
Submitted:
05 December 2023
Posted:
06 December 2023
You are already at the latest version
Abstract
Patients with schizophrenia had higher mortality risks and the role of antipsychotic medications remained inconclusive. In an aging society, elderly schizophrenia patients warrant increased attention. In this study, we aimed to explore medication dosage associations with mortality in schizophrenia patients, using Taiwan's national healthcare database from 2010 to 2014, with 102,964 patients with schizophrenia, and a subgroup of 6,433 elderly patients, compared to an age- and gender-matched control group. The findings revealed that schizophrenia patients with no antipsychotic exposure had the highest mortality risk as compared to the control sample—with a 3.61 and 3.37-fold risk for overall and cardiovascular mortality respectively in age and gender-adjusted model, followed by high, low, and moderate exposure groups. A similar pattern was observed in elderly schizophrenia patients but high exposure to antipsychotics was associated with the highest risk in both overall and cardiovascular mortality in elderly patients, with a 3.01, and 2.95-fold risk), respectively. In conclusion, the use of antipsychotics is beneficial to patients with schizophrenia, with recommended exposure levels being low to moderate. In elderly patients, high antipsychotic exposure was associated with the highest mortality risk. We should pay more attention to antipsychotic dosage in elderly schizophrenia patients.
Keywords:
antipsychotic
; mortality
; schizophrenia
; elderly
; daily defined dosage
1. Introduction
In comparison with the general population, mortality is substantially higher for individuals with schizophrenia [1,2,3]. In Taiwan, people with schizophrenia have about 15 years shorter life expectancy at birth than the general population [4], which is consistent with the existing literature [5,6]. Beyond a fairly high risk of death from unnatural causes, around three-fourths of all deaths in people with serious mental illnesses were reported to be certified as natural [1], stressing the potential relevance of sedentary lifestyles, obesity, inadequate access to health services, and adverse effects of medications [7,8,9,10], to the excess mortality.
It is speculated that excess mortality in schizophrenia may be attributable to adverse effects of antipsychotic medications including weight gain, metabolic syndrome, diabetes, and ischemic heart disease [11,12]. Several pharmaco-epidemiological studies reported a dose-related risk of sudden cardiac death among people using antipsychotic medications [13]. However, prior studies using large, and prospectively collected datasets of actual filled prescriptions, to calculate the risk of death associated with any, current, or cumulative antipsychotic exposure in schizophrenia patients have suggested that the use of an antipsychotic is associated with lower mortality than no use of an antipsychotic [5,14,15,16]. Furthermore, prior findings suggested a U-shaped curve between antipsychotic exposure and overall mortality, revealing that low and moderate antipsychotic exposure was associated with a substantially lower risk of death than either no use or high exposure [17,18]. To date, there is still a lack of evidence regarding the associations between mortality and antipsychotic exposure levels as compared to a control sample without psychiatric diagnoses when simultaneously considering socioeconomic covariates and comorbid physical conditions.
With the advancement of healthcare services, the average life expectancy has been gradually increasing. In many developed countries, individuals aged 55 years and older will soon account for a quarter or more of the population with schizophrenia [19]. Whiteford et al. reported that schizophrenia currently ranks third in causes of disability-adjusted life years for people aged 60 years and older among mental disorders and substance use disorders [20]. Besides, elderly patients with schizophrenia have a high prevalence of comorbid medical conditions [21], which may affect both the use of psychotropic medications and mortality. To date, research on elderly people with schizophrenia has been relatively scarce, accounting for approximately 1% of the schizophrenia literature [22]. Among the existing literature, the associations between exposure dosages to psychotropic medications and mortality in this geriatric population have remained under-researched.
The current study aimed to investigate the possible associations between the degree of cumulative antipsychotic exposure, indicated by filled prescriptions, and mortality, in a national cohort of patients with schizophrenia, as compared with a control group from the general population. Besides, this study examined the relationship between mortality and cumulative dosing of antipsychotics in a subgroup of elderly individuals with schizophrenia.
2. Results
Demographic and clinical characteristics are shown in Table 1. In total, 102,964 patients with schizophrenia were enrolled. The mean age of the schizophrenia cohort is 44.8 years (SD=13.2) and 47.4% of them are females. The mean age of 6,433 elderly patients with schizophrenia is 73.6 years (SD=6.7) and 59.7% of them are females. Compared to the corresponding control sample, patients with schizophrenia have higher proportions of chronic obstructive pulmonary disease (COPD), cardiovascular disease (CVD), diabetes mellitus (DM), and renal disease (RD); meanwhile, only higher proportions of COPD and CVD were noted for elderly patients in comparison with the corresponding control sample. With regards to deaths, 7,730 schizophrenia patients (7.5%) died during the five-year follow-up period. The corresponding figure among control subjects was 2,593 (2.5%). The proportion of deaths in elderly patients (31.9%) with schizophrenia is around 2 times relative to the corresponding control sample during the five-year follow-up period.
Of all patients with schizophrenia, 8,733 individuals (8.5%) had no antipsychotic exposure during the follow-up period whereas 19,017 individuals (18.5%) had high antipsychotic exposure (Table 2). Among the 6433 elderly patients with schizophrenia, 944 individuals (14.7%) had no antipsychotic treatment during the follow-up period whereas 3520 individuals (54.7%) had low antipsychotic exposure and 333 individuals (5.2%) had high antipsychotic exposure, respectively.
The demographic-adjusted model (model 1) and the fully adjusted model (model 2) were revealed in Table 2 and Table 3, respectively. Patients with schizophrenia who had no exposure to antipsychotics, compared with the control sample, had a 3.61-fold (model 1) and 2.89-fold (model 2) risk in overall mortality; for CVD-related mortality, the figures were 3.37- (model 1), and 2.96- (model 2), respectively. In the demographic-adjusted model and fully adjusted model, the results for antipsychotics had U-shaped curves in both overall mortality risk and CVD-related mortality risk (Table 2 and Table 3; Figure 1 and Figure 2). The highest overall mortality was observed among schizophrenia patients with no antipsychotic exposure (model 1: HR =3.61, 95% CI: 3.35-3.89; model 2: HR =2.89, 95% CI: 2.65-3.14), followed by high exposure group, low exposure group, and moderate exposure group. As for CVD-related mortality, no exposure group had the highest CVD-related mortality risk (model 1: HR=3.37, CI: 2.82-4.04; model 2: HR =2.96, 95% CI: 2.40-3.64), followed by high exposure group, low exposure group, and moderate exposure group.
With regards to elderly patients with schizophrenia, as compared with the control sample, a U-shaped association was also observed for both overall mortality and CVD-related mortality (Table 2 and Table 3; Figure 1 and Figure 2). The highest overall mortality was observed among elderly schizophrenia patients with high antipsychotic exposure (model 1: HR =3.01, 95% CI: 2.45–3.70; model 2: HR =2.69, 95% CI: 2.17–3.34), followed by no exposure group, low exposure group, and moderate exposure group. As for CVD-related mortality, a similar pattern was found as well. Elderly patients with schizophrenia using high-exposure antipsychotics had the highest CVD-related mortality risk (model 1: HR=2.95, CI: 1.87-4.67; model 2: HR =2.78, 95% CI: 1.72-4.50), followed by no exposure group, low exposure group, and moderate exposure group.
3. Discussion
In our study, we investigated how cumulative exposure to antipsychotics affects the excess mortality in schizophrenia as compared to an age- and gender-matched control sample. With a special focus on elderly patients with schizophrenia, we also analyzed such associations with a subgroup of elderly patients with schizophrenia. The results showed a U-shaped curve for both overall mortality and CVD-related mortality in patients with schizophrenia when exposure dosages increased; the highest risk of death was found for patients with no antipsychotic exposure, and the lowest risk of death for those with low to moderate antipsychotic exposure. With regards to elderly individuals with schizophrenia, a U-shaped association was also observed for overall and CVD-related mortality; however, high antipsychotic exposure was associated with the highest risk in both overall and CVD-related mortality. These findings showed the importance of using an adequate dosage of antipsychotic medications for patients with schizophrenia, particularly for elderly patients. The association between a high dosage of antipsychotics and an increased risk of mortality for elderly patients has been identified, which reminds clinicians to heighten vigilance when adjusting the dosage of antipsychotics for elderly patients.
In the comparisons between patients with no antipsychotic exposure and the control group, we found that the age and gender-adjusted (model 1) hazard ratio was 3.61 and the fully-adjusted (model 2) hazard ratio was 2.89 in overall mortality: in CVD-related mortality, age, and gender-adjusted (model 1) hazard ratio was 3.37, and fully-adjusted (model 2) hazard ratio was 2.96, respectively. Poor socioeconomic status was a barrier to reducing the mortality gap in patients with schizophrenia [23]. Previous studies also showed that patients with schizophrenia had a higher prevalence of comorbid physical conditions such as diabetes, COPD, and CVD compared to people without schizophrenia [16,24,25,26]. It has been speculated that the elevated mortality in schizophrenia was primarily attributed to these comorbidities, especially CVD [26], and if undetected or inadequately treated, comorbid physical illnesses may lead to increased mortality risk in patients with schizophrenia [8,16]. In the present study, we found that schizophrenia patients with no antipsychotic exposure had an around 3- fold risk of overall and CVD-related mortality as compared to the control group even after controlling for socioeconomic variables and comorbid physical illnesses (model 2). Similarly, a systematic review including 135 studies spanning from 1957 to 2021, showed a 2.9-fold increased all-cause mortality in patients with schizophrenia versus the general population and 1.6-fold increased risk versus physical disease-matched general population controls [27]. Beyond the influences of antipsychotics, it seems likely that schizophrenia per se may be independently associated with an elevated overall and CVD-related mortality as presented in the current findings for patients with no antipsychotic exposure. For instance, lack of insight is considered a symptom of schizophrenia [28]. The WHO ten-country study on schizophrenia revealed that 98% of patients with schizophrenia exhibited a lack of insight, making it the most prevalent symptom [29]. Lack of insight is the main cause of treatment nonadherence [30]. Besides, there are some interconnected factors in schizophrenia that synergistically contribute to physical morbidity and subsequent mortality in patients. Smoking, in previous research, had been found that approximately 70-80% of patients with schizophrenia were smokers and consumed higher quantities of cigarettes compared to smokers without schizophrenia [31,32]. Life expectancy for smokers is at least 10 years shorter than for nonsmokers [33,34] and smoking has long been causally associated with mortality in various CVD [35,36]. Moreover, the elevated mortality risk in patients with schizophrenia may be linked to the associated societal factors and the characteristics of the healthcare system [37]. Some evidence revealed that patients with schizophrenia having physical comorbidities may not accept appropriate medical care. A Danish study reported that patients with schizophrenia and had heart failure received lower-quality care, deviating from guidelines, compared to non-schizophrenic heart failure patients. Notably, inadequate psychosocial functioning in schizophrenia patients predicted suboptimal heart failure care, leading to a substantially higher one-year mortality risk [38]. Not only accept improper medical care but patients with schizophrenia are also faced with discrimination or have some kind of stigma that may negatively affect their health. A prior cross-sectional survey across 27 countries revealed that over 17% of patients with schizophrenia encountered discrimination while receiving treatment for physical health issues. The perception of discrimination might lead patients with schizophrenia to avoid seeking medical services, thereby contributing to less favorable outcomes in addressing their physical health issues [39]. Therefore, it was crucial for clinicians to adequately address the aforementioned habits and behaviors associated with patients with schizophrenia, and the relevant social-environmental factors.
In the present study, an increase in the level of antipsychotic exposure displayed a U-shaped curve for both overall and CVD-related mortality in patients with schizophrenia, revealing the highest risk of death among patients with no antipsychotic exposure. In a Finnish study with over 60000 patients treated for schizophrenia in inpatient settings with up to 20 years of follow-up, any antipsychotic use compared with non-use was associated with decreased all-cause mortality (HR= 0.48) [40]. Crump et al. revealed that lack of antipsychotic treatment was associated with elevated mortality [16]. However, both studies compared the usage of antipsychotic medications to non-usage without addressing the issue of different dosages within the antipsychotic medication. Our results were comparable to a prior study showing a U-shaped curve for overall mortality by different levels of cumulative antipsychotic exposure [18]; however, the above-mentioned study did not concurrently account for the impact of socioeconomic factors on mortality, and the potential high comorbidity of physical illnesses that patients with schizophrenia might possess. Besides overall mortality, we found a similar U-shaped pattern for CVD-related mortality in the present study. A 24-year national register study in Sweden revealed that CVD emerged as the leading cause of mortality among patients diagnosed with schizophrenia. In addition, patients with schizophrenia experienced CVD-related mortality that occurred ten- years earlier compared to the general population [41]. In contrast to the general population, individuals with schizophrenia exhibited elevated and earlier CVD-related mortality. This disparity can be attributed to multiple factors, encompassing patients’ comorbidities, harmful health-related behaviors, social factors such as stigma, insufficient preventive interventions, limited health literacy, suboptimal adherence to essential management, barriers to healthcare access, and a propensity for suboptimal care acceptance [42,43]. Antipsychotic medications, as the primary pharmacotherapy for treating schizophrenia, were extensively studied for their efficacy in addressing both psychiatric symptoms and potential cardiovascular complications. Existing literature showed that antipsychotics, regardless of first- or second-generation antipsychotics, had risks of metabolic and cardiovascular side effects [44,45,46]. In Ray’s research, antipsychotics were shown to have a dose-related increase in the risk of sudden cardiac death [13]. Therefore, the use of antipsychotic medications warranted particular attention to the risks of CVD and associated mortality. However, based on previous research, especially clinical database studies, the risk of CVD-related mortality may not exhibit a positive correlation with the use of antipsychotic medications. For example, in Torniainen et al. research, the cumulative antipsychotic exposure revealed a U-shaped curve for CVD-related mortality [18], which is comparable to the current findings. These findings collectively reminded us of the importance of the adequate dosage of antipsychotic use that prescribing antipsychotic medications needed to achieve a balance between effective therapeutic dosages, improvement in patient’s quality of life, and the management of side effects.
In the present study, we found that compared with the corresponding control group, elderly patients with schizophrenia who had no antipsychotic exposure had a 2.79-fold (model 1) and 2.51-fold risk (model 2) in overall mortality, respectively. As for CVD-related mortality, elderly patients with schizophrenia had a 2.54-fold (model 1) and 2.39-fold risk (model 2), respectively. Existing literature showed that the elevated mortality among patients with schizophrenia persisted into old age, but the mortality gap was smaller compared to the younger age groups [47,48]. A survivor effect might explain these findings, indicating that those patients who were still alive during the study period might be healthier than those who had died. Although the mortality gap in elderly patients with schizophrenia compared to the control group was smaller than that observed in younger patients with schizophrenia, the health status deserved greater attention in elderly patients with schizophrenia. For example, previous research had indicated that a higher proportion of elderly patients with schizophrenia, compared to the control group, received less adequate treatment for physical comorbidities [49,50]. The consequences of inadequate treatment may result in compromised health, and diminished quality of life for elderly patients with schizophrenia, and concurrently contributed to an increased both medical and societal burden. As the population ages, it is crucial to pay more attention to the vulnerability of these elderly patients with schizophrenia and ensure they receive adequate treatment for physical comorbidities.
In the present study, we found that elderly patients with schizophrenia had the highest risk of overall mortality and CVD-related mortality in the high antipsychotic exposure group. The side effects of antipsychotics which can affect any patient population, may be particularly obvious for elderly patients. The age-related changes can amplify the side effects of antipsychotic medications [51]. For instance, age-related changes in hepatic and renal functions markedly affect the absorption, distribution, metabolism, and excretion of the drugs. Liver mass, hepatic blood flow, serum albumin levels, and both renal blood flow and function tended to decrease with advancing age [52]. Additionally, age-related alterations in body composition also influenced the pharmacokinetics of antipsychotic medications for elderly patients. These changes involved a reduction in lean muscle mass and total body water, accompanied by an increase in total body fat [51]. Moreover, for elderly patients, due to the age-related increase in monoamine oxidase activity, the central nervous system exhibited heightened sensitivity to antipsychotic drugs. Additionally, there was a reduction in cerebral blood flow and a selective decline in some nerve pathways for the elderly. The age-related loss of cholinergic neurons and the exacerbation of cholinergic deficit by these drugs further increased the sensitivity of elderly patients to medications with anticholinergic effects [52]. Elderly schizophrenia patients may have comorbid chronic diseases like CVD or diabetes and antipsychotic use may lead to difficulties in the management of these chronic diseases [51]. One previous study revealed that both first- and second-generation antipsychotic medications are related to an increase in the risk of death among elderly persons [53] and dosage may be a key determinant of antipsychotic safety which affects the mortality risk [54]. In sum, the use of low or moderate dosage may be adequate in the treatment of elderly patients with schizophrenia. With advancing age and changes in physical health conditions, clinicians need to adjust the dosage of antipsychotic medications appropriately. For elderly patients with schizophrenia, high exposure to antipsychotic medications is not generally recommended. If the necessity arises for high-dose antipsychotic medication, close monitoring of associated side effects and potential risk factors is important. Regular surveillance along with adjustments in dosage as required, should be conducted.
The strengths of this study included nationwide coverage, encompassing all patients diagnosed with schizophrenia in all clinical settings, and comparisons with a control sample without psychiatric diagnoses. However, this study had several limitations. Due to its non-randomized study design, we needed to be cautious when interpreting the results due to potential selection bias. Additionally, the lack of accurate information on disease severity and patient lifestyles in the NHIRD restricted the assessment of these factors, and these factors could potentially influence mortality.
4. Materials and Methods
4.1. Settings
This research project was approved by the Research Ethics Review Committee of Far Eastern Memorial Hospital of Taiwan (109150-E). There are approximately 23 million population in Taiwan. National Health Insurance in Taiwan is a single-payer compulsory social insurance system for health services, which centralizes the disbursement and ensures identical access to healthcare for every Taiwanese citizen and legally hired foreigner who works in Taiwan. The National Health Insurance Research Database (NHIRD) consists of full records of health service utilization for almost the whole Taiwanese population, including information about their demographics, procedures, and medication, attached with corresponding medical service expenditures. Until 2016, the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) was used [55].
4.2. Study Population
The cohort participants with schizophrenia were identified in Taiwan’s NHIRD, provided by the Health and Welfare Data Science Center of Ministry of Health and Welfare in Taiwan. Individuals aged ≥ 15 years and diagnosed with schizophrenia (ICD-9-CM codes: 295) in 2010 were identified and followed up for consecutive five years (2010–2014) as the observation window. The cohort comprised both incident and existing cases with schizophrenia. This study further identified one subgroup of elderly patients with schizophrenia who were aged ≥ 65 years old on the index date. The mortality in patients with schizophrenia was compared with that of a control sample. The control sample was randomly selected from the database of the Registry for Beneficiaries of NHIRD and was age and sex-matched to the cohort participants with schizophrenia. We prioritized the selection of individuals without diagnoses of psychiatric disorders (ICD-9-CM codes: 290-319) from the registry and then considered gender matching. In terms of age matching, the matched control sample was randomly selected based on 10-year age intervals (15–20, 21–30, 31-40, 41-50, 51-60…, 91-100, and >100 years). The control sample for elderly patients with schizophrenia was drawn from the whole control sample according to age ≥ 65 years old. We identified the causes of death through linkage to Taiwan’s national mortality registry. In addition to overall mortality, deaths due to cardiovascular diseases (CVD) (ICD codes I00-I99), were also investigated.
4.3. Covariates
The data on age, sex, socioeconomic variables, possession of a catastrophic illness certification, and diagnoses of physical illnesses were extracted for both patients with schizophrenia and the control sample. Specifically, the socioeconomic variables were whether the individual belonged to a low-income household, the urbanization level of their residence, and their insurance premium level (dependent on the monthly income of the insured). Covariates regarding physical illnesses included diagnoses of COPD, CVD, cancer, DM, and RD. Additionally, for patients with schizophrenia, we extracted treatment-related data including psychiatric and nonpsychiatric health-care costs, psychiatric ward admission records, and dosage information for psychotropic medications. The mean defined daily dose (DDD) is defined as the recommended average daily maintenance dose of a drug used for its main indication in adults; the DDD guidelines of the World Health Organization were referenced in the present study [56]. We calculated the mean DDD of antipsychotics by dividing the cumulative dosage by the number of follow-up days. Subsequently, we categorized each medication into four groups: no exposure, low exposure (< 0.5 DDD), moderate exposure (0.5–1.5 DDD), and high exposure (> 1.5 DDD).
4.4. Statistical Analyses
In the preliminary comparisons, demographic and socioeconomic characteristics were described and compared between the cohort participants with schizophrenia and the control group. Those characteristics were also described and compared between elderly patients with schizophrenia and the corresponding control group. Categorical variables were analyzed with chi-squared tests and continuous variables with F-tests. A Cox regression analysis was used to compare overall mortality and CVD-related mortality among different DDD groups, in comparison with the control sample. Two regression models were used. The first model comprised only age and gender as covariates (demographic adjusted model) and the second model included covariates of gender, age, possession of catastrophic illness certification, socioeconomic variables including insurance premium level and lower-income household, and presence of comorbid physical illnesses including COPD, CVD, cancer, DM and RD (fully adjusted model). Hazard ratios (HRs) for overall mortality were calculated in groups according to different degrees of exposure to antipsychotics (no exposure, low exposure [< 0.5 DDD], moderate exposure [0.5–1.5 DDD], and high exposure [> 1.5 DDD]). HRs for CVD-related mortality were also calculated in groups based on different degrees of exposure to antipsychotics. Statistical significance was set at p < .05. All statistical analyses were performed using SPSS version 21.0 (IBM, Armonk, NY, USA).
5. Conclusions
We observed that although elevated mortality in patients with schizophrenia was partly attributed to comorbidities, schizophrenia was independently associated with an increase in overall and cardiovascular mortality. The use of antipsychotics was beneficial to patients with schizophrenia whenever indicated, with the most recommended dosage ranging from low to moderate exposure. In elderly patients with schizophrenia, a U-shaped association was observed for overall and CVD-related mortality but the high-exposure group was associated with the highest risk in both overall and CVD-related mortality. Future research is warranted to further examine the underlying mechanisms for such associations between antipsychotic dosage and mortality in different age groups of schizophrenia patients.
Author Contributions
Conceptualization, L.Y., W.L. and K.K.; methodology, Y.P.; software, L.Y.; formal analysis, L.Y.; resources, Y.P.; data curation, L.Y.; writing—original draft preparation, L.Y. and W.L.; writing—review and editing, K.K. and Y.P.; supervision, Y.P.; funding acquisition, Y.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by grants from the Ministry of Science and Technology (MOST 109-2314-B-418-010; and MOST 110-2314-B-418-004) and Far Eastern Memorial Hospital, Taiwan (FEMH-2019-C-012; FEMH-2020-C-020; FEMH-2021-C-024; and FEMH-2022-C-075).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Review Committee of Far Eastern Memorial Hospital of Taiwan (109150-E).
Informed Consent Statement
Patient consent was waived due to the de-identified nature of the data.
Data Availability Statement
There are ethical or legal restrictions on sharing the de-identified dataset, required by the research ethics review committee.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hoang, U.; Stewart, R.; Goldacre, M.J. Mortality after hospital discharge for people with schizophrenia or bipolar disorder: retrospective study of linked English hospital episode statistics, 1999-2006. BMJ 2011, 343, d5422–d5422. [Google Scholar] [CrossRef] [PubMed]
- Wahlbeck, K.; Westman, J.; Nordentoft, M.; Gissler, M.; Laursen, T.M. Outcomes of Nordic mental health systems: life expectancy of patients with mental disorders. Br. J. Psychiatry 2011, 199, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.-J.; Yeh, L.-L.; Chan, H.-Y.; Chang, C.-K. Transformation of excess mortality in people with schizophrenia and bipolar disorder in Taiwan. Psychol. Med. 2017, 47, 2483–2493. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.-J.; Yeh, L.-L.; Chan, H.-Y.; Chang, C.-K. Excess mortality and shortened life expectancy in people with major mental illnesses in Taiwan. Epidemiology Psychiatr. Sci. 2020, 29, e156. [Google Scholar] [CrossRef]
- Tiihonen, J.; Lönnqvist, J.; Wahlbeck, K.; Klaukka, T.; Niskanen, L.; Tanskanen, A.; Haukka, J. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet 2009, 374, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.M.; Wahlbeck, K.; Hällgren, J.; Westman, J.; Ösby, U.; Alinaghizadeh, H.; Gissler, M.; Nordentoft, M. Life Expectancy and Death by Diseases of the Circulatory System in Patients with Bipolar Disorder or Schizophrenia in the Nordic Countries. PLOS ONE 2013, 8, e67133. [Google Scholar] [CrossRef] [PubMed]
- Lahti, M.; Tiihonen, J.; Wildgust, H.; Beary, M.; Hodgson, R.; Kajantie, E.; Osmond, C.; Räikkönen, K.; Eriksson, J. Cardiovascular morbidity, mortality and pharmacotherapy in patients with schizophrenia. Psychol. Med. 2012, 42, 2275–2285. [Google Scholar] [CrossRef]
- Laursen, T.M.; Mortensen, P.B.; MacCabe, J.H.; Cohen, D.; Gasse, C. Cardiovascular drug use and mortality in patients with schizophrenia or bipolar disorder: a Danish population-based study. Psychol. Med. 2014, 44, 1625–1637. [Google Scholar] [CrossRef]
- Morgan, V.A.; McGrath, J.J.; Jablensky, A.; Badcock, J.C.; Waterreus, A.; Bush, R.; Carr, V.; Castle, D.; Cohen, M.; Galletly, C.; et al. Psychosis prevalence and physical, metabolic and cognitive co-morbidity: data from the second Australian national survey of psychosis. Psychol. Med. 2014, 44, 2163–2176. [Google Scholar] [CrossRef]
- Gardner-Sood, P.; Lally, J.; Smith, S.; Atakan, Z.; Ismail, K.; Greenwood, K.E.; Keen, A.; O’Brien, C.; Onagbesan, O.; Fung, C.; et al. Cardiovascular risk factors and metabolic syndrome in people with established psychotic illnesses: baseline data from the IMPaCT randomized controlled trial. Psychol. Med. 2015, 45, 2619–2629. [Google Scholar] [CrossRef]
- Owen, M.J.; Sawa, A.; Mortensen, P.B. Schizophrenia. Lancet 2016, 388, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Carli, M.; Kolachalam, S.; Longoni, B.; Pintaudi, A.; Baldini, M.; Aringhieri, S.; Fasciani, I.; Annibale, P.; Maggio, R.; Scarselli, M. Atypical Antipsychotics and Metabolic Syndrome: From Molecular Mechanisms to Clinical Differences. Pharmaceuticals 2021, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Atypical Antipsychotic Drugs and the Risk of Sudden Cardiac Death. New Engl. J. Med. 2009, 360, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Tiihonen, J.; Lönnqvist, J.; Wahlbeck, K.; Klaukka, T.; Tanskanen, A.; Haukka, J. Antidepressants and the Risk of Suicide, Attempted Suicide, and Overall Mortality in a Nationwide Cohort. Arch. Gen. Psychiatry 2006, 63, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Tiihonen, J.; Haukka, J.; Taylor, M.; Haddad, P.M.; Patel, M.X.; Korhonen, P. A Nationwide Cohort Study of Oral and Depot Antipsychotics After First Hospitalization for Schizophrenia. Am. J. Psychiatry 2011, 168, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Winkleby, M.A.; Sundquist, K.; Sundquist, J.; Jørgensen, M.; Mainz, J.; Carinci, F.; Thomsen, R.W.; Johnsen, S.P.; Tiihonen, J.; et al. Comorbidities and Mortality in Persons with Schizophrenia: A Swedish National Cohort Study. Am. J. Psychiatry 2013, 170, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Y.; Yeh, L.-L.; Pan, Y.-J. Exposure to psychotropic medications and mortality in schizophrenia: a 5-year national cohort study. Psychol. Med. 2023, 53, 5528–5537. [Google Scholar] [CrossRef] [PubMed]
- Torniainen, M.; Mittendorfer-Rutz, E.; Tanskanen, A.; Björkenstam, C.; Suvisaari, J.; Alexanderson, K.; Tiihonen, J. Antipsychotic Treatment and Mortality in Schizophrenia. Schizophr. Bull. 2015, 41, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.I.; Vahia, I.; Reyes, P.; Diwan, S.; Bankole, A.O.; Palekar, N.; Kehn, M.; Ramirez, P. Focus on Geriatric Psychiatry: Schizophrenia in Later Life: Clinical Symptoms and Social Well-being. Psychiatr. Serv. 2008, 59, 232–234. [Google Scholar] [CrossRef]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Folsom, D.P.; Lebowitz, B.D.; Lindamer, L.A.; Palmer, B.W.; Patterson, T.L.; Jeste, D.V. Schizophrenia in late life: emerging issues. Dialog- Clin. Neurosci. 2006, 8, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.I.; Meesters, P.D.; Zhao, J. New perspectives on schizophrenia in later life: implications for treatment, policy, and research. Lancet Psychiatry 2015, 2, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Seeman, M.V. Schizophrenia Mortality: Barriers to Progress. Psychiatr. Q. 2019, 90, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; Druss, B. The epidemiology of diabetes in psychotic disorders. Lancet Psychiatry 2015, 2, 431–451. [Google Scholar] [CrossRef] [PubMed]
- Carney, C.P.; Jones, L.; Woolson, R.F. Medical Comorbidity in Women and Men with Schizophrenia: A Population-Based Controlled Study. J. Gen. Intern. Med. 2006, 21, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, Incidence and Mortality from Cardiovascular Disease in Patients with Pooled and Specific Severe Mental Illness: A Large-Scale Meta-Analysis of 3,211,768 Patients and 113,383,368 Controls. World Psychiatry 2017, 16, 163–180. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Croatto, G.; Schneider, L.K.; Rohani-Montez, S.C.; Fairley, L.; Smith, N.; Bitter, I.; Gorwood, P.; Taipale, H.; et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry 2022, 21, 248–271. [Google Scholar] [CrossRef] [PubMed]
- Cuesta, M.J.; Peralta, V. Lack of Insight in Schizophrenia. Schizophr. Bull. 1994, 20, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Jablensky, A.; Sartorius, N.; Ernberg, G.; Anker, M.; Korten, A.; Cooper, J.E.; Day, R.; Bertelsen, A. Schizophrenia: manifestations, incidence and course in different cultures A World Health Organization Ten-Country Study. Psychol. Med. Monogr. Suppl. 1992, 20, 1–97. [Google Scholar] [CrossRef] [PubMed]
- Lacro, J.P.; Dunn, L.B.; Dolder, C.R.; Leckband, S.G.; Jeste, D.V. Prevalence of and Risk Factors for Medication Nonadherence in Patients with Schizophrenia: A Comprehensive Review of Recent Literature. J. Clin. Psychiatry 2002, 63, 892–909. [Google Scholar] [CrossRef]
- Winterer, G. Why Do Patients with Schizophrenia Smoke? Curr. Opin. Psychiatry 2010, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Šagud, M.; Vuksan-Ćusa, B.; Jakšić, N.; Mihaljević-Peleš, A.; Živković, M.; Vlatković, S.; Prgić, T.; Marčinko, D.; Wang, W. Nicotine dependence in Croatian male inpatients with schizophrenia. BMC Psychiatry 2018, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion (US). Office on Smoking and Health The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta (GA).
- Jha, P.; Ramasundarahettige, C.; Landsman, V.; Rostron, B.; Thun, M.; Anderson, R.N.; McAfee, T.; Peto, R. 21st-Century Hazards of Smoking and Benefits of Cessation in the United States. N. Engl. J. Med. 2013, 368, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Office of the Surgeon General (US); Office on Smoking and Health (US). The Health Consequences of Smoking: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta (GA); ISBN 9780160515767.
- Thun, M.J.; Apicella, L.F.; Henley, S.J. Smoking vs Other Risk Factors as the Cause of Smoking-Attributable Deaths. JAMA 2000, 284, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Peritogiannis, V.; Ninou, A.; Samakouri, M. Mortality in Schizophrenia-Spectrum Disorders: Recent Advances in Understanding and Management. Healthcare 2022, 10, 2366. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.; Mainz, J.; Egstrup, K.; Johnsen, S.P. Quality of Care and Outcomes of Heart Failure among Patients with Schizophrenia in Denmark. Am. J. Cardiol. 2017, 120, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Harangozo, J.; Reneses, B.; Brohan, E.; Sebes, J.; Csukly, G.; López-Ibor, J.J.; Sartorius, N.; Rose, D.; Thornicroft, G. Stigma and discrimination against people with schizophrenia related to medical services. Int. J. Soc. Psychiatry 2014, 60, 359–366. [Google Scholar] [CrossRef]
- Taipale, H.; Tanskanen, A.; Mehtälä, J.; Vattulainen, P.; Correll, C.U.; Tiihonen, J. 20-Year Follow-up Study of Physical Morbidity and Mortality in Relationship to Antipsychotic Treatment in a Nationwide Cohort of 62,250 Patients with Schizophrenia (FIN20). World Psychiatry 2020, 19, 61–68. [Google Scholar] [CrossRef]
- Westman, J.; Eriksson, S.V.; Gissler, M.; Hällgren, J.; Prieto, M.L.; Bobo, W.V.; Frye, M.A.; Erlinge, D.; Alfredsson, L.; Ösby, U. Increased cardiovascular mortality in people with schizophrenia: a 24-year national register study. Epidemiol. Psychiatr. Sci. 2018, 27, 519–527. [Google Scholar] [CrossRef]
- Hannoodee, H.; Al Khalili, M.; Theik, N.W.Y.; Raji, O.E.; Shenwai, P.; Shah, R.; Kalluri, S.R.; Bhutta, T.H.; Khan, S. The Outcomes of Acute Coronary Syndrome in Patients Suffering from Schizophrenia: A Systematic Review. Cureus 2021, 13, e16998. [Google Scholar] [CrossRef]
- Goldfarb, M.; De Hert, M.; Detraux, J.; Di Palo, K.; Munir, H.; Music, S.; Piña, I.; Ringen, P.A. Severe Mental Illness and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 918–933. [Google Scholar] [CrossRef]
- Tandon, R. Antipsychotics in the Treatment of Schizophrenia: An Overview. J. Clin. Psychiatry 2011, 72 (Suppl. 1), 4–8. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Detraux, J.; van Winkel, R.; Yu, W.; Correll, C.U. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat. Rev. Endocrinol. 2011, 8, 114–126. [Google Scholar] [CrossRef]
- Vancampfort, D.; Correll, C.U.; Galling, B.; Probst, M.; De Hert, M.; Ward, P.B.; Rosenbaum, S.; Gaughran, F.; Lally, J.; Stubbs, B. Diabetes Mellitus in People with Schizophrenia, Bipolar Disorder and Major Depressive Disorder: A Systematic Review and Large Scale Meta-Analysis. World Psychiatry 2016, 15, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Kredentser, M.S.; Martens, P.J.; Chochinov, H.M.; Prior, H.J. Cause and Rate of Death in People with Schizophrenia across the Lifespan: A Population-Based Study in Manitoba, Canada. J. Clin. Psychiatry 2014, 75, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Talaslahti, T.; Alanen, H.-M.; Hakko, H.; Isohanni, M.; Häkkinen, U.; Leinonen, E. Mortality and causes of death in older patients with schizophrenia. Int. J. Geriatr. Psychiatry 2012, 27, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Vahia, I.V.; Diwan, S.; Bankole, A.O.; Kehn, M.; Nurhussein, M.; Ramirez, P.; Cohen, C.I. Adequacy of Medical Treatment among Older Persons with Schizophrenia. Psychiatr. Serv. 2008, 59, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Brink, M.; Green, A.; Bojesen, A.B.; Lamberti, J.S.; Conwell, Y.; Andersen, K. Physical Health, Medication, and Healthcare Utilization among 70-Year-Old People with Schizophrenia: A Nationwide Danish Register Study. Am. J. Geriatr. Psychiatry 2017, 25, 500–509. [Google Scholar] [CrossRef]
- Masand, P.S. Side effects of antipsychotics in the elderly. J. Clin. Psychiatry 2000, 61 (Suppl. 8), 43–49, discussion 50-1. [Google Scholar]
- Shenoy, P.; Harugeri, A. Elderly patients’ participation in clinical trials. Perspect. Clin. Res. 2015, 6, 184–189. [Google Scholar] [CrossRef]
- Wang, P.S.; Schneeweiss, S.; Avorn, J.; Fischer, M.A.; Mogun, H.; Solomon, D.H.; Brookhart, M.A. Risk of Death in Elderly Users of Conventional vs. Atypical Antipsychotic Medications. N. Engl. J. Med. 2005, 353, 2335–2341. [Google Scholar] [CrossRef] [PubMed]
- Huybrechts, K.F.; Gerhard, T.; Crystal, S.; Olfson, M.; Avorn, J.; Levin, R.; Lucas, J.A.; Schneeweiss, S. Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population based cohort study. BMJ 2012, 344, e977. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration. 2016. Introduction of the System of the Tenth Edition of the International Classification of Diseases for National Health Insurance (ICD-10-CM/PCS). Available online: https://www.nhi.gov.tw/Resource/webdata/27361_3_%E5%85%A8%E6%B0%91%E5%81%A5%E5%BA%B7%E4%BF%9D%E9%9A%AA%E5%9C%8B%E9%9A%9B%E7%96%BE%E7%97%85%E5%88%86%E9%A1%9E%E7%AC%AC%E5%8D%81%E7%89%88(ICD-10-CM-PCS)%E5%88%B6%E5%BA%A6%E7%B0%A1%E4%BB%8B%E5%8F%8A%E8%AA%AA%E6%98%8E.pdf (accessed on 4 November 2023).
- WHO Collaborating Centre for Drug Statistics Methodology. 2012. Guidelines for ATC classification and DDD assignment, 16th edition. Available online: https://www.whocc.no/filearchive/publications/1_2013guidelines.pdf (accessed on 4 November 2023).
Figure 1.
HRs and 95% CIs for exposure to antipsychotics for overall mortality in demographic adjusted model (a.) and fully adjusted model (b.) in patients with schizophrenia and elderly patients with schizophrenia as compared to a control sample without psychiatric diagnoses.
Figure 1.
HRs and 95% CIs for exposure to antipsychotics for overall mortality in demographic adjusted model (a.) and fully adjusted model (b.) in patients with schizophrenia and elderly patients with schizophrenia as compared to a control sample without psychiatric diagnoses.
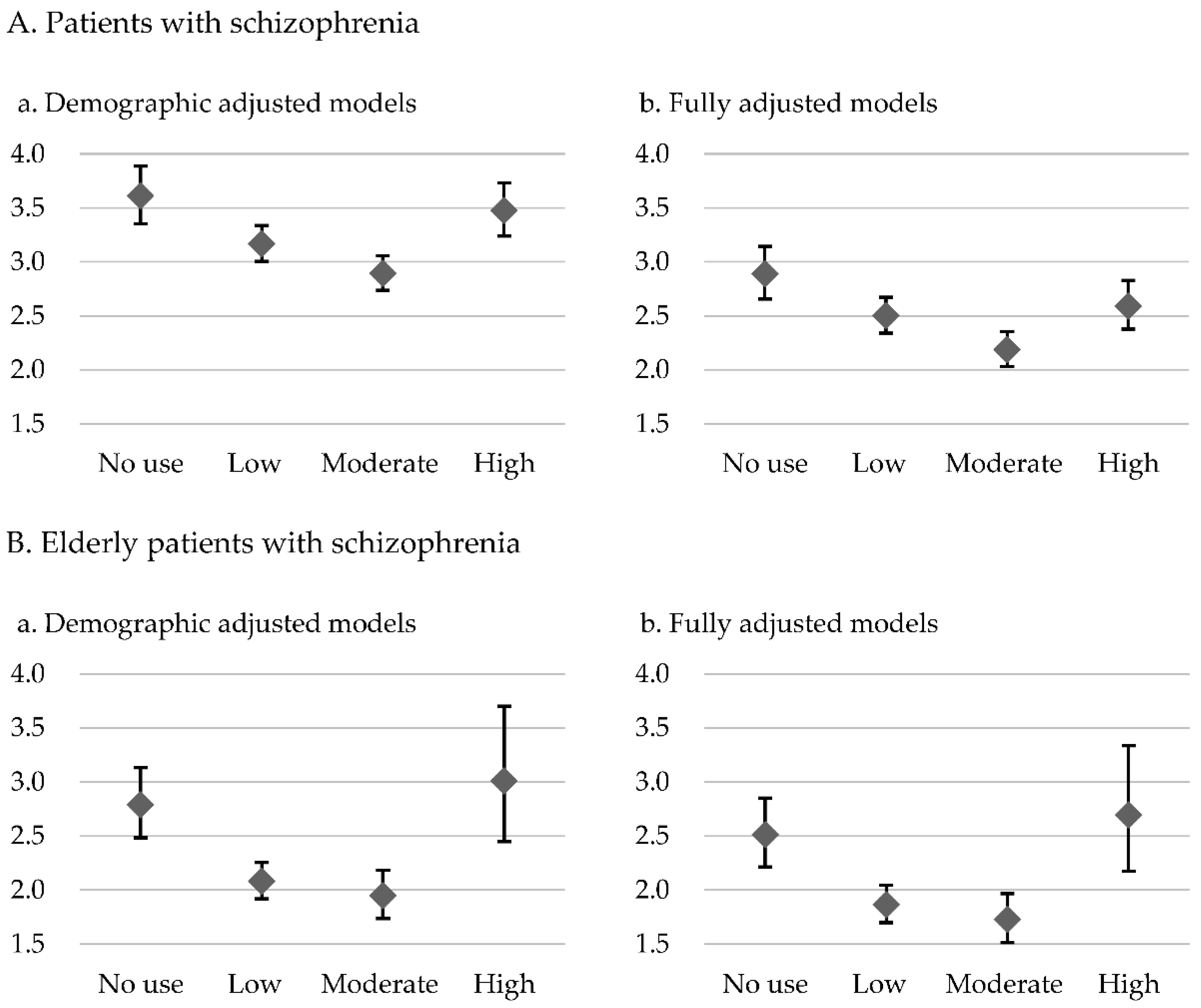
Figure 2.
HRs and 95% CIs for exposure to antipsychotics for CVD-related mortality in demographic adjusted model (a.) and fully adjusted model (b.) in patients with schizophrenia and elderly patients with schizophrenia as compared to a control sample without psychiatric diagnoses.
Figure 2.
HRs and 95% CIs for exposure to antipsychotics for CVD-related mortality in demographic adjusted model (a.) and fully adjusted model (b.) in patients with schizophrenia and elderly patients with schizophrenia as compared to a control sample without psychiatric diagnoses.


Table 1.
Demographic characteristics of patients with schizophrenia (n= 102,964), elderly patients with schizophrenia (n= 6433), and control samples.
Table 1.
Demographic characteristics of patients with schizophrenia (n= 102,964), elderly patients with schizophrenia (n= 6433), and control samples.
| Patients with schizophrenia (n=102,964) |
Control sample (n=102,964) | Significance | Elderly patients with schizophrenia (n=6433) |
Control sample (n=7485) |
Significance | |
|---|---|---|---|---|---|---|
| Age (years old)[mean (SD)] | 44.8 (13.2) | 44.8(13.6) | F=720.946** | 73.6 (6.7) | 72.9 (6.5) | F=40.762** |
| Gender [n (%)] | χ2=0.0** | χ2=0.079 | ||||
| Female | 48,813 (47.4) | 48,813(47.4) | 3843 (59.7) | 4489 (60.0) | ||
| Male | 54,151 (52.6) | 54,151(52.6) | 2590 (40.3) | 2996 (40.0) | ||
|
Lower-income household [n (%)] |
13,129 (12.8) | 778(0.8) | χ2=107017.511** | 948 (14.7) | 58 (0.8) | χ2=1005.687** |
| With catastrophic illness certificate [n (%)] | 74,540 (72.4) | 2673(2.6) | χ2=107017.511** | 4049 (62.9) | 602 (8.0) | χ2=4686.137** |
| Chronic diseases | ||||||
| COPD [n (%)] | 8796 (8.5) | 5055 (4.9) | χ2=1083.264** | 1408 (21.9) | 1085 (14.5) | χ2=128.549** |
| CVD [n (%)] | 10575 (10.3) | 9199 (8.9) | χ2=105.922** | 2151 (33.4) | 2726 (36.4) | χ2=13.520** |
| Cancer [n (%)] | 1642(1.6) | 2165(2.1) | χ2=73.202** | 309 (4.8) | 503 (6.7) | χ2=23.136** |
| DM [n (%)] | 11261(10.9) | 7001(6.8) | χ2=1090.437** | 1477 (23.0) | 1812 (24.2) | χ2=39.0484 |
| RD [n (%)] | 2414(2.3) | 2014(2.0) | χ2=36.928** | 510 (7.9) | 560 (7.5) | χ2=39.0484 |
| Death [n (%)] | χ2=2691.217** | χ2=517.351** | ||||
| All causes | 7,730 (7.5) | 2,593 (2.5) | 2053 (31.9) | 1168 (15.6) | ||
| Natural causes | 6,176 (6.0) | 843 (0.8) | χ2=695.821** | 1239 (19.3) | 475 (6.3) | χ2=161.784** |
| Cancer | 1,083 (1.1) | 909 (0.88) | 258 (4.0) | 320 (4.3) | ||
| CVD | 1,248 (1.2) | 446 (0.43) | 384 (6.0) | 247 (3.3) | ||
| DM | 449 (0.4) | 152 (0.15) | 111 (1.7) | 86 (1.1) | ||
| Unnatural causes | 1,258 (1.2) | 149 (0.14) | 33 (0.5) | 33 (0.4) | ||
| Suicide | 798 (0.8) | 68 (0.07) | 15 (0.2) | 4 (0.1) | ||
| Unknown | 296 (0.3) | 26 (0.03) | 13 (0.2) | 3 (0.0) | ||
| Follow-up days [mean (SD)] | 1735.52 (231.67) | 1741.79 (174.7) | F=261.113** | 1491.12(529.14) | 1655.51(379.63) | F=104.75** |
Continuous variables were compared using ANOVA; categorical variables were compared using a chi-squared test. aPeople diagnosed by a physician as having a condition classified as a catastrophic illness by the Ministry of Health and Welfare can apply for a catastrophic illness certificate so that they do not need to pay a co-payment to receive care for the illness. Abbreviations: SD, standard deviation; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; DM, diabetes mellitus; RD, renal disease. *p < 0.05, **p < 0.001.
Table 2.
Demographic (age and gender) adjusted hazard ratios for antipsychotics, according to degree of exposure in patients with schizophrenia and elderly patients with schizophrenia compared with the control groups. (model 1).
Table 2.
Demographic (age and gender) adjusted hazard ratios for antipsychotics, according to degree of exposure in patients with schizophrenia and elderly patients with schizophrenia compared with the control groups. (model 1).
| No exposure | Low exposure | Moderate exposure | High exposure | |||||
| Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | |
| Patients with schizophrenia (n=102,964) n (%) | 8,733 (8.5%) | 33,403 (32.4%) | 41,811 (40.6%) | 19,017 (18.5%) | ||||
| Overall mortality | 3.610 | 3.353-3.886** | 3.167 | 3.005-3.337** | 2.892 | 2.737-3.056** | 3.475 | 3.238-3.730** |
| Cardiovascular mortality | 3.370 | 2.815-4.035** | 2.907 | 2.559-3.304** | 2.856 | 2.492-3.272** | 3.529 | 2.952-4.218** |
| Elderly patients with schizophrenia (n=6,433) n (%) | 944 (14.7%) | 3,520 (54.7%) | 1,636 (25.4%) | 333(5.2%) | ||||
| Overall mortality | 2.789 | 2.483-3.133** | 2.080 | 1.917-2.256** | 1.946 | 1.735-2.183** | 3.010 | 2.448-3.701** |
| Cardiovascular mortality | 2.536 | 1.952-3.295** | 1.885 | 1.572-2.259** | 1.513 | 1.148-1.996** | 2.953 | 1.865-4.674** |
Survival analysis was conducted by Cox regressions with variables including gender and age (Reference group = control group). Hazard ratios for overall mortality and cardiovascular mortality were calculated according to the DDD group based on the degree of exposure to antipsychotics. Patients were categorized into four DDD groups: no exposure (the reference group), low exposure (<0.5DDD), moderate exposure (0.5-1.5DDD), and high exposure (>1.5DDD). Abbreviations: CI, confidence interval; DDD, defined daily dose. *p<0.05, **p<0.001.
Table 3.
Fully adjusted hazard ratios for antipsychotics, according to degree of exposure in patients with schizophrenia and elderly patients with schizophrenia compared with the control groups. (model 2).
Table 3.
Fully adjusted hazard ratios for antipsychotics, according to degree of exposure in patients with schizophrenia and elderly patients with schizophrenia compared with the control groups. (model 2).
| No exposure | Low exposure | Moderate exposure | High exposure | |||||
| Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | Adjusted Hazard ratio | 95% CI | |
| Patients with schizophrenia (n=102,964) n (%) | 8,733 (8.5%) | 33,403 (32.4%) | 41,811 (40.6%) | 19,017 (18.5%) | ||||
| Overall mortality | 2.888 | 2.654-3.142** | 2.500 | 2.340-2.671** | 2.187 | 2.032-2.354** | 2.591 | 2.375-2.826** |
| Cardiovascular mortality | 2.956 | 2.402-3.639** | 2.462 | 2.092-2.898** | 2.327 | 1.938-2.795** | 2.874 | 2.309-3.577** |
| Elderly patients with schizophrenia (n=6,433) n (%) | 944 (14.7%) | 3,520 (54.7%) | 1,636 (25.4%) | 333(5.2%) | ||||
| Overall mortality | 2.511 | 2.214-2.849** | 1.862 | 1.696-2.044** | 1.727 | 1.517-1.965** | 2.692 | 2.172-3.337** |
| Cardiovascular mortality | 2.392 | 1.796-3.185** | 1.713 | 1.388-2.114** | 1.359 | 0.996-1.854** | 2.784 | 1.724-4.495** |
Survival analysis was conducted by Cox regressions with variables including gender, age, catastrophic illness certification, socioeconomic status (insurance premium level, lower-income household, and urbanization level), and comorbid physical illnesses (chronic obstructive pulmonary disease, cardiovascular disease, cancer, diabetes mellitus, renal disease) (Reference group = control group). Hazard ratios for overall mortality and cardiovascular mortality were calculated according to the DDD group based on the degree of exposure to antipsychotics. Patients were categorized into four DDD groups: no exposure, low exposure (<0.5DDD), moderate exposure (0.5-1.5DDD), and high exposure (>1.5DDD). Abbreviations: CI, confidence interval; DDD, defined daily dose *p<0.05, **p<0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



