Submitted:
07 December 2023
Posted:
11 December 2023
You are already at the latest version
Abstract
Background: Retinal vascular abnormalities may be associated with glaucomatous damage. Adaptive optics (AO) is a new technology that enables analysis of retinal vasculature at the cellular level in vivo. The purpose of this study is to evaluate retinal arteriolar parameters using the adaptive optics fundus camera (AO -FC) rtx1 in patients with primary open-angle glaucoma (POAG) at different stages and to investigate the relationship between these parameters and changes in optical coherence tomography (OCT) and perimetry. We wanted to assess whether vascular changes could be a cause or effect of glaucomatous damage.
Methods: Parameters of retinal supratemporal and infratemporal arterioles (wall thickness (WT), lumen diameter (LD), total diameter (TD), wall-to-lumen ratio (WLR), and cross-sectional area of the vascular wall (WCSA)) were analysed with the rtx1 in 111 POAG eyes, divided into three groups according to the severity of disease and 70 healthy eyes in correlation of structural defects in retinal nerve fibre layer and visual fields defects. Results: Compared with the control group, the POAG groups showed significantly smaller TD and LD values (p<0,05) and significantly higher WLR and WT values (p<0,05) for supratemporal and infratemporal arterioles. Rtx1 parameters significantly correlated with OCT parameters (retinal nerve fibre layer, ganglion cell complex and rim area) and visual field parameters (mean deviation and pattern standard deviation) (p<0.05). Conclusion: The results suggest that vascular dysfunction may be involved in POAG pathogenesis and neurodegenerative damage, even at the very early stage of glaucoma, without visual field defects.
Keywords:
ocular vascular disease
; glaucoma
; adaptive optics
1. Introduction
Glaucoma is the leading cause of irreversible blindness worldwide, but still, its aetiology is not entirely determined [1]. Although elevated intraocular pressure (IOP) remains the most critical risk factor for glaucoma, only one-third to one-half of patients have elevated IOP at the initial stages [2]. Moreover, many patients may experience disease progression despite typical intraocular pressure values [3]. Since the pathogenesis of glaucoma is multifactorial, other factors such as reduced axoplasmic flow in retinal ganglion cells (RGC) axons, oxidative stress and genetic background may also play an important role [4,5]. Another leading theory suggests vascular abnormalities cause glaucomatous optic nerve damage [6]. The vascular theory postulates that reduced ocular perfusion flow (OPF) and impaired vascular autoregulation contribute to the progressive degeneration of RGC through ischemic injury to the optic nerve [6].
Furthermore, other factors, including hypertension, diabetes, and migraine, that affect OPF are associated with the development of glaucoma, supporting the vascular theory [1, 7]. On the other hand, it has been observed that retinal vascular abnormalities are a secondary manifestation of glaucomatous neurodegeneration, suggesting that glaucoma itself may also induce retinal vascular abnormalities [8, 9]. Studies demonstrate that impaired RGCs require reduced blood supply, causing retinal arteriolar constriction [7]. This theory is supported by retinal vasoconstriction, also observed in other optic nerve diseases [10,11]. The development of vascular hypotheses has accelerated over the past decade with new imaging techniques in ophthalmology. Substantial evidence supports structural vascular changes in the retina during glaucoma, such as reduced density and calibre of blood vessels [1,6,7,12]. Numerous studies using optical coherence tomography angiography (OCTA) have shown significant reductions in flow density, flow index and vessel density in the optic nerve head and macula in patients with glaucoma compared to controls, as well as correlations between these parameters and changes in the visual field [6,12]. Colour Doppler Imaging has demonstrated reduced velocities and increased resistivity index of the intraocular vessels in glaucoma patients [13]. Until recently, different techniques have been used to analyse the calibre of retinal vessels [14]. Semiautomated software such as VAMPIRE (Vessel Assessment and Measurement Platform for Images of the Retina) [15] and Singapore I Vessel Assessment (SIVA) [16] have been developed to quantify retinal vascular parameters from digital retinal photographs. Parameters such as vessel calibre, tortuosity and branch angle have been studied in patients using them [1,17]. Also, the studies have described the application of a retinal vessel analyser [18], SD-OCT [19] and scanning laser ophthalmoscopy [20] for assessing the calibre of retinal vessels. However, only adaptive optics (AO) makes it possible to assess the thickness of the wall and the lumen diameter, as it can distinguish the vessel wall from the blood column [21]. AO has enabled non-invasive retinal examination at the cellular level with a resolution of about two μm by measuring wavefront distortions and compensating them in real-time with deformable mirrors [22, 23]. AO alone does not produce an image and must be integrated with retinal imaging devices such as fundus camera (FC), SLO and OCT. AO evaluates individual retinal structures such as photoreceptors, blood vessels, nerve fibres, ganglion cells, lamina cribrosa and trabeculae in healthy eyes and various eye diseases [22]. The first purpose of the present study was to evaluate the parameters of retinal arteries in patients with POAG at different stages of progression using AO-FC rtx1, the first to be integrated with an AO commercially available device. Secondly, we wanted to investigate the associations between these vascular parameters and glaucoma severity, defined by structural changes in optical coherence tomography (OCT) and functional changes in the perimetry. In addition, we wanted to compare the retinal vasculature of POAG patients and healthy subjects who were closely matched in terms of age and other parameters. We hypothesise that the examinations mentioned above will help assess whether vascular changes could be a cause or effect of glaucomatous damage. This study is the first trial analysing retinal vascular morphology using AO in correlation with other structural and functional tests in POAG.
2. Materials and Methods
The present study was conducted between August 2021 and November 2022 at the Department of Ophthalmology, Faculty of Medicine, the Medical University of Warsaw, in the Ophthalmic Public Hospital in Warsaw. The Bioethical Commission approved the study protocol of the Medical University of Warsaw (approval number KB/87/2015). All investigations were carried out according to the principles of the Helsinki Declaration. Written informed consent was obtained from all participants.
Subjects We included 111 eyes of 58 POAG patients recruited from the Glaucoma Department at our hospital and 70 eyes of 38 healthy volunteers. In 9 POAG subjects and six control subjects, only one eye was included in the study, as the other eye was excluded from the analyses because it did not meet the inclusion criteria. All subjects were above 18 years old, white Europeans. The patients included in the study had been diagnosed with bilateral POAG according to the criteria of European Glaucoma Society Guidelines [24] with assessment of RNFL, GCC defects and ONH parameters in OCT and MD and PSD in perimetry. Glaucoma was diagnosed at least two years ago. The glaucoma group was divided into three subgroups:
Group A - pre-perimetric glaucoma: no visual field scotoma in perimetry (37 eyes).
Groups B and C: perimetric glaucoma according to the criteria of simplified Hodapp’s classification [24] divided as:
Group B – early glaucoma: (48 eyes).
Group C - moderate glaucoma: (26 eyes).
In 24 patients, glaucoma severity in both eyes was at the same stage; in others, it was at different levels.
The control group was selected according to the following eligibility criteria: IOP <21 mm Hg, normal appearance of the ONH, normal OCT RNFL and GCC parameters. Inclusion parameters for all groups included: absence of angle closure in gonioscopy, spherical lens less than six dioptres or cylindrical lens less than 2.5 dioptres; axial eye length less than 26 mm, best corrected visual acuity (BCVA) ≥ 0.4 on Snellen charts, explicit ocular media; high image quality; no history of intraocular surgery (excluding uncomplicated cataract surgery or uncomplicated glaucoma surgery for the glaucoma cohort); absence of diabetes mellitus; no history of trauma or other ocular diseases, and the absence of signs indicating secondary glaucoma for the POAG group.
Examination
All patients underwent ophthalmic examination, including BCVA, refractometry, slit lamp biomicroscopy, Goldmann applanation tonometry, gonioscopy and direct fundoscopy. Axial eye length was acquired using IOL Master 700 (Carl Zeiss Meditec AG, Hennigsdorf, Germany). The RNFL, GCC, thickness, and rim area were obtained by spectral domain OCT (SD-OCT) RTVue XR 100 Avanti Edition (Optovue, USA). Humphrey 24.2 Sita-standard visual field with the reliability indices of the European Glaucoma Society was performed on Humphrey Field Analyzer 3 (Zeiss, Germany). All participants were asked to fill in a questionnaire on their characteristics, including age, sex, weight, height, and history of diseases, including hypertension, diabetes, hypercholesterolemia, arrhythmia, cardiovascular diseases (stroke, infarction) and smoking status. In addition, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in the sitting position on the brachial artery.
AO fundus images were obtained using AO-FC (Rtx1™; Imagine Eyes, Orsay, France– version 3.4, also known as AO Image 3.4). Rtx1™ uses infrared light (850 nm wavelength) and is characterised by a resolution of 1.6 μm. The image dimensions are 4∘ × 4∘, representing 1.2 mm × 1.2 mm of the retina. Image acquisition in a single position lasts approximately 4 s, during which 40 individual images are acquired [25]. The Rtx1™ software provides the program AO Detect Artery to analyse retinal vessel parameters and correct distortions within frames [26]. Most examinations were done without pupil dilation; if high-quality image acquisition was unavailable, pupil dilation was obtained with topical 1% tropicamide (Polfa, Warszawa). Images of the superior and inferior temporal retinal arterioles were obtained at a distance of 0.5-1-disc diameters from the edge of the optic nerve disc, avoiding arteriovenous junctions and the adjacency of retinal veins. The following parameters are assessed to evaluate vessel morphology, lumen diameter (LD), wall thickness (WT) and total diameter (TD) calculated as single WT plus LD single WT: TD = WT + (WT + LD). The following two parameters, wall-to-lumen ratio (WLR) and the cross-sectional area of the vascular wall (WCSA) are obtained automatically from the AO artery detection software. WLR is the ratio of the vessel's WT to LD, calculated as 2 × WT/LD, while WCSA describes the relationship between LD and TD. All the above-mentioned retinal parameters were measured three times on the scan with the best quality; the arithmetic mean of these three values was used in the statistical analysis.
Statistical Analyses
The data analysis was conducted with Statistica™ v. 13.2, TIBCO Software Inc, Palo Alto, CA, USA; 2017. Continuous variables, presented as means with their standard deviations (SD), were compared between the POAG and control groups using either the student's t-test or the Mann-Whitney U-test, depending on the data distribution. The Shapiro-Wilk test was used to determine the normality of each continuous variable. The Kruskal-Wallis and chi-square tests were used to compare at least three groups in terms of the quantitative variable. Relationships between numerical variables were assessed using Pearson correlation analysis when the data met parametric test conditions and Spearman correlation analysis when they did not. A two-sided test was applied for p-values, and statistical significance was defined as p < 0.05.
3. Results
Comparison of General Data
The results of age, sex, BMI, SBP and DBP show no significant difference between all groups (p>0,05). The mean intraocular pressure in all eyes was within normal limits and higher in the control group than in the glaucoma groups (p<0,001 in the Kruskal-Wallis test). In terms of AL, there was a significant difference between group B and the control group (p<0,001), but otherwise, there was no significant difference between the groups (p>0,05). All groups were comparable to each other for the percentage of smokers and patients diagnosed with hypertension, hypercholesterolemia and history of stroke and heart attack (p>0,05). The clinical characteristics of the groups are presented in Table 1.
The glaucoma groups were compared in terms of cup-to-disc ratio, estimated during direct fundoscopy, OCT parameters (mean RNFL, mean GCC, Rim area) and visual field parameters (mean deviation (MD), pattern standard deviation (PSD)). The results are presented in Table 2.
In addition, the course of glaucoma treatment is shown in Table 3.
In the POAG groups (from A through B up to C), there was a significant decrease in the mean RNFL thickness (with a significant difference between groups A and B vs C p<0,001)) and the mean GCC thickness ((with a significant difference between groups A and B vs C (p<0,001). We also observed in POAG groups from A up to C rim area narrowing with a significant difference between groups A and B vs C with p<0,001 and p=0,005, respectively, as well as the c/d ratio increase with a significant difference between groups A and B vs C and B with p<0,001. Perimetry in the POAG groups showed an increase in PSD values with a significant difference between all groups (p<0,001) and a decrease in MD values with a significant difference between all groups (p<0,001).
Comparison of supratemporal retinal arterioles between POAG groups versus the control group
The results are presented in Table 4.
The mean 1WT value was significantly higher in all glaucoma groups than in the control group (for A vs control, p =0,017; for B and C vs control, p< 0,001). The mean 2WT value was significantly higher in all glaucoma groups than in the control group (for A, B, C vs control p <0,001). The mean WLR value was significantly higher in all glaucoma groups than in the control group (p <0,001). The mean LD value was significantly smaller in all glaucoma groups than in the control group (p=0,004, p=0,011 and p<0,001, respectively, for groups A, B and C). The mean TD value was significantly smaller in all glaucoma groups than in the control group (p=0,019, p=0,044 and p=0,003, respectively, for groups A, B and C). No statistically significant differences were observed between all glaucoma and the control groups in the mean WCSA (p=0,604 in the Kruskal-Wallis test). Figure 3 and the healthy subject in Figure 2 show the evaluation of the supratemporal arteriole parameters in a patient with POAG.
Figure 1.
Image of the supratemporal arteriole in a patient with primary open-angle glaucoma (POAG). Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Figure 1.
Image of the supratemporal arteriole in a patient with primary open-angle glaucoma (POAG). Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
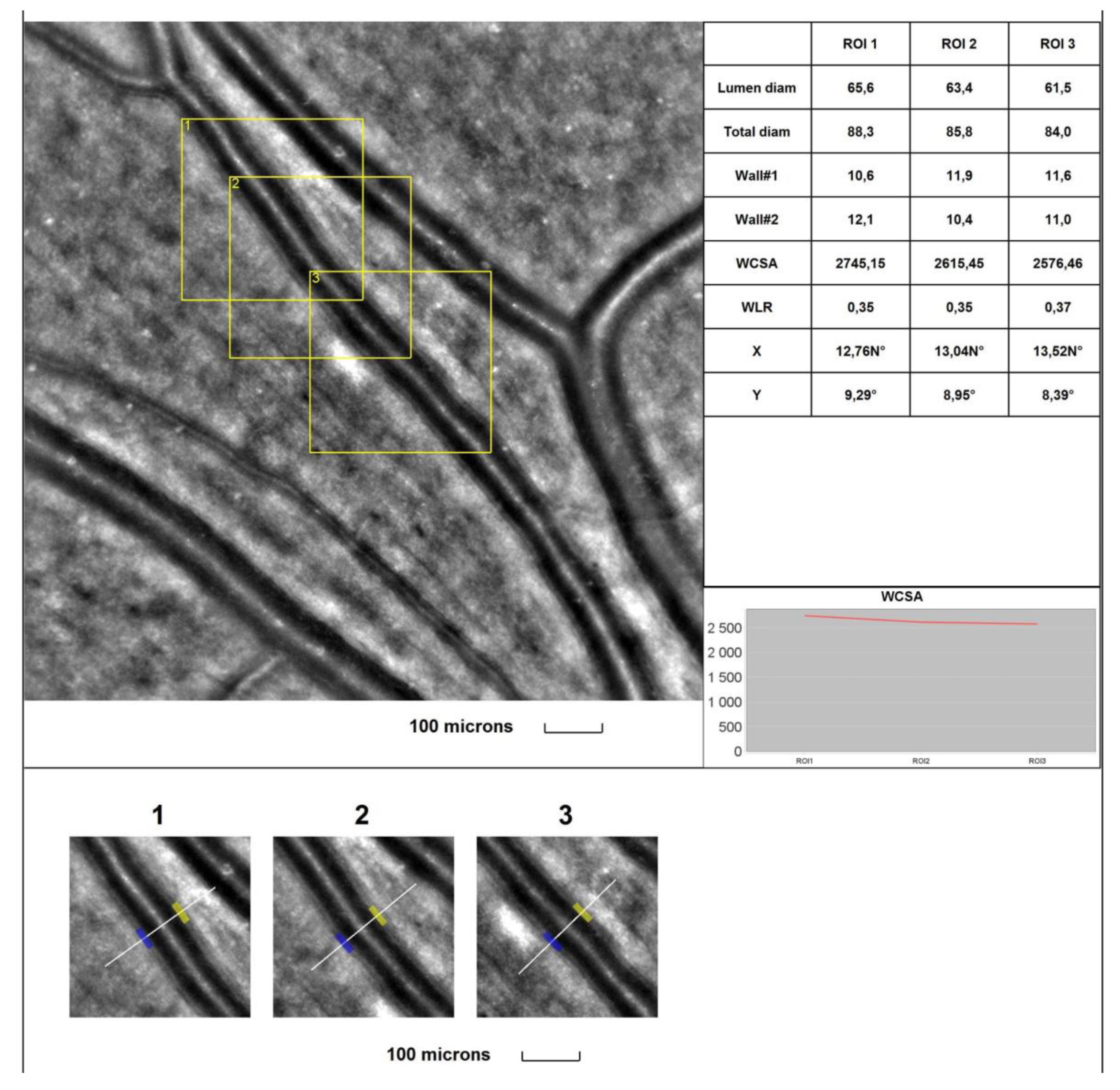
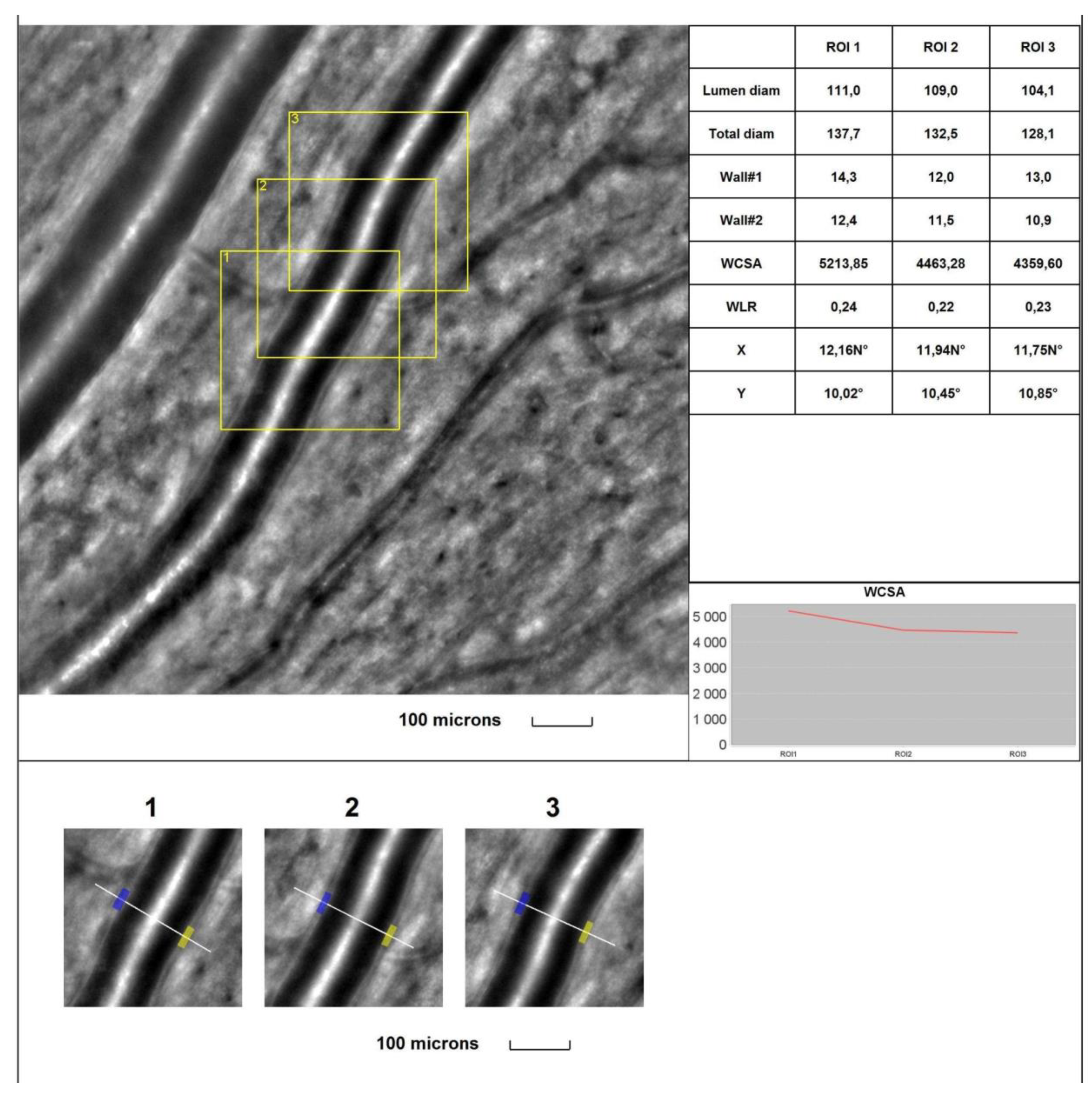
Figure 2.
Image of the supratemporal arteriole in the healthy subject. Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Figure 2.
Image of the supratemporal arteriole in the healthy subject. Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Comparison of infratemporal retinal arterioles between POAG groups versus the control group results are presented in Table 5.
The mean 1WT value was significantly higher in all glaucoma groups than in the control group (for A vs control p <0,001; for B vs control p= 0,003; for C vs control p <0,001). The mean 2WT value was significantly higher in all glaucoma groups vs the control group (for A, B, and C vs control p <0,001). The mean WLR value was significantly higher in all glaucoma groups than in the control group (for A vs control p <0,001; for B vs control p< 0,001; for C vs control p <0,001). The mean LD value was significantly smaller in all glaucoma groups than in the control group (for A, B, C vs control p <0,001). The mean TD value was smaller in all glaucoma groups than in the control group, but for group C, the difference is significant (for A vs control p = 0,087; for B vs control p=0,054; for C vs control p = 0,008). No statistically significant differences were observed between all glaucoma groups versus the control group in the mean WCSA ((p=0,248 in the Kruskal-Wallis test). The evaluation of the parameters of the infratemporal arteriole in a patient with POAG is shown in Figure 2.
Figure 3.
Image of the infratemporal arteriole in a patient with primary open-angle glaucoma (POAG). Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Figure 3.
Image of the infratemporal arteriole in a patient with primary open-angle glaucoma (POAG). Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
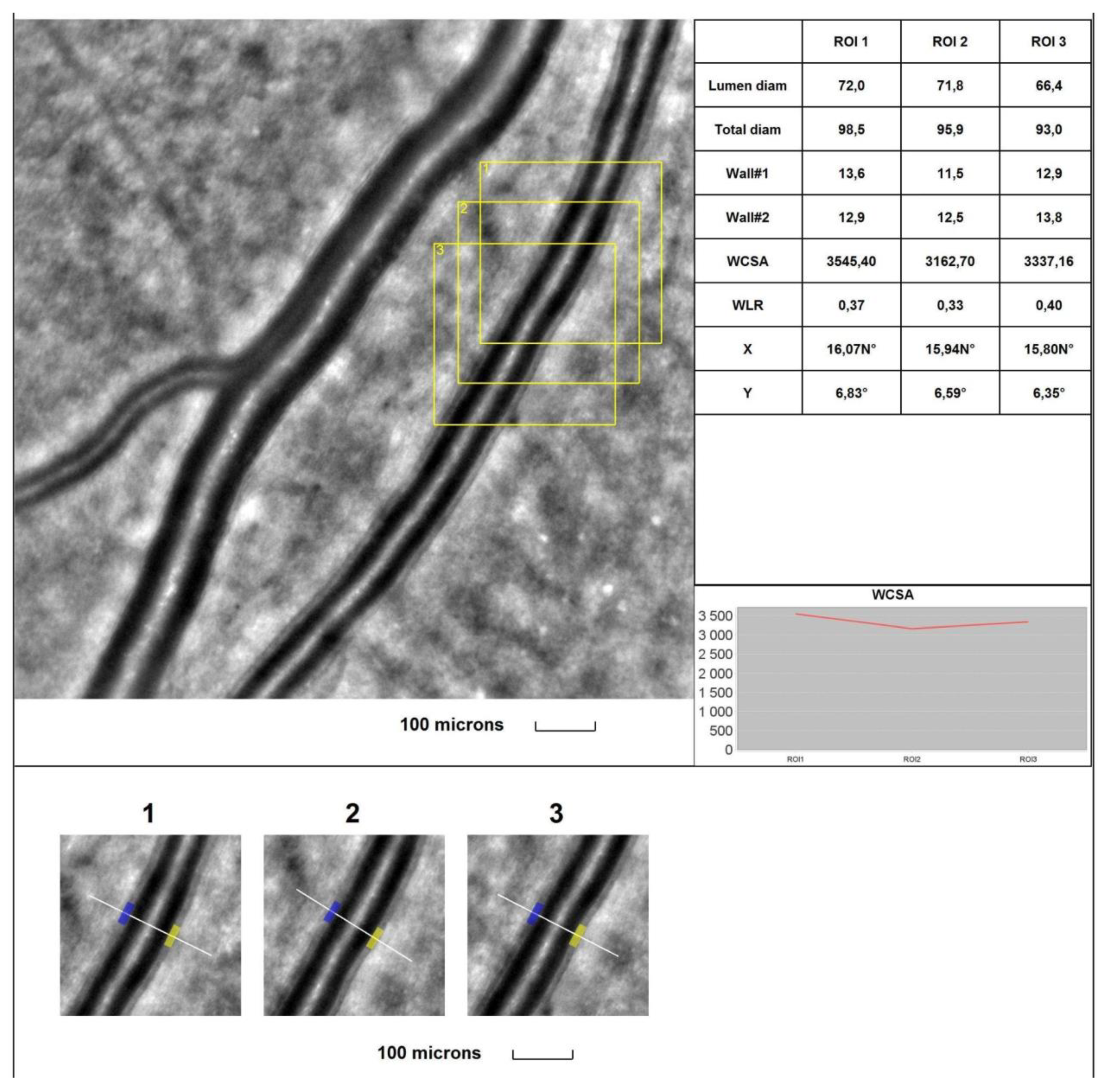
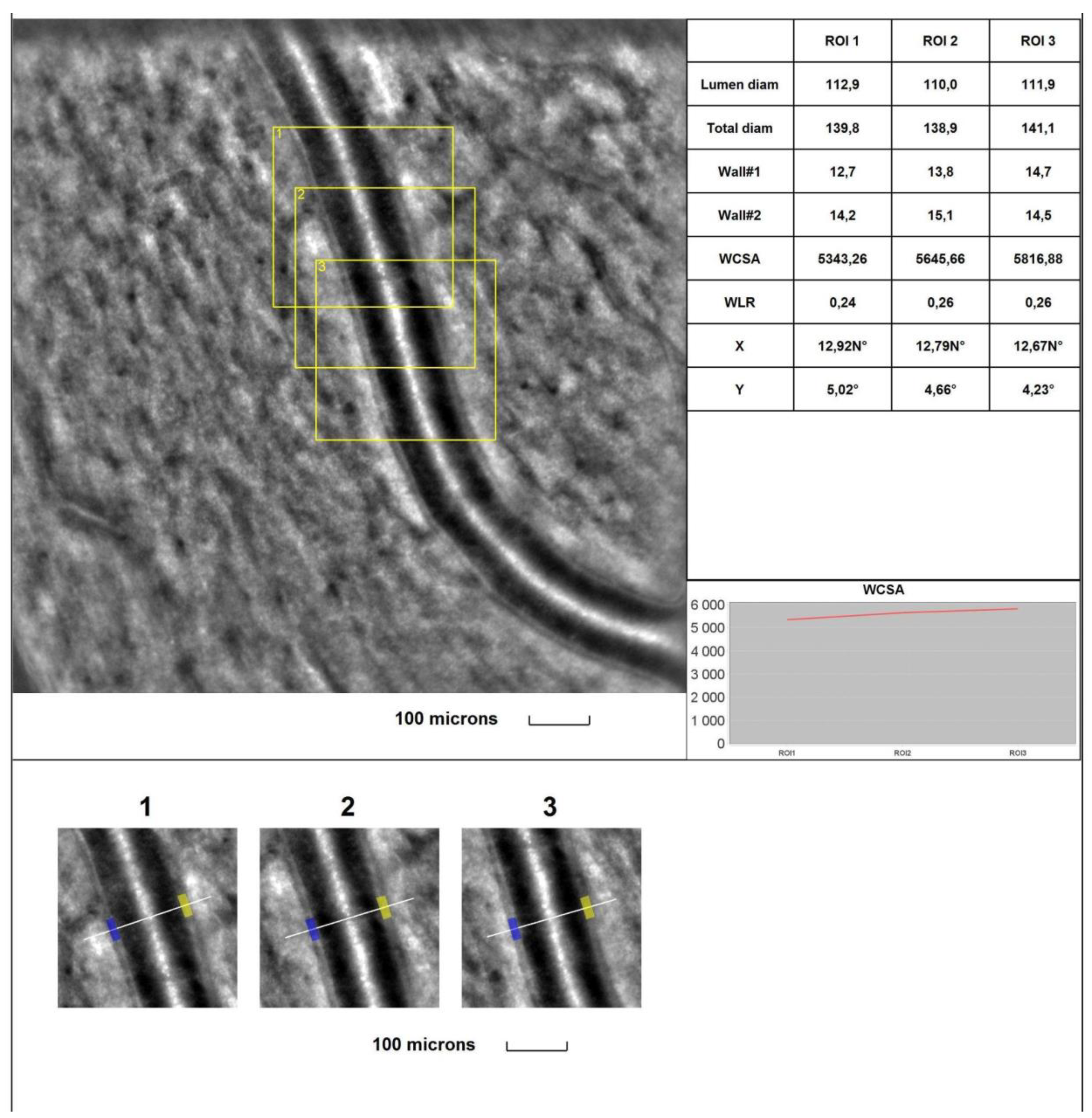
Figure 4.
Image of the infratemporal arteriole in a healthy subject. Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Figure 4.
Image of the infratemporal arteriole in a healthy subject. Evaluation of retinal arteriolar morphology in a POAG patient with adaptive optics camera 4°×4° degree square (Rtx-1, Imagine Eyes, Orsay, France) and measurement of morphological parameters using AOdetect software. The parameters were calculated from the three selected regions of interest for each time landmark (100 μm width and height each) (bottom). The charts represent the following parameters: Lumen diam - lumen diameter; Total diam - total diameter; wall1 and wall2, WCSA - cross-sectional area; WLR - wall-to-lumen ratio. The image has come from the author’s collection.
Comparison of RTX 1 arteriolar parameters between glaucoma groups. There were no significant differences between rtx1 parameters between all glaucoma groups for supratemporal (p>0,05) and infratemporal (p>0,05) retinal arterioles.
Correlation analysis of supratemporal retinal arteriole parameters in POAG group. TD correlated significantly positively with RNFL (r = 0,238) and rim area (r = 0,225) (p<0,05). LD correlated significantly positively with RNFL (r = 0,313), GCC (r =0,199) and rim area (r = 0,265) (p<0,05). WLR correlated significantly negatively with RNFL (r = -0,329, GCC (r =-0,265), rim area (r =-0,285), and MD (r =-0,290) (p<0,05), while significantly positively with c/d ratio (r = 0,191) and PSD (r =0,353) (p<0,05).
Correlation analysis of infratemporal retinal arteriole parameters in POAG group. A significant, positive correlation was found between the RNFL and LD (r=0,193, p<0,05). A significant, negative correlation was noted between the mean RNFL and WLR (r= -0,266, p<0,05).
4. Discussion
Glaucoma is a multifactorial disease. Even though IOP is a significant risk factor, various additional theories have been proposed to explain glaucoma’s aetiology. Vascular theory suggests that altered OBF causes unstable oxygen supply and thus causes glaucoma damage [27,28]. Oxidative DNA damage can affect trabeculae, which induces resistance to aqueous outflow and RGCs, driving neurodegenerative changes [29,30]. Disruption of vascular autoregulation in ONH [27, 31, 32] and higher retinal vascular resistance [33] also seem to play an essential role in the aetiology and progression of glaucoma. In addition, the imbalance between vasoconstrictor ET-1 and vasodilator nitric oxide has been observed in glaucoma, which can lead to endothelial dysfunction, resulting in retinal vascular impairment in glaucoma patients [7]. Therefore, evaluation of vasculature in eyes with POAG is crucial for diagnosis, monitoring and understanding the pathogenesis of the disease. The high resolution of AO images makes them an ideal reference target for retinal vessel morphology measurements [34], with excellent intra-observer and inter-observer repeatability [35] and good correlation with SD-OCT measurements [36].
The present AO study shows that retinal arterioles in glaucomatous patients differ from normal eyes. Each eye of patients with glaucoma diagnosis has been qualified into one of 3 groups according to the severity of the disease. The first subgroup – A, included eyes without visual field defects, with typical structural changes in ONH and SD-OCT. The subgroups B and C represent perimetric glaucoma of different stages. To enhance the statistical strength of comparisons, we carefully matched all groups for age, BMI, and systemic blood pressure - well-known factors affecting retinal vascular calibres [21]. The TD of retinal arterioles was smaller in all glaucoma groups in both analysed localisations: supra- and infra-temporal. Previously, the narrowing of retinal arterioles in POAG has been shown in numerous studies, mainly using colour fundus photographs [17, 37-41]. In some studies, measurements were taken using manual strategies [37-39], and in others - with the help of semi-automatic software and standardised measurements [17, 40, 41]. In addition, the narrowing diameter of retinal vessels in glaucoma has been observed on SD-OCT images using near-infrared images [42]. However, the methods did not provide information on the arteriolar LD. In our study, using adaptive optics, we showed significantly smaller LD in all POAG groups compared to the control group. Our study confirms the result of Hugo et al., who was the first to use AO to evaluate retinal vasculature in glaucoma and found a significant reduction in TD and LD in POAG patients compared to healthy individuals [14]. Our study also found that WT and WLR in the POAG group were significantly higher than in the control group. Hugo et al.'s previous study [14] does not support our results regarding WT and WLR. Still, they analysed smaller groups (n=31) than in our study (n=111), and there was no description of structural changes in OCT and functional changes in the visual field.
On the other hand, WRL and WT have been widely studied in other diseases, such as hypertension and diabetes. They showed significantly higher WT and WLR in hypertensive [23, 43] and diabetic [44] patients than healthy subjects. By assessing both WCSA and WRL, it is possible to distinguish between eutrophic and hypertrophic vascular remodelling [45]. Eutrophic remodelling is characterised by increased WRL and unchanged WCSA, as we obtained in glaucoma patients in the present study. In eutrophic remodelling, the reduction in LD is caused by vasoconstriction by smooth muscle cells without a growth response [45]. On the contrary, hypertrophic remodelling is characterised by a simultaneous increase in WRL and WCSA caused by the growth of smooth muscle cells [45]. Therefore, the vascular morphological parameters in glaucoma (such as WT, WRL, WCSA) should be further investigated in larger groups and with consideration of other confounding factors.
Our study also found several significant correlations for structural OCT parameters with LD and TD. In turn, WRL showed numerous significant correlations with structural and functional parameters, thus potentially becoming a good candidate as a biomarker of glaucomatous changes in the future. Our results support the concept that retinal vasoconstriction is associated with the progression of glaucoma changes in OCT and perimetry, as demonstrated in previous studies [41, 46-49]. Regarding these observations, two possible explanations have been postulated for the relationship between retinal vasoconstriction and POAG. On the one hand, losing RGCs leads to reduced metabolic demands and consequent vasoconstriction. Alternatively, it has been recommended that vasoconstriction leads to impaired perfusion and loss of RGCs in POAG. Considering the results of our study:
1. statistically significant changes in the structure of the arterioles are found in the initial preperimetric stage of POAG compared to healthy subjects.
2. a significant correlation was observed between retinal vasoconstriction, structural changes in OCT, and functional changes in VF in glaucoma patients.
Vascular dysfunction may be involved in the POAG pathogenesis, and retinal arteriolar narrowing could lead to neurodegenerative damage. These observations add further support to previous findings from cohort population-based studies, including the Blue Mountains Eye Study [50], the Beijing Eye Study [37], and the Singapore Malays Eye Study [51]. Prospective studies also support the concept of vascular pathogenesis. Kawasaki et al. observed a prospective association between baseline arteriolar calibre narrowing and increased long-term risk of POAG in a cohort study over ten years [52]. Timothy P H Lin et al.'s study found that each standard deviation decrease in the baseline retinal vessel calibres was associated with a more than 30% increase in the risk of RNFL thinning and a more than 90% increase in the risk of VF deterioration during the 24-month follow-up period [53]. Eunjoo Yoo et al. investigated retinal vessel diameter in patients classified as bilateral glaucoma suspects who showed unilateral glaucomatous conversion during a more than two years follow-up period. There was a significant inter-eye difference in retinal arteriolar diameter at baseline between eyes that converted to glaucoma and those that did not [54]. Rong et al. also analysed retinal arteries in patients with newly diagnosed normal tension glaucoma (NTG). Retinal arteriolar calibres were significantly reduced in individuals with first diagnosed NTG compared to age-matched controls, thus adding to the growing evidence that the pathogenesis of glaucoma has a vascular component [55]. All these observations suggest that significant vascular alterations are primary in POAG. These investigations may enable the identification of potential targets for future glaucoma treatments, such as endothelin or Caveolin receptors, which can dilate retinal vessels and increase blood flow [2, 56]. While numerous studies substantiate the existence of a vascular mechanism leading to neurodegenerative glaucoma damage, it is essential not to forget that glaucoma itself can initiate retinal vascular abnormalities as secondary manifestations of the disease [7,9, 57, 58]. In addition, it should not be ignored that vascular abnormalities represent only one of many factors contributing to the neurodegenerative processes observed in glaucoma. Therefore, further studies should be performed to determine the causal relationship between vascular abnormalities and glaucoma and ultimately use this aspect of pathogenesis for better diagnosis and treatment of glaucoma patients.
5. Limitations
This study has several limitations. First, the size of our study group could have been more significant. The study was conducted during the pandemic, which affected the size of the group. Second, the group with advanced-stage glaucoma was not analysed. Third, the study was not prospective, which cannot reflect long-term changes in blood vessels in patients with POAG.
6. Conclusions
The present study is the first assessment of microvascular morphology using AO in POAG in correlation with structural and functional parameters. Vascular changes at early stages of the disease and their association with disease progression are shown. This study may provide better insight into the pathogenesis and progression of POAG, which may contribute to better diagnosis and treatment of the disease.
Author Contributions
Conceptualisation, AS and AZ; methodology, AS, ZW, AZ; validation, ZW; formal analysis, AS, AZ, ZW; investigation, AS and AZ..; writing—original draft preparation, AS; writing—review and editing AS, AZ, ZW, JS. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki and approved by the Ethics Committee of the Medical University of Warsaw (KB/87/2015; 07.04.2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent to publish this paper has been obtained from the patients.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chan, K.K.W.; Tang, F.; Tham, C.C.Y.; Young, A.L.; Cheung, C.Y. Retinal vasculature in glaucoma: a review. BMJ Open Ophthalmol. 2017, 1, e000032. [Google Scholar] [CrossRef]
- Almeida, I.N.F.; Taniguchi, E.; Tito, C.V.A.; Dias, D.T.; Ushida, M.; Dorairaj, S.; Ritch, R.; Teixeira, S.H.; Paranhos, A.; Gracitelli, C.P.B.; et al. Vascular parameters and endothelin-1 measurements in glaucoma patients with low- and high-tension optic disc hemorrhages. Sci. Rep. 2023, 13, 5023. [Google Scholar] [CrossRef]
- Yanagi, M.; Kawasaki, R.; Wang, J.J.; Wong, T.Y.; Crowston, J.; Kiuchi, Y. Vascular risk factors in glaucoma: a review. Clin. Exp. Ophthalmol. 2011, 39, 252–258. [Google Scholar] [CrossRef]
- Gupta, S.K.; Agarwal, R.; Agarwal, P.; Saxena, R.; Agrawal, S.S. Current concepts in the pathophysiology of glaucoma. Indian J. Ophthalmol. 2009, 57, 257–266. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Fan, X.; Ying, Y.; Zhai, R.; Sheng, Q.; Sun, Y.; Xu, H.; Kong, X. The characteristics of fundus microvascular alterations in the course of glaucoma: a narrative review. Ann. Transl. Med. 2022, 10, 527. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, M.; Liu, H.; Mercieca, K.; Prinz, J.; Feng, Y.; Prokosch, V. The Association between Vascular Abnormalities and Glaucoma—What Comes First? Int. J. Mol. Sci. 2023, 24, 13211. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.; Anders, F.; Liu, H.; Brockhaus, K.; Liu, A.; Grus, F.H.; Pfeiffer, N.; Thanos, S.; Prokosch, V. Erhöhter Augeninnendruck für 7 Wochen induziert lokale Gefäßveränderungen im experimentellen Glaukommodell in vivo [Morphological and Quantitative Changes in Retinal and Optic Nerve Vessels in Experimental Glaucoma Model with Elevated IOP for 7 Weeks]. Klin Monbl Augenheilkd, 2019; 236, 871–876. [Google Scholar] [CrossRef]
- Na, K.I.; Jeoung, J.W.; Kim, Y.K.; Lee, W.J.; Park, K.H. Incidence of Open-angle Glaucoma in Newly Diagnosed Retinal Vein Occlusion: A Nationwide Population-based Study. Eur. J. Gastroenterol. Hepatol. 2019, 28, 111–118. [Google Scholar] [CrossRef]
- Jonas, J.B.; Fernández, M.C.; O Naumann, G. Parapapillary atrophy and retinal vessel diameter in nonglaucomatous optic nerve damage. . 1991, 32, 2942–7. [Google Scholar]
- Frisén, L.; Claesson, M. Narrowing of the Retinal Arterioles in Descending Optic Atrophy. Ophthalmology 1984, 91, 1342–1346. [Google Scholar] [CrossRef]
- Shin, J.D.; Wolf, A.T.; Harris, A.; Vercellin, A.V.; Siesky, B.; Rowe, L.W.; Packles, M.; Oddone, F. Vascular biomarkers from optical coherence tomography angiography and glaucoma: where do we stand in 2021? Acta Ophthalmol. 2021, 100, E377–E385. [Google Scholar] [CrossRef] [PubMed]
- Banou, L.; Dastiridou, A.; Giannoukas, A.; Kouvelos, G.; Baros, C.; Androudi, S. The Role of Color Doppler Imaging in the Diagnosis of Glaucoma: A Review of the Literature. Diagnostics 2023, 13, 588. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Chavane, F.; Beylerian, M.; Callet, M.; Denis, D.; Matonti, F. Morphologic Analysis of Peripapillary Retinal Arteriole Using Adaptive Optics in Primary Open-angle Glaucoma. Eur. J. Gastroenterol. Hepatol. 2020, 29, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rovira, A.; MacGillivray, T.; Trucco, E. et al. / VAMPIRE: Vessel Assessment and Measurement Platform for Images of the REtina. 2011 ANNUAL INTERNATIONAL CONFERENCE OF THE IEEE ENGINEERING IN MEDICINE AND BIOLOGY SOCIETY (EMBC). NEW YORK: IEEE, 2011. pp. 3391. [Google Scholar]
- Cheung, C.Y.; Tay, W.T.; Mitchell, P.; Wang, J.J.; Hsu, W.; Lee, M.L.; Lau, Q.P.; Zhu, A.L.; Klein, R.; Saw, S.M.; et al. Quantitative and qualitative retinal microvascular characteristics and blood pressure. J. Hypertens. 2011, 29, 1380–1391. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Cheung, C.Y.-L.; Saw, S.M.; Mitchell, P.; Aung, T.; Wong, T.Y. Retinal Vascular Geometry and Glaucoma: The Singapore Malay Eye Study. Ophthalmology 2012, 120, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Garhofer, G.; Bek, T.; Boehm, A.G.; Gherghel, D.; Grunwald, J.; Jeppesen, P.; Kergoat, H.; Kotliar, K.; Lanzl, I.; Lovasik, J.V.; et al. Use of the retinal vessel analyzer in ocular blood flow research. Acta Ophthalmol. 2009, 88, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Shao, Q.; Scharf, D.; Joussen, A.M.; Heussen, F.M. Retinal vessel diameter measurements by spectral domain optical coherence tomography. Graefe's Arch. Clin. Exp. Ophthalmol. 2014, 253, 499–509. [Google Scholar] [CrossRef]
- Pellegrini, E.; Robertson, G.; Trucco, E.; MacGillivray, T.J.; Lupascu, C.; van Hemert, J.; Williams, M.C.; Newby, D.E.; van Beek, E.J.; Houston, G. Blood vessel segmentation and width estimation in ultra-wide field scanning laser ophthalmoscopy. Biomed. Opt. Express 2014, 5, 4329–37. [Google Scholar] [CrossRef]
- Bakker, E.; Dikland, F.A.; van Bakel, R.; De Jesus, D.A.; Brea, L.S.; Klein, S.; van Walsum, T.; Rossant, F.; Farías, D.C.; Grieve, K.; et al. Adaptive optics ophthalmoscopy: a systematic review of vascular biomarkers. Surv. Ophthalmol. 2021, 67, 369–387. [Google Scholar] [CrossRef]
- Akyol, E.; Hagag, A.M.; Sivaprasad, S.; Lotery, A.J. Adaptive optics: principles and applications in ophthalmology. Eye 2020, 35, 244–264. [Google Scholar] [CrossRef]
- Gallo, A.; Mattina, A.; Rosenbaum, D.; Koch, E.; Paques, M.; Girerd, X. Retinal arteriolar remodeling evaluated with adaptive optics camera: Relationship with blood pressure levels. Ann. de Cardiol. et d'Angéiologie 2016, 65, 203–207. [Google Scholar] [CrossRef] [PubMed]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br. J. Ophthalmol. 2021, 105, 1–169. [CrossRef] [PubMed]
- Samelska, K.; Szaflik, J.P.; Śmigielska, B.; Zaleska-Żmijewska, A. Progression of Rare Inherited Retinal Dystrophies May Be Monitored by Adaptive Optics Imaging. Life 2023, 13, 1871. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Parravano, M.; Serrao, S.; Ducoli, P.; Stirpe, M.; Lombardo, G. Analysis of retinal capillaries in patients with type 1 diabetes and nonproliferative diabetic retinopathy using adaptive optics imaging. Retina 2013, 33, 1630–1639. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.S. Controversies in the vascular theory of glaucomatous optic nerve degeneration. Taiwan J. Ophthalmol. 2016, 6, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Flammer, J.; Konieczka, K.; Flammer, A.J. The Role of Ocular Blood Flow in the Pathogenesis of Glaucomatous Damage. US Ophthalmic Rev. 2011, 4, 84. [Google Scholar] [CrossRef]
- Takayanagi, Y.; Takai, Y.; Kaidzu, S.; Tanito, M. Association between Systemic Antioxidant Capacity and Retinal Vessel Diameters in Patients with Primary-Open Angle Glaucoma. Life 2020, 10, 364. [Google Scholar] [CrossRef]
- Garhöfer, G.; Bata, A.M.; Popa-Cherecheanu, A.; Hommer, A.; Vass, C.; Resch, H.; Schmidl, D.; Werkmeister, R.M.; Schmetterer, L. Retinal Oxygen Extraction in Patients with Primary Open-Angle Glaucoma. Int. J. Mol. Sci. 2022, 23, 10152. [Google Scholar] [CrossRef]
- Gugleta, K.; Kochkorov, A.; Waldmann, N.; Polunina, A.; Katamay, R.; Flammer, J.; Orgul, S. Dynamics of retinal vessel response to flicker light in glaucoma patients and ocular hypertensives. Graefe's Arch. Clin. Exp. Ophthalmol. 2011, 250, 589–594. [Google Scholar] [CrossRef]
- Feke, G.T.; Pasquale, L.R. Retinal Blood Flow Response to Posture Change in Glaucoma Patients Compared with Healthy Subjects. Ophthalmology 2008, 115, 246–252. [Google Scholar] [CrossRef]
- Gardiner, S.K.; Cull, G.; Fortune, B. Retinal Vessel Pulsatile Characteristics Associated With Vascular Stiffness Can Predict the Rate of Functional Progression in Glaucoma Suspects. Investig. Opthalmology Vis. Sci. 2023, 64, 30–30. [Google Scholar] [CrossRef]
- Mautuit, T.; Semecas, R.; Hogg, S.; Daien, V.; Gavard, O.; Chateau, N.; MacGillivray, T.; Trucco, E.; Chiquet, C. Comparing Measurements of Vascular Diameter Using Adaptative Optics Imaging and Conventional Fundus Imaging. Diagnostics 2022, 12, 705. [Google Scholar] [CrossRef] [PubMed]
- De Ciuceis, C.; Rosei, C.A.; Caletti, S.; Trapletti, V.; Coschignano, M.A.; Tiberio, G.A.; Duse, S.; Docchio, F.; Pasinetti, S.; Zambonardi, F.; et al. Comparison between invasive and noninvasive techniques of evaluation of microvascular structural alterations. J. Hypertens. 2018, 36, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Arichika, S.; Uji, A.; Ooto, S.; Muraoka, Y.; Yoshimura, N. Comparison of retinal vessel measurements using adaptive optics scanning laser ophthalmoscopy and optical coherence tomography. Jpn. J. Ophthalmol. 2016, 60, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xu, L.; Wang, Y.; Wang, Y.; Jonas, J.B. Retinal vessel diameter in normal and glaucomatous eyes: the Beijing eye study. Clin. Exp. Ophthalmol. 2007, 35, 800–807. [Google Scholar] [CrossRef]
- Jonas JB, Nguyen XN, Naumann GO. Parapapillary retinal vessel diameter in normal and glaucoma eyes. I. Morphometric data. Invest Ophthalmol Vis Sci. 1989;30(7):1599-1603.
- Rader, J.; Feuer, W.J.; Anderson, D.R. Peripapillary Vasoconstriction in the Glaucomas and the Anterior Ischemic Optic Neuropathies. Arch. Ophthalmol. 1994, 117, 72–80. [Google Scholar] [CrossRef]
- Zhang, Q.; Jan, C.; Guo, C.Y.; Wang, F.H.; Liang, Y.B.; Cao, K.; Zhang, Z.; Yang, D.Y.; Thomas, R.; Wang, N.L.; et al. Association of intraocular pressure-related factors and retinal vessel diameter with optic disc rim area in subjects with and without primary open angle glaucoma. Clin. Exp. Ophthalmol. 2017, 46, 389–399. [Google Scholar] [CrossRef]
- Chiquet, C.; Gavard, O.; Arnould, L.; Mautuit, T.; Macgillivray, T.J.; Bron, A.M.; Semecas, R.; Trucco, E.; Florent, A. Retinal vessel phenotype in patients with primary open-angle glaucoma. Acta Ophthalmol. 2019, 98, e88–e93. [Google Scholar] [CrossRef]
- Cheng, J.; Zhao, H.; Jiang, C.; Kong, X.; Sun, X. Change of Retinal Vessels in Different Sectors of the Parapapillary Area in Primary Open-Angle Glaucoma. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Koch, E.; Rosenbaum, D.; Brolly, A.; Sahel, J.-A.; Chaumet-Riffaud, P.; Girerd, X.; Rossant, F.; Paques, M. Morphometric analysis of small arteries in the human retina using adaptive optics imaging. J. Hypertens. 2014, 32, 890–898. [Google Scholar] [CrossRef]
- Zaleska-Żmijewska, A.; Wawrzyniak, Z.M.; Dąbrowska, A.; Szaflik, J.P. Adaptive Optics (rtx1) High-Resolution Imaging of Photoreceptors and Retinal Arteries in Patients with Diabetic Retinopathy. J. Diabetes Res. 2019, 2019, 1–12. [Google Scholar] [CrossRef]
- Meixner, E.; Michelson, G. Measurement of retinal wall-to-lumen ratio by adaptive optics retinal camera: a clinical research. Graefe's Arch. Clin. Exp. Ophthalmol. 2015, 253, 1985–1995. [Google Scholar] [CrossRef]
- Lim, L.S.; Saw, S.M.; Cheung, N.; Mitchell, P.; Wong, T.Y. Relationship of Retinal Vascular Caliber with Optic Disc and Macular Structure. Arch. Ophthalmol. 2009, 148, 368–375. [Google Scholar] [CrossRef]
- Hall, J.K.; Andrews, A.P.; Walker, R.; Piltz-Seymour, J.R. Association of retinal vessel caliber and visual field defects in glaucoma. Arch. Ophthalmol. 2001, 132, 855–859. [Google Scholar] [CrossRef]
- De Leon, J.M.S.; Cheung, C.Y.; Wong, T.-Y.; Li, X.; Hamzah, H.; Aung, T.; Su, D.H.-W. Retinal vascular caliber between eyes with asymmetric glaucoma. Graefe's Arch. Clin. Exp. Ophthalmol. 2015, 253, 583–589. [Google Scholar] [CrossRef]
- Lin, T.P.H.; Wang, Y.M.; Ho, K.; Wong, C.Y.K.; Chan, P.P.; Wong, M.O.M.; Chan, N.C.Y.; Tang, F.; Lam, A.; Leung, D.Y.L.; et al. Global assessment of arteriolar, venular and capillary changes in normal tension glaucoma. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Mitchell, P.; Leung, H.; Wang, J.J.; Rochtchina, E.; Lee, A.J.; Wong, T.Y.; Klein, R. Retinal vessel diameter and open-angle glaucoma: The Blue Mountains Eye Study. Ophthalmology 2005, 112, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Amerasinghe, N.; Aung, T.; Cheung, N.; Fong, C.W.; Wang, J.J.; Mitchell, P.; Saw, S.-M.; Wong, T.Y. Evidence of Retinal Vascular Narrowing in Glaucomatous Eyes in an Asian Population. Investig. Opthalmology Vis. Sci. 2008, 49, 5397–5402. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, R.; Wang, J.J.; Rochtchina, E.; Lee, A.J.; Wong, T.Y.; Mitchell, P. Retinal Vessel Caliber Is Associated with the 10-year Incidence of Glaucoma. Ophthalmology 2013, 120, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.P.; Hui, H.Y.; Ling, A.; Chan, P.P.; Shen, R.; Wong, M.O.; Chan, N.C.; Leung, D.Y.; Xu, D.; Lee, M.L.; et al. Risk of Normal Tension Glaucoma Progression From Automated Baseline Retinal-Vessel Caliber Analysis: A Prospective Cohort Study. Arch. Ophthalmol. 2022, 247, 111–120. [Google Scholar] [CrossRef]
- Yoo, E.; Yoo, C.; Lee, T.-E.; Kim, Y.Y. Retinal vessel diameter in bilateral glaucoma suspects: comparison between the eye converted to glaucoma and the contralateral non-converted eye. Graefe's Arch. Clin. Exp. Ophthalmol. 2016, 254, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Rong, X.; Cai, Y.; Li, M.; Fang, Y.; Tian, T.; Pan, Y. Peripapillary retinal artery in first diagnosed and untreated normal tension glaucoma. BMC Ophthalmol. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Loo, J.H.; Wang, Z.; Chong, R.S. Caveolin-1 in vascular health and glaucoma: A critical vascular regulator and potential therapeutic target. Front. Med. 2023, 10, 1087123. [Google Scholar] [CrossRef]
- Gericke, A.; Mann, C.; Zadeh, J.K.; Musayeva, A.; Wolff, I.; Wang, M.; Pfeiffer, N.; Daiber, A.; Li, H.; Xia, N.; et al. Elevated Intraocular Pressure Causes Abnormal Reactivity of Mouse Retinal Arterioles. Oxidative Med. Cell. Longev. 2019, 2019, 1–12. [Google Scholar] [CrossRef]
- Zhang, S.; Wu, C.; Liu, L.; Jia, Y.; Zhang, Y.; Zhang, Y.; Zhang, H.; Zhong, Y.; Huang, D. Optical Coherence Tomography Angiography of the Peripapillary Retina in Primary Angle-Closure Glaucoma. Arch. Ophthalmol. 2017, 182, 194–200. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Clinical characteristics of the groups.
| Parameters | group A | group B | group C | Control group | p-value† |
|---|---|---|---|---|---|
| total number of eyes | 37 | 48 | 26 | 70 | 0,370 |
| age (m ± SD) (years) | 51,1±7,8 | 52,7±8,2 | 53,5±8,8 | 50,5±5,9 | 0,232 |
| sex (men/female) | 12/25 | 24/24 | 11/15 | 26/44 | 0,489 0,559§ |
| BMI (m ± SD) (kg/m2) | 23,6±2,4 | 24,3±1,8 | 24,3±2,0 | 23,8±2,2 | 0,358 |
| SBP (m ± SD) (cm Hg) |
124,4±11,4 | 126,7±11,8 | 126,9±9,9 | 121,5±11,9 | 0,404‡ |
| DBP (m ± SD) (cm Hg) |
77,9±8,4 | 78,4±7,6 | 78,3±7,3 | 78,7±8,7 | 0,876 |
| BCVA (m ± SD) | 0,905±0,118 | 0,908±0,133 | 0,865±0,147 | 0,989±0,040 | <0,001† A**, B*, C*** vs Control*** |
| IOP (m ± SD) (cm Hg) |
13,2±2,6 | 13,2±2,5 | 13,0±2,8 | 15,2±2,5 | <0,001† A**, B**, C** vs Control** |
| AL (m ± SD) (mm) | 24,0±0,9 | 24,4±1,2 | 23,9±1,3 | 23,5±0,9 | 0,905‡ B*** vs Control*** |
| Lens status (Pseudophakic) [(%)] | 2 (5,4%) | 4 (8,3%) | 5 (23,1%) | 3 (4,3%) |
* p<0,05; **p<0,01; ***p<0,001; †Kruskal-Wallis test; ‡test Chi2; §Mann-Whitney test for proportion female and man; m – mean; SD -standard deviation; BMI - Body Mass Index; SBP -systolic blood pressure; DBP - diastolic blood pressure; BCVA - best corrected visual acuity; IOP - intraocular pressure; AL - axial length; n- number.
Table 2.
Characteristics of the disease severity in the glaucoma groups.
| Parameters | Group A | Group B | Group C | p-value† |
|---|---|---|---|---|
| Duration of glaucoma (m ± SD) (years) | 7,1 ±4,3 | 8,2±5,2 | 9,0±6,0 | 0,489 |
| Cup to disc ratio (m ± SD) | 0,554 ±0,051 | 0,590±0,031 | 0,815±0,067 | <0,001 A***, B*** vs C*** |
| RNFL (m ± SD) (µm) | 87,3± 10,0 | 83,3±10,7 | 72,6 ±13,9 | <0,001 A***, B*** vs C*** |
| GCC (m ± SD) (µm) | 90,0±11,2 | 84,4±9,7 | 74,0±13,7 | <0,001A***, B*** vs C*** |
| Rim area (m ± SD) (mm) | 0,873±0,262 | 0,857±0,367 | 0,656±0,381 | <0,001 A***, B** vs C*** |
| MD (m ± SD) (dB) | 0,02 ±1,02 | -1,99 ±1,74 | -9,45±2,95 | <0,001 A*** vs B***, A*** vs C***, B***vs C*** |
| PSD (m ± SD) (dB) | 1,58±0,3 | 3,6 ±1,9 | 10,54±3,58 | <0,001 A*** vs B***, A*** vs C***, B***vs C*** |
**p<0,01; ***p<0,001; †Kruskal-Wallis test; M – mean; SD - standard deviation; RNFL - retinal nerve fibre layer, GCC - ganglion cell complex; MD- mean deviation; PSD - pattern standard deviation.
Table 3.
Treatment history of glaucoma patients.
| Parameters | Filtering surgery [n (%)] |
Canaloplasty [n (%)] |
SLT [n (%)] |
Monotherapy [n (%)] |
Bi therapy [n (%)] |
Tri therapy [n (%)] |
Quadric therapy [n (%)] |
|---|---|---|---|---|---|---|---|
| Groups | |||||||
| Group A | 1 (2,7%) | 4 (10,8%) | 1 (2,7%) | 21 (56,8%) | 9 (24,3%) | 1 (2,7%) | 1 (2,7%) |
| Group B | 6 (12,5%) | 14 (29,2%) | 2 (4,2%) | 10 (20,8%) | 13 (27,9%) | 5 (10,4%) | 0 (0,0%) |
| Group C | 7 (18,2%) | 6 (26,9%) | 1 (3,8%) | 5 (19,2%) | 7 (26,9%) | 5 (19,2%) | 5 (7,7%) |
n-number, SLT = selective laser trabeculoplasty. Anti-glaucoma medications included alpha two adrenergic agonists, beta-blockers, carbonic anhydrase inhibitors and prostaglandins.
Table 4.
Characteristic of rtx1 supratemporal retinal artery parameters.
| Parameters | Group A | Group B | Group C | Control group | p- value† |
|---|---|---|---|---|---|
| 1WT | 13,0±2,0 | 13,1±1,4 | 13,6±2,0 | 12,0±1,2 | <0,001 A*, B***, C*** vs Control*** |
| 2WT | 12,5±1,3 | 12,9±1,2 | 13,6±1,7 | 11,4±1,1 | <0,001 A***, B***, C*** vs Control*** |
| WLR | 0,294±0,035 | 0,298±0,044 | 0,329±0,045 | 0,241±0,023 | <0,001 A***, B***, C*** vs Control*** |
| LD | 87,8±10,2 | 88,6±11,1 | 79,9±17,7 | 95,6±15,2 | <0,001 A**, B*, C*** vs Control*** |
| TD | 112,3±13,0 | 113,2±12,3 | 110,5±9,8 | 120,9±11,9 | 0,001 A*, B*, C** vs Control** |
| WCSA | 4041,9±732,3 | 4161,3±596,0 | 4148,1±663,8 | 4033,5±697,0 | 0,604 |
*p<0,05; **p<0,01; ***p<0,001; †Kruskal-Wallis test; WT - wall thickness; WLR - wall-to-lumen ratio; LD - lumen diameter; TD - total diameter; WCSA - cross-sectional area of the vascular walls.
Table 5.
Characteristic of rtx1 infratemporal retinal artery parameters.
| Parameters | Group A | Group B | Group C | Control group | p- value† |
|---|---|---|---|---|---|
| 1WT | 13,6±1,7 | 13,3±2,1 | 14,1±2,0 | 11,9±1,3 | <0,001 A***, B**, C*** vs Control*** |
| 2WT | 13,7±1,6 | 13,3±1,7 | 13,81±1,7 | 11,8±1,2 | <0,001 A***, B***, C*** vs Control*** |
| WLR | 0,307±0,034 | 0,298±0,048 | 0,336±0,047 | 0,239±0,018 | <0,001 A***, B***, C*** vs Control***, B***vs Control*** |
| LD | 90,3±11,1 | 90,3±9,7 | 84,2±12,0 | 99,4±10,3 | <0,001 A***, B***, C*** vs Control*** |
| TD | 116,6±9,9 | 115,4±13,2 | 111,2±13,8 | 123,0±11,6 | 0,003 C*** vs Control*** |
| WCSA | 4420,0±712,7 | 4338,7±801,9 | 4349,8±913,6 | 4136,5±688,6 | 0,248 |
**p<0,01; ***p<0,001; †Kruskal-Wallis test; WT - wall thickness; WLR - wall-to-lumen ratio; LD - lumen diameter; TD - total diameter; WCSA - cross-sectional area of the vascular walls.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



