
Submitted:
05 December 2023
Posted:
06 December 2023
You are already at the latest version
Abstract
We performed arthroscopically assisted coracoclavicular (CC) stabilization using a suture button device for modified Neer type IIb lateral clavicle fractures accompanied by CC ligament injury. The purpose of the present study was to evaluate the radiological and clinical outcomes of this procedure. Six consecutive patients with modified Neer type IIb fractures were treated with the technique and followed for 12 months. Postoperative ranges of motion (ROMs) and X-rays were evaluated every 3 months. Shoulder functional scores (University of California Los Angeles score, Japanese Orthopedics Association score), visual analog scale (VAS) scores for pain at rest, at night, and during motion, and VAS score for satisfaction were analyzed at 12 months after surgery. For the clinical outcomes, early ROM recovery and excellent outcomes were achieved. For the radiological outcomes, all patients accomplished bone union, slight superior displacement was noted in the CC distance and Dog Bone distance, and bone hole dilation was observed in the superior coracoid and inferior clavicle, but there were no critical complications. The present findings indicate that arthroscopically assisted CC stabilization with a suture button device for unstable lateral clavicle fractures can produce satisfactory radiological and clinical results.
Keywords:
lateral clavicle fracture
; coracoclavicular ligament
; modified Neer classification
; arthroscopic surgery
1. Introduction
Lateral clavicle fractures represent approximately 10%–15% of all clavicle fractures [1] and 50% of all ununited clavicular fractures [2]. These fractures have a high nonunion rate (33%) after nonsurgical treatment [2]. Nonunions and malunions can result in persistent pain, restricted range of motion (ROM), and loss of strength. In the largest available series of nonoperatively managed displaced lateral clavicle fractures, 14% of patients eventually required surgery [3], and reconstruction of an established nonunion can be technically challenging [4]. Therefore, surgical management is commonly offered for displaced lateral clavicle fractures, and multiple surgical procedures are available. Lateral clavicle fractures are commonly classified using the Neer classification as modified by Craig [5,6,7,8,9,10,11,12]. The modified Neer classification divides lateral clavicle fractures into types I to V. Types I and III fractures with an intact CC ligament are stable and can be treated conservatively [13]. Type II fractures are regarded as unstable with higher risk of nonunion or malunion and are more often considered for surgical management. Type II fractures are further subcategorized into types IIA and IIB. In type IIA fractures, the CC ligament remains intact, whereas in type IIB injuries, the CC ligament is partially or completely detached [14]. The optimal treatment of type IIB lateral clavicle fractures is controversial because of the instability associated with the CC ligament injury and the difficulty in accurate fixation with a small lateral fragment [15].
Numerous surgical techniques for type IIB lateral clavicle fractures, including K-wire fixation, tension band wiring (TBW), CC screw fixation, hook plate, anatomical locking plate, and CC ligament reconstruction, have been reported [16]. However, there is no gold standard for surgical treatment of this type of fracture [14]. A review found no superiority for any techniques based on functional outcomes and union rates [17].
CC stabilization using a suture button device is a relatively new treatment for type IIB lateral clavicle fractures. A biomechanical study revealed that CC stabilization using a CC button and suture tapes produced greater stability for superior loading compared with a distal third locking plate in type IIB lateral clavicle fractures [18]. Other advantages of CC stabilization for type IIB lateral clavicle fractures were lower necessity for implant removal and no need for acromioclavicular (AC) joint fixation compared with prior hook plate (HP) fixation. Several studies have reported satisfactory clinical and radiological results after CC stabilization using a suture button device for type IIB lateral clavicle fractures [6,7,19,20,21].
Since 2021, we have performed mini-open reduction and arthroscopically assisted CC stabilization using an AC Dog Bone Button device (Arthrex, Naples, FL, USA) as a suspension system. The system showed higher stability for superior loading and required minimal bone tunnels (2.4 mm) for the coracoid and clavicle compared with other systems, thereby reducing the risk of bone tunnel-related fractures in the coracoid and clavicle [18]. The purpose of the present study was to evaluate the clinical and radiological outcomes of open reduction and arthroscopically assisted CC stabilization using the AC Dog Bone Button device for type IIB lateral clavicle fractures accompanied by CC ligament injury.
2. Materials and Methods
2.1. Patients
From January 2021 to February 2022, six consecutive patients with modified Neer type IIB lateral clavicle fractures and CC ligament injury underwent mini-open reduction and arthroscopically assisted CC stabilization using the AC Dog Bone Button device by a senior surgeon (D.M.). All patients were classified by preoperative X-ray and computed tomography (CT) examinations and were followed up for a minimum of 12 months.
2.2. Surgical technique
2.2.1. Presurgical measurement
Using bilateral X-rays and CT images, the position of the smallest distance between the clavicle and coracoid process was measured for bone tunnel creation in the clavicle and coracoid.
2.2.2. Installation and anesthesia
All surgical interventions were conducted under general anesthesia with the patient in the beach chair position, and an image intensifier was positioned opposite the operated shoulder.
2.2.3. Mini-open reduction
A 5-cm incision (4 cm proximal and 1 cm distal to the fracture) was created on the clavicle and AC joint. The delta-trapezius fascia was incised to expose the clavicle periosteum. The anterior and posterior limits of the fracture and the AC joint were localized to identify the landmark for reduction, and the fixation point based on the presurgical measurement was marked. Manual open reduction was performed, and the reduction was directly confirmed. A 1.8-mm K-wire was then inserted from the acromion to the clavicle for fixation. Accurate reduction was identified by intraoperative fluoroscopy.
2.2.4. Arthroscopic approaches
Two standard portals were used. The posterior glenohumeral portal was created first, and the instrumental anterior portal was established through the rotator interval using an outside-in technique.
2.2.5. Arthroscopic exploration and exposure
A diagnostic shoulder arthroscopy was initially conducted to detect any associated lesions. After opening the rotator interval, the anterolateral portal was created to allow easy access to the coracoid base using an outside-in technique. Using the scope from the posterior portal, the base of the coracoid process was progressively exposed to electrocoagulation [6]. During this step, a 70° camera was used to clearly show the medial coracoid base.
2.2.6. Fixation
A C-shaped ancillary drill guide was inserted through the anterolateral portal positioned under the center of the coracoid process. The other end of the guide was applied and placed on the presurgically marked point [22]. A 2.4-mm cannulated drill was passed through the clavicle and coracoid process under radioscopic guidance. After removal of the ancillary instrument, leaving the pin, a lasso was passed through the cannulated drill and retrieved through the anterolateral portal. The drill was then removed. Two FiberTapes and the Dog Bone Button (Arthrex) were passed from the inferior side of the coracoid process. A superficial Dog Bone Button was also set, and the dislocation was reduced by tightening its proximal end. The image was checked while removing the fixation K-wire, and the FiberTapes were tightened four times to secure the system. Finally, the incisions were closed, with fascia wrapping for knotting and implant.
2.2.7. Postoperative care
The patients used an arm sling for 4 weeks. At 2 weeks after surgery, the patients started passive and active ROM exercises of anterior elevation (AE) and abduction (ABD) within 90 degrees. At 4 weeks after surgery, the patients were allowed to conduct passive and active shoulder ROM exercises with no limitation. All patients were seen at 1 month for the first radiological and clinical follow-up visit and every 3 months until 12 months after surgery.
2.2.8. Evaluation criteria and follow-up
Postoperative follow-up took place as consultations, with systematic ROM measurements (AE, external rotation [ER], internal rotation [IR]) every 3 months. Shoulder functional scores (University of California Los Angeles [UCLA] score, Japanese Orthopedics Association [JOA] score), visual analog scale (VAS) scores for pain at rest, at night, and during motion, and VAS score for satisfaction were analyzed at 12 months after surgery.
Standard anteroposterior and axial clavicle X-rays were taken systematically. Bone union, CC displacement, and bone hole sizes were assessed. Clavicular displacement was evaluated by measuring both the CC distance and the Dog Bone distance (Figure 1). Bone hole sizes were measured on the superficial side of the coracoid process and inferior side of the clavicle in the axial position immediately after surgery and at 3, 6, 9, and 12 months after surgery (Figure 1).
2.3. Statistical analysis
The differences between the follow-up visits were analyzed by the Friedman test to determine which pairwise comparisons reached statistical significance among the CC distance, Dog Bone distance, and bone hole sizes in the superior coracoid and inferior clavicle. An α level of 0.05 was considered significant for all analyses. Calculations were performed using IBM SPSS v.20 statistical software (IBM Corp., Armonk, NY, USA) on a personal computer.
3. Results
The patient characteristics and injury types are shown in Table 1. The patients comprised five men and one woman, and the mean age was 46.7±12.2 years. The mean surgery time and amount of bleeding were 75.8±8.2 min and 20.2±10.8 mL, respectively.
3.1. Functional outcomes
The postoperative ROMs at 3, 6, 9, and 12 months after surgery were 141.7±19.5, 153.3±18.9, 170.0±8.2, and 174.2±7.3 for AE, 45.0±10.0, 53.3±14.6, 70.0±5.8, and 73.3±7.5 for ER, and L2±2.7, Th11±3.4, Th10±2.7, and Th8±1.6 for IR, respectively (Table 1 and Figure 2). Regarding the shoulder functional scores, the mean JOA and UCLA scores were 98.0±3.1 and 34.3±1.0, respectively, at 12 months after surgery (Table 1). The mean VAS scores for pain at 12 months after surgery were 0 at rest, 0 at night, and 0.3±0.8 during motion (Table 1). The mean VAS score for patient satisfaction was 91.7±5.2 at 12 months after surgery (Table 1).
3.2. Radiological analysis
All six patients showed complete bony union, with two showing union at 3 months and four showing union at 6 months. Representative X-rays before and after surgery are shown in Figure 3.
For the CC distance, there were significant differences between day 0 and 6, 9, and 12 months after surgery (p=0.016, p=0.046, and p=0.003, respectively) and between 3 and 12 months after surgery (p=0.016) (Table 2). Otherwise, there were no significant differences at 6 months after surgery. For the Dog Bone distance, there were significant differences between day 0 and 12 months after surgery (p=0.028) and between 6 and 12 months after surgery (p=0.046) (Table 2).
For the bone hole size in the superior coracoid, there were significant differences between day 0 and 6, 9, and 12 months after surgery (p=0.028, p=0.005, and p=0.001, respectively) and between 3 and 12 months after surgery (p=0.003) (Table 3). For the bone hole size in the inferior clavicle, there were significant differences between day 0 and 6, 9, and 12 months after surgery (p=0.028, p=0.009, and p=0.001, respectively) and between 3 and 12 months after surgery (p=0.046). There was no significant differences for the bone hole sizes in both the superior coracoid and inferior clavicle at 6 months after surgery (Table 3).
There were no perioperative complications, including surgical site infection, nerve injury, and coracoid and clavicle fractures.
4. Discussion
In the present study, we analyzed the clinical and radiological results of arthroscopically assisted CC stabilization using a suture button device for lateral clavicle fractures accompanied by CC ligament injury (type IIB fracture in the modified Neer classification). The major findings of the study were early recovery of active shoulder ROMs, satisfactory clinical outcomes, excellent bone union with slightly delayed healing, and low complication rate.
For the recovery of active shoulder ROMs, to the best of our knowledge, this is the first study to analyze the detailed active ROM recovery after arthroscopically assisted CC ligament reconstruction. The recovery of active shoulder ROMs was already noticeable at 3 months after surgery despite the restriction of active ROM exercises for AE and ABD within 90 degrees for 1 month. Almost full recovery of ROMs was achieved at 9 months after surgery, and movement-concomitant complications did not occur. This early recovery can possibly be attributed of the enhanced construct strength against superior loading and reduced invasion of soft tissues [18]. Enhanced construct strength may lead to decreased pain during shoulder motion, and reduced invasion of soft tissues may enable early recovery of muscle strength, and thus early recovery of active shoulder ROMs was accomplished.
Regarding the functional outcomes, the study showed satisfactory clinical outcomes, with mean JOA and UCLA scores of 98.0±3.1 and 34.3±1.0, respectively, at 12 months after surgery. Malik et al. [16] reported that the shoulder function scores after arthroscopically assisted CC ligament reconstruction ranged from 81.8 to 96.2, as assessed by the Constant–Murley score (CMS). For other fixation methods, the mean CMS was 85.3 to 88 in the TBW group [23,24], 79.9 to 93.3 in the hook plate group, and 82.8 to 98.1 in the locking plate group [25,26]. The present method accomplished relatively better ROM recovery and better clinical outcomes compared with similar methods and other fixation methods, suggesting that arthroscopically assisted CC ligament reconstruction can be an optimal treatment for lateral clavicle fractures accompanied by ligament injury.
In the radiological outcomes, bone union was achieved in all patients, and the mean union time was 5 months. In a previous study on the nonunion rate of this fracture surgery, Raval et al. [13] reported a nonunion rate of 18% for fractures with CC ligament injury if treated properly with plate fixation. In other studies, arthroscopic CC ligament reconstruction with a suture device had bone union rates of 70% to 100% [6,7,8,10,11,12,27,28] and union times of 3.5 to 8.4 months [8,10,27]. The discrepancy in these results can be attributed to differences in the fixation methods, including fixation points, implants, and reductions. Meanwhile, the union rates for the TBW procedure ranged from 52.6% to 95.6% [29,30,31,32]. Uittenbogaard et al. [33] reported that the highest revision rate (30%) was observed in TBW compared with other procedures. Malik et al. [17] found that hook plate fixation had a good union rate (96.4%), and the mean union time was 3 months. Anatomical locking plates also had good union rates (96.9%). Zhang et al. [25] demonstrated that anatomical locking plates and hook plates had almost the same union time. In the present study, the rate of bone union was 100%, and this result was possibly derived from the accurate bone tunnel placement based on presurgical measurement and anatomical reduction with the mini-open technique. Slight superior displacement and bone hole dilations were also found with our method. However, there were no significant differences at 6 months after surgery and there was also no implant migration in the coracoid and clavicle. Hence, these changes did not appear to be critical events.
No complications were observed with our procedure. In a previous review, the complication rate for CC stabilization of lateral clavicle fractures was 4.3% [34]. Furthermore, the rate of major complications was 1.0%, including nonunion, implant failure, per-implant fracture, deep infection, and coracoid and acromial fractures, while the rate of minor complications was 3.3%, including delayed union, hardware troubles, subacromial osteolysis, clavicular erosion, peri-anchor problems, loss of reduction, AC joint arthrosis, pain, and superficial infection. In addition, the predominant major complication was nonunion and the predominant minor complication was hardware troubles for CC stabilization. For other procedures, the complication rate of HP was 45% and its major and minor complication rates were 4.5% and 41%, respectively, while the complication rate of LP was 26% and its major and minor complication rates were 2% and 24%, respectively. Our method may reduce major and minor complications through the anatomical reduction with the mini-open technique and intense fascia wrapping of the hardware.
The main limitations of the present study were the small sample size, the lack of a randomized control study design, and the short follow-up time. However, the study was comparable with the majority of other studies.
In the present study, our method achieved early ROM recovery, excellent clinical scores, and bone union in all patients, with no complications. The major advantages of the method compared with other implant fixation methods and previous similar methods are the reduced implant irritation, thus reducing the need for a second surgery to remove the implant, and complete bone union. Hence, our method can become a favorable procedure for lateral clavicle fractures accompanied by CC ligament injury.
5. Conclusions
This study reports the results of arthroscopically assisted CC stabilization using the Dog Bone Button device for lateral clavicle fractures accompanied by CC ligament injury. CC stabilization can achieve early ROM recovery, satisfactory outcomes, 100% bone union rate, and 0% complication rate.
Author Contributions
Conceptualization, D.M.; methodology, D.M., Y.S.; software, Y.S.; validation, Y.S. and D.M.; formal analysis, Y.S.; investigation, D.M., Y.S., T.Kawasaki., T.Kaketa., K.S., and H.U.; resources, D.M.; data curation, Y.S., H.T., F.H., Y.Y., K.Y., and H.U.; writing—original draft preparation, Y.S.; writing—review and editing, Y.S., D.M., and Y.I.; visualization, Y.S.; supervision, D.M. and M.I.; project administration, M.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval is not applicable for the article.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
There are no additional data.
Acknowledgments
The authors thank Alison Sherwin, from Edanz (https://www.edanz.com/ac) for editing a draft of this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Postacchini, F.; Gumina, S.; De Santis, P.; Albo, F. Epidemiology of clavicle fractures. J. Shoulder Elb. Surg. 2002, 11, 452–456. [Google Scholar] [CrossRef]
- Nordqvist, A.; Petersson, C.; Redlund-Johnell, I. The natural course of lateral clavicle fracture: 15 (11–21) year follow-up of 110 cases. Acta Orthop. 1993, 64, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.M.; Cairns, D.A. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J. Bone Jt. Surg. 2004, 86, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.J.; Kavanagh, T.G.; Flannery, M.C. Fractures of the distal clavicle: a case for fixation. Injury 1992, 23, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Takase, K.; Kono, R.; Yamamoto, K. Arthroscopic stabilization for Neer type 2 fracture of the distal clavicle fracture. Arch. Orthop. Trauma Surg. 2012, 132, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Kraus, N.; Stein, V.; Gerhardt, C.; Scheibel, M. Arthroscopically assisted stabilization of displaced lateral clavicle fractures with coracoclavicular instability. Arch. Orthop. Trauma Surg. 2015, 135, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Loriaut, P.; Moreau, P.-E.; Dallaudière, B.; Pélissier, A.; Vu, H.D.; Massin, P.; Boyer, P. Outcome of arthroscopic treatment for displaced lateral clavicle fractures using a double button device. Knee Surg. Sports Traumatol. Arthrosc. 2013, 23, 1429–1433. [Google Scholar] [CrossRef] [PubMed]
- Cisneros, L.N.; Reiriz, J.S. Management of unstable distal third clavicle fractures: clinical and radiological outcomes of the arthroscopy-assisted conoid ligament reconstruction and fracture cerclage with sutures. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Sautet, P.; Galland, A.; Airaudi, S.; Argenson, J.-N.; Gravier, R. Arthroscopy-assisted fixation of fracture of the distal part of the clavicle by subcoracoid suture and clavicle button. Orthop. Traumatol. Surg. Res. 2018, 104, 1237–1240. [Google Scholar] [CrossRef]
- Kapicioglu, M.; Erden, T.; Bilgin, E.; Bilsel, K. All arthroscopic coracoclavicular button fixation is efficient for Neer type II distal clavicle fractures. Knee Surg. Sports Traumatol. Arthrosc. 2020, 29, 2064–2069. [Google Scholar] [CrossRef]
- Flinkkilä, T.; Heikkilä, A.; Sirniö, K.; Pakarinen, H. TightRope versus clavicular hook plate fixation for unstable distal clavicular fractures. Eur. J. Orthop. Surg. Traumatol. 2014, 25, 465–469. [Google Scholar] [CrossRef]
- Xiong, J.; Chen, J.-H.; Dang, Y.; Zhang, D.-Y.; Fu, Z.-G.; Zhang, P.-X. Treatment of unstable distal clavicle fractures (Neer type II): A comparison of three internal fixation methods. J. Int. Med Res. 2018, 46, 4678–4683. [Google Scholar] [CrossRef]
- Raval, P.; See, A.; Singh, H.P. Distal third clavicle fractures: a nationwide trainee-led collaborative review of current practice. Bone Jt. Open 2022, 3, 953–959. [Google Scholar] [CrossRef]
- Khan, L.K.; Bradnock, T.J.; Scott, C.; Robinson, C.M. Fractures of the clavicle. J. Bone Jt. Surg. 2009, 91, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Craig, E.V. Fractures of the clavicle. The Shoulder, 1990, Volume 1, pp. 299–304.
- Malik, S.S.; Tahir, M.; Malik, S.; Kwapisz, A.; Jordan, R.W. Arthroscopically Assisted Coraco-Clavicular Ligament Reconstruction in Treatment of Acute Displaced Distal Clavicle Fractures Provides Good to Excellent Shoulder Function Despite Low Union Rates and High Complication Rates: A Systematic Review. Arthroscopy 2022, 38, 567–582. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.S.; Tahir, M.; Remtulla, M.; Malik, S.; Jordan, R.W. A systematic review and meta-analysis comparing the use of hook plates and superior plates in the treatment of displaced distal clavicle fractures. Arch. Orthop. Trauma Surg. 2023, 143, 329–352. [Google Scholar] [CrossRef] [PubMed]
- Yagnik, G.P.; Brady, P.C.; Zimmerman, J.P.; Jordan, C.J.; Porter, D.A. A biomechanical comparison of new techniques for distal clavicular fracture repair versus locked plating. J. Shoulder Elb. Surg. 2019, 28, 982–988. [Google Scholar] [CrossRef]
- Kim, D.J.; Lee, Y.M.; Yoon, E.J.; Sur, Y.J. Comparison of Locking Plate Fixation and Coracoclavicular Ligament Reconstruction for Neer Type 2B Distal Clavicle Fractures. Orthop. J. Sports Med. 2022, 10, 23259671221086673. [Google Scholar] [CrossRef]
- Salazar, B.P.; Chen, M.J.; Bishop, J.A.; Gardner, M.J. Outcomes after locking plate fixation of distal clavicle fractures with and without coracoclavicular ligament augmentation. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 473–479. [Google Scholar] [CrossRef]
- Takase, K.; Yamamoto, K. Outcomes and function of conoid ligament on the basis of postoperative radiographic findings of arthroscopic stabilization for the distal clavicle fractures. Orthop. Traumatol. Surg. Res. 2019, 105, 281–286. [Google Scholar] [CrossRef]
- Cohen, G.; Boyer, P.; Pujol, N.; Ferjani, B.H.; Massin, P.; Hardy, P. Endoscopically assisted reconstruction of acute acromioclavicular joint dislocation using a synthetic ligament. Outcomes at 12 months. Orthop. Traumatol. Surg. Res. 2011, 97, 145–151. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Lau, M.-J.; Tseng, Y.-C.; Chen, W.-C.; Kao, H.-Y.; Wei, J.-D. Comparison of the efficacy of hook plate versus tension band wire in the treatment of unstable fractures of the distal clavicle. Int. Orthop. 2009, 33, 1401–1405. [Google Scholar] [CrossRef]
- Wu, K.; Chang, C.-H.; Yang, R.-S. Comparing Hook Plates and Kirschner Tension Band Wiring for Unstable Lateral Clavicle Fractures. Orthopedics 2011, 34, e718–e723. [Google Scholar] [CrossRef]
- Zhang, C.; Huang, J.; Luo, Y.; Sun, H. Comparison of the efficacy of a distal clavicular locking plate versus a clavicular hook plate in the treatment of unstable distal clavicle fractures and a systematic literature review. Int. Orthop. 2014, 38, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Elrih, M.; Quinlan, J. Hook Plate Versus Distal Locking Plate for the Fixation of Unstable Distal Clavicle Injuries, Outcomes and Complications: A Meta-Analysis. Cureus 2022, 14, e30806. [Google Scholar] [CrossRef] [PubMed]
- Kuner, E.; Beeres, F.J.P.; Babst, R.; Schoeniger, R. Which lateral clavicle fractures can be treated by an arthroscopic-assisted endobutton procedure? An analysis of risk factors. Arch. Orthop. Trauma Surg. 2018, 139, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Motta, P.; Bruno, L.; Maderni, A.; Tosco, P.; Mariotti, U. Acute lateral dislocated clavicular fractures: arthroscopic stabilization with TightRope. J. Shoulder Elb. Surg. 2014, 23, e47–e52. [Google Scholar] [CrossRef] [PubMed]
- Flinkkilä, T.; Ristiniemi, J.; Hyvönen, P.; Hämäläinen, M. Surgical treatment of unstable fractures of the distal clavicle.A comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop. Scand. 2002, 73, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Charles S Neer, I.I. 5 Fractures of the distal third of the clavicle. Clin. Orthop. Relat. Res. 1968, 58, 43–50. [Google Scholar]
- Kona LC, J.; Bosse, M.J.; Staeheli, J.W.; Rosseau, R.L. Type II distal clavicle fractures: a retrospective review of surgical treatment. J. Orthop. Trauma 1990, 4, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Eskola, A.; Vainionpää, S.; Pätiälä, H.; Rokkanen, P. Outcome of operative treatment in fresh lateral clavicular fracture. Ann. Chir. Et Gynaecol. 1987, 76, 167–169. [Google Scholar]
- Uittenbogaard, S.J.; van Es, L.J.; Haan, C.D.; van Deurzen, D.F.; Bekerom, M.P.v.D. Outcomes, Union Rate, and Complications After Operative and Nonoperative Treatments of Neer Type II Distal Clavicle Fractures: A Systematic Review and Meta-analysis of 2284 Patients. Am. J. Sports Med. 2023, 51, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, A.; Solou, K.; Tatani, I.; Triantafyllopoulos, I.K.; Lakoumentas, J.; Kouzelis, A.; Athanasiou, V.; Kokkalis, Z.T. What is the optimal surgical treatment for Neer type IIB (IIC) distal clavicle fractures? A systematic review and meta-analysis. J. Orthop. Surg. Res. 2022, 17, 215. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual authors and contributors and not of MDPI and the editors. MDPI and the editors disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Figure 1.
Measurements of the CC distance, Dog Bone distance, and bone holes on the superior coracoid and inferior clavicle. ①: CC distance; ②: Dog Bone distance; ③: superior coracoid bone hole; ④: inferior clavicle bone hole.
Figure 1.
Measurements of the CC distance, Dog Bone distance, and bone holes on the superior coracoid and inferior clavicle. ①: CC distance; ②: Dog Bone distance; ③: superior coracoid bone hole; ④: inferior clavicle bone hole.
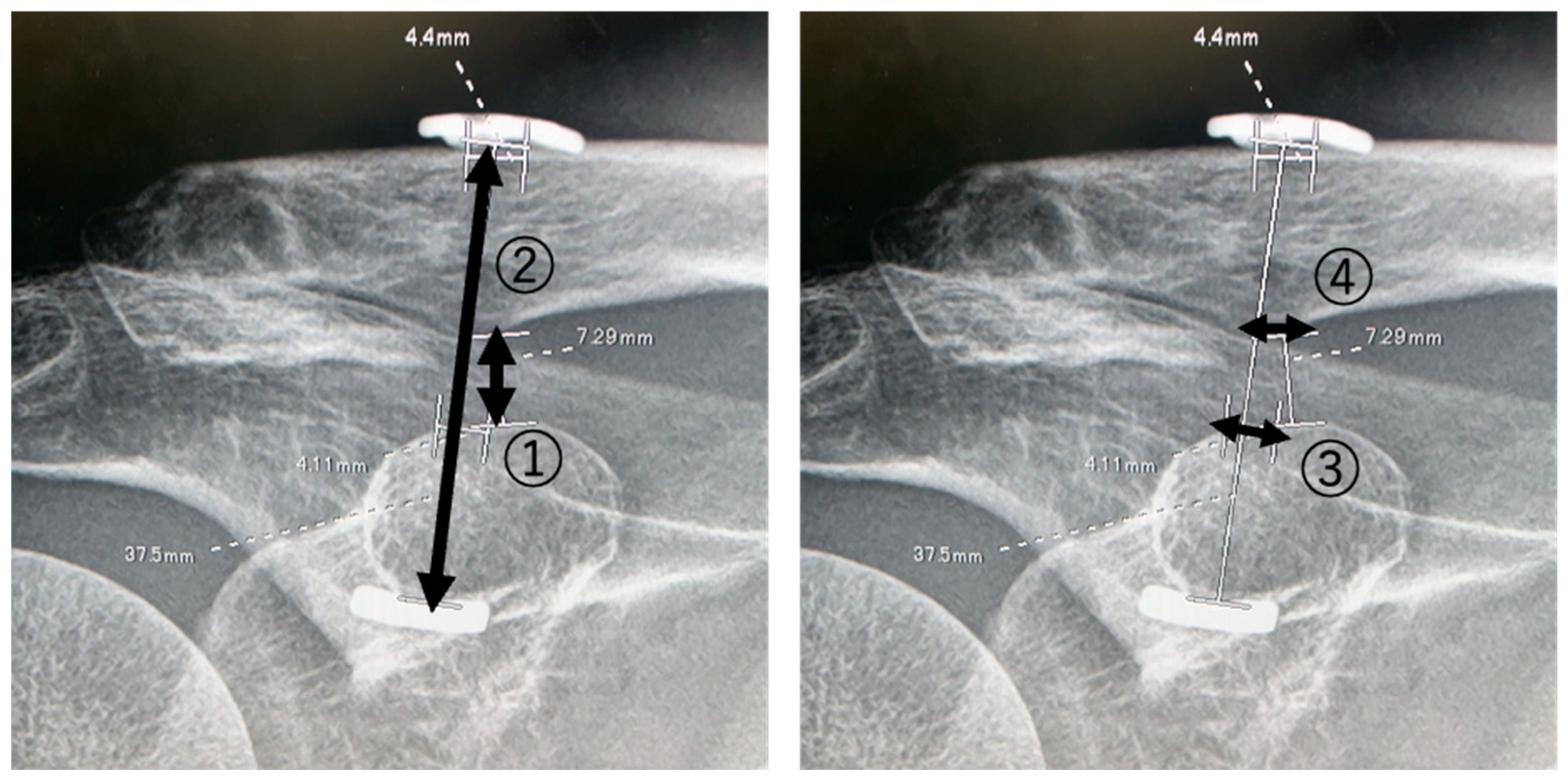
Figure 2.
Postoperative ROMs.
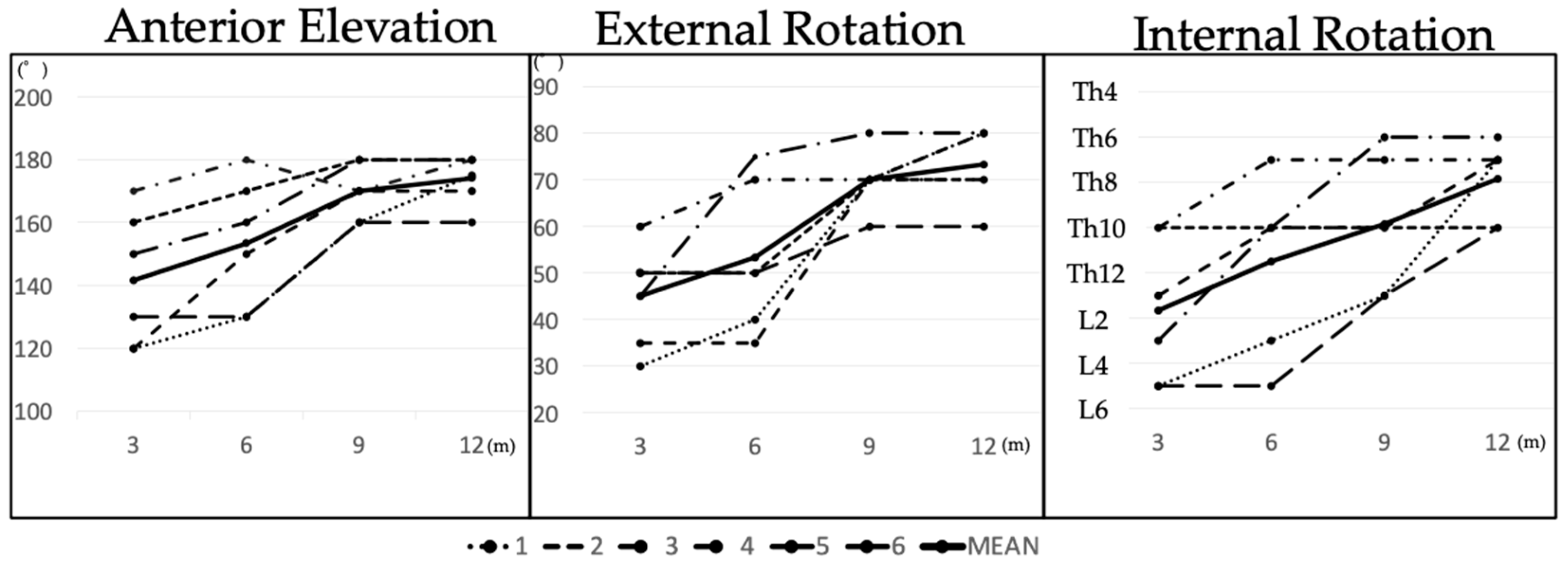
Figure 3.
Representative X-rays before and after surgery. (A) Preoperative radiograph. (B) Postoperative radiograph immediately after surgery. (C) Radiograph at 3 months after surgery. (D) Radiograph at 6 months after surgery showing complete bony union with subsidence of the clavicular button. (E) Radiograph at 9 months after surgery showing no dislocation. (F) Radiograph at 12 months after surgery showing no dislocation.
Figure 3.
Representative X-rays before and after surgery. (A) Preoperative radiograph. (B) Postoperative radiograph immediately after surgery. (C) Radiograph at 3 months after surgery. (D) Radiograph at 6 months after surgery showing complete bony union with subsidence of the clavicular button. (E) Radiograph at 9 months after surgery showing no dislocation. (F) Radiograph at 12 months after surgery showing no dislocation.
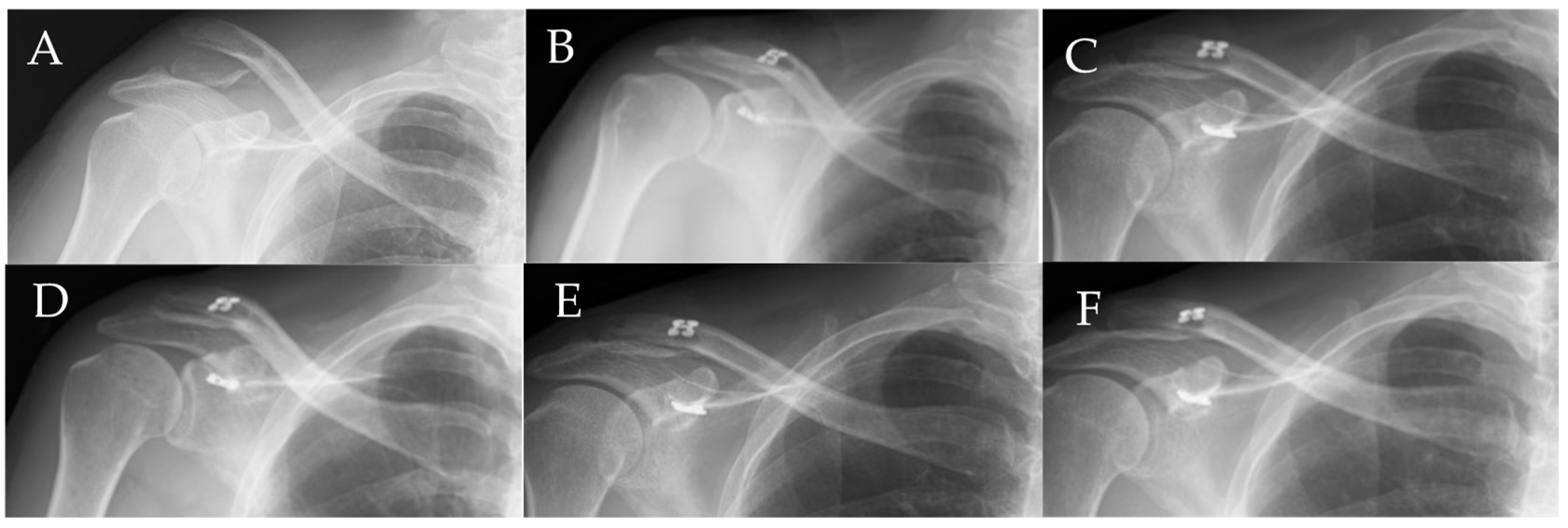

Table 1.
Summary of the patient characteristics and final outcomes.
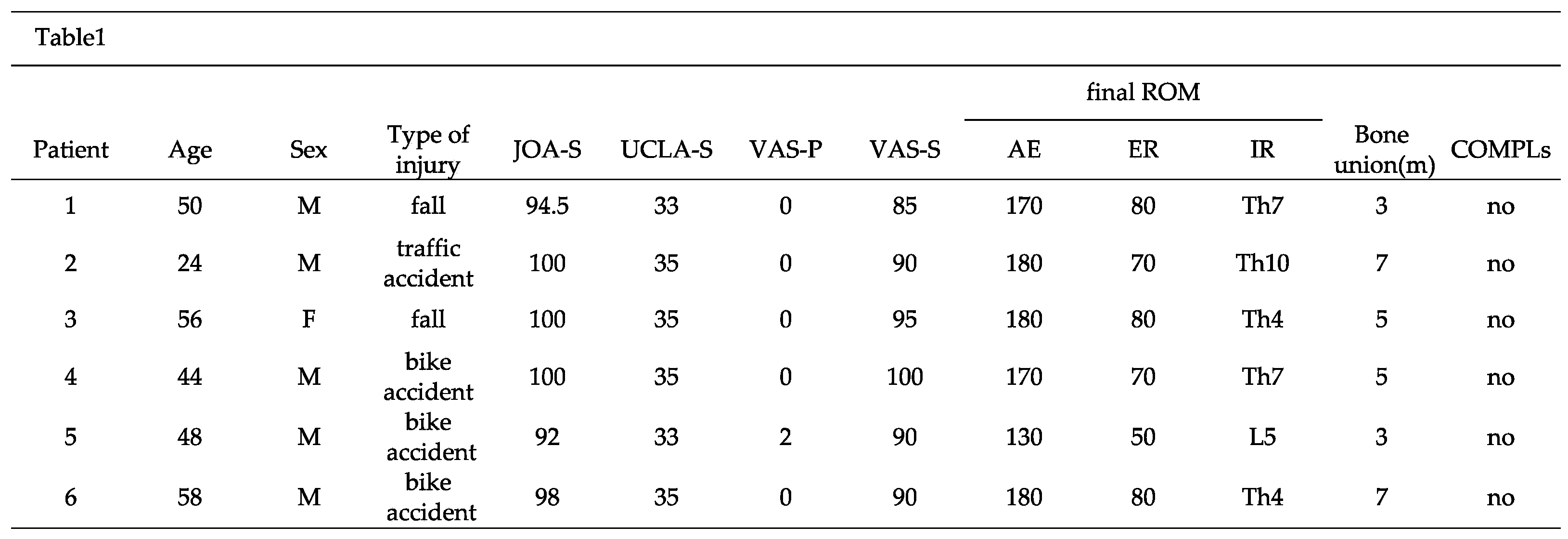 |
F: female; M: male; JOA-S: Japanese Orthopedic Association score; UCLA-S: University of California Los Angeles score; VAS-P: visual analog score-pain; VAS-S: visual analog score-satisfaction; m: months; ROM: range of motion; AE: anterior elevation; ER: external rotation; IR: internal rotation; COMPLs: complications.
Table 2.
CC distances and Dog Bone distances.
 |
m: months; ap<0.05 versus day 0; bp<0.01 versus day 0; cp<0.05 versus 3 months; dp<0.05 versus 6 months; *missing data.
Table 3.
Bone hole sizes in the superior coracoid and inferior clavicle.
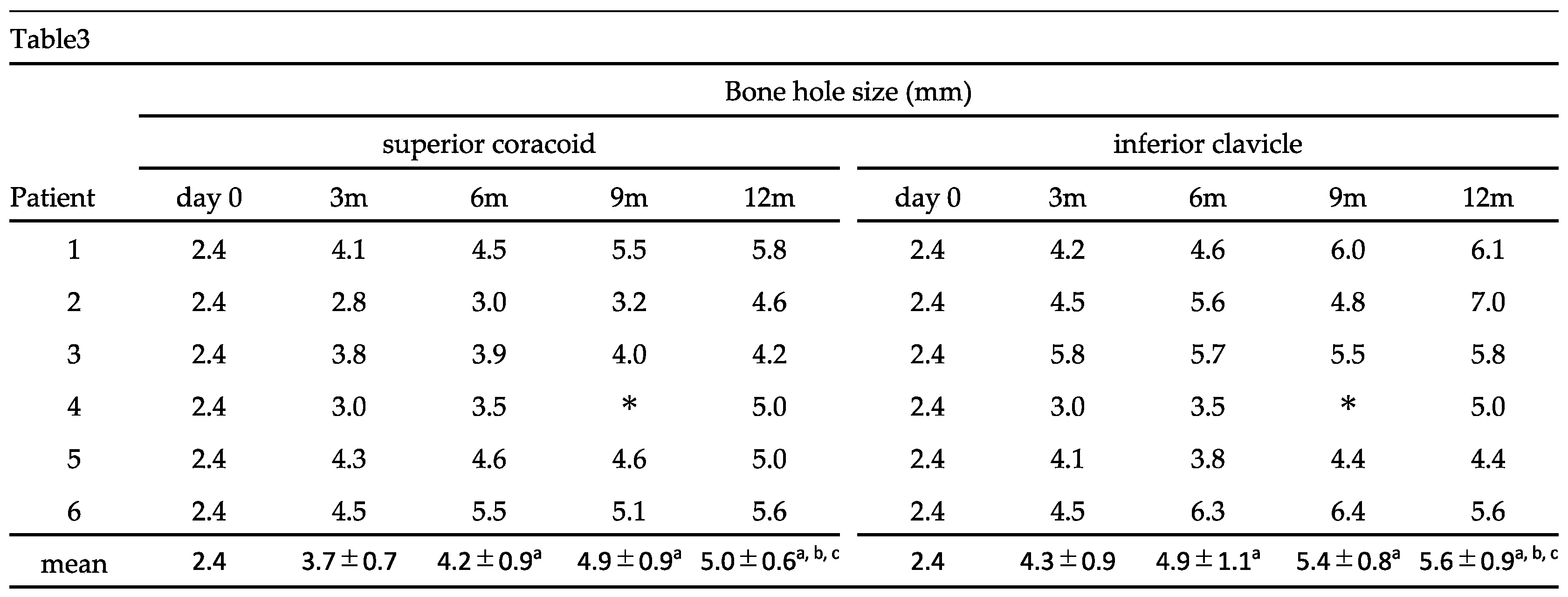 |
m: months; ap<0.05 versus day 0; bp<0.01 versus day 0; cp<0.05 versus 3 months; *missing data.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



