
Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
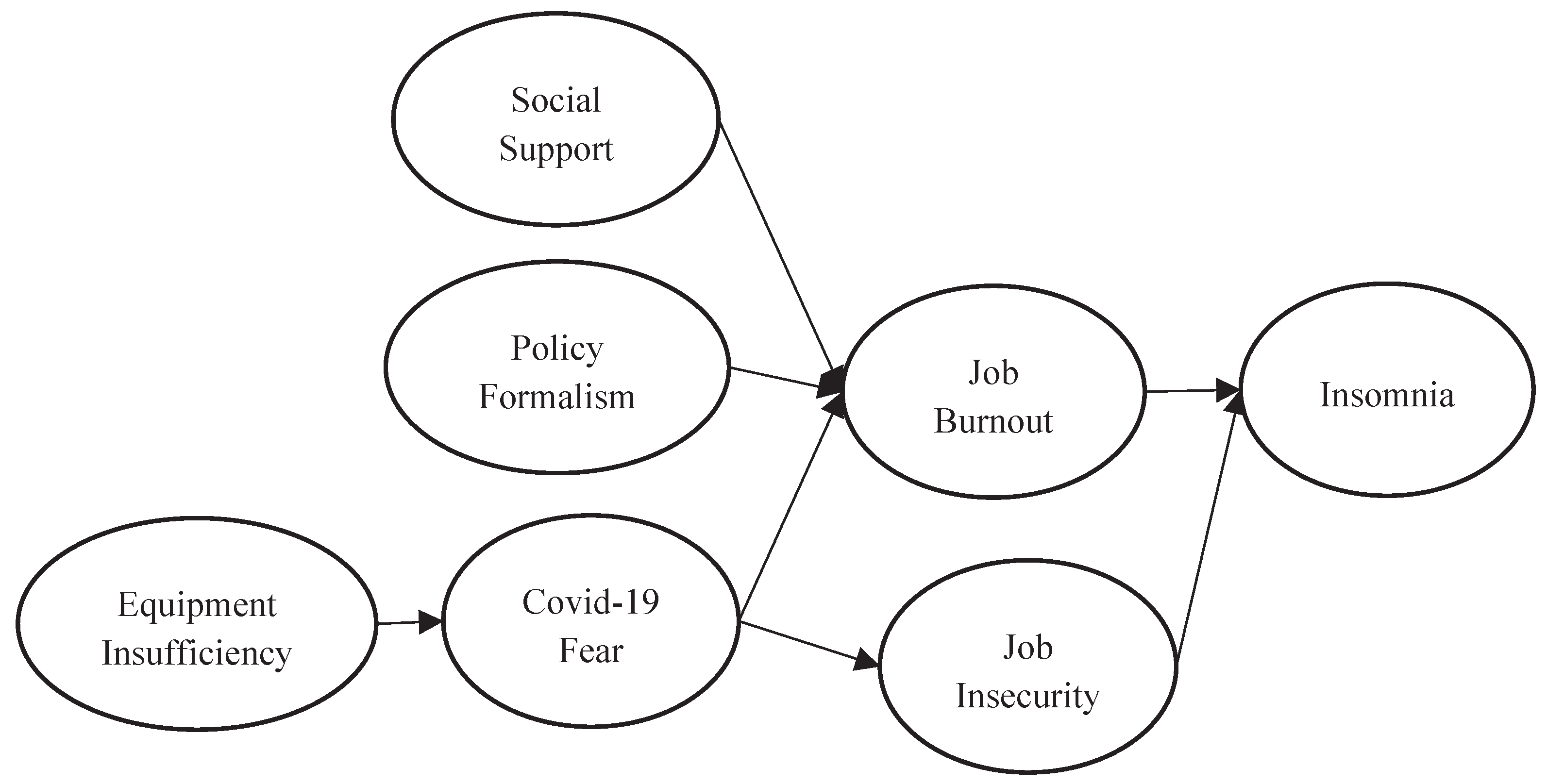
This study mainly explores the effect of policy formalism, equipment insufficiency, covid-19 fear and job insecurity on construction workers’ insomnia during the epidemic. The main contribution of this article is to introduce policy formalism into the exploration of the causes of insomnia among construction site workers during the epidemic. This study collected 733 valid samples of construction site workers. We tested the established hypotheses using confirmatory factor analysis and structural equation modeling. The research results found that equipment insufficiency positively affects Covid-19 fear. Policy formalism and Covid-19 fear positively affect job burnout. Social support negatively affects job burnout. Job burnout and job insecurity positively affect insomnia.
Keywords:
Policy Formalism
; Equipment Insufficiency
; COVID-19 Fear
; Job Insecurity
; Insomnia
1. Introduction
During the epidemic, construction sites were considered to be places where the virus spread rapidly [1]. There were many workers at the construction site, including directors, engineer, supervisor, administrator, technical staff and worker. This study refers to all the categories listed above as construction site workers. Many workers at this construction site are at risk of COVID-19 infection [2]. Social distancing policies, personal protective equipment, and video conferencing have all changed worksite operations [3,4].
During the pandemic, construction workers at the primary site faced mounting fears, insecurities, job burnout, and insomnia. Insomnia is characterized by interrupted sleep, difficulty falling asleep, and poor sleep quality, which negatively affects normal body functions and health and in turn affects daily life routines [5,6]. Insomnia can be caused by stress, anxiety, and traumatic events [7]. Studies have found that stressors related to work, family, and health—including work overload and lack of support—are the main causes of insomnia; more recently, COVID-19 anxiety has also been confirmed as a cause [8]. The current study explored whether job burnout and insecurity have an impact on insomnia among workers.
Many studies have confirmed the occurrence of severe sleep disorders during the COVID-19 pandemic [9,10]. Severe insomnia led to subsequent physical and psychological problems among frontline workers [11]. Many researchers have identified hyperarousal as a major cause of insomnia [12]. Insomnia is mostly caused by stressful situations [13]; when individuals are unable to cope with the challenges of stressful events, it can be difficult to fall asleep. The COVID-19 outbreak inevitably also contributed to job burnout and insomnia among construction site workers.
Job burnout is a symptom of prolonged work stress [14]. It can cause emotional exhaustion, depersonalization, and diminished personal accomplishment. Emotional exhaustion causes employees to feel unmotivated to work [15]. Depersonalization occurs when an individual is blamed for problems at work and therefore feels negative emotions and attitudes [16]. Diminished personal accomplishment is a negative evaluation of one’s ability to perform tasks and interact with people, along with feelings of dissatisfaction and unhappiness [17]. Employees who suffer from job burnout are prone to anxiety and depression [18]. The sudden onset of COVID-19 affected many aspects of the economy, and it impacted many part-time and full-time workers [8]. Although most natural disasters are short-lived, the COVID-19 pandemic lasted 2–3 years, and during that time, one out of every five frontline workers was confirmed to have experienced job burnout [19].
Zhang found that group support reduced job burnout for psychological counselors [20]. In a study of healthcare workers, Zhao et al. found that social support enhanced workers’ self-efficacy, which in turn reduced job burnout [21]. A nursing study in South Korea found that social support was beneficial for frontline personnel to face the hardships of the pandemic [22]. Multiple studies have noted that frontline workers faced anxiety, depression, and burnout during the pandemic [23]. Job demands require employees to be committed to their work, which creates psychological and physical stress [24].
From the perspective of the conservation of resources theory, individuals who have social support resources are more likely to effectively cope with stress and reduce burnout [25]. Conversely, when individuals lack personal, social, and material resources, it is more difficult for them to cope with stress [26]. According to the conservation of resources theory, individuals will strive to acquire and conserve the physical and psychological resources they value [27]. The loss of these valuable resources can cause individuals to feel stressed. Economic crises, natural disasters, and the spread of disease can all cause individuals to feel a sense of loss in terms of resources.
According to the job demand–resources model, job demands are job requirements that tend to create job stress for workers, whereas job resources are the provision of job skills and resources that help to reduce job burnout [28]. The job demand–resources model stipulates that when job demands exceed job resources, employees are prone to burnout and health problems [29].
The outbreak of the pandemic in 2019 led to changes in working hours and workloads for many frontline workers, in addition to contributing to job burnout [30]. Furthermore, the lockdown policy during the pandemic containment period disrupted social support for workers. Some studies have demonstrated that social support during outbreaks can reduce job burnout [31]; conversely, a lack of social support can cause anxiety, depression, and insomnia in workers [32].
Many studies have emphasized the importance of personal protective equipment during a pandemic. A study by Gallop et al. revealed that the greatest fear among caregivers for HIV patients was that of being infected [33]. During the Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) outbreaks, the WHO found that failure to ensure the proper use of personal protective equipment contributed to the spread of the diseases [34]. Inadequate personal protective equipment also led to a high risk of infection during the 2014 Ebola virus disease (EVD) outbreak [35]. Therefore, the lack of personal protective equipment increased the fear of COVID-19 among frontline workers [36]. Frontline workers were also concerned about transmission to their families as a result of their work [37]. Construction workers also faced fears of COVID-19 infection while working at construction sites.
Job insecurity is the feeling of powerlessness to maintain a stable job in dangerous situations [38]. Job insecurity is recognized as a source of stress in the work environment, and it has a negative impact on the physical and mental health of workers [39]. The COVID-19 pandemic created a sense of uncertainty and insecurity about future construction site work. In addition to feeding insecurities about future job stability, the COVID-19 outbreak necessitated increased safety behavior in the workplace, i.e., the need for workers to comply with protocols in the face of risky situations [40]. Being asked to conduct temperature checks, wear masks, and practice social distancing at the worksite during the pandemic were all causes of stress for workers. At the same time, high environmental stress, work overload, uncertainty, and excessive demands are known to affect the safety behavior of workers [41].
Job security is the degree to which an existing job is stable or consistently threatened [42]. Individuals’ feelings of uncertainty about job security can increase their stress levels [43]. The perception of job insecurity can lead to insomnia, and self-regulatory resource theory suggests that insomnia affects self-recovery [44]. When individuals lack sufficient resources to cope with hazardous environments, they can develop sleep disorders and sleep impairments. Economic depression, travel restrictions, and material shortages caused by the COVID-19 pandemic all affected individuals and negatively impacted the work and life aspects of construction site workers.
The main contribution of the current study was the incorporation of Riggs’ formalism into the COVID-19 study of construction site workers. When there is a discrepancy between pandemic prevention regulations and their implementation, it can lead to anxiety and job burnout among workers. Riggs described the formalism of administrative agencies mainly in the context of developing countries [45]. His criterion of using American society as a diffracted society has been challenged by scholars who argue that, although the United States is the benchmark for developed and industrialized societies, it is a mistake to claim that American society is totally devoid of formalism [46]. Some scholars have argued that prismatic societies exist not only in underdeveloped countries, but are also common in countries with different levels of development [46]. Taiwan is also gradually emerging from its status as a developing country; however, due to the influence of Asian and Chinese cultures in the past, studies have also confirmed the existence of formalism in Taiwan [47,48,49].
Formalism as proposed by Riggs involves ritualistic methods, lack of authorization, and centralization. Ritualistic methods create a gap between the norms of law and their effective implementation, along with a gap between administrative norms and realities. The absence of objective evaluation standards and the lack of pressure on civil servants to implement programs allow formalism to develop easily [45]. Riggs therefore concluded that there is a difference between administrative ritualistic procedures and the rationalistic procedures of developed countries. Ritualistic procedures are not implemented in practice, and thus leave a gap between administrative requirements and actual implementation performance. When epidemic prevention measures are not implemented in practice, workers’ psychological exhaustion and burnout increase. In countries with higher levels of formalism, the lack of shared values at the administrative level and inconsistency between governmental and social values creates a gap between administrative planning and people's expectations [50]. Workers’ job burnout therefore increases due to dissatisfaction with epidemic prevention measures at work.
2. Literature Review and Hypotheses Development
2.1. The relationship between equipment insufficiency and Covid-19 fear
During the first 2 years of the COVID-19 pandemic, rapid transmission and ease of infection led to fear among frontline workers, who were at high risk of infection due to their exposure to patients and inadequate personal protective equipment [51,52]. Early in the outbreak, frontline workers had yet to determine the route of transmission; therefore, many became infected [53]. In Spain, the lack of personal protective equipment at the beginning of the outbreak increased the risk of infection, leading to a fear of contact between frontline workers and patients [54,55]. Studies at the time confirmed the link between infection and lack of personal protective equipment for frontline workers [56], so the lack of effective and adequate personal protective equipment for workers during the pandemic naturally led to increased fear.
One study noted a relationship between personal protective equipment and psychological stress and fear [57]. Wearing personal protective equipment has been recognized as a key measure to prevent the spread of COVID-19. Personal protective equipment can protect frontline workers from droplet infection [58]. However, when personal protective equipment becomes contaminated, frontline workers discontinue its use, which increases the risk of infection for patients and workers alike [59]. Workers at construction sites experienced increased fear due to inadequate protective equipment and infections.
Hypothesis 1: Equipment insufficiency positively affects Covid-19 fear.
2.2. The relationship between social support and job burnout
Many studies have confirmed that burnout is a negative outcome of prolonged exposure to stressful events [60]. Job burnout can be summarized as emotional exhaustion caused by physical and psychological exhaustion. Maslach and Jackson defined job burnout as a syndrome of ineffectiveness, exhaustion, and ridicule that occurs in the workplace [61]. Heavy workloads and high levels of work stress can lead to job burnout [62].
Social support is recognized as a resource for dealing with stressful events [63]. Individuals who perceive higher levels of social support demonstrate more optimism and motivation when faced with difficult situations [64]. Therefore, social support is negatively correlated with job burnout [65]. Social support is characterized as interpersonal interactions and relationships that provide care and emotional attachment [66]. Individuals feel social support when they are helped by others. Social supporters are mostly coworkers, family members, and friends. Some studies have demonstrated that social support can alleviate the stressful feelings of frontline workers [67]. A study by Dir et al. suggested that social support can mediate the relationship between job burnout and stigmatization [68]. Anxiety and burnout caused by frontline work at construction sites necessitates immediate social support.
Social support is the moral or material support provided by organizations, supervisors, and co-workers. Social support reflects the quality of an individual’s social relationships and affects their physical and mental health [69]. The more social support an individual receives, the more likely it is that they will be able to cope with difficult problems. Lee et al. discovered a negative correlation between social support and job burnout [70]. In a study on transportation industry employees, Feldman et al. found that family support reduced job burnout [71]. The job demand–resources (JD-R) model is a theory that was developed to explain job burnout. Job stress and social support are important factors in the JD-R model [72]. Job stress can cause internalized tension and frustration in individuals, which in turn can lead to job burnout. Social support is a work resource that can reduce job stress and job burnout.
Frontline workers faced many job demands related to outbreak screening and control. Many frontline workers felt weary due to outbreak screening [73]. The workflows at many worksites were altered due to the outbreak, resulting in job burnout due to reduced autonomy [74]. Job resources are believed to assist in achieving goals and reducing the physical and psychological stress caused by job demands. Job resources are also thought to increase work engagement while reducing health threats caused by job demands [75]. Job demands at construction sites during the pandemic were higher than usual, and the social distancing, protective equipment, disinfection, and temperature-taking protocols implemented at construction sites due to the pandemic increased the job demands of workers.
Hypothesis 2: Social support negatively affects job burnout.
2.3. The relationship between Covid-19 fear and job burnout
Fear is a functional emotion that occurs when an individual perceives a threat. However, fear of COVID-19 infection is a dysfunctional fear that can be physically and psychologically harmful at high levels [76,77]. Furthermore, fear of COVID-19 is thought to increase job burnout, as indicated by the first responders who experienced higher levels of job burnout during the pandemic [78].
Fear is a psychological response to environmental stressors. The social distancing policy and demands for virus screening during the pandemic increased individuals’ perceived fear [79]. Quarantine, job insecurity, lifestyle changes, and the death of loved ones all contributed to this heightened sense of fear. Fear of COVID-19 is thought to be associated with job burnout as well [80]. At construction sites, workers’ first job was to face the fear of COVID-19 infection. When individuals have more resources and experience in facing situations of uncertainty, their feelings of fear can be reduced. Conversely, when individuals have low tolerance for uncertainty, they are prone to fear and anxiety [81]. COVID-19 is a novel coronavirus, having only been discovered in 2019, and this led to a high sense of uncertainty.
The lack of personal protective equipment, uncertainty surrounding the outbreak, and the lack of an effective vaccine all contributed to the fear felt by frontline workers [82]. The most worrying aspect of the COVID-19 virus was its spread by asymptomatic carriers, which was a source of stress and fear for frontline workers. At construction sites, as well, fear among workers further contributed to job burnout [82]. During the COVID-19 pandemic, the rising number of infections and the lack of resources resulted in job burnout. The risk of death from COVID-19 infection led to many psychological problems including stress, anxiety, and fear [83]. Many frontline workers experienced these negative physical and psychological problems [80]. Increased workloads, deaths of colleagues due to infection, and lack of social support all contributed to anxiety and burnout.
Hypothesis 3: Covid-19 fear positively affects job burnout.
2.4. The relationship between policy formalism and job burnout
The gap between formal power and effective power has resulted in a highly formalistic administration that centralizes power but lacks administrative efficiency. The COVID-19 pandemic came on quickly, and government agencies were often unable to respond to it accordingly, leaving construction site workers with a higher sense of job burnout. Thompson found that developing countries had a relatively large number of generalists [84], and that they emphasized hierarchy and procedures while forgetting their purely instrumental origins; generalist civil servants would incorporate programmatic procedures into the law, forgetting that they were merely tools. Even scholars have pointed out that the generalists in developing countries are superior to the professionals [85].
Bureaucracies with a high degree of formalism are full of pathological behavior, such as lack of authorization, over-emphasis of control, red tape, indifference, and fear of innovation. Most civil servants wait for orders from the top and lack a sense of personal security [86]. When faced with the inaccurate implementation of epidemic policies, workers are prone to feel a higher level of job burnout. Burns and Stalker argued that in organizations with an organic model, the responsibilities and duties of professionals are not clearly defined; work content is generated through continuous interaction with colleagues, and not everything is decided by the supervisor [87]. In a mechanistic system, the supervisor decides whether the work of the professionals aligns with the goals of the organization. Most formalist government agencies belong to the mechanistic system. During the pandemic, the influence of administrative generalists exceeded that of professionals, which made it easier for a gap to form between the pandemic prevention laws and their actual implementation. It is difficult for a developing country to implement organizations with an organic model [88], because the flexible design causes anxiety for executives [87]. Organic systems require a sense of trust among members, which developing countries often lack [89].
Countries with a low degree of formalism encourage creativity and motivate civil servants to achieve their goals. However, countries with a high degree of formalism are characterized by authoritarianism and inherent work practices that inhibit creativity [90]. Administrations in developing countries are characterized by “irrational management”. Due to the lack of authorization, many minor decisions must be made by administrative executives. Many civil servants in developing countries set themselves apart from the general public—they are mainly concerned with their own interests, and care little about the public interest [90]. During the COVID-19 outbreak, many delays in handling the crisis were attributable to civil servants waiting for orders from their superiors. When construction site workers feel higher policy formalism will increase their job burnout.
Hypothesis 4: Policy formalism positively affects job burnout.
2.5. The relationship between Covid-19 fear and job insecurity
For the general public, concerns about COVID-19 infection could be attributed to the high infection and mortality rates [76]. Later studies also associated fear of COVID-19 with job insecurity, psychological stress, and anxiety [76]. Job security is an important tool for securing personal resources [91]; therefore, job insecurity can easily lead to fear of poverty, stigmatization, and social exclusion [92]. Literature has confirmed the association of job insecurity with anxiety, depression, and mental health [39].
Frone found that in times of economic downturn, individuals experience job insecurity through pay cuts, reduced hours, and physical and mental anguish [93]. During the early stages of the pandemic, the rapid spread of COVID-19 led to urban lockdowns and increased remote work. Company closures caused by the pandemic caused employees to experience job insecurity [94]. Furthermore, uncertainty about the future of the economy at the time caused many people to worry about their family finances.
Sudden destabilizing events can cause social, economic, and psychological disruptions to an individual’s life. The COVID-19 pandemic affected paychecks and employment and sparked family–work conflicts [95]. It led to a decrease in job opportunities, and the resulting financial stress caused individuals to become anxious. Indeterminate stressors increased job insecurity, which in turn created anxiety, restlessness, and depression in individuals. The economic downturn caused by the pandemic also contributed to psychological depression among workers [96].
Depression and anxiety caused by the pandemic affected the mood in the workplace. Work tasks and priorities were altered following the escalation of the outbreak. Fear of the pandemic, insecurity, and loss of income all contributed to the loss of psychological resources [97]. From the perspective of conservation of resources theory, job insecurity makes it necessary to expend energy to cope with stressful situations. Herzberg asserted that job security is the combination of a stable work environment and employment protection, i.e., retirement security, stable salary, and opportunities for self-development and advancement [98]. Therefore, job security encompasses the provision of financial, economic, and social security within an organization [98]. Fear of COVID-19 is thought to influence the relationship between job insecurity and depression [99].
Hypothesis 5: Covid-19 fear positively affects job insecurity.
2.6. The relationship between job burnout and insomnia
High levels of emotional and physical exhaustion tend to cause sleep problems. Cognitive and emotional demands in the workplace make it difficult for workers to fall asleep [100]. COVID-19 posed new challenges and threats to the workplace. Frontline workers faced a high risk of contracting the virus during the pandemic [101]. Their stress factors included lack of personal protective equipment, high workloads, quarantine, and loss of loved ones [102].
Prolonged anxiety about the pandemic led to insomnia, stress disorders, and job burnout [103]. Furthermore, long shifts and working hours were required during this period, something known to cause work stress, insomnia, and fatigue problems. Working late shifts can result in poor sleep quality and difficulty falling asleep. Prolonged exposure to emotionally challenging work can lead to physical and mental health problems [104]. Job burnout occurs when individuals experience chronic stress that is difficult to cope with in the workplace. The relationship between job burnout and insomnia has been explored, and it has been determined that increased job burnout causes insomnia and psychological exhaustion [105]. Workers at construction sites during the pandemic often suffered from insomnia due to job burnout.
Hypothesis 6: Job burnout positively affects insomnia.
2.7. The relationship between job insecurity and insomnia
Davy, Kinicki, and Scheck defined job insecurity as an individual’s expectation of job continuity [106]. Perceived job insecurity is heightened when the job is threatened by uncertainty. Insecurity is a precursor to long-term personal stress and leaves employees feeling that they are powerless to determine their own job continuity. Workers’ fear and dread about their jobs is job insecurity [42]. Such worries and fears can lead to insomnia, depriving workers of the sleep needed to maintain energy and motivation. Poor sleep quality makes it difficult to relieve fatigue, and inability to concentrate due to insomnia can lead to workplace safety problems [107].
Multiple studies have pointed to job insecurity as a source of stress that exacerbates insomnia problems [108]. Worrying about lack of job continuity leads to stress and insomnia. Sleep is a way for individuals to regain energy and cognitive clarity, as well as a means to recover self-regulating resources. Additionally, sleep grants individuals sufficient resources to respond to safety regulations [109]. Studies have indicated that people with sleep problems are more likely to have work accidents [110]. Work stress, work overload, and role conflicts due to job demands are all factors that contribute to insomnia, and workers were subjected to greater job demands during the pandemic.
Hypothesis 7: Job insecurity positively affects insomnia.
We draw out the Research Framework based on the above hypothesis argument.
Figure 1.
Research Framework.
3. Materials and Methods
3.1. Sample, Tools, and Procedure
This study takes construction site workers in Taiwan as the research subjects. The Taiwan government announced on May 1, 2023 that the epidemic prevention threat had been lowered. We obtained a total of 733 valid construction site worker samples from 2022-early 2023, with a recovery rate of 48.3%. Demographic information of respondents: male accounts for 72.0%. In terms of occupation category, Director accounts for 3.0%, Engineer accounts for 3.1%, Supervisor accounts for 3.3%, Administrators account for 17.7%, Technical staff accounts for 14.9%, Workers account for 58.00%. This study advocates that all construction site workers are affected by epidemic prevention policies during the epidemic. Among the respondents, 49.8% of construction site workers have more than 8 years of experience. A total of 63.6% of the respondents are married.

Table 1.
Sample basic information.
| Gender | Percentage (%) | Seniority | Percentage (%) |
|---|---|---|---|
| Male | 72.0 % | 1-3 years | 34.1 % |
| Female | 28.0 % | 4-7 years | 16.1 % |
| Age | 8-11 years | 13.5 % | |
| 20–29 years old | 25.0 % | 12-15 years | 5.7 % |
| 30–39 years old | 43.0 % | 16 years or above | 30.6 % |
| 40–49 years old | 9.1 % | Marriage | |
| 50 years old or older | 22.9 % | Unmarried | 31.2 % |
| Occupation | Married | 63.6 % | |
| Director | 3.0 % | other | 5.2 % |
| Engineer | 3.1 % | ||
| Supervisor | 3.3 % | ||
| Administrator | 17.7 % | ||
| Technical staff | 14.9 % | ||
| Worker | 58.00% |
3.2. Measures
Social Support was modified with reference to the scale of Sarason et al. [111]. Example items are as follows: I can share my most private worries and fears with colleagues. There is someone I can turn to for advice about handling problems with my job. When I need suggestions on how to deal with a personal problem, I know someone I can turn to. If a family crisis arose, it would be difficult to find someone who could give me good advice about how to handle it. Job burnout refers to the scale of Maslach et al. [14]. Example items are as follows: I feel burned out from my work. I have become more callous toward people since I took this job. I feel burned out from my work. Covid-19 Fear refers to the scale developed by Ahorsu et al. [76]. Example items are as follows: I am most afraid of coronavirus-19. It makes me uncomfortable to think about coronavirus-19. I worry a lot about coronavirus-19. Coronavirus-19 is almost always terminal. Equipment insufficiency refers to the Cohen and Rodgers article [112] and designs the following items: There are not enough personal face masks at the construction site. I can't assign eye protection to every job. Gloves are not easy to obtain. Personal epidemic prevention equipment is a scarce resource. Job insecurity refers to the scale developed by Vander Elst and others [113] and designs the following items: Chances are, I will soon lose my job. I am sure I can keep my job(R). I feel insecure about the future of my job. I think I might lose my job in the near future. Insomnia refers to the Pittsburgh Sleep Quality Index [114] and designs the following items: I couldn't fall asleep within 30 minutes. I would wake up suddenly in the middle of the night or early in the morning. I would have nightmares while sleeping.
Based on the definition of policy formalism and questionnaires used in the past, the following items are designed: I believe that the actual implementation of epidemic prevention regulations and construction sites will not be exactly the same. I think it is sometimes difficult to implement anti-epidemic protocols on construction sites. I think many anti-epidemic plans are not so easy to implement. It is believed that there are differences between anti-epidemic regulations and current construction site practices. The Cronbach's α value of each factor in this study ranges from 0.92 to 0.96 (Table 2), which is higher than the minimum reliability standard of 0.60 set by Nunnally [115].
3.3. Controlling for Common Method Variance (CMV)
Common method variance (CMV) is considered to be the variance caused by measurement error, the internal consistency bias caused by CMV should be controlled [116,117]. The self-administered questionnaire used in this study is prone to CMV problems. This study used an anonymous method to fill in the questionnaire, and used a mix of 5 and 7-point Likert scales [116]. The questionnaire is designed according to standard operating procedures, and the items are designed to be as simple and easy to understand as possible. Items that are difficult to understand, easy to misunderstand, and difficult to answer are deleted.
Harman's one factor test is considered a tool for subsequent testing [118]. In the exploratory factor analysis without rotation, the explained variance of the first factor extracted was 46.79%. The explained variance of the first factor does not exceed 50%, indicating that the CMV problem in this study is not serious.
4. Results
4.1. Validity and Reliability Analysis
This study used confirmatory factor analysis (CFA) in SEM (Structural Equation Modelling) software to test the reliability and validity of constructs. Among model overall fit measures, the SRMR of the conceptual model was 0.081. Although the SRMR is higher than the critical value of 0.05, it is still within the acceptable range. GFI=0.98 is higher than 0.90. The NNFI =0.97, NFI = 0.97, CFI = 0.97, IFI=0.97, and RFI= 0.97, all higher than the specified 0.90. These indicators confirm that the hypothetical model of this study is good. In the model parsimonious fit measures, PNFI = 0.89, and PGFI 0.81, are all higher than the critical value of 0.50. It confirms that the conceptual model and data of this study are fit.
The factor loading λ values of all the constructs in this study ranged from 0.67 to 0.94, which is higher than the 0.5 recommended by Hair, Anderson, Tatham, and Black [119]. It means that the individual items in this study have good reliability and validity. The item loading t-values of all factors have reached statistically significant levels, which also confirms the construct validity and convergent validity of this research construct. The composite reliability (CR) of the latent constructs can measure the consistency of the items in the construct. Previous scholars have proposed that the CR value must be greater than 0.7 [119]. The CR values of the latent constructs in this study ranged from 0.92-0.96. It indicates that the latent constructs in this study have good internal consistency.
The average variance extraction (AVE) is the percentage of latent constructs that can be measured by observed items. AVE can test the reliability, discriminant validity and convergent validity of research variables. The AVE values of latent constructs in this study range from 0.66 to 0.84, all greater than 0.5. It means that the latent constructs in this study have good discriminant and convergent validity.
The square root of the average variance extracted (AVE) must be higher than the correlation coefficient between constructs and is considered to have discriminant validity [120]. The lower left corner of Table 3 is the matrix of correlation coefficients between the constructs, and the diagonal is the square root of the construct’s AVE. The square roots of the constructs' AVEs in this study ranged from 0.53 to 0.83, which are all higher than the correlation coefficients between constructs. The upper right half of the table is the heterotrait–monotrait (HTMT) ratio of correlations. The HTMT values of this study are lower than 0.90, which also confirms the discriminant validity between constructs [121]. AVEs are larger than MSV and ASV, which again confirms the discriminant validity of this study [115].
The correlation matrix allows observing preliminary relationships between constructs. Policy formalism is negatively related to job burnout and insomnia, and their coefficients are 0.42 and 0.38. Covid-19 fear negatively affects job burnout, job insecurity, the coefficients are 0.78 and 0.81. It indicates that when the fear of COVID-19 among construction site workers is high, their job burnout and job insecurity will also increase. Social support negatively affects job burnout (-0.02). It means that high social support for workers can reduce their job burnout. The correlation coefficients of job burnout, job insecurity and insomnia are 0.77 and 0.62. It represents the high degree of job burnout and job insecurity of workers, which will cause Insomnia.
4.2. Path coefficients
This study uses lavaan in the R statistical programming language for path coefficient analysis and hypothesis testing [122]. It can be seen from Table 4 that equipment insufficiency positively affects Covid-19 fear and path coefficient =0.63, which supports the argument of hypothesis 1. Insufficient personal protective equipment can easily put workers on construction sites in fear of infection. Such findings are similar to previous research results conducted by Zhan et al. [8].
Social support negatively affects job burnout, with a causal coefficient of -0.17, supporting hypothesis 2. Observed from the JD-R model, social support is regarded as a resource that can reduce job burnout. During the epidemic, many virus tests, process changes, and work requirements can easily cause job burnout among construction site workers. This empirical finding is similar to the research results of Psychiatrist and Bearman [73,74]. Social support can reduce job burnout among construction site workers.
Covid-19 fear positively affects job burnout, with a causal coefficient of 0.80, supporting Hypothesis 3. Fear of COVID-19 infection is considered dysfunctional fear during the epidemic [76]. There are no existing drugs to treat COVID-19 in the early stages of its spread. Increased work demands, infections, and deaths of relatives and friends can easily cause job burnout among construction site workers.
This study found that policy formalism positively affects job burnout, with a causal coefficient of 0.16, which supports Hypothesis 4. When workers experience disparities in epidemic prevention policies and implementation at work sites, they are exposed to long-term work fear and stress. Countries with high formalism are full of pathological behavior, such as lack of authorization, over-emphasis of control, red tape, indifference, and fear of innovation. These irrational managements can easily lead to gaps between epidemic prevention policies and implementation [87]. Construction site workers suffer from job burnout due to inaccurate epidemic prevention.
Covid-19 fear positively affects job insecurity, with a causal coefficient of 0.84, which supports Hypothesis 5. Construction site workers' fear of COVID-19 makes them also worried about the continuation of work due to the epidemic. Construction site workers' fear of COVID-19 makes them also worried about the continuation of work due to the epidemic. The COVID-19 epidemic has caused disruptions in social, economic, and personal lives [95]. COVID-19 fear not only causes physical signs of fear among construction site workers, but also makes them feel unsafe at work.
This study confirms that job burnout positively affects insomnia, with a causal coefficient of 0.77, which supports Hypothesis 6. Continuous emotional exhaustion among construction site workers can easily lead to sleep disruption and insufficient sleep. Such empirical findings are similar to the research results conducted by Lee [103]. Changes in shift systems, increased worksite safety inspections, and social distancing policies have all caused worksite workers to experience burnout. Long-term stress and work burnout can cause insomnia problems.
Job insecurity positively affects insomnia, with a causal coefficient of 0.13, which supports Hypothesis 7. Past research has found that job insecurity contributes to insomnia. Social isolation, economic disruption, and job instability caused by the epidemic can easily cause insomnia among construction site workers.
5. Discussion
This study used path coefficient analysis of structural equation modeling (SEM) to verify all research hypotheses. First, this study confirms that insufficient protective equipment will increase COVID-19 fear among construction site workers. The problem of insufficient personal protective equipment has arisen during the COVID-19, Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) epidemics. These diseases all have the characteristics of sudden appearance, rapid spread, and lack of vaccines and drugs. These characteristics can easily cause COVID-19 fear among construction site workers when they lack adequate personal protective equipment [55,57].
This study confirms that social support can reduce job burnout among construction site workers. From the perspective of conservation of resources theory, social support can help construction site workers cope with work stress and burnout [25]. The job demand–resources model regards job resources as a kind of job skills and resources, which can reduce job burnout caused by job demand [29]. Construction site workers during the epidemic face many work demands and new work processes, and they need more social support to reduce work burnout.
COVID-19 fear among construction site workers has caused physical and psychological burdens on construction site workers [77]. COVID-19 fear among construction site workers further contributes to burnout [78]. Insufficient personal protective equipment at construction sites creates greater fear and burnout among construction site workers [82].
Natural disasters and epidemics require government agencies to make quick decisions and effectively implement policy plans. However, institutions in developing countries will make people feel that policies and implementation are inconsistent. Agencies in developing countries often view compliance with work processes as the primary goal, rather than using work processes as a tool to achieve policy goals [84]. Pathological behaviors with high formalism include: overemphasis on process, red tape, lack of concern for public interests, and fear of innovation [90]. Construction site workers feel that the failure to implement epidemic prevention policies will increase their emotional exhaustion.
The high infection and mortality rates of COVID-19 infection can create a sense of fear among construction site workers [76]. The epidemic has caused factory closures, economic stagnation, and remote work, all of which have increased job insecurity among construction site workers [94]. Reductions in work and financial pressure can create perceptions of job insecurity among workers on the job site.
Long-term emotional and physical exhaustion among construction site workers can easily lead to insomnia [103]. Shift changes and increased epidemic prevention work during the epidemic can easily cause burnout and insomnia among construction site workers. This study confirms that job insecurity of construction site workers affects their insomnia. Self-regulatory resource theory advocates that sleep allows individuals to restore energy. Insomnia can lead to more accidents and injuries among construction site workers [109]. It can be seen that the job insecurity caused by the epidemic has a negative impact on the safety of construction site workers.
6. Conclusions
6.1. Theoretical Implications
The greatest contribution of this study is to introduce policy formalism into the physical and psychological exploration of construction workers during the epidemic. Construction site workers feel that failure to implement epidemic prevention policies will increase their job burnout. Insomnia caused by burnout among construction site workers will increase their work accidents. Most of the past research on formalism was qualitative discussion [45]. This article uses empirical data to confirm the negative impact of formalism on construction site workers.
Secondly, this study applies and supplements the conservation of resources theory and job demand–resources model. This study confirms that policy formalism is a negative antecedent of job burnout. Construction site workers' formalistic perceptions of public policies will increase their job burnout. The physical and psychological cognition of construction site workers during the epidemic has rarely been studied. It is even rarer to incorporate the macro-psychological perceptions of public policy into research on construction site workers.
6.2. Practical Implications
If government agencies want to avoid construction site workers’ awareness of the gaps in epidemic prevention policies and implementation. Government agencies should create a fair and transparent performance evaluation system that links civil servants' performance to rewards. This can motivate civil servants to engage in job performance rather than just respond to external pressures. Secondly, government agencies should actively establish a positive and pragmatic organizational culture. Let civil servants truly care about the interests of the people while shortening the gap between policy and implementation. Some studies in the past have confirmed that formalism has a negative impact on both civil servants and the public [47,48,49].
After the COVID-19 epidemic, government agencies can foresee and plan the masks, gloves, protective clothing, and inspection equipment needed during future epidemic disasters. Obtaining trustworthy epidemic information, using social media cautiously, and seeking professional psychological support can all reduce the COVID-19 fear of construction site workers. During the epidemic, construction site workers need to stay in touch with their organizations, families, and friends, and also seek support from medical and psychological professionals. Worksite workers also need to adapt to shift changes and uncertainty about working hours during the pandemic. Construction site workers should try to maintain a regular schedule, limit the use of electronic products, and continue healthy exercise. These activities can reduce the insomnia problem of construction site workers during the epidemic.
7. Further study
Most of the past research on policy formalism was qualitative, resulting in insufficient citations of causal relationships. This study did not adopt longitudinal study, which requires a lot of time and cost. It is recommended that future researchers adopt longitudinal studies to discover causal relationships in depth. This study has collected 733 samples for analysis, and it is recommended that future researchers collect more samples for exploration. The self-reported questionnaire used in this study may have problems with recall bias, social desirability, question understanding, and selective responses. We look forward to researchers adopting more diverse research designs and methods in the future. Research using samples from Taiwan will have issues of cultural differences and bias. We look forward to more researchers from different regions around the world collecting different samples to explore in the future.
| use variable names in the paper |
| Social Support |
| Job Burnout |
| Covid-19 Fear |
| Policy Formalism |
| Equipment Insufficiency |
| Job Insecurity |
| Insomnia |
Author Contributions
“Conceptualization, Wu, T. L., Chu, T. F. and Liu, H. T.; methodology, Liu, H. T.; software, Liu, H. T.; validation, Wu, T. L. , Chu, T. F. and Liu, H. T.; formal analysis, Wu, T. L. and Liu, H. T.; investigation, Wu, T. L.; resources, Wu, T. L. , Chu, T. F. and Liu, H. T.; data curation, Wu, T. L. , Chu, T. F. and Liu, H. T.; writing—original draft preparation, Wu, T. L. , Chu, T. F. and Liu, H. T.; writing—review and editing, Wu, T. L. and Liu, H. T.; visualization, Liu, H. T.; supervision, Wu, T. L. , Chu, T. F. and Liu, H. T.
Funding
This research received no external funding/
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Liu, X.; Zhang, M.; Cheng, Q.; Zhang, Y.; Ye, G.; Huang, X.; Kang, M. Dengue fever transmission between a construction site and its surrounding communities in China. Parasites Vectors 2021, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Koh, D. Migrant workers and COVID-19. Occup. Environ. Med. 2020, 77, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Penaloza, G.A.; Saurin, T.A.; Formoso, C.T. Monitoring complexity and resilience ˜ in construction projects: the contribution of safety performance measurement systems. Appl. Ergon. 2020, 82, 102978. [Google Scholar] [CrossRef] [PubMed]
- Selleck, R.; Hassall, M.; Cattani, M. Determining the Reliability of Critical Controls in Construction Projects. Safety 2022, 8, 64. [Google Scholar] [CrossRef]
- Doi, Y. An epidemiologic review of occupational sleep research among Japanese workers. Ind. Health. 2005, 43, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J.; Doghramji, K.; Hauri, P.J.; Morin, C.M. Evaluation of chronic insomnia. An American academy of sleep medicine review. Sleep 2000, 15, 243–308. [Google Scholar]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep. 2013, 36, 1059–68. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H. China's employment stabilization policies in response to the impact of the COVID-19 pandemic. International Journal of Sociology and Social Policy 2022, 42, 201–209. [Google Scholar] [CrossRef]
- Gupta, R.; Grover, S.; Basu, A.; et al. Changes in sleep pattern and sleep quality during COVID-19 lockdown. Indian J Psychiatr 2020, 62, 370. [Google Scholar]
- Voitsidis, P.; Gliatas ,I.; Bairachtari, V., et al. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatr Res, 2020; 1307.
- Fernandez-Mendoza, J.; Vgontzas, A.N. Insomnia and its impact on physical and mental health. Curr Psychiatr Rep 2013, 15, 418. [Google Scholar] [CrossRef]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia: state of the science. Sleep Med Rev 2010, 14, 9e15. [Google Scholar] [CrossRef]
- Drake, C.L.; Friedman, N.P.; Wright Jr, K. P, et al. Sleep reactivity and insomnia: genetic and environmental influences. Sleep 2011, 34, 1179e88. [Google Scholar] [CrossRef]
- Maslach, C. Maslach, C.; and Jackson; S. E. The measure of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Chiara, P.; Luca, C.; Annalisa, P.; Chiara, R. Emotional exhaustion among healthcare professionals: The effects of role ambiguity, work engagement and professional commitment. Acta Bio. Med. Atenei Parm. 2019, 90, 60. [Google Scholar]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, e0238217. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians: A systematic review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; Sanz-Vergel, A.I. Burnout and work engagement: the JD–R approach. Ann Rev Organ Psychol Organ Behav. 2014, 1, 389–411. [Google Scholar] [CrossRef]
- Roslan, N.; Yusoff, M.; Razak, A.; Morgan, K. Burnout prevalence and its associated factors among Malaysian healthcare workers during COVID-19 pandemic: An embedded mixed-method study. Healthcare 2021, 9, 90. [Google Scholar] [CrossRef]
- Zhang, M. Research on correlation of psychological counselor’s job burnout with self-efficacy and social support and professional identity. Hunan Agric. Univ. 2016, 8, 1–55. [Google Scholar]
- Zhao, Y. G.; Li, X. X.; Cui, Y. Analysis of the impact of social support on job burnout among doctors and nurses: based on mediation effect of self-efficacy [J]. Chin. Hosp. Manage. 2019, 39, 48–50. [Google Scholar]
- Kim, Y. Nurses’ experiences of care for patients with Middle East respiratory syndrome- coronavirus in South Korea. American Journal of Infection Control 2018, 46, 781–787. [Google Scholar] [CrossRef]
- Chirico, F.; Ferrari, G.; Nucera, G.; Szarpak, L.; Crescenzo, P.; Ilesanmi, O. Prevalence of anxiety, depression, burnout syndrome, and mental health disorders among healthcare workers during the COVID-19 pandemic: a rapid umbrella review of systematic reviews. J Health Soc Sci. 2021, 6, 209–20. [Google Scholar]
- Hu, Q.; Schaufeli, W.B.; Taris, T.W. The job demands–resources model: an analysis of additive and joint effects of demands and resources. J Vocat Behav. 2011, 79, 181–90. [Google Scholar] [CrossRef]
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of work life and contribution to productivity: Assessing the moderator effects of burnout syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2425. [Google Scholar] [CrossRef]
- Ojo, A.O.; Fawehinmi, O.; Yusliza, M.Y. Examining the predictors of resilience and work engagement during the COVID-19 pandemic. Sustainability 2021, 13, 2902. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am Psychol. 1989, 44, 513–24. [Google Scholar] [CrossRef] [PubMed]
- Demerouti, E.; Bakker, A.; Nachreiner, F.; and Ebbinghaus, M. From mental strain to burnout. Eur. J. Work Organ. Psychol. 2002, 11, 423–441. [Google Scholar] [CrossRef]
- Schaufeli, W. The job demands-resources model: a ‘how to’guide to increase work engagement and prevent burnout. Organ Dyn. 2017, 46, 120–32. [Google Scholar] [CrossRef]
- Woon, L.S.-C.; Mansor, N.S.; Mohamad, M.A.; Teoh, S.H.; Leong Bin Abdullah, M.F.I. Quality of life and its predictive factors among healthcare workers after the end of a movement lockdown: The salient roles of covid-19 stressors, psychological experience, and social support. Front. Psychol. 2021, 12, 1164. [Google Scholar] [CrossRef]
- Gleason ,F.; Malone, E.; Wood, L, et al. The job demands-resources model as a framework to identify factors associated with burnout in surgical residents. J Surg Res. 2020, 247, 121–127. [CrossRef]
- Arafa, A.; Mohammed, Z.; Mahmoud, O, et al. Depressed, anxious, and stressed: what have healthcare workers on the frontlines in Egypt and Saudi Arabia experienced during the COVID-19 pandemic? J Affect Disord. 2021, 278, 365–71. [CrossRef] [PubMed]
- Gallop, R. M.; Lancee, W. J.; Taerk, G.; Coates, R. A.; Fanning, M. Fear of contagion and AIDS: Nurses’ perception of risk. AIDS Care 1992, 4, 103–109. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Clinical management of human infection with avian influenza A (H5N1) virus. Available online: https://cdn.who.int/media/docs/default-source/wpro---documents/emergency/surveillance/avian-influenza/ai_20231110.pdf?sfvrsn=5f006f99_122.
- Reidy, P.; Fletcher, T.; Shieber, C.; Shallcross, J.; Towler, H.; Ping, M.; Kenworthy, L.; Silman, N.; Aarons, E. Personal protective equipment solution for UK military medical personnel working in an Ebola virus disease treatment unit in Sierra Leone. Journal of Hospital Infection 2017, 96, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Donoso, L.M.; Moreno-Jiménez, J.; Amutio, A.; Gallego-Alberto, L.; Moreno-Jiménez, B.; Garrosa, E. Stressors, Job Resources, Fear of Contagion, and Secondary Traumatic Stress Among Nursing Home Workers in Face of the COVID-19: The Case of Spain. J Appl Gerontol. 2021, 40, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Pincha Baduge, M. S.; Moss, C.; Morphet, J. Emergency nurses’ perceptions of emergency department preparedness for an Ebola outbreak: A qualitative descriptive study. Australasian Emergency Care 2017, 20, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, L.; and Rosenblatt, Z. Job insecurity: toward conceptual clarity. Acad. Manage. Rev. 1984, 9, 438–448. [Google Scholar] [CrossRef]
- Llosa, J. A.; Menéndez-Espina, S.; Agulló-Tomás, E.; Rodríguez-Suárez, J. Job insecurity and mental health: a meta-analytical review of the consequences of precarious work in clinical disorders. An. de Psicol. 2018, 34, 211–223. [Google Scholar]
- Zhou, Z.; Goh, Y.M.; Li, Q. Overview and analysis of safety management studies in the construction industry. Saf. Sci. 2015, 72, 337–350. [Google Scholar] [CrossRef]
- Wang, D.; Wang, X.; Xia, N. How safety-related stress affects workers’ safety behavior: The moderating role of psychological capital. Saf. Sci. 2018, 103, 247–259. [Google Scholar] [CrossRef]
- Sverke, M.; Hellgren, J.; Näswall, K. No security: A meta-analysis and review of job insecurity and its consequences. J. Occup. Health Psychol. 2002, 73, 242–264. [Google Scholar] [CrossRef]
- Giunchi, M.; Emanuel, F.; Chambel Maria, J.; Ghislieri, C. Job insecurity, workload and job exhaustion in temporary agency workers (TAWs): Gender differences. Career Dev. Internatl. 2016, 21, 3–18. [Google Scholar] [CrossRef]
- Barnes, C.M.; Hollenbeck, J.R. Sleep Deprivation and Decision-Making Teams: Burning the Midnight Oil or Playing with Fire? Acad. Manag. Rev. 2009, 34, 56–66. [Google Scholar] [CrossRef]
- Riggs, F. W. An ecological approach: the 'Sala' model. In Papers in Comparative Administration; Heady F. and Stokes S. Eds.; University of Michigan Press: Ann, Arbor, 1962; pp. 19–36. [Google Scholar]
- Amaechi, Obinna; AYENI, Evans; Madu, Chidi Paul. The Prismatic Sala Model and its Relevance to Nigeria's Public Administrative System. CCU Journal of Humanities 2019, 1, 113–122. [Google Scholar]
- Liu, H.T. Analysis of formalism’s moderating effect on the relationships between role stressors and work anxiety—Viewpoints from oriental public administration. Int. J. Inf. Manag. Sci. 2015, 26, 85–101. [Google Scholar]
- Liu, H.-T. The Influence of Public Servant’s Perceived Formalism and Organizational Environmental Strategy on Green Behavior in Workplace. Sustainability 2021, 13, 11020. [Google Scholar] [CrossRef]
- Huang, F.F.-Y.; Liu, H.-T. Path Model Analysis of the Effects of Perceived Formalism, and Fear of COVID-19 on Police Officers’ PTSD and Insomnia. Behav. Sci. 2023, 13, 867. [Google Scholar] [CrossRef] [PubMed]
- Braibanti, Ralph Transnational inducement of administrative reform: a survey of scope and critique of issues. In Approaches to Development; Montgomery, J. D. and Sffin, W. J. Eds.; McGraw-Hill: New York, 1966, 133-183.
- Liu, Q.; Luo, D.; Haase, J. E.; Guo, Q.; Wang, X. Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B. X. The experiences of health- care providers during the COVID- 19 crisis in China: A qualitative study. The Lancet Global Health 2020, 8, e790–e798. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.- H.; Huang, Q.; Wang, Y.- Y.; Zeng, X.-T .; Luo, L.- S.; Pan, Z.- Y.; Yuan, Y.- F.; Chen, Z.- M.; Cheng, Z.- S.; Huang, X.; Wang, N. A.; Li, B.- H.; Zi, H.; Zhao, M.- J.; Ma, L.- L.; Deng, T.; Wang, Y.; Wang, X.- H. Perceived infection transmission routes, infection control practices, psychosocial changes, and management of COVID- 19 infected healthcare workers in a tertiary acute care hospital in Wuhan: A cross- sectional survey. Military Medical Research 2020, 7, 24.
- Wei, X.- S.; Wang, X.- R.; Zhang, J.- C.; Yang, W.- B.; Ma, W.- L.; Yang, B.- H.; Jiang, N.- C.; Gao, Z.- C.; Shi, H.- Z.; & Zhou, Q. A cluster of health care workers with COVID- 19 pneumonia caused by SARS- CoV- 2. Journal of Microbiology, Immunology and Infection 2020, 54, 54–60.
- Lázaro- Pérez, C.; Martínez- López, J. A.; Gómez- Galán, J.; López- Meneses, E. Anxiety about the risk of death of their patients in health professionals in Spain: Analysis at the peak of the covid- 19 pandemic. International Journal of Environmental Research and Public Health 2020, 17, 1–16. [Google Scholar] [CrossRef]
- Zhan, M.; Anders, R. L.; Lin, B.; Zhang, M.; Chen, X. Lesson learned from China regarding use of personal protective equipment. American Journal of Infection Control 2020, 48, 1462–1465. [Google Scholar] [CrossRef] [PubMed]
- Suárez- García, I.; de Aramayona, M.; López, M. J.; Sáez Vicente, A.; Lobo Abascal, P. SARS- CoV- 2 infection among healthcare workers in a hospital in Madrid, Spain. The Journal of Hospital Infection 2020, 106, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Ales, G.; Domingo-Relloso, A.; Arribas, J.R.; Quintana-Díaz, M.; Her´nan, M. ,´Critical Care Requirements Under Uncontrolled Transmission of SARS-CoV-2. Am J Public Health. 2021, 111, 923–926. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, J. H.; Rajamaki, B.; Ijaz, S.; Sauni, R.; Toomey, E.; Blackwood, B.; Tikka, C.; Ruotsalainen, J. H.; & Kilinc Balci, F. S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. The Cochrane Database of Systematic Reviews 2020, 4, Cd011621.
- Okamoto, K.; Rhee, Y.; Schoeny, M.; Lolans, K.; Cheng, J.; Reddy, S.; Weinstein, R. A.; Hayden, M. K.; & Popovich, K. J. Impact of doffing errors on healthcare worker self- contamination when caring for patients on contact precautions. Infection Control and Hospital Epidemiology 2019, 40, 559–565.
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demandsresource model of burnout. J Appl Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson ,S.E. The measurement of experienced burnout. J Organ Behav. 1981, 2, 99–113. [CrossRef]
- Sun, H. P.; and Liu, J. Research on the influencing factors of professional social worker retention: based on qualitative comparative analysis method (QCA). J. Soc. Work, 2017, 4, 77–85.
- Heaney, C.A.; Israel, B.A. Social networks and social support. Health Behav Health Educ Theory Res Pract. 2008, 4, 189–210. [Google Scholar]
- Schulz, R.; Decker, S. Long-term adjustment to physical disability: the role of social support, perceived control, and self-blame. J Pers Soc Psychol. 1985, 48, 1162. [Google Scholar] [CrossRef]
- Russell, S.; Subramanian, B.; Russell, PS.; et al. Psychopathology, traumatic life events, and coping skills among patients attending a primary-care adolescent clinic. Indian J Pediatr. 2012, 79, 52–59. [CrossRef] [PubMed]
- Hobfoll,S. The ecology of stress. Washington DC: Hemisphere, 1988.
- Lee, J-S.; Koeske, GF.; Sales, E. Social support buffering of acculturative stress: a study of mental health symptoms among Korean international students. Int J Intercult Relat. 2004, 28, 399–414. [CrossRef]
- Dir, AL.; Saldana, L.; Chapman, JE.; Aalsma, MC. Burnout and mental health stigma among juvenile probation officers: the moderating effect of participatory atmosphere. Adm Policy Ment Health. 2019, 46, 167–74. [CrossRef] [PubMed]
- Blumenthal, J. A.; Burg, M. M.; Barefoot, J.; Williams, R. B.; Haney, T.; and Zimet, G. Social support, type A behavior, and coronary artery disease. Psychosom. Med. 1987, 49, 331–340. [CrossRef]
- Lee, C.; Ashford, S. J.; and Bobko, P. Interative effects of type A behavior and perceived control on worker performance, job satisfaction, and somatic complaints. Acad. Manag. J. 1990, 33, 870–881. [CrossRef]
- Feldman, C. B.; Brondolo, E.; and Dayan, D. B. Sources of social support and burnout, job satisfaction and productivity. J. Occup. Health Psychol. 2002, 7, 84–93. [CrossRef]
- Schaufeli, WB.; Bakker, AB.; Van Rhenen, W. How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. J Organ Behav. 2009, 30, 893–917. [Google Scholar] [CrossRef]
- Psychiatrist, M.; Naserbakht, MM.; Psychology B, et al. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2020. [CrossRef]
- Bearman, G.; Hota, SS.; Haessler, SD. Physician burnout and healthcare epidemiology: dual implications worthy of greater scrutiny. Infect Control Hosp Epidemiol. 2020, 41, 250–1.
- Brauchli, R.; Jenny, GJ.; Füllemann, D, et al. Towards a job demandsresources health model: empirical testing with generalizable indicators of job demands, job resources, and comprehensive health outcomes. Biomed Res Int. 2015; 959621.
- Ahorsu, D.K. Ahorsu, D.K..; Lin, C.Y..; Imani, V..; Saffari, M..; Griffiths, M.D..; Pakpour, A.H.The fear of COVID-19 scale: development and initial validation. Int. J. Ment. Health Addict. 2020; 1–9. [Google Scholar]
- Sloan, M. M.; Haner, M.; Graham, A.; Cullen, F. T.; Pickett, J. T.; & Jonson, C. L. Pandemic emotions: The extent, correlates, and mental health consequences of fear of COVID-19. Sociological Spectrum 2021, 41, 1–18.
- Dimitriu, M. C.; Pantea-Stoian, A.; Smaranda, A. C.; Nica, A. A.; Carap, A. C.; Constantin, V. D.; Socea, B.; Cirstoveanu, C.; Bacalbasa, N.; Bratu, O. G.; Jacota-Alexe, F.; Badiu, C. D.; Smarandache, C. G.; & Socea, B. Burnout syndrome in Romanian medical residents in time of the COVID-19 pandemic. Medical Hypotheses, 2020, 144, 109972.
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu ,LX, et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: a large-scale cross-sectional study. EClin Med 2020, 24, 100424.
- Yıldırım ,M.; Solmaz F. COVID-19 burnout, COVID-19 stress and resilience: initial psychometric properties of COVID-19 burnout scale. Death Stud 2022, 46, 524–32. [CrossRef]
- Raja, U.; Jahanzeb ,S.; Malik, MAR.; Baig, MUA. Dispositional causes of burnout, satisfaction, and performance through the fear of COVID-19 during times of pandemic. Appl Psychol. 2022, 10, 1111.
- Zare, S.; Kazemi, R.; Izadi, A.; & Smith, A. Beyond the outbreak of COVID- 19: Factors affecting burnout in nurses in Iran. Annals of Global Health 2021, 87, 51. [PubMed]
- Brooks, S. K.; Webster, R.; Smith, L.; Woodland, L.; Wessely, S.; Greenberg, N.; & Rubin, G. J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet 2020, 395, 912–920.
- Thompson, Vietor A. Administrative objectives for development administration. Administrative Science Quarterly 1964, 9, 91–108. [CrossRef]
- Guyot, James F. Bureaucratic transformation in Burma; In Ralph Braibanti Ed.; Asian Bureaucratic Systems Emergent from the British Imperial Tradition; Duke University Press: Durham, 1966, pp. 354-443.
- Pye, L. W. Politics, Personality, and Nation Building: Burma’s Search for Identity; Yale Univ. Press: New Haven, 1962.
- Burns, T.; Stalker, G. M. The Management of Innovation; Tavistock: London, 1961. [Google Scholar]
- Milne, R. Mechanistic and organic models of public administration in developing countries. Adm. Sci. Q. 1970, 15, 57. [Google Scholar] [CrossRef]
- Bennis, W. G. A new role for the behavioral sciences: effecting organizational change. Administrative Science Quarterly 1963, 8, 125–165. [Google Scholar] [CrossRef]
- Fox, G.; Joiner, C. Perceptions of the Vietnamese public administration system. Administrative Science Quarterly 1964, 8, 443–481. [Google Scholar] [CrossRef]
- Huang, J. Z.; Han, M. F.; Luo, T. D.; Ren, A. K.; and Zhou, X. P. [Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2020, 38, 192–195.
- Rafi, M.; Mamun, M. A.; Hsan, K.; Hossain, M.; and Gozal, D. Psychological implications of unemployment among bangladesh civil service job seekers. Front. Psychiatry 2019, 10, 578. [CrossRef] [PubMed]
- Frone, M.R. What happened to the employed during the Great Recession? A U.S. Population study of net change in employee insecurity, health, and organizational commitment. J. Vocat. Behav. 2018, 107, 246–260. [Google Scholar] [CrossRef] [PubMed]
- Spurk, D.; Straub, C. Flexible employment relationships and careers in times of the COVID-19 pandemic. Journal of Vocational Behaviour 2020, 119, 103–435. [Google Scholar] [CrossRef] [PubMed]
- Kawohl, W.; & Nordt, C. COVID-19, unemployment, and suicide. The Lancet Psychiatry, 7, 389–390.
- Dozois, D. J. (2021). Anxiety and depression in Canada during the COVID-19 pandemic: A national survey. Canadian Psychology/ psychologie Canadienne 2020, 62, 136. [Google Scholar] [CrossRef]
- Jofre-Bonet, M.; Serra-Sastre, V.; and Vandoros, S. The impact of the Great Recession on health-related risk factors, behaviour and outcomes in England. Soc. Sci. Med. 2018, 197, 213–225. [CrossRef] [PubMed]
- Herzberg, F. Motivation to Work. Routledge, 2017.
- Gasparro, R.; Scandurra, C.; Maldonato, N. M.; Dolce, P.; Bochicchio, V.; Valletta, A.; and Marenzi, G. Perceived Job Insecurity and Depressive Symptoms among Italian Dentists: the Moderating Role of Fear of COVID-19. Int. J. Environ. Res. Public. Health 2020, 17, 5338. [CrossRef] [PubMed]
- Loft ,M.; Cameron, L. The importance of sleep: relationships between sleep quality and work demands, the prioritization of sleep and pre-sleep arousal in day-time employees. Work Stress 2014, 28, 289e304.
- Pappa, S.; Ntellac, V.; Giannakasc, T.; Giannakoulisc, V.; Papoutsic, E.; Katsaounouc, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun. 2020, 88, 901–7. [Google Scholar] [CrossRef]
- Abdulah, D.M.; Musa, D.H. Insomnia and stress of physicians during COVID-19 outbreak. Sleep Med. 2020, X2, 100017. [Google Scholar] [CrossRef]
- Lee, S.A.; Mathis, A.A.; Jobe, M.C. Mental health characteristics associated with dysfunctional Coronavirus Anxiety. Psychol Med. 2020, 16, 1–2. [Google Scholar] [CrossRef]
- Leiter, M.P.; Maslach, C. Burnout: 35 years of research and practice. Career. Dev. Int. 2009, 14, 204–220. [Google Scholar]
- Ekstedt, M.; Söderström, M.; Akerstedt, T.; Nilsson, J.; Søndergaard, H.P.; Aleksander, P. Disturbed sleep and fatigue in occupational burnout. Scand. J. Work Environ. Health 2006, 32, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Davy, J. A.; Kinicki, A. J.; & Scheck, C. L. A test of job security’s direct and mediated effects on withdrawal cognitions. Journal of Organizational Behavior 1997, 18, 323–349.
- Nahrgang, J.D.; Morgeson, F.P.; Hofmann, D.A. Safety at work: A meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J. Appl. Psychol. 2011, 96, 71–94. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, B.; Reisel, W.; De Witte, H. Understanding the Relationship Between Job Insecurity and Performance: Hindrance or Challenge Effect? J. Career Dev. 2019. [Google Scholar] [CrossRef]
- Kao, K.Y.; Spitzmueller, C.; Cigularov, K.; Wu, H. Linking insomnia to workplace injuries: A moderated mediation model of supervisor safety priority and safety behavior. J. Occup. Health Psychol. 2016, 21, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Durando, P.; Guglielmi, O.; Dini, G.; Bersi, F.; Fornarino, S.; Toletone, A.; Chiorri, C.; Magnavita, N. Sleep Apnea, Sleep Debt and Daytime Sleepiness Are Independently Associated with Road Accidents. A Cross-Sectional Study on Truck Drivers. PLoS ONE 2016, 11, e0166262. [Google Scholar] [CrossRef] [PubMed]
- Sarason, I.G.; Levine, H.M.; Basham, R.B., et al. Assessing social support: The Social Support Questionnaire. Journal of Personality and Social Psychology 1983, 44, 127–139. [CrossRef]
- Cohen, J; Rodgers, YVM. Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Prev Med. 2020, 141, 106263. [CrossRef]
- Vander Elst, T., De Witte, H.; & De Cuyper, N. The Job Insecurity Scale: A psychometric evaluation across five European countries. European Journal of Work and Organizational Psychology 2014, 23, 364–380.
- Buysse, DJ; Reynolds, CF 3rd; Monk, TH; Berman, SR; Kupfer, DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [CrossRef] [PubMed]
- Nunnally, J. C. Psychometric Theory; McGraw-Hill: New York, 1967. [Google Scholar]
- Podsakoff, P. M.; MacKenzie, S. B.; Lee, J. Y.; Podsakoff, N. P. Common method biases in behavioral research: a critical review of the literature and recommended remedies. Journal of Applied Psychology 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Murray, J. Y.; Kotabe, M.; Zhou, J. N. Strategic alliance-based sourcing and market performance: evidence from foreign firms operating in China. Journal of International Business Studies 2005, 36, 187–208. [Google Scholar] [CrossRef]
- Fuller, C. M.; Simmering, M. J.; Atinc, G.; Atinc, Y.; Babin, B. J. Common methods variance detection in business research. Journal of Business Research 2016, 69, 3192–3198. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate data analysis; Prentice-Hall, Inc.: Upper Saddle River, NJ, 2010. [Google Scholar]
- Hulland, J. S. Use of partial least squares (PLS) in strategic management research: a review of four recent studies. Strategic Management Journal 1999, 20, 195–204. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equa-tion modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef]
- Jöreskog, K. G.; Söbom, D. LISREL 8: Structural Equation Modeling with the SIMPLIS Command Language; Scientific Software International: Chicago, 1993. [Google Scholar]
Table 2.
Item loading and reliability.
| Variables | Items | Lambda | Z values | Composite Reliability | Cronbach’s Alpha |
|---|---|---|---|---|---|
| Policy formalism | Policy formalism 1 | 0.90 | -- | 0.95 | 0.95 |
| Policy formalism 2 | 0.92 | 109.8 | |||
| Policy formalism 3 | 0.93 | 108.2 | |||
| Policy formalism 4 | 0.90 | 104.9 | |||
| Social support | Social support1 | 0.80 | -- | 0.94 | 0.94 |
| Social support2 | 0.91 | 45 | |||
| Social support3 | 0.88 | 45.5 | |||
| Social support4 | 0.91 | 45.5 | |||
| Social support5 | 0.81 | 43.4 | |||
| Job Burnout | Job Burnout1 | 0.89 | -- | 0.96 | 0.96 |
| Job Burnout2 | 0.85 | 180.4 | |||
| Job Burnout3 | 0.94 | 191.1 | |||
| Job Burnout4 | 0.87 | 191.7 | |||
| Job Burnout5 | 0.90 | 188.8 | |||
| Job Burnout6 | 0.93 | 193.7 | |||
| Job Insecurity | Job Insecurity1 | 0.83 | -- | 0.92 | 0.92 |
| Job Insecurity2 | 0.90 | 173.3 | |||
| Job Insecurity3 | 0.86 | 173 | |||
| Job Insecurity4 | 0.87 | 180.7 | |||
| Covid-19 Fear | Covid-19 fear1 | 0.77 | -- | 0.92 | 0.92 |
| Covid-19 fear2 | 0.82 | 149.1 | |||
| Covid-19 fear3 | 0.76 | 147.8 | |||
| Covid-19 fear4 | 0.88 | 158.2 | |||
| Covid-19 fear5 | 0.88 | 162.1 | |||
| Covid-19 fear6 | 0.76 | 154.1 | |||
| Equipment Insufficiency | Equipment Insufficiency1 | 0.72 | -- | 0.82 | 0.93 |
| Equipment Insufficiency2 | 0.83 | 155.6 | |||
| Equipment Insufficiency3 | 0.67 | 143.4 | |||
| Equipment Insufficiency4 | 0.68 | 146.3 | |||
| Insomnia | Insomnia1 | 0.80 | -- | 0.93 | 0.93 |
| Insomnia2 | 0.86 | 190.3 | |||
| Insomnia3 | 0.88 | 196.9 | |||
| Insomnia4 | 0.81 | 178.6 | |||
| Insomnia5 | 0.89 | 189.3 |
Note: The first item of each variable is set to 1, so there is no Z value.
Table 3.
Square root of AVE and inter-correlations.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ASV | MSV | AVE | |
|---|---|---|---|---|---|---|---|---|---|---|
| Policy Formalism(1) | (0.91) | 0.12 | 0.46 | 0.43 | 0.39 | 0.78 | 0.41 | 0.20 | 0.54 | 0.83 |
| Covid-19 Fear(2) | 0.44 | (0.87) | 0.08 | 0.06 | 0.10 | 0.13 | 0.10 | 0.39 | 0.65 | 0.75 |
| Social Support(3) | 0.16 | 0.08 | (0.82) | 0.82 | 0.88 | 0.62 | 0.79 | 0.01 | 0.02 | 0.67 |
| Job Burnout(4) | 0.42 | 0.78 | -0.02 | (0.90) | 0.69 | 0.64 | 0.82 | 0.36 | 0.60 | 0.81 |
| Job Insecurity(5) | 0.37 | 0.81 | 0.11 | 0.65 | (0.86) | 0.53 | 0.67 | 0.31 | 0.65 | 0.75 |
| Equipment Insufficiency(6) | 0.73 | 0.58 | 0.15 | 0.61 | 0.49 | (0.73) | 0.60 | 0.30 | 0.53 | 0.53 |
| Insomnia(7) | 0.38 | 0.74 | -0.08 | 0.77 | 0.62 | 0.55 | (0.85) | 0.33 | 0.60 | 0.73 |
Note: The figures in parentheses indicate the square root of AVE of the study constructs. The lower left table on the diagonal is the Pearson correlation coefficient, and the upper right table is the heterotrait–monotrait (HTMT) ratio of correlations. MSV = maximum share variance, ASV = average share variance.
Table 4.
Path coefficients.
| Causal Path | Path Coefficient | Standard Error | Z Value | p Value | |||
|---|---|---|---|---|---|---|---|
| H1 | Equipment Insufficiency | -> | Covid-19 Fear | 0.63*** | 0.00 | 113.40 | < 0.001 |
| H2 | Social Support | -> | Job Burnout | -0.17*** | 0.01 | -33.80 | <0 .001 |
| H3 | Covid-19 Fear | -> | Job Burnout | 0.80*** | 0.01 | 118.90 | <0 .001 |
| H4 | Policy Formalism | -> | Job Burnout | 0.16*** | 0.01 | 29.00 | <0 .001 |
| H5 | Covid-19 Fear | -> | Job Insecurity | 0.84*** | 0.01 | 148.50 | <0 .001 |
| H6 | Job Burnout | -> | Insomnia | 0.77*** | 0.01 | 82.00 | <0 .001 |
| H7 | Job Insecurity | -> | Insomnia | 0.13*** | 0.01 | 14.30 | < 0.001 |
Note: **, and *** represent statistical significance at p < 0.01, and p < 0.001, respectively.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



