Submitted:
11 December 2023
Posted:
13 December 2023
You are already at the latest version
Abstract
Aggressive angiomyxoma (AAM) is a rare and benign mesenchymal tumor, localized predominantly in the female pelvis. Its invasive growth and local recurrence are challenging for professionals. Histologically, AAM is a tumor with a myxoid, highly vascularized stroma. The diagnosis is made relatively late due to nonspecific symptoms. Treatment of AAM is extensive local surgical excision. Gonadotropin-releasing hormone agonists are added postoperatively. The prognosis is good and metastasis is rare.
We present a case of an AAM located in the left greater labial area in a 50-year-old woman initially diagnosed as left inguinal hernia.
The tumor was extirpated under epidural anaesthesia on the date of the patient's informed consent.
The patient was prescribed postoperative therapy with Zoladex 3,6 mg according to the schedule. The patient was subjected to monthly gynecological check-ups for one year after the surgical intervention. To date, no recurrence of the underlying disease has been detected. Long-term results show a good trend.
In conclusion, we can say that the optimal treatment of AAM is wide local excision. Рadicality is not recommended because of the risk of postoperative complications. Postoperative administration of GnRH-a is advisable to avoid recurrences. All patients undergo regular follow-up examinations for long-term.
Keywords:
aggressive angiomyxoma
; soft tissue tumors
We present a clinical case of an aggressive angiomyxoma located in the left greater labial area in a 50-year-old woman, initially diagnosed as a left inguinal hernia. The patient was referred to a surgeon with a suspected left inguinal hernia. The surgeon rejected the diagnosis and the woman was referred for a consultation with a gynecologist. The history revealed the following information: the patient was 50 years old and had no family history. She reported two children born by caesarean section in 1995 and 2003 and regular menstrual cycles. She denies any concomitant illnesses. According to the patient, an attempted extirpation of a left Bartholin’s gland cyst was performed 12 years ago, but the results were not followed up and medical records were lacking. Gynecologic examination revealed the following: an External genitalia of non-parturition, with a spherical, lobulated, mobile tumor, elastic consistency, located in the left greater labial area, measuring approximately 6/4 cm, without fluctuation. Vagina - compressed by the described formation; PVCU - conical, pink; OECC - round; canalis cervicalis - closed; Ex utero - nihil; Uterus - in AVF, slightly enlarged overall on account of one intramural myoma node located in the area of the anterior uterine wall, 2 cm in diameter. Adnexa and parameters - bilateral normal. Cavum Douglassi - free. Ultrasonography of small pelvis and the described tumor formation was performed: Uterus - in AVF, with increased size on account of one intramural myoma node located in the area of anterior uterine wall with dimensions 20x18 mm; Endometrium - 7 mm thick; Adnexa - accessible, with normal shape and size; Cavum Douglassi - no freely mobile fluid. A superficial, spherical, lobulated and mobile tumor formation, with indistinct borders, with echo heterogeneous contents and measuring 62x40 mm was visualized in the left greater labial area. In Figure 1, we have demonstrated the sonographic image of the described formation (Figure 1). After discussion and informed consent signed by the patient, antibiotic and anticoagulant prophylaxis was administered. On the 27th of January 2023 at the University Hospital “St. Marina” Pleven, under epidural anaesthesia, extirpation of the tumour formation was performed. The stages of the operation are presented in Figure 2, Figure 3 and Figure 4 (Figure 2, Figure 3 and Figure 4).
In Figure 5 we have demonstrated the macroscopic appearance of the lesion (Figure 5). The patient tolerated the manipulation well, without complications, and was discharged on the third postoperative day. We obtained the following histological result: “Non-encapsulated and locally infiltrative tumor formation, represented by monomorphic, relatively small-sized spindle-shaped or stellate cells with delicate chromatin, mostly hypocellular, with focal increased cellularity. Myxoid stroma with scattered delicate collagen fibers at periphery with accumulation of mature mast cells. Focal erythrocyte extravasates. Dilated capillaries and scattered large, thick-walled (with medial hypertrophy) or hyalinized vessels. Clustering of stromal smooth muscle bundles around vessels. Resection lines uninvolved”. Immunohistochemical result shows: “High expression of desmin and vimentin (100%). Positive ER expression. Lack of expression of the Ki-67 marker’.
Diagnosis: Aggressive angiomyxoma of the external genitalia (Note. Although distant metastases in this tumor are extremely rare, approximately 30% of lesions recur locally).
Aggressive angiomyxoma (AAM) is a slow-growing mesenchymal tumor that is relatively rare. Characteristically, it localizes predominantly in the soft tissues located in the small pelvic area of women (external genitalia, vagina and perineum). This tumour is benign. It is aggressive because in most cases there is marked infiltration of adjacent tissues and a high incidence of local recurrence. AAM was first introduced in 1983 by Steeper and Rosai. They described nine cases of women with benign tumor formations that showed a tendency to infiltrate adjacent tissues and recur locally. Although, this lesion is perceived to be safe, there have been reports of metastasis. To date, approximately 400 cases have been described in the world literature. It is mainly diagnosed in women of reproductive age, premenopausal and manopausal. The peak incidence has been shown to be around forty years of age. The female to male ratio is about 7:1. In males, aggressive angiomyxoma is localized in the inguinoscrotal region (1, 2). Cases with multifocal localization have also been reported in the literature. In these patients, the external genital organs and the pelvic cavity, the vagina and perineum, the small intestine and lung, the pelvis and the heart are simultaneously affected (3, 4). Under experimental conditions, a possible invasion of AAM into the colon of rats has also been found with neurotransmitter consequences in its longitudinal and circular muscles (4, 5, 6).The patient was assigned postoperative therapy with GnRH-agonists (Zoladex 3.6 mg implant) according to the following schedule: one subcutaneous application every 28 days for 6 months. Administration of the GnRH agonist ended in August 2023.
In Figure 6, we demonstrate the aesthetic outcome of the surgical intervention at the seventh postoperative month (Figure 6). The patient underwent monthly control gynecological examinations for one year after the surgical intervention. To date, no recurrence of the underlying disease has been detected. Long-term results show a good trend.
Aggressive angiomyxoma is a benign mesenchymal tumor, but its clinical symptoms cause discomfort and reduce patients’ quality of life. The optimal treatment of AAM is wide local excision. It is not recommended to aim for radicality because of the risk of postoperative complications and the lack of a statistically significant difference in recurrence rates between patients with intact and involved resection lines. Preoperative GnRH-a therapy provides tumor volume reduction. Postoperative administration of GnRH-a is recommended to avoid recurrences. All patients underwent regular follow-up examinations for long-term follow-up.
References
- Geng J, Cao B, Wang L.. Aggressive angiomyxoma: an unusual presentation. Korean J Radiol 2012; 13: 90. [CrossRef]
- Steeper TA, Rosai J. Aggressive angiomyxoma of the female pelvis and perineum: report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol 1983; 7: 463–476. [CrossRef]
- Tomov, S.T., Gorchev, G.A., Kiprova, D.K., Gorcheva, Z.V., Ahmad, S. Peri-operative and survival outcomes analysis of patients with endometrial cancer managed by three surgical approaches: a long-term Bulgarian experience. Journal of Robotic Surgery, 2022, 16(6), pp. 1367–1382. [CrossRef]
- Gorcheva, Z. V., Stavreva, G. T., Dikova, N. N., Negrev, N. N., & Radomirov, R. G. Neurotransmissions Contributing to Ascending Reflex Responses of Colonic Circular Muscle in a Rat Model. Comptes rendus de l Academie bulgare des Sciences, 2019; 72(9), 1276-1283. [CrossRef]
- Gorcheva, Z. V., Stavreva, G. T., & Radomirov, R. G. Neurotransmitter implications in descending motility of longitudinal and circular muscles in rat colon. Archives of the Balkan Medical Union, 2018;53(1), 14-22.
- Stavreva, G. T., Gorcheva, Z. V., Negrev, N. N., & Radomirov, R. G. Cholinergic, Tachykininergic and Nitrergic Transmission in Ascending Motor Activity of Colonic Longitudinal Muscle in a Rat Model. Comptes rendus de l’Académie bulgare des Sciences, 2016; 69(3), 357-365.
Figure 1.
Sonographic image of the tumor formation.

Figure 2.
Dissection of the tumor formation.
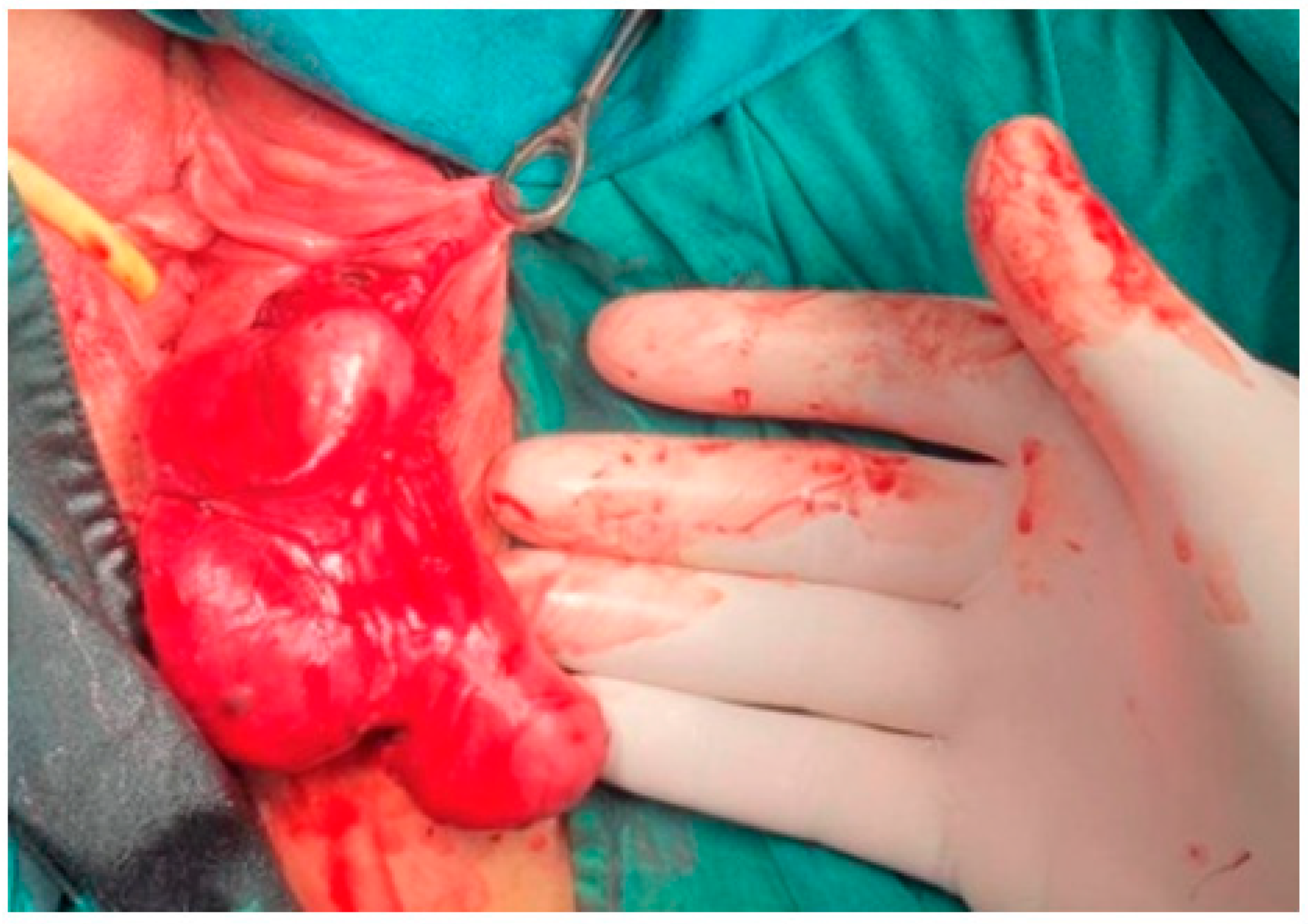
Figure 3.
The tumor formation before extirpation.

Figure 4.
Repair of the surgical wound with single sutures.

Figure 5.
Macroscopic appearance of the lesion.
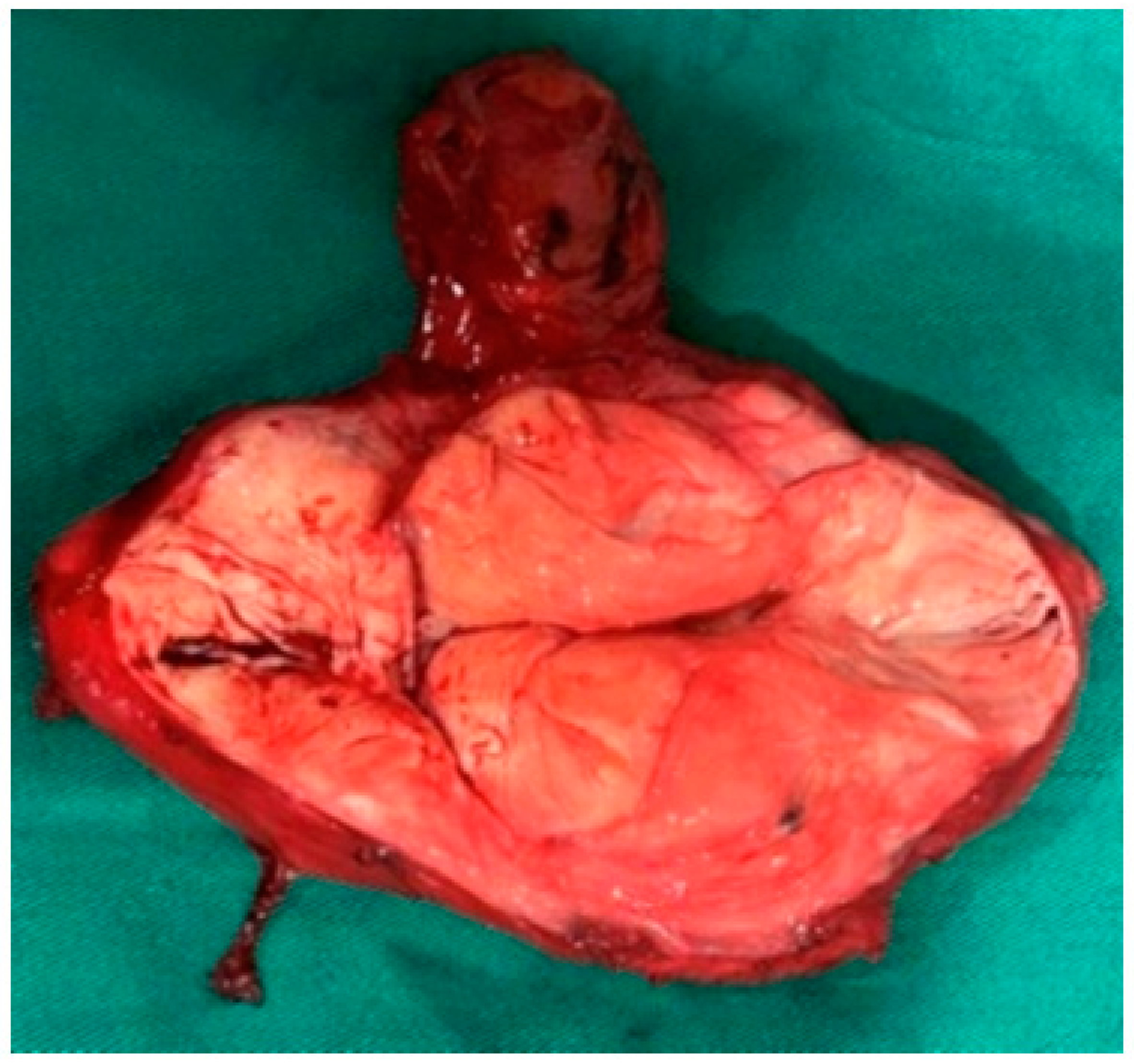
Figure 6.
Aesthetic result of surgical intervention 7 months after tumor extirpation.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



