
Submitted:
12 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
Measles is targeted for elimination since 2001, with significant reduction in cases recorded worldwide, but outbreaks occur periodically due to immunization gaps. The present study analyzes the evolution of vaccination coverage rates (VCR) in Romania, a EU country with large measles epidemics during the last two decades, including an ongoing outbreak in 2023. Vaccination against measles is included in the National Immunization Program from 1979, initially as a single dose, and since 1994, with 2 doses. The vaccine uptake was initially high, with national VCR of >97%. However, from 2010 onwards, the VCR dropped and remained constantly under 90%. This decline was caused by several factors, including a decreasing number of general practitioners, discontinuities in vaccine supply, emigration, with increased numbers of children lost to follow-up and a surge in vaccine hesitancy. Additional decreases in the already low levels of VCR were recorded during the COVID-19 pandemic: in 2022 the VCR reached the lowest level in the last decade, with 83.4% for the first dose (6.6% decrease compared to 2019) and 71.4% for the second dose (4.4% decrease compared to 2019), with important subregional differences. The constant suboptimal vaccination coverage rate in Romania threatens the progress toward measles elimination.
Keywords:
measles
; vaccine coverage
; outbreak
; Romania
; vaccine hesitancy
1. Introduction
Measles is an acute, self-limiting viral infection, with universal spread and high contagiousness, that primarily affects children, with potential severe complications: pneumonia, otitis, acute encephalitis, subacute sclerosing panencephalitis and prolonged anergy.
Measles elimination is a feasible target, but requires vaccination coverage rates of more than 95%, with two doses of the highly effective live attenuated measles-containing vaccine administered in all population groups and in all geographic areas [1,2,3] to interrupt the transmission chains.
Important milestones in the WHO strategy toward measles and rubella elimination [2] have been achieved globally during the last two decades, with significant reductions in the burden of both diseases, improved surveillance and increased vaccine uptake in the national immunization programs. Nevertheless, outbreaks occur periodically, due to immunization gaps, and measles remains one of the leading causes of death in children worldwide [4,5]. In Europe, a resurgence of measles cases was seen during 2016-2019, followed by a period of substantial decrease during the COVID-19 pandemic years, most probably reflecting both the efficacy of nonpharmacological control measures, with global low transmission of all respiratory viruses, and underreporting [6,7]. Worldwide, the COVID-19 pandemic has caused a significant delay in all immunization programmes, with a decrease in the percentage of children receiving a first dose of measles vaccine (from 86% in 2019 to 81% in 2021) [8]. Although in 2022 there is a positive trend toward vaccination recovery, it is estimated that globally, 21.9 million children did not receive measles vaccine [8]. Large disparities in measles immunization rates exist worldwide, between high-, middle- and low-income countries [8]. The overall population-weighted vaccination coverage rate in EU remains under 95% for both doses of measles containing vaccine (MCV), with several countries reporting significantly lower rates [9].
Romania is an EU country with over 19 million inhabitants [10] situated in South-Eastern Europe, with a border with Ukraine, where the current armed conflict caused large displacement of population, influx of migrants in the neighboring countries and disruption of medical services, including immunization programs. Measles vaccination has been introduced in the National Immunization Program (NIP) in Romania in 1979, using a monovalent live attenuated vaccine, and is presently carried out with the combined MMR (measles-rubella-mumps) vaccine, administered in a 2 doses schedule (at 12 months of age and at 5 years). Vaccination is not mandatory, but is highly recommended and vaccines are provided free of charge to every children registered in the healthcare system. In the pre-vaccination era, measles incidence rates in Romania were high (120-140 cases/100 000 inhabitants). An important decline was registered after the introduction of monovalent measles vaccination in the NIP, with incidences below 60 cases/100 000 inhabitants, and smaller measles epidemics that occurred at longer intervals compared to the pre-vaccination years [11]. After a national immunization campaign in 1998-1999 (targeting all children aged 7-18 years who lacked immunization records of 2 vaccine doses) [12] and the implementation of a national case-based surveillance in 1999, a further drop in measles incidence was recorded (0.3 cases per 100 000 inhabitants in 2000). Romania entered the measles elimination phase and 2008-2009 was the first period with measles notification rates < 1 case/million inhabitants. In 2010 there were 193 measles cases (notification rate 0.9%000 ), mostly due to a small outbreak in counties in the North and North-eastern regions [13].
Nevertheless, two large measles epidemics emerged at short intervals of time during the last 2 decades (2011-2012 and 2016-2020). During the 2011-2012 outbreak there were 12,234 confirmed cases of measles, of which 3 deaths. The most prevalent viral strain identified belonged to genotype D4, endemic to Romania [14]. The most affected group (incidence >700/100 000) were children under 1 year of age, who are not eligible for MCV vaccination. Between 2011 and 2012, Romania faced a concurrent epidemic of rubella, caused by genotype 2B, with 24 627 confirmed cases, without deaths [15]. The most affected age group by rubella was 15-19 years, adolescents belonging to cohorts born in 1995 – 1997, who were not vaccinated against rubella (the combined measles, mumps and rubella vaccine was introduced in the national schedule in 2004). During the 2016-2020 measles epidemic there were more than 20,000 confirmed cases and 64 deaths [16]. Again, the most affected age group (incidence > 900/100 000) was under 1 year of age, not eligible for MCV vaccination, followed by unvaccinated children aged 1-5 years. One of the reasons that contributed to the spread of the epidemic was non-compliance with isolation conditions in hospitals/pediatric wards. The epidemic started in the North and Northwestern regions of the country, in communities whose members frequently migrate from one county to another, but also outside Romania, and do not vaccinate their children. The prevalent viral strain identified belonged to an imported genotype B3 [17].
With this background, the present study aims to analyze the evolution of measles vaccine coverage rates and its impact on the measles elimination process in Romania.
2. Materials and Methods
National measles surveillance data and MMR vaccination coverages rates were extracted from the data collected by the National Centre for Communicable Diseases Surveillance and Control in Bucharest (NCDC). In Romania measles is a notifiable disease since 1978, suspected measles cases must be immediately reported to the local Public Health Authorities and data are collected and analyzed at the NCDC. A national case-based notification for measles was initiated in 1999, the European Union (EU) case definition and classification [18] have been adopted since 2005 and monthly reports are submitted to the ECDC and WHO through the electronic European surveillance system (TESSy). Like most vaccinations included in the Romanian NIP, MMR vaccination is carried out by general practitioners. Vaccination coverage rates for each vaccine dose are estimated by reviewing the immunization records in all general practitioners’ offices, information is gathered from each of the 42 districts in Romania and assessed repeatedly for each year’s birth cohort at 12, 18, and 24 months of age. A dedicated questionnaire, with items on the number of vaccinated children, reasons for non-vaccination, vaccination refusal; missed presentation; vaccines shortages (all by type of vaccine and number of doses) is filled in for every district. Data segregated by high-risk subpopulations are not available. A supplementary analysis of the national questionnaires distributed during the last measles epidemic (2016-2020) was conducted in order identify to factors related to suboptimal vaccination uptake.
3. Results
3.1. Description of measles vaccination in the national immunization program
From 1979 to 1993 a single dose of the monovalent measles vaccine was recommended for children aged 9-11 months. In 1994, a second measles vaccine dose was introduced for children 6-7 years of age (first school grade). Supplementary immunization activities (SIA) were organized periodically to increase the vaccine coverage rates: in 1993 (catch-up SIA for all children aged 1-14 years, with a reported vaccine coverage of 97%) and 2002 (follow-up SIA for children aged 1-4 years with reported vaccine coverage of 87%). The combined measles, mumps and rubella vaccine replaced the monovalent vaccine in 2004, with a first dose (MCV1) administered at 12 months of age and a second dose (MCV2) administered at 6-7 years (age at school entry) from 2005 onwards. Since 2015, MCV2 is administered at age 5 years, in order to ensure catch-up vaccination before school admission, for those who missed the first dose.
3.2. Evolution of vaccine coverage rates
According to the national database, after the introduction of the combined measles mumps rubella vaccine, during 2005-2009, the national vaccine coverage rates reached 96%-97% for both MCV1 and MCV2. However, from 2010 onwards, a decreasing trend was observed, with MCV1 coverage rates constantly under 90%., reaching the lowest level of 85% in 2015. The MCV2 coverage rate declined slowly, with vaccine coverage rates between 87- 93% during 2010-2014, and dropped under 75% during 2015-2019 (with a temporary increase to 82% in 2018) (Figure 1).
Comparing MMR vaccine coverage data from the pre-pandemic year (2019) with data from the subsequent pandemic years (2020 and 2021) we note a decrease in the vaccination coverage rates with more than 2% in 2020 and 2021 for MCV1, as well as an additional drop of more than 0.5% in the already low MCV2 coverage. In 2022 the vaccine coverage rates reached the lowest level in the last decade with 83.4% for MCV1 (6.6% decrease compared to 2019) and 71.4% for MCV2 (4.4% decrease compared to 2019). (Figure 1).
3.3. Sub-national vaccination coverage rates
Significant differences in the vaccine coverage rates are present between Romania’s 42 counties. During the last two years, there was a significant growth in the percentage of counties with vaccine coverage rates of less than 75% assessed in children aged 12 months, when the first dose of MMR is administered according to the national schedule (38% in 2021 vs 78% in 2022). Only 3 counties had a vaccine coverage rate higher than 90% each year and none have attained the 95% coverage required for interruption of measles transmission (Table 1). However, a global increase was recorded at age 18 months (Table 1), with 35.7% of counties in 2021 and 21.4% in 2022 reaching in vaccine coverage rates of more than 90% (vs 7.1% at 12 months). Still, a vaccine coverage of more than 95% was reached in only 3 counties in 2021 and 4 in 2022.
3.4. Reasons for non-vaccination
An analysis of the questionnaires’ data collected from the 42 counties by the National center for Disease Control, in the pre-pandemic years, revealed that the main reasons for non - vaccination were: failure to attend the GP’s office- with significant differences in urban vs rural communities, (45.9 % in urban vs 37.9% in rural, p = 0.001) and temporary medical contraindications, without significant differences in urban vs rural communities (25.9% in urban vs 25.5% in rural, p = 0.85). Other reasons were vaccination refusal (higher for MCV compared to other vaccines included in the national immunization programme), without significant differences in urban vs rural settings (9.9% in urban vs 7.8% in rural, p = 0.61) and the percentage of children lost to follow-up (born/living abroad), without significant differences in urban vs rural communities (7.6% in urban vs 11.7% in rural, p = 0.15).
3.5. Measles incidence 2020-2023
The last measles epidemic in Romania ended in the summer of 2020, although 1004 measles cases were still confirmed in the first 6 months of the year, despite all nonpharmacologic measures installed during the COVID 19 pandemic (incidence 5,2 cases/ 100 000 inhabitants, 4 times lower compared to 2019- 20 cases/ 100 000 inhabitants). During 2021-2022 the number of reported measles case was very low (2 cases in 2021 and 10 in 2022), mirroring the general EU pattern.
Yet, during the first 10 months of 2023, 1560 measles cases have been already reported, 91% were recorded in unvaccinated persons. Most measles cases (42.6%) in 2023 are registered in the age group 1-4 years old - the target group for vaccination (94.9% in unvaccinated children), and 11.9% of the total number of cases diagnosed until now are in children < 1 year old, who are not eligible for MCV vaccination, according to the national immunization programme - Figure 2.
For now, the epidemic is concentrated mostly in center and western regions of Romania, but starts spreading to the southern part of the country. Out of the total number of cases, 620 (39.7%) are recorded in a single county- Mures, followed by two neighboring counties Brasov -268 (17,1%) and Cluj -186 (11,9%). The 2022 vaccine coverage for both MCV1 and MCV2 in the most affected counties is presented in Table 2.
During the previous 5 years, counties with the highest number of cases tend to have constantly lower MCV1 coverage rates than the national average rate, both when assessed at 12 months and 18 months of age (Figure 3), with the exception of Cluj, which is the second most populated county in Romania (>710 000 registered residents), and has a high influx of non-residents commuting from neighboring cities for work and high number of national and international students.
4. Discussion
Measles remains endemic in Romania, due to a constant decline in the vaccination coverage rates since 2010. This reversal of the progress made during the previous decade has several reasons including: (a) high migration rates with families moving frequently and children lost to follow-up, missing vaccination appointments, or not attending general practitioners office, (b) a decreasing number of general practitioners, with dissimilar inter-counties distribution (c) heterogeneous and sometimes suboptimal caregivers’ information on the vaccination schedule and temporary contraindications for vaccination, (d) discontinuities in the supplies of MMR vaccines, (e) a constant increase in vaccine hesitancy and widespread anti-vaccination movements. Further reduction in the vaccination rates during 2000-2022 can be explained by a decrease in addressability following movement restrictions and by disruptions in the health system, with significant human resources concentrated for the pandemic management. However, the most concerning factor is vaccine hesitancy, with an increasing mistrust regarding the safety of vaccination, observed worldwide [19]. Fear of unproved long term adverse reactions became an important reason for not vaccinating in Romania [20]. Accordingly, the country has one of the lowest COVID 19 vaccination rates in the European Union, with 50.7% of the population vaccinated with a primary scheme and less than 10% with a first booster (compared to the global rate of 82.4% and 54.8% respectively in EU/EEA) and the overall coverage rate for all vaccines is decreasing [21]. In order to increase vaccine acceptance, extensive and sustained communication campaigns are needed and a national communication strategy on vaccination must by implemented, building upon the European information campaigns with high-quality scientific information for both health personnel and the general population on the benefits of vaccination and a correct and balanced view on the risk of adverse events following immunization [22].
A recently published ethnographic study on the barriers and drivers towards vaccination in Romania identified disparities in clinics with low and high vaccine coverage rates ( in terms of contraindication assessment, type of information provided to the child’s caregiver related to adverse events, openness to questions, appointment scheduling and correctitude of administration techniques ) and defined interventions to increase the training of healthcare providers and to improve the services for vulnerable, disadvantaged population [23]. The general practitioner’s network does not cover uniformly all country’s regions [24], there are areas with scarce human resources and difficult access for the most vulnerable populations (unemployed persons with no health insurance, mono-parental families, people living in poverty, Roma minorities). During the previous measles epidemic these groups have been over-represented among cases, proving little addressed health inequities [20]. A mid-term term solution could be the establishment of community centers, delivering integrated health care and prevention activities, including vaccination and vaccine-related education. Integrated community centers, established by the Ministry of Health [25], can serve more efficiently the rural communities, ensuring a dedicated space for community nurses, as well as of socio-educational assistance services. This type of facilities will ensure patients’ privacy, confidentiality and dignity and will favor teaming up with other specialists (doctors, other community nurses, midwives, health mediators). Nevertheless, support from the local authorities is necessary, to establish health community assistance programs and to increase access of the most vulnerable groups to social and medical services.
The constant decreasing measles containing vaccine coverage in Romania explain the recurrent measles epidemics seen during the last decade. These epidemics were largely predictable. In 2015, using a mathematical model [26], a high risk score was calculated for 13 counties (taking into account the vaccine coverages rates for MCV 1 and 2, the number of measles cases during the previous three years and other contributing factors at the county level: refusal to vaccinate, vaccine hesitancy due to fears regarding the safety of vaccines, difficult access to the family doctor's office, mobile population) - these counties, mostly in the Western part of Romania, accounted for the highest number of cases during the 2016 epidemic. The same observation is true for the ongoing 2023 outbreak, as indicated by the present study, the highest attack rates are registered in counties with low vaccine coverage rates. In addition, the existence of high mobility populations who are frequently moving between counties in search for work and miss children’s vaccinations, may contribute to measles spread in pockets of unvaccinated children, even in counties with an overall better vaccination coverage. As reflected by the results of the present study, vaccine coverage rates increase at 18 months compared to 12 months of age, this may reflect delays in vaccinations and/or reporting, that allow accumulation of susceptible children. Cases in adults remain infrequent, reflecting both a better vaccine coverage rate for those aged >18 years and the long-term persistence of immunity after natural infection (for older adults, born before the introduction of measles vaccination). As a response to the current measles outbreak, supplementary immunization activities are ongoing, with catch-up vaccination campaigns organized in each county, especially in communities with suboptimal vaccination coverage. Still, the results are modest, with only 10% of those aged between 1 and 18 years recovered for vaccination until October 2023. At mid-November, an early-age vaccination campaign was initiated for children aged 9-11 months, who remain at high risk for measles, as long as herd immunity is not ensured.
The risk of future outbreaks might be further amplified by a high risk of measles importation, due to the influx of immigrants for neighboring Ukraine, where vaccine coverage is also suboptimal and large measles outbreaks were recorded in 2017-2019 [27]. Romania has also a growing influx of immigrant workers and import of new measles strains from these regions is highly probable. The identified measles virus strain in the current outbreak in Romania belongs to genotype D8, is phylogenetically related to Asian strains and different from the one circulating during the last measles outbreak [28]. The Romanian Ministry of Health and public health authorities have implemented, with WHO support [29], enhanced measles surveillance activities nationwide, along with a rapid implementation of catch-up vaccination strategies. In addition, specific actions are implemented to check the immunization status of all refugee children under 6 years of age, and free MCV vaccination is offered for immigrants, prioritizing children with missed doses in the first 14 days since entry [30]. Immunizations are reported in the national electronic system (RENV) and vaccination certificates are issued for foreign citizens. Routine immunization activities and public information were intensified, with distribution of multilingual health information booklets and leaflets beyond border crossing points and provinces, post on Facebook and official website in four languages.
It is well known that measles vaccination status is “the canary in the cold mine”, reflecting deficiencies in the overall performance of the immunization programme. Indeed, the vaccination coverage is decreasing in Romania for almost all vaccines included in the national immunization program (inactivated polio vaccine, dipthero-tetano-pertusis vaccine, Hemophilus influenza vaccine, pneumococcal vaccine- all with vaccine coverage of 78.5% and hepatitis B vaccine – 75.4% vaccine coverage) [31]. According to the last UNICEF report, in 2021, Romania had one of the highest shares of children with zero dose (9723, 5 % share of children under 1 year) and under-vaccinated children (17 510, 9% share of children under 1 year) from countries in Europe [32].
The ongoing measles outbreak in Romania represent a risk for transmission in the neighboring countries and all over the European Union. Despite the fact that the European regional MCV1 coverage was 93% in 2022, decreases in the vaccination coverage rates were reported in 2021 by 15 countries in the EU/EEA [9]. Until now, the total burden of cases the European Union remain low: according to the last available ECDC report, apart from the epidemic in Romania, only Austria has reported 154 cases, France 64 cases, Germany 51 cases, Belgium 34 cases, other countries have less than 10 reported cases) [33]. The same is true for neighboring Romanian countries, including Ukraine, where 44 cases have been reported until September 2023 [33].
The European Immunization Agenda 2030 [3], launched at the end of 2021, aims to reduce discrepancies in the vaccination coverage between countries, addressing both vaccine acceptance and vaccine procurement and logistic. In Romania, a national vaccination strategy and a specific plan for measles and rubella elimination were recently developed, with specific measures aimed at ensuring a constant vaccine supply, an efficient and equitable vaccine distribution and increased accessibility [34]. A life-long vaccination approach was implemented for the first time, with MCV recommended and reimbursed for bone marrow transplant recipients and their family contacts who do not have specific detectable antibodies. Hopefully, taken together, these measures will sustain a progressive increase in vaccination uptake, which in turn, will help reach the measles elimination target.
5. Conclusions
A suboptimal measles vaccination coverage was maintained in Romania during the last decade, reversing the progress made toward measles elimination. The accumulating immunizations gaps in the susceptible population was at the origin of several large outbreaks, including an ongoing one in 2023. An increasing vaccine hesitancy, amplified by the COVID 19 pandemic, as well as the increased population movements (with both Romanian emigrating and increasing number of immigrants and refugees) represents a real threat for future epidemics, with potential dissemination in the European Union.
Author Contributions
Conceptualization, SR and AS; methodology, AP, CC, SR; data acquisition and analysis: AS, SR.; validation, SR, CC and AP.; formal analysis, AS, SR.; resources, SR; writing—original draft preparation, AS, SR.; writing—review and editing SR, CC, AP supervision, CC, SR.; funding acquisition SR, AP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data presented are available upon request from first author (AS).
Acknowledgments
The publication of this paper was supported by Carol Davila University of Medicine and Pharmacy through the program “Publish not Perish”. The authors express their gratitude to all 42 local public health authorities for their constantly effort to prepare and send us in real time all surveillance and vaccination coverages data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Measles and rubella strategic framework 2021–2030. Geneva:; 2020. Licence: CC BY-NC-SA 3.0 IGO. ISBN 978-92-4-001562-3. Available online: https://iris.who.int/bitstream/handle/10665/339801/9789240015616-eng.pdf?sequence=1 (accessed on 28 October 2023).
- European Immunization Agenda 2030. Copenhagen:WHO Regional Office for Europe; 2021. Licence: CC BY-NC-SA 3.0 IGO. ISBN: 978-92-890-5605-2.
- World Health Organization. WHO-UNICEF estimates of MCV1 coverage. 2020. Available online: https://apps.who.int/immunization_monitoring/globalsummary/timeseries/tswucoveragemcv1.html (accessed on 8 October 2023).
- Sbarra AN, Mosser JF, Jit M, et al. Estimating national-level measles case-fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study. Lancet Glob Health 2023, 11, e516–24. [CrossRef] [PubMed]
- Minta AA, Ferrari M, Antoni S, et al. Progress toward regional measles elimination—worldwide, 2000–2021. MMWR Morb Mortal Wkly Rep 2022, 71, 1489–95. [CrossRef] [PubMed]
- Minta AA, Ferrari M, Antoni S, et al. Progress Toward Measles Elimination — Worldwide, 2000–2022. MMWR Morb Mortal Wkly Rep 2023;72:1262–1268. [CrossRef]
- WHO. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
- European Centre for Disease Prevention and Control. Measles. In: ECDC. Annual Epidemiological Report for 2022. Stockholm: ECDC; 2023.
- National Institute of Statistics. Statistical data (population by county). Available online: http://statistici.insse.ro:8077/tempo-online/#/pages/tables/insse-table.
- National Center for Disease Control. Evolution analysis of communicable diseases under surveillance, Annual reports. https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/rapoarte-anuale/Romanian accessed January 2023.
- Ion-Nedelcu N, Craciun D, Pitigoi D, Popa M, Hennessey K, Roure C, Aston R, Zimmermann G, Pelly M, Gay N, Strebel P. Measles elimination: a mass immunization campaign in Romania. Am J Public Health 2001, 91, 1042-5. [CrossRef]
- National Center for Disease Control. Analysis of transmissible diseases evolution for 2010, available at https://www.cnscbt.ro/index.php/rapoarte-anuale/544-analiza-evolutiei-bolilor-transmisibile-aflate-in-supraveghere-raport-pentru-anul-2010. accessed June 2023.
- Stanescu A, Janta D, Lupulescu E, Necula G, Lazar M, Molnar G, Pistol A. Ongoing measles outbreak in Romania, 2011. Euro Surveill. 2011, 16, pii=19932.
- Lazar M, Abernathy E, Chen MH, Icenogle J, Janta D, Stanescu A, Pistol A, Santibanez S, Mankertz A, Hübschen JM, Mihaescu G, Necula G, Lupulescu E. Epidemiological and molecular investigation of a rubella outbreak, Romania, 2011 to 2012. Euro Surveill. 2016, 21, 30345. [CrossRef]
- National Institute of Public Health. National Centre for Communicable Diseases Surveillance and Control, Weekly reports. Romanian. Available from: https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/informari-saptamanale/Accessed June 2023.
- Lazar M, Stănescu A, Penedos AR, Pistol A. Characterisation of measles after the introduction of the combined measles-mumps-rubella (MMR) vaccine in 2004 with focus on the laboratory data, 2016 to 2019 outbreak. Euro Surveill. 2019, 24, 1900041. [CrossRef]
- Commission decision of 19 March 2002 laying down case definitions for reporting communicable diseases to the Community network under Decision No 2119/98/EC of the European Parliament and of the Council (2002/253/EC), Official Journal of the European Communities 03.04.2002. Available online: http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2002:086:0044:0062:EN:PDF.
- Larson HJ, Gakidou E, Murray CJL. The Vaccine-Hesitant Moment. N Engl J Med. 2022 Jul 7;387(1):58-65. [CrossRef]
- Habersaat KB, Pistol A, Stanescu A, Hewitt C, Grbic M, Butu C, Jackson C. Measles outbreak in Romania: understanding factors related to suboptimal vaccination uptake. Eur J Public Health. 2020, 30, 986–992. [CrossRef] [PubMed]
- ECDC. COVID-19 Vaccine Tracker, available at: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab, accessed May 2023.
- Gastañaduy PA, Banerjee E, DeBolt C, Bravo-Alcántara P, Samad SA, Pastor D, Rota PA, Patel M, Crowcroft NS, Durrheim DN. Public health responses during measles outbreaks in elimination settings: Strategies and challenges. Hum Vaccin Immunother. 2018, 14, 2222–2238. [CrossRef] [PubMed]
- Dube E, Pistol A, Stanescu A, Butu C, Guirguis S, Motea O, Popescu AE, Voivozeanu A, Grbic M, Trottier MÈ, Brewer NT, Leask J, Gellin B, Habersaat KB. Vaccination barriers and drivers in Romania: a focused ethnographic study. Eur J Public Health. 2023, 33, 222–227. [CrossRef]
- National Institute of Statistics. The heath network activity in 2020, 2021, Romanian, available at https://insse.ro/cms/files/publicatii/publicatii%20statistice%20operative/activitatea_retelei_sanitare_in_anul_2020.pdf.
- Ministry of Health Romania. Annex to the Order of the Minister of Health nr. 2.931/2021 regarding the approval of the Manual of integrated community centers published in the Official Gazette of Romania No. 1240 bis, Romanian, available at https://legislatie.just.ro/Public/DetaliiDocumentAfis/250002.
- Kriss JL, Stanescu A, Pistol A, Butu C, Goodson JL. The World Health Organization Measles Programmatic Risk Assessment Tool-Romania, 2015. Risk Anal. 2017, 37, 1096–1107. [CrossRef] [PubMed]
- Rodyna R, Measles situation in Ukraine during the period 2017-2019. European Journal of Public Health 2019, 29 (Suppl 4), ckz186.496. [CrossRef]
- Lazar M, Pascu C, Roșca M, Stănescu A. Ongoing measles outbreaks in Romania, March 2023 to August 2023. Euro Surveill. 2023, 28, pii=2300423. [CrossRef]
- WHO. Guidance for host countries in the context of mass population movement from Ukraine WHO/EURO:2022-5135-44898-63834. Available online: https://iris.who.int/bitstream/handle/10665/352373/WHO-EURO-2022-5135-44898-63834-eng.pdf?sequence=1 (accessed on 10 September 2023).
- Ministry of Health. Romania Emergency ordinance No. 15/2022 on the provision of support and humanitarian assistance by the Romanian state to foreign citizens or stateless persons in special situations, coming from the area of the armed conflict in Ukraine.
- National Institute of Public Health. National Centre for Communicable Diseases Surveillance and Control, Weekly reports. Romanian. Vaccine coverage Romania, 2022. Available online: https://www.cnscbt.ro/index.php/analiza-date-supraveghere/evaluarea-acoperirii-vaccinale/3514-analiza-rezultatelor-estimarii-acoperirii-vaccinale-la-varsta-de-18-luni-februarie-2023/file (accessed on 20 November 2023).
- UNICEF. The State of the World’s children. Regional Brief. European and Central Asia 2023. Available online: https://www.unicef.org/eca/reports/sowc2023-eca (accessed on 20 November 2023).
- European Centre for Disease Prevention and Control, Communicable Disease Threats Report, week 5-11 November, 2023, available at file:///Users/simonaruta/Desktop/Aurora%20stanescu%20MMR/communicable-disease-threats-report-week-45-2023.pdf, accessed November 22, 2023.
- Ministry of Health, Romania. Order 3494/2023 for the approval of the Action Plan for the elimination of measles, rubella and prevention of congenital rubella infection/congenital rubella syndrome, Romanian, available at https://www.lege-online.ro/lr-PLAN-din%20-2022-(261696)-(9).html.
Figure 1.
Vaccination coverage with the first and the second dose of MMR vaccine in Romania, 2005-2022.
Figure 1.
Vaccination coverage with the first and the second dose of MMR vaccine in Romania, 2005-2022.
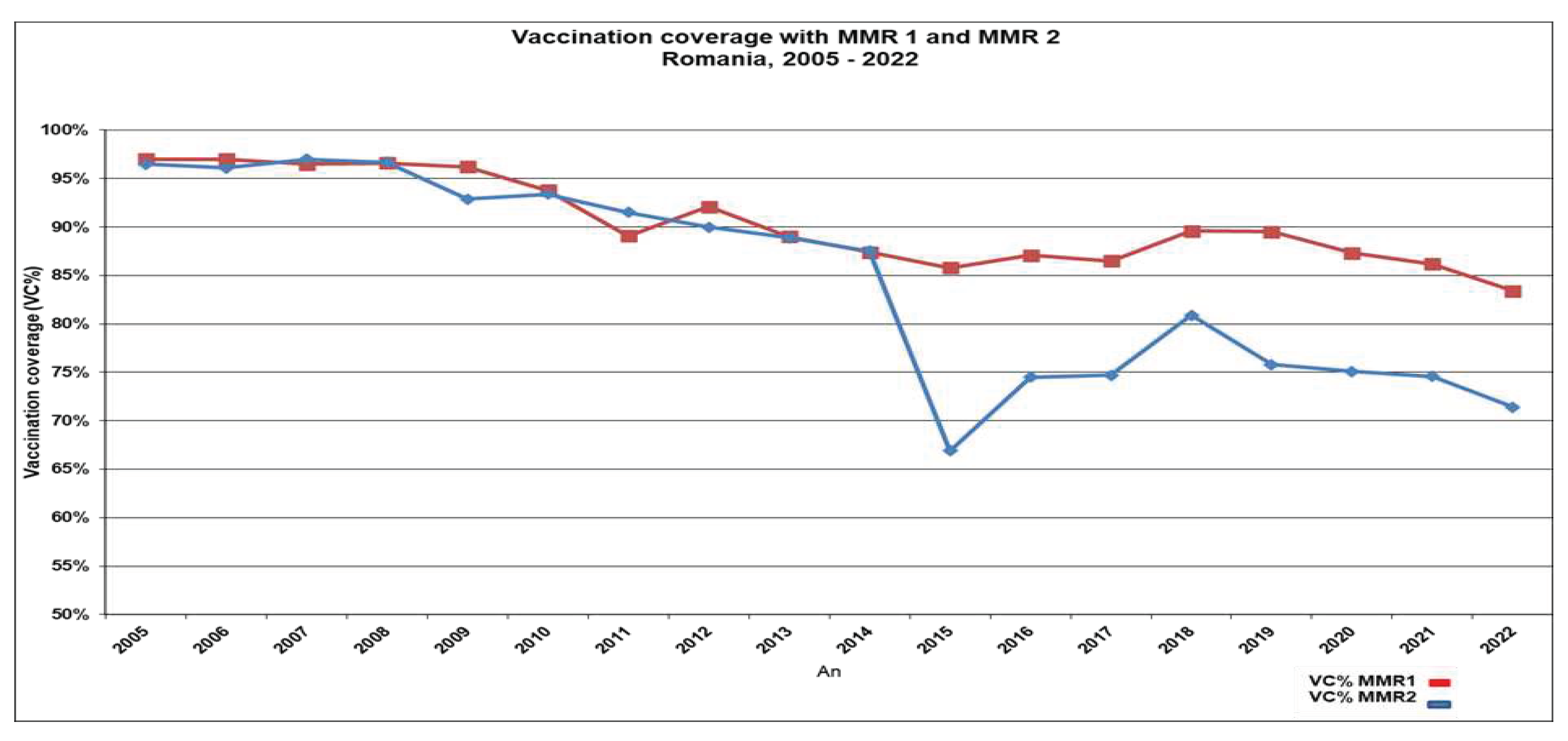
Figure 2.
Age distribution of measles case in Romania, January- October 2023.
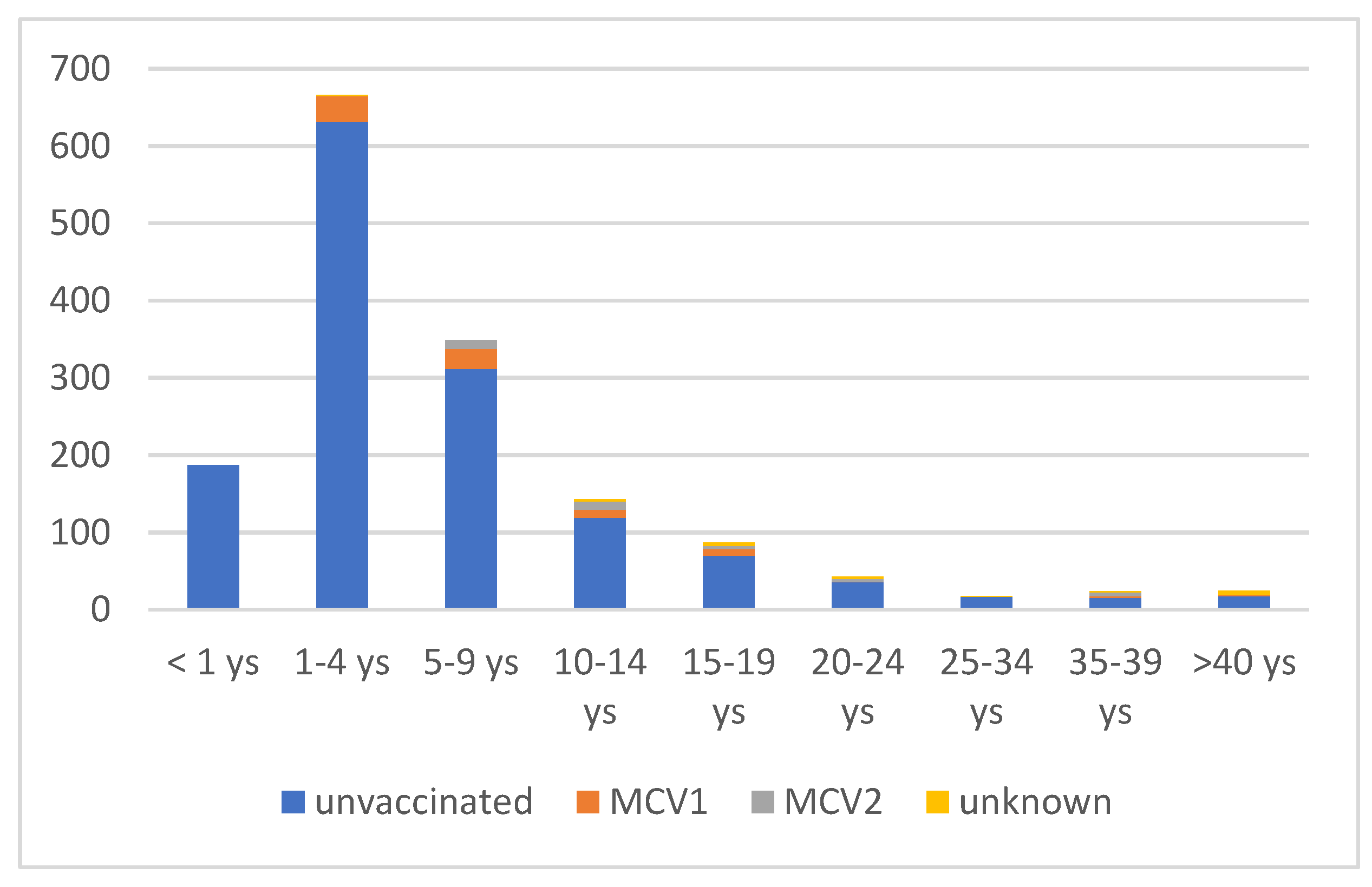
Figure 3.
Evolution of the MCV1 vaccine coverage rates (reported at 12 months and 18 months) in the most affected counties during the 2023 measles outbreak, compared to the national average.
Figure 3.
Evolution of the MCV1 vaccine coverage rates (reported at 12 months and 18 months) in the most affected counties during the 2023 measles outbreak, compared to the national average.
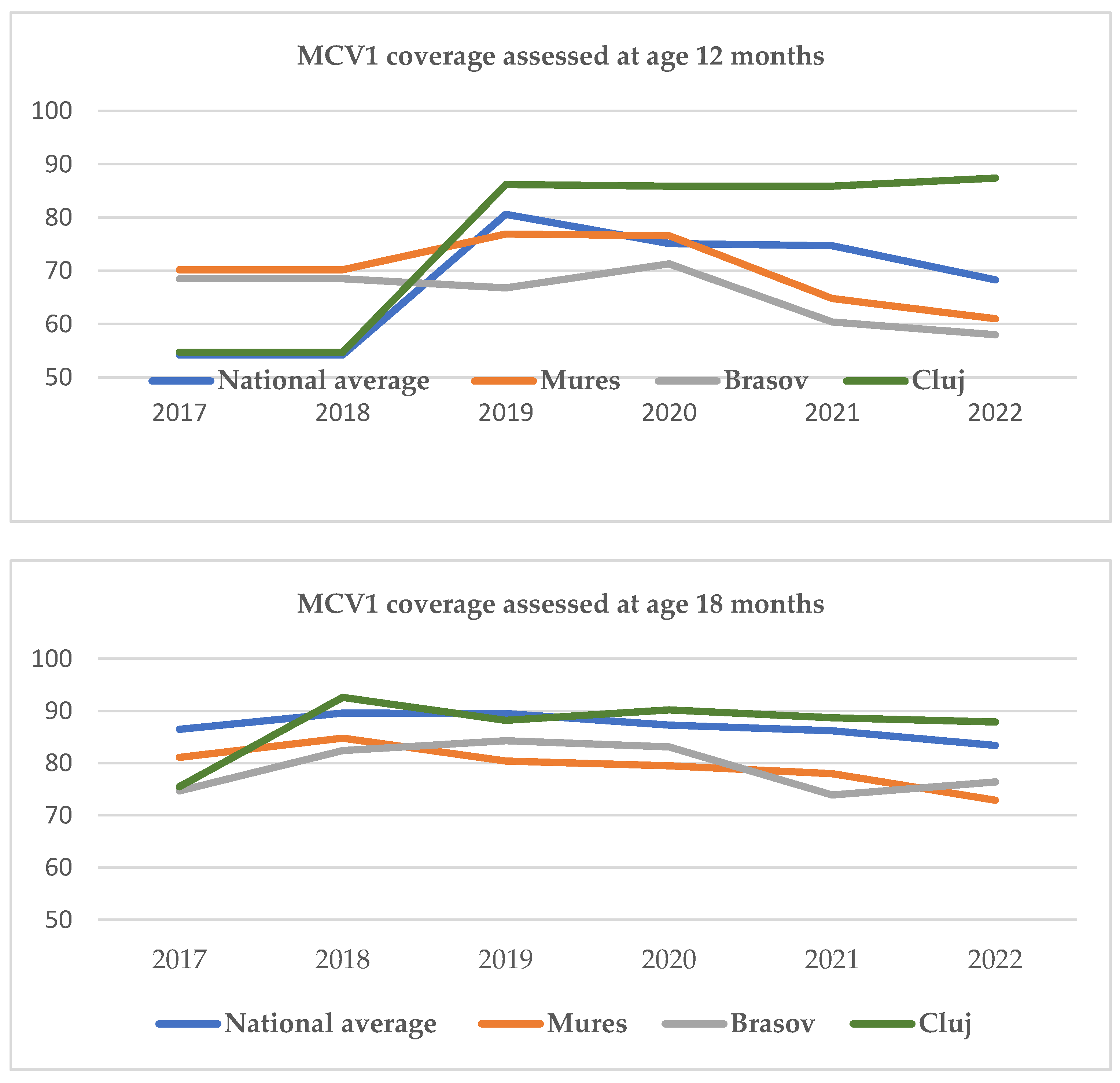

Table 1.
Distribution of low and high vaccination coverage rates assessed for children at 12 months of age and 18 months of age in the 42 counties of Romania.
Table 1.
Distribution of low and high vaccination coverage rates assessed for children at 12 months of age and 18 months of age in the 42 counties of Romania.
| Counties with VCR < 75% n, (%) |
Counties with VCR >90 % n, (%) |
Counties with VCR >95 % n, (%) |
||||
|---|---|---|---|---|---|---|
| Age | 12 mo | 18 mo | 12 mo | 18 mo | 12 mo | 18 mo |
| 2019 | 8 (19%) | 1 (2.3%) | 7 (16.6%) | 24 (57.1%) | 2 (52.3%) | 3(7.1%) |
| 2020 | 13 (30%) | 1 (2.3%) | 4 (9.5%) | 22 (52.3%) | 0 | 7(16.6%) |
| 2021 | 16 (38%) | 2 (4.6%) | 3 (7,1%) | 15 (35.7%) | 0 | 3 (7.1%) |
| 2022 | 31(73%) | 9 (21,4%) | 3 (7.1%) | 9 (21.4%) | 0 | 4 (9.5%) |
Table 2.
Measles vaccine coverage rates for the 3 most affected counties during the 2023 measles outbreak in Romania.
Table 2.
Measles vaccine coverage rates for the 3 most affected counties during the 2023 measles outbreak in Romania.
| County | MCV1 (%) 2022 | Number of eligible children aged 12 mo |
MCV2 (%) 2022 | Number of eligible children aged 5 ys |
|---|---|---|---|---|
| National average | 83.4 | 71.4 | ||
| Mures | 72.9 | 4 665 | 68.7 | 6223 |
| Brasov | 76.4 | 5 175 | 59.4 | 6736 |
| Cluj | 87.9 | 6 399 | 73.4 | 7524 |
MCV1- measles containing vaccine, first dose-administered at age 12 months (birth cohort 2021) ; MCV2 measles containing vaccine, second dose administered at age 5 years, (birth cohort 2017).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



