
Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
Febrile infections are a common cause of presentation to the emergency department (ED) in chil-dren. While viral infections are usually self-limiting, sometimes bacterial illnesses may lead to sepsis and severe complications. Inflammatory biomarkers such as C reactive protein (CRP) and procalcitonin are usually the first blood exams performed in the ED to differentiate bacterial and viral infections; the better understanding of immunochemical pathways has nowadays led to the discovery of new and more specific biomarkers that could play a role in the emergency setting. The aim of this narrative review is to provide the most recent evidence on biomarkers and predictor models combining them for serious bacterial infections (SBI) diagnosis in febrile children. Litera-ture analysis showed that inflammatory response is a complex mechanism in which many bio-chemical and immunological factors contribute to host response in SBI. CRP and procalcitonin still represent the most used biomarkers in the pediatric ED for the diagnosis of SBI. Their sensibility and sensitivity increase when combined and for this reason it is reasonable to take them both into consideration in the evaluation of a febrile children. The potential of machine learning tools, who represent a real novelty in medical practice, in conjunction with routine clinical and biological in-formation, may improve accuracy of diagnosis and target therapeutic options in SBI. However, studies on this matter are not yet validated in younger populations, making their relevance in pe-diatric precision medicine still uncertain. More data from further researches are needed to improve clinical practice and decision making using these new technologies.
Keywords:
biomarker
; C reactive protein
; interleukin
; presepsin
; procalcitonin
; serious bacterial infection.
1. Introduction
Febrile illness is a common pediatric presentation, accounting for 14-20% of attendances to the pediatric emergency department (ED) [1,2,3]. It is frequently the expression of an underlying infection, and a large proportion of these cases will be viral in origin, with a benign and self-limiting course. However, in a certain percentage of children, fever can be the manifestation of a bacterial infection which can be serious (as septicemia, meningitis, confirmed appendicitis, pneumonia, osteomyelitis, cellulitis, or complicated urinary tract infection) and the consequences of missing the diagnosis can potentially be catastrophic. Neonates and infants are at higher risk of serious bacterial infection (SBI) and may not display the same clinical features of infection and sepsis as older children, making the assessment more challenging. Distinguishing between a SBI requiring antibiotics and a viral infection is mostly a clinical decision and international evidence-based guidelines are a useful tool in that scenario [4,5].
Inflammatory biomarkers are usually the first investigations required in the ED which aid differentiating bacterial from nonbacterial infections in febrile infants and their result influences the subsequent case management. Stol et al. summarized the properties of the perfect biomarker for infections: has a positive test result in infected patient, has a negative test result in patients without an infection, distinguishes etiology, is independent of comorbidities, is a predictor of severity, is a predictor of outcome, is a quick and easy test with small variation coefficient, is affordable [6]. Currently no single biomarker has sufficient diagnostic accuracy to satisfy all these properties and the clinical context remains vital in the diagnostic and therapeutic process. In this review, we summarize the current knowledge about the role of biomarkers for SBI in children presenting with fever in the ED and we discuss the future perspective in this field. To this end, we conducted electronic research in the PubMed database from September 2018 to September 2023 to using “sepsis” OR “severe bacterial infection” AND “infant” OR “children” OR “pediatric” OR “paediatric" OR “biomarker” OR “blood culture” OR “blood cell count” OR “neutrophil count” OR “ANC” OR “C-reactive protein “ OR “CRP” OR “procalcitonin” OR “PCT” OR “inflammatory markers” OR “cytokine“ OR “IL-2” OR “IL-6” OR “IL-10” OR “IL-27” OR “soluble triggering receptor” OR “sTREM-1” OR “platelet” OR “TRAIL” OR “IP-10” OR “presepsin” as keywords. Only articles written in English were selected, and a manual search of the references of eligible articles was made.
2. Hematological biomarkers
2.1. White blood cell count (WBC) and absolute neutrophil count (ANC)
WBC and ANC have been widely used worldwide as predictors of SBI in febrile children. During a bacterial infection, neutrophils are rapidly recruited to infection sites where they evoke an immune response, bind, and ingest microorganisms by phagocytosis and kill microbes [7]. A larger number of neutrophils are consumed at the site of SBI, and they continue to be supplied to the infected site from the bone marrow via the bloodstream. Therefore, dynamic changes occur in WBC and ANC, that may reflect the real-time condition of a patient with bacterial infection. However, a recent systematic review and meta-analysis of diagnostic studies showed that the WBC offers a low sensitivity (58%) and a specificity of 73%, lower if comparted to procalcitonin (PCT) and C-reactive protein (CRP) analysis [8]. Similarly, a study that compared the WBC, ANC and CRP in relation to the onset of fever founded that CRP had a better sensitivity and specificity than either WBC or ANC, regardless of the duration of fever. Interestingly, in this study all biomarkers performed better with a duration of fever of >12 hours [9]. Van den Bruel et al. investigated the diagnostic value of laboratory tests for the diagnosis of SBI in febrile children in ambulatory settings founding that WBC probably provide some diagnostic value in ruling in serious infection, but less than PCT and PCR, and have no value at ruling it out [10].
2.2. Platelet indices
Studies have identified platelets as one of the first-line indicators in response to pathogens with participation to phagocytosis through proteins from their granules. Different platelet indices, such as PNLR (platelet-to-neutrophil/lymphocyte ratio), PNR (platelet-to-neutrophil ratio) and secreted proteins, such as sP-selectin, CXCL4, CXCL7 and serotonin have been studied as markers to discriminate viral and bacterial infection pathogenesis [11].
Considering children who access in ED with early onset of fever (<12 h), it has been observed a higher PNLR value in whose suffering from bacterial infections [12]. sP-selectin in ED may discriminate between septic and non-septic patients [12].
CXCL7 has a valid specificity and sensibility in detecting early signs of sepsis and excluding other causes of SIRS. CXCL7 and sP-selectin, alone and combined, are statistically significant to discriminate sepsis and bacterial infections from other diseases [13]. In pediatric patients in whom an acute infectious event is suspected CXCL4 and serotonin levels are not indicative in discriminating the etiology of the event in progress; CXCL4 has a role during the viral response and its elevation in blood stream is not significant in patients with sepsis or bacterial infections [14]. However, the values are not yet standardized in pediatric population and more studies are necessary to confirm normal values in healthy children and in different clinical conditions i.e. chronic inflammation, trauma, and acute infection [15]. CXCL7 and sP-selectin are promising for the future and the aim is to understand how to correlate early signs of infection to these biomarkers’ levels, improving the recognition of a bacterial infection from a viral one and contextually SBI [16].
3. Inflammatory biomarkers
3.1. C-reactive protein (CRP)
CRP is currently one of the most frequently used biomarkers for infection in the ED worldwide. It is a short pentraxin, which is synthesized in the liver following stimulation by cytokines (IL-1beta, IL-6 and TNF-alfa) within 4–6 hours after tissue injury, doubling every 8 hours and peaking at 36-50 hours [17,18]. CRP plays an important role in host defense through complement activation via the classic pathway, modulation of the function of phagocytic cells, and increase in cell-mediated cytotoxicity [19].
A rise of CRP levels can be caused by conditions other than infections, for example trauma, malignancy, rheumatologic disorders, burns, pancreatitis, and periodic fever syndromes and CRP values should be interpreted cautiously in these cases [20]. On the contrary, suppressed levels of CRP can be present in liver failure and immunocompromise patients [21]. Nevertheless, several studies demonstrate the utility of CRP for early identification of febrile children at risk for SBI [10].
A recent systematic review and meta-analysis evaluated the diagnostic value of CRP for early identification of young children at risk for SBI among those presenting with fever without source, founding that overall sensitivity was 0.74 (95% confidence interval [CI], 0.65 to 0.82) and overall specificity was 0.76 (95% CI, 0.70 to 0.81) [8].
A crucial dilemma in clinical practice is the threshold to use for the identification of SBI. A very low cut-off value will be very sensitive but poorly specific and a very high cut-off will be specific but poorly sensitive [21]. In a recent study by Verbakel et al., the cut-off value of 75 mg/L has been suggested as highlighting those children at greater risk of SBI and a CRP cut-off of 20 mg/L was suggested as being useful in identifying children at low risk of SBI [22]. CRP value must be interpreted with caution when fever has been present <12 h based on the kinetics of this biological marker [9].
Studies showed that high levels of CRP and PCT are strongly predictive of SBI in children with fever, independent of duration of disease; on the contrary, low CRP levels should not be used to rule out or confirm SBI in children with a short duration of fever and PCT seems superior to CRP in detecting SBI at an earlier stage of the disease [9,23,24].
Neonates and infants <3 months deserve specific considerations [25]. A large multicentered European study of over 2000 infants under 3 months of age admitted to a pediatric ED with fever without source found that CRP was a poor predictor of SBI [26]. A 70 mg/L cut-off had a specificity of 93.8%, but sensitivity of only 69.6%. In this study, CRP value was higher than WBC and ANC in detecting bacteremia, but the most accurate predictor of SBI was appearing unwell [26]. Similarly, one large multicentered American study of suspected sepsis in neonates found the initial CRP value to be poorly sensitive for SBI [27]. However, they reported that an elevated CRP >10 mg/L at 24–48 hours after presentation demonstrated a 97.6% and 94.4% sensitivity for proven (culture positive) or probable (clinical features but no positive cultures) bacterial infection, making serial CRP measurements more accurate in diagnosing SBI in neonates.
3.2. Procalcitonin
Procalcitonin (PCT) is a 116 – amino acid protein precursor for calcitonin produced by parafollicular cells [28]. In normal conditions serum levels of PCT are lower than 0.05 ng/mL, while during SBI they can increase up to 700 ng/L [29]. During SBI, the site of PCT production is not limited to the neuroendocrine cells. The release of PCT is induced by increasing the CALC1 gene expression in parenchymal cells throughout the body triggered by endotoxin or by humoral factors i.e. IL-1, TNF- alfa, and IL-6 [30,31].
PCT concentrations increase more rapidly than CRP levels in patients with SBI. PCT levels begin to increase at two hours from the onset of infection and reach a serum peak at 24 to 36 hours [32]. For this reason, PCT has been shown to be a superior biomarker as compared with CRP for detecting SBI in ED [33]. However, the specificity for detecting SBI is limited, especially between infant < 3 months [25,34].

Table 1.
Kinetics of C reactive protein (CRP) versus procalcitonin (PCT) from the onset of inflammation.
Table 1.
Kinetics of C reactive protein (CRP) versus procalcitonin (PCT) from the onset of inflammation.
| Biomarker | Start of serum increase | Serum peak |
|---|---|---|
| CRP | 4-6 hours | 36-50 hours |
| PCT | 2 hours | 24-36 hours |
In a consistent meta-analysis England et al. showed that serum PCT concentrations <0.3 ng/mL identify a population of febrile infants < 91 days of age at low risk for SBI [35]. They concluded that serum PCT concentration alone is anyway poorer predictor of SBI and may be used in combination with clinical valuation.
A meta-analysis to investigate the diagnostic accuracy of PCT as early biomarker of sepsis was performed including 1408 patients (1086 neonates and 322 children) [36]. In neonatal group PCT showed sensitivity of 85% (95% CI, 76% to 90%) and specificity of 54% (95% CI, 38% to 70%) at the PCT cut-off of 2.0-2.5 ng/mL. In the pediatric group it was not possible to undertake a pooled analysis at the PCT cut-off of 2.0-2.5 ng/ml, due to the paucity of the studies [36]. In a recent prospective multi-centre cohort study Waterfield et al. revealed no difference and only a moderate accuracy for PCT and CRP in detection of SBI in the ED reporting that the area under the curve was identical at 0.70 [37].
The diagnostic power of PCT in pediatric intensive care unit (PICU) is uncertain. PCT showed to adequately predict SBI in a heterogeneous PICU population, with a PCT of ≥1.28 ng/mL as the ideal threshold for detection of SBI as reported in a recent a retrospective cohort study [38]. Another retrospective study performed in PICU identified PCT value of ≥1 ng/mL as able to predict SBI with sensitivity of 70% and specificity of 68% [39]. In a retrospective observational study involving 646 critically ill children, Lautz et al. have found that peak blood PCT measured within 48 hours of PICU admission was not superior to CRP in differentiating SBI from viral illness and sterile inflammation, raising doubts about right timing to perform PCT in PICU [40]. Zeng et al. in a recent retrospective analysis found that PCT alone wasn’t better be able to diagnose the hyperinflammatory state than CRP in PICU [41]. Furthermore, when both biomarkers are simultaneously elevated the diagnostic specificity of SBI increased.
3.3. Cytokines and chemokines
After infecting pathogens are recognized by toll-like receptors, host immune response is initiated mainly by the release of proinflammatory cytokines from macrophages and monocytes [25]. Because of this early involvement in the host immune response to infections, cytokines and chemokines have been considered as promising biomarkers of SBI, especially in recent years when most problems of their detection in blood samples have been solved. Moreover, as CRP and PCT production depends on cytokine release, it was thought that the measure of cytokines could offer an earlier and more effective evaluation of sepsis development compared to the traditionally used biomarkers [25]. Unfortunately, not all the expected benefits have materialized.
3.3.1. Interleukines (IL)
IL-2 is indicated as the most specific biomarker in patients with SBI, with low sensitivity and moderate specificity (54% and 86%, respectively) [42]. However, the poor predictive accuracy of this molecule doesn’t outperform the discrimination of traditional sepsis biomarkers in the clinical practice.
IL-6 has been studied for its role in systemic inflammation. It is described as an acute phase pro-inflammatory cytokine, which increases its blood level within the first 6 hours, earlier than CRP, during bacterial infections [43]. It turns out to be useful in predicting SBI diagnosis in children with fever without apparent source [44]. In a large prospective study, even if blood level of IL-6 was higher in septic children, the difference between septic and non-septic group was not statistically significant [45]. Comparing blood draws collected at different arrival times, the sensitiveness decreases as the hours pass from the onset of the fever. Although pediatric data are few, evidence on the role of IL-6 in neonates with sepsis is promising [46,47]. IL-6 appeared as an early marker of neonatal sepsis, even if its levels tend to normalize during the development of infection, increasing false-negative findings [48,49].
The key role of increasing levels of IL-10 in anti-inflammatory response deals its relationship with worse outcomes in oncologic neutropenic patients with sepsis [50]. In recent findings, IL-10 appeared with high specificity and moderate sensitivity. While IL-6 decreases quickly in the first 12 ore from the onset of the blood infection, IL-10 tends to persist for longer during the septic state and performs as a valuable diagnostic biomarker [50].
However, many authors declared the superiority of combinations of blood biomarkers over individual tests in differential diagnosis of infection etiology [51,52]. It has been described that combination of WBC, ANC, CRP, IL-2 and IL-6 increase sensitivity to 96%, specificity of 81%, and a large AUC 0.942 (CI 95%, 0.859 to 0984) in differentiate bacterial pathogenesis [41]. Similarly, matching CRP with IL-10 levels, the clinician got a higher discriminative ability in etiology of infection (specificity from 77% to 98%, sensitivity 75%) [53].
Finally, recent preliminary studies have shown promising results on the specificity of IL-27 in early prediction of SBI in critical pediatric patients. Using a large genome-wide expression database of critical children in pediatric ED, predictors genes coding for IL-27 protein were described; in particular, EB13, a subunit of IL-27, appeared to have a high predictive role for bacterial infections (more than 90%) [54]. In comparison to PCT, IL-27 performed better in discriminating bacterial from viral infections. These findings, although preliminary, lead to consider IL-27 as an effective biomarker in bacterial sepsis, exhibiting a specificity of 95% in detection of infection. A CART-generated algorithm including IL-27, PCT and immune status led to an undisputed improvement in predictive value, statistically improved from either IL-27 or PCT alone [55].
3.3.2. TRAIL and IP-10
Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL) is a type II transmembrane protein belonging to the TNF superfamily, which is involved in infection control and in the regulation of both innate and adaptive immune responses [56]. TRAIL is involved in sepsis by inducing apoptosis of inflammatory cells and down-regulating inflammation [57]. Many authors had explored the association between soluble TRAIL (sTRAIL) levels in septic patients and the risk of mortality: low sTRAIL levels seem to be associated with a high risk of mortality, with survivor patients who had significantly higher levels of sTRAIL than non-survivors [58].
IP-10 (i.e. interferon-gamma-inducible protein 10) is a chemokine that is expressed by antigen-presenting cells in response to IFN-γ and attracts activated T-cells to foci of inflammation [59]. This biomarker plays a role in the response to bacterial infections in particular in diagnosis and management of urinary tract infections, tuberculosis, and inflammatory diseases such as Kawasaki disease [60,61,62]
Van Houten et al. found that an assay combining three biomarkers, i.e. TRAIL, IP-10 and CRP, it is possible to distinguish bacterial from viral infections in febrile children with a sensitivity of 86.7% and a specificity of 91.1% [63]. In a proteomics-based study focusing on the host immune response, Oved and al. demonstrated that the combination of these three biomarkers showed a better performance compared to different combinations of routine biomarkers of inflammation in patients suffering from infectious diseases or from fever with unknown disease [64]. Papan et al. in a multinational, prospective, cohort study, validated the diagnostic performance of the novel host-response-based signature comprising TRAIL, IP-10, and CRP in a broad cohort of pediatric patients with respiratory tract infection or fever without source, demonstrating its capability to support diagnosis of viral etiology and reducing prescription of antibiotics [65]. Figure 1 shows how the novel host-response-based signature comprising TRAIL, IP-10, and CRP works.
4. Cell adhesion molecules
Several cell adhesion molecules including presepsin, cluster differentiation molecule-64 (CD64), soluble trigger receptor expressed on myeloid cell-1 (sTREM1), and pentraxin3 were tentatively used to differentiate septic children from non-septic ones [66]. However, only presepsin and sTREM1 were used in a number of studies useful for drawing some conclusion regarding their role in this regard.
4.1. Presepsin
Presepsin (sCD14-ST) is a protein related to cleavage of CD14, a soluble form of lipopolysaccharide (LPS) receptor, which recognizes pathogen-associated molecular patterns (PAMPs) and triggers the innate immune response [67]. This explains its specific elevation in bacterial infections, in which the underlying pathogenetic mechanism is expressed through the action of LPS.
Presepsin seems to have good specificity and sensitivity in sepsis and correlates to in-hospital mortality in patients with sepsis and septic shock, with a diagnostic potential that can increase if it is combined with clinical scores [68]. During the bacterial infectious state, the concentration in absolute value increases within 2 hours. Different studies reported that presepsin is the only biomarker that if remains elevated in patient with a SBI, it could be associated to higher risk of mortality throughout the follow-up period [69]. However, despite literature supporting its potential role in ED and in intensive care setting, some studies don’t indicate a superiority of presepsin compared to other biomarkers in terms of sensitivity and specificity [70].
In neonatal sepsis, presepsin offers the advantage of identifying culture-negative sepsis, with the possibility of early initiation of antibiotic therapy [71]. Meanwhile, presepsin excludes the diagnosis of sepsis in newborns not likely to be affected, reducing the misuse of antibiotics, minimizing hospital stays, and avoiding selection pressure for resistant strains [72]. Levels of presepsin are significantly higher in neonates with sepsis than in healthy ones and they increased earlier than PCT or CRP; the rise in blood values of CRP and PCT is similarly high during early phase of infection, but presepsin alone decreases with antibiotic treatment [73,74].
The use in clinical practice of a combination model including presepsin in addition to CRP and PCT may be useful for early detection of SBI in children with fever admitted to ED and for monitoring response to therapy.
4.2. STREM-2
Previous literature data show that sTREM-1 could be used as a marker of severity and outcome in septic neonates [75,76], while its diagnostic potential in pediatric patients older than one month seems to be moderate [78]. Systematic reviews and meta-analysis have recently evaluated the potential role of sTREM as a support in SBI diagnosis. However, low sensitivity and moderate specificity for sTREM-1 in distinguishing bacterial or viral etiology of infections were reported [78,79].
5. Future perspective
In pediatric patients, SBI is defined as the presence of systemic inflammatory response syndrome (SIRS) during evidence of an infection based on pathogen identification in the bloodstream or by the presence of symptoms directly linked to a high probability of systemic bacterial infection [80]. Early recognition of sepsis in children based on these definitions is often problematic, since blood cultures often provide false negative results and clinical symptoms are very unspecific, so emergencial setting management results in a delay of an adequate antimicrobial administration [81,82].
It is nowadays clear that combination of several SBI biomarkers instead of using one of the at the time can improve accuracy in SBI identification by unifying them into one diagnostic model/algorithm, as seen in adult patients [83]. Researchers also agree on the fact that crossing sepsis biomarkers with clinical and epidemiological information further optimizes accuracy. A retrospective cohort study aimed to evaluate the performance of a 2-step decision support algorithm based on an electronic health record best-practice alert (BPA) with age-adjusted vital sign ranges and physician screen [84]. The BPAs rely on presence of clinical markers of possible infection and incorporate patient risk factors, using demographic data, prior surgeries, or the patient’s problem list and/or medication list, to recognize three different types of SBI risk stratified by the severity of the patient’s underlying disease, with results that seem less specific in adults compared with children [85].
A German group has tried to develop and validate a diagnostic model for the discrimination of pediatric SBI and non-infectious SIRS, which could be set as an algorithm immediately ready for clinical practice [86]. Starting from a secondary analysis of a randomized controlled trial, they created a model including four clinical (length of PICU stay until onset of non-infectious SIRS/SBI, central line, core temperature, number of non-infectious SIRS/SBI episodes prior to diagnosis) and four laboratory parameters (interleukin-6, platelet count, procalcitonin, CRP), through a data driven analysis approach. Authors stated that the model could potentially reduce antibiotic treatment by 30% in non-infectious SIRS, emphasizing the importance of combining biomarkers and clinical parameters [86].
On this matter, there have been advances in the use of data-driven techniques to improve recognition of early signs of SBI: prediction models have been studied to obtain with machine learning a class of mathematical methods that attempt to generate knowledge and insight from large datasets [87]. Machine learning techniques has been shown useful also for the evaluation of inflammatory sub-phenotypes based on measurements of panels of inflammatory mediators either alone or in conjunction with clinical variables.
Considering both routine variables and inflammatory biomarkers in patients affected by acute respiratory distress syndrome (ARDS), a common complication of SBI, two sub-phenotypes have been consistently identified: hyper-inflammatory sub-phenotype with features such as higher levels of IL-6, IL-8, sTNFR1, higher rates of vasopressor use and lower circulating protein C and bicarbonate than a second hypo- inflammatory sub-phenotype [88]. The two phenotypes have been related to different responses to several therapies and highlighted bicarbonate, IL-6, IL-8, CRP, sTNFR-1 and vasopressor biomarkers as the most predictive variables for ventilator-free days and organ failure-free days.
Regarding septic shock therapy, another randomised trial highlighted data obtained from machine learning that has shown the IFNγ/IL10 ratio to be a good biomarker for the decision to administer hydrocortisone in septic shock [64]. Antibiotic administration and its optimization in critical ill children have also been studied as a field for potential algorithms implementation [89,90]. In a recent study it has been analysed the impact of a biomarker-based algorithm on broad-spectrum antibiotic prescribing in children with new-onset SIRS without proven bacterial infections admitted in a PICU [89]. This algorithm stated that PICU physicians should consider stopping antibiotics if: sterile site cultures obtained at SIRS onset revealed no growth after 48 hours, onset CRP and PCT were low and there was no sign of infection at exam or imaging. The authors noted a reduction of excessive broad-spectrum antibiotic therapy after algorithm implementation in patients in which a bacterial infection had been found, while no differences were seen in the so called uninfected patients except for the ones who had low biomarkers at the onset [89]. While de-escalation of antibiotic therapy in critically ill children remains a controversial topic, algorithms might ease the decision for patients with low biomarkers.
6. Conclusions
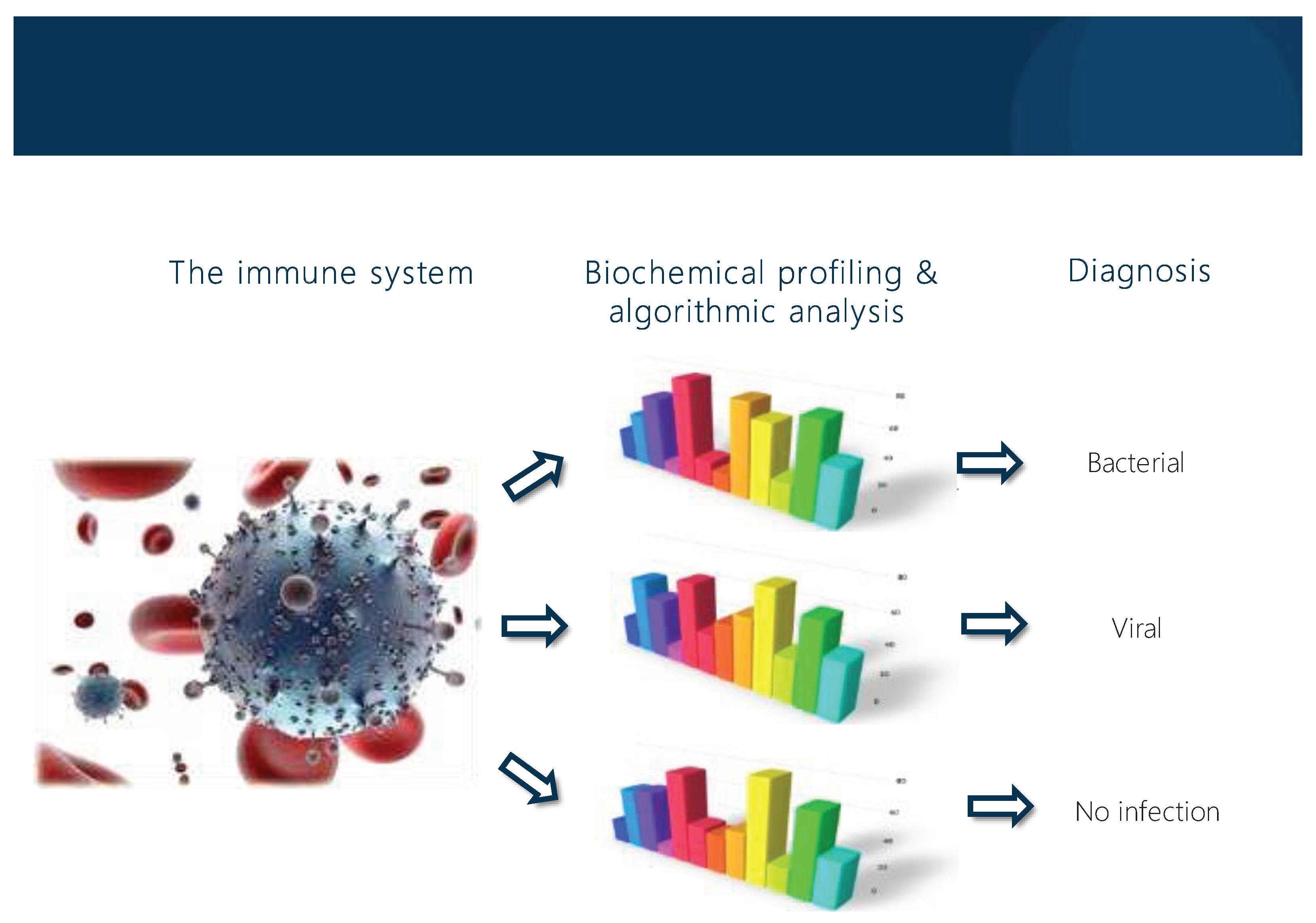
Inflammatory response is a complex mechanism in which many biochemical and immunological factors contribute to host response in SBI. Perfecting biomarkers accuracy could be useful for antimicrobial stewardship, pointing to more appropriateness in antibiotic prescription and dosage (Figure 2).
CRP and procalcitonin still represent the most used biomarkers in the pediatric ED for the diagnosis of SBI. Their sensibility and sensitivity increase when combined and for this reason it is reasonable to take them both into consideration in the evaluation of a febrile children. The potential of machine learning tools, who represent a real novelty in medical practice, in conjunction with routine clinical and biological information, may improve accuracy of diagnosis and target therapeutic options in SBI. However, studies on this matter are not yet validated in younger populations, making their relevance in pediatric precision medicine still uncertain. More data from further studies are necessary to improve clinical practice and decision making using these new technologies.
Author Contributions
L.B. and G.B. wrote the first draft of the manuscript; G.D.C. and G.G. performed the literature review; S.E. supervised the project, revised the manuscript and gave a substantial scientific contribution. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Armon K, Stephenson T, Gabriel V, MacFaul R, Eccleston P, Werneke U, Smith S. Determining the common medical presenting problems to an accident and emergency department. Arch Dis Child. 2001 May;84(5):390-2.
- Sands R, Shanmugavadivel D, Stephenson T, Wood D. Medical problems presenting to paediatric emergency departments: 10 years on. Emerg Med J. 2012 May;29(5):379-82. [CrossRef]
- Chiappini E, Venturini E, Remaschi G, Principi N, Longhi R, Tovo PA, Becherucci P, Bonsignori F, Esposito S, Festini F, Galli L, Lucchesi B, Mugelli A, Marseglia GL, de Martino M; Italian Pediatric Society Panel for the Management of Fever in Children. 2016 Update of the Italian Pediatric Society Guidelines for Management of Fever in Children. J Pediatr. 2017 Jan;180:177-183.e1.
- Fever in under 5s: assessment and initial management. London: National Institute for Health and Care Excellence (NICE); 2021 Nov 26. PMID: 31891472.;
- Pantell RH, Roberts KB, Adams WG, Dreyer BP, Kuppermann N, O'Leary ST, Okechukwu K, Woods CR Jr; SUBCOMMITTEE ON FEBRILE INFANTS. Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old. Pediatrics. 2021 Aug;148(2):e2021052228. [CrossRef]
- Stol K, Nijman RG, van Herk W, van Rossum AMC. Biomarkers for Infection in Children: Current Clinical Practice and Future Perspectives. Pediatr Infect Dis J. 2019 Jun;38(6S Suppl 1):S7-S13.
- Nauseef WM. How human neutrophils kill and degrade microbes: an integrated view. Immunol Rev. 2007 Oct;219:88-102. [CrossRef]
- Yo CH, Hsieh PS, Lee SH, Wu JY, Chang SS, Tasi KC, Lee CC. Comparison of the test characteristics of procalcitonin to C-reactive protein and leukocytosis for the detection of serious bacterial infections in children presenting with fever without source: a systematic review and meta-analysis. Ann Emerg Med. 2012 Nov;60(5):591-600. [CrossRef]
- Pratt A, Attia MW. Duration of fever and markers of serious bacterial infection in young febrile children. Pediatr Int. 2007 Feb;49(1):31-5.
- Van den Bruel A, Thompson MJ, Haj-Hassan T, Stevens R, Moll H, Lakhanpaul M, Mant D. Diagnostic value of laboratory tests in identifying serious infections in febrile children: systematic review. BMJ. 2011 Jun 8;342:d3082. [CrossRef]
- Semple JW, Italiano JE Jr, Freedman J. Platelets and the immune continuum. Nat Rev Immunol. 2011 Apr;11(4):264-74. [CrossRef]
- Vassiliou AG, Mastora Z, Orfanos SE, Jahaj E, Maniatis NA, Koutsoukou A, Armaganidis A, Kotanidou A. Elevated biomarkers of endothelial dysfunction/activation at ICU admission are associated with sepsis development. Cytokine. 2014 Oct;69(2):240-7. [CrossRef]
- Zonneveld R, Martinelli R, Shapiro NI, Kuijpers TW, Plötz FB, Carman CV. Soluble adhesion molecules as markers for sepsis and the potential pathophysiological discrepancy in neonates, children and adults. Crit Care. 2014 Feb 18;18(2):204. [CrossRef]
- Feketea G, Vlacha V, Pop RM, Bocsan IC, Stanciu LA, Buzoianu AD, Zdrenghea M. Relationship Between Vitamin D Level and Platelet Parameters in Children With Viral Respiratory Infections. Front Pediatr. 2022 Apr 7;10:824959. [CrossRef]
- Heijnen H, van der Sluijs P. Platelet secretory behaviour: as diverse as the granules … or not? J Thromb Haemost. 2015 Dec;13(12):2141-51.
- Pociute A, Kottilingal Farook MF, Dagys A, Kevalas R, Laucaityte G, Jankauskaite L. Platelet-Derived Biomarkers: Potential Role in Early Pediatric Serious Bacterial Infection and Sepsis Diagnostics. J Clin Med. 2022 Oct 31;11(21):6475. [CrossRef]
- Jaye DL, Waites KB. Clinical applications of C-reactive protein in pediatrics. Pediatr Infect Dis J. 1997 Aug;16(8):735-46; quiz 746-7. [CrossRef]
- McWilliam S, Riordan A. How to use: C-reactive protein. Arch Dis Child Educ Pract Ed. 2010 Apr;95(2):55-8.
- Marnell L, Mold C, Du Clos TW. C-reactive protein: ligands, receptors and role in inflammation. Clin Immunol. 2005 Nov;117(2):104-11. [CrossRef]
- Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003 Jun;111(12):1805-12. doi: 10.1172/JCI18921. Erratum in: J Clin Invest. 2003 Jul;112(2):299. [CrossRef]
- Dyer EM, Waterfield T, Baynes H. How to use C-reactive protein. Arch Dis Child Educ Pract Ed. 2019 Jun;104(3):150-153.
- Verbakel JY, Lemiengre MB, De Burghgraeve T, De Sutter A, Aertgeerts B, Bullens DMA, Shinkins B, Van den Bruel A, Buntinx F. Point-of-care C reactive protein to identify serious infection in acutely ill children presenting to hospital: prospective cohort study. Arch Dis Child. 2018 May;103(5):420-426. [CrossRef]
- Fernández Lopez A, Luaces Cubells C, García García JJ, Fernández Pou J; Spanish Society of Pediatric Emergencies. Procalcitonin in pediatric emergency departments for the early diagnosis of invasive bacterial infections in febrile infants: results of a multicenter study and utility of a rapid qualitative test for this marker. Pediatr Infect Dis J. 2003 Oct;22(10):895-903.
- Segal I, Ehrlichman M, Urbach J, Bar-Meir M. Use of time from fever onset improves the diagnostic accuracy of C-reactive protein in identifying bacterial infections. Arch Dis Child. 2014 Nov;99(11):974-8. [CrossRef]
- Boscarino G, Migliorino R, Carbone G, Davino G, Dell'Orto VG, Perrone S, Principi N, Esposito S. Biomarkers of Neonatal Sepsis: Where We Are and Where We Are Going. Antibiotics (Basel). 2023 Jul 26;12(8):1233. [CrossRef]
- Gómez B, Mintegi S, Benito J, Egireun A, Garcia D, Astobiza E. Blood culture and bacteremia predictors in infants less than three months of age with fever without source. Pediatr Infect Dis J. 2010 Jan;29(1):43-7. [CrossRef]
- Benitz WE, Han MY, Madan A, Ramachandra P. Serial serum C-reactive protein levels in the diagnosis of neonatal infection. Pediatrics. 1998 Oct;102(4):E41. [CrossRef]
- Samraj RS, Zingarelli B, Wong HR. Role of biomarkers in sepsis care. Shock. 2013;40(5):358–65. [CrossRef]
- Casado-Flores J, Blanco-Quiros A, Asensio J, et al. Serum procalcitonin in children with suspected sepsis: a comparison with C-reactive protein and neutrophil count. Pediatr Crit Care Med. 2003;4:190Y195. [CrossRef]
- Muller B, White JC, Nylen ES, et al. Ubiquitous expression of the calcitonin-I gene in multiple tissues in response to sepsis. J Clin Endocrinol Metab. 2001;86:396Y404. [CrossRef]
- Linscheid P, Seboek D, Schaer DJ, et al. Expression and secretion of procalcitonin and calcitonin geneYrelated peptide by adherent monocytes and by macrophage-activated adipocytes. Crit Care Med. 2004;32:1715Y1721.
- Principi N, Esposito S. Biomarkers in Pediatric Community-Acquired Pneumonia. Int J Mol Sci. 2017 Feb 19;18(2):447. [CrossRef]
- Arkader R, Troster EJ, Lopes MR, Júnior RR, Carcillo JA, Leone C, Okay TS. Procalcitonin does discriminate between sepsis and systemic inflammatory response syndrome. Arch Dis Child. 2006 Feb;91(2):117-20. [CrossRef]
- Milcent K, Faesch S, Gras-Le Guen C, Dubos F, Poulalhon C, Badier I, Marc E, Laguille C, de Pontual L, Mosca A, Nissack G, Biscardi S, Le Hors H, Louillet F, Dumitrescu AM, Babe P, Vauloup-Fellous C, Bouyer J, Gajdos V. Use of Procalcitonin Assays to Predict Serious Bacterial Infection in Young Febrile Infants. JAMA Pediatr. 2016 Jan;170(1):62-9. [CrossRef]
- England JT, Del Vecchio MT, Aronoff SC. Use of serum procalcitonin in evaluation of febrile infants: a meta-analysis of 2317 patients. J Emerg Med. 2014 Dec;47(6):682-8. [CrossRef]
- Pontrelli G, De Crescenzo F, Buzzetti R et al. Accuracy of serum procalcitonin for the diagnosis of sepsis in neonates and children with systemic inflammatory syndrome: a meta-analysis. BMC Infect. Dis. 2017;17(1):302. [CrossRef]
- Waterfield T, Maney JA, Lyttle MD, McKenna JP, Roland D, Corr M, Patenall B, Shields MD, Woolfall K, Fairley D; Paediatric Emergency Research in the UK and Ireland (PERUKI). Diagnostic test accuracy of point-of-care procalcitonin to diagnose serious bacterial infections in children. BMC Pediatr. 2020 Oct 21;20(1):487. [CrossRef]
- Jacobs DM, Holsen M, Chen S, Fusco NM, Hassinger AB. Procalcitonin to Detect Bacterial Infections in Critically Ill Pediatric Patients. Clin Pediatr (Phila). 2017 Aug;56(9):821-827. [CrossRef]
- Cies JJ, Chopra A. Procalcitonin use in a pediatric intensive care unit. Pediatr Infect Dis J. 2014 Sep;33(9):984-6. [CrossRef]
- Lautz AJ, Dziorny AC, Denson AR, O'Connor KA, Chilutti MR, Ross RK, Gerber JS, Weiss SL. Value of Procalcitonin Measurement for Early Evidence of Severe Bacterial Infections in the Pediatric Intensive Care Unit. J Pediatr. 2016 Dec;179:74-81.e2. [CrossRef]
- Zeng G, Chen D, Zhou R, Zhao X, Ye C, Tao H, Sheng W, Wu Y. Combination of C-reactive protein, procalcitonin, IL-6, IL-8, and IL-10 for early diagnosis of hyperinflammatory state and organ dysfunction in pediatric sepsis. J Clin Lab Anal. 2022 Jul;36(7):e24505. [CrossRef]
- Dagys A, Laucaitytė G, Volkevičiūtė A, Abramavičius S, Kėvalas R, Vitkauskienė A, Jankauskaitė L. Blood biomarkers in early bacterial infection and sepsis diagnostics in feverish young children. Int J Med Sci. 2022 Apr 11;19(4):753-761. [CrossRef]
- Biron BM, Ayala A, Lomas-Neira JL. Biomarkers for Sepsis: What Is and What Might Be? Biomark Insights. 2015 Sep 15;10(Suppl 4):7-17.
- Fuster JJ, Walsh K. The good, the bad, and the ugly of interleukin-6 signaling. EMBO J. 2014 Jul 1;33(13):1425-7.
- Vasconcellos ÂG, Clarêncio J, Andrade D, Cardoso MA, Barral A, Nascimento-Carvalho CM. Systemic cytokines and chemokines on admission of children hospitalized with community-acquired pneumonia. Cytokine. 2018 Jul;107:1-8. [CrossRef]
- Du J, Li L, Dou Y, Li P, Chen R, Liu H. Diagnostic utility of neutrophil CD64 as a marker for early-onset sepsis in preterm neonates. PLoS One. 2014 Jul 17;9(7):e102647. [CrossRef]
- Foo CPZ, Seabrook JA, Sangha G, Foster JR. Presumed Systemic Inflammatory Response Syndrome in the Pediatric Emergency Department. Pediatr Emerg Care. 2019 Aug;35(8):522-526. [CrossRef]
- Umlauf VN, Dreschers S, Orlikowsky TW. Flow cytometry in the detection of neonatal sepsis. Int J Pediatr. 2013;2013:763191. [CrossRef]
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G; SCCM/ESICM/ACCP/ATS/SIS. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003 Apr;31(4):1250-6.
- Urbonas V, Eidukaitė A, Tamulienė I. Increased interleukin-10 levels correlate with bacteremia and sepsis in febrile neutropenia pediatric oncology patients. Cytokine. 2012 Mar;57(3):313-5. [CrossRef]
- Theodosiou AA, Mashumba F, Flatt A. Excluding Clinically Significant Bacteremia by 24 Hours in Otherwise Well Febrile Children Younger Than 16 Years: A Study of More Than 50,000 Blood Cultures. Pediatr Infect Dis J. 2019 Sep;38(9):e203-e208.
- Tamelytė E, Vaičekauskienė G, Dagys A, Lapinskas T, Jankauskaitė L. Early Blood Biomarkers to Improve Sepsis/Bacteremia Diagnostics in Pediatric Emergency Settings. Medicina (Kaunas). 2019 Apr 10;55(4):99. [CrossRef]
- Romagnoli C, Frezza S, Cingolani A, De Luca A, Puopolo M, De Carolis MP, Vento G, Antinori A, Tortorolo G. Plasma levels of interleukin-6 and interleukin-10 in preterm neonates evaluated for sepsis. Eur J Pediatr. 2001 Jun;160(6):345-50. [CrossRef]
- Wong HR, Cvijanovich NZ, Hall M, Allen GL, Thomas NJ, Freishtat RJ, Anas N, Meyer K, Checchia PA, Lin R, Bigham MT, Sen A, Nowak J, Quasney M, Henricksen JW, Chopra A, Banschbach S, Beckman E, Harmon K, Lahni P, Shanley TP. Interleukin-27 is a novel candidate diagnostic biomarker for bacterial infection in critically ill children. Crit Care. 2012 Oct 29;16(5):R213.
- Hanna WJ, Berrens Z, Langner T, Lahni P, Wong HR. Interleukin-27: a novel biomarker in predicting bacterial infection among the critically ill. Crit Care. 2015 Oct 30;19:378.
- Gyurkovska V, Ivanovska N. Distinct roles of TNF-related apoptosis-inducing ligand (TRAIL) in viral and bacterial infections: from pathogenesis to pathogen clearance. Inflamm Res. 2016 Jun;65(6):427-37. [CrossRef]
- Unsinger J, Kazama H, McDonough JS, Griffith TS, Hotchkiss RS, et al. Sepsis – induced apoptosis leads to active suppression of delayed-type hypersensitivity by CD8+ regulatory T cells through a TRAIL-dependent mechanism. J Immunol 2010;184(12): 6766–6772. [CrossRef]
- Tian Y, Tao T, Zhu J, Zou Y, Wang J, Li J, Bo L, Deng X, Soluble Tumor Necrosis Factor Related Apoptosis Inducing Ligand Level as a Predictor of Severity of Sepsis and the Risk of Mortality in Septic Patients, PLoS One. 2013 Dec 12;8(12):e82204. [CrossRef]
- Ashkenazi-Hoffnung L, Livni G, Scheuerman O, Berger I, Eden E, Oved K, Shani L, Kronenfeld G, Simon E, Boico O, Navon R, Gottlieb TM, Barash E, Paz M, Yuhas Y, Berent E, Ashkenazi S. Differential Serum and Urine CRP, IP-10, and TRAIL Levels in Pediatric Urinary Tract Infection. Front Pediatr. 2021 Dec 13;9:771118. [CrossRef]
- Ko TM, Kuo HC, Chang JS, Chen SP, Liu YM, Chen HW, Tsai FJ, Lee YC, Chen CH, Wu JY, Chen YT. CXCL10/IP-10 is a biomarker and mediator for Kawasaki disease. Circ Res. 2015 Feb 27;116(5):876-83.
- Azzurri A, Sow OY, Amedei A, Bah B, Diallo S, Peri G, Benagiano M, D'Elios MM, Mantovani A, Del Prete G. IFN-gamma-inducible protein 10 and pentraxin 3 plasma levels are tools for monitoring inflammation and disease activity in Mycobacterium tuberculosis infection. Microbes Infect. 2005 Jan;7(1):1-8.
- Esposito S, Tagliabue C, Picciolli I, Semino M, Sabatini C, Consolo S, Bosis S, Pinzani R, Principi N. Procalcitonin measurements for guiding antibiotic treatment in pediatric pneumonia. Respir Med. 2011 Dec;105(12):1939-45. [CrossRef]
- van Houten CB, de Groot JAH, Klein A, Srugo I, Chistyakov I, de Waal W, Meijssen CB, Avis W, Wolfs TFW, Shachor-Meyouhas Y, Stein M, Sanders EAM, Bont LJ. A host-protein based assay to differentiate between bacterial and viral infections in preschool children (OPPORTUNITY): a double-blind, multicentre, validation study. Lancet Infect Dis. 2017 Apr;17(4):431-440. [CrossRef]
- König R, Kolte A, Ahlers O, Oswald M, Krauss V, Roell D, Sommerfeld O, Dimopoulos G, Tsangaris I, Antoniadou E, et al. Use of IFNγ/IL10 Ratio for Stratification of Hydrocortisone Therapy in Patients With Septic Shock. Front Immunol. 2021 Mar 9;12:607217. [CrossRef]
- Papan C, Argentiero A, Adams O, Porwoll M, Hakim U, Farinelli E, Testa I, Pasticci MB, Mezzetti D, Perruccio K, Simon A, Liese JG, Knuf M, Stein M, Yacobov R, Bamberger E, Schneider S, Esposito S, Tenenbaum T. Association of viral load with TRAIL, IP-10, CRP biomarker signature and disease severity in children with respiratory tract infection or fever without source: A prospective, multicentre cohort study. J Med Virol. 2022 Aug 31. [CrossRef]
- Papan C, Argentiero A, Porwoll M, Hakim U, Farinelli E, Testa I, Pasticci MB, Mezzetti D, Perruccio K, Etshtein L, Mastboim N, Moscoviz E, Ber TI, Cohen A, Simon E, Boico O, Shani L, Gottlieb TM, Navon R, Barash E, Oved K, Eden E, Simon A, Liese JG, Knuf M, Stein M, Yacobov R, Bamberger E, Schneider S, Esposito S, Tenenbaum T. A host signature based on TRAIL, IP-10, and CRP for reducing antibiotic overuse in children by differentiating bacterial from viral infections: a prospective, multicentre cohort study. Clin Microbiol Infect. 2022 May;28(5):723-730. [CrossRef]
- Velissaris D, Zareifopoulos N, Karamouzos V, Karanikolas E, Pierrakos C, Koniari I, Karanikolas M. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus. 2021 May 13;13(5):e15019. [CrossRef]
- Henriquez-Camacho C, Losa J. Biomarkers for sepsis. Biomed Res Int. 2014;2014:547818.
- Wu CC, Lan HM, Han ST, Chaou CH, Yeh CF, Liu SH, Li CH, Blaney GN 3rd, Liu ZY, Chen KF. Comparison of diagnostic accuracy in sepsis between presepsin, procalcitonin, and C-reactive protein: a systematic review and meta-analysis. Ann Intensive Care. 2017 Sep 6;7(1):91.
- Romualdo LG, Torrella PE, González MV, Sánchez RJ, Holgado AH, Freire AO, Acebes SR, Otón MD. Diagnostic accuracy of presepsin (soluble CD14 subtype) for prediction of bacteremia in patients with systemic inflammatory response syndrome in the Emergency Department. Clin Biochem. 2014 May;47(7-8):505-8. [CrossRef]
- Vouloumanou EK, Plessa E, Karageorgopoulos DE, Mantadakis E, Falagas ME. Serum procalcitonin as a diagnostic marker for neonatal sepsis: a systematic review and meta-analysis. Intensive Care Med. 2011 May;37(5):747-62. [CrossRef]
- Schuetz P, Christ-Crain M, Müller B. Procalcitonin and other biomarkers to improve assessment and antibiotic stewardship in infections--hope for hype? Swiss Med Wkly. 2009 Jun 13;139(23-24):318-26.
- Poggi C, Bianconi T, Gozzini E, Generoso M, Dani C. Presepsin for the detection of late-onset sepsis in preterm newborns. Pediatrics. 2015 Jan;135(1):68-75. [CrossRef]
- Kumar N, Dayal R, Singh P, Pathak S, Pooniya V, Goyal A, Kamal R, Mohanty KK. A Comparative Evaluation of Presepsin with Procalcitonin and CRP in Diagnosing Neonatal Sepsis. Indian J Pediatr. 2019 Feb;86(2):177-179. [CrossRef]
- Adly AA, Ismail EA, Andrawes NG, El-Saadany MA. Circulating soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) as diagnostic and prognostic marker in neonatal sepsis. Cytokine. 2014 Feb;65(2):184-91. [CrossRef]
- Sarafidis K, Soubasi-Griva V, Piretzi K, Thomaidou A, Agakidou E, Taparkou A, Diamanti E, Drossou-Agakidou V. Diagnostic utility of elevated serum soluble triggering receptor expressed on myeloid cells (sTREM)-1 in infected neonates. Intensive Care Med. 2010 May;36(5):864-8. [CrossRef]
- Pontrelli G, De Crescenzo F, Buzzetti R, Calò Carducci F, Jenkner A, Amodio D, De Luca M, Chiurchiù S, Davies EH, Simonetti A, Ferretti E, Della Corte M, Gramatica L, Livadiotti S, Rossi P. Diagnostic value of soluble triggering receptor expressed on myeloid cells in paediatric sepsis: a systematic review. Ital J Pediatr. 2016 Apr 27;42:44. [CrossRef]
- Jiyong J, Tiancha H, Wei C, Huahao S. Diagnostic value of the soluble triggering receptor expressed on myeloid cells-1 in bacterial infection: a meta-analysis. Intensive Care Med. 2009 Apr;35(4):587-95. [CrossRef]
- Esposito S, Di Gangi M, Cardinale F, Baraldi E, Corsini I, Da Dalt L, Tovo PA, Correra A, Villani A, Sacco O, Tenero L, Dones P, Gambino M, Zampiero A, Principi N; Ita-CAP Study Group. Sensitivity and Specificity of Soluble Triggering Receptor Expressed on Myeloid Cells-1, Midregional Proatrial Natriuretic Peptide and Midregional Proadrenomedullin for Distinguishing Etiology and to Assess Severity in Community-Acquired Pneumonia. PLoS One. 2016 Nov 15;11(11):e0163262.
- Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005 Jan;6(1):2-8.
- Balamuth, F.; Scott, H.F.; Weiss, S.L.; Webb, M.; Chamberlain, J.M.; Bajaj, L.; Depinet, H.; Grundmeier, R.W.; Campos, D.; Deakyne Davies, S.J.; et al. Validation of the Pediatric Sequential Organ Failure Assessment Score and Evaluation of Third International Consensus Definitions for Sepsis and Septic Shock Definitions in the Pediatric Emergency Department. JAMA Pediatr. 2022;176: 672–678. [CrossRef]
- Esposito S, Rinaldi VE, Argentiero A, Farinelli E, Cofini M, D'Alonzo R, Mencacci A, Principi N. Approach to Neonates and Young Infants with Fever without a Source Who Are at Risk for Severe Bacterial Infection. Mediators Inflamm. 2018 Nov 26;2018:4869329. [CrossRef]
- Han, J.H.; Nachamkin, I.; Coffin, S.E.; Gerber, J.S.; Fuchs, B.; Garrigan, C.; Han, X.; Bilker, W.B.; Wise, J.; Tolomeo, P.; et al. Use of a Combination Biomarker Algorithm To Identify Medical Intensive Care Unit Patients with Suspected Sepsis at Very Low Likelihood of Bacterial Infection. Antimicrob Agents Chemother. 2015 Oct;59(10):6494-500. [CrossRef]
- Witting, C.S.; Simon, N.J.E.; Lorenz, D.; Murphy, J.S.; Nelson, J.; Lehnig, K.; Alpern, E.R. Sepsis Electronic Decision Support Screen in High-Risk Patients Across Age Groups in a Pediatric Emergency Department. Pediatr Emerg Care. 2022 Aug 1;38(8):e1479-e1484. [CrossRef]
- Narayanan, N.; Gross, A.K.; Pintens, M.; Fee, C.; Macdougall, C. Effect of an electronic medical record alert for severe sepsis among ED patients. Am J Emerg Med. 2016 Feb;34(2):185-8. [CrossRef]
- Lamping, F.; Jack, T.; Rübsamen, N.; Sasse, M.; Beerbaum, P.; Mikolajczyk, R.T.; Boehne, M.; Karch, A. Development and validation of a diagnostic model for early differentiation of sepsis and non-infectious SIRS in critically ill children-a data-driven approach using machine-learning algorithms. BMC Pediatr. 2018 Mar 15;18(1):112. [CrossRef]
- Komorowski, M.; Green, A.; Tatham, K.C.; Seymour, C.; Antcliffe, D. Sepsis biomarkers and diagnostic tools with a focus on machine learning. EBioMedicine. 2022 Dec:86:104394. [CrossRef]
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A. Subphenotypes in acute respiratory distress syndrome: latent class analysis of data from two randomised controlled trials. Lancet Resp Med. 2014;2:611–620. [CrossRef]
- Downes, K.J.; Fitzgerald, J.C.; Schriver, E.; Boge, C.L.K.; Russo, M.E.; Weiss, S.L.; Balamuth, F.; Kubis, S.E.; Tolomeo, P.; Bilker, W.B.; et al. Implementation of a Pragmatic Biomarker-Driven Algorithm to Guide Antibiotic Use in the Pediatric Intensive Care Unit: the Optimizing Antibiotic Strategies in Sepsis (OASIS) II Study. J Pediatric Infect Dis Soc. 2020 Feb 28;9(1):36-43.
- Bos DAG, De Burghgraeve T, De Sutter A, Buntinx F, Verbakel JY. Clinical prediction models for serious infections in children: external validation in ambulatory care. BMC Med. 2023 Apr 18;21(1):151. [CrossRef]
Figure 1.
Novel host-immune signature for distinguishing between bacterial and viral infections.
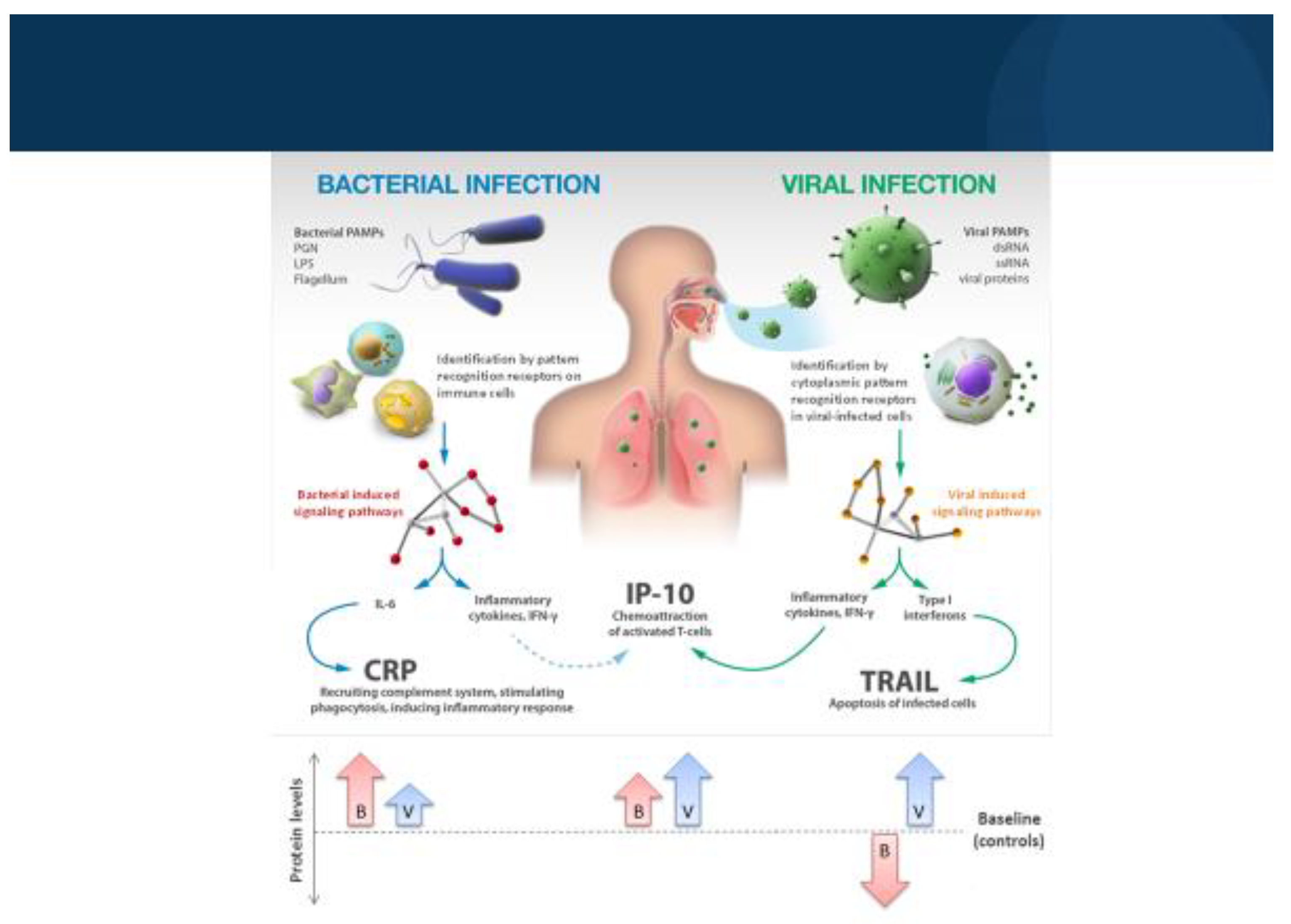
Figure 2.
Decoding the body’s immune system in order to detect the infection cause.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



