2 | 0.45 | 1.41 | 1.000 | -3.72 | 4.62 | |||
| A3-B3 | 24.70 | 4.90 | 0.04 | 10.27 | 39.14 | |||
| Fibrinogen day 1 | A1-B1 | 5.2 | <0.001 | 43.9 | 55.08 | 1.000 | -118.29 | 206.09 |
| A2-B2 | 1.41 | 9.02 | 1.000 | -25.16 | 27.98 | |||
| A3-B3 | 1.34 | 10.40 | 1.000 | -29.28 | 31.97 | |||
| Fibrinogen day 3 | A1-B1 | 4.96 | <0.001 | -7.19 | 63.63 | 1.000 | -195.52 | 181.14 |
| A2-B2 | 5.60 | 1.61 | 0.008 | 0.86 | 10.36 | |||
| A3-B3 | -90.39 | 42.92 | 0.541 | -217.45 | 36.65 | |||
| Fibrinogen day 5 | A1-B1 | 0.73 | 0.59 | 21.16 | 50.95 | 1.000 | -130.06 | 172.39 |
| A2-B2 | 22.34 | 16.88 | 1.000 | -27.75 | 72.44 | |||
| A3-B3 | -1.23 | 2.34 | 1.000 | -8.14 | 5.68 | |||
* Table 9 legend: WBC- white blood cells; CRP- c- reactive protein; I/T- immature/total neutrophils ratio.
Table 10.
Random Effects Random Effects Generalized Least Squares regression of biochemical predictors for neonatal sepsis.
Table 10.
Random Effects Random Effects Generalized Least Squares regression of biochemical predictors for neonatal sepsis.
| Serum biomarkers | P value | 95% Confidence interval |
|---|---|---|
| WBC day 1 | 0.005 | 0.016- 0.09 |
| WBC day 3 | 0.028 | -0.08- -0.004 |
| WBC day 5 | 0.769 | -0.04- 0.03 |
| CRP day 1 | 0.004 | -0.01- 0.02 |
| CRP day 3 | 0.063 | -0.0008- 0.03 |
| CRP day 5 | 0.483 | -0.044- 0.021 |
| Fibrinogen day 1 | 0.642 | -0.002- 0.001 |
| Fibrinogen day 3 | 0.823 | -0.002- 0.002 |
| Fibrinogen day 5 | 0.117 | -0.004- 0.0004 |
* Table 10 legend: WBC- white blood cells; CRP- c- reactive protein.
Table 11.
AUC for proven sepsis.
| Biomarker | AUC value |
|---|---|
| WBC day 1 | 0.55 |
| WBC day 3 | 0.47 |
| WBC day 5 | 0.49 |
| CRP day 1 | 0.76 |
| CRP day 3 | 0.66 |
| CRP day 5 | 0.62 |
| Fibrinogen day 1 | 0.34 |
| Fibrinogen day 3 | 0.37 |
| Fibrinogen day 5 | 0.35 |
| I/T | 0.58 |
| PCT | 0.78 |
| WBC+ CRP+Fibrinogen (day 1) | 0.83 |
| WBC+ CRP+Fibrinogen (day 3) | 0.90 |
| WBC+ CRP+Fibrinogen (day 5) | 0.70 |
| I/T+ PCT | 0.76 |
* Table 11 legend: WBC- white blood cells; CRP- c- reactive protein; I/T- immature/total neutrophils ratio; PCT- procalcitonin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



