
Submitted:
12 December 2023
Posted:
13 December 2023
You are already at the latest version
Abstract
Breast Angiosarcoma is a rare malignancy, accounting less than 1% of all soft tissue. It comprises primitive and secondary subtypes, such as radiogenic breast angiosarcoma (RAS).
Despite the multimodal treatment, angiosarcomas represent an incurable disease for many patients and represent a cause of substantial deterioration of their quality of life. Surgery represents the cornerstone in the management, but high recurrence rates are reported. Electrochemotherapy (ECT) is practicable locoregional treatment in patients with advanced angiosarcoma, in a multimodal therapeutic strategy. ECT palliative benefit includes optimal patient compliance, good local hemostasis control, and local responses. Considering that only 22 cases are described in literature, we reported a rare case of RAS treated with ECT, after a multidisciplinary approach including Next Generation Sequencing (NGS). A literature review about the feasibility of ECT in RAS management was also performed.
Keywords:
breast angiosarcoma
; post-irradiation angiosarcoma
; elettrochemotherapy
Introduction
Breast angiosarcoma is a rare malignancy, accounting for less than 1% of all soft tissue sarcomas [1]. It originates from the aberrant proliferation of endothelial cells in a small blood or lymphatic vessels. Nuclear atypia, frequent mitosis, hyperchromatic nuclei, and large nucleoli are the most known microscopic features [2].
Primitive angiosarcoma (PAS) comprises only 0.04% of all breast malignancies [3] and arises as an intraparenchymal enlarging mass. It affects younger women, and the diagnosis is often delayed due to its rarity and gland density [4]. Secondary angiosarcoma usually interests older women and compromises the cutaneous layers. It is associated with lymphoedema conditions such as Stewart and Treves Syndrome which is a complication of post demolitive breast surgery. Although, the spreading of breast conservative surgery was not able to reduce the breast angiosarcoma risk because post-irradiation subtypes are correlated to adjuvant radiotherapy (RT) [5].
Primitive and radiogenic angiosarcomas (RAS) are morphologically undistinguishable while pathogenetic differences are evident. For example, the C-MYC amplification was strongly associated with post-irradiation and not with primitive subtypes, suggesting a specific oncogenic pathway and a potential targeted therapy [6].
The extreme rarity of this condition limits the possibility of clinical trials able to assess the most adequate treatment strategy, therefore decisions are based on retrospective case reviews [7]. Moreover, surgery is the cornerstone for the treatment of breast angiosarcomas, and the most important prognostic factor is the status margins. [8]. Radiotherapy (RT) and adjuvant chemotherapy (CT) have an unclear role and guidelines are not available. In the 2000s, electrochemotherapy (ECT) was proposed as a potential treatment for superficial malignant lesions. Particularly, the first evaluation of its potential therapeutic role in angiosarcoma management was conducted in 2001, in veterinary medicine, reaching better results than the cisplatin treatment alone [9]. ECT is gaining recognition as an effective local therapy based on systemic or local injection of bleomycin or cisplatin, combined with electroporation.
This technique is based on the administration of electric pulses able to permeabilize cells in the tissue exposed. The cellular pores are enabled to increase the uptake of hydrophilic chemotherapeutics that have hampered transport through the cell membrane [10].
This procedure has got many advantaged, such as the drug concentration into the neoplastic cells and the reduction of general cytotoxic effects [11]. Moreover, the use of electrochemotherapy is spread and many studies have evaluated the effectiveness for angiosarcoma management [12].
Despite the multimodal treatment, angiosarcomas represent an incurable disease for many patients and represent a cause of substantial deterioration of their quality of life.
Also, genomic molecular characterizations such as NGS (next generation sequencing) that are often performed to investigate the aggressiveness of the tumors and potential experimental therapeutic choices, may be performed to evaluate the therapeutic responsiveness of the traditional treatments and the possible use of ECT.
We present a case of a 57-year-old woman affected by post-irradiation breast angiosarcoma treated with ECT and a literature review of the impact of ECT on angiosarcoma therapies.
Case Presentation
Previous an informed written consensus, we present the case of a 57-year-old woman with a history of atrial fibrillation and a breast invasive ductal carcinoma in 2014, treated with breast conservative surgery, RT, ed hormonal therapy (OT) with Femara. It was an early breast cancer (pT1c N0 M0) with expressed estrogen- and progesterone-receptors (ER=90% and PgR=30%), moderate proliferation index (Ki-67=30%) and not amplified c-ERB-2 gene. So, the patient underwent quadrantectomy and axillary lymph nodes sampling, followed by standard RT protocols (60 Gy in 30 fractions). Five years later, the woman noticed an exophytic lump on the skin region corresponding to the lower lateral quadrant in the right breast (Figure 1). At first, she considered it a pimple but, six months later, she was alarmed by the increase. So, she underwent a dermatological examination. The lesion reached 20 mm in diameter and was not painful, but erythema and orange peel skin were identified. Moreover, during the medical visit, it started to bleed, and a breast SBA was suspected (Figure 1). The patient was referred to our General Surgery Unit at Campania University "Vanvitelli" in Naples (Italy). We advised her to perform bilateral mammography and breast ultrasound (US), but the patient cannot tolerate the right breast compression. So, only breast US was realized, showing a 22-millimeters exophytic lesion, with a hypoechoic pattern, irregular margins, and rich peri- and intra-tumoral vascularization. The patient was a candidate for a surgical biopsy that confirmed the suspect of breast angiosarcoma intermediate grade sec French Federation of Cancer Centers (FNCLCC) [13]. The "Vanvitelli" Oncological Multidisciplinary Group (OMG) candidate the patient for radical right mastectomy and instrumental follow-up. Also, genomic molecular characterization was ordered by NGS (next generation sequencing) on tumor sample in order to investigate potential experimental therapeutic choices. No targetable alterations were detected, however tumor harbors mutations in NF1 gene and MYC amplification, thus highlighting the biological aggressiveness of the disease. Also, tumor is MSS (microsatellite-stable) and depicts low TMB (tumor mutational burden), confirming the negative profile in terms of immune-responsiveness. Although, 18 months later, new skin purple lesions appeared in the anterior right thoracic region and an 18-fludeoxyglucose-Positrone Emission Tomography (18-FDG-PET) was performed, showing pectorals muscle involvement (Figure 2). Moreover, the patient received 14 Paclitaxel cycles (Doxorubicin was contraindicated for atrial fibrillation comorbidity) and re-irradiation (40.5 Gy for 15 cycles). Despite the treatments, a new lesion spread on thoracic and abdominal skin regions and a right neoplastic pulmonary effusion was diagnosed. So, OMG candidate the women for thoracentesis, ECT, and Gemcitabine treatment. Unfortunately, the patient did not tolerate the latter therapy for the development of a severe skin rash while underwent to three ECT sessions. She received Bleomycin at the standard regimen of 15.000 UI, with intravenous injection, during deep sedation. After accurate skin disinfection, the electrodes were applicated. The procedures lasted about 40 minutes and no complications were noticed. Bleeding lesions underwent an accurate hemostatic control. ECT cycles were performed monthly in day surgery hospitalization (Figure 3). The patient developed a severe neoplastic pulmonary effusion and ECT has been stopped for lung contraindication. So, local lesions improved with frequent bleeding and infections. Unfortunately, the patient died 24 months after the diagnosis of RAS due a respiratory failure.
Literature Review
In a systematic review literature search of the database PubMed (search date 10-02-2023) using the search terms "angiosarcoma and electrochemotherapy" we identified only 14 citations [14,15,16,17,18,19,20,21,22,23,24,25,26,27]. Seven studies were excluded because two of them were were commentary [15,16], one referred to animal population [9], another was about melanoma or not melanoma diseases [21], two were about the Stewart-Treves Syndrome [23,24,25,26,27] and one was not about RAS [26]. So, only seven studies reported cases of RAS treated also with ECT. Twenty-two cases were reported in the literature.
The clinical studies describing patients with RAS of the breast treated also with ECT are reported in Table 1. The most affected age is between 61 and 77 years, with a period latency from the irradiation of 48-108 months. Only six studies reported the histology of the previous breast cancer, and luminal subtypes are prevalent (6/6 cases reported). All the patients received a conservative surgical approach (quadrantectomy), except a patient undergone mastectomy [14]. Only two women received adjuvant CT [14,15,16,17,18,19,20,21,22,23,24,25,26]. All the patients (6/6) were treated with hormonal therapy and adjuvant RT. Only in one case, 25 Gy were administered [14], while the other patients received 60 Gy in total 30 fractions.
The most frequent clinical sign of RAS was a red-purple nodular near the surgical scar or on the same breast. In 22/23 cases, the patients underwent to surgery while only 8/23 received a new CT, with doxorubicin as the first choice in almost 3 cases. Docetaxel, paclitaxel, and gemcitabine were considered when doxorubicin was contraindicated. Only 12/22 underwent a re-irradiation.
Twenty-two patients received ECT for 1-8 cycles (mean 1.35 cycles per patient). Bleomycin 15.000 UI is the most favorite treatment and common adverse reactions were pain, edema, ulceration, and necrosis. Complete and partial responses (CR and PR) were reported for 7/22 and 8/22 patients, respectively. Overall survival (OS) was 3-29.9 months (mean value: 4.1 months) while free progression survival (FPS) was 1-24 months (mean value: 3.6 months).
Discussion
Breast cancer is the most prevalent cancer in women, and its incidence continues to rise annually. Current treatment modalities include surgical resection, chemotherapy (CT), radiotherapy (RT), and hormone therapy. Approximately one-third of lesions are estimated to be non-palpable cancers, leading to an increasing preference for conservative surgery followed by RT [28,29,30].
Electrochemotherapy (ECT), which exposes tumor cells to electric pulses through a process known as electroporation, in combination with cytostatic drugs, appears to be a safer and more effective treatment for breast cancer in both in vitro and in vivo settings. Indeed, this approach has found applications in the treatment of breast cancer and its metastases. Furthermore, palliative effects have been established, with noted reductions in pain for patients. Its utilization has also been extended to lesions related to radiogenic angiosarcomas (RAS).
It behaves aggressively and carries a poor prognosis, with a 5-year overall survival rate of 27–48%. Due to its scarcity, most of the information regarding the diagnosis and management of this condition is from case reports and retrospective series analyses with relatively small patient numbers. RAS is even less common [35].
ECT is also now recognized as a loco-regional therapy for disseminated cutaneous and subcutaneous tumor lesions, improving the patient’s quality of life. The safety and efficacy of ECT for primary basal cell carcinoma and primary squamous cell carcinoma, which are the most common types of skin cancer, is well known.
Surgery represents the main treatment for RAS as a diagnostic and therapeutic procedure. Although, it is particularly challenging for advanced and multifocal types and is often associated with recurrences. A delayed diagnosis is an important concern. Initial skin changes in radiogenic angiosarcoma are subtle, therefore, these alterations may be confused with other benign skin conditions such as telangiectasia. In these situations, CT e re-irradiations are also performed, even if the drug regimen is empirical and no standard regimen is approved for RAS. However, doxorubicin and taxanes are considered the most common option in patient with metastatic angiosarcomas and the overall response rate has been estimated at 30%. Unfortunately, it has been verified that complete responses are about 6%, partial responses 29.5%, and stable responses 13% [31,32]. In a recent review, Depla et al. evaluate the effect of treatment modalities surgery, RT, and CT on RAS patients. They focused on a high recurrence rate after surgery (65%, of which 91% were local). Better results were obtained when surgery was combined with RT (51%, of which 68% were local) while no improvement was identified in the group treated with surgery and CT [33]. Despite the multimodal treatment, angiosarcomas represent an incurable disease for many patients and represent a cause of substantial deterioration of their quality of life. So, the introduction of the most recent technologies is strongly encouraged.
ECT has demonstrated clinical utility in the management of superficial cancer, and it has been associated with better tumor control and patients’ outcomes [34,36,37,38]. One of the larger studies about ECT in angiosarcoma treatment was performed by Campana et al. Twenty patients received 24 ECT courses, at the standard regimen of Bleomycin 15.000 UI and 51 lesions were treated. The mean duration of the procedures was 28 minutes and 15% of the patients were candidate to other systemic therapies. Considering per-tumoral local response they obtained the following results: CR=61%, PR=22%, and disease stabilization (SD)=18%. Per-patient response were CR=40%, PR=40% and SD=15%. Unfortunately, 35% of the patients experienced local recurrence after a median period of 3.4 months. The main adverse reactions reported were a pain for 30% of the patients and skin toxicity with ulceration (25%) [12] (Table 1).
Our clinical case was characterized by a partial response to ECT courses, but skin toxicity was elevated. Unfortunately, the patient developed lung metastasis with respiratory failure, preventing further treatments and limiting ECT effectiveness. During lung center hospitalization, the patient reported an evident progression of local lesions, with difficult management of bleeding and infected areas.
Contrary to other skin cancers (such as Kaposi's sarcoma) and breast cancer, the clinical experience with ECT in angiosarcoma is limited yet and is accepted as a palliative strategy. However, some case reports are suggesting the feasibility of ECT. For example, Benevento et.al. reported the case of a 76-year-old woman treated with a multimodal approach (breast conservative surgery, RT, CT, and ECT), focusing on the complete local response in all the lesions and improving life quality [18].
Despite the multimodal therapeutic approach, angiosarcomas represent an incurable disease for many patients. Genomic molecular characterizations could be routinary performed to investigate the aggressiveness of the tumors and to predict the therapeutic responsiveness of the traditional treatments. More aggressive phenotype could be candidate to close follow up and to earlier ECT cycles.
Also, genomic molecular characterizations such as NGS (next generation sequencing) that are often performed to investigate the aggressiveness of the tumors and potential experimental therapeutic choices, may be performed to evaluate the therapeutic responsiveness of the traditional treatments and the possible use of ECT.
The reported experiences indicate that ECT is practicable locoregional treatment in patients with advanced angiosarcoma, in a multimodal therapeutic strategy. In the case reported by Cencelj-Arnez, ECT was performed in the breast reconstructed by autologous free-flap. Only four similar cases were reported in literature describing RAS after mastectomy, autologous breast reconstruction and adjuvant RT. The technique was feasible, safe and effective in treatment of the disease. Most of the treated lesions in several consecutive ECT sessions reached a complete response, but multiple recurrences occurred in non-treated areas [14]. ECT may represent one of the feasible options in the management of RAS. Patients undergone the skin-sparing mastectomy and immediate breast reconstruction, who receive RT, should be monitored by regular long-term follow up and the biopsy of any suspicious lesions is mandatory.
The use of ECT could be realized also in case of prosthetic reconstruction. Campana et al. reported the case of a 55-year-old woman with previous skin-sparing mastectomy and prosthetic reconstruction for multifocal ductal carcinoma who developed homolateral axillary recurrence. After the surgery the pathology report revealed a positive cutaneous margin. Since further breast skin excision or RT would have compromised the prosthetic implant, and the patient rejected further surgical or RT therapies, the multidisciplinary recommendation included ECT. The procedure lasted 20 minutes under mild general sedation and included a bolus of intravenous bleomycin followed by local application of electric pulses using a needle electrode. There were no postprocedural complications. At the 5-year-follow up, the patient is disease-free with the implant in situ. This report illustrates the role of ECT to sterilize resection margins and preserve a breast implant [37].
CT is becoming an increasingly challenging antitumor therapy to administer due to the numerous mechanisms of drug resistance. To address this issue, alternative techniques, such as ECT can be employed. This latter involves the simultaneous administration of electrical pulses (electroporation) and drug treatment to enhance the drug's effectiveness against the tumor. Promising results have been observed in in vitro studies, veterinary applications, and clinical oncology research, particularly in various cancers like metastatic melanoma.
All the reported cases described a local improvement and three studies reported complete responses. ECT is useful as palliative option too, because it is associated to optimal patient compliance, good local hemostasis control, and infection prevention. Other future studies are necessary to establish the optimal timing, the extension of treatment, and the most appropriate combination of surgery and systemic treatments. So, genomic molecular characterizations may play a role in RAS management.
Moreover, ECT has emerged as a promising palliative treatment, raising interest in exploring its combination with RT to enhance tumor response. However, the potential benefits and challenges of combining these treatments remain unclear, even if their combination consistently improved tumor response compared to that with individual therapies [37].
Conclusion
Although surgery represents the cornerstone in the management of RAS, high recurrence rates are reported. ECT is practicable locoregional treatment in patients with advanced angiosarcoma realizing a local improvement of the lesions or a palliative management of the complications. Other possible applications include skin lesions in patients undergone to reconstructive breast surgery. Further studies are necessary to establish the timing, the extension of treatment, and the possible role of genomic characterizations in RAS management and patients’ selection.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
References
- Shah S, Rosa M. Radiation-associated angiosarcoma of the breast. Clinical and pathologic features. Arch Pathol Lab Med. 2016 May;140((5)):477–81. [CrossRef]
- Seo IS, Min K-W. Postirradiation epithelioid angiosarcoma of the breast. A case report with immunohistochemical and electron microscopic study. Ultrastruct Pathol. 2003 Jun; 27((3)):197–203. [CrossRef]
- Desbiens C, Hogue JC, Lévesque Y. Primary breast angiosarcoma: avoiding a common trap. Case Rep Oncol Med. 2011; Jul 2011: 517047. [CrossRef]
- Arora TK, Terracina KP, Soong J, Idowu MO, Takabe K. Primary and secondary angiosarcoma of the breast. Gland Surg. 2014 Feb;3((1)):28-34. [CrossRef]
- Brenn T, Fletcher CD. Postradiation vascular proliferations: an increasing problem. Histopathology. 2006 Jan;48((1)):106-14. [CrossRef]
- Laé M, Lebel A, Hamel-Viard F, Asselain B, Trassard M, Sastre X, Kirova YM. Can c-myc amplification reliably discriminate post-radiation from primary angiosarcoma of the breast? Cancer Radiother. 2015 May;19((3)):168–74. [CrossRef]
- Singh R, Chufal KS, Pahuja AK, Suresh T, Chowdhary RL, Ahmad I. Primary angiosarcoma of the breast: a radiation oncologist's perspective with a concise review of the literature. BMJ Case Rep. 2019 Jul 18;12((7)):e227036. [CrossRef]
- Bousquet G, Confavreux C, Magné N, de Lara CT, Poortmans P, Senkus E, de Lafontan B, Bolla M, Largillier R, Lagneau E, Kadish S, Lemanski C, Ozsahin M, Belkacémi Y. Outcome and prognostic factors in breast sarcoma: a multicenter study from the rare cancer network. Radiother Oncol. 2007 Dec;85((3)):355-61. [CrossRef]
- Tozon N, Sersa G, Cemazar M. Electrochemotherapy: potentiation of local antitumor effectiveness of cisplatin in dogs and cats. Anticancer Res. 2001 Jul-Aug;21((4A)):2483-8.
- Gehl J, Sersa G, Matthiessen LW, Muir T, Soden D, Occhini A, Quaglino P, Curatolo P, Campana LG, Kunte C, Clover AJP, Bertino G, Farricha V, Odili J, Dahlstrom K, Benazzo M, Mir LM. Updated standard operating procedures for electrochemotherapy of cutaneous tumors and skin metastases. Acta Oncol. 2018 Jul;57((7)):874-82. [CrossRef]
- Cemazar M, Sersa G. Recent Advances in Electrochemotherapy. Bioelectricity. 2019 Dec 1;1((4)):204-213. [CrossRef]
- Campana LG, Kis E, Bottyán K, Orlando A, de Terlizzi F, Mitsala G, Careri R, Curatolo P, Snoj M, Sersa G, Valpione S, Quaglino P, Mowatt D, Brizio M, Schepler H. Electrochemotherapy for advanced cutaneous angiosarcoma: A European register-based cohort study from the International Network for Sharing Practices of electrochemotherapy (InspECT). Int J Surg. 2019 Dec;72:34-42. [CrossRef]
- Coindre JM, Trojani M, Contesso G, David M, Rouesse J, Bui NB, Bodaert A, De Mascarel I, De Mascarel A, Goussot JF. Reproducibility of a histopathologic grading system for adult soft tissue sarcoma. Cancer. 1986 Jul 15;58((2)):306-9. [CrossRef]
- Cencelj-Arnez R, Novak J, Klevisar Ivancic A, Bosnjak M, Cemazar M, Snoj M.Radiotherapy-associated angiosarcoma in the breast reconstructed by autologous Free-flap and treated with electrochemotherapy. Radiol Oncol. 2020 Dec 29;55((1)):77-81. [CrossRef]
- Zhou G, Mei Z. Electrochemotherapy for advanced cutaneous angiosarcoma: A european register-based cohort study from the international network for sharing practices of electrochemotherapy (InspECT)-An invited commentary. Int J Surg. 2019 Dec;72:232-3. [CrossRef]
- Alagkiozidis I. A Commentary on "Electrochemotherapy for advanced cutaneous angiosarcoma: A European register-based cohort study from the International Network for Sharing Practices of Electrochemotherapy (InspECT)" Int J Surg 2019 Dec;72:196-7. [CrossRef]
- Campana LG, Kis E, Bottyán K, Orlando A, de Terlizzi F, Mitsala G, Careri R, Curatolo P, Snoj M, Sersa G, Valpione S, Quaglino P, Mowatt D, Brizio M,Schepler H. Electrochemotherapy for advanced cutaneous angiosarcoma: A European register-based cohort study from the International Network for Sharing Practices of electrochemotherapy (InspECT). Int J Surg. 2019 Dec;72:34-42. [CrossRef]
- Benevento R, Carafa F, Di Nardo D, Pellino G, Letizia A, Taddeo M, Gambardella A, Canonico S, Santoriello A. Angiosarcoma of the breast: a new therapeutic approach? Int J Surg Case Rep. 2015;13:30-2. [CrossRef]
- Guida M, Ruggieri E, Fucci L, Ressa M, D'Aluisio L, Fanelli G, Strippoli S. Image Gallery: A case of cutaneous giant angiosarcoma treated successfully with electrochemotherapy. Br J Dermatol. 2017 Aug;177(2):e27. [CrossRef]
- Guida M, Campana LG, Curatolo P, Strippoli S, Bonadies A, Grilz G, Cabula C, Rotunno R, Bucher S, Solari N, Santoriello A, Valpione S, Rossi CR. Local treatment with electrochemotherapy of superficial angiosarcomas: Efficacy and safety results from a multi-institutional retrospective study. J Surg Oncol. 2016 Aug;114(2):246-53. [CrossRef]
- Borgognoni L, Pescitelli L, Gerlini G, Brandani P, Gelli R, Giannotti V, Bellucci F, Sestini S. Efficacy of Electrochemotherapy in the Treatment of Cutaneous Melanoma Metastases and Rare Non-melanoma Skin Cancer. Anticancer Res. 2020 Nov;40((11)):6485-6492. [CrossRef]
- Tozon N, Sersa G, Cemazar M. Electrochemotherapy: potentiation of local antitumour effectiveness of cisplatin in dogs and cats. Anticancer Res. 2001 Jul-Aug;21((4A)):2483-8.
- Campana LG, Valpione S, Tosi A, Rastrelli M, Rossi CR, Aliberti C. Angiosarcoma on Lymphedema (Stewart-Treves Syndrome): A 12-Year Follow-up after Isolated Limb Perfusion, Limb Infusion, and Electrochemotherapy. J Vasc Interv Radiol. 2016 Mar;27((3)):444-6.
- Solari N, Spagnolo F, Ponte E, Quaglia A, Lillini R, Battista M, Queirolo P, Cafiero F. Electrochemotherapy for the management of cutaneous and subcutaneous metastasis: a series of 39 patients treated with palliative intent. J Surg Oncol. 2014 Mar;109((3)):270-4. [CrossRef]
- Mocerino C, Iannaci G, Sapere P, Luise R, Canonico S, Gambardella A. Multidisciplinary approach to breast angiosarcoma in an elderly patient: Repeated local relapses and significant objective responses. Int J Immunopathol Pharmacol. 2016 Sep;29((3)):537-42. [CrossRef]
- Laurino S, Omer LC, Albano F, Marino G, Bianculli A, Solazzo AP, Sgambato A, Falco G, Russi S, Bochicchio AM. Radiation-induced sarcomas: A single referral cancer center experience and literature review. Front Oncol. 2022 Sep 30;12:986123. [CrossRef]
- di Meo N, Drabeni M, Gatti A, Trevisan G. A Stewart-Treves syndrome of the lower limb. Dermatol Online J. 2012 Jun 15;18((6)):14. [CrossRef]
- Parisi S, Ruggiero R, Gualtieri G, Volpe ML, Rinaldi S, Nesta G, Bogdanovich L, Lucido FS, Tolone S, Parmeggiani D, Gambardella C, Docimo L. Combined LOCalizer™ and Intraoperative Ultrasound Localization: First Experience in Localization of Non-palpable Breast Cancer. In Vivo. 2021 May-Jun;35((3)):1669-76. [CrossRef]
- Parisi S, Gambardella C, Conzo G, Ruggiero R, Tolone S, Lucido FS, Iovino F, Fisone F, Brusciano L, Parmeggiani D, Docimo L. Advanced Localization Technique for Non-Palpable Breast Cancer: Radiofrequency alone VS Combined Technique with Ultrasound. J Clin Med. 2023 Aug 2;12((15)):5076. [CrossRef]
- Parisi S., Gambardella C., Ruggiero R., Tolone S., Lucido F.S., Docimo L. Radiofrequency Identification—RFID using LOCalizer-Tag in Non-palpable Breast Lump. Indian J. Surg. 2022. [CrossRef]
- Dogan A, Kern P, Schultheis B, Häusler G, Rezniczek GA, Tempfer CB. Radiogenic angiosarcoma of the breast: case report and systematic review of the literature. BMC Cancer. 2018 Apr 24;18((1)):463. [CrossRef]
- D'Angelo SP, Munhoz RR, Kuk D, Landa J, Hartley EW, Bonafede M, Dickson MA, Gounder M, Keohan ML, Crago AM, Antonescu CR, Tap WD. Outcomes of systemic therapy for patients with metastatic angiosarcoma. Oncology. 2015;89:205–14. [CrossRef]
- Depla AL, Scharloo-Karels CH, de Jong MAA, Oldenborg S, Kolff MW, Oei SB, van Coevorden F, van Rhoon GC, Baartman EA, Scholten RJ, Crezee J, van Tienhoven G. Treatment and prognostic factors of radiation-associated angiosarcoma (RAAS) after primary breast cancer: a systematic review. Eur J Cancer. 2014 Jul;50((10)):1779-88. [CrossRef]
- Bertino G, Sersa G, De Terlizzi F, Occhini A, Plaschke CC, Groselj A, Langdon C, Grau JJ, McCaul JA, Heuveling D, Cemazar M, Strojan P, de Bree R, Leemans CR, Wessel I, Gehl J, Benazzo M. European Research on Electrochemotherapy in Head and Neck Cancer (EURECA) project: Results of the treatment of skin cancer. Eur J Cancer. 2016 Aug;63:41-52. [CrossRef]
- Al-Hadithy N, Dehnel A, George A, Kisiel R, Lunt C, Stone C. Patient reported outcomes in prospective cohort study of Electrochemotherapy. Int J Surg. 2018 Apr;52:110-9. [CrossRef]
- Campana LG, Balestrieri N, Menin N. Adjuvant skin-sparing electrochemotherapy in a breast cancer patient with a prosthetic implant: 5-year follow-up outcomes. J Surg Case Rep. 2022May;5:rjac199. [CrossRef]
- Ferioli M, Perrone AM, Buwenge M, Arcelli A, Vadala' M, Fionda B, Malato MC, De Iaco P, Zamagni C, Cammelli S, Tagliaferri L, Morganti AG. Combination of Electrochemotherapy with Radiotherapy: A Comprehensive, Systematic, PRISMA-Compliant Review of Efficacy and Potential Radiosensitizing Effects in Tumor Control. Curr Oncol. 2023 Nov 13;30(11):9895-9905. PMID: 37999139; PMCID: PMC10670517. [CrossRef]
Figure 1.
Bleeding of the lower lateral quadrant in the right breast.

Figure 2.
pectorals muscle involvement after 18-fludeoxyglucose-Positrone Emission Tomography (18-FDG-PET) 18 month.
Figure 2.
pectorals muscle involvement after 18-fludeoxyglucose-Positrone Emission Tomography (18-FDG-PET) 18 month.
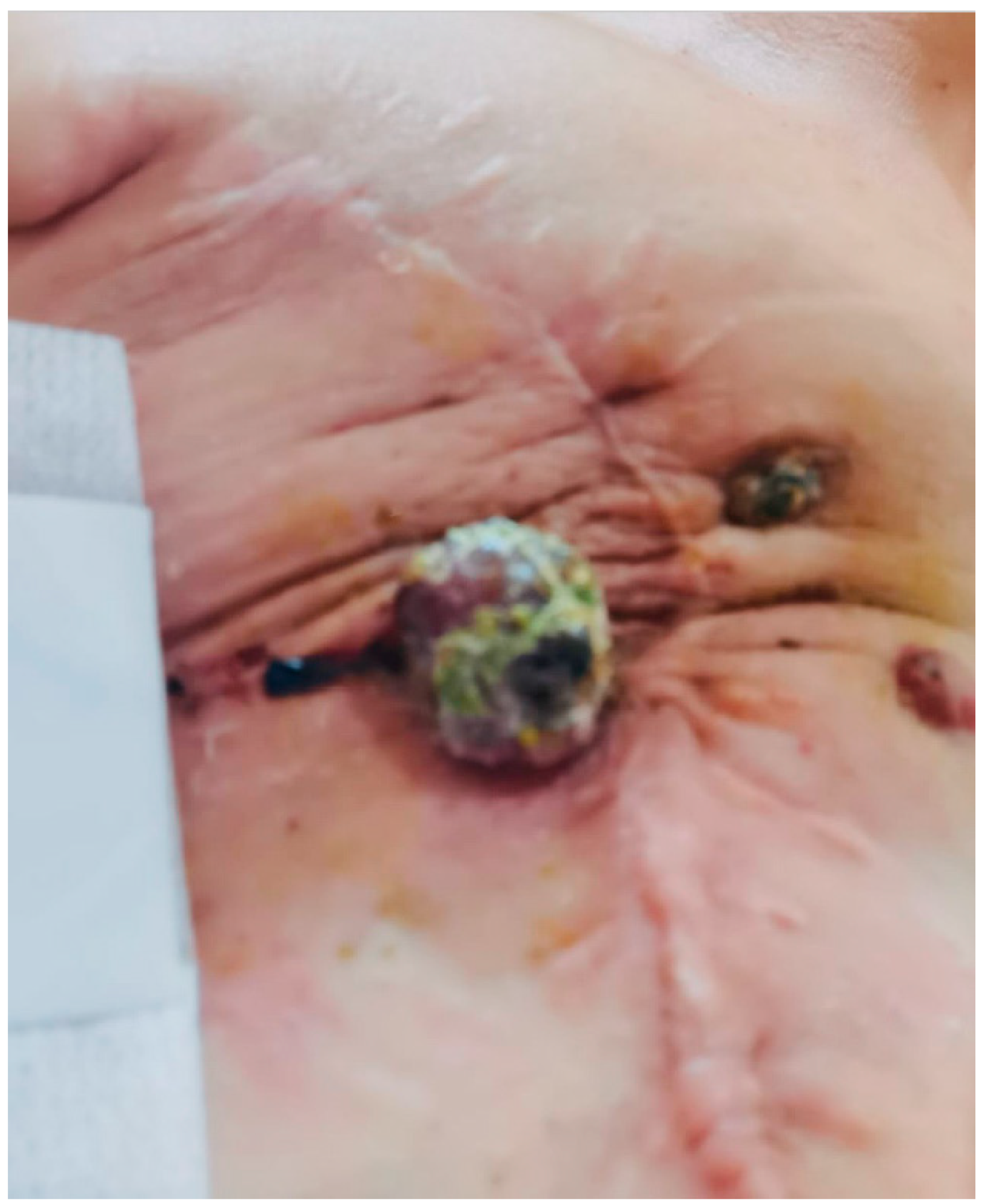
Figure 3.
pectorals muscle involvement after ECT cycles.


Table 1.
Clinical study describing patient with radiogenic angiosarcoma (RAS) of the breast treated also with electrochemotherapy (ECT).
Table 1.
Clinical study describing patient with radiogenic angiosarcoma (RAS) of the breast treated also with electrochemotherapy (ECT).
| STUDY | Type of study | Patients | AGE | History | FIRST TREATMENT | LATENCY PERIOD months |
CLINICAL FEATURES | SKIN REGION | RE-TREATMENT | Histology | C myc amplification |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cencelj-Arnez 2020 [16] |
CR | 1 | 63 | Syncronus bilateral Luminal BC (right breast) |
Mastectomy + 6 cicles x 5-fluorouracil, epirubicin, Cyclophosphamide+ letrozole + RT 25Gy |
60 | Ulcerated red lesion | Lower-medial quadrant In right breast |
Excision + ECT + doxorubicin | High grade RAS | Yes |
| Campana 2019 [19] |
CS | 20 (10 breast RAS) |
/ | / | / | / | / | / | / | / | / |
| Benevento 2015 [20] |
CR | 1 | 76 | Invasive ductal carcinoma Luminal BC (left breast) pT1 pN0 M0 G2 |
BCS + 50 Gy in 25 fractions of 200 cGy/daily with boost of 10 Gy in 5 fractions of 200 cGy/daily + Tamoxifene |
48 | painful, violet, multi-nodular mass |
Left>right breast | Excision + Mastectomy (after 4 years)+ doxorubicin |
grade-II RAS |
/ |
| Guida 2016 [20] |
RS | 19 (6 breast RAS) |
69 | / | / | 96 | / | Scalp (5) Breast (8) Skin (3) Soft tissue (3) |
ECT (19/19)+ Surgery (17/19) + RT (5/19) + CT (3/19) |
RAS | / |
| Mocerino 2015 [26] |
CR | 1 | 77 | invasive ductal carcinoma pT1N0M0 ER +15%; PgR +30%; HER2 IHC 1+ (left breast) |
BCL + 60 Gy in 30 fractions + tamoxifen |
84 | ecchymotic lesion (1.3 cm) |
near the scar |
Excision + left mastectomy (after 1 year)+ right mastectomy (after 2 years) + ECT+ 69 Gy + Doxorubicin |
low-grade RAS |
/ |
| Laurino 2022 [27] |
CR | 1 | 61 | infiltrating ductal carcinoma, pT1cN0, grade G2, ER 98%, PGR 20%, HER2+, left breast |
BCL + 50 Gy in 25 fractions + 10 Gy in 5 fractions by photons+ Adjuvant CT + letrozole |
72 | / | Left breast | Neoadjuvant CT + mastectomy (after 1 year) + ECT+ Re-excision |
high-grade RAS (G3), positive for Factor VIII and CD31, with extensive areas of necrosis and ulceration. | / |
| Laurino 2022 [27] |
CR | 1 | 63 | infiltrating ductal breast cancer pT1cN1(1/18), G2, ER: 90%, PGR: 60%, Ki67 index at 15%, and HER2 negative Left breast |
BCS+ 5-fluorouracil, epidoxorubicin, and cyclophosphamide+ 50 Gy in 25 fractions + 10 Gy in 5 fractions by photons+ letrozole |
108 | ulcerated and bleeding left breast lump, 7 cm in diameter, adherent to the chest wall | Left breast | Radiofrequency termoablation + gemcitabine and docetaxel + ECT + |
RAS | / |
| Parisi 2023 | CR | 1 | 59 | breast invasive ductal Luminal B carcinoma pT1c N0 M0 (right breast) |
BCL + 60 Gy in 30 fractions+ femara |
60 | exophytic lump | near the scar |
Excision + right mastectomy + Paclitaxel (doxorubicin contraindicated) + 40.5 Gy in 15 fractions + ECT |
Grade II RAS | / |
CR= case report. CS= cohort study. Rs= retrospective study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



