
Submitted:
18 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
Gastric outlet obstruction (GOO) poses a common and challenging clinical scenario, characterized by mechanical blockage in the pylorus, distal stomach, or duodenum, resulting in symptoms such as nausea, vomiting, abdominal pain, and early satiety. Its diverse etiology encompasses both benign and malignant disorders. The spectrum of current treatment modalities extends from conservative approaches to more invasive interventions, incorporating procedures like surgical gastroenterostomy (SGE), self-expandable metallic stents (SEMS) placement, and the advanced technique of endoscopic ultrasound-guided gastroenterostomy (EUS-GE). While surgery is favored for longer life expectancy, stents are preferred in malignant gastric outlet stenosis. The novel EUS-GE technique, employing a lumen-apposing self-expandable metal stent (LAMS), combines the immediate efficacy of stents with the enduring benefits of gastroenterostomy. Despite its promising outcomes, EUS-GE is a technically demanding procedure requiring specialized expertise and facilities.
Keywords:
Endoscopic ultrasound-guided gastroenterostomy
; Gastric outlet obstruction
; Endosonography
; Self expandable metal stent
; Gastroenterostomy
1. Introduction
Gastric outlet obstruction (GOO) is the intrinsic or extrinsic mechanical blockage of gastric emptying at the level of the distal stomach, pyloric antrum, or duodenum resulting from various benign or malignant conditions[1,2,3]. Most common benign conditions are gastric and duodenal ulcers. Other benign conditions causing GOO are post ulcer stenosis, acute pancreatitis and pancreatic fluid collections, chronic pancreatitis, annular pancreas, postsurgical scarring, post endoscopic therapy, non steroidal anti-inflammatory drug-associated or radiation-induced stricture, caustic ingestion, foreign body, benign tumor (adenoma, lipoma), pancreatic heterotopia, Crohn´s disease, eosinophilic gastroenteritis, tuberculosis, amyloidosis, Bouveret syndrome, Ladd band, diaphragmatic hernia, gastric volvulus and percutaneous endoscopic gastrostomy tube migration[1,2,4]. In the past, ulcer induced GOO was very common (up to 90% in 1990), but with the advent of PPIs and helicobacter pylori eradication the most common cause of GOO nowadays is malignancy (50-80%)[1]. Malignant gastric outlet obstruction (mGOO) can result from cancers of the stomach, duodenum, pancreas, biliary tree, liver as well as from metastases, lymphoma and retroperitoneal sarcoma[1,4,5]. Pancreatic adenocarcinoma is the most common cause of mGOO in the western world, while gastric adenocarcinoma is responsible for most mGOOs in Asia [5].
Patients with GOO generally present with progressive symptoms like epigastric pain, early satiety, nausea and vomiting. These symptoms can also appear due to the primary condition’s manifestations or complications of treatment (e.g. radiation or chemotherapy) in case of known malignancy.[4] For this reason a careful differential diagnosis should be performed. Diagnosis should be made early since malnutrition can appear as a result of poor oral food intake, which in turn can negatively influence patient prognosis [1,4].
Clinical examination may reveal a palpable mass due to stomach distension (15% of the cases)[1]. This can be easily confirmed initially through transabdominal ultrasound or an x-Ray of the abdomen – even though a CT-scan will almost always follow. Both exams can show the enlarged stomach and the lack of small or large intestine distension. Thus, intestinal blockage can be excluded, which is also an important differential diagnosis of vomiting. Furthermore, it is very important to assess the presence of more than one stenotic segments or ascites (benign or malignant)[2]. In suspicion of GOO a CT-scan and a gastroscopy are always necessary. CT-scan of the abdomen offers the advantage of revealing the extent of the disease, especially in the case of malignancy, the presence of metastasis or peritoneal carcinomatosis. Upper gastrointestinal endoscopy can directly determine the cause of the stenosis with or without biopsy and in cases of extraluminal compression, endoscopic ultrasonography is needed for tissue sampling as well as locoregional staging. All the above information along with estimated patient survival and patient preferences will determine which is the most appropriate therapeutic management[4,5].
In previous decades SGE has been the treatment of choice for GOOs. Nowadays, SEMS and EUS-GE have gained wide acceptance and have replaced surgery for selected patients[2,4].
In this narrative review we describe the available methods for the management of GOOs, explain patient selection for each method and compare available methods based on current data discussing their efficacy and safety. Notably, our primary emphasis is on EUS-GE, with special attention given to the occurrence of stent misdeployment during the procedure.
2. Management
2.1. Surgical Gastrojejunostomy
This method was considered the traditional bypass method to alleviate obstructive symptoms of GOO and ameliorate patients’ quality of life before the emergence of more synchronous endoscopic techniques. It can be performed either as an open or a laparoscopic surgery. It is important that the site of the gastrostomy is 3-5 cm proximal to either the obstructing mass or the pylorus. The anastomosis should be formed low on the greater curvature, as selecting the site too high can lead to intractable biliary reflux and reduced gastric emptying. A loop of jejunum 10-15 cm distal to the ligament of Treitz is selected and placed near the stomach in an isoperistaltic conformationand not under tension either in an antecolic or a retrocolic fashion.[6]
Complications of the SGE include postoperative nausea and emesis, hemorrhage, deep vein thrombosis, anastomotic leak (mostly between the third to fifth postoperative day), bowel obstruction (early: secondary to a technical error such as excessive kinking of the bowel or late: secondary to adhesions), internal herniation, nutritional deficiency (when a significant amount of intestine is bypassed), early or late dumping syndrome, marginal ulcer (gastrojejunostomy predisposes the region of the jejunum closest to the stomach to developing an ulcerbecause it lacks the protective mechanismsof the duodenum) and bile reflux[6,7].The laparoscopic version of the technique has been associated with improved morbidity and mortality rates, as well as shorter hospitalization, shorter intervals to resume eating, reduced intraoperative haemorrhage and reduced needs for postoperative opiates. [8]
Surgery is performed in patients with life expectancy of several months, which should be long enough to overcome the short-term morbidity and mortality burden of the surgical procedure and therefore patients can benefit from a long-lasting palliative gastric bypass.[4]Also surgery may be performed as a salvage option in selected patients after unsuccessful EUS-GE. [9]
2.2. Self-Expandable Metallic Stents
SEMS is the oldest one of the endoscopic techniques used for GOO. SEMS are available in a compressed manner in a device that can be placed through the working channel of an endoscope over a wire that has already been placed through the obstruction.[4] The stent can then be deployed under endoscopic and/or fluoroscopic control. The stent self-expands to reach its maximum diameter in the following 24 to 48 hours. An endoscope with a large working channel (i.e., = 3.7 mm) is required. Most cases are managed with therapeutic gastroscopes, but cases of dilated stomachs or strictures in the distal duodenum could be better managed with a colonoscope or even a duodenoscope[10,11].
There are three types of SEMS, uncovered (uSEMS), partially covered (pcSEMS) and fully covered (fcSEMS). In general, it seems that both uSEMS and fcSEMS are comparably effective. Studies suggest that all SEMS have similar technical success (ranging between89% and 98%) and clinical success, usually defined as the relief of obstructive symptoms and improvement of oral intake[5],ranging between 63% and 93% [12]. The choice of the stent type is based on the individual characteristics of the stenosis, knowing that fcSEMS have higher migration rates, whereas stent ingrowth rate is higher with uSEMS. The latter offer the additional advantage of better bile outflow (through the stent’s mesh interstices) in case the stent is placed across the duodenal papilla[4,5].
Adverse event (AE) rate related to SEMS placement ranges from 0% to 30%depending on the definition of each study. This may include minor AEs such as nausea, vomiting, mild abdominal pain, or major AEs, such as bleeding, perforation, stent migration/displacement or cholangitis.[5]Delayed AEs are usually related to stent dysfunction, secondary to migration or occlusion by food impaction and/or tumor ingrowth/overgrowth. Several methods (e.g., stent clipping or suturing, anti-migratory design) have been proposed to reduce the migration risk[13].
The placement of a SEMS is the first-line strategy in patients with short life expectancy (< 3 months) and can also be an alternative if EUS-GE is not successful. [9]
2.3. EUS-Guided Gastroenterostomy
EUS – GE has emerged as new endoscopic therapeutic option for GOO offering equivalent efficacy compared to other techniques but with possibly fewer adverse events in experienced hands. During EUS-GE stomach and small intestine are fused with the application of a new type of stent, the lumen apposing metallic stent (LAMS), which was introduced in 2012[14].LAMS is a double flanged, fully covered stent that provides a stable anastomosis between two adjacent organs (Figure 1). The presence of wide flanges (flared ends of 24mm for the 15mm stent) on both ends results in a better anchoring and allows for equal distribution of pressure on the luminal wall, thus decreasing the risk of migration[14]. For this procedure a linear echoendoscope with forward or oblique viewing is needed[2].In order to place LAMS between the stomach and the distal duodenum or proximal jejunum many methods have been developed. They can be divided in 2 groups, the direct method and the assisted methods including a. the antegrade EUS-GE traditional downstream method, b. the antegrade EUS-GE rendezvous method, c. the retrograde EUS- enterogastrostomy and the EUS balloon occluded GE bypass (EPASS)[2,15].The first two, are the most frequently used[2,9]. Here we describe the basic steps of each procedure[2,15].The decision on which target site is selected is based on the proximity of that portion of the small bowel to the gastric wall and whether there is tumor involvement of the third part of the duodenum. If there is diffuse malignant gastric involvement/infiltration, a gastroenterostomy (surgical or endoscopic) may not be feasible[2].
2. Antegrade EUS-GE Direct Method
Step 1: Visualize the target intestinal loop by injecting saline or diluted contrast (methylene blue) distal to the obstruction through a duodenal tube that was previously inserted under endoscopic guidance.
Step 2: Perform an EUS-guided puncture of the small bowel loop adjacent to the gastric wall using a 19-gauge needle.
Step 3: Aspirate; methylene blue aspiration confirms correct localisation of the needle in the jejunum (and not in the transverse colon).
Step 4: Pass either a guidewire through the needle, in order to place a LAMS, or alternatively use directly a cautery-enhanced LAMS (HOT AXIOS; Boston Scientific Corp.).
3. Antegrade EUS-GE Traditional Downstream Method
Step 1: Place a guidewire in the proximal jejunum past the obstruction under endoscopic guidance. Withdraw the endoscope, leaving the guidewire in the jejunum.
Step 2: Over this wire and under fluoroscopic control advance a dilating balloon to the jejunum.
Step 3: From the stomachperform anEUS-guided puncture of the balloonwith a 19-gauge needle.
Step 4: Pass a new guidewire downstream into the jejunum through this needle.
Step 5: Over this guidewiredeploy the LAMS.
4. Antegrade EUS-GE Rendezvous Method
Steps 1 to 3 are the same as in Technique2.
Step 4: Instead of passing a guidewire downstream into the jejunum, the puncturing guidewire is trapped in the dilating balloon that was punctured, or an ERCP extraction balloon and basket, and pulled back through the duodenal obstruction, out of the mouth, securing it.
Step 5: The LAMS is then deployed over this guidewire under traction.
5. Retrograde EUS-EG Enterogastrostomy
Steps 1 to 4 are the same as in Technique 2, with the guidewire secured across the stricture and out of the mouth.
Step 5: Advance a therapeutic endoscope over the guidewire, traversing the obstruction to the point of duodenal/jejunal insertion of the guidewire.
Step 6: Deploy the LAMS from the jejunum (gastric flange opens first)
6. EUS Balloon Occluded GE Bypass (EPASS)
Step 1: Using a double-balloon enteroscope (DBE) place a guidewire in the proximal jejunum.
Step 2: Withdraw the DBE leaving the overtube in the antrum or duodenal bulb.
Step 3: Use a double-balloon-occlusion catheter. This catheter is endowed with two balloons (with 20 cm distance between them). Insert it distal to the obstruction under endoscopic control and theninflate both balloons to fix a segment of duodenum or jejunum. Then fill this segment with contrast.
Step 4: Perform an EUS-guided puncture between these 2 balloons.
Step 5: Deploy the LAMS
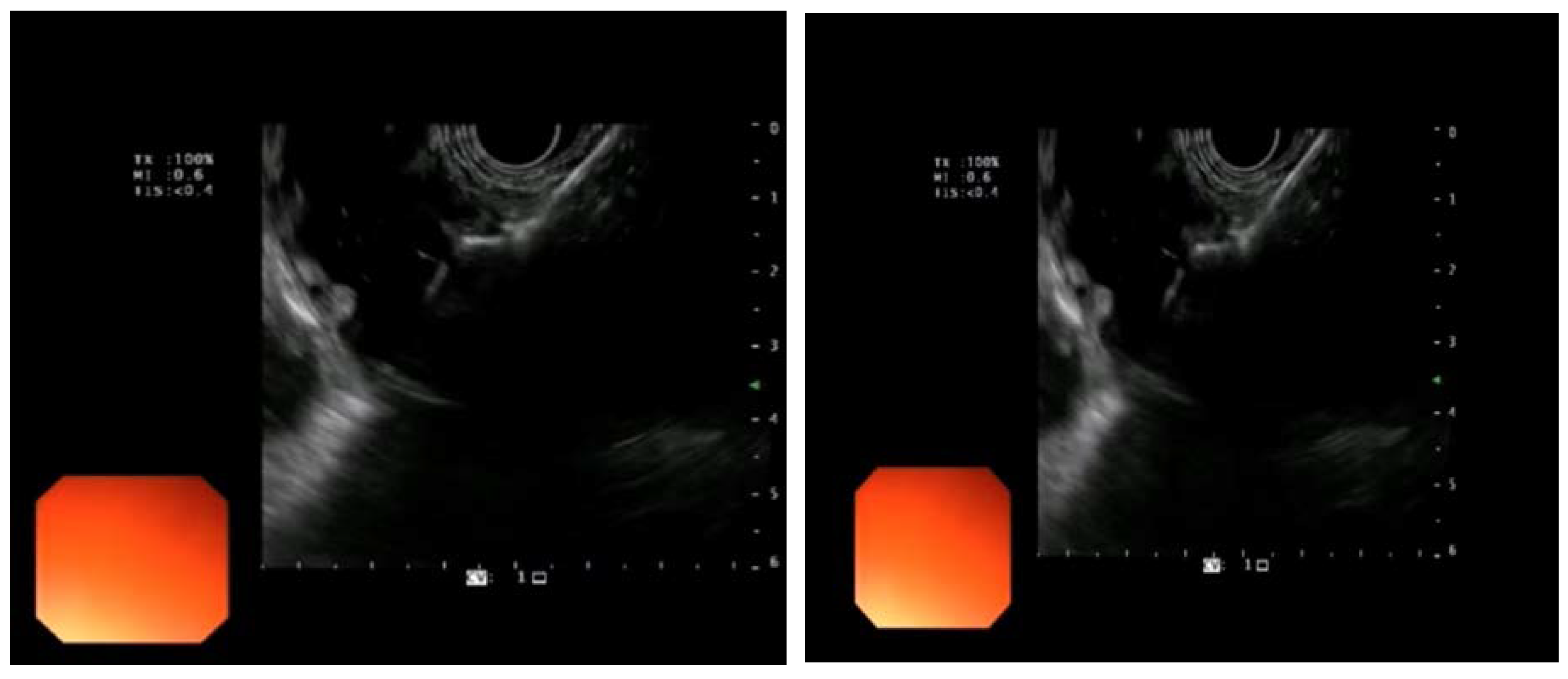
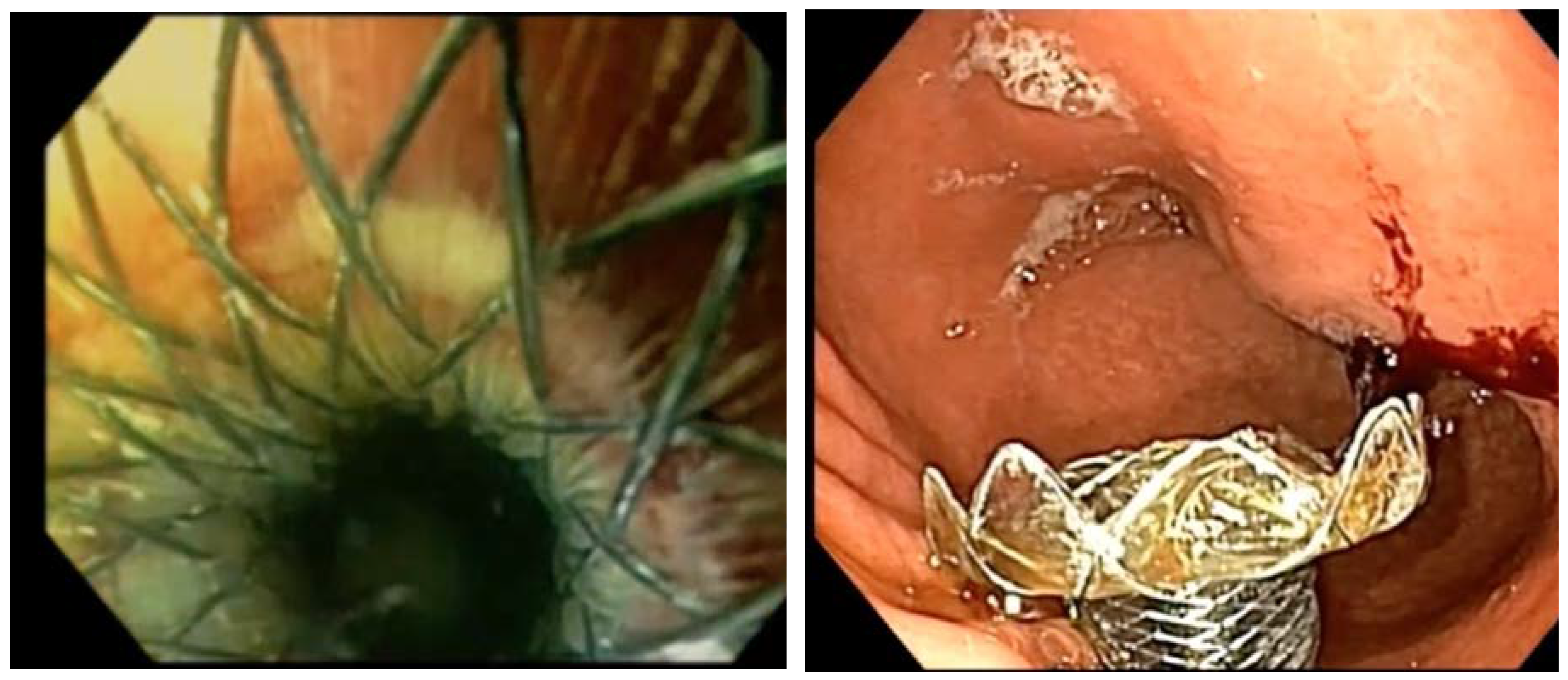
Figure 1.
Images courtesy of Dr. Benedetto Mangiavillano. EUS-guided Gastroenterostomy. (A), (B): placement of LAMS in the jejunal loop, (C), (D): endoscopic view of the gastrojejunostomy.
Figure 1.
Images courtesy of Dr. Benedetto Mangiavillano. EUS-guided Gastroenterostomy. (A), (B): placement of LAMS in the jejunal loop, (C), (D): endoscopic view of the gastrojejunostomy.
Regarding complications of EUS-GE, existing literature shows that EUS-GE is an effective and safe procedure. The first study assessing EUS-GE was a retrospective study by Khashab et al. [16], in which EUS-GE was performed in 10 patients with GOO (3 malignant and 7 benign) by using the direct or the balloon-assisted technique. EUS-GE had a technical success of 90% and clinical success of 100%, while no adverse effects were described. According to a recent review including fourteen studies, technical and clinical success of EUS-GE ranged from 87%–100% and 84%–100%, respectively, irrespective of the technique performed [17,18,19,20]. Another recent systematic review and meta-analysis including twelve, mainly retrospective studies (n=285), conducted by Iqbal et al. [18], assessed the performance of EUS-GE in the treatment of GOO. The pooled technical and clinical success rates were 92% (95% CI: 88%–95%) and 90% (95% CI: 85%–94%), respectively. Wannhof et al. [21] aimed to determine factors affecting technical success in 35 patients underwent EUS-GE for GOO. On multivariate analysis, the distance between the two lumina where LAMS was deployed was the only predictor of technical success, with a cut-off value of 19mm as the best distance.
The rate of adverse effects ranges from 0 to 21%, including stent misdeployment, pneumoperitoneum, gastric leak, bleeding, peritonitis or abdominal pain[22,23]. Itoi et al, reported only a 10% stent misdeployment, but no further AEs were reported and no patients reported stent migration or occlusion needing re-interventionswhen applying the EPASS method[24]. Mahagis et al., described an acute worsening of gastric outlet obstruction following an EUS-GE. The cause was that the LAMS axis was positioned in a sharply angulated orientation towards the afferent limb, thereby creating a closed loop. This was managed by placing a fcSEMS through the LAMS into the efferent loop[25]. The fluctuation of the technical success rates but also of the AE rates may be attributed to its technical difficulty and long learning curve.
Two studies also examined EUS-GE regarding long-term efficacy and patency. In a retrospective study of 57 patients by Kerdsirichairat et al., clinical success was achieved in 89.5% of patients over a median follow-up period of 196 days for patients with malignant GOO and 319.5 days for patients with benign GOO[26]. During the follow-up time, reintervention with upper endoscopy due to recurrence of GOO symptoms was needed in eight patients (15.1%), of whom stent occlusion was present in two. Similarly, On et al. reported that over a median follow-up period of 162 days, reintervention for recurrent GOO was required for only one patient from the 21 with a technically successful EUS-GE and available follow-up data [27].
7. Comparison of the Available Treatments
7.1. Comparison of the Available LAMS
Commonly used types of LAMS include the AXIOS stent (Boston Scientific Corp., Marlborough, MA, USA), which is the type of stent initially used, Niti-S Spaxus stent (Taewoong Medical Co.) and NAGI stent (Taewoong Medical Co., Goyang, Korea). LAMS deployment initially requires the placement of a guidewire and then the expansion of the transluminal tract with a dilation balloon. More recently, electrocautery-enhanced LAMS (EC-LAMS, HOT AXIOS) have been created, permitting puncture, tract dilation and stent deployment in a single-step without the use of a guidewire, thus simplifying the procedure and reducing the risk of complications. Moreover, by avoiding the use of a guidewire, the risk of small bowel moving away from the stomach diminishes [28], thus reducing the risk of misdeployment of the distal flange.
Historically, the 15mm LAMS has been most commonly used for EUS-GE, but recently 20mm LAMS has been developed as an alternative choice. It is hypothesized that the wider lumen of 20mm LAMS may be associated with better patency and improved clinical outcomes, as its lumen size is not divergent from the physiologic gastric outlet size (20 to 23mm)[29]. However, this theoretical advantage may be counterbalanced from increased risk of adverse effects, due to more difficult deployment of the large flange size. In a multicenter retrospective study including 267 patients, Bejjani et al. [30] reported that 20mm LAMS was comparable to the 15mm LAMS concerning efficacy and safety for the treatment of malignant GOO. Notably, more patients in the 20 mm LAMS group tolerated a soft/complete diet. This study along with twelve more, were pooled in a recent meta-analysis assessing the efficacy and safety of 20mm LAMS compared to 15mm LAMS for the treatment of GOO [31]. No difference was found in the pooled technical success rate (20mm: 92,1% vs. 15mm: 93,2%, p=0.47), pooled clinical success rate (89.6% vs. 88.6%, p= 0.62), and pooled adverse event rate (14.7% vs. 11.4%, p= 0.08) between the two groups. However, significant difference was noticed in the pooled reintervention rate, which was significantly decreased for 20mm LAMS (3.5% vs. 10.3%, p= 0.008). Many variables should be considered regarding the stent diameter that should be used in each patient, such as the echoendoscopist’s experience, the selected EUS-GE technique, the etiology of GOO and the anatomy of upper gastrointestinal tract. More data are required to draw more reliable conclusions.
7.2. Comparison for the Different Techniques for EUS-GE
Few data are available concerning the comparison of the available EUS-GE techniques in terms of efficacy and safety. Chen et al., performed a retrospective multicenter study including 74 patients to compare the direct with the balloon-assisted method[32]. Technical success, clinical success and incidence of AEs were similar among the two techniques, while the direct technique was associated with an average of 54.5 minutes shorter procedure duration than the balloon method. Recently, a meta-analysis including 20 studies demonstrated a significant lower AEs rate for the direct technique compared to balloon-assisted techniques, either single-balloon or double balloon (EPASS) (9.3% vs. 21.4%, p=0.001)[33]. The rate of severe AEs was also lower for the direct technique group, although without significant difference between the two groups (3.1% vs 8.2% p=0.099). This comes in contrary to the hypothesis that the direct technique as an unassisted method, would have an increased risk of AEs compared to the balloon-assisted methods [32,33]. Technical and clinical success rates were also similar between the two procedures. In subgroup analysis, no differences were found between the single-balloon or double balloon methods in regard to technical success, clinical success, or procedure time and only the total AEs rate was significantly lower for the single balloon group (8.9% vs. 28.5%, p=0.004).
7.3. Comparison between Methods
7.3.1. EUS-GE vs SGE
So far only a few studies exist, that assess the performance of EUS-GE compared to SGE in malignant GOO. A recent meta-analysis by Bomman et al. pooling six retrospective studies and 484 patients demonstrated that EUS-GE was associated with significantly decreased technical success (95 %CI: 0.054–0.702; P = 0.012; Q = 1.909; I 2 = 0) but had a favorable clinical success rate compared to SGE; however the latter result did not reach statistical significance (OR = 1.566; 95 %CI: 0.585–4.197; P = 0.372). [34]Moreover, EUS-GE was related with a lower rate of adverse effects (OR = 0.295; 95 % CI: 0.172–0.506; P < 0.005; Q = .40: I 2 = 0). This result was expected, given the minimally invasive nature of EUS-GE in contrast to a surgical or laparoscopic intervention such as SGE. The inferiority of EUS-GE in technical success in the aforementioned meta-analysis could be attributed to the fact that as a new intervention it is still technically challenging and demands further expertise. Of note, two more recent studies by Jaruvongvanich et al. and Canakis et al. reported comparable technical success rates for EUS-GE vs SGE in the management of both malignant and benign GOO (98.3 % vs 100 % and 97.9% vs 100%, respectively) [35,36]. In their retrospective study Jaruvongvanich et al. also showed that in a median follow up period of 185.5 days, EUS-GE in comparison with SGE was related with significantly higher clinical success rate (98.3 % vs 90.4 %, P = 0.002), significantly lower reintervention rate for recurrent GOO (0.9 %, and 13.7 %, respectively, P < 0.0001) and lower adverse effects rate, indicating that EUS-GE could secure long-term patency and clinical improvement equally to SGE [36]. Furthermore, EUS-GE compared to SGE required a shorter post-procedure length of hospital stay (MD: –5.95; 95% CI: –6.99 to –4.91; p < 0.001; I2 = 95%) and led to faster resumption of both oral intake and chemotherapy in cases of malignant GOO [35,37]. This is of great importance since these patients often have unresectable tumors and palliative chemotherapy is the only available therapy to improve their prognosis. Altogether, it is apparent that when performed in specialized and experienced centers, EUS-GE is an excellent alternative to SGE as a treatment of GOO, which however needs further standardization and expertise. Thus, more studies, ideally randomized controlled trials comparing these two interventions are essential to reach a more reliable conclusion.
7.3.2. EUS-GE vs. SEMS
A recent meta-analysis including eight studies demonstrated that EUS-GE had significantly higher clinical success (OR, 5.08; 95% CI, 3.42–7.55) and comparable technical success (OR, 0.44; 95% CI, 0.18–1.12) for the management of malignant GOO compared to SEMS.[38] Regarding adverse effects rate, the authors found no statistically significant difference (OR, 0.57; 95% CI, 0.29–1.14). In addition, another meta-analysis with five retrospective studies and 659 patients showed that the rates of both overall and severe (per ASGE Lexicon) adverse effects were similar between EUS-GE and SEMS [39]. This fact is remarkable, given that as a more invasive procedure, EUS-GE would be expected to have more severe adverse effects. Van Wanrooij et al. [40] performed a multicenter retrospective study including 214 patients (107 underwent EUS-GE and 107 SEMS), 176 of which were compared, using propensity score matching. Clinical success of EUS-GE vs SEMS was higher (91 % vs. 75 %; P = 0.008) and stent dysfunction rate was lower for EUS-GE (1 % vs. 26 %; P < 0.001). The median time to clinical success was also shorter for EUS-GE (1 vs. 2 days; P < 0.001), while technical success and median length of hospital stay were similar between the two groups. Furthermore, in a recent retrospective comparative study EUS-GE was associated with a lower rate of reintervention for recurrent GOO (0.9 % vs. 12.2 %, P < 0.0001), and a higher success rate compared to SEMS for the treatment of both malignant and benign GOO [36]. The greater clinical efficacy without the need of reintervention for recurrent GOO, which is observed with EUS-GE compared to SEMS could be explained by the lower incidence of either migration or obstruction of LAMS compared to SEMS. In fact, stent obstruction due to tumor ingrowth occurs in, to as many as 30% patients with uSEMS, since SEMS is often placed through neoplastic tissue. EUS-GE bypasses the obstruction site offering better patency and more durable treatment. Moreover, LAMS are shorter than SEMS (1.5 cm vs 6-12 cm respectively) making food passage through them easier [40]. In summary, EUS-GE is more effective and identically safe to SEMS, with a lower rate of reintervention.
7.3.3. Technique Choice
The advantages and drawbacks of the procedures utilized in the management of GOO are summarized in the Table 1. Current guidelines of the European Society of Gastrointestinal Endoscopy suggest EUS-GE, when performed by experts, as an alternative to SEMS or SGE for the treatment of malignant GOO. For benign GOO, EUS-GE is recommended in patients who are poor surgical candidates, as a weak recommendation based on low-quality evidence [41]. The decision about which treatment to perform is complex and should be individualized, considering patient characteristics, the location and type of obstruction, the presence of ascites and the experience of the endoscopic team. When adequate expertise is available, EUS-GE should be considered as a reliable choice equivalent to SGE for the treatment of malignant GOO, in patients with life expectancy greater than three months. EUS-GE combined with EUS-guided biliary drainage (EUS-BD) is also feasible and efficient when malignant GOO co-exist with biliary obstruction. Double endoscopic bypass offers the advantage of longer patency compared to the traditional methods of SEMS and Endoscopic retrograde cholangiopancreatography (ERCP), since the site of anastomosis is separate from the obstruction site [42]. On the contrary, SEMS could be the preferable option in case of an advanced disease leading to short-life expectancy of less than two to three months, and when EUS-GE is not feasible, for example in the presence of a large volume ascites, malignant ascites or a diffuse infiltration of the gastric wall. Finally, and above all, randomized trials evaluating the performance of EUS-GE compared to the other two methods are required to better determine its role as a treatment option for GOO.
It should be pointed out that in cases where the above-mentioned therapies are contraindicated or have failed, a percutaneous gastrostomy for gastric decompression, combined with subsequent placement of a jejunal feeding tube can provide palliative treatment.

Table 1.
Advantages and disadvantages of techniques employed for managing Gastric Outlet Obstruction.
Table 1.
Advantages and disadvantages of techniques employed for managing Gastric Outlet Obstruction.
| Method | Advantages | Disadvantages |
|---|---|---|
| Surgical Gastroenterostomy | Long-term durability Salvage solution if endoscopic treatments have failed |
Invasive method High morbidity, contraindicated in critically ill patients Gastroparesis |
| SEMS | Less invasive, safe Widely available in daily clinical practice Rapid alleviation of symptoms, early resumption of chemotherapy, oral intake |
High reintervention rate due to stent obstruction |
| EUS-GE | Less invasive, safe procedure compared to SGE Sustained patency, long-term efficacy Rapid alleviation of symptoms, early resumption of chemotherapy, oral intake Feasible in patients with concomitant biliary obstruction |
Not standardized More expertise is required Poor performance in case of uncontrolled ascites, diffuse peritoneal disease, or diffuse Infiltration of gastric wall |
7.3.4. Misdeployment
One of the most common difficulties that endoscopists will encounter during EUS-GE is stent misdeployment (SM). Collectively, the rate of SM ranges from 6.8% to 27%, even in expert hands [9]. For this reason, advanced endoscopists declare this method as a technically challenging procedure. Furthermore, misdeployment associated adverse events have hindered its dissemination thus far[9].
Currently, there is only one multicentric retrospective study that examines this issue and ways to manage it[9].EUS-GE was performed with either the direct method or the antegrade EUS-GE traditional downstream method in 467 patients. The SM rate of this study was 9.85%. Interestingly, 73.2% of SM occurred during the first 13 EUS-GE cases of the performing endoscopists, with only 17% occurring after 25 cases. For this reason, ESGE recommends that this procedure takes place only in expert centres [43].
This study observed and classified misdeployment into four types; these were the following: Type I occurs when the distal flange is deployed in the peritoneum with no puncture of the small intestine (rate: 63.1%). Type II happens when the distal flange in deployed in the peritoneum, but puncture of small intestine was achieved (rate: 30.4%). Type III refers to the deployment of the proximal flange in the peritoneum, which was observed only once and Type IV refers to the deployment of the distal flange in the colon, thus creating a gastrocolic anastomosis whichoccurred twice. Overall, the adverse events that resulted from SM were graded as mild in 28 (60.9%) patients, moderate in 11 (23.9%) patients, severe in 6 (13.0 %) patients, and fatal in 1 (2.2%) patient. Only 5 (10.9%) patients required surgical intervention[9].Following salvage strategies were implemented to correct SM.
- For SM Type 1 removal of the LAMS and closure of the gastrotomy can be performed using over-the-scope clips (OTSCs), through-the-scope clips (TTSCs) or endoscopic suturing,while two patients were managed conservatively without any closure of the gastrotomy, both recovering with no adverse events.Same-session endoscopic salvage management of GOO can be performed, via EUS-GE at the same or different gastric site, change of method and placement of a duodenal stent or balloon dilatation. In this cohort 3 patients were operated due to clinical signs of peritonitis and a SGE was performed[9]. Overall, most Type I SM events were rated as mild (n=22, 75.9%), two were moderate (6.9%), and 5 severe (17.2%). The 5 severe cases included the 3 patients who underwent surgical intervention and 2 patients who required ICU admission[9].
- For Type II SM, LAMS was removed and a new LAMS using the same EUS-GE method or NOTES (natural orifice translumenal endoscopic surgery) was placed; alternatively a fcSEMS through the initial misdeployed LAMSwas placed to bridge the gap. Endoscopic closure of the gastrotomy onlywith OTSC or TTSC is an alternative. These patients developed abdominal pain requiring narcotics (n=2), pneumoperitoneum requiring drainage (n=1) or no adverse events (n=2). These patients were treated either with a duodenal stent during the same session or with subsequent SGE. Only half of Type II SM patients experienced adverse events; abdominal pain requiring narcotics was the most common (28.6%). Overall, the majority of the Type II SM adverse events were rated as mild (n=6, 42.9%) or moderate (n=7; 50.0%).Overall, one patient was operated due to peritonitis[9].
- For the one case of Type III SM NOTES was used to reposition the proximal flange into the stomach, but it was not successful. For this reason, the LAMS had to be removed surgically and a SGE was performed. [9]
- Type IV SM occurred twice with one being recognized intraprocedurally, whereas the other was identified 3 weeks later due to diarrhea induced by food intake. In both cases, LAMS was removed about 4 weeks after the initial EUS-GE, along with concomitant endoscopic closure of the inadvertent anastomosis via endoscopic suturing in one and TTS in the other. [9]
An additional alternative salvage treatment in cases of SM was proposed by Fabbri et al. The authors performed a laparoscopic assisted EUS-guided gastroenterostomy [44].
To acquire a proper understanding of the procedure and effectively mitigate the risks of complications, including stent misdeployment, novice echoendoscopists may consider following these expert-recommended instructions: careful review of available videos of EUS-GE, discussions with colleagues experienced in EUS-GE and a well-thought-out plan in case of stent misdeployment. Additionally, the initial placements should be done in the operating room with surgical backup[45].
8. Conclusions and Future Perspectives
Irrespective of the etiology (malignant or benign) an efficient, durable and safe intervention to alleviate GOO is essential in order to improve patient quality of life and prognosis. It is now apparent that in the hands of experts, EUS-GE is effective for the treatment of GOO and safer than the previous therapies, SEMS and SGE. This procedure integrates the advantages of the other two methods, providing long-term patency and efficacy without need of reinterventions of SGE, with a favorable safety profile such as SEMS. Nonetheless, most reports of EUS-GE arise from experienced centers, where this procedure is mainly used. EUS-GE is still technically challenging for many endoscopists and must be simplified and standardized further to be more commonly applied in clinical practice [46].
Therefore, in order for this method to become widely adopted, more endoscopists need to receive training on this procedure. Currently, there are not a lot of recommendations concerning this topic published in the literature reflecting lack of high evidence level studies.
Author Contributions
D.Z.; Conceptualization, methodology, writing—original draft preparation writing, review and editing, T.V.; Conceptualization, methodology, writing—original draft preparation writing, review and editing, I. P.; Conceptualization, writing—review and editing, supervision, C. K.; Writing - review & editing, G. T.; Writing - original draft preparation, P. G.; Writing - original draft preparation, E. K.; writing—original draft preparation, A.F. .; writing—original draft preparation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Koop, A.H.; Palmer, W.C.; Stancampiano, F.F. Gastric outlet obstruction: A red flag, potentially manageable. Cleveland Clinic journal of medicine 2019, 86, 345-353. [CrossRef]
- Irani, S.; Baron, T.H.; Itoi, T.; Khashab, M.A. Endoscopic gastroenterostomy: techniques and review. Curr Opin Gastroenterol 2017, 33, 320-329. [CrossRef]
- Carbajo, A.Y.; Kahaleh, M.; Tyberg, A. Clinical Review of EUS-guided Gastroenterostomy (EUS-GE). J Clin Gastroenterol 2020, 54, 1-7. [CrossRef]
- Papanikolaou, I.S.; Siersema, P.D. Gastric Outlet Obstruction: Current Status and Future Directions. Gut Liver 2022, 16, 667-675. [CrossRef]
- Troncone, E.; Fugazza, A.; Cappello, A.; Del Vecchio Blanco, G.; Monteleone, G.; Repici, A.; Teoh, A.Y.B.; Anderloni, A. Malignant gastric outlet obstruction: Which is the best therapeutic option? World journal of gastroenterology 2020, 26, 1847-1860. [CrossRef]
- Sigmon DF, L.P. Gastrojejunostomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan- [Updated 2023 Jul 24]. .
- Kumar, A.; Chandan, S.; Mohan, B.P.; Atla, P.R.; McCabe, E.J.; Robbins, D.H.; Trindade, A.J.; Benias, P.C. EUS-guided gastroenterostomy versus surgical gastroenterostomy for the management of gastric outlet obstruction: a systematic review and meta-analysis. Endosc Int Open 2022, 10, E448-E458. [CrossRef]
- Cheung, S.L.H.; Teoh, A.Y.B. Optimal Management of Gastric Outlet Obstruction in Unresectable Malignancies. Gut and liver 2022, 16, 190-197. [CrossRef]
- Ghandour, B.; Bejjani, M.; Irani, S.S.; Sharaiha, R.Z.; Kowalski, T.E.; Pleskow, D.K.; Do-Cong Pham, K.; Anderloni, A.A.; Martinez-Moreno, B.; Khara, H.S.; et al. Classification, outcomes, and management of misdeployed stents during EUS-guided gastroenterostomy. Gastrointestinal endoscopy 2022, 95, 80-89. [CrossRef]
- Jeurnink, S.M.; Repici, A.; Luigiano, C.; Pagano, N.; Kuipers, E.J.; Siersema, P.D. Use of a colonoscope for distal duodenal stent placement in patients with malignant obstruction. Surgical endoscopy 2009, 23, 562-567. [CrossRef]
- Park, J.M.; Min, B.H.; Lee, S.H.; Chung, K.H.; Lee, J.M.; Song, B.J.; Lee, J.K.; Ryu, J.K.; Kim, Y.T. Feasibility of self-expandable metal stent placement with side-viewing endoscope for malignant distal duodenal obstruction. Digestive diseases and sciences 2015, 60, 524-530. [CrossRef]
- van Halsema, E.E.; Rauws, E.A.; Fockens, P.; van Hooft, J.E. Self-expandable metal stents for malignant gastric outlet obstruction: A pooled analysis of prospective literature. World journal of gastroenterology 2015, 21, 12468-12481. [CrossRef]
- Kim, I.D.; Kang, D.H.; Choi, C.W.; Kim, H.W.; Jung, W.J.; Lee, D.H.; Chung, C.W.; Yoo, J.J.; Ryu, J.H. Prevention of covered enteral stent migration in patients with malignant gastric outlet obstruction: a pilot study of anchoring with endoscopic clips. Scandinavian journal of gastroenterology 2010, 45, 100-105. [CrossRef]
- Binmoeller, K.F.; Shah, J.N. Endoscopic ultrasound-guided gastroenterostomy using novel tools designed for transluminal therapy: a porcine study. Endoscopy 2012, 44, 499-503. [CrossRef]
- Irani, S.; Itoi, T.; Baron, T.H.; Khashab, M. EUS-guided gastroenterostomy: techniques from East to West. VideoGIE : an official video journal of the American Society for Gastrointestinal Endoscopy 2020, 5, 48-50. [CrossRef]
- Khashab, M.A.; Kumbhari, V.; Grimm, I.S.; Ngamruengphong, S.; Aguila, G.; El Zein, M.; Kalloo, A.N.; Baron, T.H. EUS-guided gastroenterostomy: the first U.S. clinical experience (with video). Gastrointest Endosc 2015, 82, 932-938. [CrossRef]
- Harb, M.; Kamath, A.; Marx, G.; Gupta, S. Outcomes of endoscopic ultrasound-guided gastro-enterostomy for gastric outlet obstruction in a two-centre Australian Cohort (with video). Asia Pac J Clin Oncol 2023. [CrossRef]
- Iqbal, U.; Khara, H.S.; Hu, Y.; Kumar, V.; Tufail, K.; Confer, B.; Diehl, D.L. EUS-guided gastroenterostomy for the management of gastric outlet obstruction: A systematic review and meta-analysis. Endosc Ultrasound 2020, 9, 16-23. [CrossRef]
- Kahaleh, M.; Tyberg, A.; Sameera, S.; Sarkar, A.; Shahid, H.M.; Abdelqader, A.; Gjeorgjievski, M.; Gaidhane, M.; Muniraj, T.; Jamidar, P.A.; et al. EUS-guided Gastroenterostomy: A Multicenter International Study Comparing Benign and Malignant Diseases. J Clin Gastroenterol 2023. [CrossRef]
- Tonozuka, R.; Tsuchiya, T.; Mukai, S.; Nagakawa, Y.; Itoi, T. Endoscopic Ultrasonography-Guided Gastroenterostomy Techniques for Treatment of Malignant Gastric Outlet Obstruction. Clin Endosc 2020, 53, 510-518. [CrossRef]
- Wannhoff, A.; Ruh, N.; Meier, B.; Riecken, B.; Caca, K. Endoscopic gastrointestinal anastomoses with lumen-apposing metal stents: predictors of technical success. Surg Endosc 2021, 35, 1997-2004. [CrossRef]
- Chen, Y.I.; Itoi, T.; Baron, T.H.; Nieto, J.; Haito-Chavez, Y.; Grimm, I.S.; Ismail, A.; Ngamruengphong, S.; Bukhari, M.; Hajiyeva, G.; et al. EUS-guided gastroenterostomy is comparable to enteral stenting with fewer re-interventions in malignant gastric outlet obstruction. Surgical endoscopy 2017, 31, 2946-2952. [CrossRef]
- Perez-Miranda, M.; Tyberg, A.; Poletto, D.; Toscano, E.; Gaidhane, M.; Desai, A.P.; Kumta, N.A.; Fayad, L.; Nieto, J.; Barthet, M.; et al. EUS-guided Gastrojejunostomy Versus Laparoscopic Gastrojejunostomy: An International Collaborative Study. Journal of clinical gastroenterology 2017, 51, 896-899. [CrossRef]
- Itoi, T.; Ishii, K.; Ikeuchi, N.; Sofuni, A.; Gotoda, T.; Moriyasu, F.; Dhir, V.; Teoh, A.Y.; Binmoeller, K.F. Prospective evaluation of endoscopic ultrasonography-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) for malignant gastric outlet obstruction. Gut 2016, 65, 193-195. [CrossRef]
- Magahis, P.T.; Westerveld, D.; Salgado, S.; Carr-Locke, D.L.; Sampath, K.; Sharaiha, R.Z.; Mahadev, S. Acute worsening of gastric outlet obstruction following EUS-guided gastrojejunal bypass. VideoGIE : an official video journal of the American Society for Gastrointestinal Endoscopy 2023, 8, 235-238. [CrossRef]
- Kerdsirichairat, T.; Irani, S.; Yang, J.; Brewer Gutierrez, O.I.; Moran, R.; Sanaei, O.; Dbouk, M.; Kumbhari, V.; Singh, V.K.; Kalloo, A.N.; Khashab, M.A. Durability and long-term outcomes of direct EUS-guided gastroenterostomy using lumen-apposing metal stents for gastric outlet obstruction. Endosc Int Open 2019, 7, E144-E150. [CrossRef]
- On, W.; Huggett, M.T.; Young, A.; Pine, J.; Smith, A.M.; Tehami, N.; Maher, B.; Pereira, S.P.; Johnson, G.; Paranandi, B. Endoscopic ultrasound guided gastrojejunostomy in the treatment of gastric outlet obstruction: multi-centre experience from the United Kingdom. Surg Endosc 2023, 37, 1749-1755. [CrossRef]
- Yi, H.; Liu, Q.; He, S.; Zhong, L.; Wu, S.H.; Guo, X.D.; Ning, B. Current uses of electro-cautery lumen apposing metal stents in endoscopic ultrasound guided interventions. Front Med (Lausanne) 2022, 9, 1002031. [CrossRef]
- Sobani, Z.A.; Paleti, S.; Rustagi, T. Endoscopic ultrasound-guided gastroenterostomy using large-diameter (20 mm) lumen apposing metal stent (LLAMS). Endosc Int Open 2021, 9, E895-E900. [CrossRef]
- Bejjani, M.; Ghandour, B.; Subtil, J.C.; Martinez-Moreno, B.; Sharaiha, R.Z.; Watson, R.R.; Kowalski, T.E.; Benias, P.C.; Huggett, M.T.; Weber, T.; et al. Clinical and technical outcomes of patients undergoing endoscopic ultrasound-guided gastroenterostomy using 20-mm vs. 15-mm lumen-apposing metal stents. Endoscopy 2022, 54, 680-687. [CrossRef]
- Vedantam, S.; Shah, R.; Bhalla, S.; Kumar, S.; Amin, S. No difference in outcomes with 15 mm vs. 20 mm lumen-apposing metal stents for endoscopic ultrasound-guided gastroenterostomy for gastric outlet obstruction: a meta-analysis. Clin Endosc 2023, 56, 298-307. [CrossRef]
- Chen, Y.I.; Kunda, R.; Storm, A.C.; Aridi, H.D.; Thompson, C.C.; Nieto, J.; James, T.; Irani, S.; Bukhari, M.; Gutierrez, O.B.; et al. EUS-guided gastroenterostomy: a multicenter study comparing the direct and balloon-assisted techniques. Gastrointest Endosc 2018, 87, 1215-1221. [CrossRef]
- Ribas, P.; De Moura, D.T.H.; Proenca, I.M.; Do Monte Junior, E.S.; Yvamoto, E.Y.; Hemerly, M.C.; De Oliveira, V.L.; Ribeiro, I.B.; Sanchez-Luna, S.A.; Bernardo, W.M.; De Moura, E.G.H. Endoscopic Ultrasound-Guided Gastroenterostomy for the Palliation of Gastric Outlet Obstruction (GOO): A Systematic Review and Meta-analysis of the Different Techniques. Cureus 2022, 14, e31526. [CrossRef]
- Bomman, S.; Ghafoor, A.; Sanders, D.J.; Jayaraj, M.; Chandra, S.; Krishnamoorthi, R. Endoscopic ultrasound-guided gastroenterostomy versus surgical gastrojejunostomy in treatment of malignant gastric outlet obstruction: Systematic review and meta-analysis. Endosc Int Open 2022, 10, E361-E368. [CrossRef]
- Canakis, A.; Bomman, S.; Lee, D.U.; Ross, A.; Larsen, M.; Krishnamoorthi, R.; Alseidi, A.A.; Adam, M.A.; Kouanda, A.; Sharaiha, R.Z.; et al. Benefits of EUS-guided gastroenterostomy over surgical gastrojejunostomy in the palliation of malignant gastric outlet obstruction: a large multicenter experience. Gastrointest Endosc 2023, 98, 348-359 e330. [CrossRef]
- Jaruvongvanich, V.; Mahmoud, T.; Abu Dayyeh, B.K.; Chandrasekhara, V.; Law, R.; Storm, A.C.; Levy, M.J.; Vargas, E.J.; Marya, N.B.; Abboud, D.M.; et al. Endoscopic ultrasound-guided gastroenterostomy for the management of gastric outlet obstruction: A large comparative study with long-term follow-up. Endosc Int Open 2023, 11, E60-E66. [CrossRef]
- Martins, R.K.; Brunaldi, V.O.; Fernandes, A.L.; Otoch, J.P.; Artifon, E.L.A. Palliative therapy for malignant gastric outlet obstruction: how does the endoscopic ultrasound-guided gastroenterostomy compare with surgery and endoscopic stenting? A systematic review and meta-analysis. Ther Adv Gastrointest Endosc 2023, 16, 26317745221149626. [CrossRef]
- Miller, C.; Benchaya, J.A.; Martel, M.; Barkun, A.; Wyse, J.M.; Ferri, L.; Chen, Y.I. EUS-guided gastroenterostomy vs. surgical gastrojejunostomy and enteral stenting for malignant gastric outlet obstruction: a meta-analysis. Endosc Int Open 2023, 11, E660-E672. [CrossRef]
- Chandan, S.; Khan, S.R.; Mohan, B.P.; Shah, A.R.; Bilal, M.; Ramai, D.; Bhogal, N.; Dhindsa, B.; Kassab, L.L.; Singh, S.; et al. EUS-guided gastroenterostomy versus enteral stenting for gastric outlet obstruction: Systematic review and meta-analysis. Endosc Int Open 2021, 9, E496-E504. [CrossRef]
- van Wanrooij, R.L.J.; Vanella, G.; Bronswijk, M.; de Gooyer, P.; Laleman, W.; van Malenstein, H.; Mandarino, F.V.; Dell'Anna, G.; Fockens, P.; Arcidiacono, P.G.; et al. Endoscopic ultrasound-guided gastroenterostomy versus duodenal stenting for malignant gastric outlet obstruction: an international, multicenter, propensity score-matched comparison. Endoscopy 2022, 54, 1023-1031. [CrossRef]
- van der Merwe, S.W.; van Wanrooij, R.L.J.; Bronswijk, M.; Everett, S.; Lakhtakia, S.; Rimbas, M.; Hucl, T.; Kunda, R.; Badaoui, A.; Law, R.; et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 185-205. [CrossRef]
- Brewer Gutierrez, O.I.; Nieto, J.; Irani, S.; James, T.; Pieratti Bueno, R.; Chen, Y.I.; Bukhari, M.; Sanaei, O.; Kumbhari, V.; Singh, V.K.; et al. Double endoscopic bypass for gastric outlet obstruction and biliary obstruction. Endosc Int Open 2017, 5, E893-E899. [CrossRef]
- van Wanrooij, R.L.J.; Bronswijk, M.; Kunda, R.; Everett, S.M.; Lakhtakia, S.; Rimbas, M.; Hucl, T.; Badaoui, A.; Law, R.; Arcidiacono, P.G.; et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Technical Review. Endoscopy 2022, 54, 310-332. [CrossRef]
- Fabbri, C.; Binda, C.; Fugazzola, P.; Sbrancia, M.; Tomasoni, M.; Coluccio, C.; Jung, C.F.M.; Prosperi, E.; Agnoletti, V.; Ansaloni, L. Hybrid gastroenterostomy using a lumen-apposing metal stent: a case report focusing on misdeployment and systematic review of the current literature. World journal of emergency surgery : WJES 2022, 17, 6. [CrossRef]
- Baron, T.H. EUS gastroenterostomy: Why do bad things happen to good procedures? Gastrointest Endosc 2022, 95, 90-91. [CrossRef]
- Park, K.H.; Rosas, U.S.; Liu, Q.Y.; Jamil, L.H.; Gupta, K.; Gaddam, S.; Nissen, N.; Thompson, C.C.; Lo, S.K. Safety of teaching endoscopic ultrasound-guided gastroenterostomy (EUS-GE) can be improved with standardization of the technique. Endosc Int Open 2022, 10, E1088-E1094. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



