
Submitted:
06 December 2023
Posted:
07 December 2023
You are already at the latest version
Abstract
.Background: Neither radiological phenotypic characteristics nor reconstruction CT scan to study the cranial contour in children with the so called the idiopathic type of West syndrome has been implemented to reach the etiology understanding.
Material and Methods: The basic diagnostic measures and the traditional antiepileptic treatments have been applied to these children in accordance with the conventional protocol of investigations and treatment for children with West syndrome. Boys from three unrelated families were given the diagnosis of idiopathic type of West syndrome. Three boys aged 6,7,9 and three parents (age range of 28-41 year) were included in this study. These children and their parents were referred to our orthopedic departments because of variable skeletal deformities. All showed the history of intellectual disabilities, cryptogenic epileptic spasms and fragmented hypsarrhythmia. Recently, variable forms skeletal deformities of flat foot, torticollis and early onset osteoarthritis. We performed detailed clinical and radiological phenotypic characterization of every affected child, siblings and parents. All affected children underwent whole exome sequence analysis
Results: The craniofacial phenotype of all children revealed apparent disruption of development of the cranial bones. Palpation of the skull bones showed unusual palpable boney ridges along different sutural locations. A-7-year-old child showed abnormal bulging over the sagittal suture associated with bilateral boney ridges over the sequamosal sutures. Examining his parents, we noticed a similar skull radiographic abnormality in his mother radiographs. A-10-year-old boy showed an extremely narrow frontal area, facial asymmetry and a well palpable ridge over the lambdoid sutures. 3D reconstruction CT scan confirmed the diagnosis of early closure . His mother showed typical radiographic skull phenotype with a history of postadulthood scoliosis. A- 12-year-old boy showed brachycephaly. Investigating his parents revealed a brachycephalic mother with border line intellegence. We affirm that the pattern of inheritance in the three boys was compatible with X-linked recessive pattern of inheritance . Whole exome sequencing showed non definite phenotype/genotype correlation.
Conclusion: The aim of this study was fivefold. First, to refute the common usage of the term idiopathic and we affirm that our findings are Novel. Second, it could be possible that West syndrome is a symptom complex rather than a separate diagnostic entity. Third, to further detect the genetic carrier , we explored the connection between the cranial bones in the children with West syndrome with what is seen in parents.. Fourth, the differences in cranial bones abnormalities among every child and another seems to be heterogeneous. Fifth, it seems that the progressive deceleration in the development of this group of children is highly connected to the progressive closure of the cranial sutures.
Keywords:
Idiopathic type of West syndrome
; Cryptogenic epileptic spasms
; Cranial bones
; Radiology
; CT scan
1. Introduction
West syndrome is characterized by early epileptic seizures of infancy or might occur later on in early childhood (cryptogenic epileptic spasms). West syndrome is an unpleasant type of childhood epilepsy because of uncontrolled seizures which are associated with different grades of intellectual disability [1,2].
The etiology understanding of West syndrome encompasses several pathological/syndromic entities, in which West syndrome is a symptom complex rather than a definite diagnostic entity. Aicardi syndrome is an X-linked dominant condition is characterized by infantile spasms, a chorio-retinopathy which is almost distinctive in having footprint shaped lacunae and agenesis of the corpus callosum. Additional malformations include staphyloma, coloboma of the optic nerve, microphthalmia and vertebral body anomalies such as hemivertebrae, vertebral malsegmentation, scoliosis and abnormal costovertebral articulations. Some patients manifested cleft lip and palate [3,4,5,6]. The Schinzel-Giedion syndrome (SGS)which is characterized by seizures and abnormal EEG as well as global developmental retardation and intellectual disability. SGS is characterized by distinctive clinical features, specifically abnormal craniofacial contour as viewed from the front the forehead is tall and prominent, there is severe temporal narrowing leads to mid-face retraction. Hypoplasia /agenesis of the corpus callosum, hydrocephaly and large ventricles are the main cerebral malformation complex [7,8,9].
Sotos syndrome (cerebral gigantism), infants are born with increased birth-weight with an enlarged head circumference. Infantile spasm occurs in connection with dilated cerebral ventricles and in some hypoplasia of the corpus callosum and common occurrence of cavum as well as varibale cerebral abnormalities [10,11,12,13,14]. The classical type of Alexander´s disease which is characterized by infantile onset with seizures, neuro-degeneration and spasticity. An important clinical sign is macrocephaly, hydrocephaly and large ventricles. In some cerebral atrophy/myelin abnormality, and most cases die within five years [15,16,17,18]. West syndrome can occurs in children with variable forms of metabolic disorders. Pyruvate dehydrogenase complex deficiency is an example, which is a major etiology behind congenital lactic acidemia, in which seizures are a major clinical presentation [19,20]. West syndrome has been also described in the literature as Salaam tics or Blitz-Nick-Salaam Krämpfe as a form of generalized/ difficult forms of seizures associated with characteristic EEG readings [21]. It well known that the most difficult aspect of any long term disability is the proper understanding of the correlated anatomical disruption which can enhance the explanation of the pathological series within the natural history of the disease.
2. Materials and Methods
The study was carried out between 2016-2020, within the children orthopedic departments of Speising (Vienna, Austria), Ilizarov Institute of orthopedics (Kurgan-Russia), Ibn Zohr Institute of Diagnostic Radiology (Tunis,Tunisia) and the department of Foot and Ankle Surgery, Neuroorthopaedics and Systemic Disorders, Pediatric Orthopedic Institute (Saintpetersburg-Russia)
The study protocol was approved by Ethics Committee of the (Ilizarov Scientific Research Institute, No.4(50)/13.12.2016, Kurgan, Russia). Informed consents were obtained from the patient’s Guardians. We fully documented the affected children, siblings and parents by means of comprehensive clinical and radiological studies of each individual. The senior author with the great assistance of the colleagues in Vienna and abroad agreed upon a clear cut strategy of comprehensive clinical documentation. Three boys aged 7-10 and 12 year-old-boy from three unrelated families have been diagnosed with the idiopathic type of West syndrome. Recently, referral to orthopedic departments took place because of a diverse form of skeletal deformities such as flat foot, ligamentous hyperlaxity, and early onset osteoarthritis. Clinical examination of parents has been considered a cornerstone in the diagnostic process. Our major clinical strategy is primarily based on detailed clinical and radiological documentation. Family history and multigenerational exploration of family subjects is mandatory when dealing with patients with unknown etiology (idiopathic). Maternal history of spontaneous miscarriages, stillbirths, weak or hyperactive in utero foetal movements, hyperemesis gravidarum, stillbirths, perinatal mortalities, history of sudden infant death syndrome are essential markers required for proper management. Clinical examination of parents can be of tremendous help to understand the mode of the transmitted gene. Meanwhile assessing the educational levels of the parents was a priority. All mothers showed border line intellegence and a history of poor schooling achievements. The detailed clinical examination of these children has been followed up by a skeletal survey. All laboratory investigations were negative and karyotyping of lymphocytes from peripheral blood with GTG banding was normal (46,XY). Full haematological investigations revealed nothing of significance. Syndromic craniosynostosis with FGFRs and TWIST genes mutation have been ruled out. Full haematological investigations revealed nothing of significance. Whole exome sequencing showed no definite reason. We think that it is highly likely that the applied technique missed or did not include the required part of the DNAs that might be responsible for causing the constellation of disorders in this group of children. The first and foremost notable clinical observation was the variable abnormality in the craniofacial phenotype in all children. Interestingly, we detected similar cranial abnormalities in all mothers. All children underwent a series of Conventional radiographs, tomographic studies, and MRI imaging. Interestingly, despite the anatomical disruption of the development of the calvaria. Cerebral MRI showed no concomitant pre-existing pathology.
3. Results
3.1. Family 1
7-year-old- boy with West syndrome associated with hyperkinetic disorder was referred to our department because of ligamentous hyperlaxity and flat foot. Clinical examination showed growth defieciency (10 th percentile). Surprisingly he manifested an abnormal cranial phenotype almost typical for his mother. Palpation of his skull showed a bony ridge over the metopic suture associated unusual bulge over the mid-sagittal suture. Bilateral boney ridges over the squamosal sutures have been well delineated. Palpation of the his mother skull showed a prominent boney bulge over her sagittal suture. AP Skull radiograph of the boy showed facial asymmetry with early closure of the metopic suture and other sutures seemed ill-defined (Figure 1,b). 3D reformatted frontal cranial CT of a-35- year-old- mother clearly showed the closure of the metopic and the sagittal sutures causing a mid sagittal boney bulge (Figure 1,b).
3D reconstruction CT scan of the skull (showed early closure of the metopic suture -arrow(Figure 2,a). 3D reconstruction CT scan while the patient is with mild flexion of the skull showed early closure of the sequamosal sutures pressing the brain contents upward causing the development of a prominent bulge at the top of the mid-sagittal suture-arrows (Figure 2,b). Another 3D reconsruction CT scan confirmed the billateral closure of the sequamosal suture (Figure 2,c).
3.2. Family 2
A- 10-year-old- boy received the diagnosis of West syndrome at the age of 3-years and was referred to our department because of torticollis. Clinical examination showed growth defieciency (10 th percentile). Craniofacial asymmetry was a noticeable clinical feature. Examining the skull, we noticed asymmetrical massive boney ridges over the lambdoid sutures with apparent but asymmetrical bulging of the occiput. The asymmetry was marked over the left partion of the left lambdoid causing a bigger cranial compartment of the lft over the right side of the occiput. 3D axial reconstruction CT scan illustrated the asymmetry of the posterior cranial bones along the lambdoid sutures. Intresetingly, his 28 year-old mother was aclient at the department of spine surgery since she was 14 years-old. 3D reconstruction CT scan of the mother showed noticeable boney ridge extends from the metopic suture upwards to involve the sagittal suture (red arrow heads. The balck arrow showed a well demarcated boney ridge over the squamosal suture (Figure 3,b). 3D reconstruction CT scan of the skull and spine showed the thick boney ridge of the metopic and the anterior sagittal as well as bilateral involvement of the squamosal causing apperant anterior narrowing of the craniofacial contour. Note the lumbar scoliosis (Figure 3,c).
3.3. Family 3
A-12-year-old-boy with the diagnosis of West syndrome was referred to our department because of early onset osteoarthritis. Interestingly the child's craniofacial contour resembles his 38-year-old-mother.
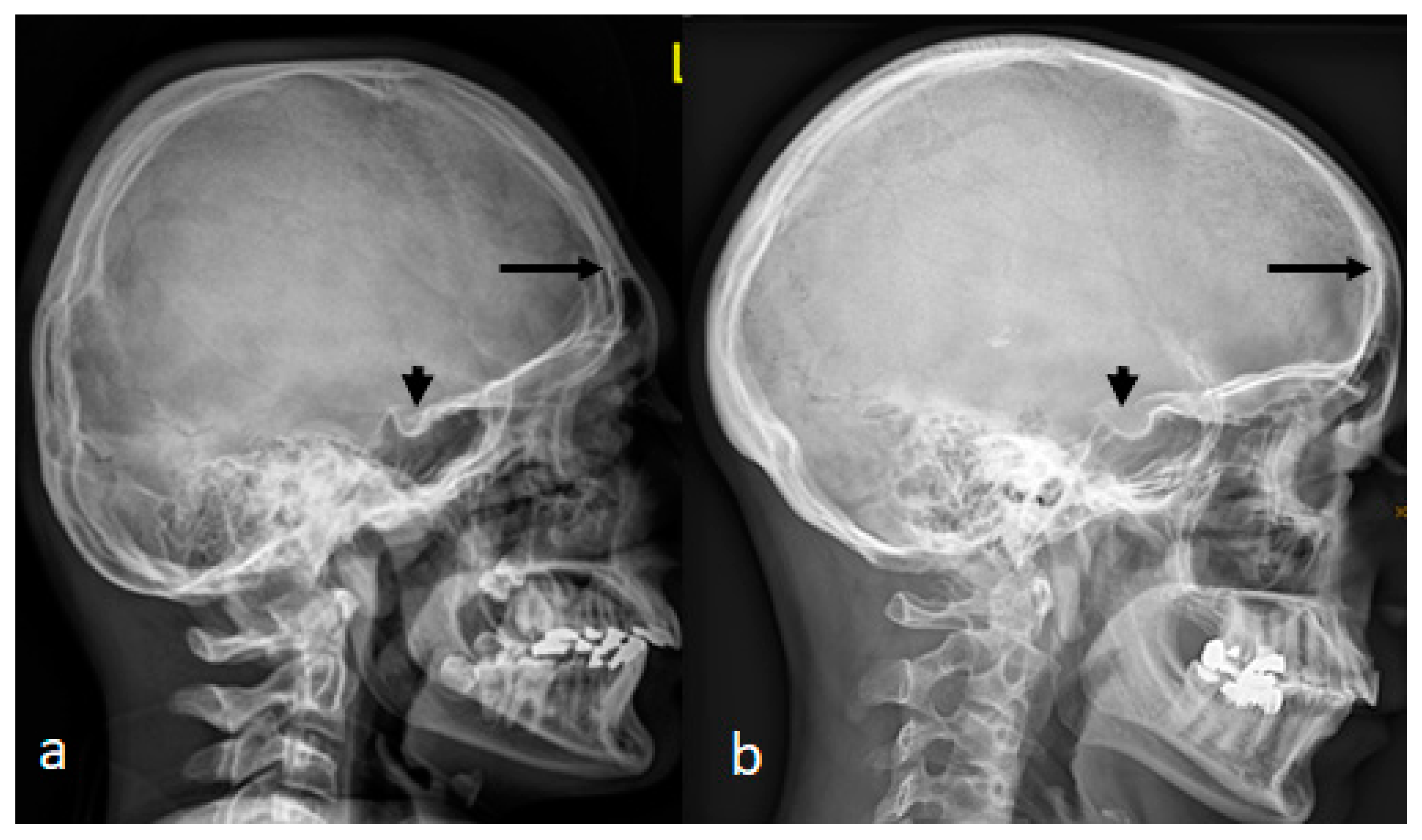
Lateral skull radiograph of a-12-year-old-boy with West syndrome showed premature sutural fusion begets an abnormal growth pattern, resulting in cranial deformity. The nature of the deformity depends on which sutures are involved, the time of onset and the sequence in which individual sutures fuse. In this child brachycephalic secondary to craniosynostosis which occurred because of bilateral early ossification of the coronal sutures leads to bi-coronal craniosynostosis. Note the ossified interclinoid ligament of the sella turcica (Figure 4,a). Lateral skull radiograph of a -38-year-old-mother with a history of poor schooling achievements showed almost very similar cranial contour of brachycephaly and massive ossification of the clinoid ligament of the sella turcica. Maternal history revealed a history of multiple spontaneous miscarriages in the first trimester of more than 5 times.
4. Discussion
West syndrome is a well-known sub-variety of infantile spasm syndrome and considered the most common.
The age of onset of West syndrome is variable (can occurs between the early months of life to early child hood). West syndrome patients are manifesting a constellation of three main diagnostic elements of cryptogenic epileptic spasms, awkward deceleration of development/intellectual disability (though it can be within normal limits) as well as interictal EEG pattern (fragmented hypsarrhythmia). The etiology understanding is a decisive and a paramount basic tool from which the route of the natural history of the disease can be comprehended [22,23].
Previous studies described the genetic background of West syndrome as being vast and correlated with diverse forms of genetic background.
Bruyere et al, performed a multi-generational- family-study in Canada, they observed the occurrence of West syndrome in boys, though the mothers showed no signs. They confirmed their study as West syndrome is an X-linked recessively inherited disorder (mapped to Xp11.4-Xp22.11 [24].
Claes et al, studied the genetic marker in two families with West syndrome and described the disorder as X-linked West syndrome mapped to to Xp21.3-Xp22.1 [25].
Stromme et al, further described ARX gene mutation coding for an aristaless-related homeobox protein. A polyalanine expansion was encountered in the aforementioned families as described by Bruyere et al, and Claes et al, and compared to a previous study by Stromme et al [26,27].
Stromme and co-workers studied the clinical data from fifty intellectually disabled patients with ARX mutation. They concluded that seizures were encountered in 29 patients, also one family with a novel myoclonic epilepsy syndrome associated with a missense mutation. Seventeen patients had infantile spasms. Other phenotypes were variable and ranged between mild to moderate intellectual disability. Some of the patients with intellectual disability showed dystonia, ataxia and also autism [28].
Scheffer et al, published an Australian family manifested ARX gene mutation. The family presented with seizures and developmental retardation. The findings in this family showed spasticity and the carrier females had hyperreflexia. The authors have decided to name this condition ( X-linked recessive myoclonic epilepsy with spasticity and intellectual disability in boys XMESID) [29].
Elia et al, described 3 boys with early-onset intractable epilepsy (drug resistant myoclonic, tonic or infantile spasms) with profound intellectual disability and CDKL5 mutations [30].
Interestingly CDKL5 mutations were confirmed in a girl and boy patients who gave features of Rett syndrome [31,32].
Striano et al, described two West syndrome patients with duplications of 14q12, including FOXG1 who showed no X-linked recessive trait [33].
Yuskaitis et al, assessed the clinical phenoytpe /genotype of 131 patients with idiopathic type of infantile spasm. Through retrospective analysis of the medical records, imaging and EEG results. They focussed on main two elements of retarded development and the associated seizures as the foremost key factors in patients with infantile spasm of unknown etiology [34].
None of the above mentioned studies described the cranial and the skeletal development of individuals and parents with West syndrome and most of the studies emphasized heavily on the genetic markers of the disease.
5. Conclusion
The significance of diagnosing children/adults with long term ailment is to establish a well structured management. The clinical /radiological phenotype are the main indices that guide the physician towards a definite diagnosis. Aiming to obtain optimal level of etiological understanding is a top requierment to overcome any emotional or psychosomatic complications for both the children and their families. If any skeletal or extra-skeletal abnormality is present, it should be carefully studied and evaluated via comprehending its nature, severity, the degree of disability anticipated, and the efficacy of treatment. In all types of disabilities, treatment solely depends on definite diagnosis. The patient should be evaluated as a whole, his physical potential should be determined as it represents an important element to approach the diagnosis. Disabilities of the musculoskeletal system encompass a broad spectrum of etiological backgrounds. The final objective in any diagnostic process is to approach what has been called the “Precise classification” of disabilities. The latter can never be achieved unless the clinician succeeded in connecting the disability to one of the etiological backgrounds, osteogenic, neurogenic, myogenic, or stemmed from other different reasons. We wish to point out that the main limitation in our study is the small number of patients with the diagnosis of West syndrome. Neveretheless, we believe that the results of our findings can be used as an impactful inducement for further impingement to clarify the etiological understanding in children with the idiopathic type of West syndrome. We stress that the necessity of correlating the clinical phenotype via precise conduct of high quality clinical and investigative efforts. Despite the limited number of children and parents in this study, the abnormal cranial contour in children with West syndrome can be considered accountable for future assessment
6. Patents
Non contributory
Author Contributions
AAK conceptualization and methodology; validation, AAK., FG, FBC, VK.; formal analysis, AKK, SR, HAK, SGK.; investigation, FBC, SGK; data curation, VD, SR, FG; writing— original draft preparation, AKK.; writing—review and editing, FG.; visualization, AKK.; supervision, AKK. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by Ethics Committee of the (Ilizarov Scientific Research Institute, No. 4(50)/13.12.2016, Kurgan, Russia). Informed consents were obtained from the patient’s Guardians. Informed Consent Statement: A signed consent form was obtained from the patient’s Guardians.
Acknowledgments
We wish to thank Dr. Rainer Wunn, Institut for CT und MRI am Schillerpark –Linz, Austria for the preperation of high standard tomographic images. Also we aknowledge the collaboration of the families and the guardians of the patients.
Conflicts of Interest
The authors declare no conflict of interest.
References
- West WS. On a particular form of infantile convulsions. Lancet. 1841, 1, 724–725.
- Shields WD. Infantile spasms: little seizures, BIG consequence. Epilepsy Curr. 2006, 6, 63–69. [CrossRef] [PubMed]
- Aicardi J, Chevrie JJ, Rousselie F. Le syndrome spasmes en flexion, agenesie calleuse, anomalies chorio-retiniennes. Arch Fr Pediatr 1969, 26, 1103–1120.
- Aicardi J. Aicardi syndrome. Brain Dev 2005, 27, 164–171. [CrossRef]
- Yu JT, Culican SM, Tychsen L. Aicardi-like chorioretinitis and maldevelopment of the corpus callosum in congenital lymphocytic choriomeningitis virus. J AAPOS 2006, 10, 58–60. [CrossRef] [PubMed]
- Glasmacher MAK, Sutton VR, Hopkins B, et al. Phenotype and management of Aicardi syndrome: new findings from a survey of 69 children. J Child Neurol 2007, 22, 176–184. [CrossRef]
- Schinzel A, Giedion A. A syndrome of severe midface retraction, multiple skull anomalies, clubfeet, and cardiac and renal malformations in sibs. Am J Med Genet 1978, 1, 361–375. [CrossRef]
- Grosso S, Pagano C, Cioni M, Di Bartolo RM, Morgese G, Balestri P. Schinzel-Giedion syndrome: a further cause of West syndrome. Brain Dev 2003, 25, 294–8. [CrossRef] [PubMed]
- Minn D, Christmann D, De Saint-Martin A, Alembik Y, Eliot M, Mack G, Fischbach M, Flament J, Veillon F, Dollfus H. Further clinical and sensorial delineation of Schinzel-Giedion syndrome: Report of two cases. Am J Med Genet 2002, 109, 211–217. [CrossRef]
- Sotos JF, Dodge PR, Muirhead D, et al. Cerebral gigantism in childhood. New Engl J Med 1964, 271, 109–116.
- Sotos JF, Cutler E. Cerebral gigantism. Am J Dis Child 1977, 131, 625–627.
- Schaefer GB, Bodensteiner JB, Buehler BA, Lin A, Cole TRP. The neuroimaging findings in Sotos syndrome. Am J Med Genet 1997, 68, 462–465.
- Ray M, Malhi P, Bhalla AK, Singhi PD. Cerebral gigantism with West syndrome. Indian Pediatr. 2003, 40, 673–675.
- Wit JM, Beemer FA, Barth PG, et al. Cerebral gigantism (Sotos syndrome). Compiled data of 22 cases. Analysis of clinical features, growth and plasma somatomedin. Eur J Pediatr 1985, 144, 131–14. [CrossRef] [PubMed]
- Alexander WS. Progressive fibrinoid degeneration of fibrillary astrocytes associated with mental retardation in a hydrocephalic infant. Brain 1949, 72, 373–381. [CrossRef]
- Borrett D, Becker LE. Alexander's disease: a disease of astrocytes. Brain 1985, 108, 367–385.
- Lee JM, Kim SJ, Lee SJ. A case of infantile spasms Alexander disease accompanied by infantile spasms diagnosed by DNA analysis. J Korean Med Sci. 2006, 21, 954–957. [CrossRef]
- Deprez M, D'Hooge M, Misson JP, et al. Infantile and juvenile presentations of Alexander's disease: a report of two cases. Acta Neurol Scand 1999, 99, 158–165. [CrossRef] [PubMed]
- Salar S, Moshé SL, Galanopoulou AS. Metabolic etiologies in West syndrome. Epilepsia Open. 2018, 3, 134–166. [CrossRef] [PubMed]
- Naito E, Ito M, Yokota I. Gender-specific occurrence of West syndrome in patients with pyruvate dehydrogenase complex deficiency. Neuropediatrics. 2001, 32, 295–298.
- Dreifuss FE. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia. 1981, 22, 249–260.
- Dulac, O. What is West syndrome? Brain Dev. 2001, 23, 447–52. [CrossRef] [PubMed]
- Lux AL. Latest American and European updates on infantile spasms. Curr Neurol Neurosci Rep. 2013, 13, 334–341. [CrossRef]
- Bruyere H, Lewis MES, Wood S. Cofirmation of linkage in X-linked infantile spasms (West syndrome) and refinement of the disease locus to Xp21.3-Xp22.1. Clin Genet 1999, 55, 173–181. [CrossRef] [PubMed]
- Claes S, Devriendt K, Lagae L, et al. The X-linked infantile spasms syndrome (MIM 308350) maps to Xp11.4-Xpter in two pedigrees. Ann Neurol 1997, 42, 360–364. [CrossRef] [PubMed]
- Stromme P, Mangelsdorf ME, Scheffer IE, Gecz J. Infantile spasms, dystonia, and other X-linked phenotypes caused by mutations in Aristaless related homeobox gene, ARX. Brain Dev 2002, 24, 266–8. [CrossRef]
- Stromme P. ARX and other single genes in X-linked mental retardation: revisiting a population-based study. J Pediatr Neurol 2005, 3, 121–122.
- Stromme P, Mangelsdorf ME, Shaw MA, Lower KM, Lewis SM, Bruyere H, Lutcherath V, Gedeon AK, Wallace RH, Scheffer IE, Turner G, Partington M, Frints SG, Fryns JP, Sutherland GR, Mulley JC, Gecz J. Mutations in the human ortholog of Aristaless cause X-linked mental retardation and epilepsy. Nature Genetics 2002, 30, 441–5.
- Scheffer IE, Wallace RH, Phillips FL, Hewson P, Reardon K, Parasivam G, Stromme P, Berkovic SF, Gecz J, Mulley JC. X-linked myoclonic epilepsy with spasticity and intellectual disability: mutation in the homeobox gene ARX. Neurology 2002, 59, 348–56. [CrossRef]
- Elia M, Falco M, Ferri R, et al. CDKL5 mutations in boys with severe encephalopathy and early-onset intractable epilepsy. Neurology 2008, 71, 997–999. [CrossRef]
- Bahi-Buisson N, Nectoux J, Rosas-Vargas H, et al. Key clinical features to identify girls with CDKL5 mutations. Brain 2008, 131, 2647–2661. [CrossRef] [PubMed]
- Castren M, Gaily E, Tengstrom C, et al. Epilepsy caused by CDKL5 mutations. Eur J Ped Neurol 2011, 15, 65–69. [CrossRef] [PubMed]
- Striano p, Paravidino R, Sicca F, et al. West syndrome associated with 14q12 duplications harboring FOXG1. Neurology 2011, 76, 1600–1602. [CrossRef] [PubMed]
- Yuskaitis CJ, Ruzhnikov MRZ, Howell KB, Allen IE, Kapur K, Dlugos DJ, Scheffer IE, Poduri A, Sherr EH. Infantile Spasms of Unknown Cause: Predictors of Outcome and Genotype-Phenotype Correlation. Pediatr Neurol. 2018, 87, 48–56. [CrossRef] [PubMed]
Figure 1.
AP Skull radiograph of a-7-year-old boy with West syndrome showed facial asymmetry with early closure of the metopic suture and other sutures seemed ill-defined (Figure 1,b). 3D reformatted frontal cranial CT of a-35-years-old- mother clearly showed the closure of the metopic and the sagittal sutures causing a mid sagittal boney bulge (red arrow) (Figure 1,b).
Figure 1.
AP Skull radiograph of a-7-year-old boy with West syndrome showed facial asymmetry with early closure of the metopic suture and other sutures seemed ill-defined (Figure 1,b). 3D reformatted frontal cranial CT of a-35-years-old- mother clearly showed the closure of the metopic and the sagittal sutures causing a mid sagittal boney bulge (red arrow) (Figure 1,b).
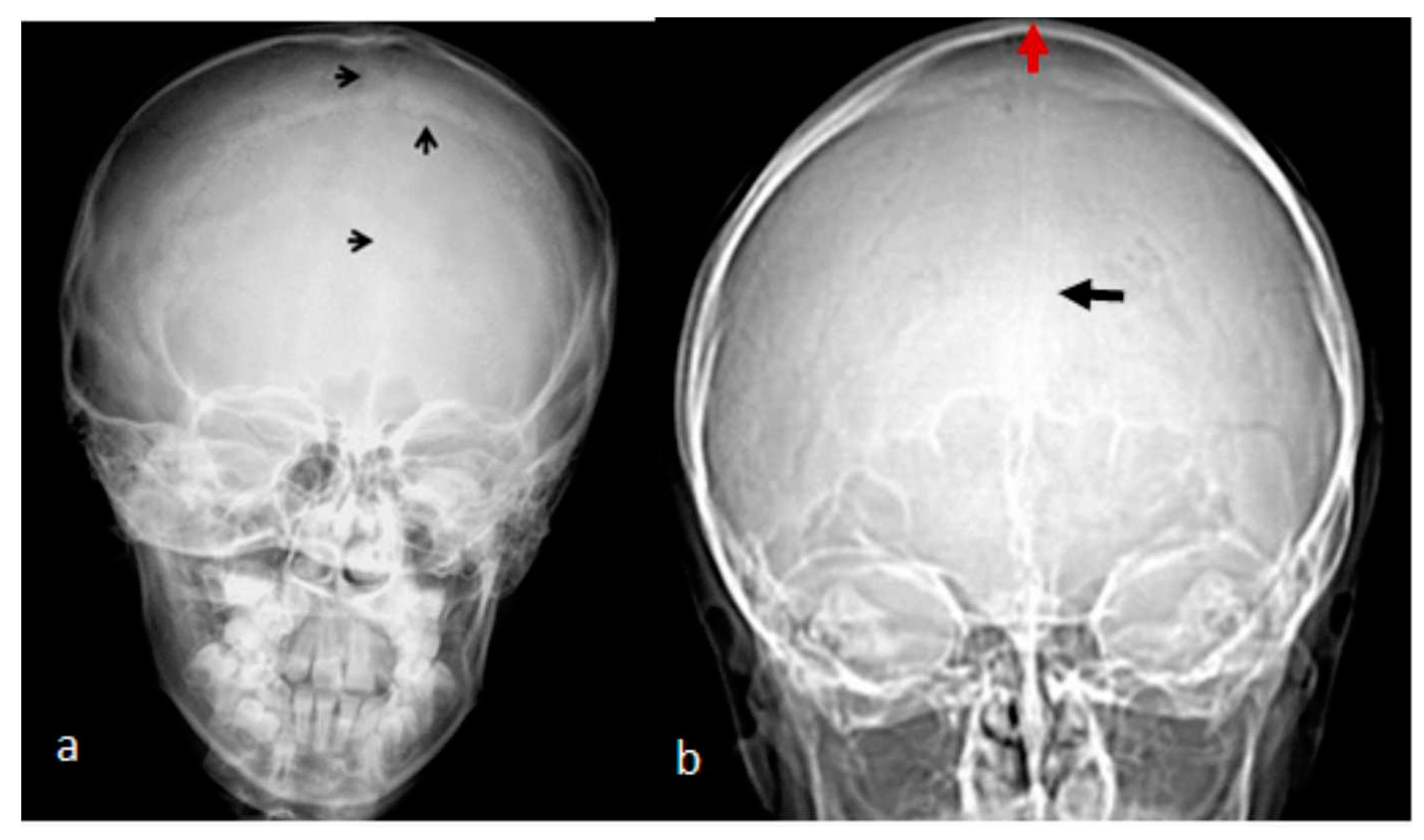
Figure 2.
3D reconstruction CT scan of the skull of a-7year-old –boy with West syndrome showed closure of the metopic suture -arrow(a). 3D reconstruction CT scan showed early closure of the sequamosal sutures pressing the brain contents upward causing the development of a prominent bulge at the top of the mid-sagittal suture-arrows (b). Another 3D reconsruction CT scan confirmed the billateral closure of the sequamosa suture (c).
Figure 2.
3D reconstruction CT scan of the skull of a-7year-old –boy with West syndrome showed closure of the metopic suture -arrow(a). 3D reconstruction CT scan showed early closure of the sequamosal sutures pressing the brain contents upward causing the development of a prominent bulge at the top of the mid-sagittal suture-arrows (b). Another 3D reconsruction CT scan confirmed the billateral closure of the sequamosa suture (c).
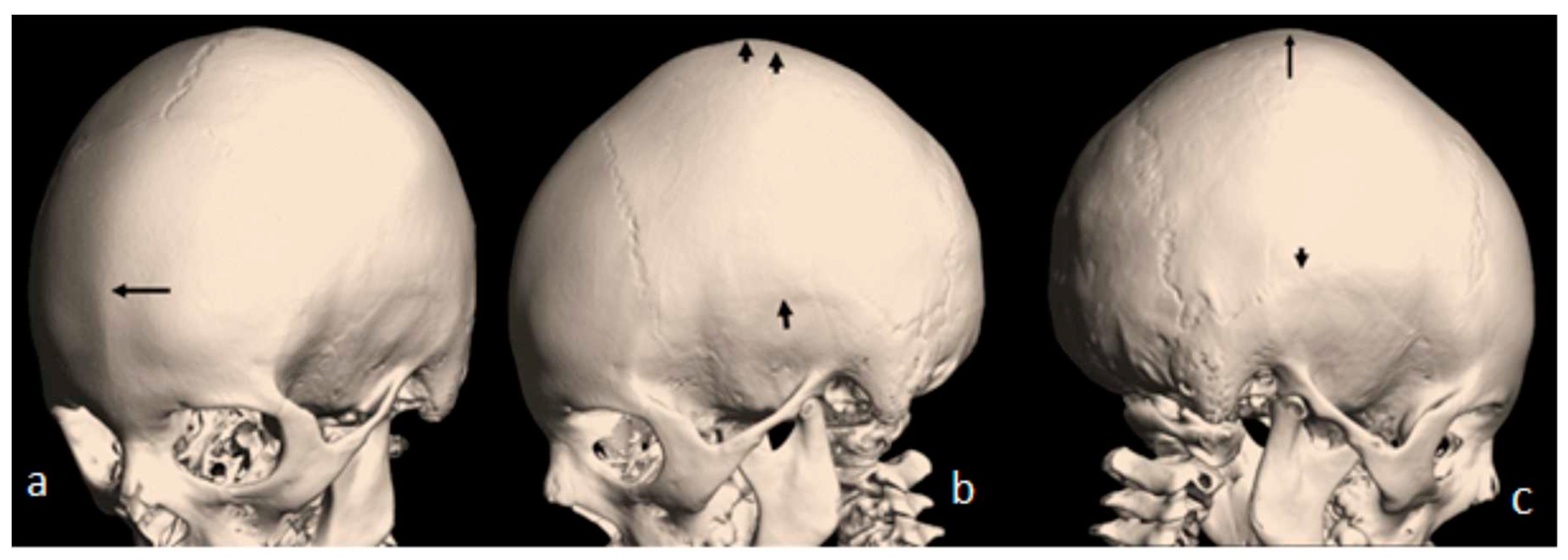
Figure 3.
3D axial reconstruction CT scan of a-10-year-old-boy with West syndrome illustrated the asymmetry of the posterior cranial bones along the lambdoid sutures. Intresetingly, his 28 year-old mother was aclient at the department of spine surgery since she was 14 years-old. 3D reconstruction CT scan of the mother showed noticeable boney ridge extends from the metopic suture upwards to involve the sagittal suture (red arrow heads. The balck arrow showed a well demarcated boney ridge over the squamosal suture (Figure 3,b). 3D reconstruction CT scan of the skull and spine showed the thick boney ridge of the metopic and the anterior sagittal as well as bilateral involvement of the squamosal causing apperant anterior narrowing of the craniofacial contour. Note the lumbar scoliosis (Figure 3,c).
Figure 3.
3D axial reconstruction CT scan of a-10-year-old-boy with West syndrome illustrated the asymmetry of the posterior cranial bones along the lambdoid sutures. Intresetingly, his 28 year-old mother was aclient at the department of spine surgery since she was 14 years-old. 3D reconstruction CT scan of the mother showed noticeable boney ridge extends from the metopic suture upwards to involve the sagittal suture (red arrow heads. The balck arrow showed a well demarcated boney ridge over the squamosal suture (Figure 3,b). 3D reconstruction CT scan of the skull and spine showed the thick boney ridge of the metopic and the anterior sagittal as well as bilateral involvement of the squamosal causing apperant anterior narrowing of the craniofacial contour. Note the lumbar scoliosis (Figure 3,c).
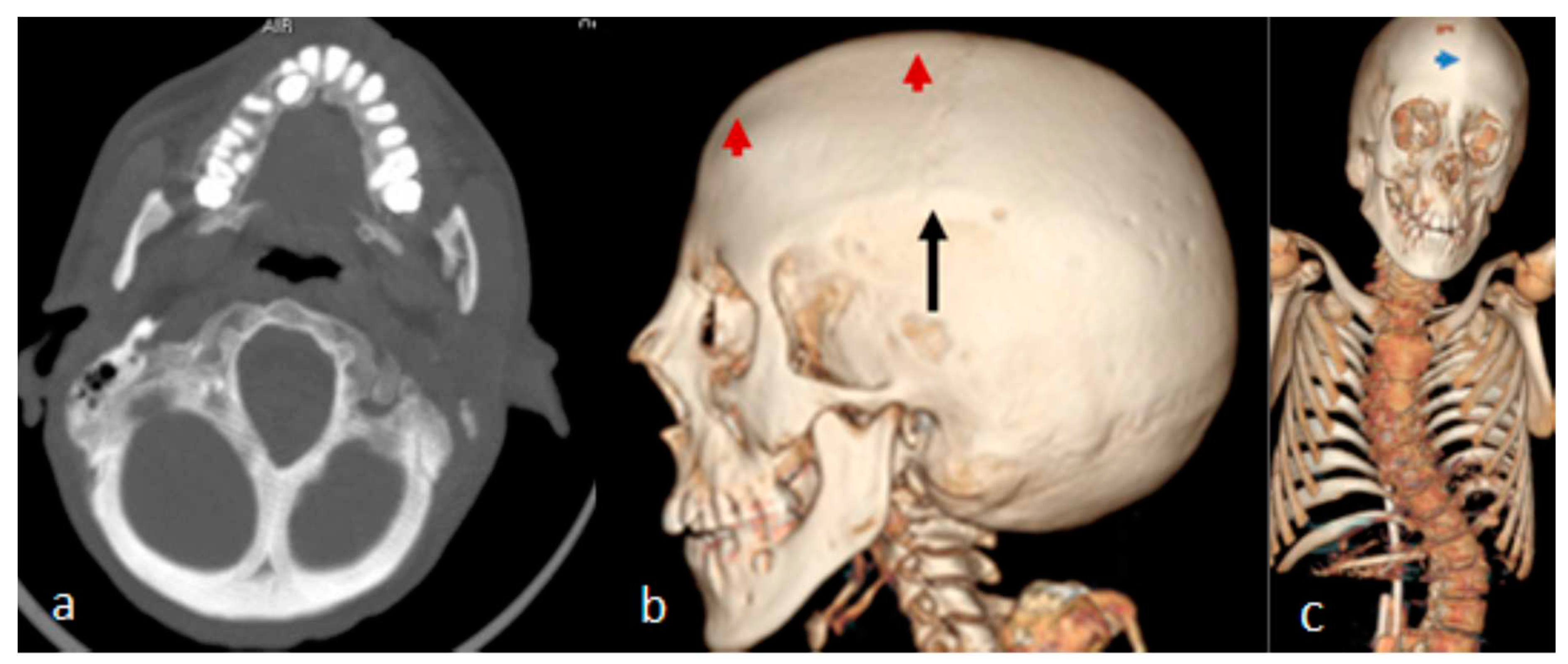
Figure 4.
Lateral skull radiograph of a-12-year-old-boy with West syndrome showed premature sutural fusion begets an abnormal growth pattern, resulting in cranial deformity. The nature of the deformity depends on which sutures are involved, the time of onset and the sequence in which individual sutures fuse. In this child brachycephalic secondary to craniosynostosis which occurred because of bilateral early ossification of the coronal sutures leads to bi-coronal craniosynostosis. Note the thickened frontal bones (arrow) and the ossified interclinoid ligament of the sella turcica (arrow) (a). Lateral skull radiograph of a -38-year-old-mother with a history of poor schooling achievements showed almost very similar cranial contour of brachycephaly, thickening of the frontal bones (arrow) and massive ossification of the clinoid ligament of the Sella turcica (arrow head). Maternal history revealed a history of multiple spontaneous miscarriages in the first trimester of more than 5 times (b).
Figure 4.
Lateral skull radiograph of a-12-year-old-boy with West syndrome showed premature sutural fusion begets an abnormal growth pattern, resulting in cranial deformity. The nature of the deformity depends on which sutures are involved, the time of onset and the sequence in which individual sutures fuse. In this child brachycephalic secondary to craniosynostosis which occurred because of bilateral early ossification of the coronal sutures leads to bi-coronal craniosynostosis. Note the thickened frontal bones (arrow) and the ossified interclinoid ligament of the sella turcica (arrow) (a). Lateral skull radiograph of a -38-year-old-mother with a history of poor schooling achievements showed almost very similar cranial contour of brachycephaly, thickening of the frontal bones (arrow) and massive ossification of the clinoid ligament of the Sella turcica (arrow head). Maternal history revealed a history of multiple spontaneous miscarriages in the first trimester of more than 5 times (b).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



