
Submitted:
08 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
This study introduces a novel approach by proposing a dressing impregnated with vancomycin and chlorhexidine for postoperative care, specifically targeting patients undergoing orthopedic surgeries. The research design involved a pilot study with a randomized control group, aiming to evaluate the vancomycin with chlorhexidine dressing's efficacy and safety. A total of 12 patients used impregnated dressing and 9 used the same dressing without impregnation. Despite limitations, including the small sample size and single-center study location, our findings demonstrate the safety of the impregnated dressing in trauma surgeries, indicating potential applicability in broader surgical contexts. In conclusion, this study contributes to the discourse on preventive strategies for SSIs, presenting a pioneering approach with the vancomycin and chlorhexidine-impregnated dressing. Future research endeavors, incorporating larger-scale studies and addressing study limitations, are crucial for advancing the understanding and implementation of effective postoperative care strategies.
Keywords:
dressing
; antibiotics
; trauma
; vancomycin
; chlorhexidine
1. Introduction
The introduction should briefly place the study in a broad context and highlight why Advancements in medical technology have expanded surgical options, enabling more specific procedures across various medical domains worldwide. Despite these advancements, the management of surgical incisions remains a significant concern, irrespective of the surgical category or location [1]. Over the past decades, there has been a growing emphasis on postoperative care, exemplified by the emergence of the Enhanced Recovery After Surgery (ERAS) protocol, which advocates interventions aimed at enhancing patient recovery and reducing postoperative complications [2]. However, recommendations regarding the selection of dressings for postoperative surgical incision care, despite surgical site infection (SSI) being a common nosocomial infection, are notably lacking [3].
SSI affects up to 23.6 per 100 surgical procedures, with considerable implications for patients and healthcare systems [4]. These infections are associated with increased morbidity, mortality, and treatment costs, resulting in an additional postoperative period of 7 to 11 days and an elevated risk of death by 2 to 11 times compared to postoperative patients without SSI [5]. In the field of orthopedic surgery, SSIs are recognized as a crucial risk factor for complications and unfavorable outcomes [6,7,8,9,10,11]. While the incidence of SSIs associated with closed fracture repair and elective arthroplasty is relatively low, the rare infections that do occur can lead to devastating consequences, such as non-union, implant failure, revision surgery, or even amputation [12]. The healthcare costs associated with these complications exceed $1.6 billion in the United States alone [12]. Furthermore, there is a high rate of false negatives (10-30%) in the diagnosis of orthopedics-related infections, underscoring the need for more effective prevention strategies to mitigate the impact of SSIs in orthopedic surgery [12].
Among the resources for preventing SSIs in orthopedics, various types of dressings can be employed to preserve the physiological wound healing process and prevent potential infections, improving early discharge [13,14]. These dressings can be broadly classified into four categories: traditional or passive, skin substitutes, interactive materials, and bioactive dressings [15]. Bioactive dressings, in particular, play a significant role by providing active materials, such as antibiotics, to the wound site [16]. These materials can be impregnated in structures like nanofibers, wafers, foams, sponges, hydrogels, membranes, and films, each with advantages to enhance their biological activity [17]. Moreover, the widespread use of antibiotics has led to the emergence of resistant strains, and postoperative bioactive dressings emerge as a potential solution by minimizing systemic effects through local release, reducing the likelihood of microbial resistance [18,19,20,21,22,23,24,25]. Additionally, surgical site infections can occur post-discharge, where dressings have the convenience and adherence superiority to treatment [26].
Different dressing structures have distinct advantages and disadvantages. Sponges provide thermal insulation, maintain a moist environment at the wound site, and exhibit high porosity but are mechanically fragile [27]. On the other hand, hydrogels can store a significant amount of water within their 3D polymeric network, facilitating a moist environment for healing but require a secondary dressing due to their mechanically fragile properties [28]. Hydrocolloids, as non-adherent and painless dressings, can be easily removed by saline or sterile water but may be cytotoxic, have an unpleasant odor, and maintain an acidic pH at the wound site. Films effectively block the flow of liquids and bacteria while allowing free passage of oxygen and water vapor [29]. Due to their flexible, lightweight, and low water absorption characteristics, films are suitable for treating delicate skin and superficial wounds with low exudation, though they can be challenging to handle, adhere to the wound bed, and cause exudate accumulation. Membranes are known to act as physical barriers, replicate the three-dimensional architecture of the native extracellular matrix, and ensure cell proliferation, gas exchange, and nutrient supply. They are a semipermeable biomaterial similar to films, except for having a more significant water absorption capacity. However, their use is limited by the materials and solvents used in their production [30].
In the context of various dressing types, a Cochrane review conducted in 2011 and subsequent updated (2022) examined different dressing strategies, including studies of wounds without dressings, but found insufficient evidence to draw a reliable conclusion about the superiority of any one dressing [17]. This was due to the inadequate quality of available evidence, with most studies being limited in size and considered susceptible to systematic errors. Therefore, the authors recommend further research to advance this field.
Among the drugs producing the desired antimicrobial effect in dressings, chlorhexidine gluconate (CHG), an antiseptic that has demonstrated efficacy in reducing the risk of catheter-associated blood infections, is noteworthy [31]. However, despite its promising use, there is still a gap in scientific knowledge regarding the use of dressings impregnated with CHG in preventing surgical site infections and reducing bacterial load.
Other drugs with similar effects are antibiotics, among which vancomycin stands out for its widespread use in clinical therapies and antimicrobial potential against resistant gram-positive pathogens present in the early stages of infection [32]. However, maintaining therapeutic systemic levels of this antibiotic can be challenging and lead to adverse effects such as nephrotoxicity. Local vancomycin release avoids systemic side effects, with topical use already showing promise in the treatment of osteomyelitis, for example. Thus, this research proposes a dressing impregnated with vancomycin and CHG for postoperative care of patients undergoing orthopedic surgeries with the aim of preventing surgical site infections by delivering antimicrobials directly to the affected site.
2. Materials and Methods
2.1. Dressing development
The impregnated dressing was developed based on a 20% chlorhexidine digluconate solution, diluted with vancomycin. The concentrations and dilutions are protected by patent. Following the formulation of the solution, a 300 gsm filter paper was immersed for a sufficient absorption period and subsequently subjected to freeze-drying, followed by ethylene oxide sterilization. Preliminary microbiological tests for the dressing were conducted using the Kirby-Bauer method [33]. For this, 6 mm diameter disks were created and placed on a Muller-Hinton agar plate previously inoculated with Staphylococcus aureus ATCC® 25923 [34]. The resulting inhibition zone was compared with a disk made of the same material but without impregnation [35].
The impregnated dressings were assessed for efficacy over 7 days on human skin. Volunteers received the dressing in the form of 6 mm diameter disks, placed on healthy skin for the duration of 7 days. After this period, the disks were removed from the skin and placed on a Muller-Hinton plate previously inoculated with S. aureus ATCC® The inhibition zone was compared with a disk made of the same material but without impregnation.
2.2. Study design and sample size
This is a pilot study of a vancomycin and CHG dressing for immediate wound covering (post operative) for seven days to prevent surgical site infection. It was a controlled and randomized study (non-impregnated dressing) with a total of 23 participants undergoing elective and emergency fracture repair surgery at a University Hospital in Curitiba-PR. Participants receiver vancomycin and CHG impregnated dressing or non-impregnated dressing during the period of March 2023 to October The sample size was based on convenience considering the pilot study, even though it was randomized and blinded, this study was not a clinical trial.
2.3. Ethical aspects
The study was submitted and approved by the Research Ethics Committee of the Pontificia Universidade Catolica do Paraná. Dressings impregnated with vancomycin and CHG were produced at the LEID (Laboratory of Emerging Infectious Diseases) of the Pontifical Catholic University of Paraná. The proportions and properties of the dressings used in this study cannot be disclosed at this time, as they are protected by patent law (Law No. 9.279, May 14, 1996, Brazil). The control dressing consisted of the same material without impregnation. All participants must sign the Informed Consent Form, and interventions occurred only after the signing of this document.
2.4. Inclusion and exclusion criteria
Inclusion criteria are adult patients (18 years or older) already scheduled for the surgical procedure who provide informed consent to participate in the study. Exclusion criteria were patients allergic to vancomycin or CHG, with a known history of allergy to any of the drugs, recent infectious process, and immunocompromised.
2.5. Randomization
Randomization was done through sealed envelopes indicating the type of dressing to be used. The patient and the surgeon were blinded, with only the person responsible for the dressing production aware of the dressing type. The statistical analysis was blinded, and the groups were recognized after the final analysis.
2.6. Intervention and outcome
On the surgery day (day 0), the assigned dressing was be applied to the surgical site intraoperatively after suturing. A photograph of the sutured surgical incision was taken with pre-calibrated rulers placed adjacent to the surgical site for subsequent 2D morphometric analysis. Gauze will then be placed over the dressing, followed by a bandage over the entire surgical area. Participants were instructed not to disturb the dressings for the first 24 h. The first dressing change occurred after 24 h (day 1) in the hospital setting, still during the hospitalization. The second change occurred 48 h post-procedure (day 2), after discharge, to be done by the patient, who was instructed accordingly.
The next assessment was taken place after seven days (day 7) post-surgery in an outpatient setting at the same hospital. 2D morphometric analysis of the wound was conducted, with pre-calibrated rulers placed adjacent to the surgical site for a new photograph. Additionally, the doctor executed the Bluebelle Wound Healing Questionnaire (WHQ) and collect sociodemographic data for qualitative analysis of the surgical wound and the healing process.
Surgical site infection was the primary outcome and evaluated until day The definition of SSI was based on CDC (Center for Diseases Control) criteria, which included: 1) occurs within the first 30 days after surgery and involves only the skin and subcutaneous tissue; 2) purulent drainage from the superficial incision OR positive culture of secretion or tissue from the superficial incision, obtained aseptically (cultures collected by swab are not considered); 3) the superficial incision is intentionally opened by the surgeon in the presence of at least one of the following signs or symptoms: pain, increased sensitivity, local edema, hyperemia, or warmth, UNLESS the culture is negative.
2.7. Statistical analysis
Continuous variables were compared by student t test and expressed in absolute number or percentages. The categorical variables were analyzed by chi-square or Fisher test and expressed as absolute numbers or percentages. Statistical difference was considered when p <0.SPSS v23 was used for statistical analysis (IBM, Armonk NY).
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3. Materials and Methods
Microbiological tests demonstrated that the dressings exhibited significant antimicrobial activity against S. aureus, a pivotal bacterium in SSI (Figure 1). In the 7-day validation, the dressings maintained their activity. This test is crucial for defining the duration of dressing use, preventing unnecessary application due to activity loss, and potentially extending the usage time for patients lacking optimal wound care conditions, a common scenario in developing countries.
A total of 23 randomized patients were enrolled, with 2 excluded due to non-infectious compartment syndrome requiring re-intervention. Consequently, 21 patients were included for dressing application. Among the 21 included patients, 12 received the impregnated dressing (57.14%), and 9 received the control dressing (52.38%). The mean age was 38.35 years with a standard deviation of 14.59 years. Comorbidities were observed in 28.57% of patients, including three with systemic arterial hypertension and two with diabetes mellitus, one of whom had both comorbidities. Smoking, a risk factor for healing, was present in 21.74% of patients. Regarding gender, 90.47% (19/21) were male. Data for group comparison are structured in Table 1.
Considering the small number of patients in the pilot study, no statistical difference was observed between the groups. Only one case of SSI occurred, which was identified in the control group. Therefore, it is possible to consider that the impregnated dressing is equivalent to the control group, demonstrating its safe use. In Figure 2, the appearance of the dressing in the surgical area before covering with a transparent film can be observed.
4. Discussion
Antimicrobial dressings are routinely applied in the care of postoperative incisions, and the development of these dressings has garnered significant attention to meet the growing demands for wound protection against Surgical Site Infections (SSIs) and wound healing promotion [36]. Aligned with the global purpose of developing dressings with these attributes, our study, albeit in a pilot phase, enriches this discussion by presenting a potential strategy in the form of a dressing impregnated with vancomycin and CHG. This specific antimicrobial combination lacks prior investigations, highlighting the pioneering nature of this research in SSI prevention.
Regarding CHG, its efficacy in reducing MRSA contamination in surgical wounds has been previously tested in a porcine model, demonstrating significant antimicrobial activity and emphasizing the potential of CHG dressings against MRSA [37]. Furthermore, meta-analyses support this by stating that dressings impregnated with CHG significantly reduce infections related to central venous catheters, with rare adverse effects [38,39]. As for vancomycin, studies such as Kalalinia et al. (2021) presented vancomycin-loaded hybrid nanofibers, demonstrating a significant absence of cytotoxicity and effective inhibition of bacterial growth, highlighting the safe and effective use of vancomycin in this topical application [40]. However, the effectiveness of the dressing proposed by our pilot study cannot be compared with those described at this time due to the small sample size.
Therefore, given the lack of consensus regarding postoperative wound care, leaving the choice of dressing to the individual discretion of the physician, coupled with the limitations and uncertainties raised by previous studies, the urgent need for advancing research in this domain is emphasized [36,37]. Given the increasing relevance of the topic, the lack of substantial data, and the pilot nature of this study, we foresee, in line with the envisioned approach in previous research, the conception and execution of a randomized, double-blind, large-scale study with homogeneous sampling addressing the new dual-action antimicrobial dressing impregnated with vancomycin and CHG in operative wounds, aiming to achieve both statistical and clinical significance. Despite the small number of patients in our study, which precluded a comparative evaluation of infection rates due to the low incidence of this type of trauma at this time, the new dressing proved to be safe in trauma surgeries, indicating promising applicability in other surgeries.
Regarding the study limitations, this is a pilot study rather than a large-scale clinical trial, limiting the ability to draw robust conclusions about the effectiveness of the vancomycin and CHG dressing. Additionally, undisclosed properties of the dressings hinder replication in studies at other centers at the moment. Conducted in a single University Hospital in Curitiba-PR, the findings of the study may not be universally applicable. Therefore, future research addressing these limitations can enhance the overall assessment of the dressing's effectiveness in preventing Surgical Site Infections.
This study aimed to evaluate the efficacy and safety of operative wound dressings impregnated with vancomycin and CHG, standing out as an innovative approach in preventing SSI and highlighting the lack of prior research on this specific antimicrobial combination. We grounded our research in previous studies by considering the individual efficacy of CHG and vancomycin. However, the small number of patients did not allow for a comparative evaluation of the infection rate due to the low incidence of this type of trauma. Finally, based on the absence of adverse effects in the sample, our study demonstrated that this new dressing is safe for use in trauma surgeries, with potential applicability in other surgical procedures.
Author Contributions
Conceptualization, F.T. and L.D.; methodology, P.S.; validation, P.C., A.M. and M.M.; formal analysis, F.T.; investigation, L.D.; resources, F.T.; writing—original draft preparation, L.D.; writing—review and editing, F.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of PUCPR (protocol code 43295821.5.0000.0020, date 02/12/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request..
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sartelli M, Labricciosa FM, Coccolini F, Coimbra R, Abu-Zidan FM, Ansaloni L, et al. It is time to define an organizational model for the prevention and management of infections along the surgical pathway: a worldwide cross-sectional survey. World J Emerg Surg. 2022;17(1):17. [CrossRef]
- Tao J, Yan Z, Bai G, Zhang H, Li J. Enhanced Recovery after Surgery Rehabilitation Protocol in the Perioperative Period of Orthopedics: A Systematic Review. J Pers Med. 2023;13(3). [CrossRef]
- Rousseau T, Plomion C, Sandy-Hodgetts K. An advanced transparent hydropolymer wound dressing for undisturbed post-op management of surgical wounds following hip and knee replacement: A prospective observational series. Int Wound J. 2022;19(6):1456-62. [CrossRef]
- Birhanu A, Amare HH, M GM, Girma T, Tadesse M, Assefa DG. Magnitude of surgical site infection and determinant factors among postoperative patients, A cross sectional study. Ann Med Surg (Lond). 2022;83:104324. [CrossRef]
- Wolfe PN, Campfield BD, Crist BD, Keeney JA, Smith MJ, Cook JL, et al. Bacterial DNA screening to characterize surgical site infection risk in orthopaedic patients. J Orthop. 2021;27:56-62. [CrossRef]
- Tuon FF, Suss PH, Telles JP, Dantas LR, Borges NH, Ribeiro VST. Antimicrobial Treatment of Staphylococcus aureus Biofilms. Antibiotics (Basel). 2023;12(1). [CrossRef]
- Ribeiro VST, Cieslinski J, Bertol J, Schumacher AL, Telles JP, Tuon FF. Detection of Microorganisms in Clinical Sonicated Orthopedic Devices Using Conventional Culture and qPCR. Rev Bras Ortop (Sao Paulo). 2022;57(4):689-96. [CrossRef]
- Tuon FF, Dantas LR, Suss PH, Tasca Ribeiro VS. Pathogenesis of the Pseudomonas aeruginosa Biofilm: A Review. Pathogens. 2022;11(3). [CrossRef]
- da Rocha L, Ribeiro VST, de Andrade AP, Goncalves GA, Kraft L, Cieslinski J, et al. Evaluation of Staphylococcus aureus and Candida albicans biofilms adherence to PEEK and titanium-alloy prosthetic spine devices. Eur J Orthop Surg Traumatol. 2022;32(5):981-9. [CrossRef]
- Cieslinski J, Ribeiro VST, Kraft L, Suss PH, Rosa E, Morello LG, et al. Direct detection of microorganisms in sonicated orthopedic devices after in vitro biofilm production and different processing conditions. Eur J Orthop Surg Traumatol. 2021;31(6):1113-20. [CrossRef]
- Tuon FF, Cieslinski J, Ono AFM, Goto FL, Machinski JM, Mantovani LK, et al. Microbiological profile and susceptibility pattern of surgical site infections related to orthopaedic trauma. Int Orthop. 2019;43(6):1309-13. [CrossRef]
- Worldwide Antimicrobial Resistance National/International Network Group C. Ten golden rules for optimal antibiotic use in hospital settings: the WARNING call to action. World J Emerg Surg. 2023;18(1):50. [CrossRef]
- Cruz JAW, da Cunha M, de Moraes TP, Marques S, Tuon FF, Gomide AL, et al. Brazilian private health system: history, scenarios, and trends. BMC Health Serv Res. 2022;22(1):49. [CrossRef]
- Loesch GH, Cruz JAW, Gasparetto J, Oliveira DDS, Telles JP, Tuon FF. Cost minimization analysis of outpatient parenteral/oral antibiotic therapy at a trauma hospital: Public health system. Infect Control Hosp Epidemiol. 2021;42(12):1445-50. [CrossRef]
- Motelica L, Vasile BS, Ficai A, Surdu AV, Ficai D, Oprea OC, et al. Antibacterial Activity of Zinc Oxide Nanoparticles Loaded with Essential Oils. Pharmaceutics. 2023;15(10). [CrossRef]
- Aldakheel FM, Mohsen D, El Sayed MM, Fagir MH, El Dein DK. Employing of Curcumin-Silver Nanoparticle-Incorporated Sodium Alginate-Co-Acacia Gum Film Hydrogels for Wound Dressing. Gels. 2023;9(10). [CrossRef]
- Ribeiro CT, Dias FA, Fregonezi GA. Hydrogel dressings for venous leg ulcers. Cochrane Database Syst Rev. 2022;8(8):CD010738. [CrossRef]
- Arend L, Bergamo R, Rocha FB, Bail L, Ito C, Baura VA, et al. Dissemination of NDM-producing bacteria in Southern Brazil. Diagn Microbiol Infect Dis. 2023;106(2):115930. [CrossRef]
- Chaiben V, Yamada CH, Telles JP, de Andrade AP, Arend L, Ribeiro VST, et al. A carbapenem-resistant Acinetobacter baumannii outbreak associated with a polymyxin shortage during the COVID pandemic: an in vitro and biofilm analysis of synergy between meropenem, gentamicin and sulbactam. J Antimicrob Chemother. 2022;77(6):1676-84. [CrossRef]
- Telles JP, Yamada CH, Dario TM, Miranda AN, Pacheco A, Tuon FF. Impact of an antimicrobial stewardship program in a COVID-19 reference hospital according to the AWaRe classification. Am J Infect Control. 2022;50(10):1182-4. [CrossRef]
- Ito CAS, Bail L, Arend L, Nogueira KDS, Tuon FF. The activity of ceftazidime/avibactam against carbapenem-resistant Pseudomonas aeruginosa. Infect Dis (Lond). 2021;53(5):386-9. [CrossRef]
- Bail L, Ito CAS, Arend L, Pilonetto M, Nogueira KDS, Tuon FF. Distribution of genes encoding 16S rRNA methyltransferase in plazomicin-nonsusceptible carbapenemase-producing Enterobacterales in Brazil. Diagn Microbiol Infect Dis. 2021;99(2):115239. [CrossRef]
- Zequinao T, Telles JP, Gasparetto J, Tuon FF. Carbapenem stewardship with ertapenem and antimicrobial resistance-a scoping review. Rev Soc Bras Med Trop. 2020;53:e20200413. [CrossRef]
- Tuon FF, Cieslinski J, Rodrigues SDS, Serra FB, Paula MD. Evaluation of in vitro activity of ceftolozane-tazobactam against recent clinical bacterial isolates from Brazil - the EM200 study. Braz J Infect Dis. 2020;24(2):96-103. [CrossRef]
- Zequinao T, Gasparetto J, Oliveira DDS, Silva GT, Telles JP, Tuon FF. A broad-spectrum beta-lactam-sparing stewardship program in a middle-income country public hospital: antibiotic use and expenditure outcomes and antimicrobial susceptibility profiles. Braz J Infect Dis. 2020;24(3):221-30. [CrossRef]
- Chiquin CA, Silva JH, Ciruelos MJ, Lemes MC, Penteado-Filho SR, Tuon FF. Postdischarge surveillance system for nontuberculous mycobacterial infection at a Brazilian regional referral hospital after an outbreak. Infect Control Hosp Epidemiol. 2009;30(4):399-401. [CrossRef]
- Oprica GM, Panaitescu DM, Usurelu CD, Vlasceanu GM, Stanescu PO, Lixandru BE, et al. Nanocellulose Sponges Containing Antibacterial Basil Extract. Int J Mol Sci. 2023;24(14). [CrossRef]
- Suneetha M, Won SY, Zo SM, Han SS. Fungal Carboxymethyl Chitosan-Impregnated Bacterial Cellulose Hydrogel as Wound-Dressing Agent. Gels. 2023;9(3). [CrossRef]
- Awasthi A, Gulati M, Kumar B, Kaur J, Vishwas S, Khursheed R, et al. Recent Progress in Development of Dressings Used for Diabetic Wounds with Special Emphasis on Scaffolds. Biomed Res Int. 2022;2022:1659338. [CrossRef]
- Wali N, Wajid N, Shabbir A, Ali F, Shamim S, Abbas N, et al. Safety Considerations for Lyophilized Human Amniotic Membrane Impregnated with Colistin and Silver Nanoparticles. Appl Biochem Biotechnol. 2023. [CrossRef]
- Xu H, Hyun A, Mihala G, Rickard CM, Cooke ML, Lin F, et al. The effectiveness of dressings and securement devices to prevent central venous catheter-associated complications: A systematic review and meta-analysis. Int J Nurs Stud. 2023;149:104620. [CrossRef]
- Cerchiara T, Abruzzo A, Nahui Palomino RA, Vitali B, De Rose R, Chidichimo G, et al. Spanish Broom (Spartium junceum L.) fibers impregnated with vancomycin-loaded chitosan nanoparticles as new antibacterial wound dressing: Preparation, characterization and antibacterial activity. Eur J Pharm Sci. 2017;99:105-12. [CrossRef]
- de Andrade AP, Arend L, Ribeiro VST, Tuon FF. Resistance of clinical and environmental Acinetobacter baumannii against quaternary ammonium. Infect Control Hosp Epidemiol. 2022;43(4):527-30. [CrossRef]
- Mendonca JR, Dantas LR, Tuon FF. Activity of multipurpose contact lens solutions against Staphylococcus aureus, Pseudomonas aeruginosa, Serratia marcescens and Candida albicans biofilms. Ophthalmic Physiol Opt. 2023;43(5):1092-9. [CrossRef]
- Pedroni MA, Ribeiro VST, Cieslinski J, Lopes APA, Kraft L, Suss PH, et al. Different concentrations of vancomycin with gentamicin loaded PMMA to inhibit biofilm formation of Staphylococcus aureus and their implications. J Orthop Sci. 2022;14(14):S0949-2658(22)00336-0. [CrossRef]
- Jiang N, Rao F, Xiao J, Yang J, Wang W, Li Z, et al. Evaluation of different surgical dressings in reducing postoperative surgical site infection of a closed wound: A network meta-analysis. Int J Surg. 2020;82:24-9. [CrossRef]
- Mana TSC, Donskey C, Carty N, Perry L, Leaper D, Edmiston CE, Jr. Preliminary analysis of the antimicrobial activity of a postoperative wound dressing containing chlorhexidine gluconate against methicillin-resistant Staphylococcus aureus in an in vivo porcine incisional wound model. Am J Infect Control. 2019;47(9):1048-52. [CrossRef]
- Safdar N, O'Horo JC, Ghufran A, Bearden A, Didier ME, Chateau D, et al. Chlorhexidine-impregnated dressing for prevention of catheter-related bloodstream infection: a meta-analysis*. Crit Care Med. 2014;42(7):1703-13. [CrossRef]
- Buetti N, Rickard CM, Timsit JF. Catheter dressings. Intensive Care Med. 2022;48(8):1066-8. [CrossRef]
- Kalalinia F, Taherzadeh Z, Jirofti N, Amiri N, Foroghinia N, Beheshti M, et al. Evaluation of wound healing efficiency of vancomycin-loaded electrospun chitosan/poly ethylene oxide nanofibers in full thickness wound model of rat. Int J Biol Macromol. 2021;177:100-10. [CrossRef]
Figure 1.
Disk testing of vancomycin-CHG impregnated dressing 24 h after impregnation and 7 days after continuous skin contact.
Figure 1.
Disk testing of vancomycin-CHG impregnated dressing 24 h after impregnation and 7 days after continuous skin contact.
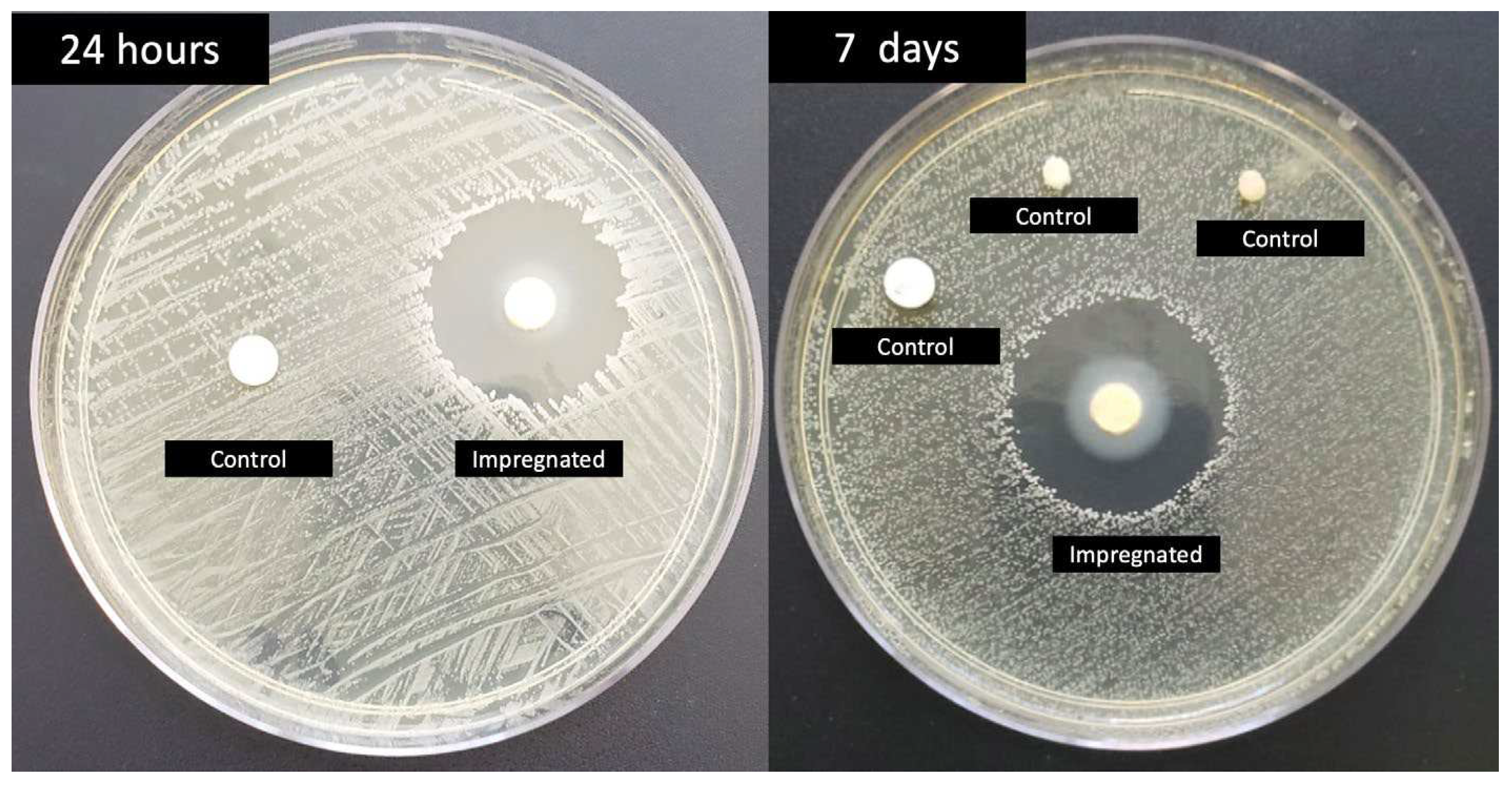
Figure 2.
Surgical wound before (A) and after (B) vancomycin-CHG impregnated dressing.
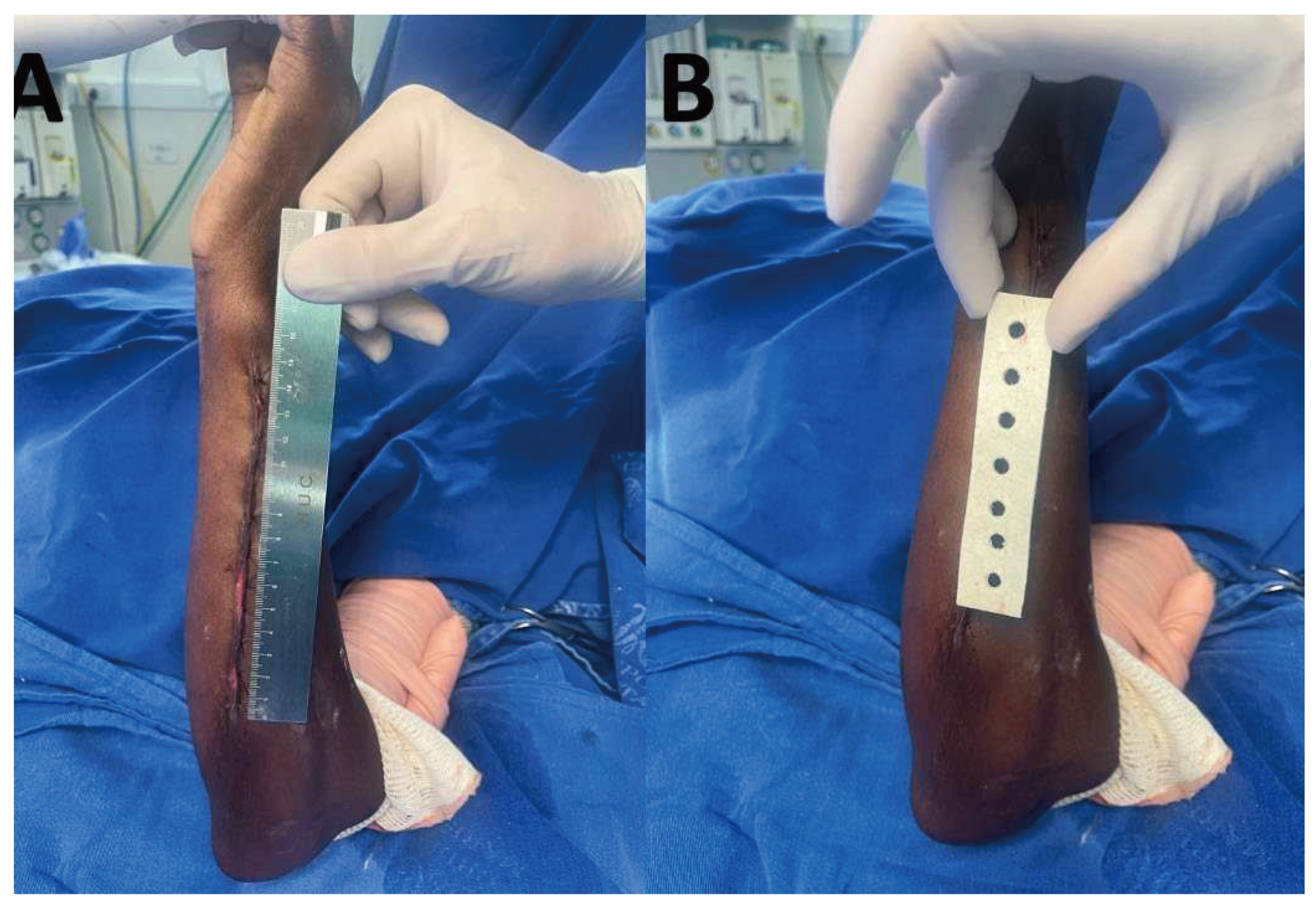

Table 1.
Clinical and outcome data of patients under vancomycin-chlorhexidine impregnated dressing and control group. SAH – Systemic arterial hypertension; DM – diabetes mellitus; SD – Standard deviation.
Table 1.
Clinical and outcome data of patients under vancomycin-chlorhexidine impregnated dressing and control group. SAH – Systemic arterial hypertension; DM – diabetes mellitus; SD – Standard deviation.
| Impregnated dressing (n=12) | % | Control (n=9) | % | total | % | ||
| Aging (years/SD) | 42.91+/-17.46 | 34.77+/-9.41 | 39.42+/-14.84 | ||||
| Male sex | 11 | 91.66 | 8 | 88.88 | 19 | 90.47 | |
| Comobidities | 1 | 11.11 | 1 | 4.76 | |||
| SAH | 3 | 25 | 1 | 11.11 | 4 | 19.04 | |
| DM | 2 | 16.67 | 1 | 11.11 | 3 | 14.28 | |
| Smoking | 2 | 16.67 | 2 | 22.22 | 4 | 19.04 | |
| Trauma | |||||||
| Lower limbs | 9 | 75 | 6 | 66.67 | 15 | 71.42 | |
| Upper limbs | 3 | 25 | 3 | 33.33 | 6 | 28.57 | |
| Infection | 0 | 0 | 1 | 11.11 | 1 | 4.76 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



