
Submitted:
03 December 2023
Posted:
05 December 2023
You are already at the latest version
Abstract
Background: Caffeine is an ergogenic aid that still needs to be investigated in female sports per-formance. Methods: Eight semi-professional female volleyball (Heigth=1.63±0.08 m; Weigth= 66.67 ± 4,.74 kg) players voluntarily participated in this study. A randomised crossover design was carried out. Players went through the caffeine and placebo condition. In the caffeine condi-tion, participants consumed 5 mg/kg of caffeine. The evaluations were performed over two weeks of training. In both conditions, the countermovement jump test, repeated jumps for 15s and hand-grip were performed. Change of direction was assessed using the 505 test. Well-being was also assessed by a wellness questionnaire. A repeated measures Anova and correlation analysis were performed. Results: The repeated-measures ANOVA revealed a main effect of supplementation (F (1.7) = 8.41, p = 0.02, η2 = 0.54) across the training week on physical performance. Besides, there was a positive effect on perceived fatigue (F (1.7) = 7.29, p = 0.03, η2 = 0.51). Conclusions: Caf-feine improved performance and fatigue parameters over one week of training.
Keywords:
supplementation
; caffeine
; sport perfomance
; volleyball
; ergogenic aids.
1. Introduction
It is well known that high-performance athletes are exposed to a multitude of training sessions and competitions that cause a lot of physical and mental stress, a fact that encourages many athletes to use ergogenic aids to cope with this stressful situation. Particularly volleyball is considered one of the most popular sports in the world [1]. It involves specific tasks such as jumping, landing, blocking and throwing the ball, which in turn must be combined with fast movements, a fact that places high demands on the musculoskeletal system [2].
Elsewhere, the use of caffeine it is considered as a potential ergogenic aid able to enhance the athletic performance of volleyball players [3]. it is widely used as an ergogenic aid in both individual and team sports because of its rapid perceived stimulant effect in a wide range of sporting disciplines [4]. In addition, it has been classified as a safe supplement by the International Society of Sports Nutrition (ISSN) [5]. Its intake has been increased according with his positive effect on aerobic [6,7] and anaerobic activities [3,6,8], increasing strength and power capacity [9] by an enhance of intracellular calcium and Na+-K+ ATPase pump activity [10], and delaying the onset of fatigue [11] through activation on central nervous system blocks adenosine receptors [11,12,13].
In this respect, caffeine has been well documented its effect in jump capacity [3], nevertheless the effect on agility tests like change of direction is unclear, there is some evidence that conclude that caffeine did not improve it [8], while other study in female volleyball players describe a significant positive effect [14]. More evidence is needed to determine the effect of caffeine on agility, especially in women's volleyball. Gomez-Bruton et al (2021) concludes that acute caffeine intake is capable of enhance team sports performance in female athletes. Therefore, it could be effective as an ergogenic aid in female team athletes [15].
Regarding to dose intake, its well stablished that a range from 3 to 9 mg/Kg enhance the athletic performance [6,8,16,17]. Concerning to the timing ingestion, because of his rapid absorption and plasma availability [11], caffeine intake one hour before training session have been shown as an optimal strategy to enhance performance [18]. Therefore, in the present study our team programmed a caffeine intake of 5mg/Kg of body mass one hour before the training session.
Volleyball has a pre-competitive phase and a long-competitive phase on its calendar, as with other team sports. The aim of the pre-competitive season is to prepare the athletes to maximize their adaptative response to competitions and to copy with psychophysiological demands of the competitive season. In this sense, appropriate load control must be managed in order to balance stress-recovery cycle and to maintain high performance during all season [19,20]. In recent decades, the term internal load in team sports is in the process of highlight the importance to control the fatigue and stress induced by competitions, training sessions and daily life, since it is a determinant, along with external load, of training outcome [21,22,23]).
Accordingly, subjective wellness questionnaires are suggested as convenient instruments for measuring internal load in team sport athletes [21,24,25]. The questionnaires reflect player's perception of muscle pain [26], general fatigue [25] sleep quality [27], ratio of perceived exertion [28] and psychological stress [29].
Caffeine has been proven to deliver positive outcomes in reducing rating of perceived exertion [30,31,32,33], diminishes muscular soreness or damage [34,35] although to a lesser degree than males [30,33], and enhances performance in eumenorrhoeic female population [4,10,36]. However, a main undesiderable aspect to consider of caffeine supplementation in athletes is that could affect negatively to quality sleep [37], especially in female athletes due to the effect of caffeine remains longer in women than in men [38]. Recent studies have highlighted the lack of research on caffeine dose-response including sleep, fatigue and performance assessments [39,40]. Indeed, recent studies reported that there are still more studies in males, with studies in females being scarce [18], specifically on strength [41]. Thus, studies on the effect of caffeine on strength in women are required.
Therefore, the purpose of this study is to establish the ergogenic effect of 5 g /Kg caffeine on wellness (sleep, fatigue, stress and muscle soreness) and physical performance (COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count) in female volleyball team athletes.
2. Materials and Methods
2.1. Participants
Eight female volleyball players from the "Spanish Women's Superleague 2" voluntarily participated in this study. The anthropometric characteristics are shown in Table 1. All of them were informed of the purpose of the study and signed an informed consent form. This study was reviewed and approved by the Bioethics Committee of the University of Granada (registration number: 3014/CEIH/2022). This research was conducted under the guidelines of the World Helsinki Assembly, updated in Fortaleza in 2013 at the World Medical Assembly, for the study in human subjects. All participants were advised not to take drugs or medications before or during this study, and to maintain their usual dietary habits. They were also instructed not to take any supplements for at least 2 weeks prior to the study.
2.2. Familiarization
Prior to the experimental phase, the players underwent a familiarization session with the tests (505 test, handgrip, CMJ and RJ). In the same week, another session was held for the participants to perform the Yo-Yo Test and anthropometric features.
2.3. Experimental Design
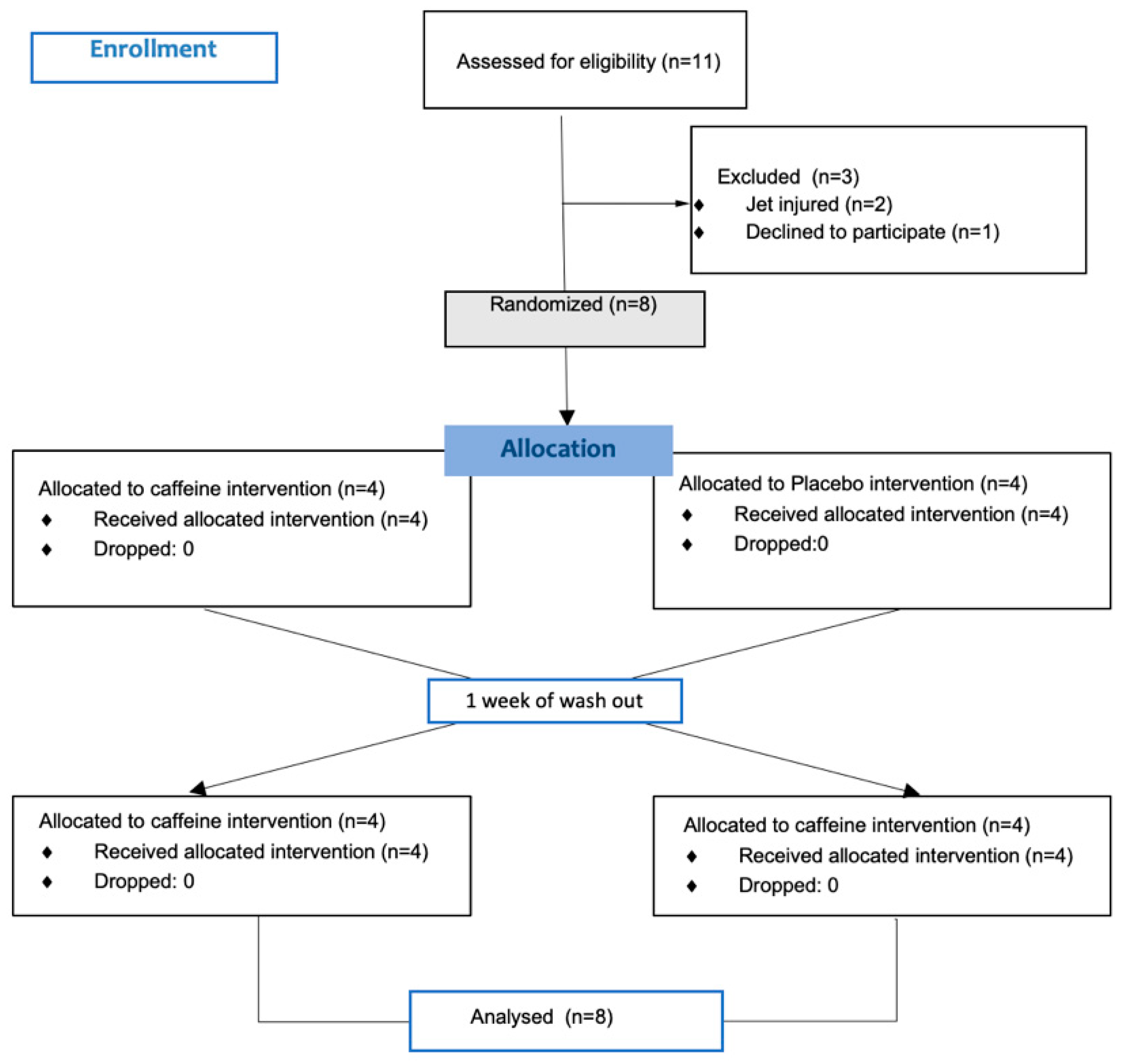
In this study, a randomised, double-blind, crossover design was used. Each participant underwent the PLACEBO condition for one week and the SUPPLEMENTATION condition for another week. During the supplementation participants intake 5 mg/kg mixed with a maltodrextin-based beverage one hour before the measurements while during the placebo they ingested only the maltodextrin-based beverage. Both conditions were ingested one hour before the measurements. The dose and timing of intake was established following previous studies carried out in male volleyball players [3] . Simultaneously, the players filled in the Hooper & Mackinnon, 1995) wellness questionnaire one hour before training. Consult González-Fernández et al. (2022) for further information. The physical. measurements took place in the volleyball court just before training (Tuesday Thursday and Friday). The players performed a warm-up similar to the match warm-up. Afterwards, they performed the measurements in the following order: Handgrip, CMJ, 505 test and RJ15". For each of the measurements, two attempts were made, separated by 3 min and the better score was taken, excluding RJ15”, which only one set was assessed. Between each of the tests there was a 3 min recovery time. Before start session 1, anthropometric data also were measured.
Figure 1.
Consort flow diagram.
2.4. Procedure
Anthropometric characteristics. First, body composition was evaluated before the training (09:00 pm) with shorts and removed shoes and any metal and jewelry prior to assessment. For the evaluation of body composition, the Bioelectrical Impedance Analysis (BIA) method was used with a TANITA® (MC980MA PLUS, Arlington Heights, Illinois).
Countermovement jump (CMJ). The CMJ was evaluated using the Chronojump-Boscosystem® (Barcelona, Spain) (version 2.0.2.) that presents an intraclass correlation between 0.821 and 0.949 to measure the high jump. This system was connected to a Microsoft Windows Computer (w.11). Participants were instructed to keep the hands-on-waist CMJ a knee angle of~90° and to land with their legs extended with maximal feet plantar flexion. All participants performed 3 trials with 20 s (sec) of recovery between repetitions to minimize the effect of fatigue and three minutes between the different load jumps. The best jump in centimeters (cm) was considered as the final outcome.
Repeated Jump 15” (RJ15”). After performing the 5-0-5 test, and following a 3-minute rest period, the participants carried out one bout of maximal intensity (CMJs) for 15 seconds. Leg muscle power and jumping ability were assessed based on the jump height. The same instrument used for CMJ measurements was employed. Based on this process, the maximum and minimum values were taken into account. Besides, the fatigue index (FI) and reactive strength index (RSI) was calculated. FI was calculated by taking the average height (H) of the first 4 jumps and the average height of the last 4 jumps, as per Equation [44]:
Elsewhere, RSI was calculated according to the following equation [45]:
Handgrip. Handgrip strength encompasses the maximum force generated through the combined contraction of extrinsic and intrinsic muscles of the hand, resulting in the flexion of hand joints [46]. A hand-dynamometer (TKK-5401, Takei Scientific Instruments, NiigataCity, Japan) was employed to quantify this parameter. The players were seated in an upright position, facing the researcher, with their shoulder adducted and elbow flexed at a 90-degree angle, while allowing the forearm to rest lightly on the arm of the chair or on the subject's thigh. Alternating hand testing was conducted, with each hand undergoing two rounds of assessment, interspersed with 10-second rest intervals [47].
505 COD test. The methodology for the 505-COD was as per originally established methods [48]. Therefore, this involved a 10-m linear sprint from a static start, as well as a 5-m returning through an identified finish line. The time between 5-m and turning sprint line was recorded (seconds) (see Figure 2). All participants performed 2 attempts with 3 minutes (min) of recovery between repetitions. The best time in seconds (sec) was recorded in a Microsoft Windows® Excel template (Redmond, Washington, USA). Chronojump Photocell ® (Chronojump, Barcelona, Spain) and Chronojump software version 1.7.1.8 were used to measure time [49].
YOYO test. YYIRT—Level 1 was used as a means of assessing participants' aerobic capacity. The original protocol established by Krustrup et al., 2003) [50] is meticulously respected. The test consisted of performing a 2×20 m sprint, interspersed with a short 10-second walking recovery period. Starting at 10 km/h, determined by a beep, the intensity increases by 0.5 km/h until the player is exhausted. In the 10–13 km/h range, four 2 × 20 m sprints were performed, followed by seven runs at 13.5–14 km/h. Afterward, eight series were made for each stage [51]. The test was conducted within the confines of an indoor volleyball court. The conclusion of the test is determined when a player does not reach the required speed or does not reach the indicated line when beeps on two consecutive occasions. The total distance traveled during the test is recorded as the primary result.
2.5. Statistical Analysis
Descriptive statistics were calculated for each variable. For data processing, the mean and standard deviation were used. The Kolmogorov–Smirnov was conducted to verify whether all data were normally distributed. The experiment consisted on the within-participants factor of supplementation condition (supplementation condition and placebo condition) and moment condition (MD-4, MD-3, and MD-1). Internal intensity (sleep, fatigue, stress and muscle soreness) and external intensity (Handgrip dominant hand and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count) were analyzed using a repeated-measures ANOVA. Effect size is indicated with partial eta squared for Fs. Posteriorly, a Pearson correlation coefficient r was used to examine the relationship between values of internal load and values of external load, and to interpret the magnitude of these correlations, we adopted the following criteria: very small (0.01), small (0.20), medium (0.50), large (0.80), very large (1.20), huge (2.0) as initially suggested by Cohen (1988) [52] and expanded by Sawilowsky (2009 [53]. In addition, the regression analysis was used to identify which values of internal load can better explain the values of external load. The magnitude of r2 was interpreted as follows: >0.02, small; >0.13, medium; >0.23, large. The inflation factors of the variance were calculated to verify that the collinearity was not a serious concern. The data were analyzed using the software Statistics (version 13.1; Statsoft, Inc., Tulsa, OK, USA) and the alpha level was set at p < 0.05.
3. Results
Descriptive statistics were calculated for each internal intensity (Sleep, Stress, Fatigue and Muscle soreness) and external intensity variables (Handgrip dominant hand and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count) (see Table 1).
Table 1 Within-week variations (MD-4, MD-3, and MD-1) of (i) internal intensity: Sleep, Stress, Fatigue and Muscle soreness, and (ii) external intensity: Handgrip dominant hand and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count (mean ± SD).
First, a repeated measures ANOVA with participants’ mean sleep did not reveal any significant main effect of supplementation condition, moment condition and interaction, F (1.7) = 2.85, p = 0.13, η2 = 0.28, F (2.14) = 2.88, p = 0.09, η2 = 0.29, and F<1, respectively. Second, a new repeated measures ANOVA with participants’ mean fatigue revealed a significant main effect of supplementation condition, F (1.7) = 7.29, p = 0.03, η2 = 0.51, with lower values in the supplementation condition (3.13± 1.69) than in the placebo condition (3.71± 1.71). However, the analysis did not reveal a significant effect of moment, F<1. The interaction between supplementation condition and moment condition, F (2.14) = 1.04, p = 0.37, η2 = 0.1, was not significant. Third, a new repeated measures ANOVA with participants’ mean stress did not showed a significant main effect of supplementation condition, F<1. Nevertheless, dataset revealed a significant effect of moment (2.14) = 4.69, p = 0.02, η2 = 0.40, with a decrement of values thought the week (3.81 to 2.88). The interaction between supplementation condition and moment condition, F (2.14) = 1.58, p = 0.23, η2 = 0.18, was not significant. Last, another repeated measures ANOVA with participants’ mean muscle soreness showed a significant main effect of supplementation condition, F (1.7) = 7.54, p = 0.02, η2 = 0.52, with lower values in the supplementation condition (3.08± 1.69) than in the placebo condition (3.88± 1.30). However, the analysis did not show a significant effect of moment, (2.14) = 2.46, p = 0.12, η2 = 0.26. The interaction between supplementation condition and moment condition, F<1, was not significant.
In the same direction, a news repeated-measures ANOVA with participants’ mean external intensity (handgrip dominant and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count) were performed to try to elucidate the main effects and interactions of different measures. Elsewhere, a repeated measures ANOVA with participants’ mean handgrip dominant did not reveal any significant main effect of supplementation condition, F (1.7) = 1.18, p = 0.32, η2 = 0.19, and moment condition, F<1. However, the dataset revealed an interaction supplementation x moment condition, F (2.14) = 9.56, p = 0.004, η2 = 0.65. Otherwise, another repeated measures ANOVA with participants’ mean handgrip non dominant did not revealed a significant main effect of supplementation condition, moment condition or interaction, F<1, in all cases. A repeated measures ANOVA with participants’ mean COD 505 test did not reveal any significant main effect of supplementation condition and interaction between supplementation condition and moment condition, F<1 in both cases. However, we found a main effect of moment, (2.14) = 4.61, p = 0.03, η2 = 0.39, with a decrement of values thought the week (4.31 to 4.14). Another repeated measures ANOVA with participants’ mean CMJ height revealed a significant main effect of supplementation condition, F (1.7) = 8.41, p = 0.02, η2 = 0.54, with higher values in the supplementation condition (35.61±5.47) than in the placebo condition (33.10±5.79). Notwithstanding, we found a main effect of moment, (2.14) = 6.40, p = 0.01, η2 = 0.47, with a decrement of values thought the week (32.44 to 34.68). The interaction between supplementation condition and moment condition, F<1, was not significant. Similar to above analysis, a repeated measures ANOVA with participants’ mean RJ height showed a significant main effect of supplementation condition, F (1.7) = 5.97, p = 0.04, η2 = 0.46, with higher values in the supplementation condition (29.61±2.86) than in the placebo condition (27.50±3.37). In addition, we found a main effect of moment, (2.14) = 8.57, p = 0.001, η2 = 0.55, with an increment of values since MD-4 to MD-1 (27.22 to 29.04). However, the interaction between supplementation condition and moment condition, F<1, was not significant. Regarding RJ RSI, a repeated measures ANOVA with participants’ mean RJ RSI revealed a significant main effect of supplementation condition, F (1.7) = 22.88, p = 0.001, η2 = 0.76, with higher values in the supplementation condition (1.29±0.22) than in the placebo condition (1.16±0.16). Thus, we found a main effect of moment, (2.14) = 12.91, p = 0.001, η2 = 0.64, with an increment of values thought the week (1.10 to 1.27). The interaction between supplementation condition and moment condition, F<1, was not significant. Another repeated measures ANOVA with participants’ mean RJ min jump revealed a significant main effect of of moment, (2.14) = 15.18, p = 0.001, η2 = 0.68, with an increment of values thought the week (18.89 to 23.77). Nonetheless, the main effect of supplementation condition neither the interaction between supplementation condition and moment condition, F<1, was not significant. Crucially, the repeated measures ANOVA with participants’ mean RJ max jump did not revealed any significant main effects [Supplementation, (1.7) = 1.53, p = 0.25, η2 = 0.17; Moment, F<1]. The interaction between supplementation condition and moment condition, (2.14) = 1.85, p = 0.19, η2 = 0.29, neither was significant. Another repeated measures ANOVA with participants’ mean RJ fatigue index revealed a significant main effect of supplementation condition, F (1.7) = 7.33, p = 0.03, η2 = 0.51, with higher values in the supplementation condition (102.81±12.04) than in the placebo condition (95.28±11.94). However, the main effect of moment, (2.14) = 1.20, p = 0.32, η2 = 0.14, and the interaction between supplementation condition and moment condition, F<1, were not significant. Last, a repeated measures ANOVA with participants’ mean stress did not showed a significant main effect of supplementation condition, F<1. Nevertheless, dataset revealed a significant effect of moment (1.7) = 4.69, p = 0.02, η2 = 0.40, with a decrement of values thought the week (3.81 to 2.88). The interaction between supplementation condition and moment condition, F (2.14) = 1.58, p = 0.23, η2 = 0.18, was not significant. Last, another repeated measures ANOVA with participants’ mean RJ time cont. revealed a significant main effect of moment, F (2.14) = 20.81, p = 0.001, η2= 0.74. In this sense, dataset did not reveal any main effect of supplementation condition, neither interaction between supplementation condition and moment condition, F<1, in both cases.
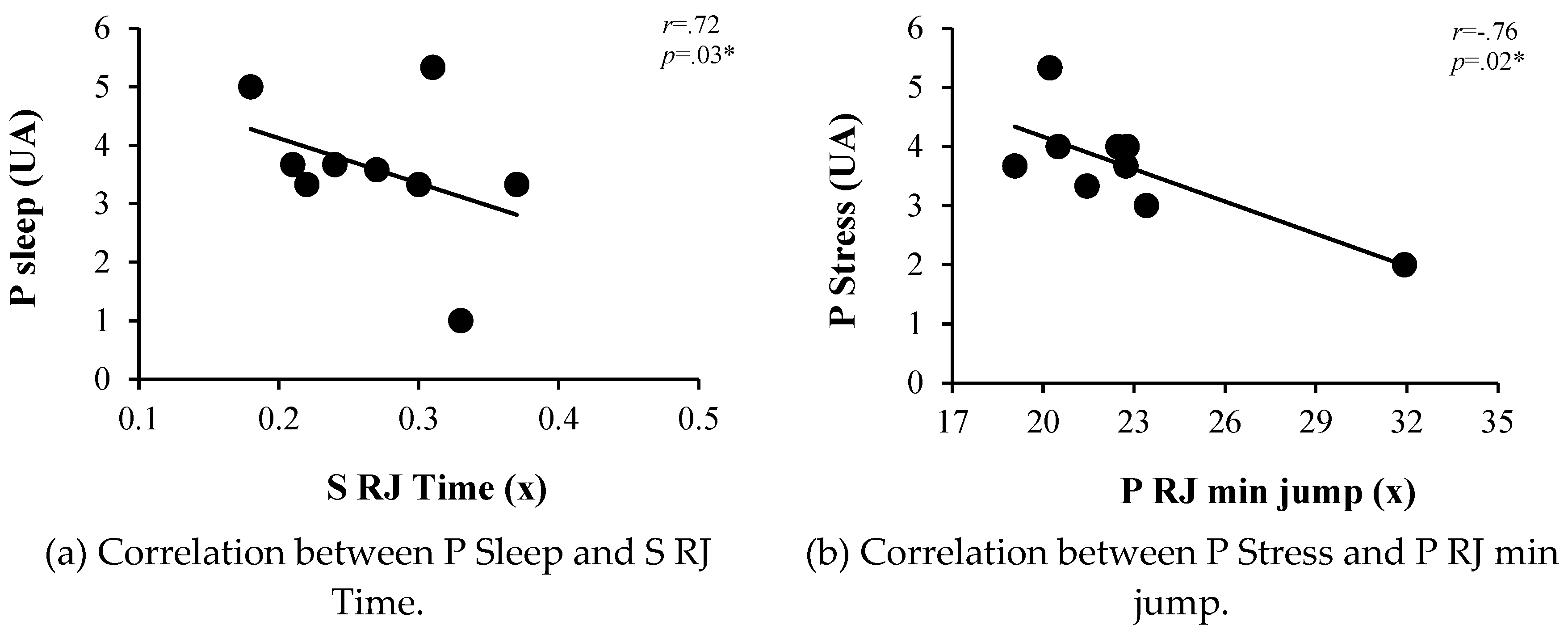
At this point, a correlation analysis was performed between participants’ mean of supplementation condition (supplementation and placebo) of external intensity: Handgrip dominant and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count, and participants’ mean of supplementation condition (supplementation and placebo) of internal intensity: Sleep, Stress, Fatigue and Muscle soreness. Negative large correlations were found between placebo RJ min jump and placebo stress (r=-.75 and p=.02*). In addition, other supplementation RJ time con and Placebo Sleep (r=.72 and p=.03*). No other correlations were found. (See Table 2 and Figure 1, for more information).

Table 2.
Internal and external values.
| Suplementation Condition | Placebo condition | |||||
|---|---|---|---|---|---|---|
| MD-4 | MD-3 | MD-1 | MD-4 | MD-3 | MD-1 | |
| Internal intensity | ||||||
| Sleep (AU) | 3.38 ± 1.92 | 2.88 ± 2.10 | 2.88± 1.81 | 4.38 ±1.77 | 3.50 ± 1.51 | 2.88 ± 1.81 |
| Fatigue (AU) | 3.00 ± 1.51 | 3.13 ± 1.36 | 3.25 ± 2.19 | 4.00 ± 1.60 | 3.63 ± 1.60 | 3.50 ± 1.93 |
| Stress (AU) | 3.75 ± 1.28 | 3.50 ± 1.85 | 2.88 ± 1.73 | 3.88 ± 0.99 | 4.25 ± 1.39 | 2.88 ± 1.13 |
| Muscle Soreness (AU) | 2.63 ± 1.19 | 3.13 ± 1.55 | 3.50 ± 2.33 | 3.25 ± 1.04 | 3.88 ± 1.46 | 4.50 ± 1.41 |
| External Intensity | ||||||
| Handgrip dominant (kg) | 33.61 ± 4.10 | 35.58 ± 3.71 | 35.04 ± 3.46 | 34.46 ± 3.73 | 33.19 ± 3.21 | 35.35 ± 4.71 |
| Hand non-dominant(kg) | 31.83 ± 4.39 | 32.51 ± 4.16 | 31.01 ± 4.63 | 32.62 ± 2.08 | 32.23 ± 4.47 | 32.60 ± 3.89 |
| COD 505 test (sec) | 4.32 ± 0.19 | 4.17 ± 0.19 | 4.13 ± 0.14 | 4.31 ± 0.23 | 4.17 ± 0.19 | 4.15 ± 0.11 |
| CMJ height (cm) | 34.18 ± 5.60 | 37.18 ± 4.70 | 35.47 ± 6.09 | 30.69 ± 4.42 | 34.72 ± 5.95 | 33.88 ± 6.99 |
| RJ height (cm) | 28.27 ± 2.76 | 30.28 ± 2.40 | 30.29 ± 3.41 | 26.18 ± 2.61 | 28.54 ± 4.53 | 27.79 ± 2.98 |
| RJ RSI (m/s) | 1.18 ± 0.16 | 1.35 ± 0.25 | 1.35 ± 0.26 | 1.02 ± 0.16 | 1.26 ± 0.17 | 1.19 ± 0.15 |
| RJ min Jump (cm) | 20.32 ± 2.36 | 24.73 ± 2.58 | 23.07 ± 2.68 | 19.45 ± 3.68 | 24.25 ± 5.30 | 24.48 ± 4.37 |
| RJ max jump (cm) | 34.16 ± 2.09 | 32.77 ± 3.63 | 32.09 ± 3.79 | 31.33± 3.71 | 32.64 ± 3.75 | 32.53 ± 3.68 |
| RJ fat index (%) | 108.70 ± 14.40 | 101.98 ± 12.02 | 97.75 ± 9.69 | 94.98 ± 12.85 | 96.25 ± 11.51 | 94.60 ±11.47 |
| RJ contact time (s) | 0.34 ± 0.11 | 0.25 ± 0.04 | 0.23 ± 0.03 | 0.32±0.11 | 0.25 ± 0.06 | 0.25 ± 0.05 |
Table 3.
Pearson correlation coefficient between (i) internal intensity: Sleep, Stress, Fatigue and Muscle soreness, and (ii) external intensity: Handgrip dominant and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count (mean ± SD). *Significance at p < 0.05. **Significance at p < 0.01.
Table 3.
Pearson correlation coefficient between (i) internal intensity: Sleep, Stress, Fatigue and Muscle soreness, and (ii) external intensity: Handgrip dominant and non-dominant, COD 505 test, CMJ height, RJ height, RJ RSI, RJ min Jump, RJ max jump, RJ fat index, RJ time count (mean ± SD). *Significance at p < 0.05. **Significance at p < 0.01.
| S Sleep | P Sleep | S Fat | P Fat | S Stress | P Stress | S MS | P MS | ||
|---|---|---|---|---|---|---|---|---|---|
| S HG Dom | r=.12 | r=-.01 | r=.13 | r=-.12 | r=.12 | r=-.57 | r=.01 | r=-.13 | |
| p=.76 | p=.98 | p=.73 | p=.74 | p=.75 | p=.10 | p=.97 | p=.73 | ||
| P HG Dom | r=-.17 | r=-.17 | r=.11 | r=-.05 | r=.14 | r=-.59 | r=.14 | r=.02 | |
| p=.65 | p=.65 | p=.76 | p=.89 | p=.70 | p=.09 | p=.70 | p=.94 | ||
| S HG Non-Dom | r=-.38 | r=-.29 | r=.06 | r=.11 | r=.25 | r=-.48 | r=.32 | r=.16 | |
| p=.31 | p=.43 | p=.87 | p=.76 | p=.50 | p=.18 | p=.38 | p=.67 | ||
| P HG Non-Dom | r=-.01 | r=-.03 | r=.27 | r=-.13 | r=.12 | r=-.57 | r=.01 | r=-.17 | |
| p=.99 | p=.93 | p=.47 | p=.75 | p=.75 | p=.10 | p=.97 | p=.66 | ||
| S COD 505 test | r=.17 | r=-.10 | r=.08 | r=.20 | r=.11 | r=.06 | r=.23 | r=.44 | |
| p=.65 | p=.78 | p=.83 | p=.59 | p=.76 | p=.85 | p=.54 | p=.22 | ||
| P COD 505 test | r=.15 | r=-.17 | r=.09 | r=.32 | r=.15 | r=.26 | r=.29 | r=.50 | |
| p=.69 | p=.65 | p=.79 | p=.39 | p=.68 | p=.48 | p=.44 | p=.17 | ||
| S CMJ height | r=-.01 | r=.25 | r=.03 | r=.01 | r=-.04 | r=.16 | r=.03 | r=-.22 | |
| p=.96 | p=.51 | p=.93 | p=.98 | p=.90 | p=.67 | p=.93 | p=.55 | ||
| P CMJ height | r=-.04 | r=.32 | r=-.04 | r=-.21 | r=-.16 | r=-.08 | r=-.14 | r=-.43 | |
| p=.89 | p=.39 | p=.90 | p=.58 | p=.67 | p=.82 | p=.71 | p=.24 | ||
| S RJ height | r=-.09 | r=-.26 | r=-.14 | r=.06 | r=.04 | r=.08 | r=.02 | r=.45 | |
| p=.80 | p=.49 | p=.70 | p=.87 | p=.91 | p=.83 | p=.95 | p=.21 | ||
| P RJ height | r=-.13 | r=-.37 | r=-.26 | r=-.06 | r=.08 | r=.40 | r=-.05 | r=.28 | |
| p=.73 | p=.32 | p=.49 | p=.86 | p=.83 | p=.28 | p=.88 | p=46 | ||
| S RJ RSI sup | r=-.19 | r=-.13 | r=-.05 | r=.01 | r=-.09 | r=-.34 | r=.17 | r=.17 | |
| p=.62 | p=.73 | p=.88 | p=.98 | p=.81 | p=.36 | p=.65 | p=.65 | ||
| P RJ RSI plac | r=.06 | r=.18 | r=.07 | r=.04 | r=-.05 | r=-.24 | r=.24 | r=.12 | |
| p=.86 | p=.62 | p=.84 | p=.91 | p=.88 | p=.53 | p=.52 | p=.75 | ||
| S RJ min jump | r=.09 | r=.17 | r=.15 | r=.11 | r=.16 | r=-.21 | r=.05 | r=.32 | |
| p=.79 | p=.66 | p=.69 | p=.77 | p=.67 | p=.57 | p=.88 | p=.39 | ||
| P RJ min jump | r=-.20 | r=.07 | r=-.27 | r=-.51 | r=-.49 | r=-.75 | r=-.41 | r=-.52 | |
| p=.59 | p=.85 | p=.47 | p=.15 | p=.17 | p=.02* | p=.26 | p=.14 | ||
| S RJ max jump | r=.18 | r=.44 | r=.13 | r=.02 | r=-.20 | r=-.36 | r=.07 | r=-.09 | |
| p=.63 | p=.22 | p=.72 | p=.94 | p=.60 | p=.33 | p=.85 | p=.81 | ||
| P RJ max jump | r=.24 | r=.38 | r=-.10 | r=-.29 | r=-.33 | r=-.22 | r=-.22 | r=-.30 | |
| p=.53 | p=.31 | p=.79 | p=.43 | p=.37 | p=.55 | p=.56 | p=.42 | ||
| S RJ Fat index | r=-.27 | r=-.42 | r=-.32 | r=-.11 | r=-.17 | r=.08 | r=-.34 | r=.07 | |
| p=.47 | p=.24 | p=.38 | p=.76 | p=.65 | p=.82 | p=.35 | p=.84 | ||
| P RJ Fat Index | r=.18 | r=.07 | r=.26 | r=.41 | r=.28 | r=.54 | r=.13 | r=.17 | |
| p=.63 | p=.84 | p=.49 | p=.27 | p=.45 | p=.13 | p=.73 | p=.64 | ||
| S RJ time | r=.60 | r=.72 | r=.46 | r=.36 | r=.27 | r=.40 | r=.20 | r=.09 | |
| p=.08 | p=.03* | p=.20 | p=.33 | p=.47 | p=.28 | p=.59 | p=.81 | ||
| P RJ time | r=-.22 | r=-.38 | r=-.45 | r=-.46 | r=-.25 | r=.15 | r=-.53 | r=-.37 | |
| p=.55 | p=.30 | p=.21 | p=.20 | p=.51 | p=.70 | p=.13 | p=.31 | ||
Figure 3.
Significant correlations between values with significant correlation.
Posteriorly, a multilinear regression analysis was performed to verify which values of internal intensity could be used to better explain the performance of external intensity variables. Table 4.
4. Discussion
This study aimed to observe the acute effect of caffeine intake over the course of one week of training in semi-professional women's volleyball players. Regarding physical parameters, the CAF condition obtained better results in handgrip, but only in the dominant hand. In a similar study, an enhancement of handgrip was found after ingestion of a drink containing 3 mg of caffeine per kilogram of body weight in male players, so the results of handgrip improvement are similar in both men and women. Other studies also found similar results for improvements in CMJ after caffeine administration in lower dose (3 mg/kg) male volleyball players [4] and badminton players. Otherwise, other studies reported an enhacement in CMJ with higher doses (≥ 6 mg/kg-1) in both female volleyball players [39] and male volleyball players [54].
Similarly, a subsequent study indicated that increased fiber recruitment by calcium release is associated with such high doses [55], indicating an improvement in isometric, concentric and eccentric maximal voluntary contractions [56]. However, in this study, the ability to maintain this improvement over a week of training with an intake of 5 mg/kg is also assessed. A main effect of supplementation was found in the repeated-measures ANOVA (F (1.7) = 8.41, p = 0.02, η2 = 0.54) over the training week. Elsewhere, as mentioned above, volleyball is a sport where different jumps take place throughout the match, so it is essential to observe the effect of caffeine on repeated jumps as the assessment of CMJ alone could not reveal a real match situation. Thus, previous studies have investigated the effect of caffeine in RJ, obtaining improvements in male volleyball players in RJ 15 s [4] and RJ 30 s [54]. It should be noted that no studies have been found on the effect of caffeine on RJ 15 s in female volleyball players. Therefore, this is the first study that evaluates this parameter in women, even though it is of vital importance as previously explained. Besides, it has been observed that when evaluating this parameter there were improvements in the RSI and RJ min [54]. Furthermore, it has been observed that when evaluating this parameter there were improvements in the RSI and RJ min.
This is evidence that caffeine could produce a better resistance to fatigue in terms of repeated jumps. This phenomenon could be due to several physiological mechanisms. Firstly, caffeine has been reported to produce hypoalgesia, whereby the decrease in pain inhibits the perception of overexertion and fatigue [57]. Alternatively, there is stimulation of the CNS through inhibition of the adenosine antagonist receptor, as well as increased production of catecholamines, epinephrine and norepinephrine. Contradictorily, Karayigit et al. (2022) observed in women an increase in catecholamines after administration of 5.4 mg/kg body weight [58], but this was not reflected in the FI in repeated sprints, nor in peak power, which was the case in the present investigation. However, the aforementioned study found an improvement in the mean power output of repeated sprints compared to placebo. Another important aspect of caffeine is the increased production of lactate, which would aid the increased production of lactic anaerobic power [15,57,58,59]. Besides, caffeine enhances sodium potassium ATPase activity and intracellular calcium mobilization, indirectly affecting acetylcholine and dopamine release [57,58].
Caffeine attenuates the effects of fatigue by binding to adenosine receptors, reducing the RPE. However, the action of caffeine on the release and subsequent reuptake of calcium from the sarcoplasmic reticulum appears to be the reason for the attenuation of fatigue in short-duration, high-intensity tests [60] This could be the reason for the improvement of fatigue in the 505 test, CMJ, RSI and RJ minimum. This fact could also explain the improvement in perceived fatigue with caffeine in this study (F (1.7) = 7.29, p = 0.03, η2 = 0.51). Contradictorily, a recent meta-analysis [15] did not find an effect on RPE and agility. Similarly, a review conducted in football players also reported no statistical change in perceived fatigue in women [33]. A recent study reported an increased RPE with the administration of high doses of caffeine (>6mg/kg of) [55], while Del Coso et al. (2014) reported a lower RPE score (although not significant) in male volleyball players [4]. In addition, these authors documented a higher insomnia when caffeine was consumed, in contrast to the present study, which did not find a decrease in sleep. Filip-Stachnik (2022) assessed sleep by actigraphy after caffeine intake (3 mg/kg) prior to an evening training session and found no sleep disturbance [39] as in this study. In this sense, the results are contradictory, as other previous studies have found a decrease in sleep. Miller et al., (2014) showed a decrease in sleep efficiency in triathletes after administration of two doses of 3 mg/kg [61]. A subsequent study found similar results in 800 m athletes with the administration of 6 mg/kg caffeine [37]. It has been suggested that the differences found in the studies could be due to the difference in dose, due to a stimulation of catecholamines and a decrease in 6-sulphatoxymelatonin [39]. However, in the present study no differences were found after administration of 5 mg/kg.
Concerning muscle damage, a main effect of caffeine was found in relation to perceived muscle damage (F (1.7) = 7.29, p = 0.03, η2 = 0.51). Accordingly, it has been suggested that pre-exercise caffeine intake could improve perceived muscle damage [40]. In this regard, a meta-analysis revealed that caffeine decreased muscle damage after 48h post-exercise compared to placebo [62]. Thus, in this study, the participants trained on Tuesdays, Thursdays and Fridays, with the results coinciding with the aforementioned study. This could be since caffeine could improve peripheral neuromuscular transmission [63] Caffeine would delay the failure of postsynaptic transmission [64], as well as the decrease of membrane action potentials [65], and inhibition of the nervous system central on motor neurons [66].
This study has some limitations. Firstly, the number of the sample-size, although a sample calculation was previously carried out in a similar study. The power analysis conducted in the aforementioned study determined that a minimum sample size of 5 athletes was necessary [67]. Secondly, although the players were urged not to consume caffeine on measurement days, they were regular coffee drinkers, which could affect the results of the study. However, recent research found that regular caffeine consumption did not interfere with the potential of caffeine as an ergogenic aid in explosive exercise enhancement [68]. Similarly, a recent study reported that caffeine intake of 3-6 mg/kg improved 1RM in women habituated to caffeine ingestion [69]. Finally, the menstrual cycle of the women was not controlled. However, several studies reported that caffeine has ergogenic effect in all phases of the menstrual cycle [41,70,71].
5. Conclusions
It appears that administration of 5 mg/kg body weight increases CMJ, RSI and Handgrip in semi-professional female volleyball players over one week of training. Besides, it seems that caffeine supplementation enhances RSI and FI. Otherwise, this ergogenic aid improves the perception of fatigue. Further similar research is needed in women that collects both physical performance and well-being parameters and correlates these variables. Particularly in highly competitive periods such as the play-offs.
Author Contributions
Conceptualization, JS-C. and FTG.; methodology, JS-C and GD-G.; software, GD-G.; validation, AL-G., RG-P. and FS-M.; formal analysis, FTG.; investigation, JS-C, GD-G:FTG.; resources, FTG and JSC.; data curation, GD-G.; writing—original draft preparation, JS-C, FTG.; writing—review and editing, JS-C, FTG, GD-G and FS-M.; visualization, AL-G.; supervision, RG-P; project administration, JS-C and FTG.
Funding
This article was not received funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) Bioethics Committee of the University of Granada (registration number: 3014/CEIH/2022) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to thank the women's team ‘Voley CIDE Palma’ for their participation and availability for the realization of this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Verhagen, E.; Van der Beek, A.J.; Bouter, L.M.; Bahr, R.M.; Van Mechelen, W. A One Season Prospective Cohort Study of Volleyball Injuries. Br J Sports Med 2004, 38, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Bere, T.; Kruczynski, J.; Veintimilla, N.; Hamu, Y.; Bahr, R. Injury Risk Is Low among World-Class Volleyball Players: 4-Year Data from the FIVB Injury Surveillance System. Br J Sports Med 2015, 49, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Zbinden-Foncea, H.; Rada, I.; Gomez, J.; Kokaly, M.; Stellingwerff, T.; Deldicque, L.; Peñailillo, L. Effects of Caffeine on Countermovement-Jump Performance Variables in Elite Male Volleyball Players. Int J Sports Physiol Perform 2018, 13, 145–150. [Google Scholar] [CrossRef]
- Del Coso, J.; Pérez-López, A.; Abian-Vicen, J.; Salinero, J.J.; Lara, B.; Valadés, D. Enhancing Physical Performance in Male Volleyball Players with a Caffeine-Containing Energy Drink. Int J Sports Physiol Perform 2014, 9, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E. ISSN Exercise & Sports Nutrition Review Update: Research & Recommendations. J Int Soc Sports Nutr 2018, 15, 38. [Google Scholar] [PubMed]
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. Wake up and Smell the Coffee: Caffeine Supplementation and Exercise Performance—an Umbrella Review of 21 Published Meta-Analyses. Br J Sports Med 2020, 54, 681 LP–688. [Google Scholar] [CrossRef] [PubMed]
- Stadheim, H.K.; Spencer, M.; Olsen, R.; Jensen, J. Caffeine and Performance over Consecutive Days of Simulated Competition. 2015. [Google Scholar]
- Puente, C.; Abián-Vicén, J.; Salinero, J.J.; Lara, B.; Areces, F.; Del Coso, J. Caffeine Improves Basketball Performance in Experienced Basketball Players. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Grgic, J.; Trexler, E.T.; Lazinica, B.; Pedisic, Z. Effects of Caffeine Intake on Muscle Strength and Power: A Systematic Review and Meta-Analysis. J Int Soc Sports Nutr 2018, 15, 11. [Google Scholar] [CrossRef]
- Del Coso, J.; Muñoz, G.; Muñoz-Guerra, J. Prevalence of Caffeine Use in Elite Athletes Following Its Removal from the World Anti-Doping Agency List of Banned Substances. Applied Physiology, Nutrition, and Metabolism 2011, 36, 555–561. [Google Scholar] [CrossRef]
- Magkos, F.; Kavouras, S.A. Caffeine Use in Sports, Pharmacokinetics in Man, and Cellular Mechanisms of Action. Crit Rev Food Sci Nutr 2005, 45, 535–562. [Google Scholar] [CrossRef]
- Davis, J.M.; Zhao, Z.; Stock, H.S.; Mehl, K.A.; Buggy, J.; Hand, G.A. Central Nervous System Effects of Caffeine and Adenosine on Fatigue. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 2003. [Google Scholar] [CrossRef]
- Graham, T.E.; Spriet, L.L. Metabolic, Catecholamine, and Exercise Performance Responses to Various Doses of Caffeine. J Appl Physiol 1995, 78, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Perez-Lopez, A.; Salinero, J.J.; Abian-Vicen, J.; Valades, D.; Lara, B.; Hernandez, C.; Areces, F.; Gonzalez, C.; Del Coso, J. Caffeinated Energy Drinks Improve Volleyball Performance in Elite Female Players. Med Sci Sports Exerc 2015, 47, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Bruton, A.; Marin-Puyalto, J.; Muñiz-Pardos, B.; Matute-Llorente, A.; Del Coso, J.; Gomez-Cabello, A.; Vicente-Rodriguez, G.; Casajus, J.A.; Lozano-Berges, G. Does Acute Caffeine Supplementation Improve Physical Performance in Female Team-Sport Athletes? Evidence from a Systematic Review and Meta-Analysis. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Graham, T.E. Caffeine, Coffee and Ephedrine: Impact on Exercise Performance and Metabolism. Canadian journal of applied physiology 2001, 26, S186–S191. [Google Scholar] [CrossRef]
- Warren, G.L.; Park, N.D.; Maresca, R.D.; McKibans, K.I.; Millard-Stafford, M.L. Effect of Caffeine Ingestion on Muscular Strength and Endurance: A Meta-Analysis. Med Sci Sports Exerc 2010, 42, 1375–1387. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Del Coso, J. Ergogenic Effects of Acute Caffeine Intake on Muscular Endurance and Muscular Strength in Women: A Meta-Analysis. International Journal of Environmental Research and Public Health 2021, Vol. 18, Page 5773 2021, 18, 5773. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Afonso, J.; Costa, J.; Oliveira, R.; Pino-Ortega, J.; Rico-González, M. Relationships between Sleep, Athletic and Match Performance, Training Load, and Injuries: A Systematic Review of Soccer Players. In Proceedings of the Healthcare; MDPI, 2021; Vol. 9, p. 808.
- Coutts, A.J.; Reaburn, P. Monitoring Changes in Rugby League Players’ Perceived Stress and Recovery during Intensified Training. Percept Mot Skills 2008, 106, 904–916. [Google Scholar] [CrossRef] [PubMed]
- Kupperman, N.; Curtis, M.A.; Saliba, S.A.; Hertel, J. Quantification of Workload and Wellness Measures in a Women’s Collegiate Volleyball Season. Front Sports Act Living 2021, 3, 702419. [Google Scholar] [CrossRef] [PubMed]
- Saw, A.E.; Kellmann, M.; Main, L.C.; Gastin, P.B. Athlete Self-Report Measures in Research and Practice: Considerations for the Discerning Reader and Fastidious Practitioner. Int J Sports Physiol Perform 2017, 12, S2-127. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Marcora, S.M.; Coutts, A.J. Internal and External Training Load: 15 Years On. Int J Sports Physiol Perform 2019, 14, 270–273. [Google Scholar] [CrossRef]
- Cullen, B.D.; McCarren, A.L.; Malone, S. Ecological Validity of Self-Reported Wellness Measures to Assess Pre-Training and Pre-Competition Preparedness within Elite Gaelic Football. Sport Sci Health 2021, 17, 163–172. [Google Scholar] [CrossRef]
- Gastin, P.B.; Meyer, D.; Robinson, D. Perceptions of Wellness to Monitor Adaptive Responses to Training and Competition in Elite Australian Football. The Journal of Strength & Conditioning Research 2013, 27, 2518–2526. [Google Scholar] [CrossRef]
- Montgomery, P.G.; Hopkins, W.G. The Effects of Game and Training Loads on Perceptual Responses of Muscle Soreness in Australian Football. Int J Sports Physiol Perform 2013, 8, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Mendez-Villanueva, A.; Quod, M.; Quesnel, T.; Ahmaidi, S. Improving Acceleration and Repeated Sprint Ability in Well-Trained Adolescent Handball Players: Speed versus Sprint Interval Training. Int J Sports Physiol Perform 2010, 5, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Govus, A.D.; Coutts, A.; Duffield, R.; Murray, A.; Fullagar, H. Relationship between Pretraining Subjective Wellness Measures, Player Load, and Rating-of-Perceived-Exertion Training Load in American College Football. Int J Sports Physiol Perform 2018, 13, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Moalla, W.; Fessi, M.S.; Farhat, F.; Nouira, S.; Wong, D.P.; Dupont, G. Relationship between Daily Training Load and Psychometric Status of Professional Soccer Players. Research in Sports Medicine 2016, 24, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Chen, Y.-C.; Tung, K.; Chao, H.-H.; Wang, H.-S. Effects of Caffeine and Sex on Muscle Performance and Delayed-Onset Muscle Soreness after Exercise-Induced Muscle Damage: A Double-Blind Randomized Trial. J Appl Physiol 2019, 127, 798–805. [Google Scholar] [CrossRef]
- Doherty, M.; Smith, P.M. Effects of Caffeine Ingestion on Rating of Perceived Exertion during and after Exercise: A Meta-analysis. Scand J Med Sci Sports 2005, 15, 69–78. [Google Scholar] [CrossRef]
- Doherty, M.; Smith, P.M. Effects of Caffeine Ingestion on Exercise Testing: A Meta-Analysis. Int J Sport Nutr Exerc Metab 2004, 14, 626–646. [Google Scholar] [CrossRef]
- Mielgo-Ayuso, J.; Calleja-Gonzalez, J.; Del Coso, J.; Urdampilleta, A.; León-Guereño, P.; Fernández-Lázaro, D. Caffeine Supplementation and Physical Performance, Muscle Damage and Perception of Fatigue in Soccer Players: A Systematic Review. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Wang, H.-S.; Tung, K.; Chao, H.-H. Effects of Gender Difference and Caffeine Supplementation on Anaerobic Muscle Performance. Int J Sports Med 2015, 36, 974–978. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J. A Review of Nutritional Intervention on Delayed Onset Muscle Soreness. Part I. J Exerc Rehabil 2014, 10, 349. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.W.; Housh, T.J.; Schmidt, R.J.; Johnson, G.O.; Housh, D.J.; Coburn, J.W.; Malek, M.H. The Acute Effects of a Caffeine-Containing Supplement on Strength, Muscular Endurance, and Anaerobic Capabilities. The Journal of Strength & Conditioning Research 2006, 20, 506–510. [Google Scholar]
- Ramos-Campo, D.J.; Pérez, A.; Ávila-Gandía, V.; Pérez-Piñero, S.; Rubio-Arias, J.Á. Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, J.H.; Kim, I.S.; Jang, K.H.; Duffy, J.F. Self-Reported Sleep Duration, Daytime Sleepiness, and Caffeine Use in Male and Female Morning and Evening Types. Sleep Med Res 2012, 3, 32–38. [Google Scholar] [CrossRef]
- Filip-Stachnik, A. Does Acute Caffeine Intake before Evening Training Sessions Impact Sleep Quality and Recovery-Stress State? Preliminary Results from a Study on Highly Trained Judo Athletes. Applied Sciences 2022, 12. [Google Scholar] [CrossRef]
- Tallis, J.; Guimaraes-Ferreira, L.; Clarke, N.D. Not Another Caffeine Effect on Sports Performance Study—Nothing New or More to Do? Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Giráldez-Costas, V.; Del Coso, J.; Mañas, A.; Salinero, J.J. The Long Way to Establish the Ergogenic Effect of Caffeine on Strength Performance: An Overview Review. Nutrients 2023, 15, 1178. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.L.; Mackinnon, L.T. Monitoring Overtraining in Athletes. Sports medicine 1995, 20, 321–327. [Google Scholar] [CrossRef]
- González-Fernández, F.T.; Rico-González, M.; Siquier-Coll, J.; Falces-Prieto, M.; Clemente, F.M. Wellness Reports in Young Soccer Players: A within and between-Weeks Analysis. Journal of Physical Education and Sport 2022, 22, 1685–1693. [Google Scholar] [CrossRef]
- Dal Pupo, J.; Gheller, R.G.; Dias, J.A.; Rodacki, A.L.F.; Moro, A.R.P.; Santos, S.G. Reliability and Validity of the 30-s Continuous Jump Test for Anaerobic Fitness Evaluation. J Sci Med Sport 2014, 17, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, E.P.; Comyns, T.M. The Use of Contact Time and the Reactive Strength Index to Optimize Fast Stretch-Shortening Cycle Training. Strength Cond J 2008, 30, 32–38. [Google Scholar] [CrossRef]
- Mitsionis, G.; Pakos, E.E.; Stafilas, K.S.; Paschos, N.; Papakostas, T.; Beris, A.E. Normative Data on Hand Grip Strength in a Greek Adult Population. Int Orthop 2009, 33, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.G.; Pearn, J.; Barnes, A.; Young, C.M.; Kehoe, M.; Newman, J. Norms for Hand Grip Strength. Arch Dis Child 1984, 59, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Draper, J.A. The 505 Test: A Test for Agility in Horizontal Plane. Aust J Sci Med Sport 1985, 17, 15–18. [Google Scholar]
- Sánchez-Pay, A.; Martínez-Gallego, R.; Crespo, M.; Sanz-Rivas, D. Key Physical Factors in the Serve Velocity of Male Professional Wheelchair Tennis Players. Int J Environ Res Public Health 2021, 18, 1944. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Mohr, M.; Amstrup, T.; Rysgaard, T.; Johansen, J.; Steensberg, A.; Pedersen, P.K.; Bangsbo, J. The Yo-Yo Intermittent Recovery Test: Physiological Response, Reliability, and Validity. Med Sci Sports Exerc 2003, 35, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, B.; Pfeifer, C.; Kreitz, K.; Borowski, M.; Faldum, A.; Brand, S.-M. The Yo-Yo Intermittent Tests: A Systematic Review and Structured Compendium of Test Results. Front Physiol 2018, 9, 870. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences and Eii 1988.
- Sawilowsky, S.S. New Effect Size Rules of Thumb. Journal of modern applied statistical methods 2009, 8, 26. [Google Scholar] [CrossRef]
- Ribeiro, B.G.; Morales, A.P.; Sampaio-Jorge, F.; Barth, T.; de Oliveira, M.B.C.; Coelho, G.M.; Leite, T.C. Caffeine Attenuates Decreases in Leg Power without Increased Muscle Damage. J Strength Cond Res 2016, 30, 2354–2360. [Google Scholar] [CrossRef]
- Ferreira, L.H.B.; Forbes, S.C.; Barros, M.P.; Smolarek, A.C.; Enes, A.; Lancha-Junior, A.H.; Martins, G.L.; Souza-Junior, T.P. High Doses of Caffeine Increase Muscle Strength and Calcium Release in the Plasma of Recreationally Trained Men. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Behrens, M.; Mau-Moeller, A.; Weippert, M.; Fuhrmann, J.; Wegner, K.; Skripitz, R.; Bader, R.; Bruhn, S. Caffeine-Induced Increase in Voluntary Activation and Strength of the Quadriceps Muscle during Isometric, Concentric and Eccentric Contractions. Sci Rep 2015, 5, 10209. [Google Scholar] [CrossRef] [PubMed]
- Hussain, N. The Effect of Caffeine on Athletic Performance. ScienceOpen Preprints 2021. [Google Scholar] [CrossRef]
- Karayigit, R.; Forbes, S.C.; Osmanov, Z.; Yilmaz, C.; Yasli, B.C.; Naderi, A.; Buyukcelebi, H.; Benesova, D.; Gabrys, T.; Esen, O. Low and Moderate Doses of Caffeinated Coffee Improve Repeated Sprint Performance in Female Team Sport Athletes. Biology (Basel) 2022, 11, 1498. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.C.; Jesus, A.A.; Giglio, B.M.; Marini, A.C.; Lobo, P.C.B.; Mota, J.F.; Pimentel, G.D. Acute Caffeinated Coffee Consumption Does Not Improve Time Trial Performance in an 800-m Run: A Randomized, Double-Blind, Crossover, Placebo-Controlled Study. Nutrients 2018, 10, 657. [Google Scholar] [CrossRef] [PubMed]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A Review of Caffeine’s Effects on Cognitive, Physical and Occupational Performance. Neurosci Biobehav Rev 2016, 71, 294–312. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.; O’Connor, H.; Orr, R.; Ruell, P.; Cheng, H.L.; Chow, C.M. Combined Caffeine and Carbohydrate Ingestion: Effects on Nocturnal Sleep and Exercise Performance in Athletes. Eur J Appl Physiol 2014, 114, 2529–2537. [Google Scholar] [CrossRef] [PubMed]
- Muljadi, J.A.; Kaewphongsri, P.; Chaijenkij, K.; Kongtharvonskul, J. Effect of Caffeine on Delayed-Onset Muscle Soreness: A Meta-Analysis of RCT. Bull Natl Res Cent 2021, 45, 197. [Google Scholar] [CrossRef]
- Mesquita, R.N.O.; Cronin, N.J.; Kyröläinen, H.; Hintikka, J.; Avela, J. Effects of Caffeine on Neuromuscular Function in a Non-Fatigued State and during Fatiguing Exercise. Exp Physiol 2020, 105, 690–706. [Google Scholar] [CrossRef]
- Adelman, W.J.; Palti, Y.; Senft, J.P. Potassium Ion Accumulation in a Periaxonal Space and Its Effect on the Measurement of Membrane Potassium Ion Conductance. J Membr Biol 1973, 13, 387–410. [Google Scholar] [CrossRef]
- Rybicki, K.J.; Waldrop, T.G.; Kaufman, M.P. Increasing Gracilis Muscle Interstitial Potassium Concentrations Stimulate Group III and IV Afferents. J Appl Physiol 1985, 58, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.L.; Amann, M.; Duchateau, J.; Meeusen, R.; Rice, C.L. Neural Contributions to Muscle Fatigue: From the Brain to the Muscle and Back Again. Med Sci Sports Exerc 2016, 48, 2294–2306. [Google Scholar] [CrossRef] [PubMed]
- Filip-Stachnik, A.; Kaszuba, M.; Dorozynski, B.; Komarek, Z.; Gawel, D.; Del Coso, J.; Klocek, T.; Spieszny, M.; Krzysztofik, M. Acute Effects of Caffeinated Chewing Gum on Volleyball Performance in High-Performance Female Players. J Hum Kinet 2022, 84, 92–102. [Google Scholar] [CrossRef] [PubMed]
- de Salles Painelli, V.; Teixeira, E.L.; Tardone, B.; Moreno, M.; Morandini, J.; Larrain, V.H.; Pires, F.O. Habitual Caffeine Consumption Does Not Interfere With the Acute Caffeine Supplementation Effects on Strength Endurance and Jumping Performance in Trained Individuals. Int J Sport Nutr Exerc Metab 2021, 31, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Filip-Stachnik, A.; Wilk, M.; Krzysztofik, M.; Lulińska, E.; Tufano, J.J.; Zajac, A.; Stastny, P.; Del Coso, J. The Effects of Different Doses of Caffeine on Maximal Strength and Strength-endurance in Women Habituated to Caffeine. J Int Soc Sports Nutr 2021, 18, 25. [Google Scholar] [CrossRef]
- Lara, B.; Gutiérrez-Hellín, J.; García-Bataller, A.; Rodríguez-Fernández, P.; Romero-Moraleda, B.; Del Coso, J. Ergogenic Effects of Caffeine on Peak Aerobic Cycling Power during the Menstrual Cycle. Eur J Nutr 2020, 59, 2525–2534. [Google Scholar] [CrossRef]
- Romero-Moraleda, B.; Del Coso, J.; Gutiérrez-Hellín, J.; Lara, B. The Effect of Caffeine on the Velocity of Half-Squat Exercise during the Menstrual Cycle: A Randomized Controlled Trial. Nutrients 2019, 11. [Google Scholar] [CrossRef]
Figure 2.
Set up for the 505 COD test.
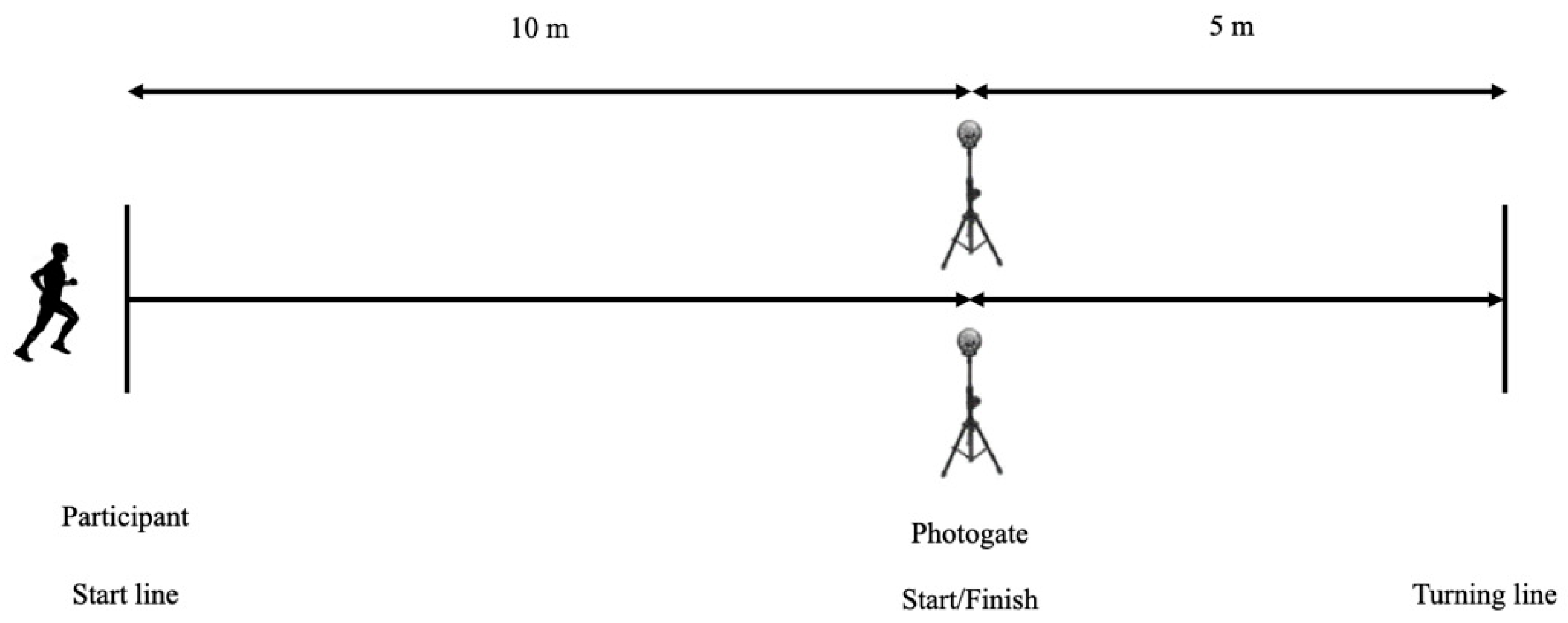
Table 1.
Characteristics of the participants.
| Heigth (m) | 1,63±0,08 |
| Weigth (kg) | 66,67±4,74 |
| Fat mass (%) | 22,32±2,5 |
| Muscle mass (kg) | 50,26±3,56 |
| Bone mass (kg) | 2,7±0,18 |
| BMI | 19,3±1,45 |
| Body Water (%) | 57,37±1,58 |
| VO2max (ml/kg/min) | 41,77±1,67 |
Table 4.
Values of regression analysis explaining the relevance of different internal intensity variables.
Table 4.
Values of regression analysis explaining the relevance of different internal intensity variables.
| R | R2 | Adjusted R2 | F | P | SE | ||
|---|---|---|---|---|---|---|---|
| P Stress | P RJ min jump | -.0.75 | .57 | .51 | 9.59 | .017 | 2.59 |
| P Sleep | S RJ time | .72 | 52 | .45 | 7.62 | 0.28 | 0.36 |
*Significance at p < 0.05. **Significance at p < 0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



