Submitted:
18 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
As an essential component of our innate immune system, the complement system is responsible for our defense against pathogens. The complement cascade has complex roles in the central nervous system (CNS), most of what we know about it stems from its role in brain development. However, in recent years, numerous reports have implicated the classical complement cascade in both brain development and decline. More specifically, complement dysfunction has been implicated in neurodegenerative disorders, such as Alzheimer’s disease (AD), which is the most common form of dementia. Synapse loss is one of the main pathological hallmarks of AD and correlates with memory impairment. Throughout the course of AD progression, synapses are tagged with complement proteins and are consequently removed by microglia which express complement receptors. Notably, astrocytes are also capable of secreting signals that induce the expression of complement proteins in the CNS. Both astrocytes and microglia are implicated in neuroinflammation, another hallmark of AD pathogenesis. In this review, we provide an overview of previously known and newly established roles for the complement cascade in the CNS and we explore how complement interactions with microglia, astrocytes, and other risk factors such as TREM2 and ApoE4, modulate the processes of neurodegeneration in both amyloid and tau models of AD.
Keywords:
complement system
; neurodegeneration
; Alzheimer’s disease
; neuroinflammation
; aging
; brain development
1. Introduction
Alzheimer’s disease (AD) is the most common form of dementia in the world and is characterized by a progressive loss of memory and other cognitive functions such as thinking and reasoning [1,2,3]. Currently, more than 55 million people worldwide are living with AD or a related dementia, and this number is estimated to double every 20 years [2,4]. A better understanding of the disease mechanism and development of efficient therapeutics are needed – both to combat the rising cost of healthcare associated with managing the disease and to address the trend towards a growing worldwide aging population which poses a risk factor for AD.
AD is characterized by two molecular pathological hallmarks: extracellular amyloid-β (Aβ) plaques and intracellular neurofibrillary tangles (NFTs) [1]. The aggregation of Aβ plaques and NFTs is associated with significant neurodegeneration and synaptic loss as well as neuroinflammation [1]. Notably, synaptic loss is the best correlate for clinical dementia and more specifically for memory impairment in AD [5,6].
The literature in the AD field has historically described observations of altered neuroimmune function using vague terms such as neuroinflammation or glial “activation”, whereas several studies have now confirmed that alterations in immune cell phenotypes, gene expression and morphology are complex processes with wide-ranging implications in human disease [7,8,9]. Interestingly, genome-wide association studies (GWAS) implicate glial cells in several neurodegenerative disorders, including AD [10,11,12]. The “traditional” concept of neuroinflammation has been modified in recent years, as a remarkable cellular heterogeneity is being noticed through the molecular profiling of the central nervous system (CNS) cell population and single-cell analysis [7,8,11,13].
The complement system is a central component of innate immunity that serves as a first line of defense against pathogens, eliminating them and removing both apoptotic cells and debris [14,15]. In the brain, the complement system serves a crucial role during brain development [16]. Within this context, separate proteins and pathways of complement have been described as key players in the formation, development, migration, and refinement of neurons [17,18,19]. In addition, there is a growing body of work, in both animal models and humans, suggesting that aberrant complement regulation may underlie several neurodegenerative diseases [20,21,22,23,24,25,26]. In this review, we provide an overview of the data supporting the link between the complement system and the pathogenesis of AD and discuss new findings in this field.
2. Neuroinflammation and AD
Neuroinflammation has been described as a prominent feature in AD [27]. Since the 1980s, there have been reports of immune-related proteins and cells (microgliosis and astrogliosis) located close to and surrounding amyloid plaques [28,29,30,31,32,33,34,35]. Some evidence indicates that excessive brain inflammation is implicated in the pathogenesis of a number of neurological disorders [36], including AD, where increased levels of inflammatory mediators such as cytokines and chemokines are elevated in patients with the disorder [37,38]. In addition to inflammatory changes, progressive neuronal loss is observed ultimately resulting in cognitive impairment [39].
Microglia and astrocytes have emerged as central players in both brain health and disease. Microglia are mononuclear phagocytes from the myeloid cell lineage and serve as the resident macrophages of the brain [40]. They originate from the yolk sac and migrate into the CNS during early embryonic development [41]. However, microglia are not evenly distributed throughout all brain regions [42]. In the normal physiological state, microglia exhibit a branched morphology with processes that lengthen and recede, allowing them to actively survey their immediate environment [43]. They also possess phagocytic capability and secrete several compounds, including trophic factors, cytokines, chemokines, nitric oxide and reactive oxygen species which are responsible for immune defense and tissue maintenance [44]. In recent years, several seminal studies have recognized microglia as being pivotal during development, aging and neurological diseases [7,8,16,17,18,20,22,23,24,45,46,47]. Remarkably, microglia can lose their homeostatic molecular signature and function during AD, and thus become inflammatory and contribute to neurodegeneration [47,48]. Moreover, genetic studies have indicated that most of the risk alleles for AD are preferentially or selectively expressed by microglia in the brain [49,50].
During development, microglia are heavily involved in a process known as synaptic pruning, in which they refine immature neuronal circuits by selectively enveloping and eradicating synaptic structures [16,17,18,51]. Studies have shown that the interruption of microglial-mediated synaptic pruning leads to defects in synaptic development and wiring [52,53,54]. Strong evidence from several studies also suggest that microglia are regulators of synaptic plasticity [55], a fundamental cellular mechanism important for learning and memory [56]. Conversely, in the AD brain, microglial function can be modified, for example by inflammasome signaling, in turn promoting neurotoxicity through the release of excessive inflammatory cytokines and contributing to excessive synapse loss by way of microglial-mediated synaptic elimination [22,48,57].
Astrocytes constitute one of the largest glial cell populations in the CNS and play several roles which are vital for optimal brain function including maintenance of ionic and osmotic concentration gradients, the control of neurotransmitter release as well as uptake and production of trophic factors which promote neuronal survival [58]. Furthermore, they secrete pro-inflammatory and/or anti-inflammatory cytokines in response to specific stimuli, and they are recognized as key modulators of neuroinflammation in the CNS [58,59,60]. Additionally, it has been shown that astrocytes play a pivotal role in synapse formation and function [61]. Thus, it is reasonable to infer that deficits in this cell type negatively impact brain health and trigger neurotoxicity in neurodegenerative diseases as shown by Liddelow et al [59]. In particular, previous studies have established that astrocytes play a central role in the pathogenesis of AD [58,59]. Recently it was suggested that astrocytic reactivity may act as an upstream link between Aβ and tau pathology in early AD [62].
Along with microglia, astrocytes are also recognized as central regulators of the complement system in AD and, therefore, they can be expected to contribute to brain dysfunction via complement-mediated pathways [45,63]. The elevated expression and activation of various complement proteins have been observed in postmortem human AD tissue as well as several AD-like mouse models [22,64,65,66,67,68,69]. Furthermore, seminal studies have demonstrated that complement system signaling can contribute to AD pathogenesis [22,23]. Next, we will provide a simplified overview of the complement system and how it mediates certain pathological aspects of AD in addition to the relevant contributions from microglia and astrocytes to neuropathogenesis and neurodegeneration.
3. Complement system
As elucidated by Nonaka et al. [70], the complement cascade is an evolutionarily conserved system dating back more than a billion years. In 1895, complement was described as a heat-labile, a bactericidal component in serum [71]. Years later, one by one, the role of each essential component of the complement cascade was identified. The role of the complement system in innate immunity was discovered and elaborated on much later [72,73,74,75,76].
Currently, there are three well-defined complement-activation pathways: the classical, lectin and alternative complement pathways (Figure 1). Notably, these pathways converge at C3 and downstream elements, which contribute to the formation of opsonins, anaphylatoxins, chemo-attractants and the membrane attack complex (MAC) [77,78]. The complement system is regulated by both soluble proteins and cell surface proteins, which continually activate and inactivate these pathways to maintain homeostasis. When an immune reaction occurs against a pathogen, this system is amplified and mediates an inflammatory response which aids immune cells in fighting infection by enhancing ("complementing") the ability of antibodies and phagocytic cells to remove microbes and damaged cells by targeting their plasma membrane.
Most of the complement proteins are produced in the liver, however, it is progressively evident that complement proteins, as well as their receptors and regulators, are expressed throughout the CNS [79]. Although the functions of the complement cascade in the periphery are well deciphered, its functions in the CNS are less clear and under constant investigation.
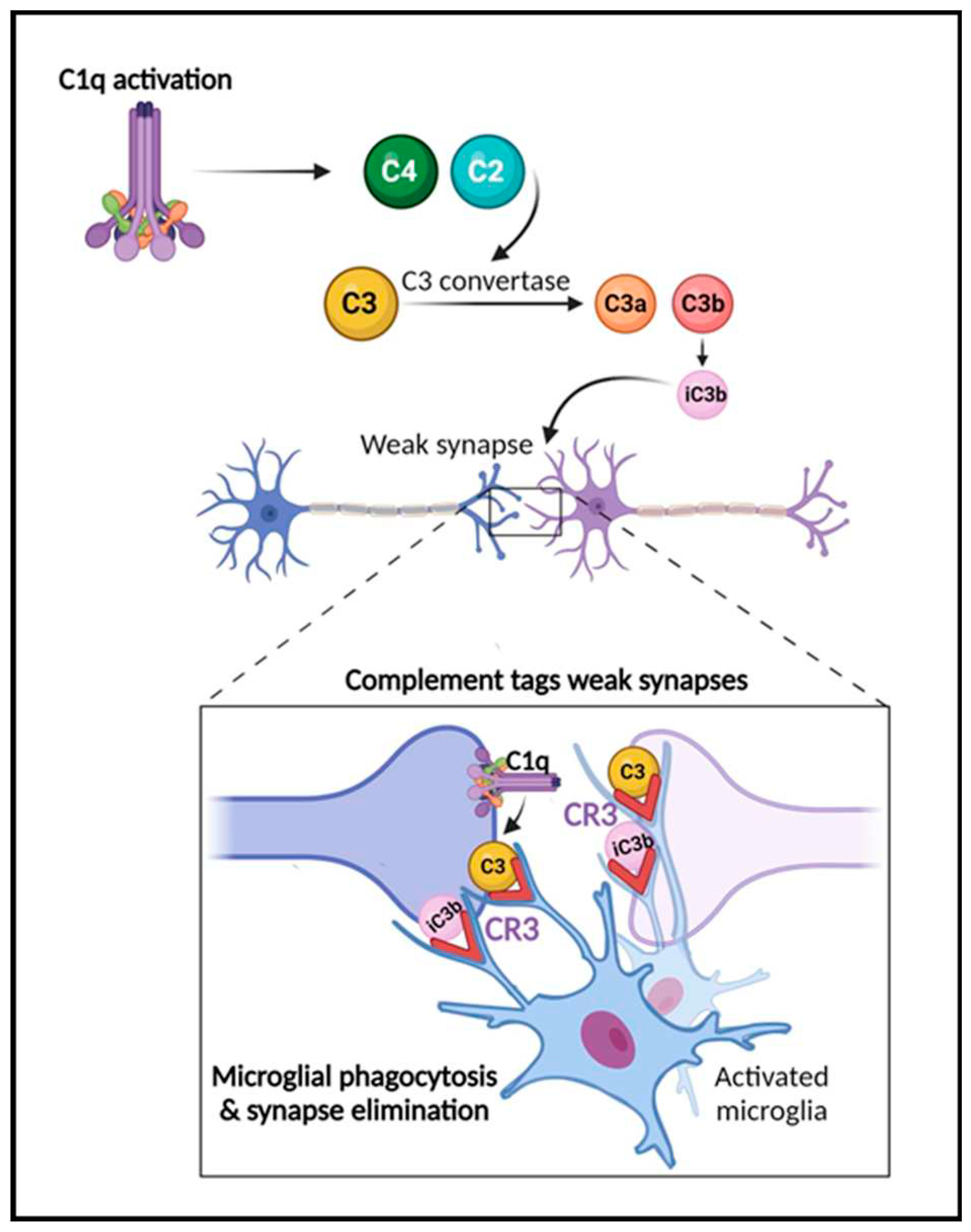
Several reports have shown that complement plays a critical role in the developmental processes of synaptic function and pruning [16,17,18,80,81] (Figure 2). In this process, inactive synapses are cleared to allow bolstering and maturation of more robust connections [17,18]. During refinement of the visual system, for example, early components of the classical complement pathway localize to synapses, tagging them for removal by microglia, which express complement receptors, e.g., CR3/CD11b [16,17,18,51]. When this process occurs inadequately, brain connectivity is affected due to inappropriate connections. Interestingly, changes in brain connectivity have been described in several neurological disorders, including traumatic brain injury [25], multiple sclerosis [12,82,83], stroke and AD [84,85]. The past decade studies have also demonstrated a role for complement in neurodevelopmental disorders such as autism and schizophrenia [86,87,88]. Significant findings have also revealed that complement components C3a, C3a receptor (C3aR), and C3 are critical in adult hippocampal neurogenesis [89,90]. Further, the role of complement in the pathogenesis of Zika virus in the CNS has been shown in mouse models [91]. Recent reports have also highlighted the key role of complement activation in the development of neurological manifestations following SARS-CoV-2 infection [92,93]. Importantly, studies in both animal models and human brain tissue indicate that the impairment of complement regulation may underlie AD pathogenesis [22,23,26,33,63,65,66,67].
4. Complement System in the pathogenesis of AD
In the last 20 years, complement activation has been broadly studied in animal models in the context of mechanisms related to AD. Most AD mouse models express multiple AD-associated gene mutations and thereby emulate features of early-onset forms of AD. Complement expression and its activation have been detected in AD brain tissue and mouse models [33,65,66,68,94,95]. It is now becoming increasingly clear that it serves a major role in AD pathology [16,21,23,96,97]. It has been shown that the classical complement proteins C1q, C3, and C4 co-localize with Aβ plaques and NFTs in memory-related areas in the AD brain [33,65,66,96,98]. Complement components and corresponding mRNA levels are also elevated in the AD brain and cerebrospinal fluid (CSF) [99,100]. Furthermore, increased levels of complement proteins have been reported in astrocyte-derived exosomes isolated from the plasma of AD patients [101]. A microarray study of young, healthy-aged and AD brains demonstrated changes in complement-related gene expression in AD compared to age-matched controls [102]. GWAS have shown complement-related genes linked to AD [50,103,104]. Encoding the membrane protein complement receptor 1 (CR1) and encoding the plasma regulator clusterin (CLU) are genes of the complement pathway that trigger late-onset AD, responsible for 95% of AD cases [103,105,106,107], however, the mechanisms by which these complement genes affect AD pathology are still under investigation. Moreover, the role of complement in the inflammatory response observed in AD has also been widely explored in various reports [22,23,45,63,108,109,110].
C1q, the molecule that initiates the classical complement cascade, and C3, the end product and an “eat me” signal that attracts macrophages expressing C3 receptors (CR3), have been identified as key players in aging and AD pathogenesis [22,23,24,26,45,63,95,108,111]. Notably, fibrillar Aβ attaches to and activates C1q when immunoglobulins are not present, indicating that the classical complement cascade could be mobilized in AD [28]. In the PS/APP mouse model, C1q co-localizes with fibrillar Aβ plaques [69], and in human AD postmortem brain tissue elevated C1q expression levels seem to positively correlate with Aβ plaques [112]. C1q has been demonstrated to localize with synapses and induce synaptic loss in AD mouse models [22], and has been suggested to act as an AD-specific modulator of the cellular crosstalk between microglia and astrocytes [113]. Recently, C1q was shown to be elevated in CSF-derived extracellular vesicles in AD patients compared to non-demented controls [114]. Furthermore, C1q has been shown to be increased in human and mouse brains with age [68,115]. On the other hand, deficiency of C1q in Tg2576 mice was shown to attenuate gliosis and synaptic degeneration without influencing Aβ levels [116]. Interestingly, deficiency of C1q in the 3xTg mouse model increased neurodegeneration [117]. These results suggest a critical role for the complement pathway in mediating AD pathology.
Recently, other complement components of synaptic dysfunction have been suggested to play a role in AD. Carpanini and colleagues showed that MAC fragments are located in the brain of APPNL-G-F AD-like mouse model [118]. Concomitantly, the treatment of anti-C7 antibody reduced synapse loss in aged mice [118]. Furthermore, deficiency of terminal pathway (C6-deficient mice) rescued synapse loss [118] . These data suggest that other complement components drive synapse dysfunction in AD, and open new avenues of therapies for neurodegenerative diseases.
5. Complement component C3 and AD
Complement C3 is the central molecule of the complement cascade, at which the different complement pathways merge (Figure 1) and serves a pivotal role in the immune system [77,78]. C3 has also been identified as a key player during brain development and aging [17,18,24,102]. More specifically, C3 levels have been shown to increase during aging and in AD patient brains and CSF, and overactivation of C3 has been associated with neuronal damage [26]. Following initiation of the classical complement cascade by C1q, C3 is activated leading to the elimination of pathogens [77,78]. Thus, knockout or inhibition of C3, which will inhibit all downstream components of complement activation, may serve as a promising therapeutic target in various disorders, including AD; however, blocking C3 throughout the body may reduce the protection against antigens. Therefore, a site-directed approach to directly lower C3 within the CNS would be more desirable.
We have been investigating the role of complement proteins during aging and AD pathogenesis for the last 20 years [22,23,24,67,69,95,111]. As mentioned above, synapse loss has been described as an early hallmark during aging and it correlates strongly with cognitive impairment in AD [5,6]. Reports have demonstrated that complement pathways mediate neurodegeneration during aging and AD [22,23,24,26]. In our work, we have shown an increase in C3 deposition at the CA3 region of hippocampus in young adult mice (wild-type mice) of 4-months of age, followed by a reduction in synaptic density and neurons in the same region in aged mice of 16-months of age [24]. This suggests that the decrease in number of synapses in CA3 of the hippocampus is functionally significant during aging. We then determined whether C3 could contribute to age-dependent synapse loss in mice. We demonstrated in C3 knockout mice (C3KO) that lifelong C3 deficiency rescued synaptic degeneration during aging and protected against long-term potentiation (LTP) impairment in aged mice, improving their memory. Interestingly, C3 deficiency also rescued neuronal loss at the CA3 region of the hippocampus in aged wild-type (WT) mice. Others have shown that C3 deficiency resulted in elevated neurogenesis in the hippocampus of adult mice due to higher survival of newborn neurons [90]. These data reveal that there are underlying mechanisms by which the hippocampus becomes more susceptible to neurodegeneration during aging and point towards C3 as a viable target for studying brain aging and memory [24].
Next, our group evaluated the role of C3 in memory impairment during neuropathological changes in an amyloidosis mouse model, specifically in APPswe/PS1Δ9 mice [23]. First, we showed that lifelong C3 deficiency in APPswe/PS1Δ9 mice rescued cognition and learning at 16 months of age. We had previously reported that aged C3-deficient J20 hAPP transgenic mice had a higher Aβ deposition and insoluble Aβ42 level in the hippocampus whereas soluble Aβ levels were decreased in aged C3-deficient APP mice [95]. These results indicate that inhibition of C3, and in effect its downstream activation products, might culminate in an age-dependent elevation in the aggregation of Aβ plaques and insoluble Aβ in the brain of these transgenic mice due to reduced phagocytic activity of microglia.
In addition to the impact of C3 on Aβ burden, C3 deficiency in APP/PS1 mice alleviated the microgliosis and astrogliosis in the hippocampus of the AD-like mice. The number of glial cells positioned within plaques was diminished in these mice, implying that C3 deficiency may alter the glial cell response to plaques to favor downregulation of some pro-inflammatory cytokine levels, including TNF-α, IFN-γ and IL-12. Further, C3 deficiency had protective effects against synaptic and neuronal loss in the hippocampal CA3 region in APP/PS1 mice [23] but not in J20 mice in which gliosis was not altered and more neuritic dystrophy was observed. The results in our C3-deficient APP/PS1 mice were corroborated by Wu et al. [26] in another amyloid mouse model, suggesting that there is something unusual about the immune response in the J20 C3-deficient line. These results indicate that during neuroinflammation C3 may play a critical role that facilitates synaptic impairment.
6. Driving mechanisms of complement-mediated CNS dysfunction
A study by Xin et al. demonstrated through in vivo lipopolysaccharides (LPS) injections how the innate immune system drives synapse loss and memory impairment in mice [119]. In humans and mice, the endotoxin in LPS induces immune cells to produce pro-inflammatory cytokines that trigger inflammation. In the study, complement protein levels (C1q and C3) were increased in the hippocampi of the LPS-injected mice and this was associated with both phagocytic activity of microglia and memory loss [119]. This is consistent with the notion that peripheral inflammation, in this case caused by LPS, induces complement-mediated synapse loss and learning impairment in mice.
Nevertheless, the mechanisms by which the complement cascade regulates and affects neuronal function and dysfunction in the brain are relatively unknown. Some reports have proposed potential mechanisms by which complement may mediate neurodegenerative pathology. It is known that C1q, along with TNF-α and IL-1α, are secreted by activated microglia to stimulate the conversion of astrocytes into their reactive pattern (A1 astrocytes), contributing to neurodegeneration, synaptic loss and impairment of synaptic pruning [59]. A1 astrocytes, which express elevated levels of C3, are found in several neurodegenerative diseases, including AD [59]. Complement C3 has been proposed as an astroglial initiator of NFκB signaling through neuronal C3aR, which is a G protein-coupled receptor expressed in many cell types [59,108]. NFκB/C3/C3aR signaling causes dendritic and synaptic loss in neurons, and hence, it makes sense that C3aR antagonist-treated APP/PS1 mice exhibit improved cognition [108].
A study by Propson et al. investigated the role of C3a/C3aR signaling in the context of blood-brain barrier (BBB) permeability during aging [120]. They showed that the C3a/C3aR pathway, specifically in endothelial cells of the brain, altered vascularity, increased BBB permeability, and enhanced microglial reactivity in aged WT mice. The deleterious effects of the signaling pathway were rescued by germline knock-out of C3aR or through elimination of C3aR using a pharmacological inhibitor [120]. The authors further elucidated the BBB vasculature phenotype which was exacerbated in AD-like PS19 tau-transgenic mice. Notably, C3aR ablation in this tau mouse model significantly improved vascular dysfunction . Taken together, these data suggest that the C3/C3aR signaling pathway is an important determinant of the BBB integrity during aging and that this pathway contributes to vascular dysfunction in tauopathy [120]. Moreover, a role for C3/C3aR signaling in mediating the interaction between astrocytes, microglia and neurons upon the presence of gut Helicobacter pylori-derived outer membrane vesicles, can contribute to the AD pathology [110]. These recent data reveal that Helicobacter pylori has a damaging effect on the brain and increases Aβ pathology via C3/C3aR signaling [110].
Microglia, the resident immune cells in the brain, are also known to express C3aR [121]. Lian et al. reported that C3 released from astrocytes interacts with C3aR on microglia and mediates Aβ pathology and neuroinflammation in AD, and these pathological features were ameliorated following treatment with a C3aR antagonist [45]. Further, C3aR deficiency rescued the dysregulated lipid profiles and ameliorated Aβ pathology and cognition improvement in an AD-like mouse model [122]. The authors also described metabolic-related changes in the transcriptome, and suggested that targeting this pathway (C3a) could be a therapeutic strategy for AD [122]. C3 and CR3 also contribute to Aβ clearance mediated by microglia, thereby supporting the beneficial functions of microglia during AD pathogenesis [95,111,123,124]. Furthermore, the microglial CR3 can regulate Aβ homeostasis via proteolytic activity, independent of phagocytosis [125].
7. Complement components as therapeutical targets in AD
Therapeutic inhibition of the complement system has been highlighted as a promising therapeutic target for the treatment of neurodegenerative diseases [20]. In addition to the C3aR antagonist mentioned above, other complement proteins have been identified as potential targets in AD immunotherapy. For instance, inhibition of the complement C5a receptor (C5aR1) with an antagonist (PMX205) reduced Aβ pathology and improved cognition in transgenic AD mice [126]. The antagonist reduced dystrophic neurites, Aβ levels and rescued the loss of pre-synaptic markers in Tg2576 mice [127], and was associated with AD rescue of memory loss and partially restored microglial homeostatic genes [127]. Another study has shown that EP67, a modified C5a receptor agonist in an AD amyloidosis mouse model (5xFAD model), boosted microglial phagocytosis of both fibrillar and non-fibrillar Aβ, improving cognitive impairment and protecting against synapse loss [128]. Furthermore, another groups showed overxpression of C5a caused cognitive decline in mice and increased the levels of complement components (e.g. C3) in the Arctic model of AD [129]. Another study also showed that C5a deficiency reduced astrogliosis and microglial activation [127]. A 2020 study by Wang et al. demonstrated that overexpression of CD55, an inhibitor of complement pathways expressed in neurons in response to inflammation, led to decreased elimination of synapses in the dentate gyrus of mice hippocampi [130]. In addition, overexpression of CD55 in the CA1 region of the mouse hippocampus also resulted in less dissociation of synapses and less forgetting of remote memories [130].
More recently, C8γ, one of the three subunits of C8 (α, β, γ), which constitutes a component of MAC, was identified for the first time as a neuroinflammation inhibitor in the AD brain [131]. Researchers revealed higher C8γ levels in the brain, CSF, and plasma of AD patients, as well as in the mouse brain, where C8γ was found to mainly localize in astrocytes, perhaps as an attempt to prevent complement overactivation. C8γ has been shown to inhibit glial hyperactivation, neuroinflammation, and cognitive decline in AD mouse models, highlighting its role as immune-modulator (acting as an anti-inflammatory marker) and subsequently its potential as a therapeutic target in AD and other neurological disorders [131].
8. Crosstalk between the complement system and other inflammatory players in AD
It is important to consider the interaction between complement proteins and cytokines since pro-inflammatory cytokines have long been implicated in neurodegenerative mechanisms. One such class of cytokines, Type I interferons (IFNs), are produced by the innate immune system especially in response to viral infections [132]. Additionally, IFNs are predominantly expressed by immune cells upon activation of intracellular innate immune sensors [132]. In AD, its role has been extensively investigated. One study demonstrated the role of IFN responses leading to the neuroinflammation and synaptic loss in AD [46]. Overactivation of the IFN pathway was observed in amyloidosis mice models with its activation manifested in plaque-associated microglia. Furthermore, IFN activation led to microglial activation and a pronounced synaptic degeneration in mice. Also, IFN stimulated the complement cascade, with an increase of complement proteins (e.g., C1q and C3) in both in vitro and in vivo models. Notably, APPNL-G-F/NL-G-F mice that were treated with IFN blocking antibodies showed a protection of synapses and decreased C3 expression. Lack of IFN signaling also showed protective effects in APP/PS1 and 5xFAD mice, as reflected in decreased synapse loss and microglial activation [133,134]. In C3KO mice that received recombinant IFN, the brains were protected against synaptic degeneration, despite the activation of microglia. These findings suggest that IFN-C3 axis is important in promoting synapse loss in AD-like mice models [46].
Apolipoprotein-E (ApoE) is another molecule that has been linked to AD, atherosclerosis, and other inflammatory conditions [135]. In particular, the ApoE4 allele has been associated with an elevated risk of AD [135,136]. In an extensive report in 2014, Yin et al. showed that the complement pathway in ApoE-deficient mice is activated in atherosclerosis and AD [137]. Interestingly, this group has shown that ApoE binding to activated C1q inhibits activation of classical complement cascade; however, formation of C1q-ApoE complexes is seen within Aβ plaques and arteries, and correlated with cognitive impairment and atherosclerosis [137]. Taken together, these results suggest that ApoE may be a checkpoint inhibitor for activation of the classical complement cascade. The C1q-ApoE complex was suggested to further affect AD pathology by modulating microglia-mediated synaptic clearance [138]. Furthermore, upon intracerebroventricular injections of Aβ oligomers, a profound increase of C3 reactivity was observed in the choroid plexus [139]. Aβ oligomers are synaptotoxins linked to synapse dysfunction in AD [1], and possibly this data could be associated to early stages of AD and impacting the choroid plexus. On the other hand, ApoE2 allele has been associated with a decreased risk of AD [140,141]. Panitch and colleagues revealed an interaction of ApoE2 with complement components C4A and C4B, as well as with HSPA2 oligodendrocyte-specific protein, which was significantly linked to the complement cascade, that leads to neuroprotective effects against AD [142]. This finding indicates a strong link between the complement system and the protective effects of ApoE2 allele in AD.
The triggering receptor expressed on myeloid cells 2 (TREM2) is an innate immune receptor of the immunoglobulin superfamily, expressed in different populations of myeloid cells including microglia in the CNS [143]. Its variants have been associated with an increased risk for AD [144,145]. Functionally, TREM2 is required for important cellular functions such as chemotaxis, maintenance of energy metabolism and phagocytosis of Aβ fibrils [146]. Along with ApoE, TREM2 is also upregulated in microglia responding to brain lesions [8,48,143]. Pointing towards a possible interaction between microglial activity and TREM2, it was demonstrated that in TREM2 knockout mice, there is persistent impairment of synaptic refinement during the early stages of brain development [53], suggesting that TREM2 regulates microglial activity at this critical time. Furthermore, TREM2 receptor deficiency results in impaired synaptic clearance, elevated dendritic spine density and enhanced excitatory neurotransmission [147]. These findings indicate that microglial TREM2 could impact the process of synapse elimination. Importantly, studies have inferred an association between TREM2 and C1q in microglia-mediated synaptic pruning, due to their co-localization around Aβ plaques [148,149]. As mentioned above, C1q also interacts with ApoE, forming the C1q-ApoE complex. Consequently, Qin and colleagues recently highlighted as a potential underlying mechanism of the microglia-mediated synaptic loss induced in AD, the interaction between TREM2, APOE and C1q [138].
TYROBP (tyrosine motif binding protein, aka DAP12 or DNAX-binding protein-12) regulates multiple genes involved in microglia phagocytosis, and its expression is increased in aged human AD brains [150] and AD-like mouse models [151]. Interestingly, TYROBP serves as an adaptor for some immune receptor ectodomains, including TREM2 and CR3 [152]. A study by Haure-Mirande et al. proposed that the absence of TYROBP in a mouse model of AD-type cerebral Aβ amyloidosis (APP/PSEN1 mouse model) protected against the dysregulation of complement transcriptomic network during AD pathogenesis [153]. Furthermore, the absence of TYROBP decreased C1q expression in APP/PSEN1 mice [153,154]. The absence of TYROBP in these AD-like mice led to decreased C3 levels in the brain in the early stage of Aβ pathology [152], demonstrating an important interaction between TYROBP and the complement pathway which should be further explored in the future.
9. Complement and Tau pathology
Previous work has shown that amyloid pathology long precedes clinical AD symptoms, and that tau pathology and synapse loss correlate strongly with cognitive impairment [155,156]. Emerging evidence suggests that tau pathology is also associated with complement [26,157,158,159]. In fact, overexpression of a C3 inhibitor (sCrry) reduced the level of hyperphosphorylated tau in aged P301L/sCrry double transgenic mice [157]. More recently, interactions between C3, tau, ApoE4 and Aβ have been identified. In a detailed study, Bonham et al. reported an interaction between ApoE4 genotype and CSF C3 levels on CSF levels of Aβ and pTau in ADNI subjects [160]. However, CSF C3 was only associated with CSF pTau if it was also associated with CSF Aβ [160]. Additionally, in a tau mouse model expressing ApoE4, microglial C3 gene expression was observed to be elevated [161].
Another study demonstrated that C1qa levels are enhanced on postsynaptic dendritic spines in the Tau P301S (PS19) mouse model, as well as in human tissue, and a positive correlation was observed between C1qa and phospho-tau levels [158]. Interestingly, the inhibition of C1q by C1q blocking antibodies rescued the synapse loss induced by microglia in these transgenic mice [158]. Another report has shown that C3 and C3aR are positively associated with cognitive decline in the brains of AD patients [159]. This same work also illustrated the role of C3/C3aR signaling in tau pathogenesis in PS19 mice deficient in C3ar1 [159]. In this study, the authors identified a mechanism dependent on Stat3 by which C3aR regulates tau pathology in tau transgenic mice. Also, when the PS19 tau mice were crossed with mice deficient in C3ar1, there was an improvement in tau pathology, neuroinflammation, synaptic and cognitive impairment in tau transgenic mice [159]. Additionally, Wu et al. indicated that loss of C3 in PS19 mice ameliorated neuronal loss and neurodegeneration, while positively affected neurophysiological and behavioral outcomes [26]. The researchers also revealed that brain and CSF C3 levels are increased in AD patients [26]. Recently, a study demonstrated a mechanism by which astrocytes and microglia engulf excitatory and inhibitory synapses respectively in the PS19 mouse model [162]. Remarkably, excitatory synapses are found in the lysosomes of astrocytes, whereas inhibitory synapses were found in the microglial lysosomes. C1q deficiency reduced astrocyte-synapse and synaptic pruning by both cells and alleviated the synapse loss in the PS19 mouse model. These findings support a role for complement-tau interaction in the pathogenesis of AD.
10. Future directions
In recent years, sophisticated in vitro tools have been used to study the interaction between different players in the complement pathway as it relates to neurodegenerative diseases, including AD. In their 2021 paper, Guttikonda and colleagues unveiled a new triculture system which combines pure populations of neurons, astrocytes, and microglia [113]. They showed that under inflammatory conditions (triggered by LPS), microglia release factors that stimulate astrocytes to produce C3, which feeds back on microglia and triggers them to generate their own supply. The same inflammatory loop was engaged when neurons carried the APP Swedish familial Alzheimer’s mutation, with both microglia and astrocytes participating. Altogether, the data suggested that microglia containing C3 kick off an inflammatory loop by releasing TNF-α. This provokes astrocytes to release large amounts of C3, which stimulates microglia to produce even more of the complement protein. Mutant APP exacerbates this cross talk, implicating this pathway in AD [113]. Although this triculture model presents an exciting new system to promptly define cellular pathways, it must be noted that findings from this study still need to be validated in vivo, because the limitation of cell culture models such as this one lay in not being able to fully capture age- and time-dependent effects which are vital in painting a holistic picture of the AD pathology.
11. Conclusion
The role of the complement system during both healthy and diseased brain states has been widely investigated. This review summarizes pertinent evidence which emphasizes the pivotal role of aberrant complement cascade activation in neurodegenerative diseases, especially in AD. We also show that different proteins in the complement pathway interact with other key players in neuroinflammation and neurodegeneration such astrocytes, microglia, ApoE and TREM2, among others. Findings discussed in this report support the notion that targeting complement proteins, including cell-specific targeting, may represent a promising new approach to protect the brain in AD, slow the progression of the disease, and potentially improve cognitive and memory outcomes for AD patients in the future.
Author Contributions
Conceptualization: AFB; KK; MTP and, CAL; Writing- review and editing: AFB; KK; MTP; Figures: MTP; CAL; All authors have read and agreed to the submitted version of the manuscript.
Funding
NIH RF1 AG060057 – CAL.
Acknowledgments
We thank Brittani Price (Ann Romney Center for Neurologic Diseases) for critical review of the manuscript.
Conflicts of Interest
AFB, MTP, and KK have no conflicts of interest to declare. CAL serves on the scientific advisory boards or as a consultant for AC Immune, Acumen Pharmaceuticals, ADvantage Therapeutics, Alnylam Pharmaceuticals, Apellis Pharmaceuticals, Cognition Therapeutics, Cyclo Therapeutics, MEDAcorp, Novo Nordisk and Sanofi Genzyme.
References
- Selkoe, D.J. and J. Hardy, The amyloid hypothesis of Alzheimer's disease at 25 years. EMBO Mol Med, 2016. 8(6): p. 595-608. [CrossRef]
- World Alzheimer Report 2018 The State of the art of dementia research: New Frontiers. Alzheimer's Disease International, 2018.
- 2023 Alzheimer's disease facts and figures. Alzheimers Dement, 2023. 19(4): p. 1598-1695.
- Organization, W.H., World Health Organization (WHO), 2023.
- Terry, R.D., et al., Physical basis of cognitive alterations in Alzheimer's disease: synapse loss is the major correlate of cognitive impairment. Ann Neurol, 1991. 30(4): p. 572-80. [CrossRef]
- Masliah, E., et al., Immunoelectron microscopic study of synaptic pathology in Alzheimer's disease. Acta Neuropathol, 1991. 81(4): p. 428-33. [CrossRef]
- Hammond, T.R., et al., Single-Cell RNA Sequencing of Microglia throughout the Mouse Lifespan and in the Injured Brain Reveals Complex Cell-State Changes. Immunity, 2019. 50(1): p. 253-271 e6. [CrossRef]
- Keren-Shaul, H., et al., A Unique Microglia Type Associated with Restricting Development of Alzheimer's Disease. Cell, 2017. 169(7): p. 1276-1290 e17. [CrossRef]
- Stubbington, M.J.T., et al., Single-cell transcriptomics to explore the immune system in health and disease. Science, 2017. 358(6359): p. 58-63. [CrossRef]
- Felsky, D., et al., Neuropathological correlates and genetic architecture of microglial activation in elderly human brain. Nat Commun, 2019. 10(1): p. 409. [CrossRef]
- Jansen, I.E., et al., Genome-wide meta-analysis identifies new loci and functional pathways influencing Alzheimer's disease risk. Nat Genet, 2019. 51(3): p. 404-413. [CrossRef]
- Ponath, G., et al., Enhanced astrocyte responses are driven by a genetic risk allele associated with multiple sclerosis. Nat Commun, 2018. 9(1): p. 5337. [CrossRef]
- Mathys, H., et al., Temporal Tracking of Microglia Activation in Neurodegeneration at Single-Cell Resolution. Cell Rep, 2017. 21(2): p. 366-380. [CrossRef]
- Walport, M.J., Complement. Second of two parts. N Engl J Med, 2001. 344(15): p. 1140-4. [CrossRef]
- Walport, M.J., Complement. First of two parts. N Engl J Med, 2001. 344(14): p. 1058-66. [CrossRef]
- Stephan, A.H., B.A. Barres, and B. Stevens, The complement system: an unexpected role in synaptic pruning during development and disease. Annu Rev Neurosci, 2012. 35: p. 369-89. [CrossRef]
- Schafer, D.P., et al., Microglia sculpt postnatal neural circuits in an activity and complement-dependent manner. Neuron, 2012. 74(4): p. 691-705. [CrossRef]
- Stevens, B., et al., The classical complement cascade mediates CNS synapse elimination. Cell, 2007. 131(6): p. 1164-78. [CrossRef]
- Gorelik, A., et al., Developmental activities of the complement pathway in migrating neurons. Nat Commun, 2017. 8: p. 15096. [CrossRef]
- Carpanini, S.M., M. Torvell, and B.P. Morgan, Therapeutic Inhibition of the Complement System in Diseases of the Central Nervous System. Front Immunol, 2019. 10: p. 362. [CrossRef]
- Hammond, T.R., S.E. Marsh, and B. Stevens, Immune Signaling in Neurodegeneration. Immunity, 2019. 50(4): p. 955-974. [CrossRef]
- Hong, S., et al., Complement and microglia mediate early synapse loss in Alzheimer mouse models. Science, 2016. 352(6286): p. 712-716. [CrossRef]
- Shi, Q., et al., Complement C3 deficiency protects against neurodegeneration in aged plaque-rich APP/PS1 mice. Sci Transl Med, 2017. 9(392). [CrossRef]
- Shi, Q., et al., Complement C3-Deficient Mice Fail to Display Age-Related Hippocampal Decline. J Neurosci, 2015. 35(38): p. 13029-42. [CrossRef]
- Krukowski, K., et al., Traumatic Brain Injury in Aged Mice Induces Chronic Microglia Activation, Synapse Loss, and Complement-Dependent Memory Deficits. Int J Mol Sci, 2018. 19(12). [CrossRef]
- Wu, T., et al., Complement C3 Is Activated in Human AD Brain and Is Required for Neurodegeneration in Mouse Models of Amyloidosis and Tauopathy. Cell Rep, 2019. 28(8): p. 2111-2123 e6. [CrossRef]
- Heneka, M.T., et al., Neuroinflammation in Alzheimer's disease. Lancet Neurol, 2015. 14(4): p. 388-405. [CrossRef]
- Rogers, J., et al., Complement activation by beta-amyloid in Alzheimer disease. Proc Natl Acad Sci U S A, 1992. 89(21): p. 10016-20. [CrossRef]
- McGeer, P.L., et al., Activation of the classical complement pathway in brain tissue of Alzheimer patients. Neurosci Lett, 1989. 107(1-3): p. 341-6. [CrossRef]
- McGeer, P.L., et al., Occurrence of HLA-DR reactive microglia in Alzheimer's disease. Ann N Y Acad Sci, 1988. 540: p. 319-23. [CrossRef]
- McGeer, P.L., et al., Reactive microglia in patients with senile dementia of the Alzheimer type are positive for the histocompatibility glycoprotein HLA-DR. Neurosci Lett, 1987. 79(1-2): p. 195-200. [CrossRef]
- Zotova, E., et al., Inflammatory components in human Alzheimer's disease and after active amyloid-beta42 immunization. Brain, 2013. 136(Pt 9): p. 2677-96. [CrossRef]
- Eikelenboom, P. and F.C. Stam, Immunoglobulins and complement factors in senile plaques. An immunoperoxidase study. Acta Neuropathol, 1982. 57(2-3): p. 239-42. [CrossRef]
- Kamphuis, W., et al., GFAP isoforms in adult mouse brain with a focus on neurogenic astrocytes and reactive astrogliosis in mouse models of Alzheimer disease. PLoS One, 2012. 7(8): p. e42823. [CrossRef]
- Hanzel, D.K., et al., High-throughput quantitative histological analysis of Alzheimer's disease pathology using a confocal digital microscanner. Nat Biotechnol, 1999. 17(1): p. 53-7. [CrossRef]
- Stephenson, J., et al., Inflammation in CNS neurodegenerative diseases. Immunology, 2018. 154(2): p. 204-219. [CrossRef]
- Brosseron, F., et al., Body fluid cytokine levels in mild cognitive impairment and Alzheimer's disease: a comparative overview. Mol Neurobiol, 2014. 50(2): p. 534-44. [CrossRef]
- Brosseron, F., et al., Characterization and clinical use of inflammatory cerebrospinal fluid protein markers in Alzheimer's disease. Alzheimers Res Ther, 2018. 10(1): p. 25. [CrossRef]
- Tian, Z., X. Ji, and J. Liu, Neuroinflammation in Vascular Cognitive Impairment and Dementia: Current Evidence, Advances, and Prospects. Int J Mol Sci, 2022. 23(11). [CrossRef]
- Nimmerjahn, A., F. Kirchhoff, and F. Helmchen, Resting microglial cells are highly dynamic surveillants of brain parenchyma in vivo. Science, 2005. 308(5726): p. 1314-8. [CrossRef]
- Sheng, J., C. Ruedl, and K. Karjalainen, Most Tissue-Resident Macrophages Except Microglia Are Derived from Fetal Hematopoietic Stem Cells. Immunity, 2015. 43(2): p. 382-93. [CrossRef]
- Lawson, L.J., et al., Heterogeneity in the distribution and morphology of microglia in the normal adult mouse brain. Neuroscience, 1990. 39(1): p. 151-70. [CrossRef]
- Hong, S., L. Dissing-Olesen, and B. Stevens, New insights on the role of microglia in synaptic pruning in health and disease. Curr Opin Neurobiol, 2016. 36: p. 128-34. [CrossRef]
- Sarlus, H. and M.T. Heneka, Microglia in Alzheimer's disease. J Clin Invest, 2017. 127(9): p. 3240-3249. [CrossRef]
- Lian, H., et al., Astrocyte-Microglia Cross Talk through Complement Activation Modulates Amyloid Pathology in Mouse Models of Alzheimer's Disease. J Neurosci, 2016. 36(2): p. 577-89. [CrossRef]
- Roy, E.R., et al., Type I interferon response drives neuroinflammation and synapse loss in Alzheimer disease. J Clin Invest, 2020. 130(4): p. 1912-1930. [CrossRef]
- Butovsky, O. and H.L. Weiner, Microglial signatures and their role in health and disease. Nat Rev Neurosci, 2018. 19(10): p. 622-635. [CrossRef]
- Krasemann, S., et al., The TREM2-APOE Pathway Drives the Transcriptional Phenotype of Dysfunctional Microglia in Neurodegenerative Diseases. Immunity, 2017. 47(3): p. 566-581 e9. [CrossRef]
- Hansen, D.V., J.E. Hanson, and M. Sheng, Microglia in Alzheimer's disease. J Cell Biol, 2018. 217(2): p. 459-472. [CrossRef]
- Lambert, J.C., et al., Genome-wide association study identifies variants at CLU and CR1 associated with Alzheimer's disease. Nat Genet, 2009. 41(10): p. 1094-9. [CrossRef]
- Schafer, D.P., E.K. Lehrman, and B. Stevens, The "quad-partite" synapse: microglia-synapse interactions in the developing and mature CNS. Glia, 2013. 61(1): p. 24-36. [CrossRef]
- Paolicelli, R.C., et al., Synaptic pruning by microglia is necessary for normal brain development. Science, 2011. 333(6048): p. 1456-8. [CrossRef]
- Filipello, F., et al., The Microglial Innate Immune Receptor TREM2 Is Required for Synapse Elimination and Normal Brain Connectivity. Immunity, 2018. 48(5): p. 979-991 e8. [CrossRef]
- Paolicelli, R.C. and C.T. Gross, Microglia in development: linking brain wiring to brain environment. Neuron Glia Biol, 2011. 7(1): p. 77-83. [CrossRef]
- Rogers, J.T., et al., CX3CR1 deficiency leads to impairment of hippocampal cognitive function and synaptic plasticity. J Neurosci, 2011. 31(45): p. 16241-50. [CrossRef]
- Bailey, C.H., E.R. Kandel, and K.M. Harris, Structural Components of Synaptic Plasticity and Memory Consolidation. Cold Spring Harb Perspect Biol, 2015. 7(7): p. a021758. [CrossRef]
- Venegas, C., et al., Microglia-derived ASC specks cross-seed amyloid-beta in Alzheimer's disease. Nature, 2017. 552(7685): p. 355-361. [CrossRef]
- Arranz, A.M. and B. De Strooper, The role of astroglia in Alzheimer's disease: pathophysiology and clinical implications. Lancet Neurol, 2019. 18(4): p. 406-414. [CrossRef]
- Liddelow, S.A., et al., Neurotoxic reactive astrocytes are induced by activated microglia. Nature, 2017. 541(7638): p. 481-487. [CrossRef]
- Brambilla, R., et al., Transgenic inhibition of astroglial NF-kappa B leads to increased axonal sparing and sprouting following spinal cord injury. J Neurochem, 2009. 110(2): p. 765-78. [CrossRef]
- Diniz, L.P., et al., Astrocyte Transforming Growth Factor Beta 1 Protects Synapses against Abeta Oligomers in Alzheimer's Disease Model. J Neurosci, 2017. 37(28): p. 6797-6809. [CrossRef]
- Bellaver, B., et al., Astrocyte reactivity influences amyloid-beta effects on tau pathology in preclinical Alzheimer's disease. Nat Med, 2023. 29(7): p. 1775-1781. [CrossRef]
- Lian, H. and H. Zheng, Signaling pathways regulating neuron-glia interaction and their implications in Alzheimer's disease. J Neurochem, 2016. 136(3): p. 475-91. [CrossRef]
- Eikelenboom, P., et al., Complement activation in amyloid plaques in Alzheimer's dementia. Virchows Arch B Cell Pathol Incl Mol Pathol, 1989. 56(4): p. 259-62. [CrossRef]
- Ishii, T. and S. Haga, Immuno-electron-microscopic localization of complements in amyloid fibrils of senile plaques. Acta Neuropathol, 1984. 63(4): p. 296-300. [CrossRef]
- Afagh, A., et al., Localization and cell association of C1q in Alzheimer's disease brain. Exp Neurol, 1996. 138(1): p. 22-32. [CrossRef]
- Stoltzner, S.E., et al., Temporal accrual of complement proteins in amyloid plaques in Down's syndrome with Alzheimer's disease. Am J Pathol, 2000. 156(2): p. 489-99. [CrossRef]
- Reichwald, J., et al., Expression of complement system components during aging and amyloid deposition in APP transgenic mice. J Neuroinflammation, 2009. 6: p. 35. [CrossRef]
- Matsuoka, Y., et al., Inflammatory responses to amyloidosis in a transgenic mouse model of Alzheimer's disease. Am J Pathol, 2001. 158(4): p. 1345-54. [CrossRef]
- Nonaka, M. and A. Kimura, Genomic view of the evolution of the complement system. Immunogenetics, 2006. 58(9): p. 701-13. [CrossRef]
- Bordet, J., Les leukocytes et les proprietes actives du serum chez les vaccines. Ann. Inst. Pasteur, 1895. 462–506.
- Hadding, U. and H.J. Muller-Eberhard, The ninth component of human complement: isolation, description and mode of action. Immunology, 1969. 16(6): p. 719-35.
- Nilsson, U., Separation and partial purification of the sixth, seventh and eighth components of human haemolytic complement. Acta Pathol Microbiol Scand, 1967. 70(3): p. 469-80. [CrossRef]
- Nilsson, U.R. and H.J. Mueller-Eberhard, Isolation of Beta If-Globulin from Human Serum and Its Characterization as the Fifth Component of Complement. J Exp Med, 1965. 122: p. 277-98. [CrossRef]
- Mueller-Eberhard, H.J. and C.E. Biro, Isolation and Description of the Fourth Component of Human Complement. J Exp Med, 1963. 118: p. 447-66. [CrossRef]
- Pillemer, L. and E.E. Ecker, The Terminology of the Components of Complement. Science, 1941. 94(2445): p. 437. [CrossRef]
- Merle, N.S., et al., Complement System Part I - Molecular Mechanisms of Activation and Regulation. Front Immunol, 2015. 6: p. 262. [CrossRef]
- Merle, N.S., et al., Complement System Part II: Role in Immunity. Front Immunol, 2015. 6: p. 257. [CrossRef]
- Coulthard, L.G., O.A. Hawksworth, and T.M. Woodruff, Complement: The Emerging Architect of the Developing Brain. Trends Neurosci, 2018. 41(6): p. 373-384. [CrossRef]
- Bialas, A.R. and B. Stevens, TGF-beta signaling regulates neuronal C1q expression and developmental synaptic refinement. Nat Neurosci, 2013. 16(12): p. 1773-82. [CrossRef]
- Perez-Alcazar, M., et al., Altered cognitive performance and synaptic function in the hippocampus of mice lacking C3. Exp Neurol, 2014. 253: p. 154-64. [CrossRef]
- Fitzgerald, K.C., et al., Early complement genes are associated with visual system degeneration in multiple sclerosis. Brain, 2019. 142(9): p. 2722-2736. [CrossRef]
- Werneburg, S., et al., Targeted Complement Inhibition at Synapses Prevents Microglial Synaptic Engulfment and Synapse Loss in Demyelinating Disease. Immunity, 2020. 52(1): p. 167-182 e7. [CrossRef]
- Sun, Y., et al., Disrupted functional brain connectivity and its association to structural connectivity in amnestic mild cognitive impairment and Alzheimer's disease. PLoS One, 2014. 9(5): p. e96505. [CrossRef]
- Siegel, J.S., et al., Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc Natl Acad Sci U S A, 2016. 113(30): p. E4367-76. [CrossRef]
- Brown, A.S., Epidemiologic studies of exposure to prenatal infection and risk of schizophrenia and autism. Dev Neurobiol, 2012. 72(10): p. 1272-6. [CrossRef]
- Sekar, A., et al., Schizophrenia risk from complex variation of complement component 4. Nature, 2016. 530(7589): p. 177-83. [CrossRef]
- Yilmaz, M., et al., Overexpression of schizophrenia susceptibility factor human complement C4A promotes excessive synaptic loss and behavioral changes in mice. Nat Neurosci, 2021. 24(2): p. 214-224. [CrossRef]
- Rahpeymai, Y., et al., Complement: a novel factor in basal and ischemia-induced neurogenesis. EMBO J, 2006. 25(6): p. 1364-74. [CrossRef]
- Westacott, L.J., et al., Dissociable effects of complement C3 and C3aR on survival and morphology of adult born hippocampal neurons, pattern separation, and cognitive flexibility in male mice. Brain Behav Immun, 2021. 98: p. 136-150. [CrossRef]
- Figueiredo, C.P., et al., Zika virus replicates in adult human brain tissue and impairs synapses and memory in mice. Nat Commun, 2019. 10(1): p. 3890. [CrossRef]
- Jaffry M, F.I., Jaffry K, Neurological Manifestations of SARS-CoV-2 Infection and the Role of Complement Activation. touchREVIEWS in Neurology, 2022. 18(2): p. 86-92. [CrossRef]
- Lee, M.H., et al., Neurovascular injury with complement activation and inflammation in COVID-19. Brain, 2022. 145(7): p. 2555-2568. [CrossRef]
- Zhou, J., et al., Complement C3 and C4 expression in C1q sufficient and deficient mouse models of Alzheimer's disease. J Neurochem, 2008. 106(5): p. 2080-92. [CrossRef]
- Maier, M., et al., Complement C3 deficiency leads to accelerated amyloid beta plaque deposition and neurodegeneration and modulation of the microglia/macrophage phenotype in amyloid precursor protein transgenic mice. J Neurosci, 2008. 28(25): p. 6333-41. [CrossRef]
- Thambisetty, M., et al., Effect of complement CR1 on brain amyloid burden during aging and its modification by APOE genotype. Biol Psychiatry, 2013. 73(5): p. 422-8. [CrossRef]
- Hernandez, M.X., et al., Prevention of C5aR1 signaling delays microglial inflammatory polarization, favors clearance pathways and suppresses cognitive loss. Mol Neurodegener, 2017. 12(1): p. 66. [CrossRef]
- Shen, Y., et al., Complement activation by neurofibrillary tangles in Alzheimer's disease. Neurosci Lett, 2001. 305(3): p. 165-8. [CrossRef]
- Daborg, J., et al., Cerebrospinal fluid levels of complement proteins C3, C4 and CR1 in Alzheimer's disease. J Neural Transm (Vienna), 2012. 119(7): p. 789-97. [CrossRef]
- Strohmeyer, R., Y. Shen, and J. Rogers, Detection of complement alternative pathway mRNA and proteins in the Alzheimer's disease brain. Brain Res Mol Brain Res, 2000. 81(1-2): p. 7-18. [CrossRef]
- Goetzl, E.J., et al., High complement levels in astrocyte-derived exosomes of Alzheimer disease. Ann Neurol, 2018. 83(3): p. 544-552. [CrossRef]
- Cribbs, D.H., et al., Extensive innate immune gene activation accompanies brain aging, increasing vulnerability to cognitive decline and neurodegeneration: a microarray study. J Neuroinflammation, 2012. 9: p. 179. [CrossRef]
- Harold, D., et al., Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer's disease. Nat Genet, 2009. 41(10): p. 1088-93. [CrossRef]
- Bellenguez, C., et al., New insights into the genetic etiology of Alzheimer's disease and related dementias. Nat Genet, 2022. 54(4): p. 412-436. [CrossRef]
- Gatz, M., et al., Role of genes and environments for explaining Alzheimer disease. Arch Gen Psychiatry, 2006. 63(2): p. 168-74. [CrossRef]
- Crehan, H., et al., Complement receptor 1 (CR1) and Alzheimer's disease. Immunobiology, 2012. 217(2): p. 244-50. [CrossRef]
- Kucukkilic, E., et al., Complement receptor 1 gene (CR1) intragenic duplication and risk of Alzheimer's disease. Hum Genet, 2018. 137(4): p. 305-314. [CrossRef]
- Lian, H., et al., NFkappaB-activated astroglial release of complement C3 compromises neuronal morphology and function associated with Alzheimer's disease. Neuron, 2015. 85(1): p. 101-115. [CrossRef]
- El Gaamouch, F., et al., VGF-derived peptide TLQP-21 modulates microglial function through C3aR1 signaling pathways and reduces neuropathology in 5xFAD mice. Mol Neurodegener, 2020. 15(1): p. 4. [CrossRef]
- Xie, J., et al., Helicobacter pylori-derived outer membrane vesicles contribute to Alzheimer's disease pathogenesis via C3-C3aR signalling. J Extracell Vesicles, 2023. 12(2): p. e12306. [CrossRef]
- Fu, H., et al., Complement component C3 and complement receptor type 3 contribute to the phagocytosis and clearance of fibrillar Abeta by microglia. Glia, 2012. 60(6): p. 993-1003. [CrossRef]
- Tooyama, I., et al., Correlation of the expression level of C1q mRNA and the number of C1q-positive plaques in the Alzheimer Disease temporal cortex. analysis of C1q mrna and its protein using adjacent or nearby sections. Dement Geriatr Cogn Disord, 2001. 12(4): p. 237-42. [CrossRef]
- Guttikonda, S.R., et al., Fully defined human pluripotent stem cell-derived microglia and tri-culture system model C3 production in Alzheimer's disease. Nat Neurosci, 2021. 24(3): p. 343-354. [CrossRef]
- Chatterjee, M., et al., C1q is increased in cerebrospinal fluid-derived extracellular vesicles in Alzheimer's disease: A multi-cohort proteomics and immuno-assay validation study. Alzheimers Dement, 2023. [CrossRef]
- Stephan, A.H., et al., A dramatic increase of C1q protein in the CNS during normal aging. J Neurosci, 2013. 33(33): p. 13460-74. [CrossRef]
- Fonseca, M.I., et al., Absence of C1q leads to less neuropathology in transgenic mouse models of Alzheimer's disease. J Neurosci, 2004. 24(29): p. 6457-65. [CrossRef]
- Benoit, M.E., et al., C1q-induced LRP1B and GPR6 proteins expressed early in Alzheimer disease mouse models, are essential for the C1q-mediated protection against amyloid-beta neurotoxicity. J Biol Chem, 2013. 288(1): p. 654-65. [CrossRef]
- Carpanini, S.M., et al., Terminal complement pathway activation drives synaptic loss in Alzheimer's disease models. Acta Neuropathol Commun, 2022. 10(1): p. 99. [CrossRef]
- Xin, Y.R., et al., The Immune System Drives Synapse Loss During Lipopolysaccharide-Induced Learning and Memory Impairment in Mice. Front Aging Neurosci, 2019. 11: p. 279. [CrossRef]
- Propson, N.E., et al., Endothelial C3a receptor mediates vascular inflammation and blood-brain barrier permeability during aging. J Clin Invest, 2021. 131(1). [CrossRef]
- Zhang, J., et al., Microglial CR3 activation triggers long-term synaptic depression in the hippocampus via NADPH oxidase. Neuron, 2014. 82(1): p. 195-207. [CrossRef]
- Gedam, M., et al., Complement C3aR depletion reverses HIF-1alpha-induced metabolic impairment and enhances microglial response to Abeta pathology. J Clin Invest, 2023. 133(12). [CrossRef]
- Wyss-Coray, T., et al., Prominent neurodegeneration and increased plaque formation in complement-inhibited Alzheimer's mice. Proc Natl Acad Sci U S A, 2002. 99(16): p. 10837-42. [CrossRef]
- Choucair-Jaafar, N., et al., Complement receptor 3 (CD11b/CD18) is implicated in the elimination of beta-amyloid peptides. Fundam Clin Pharmacol, 2011. 25(1): p. 115-22. [CrossRef]
- Czirr, E., et al., Microglial complement receptor 3 regulates brain Abeta levels through secreted proteolytic activity. J Exp Med, 2017. 214(4): p. 1081-1092. [CrossRef]
- Fonseca, M.I., et al., Treatment with a C5aR antagonist decreases pathology and enhances behavioral performance in murine models of Alzheimer's disease. J Immunol, 2009. 183(2): p. 1375-83. [CrossRef]
- Gomez-Arboledas, A., et al., C5aR1 antagonism alters microglial polarization and mitigates disease progression in a mouse model of Alzheimer's disease. Acta Neuropathol Commun, 2022. 10(1): p. 116. [CrossRef]
- Panayiotou, E., et al., C5aR agonist enhances phagocytosis of fibrillar and non-fibrillar Abeta amyloid and preserves memory in a mouse model of familial Alzheimer's disease. PLoS One, 2019. 14(12): p. e0225417. [CrossRef]
- Carvalho, K., et al., Modulation of C5a-C5aR1 signaling alters the dynamics of AD progression. J Neuroinflammation, 2022. 19(1): p. 178. [CrossRef]
- Wang, C., et al., Microglia mediate forgetting via complement-dependent synaptic elimination. Science, 2020. 367(6478): p. 688-694. [CrossRef]
- Kim, J.H., et al., Gamma subunit of complement component 8 is a neuroinflammation inhibitor. Brain, 2021. 144(2): p. 528-552. [CrossRef]
- McNab, F., et al., Type I interferons in infectious disease. Nat Rev Immunol, 2015. 15(2): p. 87-103. [CrossRef]
- Minter, M.R., et al., Deletion of the type-1 interferon receptor in APPSWE/PS1DeltaE9 mice preserves cognitive function and alters glial phenotype. Acta Neuropathol Commun, 2016. 4(1): p. 72. [CrossRef]
- Roy, E.R., et al., Concerted type I interferon signaling in microglia and neural cells promotes memory impairment associated with amyloid beta plaques. Immunity, 2022. 55(5): p. 879-894 e6. [CrossRef]
- Holtzman, D.M., J. Herz, and G. Bu, Apolipoprotein E and apolipoprotein E receptors: normal biology and roles in Alzheimer disease. Cold Spring Harb Perspect Med, 2012. 2(3): p. a006312. [CrossRef]
- Liu, C.C., et al., Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol, 2013. 9(2): p. 106-18. [CrossRef]
- Yin, C., et al., ApoE attenuates unresolvable inflammation by complex formation with activated C1q. Nat Med, 2019. 25(3): p. 496-506. [CrossRef]
- Qin, Q., et al., The Specific Mechanism of TREM2 Regulation of Synaptic Clearance in Alzheimer's Disease. Front Immunol, 2022. 13: p. 845897. [CrossRef]
- Vandendriessche, C., et al., Importance of extracellular vesicle secretion at the blood-cerebrospinal fluid interface in the pathogenesis of Alzheimer's disease. Acta Neuropathol Commun, 2021. 9(1): p. 143. [CrossRef]
- Reiman, E.M., et al., Exceptionally low likelihood of Alzheimer's dementia in APOE2 homozygotes from a 5,000-person neuropathological study. Nat Commun, 2020. 11(1): p. 667. [CrossRef]
- Farrer, L.A., et al., Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA, 1997. 278(16): p. 1349-56. [CrossRef]
- Panitch, R., et al., Integrative brain transcriptome analysis links complement component 4 and HSPA2 to the APOE epsilon2 protective effect in Alzheimer disease. Mol Psychiatry, 2021. 26(10): p. 6054-6064. [CrossRef]
- Ulland, T.K., et al., TREM2 Maintains Microglial Metabolic Fitness in Alzheimer's Disease. Cell, 2017. 170(4): p. 649-663 e13. [CrossRef]
- Pottier, C., et al., TREM2 R47H variant as a risk factor for early-onset Alzheimer's disease. J Alzheimers Dis, 2013. 35(1): p. 45-9. [CrossRef]
- Guerreiro, R., et al., TREM2 variants in Alzheimer's disease. N Engl J Med, 2013. 368(2): p. 117-27. [CrossRef]
- Konishi, H. and H. Kiyama, Microglial TREM2/DAP12 Signaling: A Double-Edged Sword in Neural Diseases. Front Cell Neurosci, 2018. 12: p. 206. [CrossRef]
- Qu, W. and L. Li, Loss of TREM2 Confers Resilience to Synaptic and Cognitive Impairment in Aged Mice. J Neurosci, 2020. 40(50): p. 9552-9563. [CrossRef]
- Scott-Hewitt, N., et al., Local externalization of phosphatidylserine mediates developmental synaptic pruning by microglia. EMBO J, 2020. 39(16): p. e105380. [CrossRef]
- Fraser, D.A., K. Pisalyaput, and A.J. Tenner, C1q enhances microglial clearance of apoptotic neurons and neuronal blebs, and modulates subsequent inflammatory cytokine production. J Neurochem, 2010. 112(3): p. 733-43. [CrossRef]
- Zhang, B., et al., Integrated systems approach identifies genetic nodes and networks in late-onset Alzheimer's disease. Cell, 2013. 153(3): p. 707-20. [CrossRef]
- Readhead, B., et al., Molecular systems evaluation of oligomerogenic APP(E693Q) and fibrillogenic APP(KM670/671NL)/PSEN1(Deltaexon9) mouse models identifies shared features with human Alzheimer's brain molecular pathology. Mol Psychiatry, 2016. 21(8): p. 1099-111. [CrossRef]
- Haure-Mirande, J.V., et al., Deficiency of TYROBP, an adapter protein for TREM2 and CR3 receptors, is neuroprotective in a mouse model of early Alzheimer's pathology. Acta Neuropathol, 2017. 134(5): p. 769-788. [CrossRef]
- Haure-Mirande, J.V., et al., Integrative approach to sporadic Alzheimer's disease: deficiency of TYROBP in cerebral Abeta amyloidosis mouse normalizes clinical phenotype and complement subnetwork molecular pathology without reducing Abeta burden. Mol Psychiatry, 2019. 24(3): p. 431-446. [CrossRef]
- Audrain, M., et al., Integrative approach to sporadic Alzheimer's disease: deficiency of TYROBP in a tauopathy mouse model reduces C1q and normalizes clinical phenotype while increasing spread and state of phosphorylation of tau. Mol Psychiatry, 2019. 24(9): p. 1383-1397. [CrossRef]
- DeVos, S.L., et al., Synaptic Tau Seeding Precedes Tau Pathology in Human Alzheimer's Disease Brain. Front Neurosci, 2018. 12: p. 267. [CrossRef]
- Bejanin, A., et al., Tau pathology and neurodegeneration contribute to cognitive impairment in Alzheimer's disease. Brain, 2017. 140(12): p. 3286-3300. [CrossRef]
- Britschgi, M., et al., Deficiency of terminal complement pathway inhibitor promotes neuronal tau pathology and degeneration in mice. J Neuroinflammation, 2012. 9: p. 220. [CrossRef]
- Dejanovic, B., et al., Changes in the Synaptic Proteome in Tauopathy and Rescue of Tau-Induced Synapse Loss by C1q Antibodies. Neuron, 2018. 100(6): p. 1322-1336 e7. [CrossRef]
- Litvinchuk, A., et al., Complement C3aR Inactivation Attenuates Tau Pathology and Reverses an Immune Network Deregulated in Tauopathy Models and Alzheimer's Disease. Neuron, 2018. 100(6): p. 1337-1353 e5. [CrossRef]
- Bonham, L.W., et al., The relationship between complement factor C3, APOE epsilon4, amyloid and tau in Alzheimer's disease. Acta Neuropathol Commun, 2016. 4(1): p. 65. [CrossRef]
- Shi, Y., et al., ApoE4 markedly exacerbates tau-mediated neurodegeneration in a mouse model of tauopathy. Nature, 2017. 549(7673): p. 523-527. [CrossRef]
- Dejanovic, B., et al., Complement C1q-dependent excitatory and inhibitory synapse elimination by astrocytes and microglia in Alzheimer's disease mouse models. Nat Aging, 2022. 2(9): p. 837-850. [CrossRef]
Figure 1.
The complement cascade. Complement can be activated by three separate pathways: the classical, lectin and alternative pathways. Cleavage of C3 is central to complement activation and its downstream effects lead to lysis and inflammatory signaling through the formation of the membrane attack complex (MAC). The classical pathway is activated upon binding of C1q to antigen-antibody complexes, consequently activating the two serine proteases C1r and C1s to form a complex with C1q known as the C1 complex. The C1 complex causes the cleavage of C4 and then C2, whose fragments combine to form C3 convertase (C4bC2a). The lectin pathway is initiated by binding carbohydrates like mannose-binding protein (MBP) and ficolins on the surface of pathogens which activate two proteases, MASP1 and MASP2 (mannose-binding serine proteases 1 and 2) causing cleavage of C4 and then C2, whose fragments combine to form the same C3 convertase as in the classical pathway. The alternative pathway is always “on” at low levels in blood and is further activated by pathogens including viruses, fungi, bacteria, LPS, etc., leading to the spontaneous hydrolysis of C3 and amplification of C3b which binds Factor B and is cleaved by Factor D to form a different C3 convertase (C3bBb). Both C3 convertases cleave C3 into C3a and C3b. C3b can combine with the two different C3 convertases to form C5 convertase (C4bC2aC3b in the classical and lectin pathways; C3bBbC3b in the alternative pathway) which cleaves C5 into C5a and C5b. C3a and C5a are anaphylatoxins that bind their respective receptors, C3aR and C5aR, to recruit immune cells to sites of injury or infection which then secrete pro-inflammatory cytokines. [Note: There are two forms of C5aR. C5aR1 is pro-inflammatory while C5aR2 is thought to be anti-inflammatory.] Complement component C3b and its inactivated product, iC3b, opsonize or tag pathogens or immune complexes or weak synapses for phagocytic removal by microglia which bear their receptor, CR3. Complement component C5b binds C6, C7, C8 and finally multiple copies of C9 to form a channel (C5b-9 or MAC) in the cell membrane of a pathogen or cell which induces lysis. Figure created with BioRender.com.
Figure 1.
The complement cascade. Complement can be activated by three separate pathways: the classical, lectin and alternative pathways. Cleavage of C3 is central to complement activation and its downstream effects lead to lysis and inflammatory signaling through the formation of the membrane attack complex (MAC). The classical pathway is activated upon binding of C1q to antigen-antibody complexes, consequently activating the two serine proteases C1r and C1s to form a complex with C1q known as the C1 complex. The C1 complex causes the cleavage of C4 and then C2, whose fragments combine to form C3 convertase (C4bC2a). The lectin pathway is initiated by binding carbohydrates like mannose-binding protein (MBP) and ficolins on the surface of pathogens which activate two proteases, MASP1 and MASP2 (mannose-binding serine proteases 1 and 2) causing cleavage of C4 and then C2, whose fragments combine to form the same C3 convertase as in the classical pathway. The alternative pathway is always “on” at low levels in blood and is further activated by pathogens including viruses, fungi, bacteria, LPS, etc., leading to the spontaneous hydrolysis of C3 and amplification of C3b which binds Factor B and is cleaved by Factor D to form a different C3 convertase (C3bBb). Both C3 convertases cleave C3 into C3a and C3b. C3b can combine with the two different C3 convertases to form C5 convertase (C4bC2aC3b in the classical and lectin pathways; C3bBbC3b in the alternative pathway) which cleaves C5 into C5a and C5b. C3a and C5a are anaphylatoxins that bind their respective receptors, C3aR and C5aR, to recruit immune cells to sites of injury or infection which then secrete pro-inflammatory cytokines. [Note: There are two forms of C5aR. C5aR1 is pro-inflammatory while C5aR2 is thought to be anti-inflammatory.] Complement component C3b and its inactivated product, iC3b, opsonize or tag pathogens or immune complexes or weak synapses for phagocytic removal by microglia which bear their receptor, CR3. Complement component C5b binds C6, C7, C8 and finally multiple copies of C9 to form a channel (C5b-9 or MAC) in the cell membrane of a pathogen or cell which induces lysis. Figure created with BioRender.com.
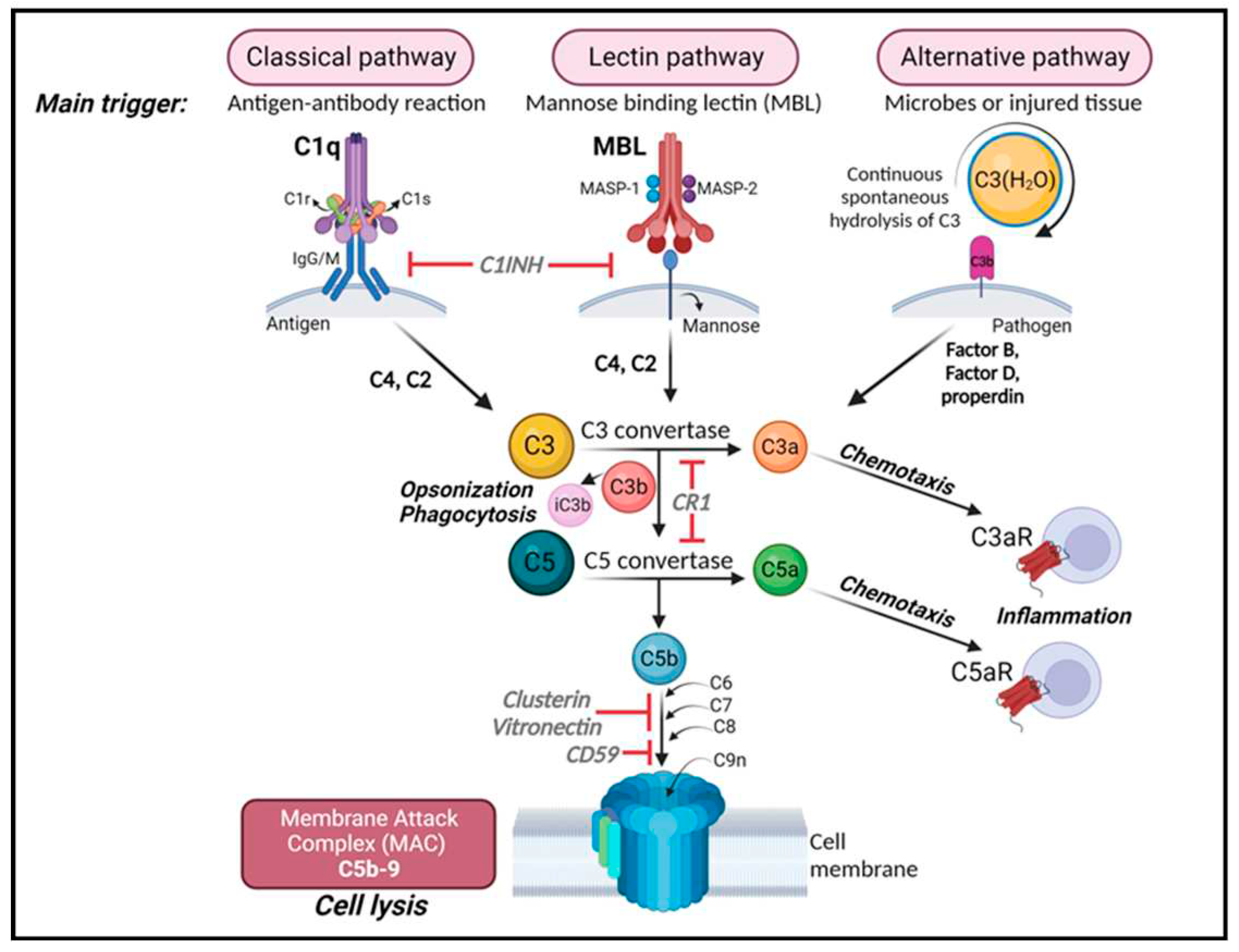
Figure 2.
The role of the complement system in synapse elimination. The complement system serves a crucial role in normal brain development, aging and AD progression by regulating synaptic pruning and elimination, as well as neuronal migration. The activation of the classical pathway leads to C1q expression causing cleavage of C4 and C2 and resulting in expression of C3 and iC3b. C3 and iC3b tag weak or unhealthy synapses representing an “eat me” signal. Microglia, which are responsible for maintaining homeostasis and surveilling the function of synapses, carry CR3 receptors (red) that recognize the tagged synapses and proceed with eliminating them via phagocytosis (synaptic engulfment). In aging and AD this process has been linked to neurodegeneration. Figure created with BioRender.com.
Figure 2.
The role of the complement system in synapse elimination. The complement system serves a crucial role in normal brain development, aging and AD progression by regulating synaptic pruning and elimination, as well as neuronal migration. The activation of the classical pathway leads to C1q expression causing cleavage of C4 and C2 and resulting in expression of C3 and iC3b. C3 and iC3b tag weak or unhealthy synapses representing an “eat me” signal. Microglia, which are responsible for maintaining homeostasis and surveilling the function of synapses, carry CR3 receptors (red) that recognize the tagged synapses and proceed with eliminating them via phagocytosis (synaptic engulfment). In aging and AD this process has been linked to neurodegeneration. Figure created with BioRender.com.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



