Submitted:
15 December 2023
Posted:
15 December 2023
You are already at the latest version
Abstract
BACKGROUND:
Current research recorded hearing loss in 8.5million Nigerians. Hearing loss can be prevented and treated. Most individuals in the communities are unaware. Available hearing screening instruments are not readily accessible in communities. Regular screening is the key. Hence, the introduction of the HearWHO App in the communities, a mobile hearing screener.
AIM: - To detect hearing loss and otological disorders
- To validate the HearWHO App in the communities
- To launch the HearWHO App in the communities
MATERIALS AND METHODS: Commenced after obtaining due ethical clearance, informed consent and permissions. A 3 year duration study (March 2020 to March 2022). Study centres were 4 motor parks in Benin City Edo State (Muyi line, Faith motors, Iyare motors and Magorawa terminal) and 2 hospitals in Ondo City, Ondo state (General Hospital and Trauma Centre of the UNIMEDTH complexes). Ambient noise was recorded. Total population sampling technique was used. Health education was given. Using the HearWHO App in mobile smartphone connected to ear piece, each participant’s ears were tested. Each ear was regarded as a separate entity. Otoscopy was done. Findings of hearWHO App were compared with Otoscopic findings. Data realized were documented and analyzed with SPSS -23. P value < 0.05 was regarded statistically significant.
RESULTS: 175 individuals participated, giving 350 ears examined. There were abnormal HearWHO findings in 77.4% ears compared to abnormal Otological findings in 65.0% ears. Predominant otological disorder was Eustachian Tube Dysfunction. Association of HearWHO finding with location was statistically significant (P=0.014).
CONCLUSION AND RECOMMENDATION:
Hearing loss and otological disorders were detected. There was agreement between HearWHO normal findings and normal otological findings.
Based on challenges encountered, there is need to develop additional Apps or modify the HearWHO App to ensure Sustainable Developmental Goal -3 (SDG -3).
Thus, creating a better future today making impact with mobile technology.
Keywords:
HearWHO App
; Otoscopy
; Otorhinolaryngological
; Service
; Community
1. Introduction
An individual is said to have hearing loss when he is unable to hear conversational speeches or loud sounds. 1
Hearing loss is a public health concern that affects 1.3 to 1.5 billion individuals globally.1 It has been documented as the fourth leading contributor to years lived with disability among the growing global health issues.2 The annual economic cost of living with hearing loss is approximately 750 billion United States dollars (US$).3 Hearing loss is a silent disability (not physically visible), only felt during communications and thus has restricted public health support.4 This is worst especially in low-income and middle-income countries, where the incidence of hearing loss is high amidst limited resources that are unequally distributed.4
It has been reported that over 430 million individuals live with disabling hearing loss worldwide and postulated that by the year 2050. 5 If nothing is done to avert the burden of hearing loss, more than 700 million people will be affected with disabling hearing loss which equates to 1 person in every 10 individuals. 6
Earlier studies in Nigeria has shown a prevalence of 26.2% hearing loss of different types and degrees affecting both males and females and almost all age groups. 7 Some of the causes of hearing loss include wax impaction, foreign body in the ears, perforated ear drum, acute or chronic suppurative otitis media, middle ear infections and disorders, ototoxicity and systemic illnesses affecting the hearing apparatus. 7, 8, 9 These disorders lead to conductive hearing loss, sensorineural hearing loss or mixed hearing loss. 7
It is worthy of note that most of these causes are preventable and the different degrees of hearing loss are either curable or can be rehabilitated. 7, 8 More than 5% of the world population require rehabilitation for hearing loss. 10 The notable consequences of untreated hearing loss include difficulties in communication ability and reduced self-esteem in such individuals. Early detection of hearing loss is the key to its effective treatment and rehabilitation. 11
The HearWHO App is a mobile Applicator developed by the World Health Organization (WHO) in order to notice hearing loss as early as possible. It is a software for hearing check. 3 The aim of the software App is to create an accessible device for all people to assess their hearing from time to time for sustained healthy hearing. 3
Due to high prevalence and incidence of hearing loss, especially in low- and middle income countries, in the year 2017, the World Health Assembly, in their Resolution on Prevention of deafness and hearing loss, called on the Stakeholders for hearing health-care, to create and enforce measures to improve health service provisions in underdeveloped and developing countries.3
The HearWHO Applicator was therefore developed as an alternative audiometer that offers the advantage of affordability and availability. 12This App is also mobile and has touchscreen functionality, 12 The WHO validated clinical tools, available directly from the HearWHO applicator providers using the iPad-based and smartphone-based hearing testing with calibrated headphones or earpiece. 13
The use of HearWHO App facilitates community and self-hearing screening and bridges the gap of lack of formally trained hearing screeners and poor access to hearing services. 14
This initiative improves livelihood of individuals in communities and makes life easier.
Although the App was developed in 2017, it was formally released on the 3rd of March, 2019, the world hearing Day of 2019. 12, 13
This App is a 23-sets of 3-digits-in-noise test. It uses the anti-phasic digit stimuli that makes the applicator sensitive to the different ranges of hearing loss, the sensorineural, conductive and asymmetrical hearing losses. 3, 14 Therefore it has no preference for quiet environment. This applicator has a scale of 0 to 49 indicating hearing disorder, 50 to 69 being documented as normal hearing and 70 to 100 denoting perfect hearing.3 This mobile App offers preventive medical care through its reproducibility. This feature gives it the ability to be done repeatedly and thus helps individuals to monitor their hearing profile by themselves. Although this App has been tested and validated by the World Health Organization, its use in different environments needs validation to ensure its usability in different cultures, ethnic groups and languages.
Even though the HearWHO App is a mobile health (m-Health) solution, it has wireless technologies incorporated into health, which provides opportunities for models in delivering hearing health services to the communities, however, it is a capital intensive advance in heath technology. 14 This technology therefore needs support from the government to ensure its sustainability.
1.1. Statement of problem
Hearing loss is a hidden disability which compromises the quality of life of individuals.15, 16, 17 Improved accessibility to mobile health technology accords medium for self-detection and early identification of hearing loss for care with improvements in quality of life. This as well helps to ensure universal health, maintaining the sustainable development goals.16
There is a gap between the individuals in the communities and access to hearing screening facilities in specialist establishments.13, 14 In addition, the number of specialist screeners to conduct or supervise community hearing programmes is low in developing and underdeveloped countries. 13 Even when there is some form of accessibility and availability of screener, there is paucity of funds to foot the bills of the hearing tests. 14 These, therefore, portray the need for a readily available, self-monitored and mobile hearing screener, the HearWHO Applicator (App) to fill the gaps. However, it is overtly clear that the need for a readily available network and browsing data cannot be overemphasized, calling therefore, on government, well-meaning individuals and philanthropists to come to the aid of the communities.
1.2. Justification for the study
The m-Health solution appeals more in the prevention of hearing loss. This is because greater proportion of individuals in these countries will have access to self-hearing check which helps in assessing the hearing status thus preventing hearing loss.4 Furthermore, hearing loss is preventable, curable and can be rehabilitated. 7, 8
1.3. Significance of the study
This study is needed for detection of hearing loss and its causes in the study communities, which can be treated or rehabilitated. If the study is not done, the etiological diseases causing the hearing loss may become complicated with life threatening conditions.
For example, Chronic Suppurative Otitis Media, if not detected and treated may be complicated with sub-periosteal abscess, mastoiditis, Meningitis and intracranial abscess which are life-threatening. 18
1.4. Aim
To detect hearing loss and otological disorders
To validate the HearWHO App in these communities
To launch the HearWHO App in the study communities
To profer solution to identified otological disorders and hearing loss.
1.5. Objective
To determine the demographic characteristics of the study population
To assess the relationship between the demographic characteristics and Otoscopy
To assess the relationship between demographic characteristics and HearWHO App
To analyze the relationship between HearWHO App findings and Otoscopic findings
1.6. Research question
What is the prevalence of hearing loss in the study communities?
What is the prevalence of otological disorder in the study communities?
Is there an agreement between the HearWHO App findings and Otoscopic findings?
1.7. Null hypothesis
There is no agreement between HearWHO App findings and Otoscopic findings
1.8. Research gap/Novelty
Most otological screenings have been with otoscopes. This study introduced the mobile App, a novel App for individuals’ self-screening practices to have ease of access to mobile health. This helps to improve prevention of hearing loss and early identification of cases for treatment and rehabilitation.
2. Materials and Methods
This study commenced after obtaining due ethical clearance from Edo Specialist Hospital, Benin City, informed consent from the participants and relatives for minors, and permission from the study centres. This, was a 3-year duration study from March 2020 to March 2022. The Study centres were 4 motor parks in Benin City Edo State which are Muyi line, Faith motors, Iyare motors and Magorawa motor terminal; and 2 hospitals in Ondo City, Ondo state which are General Hospital and Trauma Centre, both, of the University of Medical Sciences Teaching Hospital (UNIMEDTH) complexes. Ambient noise in the study centres were recorded prior to commencement of study. 67, 66, 64, 65, 57 and 55 in their respective order above.
Total population sampling technique was used. Health talk on the aim and objectives of the study and scope of the study was given. Using the HearWHO App in mobile smartphone connected to ear piece, each participant’s ears were tested. Each ear was regarded as a separate entity. Otoscopy was done. The Findings of HearWHO App were compared with Otoscopic findings. Data realized were documented and analyzed with SPSS -23. P value < 0.05 was regarded as being statistically significant.
3. Results
215 individuals listened to the health talk, out of which, 175 individuals fully participated in ear and hearing screening, giving 350 ears examined. The remaining 40 individuals who did not consent to screening exercises were excluded.
There were abnormal HearWHO findings in 77.4% ears compared to abnormal Otological findings in 65.0% ears. Most predominant otological disorder was Eustachian Tube Dysfunction. Association of HearWHO finding with location was statistically significant (P=0.014).
Figure 1.
DESCRIPTIVE STATISTICS OF DEMOGRAPHIC DATA.
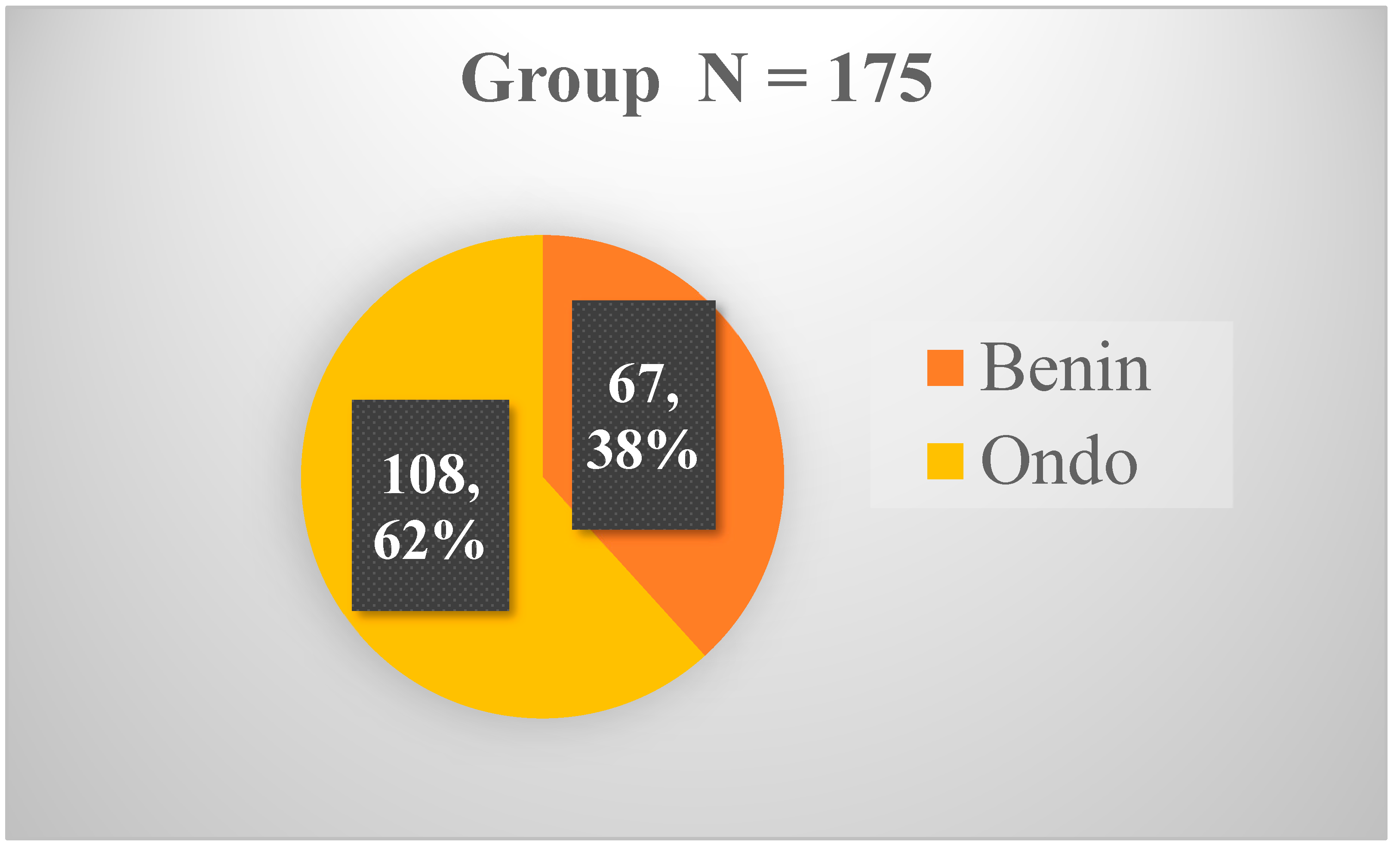

Table 1.
AGE DISTRIBUTION OF THE STUDY POPULATION.
| Age group (years) | N | % |
| 0-10 | 0 | 0.0 |
| 11-20 | 7 | 4.0 |
| 21-30 | 28 | 16.0 |
| 31-40 | 32 | 18.3 |
| 41-50 | 65 | 37.1 |
| 51-60 | 24 | 13.7 |
| 61 and above | 19 | 10.9 |
| Total | 175 | 100.0 |
Age range 0 – 100yrs, mean age 49.54 ± 12.6 years.
Figure 2.
SEX DISTRIBUTION OF THE STUDY POPULATION.
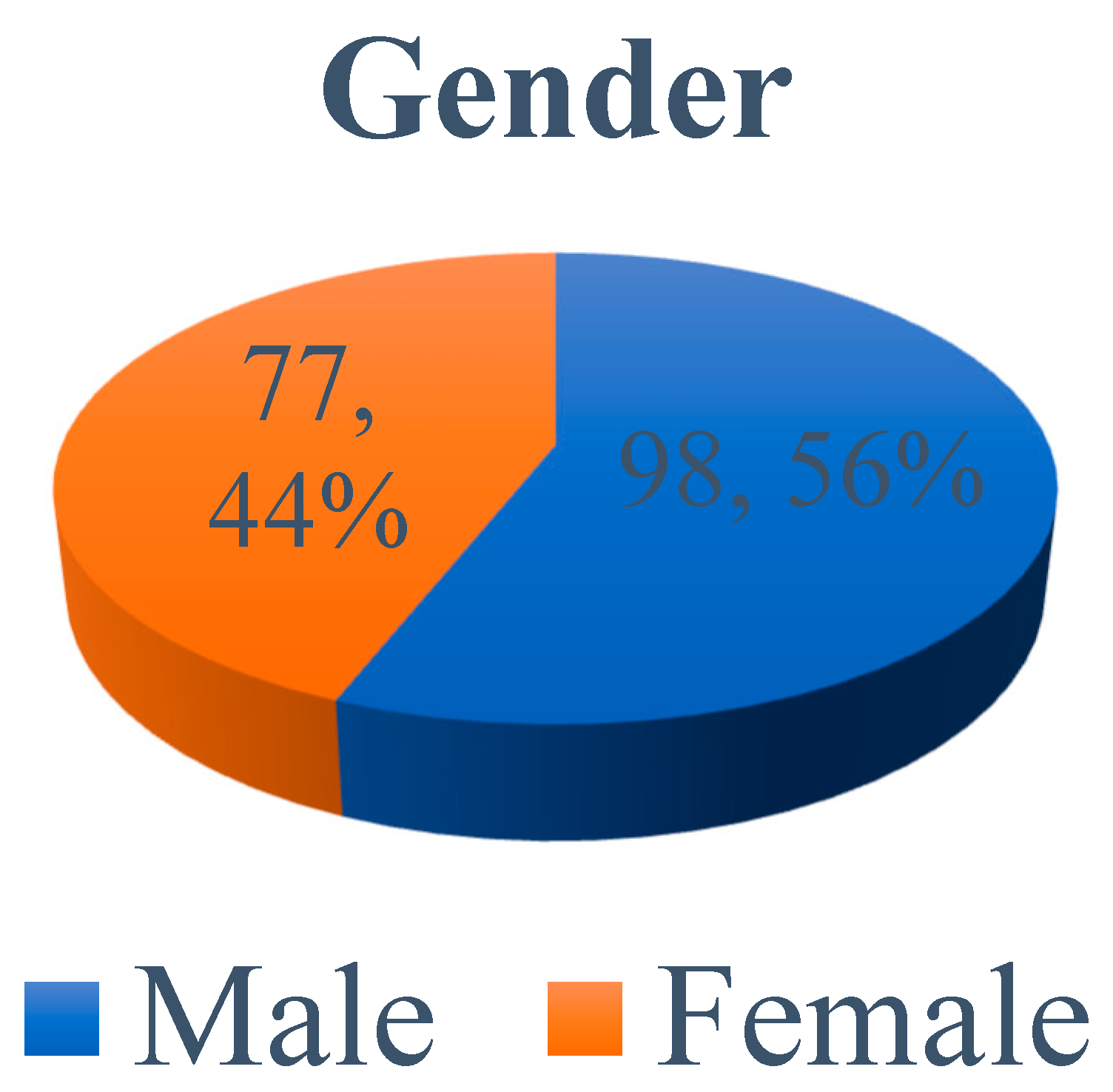
Table 2.
OCCUPATION OF THE STUDY POPULATION.
| Occupation | Benin N (%) |
Ondo N (%) |
Total N (%) |
|---|---|---|---|
| Driver | 20 (29.9) | 0 (0.0) | 20 (11.4) |
| Business | 9 (13.4) | 2 (1.9) | 11 (6.3) |
| Civil service | 16 (23.9) | 30 (27.8) | 46 (26.3) |
| Petit Trader | 9 (13.4) | 0 (0.0) | 9 (5.1) |
| Loader | 2 (3.0) | 0 (0.0) | 2 (1.1) |
| Student | 4 (6.0) | 41 (37.9) | 45 (25.7) |
| Pilot | 3 (4.5) | 0 (0.0) | 3 (1.7) |
| Mechanic | 1 (1.5) | 1 (0.9) | 2 (1.1) |
| Clergy | 2 (3.0) | 0 (0.0) | 2 (1.1) |
| Police officer | 1 (1.5) | 0 (0.0) | 1 (0.6) |
| Journalist | 0 (0.0) | 30 (27.8) | 30 (17.1) |
| Technician | 0 (0.0) | 1 (0.9) | 1 (0.6) |
| Politician | 0 (0.0) | 3 (2.8) | 3 (1.7) |
| Total | 67 (100) | 108 (100) | 175 (100) |
Figure 3.
THE STUDY POPULATION’S OCCUPATION.
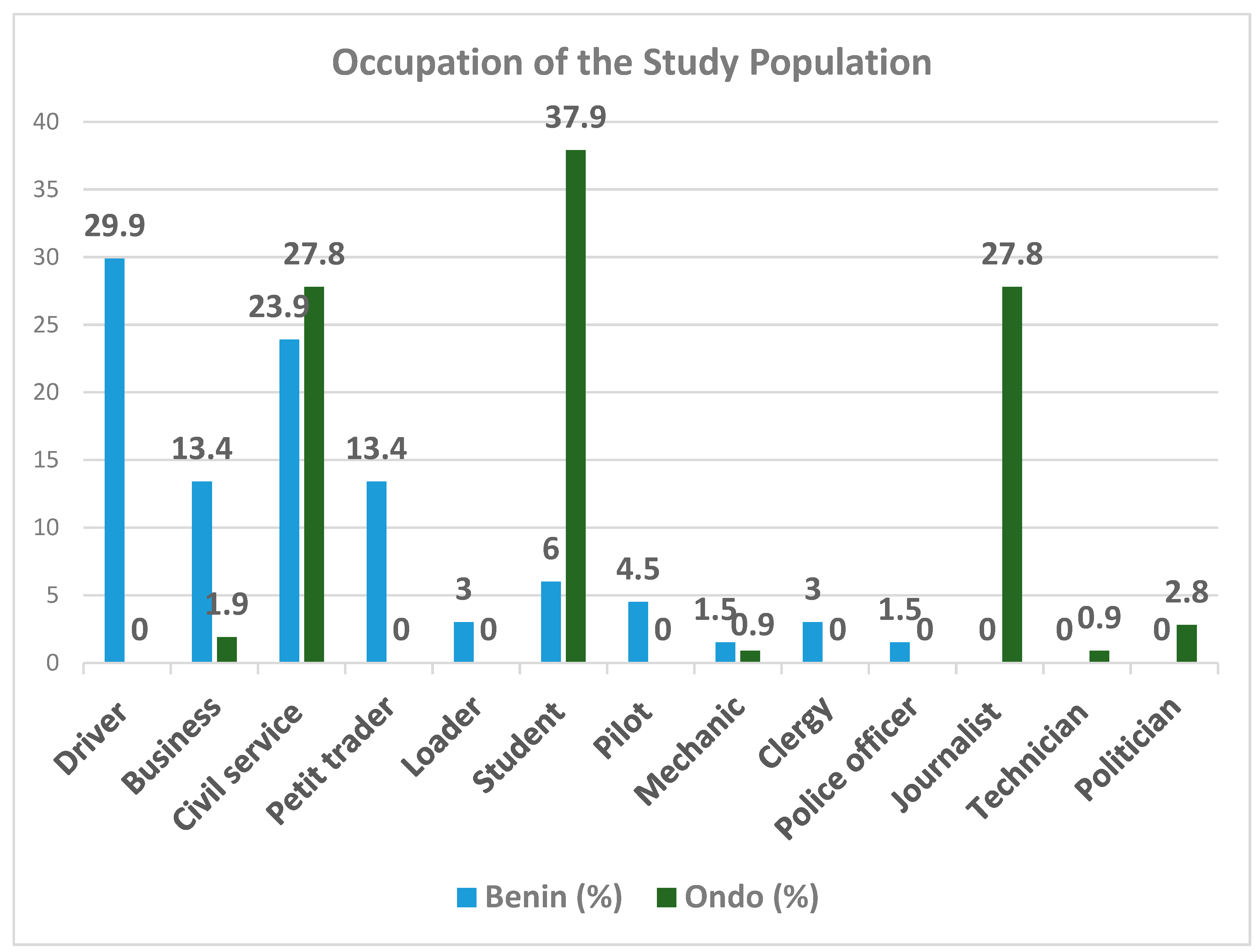
Table 3.
HEARWHO APP FINDINGS.
| HearWho App Values | BENIN | ONDO |
TOTAL N=350 ears |
Grading | Interpretation | ||
|
RIGHT (N=67) |
LEFT (N=67) |
RIGHT (N=108) |
LEFT (N=108) |
||||
| N (%) | N (%) | N (%) | N (%) | N (%) | |||
| 0 – 49 | 55 (82.1) | 56 (83.6) | 86 (79.6) | 74 (68.5) | 271 (77.4) | Abnormal hearing | Hearing loss |
| 50 - 69 | 7 (10.4) | 8 (11.9) | 10 (9.3) | 16 (14.8) | 41 (11.7) | Good | Normal hearing |
| 70 – 100 | 5 (7.5) | 3 (4.5) | 12 (11.1) | 18 (16.7) | 38 (10.9) | Excellent | Normal hearing |
| Total | 67 (100.0) | 67 (100.0) | 108 (100.0) | 108 (100.0) | 350 (100.0) | ||
Table 4.
OTOSCOPY.
| Variables | BENIN | ONDO | TOTAL N=350 ears | ||
|---|---|---|---|---|---|
| RIGHT (N=67) |
LEFT (N=67) |
RIGHT (N=108) |
LEFT (N=108) |
||
| Characteristics | N (%) | N (%) | N (%) | N (%) | N (%) |
| Shiny | 16 (23.9) | 23 (34.3) | 42 (38.9) | 42 (38.9) | 123 (35.0) |
| Wax | 4 (6.0) | 2 (3.0) | 15 (13.9) | 20 (18.5) | 41 (11.7) |
| Dull | 2 (3.0) | 39 (58.2) | 41 (38.0) | 38 (35.2) | 120 (34.3) |
| Scar | 1 (1.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.3) |
| Retracted | 43 (64.2) | 1 (1.5) | 6 (5.6) | 4 (3.7) | 54 (15.4) |
| Perforated TM | 0 (0.0) | 1 (1.5) | 1(0.9) | 0 (0.0) | 2 (0.6) |
| Narrow Canal | 1 (1.5) | 1 (1.5) | 0 (0.0) | 0 (0.0) | 2 (0.6) |
| Foreign body | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (2.8) | 3 (0.9) |
| Fungal debris | 0 (0.0) | 0 (0.0) | 1 (0.9)) | 1 (0.9) | 2 (0.6) |
| Aural polyp | 0 (0.0) | 0 (0.0) | 1 (0.9) | 0 (0.0) | 1 (0.3) |
| Inflamed canal | 0 (0.0) | 0 (0.0) | 1 (0.9) | 0 (0.0) | 1 (0.3) |
| Total | 67 (100.0) | 67 (100.0) | 108 (100.0) | 108 (100.0) | 350 (100.0) |
| Chi square | 0.940 | 0.027 | 0.030 | 0.022 | |
Table 5.
RELATIONSHIP BETWEEN SAMPLE CHARACTERISTICS AND OTOSCOPY.
| Characteristics | Otoscopy | X2 Value | df | Sig. | Remark |
|---|---|---|---|---|---|
|
Age |
Right Ear | 21.666 | 25 | .655 | Not significant |
| Left Ear | 42.577 | 25 | .016 | Significant | |
|
Sex Male/Female |
Right Ear | 3.883 | 5 | .566 | Not significant |
| Left Ear | 5.537 | 5 | .354 | Not significant | |
| Occupation | Right Ear | 39.410 | 45 | .707 | Not significant |
| Left Ear | 41.003 | 45 | .642 | Not significant |
Table 6.
RELATIONSHIP BETWEEN SAMPLE CHARACTERISTICS AND HEARWHO APP IN BENIN CITY.
| Characteristics | X2 Value | Df | Sig. | Remark |
| Location | 37.158 | 12 | .000 | Significant |
| Age | 22.633 | 20 | .307 | Not significant |
| Sex | .676 | 4 | .954 | Not significant |
| Occupation | 33.618 | 36 | .582 | Not significant |
Table 7.
RELATIONSHIP BETWEEN SAMPLE CHARACTERISTICS AND HEARWHO APP IN ONDO CITY.
| Characteristics | X2 Value | Df | Sig. | Remark |
| Location | 25.199 | 12 | .014 | Significant |
| Age | 27.474 | 20 | .122 | Not significant |
| Sex | 4.361 | 4 | .359 | Not significant |
| Occupation | 41.134 | 36 | .256 | Not significant |
Table 8.
KAPPA RESULT.
| N = 350 | TOTAL (N = 350) | |||
| FINDINGS | RIGHT (N-175) | LEFT (N-175) | ||
|
HEARWHO APP Normal findings Abnormal findings |
N (%) | N (%) | ||
| 34 (19.4) | 45 (25.7) | 79 (22.6) | Normal hearing | |
| 141 (80.6) | 130 (74.3) | 271 (77.4) | Hearing loss | |
| TOTAL | 175 (100.0) | 175 (100.0) | 350 (100.0) | |
|
OTOSCOPY Normal findings Abnormal findings |
N (%) | N (%) | ||
| 58 (33.1)) | 65 (37.1) | 123 (35.0) | Normal ear | |
| 117 (66.9) | 110 (62.9) | 227 (65.0) | Ear pathology | |
| TOTAL | 175 (100.0) | 175 (100.0) | 350 (100.0) | |
| KAPPA | 0.914 | 0.000 | ||
Kappa result interpretation according to Cohen19: Values ≤ 0 indicates No agreement; 0.01– 0.20 = None to slight agreement, 0.21– 0.40 = Fair agreement, 0.41– 0.60 = Moderate agreement, 0.61–0.80 = Substantial agreement, 0.81–1.00 = Almost perfect agreement.
Table 9.
TREATMENT / SOLUTIONS PROFFERED N = 350.
| S/N | Treatment Rendered | N (%) |
|---|---|---|
| 1 | Ear syringing | 43 (12.3_ |
| 2 | Foreign body removal | 3 (0.86) |
| 3 | Ear dressing | 3 (0.86) |
| 4 | Ear toileting | 1 (0.29) |
| 5 | Counselling | 9 (2.57) |
| 6 | Reassurance | 35 (10.0) |
| 7 | Referrals for follow up and further evaluations | |
| Otological conditions | 350 (100.0) | |
| Others (Nasal polyps, sore throat, Non otorhinolaryngological conditions) |
9 (2.57) |
4. Discussion
4.1. Demography
Comparing the two southern regions, there were more response from Ondo state than Edo state. Although three hundred and fourteen (314) individuals participated in the awareness and health education activities, only sixty seven completed the HearWHO test and had their ears examined in Benin City. There were a lot of non challant attitude exhibited by the individual at the parks especially hawkers who were selling market products. They saw the programme as a waste of time which will delay their sales. They inadvertently, deprived themselves the opportunity for free medical check, detection of otorhinolaryngological disease conditions and their possible treatment. Non challancy and ignorance is a major drawback in community studies. Similar findings were reported by Cathy et al (2023) on people who injects drugs on themselves but refused screening Hepatitis C infection.20
The predominance of the young adults in the study is not surprising as use of technologically driven screening is embraced by the younger generations compared to the elderly. However, agreeing with Pratten et al., (2005), no one should be left behind, whether young or old, in the knowledge and use of digital aids.21, 22, 23 This will further help to ensure universal health coverage for all (Sustainable Developmental Goal, SDG – 3).
There was a preponderance of civil servants in this study. This may likely be attributed to their higher level of education. However, associating occupation with both Otoscopy and HearWHO App results were not statistically significant.
Though the ambient noise in the different locations were higher in the parks, association of the demographic characteristics with all the locations was statistically significant. However, there is inbuilt tolerance of the HearWHO App for noisy environment.
4.2. Challenges
Apart from the non challancy of the dwellers, other limitations and challenges abound.
As recorded by Ibrahim et al., (2020), COVID -19 pandemic lock down in Nigeria commenced from 30th March, 2020 to 4th May, 2020.24 This lock down consequently retarded the progress of the research study during the period. Post lock down, negative attitudes of the individuals in the study communities heightened. Perception of most of them was that they are to be used as part of pilot sample for COVID – 19 studies and thus, excluded themselves from HearWHO App test and Otoscopic examination. This ideology was deep seated in some individuals. They were able to convince some interested ones to keep off from the examination aspect of the research programme irrespective of their participation in the awareness and health education section. One would actually not blame them as the impact of the COVID - 19 pandemic and lockdown was overwhelming in Nigeria which instilled a lot of fear and uncertainties in the communities.24
Some interested children who were welcomed could not complete the HearWHO App test. They lost interest in the process of the test and ended up playing with the research instruments.
In addition, individuals with special needs who were mentally retarded, brought by their relatives and caregivers for the screening study, could not participate fully due to their mental challenges.
During the study, some non-lettered participants were unable to perform the HearWHO App test as they could not identify the figures.
All the fore mentioned individuals who had some challenges and could not complete the study were excluded.
Furthermore, most of the participants who had abnormal results and were referred for further evaluations, were lost to follow up. Despite the efforts on contact tracing, some who were eventually reached declared that they were no longer interested in follow up, mostly due to time constrains. This reflects the place of misappropriation of priorities in the communities, buttressing the need for more awareness campaigns. 8
4.3. Discrepancy between HearWHO App findings and Otoscopic findings
Some individuals that had abnormal HearWHO App result had normal Otoscopic findings which necessitated further evaluation for inner ear pathologies. This reflects the need for regular ear and hearing check for prompt treatment.25
Non availability of Impedance audiometer and pure tone audiometer. Discrepancy between HearWHO App finding and Otoscopy needed confirmation, but audiometers were not available. Most of the patients referred for further evaluation were lost to follow up.
This therefore reveals the need for mobile audiometers for holistic community services to improve the quality of life of people. 26
4.4. Solutions proffered
All the participants who had abnormal otological and HearWHO App results were referred to the Ear Nose and Throat Clinic of University of Medical Sciences Teaching Hospital, Ondo for further evaluation and management. This also ensures sustained normal hearing, preventing hearing loss with frequent education and counselling on risk factors of hearing loss, during follow up visits. 27
Although the scope of this study is on otology and audiology, individuals who had other otorhinolaryngological conditions such as nasal polyps, were likewise referred for appropriate treatment. In addition, some of the participants had non – Otorhinolaryngological conditions and were referred to the appropriate Specialist for expert management. This re-emphasizes the fact reported by Akpalaba and Onyeagwara (2015) that some individuals both in urban and rural areas are not aware of what to do concerning their health conditions. This research study gave them the ample opportunity to find solution to their ailments.8. 27, 28
5. Conclusion
Hearing loss and otological disorders abound in Benin and Ondo communities at the prevalence of 77.4% and 65.0%, respectively. The HearWHO App abnormal findings agreed with the abnormal otological findings. The findings in the right ear had almost perfect agreement as validated by the Kappa result.19
6. Recommendations
Based on the challenges encountered in this research study, there is therefore need to develop additional Apps or modify the HearWHO App to embrace young children, non-lettered individuals and individuals with special needs. It is therefore a call to all the general public, to put this App in use for validation in different cultures, ethnic groups and languages. This will help to identify other challenges of the App for further modifications or changes. These will help to ensure universal health coverage for all and thus achieve the aim of the Sustainable Developmental Goal -3 (SDG -3). Hence, creating a bigger picture, granting a better Future today and making great impact with mobile technology.
References
- Emmett SD, Platt A, Gallo JJ, Labrique AB, Wang NY, Inglis-Jenson M, Jenson CD, Hofstetter P, Hicks KL, Ross AA, Egger JR. Prevalence of Childhood Hearing Loss in Rural Alaska. Ear and Hearing. 2023 Jun 8:10-97. [CrossRef]
- Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al.; GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016. October 8;388(10053):1545–1602.
- Resolution WHA70.13. Prevention of deafness and hearing loss. In: Seventieth World Health Assembly, Geneva, 31 May 2017. Geneva: World Health Organization; 2017. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_R13-en.pdf?ua=1.
- Wilson BS, Tucci DL, Merson MH, O’Donoghue GM. Global hearing health care: new findings and perspectives. Lancet. 2017. December 2;390(10111):2503–15. [PubMed] [Google Scholar]. [CrossRef]
- WHO. Deafness and Hearing loss: Key facts. Newsroom. 27 February, 2023.
- Shan A, Ting JS, Price C, Goman AM, Willink A, Reed NS, Nieman CL. Hearing loss and employment: a systematic review of the association between hearing loss and employment among adults. The Journal of Laryngology & Otology. 2020 May; 134(5):387-97. [CrossRef]
- Kodiya AM, Afolabi OA, Ahmad BM. The burden of hearing loss in Kaduna, Nigeria: a 4-year study at the National Ear Care Centre. Ear Nose Throat J. 2012 Apr; 91(4):156-63. [CrossRef]
- Akpalaba I.O, Onyeagwara C.N., Community Otorhinolaryngological service in a group of Schools in South- South Nigeria. Nigerian journal of Otorhinolaryngology, 2010 - 2015; 8-12.
- Tamblay N, Torrente MC, Huidobro B, Tapia-Mora D, Anabalon K, Polack S, Bright T. Prevalence, risk factors and causes of hearing loss among adults 50 years and older in Santiago, Chile: Results from a rapid assessment of hearing loss survey. International journal of audiology. 2023 Jan 3; 62(1):53-61. [CrossRef]
- Khan, SA. Importance of hearing and hearing loss treatment & recovery. IJSA. 2022; 3(1):14-6.
- De Raeve L, Cumpăt MC, van Loo A, Costa IM, Matos MA, Dias JC, Mârțu C, Cavaleriu B, Gherguț A, Maftei A, Tudorean OC. Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants. Medicina. 2023 Jul 24;59(7):1354. [CrossRef]
- Swanepoel DW, De Sousa KC, Smits C, Moore DR. Mobile applications to detect hearing impairment: opportunities and challenges. Bulletin of the World Health Organization. 2019: 10; 97(10):717. [CrossRef]
- Yousuf Hussein S, Swanepoel W, Mahomed F, Biagio de Jager L. Community-based hearing screening for young children using an mHealth service-delivery model. Glob Health Action. 2018;11(1):1467077. [CrossRef]
- Case study by UNESCO-Pearson initiative for literacy: improved livelihoods in a digital World. Paris: United Nations Educational, Scientific and Cultural Organization; 2017.
- Mobile industry impact report: sustainable development goals. London: Groupe Spéciale Mobile Association; 2018. Available from: https://www.gsmaintelligence.com/research/?file=ecf0a523bfb1c9841147a335cac9f6a7&download.
- Oluwakemi Ololade Odukoya, Adebola A Adejimi, Brenda Isikekpei, Chris S Jim, Akin Osibogun, Folasade Tolulope Ogunsola. Epidemiological trends of coronavirus disease 2019 in Nigeria; 2020 : 27 (4): 271 – 279. [CrossRef]
- Hansson I, Buratti S, Allwood CM. Experts' and Novices' Perception of Ignorance and Knowledge in Different Research Disciplines and Its Relation to Belief in Certainty of Knowledge. Front Psychol. 2017; 8:377. Published 2017 Mar 17. [CrossRef]
- Singh KP, Prasad A. A Study of Different Parameters In Complicated Versus Uncomplicated Chronic Suppurative Otitis Media. Int J Acad Med Pharm. 2023; 5(4):1695-7. [CrossRef]
- Więckowska B, Kubiak KB, Jóźwiak P, Moryson W, Stawińska-Witoszyńska B. Cohen’s Kappa Coefficient as a Measure to Assess Classification Improvement following the Addition of a New Marker to a Regression Model. International Journal of Environmental Research and Public Health. 2022 Aug 17;19(16):10213. [CrossRef]
- Cathy R. Balsom, Alison Farrell, Deborah V Kelly et al. Barriers and Enablers to Testing for Hepatitis C Infection in People Who Inject Drugs – A Scoping Review of the Qualitative Evidence, 14 February 2023, PREPRINT (Version 1) available at Research Square. [CrossRef]
- Pratten, Susan; Schindel Martn, Lori Dr.; Ryan, Ellen Dr.; Anas, Ann; Spadafora, Pat; and Hart, Rebecca, "Older Adults Embracing Technology: Leave No One Behind" (2005). Publications and Scholarship. 15. https://source.sheridancollege.ca/centres_elder_publ/15.
- Mustafa MW, Abdelrahim AG, Khodary MM, Aref ZF. Restoration of quality of life in elderly with hearing loss. International Journal of Otorhinolaryngology and Head and Neck Surgery. 2023 Jan;9(1):1.
- Agarwal S, LeFevre AE, Lee J, L’Engle K, Mehl G, Sinha C, et al.; WHO mHealth Technical Evidence Review Group. Guidelines for reporting of health interventions using mobile phones: mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ. 2016. March 17;352:i1174. [CrossRef]
- Ibrahim RL, Ajide KB, Olatunde Julius O. Easing of lockdown measures in Nigeria: Implications for the healthcare system. Health Policy Technol. 2020;9(4):399-404. [CrossRef]
- Phillips OR, Baguley DM, Pearson SE, Akeroyd MA. The long-term impacts of hearing loss, tinnitus and poor balance on the quality of life of people living with and beyond cancer after platinum-based chemotherapy: a literature review. Journal of Cancer Survivorship. 2023 Jan 13:1-9.
- Sarah M. Theodoroff, M. Samantha Lewis, Robert L. Folmer, James A. Henry, Kathleen F. Carlson, Hearing Impairment and Tinnitus: Prevalence, Risk Factors, and Outcomes in US Service Members and Veterans Deployed to the Iraq and Afghanistan Wars, Epidemiologic Reviews, Volume 37, Issue 1, 2015, Pages 71–85. [CrossRef]
- Muhammad, F. , Abdulkareem J.H., Chowdhury A.A. Major public health problems in Nigeria: a review. Southeast Asia J Public Health. 2017;7(1):6–11. [CrossRef]
- Dillard LK, Nelson-Bakkum ER, Walsh MC, Schultz A. Self-reported hearing loss is associated with poorer perceived health care access, timeliness, satisfaction, and quality: Findings from the Survey of the Health of Wisconsin. Disability and Health Journal. 2023; 1;16(1):101394. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



