
Submitted:
13 December 2023
Posted:
14 December 2023
You are already at the latest version
Abstract
Venous thromboembolism (VTE) is a prevalent medical condition with high morbidity, mortality, and associated cost. Anticoagulation remains the main treatment for VTE, though the decision on when, how, and for how long to administer anticoagulants is increasingly complex. This review highlights the different phases of VTE management, special circumstances for consideration such as antiphospholipid syndrome, coronary artery disease, cancer associated thrombus and COVID, and future anticoagulation options. Anticoagulation management will continue to be a complex decision, applying evidence-based medicine to individual patients with the hope to maximize effectiveness while minimizing risks.
Keywords:
Venous Thromboembolism
; Pulmonary Embolism
; Deep Vein Thrombosis
; Anticoagulation
; cardio-vascular disease
1. Introduction
Venous thromboembolism (VTE) is defined as a blood clot in the venous system, occurring as a deep vein thrombosis (DVT) or pulmonary embolism (PE). The annual incidence of VTE is estimated to be around 1-2 per 1000 people, or 300,000-600,000 cases. However, the incidence is noted to differ by age, with VTE occurring in 1 per 100 people aged ≥ 80 years old. The estimated total annual healthcare cost for VTE ranges from $2-10 billion. The disease process carries high morbidity and mortality, with 10-30% of patients having a 30-day mortality. Additionally, 20-25% of PE cases present with sudden death. [1] Around 60,000-100,000 deaths occur annually from VTE. A third of the people who have a VTE event will have a reoccurrence within 10 years while a third of the patients with DVT will develop post-thrombotic syndrome. [1,2] This highlights the high burden of VTE on the healthcare system and the importance of its management, including preventing recurrence.
Traditionally, most VTE events are characterized according to the presence or absence of provoking risk factors. Provoked events can be further characterized as a transient risk factor vs persistent risk factor. While for unprovoked events they have no provoking factor either transient or persistent. [3] (Table 1).
Venous thromboembolism management continues to be an evolving field with considerations in choice and durations for anticoagulation. This review will outline VTE management decisions, focusing on various anticoagulation options, treatment length, and special considerations.
2. Overview of Anticoagulation
Anticoagulation is the bedrock of VTE management given its proven role in preventing VTE occurrence and recurrence. For nearly all patients with a proximal DVT or acute PE, anticoagulation is recommended as first-line therapy. Treatment for VTE is typically divided into three phases: initiation phase, treatment phase (primary treatment), and extended phase (secondary prevention). (Figure 1). The goal of the initiation phase is to slow down any active thrombus formation, helping to prevent new thrombus from forming while allowing the body’s natural thrombolytic process to proceed and restore/maintain venous blood flow. This can be achieved through either oral anticoagulation, with apixaban or rivaroxaban, or through parental medication (e.g., unfractionated heparin, low-molecular-weight heparin). For the treatment phase, all patients are recommended to receive 3-6 months of treatment with anticoagulation. This is the time when patients are at highest risk of recurrence as acute thrombus is being converted to fibrin. [4] Given their overall improved safety profile (especially lower rates of intracranial hemorrhage) and ease of administration, anticoagulation with apixaban, dabigatran, edoxaban, or rivaroxaban is recommended over vitamin K antagonist (VKA) for the treatment phase. [5] (Table 2). For patients with continued risk of VTE they will continue anticoagulation in the extended phase. In this phase the risk vs benefit of full dose anticoagulation vs. reduced-dose anticoagulation vs. no anticoagulation will need to be considered dependent on patient’s risk factors. (Figure 1).
Apart from anticoagulation route selection it is also important to decide where management should take place. For patients with a DVT, if there is rapid availability to ultrasound and ease of communication, then outpatient management is usually preferred. Exceptions would be for patients with high risk of limb loss (e.g., phlegmasia cerula dolens) or inability to reliably obtain anticoagulant medications in a timely manner and clinic follow up. Most PE are first evaluated in the Emergency Department where they are risk stratified for the risk of deterioration. Patients at low risk for complications should be offered an outpatient management strategy if there is appropriate availability of testing, medications, and clinical follow. Study have estimated 20% or more of acute PE cases in the emergency department may be good candidates for outpatient treatment. [6] The remaining cases typically require a hospital stay.
An exception to routine anticoagulation for VTE treatment is in patients with distal DVT. Distal DVTs affect the deep veins with the most proximal component being distal to the popliteal vein. The 9th edition of the CHEST guideline recommends serial ultrasound in 1-2 weeks without anticoagulation if the thrombus does not extend proximally. However, if there is extension into proximal veins, anticoagulation is strongly recommended. [5]
Another exception for routine anticoagulation treatment is in patients with isolated subsegmental PE without proximal DVT. In these patients, the risk of recurrence needs to be considered. In patients with low risk of recurrent VTE clinical surveillance can be considered, while for patients with high risk of recurrent VTE anticoagulation is recommended. These are both classified as weak recommendation by the most recent CHEST guidelines. [5]
The third important exception is in patients with active bleeding, for whom anticoagulation should be avoided. It is also reasonable to consider avoiding anticoagulation in patients at very high risk of bleeding. Patient’s risk vs benefit of anticoagulation needs to be considered in setting of VTE management and bleeding, with continued re-assessment. If anticoagulation is not being pursued, then the role of an IVC filter should be reviewed.
3. Phases of Management of VTE
3.1. Initiation Phase
During initiation phase, the goal is to stop the growth of thrombus and prevent embolism of thrombus with anticoagulation. This can occur over 5 to 21 days dependent on anticoagulation chosen. Traditionally, unfractionated heparin or low-molecular-weight heparin was the anticoagulant of choice. Now, apixaban and rivaroxaban are oral options which can be used for the initiation phase. Typically, if patients are hospitalized in the acute setting for VTE, they are initially started on a parenteral heparin agent and then transitioned to oral options prior to hospital discharge. When this transition occurs before the completion of a typical initiation phase (e.g., full 7 days for apixaban or 21 days of rivaroxaban), then the higher total daily dose of these oral medications are given to complete that initiation phase duration. Some clinicians will transition to the treatment phase dosing of oral anticoagulants if at least 5 days of parenteral heparin has been given, even if this strategy was not tested in the phase 3 randomized trials or included in the package label dosing recommendations.
For patients in the outpatient setting, direct oral anticoagulants (DOACs) with apixaban and rivaroxaban are effective oral-only options for patients who do not want parenteral lead in therapy. (Figure 1). No single DOAC is recommended over another by most major society guidelines. [5,7,8] Cost should be considered for DOAC therapy, which can be a barrier for patients. However, there are assistance programs available from drug manufactures that can substantially reduce the out-of-pocket cost for many patients. Discussion with pharmacists and/or social workers are often helpful to connect patients with appropriate resources for DOAC coverage.
3.2. Treatment Phase
Treatment phase can last between 3-6 months, dependent on thrombus burden, symptoms, and patient clinical scenario. The American Society of Hematology recommends that this treatment phase last only 3-6 months rather than a more extended duration of 12 months. [7] It is important to note, however, that the duration of the treatment phase does not preclude the use of oral anticoagulation in the extended phase (secondary prophylaxis). DOACs are now the mainstay treatment in this phase. However, vitamin K antagonists (VKA) are an acceptable alternative for most patients and may be preferred in select patient groups (see below).
For patients using apixaban or rivaroxaban as an oral-only strategy during the initiation phase, these DOACs are typically continued into the treatment phase, but with a dose reduction. (Figure 1). Dabigatran and edoxaban, on the other hand, are initiated in the treatment phase after a 5-10 days run in period (initiation phase) with a parenteral anticoagulant. VKA with warfarin continues to be a well-studied anticoagulation option, though it can be difficult requiring frequent lab work and with higher risk of bleeding. Warfarin needs to be monitored through the international normalized ratio (INR) with goal INR 2-3. There can be higher variability amongst patients for warfarin dosing given patient specific factors such as diet, genetics or other medications. Pharmacy costs of warfarin can be lower than DOACs for many patients, but the cost of INR laboratory testing or home testing must also be factored into the overall cost estimates. Most patients are started on warfarin 5mg daily with frequent INR testing at least weekly to help determine warfarin dosing regimen. The mechanism of actions plus special considerations for oral anticoagulation are outlined in Table 2. Overall, treatment of choice for anticoagulation should be patient specific with shared decision making with the patient and provider.
3.2. Extended Phase
Extended phase, or anticoagulation beyond the treatment phase of 3-6 months, is considered for certain patient populations dependent on patients’ risk of recurrent VTE versus risk of bleeding with continued treatment. Patient preference as well as risk scores (e.g., HERDOO2 Rule, Vienna Prediction Model, or DASH Prediction Score) [9,10,11] can assist with the decision-making process for extended phase anticoagulation. In patients with low risk of VTE recurrence who had a transiently provoked VTE (Table 1), anticoagulation beyond 3-6 months of treatment phase is usually not be necessary. Generally, for patients with unprovoked VTE, extended phase treatment should be considered. Both DOACs and warfarin are viable options for extended phase anticoagulation. For patients continuing on warfarin for VTE prevention, an INR goal of 2-3 is recommended. Dabigatran, apixaban, and rivaroxaban are all potential options for continued anticoagulation for secondary VTE prevention. These three DOACs have been compared to placebo in studies demonstrating superiority in preventing VTE recurrence without significant rates of major bleeding. [12,13,14,15]
However, only apixaban and rivaroxaban have demonstrated both efficacy and safety in lower doses than their initial treatment phase dose for recurrent VTE prevention. In AMPLIFY-EXTEND, apixaban 5 mg BID was compared to apixaban 2.5 mg BID and placebo, demonstrating similar rates of recurrent VTE in both apixaban groups and superiority to the placebo group. [14] Patients who had a symptomatic DVT or PE, with treatment from 6-12 months without recurrent VTE episode were included in the study. The EINSTEIN-CHOICE trial studied rivaroxaban 20 mg daily with rivaroxaban 10 mg daily and aspirin 100 mg daily. Both rivaroxaban groups had similar rates of recurrent VTE and reduced rate of VTE compared to the aspirin group, while having no significant difference in rate of major bleeding. [15] Patients who had an objectively confirmed, symptomatic proximal DVT or PE, anticoagulation for 6-12 months, and no interruption in anticoagulation 7 days prior to enrollment were included in the study. Given these studies, lower dose DOACs compared to standard therapy should be considered for continued anticoagulation in prevention of recurrent VTE. Once again, this decision is patient specific, weighing the risk vs benefit of full vs reduced DOAC dosing.
4. Special Considerations
Special circumstances need to be considered when deciding management for VTE. Briefly, below we will review VTE management in cancer-associated thrombosis (CAT), antiphospholipid syndrome (APS), coronary artery disease (CAD), and COVID.
4.1. Cancer-associated Thrombosis Treatment
Cancer is among the most common risk factor for VTE, with approximately 20% of all VTE cases occurring in patients with cancer. In these patients, more than 50% of VTE cases occur within 3 months of the cancer diagnosis. Both the American College of Chest Physicians (ACCP) and ASH have guideline recommendations specifically on the management of CAT. ACCP guidelines recommend DOAC over other anticoagulation for acute VTE in setting of cancer. [5] While for ASH both DOACs (apixaban or rivaroxaban) or low molecular weight heparin (LMWH) are recommended. The SELECT-D study examined rivaroxaban vs dalteparin monotherapy and found the DOAC group at 6 months had significantly fewer recurrent VTE episodes but with higher rates of bleeding. [16] The ADAM VTE and Caravaggio study both looked at apixaban vs dalteparin noting lower risk of recurrent VTE while the Caravaggio study had no difference in major bleeding risk. [17,18] For short term treatment (3-6 months), DOAC is recommended over LMWH. In patients with active cancer and VTE, long term anticoagulation is recommended for secondary prophylaxis which can be achieved through DOAC or LMWH. In patients with cancer and recurrent VTE on anticoagulation, inferior vena cava filter is not recommended. [19] These recommendations should be considered when treating VTE for patients with cancer associated thrombosis. It is worth noting that special considerations should be made for gastrointestinal or genitourinary malignancies as in these select populations DOACs have demonstrated higher rates of bleeding. [20] Additionally, there should be close communication with the patient’s oncologist given drug-drug interactions with DOACs and caner therapies. DOACs uptake is dependent on the P-glycoprotein system while metabolism is dependent on cytochrome P450 system. DOACs should be avoided with coadministration with cancer therapies that are strong P-glycoprotein or CYP3A4 inducers or inhibitors. [21]
4.2. Thrombotic Antiphospholipid Antibody Syndrome Treatment
Warfarin and other VKAs have been the mainstream treatment for thrombotic antiphospholipid syndrome (APS). However, given increased use of DOACs for other conditions, the use of DOACs for APS remains controversial. While DOACs are far more convenient for patients and are associated with lower rates of bleeding than VKA, it’s unclear if they are as effective as VKA in patients with APS. Khairani et al conducted a system review and meta-analysis of RCTs comparing DOACs vs VKA for treatment of VTE in patients with APS. Four open labeled RCT were included as summarized in Table 3. [22,23,24,25,26] The study found that DOACs compared to VKA have increased risk of arterial thrombosis but similar risk of subsequent VTE or major bleeding. Overall, the findings did not support the routine use of DOACs for patients with thrombotic APS. [22] Additionally, all major societal guidelines recommend use of VKA over DOACs for APS. [5,7,8] However, there may still be select cases where DOAC therapy is appropriate for a patient with APS, especially if that strongly aligns with the patient’s values/preferences and they are well informed of the current outcomes data.
4.3. Concurrent Coronary Artery Disease and Venous Thromboembolism
The optimal antithrombotic regimen can be difficult to determine for patients with both CAD and VTE. Historically, patients have been treated with triple therapy including two antiplatelet agents (low-dose aspirin, P2Y12 inhibitors) and anticoagulation. However, this triple therapy combination increases the risk of bleeding up to 3-fold compared to oral anticoagulation alone. [27] Studies examining risk of bleeding on oral anticoagulation have demonstrated lower rates of bleeding in patients with VTE as compared to those with AF, likely due to younger age and fewer comorbidities. However, several key factors are critical to consider when a patient on anticoagulation for VTE undergoes percutaneous coronary intervention (PCI). These include the planned duration of anticoagulation, urgency of PCI, and how best to combine anticoagulation with anti-platelet therapy to decrease bleeding risk.
The American College of Cardiology (ACC) has developed clinical pathways to assist with anticoagulation and antiplatelet therapy. The first key distinction to make is duration for anticoagulation and if it will be indefinite therapy as discussed prior. Next, the reason for PCI (stable ischemic heart disease [SIHD] vs acute coronary syndrome [ACS]) divides the pathways in length and choice of antiplatelet therapy. (Figure 2). Finally, all patients should be started on proton pump inhibitors or H2 blockers to decrease risk of bleeding when they are using multiple antithrombotic agents concurrently. The use of DOAC is preferred over warfarin while on antiplatelet therapy given lower risk of major, intracranial, or fatal bleeding with DOAC therapy. However, special considerations (e.g., use of warfarin for APS) must be taken into account for individual patients. [28]
4.4. COVID-19 Infection
COVID-19 infection creates a pro-inflammatory state that often increases a patient’s risk for VTE, especially when the infection is severe enough to require hospitalization. For patients that develop VTE concurrent with a COVID-19 acute infection, standard anticoagulation therapy as outlined above is recommended. These patients are typically considered to have experienced a transient, reversibly provoked VTE, so a shorter course of 3-6 months of anticoagulation is most common. [29]
The pro-inflammatory and thrombotic nature of COVID-19 has led to evolving recommendations regarding the use of anticoagulation for VTE thromboprophylaxis. The recommendations require a balance between thrombotic risk and bleeding risk, as well as the patient’s overall risk of survival. In general, patients with COVID-19 can be categorized into one of three groups: ambulatory, hospitalized non-critically ill, and hospitalized critically ill. Based on the results of several randomized trials in patients who require oxygen but are not critically ill (i.e., not in intensive care), therapeutic dose of heparin (preferentially LMWH) is recommended for patients with D-dimer above upper limit of normal and without increased bleeding risk. [29,30,31,32,33] These patients should continue therapeutic-intensity thromboprophylaxis for 14 days or until discharge/escalation of care to an intensive care unit. All other hospitalized patients should receive standard VTE thromboprophylaxis with prophylactic doses of heparin. Use of DOACs for inpatient thromboprophylaxis is generally not recommended. [33,34] However, consideration can be made for the use of extended post-hospital thromboprophylaxis with low-dose rivaroxaban in select patients at high thromboembolic risk but low bleeding risk. [35] Finally, antiplatelet therapy to prevent COVID progression or death is not recommended based on negative results of the ACTIV-4a and RECOVERY trials. [30,31,32,33,34,35,36]
5. Future Anticoagulation Options
Anticoagulation management of VTE looks different today than twenty years ago. DOACs revolutionized VTE management with their increased ease of administration and lower risk of bleeding, but more limited clinical applications. There continue to be ongoing clinical trials examining new anticoagulation medications. Table 4 summarizes current ongoing trials for VTE and Factor XI/XIa inhibitors. [37,38,39] These agents might allow for further reductions in bleeding risk by uncoupling thrombosis and hemostasis. Furthermore, they may provide further advantages over DOACs by eliminating concerns about renal clearance and longer half-lives to address issues of medication compliance. However, their efficacy in preventing VTE or VTE recurrence remains to be proven in rigorous phase 3 randomized trials.
6. Final Thoughts
VTE is a highly prevalent condition associated with significant morbidity and mortality. While anticoagulation is the mainstream therapy for VTE, the decision on when, how, and for how long to administer anticoagulants is increasingly complex. By considering each individual patient’s underlying thromboembolic and bleeding risk, clinicians can then apply evidence from both randomized and observational data to personalize anticoagulation therapy. Anticoagulation management will continue to evolve with new agents and new evidence that aims to maximize effectiveness and minimize risk.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
GDB: Grant Funding – Boston Scientific; Consulting - Pfizer, Bristol-Myers Squibb, Janssen, Bayer, AstraZeneca, Sanofi, Anthos, Abbott Vascular, Boston Scientific; DSMB - Translational Sciences (Clinical Events Adjudication Committee); Board of Directors - Anticoagulation Forum. AM and NH – none.
References
- Beckman, M.G; Hooper, W.C.; Critchley, S.E.; Ortel, T.L. Venous thromboembolism: a public health concern. Am J Prev Med 2010, 38 (Suppl. 4), S495–501. [Google Scholar] [CrossRef] [PubMed]
- CDC. Data and Statistics on Venous Thromboembolism. Available online: https://www.cdc.gov/ncbddd/dvt/data.html (accessed on 11/6/2023).
- Kearon, C.; Ageno, W.; Cannegieter, S.C.; Cosmi, B.; Geersing, G.J.; Kyrle, P.A. Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. Journal of Thrombosis and Haemostasis 2016, 14, 1483. [Google Scholar] [CrossRef] [PubMed]
- Renner, E.; Barnes, G.D. Antithrombotic Management of Venous Thromboembolism: JACC Focus Seminar. J Am Coll Cardiol 2020, 76, 2142–2154. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.M.; Woller, S.C.; Baumann Kreuziger, L.; et al. Executive Summary: Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest 2021, 160, 2247–2259. [Google Scholar] [CrossRef] [PubMed]
- Vinson, D.R.; Ballard, D.W.; Huang, J.; et al. MAPLE Investigators of the KP CREST Network. Outpatient Management of Emergency Department Patients With Acute Pulmonary Embolism: Variation, Patient Characteristics, and Outcomes. Ann Emerg Med 2018, 72, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Neuman, I.; et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv 2020, 4, 4693–4738. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). European Heart Journal 2020, 41, 41–543. [Google Scholar] [CrossRef] [PubMed]
- Eichinger, S.; Heinze, G.; Jandeck, L.M.; Kyrle, P.A. Risk assessment of recurrence in patients with unprovoked deep vein thrombosis or pulmonary embolism: the Vienna prediction model. Circulation 2010, 121, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Rodger, M.A.; Kahn, S.R.; Wells, P.S.; et al. Identifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant therapy. CMAJ 2008, 179, 417–426. [Google Scholar] [CrossRef]
- Tosetto, A.; Iorio, A.; Marcucci, M.; et al. Predicting disease recurrence in patients with previous unprovoked venous thromboembolism: a proposed prediction score (DASH). J Thromb Haemost 2012, 10, 1019–1025. [Google Scholar] [CrossRef]
- Bauersachs, R.; Berkowitz, S.D.; Brenner, B.; et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010, 363, 2499–2510. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C.; Kakkar, AK.; et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med 2013, 368, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Buller, H.R.; Cohen, A.; et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med 2013, 368, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.I.; Lensing, A.W.A.; Prins, M.H.; et al. Rivaroxaban or aspirin for extended treatment of venous thromboembolism. N Engl J Med 2017, 376, 1211–1222. [Google Scholar] [CrossRef] [PubMed]
- Young, A.M.; Marshall, A.; Thirlwall, J.; et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- McBane, R. 2nd.; Wysokinski, W.E.; Le-Rademacher, J.G.; et al. Apixaban and dalteparin inactive malignancy-associated venous thromboembolism: the ADAM VTE trial. J Thromb Haemost 2020, 18, 411–421. [CrossRef] [PubMed]
- Agnelli, G.; Becattini, C.; Meyer, G. , et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N Engl J Med 2020, 382, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Carrier, M.; Ay, C.; et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv 2021, 5, 927–974. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Garcia, D.A.; Lyman, G.H.; Carrier, M. ; Direct oral anticoagulant (DOAC) versus low-molecular weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): a systematic review and meta-analysis. Thromb Res 2019, 173, 158–163. [Google Scholar] [CrossRef]
- Mosarla, R.C.; Vaduganathan, M.; Qamar, A.; et al. Anticoagulation Strategies in Patients With Cancer: JACC Review Topic of the Week. J Am Coll Cardiol, 2019, 73, 1336–1349. [Google Scholar] [CrossRef]
- Khairani, C.D.; Bejjani, A.; Piazza, G.; et al. Direct Oral Anticoagulants vs Vitamin K Antagonists in Patients With Antiphospholipid Syndromes: Meta-Analysis of Randomized Trials. Journal of the American College of Cardiology 2023, 81, 16–30. [Google Scholar] [CrossRef]
- Cohen, H.; Hunt, B.J.; Efthymiou, M.; et al. Rivaroxaban versus warfarin to treat patients with thrombotic antiphospholipid syndrome, with or without systemic lupus erythematosus (RAPS): a randomised, controlled, open-label, phase 2/3, non-inferiority trial. Lancet Haematol 2016, 3, e426–e436. [Google Scholar] [CrossRef]
- Pengo, V.; Denas, G.; Zoppellaro, G.; et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood 2018, 132, 1365–1371. [Google Scholar] [CrossRef]
- Ordi-Ros, J.; Saez-Comet, L.; Perez-Conesa, M.; et al. Rivaroxaban versus vitamin K antagonist in antiphospholipid syndrome: a randomized noninferiority trial. Ann Intern Med 2019, 171, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Woller, S.C.; Stevens, S.M.; Kaplan, D.; et al. Apixaban compared with warfarin to prevent thrombosis in thrombotic antiphospholipid syndrome: a randomized trial. Blood Adv 2022, 6, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.L.; Sorensen, R.; Clausen, M.T.; et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Archives of Internal Medicine 2010, 170, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Kumbhani, D.J.; Cannon, C.P.; Beavers, C.J.; et al. 2020 ACC Expert Consensus Decision Pathway for Anticoagulant and Antiplatelet Therapy in Patients With Atrial Fibrillation or Venous Thromboembolism Undergoing Percutaneous Coronary Intervention or With Atherosclerotic Cardiovascular Disease: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology 2021, 77, 629–658. [Google Scholar] [PubMed]
- NIH. Antithrombotic Therapy in Patients With COVID-19. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antithrombotic-therapy (accessed on 11/26/2023).
- ATTACC, ACTIV-4a, and REMAP-CAP Investigators. Therapeutic anticoagulation with heparin in noncritically ill patients with COVID-19. N Engl J Med 2021, 385, 790–802. [Google Scholar] [CrossRef]
- Sholzberg, M.; Tang, G.H.; Rahhal, H.; et al. Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with COVID-19 admitted to hospital: RAPID randomised clinical trial. BMJ 2021, 375, n2400. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; et al. Efficacy and safety of therapeutic-dose heparin vs standard prophylactic or intermediate-dose heparins for thromboprophylaxis in high-risk hospitalized patients with COVID-19: the HEP-COVID randomized clinical trial. JAMA Intern Med 2021, 181, 1612–1620. [Google Scholar] [CrossRef]
- Stone, G.W.; Farkouh, M.E.; Lala, A.; et al. Randomized trial of anticoagulation strategies for noncritically ill patients hospitalized with COVID-19. J Am Coll Cardiol 2023, 81, 1762. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; de Barros, E.S.P.G.M.; Furtado, R.H.M.; et al. Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): an open-label, multicentre, randomised, controlled trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef] [PubMed]
- Ramacciotti, E.; Agati, L.B.; Calderaro, D.; et al. Rivaroxaban versus no anticoagulation for post-discharge thromboprophylaxis after hospitalisation for COVID-19 (MICHELLE): an open-label, multicentre, randomised, controlled trial. The Lancet 2022, 399, 50–59. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Aspirin in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet 2022, 399, 143–151. [Google Scholar]
- A Study Comparing Abelacimab to Apixaban in the Treatment of Cancer-associated VTE (ASTER) Available online:. Available online: https://www.clinicaltrials.gov/study/NCT05171049 (accessed on 11/26/2023).
- A Study Comparing Abelacimab to Dalteparin in the Treatment of Gastrointestinal/Genitourinary Cancer and Associated VTE (MAGNOLIA) Available online:. Available online: https://www.clinicaltrials.gov/study/NCT05171075 (accessed on 11/26/2023).
- Xisomab 3G3 for the Prevention of Catheter-Associated Thrombosis in Patients With Cancer Receiving Chemotherapy Available online:. Available online: https://clinicaltrials.gov/study/NCT04465760 (accessed on 11/26/2023).
Figure 1.
Choice and Duration of Anticoagulation for VTE.
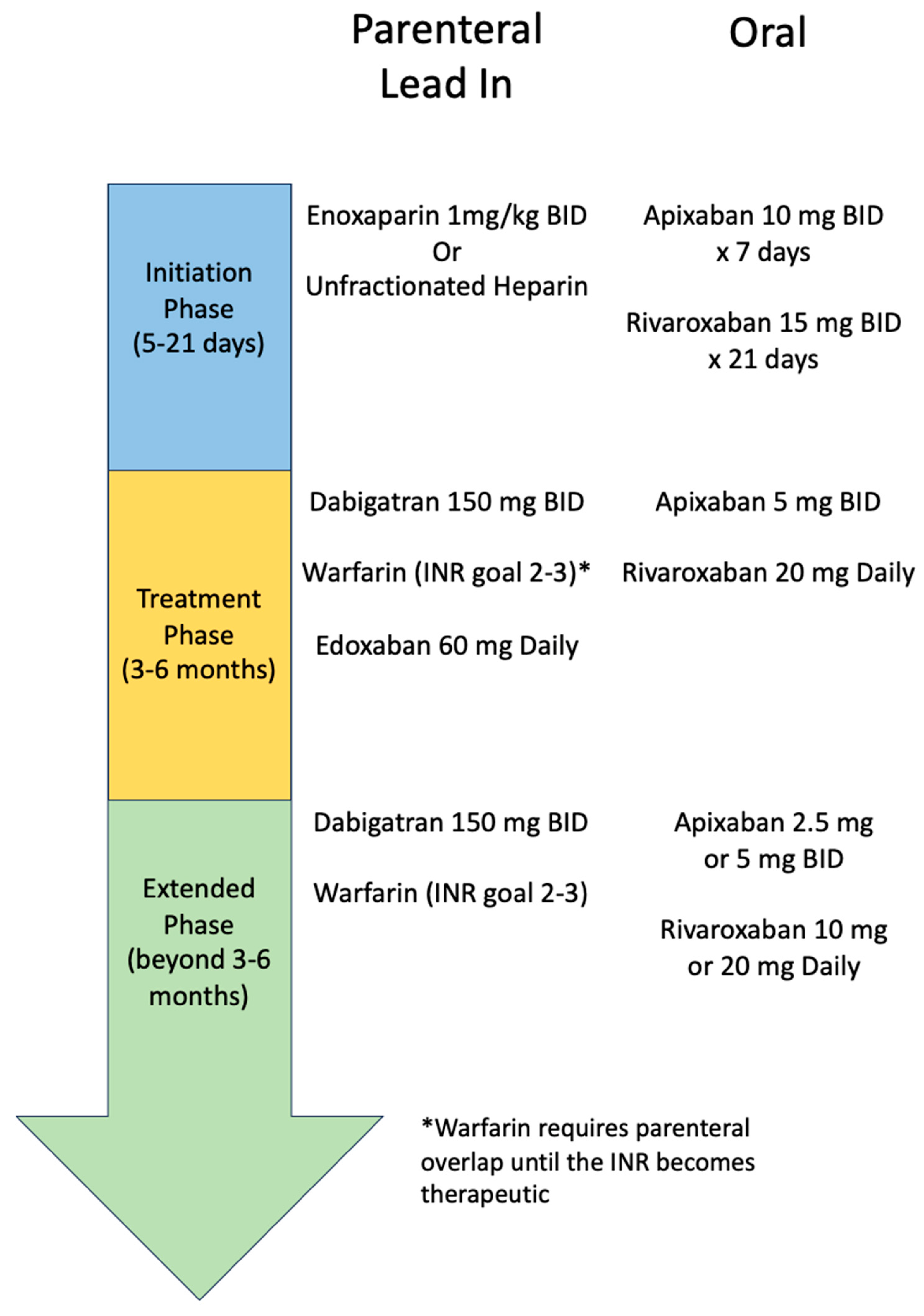
Figure 2.
VTE and CAD Antithrombotic Therapy.
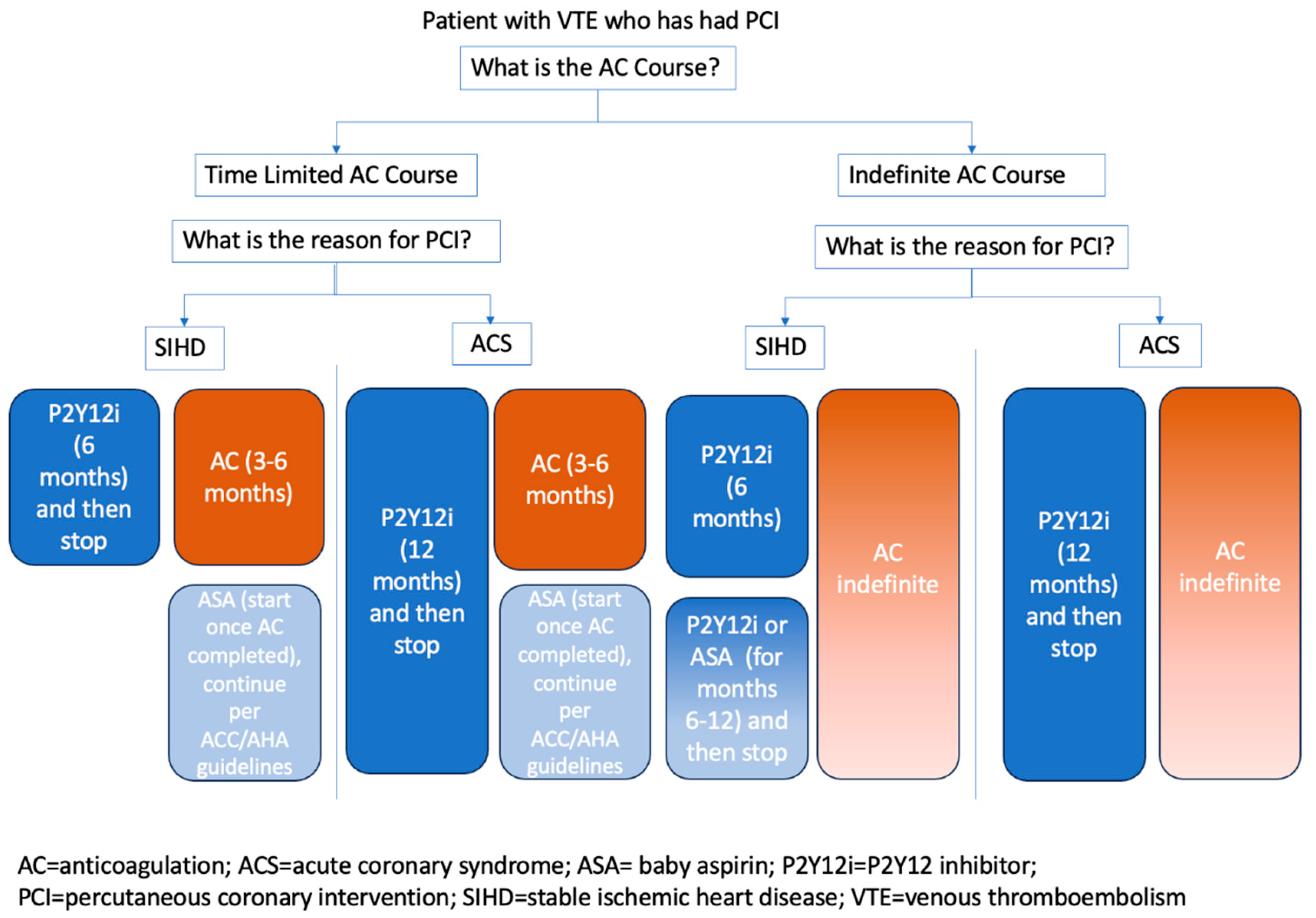

Table 1.
Examples of VTE Provoking Risk Factors.
| Major Transient Risk Factor | Minor Transient Risk Factor | Persistent Risk Factor |
| -Cesarean section -Confined to hospital bed for 3 days -Surgery with general anesthesia for >30 minutes |
-Confined to bed out of hospital for 3 days -Hospitalization < 3 days -Leg Injury -Pregnancy -Estrogen therapy -Acute infectious illness (e.g., COVID-19) without hospitalization |
-Active cancer -Inflammatory bowel disease -Obesity -Chronic inflammatory condition -Advanced age -Previous venous thromboembolism -Genetic/Acquired thrombophilia (APLS, protein C&S deficiency, etc) |
Table 2.
Oral Anticoagulation for VTE.
| Generic Name | Mechanism of Action | Dose and Regimen | Consideration of Renal Function | Consideration of Drug Interactions | Other Considerations |
| Apixaban | Factor Xa Inhibitor | 10 mg BID x7days, followed by 5 mg BID | Not studied in patients with SCr ≥ 2.5 mg/dl or CrCl <25 ml/min | Reducing dose by 50% in patients taking strong dual inhibitors of p-glycoprotein and CYP 3A4. Avoiding in patients taking dual inducers of CYP 34A and p-glycoprotein. | N/a |
| Dabigatran | Direct Thrombin Inhibitor | 150 mg BID after 5-10 days of parenteral anticoagulation lead in | Avoid in CrCl ≤ 30 ml/min | If CrCl ≤ 50 ml/min, patients taking p-glycoprotein inhibitors should avoid dabigatran. Patients taking p-glycoprotein inducers should avoid dabigatran. | N/a |
| Edoxaban | Factor Xa Inhibitor | 60 mg daily after 5-10 days of parenteral anticoagulation lead in | Renally dose to 30 mg daily for CrCl 15-50 ml/min. Avoid in CrCl <15 ml/min | Reduce dose to 30 mg daily for patients taking p-glycoprotein inhibitors. Avoid using with p-glycoprotein inducers. | Reduce dose to 30 mg daily for body weight ≤ 60 kg. |
| Rivaroxaban | Factor Xa Inhibitor | 15 mg twice a day for 21 days, then 20 mg daily | Avoid in CrCl ≤ 15 ml/min | In patients taking moderate dual inhibitors of CYP 3A4 and p-glycoprotein with CrCl ≤ 80 ml/min, use cautiously. Avoid use in patients taking strong dual inhibitors or inducers of CYP 3A4 and p-glycoprotein. | Administer with food. |
| Warfarin | Vitamin K Antagonist | Adjusted to target INR 2-3Require parenteral anticoagulation overlap at initiation | None | Consider reducing starting dose to 2.5 mg for patients with drug-drug interactions expected to increase exposure to warfarin. | Consider reducing starting dose to 2.5 mg for patients with multiple comorbidities, advanced age, and advanced end-organ dysfunction. |
BID= twice daily; CrCl= creatinine clearance as calculated by the Cockcroft-Gault equation with actual body weight; INR= international normalized ratio; N/a= not applicable; SCr= serum creatinine.
Table 3.
Randomized Trials of Oral Anticoagulation for Antiphospholipid Syndrome Patients with Venous Thromboembolism.
Table 3.
Randomized Trials of Oral Anticoagulation for Antiphospholipid Syndrome Patients with Venous Thromboembolism.
| Clinical Trial [Ref. #] | Included Patients | N | Trial Design | Length of Follow-Up | Treatment Groups | Primary Efficacy Outcomes | Efficacy Outcomes | Major Bleeding Outcomes |
| RAPS [23] | Patients with APS who were taking warfarin for previous VTE | 116 | Open label RCT | 210 days | Continue warfarin vs rivaroxaban 20 mg daily | Percentage change in endogenous thrombin potential at day 42, with non-inferiority set at less than 20% difference from warfarin | ETP (nmol/L per min): Rivaroxaban 1086 vs warfarin 548 Treatment effect (ratio): 2.0 (1.7-2.4) |
Rivaroxaban: 0 Warfarin: 0 |
|
TRAPS [24] |
Patients with APS (triple positivity) with history of thrombus | 120 | Open label RCT | 569 days (mean) | Rivaroxaban 20 mg or 15 mg daily (dependent on creatine clearance) vs warfarin | Cumulative incidence of thromboembolic events, major bleeding, and vascular death | Rivaroxaban: 19% Warfarin: 3% HR: 6.7 (1.5-30.5) |
Rivaroxaban: 7% Warfarin: 3% HR: 2.5 (0.5-13.6) |
| Ordi-Ros et al [25] | Patients with APS (positive result on aPL testing on 2 occasions at least 3 months apart) with history of thrombus | 190 | Open label RCT | 36 months | Rivaroxaban 20 mg or 15 mg daily (dependent on creatine clearance) vs warfarin | Proportion of patients with new thrombotic event | Rivaroxaban: 11.6% Warfarin: 6.3% HR: 1.94 (0.72-5.24) |
Rivaroxaban: 6.3% Warfarin: 7.4% HR: 0.88 (0.3-2.63) |
| ASTRO-APS [26] | Patients with thrombotic antiphospholipid syndrome on anticoagulation for secondary prevention | 48 | Open label RCT | 12 months | Apixaban 2.5 mg BID then increased to 5 mg BID (after 25 patient was randomized) vs warfarin | Thrombosis and vascular death | Apixaban: 6 thrombotic events Warfarin: no thrombotic events |
Apixaban: 0 Warfarin: 1 event |
APS= antiphospholipid syndrome; BID= twice daily; ETP= endogenous thrombin potential; HR= hazard ratio; RCT= randomized control trial; VTE= venous thromboembolism.
Table 4.
Factor XI Ongoing Clinical Trials for VTE.
| Clinical Trial Reference (Status) | Drug | Mechanism of Action | N | Clinical Trial Summary | Results |
| ASTER NCT05171049 (Ongoing) [37] | Abelacimab | Binds and inhibits Factor XI and Factor XIa | 1655 | Phase III trial comparing the effect of abelacimab relative to apixaban on VTE recurrence and bleeding in patients with CAT | No results currently |
| MAGNOLIA NCT05171075 (Ongoing) [38] | Abelacimab | Binds and inhibits Factor XI and Factor XIa | 1020 | Phase III trial comparing the effect of abelacimab vs. dalteparin on VTE recurrence and bleeding in patients with gastrointestinal or genitourinary CAT | No results currently |
| NCT04465760 (Recruiting) [39] | Xisomab | Binds Factor XI and blocks activation by Factor XIIa | 50 | Phase II trial examining the efficacy of xisomab as measured by incidence of catheter associated thrombosis in individuals with a central venous catheter | No results currently |
CAT=cancer associated thrombosis; VTE=venous thromboembolism.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



