
Submitted:
05 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
Suicide remains a persistent global health challenge, resisting widespread prevention efforts. According to previous findings, toxoplasmosis is particularly associated with altered deci-sion-making, which could lead to risk-taking behavior thereby increasing the likelihood for sui-cidal behavior (SB). In addition, discussion about the role of microbiome in psychiatric disorders has emerged lately, which also makes it relevant to investigate its role in the context of SB. Therefore, the current review aimed to comprehensively summarize existing knowledge regard-ing the association between microbial pathogens and SB. We conducted a systematic search with keywords including suicide and Toxoplasma gondii (Suicid* AND Toxoplasm*) and microbiome (Microbiome AND Suicid*) throughout PubMed to retrieve the related studies up to 09.11.2023. Most results reported significant association between toxoplasmosis and SB, suggesting a higher likelihood of SB in the infected population. Regarding the microbiome, only very few studies in-vestigated an association between SB and alterations in microbiota. Based on those few studies, changes in the microbiome were significantly associated with SB. The cognitive aspects of deci-sion-making in T. gondii infected individuals with SB should be further investigated to unravel underlying mechanisms. Further sufficiently powered studies are needed to establish a link be-tween SB and gut microbiota.
Keywords:
toxoplasmosis
; microbiome
; suicide
; suicidal behavior
1. Introduction
Suicide remains one of the major public health concerns. Every year, more than 700,000 people commit suicide worldwide and up to 20 times as many people attempt suicide [1]. In fact, among individuals aged 15-29 years, suicide was the third leading cause of death among girls and young women and the fourth most common cause of death among boys and young men in 2019 [2]. According to the United Nations, more people die by suicide every year than by both homicide and war [3]. Although research in the last three decades has improved our knowledge about suicide [4], it still has a limited impact on suicide prediction and prevention. Moreover, the crude suicide rate, for example, in the US rose from 11.03 to 16.14 (per 100,000), thus by nearly 46% between 2000 and 2019 [2].
One of the problems in researching suicidal phenomena is the inconsistency of the terms previously used to describe suicidal behavior (SB) [5], leading to a variety of reported cause and risk factors [6], which made our understanding of SB more difficult. According to the definitions provided by the US Centers for Disease Control and Prevention, suicidal ideation (SI) corresponds to thoughts, plans and considerations of suicide. A suicide attempt (SA) is considered as a self-directed violence with the intention to die, often resulting in nonfatal injuries [7,8]. In 2013, the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) suggested ´suicidal behavior disorder´ (SBD) as a possible independent category [9]. SBD has been defined as a condition for further Study, thus considering it not solely as a symptom of a major depressive disorder (MDD), bipolar disorder (BD), or borderline personality disorder (BPD). Recent studies have provided clear evidence that SB is ubiquitous in psychiatric disorders, but can also occur in a crisis without fulfilling the criteria of a psychiatric diagnosis, indicating the need to identify specific risk factors for SB and to develop suicide-specific interventions [10,11,12,13,14]. Furthermore, by explicitly differentiating SBD from nonsuicidal self-injury (NSSI), DSM-5 has put a strong emphasis on the intention of the individual at the time when the behaviors occur. Because of the complexity and multifactorial pathophysiological mechanisms leading to SB, our current knowledge to predict which persons will turn their suicidal thoughts into action is still very limited [15].
A widely accepted explanation for the etiology of SB is the stress-diathesis model, which explains the manifestation of SB through the interaction of two main components: stress and diathesis [16]. On the one hand, acute or chronic stress factors play a role in the transition from suicidal ideations to an act, for example, interpersonal problems as well as mental disorders. On the other hand, diathesis makes individuals vulnerable to suicidal behavior. The diathesis has been operationalized as suicide-related traits that increase the chance that a person experiencing stress might respond to it by suicidal behavior [17]. For example, specific genetic, epigenetic and neurobiological factors, such as specific polygenetic risk factors [18], specific transcriptomic features [19], decreased cortical thickness in prefrontal regions [20] or altered connectomes in individuals with SB and relatives of suicide victims [21]. Furthermore, specific psychological factors such as sensitivity to social stressors [22], abnormal processing of negative stimuli [23], and elevated levels of mental pain [24] are assumed to increase the likelihood of suicidal behavior.
In addition, alterations in neurocognitive functioning and especially decision-making (DM) have been consistently found in individuals with SB [25,26], making them a characteristic feature of SB. A recent systematic review of 46 studies [27] clearly showed altered decision-making in suicide attempters under conditions of uncertainty, showing riskier and less advantageous choices than psychiatric and healthy controls. The authors concluded that “DM impairment could be considered as a cognitive trait of suicidal vulnerability, a risk factor and an attribute of SAs.”
In a recent publication by our group, Lubbert, Bahlmann [28] reported significantly higher levels of a personality trait, i.e., sensation seeking, in suicide attempters who used violent suicidal means compared to suicide attempters. Higher sensation-seeking scores may represent a clinical correlate of riskier DM in violent attempters than in nonviolent attempters, as outlined in a recent meta-analysis [29].
Furthermore, previous studies indicated a potential association between neurocognitive deficits and inflammatory biomarkers [9,30,31]. As reported in the review by Courtet, Giner [32], a relatively consistent association between suicide and inflammatory cytokines in the orbitofrontal cortex, the brain region involved in the process of reward-related decision-making and affective control, was demonstrated in postmortem studies. A possible involvement of microglial cells, which are activated during neuroinflammation, has also been discussed in connection with suicidal behavior [33]. Significantly higher levels of peripheral C-reactive protein (CRP) have been found in individuals with suicidal behavior in contrast to participants with depressive disorders as well as healthy individuals [34]. However, there is a limited understanding of other potentially relevant factors such as the gut microbiome or toxoplasmosis, which may act as internal and external triggers for SB. There is growing evidence to consider human-associated microbes as a major player in immunological processes [35,36]. The gut-brain axis (GBA) has therefore become a recent focus of psychiatric research, and is increasingly recognized as an emerging area that could promote better understanding of mental disorders and help to develop new diagnostic and therapeutic biomarkers [37]. The gut microbiota refers to the collection of all microorganisms living in the gut. The composition of the microbiota is individual in each organism and is influenced by environmental factors such as smoking, alcohol consumption and diet [38]. Given the gut microbiome has a strong influence on immune-inflammatory processes, and specifically on stress responses, both are linked to SB [39], changes in the gut microbiome could thus increase the risk of suicidal behavior.
Moreover, microbial alterations and pathogens such as Toxoplasma gondii parasites can also lead to inflammatory processes in the central nervous system (CNS), affecting the host’s behavior. There is some evidence of a link between toxoplasmosis and suicidal behavior, which will be presented in detail in this systematic review.
1.1. Toxoplasmosis and Suicidal Behavior
Toxoplasmosis is a common zoonotic disease caused by the intracellular protozoan Toxoplasma gondii (T. gondii) which exists in roughly one-third of the world's population [40]. The global prevalence of toxoplasmosis is continuously rising. According to the U.S. Centers for Disease Control and Prevention, over 60 million individuals in the United States may have contracted the infection and in certain regions, prevalence rates are as high as 95% [41]. The most common routes of disease transmission to humans are through oral ingestion of tissue cysts containing bradyzoites, often found in undercooked or raw meat, or by food containing oocysts excreted in the feces of infected cats and by consumption of contaminated water [42,43]. On rare occasions, infection can be obtained through the transfer of tachyzoites from a pregnant mother to her unborn child across the placenta or via blood transfusions and organ transplants [44]. The clinical representation of infection in healthy subjects is in 90% of cases asymptomatic or only with mild symptoms. However, in pregnancy, the parasite might lead to several complications, such as miscarriage and damage to the baby´s eyes and brain, which later lead to psychomotor or mental disorders in infants [45].
According to earlier findings, toxoplasmosis was particularly associated with altered decision-making in nonhumans and humans. Animal models have demonstrated a strong relationship between T. gondii infection and increased risk-taking behaviors [46]. For example, mice infected with T. gondii appear to exhibit altered behavior, i.e., they are attracted to cats instead of avoiding them, which increases the likelihood that they will be caught. They are more likely to explore the novel areas in mazes and display themselves in open spaces [47,48]. Risk-taking behavior has been observed not only in T. gondii-infected rodents but also in nonfeline chronically infected mammals such as wolves and chimpanzees. Wolves with a positive serological status demonstrated a higher tendency to take high-risk actions such as dispersal and assuming the role of a pack leader [49]. Furthermore, Toxoplasma-infected chimpanzees showed loss of innate aversion toward the urine of their natural predators. They more frequently approached and investigated leopard urine than noninfected individuals [50]. The changes in the brain associated with the infection that lead to increased risk behavior are complicated and not fully understood. However, a high parasite cyst density has been shown in the amygdala [48], an important brain region for the processing of fear and, more generally, for the recognition of salient information.
Similar changes in decision-making have been suspected in T. gondii infected humans. Similar to infected mice, humans might also be more likely to show risky behavior when carrying latent toxoplasmosis, for instance, not wearing a helmet while riding a motorcycle, engaging in traffic accidents or attempting a suicide [51,52,53]. Retrospective examinations showed significant associations between T. gondii seropositivity and outcomes such as car accidents, drug abuse and committed suicide [54]. These results illustrate that parasites might carry significant consequences for intermediary hosts, extending beyond immediate infections to influence behavior. In social species, these effects can extend beyond individual organisms, impacting even groups through altering social interaction patterns. Therefore, we hypothesize that toxoplasmosis plays a role in SB by altering decision-making processes toward riskier choices.
Several studies have examined T. gondii seropositivity among suicide victims and suicide attempters. However, previous findings are inconsistent, and the underlying mechanisms remain unclear. Soleymani, Faizi [53] systematically reviewed 16 studies in which eight papers reported no association, seven papers revealed a positive association and one a negative association between T. gondii and suicide. Nevertheless, the overall rate of suicide was higher in people with T. gondii infection than in those without infection. Taking into account that Soleymani, Faizi [53] only included studies published until March 2019, we have conducted systematic search of the papers reporting a possible link between T. gondii and suicide to test our hypothesis. To reduce potential heterogeneity between previous studies due to the definition of suicidal behavior, studies were included in this systematic review, which clearly differentiated suicidal self-harm from NSSI or suicidal ideations in terms of intent to die as defined by DSM-5.
1.2. Gut-Brain Axis
The interaction of the gastrointestinal tract and the brain has been considered a ´gut-brain axis´. It is a bidirectional and dynamic communication network between the gut and brain that is modulated by the gut microbiota. Dysbiosis, i.e. disruption of the microbiome, results in changes in the production of microbial metabolites, e.g. including the short-chain fatty acids (SCFAs) acetic acid, propionic acid, and butyric acid, which have significant functions in the central nervous system [55]. The gut microbiome has a significant impact on the development of the hypothalamic‒pituitary‒adrenal (HPA) axis, which is primarily known for its role in mediating the stress response. Sudo, Chida [56] demonstrated that germ-free (GF) mice, compared to control mice, respond to mild stress with an increased release of adrenocorticotropic hormone (ACTH) and corticosterone. Conversely, chronic stress could be associated with long-lasting effects on various aspects of immune homeostasis, reduced diversity in the microbiome, increased susceptibility to infectious diseases, and altered inflammatory responses, as observed in various psychiatric disorders [35].
In recent decades, accumulating research has shown that the interplay between the brain, gut, and microbiota is implicated in the development of depression [57,58,59,60]. The vast majority of our understanding of how microbes affect mental function has come from preclinical studies in rodent models [61]. However, a growing body of research analyzing the microbiome in clinical cohorts has emerged, revealing variances across diverse taxonomic levels, albeit with occasional inconsistencies in the findings. Most consistently, elevated levels of bacteria have been linked to increased inflammation and a decrease in anti-inflammatory bacteria. Furthermore, the microbiome is intricately connected to numerous physiological aspects relevant to depression, encompassing neurotransmission, neural plasticity, stress modulation, immune response, and metabolic factors [35]. Previous studies suggest that alterations in the gut microbiome are also associated with metabolic disturbances in individuals with depression [62], which might be explained by differences in diet since diet is also a confound of microbiome composition. A longitudinal study revealed a correlation between poor nutrition and depression, whereas a healthy diet was associated with lower depressive symptoms [63]. Not only in individuals with an affective disorder, but also in individuals with SB the association between fast food consumption and past SB was reported when controlling for food insecurity, obesity, physical exercise, and consumption of fruits and vegetables in 32 countries [64]. People at risk of suicide appear to exhibit negative health-promoting behavior [65], which might be associated with alterations in the microbiome. Very few studies investigated the association between suicidal behavior and microbiome. To date, no systematic review has been conducted summarizing existing knowledge about the association between the microbiome and suicidal behavior. We aimed to outline the role of the microbiome as an additional internal factor that might increase vulnerability to suicidal behavior and summarize actual findings.
The aim of this systematic review is therefore to evaluate the findings on the role of T. gondii and of the microbiome in suicidal behavior and discuss possible mechanisms of how they could contribute to the transition from SI to SB.
2. Methods
Search Strategy
We adopted the systematic review guidelines provided by the PRISMA statement [66]. According to the PICOS principles, we selected analytical studies including case‒control, cohort, and cross‒sectional studies that reported an association between T. gondii infection (as a predictor) and suicide (as an outcome) in all age and sex groups of the population, including postmortem studies. All reviews and meta-analyses were excluded. In addition, we did not set any time limitation on the selection of the studies. We conducted a systematic search throughout the PubMed database to retrieve related studies up to 9 November 2023.
Two major keywords, suicide and T. gondii (Suicid* AND Toxoplasm*), were used to construct a search strategy for database. We selected those studies that assessed the association of T. gondii with suicide.
Studies were eligible for inclusion when they met the following criteria: participants fulfilled the criteria of SBD as defined by DSM-5; participants with self-harm were only included, if the intent to die or an expectation of the lethality of an SA was identifiable in the study definition of self-harm. Thus, we excluded all studies with unclear definitions of suicidal behavior and studies assessing only suicidal ideations. Two independent reviewers (A.Z. and J.S.) searched the databases and screened the title, abstract, and full text of the studies to choose the relevant studies.
The search procedure described above was repeated for the systematic search for studies reporting on the relationship between the microbiome and suicidality. The keywords microbiome and suicide (Microbiome AND Suicid*) were entered into PubMed. Identical inclusion and exclusion criteria were applied to the screening process.
In addition to our search algorithm, reference lists of previous relevant systematic reviews and cross-references were examined to identify further eligible studies that may have remained undetected by the employed search algorithm.
3. Results
3.1. Toxoplasmosis and Suicidal Behavior
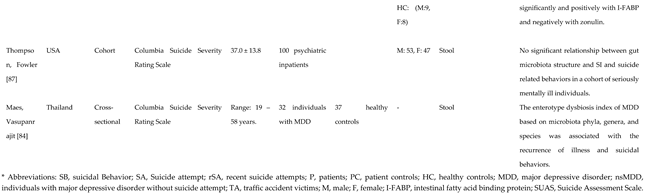
The systematic search in the databases yielded 1,774 studies, sixteen of them were included in the systematic review after removing the duplicates and assessed for eligibility (see Figure 1). The characteristics of these studies are displayed in Table 1.
Overall, twelve out of sixteen studies reported a statistically significant positive relationship between T. gondii and suicidal behavior [44,67,69,70,71,72,73,74,75,76,77,79], while four studies did not find any such association [68,78,80,81]. Thus, ten studies demonstrated an association between T. gondii seropositivity and suicidal behavior. However, one study additionally reported a significant association between suicide attempts and a positive blood alcohol test [79] which could be considered a confounding factor. Four studies investigated the relationship between serointensity and suicidal behavior. The results were contradictory: two out of the four studies reported positive associations with SA in term of higher odds ratios [72,74], while in the other two studies, the association was nonsignificant [68,69].
In three postmortem studies [68,77,79], anti-T. gondii IgG antibodies were measured in blood samples. These studies did not reveal an overall association between T. gondii seropositivity and suicide. However, when examining subgroups, statistically significant higher number of T. gondii seropositivity was observed in the 38-58 age group. The fourth postmortem study [67] investigated T. gondii immunohistochemistry in brain tissues from the prefrontal cortex and amygdala. This study reported a significant association between a history of depression and T. gondii infection in the brain of suicide victims.
3.2. Microbiome and Suicidal Behavior
Through the systematic search on PubMed, we identified 2098 papers. Ten further works were found by checking the cross-references. After screening and assessing for eligibility, six papers meeting the inclusion criteria were included in this review (Figure 2).
Table 2 presents the characteristics of the six eligible studies. Five out of six studies reported a significant association of suicidal behavior with the microbiome [82,83,84,85,86]. Only study investigating 100 psychiatric inpatients did not find any significant relationship between gut microbiota structure and suicide-related behaviors [87]. However, only 35 individuals out of the included 100 exhibited past suicidal behavior, which significantly dilutes the interpretation of the result. No separate analyses for the SB or SI groups were reported.
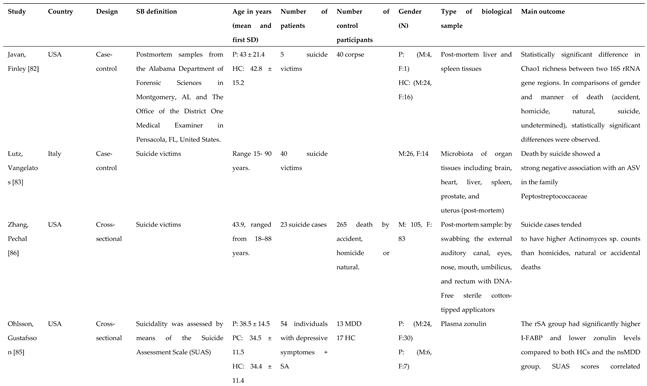
In all three postmortem studies, altered microbiome composition was found in suicide victims. SB was strongly associated with lower levels of Peptostreptococcaceae, [83] and higher level of Actinomyces [86], both gram-positive bacteria. Moreover, significant differences in Chao1 richness [82] in suicide victims were reported. A study examining stool samples revealed a significant relationship between the enterotype dysbiosis index and suicidal behavior in individuals with MDD [84]. Investigating plasma zonulin, a marker of gut permeability [88], it was found that the SB group had lower zonulin levels and additionally higher levels of intestinal-fatty acid binding protein (I-FABP) compared to depressed individuals without SB and unaffected controls [85].
4. Discussion
4.1. Toxoplasmosis
The goal of this systematic review was to comprehensively summarize existing knowledge regarding the association between T. gondii and suicidal behavior. We assumed that the parasite could influence the decision-making process in intermediate hosts, leading to risky behavior in T. gondii-infected individuals thereby increasing the likelihood of a suicidal act. To test our hypothesis, we screened 1,774 papers and incorporated 16 reports into the review. Most of the results support the assumption of a positive correlation between T. gondii and suicidal behavior. This means that individuals infected with T. gondii appear to be more prone to suicidal behavior, making the resulting infection an additional external factor contributing to the transition from suicidal ideation to action.
The underlying mechanism in humans appears to be altered decision-making in terms of lower risk aversion as a result of the infection. Relating to animals, the manipulation hypothesis says that the parasite's manipulative activity aims to shift the intermediate host's response from aversion to attraction, facilitating the chase and eating of the infected host and increasing the likelihood of transmission from an intermediate to a definitive host [89]. The mechanisms behind the conversion from aversion to attraction are complex and still a topic of discussion. Based on the results of neurobiological studies, the conversion could be explained by the effects of T. gondii on the function of certain brain regions.
Although parasite cysts are distributed throughout the entire brain of infected rodents, the amygdala appears to be particularly affected. The density of cysts found in the amygdala has been twice as high as in other regions of the brain [48], having a potential impact on fear processing or detection of other salient stimuli. This dysfunction of the amygdala could change risk-taking behavior through altered perception of the threat and thus of impending negative consequences. In addition, there is some, but still little, evidence of the effects of toxoplasmosis on the structure and function of the human brain.
In view of the available evidence for the neuronal effects of acute toxoplasmosis, further studies are urgently needed to determine the neuronal correlates of the changes in infected populations and their relationship to altered neurocognitive processes. To date, no study has examined the clinical profiles and cognitive aspects of decision-making in T. gondii infected individuals with SB, which may be a promising intervention target for future psychotherapeutic and pharmacological approaches. The latter therapies should be effective against both tachyzoites and bradyzoites that remain in the body for life.
Several limitations within the included studies could lead to challenges in the interpretation of our results. Although we included studies with clearly defined criteria for suicidal behavior disorder according to DSM-5, inconsistencies with regard to existing mental illnesses (e.g., schizophrenia, affective disorders), in the composition of the control groups (healthy controls vs. patient controls), study design (cross‒sectional, case‒control, cohort), and biological samples (brain tissue, plasma) may have contributed to the heterogeneity of the findings.
Additionally, two studies reported the association of T. gondii with SB in people with significant alcohol levels in their blood. Alcohol intoxication could serve as a trigger for the transition to suicidal behavior, as alcohol itself could influence decision-making, interfering with the effect of toxoplasmosis [90]. Another limitation refers to the lack of information on the socioeconomic status of the included individuals, which might also be a potential confounder. Furthermore, the prevalence of T. gondii is the highest in Africa [91]; however, studies included in this review exclusively have been published in high-income countries, and therefore, one should be careful about drawing general inferences regarding the developing and emerging countries.
Moreover, the inclusion of four postmortem studies, focusing on postmortem plasma or brain tissues in suicide victims, adds an additional layer of potential variation. In addition, reports indicate that the probability of suicide is significantly higher among individuals who use violent suicide means than among those using nonviolent methods [92,93]. Therefore, violent suicide attempters, using high lethality methods, might build a specific subgroup with very high-risk behavior, closer to suicide victims regarding psychopathological and neurocognitive features, such as decision-making [94,95,96]. However, the studies included in the present systematic review did not provide any information about the methods used for SB. The lack of this suicide-specific information in these studies may also contribute to some variability in the reported findings.
4.2. Microbiome
The present study is the first review summarizing the existing knowledge about the association between the microbiome and suicidal behavior. We hypothesized that there might be differences in microbiome in suicide attempters or suicide victims; therefore, through the systematic search, we identified six studies investigating this relationship. Five studies demonstrated an association between changes in the microbiome and suicidal behavior. Only Thompson, Fowler [87] reported no significant relationship between gut microbiota structure and “suicidality” in a cohort of mentally ill people. However, only 35% of the investigated individuals in that study showed actual suicidal behavior, and most individuals only expressed suicidal thoughts, which considerably limits the interpretation of the results.
In contrast, the second study, analyzing stool samples, reported an association between suicidal behaviors and the dysbiosis index in the depression enterotype [84]. All postmortem studies revealed an association or a trend between the microbiome in postmortem organ tissues and suicide. As the results are controversial, further investigation is needed to establish whether there is an association between suicidal behaviors and alterations in gut microbiota. To summarize, the number of identified studies is small, and the heterogeneity of the applied methods is relatively large, so a clear conclusion about the role of the microbiome in SB is currently not possible. Different biological samples, including brain or other organ tissues, plasma and stool samples, might also lead to differences in results. Further limitations, such as differences in the psychiatric disorders of the individuals and study design, must also be taken into consideration.
Experimental clinical studies investigating the role of the gut microbiome in suicidal behavior are lacking. Most of the current research focuses on depressed people who show signs of an altered microbiota composition [35,39]. A recent comprehensive population study demonstrated that Coprococcus and Dialister strains not only acted as predictors of an enhanced quality of life but were also consistently found to be reduced in untreated individuals with depression [97]. As discussed above, the gut microbiome has an impact on the HPA axis, which itself affects how individuals react to stress. Interestingly, recent studies demonstrated that fecal matter transplantation from non-stressed animals partially reduced certain harmful effects of stress [98]. Conversely, transplanting fecal matter from stressed to naïve mice was sufficient to induce stress-related effects in the recipient mice [98]. Moreover, transplanting fecal material from stressed mice to previously unaffected recipients led to anxiety-like behavior and to the accumulation of monocytes and activation of microglia in the hippocampus, while administering beneficial microbes from nonstressed animals improved anxiety-like behavior by alleviating inflammation in the gut [99]. These findings indicate the involvement of the gut microbiome in the stress response. Since it is assumed that an abnormal HPA axis and stress response [100] play a decisive role in the development of suicidal behavior, changes in the microbiome due to genetic/epigenetic mechanisms or due to reduced health-related behavior could be an additional factor that increases susceptibility to suicidal behavior.
In addition, the gut microbiome has a crucial role in neuroendocrinological functions and brain development. Microbial metabolites such as short-chain fatty acids (SCFAs) regulate intestinal immune function and have anti-inflammatory properties, particularly in inhibiting proinflammatory mediators in macrophages and influencing the maturation and function of microglia [101,102]. Emerging evidence suggests that the gut microbiota can influence intestinal barrier permeability and ultimately leads to the dysregulation of inflammatory responses [103]. There are some indications of a possible link between inflammation in both the peripheral and central nervous systems and suicidal behavior [104]. Therefore, we propose to systematically investigate the likely mediating role of the microbiome in inflammatory and stress-related processes associated with suicidal behavior as a focus for future research.
5. Conclusions
In this systematic review, we have demonstrated the association between T. gondii and suicidal behavior and discussed the probable underlying mechanisms. However, in order to better understand the mechanism of toxoplasmosis, further and specific studies on the influence of the parasite on risky decision-making in vulnerable individuals need to be performed. Furthermore, this is the first review summarizing existing literature on the likely link between changes in microbiome and suicidal behavior. There is some evidence that the microbiome is an additional internal factor that may increase vulnerability to suicidal behavior. However, future systematic and sufficiently powered studies should additionally investigate the mediating role of the microbiome in inflammatory and stress-related processes associated with suicidal behavior.
Author Contributions
A.Z.: systematic search; screening the records; figures and tables; writing. J.S.: screening the records, approval of the final article. A.R, M.L. and T.S.: manuscript reviewing/editing, approval of the final article. M.W.: administrative support; supervision, obtained funding, reviewing/editing, approval of the final article. G.W.: concept and design; supervision; critical revision and editing of the manuscript; administrative, technical, or material support; supervision. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung [BMBF]) and the ministry of Thüringen within the initial phase of the German Center for Mental Health (DZPG) (grant: 01EE2305F).
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data was created.
Acknowledgments
Supported by German Center for Mental Health (DZPG).
Conflicts of Interest
M.W. received institutional support for research or advisory activities by the following companies: HEEL, Janssen, Boehringer, LivaNova, Novartis, Perception Neuroscience, Ketabon, HMNC. T.S. received institutional support for consulting and lecture activities by the following companies: Janssen, ROVI.
References
- WHO, Mental health: Suicide data. 2020, WHO.
- WHO, World health statistics 2023: Monitoring health for the SDGs, Sustainable Development Goals. 2023: Geneva.
- Economic, U.N.D.o. , World Population Prospects: The 1998 Revision. Vol. 180. 1999: UN.
- Astraud, L.P.; JA Bridge, and F. Jollant. Thirty Years of Publications in Suicidology: A Bibliometric Analysis. Arch Suicide Res. 2021, 25, 751–764. [Google Scholar] [PubMed]
- Klonsky, E.D.; AM May, and B.Y. Saffer. Suicide, Suicide Attempts, and Suicidal Ideation. Annual Review of Clinical Psychology. 2016, 12, 307–330. [Google Scholar] [PubMed]
- Franklin, J.C.; et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol Bull 2017, 143, 187–232. [Google Scholar] [CrossRef] [PubMed]
- CDC, Definitions: Self-directed violence. Injury prevention and control: Division of violence, 2015a.
- Crosby, A. ; L Ortega, and C. Melanson, Self-directed violence surveillance; uniform definitions and recommended data elements. 2011.
- Oquendo, M.A.; et al. Toward a biosignature for suicide. Am J Psychiatry 2014, 171, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Baldini, V.; et al. Association between adverse childhood experiences and suicidal behavior in schizophrenia spectrum disorders: A systematic review and meta-analysis. Psychiatry Res 2023, 329, 115488. [Google Scholar] [CrossRef] [PubMed]
- Calati, R.; et al. BOrderliNe symptoms and suIcide-related outcomes: proTOcol for a systematic review/meta-analysis and an individual patient data meta-analysis (BONITO study). BMJ Open 2022, 12, e056492. [Google Scholar] [CrossRef]
- Miller, J.N. ; DW Black, Bipolar Disorder and Suicide: A Review. Curr Psychiatry Rep 2020, 22, 6. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.E.; et al. Suicidal behavior across a broad range of psychiatric disorders. Mol Psychiatry 2023, 28, 2764–2810. [Google Scholar] [CrossRef] [PubMed]
- Yuodelis-Flores, C. ; RK Ries, Addiction and suicide: A review. Am J Addict 2015, 24, 98–104. [Google Scholar] [CrossRef]
- Carter, G. ; MJ Spittal, Suicide risk assessment. 2018, Hogrefe Publishing.
- Hawton, K. and K. van Heeringen. Suicide. Lancet. 2009, 373, 1372–1381. [Google Scholar]
- Mann, J.J. ; MM Rizk, A Brain-Centric Model of Suicidal Behavior. Am J Psychiatry 2020, 177, 902–916. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.R.; et al. GWAS Meta-Analysis of Suicide Attempt: Identification of 12 Genome-Wide Significant Loci and Implication of Genetic Risks for Specific Health Factors. Am J Psychiatry 2023, 180, 723–738. [Google Scholar] [CrossRef] [PubMed]
- Punzi, G.; et al. Genetics and brain transcriptomics of completed suicide. American journal of psychiatry 2022, 179, 226–241. [Google Scholar] [CrossRef]
- Wagner, G.; et al. Prefrontal cortical thickness in depressed patients with high-risk for suicidal behavior. J Psychiatr Res 2012, 46, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; et al. Connectomics-Based Functional Network Alterations in both Depressed Patients with Suicidal Behavior and Healthy Relatives of Suicide Victims. Sci Rep 2019, 9, 14330. [Google Scholar] [CrossRef] [PubMed]
- Olie, E.; et al. The experience of social exclusion in women with a history of suicidal acts: A neuroimaging study. Sci Rep 2017, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; et al. Cognitive and emotional impairments underpinning suicidal activity in patients with mood disorders: An fMRI study. Acta Psychiatr Scand 2019, 139, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Verrocchio, M.C.; et al. Mental Pain and Suicide: A Systematic Review of the Literature. Front Psychiatry 2016, 7, 108. [Google Scholar] [CrossRef]
- Dombrovski, A.Y. ; MN Hallquist, The decision neuroscience perspective on suicidal behavior: Evidence and hypotheses. Curr Opin Psychiatry 2017, 30, 7–14. [Google Scholar] [CrossRef]
- Richard-Devantoy, S.; et al. Decision-making in unipolar or bipolar suicide attempters. J Affect Disord 2016, 190, 128–136. [Google Scholar] [CrossRef]
- Sastre-Buades, A.; et al. Decision-making in suicidal behavior: A systematic review and meta-analysis. Neurosci Biobehav Rev 2021, 131, 642–662. [Google Scholar] [CrossRef]
- Lubbert, M.; et al. Investigating the Clinical Profile of Suicide Attempters Who Used a Violent Suicidal Means. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Perrain, R. ; R Dardennes, and F. Jollant, Risky decision-making in suicide attempters, and the choice of a violent suicidal means: An updated meta-analysis. J Affect Disord. 2021, (280 Pt A), 241–249. [Google Scholar]
- Dominguez-Baleon, C.; et al. Neuroimaging Studies of Suicidal Behavior and Non-suicidal Self-Injury in Psychiatric Patients: A Systematic Review. Front Psychiatry 2018, 9, 500. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.N.; et al. Suicide Biomarkers to Predict Risk, Classify Diagnostic Subtypes, and Identify Novel Therapeutic Targets: 5 Years of Promising Research. Int J Neuropsychopharmacol 2022, 25, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Courtet, P.; et al. Neuroinflammation in suicide: Toward a comprehensive model. World J Biol Psychiatry 2016, 17, 564–586. [Google Scholar] [CrossRef] [PubMed]
- Brisch, R.; et al. The role of microglia in neuropsychiatric disorders and suicide. Eur Arch Psychiatry Clin Neurosci 2022, 272, 929–945. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; et al. Increased C-reactive protein concentrations were associated with suicidal behavior in patients with depressive disorders: A meta-analysis. Psychiatry research 2020, 292, 113320. [Google Scholar] [CrossRef] [PubMed]
- Refisch, A. ; M Walter, [The importance of the human microbiome for mental health]. Nervenarzt 2023, 94, 1001–1009. [Google Scholar] [CrossRef]
- Zheng, D.; T Liwinski, and E. Elinav. Interaction between microbiota and immunity in health and disease. Cell Res. 2020, 30, 492–506. [Google Scholar]
- Maitre, Y. Did the Brain and Oral Microbiota Talk to Each Other? A Review of the Literature. J Clin Med 2020, 9(12).
- Ahn, J. ; RB Hayes, Environmental influences on the human microbiome and implications for noncommunicable disease. Annual review of public health 2021, 42, 277–292. [Google Scholar] [CrossRef]
- Cruz-Pereira, J.S.; et al. Depression's Unholy Trinity: Dysregulated Stress, Immunity, and the Microbiome. Annu Rev Psychol 2020, 71, 49–78. [Google Scholar] [CrossRef]
- Halonen, S.K. ; LM Weiss, Toxoplasmosis. Handb Clin Neurol 2013, 114, 125–45. [Google Scholar]
- Stanić; Ž; R Fureš, Toxoplasmosis: A global zoonosis. Veterinaria 2020, 69(1).
- Guimarães, E.V.; Ld Carvalho, H.S. Barbosa, Interaction and cystogenesis of Toxoplasma gondii within skeletal muscle cells in vitro. Memórias do Instituto Oswaldo Cruz 2009, 104, 170-174.
- Robert-Gangneux, F. ; M-L Dardé, Epidemiology of and diagnostic strategies for toxoplasmosis. Clinical microbiology reviews 2012, 25, 264–296. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.M.; et al. Latent Toxoplasmosis is Associated with Depression and Suicidal Behavior. Arch Suicide Res 2022, 26, 819–830. [Google Scholar] [CrossRef]
- Dasa, T.T.; et al. Toxoplasmosis infection among pregnant women in Africa: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0254209. [Google Scholar] [CrossRef] [PubMed]
- McConkey, G.A.; et al. Toxoplasma gondii infection and behaviour–location, location, location? Journal of Experimental Biology 2013, 216, 113–119. [Google Scholar] [CrossRef]
- Berdoy, M. ; JP Webster, and D.W. Macdonald, Fatal attraction in rats infected with Toxoplasma gondii. Proceedings of the Royal Society of London. Series B: Biological Sciences. 2000, 267, 1591–1594. [Google Scholar] [PubMed]
- Vyas, A.; et al. Behavioral changes induced by Toxoplasma infection of rodents are highly specific to aversion of cat odors. Proc Natl Acad Sci USA 2007, 104, 6442–6447. [Google Scholar] [CrossRef]
- Meyer, C.J.; et al. Parasitic infection increases risk-taking in a social, intermediate host carnivore. Commun Biol 2022, 5, 1180. [Google Scholar] [CrossRef]
- Poirotte, C.; et al. Morbid attraction to leopard urine in Toxoplasma-infected chimpanzees. Current Biology 2016, 26, R98–R99. [Google Scholar] [CrossRef] [PubMed]
- Gohardehi, S.; et al. The potential risk of toxoplasmosis for traffic accidents: A systematic review and meta-analysis. Experimental parasitology 2018, 191, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Samojłowicz, D. Presence of Toxoplasma gondii infection in brain as a potential cause of risky behavior: A report of 102 autopsy cases. European Journal of Clinical Microbiology & Infectious Diseases. 2019, 38, 305–317. [Google Scholar] [PubMed]
- Soleymani, E. Association of T. gondii infection with suicide: A systematic review and meta-analysis. BMC Public Health. 2020, 20, 766. [Google Scholar] [PubMed]
- Sutterland, A.L.; et al. Driving us mad: The association of Toxoplasma gondii with suicide attempts and traffic accidents - a systematic review and meta-analysis. Psychol Med 2019, 49, 1608–1623. [Google Scholar] [CrossRef] [PubMed]
- De Vadder, F.; et al. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell 2014, 156, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Sudo, N. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J Physiol. 2004, 558 (Pt 1), 263–275. [Google Scholar]
- Refisch, A.; et al. Microbiome and immuno-metabolic dysregulation in patients with major depressive disorder with atypical clinical presentation. Neuropharmacology 2023, 235, 109568. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.A.; et al. The gut microbiota in anxiety and depression - A systematic review. Clin Psychol Rev 2021, 83, 101943. [Google Scholar] [CrossRef]
- Liu, L.; et al. Toward a Deeper Understanding of Gut Microbiome in Depression: The Promise of Clinical Applicability. Adv Sci (Weinh) 2022, 9, e2203707. [Google Scholar] [CrossRef]
- Radjabzadeh, D.; et al. Gut microbiome-wide association study of depressive symptoms. Nat Commun 2022, 13, 7128. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; et al. The Microbiota-Gut-Brain Axis. Physiol Rev 2019, 99, 1877–2013. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; et al. Landscapes of bacterial and metabolic signatures and their interaction in major depressive disorders. Science advances 2020, 6, eaba8555. [Google Scholar] [CrossRef]
- Le Port, A.; et al. Association between dietary patterns and depressive symptoms over time: A 10-year follow-up study of the GAZEL cohort. PLoS ONE 2012, 7, e51593. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; et al. Fast food consumption and suicide attempts among adolescents aged 12–15 years from 32 countries. Journal of affective disorders 2020, 266, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.Y. ; YH Yun, Health-promoting behavior to enhance perceived meaning and control of life in chronic disease patients with role limitations and depressive symptoms: A network approach. Sci Rep 2023, 13, 4848. [Google Scholar] [CrossRef]
- Moher, D. RESEARCH METHODS & REPORTING-Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement-David Moher and colleagues introduce PRISMA, an update of the QUOROM guidelines for reporting systematic reviews and meta-analyses. Bmj (Cr)-Print. 2009, 338, 332. [Google Scholar]
- Alvarado-Esquivel, C.; et al. Association between Toxoplasma gondii Infection in Brain and a History of Depression in Suicide Decedents: A Cross-Sectional Study. Pathogens 2021, 10(10).
- Mendoza-Larios, L.A.; et al. Association between Suicide and Toxoplasma gondii Seropositivity. Pathogens 2021, 10(9).
- Bak, J.; et al. The Association between Suicide Attempts and Toxoplasma gondii Infection. Clin Psychopharmacol Neurosci 2018, 16, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Coryell, W.; et al. Toxoplasmosis Titers and past Suicide Attempts Among Older Adolescents Initiating SSRI Treatment. Arch Suicide Res 2016, 20, 605–613. [Google Scholar] [CrossRef]
- Ling, V.J.; et al. Toxoplasma gondii seropositivity and suicide rates in women. J Nerv Ment Dis 2011, 199, 440–444. [Google Scholar] [CrossRef]
- Zhang, Y.; et al. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self-directed violence. J Clin Psychiatry 2012, 73, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Akgul, O.; et al. Toxoplasma gondii infection by serological and molecular methods in schizophrenia patients with and without suicide attempts: An age-sex-matched case-control study. Int J Clin Pract 2021, 75, e14449. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; et al. Suicide attempts and markers of immune response in individuals with serious mental illness. J Psychiatr Res 2017, 87, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Arling, T.A.; et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with recurrent mood disorders. J Nerv Ment Dis 2009, 197, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Sugden, K.; et al. Is Toxoplasma Gondii Infection Related to Brain and Behavior Impairments in Humans? Evidence from a Population-Representative Birth Cohort. PLoS ONE 2016, 11, e0148435. [Google Scholar]
- Samojlowicz, D. ; A Borowska-Solonynko, and E. Golab, Prevalence of Toxoplasma gondii parasite infection among people who died due to sudden death in the capital city of Warsaw and its vicinity. Przegl Epidemiol. 2013, 67, 115–118. [Google Scholar]
- Coccaro, E.F.; et al. Toxoplasma gondii infection: Relationship with aggression in psychiatric subjects. J Clin Psychiatry 2016, 77, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Samojlowicz, D. ; A Borowska-Solonynko, and M. Kruczyk, New, previously unreported correlations between latent Toxoplasma gondii infection and excessive ethanol consumption. Forensic Sci Int. 2017, 280, 49–54. [Google Scholar] [PubMed]
- Fond, G.; et al. Latent toxoplasma infection in real-world schizophrenia: Results from the national FACE-SZ cohort. Schizophr Res 2018, 201, 373–380. [Google Scholar] [CrossRef]
- Burgdorf, K.S.; et al. Large-scale study of Toxoplasma and Cytomegalovirus shows an association between infection and serious psychiatric disorders. Brain Behav Immun 2019, 79, 152–158. [Google Scholar] [CrossRef]
- Javan, G.T.; et al. Cadaver Thanatomicrobiome Signatures: The Ubiquitous Nature of Clostridium Species in Human Decomposition. Front Microbiol 2017, 8, 2096. [Google Scholar] [CrossRef] [PubMed]
- Lutz, H.; et al. Effects of Extended Postmortem Interval on Microbial Communities in Organs of the Human Cadaver. Front Microbiol 2020, 11, 569630. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; et al. Adverse childhood experiences and reoccurrence of illness impact the gut microbiome, which affects suicidal behaviours and the phenome of major depression: Towards enterotypic phenotypes. Acta Neuropsychiatr, 2023, 1-18.
- Ohlsson, L.; et al. Leaky gut biomarkers in depression and suicidal behavior. Acta Psychiatr Scand 2019, 139, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; et al. Machine learning performance in a microbial molecular autopsy context: A cross-sectional postmortem human population study. PLoS ONE 2019, 14, e0213829. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.S.; et al. Is the gut microbiota associated with suicidality? Non-significant finding among a large cohort of psychiatrically hospitalized individuals with serious mental illness. J Affect Disord Rep 2021, 6, 10.1016.
- Fasano, A. , Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol Rev 2011, 91, 151–175. [Google Scholar] [CrossRef] [PubMed]
- Flegr, J. , How and why Toxoplasma makes us crazy. Trends Parasitol 2013, 29, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Petzold, J.; et al. Value-based decision-making predicts alcohol use and related problems in young men. J Psychopharmacol, 2023, 2698811231212151.
- Bigna, J.J.; et al. Global, regional, and country seroprevalence of Toxoplasma gondii in pregnant women: A systematic review, modelling and meta-analysis. Scientific Reports 2020, 10, 12102. [Google Scholar] [CrossRef]
- Mergl, R.; et al. What Are Reasons for the Large Gender Differences in the Lethality of Suicidal Acts? An Epidemiological Analysis in Four European Countries. PLoS ONE 2015, 10, e0129062. [Google Scholar]
- Bergen, H.; et al. Shared characteristics of suicides and other unnatural deaths following non-fatal self-harm? A multicentre study of risk factors. Psychol Med 2012, 42, 727–741. [Google Scholar]
- Wyart, M.; et al. Iowa Gambling Task Performance in Elderly Persons with a Lifetime History of Suicidal Acts. Am J Geriatr Psychiatry 2016, 24, 399–406. [Google Scholar] [CrossRef]
- Jollant, F.; et al. Impaired decision making in suicide attempters. Am J Psychiatry 2005, 162, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Gorlyn, M.; et al. Iowa gambling task performance in currently depressed suicide attempters. Psychiatry Res 2013, 207, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Valles-Colomer, M.; et al. The neuroactive potential of the human gut microbiota in quality of life and depression. Nature microbiology 2019, 4, 623–632. [Google Scholar] [CrossRef]
- Langgartner, D.; et al. The role of the intestinal microbiome in chronic psychosocial stress-induced pathologies in male mice. Frontiers in behavioral neuroscience 2018, 12, 252. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.-M.; et al. Immobilization stress-induced Escherichia coli causes anxiety by inducing NF-κB activation through gut microbiota disturbance. Scientific Reports 2018, 8, 13897. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; et al. Suicide and suicide risk. Nat Rev Dis Primers 2019, 5, 74. [Google Scholar] [CrossRef] [PubMed]
- Kreutzmann, J.; et al. Sleep deprivation and hippocampal vulnerability: Changes in neuronal plasticity, neurogenesis and cognitive function. Neuroscience 2015, 309, 173–190. [Google Scholar] [CrossRef] [PubMed]
- Vinolo, M.A.; et al. Regulation of inflammation by short chain fatty acids. Nutrients 2011, 3, 858–876. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; et al. Gut microbiota modulates the inflammatory response and cognitive impairment induced by sleep deprivation. Mol Psychiatry 2021, 26, 6277–6292. [Google Scholar] [CrossRef]
- Donegan, J.J. ; CB Nemeroff, Suicide and Inflammation. Adv Exp Med Biol 2023, 1411, 379–404. [Google Scholar]
Figure 1.
Flowchart of the selection process of the studies reporting an association between Toxoplasma gondii and suicidal behavior.
Figure 1.
Flowchart of the selection process of the studies reporting an association between Toxoplasma gondii and suicidal behavior.
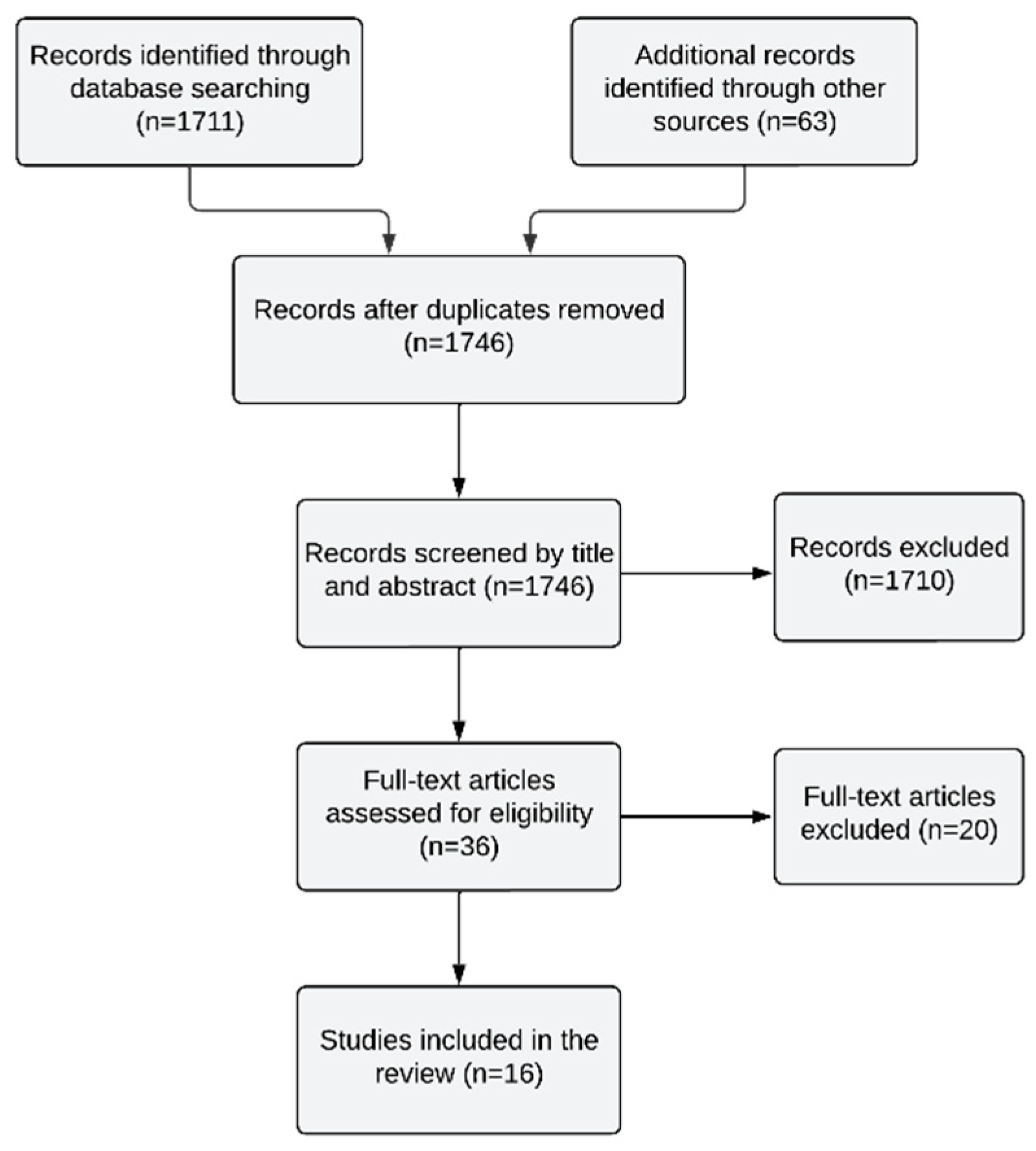
Figure 2.
Flowchart of the selection process of the studies reporting an association between microbiome and suicidal behavior.
Figure 2.
Flowchart of the selection process of the studies reporting an association between microbiome and suicidal behavior.
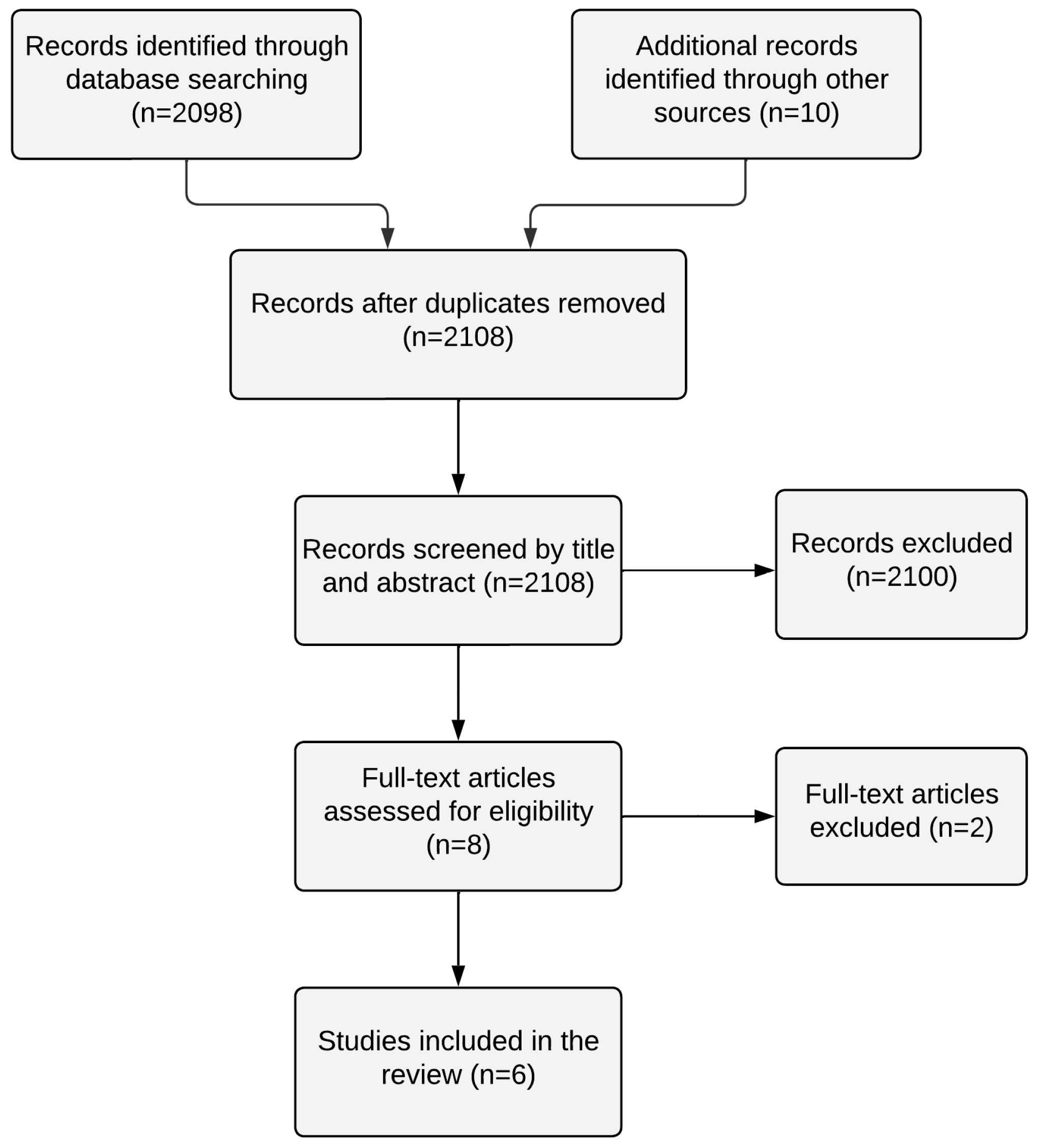

Table 1.
Individual studies used in this review reporting the association between T. gondii and suicidal Behavior.
Table 1.
Individual studies used in this review reporting the association between T. gondii and suicidal Behavior.
| Study | Country | Design | SB definition | Age in years (mean and first SD) | Number of patients | Number of control participants | Gender (N) | Type of biological sample | Main outcome |
|---|---|---|---|---|---|---|---|---|---|
| Alvarado-Esquivel, Mendoza-Larios [67] | Mexico | Cross-sectional | Decedents who died by suicide received for medico-legal routine autopsies | 34.8 ± 17.4 | 87 suicide victims | - | P: (M:67, F: 20) | Post-mortem brain(prefrontal cortex and amygdala) | A history of depression was associated with T. gondii infection of the brain in suicide victims |
| Mendoza-Larios, Garcia-Dolores [68] | Mexico | Case–control | Decedents, who died by suicide | P: 35.21 ± 17.48HC: 31.82 ± 15.01 | 89 decedents who committed suicide | 58 decedents | P: (M:68, F:21)HC: (M:48, F:10) | Post-mortem plasma | No association between T. gondii seropositivity and suicide |
| Bak, Shim [69] | South Korea | Case-control | SA according to Columbia Suicide Severity Rating Scale. | P: 43.75±16.75HC: 41.59±11.54 | 155 inpatients and outpatients with depressive symptoms + SA | 135 healthy controls | P: (M:75, F:80)HC: (M:66, F:69) | Plasma | Suicide attempters showed higher seroprevalence of T. gondii than healthy controls. |
| Coryell, Yolken [70] | USA | Case-control | SA was defined as any self-harm that was intended to cause death regardless of premeditation or potential lethality. | P: 17.5±1.7PC: 19.0±1.6 | 17 individuals with MDD + SA | 91 individuals with MDD | P: (M:4, F:13)PC: (M:26, F:65) | Plasma | A significantly higher toxoplasmosis IgG titer among individuals who had recently begun a trial of SSRIs and had a history of suicide attempts. |
| Ling, Lester [71] | WHO,Europe | Ecological Study | Suicide rates by age group were obtained from the European Mortality Database | Range 0–75+ | 432,974 individuals | Only females | Plasma | Positive relationship between rates of infection with T. gondii and suicide is apparent in women of postmenopausal age. | |
| Zhang, Traskman-Bendz [72] | Sweden | Cross-sectional | Situations in which a person has performed an actually or seemingly life-threatening behavior with the intent of jeopardizing his/her life or to give the appearance of such intent, but which has not resulted in death. | P: 38.4 ± 14.4HC: 39.8 ± 14.2 | 54 individuals with mixed diagnosis + SA | 30 HC | P: (M:23, F:31)HC: (M:11, F:19) | Plasma | Seropositivity of T gondii and serointensity of T gondii were positively associated with a history of SA. |
| Akgul, Demirel [73] | Turkey | Case-control | SA according to Suicide Behaviors Questionnaire-Revised and clinical interviews. | P: 47.51 ± 24.83PC: 43.96 ± 18.33HC: 42.27 ± 29.11 | 57 individuals with schizophrenia + SA | 60 individuals with Schizophrenia 120 HC | P: (M:34, F:23)PC: (M:32, F:28)HC: (M:53, F:67) | Plasma | The relationship between the history of SA and seroprevalence T gondii was found to be statistically significant (P < .05). The history of SA was not statistically associated (P= .831) with T gondii positivity by PCR. |
| Kamal, Kamal [44] | Egypt | cross-sectional case-control | Columbia Suicide Severity Rating Scale (C-SSRS) | P: 32.39 ± 10.47HC: 33.10 ± 11.03 | 384 depressed individuals | 400 HC | P: (M:209, F:175)HC: (M:214,F:186) | Serum | Seropositive depressed participants were more likely to have prior history of SA compared with seronegative participants. |
| Dickerson, Wilcox [74] | USA | Cross-sectional | A suicide attempt was defined as a potentially self-injurious act committed with at least some wish to die as a result of the act | P: 38.6 ± 13.0PC: 36.5 ± 13.8 | 72 individuals with psychiatric diagnosis + SA | 90 patient controls | P: (M:38, F:34)PC: (M:50, F:40) | Plasma | Strong odds of a suicide attempt history in individuals who had elevated levels of IgM antibodies to T. gondii; A significant correlation between a lifetime history of suicide attempts and the level of IgM class antibodies. |
| Arling, Yolken [75] | USA | Case-Control | The Columbia Suicide History Form, a semi-structured questionnaire, was used to gather suicide attempt history | P: 40.3 ± 9.8PC: 43.4 ± 10.9HC: 42.7 ± 11.0 | 99 individuals with MDD + SA | 119 individuals with mood disorders39 HC | P: (M:39, F:60)PC: (M:43, F:76)HC: (M:13, F:26) | Plasma | A predictive association between titers of anti- T. gondii antibodies and history of suicide attempt |
| Sugden, Moffitt [76] | USA | Prospective cohort study | Self-reported suicide attempts: Behaviors counted as attempted suicide only if accompanied by self-reported intent to die. | Range 3–38 | 67 individuals with SA | 770 individuals without SA | M:423, F:414 | Plasma | Suicide attempt was marginally more frequent among individuals with T. gondii seropositivity (p = .06). |
| Samojlowicz, Borowska-Solonynko [77] | Poland | Case-Control | People who died as a result of suicide. | P: median=40PC: median=40HC: median=51 | 41 suicide victims | 42 traffic accident victims 86 HC | P: (M:36, F:5)TA: (M:39, F:3)HC: (M:79, F:7) | Post-mortem Plasma | With respect to the prevalence of T. gondii infection no statistically significant differences were found between the study and control group. A statistically significant result was recorded in the 38-58 age group between suicide and control groups. |
| Coccaro, Lee [78] | USA | Cross-sectional | An act was considered a suicide attempt if it involved behavior with the conclusion intent do die by means that the subject believed could end his or her life. | P: 36.1 ± 8.3PC: 33.7 ± 8.1HC: 31.3 ±8.7 | 110 individuals with intermittent explosive disorder | 110 HC138 psychiatric controls | P: (M:70, F:40)PC: (M:81, F:57)HC: (M:64, F:46) | Plasma | T. gondii seropositive status did not predict history of suicide attempt |
| Samojlowicz, Borowska-Solonynko [79] | Poland | Case-control | Individuals who committed suicide | RB: median=40IRB: median=50HC: median=56 | 126 indviduals with high-risk behavior, who committed suicide | 165 HC96 individuals with inconclusively high-risk behavior; 51 individuals with Risky behavior | RB: (M:251, F:26)IRB: (M:86, F:10)HC: (M:140, F:25) | Post-mortem plasma | A strong correlation between latent T. gondii infection and engaging in high-risk behaviors leading to death. A strong positive association between T. gondii seropositivity and suicide under the influence of alcohol. |
| Fond, Boyer [80] | France | Cohort | Columbia-suicide severity Rating Scale | 32.0 ± 8.6 | 250 individuals with schizophrenia | P: (M:184, F:66) | Plasma | No significant association of latent Toxoplasma infection with suicide behavior has been found in the models. | |
| Burgdorf, Trabjerg [81] | Denmark | Case-Control | First episode of deliberate self-violence and suicide were defined by inclusion in the Danish National Patient Register, the Psychiatric Central Research Register or the Danish Register of Causes of Death | 37.4 (no SD reported) | 655 individuals with SA or suicide | 2591 psychiatric controls2724 traffic accident victims | P: (M:278, F:377)PC: (M:1277,F:1324)HC: (M:1491,F:1233) | Plasma | T. gondii infection was not statistically significantly associated with attempting or committing suicide (OR, 1·13). |
* Abbreviations: SB, suicidal Behavior; SA, Suicide attempt; P, patients; PC, patient controls; HC, healthy controls; MDD, major depressive disorder; TA, traffic accident victims; RB, risky behavior; IRB, inconclusively risky behavior, M, male; F, female.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



