Submitted:
22 January 2024
Posted:
23 January 2024
Read the latest preprint version here
Abstract
The study aimed to manage and to analyse the results of the laboratory methods, using liver samples, preparing and analizing in pathology service. This mentioned, are known as routinally practice for hepatitis C diagnosis, which conduct to hepatic cirrhosis. In this study direction, chronic liver diseases stimulate a degree of hepatocyte injury. So previously mentioned modifications, alters thet affect the liver architecture and finally ends in cirrhosis are well analyse on microscopic preparates.
Keywords:
liver
; hepatitis C
; hepatic cirrhosis
; laboratory methods
; diagnosis
Introduction
Nowadays, HCV infection could be consider as one of bad results after percutaneous blood administration to ill patients. Also good to mention that HCV infection it is known as one of the most commonly through injection drug use [1]. The first and most important step in the care cascade is testing for HCV. Actually, is an enlarge number of expansion of populations eligible for testing for HCV prevention [1,2,3].
It is know about care cascade, including multiple key points in diagnosis HCV infection. An HCV care cascade is consider as a model for identifying opportunities and barriers in order to improve laboratory tests, linkage to care, and proper treatment access [4,5].
Relativelly recently, there have been increases in HCV detection among women of childbearing age [6,7]. Reinfection with HCV after curative therapy in illness status in different patients, is an important key point for medical team [8,9,10]. The proper laboratory techniques include immunoglobulin (Ig) G antibody enzyme immunoassays (anti-HCV) and nucleic acid tests (NAT), as modern methods, in conection with blood tests [11]. In case that need to distinguish between two directions such as true or false positivity of the anti-HCV antibody result, previously mentined tests, may be done with a second FDA-approved HCV antibody assay that is different from previously used for testing [11,12]. Morphologically, HCV is an enveloped, positive-sense, single-stranded RNA virus of the Flavivirdae family [13,14,15]. The great key point knowing as a start of the direct-acting antiviral (DAA) era was in 2011. The important role in this direction was the introduction of two NS3/4A protease inhibitors. Both previously mentioned were used in combination with interferon-based regimens for chronic HCV treatment to ill patients diagnosed [16]. Results of studies show that the HCV replication process is error prone. Finally results practically could be observe in variant viruses knowing as quasispecies [17,18]. Nowadays there are 7 genotypes of HCV. So there are known 6 major genotypes and the recent addition of genotype 7. This last 7 genotip has been found only in a few cases diagnosed to HCV positive patients [19]. Hepatitis C virus (HCV) infection is a great cause of various liver diseases as cirrhosis and hepatocellular carcinoma. Following promising news, significant scientific discovering things remain in attention for reducing morbidity and mortality, associated to HCV [20,21]. Understanding the properties of hepatitis C virus (HCV) viral RNA and proteins facilitates the development of diagnosis methods and also a proper treatment, including antivirals [22,23,24]. In addition we can mention that HCV genotyping assays approved for in vitro diagnostic use are commercially available [25,26]. Cirrhosis, as a nowadays disease, is characterized by fibrosis and nodule formation of the liver. In the secondary plan, it is known as a chronic injury, which leads to alteration of the normal lobular organization of the liver. A complex of factors, such as life style, or environmentals, can injure the liver, and beside also including viral infections, toxins, hereditary. With each injury, the liver suffer alterations as fibrosis. Finally but after a long-standing injury, liver functionalteration, develop in time cirrhosis as a complex diseases. Ethiology of the chronic liver diseases usually progress unfortunately in cirrhosis, following pathological mechanisms [27].
Material and Methods
In order to assist medical staff in understanding the concerns outlined, a series of digital images have been prepared. The operative pieces are intended to bring in the pathological anatomy service for macroscopic examination for diagnostic purposes. This are examined by performing the optical microscopic analysis.
Normal liver structure, using an optical microscope analyse and a special staining namely Masson. We can observe hepatocytes and interlobular spaces and septa [Figure 1].
A similar observation on a normal liver structure but using another specific staing known as Argentic impregnation Gomori. Also is possible to observe the Kiernan space with portal vein in section and with hepatic arter in section tpgether with biliar canaliculum insection [Figure 2].
In liver cirrhosis, on samples could be observe tissue fibrosis and alterations in the normal liver architecture in abnormal structural nodules [Figure 3].
A similar coming image with specific structural changes in liver structure and with vascularized fibrotic septa in cirrhosis More than, we can mention in this disease, about portal hypertension [Figure 4].
Conclusions
Research studies predict about not so a good prognosis of patients diagnosed with cirrhosis, knowing laboratory results and clinical points. Comorbidities are bad for a good prognostic to ill person diagnosed with cirrhosis. So a proper medical abordation could be a little to hard to establish after the rules from personalized medicine. The future trends are in attention for the coming time, knowing possible unclearities in cirrhosis management.
References
- AASLD-IDSA. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C 2016. Guidance produced by the American Association for the Study of Liver Disease and the Infectious Disease Society of America (AASLD-IDSA) covering recommendations for hepatitis C testing, clinical management and treatment. Available online: http://hcvguidelines.org/sites/default/files/HCV-Guidance_October_2016_a.pdf.
- Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. Centers for Disease Control and Prevention. MMWR Recomm Rep. 1998;47(Rr-19):1–39. Recommendations from the Centers for the Disease Control and Prevention definng populations for risk-based testing of hepatitis C.
- Moyer VA. Screening for hepatitis C virus infection in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2013;159(5):349–57. Hepatitis C testing recommendations for adults from the United States Preventive Services Task Force including risk-based testing and testing for adults born from 1945–1965. [CrossRef]
- Holmberg SD, Spradling PR, Moorman AC, Denniston MM. Hepatitis C in the United States. N Engl J Med. 2013;368(20):1859–61. Description of a care cascade integrating data from the Chronic Hepatitis Cohort Study and the National Health and Nutrition Examination Survey. [CrossRef]
- Viner K, Kuncio D, Newbern EC, Johnson CC. The continuum of hepatitis C testing and care. Hepatology. 2015;61(3):783–9. Description of an HCV continuum of care in a US urban center highlighting important areas where patients become lost at each stage.
- Koneru A, Nelson N, Hariri S, Canary L, Sanders KJ, Maxwell JF, et al. Increased Hepatitis C Virus (HCV) Detection in Women of Childbearing Age and Potential Risk for Vertical Transmission - United States and Kentucky, 2011–2014. MMWR Morb Mortal Wkly Rep. 2016;65(28):705–10. Analysis finding that the proportion of infants born to HCV-infected mothers increased 68% nationally and 124% in Kentucky.
- Kuncio DE, Newbern EC, Johnson CC, Viner KM. Failure to Test and Identify Perinatally Infected Children Born to Hepatitis C Virus-Infected Women. Clin Infect Dis. 2016;62(8):980–5. Analysis of surveillance data from the Philadelphia Department of Public Health finding a significiant number of women giving birth in Philadelphia tested positive for HCV but that most of their children were not tested for HCV. [CrossRef]
- Lambers FA, Prins M, Thomas X, Molenkamp R, Kwa D, Brinkman K, et al. Alarming incidence of hepatitis C virus re-infection after treatment of sexually acquired acute hepatitis C virus infection in HIV-infected MSM. AIDS. 2011;25(17):F21–7. [CrossRef]
- Martin TC, Martin NK, Hickman M, Vickerman P, Page EE, Everett R, et al. Hepatitis C virus reinfection incidence and treatment outcome among HIV-positive MSM. AIDS (London, England) 2013;27(16):2551–7. [CrossRef]
- Ingiliz P, Martin TC, Rodger A, Stellbrink HJ, Mauss S, Boesecke C, et al. HCV reinfection incidence and spontaneous clearance rates in HIV-positive men who have sex with men in Western Europe. J Hepatol. 2016. [CrossRef]
- Testing for HCV infection: an update of guidance for clinicians and laboratorians. MMWR Morb Mortal Wkly Rep. 2013;62(18):362–5. Updated guidance for clinicians and laboratorians from the Centers for Disease Control and Prevention on diagnostic testing procedures for hepatitis C.
- Moyer VA. Screening for hepatitis C virus infection in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2013;159(5):349–57. Hepatitis C testing recommendations for adults from the United States Preventive Services Task Force including risk-based testing and testing for adults born from 1945–1965. 1945. [CrossRef]
- Thomas DL, Seeff LB. Natural history of hepatitis C. Clin Liver Dis. 2005;9(3):383–98. vi. [CrossRef]
- Mack CL, Gonzalez-Peralta RP, Gupta N, Leung D, Narkewicz MR, Roberts EA, et al. NASPGHAN practice guidelines: Diagnosis and management of hepatitis C infection in infants, children, and adolescents. J Pediatr Gastroenterol Nutr. 2012;54(6):838–55. [CrossRef]
- Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage-specific fibrosis progression rates in chronic hepatitis C virus infection: a meta-analysis and meta-regression. Hepatology. 2008;48(2):418–31.
- Conteduca V, Sansonno D, Russi S, Pavone F, Dammacco F. Therapy of chronic hepatitis C virus infection in the era of direct-acting and host-targeting antiviral agents. J Infect. 2014;68(1):1–20. [CrossRef]
- Gomez J, Martell M, Quer J, Cabot B, Esteban JI. Hepatitis C viral quasispecies. J Viral Hepat. 1999;6(1):3–16. [CrossRef]
- Duffy S, Shackelton LA, Holmes EC. Rates of evolutionary change in viruses: patterns and determinants. Nat Rev Genet. 2008;9(4):267–76. [CrossRef]
- Bukh J. The history of hepatitis C virus (HCV): Basic research reveals unique features in phylogeny, evolution and the viral life cycle with new perspectives for epidemic control. J Hepatol. 2016;65(1 Suppl):S2–s21. [CrossRef]
- Ly KN, Hughes EM, Jiles RB, Holmberg SD. Rising Mortality Associated With Hepatitis C Virus in the United States, 2003–2013. Clin Infect Dis. 2016;62(10):1287–8. Describes rising HCV-associated mortality in the United States from 2003–2013. During that time period, HCV-associated deaths surpassed 60 other nationally natofiable infectious conditions combined. [CrossRef]
- Allison RD, Tong X, Moorman AC, Ly KN, Rupp L, Xu F, et al. Increased incidence of cancer and cancer-related mortality among persons with chronic hepatitis C infection, 2006–2010. J Hepatol. 2015;63(4):822–8. Analysis of a cohort of HCV-infected persons that found the the incidence of liver cancer and many types of non-liver cancers were higher, and age at diagnosis and death younger, in patients with chronic HCV infection compared to the general population. [CrossRef]
- Alberti A, Chemello L, Benvegnù L. Natural history of hepatitis C. J Hepatol. 1999;31 Suppl 1:17–24. [CrossRef]
- Hoofnagle JH. Course and outcome of hepatitis C. Hepatology. 2002;36:S21–S29.
- Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med Sci. 2006;3:47–52. [CrossRef]
- Chevaliez S, Pawlotsky JM. Virology of hepatitis C virus infection. Best Pract Res Clin Gastroenterol. 2012;26:381–389. [CrossRef]
- Saludes V, González V, Planas R, Matas L, Ausina V, Martró E. Tools for the diagnosis of hepatitis C virus infection and hepatic fibrosis staging. World J Gastroenterol. 2014;20:3431–3442. [CrossRef]
- Naveau S, Perlemuter G, Balian A. [Epidemiology and natural history of cirrhosis]. Rev Prat. 2005 Sep 30;55(14):1527-32.
Figure 1.
Normal Liver x10 Masson staining.
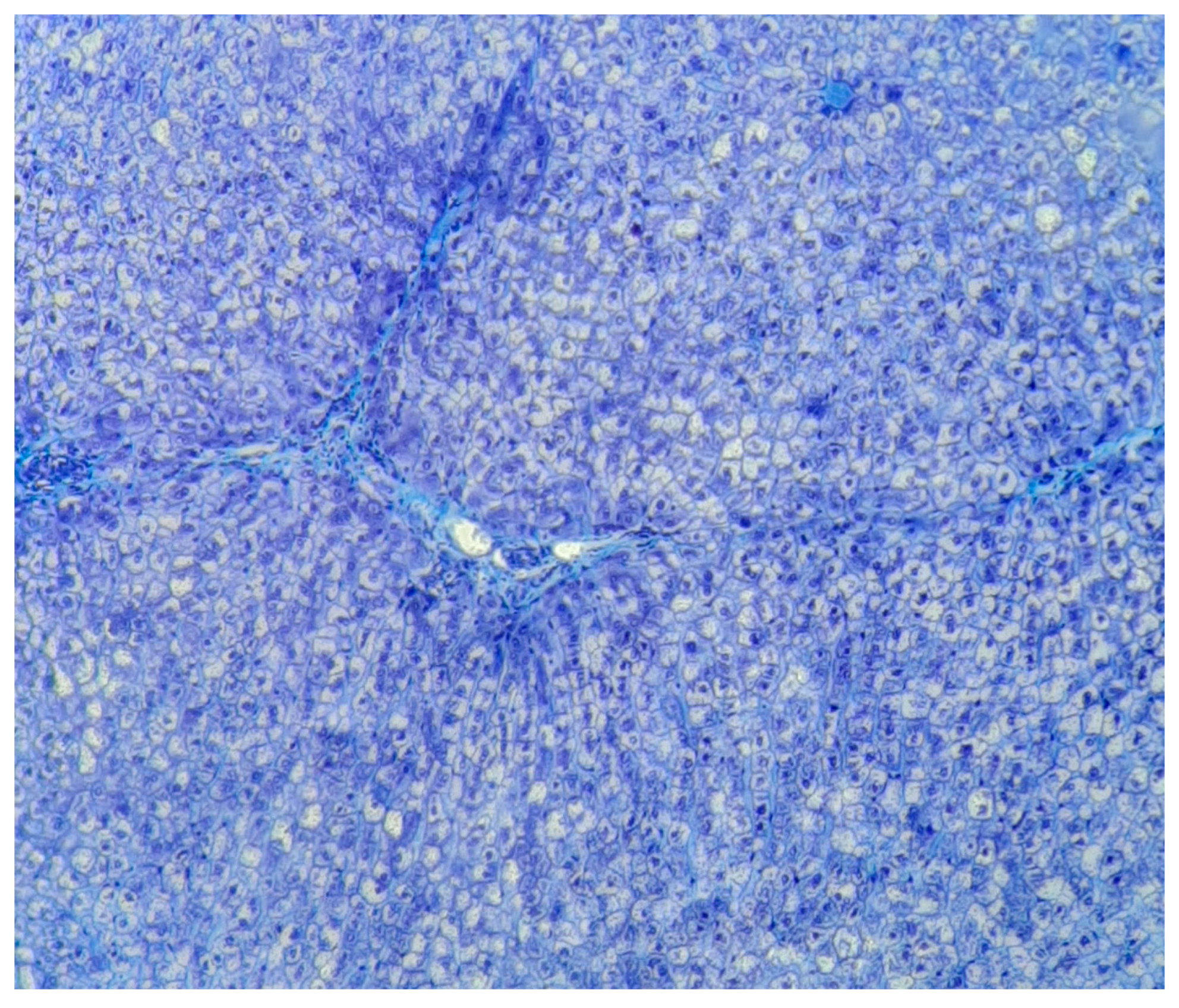
Figure 2.
Normal Liver x10. Argentic impregnation.
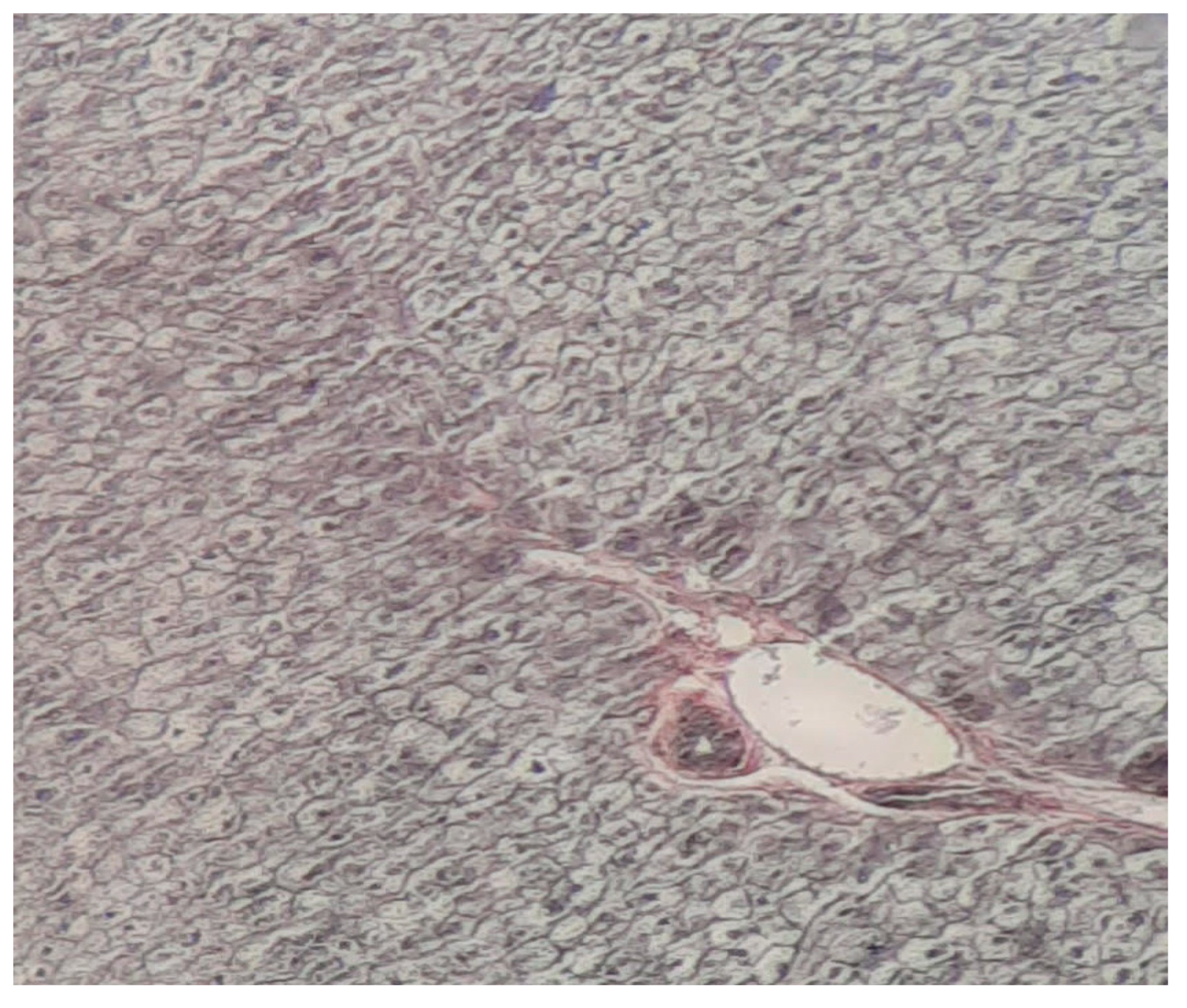
Figure 3.
Cirrhosis liver x10 HE.
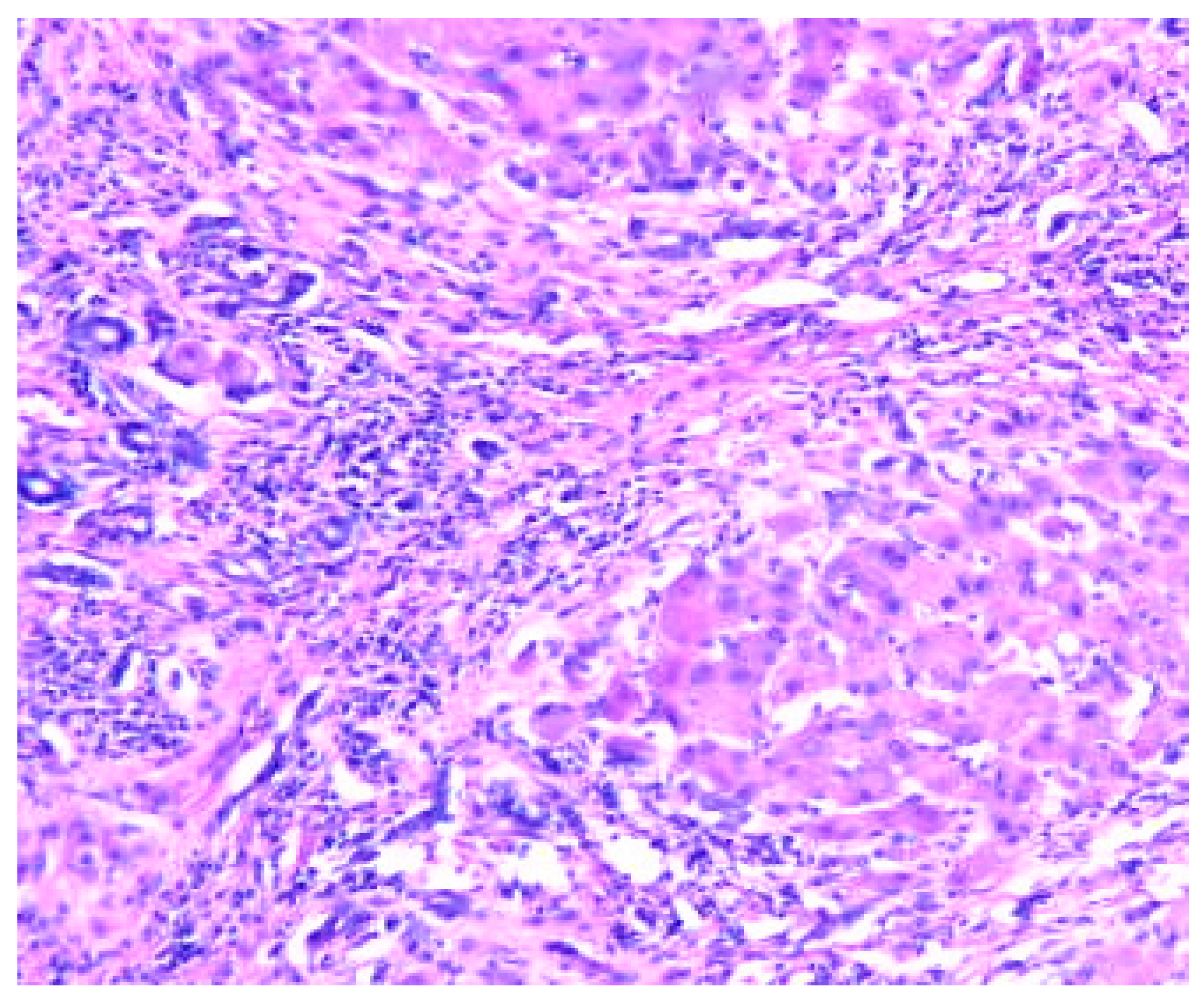
Figure 4.
Cirrhosis liver x10 HE.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



