
Submitted:
15 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
Helicobacter pylori (H. pylori) is a Gram-negative bacterium that colonizes the gastric mucosa and is associated with various gastrointestinal disorders. H. pylori is a pervasive pathogen, infecting nearly 50% of the world's population, and presents a substantial concern due to its link with gastric cancer, ranking as the third most common cause of global cancer-related mortality. This review article provides an updated and comprehensive overview of the current understanding of H. pylori infection, focusing on its pathogenesis, diagnosis, and treatment strategies. The intricate mechanisms underlying its pathogenesis, including virulence factors and host interactions, are discussed in detail. Diagnostic methods, ranging from traditional techniques to advanced molecular approaches, are explored, highlighting their strengths and limitations. The evolving landscape of treatment strategies, including antibiotic regimens and emerging therapeutic approaches, is thoroughly examined. Through a critical synthesis of recent research findings, this article offers valuable insights into the contemporary knowledge of Helicobacter pylori infection, guiding both clinicians and researchers toward effective management and future directions in combating this global health challenge.
Keywords:
Pathogenesis
; Treatment strategies
; Virulence factors
; Triple therapy
; Antibiotic resistance
; Diagnostic tools.
1. Introduction
Helicobacter pylori, an ubiquitous, microaerophilic, spiral-shaped, gram-negative bacterium residing in the human stomach, has profoundly impacted the landscape of gastroenterology and infectious diseases since its discovery in 1982 [1]. Before its identification, peptic ulcer disease was primarily attributed to stress and dietary factors, fundamentally altering our understanding of its aetiology. This revolutionary discovery earned Barry J. Marshall and Robin Warren the Nobel Prize in Physiology or Medicine in 2005 and laid the foundation for a comprehensive investigation into H. pylori's role in various gastrointestinal disorders [2]. As the scientific community has continued to unravel the complexities of this pathogen, the field of H. pylori research has witnessed remarkable advancements. H. pylori colonizes the gastric mucosa of approximately half the world's population, making it one of the most prevalent human infections [3]. Its ability to establish a persistent and often lifelong infection in the stomach lining has earned it a reputation as a formidable pathogen. The bacterium's remarkable adaptability to the acidic and inhospitable gastric environment has led to a plethora of host responses and pathological outcomes [4,5]. From its initial association with peptic ulcers, our understanding has expanded to include its role in gastritis, duodenal ulcers, gastric cancer, mucoid-associated lymphoid tissue (MALT) lymphoma, and a range of extra-gastric conditions including neurological, ocular, hematologic, cardiovascular and dermatological diseases, which afflict millions worldwide and have substantial economic and healthcare burdens [5,6,7]. The complex interplay between H. pylori and its human host has spurred intensive research efforts to elucidate its pathogenesis, develop accurate diagnostic methods, and refine treatment strategies. The significance of H. pylori lies not only in its prevalence but also in its wide-ranging impact on human health. Additionally, H. pylori is recognized as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC), the only bacterium in the list, with a strong association with gastric adenocarcinoma, one of the leading causes of cancer-related deaths globally [8]. Furthermore, the bacterium's implications extend beyond the stomach, with links to autoimmune disorders, cardiovascular diseases, and metabolic syndromes being explored. Understanding the pathogenesis, accurate diagnosis, and effective management of H. pylori infections are paramount in mitigating its impact on public health.
Significance of study
H. pylori is highly correlated with duodenal ulcers (in up to 90% of cases), gastric ulcers (in approximately 80%), and malignancies, contributing to conditions such as mucosa-associated lymphoid tissue (MALT) lymphoma and gastric cancer (seen in as many as 90% of cases) [5,9,10]. In 2014, the World Health Organization (WHO) advocated for the eradication of H. pylori to reduce global gastric cancer mortality, and in 2017, it identified clarithromycin-resistant H. pylori strains as a significant public health threat. This review provides an overview of H. pylori 's disease characteristics, encompassing epidemiology and clinical presentation, and discusses the latest advances in evaluating and managing this infection. A timeline of significant events related to H. pylori discovery and management of infection is represented in Figure 1.
This review, endeavors to synthesize the wealth of knowledge accumulated in the field of H. pylori research. Our primary objectives are to provide a comprehensive overview of the bacterium's pathogenesis, including the molecular mechanisms behind its infection, its role in triggering inflammatory responses, and its associations with gastrointestinal diseases. We will also explore the latest advancements in diagnostic techniques, emphasizing the importance of accuracy and efficiency in detection. In the context of a changing landscape of antibiotic resistance, we will assess various treatment strategies, including antibiotic therapy, proton pump inhibitors, and emerging therapeutic options. Moreover, we will highlight the concept of personalized medicine as a promising approach to combat H. pylori infections. By offering critical insights into H. pylori's contemporary landscape and future directions in its management, this review aims to serve as a comprehensive resource for clinicians, researchers, and healthcare professionals engaged in the fight against this clinically significant pathogen.
2. Pathogenesis of Helicobacter pylori
Pathogenesis of H. pylori may be studied under three distinct stages- attachment to and colonization of the gastric mucosa, triggering and evading immune responses of the host, and finally, establishment of the disease [11].
2.1. Molecular Mechanisms of Infection
2.1.1. Attachment and Colonisation
The molecular mechanisms orchestrating H. pylori infections are sophisticated processes crucial for the bacterium's successful establishment in the gastric mucosa. At the forefront of infection initiation is H. pylori's adhesion and colonization strategies. Colonisation of the pathogen is initiated firstly by the chemotaxis of the bacterial cells to the target site, which is mediated by the presence of certain receptors present on the host cells, mainly belonging to the Tlp family [12]. These receptors are known to be triggered by the presence of chemical signals including urea, lactic acid, ROS species, and gastric juice, facilitating chemotactic responses towards the gastric epithelium [12]. Flagellar motility allows H. pylori to navigate through the mucous layer and reach the gastric epithelium, contributing to its ability to firmly adhere to and colonize the mucosa [13]. Additionally, H. pylori can form biofilms, structured bacterial communities embedded in an extracellular matrix, enhancing adherence and providing protection against host defences and treatment therapies [14]. Furthermore, the bacterial outer membrane proteins aka the surface adhesins, including BabA, SabA, AlpA/B, and OipA, enable the bacterium to adhere to gastric epithelial cells, paving the way for its persistence within the stomach [15].
2.1.2. Production of virulence factors
Various virulence factors, including those involved in motility, adhesion, urease and cytotoxin production are essential for the pathogenesis of the bacterium [16].
2.1.3. CagA and VacA
Upon attachment, H. pylori engages in intricate host interactions, deploying an arsenal of virulence factors that manipulate host cell signaling. Among these, the CagA (cytotoxin associated gene A) pathogenicity island is the main orchestrator [17]. Injected into host cells via a type IV secretion system (T4SS), CagA triggers a cascade of events, disrupting cellular functions and contributing to the development of gastric pathologies [18]. CagA undergoes tyrosine phosphorylation, leading to the activation of various cellular signaling pathways [19]. This includes the aberrant activation of the mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K) pathways [20, 21]. The dysregulation of these pathways contributes to cellular morphological changes, disruption of cell polarity, and the initiation of oncogenic processes. This molecular hijacking of host cell signaling is a hallmark of H. pylori induced pathogenesis [22].
The vacuolating toxin,VacA, is another key virulence factor, that exhibits multifaceted effects on host cells [23]. As the name suggests, VacA disrupts the integrity of the gastric epithelial barrier by forming channels or pores in the cell membrane, leading to increased permeability [16]. Within host cells, VacA modulates apoptotic pathways, leading to both pro- and anti-apoptotic effects depending on the cell type and environmental conditions. Furthermore, VacA toxin contributes to the formation of vacuoles within host cells, impacting cellular structure and function [24]. This toxin also interferes with and evades the immune responses by affecting the function of T cells and other immune cells. The consequences of these molecular interactions extend to the host's immune response [10,25]. H. pylori induces a chronic inflammatory state marked by the release of multiple pro-inflammatory cytokines such as IL-8, IL-1α. IL-1β, and TNF α among others, and the recruitment of immune cells to the gastric mucosa [26]. This inflammatory milieu is closely associated with the development of peptic ulcers, as the delicate balance between protective mucosal mechanisms and bacterial aggression is disrupted [27].
The CagA and VacA proteins work together to induce H. pylori associated gastric cancer. A study conducted by Abdullah et al., (2019) showed the functional interplay between the two oncoproteins, whereby the absence of VacA aids the host’s system is able to degrade CagA, thereby preventing the accumulation of CagA in the gastric epithelial cells [28]. Importantly, the long-term consequences of H. pylori infection include an increased risk of gastric cancer. Chronic inflammation, coupled with the release of genotoxins and the induction of genetic instability, creates an environment conducive to oncogenesis and other gastric malignancies [29]. The interplay between H. pylori virulence factors such as CagA, VacA and OipA, host genetic susceptibility, and environmental factors contributes to the complexity of this association [30]. Understanding these intricate molecular mechanisms is paramount for developing targeted therapeutic approaches and preventive strategies against H. pylori infections. Advances in elucidating these processes provide critical insights into the pathogenesis of H. pylori-related diseases and inform the development of novel interventions to mitigate the associated health risks.
2.1.4. Urease production
Urease is one of the more abundantly produced proteins expressed by the pathogen, accounting for almost 15% of the total protein of the bacterium [31]. The production of urease is a characteristic feature of H. pylori and is widely used in the diagnosis of the infection as well [32]. Several studies in this regard have proved the role of urease in enabling the survival of the bacterium in the extremely low-pH acidic environment of the stomach, by breaking down urea into ammonia and carbon dioxide, thereby forming a pH-neutral environment around the bacterial cells (Figure 2). The hydrolysis of urea into ammonia also provides the pathogen with a steady source of nitrogen [33, 34].
2.2. Immune system modulation and induction of inflammatory responses
The immune response to H. pylori infection is a dynamic interplay between the bacterial factors and the host's immune system [35]. The pathogenesis of H. pylori infections unfolds through a complex and multifaceted localised gastric inflammatory response [36]. In the innate immune phase, H. pylori induces a chronic inflammatory response in the gastric mucosa, mediated by the lipopolysaccharides and the peptidoglycan of the cell wall, and characterized by the release of neutrophils, macrophages, lymphocytes, and the pro-inflammatory cytokines (such as interleukin-1β, interleukin-6, and tumor necrosis factor-α) and the recruitment of immune cells [37, 38]
Innate immune activation, spurred by bacterial components like lipopolysaccharide and peptidoglycan, further amplifies the inflammatory cascade through pattern recognition receptors such as Toll-like receptors [39]. This sets the stage for the adaptive immune response, where CD4+ T-helper cells play a crucial role, particularly in promoting a Th1 response characterized by interferon-gamma secretion. Regulatory T cells are recruited, contributing to immune suppression, while B-cells produce antibodies against H. pylori [40] [41]. However, the bacterium employs immune evasion strategies, such as urease production, antigenic variation, inhibition of recognition by PRRs, and molecular mimicry, to subvert recognition and signalling by T and B cells [42].
The sustained presence of H. pylori leads to chronic inflammation, causing ongoing tissue damage and remodelling. Gastric epithelial cells undergo changes in turnover, with increased proliferation contributing to mucosal damage and ulcer formation [43]. Concurrently, disruptions in tight junctions compromise mucosal barrier integrity, facilitating H. pylori infiltration into deeper mucosal layers [44]. The sustained release of inflammatory mediators, coupled with the induction of genetic instability, creates an environment conducive to oncogenesis ([45]. This sustained inflammation is a central component of H. pylori associated diseases and is implicated in the development of peptic ulcers and gastric cancer [46]. However, in the neighboring non-infected gastric cells, an adaptive immune response is triggered which prompts increased survival and proliferation, ultimately leading to the development of precancerous lesions in the gastric epithelium [47].
2.3. Modulation of Mucin Production
H. pylori influences mucin production in the gastric mucosa, impacting the protective mucous layer. The carbohydrate component of the mucins act as ligands that enable the binding of the bacterium to the gastric mucosal lining [48]. The bacterium can alter the expression of mucin genes and interact with mucins like MUC5A and MUC1 directly, resulting in the inhibition or impairment in mucin turnover [49]. Changes in mucin production influence the composition of the mucosal glycocalyx, affecting the adherence and colonization of H. pylori. Moreover, this modulation of mucin production contributes to the bacterium's ability to evade host defenses and establish persistent infections [50].
Unraveling the nuances of immune system modulation in H. pylori infection is paramount for devising effective therapeutic interventions and preventive strategies in the ongoing pursuit of managing associated diseases. Ongoing research continues to unveil the complexities of this host-pathogen interaction.
3. Disease Associations
H. pylori mainly infects the mucosal layer of the stomach, owing to its ability to adapt to the acidic environment by neutralizing the local environment, owing to the production of urease and other factors [51]. Although the exact mode of transmission remains widely unclear, it is usually transmitted through the oral-fecal route, or the gastric-oral, or oral-oral route, and may spread through ingestion of contaminated food and water. Tendencies for vertical or parental transfer have also been reported [52, 53] The infection is usually acquired during childhood, and only about 20-30% of the infected people actually show symptoms of infection, i.e., the infection is widely asymptomatic [52,54] As a result, undiagnosed infections may lead to chronic inflammations including non-atrophic and eventually, atrophic gastritis, ie., inflammation of the gastric mucosa. Such chronic gastritis has often been linked with the development of gastric cancer, including adenarcinomas and MALT lymphomas [55, 56]. Approximately 10% of the infected individuals may develop peptic ulcers, while gastric adenocarcinoma is reportedly found to occur in almost 3% of the infected patients. H. pylori is also commonly associated with a number of gastric issues including dyspepsia, commonly characterized by pain or discomfort in the abdomen [57]. Studies in this regard have frequently pointed towards a link between H. pylori infection and dyspepsia, as eradication-based studies have clearly demonstrated a reduction in functional dyspeptic symptoms [4, 58]. H. pylori has frequently been credited as one of two the major risk factors (the other being NSAIDs) for the development of peptic ulcer disease (PUD), characterized by the formation of gastric lesions in the duodenum and the stomach, due to penetration of the muscular mucosa [59-60].
Gastric cancer is reported to be the third most common type of cancer globally [61]. H. pylori is notoriously well-recognised for its involvement in the genesis of gastric cancer. In fact, more than 90% cases of all non-cardia gastric cancer cases are caused by H. pylori infection [55]. Various metanalytical studies in this regard have confirmed the correlation between H. pylori infection and the development of noncardia GC [62]. The CagA cytotoxin discussed in the previous section is considered to be the first bacterial oncoprotein integrally associated with the development of gastric carcinoma among infected individuals [63]. A range of host factors, including the interleukins (IL-β) and the TNF are known to increase the risk of noncardia GC [64] In general, the beta-catenin signaling pathway has been linked to the onset of carcinogenesis post-infection by H. pylori [65]. Inflammation of the gastric epithelium and factors including cyclooxygenase, prostaglandins, disrupted cadherin-catenin interactions, etc. are reported to play a role in the development of the gastric adenocarcinoma [66].
4. Diagnosis of Helicobacter pylori Infections
Most cases of H. pylori infections are asymptomatic, therefore often going unrecognized, leading to the development of chronic gastritis, which may further lead to the development of gastric cancer [67, 68]. Additionally, H. pylori infection may manifest itself in the form of mild dyspepsia, and occasionally, more serious conditions such as intestinal metaplasia, peptic ulcers, and MALT lymphomas [69]. The American College of Gastroenterology recommends testing for H. pylori under conditions of PUD, MALT lymphomas, dyspepsia, and cases of gastric cancer [70]. Alarm symptoms usually include vomiting, GI bleeding, dysphagia, and weight loss among others [71].
The generally accepted diagnosis method involves a test-and-treat approach, and various invasive and non-invasive tests are available to detect H. pylori infections, the choice depending upon the patient’s age and their symptoms [72]. Invasive tests involve procedures such as endoscopy, histology, rapid urease test, and cultural tests, while non-invasive tests include breath tests and faecal tests among others [73, 74]. Although on the whole, most experts are of the opinion that no single test can be considered the gold standard for the diagnosis of H. pylori mediated gastritis, certain tests are considered more reliable and preferable over others. These include the urea breath test (UBT) and histological examinations post biopsy [75]. While making a choice for the detection method, a clear analysis of the intent, the specificity, sensitivity, availability, costs, and limitations must be made [76]. Keeping in mind the individual shortcomings of each of the invasive and non-invasive examinations, a combination-based approach such as RUT combined with histological examination and bacterial culture, for the detection of H. pylori infection may be a more suitable approach, for an accurate diagnosis [77]. Such an effective diagnosis and eradication can further prevent the progression of gastric carcinogenesis and also has the potential to reverse unregulated cell growth [78].
4.1. Non-invasive tests
4.1.1. Serological Assays
Serological tests are considered to be the more accurate of the non-invasive methods to diagnose a suspected case of H. pylori infection. These tests are based on the detection of pathogen-specific antibodies in bodily fluids such as the serum, saliva, or urine samples [79]. Serological examinations relying on the presence of anti-H. pylori IgG antibody are commonly employed for an accurate diagnosis of suspected infection. Additionally, other antigenic proteins including CagA, Omp, UreA and VacA are effective candidates to confirm infection [73] Advantages of using serological tests for the detection of H. pylori infection include the accuracy of the tests, and that such tests are unaffected by the use of PPI and antibiotics, which can often cause false negative results in case of other diagnostic tests [80]. However, serology-based detection is not reliable for confirmation of eradication, as the H. pylori-specific antibodies may persist even after eradication [7].
4.1.2. Urea Breath Test (UBT)
The 13C urea breath test (UBT) relies on the characteristic production of ammonia and carbon dioxide following the hydrolysis of urea by the enzyme urease [75]. The fact that urease is not produced by mammalian cells, is suitably considered a sign of H. pylori infection, as this microbe can effectively use urease to degrade urea [81]. Essentially this test involves a C13 or C14 isotope-containing urea substrate, which is ingested by the patient. Exhalation samples of the patient both, before and after ingestion are collected to detect the infection [82]. The use of radio-labelled (14C-UBT) or non-radiolabelled (13C-UBT) carbon isotope in the urea substrate helps in the detection of labelled CO2 after exhalation using analytical techniques like mass spectrometry, indicating the presence of the pathogenic bacterium [82]. Preparation for this test involves discontinuation of antibiotics and intake of bismuth compounds and other such drugs which may reduce the activity of bacterial urease, to avoid chances of a false negative result. The UBT is a reliable and highly sensitive and specific test, with sensitivity above 95% and specificity above 93% [83]. Given its principle, easy procedure and reliability, this test is suitable in the absence of alarm symptoms (Vomiting, Bleeding, Abdominal mass, and Dysphagia-VBAD), for both the initial diagnosis and the post-treatment tests [72, 84] However, certain questions have been raised regarding its reliability, as urease may be produced by other gut-inhabiting bacteria as well [75].
4.1.3. Stool Antigen Test (SAT)
The stool antigen test (SAT) or the faecal antigen test (FAT) is another reliable non-invasive test that is commonly employed to detect the presence of H. pylori in the fecal matter of suspected patients [85]. There are two types of SAT, based on the choice of analytical technique employed after stool collection, namely, enzyme immunoassay (EIA), while the other is based on immunochromatography (ICA) [86]. According to a study conducted by Gisbert et al. (2006), the accuracy of monoclonal SAT was found to be higher than that of polyclonal SAT, especially for the confirmation of post-treatment eradication efficiency [87].
4.2. Invasive tests
Invasive tests for H. pylori detection include collection of specimens via endoscopic biopsy procedures, which are followed by histological examinations, cultural approaches, the rapid urease test, and PCR-based analyses, all of which are carried out after a biopsy procedure [88]. Esophagogastroduodenoscopy (EGD) is, by and large, the most reliable and the most recommended diagnostic procedure for the accurate confirmation of a suspected H. pylori infection, and is considered the gold standard diagnostic procedure for the infection [89]. This test may be followed by other confirmations including immunohistochemical procedures, cultural tests, and molecular methods including PCR-based analysis [82]. Table 1 represents the different techniques available for diagnosis of H. pylori.
4.2.1. Histology
Histopathological examination for suspected cases of infection by H. pylori are considered among the more reliable and specific diagnostic procedures, offering advantageous information about the extent of inflammation, and associated pathologies such as gastric cancer, intestinal metaplasia, and gastritis [90]. Staining method usually involves employed haematoxylin and eosin (H&E), although ancillary tests involving Geimsa, Genta stain, or Warthin-Starry silver stain and immunohistochemistry are used for an accurate histological diagnosis, especially when H&E staining provides insufficient results, under conditions of the low density of the bacterium in the sample [90, 91] Immunohistochemistry (IHC) is a precise and highly sensitive and specific method for detecting H. pylori in gastric biopsies [90]. Histological diagnosis is affected by various factors including the site, size, and number of biopsy specimens taken. The Sydney system recommends extracting biopsy specimens from five sites, including the pylorus, antrum, corpus, and angularis, to ensure optimal detection [92]. Histological examinations remain the most available, accurate, and cost-effective method, offering higher sensitivity than the non-invasive and most of invasive methods, and are the more commonly preferred diagnostic choice when confirming suspected cases of H. pylori infection [93].
4.2.2. Culture examinations
In accordance with Koch’s postulates, Microbilogical examinations based on in-vitro culturing of the bacterium from biopsy specimens obtained after an endoscopy are also viable options for the accurate detection of H. pylori. However, certain disadvantages are associated with this test, including the fastidious nature of the microbe, the requirement of specific growth conditions and microbiological equipment, and low recovery rates of the bacterium from infected samples [75]. Critical reviews in this regard deem the method to be invasive, time-expensive, and with low sensitivity, and therefore, other methods may be preferable over culture-based diagnosis [94]. However, the fact remains that culture examination is the only test that allows for a specific analysis of the microbiological characteristics, of the strain type, and also determines antibiotic sensitivity [95].

Table 1.
Comparison of different techniques available for diagnosis of H. pylori.
| Diagnostic test | Sensitivity | Specificity | Advantages/Disadvantages | References |
|---|---|---|---|---|
| Urea breath test (UBT) | >95% | >95% |
Advantages: Gold standard in many clinical diagnoses, Cost-effective, reliable, simple, non-invasive, can be used for confirming eradication of infection Disadvantages: May give false negatives in presence of other urease producing bacteria and Helicobacter species. Low accuracy under conditions of gastritis and gastric malignancies, requires a high load of bacteria in the specimen. Requires expensive equipment. |
[96, 83] |
| Stool Antigen test (SAT) | 96% | 97% |
Advantages: Cost-effective, simple, rapid, doesn’t require expensive instruments Disadvantages: It may give false negatives under low bacterial count, and accuracy is affected by recent intake of PPI and CAM, not useful for post-eradication confirmation |
[87, 86] |
| Serological tests | 85% | >80% |
Advantages: Inexpensive, can be employed for patients who have recently undergone triple therapy. Only test not affected by PPI intake or use of antibiotics Disadvantages: Unreliable for ongoing infections, cannot be used to confirm eradication |
[74] |
| Rapid urease test (RUT) | 80-90% | 93-100%. |
Advantages: Rapid, inexpensive, simple Disadvantages: Invasive, requires additional confirmatory tests, accuracy affected by intake of PPI and antibiotics |
[45] |
| Culture | 70-90% | 100% |
Advantages: Gold standard for confirmation, can be used to ascertain antibiotic sensitivity Disadvantages: Elaborate, time-consuming, expensive, requires specific expertise in microbiology |
[97] |
| Histopathology | >95% | 99% | Advantages: Gold standard in routine clinical diagnostics, provides additional information about associated pathologies, extremely sensitive and specific | [88] |
| Molecular methods (PCR) | 96% | 98% |
Sensitive even at very low bacterial counts Disadvantages: Expensive, requires sophisticated equpiments, may give false positive results |
[75] |
4.2.3. Molecular and Genetic Markers
Recent advances in molecular biology have provided new avenues for detecting H. pylori. Given their accuracy and reliability, molecular diagnostic procedures should be preferred over the other methods discussed above. Methods such as RT-PCR allow for not only detection of the bacteria, but also their possible resistance against the recommended antibiotics for the eradication of the infection [98] Other approaches rely on the use of biomolecules as markers, enabling the early diagnosis of an H. pylori infection using such biosensors. These markers include 16S rRNA, 16S rDNA, cagA, vacA, and other factors associated with H. pylori [93]. In a study conducted in 2021, 16S rRNA amplicon sequencing was proposed as a suitable and accurate method for the detection of H. pylori infection, using gastric biopsy specimens. Additionally, this method was especially advantageous in confirming the presence of the pathogen in cases with a negative test result using routine test methods [99]. In a recent study conducted, a novel RPA-CRISPR-Cas12a-based method was developed for the detection of virulence factors CagA and VacA, and the 16S rDNA gene as well. This technique was found to be very sensitive (2ng/microliter), and therefore, may be applied for the rapid, accurate, and sensitive detection of H. pylori in various settings [78].
5. Treatment Strategies
5.1. Antibiotic therapy and selection of antibiotics
Currently, the widely accepted standard treatment strategy involves a triple therapy approach, whereby at least two antibiotics (usually amoxicillin and clarithromycin) and one proton pump inhibitor (PPI) are administered to the infected individual [100]. These antimicrobials, recommended in the Maastricht IV/Florence Consensus report, when used in combination exert a triple mode of action, affecting cell wall, and bacterial protein synthesis by binding to the 50S ribosomal unit and affecting DNA integrity [101, 7], However, such an antibiotic-based treatment strategy is impeded by the prevalence of antibiotic resistance to the primary or the secondary antibiotic, the possible occurrence of problematic side effects, mucosal drug concentrations, and the expensive nature of such drugs [102,103,104] In the case of failure of the first regimen of treatment, a triple treatment comprising Levofloxacin is recommended [105]. However, the fact remains that the growing prevalence of antibiotic resistance among various clinical and non-clinical bacteria reduces the effectiveness of treatment strategies that rely on antibiotics. Second-line therapy in cases of failure of first-line regimen includes a bismuth quadruple therapy (BQT) approach, comprising of a bismuth salt in addition to a proton pump inhibitor, metronidazole and tetracycline [106]. BQT may also be the treatment of choice under the condition of clarithromycin resistance [107]. In terms of effectiveness in treatment, a study conducted by Luther et al., (2010) revealed almost equivalent results, with similar outcomes for patient compliance, the side effects and eradication rates [108]. According to the Maastricht V/ Florence Consensus Report, a concomitant fluoroquinolone-amoxicillin triple/ quadruple therapy may also be employed as the second-line treatment option, as an alternative to BQT [109]. Alternatively, concomitant therapy, a type of non-bismuth quadruple therapy involving the concomitant administration of a PPI, amoxicillin, clarithromycin, and a nitrimidazole has also been identified as an effective treatment option against triple therapy-resistant infections [90, 110].
5.2. Proton pump inhibitors
PPIs are a group of chemical compounds that inhibit the gastric acid pump (H+/K+-ATPase) by binding to the cysteine residues of the proton pumps [111]. Examples of proton pump inhibitors include pantoprazole, rabeprazole, omeprazole, tenatoprazole, etc. First introduced in 1989, such bezimadazole-derived acid suppressors are excellent healers of peptic ulcers and are given in combination with antibiotics in the treatment and eradication of H. pylori infections, which lead to exaggerated acid production in infected individuals [112, 113]. The administration of PPI in the eradication of H. pylori provides the benefit of increasing the bioavailability of the acid-susceptible antibiotics, and also having a direct effect on the H. pylori growth and metabolism [114]. Although currently indispensable in the treatment of H. pylori infections, certain concerns have been raised regarding a few mild side-effects including increased risk of infections by enteric bacteria such as C. difficile and Salmonella, acute kidney injury, interference with calcium and magnesium homeostasis, and probably an increased risk of coronary diseases [113]
5.3. The rising issue of Antibiotic Resistance
The now highly prevalent occurrence of antibiotic resistance has continued to plague the treatment strategies for various infectious diseases, and H. pylori infections are no different. Over the years, a higher incidence of treatment failures has been reported on a global scale [115]. The rates of resistances against the conventionally employed antibiotics are widely variable, i.e., cases of heteroresistanc depending upon the region and the antibiotic class, with considerable variation in each region has been recorded against H. pylori [113]. Generally, such resistance in H. pylori is mainly due to chromosomal mutations, although another factor such as biofilm formation, expression of efflux pumps, etc. may also contribute to the development of resistance [116]. The highest cases of resistance are recorded against clarithromycin, especially in the Pacific, Mediterranean, and the European regions. Resistance against Levoflaxacin shows a similar pattern, with wider prevalence in the Eupropean region, North and South America, and Africa, while Metronidazole shows the highest occurrence of resistance, with as much as 91% cases being resistance, while the lowest cases of resistance has been the recorded against Amoxicillin, with less than 1% in most countries [115, 117, 118]. Following the rising cases of antibiotic resistance and the failure of triple therapy in eradicating the infection, different models of alternative treatment have been proposed in the Maastricht V/Florence consensus report. These include bismuth-based therapy and the quadruple therapy [113] (Table 2).
6. Future Directions
6.1. Challenges and Opportunities
Over the past years, significant progress has been made to facilitate our understanding of the pathogenic bacterium that is H. pylori. Its role in chronic gastritis and the development of peptic ulcer disease is now well-recognized. More importantly, the role of H. pylori as a risk factor in the development of gastric cancer has emerged as one of the most sought-after fields of research, with appreciable efforts being made for timely diagnosis, treatment and eradication of the disease and prevention/ treatment of resulting oncogenesis. A meta-analysis conducted in 2023 revealed a reduced rate off occurrence of H. pylori infections, resulting in a concomitant decline in the development of peptic ulcer disease, while the prevalence of antibiotic-resistant H. pylori is higher than in the past 40 years [124]. Among the newer treatment options being developed, including a quadruple therapy comprising of bismuth, and the use of probiotics, tailored therapy, phytomedicine, and nanotechnology [106].
6.2. Advancements in Research
Considering the varied resistance profiles exhibited by H. pylori including single drug, multidrug and the previously described heteroresistance, alternative treatment strategies are needed, and improved diagnostic tools are warranted for optimized selection of treatment choice. The intimate correlation between H. pylori infection and the development of gastric cancer provides the potential for an effective vaccination strategy, which may be used to prevent or treat the onset and establishment of gastric cancer in patients infected with the bacterium. However, such vaccination strategies are challenging owing to the variation in the strains, and the complicated mechanisms of the bacteria to evade the immune responses of the host. Surface adhesins such as BabA, SabA, OipA, etc. have the potential to be employed as biomarkers to help detect the onset of gastric carcinoma, as revealed by a study conducted by Su et al., (2016) [125]. Such biomarkers could also be used as immune system triggers in the form of vaccines to eradicate the infection. Nanotechnology has in the recent years emerged as an interesting field in biomedical research, providing new avenues for treatment of various diseases, including H. pylori-related diseases. Their targeted drug-delivery potential, and the unlimited scope for designability presents them as suitable candidates for the development of novel anti H. pylori nanomedicines. Additionally, nanoparticles can also be employed for the accurate and timely diagnosis of the infection, further promoting efficient management of the disease. Excellent reviews in this regard have already been published [126-128]. Similarly, phage therapy, a well-known alternative approach to combat bacterial infections, offers considerable potential to be explored for effective eradication of H. pylori infections [129]. Additionally, the use of probiotics in the treatment of H. pylori infection has gained significant traction in the recent years. Probiotic bacteria such as Lactobacilli and Bifidobacterium have been shown to alleviate the infection caused by H. pylori, while also impriving the immune system function and the performance of antibiotics [130]. Personalised therapy is another novel approach being explored for the effective treatment of H. pylori infections. It relies on confirmation of antibiotic susceptibility of H. pylori serotypes extracted from patients, after subjecting the bacterial strain to a series of antibiotic susceptibility tests. Additionally, it involves a treatment regime specifically tailored to the individual’s needs, according to their family history, genomic makeup, health history, etc. Such an approach is especially useful considering the steadily rising cases of H. pylori resistance against conventional choice of treatment, i.e., PPI and CAM [131]. While antibiotic therapy has proven to be significantly successful in the management of the infection, the steadily growing cases of antibiotic resistance and resistance against other agents like proton pump inhibitors, highlights the need for the development of alternative therapies, and for now, a careful monitoring of antibiotic administration, weighed on case-by-case basis. Undeniably, antibiotic stewardship has a significant role to play in the effective management of the infection and its wider effects. Judicious and well-regulated use of antibiotics can help minimise the development of resistance cases and still effectively combat the infection, providing the much-needed paradigm shift in the treatment approaches against H. pylori. Optimisation of dosage and duration of antibiotics, coupled with susceptibility testing and surveillance programs is critical for the effective management of the infection [132].
Effective diagnosis calls for the development of new diagnostic procedures, and certain novel tools have recently emerged as an interesting alternative to currently used methods, including multiplex PCR, fecal microbiota analysis, novel point-of-care testing techniques based on loop-mediated isothermal amplification (LAMP) and PCR detection or rapid antigen tests, confocal laser endomicroscopy (CLE), endoscopic submucosal dissection (ESD), etc [133]. Although such efforts and emerging technologies seem promising, certain challenges and limitations still remain, including poor patient compliance, prevailing intrinsic physiological conditions during treatment, bacterial resistance to antibiotics and other antimicrobials, etc. which must be carefully addressed in order to optimise diagnosis, treatment and successful eradication of H. pylori and further eradicate the risks of complications.
7. Conclusion
The review not only consolidates current knowledge but also illuminates potential avenues for future research and clinical interventions. Its relevance to healthcare professionals, researchers, and clinicians is underscored by the emphasis on accuracy in diagnosis, the imperative need for antibiotic stewardship, and the promising horizon of personalized medicine. Additionally, it is not only serves as a valuable reference for those navigating the complexities of H. pylori but also inspires further inquiries into refining diagnostic and therapeutic approaches in the ongoing pursuit of mitigating the impact of this prevalent and dynamic gastrointestinal pathogen.
Author Contributions
AA, and KIAH: Conceptualized and designed the study. AA: Wrote the original draft. KIAH: Reviewed and edited the manuscript. Both authors have read and approved the final version of the manuscript.
Acknowledgments
This work was supported and funded by the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University (IMSIU) (grant number IMSIU-RP23026).
References
- Warren, J.R.; Marshall, B. Unidentified Curved Bacilli on Gastric Epithelium in Active Chronic Gastritis. Lancet 1983, 1, 1273–1275. [Google Scholar] [PubMed]
- Krienitz, W. Ueber Das Auftreten von Spirochäten Verschiedener Form Im Mageninhalt Bei Carcinoma Ventriculi. DMW - Deutsche Medizinische Wochenschrift 1906, 32, 872–872. [Google Scholar] [CrossRef]
- Wroblewski, L.E.; Peek, R.M.; Wilson, K.T. Helicobacter pylori and Gastric Cancer: Factors That Modulate Disease Risk. Clin Microbiol Rev 2010, 23, 713–739. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Moayyedi, P. Helicobacter pylori Infection in Functional Dyspepsia. Nat Rev Gastroenterol Hepatol 2013, 10, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Fong, I.W. Helicobacter pylori Infection: When Should It Be Treated? In Current Trends and Concerns in Infectious Diseases; Springer International Publishing: Cham, 2020; pp. 81–102. ISBN 978-3-030-36966-8. [Google Scholar]
- Gravina, A.G.; Zagari, R.M.; De Musis, C.; Romano, L.; Loguercio, C.; Romano, M. Helicobacter pylori and Extragastric Diseases: A Review. World J Gastroenterol 2018, 24, 3204–3221. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori Infection - The Maastricht IV/ Florence Consensus Report. Gut 2012, 61, 646–664. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer.; World Health Organization. Schistosomes, Liver Flukes and Helicobacter pylori.; IARC, 1994; ISBN 9283212614.
- Farinha, P.; Gascoyne, R.D. Helicobacter pylori and MALT Lymphoma. Gastroenterology 2005, 128, 1579–1605. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Belayneh, Y.M. Helicobacter pylori and Duodenal Ulcer: Systematic Review of Controversies in Causation. Clin Exp Gastroenterol 2019, 12, 441–447. [Google Scholar] [CrossRef]
- Elbehiry, A.; Marzouk, E.; Aldubaib, M.; Abalkhail, A.; Anagreyyah, S.; Anajirih, N.; Almuzaini, A.M.; Rawway, M.; Alfadhel, A.; Draz, A.; et al. Helicobacter pylori Infection: Current Status and Future Prospects on Diagnostic, Therapeutic and Control Challenges. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Hikaru, H.; A, E.K.; L, M.A.; M, O.K.; H, M.M.; Eitaro, A. Helicobacter pylori Uses the TlpB Receptor To Sense Sites of Gastric Injury. Infect Immun 2019, 87. [Google Scholar] [CrossRef] [PubMed]
- Gu, H. Role of Flagella in the Pathogenesis of Helicobacter pylori. Curr Microbiol 2017, 74, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Yonezawa, H.; Osaki, T.; Kamiya, S. Biofilm Formation by Helicobacter pylori and Its Involvement for Antibiotic Resistance. Biomed Res Int 2015, 2015, 914791. [Google Scholar] [CrossRef] [PubMed]
- Salama, N.R.; Hartung, M.L.; Müller, A. Life in the Human Stomach: Persistence Strategies of the Bacterial Pathogen Helicobacter pylori. Nat Rev Microbiol 2013, 11, 385–399. [Google Scholar] [CrossRef]
- Reyes, V.E. Helicobacter pylori and Its Role in Gastric Cancer. Microorganisms 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Backert, S.; Tegtmeyer, N.; Fischer, W. Composition, Structure and Function of the Helicobacter pylori Cag Pathogenicity Island Encoded Type IV Secretion System. Future Microbiol 2015, 10, 955–965. [Google Scholar] [CrossRef] [PubMed]
- HATAKEYAMA, M. Structure and Function of Helicobacter pylori CagA, the First-Identified Bacterial Protein Involved in Human Cancer. Proceedings of the Japan Academy, Series B 2017, 93, 196–219. [Google Scholar] [CrossRef] [PubMed]
- Yong, X.; Tang, B.; Li, B.-S.; Xie, R.; Hu, C.-J.; Luo, G.; Qin, Y.; Dong, H.; Yang, S.-M. Helicobacter pylori Virulence Factor CagA Promotes Tumorigenesis of Gastric Cancer via Multiple Signaling Pathways. Cell Communication and Signaling 2015, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Kusters, J.G.; van Vliet, A.H.M.; Kuipers, E.J. Pathogenesis of Helicobacter pylori Infection. Clin Microbiol Rev 2006, 19, 449–490. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S.; Mentis, A.F. Pathogenesis of Helicobacter pylori Infection. Helicobacter 2007, 12, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Messina, B.; Lo Sardo, F.; Scalera, S.; Memeo, L.; Colarossi, C.; Mare, M.; Blandino, G.; Ciliberto, G.; Maugeri-Saccà, M.; Bon, G. Hippo Pathway Dysregulation in Gastric Cancer: From Helicobacter pylori Infection to Tumor Promotion and Progression. Cell Death Dis 2023, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Cover, T.L.; Blanke, S.R. Helicobacter pylori VacA, a Paradigm for Toxin Multifunctionality. Nat Rev Microbiol 2005, 3, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Foegeding, N.J.; Caston, R.R.; McClain, M.S.; Ohi, M.D.; Cover, T.L. An Overview of Helicobacter pylori VacA Toxin Biology. Toxins (Basel) 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, N.; Tay, A.C.Y.; Marshall, B.J.; Jain, U. Helicobacter pylori VacA, a Distinct Toxin Exerts Diverse Functionalities in Numerous Cells: An Overview. Helicobacter 2019, 24, e12544. [Google Scholar] [CrossRef]
- Dincă, A.L.; Meliț, L.E.; Mărginean, C.O. Old and New Aspects of H. pylori-Associated Inflammation and Gastric Cancer. Children 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Hu, B. Immunological Perspective: Helicobacter pylori Infection and Gastritis. Mediators Inflamm 2022, 2022, 2944156. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.; Greenfield, L.K.; Bronte-Tinkew, D.; Capurro, M.I.; Rizzuti, D.; Jones, N.L. VacA Promotes CagA Accumulation in Gastric Epithelial Cells during Helicobacter pylori Infection. Sci Rep 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Venerito, M.; Krieger, T.; Ecker, T.; Leandro, G.; Malfertheiner, P. Meta-Analysis of Bismuth Quadruple Therapy versus Clarithromycin Triple Therapy for Empiric Primary Treatment of Helicobacter pylori Infection. Digestion 2013, 88, 33–45. [Google Scholar] [CrossRef]
- Yamaoka, Y. Mechanisms of Disease: Helicobacter pylori Virulence Factors. Nat Rev Gastroenterol Hepatol 2010, 7, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.-C.; Oh, S.-T.; Sung, J.Y.; Cha, K.A.; Lee, M.H.; Oh, B.-H. Supramolecular Assembly and Acid Resistance of Helicobacter pylori Urease. Nat Struct Biol 2001, 8, 505–509. [Google Scholar] [CrossRef]
- Mobley, H.L.; Mendz, G.L.; Hazell, S.L. Helicobacter pylori: Physiology and Genetics; 2001; ISBN 1555812139.
- Malfertheiner, P.; Camargo, M.C.; El-Omar, E.; Liou, J.-M.; Peek, R.; Schulz, C.; Smith, S.I.; Suerbaum, S. Helicobacter pylori Infection. Nat Rev Dis Primers 2023, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Idowu, S.; Bertrand, P.P.; Walduck, A.K. Gastric Organoids: Advancing the Study of H. pylori Pathogenesis and Inflammation. Helicobacter 2022, 27, e12891. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-Y.; Sheu, B.-S.; Wu, J.-J. Helicobacter pylori Infection: An Overview of Bacterial Virulence Factors and Pathogenesis. Biomed J 2016, 39, 14–23. [Google Scholar] [CrossRef] [PubMed]
- White, J.R.; Winter, J.A.; Robinson, K. Differential Inflammatory Response to Helicobacter pylori Infection: Etiology and Clinical Outcomes. J Inflamm Res 2015, 8, 137–147. [Google Scholar] [CrossRef] [PubMed]
- D’Elios, M.M.; Amedei, A.; Cappon, A.; Del Prete, G.; de Bernard, M. The Neutrophil-Activating Protein of Helicobacter pylori (HP-NAP) as an Immune Modulating Agent. FEMS Immunol Med Microbiol 2007, 50, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Zeyaullah, Md.; AlShahrani, A.M.; Ahmad, I. Association of Helicobacter pylori Infection and Host Cytokine Gene Polymorphism with Gastric Cancer. Can J Gastroenterol Hepatol 2021, 2021, 8810620. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Ceponis, P.J.M.; Lebel, S.; Huynh, H.; Sherman, P.M. Helicobacter pylori Activates Toll-Like Receptor 4 Expression in Gastrointestinal Epithelial Cells. Infect Immun 2003, 71, 3496–3502. [Google Scholar] [CrossRef] [PubMed]
- Larussa, T.; Leone, I.; Suraci, E.; Imeneo, M.; Luzza, F. Helicobacter pylori and T Helper Cells: Mechanisms of Immune Escape and Tolerance. J Immunol Res 2015, 2015, 981328. [Google Scholar] [CrossRef] [PubMed]
- Bergman, M.P.; D’Elios, M.M. Cytotoxic T Cells in H. pylori-Related Gastric Autoimmunity and Gastric Lymphoma. J Biomed Biotechnol 2010, 2010, 104918. [Google Scholar] [CrossRef] [PubMed]
- Reyes Victor, E. and Peniche, A.G. Helicobacter pylori Deregulates T and B Cell Signaling to Trigger Immune Evasion. In Molecular Mechanisms of Inflammation: Induction, Resolution and Escape by Helicobacter pylori; Backert, S., Ed.; Springer International Publishing: Cham, 2019; pp. 229–265. ISBN 978-3-030-15138-6. [Google Scholar]
- Kumar, S.; Patel, G.K.; Ghoshal, U.C. Helicobacter pylori-Induced Inflammation: Possible Factors Modulating the Risk of Gastric Cancer. Pathogens 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Caron, T.J.; Scott, K.E.; Fox, J.G.; Hagen, S.J. Tight Junction Disruption: Helicobacter pylori and Dysregulation of the Gastric Mucosal Barrier. World J Gastroenterol 2015, 21, 11411–11427. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Miftahussurur, M.; Yamaoka, Y. Helicobacter pylori as an Oncogenic Pathogen, Revisited. Expert Rev Mol Med 2017, 19, e4. [Google Scholar] [CrossRef] [PubMed]
- Wroblewski, L.E.; Peek, R.M.; Wilson, K.T. Helicobacter pylori and Gastric Cancer: Factors That Modulate Disease Risk. Clin Microbiol Rev 2010, 23, 713–739. [Google Scholar] [CrossRef] [PubMed]
- Díaz, P.; Valenzuela Valderrama, M.; Bravo, J.; Quest, A.F.G. Helicobacter pylori and Gastric Cancer: Adaptive Cellular Mechanisms Involved in Disease Progression. Front Microbiol 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Skoog, E.; Göteborgs universitet. Helicobacter Spp. Interactions with Mucins : Adhesion and Mucin Regulation of Pathogen Proliferation and Gene Expression; Department of Medical Biochemistry and Cell Biology, Institute of Biomedicine, Sahlgrenska Academy at University of Gothenburg, 2014; ISBN 9789162888718.
- Nazanin, N.; V, J.M.E.; Sukanya, R.; K, L.S. Helicobacter pylori Infection Impairs the Mucin Production Rate and Turnover in the Murine Gastric Mucosa. Infect Immun 2013, 81, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Padra Médea and Benktander, J. and Benktander, J. and R.K. and L.S.K. Carbohydrate-Dependent and Antimicrobial Peptide Defence Mechanisms Against Helicobacter pylori Infections. In Molecular Mechanisms of Inflammation: Induction, Resolution and Escape by Helicobacter pylori; Backert, S., Ed.; Springer International Publishing: Cham, 2019; ISBN 978-3-030-15138-6. [Google Scholar]
- Fock, K.M. Review Article: The Epidemiology and Prevention of Gastric Cancer. Aliment Pharmacol Ther 2014, 40, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Duan, C.; Cao, H.; Zhang, L.-H.; Xu, Z. Harnessing the CRISPR-Cas Systems to Combat Antimicrobial Resistance. Front Microbiol 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Zagari, R.M.; Bazzoli, F. Epidemiology of Helicobacter pylori Infection. Helicobacter 2014, 19, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kayali, S.; Manfredi, M.; Gaiani, F.; Bianchi, L.; Bizzarri, B.; Leandro, G.; Di Mario, F.; De’angelis, G.L. Helicobacter pylori, Transmission Routes and Recurrence of Infection: State of the Art. Acta Biomedica 2018, 89, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Moss, S.F. The Clinical Evidence Linking <em>Helicobacter pylori</Em> to Gastric Cancer. Cell Mol Gastroenterol Hepatol 2017, 3, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Sipponen, P.; Hyvärinen, H. Role of Helicobacter pylori in the Pathogenesis of Gastritis, Peptic Ulcer and Gastric Cancer. Scand J Gastroenterol 1993, 28, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Hassan, C.; De Francesco, V.; Repici, A.; Manta, R.; Tomao, S.; Annibale, B.; Vaira, D. Helicobacter pylori and Functional Dyspepsia: An Unsolved Issue? World J Gastroenterol 2014, 8957–8963. [Google Scholar]
- Moayyedi P, S.S.D.J.J.D.B.H.A.I.M.O.R.W.S.R.A.B.C.; Forman, D. Eradication of Helicobacter pylori for Non-ulcer Dyspepsia. Cochrane Database of Systematic Reviews 2006. [CrossRef] [PubMed]
- Majumdar, D.; Bebb, J. Helicobacter pylori Infection and Peptic Ulcers. Medicine 2019, 47, 292–300. [Google Scholar] [CrossRef]
- Narayanan, M.; Reddy, K.M.; Marsicano, E. Peptic Ulcer Disease and Helicobacter pylori Infection. Mo Med 2018, 115, 219–224. [Google Scholar]
- Ferro, A.; Peleteiro, B.; Malvezzi, M.; Bosetti, C.; Bertuccio, P.; Levi, F.; Negri, E.; La Vecchia, C.; Lunet, N. Worldwide Trends in Gastric Cancer Mortality (1980–2011), with Predictions to 2015, and Incidence by Subtype. Eur J Cancer 2014, 50, 1330–1344. [Google Scholar] [CrossRef] [PubMed]
- Khatoon, J.; Rai, R.P.; Prasad, K.N. Role of Helicobacter pylori in Gastric Cancer: Updates. World J Gastrointest Oncol 2016, 8, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Mégraud, F.; Bessède, E.; Varon, C. Helicobacter pylori Infection and Gastric Carcinoma. Clinical Microbiology and Infection 2015, 21, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.G. Cellular and Molecular Aspects of Gastric Cancer. World J Gastroenterol 2006, 12, 2979. [Google Scholar] [CrossRef] [PubMed]
- Polk, D.B.; Peek, R.M. Helicobacter pylori: Gastric Cancer and Beyond. Nat Rev Cancer 2010, 10, 403–414. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Zhang, P.Y.; Aboul-Soud, M.A.M. From Inflammation to Gastric Cancer: Role of Helicobacter pylori. Oncol Lett 2017, 13, 543–548. [Google Scholar] [CrossRef]
- Kalali, B.; Formichella, L.; Gerhard, M. Diagnosis of Helicobacter pylori: Changes towards the Future. Diseases 2015, 3, 122–135. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.M.; Retnakumar, R.J.; Chouhan, D.; Devi, T.N.B.; Dharmaseelan, S.; Devadas, K.; Thapa, N.; Tamang, J.P.; Lamtha, S.C.; Chattopadhyay, S. Helicobacter pylori in Human Stomach: The Inconsistencies in Clinical Outcomes and the Probable Causes. Front Microbiol 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Mladenova, I. Clinical Relevance of Helicobacter pylori Infection. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Official journal of the American College of Gastroenterology | ACG 2017, 112.
- Shatila, M.; Thomas, A.S. Current and Future Perspectives in the Diagnosis and Management of Helicobacter pylori Infection. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Pes, G.M. What Is New in Helicobacter pylori Diagnosis. An Overview. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-K. Diagnosis of Helicobacter pylori Infection: Current Options and Developments. World J Gastroenterol 2015, 21, 11221. [Google Scholar] [CrossRef] [PubMed]
- Miftahussurur, M.; Yamaoka, Y. Diagnostic Methods of Helicobacter pylori Infection for Epidemiological Studies: Critical Importance of Indirect Test Validation. Biomed Res Int 2016, 2016, 4819423. [Google Scholar] [CrossRef]
- Patel, S.K.; Pratap, C.B.; Jain, A.K.; Gulati, A.K.; Nath, G. Diagnosis of Helicobacter pylori: What Should Be the Gold Standard? World J Gastroenterol 2014, 20, 12847–12859. [Google Scholar] [CrossRef]
- Mohammadian, T.; Ganji, L. The Diagnostic Tests for Detection of Helicobacter pylori Infection. Monoclon Antib Immunodiagn Immunother 2019, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Rengifo, D.F.; Mendoza, B.; Jaramillo, C.; Rodríguez-Urrego, P.A.; Vera-Chamorro, J.F.; Alvarez, J.; Delgado, M. del P.; Jimenez-Soto, L.F. Helicobacter pylori Culture as a Key Tool for Diagnosis in Colombia. The Journal of Infection in Developing Countries 2019, 13, 720–726. [CrossRef] [PubMed]
- Zhu, F.; Zhang, X.; Li, P.; Zhu, Y. Effect of Helicobacter pylori Eradication on Gastric Precancerous Lesions: A Systematic Review and Meta-Analysis. Helicobacter 2023, 28, e13013. [Google Scholar] [CrossRef] [PubMed]
- Herbrink, P.; van Doorn, L.J. Serological Methods for Diagnosis of Helicobacter pylori Infection and Monitoring of Eradication Therapy. European Journal of Clinical Microbiology and Infectious Diseases 2000, 19, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Siavoshi, F.; Saniee, P.; Khalili-Samani, S.; Hosseini, F.; Malakutikhah, F.; Mamivand, M.; Shahreza, S.; Sharifi, A.H. Evaluation of Methods for H. pylori Detection in PPI Consumption Using Culture, Rapid Urease Test and Smear Examination. Ann Transl Med 2015, 3. [CrossRef]
- Skrebinska, S.; Mégraud, F.; Bessède, E. Diagnosis of Helicobacter pylori Infection. Helicobacter 2018, 23, e12515. [Google Scholar] [CrossRef] [PubMed]
- Sankararaman, S.; Moosavi, L. Urea Breath Test; 2023.
- Ferwana, M.; Abdulmajeed, I.; Alhajiahmed, A.; Madani, W.; Firwana, B.; Hasan, R.; Altayar, O.; Limburg, P.J.; Murad, M.H.; Knawy, B. Accuracy of Urea Breath Test in Helicobacter pylori Infection: Meta-Analysis. World J Gastroenterol 2015, 21, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, D.C.; van Zanten, S.V. Dyspepsia. Can Med Assoc J 2015, 187, 276–276. [Google Scholar] [CrossRef] [PubMed]
- Crowe, S.E. Helicobacter pylori Infection. New England Journal of Medicine 2019, 380, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, T. Stool Antigen Tests for the Management of Helicobacter pylori Infection. World J Gastroenterol 2013, 19, 8188–8191. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; de la Morena, F.; Abraira, V. Accuracy of Monoclonal Stool Antigen Test for the Diagnosis of H. pylori Infection: A Systematic Review and Meta-Analysis. Official journal of the American College of Gastroenterology | ACG 2006, 101.
- Ricci, C.; Holton, J.; Vaira, D. Diagnosis of Helicobacter pylori: Invasive and Non-Invasive Tests. Best Pract Res Clin Gastroenterol 2007, 21, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Best, L.M.J.; Takwoingi, Y.; Siddique, S.; Selladurai, A.; Gandhi, A.; Low, B.; Yaghoobi, M.; Gurusamy, K.S. Non-Invasive Diagnostic Tests for Helicobacter pylori Infection. Cochrane Database of Systematic Reviews 2018, 2018. [Google Scholar]
- Lee, H.S. Histopathologic Diagnosis of H. pylori Infection and Associated Gastric Diseases. In Helicobacter pylori; Kim, N., Ed.; Springer Singapore: Singapore, 2016; ISBN 978-981-287-706-2. [Google Scholar]
- Yadav, R.; Sagar, M. Comparison of Different Histological Staining Methods for Detection of Helicobacter pylori Infection in Gastric Biopsy. Cureus 2022. [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P.; the Participants in the International Workshop on the Histopathology of Gastritis, H. 1994 Classification and Grading of Gastritis: The Updated Sydney System. Am J Surg Pathol1996; 20.
- Mărginean, C.O.; Meliț, L.E.; Săsăran, M.O. Traditional and Modern Diagnostic Approaches in Diagnosing Pediatric Helicobacter pylori Infection. Children 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Hassan, C.; Lorenzetti, R.; Winn, S.; Morini, S. A Clinical Practice Viewpoint: To Culture or Not to Culture Helicobacter pylori. Digestive and Liver Disease 2003, 35, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Hirschl, A.M.; Makristathis, A. Methods to Detect Helicobacter pylori: From Culture to Molecular Biology. Helicobacter 2007, 12, 6–11. [Google Scholar] [CrossRef]
- Nurgalieva, Z.Z.; Conner, M.E.; Opekun, A.R.; Zheng, C.Q.; Elliott, S.N.; Ernst, P.B.; Osato, M.; Estes, M.K.; Graham, D.Y. B-Cell and T-Cell Immune Responses to Experimental Helicobacter pylori Infection in Humans. Infect Immun 2005, 73, 2999–3006. [Google Scholar] [CrossRef] [PubMed]
- Macin, S.; Alp, A.; Sener, B.; Sokmensuer, C.; Orhan, D.; Ozen, H.; Kav, T.; Akyon, Y. Comparison of Culture, Real- Time-PCR, ELISA, and Histopathological Examination Methods for Identification of Helicobacter pylori. Istanbul Medical Journal 2018, 19, 138–142. [Google Scholar] [CrossRef]
- Bénéjat, L.; Ducournau, A.; Lehours, P.; Mégraud, F. Real-Time PCR for Helicobacter pylori Diagnosis. The Best Tools Available. Helicobacter 2018, 23, e12512. [Google Scholar] [CrossRef] [PubMed]
- Gantuya, B.; El Serag, H.B.; Saruuljavkhlan, B.; Azzaya, D.; Matsumoto, T.; Uchida, T.; Oyuntsetseg, K.; Oyunbileg, N.; Davaadorj, D.; Yamaoka, Y. Advantage of 16S RRNA Amplicon Sequencing in Helicobacter pylori Diagnosis. Helicobacter 2021, 26, e12790. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; González, L.; Calvet, X.; García, N.; López, T.; Roqué, M.; Gabriel, R.; Pajares, J.M. Proton Pump Inhibitor, Clarithromycin and Either Amoxycillin or Nitroimidazole: A Meta-Analysis of Eradication of Helicobacter pylori. Aliment Pharmacol Ther 2000, 14, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Rokkas, T.; Gisbert, J.P.; Malfertheiner, P.; Niv, Y.; Gasbarrini, A.; Leja, M.; Megraud, F.; O’Morain, C.; Graham, D.Y. Comparative Effectiveness of Multiple Different First-Line Treatment Regimens for Helicobacter pylori Infection: A Network Meta-Analysis. Gastroenterology 2021, 161, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Sabourian, R.; Foroumadi, A. Treatment of Helicobacter pylori Infection: Current and Future Insights. 2016. [CrossRef]
- Molina-Infante, J.; Gisbert, J.P. Optimizing Clarithromycin-Containing Therapy for Helicobacter pylori in the Era of Antibiotic Resistance. World J Gastroenterol 2014, 20, 10338–10347. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori Treatment in the Era of Increasing Antibiotic Resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Hadzhiyski, P.; Gergova, R.; Markovska, R. Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y. Antibiotic Treatment for Helicobacter pylori : Is the End Coming? World J Gastrointest Pharmacol Ther 2015, 6, 183. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.K.; Kang, S.J.; Lee, Y.C.; Yang, H.J.; Park, S.Y.; Shin, C.M.; Kim, S.E.; Lim, H.C.; Kim, J.H.; Nam, S.Y.; et al. Evidence-Based Guidelines for the Treatment of Helicobacter pylori Infection in Korea 2020. Gut Liver 2021, 15, 168–195. [Google Scholar] [CrossRef] [PubMed]
- Luther, J.; Higgins, P.D.R.; Schoenfeld, P.S.; Moayyedi, P.; Vakil, N.; Chey, W.D. Empiric Quadruple vs. Triple Therapy for Primary Treatment OfHelicobacter pyloriInfection: Systematic Review and Meta-Analysis of Efficacy and Tolerability. Official journal of the American College of Gastroenterology | ACG 2010, 105.
- Lin, T.F.; Hsu, P.I. Second-Line Rescue Treatment of Helicobacter pylori Infection: Where Are We Now? World J Gastroenterol 2018, 24, 4548–4553. [Google Scholar] [CrossRef] [PubMed]
- Essa, A.S.; Kramer, J.R.; Graham, D.Y.; Treiber, G. Meta-Analysis: Four-Drug, Three-Antibiotic, Non-Bismuth-Containing “Concomitant Therapy” Versus Triple Therapy for Helicobacter pylori Eradication. Helicobacter 2009, 14, 109–118. [Google Scholar] [CrossRef] [PubMed]
- SACHS, G.; SHIN, J.M.; HOWDEN, C.W. Review Article: The Clinical Pharmacology of Proton Pump Inhibitors. Aliment Pharmacol Ther 2006, 23, 2–8. [Google Scholar] [CrossRef]
- Shin, J.M.; Sachs, G. Pharmacology of Proton Pump Inhibitors. Curr Gastroenterol Rep 2008, 10, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Kandulski, A.; Venerito, M. Proton-Pump Inhibitors: Understanding the Complications and Risks. Nat Rev Gastroenterol Hepatol 2017, 14, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.; Qian, X.; Liu, X.; Song, Y.; Song, C.; Wu, S.; An, Y.; Yuan, R.; Wang, Y.; Xie, Y. The Effect of Antibiotic Resistance on Helicobacter pylori Eradication Efficacy: A Systematic Review and Meta-Analysis. Helicobacter 2020, 25, e12714. [Google Scholar] [CrossRef] [PubMed]
- Zanotti Giuseppe and Cendron, L. Structural Aspects of Helicobacter pylori Antibiotic Resistance. In Helicobacter pylori in Human Diseases: Advances in Microbiology, Infectious Diseases and Public Health Volume 11; Kamiya Shigeru and Backert, S., Ed.; Springer International Publishing: Cham, 2019; ISBN 978-3-030-21916-1. [Google Scholar]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-Analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Keikha, M.; Karbalaei, M. Prevalence of Antibiotic Heteroresistance Associated with Helicobacter pylori Infection: A Systematic Review and Meta-Analysis. Microb Pathog 2022, 170, 105720. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Calvet, X. Update on Non-Bismuth Quadruple (Concomitant) Therapy for Eradication of Helicobacter pylori. Clin Exp Gastroenterol 2012, 5, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-C.; Chang, W.-L.; Chen, W.-Y.; Yang, H.-B.; Wu, J.-J.; Sheu, B.-S. Levofloxacin-Containing Triple Therapy to Eradicate the Persistent H. pylori after a Failed Conventional Triple Therapy. Helicobacter 2007, 12, 359–363. [Google Scholar] [CrossRef]
- Hsu, P.-I.; Tsai, F.-W.; Kao, S.-S.; Hsu, W.-H.; Cheng, J.-S.; Peng, N.-J.; Tsai, K.-W.; Hu, H.-M.; Wang, Y.-K.; Chuah, S.-K.; et al. Ten-Day Quadruple Therapy Comprising Proton Pump Inhibitor, Bismuth, Tetracycline, and Levofloxacin Is More Effective than Standard Levofloxacin Triple Therapy in the Second-Line Treatment of Helicobacter pylori Infection: A Randomized Controlled Trial. Official journal of the American College of Gastroenterology | ACG 2017, 112. [CrossRef]
- Hsu, P.-I.; Tsay, F.-W.; Kao, J.Y.; Peng, N.-J.; Chen, Y.-H.; Tang, S.-Y.; Kuo, C.-H.; Kao, S.-S.; Wang, H.-M.; Wu, I.-T.; et al. Tetracycline-Levofloxacin versus Amoxicillin-Levofloxacin Quadruple Therapies in the Second-Line Treatment of Helicobacter pylori Infection. Helicobacter 2021, 26, e12840. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X.; O’Connor, A.; Mégraud, F.; O’Morain, C.A. Sequential Therapy for Helicobacter pylori Eradication: A Critical Review. J Clin Gastroenterol 2010, 44. [Google Scholar] [CrossRef]
- O’Connor, H.J. Forty Years of Helicobacter pylori Infection and Changes in Findings at Esophagogastroduodenoscopy. Helicobacter 2023, 28, e13026. [Google Scholar] [CrossRef]
- Su, Y.-L.; Huang, H.-L.; Huang, B.-S.; Chen, P.-C.; Chen, C.-S.; Wang, H.-L.; Lin, P.-H.; Chieh, M.-S.; Wu, J.-J.; Yang, J.-C.; et al. Combination of OipA, BabA, and SabA as Candidate Biomarkers for Predicting Helicobacter pylori-Related Gastric Cancer. Sci Rep 2016, 6, 36442. [Google Scholar] [CrossRef]
- Safarov, T.; Kiran, B.; Bagirova, M.; Allahverdiyev, A.M.; Abamor, E.S. An Overview of Nanotechnology-Based Treatment Approaches against Helicobacter pylori. Expert Rev Anti Infect Ther 2019, 17, 829–840. [Google Scholar] [CrossRef]
- Qin, Y.; Lao, Y.-H.; Wang, H.; Zhang, J.; Yi, K.; Chen, Z.; Han, J.; Song, W.; Tao, Y.; Li, M. Combatting Helicobacter pylori with Oral Nanomedicines. J. Mater. Chem. B 2021, 9, 9826–9838. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, W.; Zhang, J.; Xia, X. Eradication of Helicobacter pylori: The Power of Nanosized Formulations. Nanomedicine 2020, 15, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Kortright, K.E.; Chan, B.K.; Koff, J.L.; Turner, P.E. Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacteria. Cell Host Microbe 2019, 25, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Mestre, A.; Sathiya Narayanan, R.; Rivas, D.; John, J.; Abdulqader, M.A.; Khanna, T.; Chakinala, R.C.; Gupta, S. Role of Probiotics in the Management of Helicobacter pylori. Cureus 2022, 14, e26463. [Google Scholar] [CrossRef] [PubMed]
- Mestrovic, A.; Perkovic, N.; Tonkic, A.; Sundov, Z.; Kumric, M.; Bozic, J. Personalized Approach in Eradication of Helicobacter pylori Infection. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y. Transitioning of Helicobacter pylori Therapy from Trial and Error to Antimicrobial Stewardship. Antibiotics 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Addissouky, T.A.; Wang, Y.; El Sayed, I.E.T.; Baz, A. El; Ali, M.M.A.; Khalil, A.A. Recent Trends in Helicobacter pylori Management: Harnessing the Power of AI and Other Advanced Approaches. Beni Suef Univ J Basic Appl Sci 2023, 12. [Google Scholar] [CrossRef]
Figure 1.
A timeline of significant events related to H. pylori discovery and management of infection.
Figure 1.
A timeline of significant events related to H. pylori discovery and management of infection.
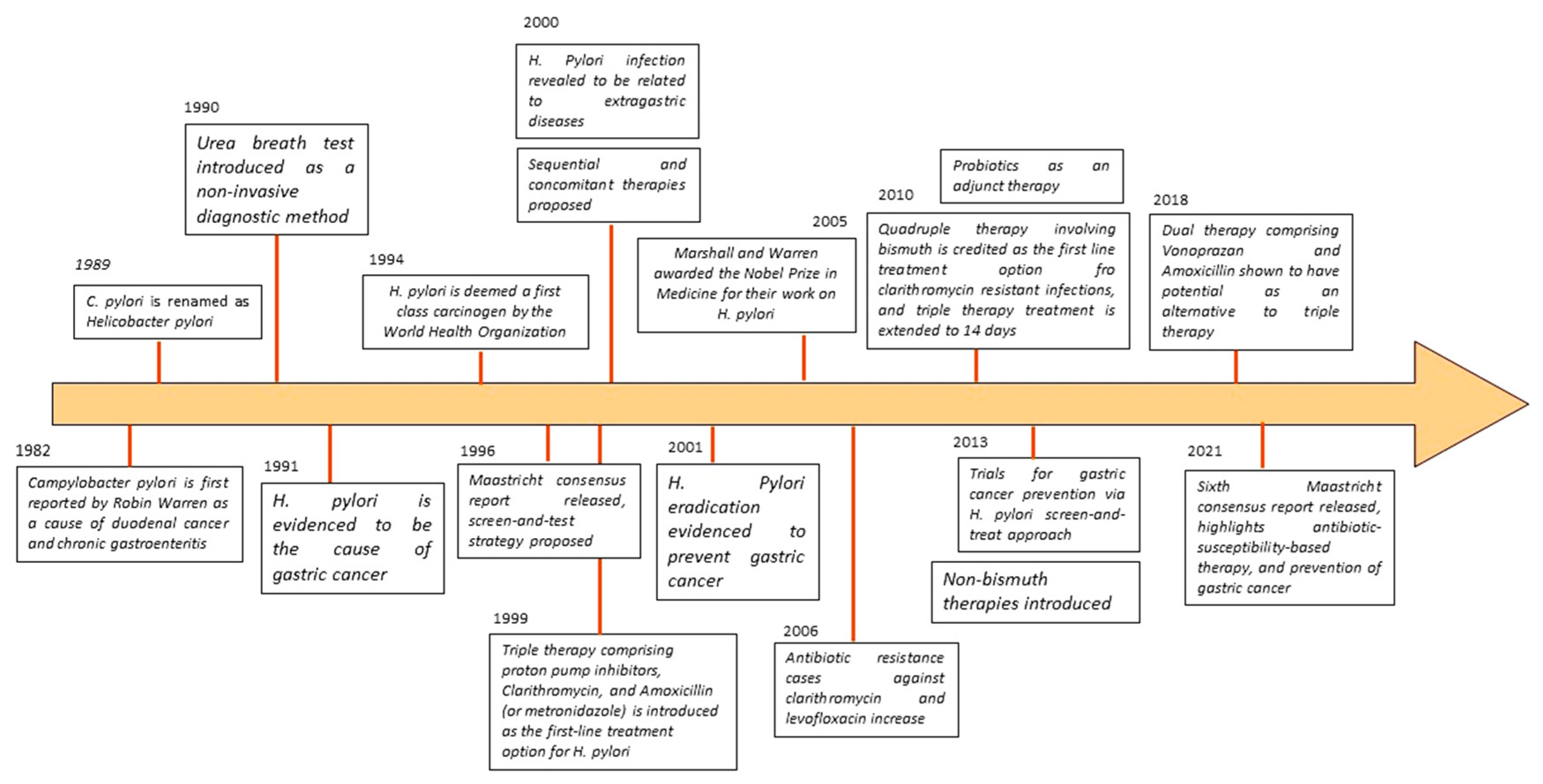
Figure 2.
Pathogenesis of H. pylori .
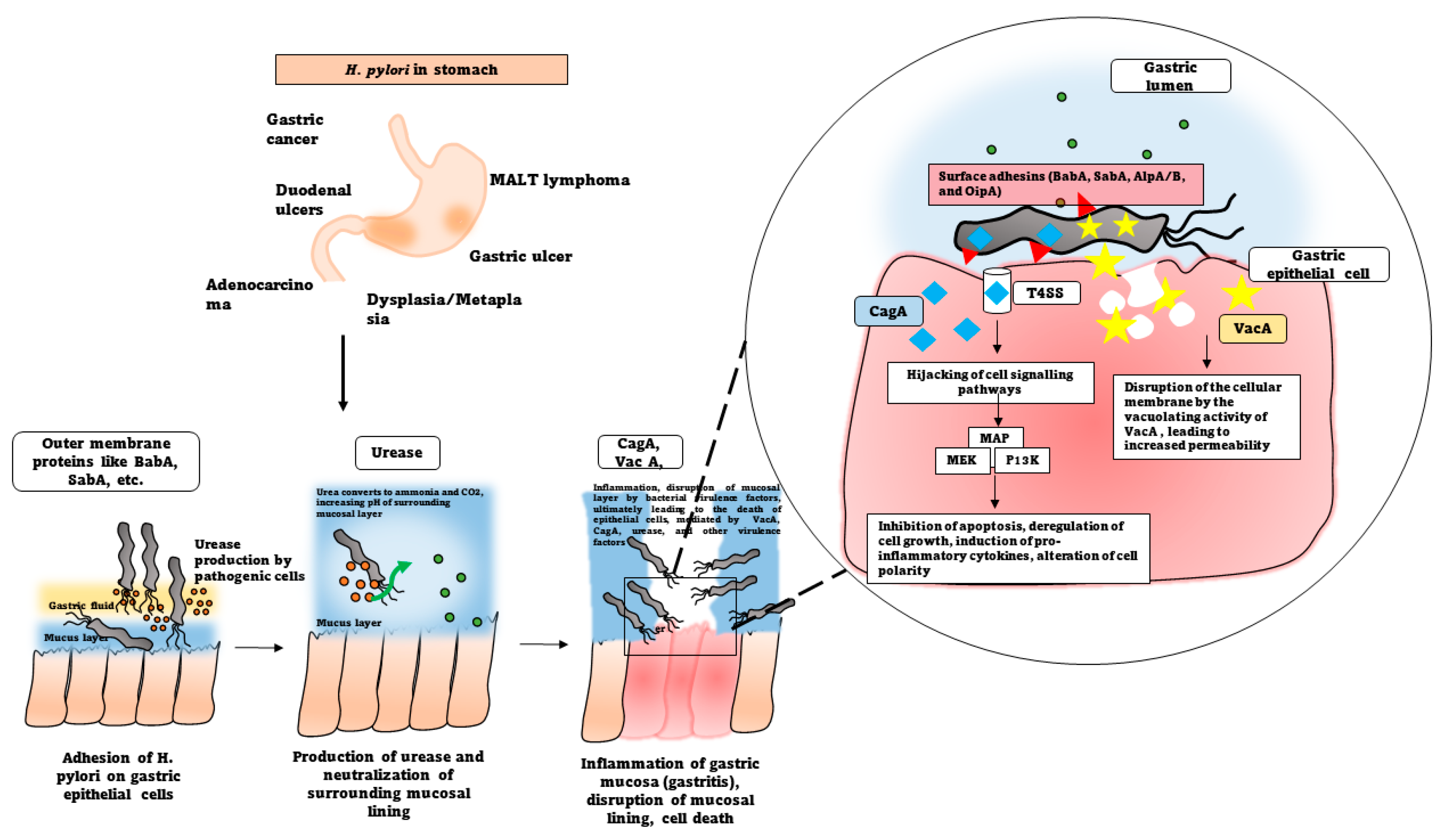
Table 2.
Comparison of the treatment strategies currently available against H. pylori.
| Treatment option | Drugs employed | Duration of therapy | References |
|---|---|---|---|
|
Triple therapy (PPI+ two antibiotics) |
PPI, Clarithromycin, Amoxicillin (or Metronidazole) | 7 days | [119] |
| Bismuth Quadruple therapy (BQT) | PPI, bismuth, tetracycline, and metronidazole | 14 days | [29] |
| Levofloxacin-containing triple therapy | PPI, levofloxacin, amoxicillin | 14 days | [120] |
| Levofloxacin-amoxicillin quadruple therapy | PPI, bismuth, levofloxacin, amoxicillin | 10 days | [121] |
| Tetracycline-levofloxacin quadruple therapy | PPI, bismuth, levofloxacin, tetracycline | 10 days | [122] |
| Concomitant therapy (non-bismuth therapy) | PPI, amoxicillin, clarithromycin, and a nitrimidazole | [119] | |
| Sequential therapy (dual) | PPI and amoxicillin for 5 days, followed by triple therapy (PPI, clarithromycin, and tinidazole) for next 5 days | 10 days | [123] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



