
Submitted:
07 December 2023
Posted:
08 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
(1) Background: Until December 2021, French Guiana (FG), located in South America, faced four consecutive COVID-19 epidemic waves. This study sought to analyze the mortality trend of severe COVID-19 patients admitted to the referral ICU of FG. (2) Methods: We conducted a prospective, observational, and non-interventional study in ICU at Cayenne Hospital. We included 383 patients older than 18 admitted with SARS-CoV-2-related pneumonia hospitalized from May 2020 to December 2021. The study covers three periods. Period 1 (Waves 1 and 2, original variant), period 2 (Wave 3, gamma variant), and period 3 (Wave 4, delta variant). (3) Results: The median age was 63 years (52-70). Frailty was diagnosed in 36 patients over 70 (32.4%). Only 4.8% of patients were vaccinated. The median ICU LOS was 10 days (6-19). Hospital mortality was 37.3%. It was 30.9% in period 1, 36.6% in period 2 (p=0.329 vs. period 1), and 47.1% in period 3 (0.015 vs. period 1). In multivariate analysis, independent factors associated with hospital mortality were age more than 40 years (]40-60 years] OR=5.2, 95%CI: 1.4-19.5; (]60-70 years] OR=8.5 95%CI: 2.2-32; (]70+ years] OR=17.9, 95%CI: 4.5-70.9), frailty (OR=5.6, 95%CI: 2.2-17.2), immunosuppression (OR=2.6, 95%CI: 1.05-6.7), and MV use (OR=11, 95%CI: 6.1-19.9). This model had an overall sensitivity of 72%, a specificity of 80.4%, a positive predictive value of 68.7%, and a negative predictive value of 82.8%. (4) Conclusions: The mortality of severe COVID-19 patients in French Amazonia was higher during the delta variant wave. This over-death is explained by the virulence of the responsible SARS-CoV-2 variant and the under-vaccination coverage of the studied population.
Keywords:
COVID-19
; delta variant
; gamma variant
; mortality
; French Guiana
1. Introduction
The first COVID-19 epidemic wave was declared in French Guiana (FG) in South America in May 2020. Until December 2021, FG faced four waves of SARS-CoV-2 epidemic. The first wave was delayed from that encountered in mainland France, and its peak was reached gradually within five weeks. This allowed for increasing the healthcare system preparedness, surging the intensive care bed capacity, and training medical and non-medical teams. It also allowed the benefit of national solidarity aid regarding equipment and human resources.
SARS-CoV-2 waves in FG were declared when the incidence density in the community exceeded a threshold of 150 infected cases/100,000 inhabitants or when the dominant variant changed [1]. Accordingly, patients’ characteristics and outcomes can vary from wave to wave. Many studies have described the characteristics of patients with COVID-19 [2,3,4]. They have investigated outcomes, especially among older and vulnerable populations [5,6]. In some studies, the mortality rate reached 60% [7,8] and decreased over time, mainly because of vaccination coverage [9,10]. The main factors associated with increased mortality were age>55, pre-existing comorbidities, acute respiratory distress syndrome, extensive lung involvement in computed tomography findings, and organ failure [9,11].
Complete vaccination for SARS-CoV-2 showed protective effectiveness in saving lives, mainly when the vaccine coverage rate exceeds 60% [12,13]. Tenforde et al., in a large case-control study of adults hospitalized for COVID-19, showed that complete vaccination reduces progression to death or invasive mechanical ventilation [14]. In FG, the Pfizer-BioNTech COVID-19 vaccine has been rolled out for free by the local sanitary authorities since January 2021. Unfortunately, there was a high rate of vaccine hesitancy with a low coverage rate in the local population. This may have driven a higher rate of hospitalizations, ICU admissions, and over-deaths [15].
The primary objective of this study was to describe the mortality trend related to severe COVID-19 in an under-vaccinated population in French Amazonia. The secondary objective was to investigate factors associated with mortality in these patients.
2. Materials and Methods
Our study is prospective, observational, and non-interventional. It was conducted from May 01, 2020, to December 31, 2021, in the ICU at Cayenne General Hospital. We included all patients older than 18 admitted with COVID-19 pneumonia. We excluded patients with positive SARS-CoV-2 screening without respiratory symptoms. Only the first ICU admission during the same hospital stay was considered.
Our unit is the referral ICU in FG [16]. It works per European and French standards. The initial ICU capacity accounted for 11 beds. It was increased to 41 beds during the crisis with a consequent surge in human resources and equipment needs.
The management protocol of severe COVID-19 pneumonia associated High Flow Nasal Cannula Oxygen (HFNCO), non-invasive mechanical ventilation (NIV), invasive mechanical ventilation (MV), and prone position in sedated and non-sedated patients. We used therapeutic anticoagulation with Heparin (target anti-Xa at 0.4-0.6 UI/ml). This regimen was changed in September 2021 to pharmacologic thromboprophylaxis [17]. Dexamethasone was used with an initial protocol similar to Villar et al. (20 mg daily for 5 days followed by 10 mg daily for 5 days) [18] and changed to 6 mg daily for 10 days in August 2020 [19]. Systematic antimicrobial therapy by cefotaxime alone or in combination with levofloxacin was prescribed at admission to ICU till September 2020. Antibiotics were then reserved only for documented infections.
Data were collected in a datasheet, and patients were referred by numbers to grant privacy protection. The following parameters were collected: gender, age, BMI score, simplified acute physiology score (SAPS II) [20], organ failure [21], comorbidities, frailty [22], the management strategy (respiratory support, vasopressors, renal replacement therapy, etc.), and outcome (ICU and hospital length of stay (LOS) and mortality).
The waves’ dates were defined by the local sanitary authority according to epidemiological data on the responsible strain [1]. In our study, we classified the four epidemic waves in three periods as follows:
- − Period 1 (Waves 1 and 2): from May to September 2020, and from November 2020 to February 2021 caused by the original SARS-CoV-2 strain.
- − Period 2 (Wave 3): from March to July 2021, caused by gamma (P.1) and alpha (B.1.1.7) variants circulation (88% and 12%, respectively).
- − Period 3 (Wave 4): from August to December 2021, caused by delta (B.1.617) and gamma (P.1) variants circulation (78% and 21%, respectively).
We calculated the weekly occupancy rates (WOR), defined as the number of hospitalized patients (COVID and non-COVID) divided by the number of ICU bed capacity during the considered week (cumulative number of daily open beds during the week). Occupancy rate per period was calculated as the mean WOR during the studied period.
Results are reported as number of patients in whom the data was recorded (Nb), median and inter-quartile range (IQR:1st–3rd quartiles), or numbers with percentages. Initial bivariate statistical comparisons for categorical variables were conducted using the Chi-square or Fisher’s exact test. Continuous variables were compared using the Mann–Whitney U-test. We used multivariable logistic regression to identify patients’ characteristics associated with hospital death. Non-redundant variables selected by bivariate analysis (p ≤ 0.05) and considered clinically relevant were entered into the logistic regression model. Postestimation commands allowed for obtaining the sensitivity and specificity of the model and the area under the curve. Kaplan Meier analysis was used to estimate the survival function. Results are expressed as odds ratios (OR) with 95% confidence intervals (95%CI). Statistical tests were two-tailed, and p ≤0.05 was considered significant.
Statistical analyses were carried out with Excel (2010 Microsoft Corporation, Redmond, USA) and IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, N.Y., USA), and STATA (STATA Corp., Texas, USA).
3. Results
During the study period, 1073 patients were admitted to ICU. SARS-CoV-2 screening was positive in 409 patients, and 383 suffered from COVID-19 pneumonia (Figure 1). The median WOR was 90.6% (IQR: 74.3-104.7) (Figure 2). It was 85.1% (IQR: 67.6-109.8) in period 1, 89.5% (IQR: 83.4-97) in period 2 (p = 0.723 compared to period 1), and 101.9% (IQR: 81.9-107.8) in period 3 (p = 0.247 compared to period 1).
3.1. Demographic characteristics and comorbidities
The number of patients hospitalized for COVID-19 pneumonia was 110 during the first period, 161 during the second, and 104 during the third period. The vaccination rate (at least 1 dose) was 4.8% (18/373) and a complete vaccination (2 doses) was registered in only 4 patients. It was zero during period 1, 6.4% (10/157) during period 2, and 8.2% (8/98) during period 3. Overall (383 patients), the median age was 63 years (IQR: 52-70), and 208 patients (54.3%) were male gender. Patients were aged more than 70 in 111 cases (29%). The median age was 63 years (IQR: 53-70) in men and 54 (IQR: 54-73) in women (p = 0.223). BMI was 30 kg/m2 (IQR: 26-33) in men and 32 (IQR: 28-36) in women (p = 0.043). Frailty was diagnosed in 36 patients aged more than 70 (32.4%) and in 6 patients (4.8%) aged 60 to 69. The most registered comorbidities were arterial hypertension (61.4%), obesity (49.1%), and diabetes (42.3%). These comorbidities were concomitant in 75 patients (19.6%). The time between the onset of symptoms and hospitalization was 7 days (IQR: 4-9). At admission to ICU, 179 patients (46.7%) received HFNCO, 102 (26.6%) received HFNCO+NIV, 6 (1.5%) received NIV, and 96 (25.1%) received MV. The maximal respiratory support used during ICU stay was MV in 48.3% (+92.7%) and HFNCO in 36% of cases (-22.9%) (Table S1).
The analysis of period two compared to period one showed a lower SAPS II, a lower rate of male gender, diabetes mellitus, MV use, and RRT use; and a higher rate of NIV use. The analysis of period three compared to period one showed a lower rate of male gender, MV use, and RRT use; and a higher rate of NIV use. The time from admission to MV was longer in period 3. (Table S1).
3.2. Outcome
ICU LOS was 10 days (IQR: 6-19). It was 9 days (IQR: 6-15) in survivors and 14 (IQR: 7-23) in non-survivors (p = 0.003). It was equal to or higher than 30 days in 47 cases (12.3%). Hospital LOS was 18 days (IQR: 12-29). It was higher in survivors (17 vs. 18, p = 0.010). Deceased patients were more severe at admission (SAPS II at 33 vs. 29, p<0.001) and more likely to receive MV (93.6%, p = 0.003) (Table S2). ICU and hospital LOS were lower in period 2. Hospital mortality was higher in period 2 but without statistically difference (30.9% vs. 36.6% in period 1, p = 0.329). The ICU and hospital LOS were lower, and the hospital mortality rate was higher during period 3 (30.9% vs. 47.1% in period 1, p = 0.015) (Table S3).
ICU mortality rate was 36%, and hospital mortality was 37.3%. The causes of death were septic shock in 67 cases (46.9%), refractory hypoxemia in 53 cases (37.1%), probable pulmonary embolism in 11 cases (7.7%), myocardial infarction in 6 cases (4.2%), cardiogenic shock in 2 cases (1.4%), hemorrhagic shock in 2 cases (1.4%), hemorrhagic stroke in 1 case, and decompensated liver cirrhosis in 1 case. In 54 cases (37.8%), withholding or withdrawing life-sustaining support was decided. Hospital mortality in frail patients was 71.4%. Hospital mortality was 30.9% in period 1, 36.6% in period 2 (p = 0.329 vs. period 1), and 47.1% in period 3 (p = 0.015 vs. period 1) (Figure 3). There was a significant relationship between hospital mortality and patients’ age (r2 = 0.883, p<0.001) (Figure 4). ICU and hospital LOS were more prolonged, and hospital mortality was higher in patients receiving MV regardless of the study period (Table 1).
Factors associated with hospital mortality in univariate analysis are reported in Table S2. The main parameters were age, frailty, severity at admission (SAPS II), comorbidities (hypertension, diabetes, chronic renal failure, and immunosuppression), organ failure at ICU admission (hemodynamic, neurologic, and renal), and MV use. Multivariate analysis including these variables in the model found that older age groups were at much greater risk than those aged 40 years or less ([40-60 years] OR = 5.2, 95%CI: 1.4-19.5, p = <0.001; ([60-70 years] OR = 8.5 95%CI: 2.2-32, p = 0.002; ([70+ years] OR = 17.9, 95%CI: 4.5-70.9, p<0.001), frailty (OR = 5.6, 95%CI: 2.2-17.2, p<0.001), immunosuppression (OR = 2.6, 95%CI: 1.05-6.7, p = 0.04), and MV use (OR = 11, 95%CI: 6.1-19.9, p<0.001) as factors independently associated with hospital mortality. The above model had an overall sensitivity of 72%, a specificity of 80.4%, a positive predictive value of 68.7%, and a negative predictive value of 82.8%. The area under the ROC curve was 0.843.
4. Discussion
Our study describes the epidemiology and mortality trend of severe COVID-19 patients admitted to ICU during four epidemic waves in an under-vaccinated population in French Amazonia. It shows that the mortality rate increased from wave to wave. Age, frailty, immunosuppression, and MV use are independently associated with hospital mortality.
The rapid progression of COVID-19 has put hospitals under significant pressure. To deal with the crisis, emergency and intensive care physicians were forced to select patients, a process called “triage” [23,24]. Patients were categorized based on age and previous physiological status [22]. Overall, patients’ admission to ICU and outcomes were influenced by the severity of the disease, comorbidities, and ICU bed availability. In FG, due to the epidemic spread, we increased the ICU bed capacity, and we created new ICUs in the other two hospitals in the department called “ephemeral ICU beds”. As a result, there was no need for “triage” in our hospital. However, the average occupancy rate was 90.6%, without a difference between the periods. In this context, it is well described that surging ICU during COVID-19 pandemic can be associated with a lower quality of care and a greater risk of death [25].
Several studies investigated mortality in COVID-19 patients at 28 [19], 30 [26,27], and 90 days [9,28] from ICU admission. While others have focused on ICU and hospital mortality [27,29]. In our study, we assessed the hospital mortality of severe COVID-19 patients. Indeed, 45 patients (11.7%) were hospitalized in ICU for more than 30 days, and 22 deceased patients were still alive on day 30. In addition, patients hospitalized for more than 30 days were the most severe at admission and were most often under MV. Accordingly, assessing mortality at 30 days from ICU admission can underestimate the potentially unfavorable outcome.
At the beginning of the COVID-19 crisis, the mortality rate was as high as 60% [7,8] and reached 70.3% in patients receiving MV [30]. Some studies have reported a decreased mortality trend over time [9,10,31,32,33], whereas others found that mortality did not differ between waves [29]. Overall, the reported mortality rate in large trials was about 30%. Indeed, in a multicenter Spanish study, Carbonell et al. [30] found 30.7% overall mortality in ICU without difference between COVID-19 waves. Nevertheless, they found a significant reduction in the ICU and hospital LOS in survivors during the second/third waves, which they explained by the change of the management protocol over time and that physicians became more familiar with the disease. In the COVID-ICU group study [9], the 90-day mortality was 31% and decreased from 42 to 25% over the study period. In a Dutch study [10], the crude hospital mortality was 29.9% in wave 1, 32.0% in wave 2, and it decreased to 23.4% in wave 3. This study found fewer patients treated with MV and vasopressors during wave 3. Accordingly, the authors cannot exclude that patients’ triage might have influenced their results. In a Brazilian study [34], the mortality rate in ICU was 57%. It increased by 3.3% per day during ICU stay. Finally, Serafim et al. [35], in a review including 69,093 patients, found an overall ICU mortality rate of 32.3%. More than half the patients admitted to ICU required MV (58%) and had a mortality rate of 59%. In our study, the overall ICU mortality rate was 36%. It was respectively 30, 34.2, and 47.1% during periods 1, 2, and 3, and hospital mortality was within similar ranges. The rates recorded in periods 1 and 2 were like those reported in the literature. Meanwhile, mortality recorded in period three was higher without significant difference in patients’ characteristics. However, in period 3, time between the first symptoms and hospitalization, NIV use, and time from ICU admission to MV were higher than in period 1. On the other hand, patients in period 3 were less exposed to antibiotics prior to MV, and had a lower need to RRT. These differences are probably related to the involved virus variant and the subsequent characteristics of the disease. Overall, one can suppose that the higher mortality rate observed in period 3 could be explained by the responsible SARS-CoV-2 variant. Nevertheless, we cannot exclude the impact of changes in the management strategy on outcome.
Several studies have focused on factors associated with mortality in COVID patients. They include age, frailty, ventilatory support, time to introduce MV, the causal virus variant, and vaccination coverage [36,37,38,39]. Wendel-Garcia et al. found that HFNC use was associated with lower ICU mortality, while NIV was associated with higher ICU mortality [36]. Camous et al., in a large case series from Guadeloupe, showed that very late MV, defined as intubation after day 7 of dexamethasone therapy, was associated with a high mortality rate of 87% [37]. Manrique et al. reported that implementing an early intubation approach is an independent protective factor for mortality [38]. In this study, late intubation was defined as intubation >24 hours after ICU admission, and the severity of the disease was lower in the late intubation group. Our study is prospective observational and non-interventional. Intubation and respiratory support were left to the discretion of attending physicians. We find that NIV use was higher in periods 2 and 3 than in period 1. Mechanical ventilation use was higher in period 1 than in periods 2 and 3. Also, the time from ICU admission to MV was higher in period 3 than periods 1 and 2. However, NIV use was not statistically different between survivors and non-survivors. While MV use and the time from ICU admission to MV were higher in non-survivors. Accordingly, we can suggest that these two parameters may have influenced the outcome of our patients.
Several studies focused on elderly and vulnerable patients whose predicted outcome is poor when MV is needed. These patients were recused from critical care and MV, especially in case of ICU bed shortage. The clinical frailty score was used mainly in patients older than 70 [6,28] and sometimes in those over 65 years [22,42]. In patients over 70 years with COVID-19 admitted to the ICU, the 90-day mortality was 46% and reached 67% among patients over 80 [28]. In the COVIP study [6], the mortality rate was 34% in fit, 47% in vulnerable, and 59% in frail patients, without difference in 30-day survival between different age categories in frail patients. After controlling for confounding variables, frailty was independently associated with lower survival. In our study, age was an independent risk factor for mortality. Frailty was diagnosed in 11% of patients. Mortality in frail patients was 71.4%. Our results align with the literature and sustain the use of age and frailty in selecting patients for ICU admission mainly in case of ICU bed shortage.
In our study, the dominant variants were gamma during period 2 and delta during period 3. Gamma variant emerged in Brazil in June 2020 [43] and reached FG because of the geographical proximity. Interestingly, FG is the sole French territory where the gamma variant was registered. Delta variant emerged in India in late 2020. It showed a 40–60% increase in transmissibility compared to the alpha variant, which was twice as contagious as the original strain [44]. In a large Canadian study, ICU admission and death probability were 1.9 and 1.33 fold higher with the delta variant than non-variants of interest [45]. Additionally, unvaccinated patients faced 11 times the risk of death from the delta variant than vaccinated people [46]. Tabatabai et al. showed that the odds of death was 3.45-fold higher during delta than alpha periods [47]. Liu et al. in a large study in the United States, showed a 73.8% decrease in the case-fatality rate related to delta variant in fully vaccinated people compared to unvaccinated people [48]. In our study, the ICU and hospital mortality were higher during the third period where 84.8% of patients under MV died. These findings could be explained by the dominant circulating strain (80% of screened variants were delta) and the under-vaccination coverage (8.2% of patients received one vaccine dose and only 4 patients were completely vaccinated). Indeed, with the same vaccination rates as mainland France, Nacher et al. estimated that 62.4% of ICU admissions would have been avoided in FG [15]. This result corroborates with a large French study showing that vaccination is associated with a lower risk of invasive MV and in-hospital death [39].
This study has potential limitations. First, this is a monocentric study. However, our unit accounted for 76% of ICU beds in FG and most severe patients were transferred to our unit. In addition, ICU hospitalizations, and death were monitored by the local French sanitary authorities. Accordingly, 80% of severe COVID-19 patients in FG were managed in our unit. For this, our study accurately shows what happened in FG during the COVID-19 crisis. Second, there were changes in the management protocol during the study period. These changes followed the scientific updates during the crisis and were observed in all studies dealing with COVID-19 [19,29,30]. Third, we separate three different periods according to the dominant circulating virus variant. Indeed, in period 1 there were two distinct waves with changes in the protocol management. Subgroup’s analysis comparing wave 1 to wave 2 did not show differences in patients’ epidemiological characteristics and outcomes. However, this study describes the epidemiology and outcome of severe COVID-19 patients admitted to ICU in a high-income context (French department) with a middle- to low-income and under-vaccinated population in South America.
5. Conclusions
Our study shows that the mortality of severe COVID-19 patients was higher during the delta variant wave in French Amazonia, with a shorter period from the onset of symptoms to ICU admission. This over-death could be explained by the virulence of the responsible SARS-CoV-2 variant and the under-vaccination coverage of the studied population without excluding the impact of changes in the management strategy on outcome.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Epidemiologic characteristics and management according to the study periods; Table S2: Comparison of survivors and non-survivors at hospital discharge; Table S3: Outcome of patients according to the study periods.
Author Contributions
Conceptualization, S.M., S.H., D.H., J.M.P. and H.K.; methodology, S.M., F.C., F.D., M.N. and H.K.; software, N.H., G.L.N., M.D., F.N. and H.K.; validation, H.K., F.C., C.G., D.H. and D.R.; formal analysis, S.M., M.N. and H.K.; investigation, S.M., A.B., N.H., G.L.N. and H.K.; resources, H.K.; data curation, S.M., M.N. and H.K.; writing—original draft preparation, S.M. and S.H.; writing—review and editing, H.K., D.H., F.C. and M.N.; visualization, H.K.; supervision, H.K.; project administration, H.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study received institutional review board approval from the “ethics committee of Cayenne General Hospital” on March 20, 2020 (CHC-CE-200320 REA, COVID-REA: Epidémiologie et prognostic du COVID en Réanimation), and procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975. Our database was registered at the “Commission National de l’Informatique et des Libertés” (registration n° 2226038 v 0), complying with French law on electronic data sources.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written information was distributed to all patients or their relatives indicating that their data could be used for research purposes in compliance with the French and EU Regulation n°2016/679 on the protection of personal data (RGPD) and the Law n°78-17 of January 6, 1978 known as the “Loi informatique et libertés” amended by the Law of June 20, 2018. This information allowed patients and their relatives to oppose using their data according to the conditions defined by Article 21-6 of the RGPD.
Data Availability Statement
All data supporting reported results can be are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Miliu, A.; Lavergne, A.; Succo, T.; Laizé, C.; Andrieu, A.; Enfissi, A.; Enouf, V.; Van der Werf, S.; Blanchet, D.; Demar, M.; et al. Dynamics of SARS-CoV-2 Lineages in French Guiana in 2020–2021: 4 Epidemic Waves with Cross-Influences from Europe and South America. Infect Genet Evol 2022, 105, 105370. [Google Scholar] [CrossRef]
- Chang, R.; Elhusseiny, K.M.; Yeh, Y.-C.; Sun, W.-Z. COVID-19 ICU and Mechanical Ventilation Patient Characteristics and Outcomes-A Systematic Review and Meta-Analysis. PLoS One 2021, 16, e0246318. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, Laboratory and Imaging Features of COVID-19: A Systematic Review and Meta-Analysis. Travel Med Infect Dis 2020, 34, 101623. [Google Scholar] [CrossRef]
- Zhang, J.J.Y.; Lee, K.S.; Ang, L.W.; Leo, Y.S.; Young, B.E. Risk Factors for Severe Disease and Efficacy of Treatment in Patients Infected With COVID-19: A Systematic Review, Meta-Analysis, and Meta-Regression Analysis. Clin Infect Dis 2020, 71, 2199–2206. [Google Scholar] [CrossRef]
- Jung, C.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; Beil, M.; et al. Differences in Mortality in Critically Ill Elderly Patients during the Second COVID-19 Surge in Europe. Crit Care 2021, 25, 344. [Google Scholar] [CrossRef]
- Jung, C.; Flaatten, H.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; et al. The Impact of Frailty on Survival in Elderly Intensive Care Patients with COVID-19: The COVIP Study. Crit Care 2021, 25, 149. [Google Scholar] [CrossRef]
- Xu, J.; Yang, X.; Yang, L.; Zou, X.; Wang, Y.; Wu, Y.; Zhou, T.; Yuan, Y.; Qi, H.; Fu, S.; et al. Clinical Course and Predictors of 60-Day Mortality in 239 Critically Ill Patients with COVID-19: A Multicenter Retrospective Study from Wuhan, China. Crit Care 2020, 24, 394. [Google Scholar] [CrossRef]
- Bilinski, A.; Emanuel, E.J. COVID-19 and Excess All-Cause Mortality in the US and 18 Comparison Countries. JAMA 2020, 324, 2100–2102. [Google Scholar] [CrossRef]
- COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators Clinical Characteristics and Day-90 Outcomes of 4244 Critically Ill Adults with COVID-19: A Prospective Cohort Study. Intensive Care Med 2021, 47, 60–73. [CrossRef]
- Dongelmans, D.A.; Termorshuizen, F.; Brinkman, S.; Bakhshi-Raiez, F.; Arbous, M.S.; de Lange, D.W.; van Bussel, B.C.T.; de Keizer, N.F. ; Dutch COVID-19 Research Consortium Characteristics and Outcome of COVID-19 Patients Admitted to the ICU: A Nationwide Cohort Study on the Comparison between the First and the Consecutive Upsurges of the Second Wave of the COVID-19 Pandemic in the Netherlands. Ann Intensive Care 2022, 12, 5. [Google Scholar] [CrossRef]
- Kumar A K, A.; Mishra, N. Mortality during the COVID-19 Pandemic: The Blind Spots in Statistics. Lancet Infect Dis 2022, 22, 428–429. [Google Scholar] [CrossRef]
- Wang, C.; Liu, B.; Zhang, S.; Huang, N.; Zhao, T.; Lu, Q.-B.; Cui, F. Differences in Incidence and Fatality of COVID-19 by SARS-CoV-2 Omicron Variant versus Delta Variant in Relation to Vaccine Coverage: A World-Wide Review. J Med Virol 2023, 95, e28118. [Google Scholar] [CrossRef]
- Huang, C.; Yang, L.; Pan, J.; Xu, X.; Peng, R. Correlation between Vaccine Coverage and the COVID-19 Pandemic throughout the World: Based on Real-World Data. Journal of Medical Virology 2022, 94, 2181–2187. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 1–12. [Google Scholar] [CrossRef]
- Nacher, M.; Vignier, N.; Rousseau, C.; Adenis, A.; Douine, M.; Basurko, C.; de Toffol, B.; Elenga, N.; Kallel, H.; Pujot, J.; et al. The Burden of COVID-19 in French Guiana: Vaccine-Averted Deaths, Hospitalizations and Costs. Vaccine X 2023, 13, 100271. [Google Scholar] [CrossRef]
- Kallel, H.; Resiere, D.; Houcke, S.; Hommel, D.; Pujo, J.M.; Martino, F.; Carles, M.; Mehdaoui, H. ; Antilles-Guyane Association of Critical Care Medicine Critical Care Medicine in the French Territories in the Americas: Current Situation and Prospects. Rev. Panam. Salud Pública 2021, 45, e46. [Google Scholar] [CrossRef]
- Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. New England Journal of Medicine 2021, 385, 777–789. [CrossRef]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone Treatment for the Acute Respiratory Distress Syndrome: A Multicentre, Randomised Controlled Trial. Lancet Respir Med 2020, 8, 267–276. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med 2021, 384, 693–704. [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Sablerolles, R.S.G.; Lafeber, M.; van Kempen, J.A.L.; van de Loo, B.P.A.; Boersma, E.; Rietdijk, W.J.R.; Polinder-Bos, H.A.; Mooijaart, S.P.; van der Kuy, H.; Versmissen, J.; et al. Association between Clinical Frailty Scale Score and Hospital Mortality in Adult Patients with COVID-19 (COMET): An International, Multicentre, Retrospective, Observational Cohort Study. Lancet Healthy Longev 2021, 2, e163–e170. [Google Scholar] [CrossRef]
- Kucewicz-Czech, E.; Damps, M. Triage during the COVID-19 Pandemic. Anaesthesiol Intensive Ther 2020, 52, 312–315. [Google Scholar] [CrossRef]
- Azoulay, É.; Beloucif, S.; Guidet, B.; Pateron, D.; Vivien, B.; Le Dorze, M. Admission Decisions to Intensive Care Units in the Context of the Major COVID-19 Outbreak: Local Guidance from the COVID-19 Paris-Region Area. Crit Care 2020, 24, 293. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Myatra, S.N.; Lobo, S.M. Surging ICU during COVID-19 Pandemic: An Overview. Curr Opin Crit Care 2022, 28, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Guidet, B.; Jung, C.; Flaatten, H.; Fjølner, J.; Artigas, A.; Pinto, B.B.; Schefold, J.C.; Beil, M.; Sigal, S.; van Heerden, P.V.; et al. Increased 30-Day Mortality in Very Old ICU Patients with COVID-19 Compared to Patients with Respiratory Failure without COVID-19. Intensive Care Med 2022, 48, 435–447. [Google Scholar] [CrossRef]
- Subramaniam, A.; Shekar, K.; Afroz, A.; Ashwin, S.; Billah, B.; Brown, H.; Kundi, H.; Lim, Z.J.; Ponnapa Reddy, M.; Curtis, J.R. Frailty and Mortality Associations in Patients with COVID-19: A Systematic Review and Meta-Analysis. Intern Med J 2022. [Google Scholar] [CrossRef]
- Dres, M.; Hajage, D.; Lebbah, S.; Kimmoun, A.; Pham, T.; Béduneau, G.; Combes, A.; Mercat, A.; Guidet, B.; Demoule, A.; et al. Characteristics, Management, and Prognosis of Elderly Patients with COVID-19 Admitted in the ICU during the First Wave: Insights from the COVID-ICU Study : Prognosis of COVID-19 Elderly Critically Ill Patients in the ICU. Ann Intensive Care 2021, 11, 77. [Google Scholar] [CrossRef] [PubMed]
- Carbonell, R.; Urgelés, S.; Rodríguez, A.; Bodí, M.; Martín-Loeches, I.; Solé-Violán, J.; Díaz, E.; Gómez, J.; Trefler, S.; Vallverdú, M.; et al. Mortality Comparison between the First and Second/Third Waves among 3,795 Critical COVID-19 Patients with Pneumonia Admitted to the ICU: A Multicentre Retrospective Cohort Study. Lancet Reg Health Eur 2021, 11, 100243. [Google Scholar] [CrossRef]
- Quah, P.; Li, A.; Phua, J. Mortality Rates of Patients with COVID-19 in the Intensive Care Unit: A Systematic Review of the Emerging Literature. Crit Care 2020, 24, 285. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Mulholland, R.H.; Lone, N.I.; Cheyne, C.P.; De Angelis, D.; Diaz-Ordaz, K.; Donegan, C.; Drake, T.M.; Dunning, J.; Funk, S.; et al. Changes in In-Hospital Mortality in the First Wave of COVID-19: A Multicentre Prospective Observational Cohort Study Using the WHO Clinical Characterisation Protocol UK. Lancet Respir Med 2021, 9, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Emmons-Bell, S.; Alger, H.M.; Bradley, S.M.; Das, S.R.; de Lemos, J.A.; Gakidou, E.; Elkind, M.S.V.; Hay, S.; Hall, J.L.; et al. Trends in Patient Characteristics and COVID-19 In-Hospital Mortality in the United States During the COVID-19 Pandemic. JAMA Netw Open 2021, 4, e218828. [Google Scholar] [CrossRef] [PubMed]
- Doidge, J.C.; Gould, D.W.; Ferrando-Vivas, P.; Mouncey, P.R.; Thomas, K.; Shankar-Hari, M.; Harrison, D.A.; Rowan, K.M. Trends in Intensive Care for Patients with COVID-19 in England, Wales, and Northern Ireland. Am J Respir Crit Care Med 2021, 203, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Sobral, M.F.F.; Roazzi, A.; da Penha Sobral, A.I.G.; de Oliveira, B.R.B.; Duarte, G.B.; da Silva, J.F.; Nogueira, R.M.T.B.L. A Retrospective Cohort Study of 238,000 COVID-19 Hospitalizations and Deaths in Brazil. Sci Rep 2022, 12, 3629. [Google Scholar] [CrossRef] [PubMed]
- Serafim, R.B.; Póvoa, P.; Souza-Dantas, V.; Kalil, A.C.; Salluh, J.I.F. Clinical Course and Outcomes of Critically Ill Patients with COVID-19 Infection: A Systematic Review. Clin Microbiol Infect 2021, 27, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Wendel-Garcia, P.D.; Mas, A.; González-Isern, C.; Ferrer, R.; Máñez, R.; Masclans, J.-R.; Sandoval, E.; Vera, P.; Trenado, J.; Fernández, R.; et al. Non-Invasive Oxygenation Support in Acutely Hypoxemic COVID-19 Patients Admitted to the ICU: A Multicenter Observational Retrospective Study. Critical Care 2022, 26, 37. [Google Scholar] [CrossRef] [PubMed]
- Camous, L.; Pommier, J.-D.; Martino, F.; Tressieres, B.; Demoule, A.; Valette, M. Very Late Intubation in COVID-19 Patients: A Forgotten Prognosis Factor? Critical Care 2022, 26, 89. [Google Scholar] [CrossRef]
- Manrique, S.; Claverias, L.; Magret, M.; Masclans, J.R.; Bodi, M.; Trefler, S.; Canadell, L.; Díaz, E.; Sole-Violan, J.; Bisbal-Andrés, E.; et al. Timing of Intubation and ICU Mortality in COVID-19 Patients: A Retrospective Analysis of 4198 Critically Ill Patients during the First and Second Waves. BMC Anesthesiology 2023, 23, 140. [Google Scholar] [CrossRef]
- Naouri, D.; Vuagnat, A.; Beduneau, G.; Dres, M.; Pham, T.; Mercat, A.; Combes, A.; Demoule, A.; Kimmoun, A.; Schmidt, M.; et al. Trends in Clinical Characteristics and Outcomes of All Critically Ill COVID-19 Adult Patients Hospitalized in France between March 2020 and June 2021: A National Database Study. Annals of Intensive Care 2023, 13, 2. [Google Scholar] [CrossRef]
- Rossman, H.; Meir, T.; Somer, J.; Shilo, S.; Gutman, R.; Ben Arie, A.; Segal, E.; Shalit, U.; Gorfine, M. Hospital Load and Increased COVID-19 Related Mortality in Israel. Nat Commun 2021, 12, 1904. [Google Scholar] [CrossRef]
- Bravata, D.M.; Perkins, A.J.; Myers, L.J.; Arling, G.; Zhang, Y.; Zillich, A.J.; Reese, L.; Dysangco, A.; Agarwal, R.; Myers, J.; et al. Association of Intensive Care Unit Patient Load and Demand With Mortality Rates in US Department of Veterans Affairs Hospitals During the COVID-19 Pandemic. JAMA Netw Open 2021, 4, e2034266. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.G.; Breckons, M.; Lee, R.P.; Dotchin, C.; Walker, R. Rationing Care by Frailty during the COVID-19 Pandemic. Age Ageing 2021, 50, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Faria, N.R.; Mellan, T.A.; Whittaker, C.; Claro, I.M.; Candido, D. da S.; Mishra, S.; Crispim, M.A.E.; Sales, F.C.S.; Hawryluk, I.; McCrone, J.T.; et al. Genomics and Epidemiology of the P.1 SARS-CoV-2 Lineage in Manaus, Brazil. Science 2021, 372, 815–821. [Google Scholar] [CrossRef]
- Shiehzadegan, S.; Alaghemand, N.; Fox, M.; Venketaraman, V. Analysis of the Delta Variant B.1.617.2 COVID-19. Clinics and Practice 2021, 11, 778–784. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R. Evaluation of the Relative Virulence of Novel SARS-CoV-2 Variants: A Retrospective Cohort Study in Ontario, Canada. CMAJ 2021, 193, E1619–E1625. [Google Scholar] [CrossRef]
- Dyer, O. Covid-19: Unvaccinated Face 11 Times Risk of Death from Delta Variant, CDC Data Show. BMJ 2021, 374, n2282. [Google Scholar] [CrossRef]
- Tabatabai, M.; Juarez, P.D.; Matthews-Juarez, P.; Wilus, D.M.; Ramesh, A.; Alcendor, D.J.; Tabatabai, N.; Singh, K.P. An Analysis of COVID-19 Mortality During the Dominancy of Alpha, Delta, and Omicron in the USA. J Prim Care Community Health 2023, 14, 21501319231170164. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wei, H.; He, D. Differences in Case-Fatality-Rate of Emerging SARS-CoV-2 Variants. Public Health Pract (Oxf) 2023, 5, 100350. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The flow-chart of the study.
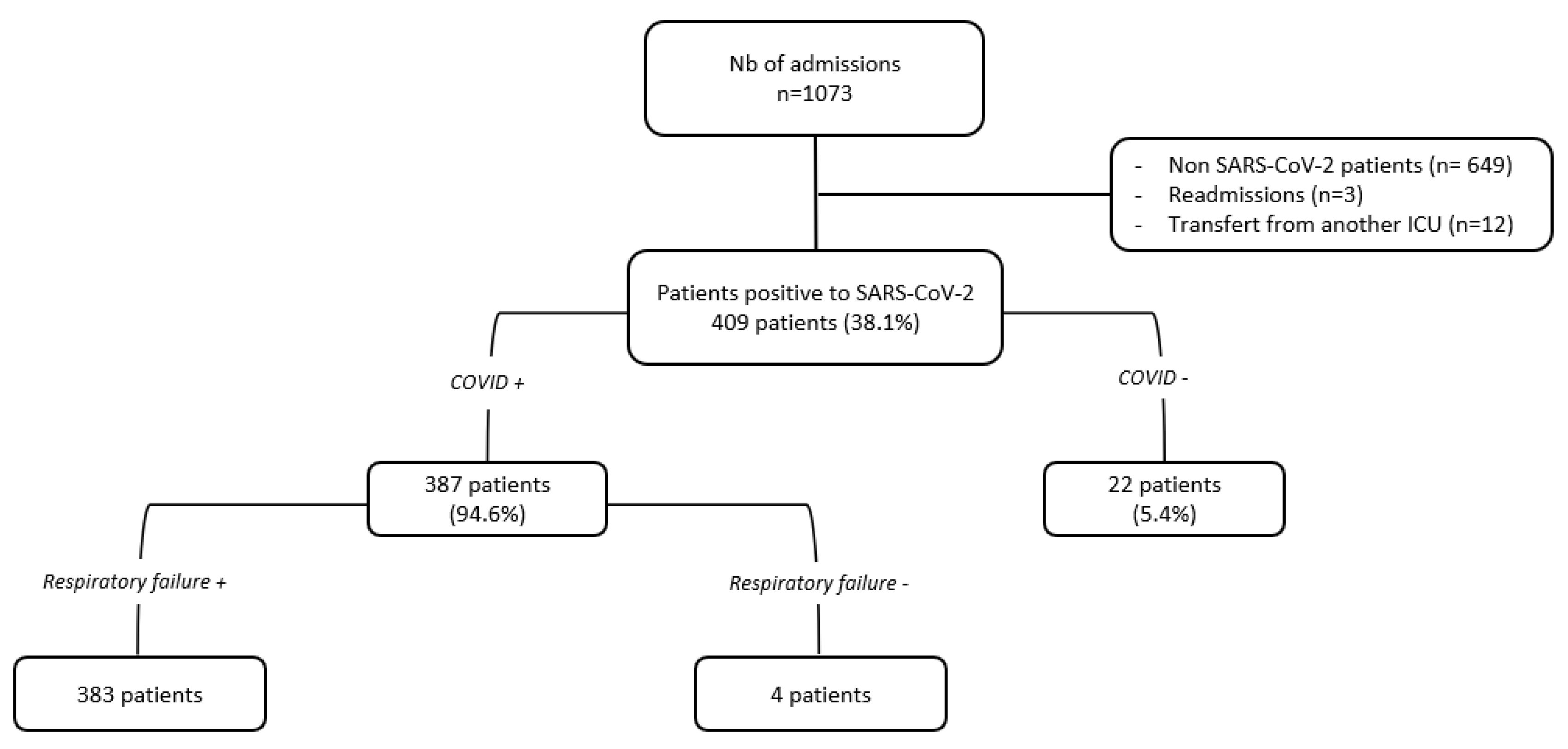
Figure 2.
ICU-bed capacity (in line) and occupancy rate (in bars) during the study period.
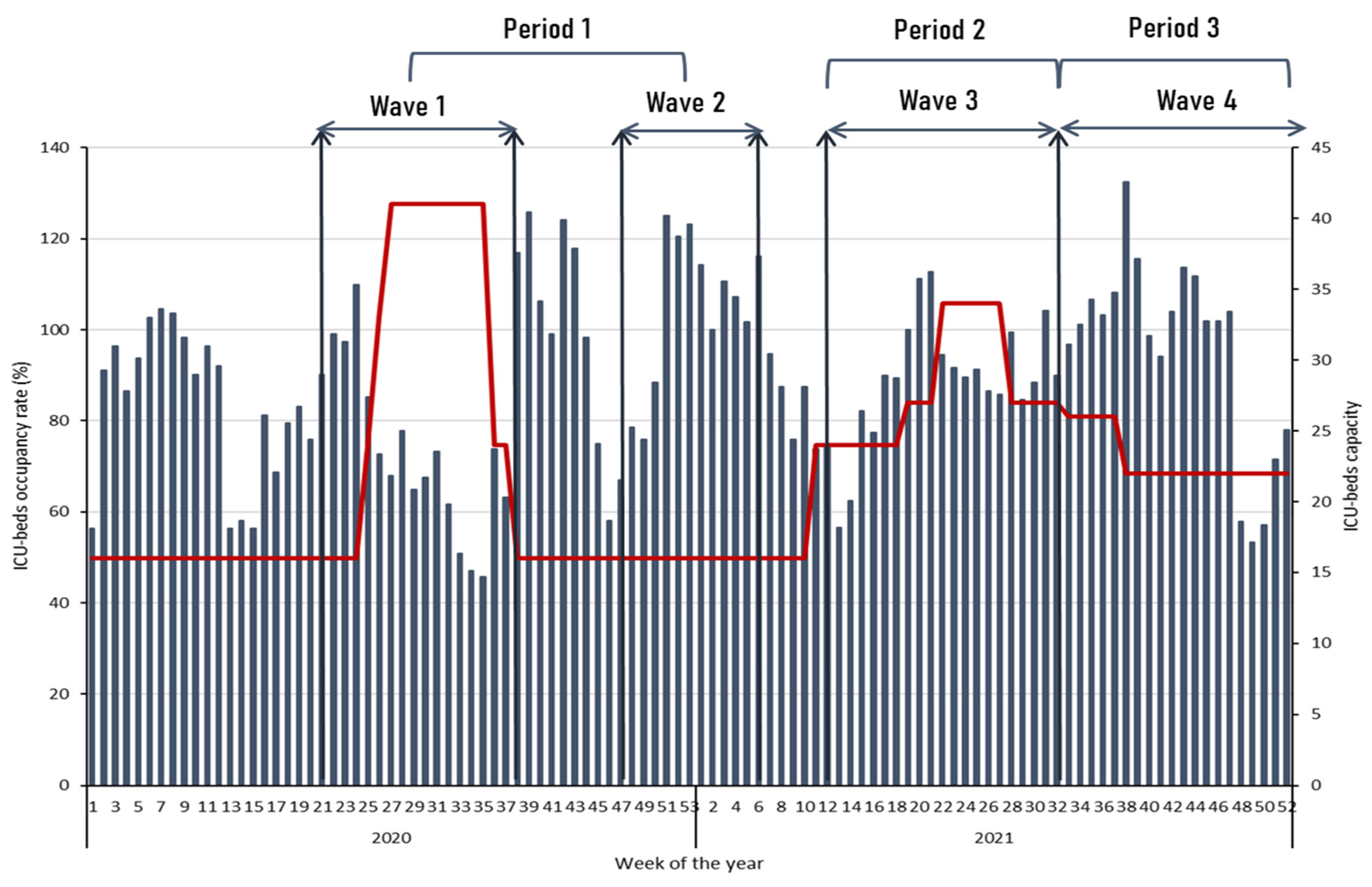
Figure 3.
Sixty-day mortality according to the period of analysis. Period 1 vs. period 2 (Log Rank = 0.176), Period 1 vs. period 3 (Log Rank = 0.005).
Figure 3.
Sixty-day mortality according to the period of analysis. Period 1 vs. period 2 (Log Rank = 0.176), Period 1 vs. period 3 (Log Rank = 0.005).
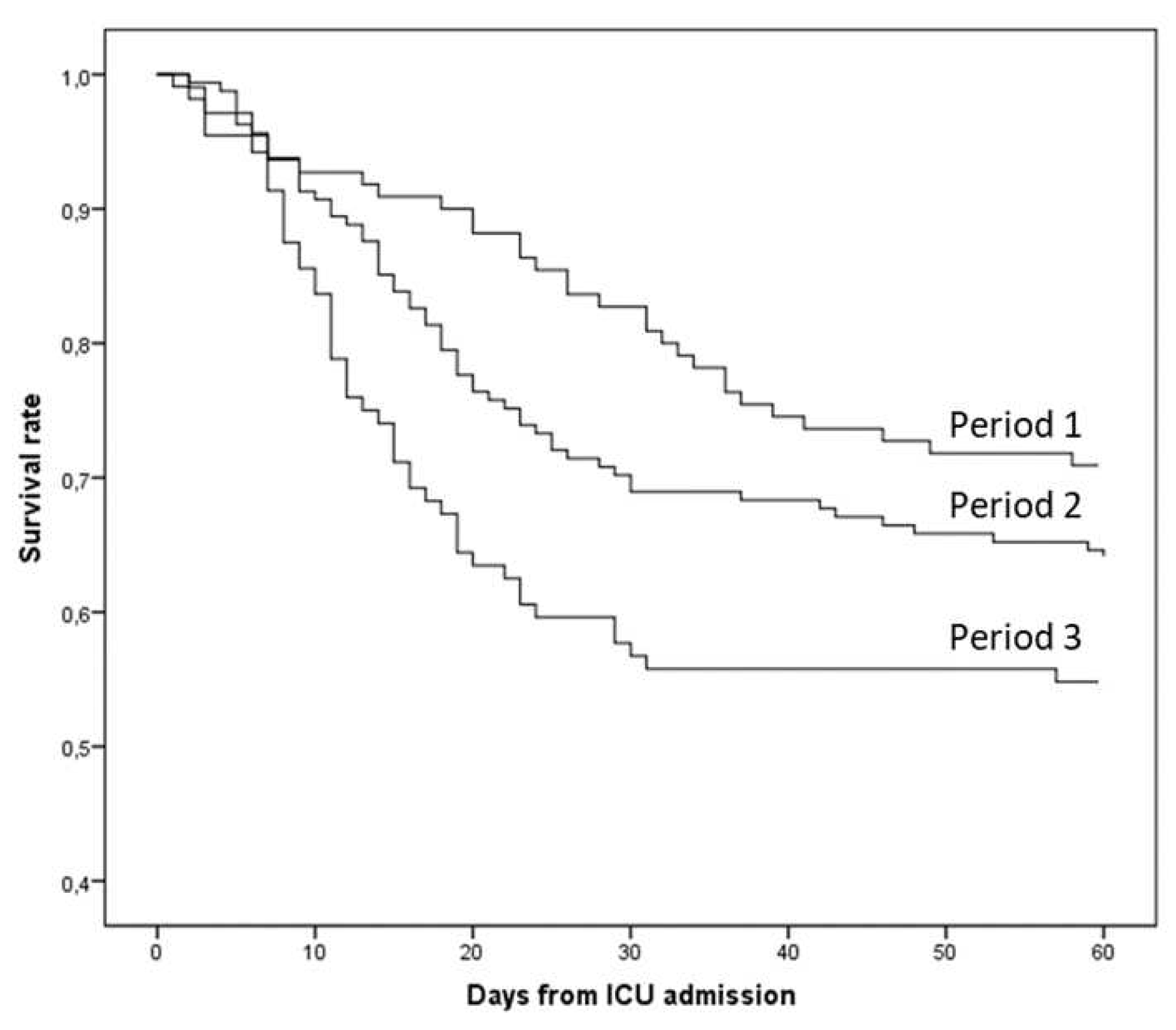
Figure 4.
Hospital mortality according to age groups (r = 0.939, p < 0.001). Bars indicate the number of patients in each age group, the red line represents the hospital mortality rate, and the black line represents the tendency line of hospital mortality according to age groups.
Figure 4.
Hospital mortality according to age groups (r = 0.939, p < 0.001). Bars indicate the number of patients in each age group, the red line represents the hospital mortality rate, and the black line represents the tendency line of hospital mortality according to age groups.
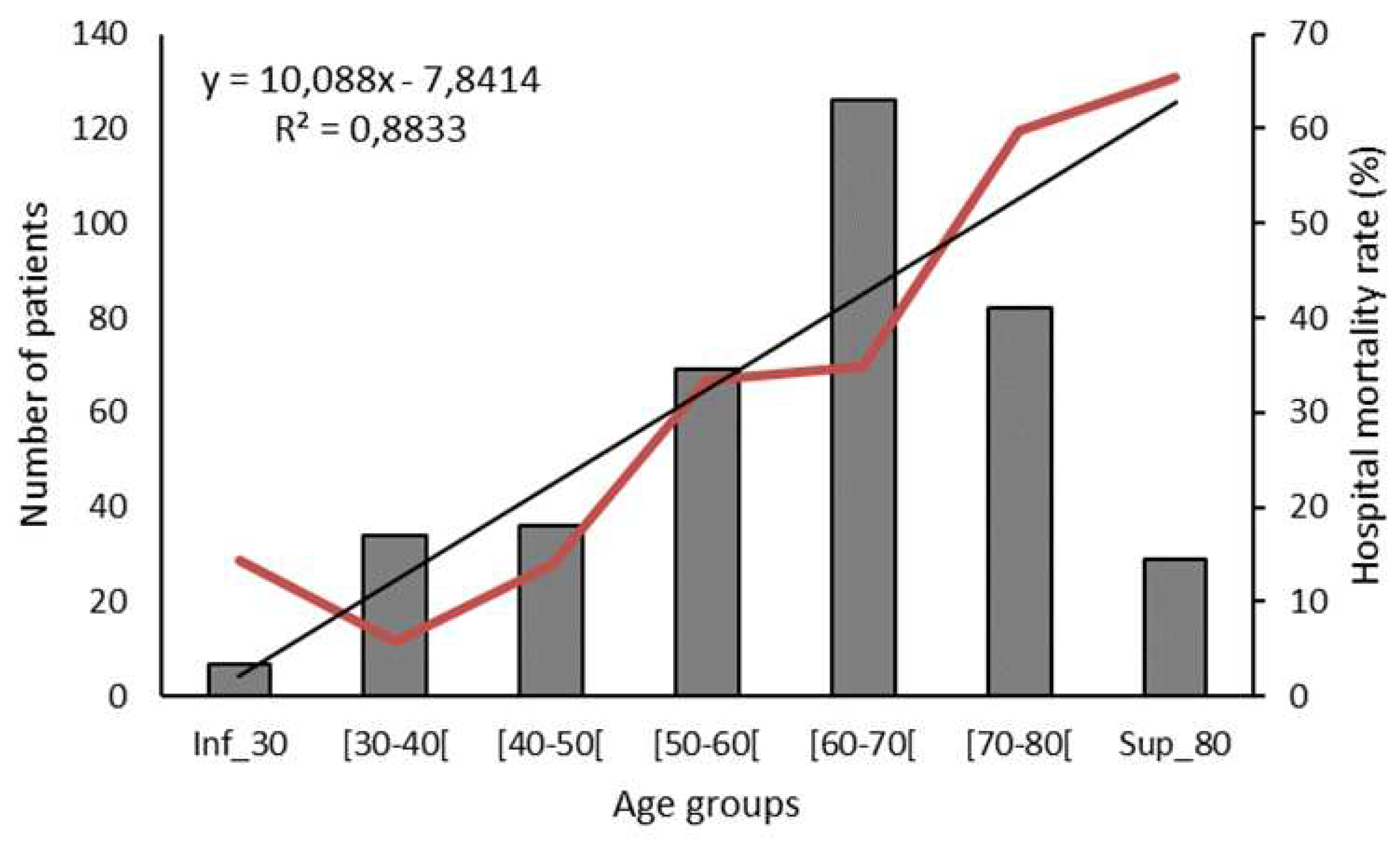

Table 1.
Hospital mortality, ICU and Hospital LOS according to the period of the study and the maximal respiratory support.
Table 1.
Hospital mortality, ICU and Hospital LOS according to the period of the study and the maximal respiratory support.
| Maximal respiratory support | Overall (n = 383) |
Period 1 (n = 110) |
Period 2 (n = 161) |
p * | Period 3 (n = 104) |
p $ |
|---|---|---|---|---|---|---|
| High-flow nasal cannula oxygen | n = 138 (36.0%) | n = 39 (35.5%) | n = 61 (37.9%) | 0.683 | n = 34 (32.7%) | 0.670 |
| Hospital mortality | 18 (13%) | 2 (5.1%) | 10 (16.4%) | 0.091 | 5 (14.7%) | 0.166 |
| ICU LOS (days) | 7 (5–9) | 8 (6–12) | 6 (4–8) | 0.004 | 6 (5–10) | 0.095 |
| Hospital LOS (days) | 16 (12–20) | 19 (16–23) | 14 (11–17) | 0.000 | 15 (11–18) | 0.011 |
| Non-invasive mechanical ventilation | n = 60 (15.7%) | n = 4 (3.6%) | n = 30 (18.6%) | <0.001 | n = 24 (23.1%) | <0.001 |
| Hospital mortality | 16 (26.7%) | 2 (50%) | 9 (30%) | 0.580 | 5 (20.8%) | 0.212 |
| ICU LOS (days) | 10 (7–14) | 13 (7–29) | 9 (5–10) | 0.180 | 11 (7–15) | 0.776 |
| Hospital LOS (days) | 17 (12–26) | 16 (9–48) | 16 (12–25) | 0.979 | 17 (11–23) | 0.975 |
| Invasive mechanical ventilation | n = 185 (48.3%) | n = 67 (60.9%) | n = 70 (43.5%) | 0.005 | n = 46 (44.2%) | 0.015 |
| Hospital mortality | 109 (58.9%) | 30 (44.8%) | 40 (57.1%) | 0.148 | 39 (84.8%) | <0.001 |
| ICU LOS (days) | 18 (10–28) | 21 (9–33) | 19 (11–28) | 0.411 | 13 (7–25) | 0.088 |
| Hospital LOS (days) | 23 (13–39) | 26 (13–42) | 25 (15–41) | 0.973 | 16 (9–29) | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



