
Submitted:
20 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
Weight increase after tonsillectomy has been reported in different studies and systematic reviews. However, the odds of a child being overweight or obese after tonsillectomy were no other than before surgery, according to a few studies. This systematic review aimed to analyze the impact of adenotonsillectomy (TA) on weight gain and to identify subgroups of children and adolescents at risk of obtaining weight gain. A systematic search was performed, including studies published in the last ten years. The PICO framework was used in the selection process, and evidence was as-sessed using the GRADE system. A total of 26 studies were included, and moderate-high level quality ones showed that children who underwent TA could present an increase in BMI z-score. However, this weight gain was significant in individuals younger than six years old and was considered a catch-up growth in subjects who were underweight at baseline. In contrast, in nor-mal-weight or overweight individuals, TA did not lead to overweight per se. At the same time, diet changes and overfeeding seem to not have a leading role in weight gain. In conclusion, TA may not be an independent risk factor for unfavorable weight gain in children; however, individuals who were underweight pre-operatively or younger than six years reported more weight gain after TA than expected.
Keywords:
weight gain
; overweight
; tonsillectomy
1. Introduction
In the last 20 years, the prevalence of overweight and obesity among children and adolescents has increased rapidly. The principal cause is an imbalance between calorie intake and physical activity, with socioenvironmental factors playing a crucial role [1].
Tonsillectomy is a standard surgical procedure in the pediatric age, and it is indicated for treating obstructive sleep apnea (OSA) and chronic throat infections. Adenoidectomy is done for nasal passage obstruction, OSA, recurrent otitis media, and rhinosinusitis. Obesity has been recognized as a risk factor for OSA [2], and children with obesity have more tonsillectomy/adenoidectomy procedures compared with peers [3,4]. Although tonsillectomy with or without adenoidectomy is relatively safe surgery, postoperative complications have been reported in multiple studies. Among these, post-tonsillectomy hemorrhage is the most common, followed by possible infections, taste disturbances, breathing problems, and dehydration [5].
The connection between tonsillectomy and weight gain and growth has been controversial and discussed for decades [6,7]. Weight increase after tonsillectomy has been reported in different studies and the most recent systematic reviews [8,9], but the odds of a child being overweight or obese after tonsillectomy in the next 12-18 months were not different than they were before surgery according to a few studies [10,11]. Other study designs, methods, baseline weight and age of the subjects, additional indications for tonsillectomy, and outcomes analyzed likely explain the heterogeneity in the literature results.
The mechanisms underlying weight gain after adenotonsillectomy (TA) surgery are still unknown [12]: i) children with enlarged adenoids and/or tonsils could lead more frequent infections, swallowing problems, dysphagia or odynophagia, and these disorders can lead to decreased calorie intake; when the tonsils are removed, children can consume a more significant amount of calories [13]; ii) in children with OSA, intermittent upper airway obstruction during sleep has been thought to increase the work of breathing, and therefore increase energy expenditure at night, and probably after TA this energy expenditure decreases [9]; iii) in addition, reduced episodes of OSA after TA, could lead to hormonal dysregulation, increasing levels of insulin-like growth factor-1 and insulin growth factor binding protein -3 [14].
The aims of this systematic review are:
1) to provide an up-to-date summary of the available evidence on the impact of TA on weight gain and eventually increased prevalence of overweight and obesity;
2) to identify subgroups of children and adolescents at risk of weight gain;
3) to elucidate mechanisms beyond increased caloric intake that underlie weight gain.
2. Materials and Methods
2.1. Search strategy
We searched electronic databases (Pubmed, EMBASE, The Cochrane Library, Web of Science, Clinicaltrial.gov, International Clinical Trials Registry Platform) for studies published between January 1, 2013, and August 1, 2023. Search terms, or “MESH” (MEdical Subject Headings) for this systematic review included different combinations: “weight gain” or “overweight,” or “obesity” or “obese,” or “BMI” or “weight” or “unhealthy weight” or “fat” AND “tonsillectomy” or “adenoidectomy” or “adenotonsillectomy.”
We also screened the reference list of eligible studies to avoid missing any relevant studies.
2.2. Criteria for study selection
We conducted a systematic search of the literature according to the PICOS model (Population, Intervention, Comparison, Results, Study design):
| Population | Children and adolescents (1-18 years) who had undergone tonsillectomy |
| Intervention | Tonsillectomy with or without adenoidectomy |
| Comparison | Healthy control subjects |
| Outcomes | -Preoperative and postoperative (up to 24 months after) growth (weight, height, BMI (body mass index), and relative percentiles for age, body composition, metabolic and hormonal changes - and/or comparison with a control group |
| Study design | Randomized clinical trials (RCTs), observational studies (cohort, case-control, cross-sectional studies), exploratory studies, mix of qualitative and quantitative studies |
Inclusion criteria were: i) study population: children and adolescents (aged 1–18 years) who had undergone tonsillectomy with or without adenoidectomy; ii) study type: observational studies (cohort, case-control, cross-sectional studies), exploratory studies, a mix of qualitative and quantitative studies; iii) review articles were excluded, but their reference lists were screened to identify potentially eligible studies; iv) only published full papers were included, whereas abstract only were not included; v) data on weight gain: weight, height, BMI and relative percentiles, metabolic and hormonal changes, before and after tonsillectomy; vi) publication date: last ten years (2013-2023) to include studies after the last systematic review reported in literature [9].
Exclusion criteria: i) data available only for adults ≥18 years or subjects with syndromes (Down, Prader Willi, Rohadnet etc.; ii) animal data; iii) case reports; studies with < 10 patients who undergone tonsillectomy; iv) full paper not available; v) study not yet published; vi) studies on tonsillectomy not reporting weight variation within 24 months; vii) languages other than English were not “a priori” exclusion criteria.
2.3. Data extraction and management
Using the search strategy, two independent investigators (AN, LO) screened for inclusion in the identified studies' titles and abstracts. Any discrepancies were resolved by consensus or consultation with a third investigator (RF). After abstract selection, four investigators conducted the complete paper analysis (EMA, LL, LF, LO).
The following characteristics were evaluated for each study in the full paper: i) reference details: authorship(s); published or unpublished; year of publication; period in which the study was conducted; other relevant cited papers; ii) study characteristics: study design, topic, treatment period, follow up duration, region; iii) population characteristics: number of participants who undergone tonsillectomy with or without adenoidectomy, number with OSA, age and demographic data, baseline weight, BMI, fat, waist circumference and other related parameters; comparator characteristics; iv) methodology: assessment of growth measurements, metabolic and hormone changes, caloric intake, physical exercise; v) main results: growth pattern, body composition parameters, factors influencing post-operative growth.
2.4. Assessment of the certainty of the evidence
We used the GRADE approach (Grading of Recommendations Assessment, Development, and Evaluation) to rank the quality of evidence (www.gradeworkinggroup.org) for the included studies. Two authors (EM and RF) independently assessed the certainty of the evidence for each of the outcomes, and MM resolved discrepancies. In the case of risk bias in the study design, imprecision of estimates, inconsistency across studies, indirectness of the evidence, and publication bias, the recommended option of decreasing the level of certainty by one or two levels according to the GRADE guidelines was applied [15]. The GRADE approach results in an assessment of the certainty of a body of evidence and allocation to one of four grades:
| High: | Further research is very unlikely to change confidence in the estimate of the effect |
| Moderate | Further research is likely to have an important impact on confidence in the estimate of the effect and may change the estimate |
| Low | Further research is very likely to have an important impact |
| Very low | Any estimate of effect is very uncertain |
3. Results
After duplicates were removed, 278 studies were identified following the literature review. After reviewing titles and abstracts, 229 additional records were excluded: 39 review articles, two guidelines, nine studies including only participants with peculiar syndromes (Prader Willi, Down syndrome), 168 studies reporting outcomes different from those of interest, eight studies not available as full paper, three studies with publication period before 2013, 1 study for the number of patients less than 10.
A total of 49 full-text manuscripts were assessed for eligibility: after full-text examination, 23 studies were excluded, and a final number of 26 studies were included in this systematic review. The PRISMA flow diagram (Figure 1) summarizes the study screening process. A summary of the studies included in this systematic review and the grading of evidence is reported in Table 1 [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40].
Studies with a sample size of < 50 patients or with short follow-up (< 6 months) have been considered at risk of bias in the study design and/or at risk of imprecision for estimating the analyzed outcome, and therefore were assigned a low level of evidence. In the same way, other studies, retrospective in design or prospective without a control group, were evaluated in the entire design considering sample size, follow-up range (a wide range makes comparisons less reliable), and outcome results. In some cases, the level of certainty was considered “low”. Below we report the results on growth outcomes based on the 14 studies which were graded as of moderate-high quality level (Table 2A). In none of these studies were body composition or hormonal changes evaluated. Therefore, we reported available evidence of low-quality grades.
3.1. Changes in growth pattern after tonsillectomy
Among growth pattern outcomes, all the studies included in this review evaluated BMI z-score pre- and post-tonsillectomy (T) or TA; 5 studies analyzed the impact on height and/or height z-score, one on waist circumference [40], and in 2 studies change in the percentage of subjects with overweight/obesity was reported (Table 2A). Below, we write a summary of the evidence.
BMI z-score
The baseline BMI z-score was reported as normal in three studies [17,37,40], while in the other 11, the population was classified according to percentiles in two or more among these classes: underweight (Uw), normal weight (Nw), overweight (Ow) and obese (Ob); for these studies the postoperative data were analyzed accordingly [16,22,23,24,25,27,32,33,35,36,39]. Two studies analyzed data from the same cohort of a RCT named Childhood Adenotonsillectomy trial (CHAT) [35,36].
BMI z-score did not change significantly compared to the control group in the two prospective studies in which participants were normal weight at baseline [17,37], in 1 RCT [40], and the 2 RCTs referred to the re-analysis of data of the CHAT cohort [35,36] (Table 2A). In one large population-based cohort study, shortly after TA, the BMI z-score increased significantly in the operation group (0.41±0.02) vs the control group (0.18±0.01; p<0.001) [23]. In 4 studies that included subjects Uw, Nw, Ow, and Ob [22,24,27,32], BMI z-score resulted increased considering all the cohorts, but determinant to this result was the data of the Uw group that was not the most prevalent (3,5%, 9,2%, 14,9%, 1,3% respectively). Three studies, mainly patients Ow or Ob at baseline, reported an increased BMI z-score after TA [16,25,33]. A recent RCT in children with OSA concluded that there is an increase in BMI z-score between 0 and 12 months but not from 12-24 months, and the mean BMI z-score included catch-up of Uw subjects, while only 8 of the TA group had undesirable weight gain [39].
Given the differences in ethnic origin, growth chart used for percentiles, and follow-up timing recorded in the various papers, a meta-analysis using BMI z-score as the outcome was not conducted, while we performed an analysis to search for determinants of BMI z-score.
Determinants of BMI z-score after TA
Baseline BMI z-score: a correlation between baseline BMI z-score and BMI z-score after TA was found in 7 studies. Reduced BMI z-score at baseline (Uw population) was correlated to an increase in BMI z-score after TA in 5 studies [22,24,27,32,35], but not in the other two that vice-versa reported increased BMI z-score after TA in Ow-Ob subjects at baseline [25,33];
Age: younger age (age < 4-6 years) was correlated to an increase in BMI z-score after TA in 3 studies [16,24,32] but not in the other two [22,33]; Weight gain duration after TA: among the studies that reported an increase in BMI z-score, a rise between 0 and 12 months but not from 12-24 months was reported in one RCT study [39]. The other two studies reported an increase in BMI z-score up to 24 months [22,33]. Most weight gain has been reported in the first six months after TA and only plateau one year after surgery in another study [32].
Surgery indication: obstruction or OSA as an indication for TA, compared to recurrent upper airway infections, was correlated to an increase in BMI z-score after TA in one study [24] but not in the other three that evaluated this risk factor [16,22,33];
Gender: no significant difference was noted in BMI z-score between boys and girls in either the aggregate or sub-group analysis in the studies that analyzed this parameter [16,22,32,33,35];
Ethnicity: African-American children were noted to have significantly more weight gain increase than white or Hispanic and Asian children in one study [32], but this data was not confirmed in the other two studies [16,33];
Caloric intake: Increased caloric intake after TA was reported only in one study, classified as a low level of evidence [13], and none investigated physical activity levels. HT z-score increased significantly, more than 12 months after TA, compared to the control group in three studies [23,24,33] but not in the other two after 18-24 months [32,39] (Table 2A).
Waist circumference
Waist circumference was evaluated only in one study and did not change significantly after TA during the follow-up period of about ten months [40].
Percentage of overweight/obesity
In most of the studies, an increase in the prevalence of Ow or Ob was not reported, as the increase in BMI z-score was minimal or absent during the follow-up period. In one study, children with Ow/Ob decreased in BMI z-score [22], whereas, in another, the Ow group had a 27% (6/22) shift to Ob [27] (Table 2A).
3.2. Changes in body composition after tonsillectomy
Only one study was selected for this systematic review and classified as low evidence. It showed a significant increase in body muscle mass after TA [18]. No study reported data on fat mass.
3.3. Hormonal changes influencing post-operative growth after tonsillectomy.
Only three studies classified as low level of evidence reported data on hormonal changes, and below, we report a summary of the results [20,29,30] (Table 2B).
IGF-1: the three studies measured IGF-1 levels pre-op and post-operation. IGF-1 levels increased significantly post-op vs pre-op (p < 0.001) in two studies [29,30], whereas in the other study, only the obstructive group showed an increase in IGF-1 (p < 0.0001), but not the infection group (p = 0.0883) [20];
IGF-BP3: IGF-BP3 levels at 1-year post-op were significantly increased vs pre-op (p = 0.001) in the only study that measured this hormone [29];
Ghrelin: ghrelin levels increased significantly post-op vs pre-op (p < 0.001) as reported in one study [30] and decreased 1-year post-op as showed in another study (p < 0.001) [29];
Leptin: pre-op leptin levels were significantly higher in patients than in controls (p < 0.001) and increased significantly post-op (p = 0.036) as reported in only one study [29].

Table 2.
A: Summary of studies with moderate-high level quality of evidence.
| Reference | Initial WT status | Number / Design | Intervention (f/up) | WT | HT | BMIz | Risk factors for WT/BMI change | Level of evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|
| Smith DF . et al. [16] | Nw-Ow | 115/R | TA (6m) |
↑ | < age (<6y) No OSA indication |
M | ||
| Huang YS et al. [17] | Nw | 88/P | TA (36m) | = | M | |||
| Beauchamp MT et al. [22] | Uw, Nw, Ow, Ob | 1751/R | TA or T (24m) | ↑in Uw/Nw ↓ in Ob-Ow |
Uw No age, no surgery indication |
M | ||
| Ha EK et al. [23] | Uw, Nw, Ow, Ob | 3172/P | TA (66-71) | ↑ | ↑ HTz | ↑ | M | |
| Han SC et al. [24] | Nw, Ow, Ob | 206/R | TA (12m) | ↑ WTz | ↑HTz | ↑ | <age < BMI pre > adenoid grade |
M |
| Kim JY et al. [25] | Nw, Ow, Ob | 170/P | TA (15m) | ↑ (and > Ow) | TA | M | ||
| Hsu WC et al. [27] | Uw, Nw, Ow, Ob | 161/P | TA (6m) | ↑ | Uw | M | ||
| Czechowicz et al. [32] | Uw, Nw, Ow, Ob | 815/R | TA (18m) | ↑ WTz | =HTz | ↑ | <age (<4y) < BMI pre African-American |
M |
| Lewis TL et al. [33] | Nw, Ow, Ob | 154/R | TA (24m) | ↑ | ↑ | ↑ | No age Ob and Nw pre No surgery indication |
M |
| Jensen AM et al. [35] | Uw, Nw, Ow, Ob | 396/RCT | TA (7m) | ↑ | = | Uw at baseline | H | |
| Kirkham et al. [36] | Uw, Nw, Ow, Ob | 396/RCT | TA (7m) |
= | = | Uw at baseline | H | |
| AlAbdullah ZA et al. [38] | Nw | 53/P | T (12m) | = | M | |||
| Kevat A et al. [39] | Uw, Nw, Ow, Ob | 126/RCT | TA (24m) | ↑ | =HTz | ↑ | H | |
| Au CT et al. [40] | Nw | 71/RCT | T-TA (10m) | ↑ | = | H |
Uw: underweight, Nw: normal weight, Ow: overweight, Ob: obese, R: retrospective, P: prospective, RCT: randomized controlled trial, WT: weight, WTz: weight z-score, HT: height, HTz: height z-score, BMI: body mass index, BMIz: BMI z—score, OSA: obstructive sleep apnea, T: tonsillectomy, TA: adenotonsillectomy, M: moderate, H: high. ↓: reduced; ↑: increased; = : no variation.
Table 2.
B: Summary of studies with low quality of evidence.
| Reference | Intervention (f/up) | WT | HT | BMIz | relBMI% | Body composition | Hormonal change | Risk factors for WT/BMI change | Level of evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|---|
| Koycu A et al. [18] | TA or A (6m) Nw |
= | = | ↑ relBMI% ↑ BMIz in TA |
↑ body muscle mass | TA vs T | L | ||
| Inja RR et al. [19] | TA or A (3m) | ↑ | L | ||||||
| Elnashar I et al. [20] | T (3m) | ↑ IGF-1 in obstructive group, not in infective | L | ||||||
| Costa Pinto R et al. [21] | TA (4m) | ↑ | ↑ | L | |||||
| Voora RS et al. [26] | T or TA (6m) | ↑ | ↑BMI pre-op Younger Male Obstruction as indication |
||||||
| Koren D et al. [28] | TA (8m)- OSA | ↑ | L | ||||||
| Karalok ZS et al. [29] | T or TA (12m) | ↑ WTz | ↑ WTz | = | Pre-OP. ↑leptin = GHrelin, IGF.1 +1y post-op: ↑IGF-1, IGFBP3, leptin and ↓ GHrelin |
L | |||
| Moghaddam YJ et al. [30] | TA (12m)-OSA | ↑ | ↑ | ↑ | Post-op: ↑IGF-1, leptin, and Ghrelin |
L | |||
| S YB et al. [31] | TA (6m) | = | L | ||||||
| Katz ES et al. [34] | TA (7m)-OSA Uw, Nw, Ow, Ob |
↑ WTz | = | ↑ | No race and gender | L | |||
| Nachalon Y et al. [13] | TA (5m)-OSA | ↑/WTz | ↑ | ↑ | Increased caloric intake | L | |||
| Al Abdulla A et al. [37] | TA (6m) | ↑ | L |
Uw: underweight, Nw: normal weight, Ow: overweight, Ob: obese, WT: weight, WTz: weight z-score, HT: height, HTz: height z-score, BMI: body mass index, BMIz: BMI z—score, relBMI%: relative BMI percentage, IGF-1: insulin like growth factor-1, pre-OP: pre-operation, OSA: obstructive sleep apnea, T: tonsillectomy, TA: adenotonsillectomy, M: moderate, H: high. ↓: reduced; ↑: increased; = : no variation.
4. Discussion
This systematic review selected 26 studies, considering 14 with moderately high-quality evidence. This allowed us to conclude that children who underwent TA could present an increase in BMI z-score. However, this weight gain is considered a catch-up growth in subjects that are Uw at baseline, while normal weight or over-weight TA did not lead to overweight per se. This data must be contextualized in an obesogenic environment where overweight subjects in the short term could gain more weight percentiles if they do not change their lifestyle [16,25,33,41,42], and studies with randomized controlled design consented to the separation of treatment effect from natural history [35,36,39,40].
The most recent systematic review on TA as a risk factor for childhood obesity was published in 2016 by Van M et al. and included six studies in children with OSA [9]; among these studies, four showed a significant weight gain after TA and the others did not. Most of the included studies were observational and involved relatively few patients. One RCT, conducted by Katz et al. obtained in that review the greatest level of evidence [34], but in 2021 it was revised in the statistical analysis leading to the opposite conclusion [35,36]. At that time, Van M et al. concluded an association between TA and weight gain in patients with OSA in the short term [9]. This conclusion was the same reported in 2011 in a previous systematic review by Jeyakumar et al. who included nine studies and suggested a correlation between TA and weight gain in normal weight and overweight children, with a mean BMI increase of 7% [8]. They suggested large RCTs not available then to answer some of their questions [8].
In our systematic review, we attributed the highest level of evidence to the RCTs, even if GRADE classification is outcome specific and RCTs don't need to have a high quality of evidence for the particular outcome we decided to analyze; however, the RCTs that we selected were well designed to answer to our questions, and according to us, they add quality to the results of this systematic review. Notably, the children in the no-intervention group in these trials are not healthy ones but rather those who have OSA, a condition that appears to restrict their growth [9]. One RCT, conducted by Kevat et al., reported increased BMI z-score in the 12 months after TA, but not after, reporting a catch-up growth in Uw subjects, while undesirable weight gain was experienced only by 8 participants (17% of the TA group) [39]. Another RCT showed that the BMI z-score remained similar at baseline and follow-up for both groups and waist circumference did not increase in the TA group [40].
In two studies, Jensen et al. and Kirkham et al. presented a reanalysis of a multicenter randomized controlled trial (CHAT) comparing watchful waiting to early TA in 464 pre-pubertal OSA children between 2008 and 2011, with a 7-month follow-up [35,36]. This trial did not demonstrate differences in unwanted weight gain seven months after TA versus watchful waiting. Children in both arms experienced undesirable weight gain over seven months but did so similarly in the two arms (45% adenotonsillectomy vs 41% watchful waiting; p=0.400) [35,36]. A first analysis performed by Katz et al. in 2014 showed more significant weight increases seven months after TA in all weight categories, with children who failed to thrive that TA normalized weight but with increased risk for obesity in overweight children [34]. Years later, Jensen et al. and Kirkham et al. repeated the statistical analysis, and after excluding the thinnest children based on BMI <20th percentile, regression models with a sensitivity analysis that excluded children who were underweight at baseline reported no longer a significant effect of TA on BMI z-score [35,36].
In our systematic review, there was heterogeneity in the outcomes of the ten prospective or retrospective studies that we rated as having moderate quality of evidence, primarily due to variations in the population covered and in the study design. Firstly, there were differences in the study population enrolled in the studies regarding BMI percentile before surgery. The percentage of patients categorized by BMI percentile as Uw was not high (1,3-14,9%) in the studies that reported this data [22,24,27,32]; however, after TA, they showed a catch-up growth that influenced the mean BMI z-score of the whole cohort (as demonstrated by correlation analysis). We emphasize the fact that 4.5% of Uw in the CHAT RCT, if not excluded in the regression model, were able to show or not a significant effect of TA on BMI z-score [35]. Secondly, considering the study design, the sample size was fundamental in these studies to determine whether the BMI z-score comparison was statistically significant. In the study of Ha EK et al.[23], the BMI z-score after TA of 0.41±0.02 compared to 0.18±0.01 in the control group was significant in this large Korean population study on 3172 children with TA and 31,663 controls, but this could have had no clinical impact at the individual level [23]; vice-versa other studies included in this review presented sample sizes in the low hundreds in total and were then divided among the various weight categories, therefore the study could be underpowered for some conclusions and results should be viewed with caution [25]. The length of follow-up and the national growth charts used for BMI percentiles in various nations are two additional differences that may impact direct comparisons of study results.
A second outcome of this systematic review was identifying subgroups of children and adolescents at risk of weight gain. Not all the studies with moderately high levels of evidence were concordant, but from different studies emerged that those who were underweight at the baseline [22,24,27,32,35,36] or younger than 4-6 years [16,24,32] gained more weight after TA. Weight gain in children with failure-to-thrive after TA has been previously reported [43], while age at risk is important to be considered for clinical practice, as greater preoperative counseling, closer follow-up, and it might be required for these young patients receiving TA to take extra measures to manage their obesity. Otolaryngologists and primary care providers should counsel families that increased weight gain could be possible in the first 6-12 months after TA, particularly in those under 6 years old [32].
As a third outcome, we aimed to elucidate mechanisms beyond increased caloric intake that underlie weight gain. This was not possible due to the absence of caloric intake and physical activity reports before and after TA, in most of the studies included in this review. Only one study that we included, classified as low-quality level of evidence, explored this outcome [13]. Dietary and physical records could be helpful in determining whether weight gain is caused by surgery or by parents who support specific recovery practices (overfeeding and restricting physical activity), and they could determine whether there is more to the story (i.e., hormonal, and metabolic changes), which could be intriguing for future research directions.
Previous studies, not included in this review because of publication date before 2013 and/or not reporting weight variation within 24 months, showed conflicting results pre- and post-TA. In these studies, Authors used diet records, even if they are not a precise measurement of food intake, they are a practical and frequently used method of assessing caloric intake, type of food eaten, and source of calories, and they have been shown to provide reliable assessments of food intake in children [12].
A few studies compared children whose tonsils were removed and those who retained their tonsils: TA was not associated with higher levels of caloric intake and weight gain according to diet records reported in one of these studies [6], or in others reported in prepubertal children significant weight gain associated with decreased mean caloric expenditure [44]. In the latter study, the composition of the diet was similar in both groups, with no significant differences in the percentage of calories derived from protein, carbohydrates, or fat [44].
A few studies compared caloric intake pre- and post-TA in prepubertal children and found increased caloric intake after TA. Gkouskou et al. found that pre-operatively, the total calories received by children with tonsillar hypertrophy did not differ significantly compared to the control group. Six months after TA, they increased the calories they were consuming daily, taking even more significant amounts of this food in relation to the control group, gaining weight significantly but not leading to overweight (catch-up growth) [45]. Selimoglu et al. found that pre-operatively, healthy children had higher mean energy intake, weight, and height z-scores than children with adenotonsillar hypertrophy, and mean energy intake, weight, and height significantly increased after TA, again not leading to overweight [46]. Nachalon et al., in the study that we included in this review, reported increased caloric intake, weight, and height z-scores (not leading to overweight) after TA, as assessed by the Short Food Frequency Questionnaire (SFFQ), before and after TA, without considering a control group [13].
About diet composition reported in these studies, Gkouskou et al. found that percentages of calories received through the consumption of sugar products, soft drinks, and edible fats were greater in children who had TA, compared to the control group, whereas total calories received from other types of foods (meat, vegetables or legumes) did not differ between children that had TA, and the control group [45]. Authors interpreted these differences as due to parents’ recovery practices: they detected a possible inadequate caloric intake and so they provided the rest of the calories in the form of soft drinks and candies, as an easier and more pleasant form of food to consume [45]. Selimoglu et al. analyzed protein intake and it was not statistically different in healthy children compared to children with adenotonsillar hypertrophy before and after TA. Nachalon et al. reported a rise of 2% in protein and a decline of 4.49% in fat consumption. Although these changes were found to be significant, their actual effect on growth patterns was not clear [13].
All these data suggest an increased caloric intake in children after TA as a possible mechanism that underlies catch-up weight gain, but data on diet composition in children after TA are conflicting, and dietary interviews in the first few months after TA could probably elucidate this aspect.
The main strengths of this review are the inclusion of all subjects who underwent tonsillectomy (not only for OSA) and therefore, but our data is also transferable to the general population; a significant period of observation (10 years); the application of the PICOS model for studies’ selection and the GRADE system for assessment of evidence; the presence of RCTs on the topic. Limitations are the heterogeneity of the analyzed studies reported above regarding the population analyzed and study design.
5. Conclusions
Our findings suggest that TA may not be an independent risk factor for unfavorable weight gain in children undergoing TA. RCT studies support this evidence by distinguishing the effect of TA from natural history in an obesogenic context. However, children who were Uw pre-operatively or younger than six years are reported as gaining more weight after TA than expected. Therefore, otolaryngologists and primary care providers should counsel families that increased weight gain could occur in the first 6-12 months after TA, particularly in those under six.
This systematic review highlights the need for further studies, including caloric intake reports, to understand better the mechanisms underlying weight gain in these categories of patients.
Author Contributions
RF: EM, MM conceived the study. RF, EM and PB made a substantial contribution to the design of this literature review. NA and LO screened abstracts. EMA, LL, LF and LO conducted the full paper analysis. EM and RF independently assessed the certainty of the evidence for each of the outcomes. MM resolved discrepancies. RF, EM, and MM wrote the manuscript. EMA and CM revised the manuscript. All the authors approved the final version of the manuscript.
Funding
The authors received no specific funding for this work.
Informed Consent Statement
For this type of study, formal consent is not required.
Data Availability Statement
All databases generated for this study are included in the article.
Conflicts of Interest
The authors have no financial or non-financial conflicts of interest to declare.
Human and Animal Rights Statement
This article does not contain any studies with human participants performed by any of the authors.
References
- Maffeis, C.; Olivieri, F.; Valerio, G.; Verduci, E.; Licenziati, M. R.; Calcaterra, V.; Pelizzo, G.; Salerno, M.; Staiano, A.; Bernasconi, S.; Buganza, R.; Crinò, A.; Corciulo, N.; Corica, D.; Destro, F.; Di Bonito, P.; Di Pietro, M.; Di Sessa, A.; deSanctis, L.; Faienza, M. F.; Filannino, G.; Fintini, D.; Fornari, E.; Franceschi, R.; Franco, F.; Franzese, A.; Giusti, L. F.; Grugni, G.; Iafusco, D.; Iughetti, L.; Lera, R.; Limauro, R.; Maguolo, A.; Mancioppi, V.; Manco, M.; Del Giudice, E. M.; Morandi, A.; Moro, B.; Mozzillo, E.; Rabbone, I.; Peverelli, P.; Predieri, B.; Purromuto, S.; Stagi, S.; Street, M. E.; Tanas, R.; Tornese, G.; Umano, G. R.; Wasniewska, M. The Treatment of Obesity in Children and Adolescents: Consensus Position Statement of the Italian Society of Pediatric Endocrinology and Diabetology, Italian Society of Pediatrics and Italian Society of Pediatric Surgery. Ital J Pediatr 2023, 49 (1), 69. [CrossRef]
- Frye, S. S.; Fernandez-Mendoza, J.; Calhoun, S. L.; Gaines, J.; Vgontzas, A. N.; Liao, D.; Bixler, E. O. Childhood Obesity, Weight Loss and Developmental Trajectories Predict the Persistence and Remission of Childhood Sleep-disordered Breathing. Pediatric Obesity 2019, 14 (1), e12461. [CrossRef]
- Paul, M. E.; Wallace, J. G.; Coakley, B. A. An Assessment of the Relationship Between BMI and Children Undergoing Surgical Procedures: A Retrospective Study. Childhood Obesity 2023, 19 (4), 249–257. [CrossRef]
- Ng, H.; Wong, E.; Curotta, J.; Trapani, S.; Cheng, A. T. Tertiary Hospital Retrospective Observational Audit of Tonsillectomy. International Journal of Pediatric Otorhinolaryngology 2019, 121, 20–25. [CrossRef]
- Nguyen, B. K.; Quraishi, H. A. Tonsillectomy and Adenoidectomy - Pediatric Clinics of North America. Pediatric Clinics of North America 2022, 69 (2), 247–259. [CrossRef]
- Roche, A.F. The Influence of Tonsillectomy on Growth and Caloric Intake. J Pediatr 1964, 65, 360-367. [CrossRef]
- Bolling, C.F. 50 Years Ago in The Journal of Pediatrics. The influence of tonsillectomy on growth and caloric intake. The Journal of Pediatrics 2014, 165, 496. [CrossRef]
- Jeyakumar, A.; Fettman, N.; Armbrecht, E. S.; Mitchell, R. A Systematic Review of Adenotonsillectomy as a Risk Factor for Childhood Obesity. Otolaryngol.--head neck surg. 2011, 144 (2), 154–158. [CrossRef]
- Van, M.; Khan, I.; Hussain, S. S. M. Short-Term Weight Gain after Adenotonsillectomy in Children with Obstructive Sleep Apnoea: Systematic Review. J. Laryngol. Otol. 2016, 130 (3), 214–218. [CrossRef]
- Levi, J.; Leoniak, S.; Schmidt, R. Evaluating Tonsillectomy as a Risk Factor for Childhood Obesity. Arch Otolaryngol Head Neck Surg 2012, 138 (10), 897. [CrossRef]
- Topal, K.; Kara, C. O.; Bozkurt, A. I.; Saatci, E. The Risk of Overweight and Obesity in Children after Tonsillectomy: A Cross-Sectional Study. Eur Arch Otorhinolaryngol 2013, 270 (2), 689–694. [CrossRef]
- Wei, J. L. Weight Gain after Tonsillectomy: Myth or Reality? Interpreting Research Responsibly. Otolaryngol.--head neck surg. 2011, 144 (6), 855–857. [CrossRef]
- Nachalon, Y.; Lowenthal, N.; Greenberg-Dotan, S.; Goldbart, A. D. Inflammation and Growth in Young Children with Obstructive Sleep Apnea Syndrome before and after Adenotonsillectomy. Mediators of Inflammation 2014, 2014, 1–7. [CrossRef]
- Nieminen, P.; Löppönen, T.; Tolonen, U.; Lanning, P.; Knip, M.; Löppönen, H. Growth and biochemical markers of growth in children with snoring and obstructive sleep apnea. Pediatrics 2002 109(4):e55. [CrossRef]
- Schünemann, H. J.; Cuello, C.; Akl, E. A.; Mustafa, R. A.; Meerpohl, J. J.; Thayer, K.; Morgan, R. L.; Gartlehner, G.; Kunz, R.; Katikireddi, S. V.; Sterne, J.; Higgins, J. P.; Guyatt, G. GRADE Guidelines: 18. How ROBINS-I and Other Tools to Assess Risk of Bias in Nonrandomized Studies Should Be Used to Rate the Certainty of a Body of Evidence. Journal of Clinical Epidemiology 2019, 111, 105–114. [CrossRef]
- Smith, D. F.; Vikani, A. R.; Benke, J. R.; Boss, E. F.; Ishman, S. L. Weight Gain after Adenotonsillectomy Is More Common in Young Children. Otolaryngol.--head neck surg. 2013, 148 (3), 488–493. [CrossRef]
- Huang, Y.-S.; Guilleminault, C.; Lee, L.-A.; Lin, C.-H.; Hwang, F.-M. Treatment Outcomes of Adenotonsillectomy for Children with Obstructive Sleep Apnea: A Prospective Longitudinal Study. Sleep 2014, 37 (1), 71–76. [CrossRef]
- Koycu, A.; Aydin, E.; Tulgar, Kinik, S. Changes in body composition and growth pattern after adenotonsillectomy in prepubertal children. Int J Pediatr Otorhinolaryngol 2016, 81, 46-50. [CrossRef]
- Inja, R.R.; Paul, R.R.; Varghese, L.; Sebastian, T.; Mathews, S.S. Impact of tonsillectomy on dysphagia symptoms and body weight in children. Am J Otolaryngol 2020, 41(6):102682. [CrossRef]
- Elnashar, I.; El-Anwar, M. W.; Raafat, A.; Aesa, E.; Fathy, S. Insulin-like Growth Factor Alpha Changes after Tonsillectomy for Obstructive and Nonobstructive Causes. Egypt J Otolaryngol 2014, 30 (4), 343–346. [CrossRef]
- Costa Pinto Ribeiro, A., Capelo Candido, T., Almeida Nascimento, P. H., Ferraz Rodrigues, P., & Benini Guércio, W. (2021). Crescimento pôndero-estatural de crianças e adolescentes submetidos à adenoamigdalectomia. Scientia Medica 2021, 31(1), e39746. [CrossRef]
- Beauchamp, M. T.; Regier, B.; Nzuki, A.; Swinburne Romine, R.; Sweeney, B.; Liu, M.; M. Davis, A. Weight Change before and after Adenotonsillectomy in Children: An Analysis Based upon Pre-surgery Body Mass Category. Clinical Otolaryngology 2020, 45 (5), 739–745. [CrossRef]
- Ha, E. K.; Lee, S. W.; Kim, J. H.; Lee, J. E.; Jee, H. M.; Chae, K. Y.; Han, M. Y.; Rhie, S. Changes in Childhood Growth after Adenotonsillectomy: A Population-Based Cohort Study. Sleep Medicine 2022, 89, 114–121. [CrossRef]
- Han, S.C.; Yang, S.K.; Han, S.Y.; Rhee, C.S.; Choi, Y.; Shin, C.H.; Lee, Y.J.; Han, D.H. Investigating factors influencing post-operative growth in pre-pubertal children after adenotonsillectomy. Eur Arch Otorhinolaryngol. 2023, 280(6), 2841-2848. [CrossRef]
- Kim, J. Y.; Lee, C. H.; Kim, H.-M. Behavioral Consequences of Children with Sleep-Disordered Breathing after Adenotonsillectomy. World J Pediatr 2018, 14 (1), 57–65. [CrossRef]
- Voora, R.S.; Carvalho, D.; Jiang, W. Impact of Tonsillectomy on Obesity in Pediatric Patients With Sleep-Disordered Breathing. OTO Open 2021, 22; 5(4):2473974X211059105. [CrossRef]
- Hsu, W.-C.; Kang, K.-T.; Weng, W.-C.; Lee, P.-L. Impacts of Body Weight after Surgery for Obstructive Sleep Apnea in Children. Int J Obes 2013, 37 (4), 527–531. [CrossRef]
- Koren, D.; Gozal, D.; Bhattacharjee, R.; Philby, M.F.; Kheirandish-Gozal, L. Impact of Adenotonsillectomy on Insulin Resistance and Lipoprotein Profile in Nonobese and Obese Children. Chest 2016, 149(4): 999-1010. [CrossRef]
- Karalok, Z. S.; Akdag, M.; Turhan, M.; Uzun, G.; Ozdem, S.; Dinc, O.; Bircan, I. Leptin and Ghrelin Levels in Children before and after Adenoidectomy or Adenotonsillectomy. Horm Res Paediatr 2014, 81 (1), 20–24. [CrossRef]
- Moghaddam, Y. J.; Golzari, S. E. J.; Saboktakin, L.; Seyedashrafi, M. H.; Sabermarouf, B.; Gavgani, H. A. E.; Haghjo, A. G.; Lotfi, A.; Ghabili, K. Does Adenotonsillectomy Alter IGF-1 and Ghrelin Serum Levels in Children with Adenotonsillar Hypertrophy and Failure to Thrive? A Prospective Study. International Journal of Pediatric Otorhinolaryngology 2013, 77 (9), 1541–1544. [CrossRef]
- S, Y. B.; Arumugam, S.; Maradi, N. Impact of Adenotonsillectomy on Weight Gain in Children. BJOHNS 2020, 28, 157-160. [CrossRef]
- Czechowicz, J. A.; Chang, K. W. Analysis of Growth Curves in Children After Adenotonsillectomy. JAMA Otolaryngol Head Neck Surg 2014, 140 (6), 491. [CrossRef]
- Lewis, T. L.; Johnson, R. F.; Choi, J.; Mitchell, R. B. Weight Gain after Adenotonsillectomy: A Case Control Study. Otolaryngol.--head neck surg. 2015, 152 (4), 734–739. [CrossRef]
- Katz, E. S.; Moore, R. H.; Rosen, C. L.; Mitchell, R. B.; Amin, R.; Arens, R.; Muzumdar, H.; Chervin, R. D.; Marcus, C. L.; Paruthi, S.; Willging, P.; Redline, S. Growth After Adenotonsillectomy for Obstructive Sleep Apnea: An RCT. Pediatrics 2014, 134 (2), 282–289. [CrossRef]
- Jensen, A. M.; Herrmann, B. W.; Mitchell, R. B.; Friedman, N. R. Growth After Adenotonsillectomy for Obstructive Sleep Apnea: Revisited. The Laryngoscope 2022, 132 (6), 1289–1294. [CrossRef]
- Kirkham, E. M.; Leis, A. M.; Chervin, R. D. Weight Gain in Children after Adenotonsillectomy: Undesirable Weight Gain or Catch-up Growth? Sleep Medicine 2021, 85, 147–149. [CrossRef]
- Al Abdulla, A.; Prabhu, S.; Behzad, K. Prospective Controlled Study on Post-Tonsillectomy Weight Gain-by Objective and Subjective Methods. Egyptian Journal of Ear, Nose, Throat and Allied Sciences 2018, 1 (1), 24–26. [CrossRef]
- AlAbdullah, Z. A.; Alali, K.; Al Jabr, I. Clinical Assessment of Weight Gain in Pediatric Patients Post-Tonsillectomy: A Retrospective Study. Cureus 2020, 12(12): e12005. [CrossRef]
- Kevat, A.; Bernard, A.; Harris, M.-A.; Heussler, H.; Black, R.; Cheng, A.; Waters, K.; Chawla, J. Impact of Adenotonsillectomy on Growth Trajectories in Preschool Children with Mild–Moderate Obstructive Sleep Apnea. Journal of Clinical Sleep Medicine 2023, 19 (1), 55–62. [CrossRef]
- Au, C. T.; Chan, K. C. C.; Lee, D. L. Y.; Leung, N.; Chow, S. M. W.; Chow, J. S.; Wing, Y. K.; Li, A. M. Effect of Surgical Intervention for Mild Childhood Obstructive Sleep Apnoea on Attention and Behavioural Outcomes: A Randomized Controlled Study. Respirology 2021, 26 (7), 690–699. [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017-2018. NCHS Data Brief 2020 Feb;(360):1-8.
- Stierman, B.; Afful, J.; Carroll, M.D.; Chen, T.C.; Fink, S.; Fryar, C.D.; Gu, Q.; Hales, C.M.; Hughes, J.P.; Ostchega, Y.; Storandt, R.J.; Akinbami, L.J. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files. National Health Statistics Reports Number 2021, 158. Hyattsville, MD: National Center for Health Statistics. 2021. [CrossRef]
- Bonuck, K.; Parikh, S.; Bassila, M. Growth failure and sleep disordered breathing: a review of the literature. International journal of pediatric otorhinolaryngology 2006, 70(5), 769–778. [CrossRef]
- Marcus, C. L.; Carroll, J. L.; Koerner, C. B.; Hamer, A.; Lutz, J.; Loughlin, G. M. Determinants of Growth in Children with the Obstructive Sleep Apnea Syndrome. The Journal of Pediatrics 1994, 125 (4), 556–562. [CrossRef]
- Gkouskou, K. K., Vlastos, I. M., Hajiioannou, I., Hatzaki, I., Houlakis, M., & Fragkiadakis, G. A. Dietary habits of preschool aged children with tonsillar hypertrophy, pre- and post-operatively. European review for medical and pharmacological sciences 2010, 14(12), 1025–1030.
- Selimoğlu, E.; Selimoğlu, M.; Orbak, Z. Does Adenotonsillectomy Improve Growth in Children with Obstructive Adenotonsillar Hypertrophy? J Int Med Res 2003, 31 (2), 84–87. [CrossRef]
Figure 1.
The PRISMA flow diagram.
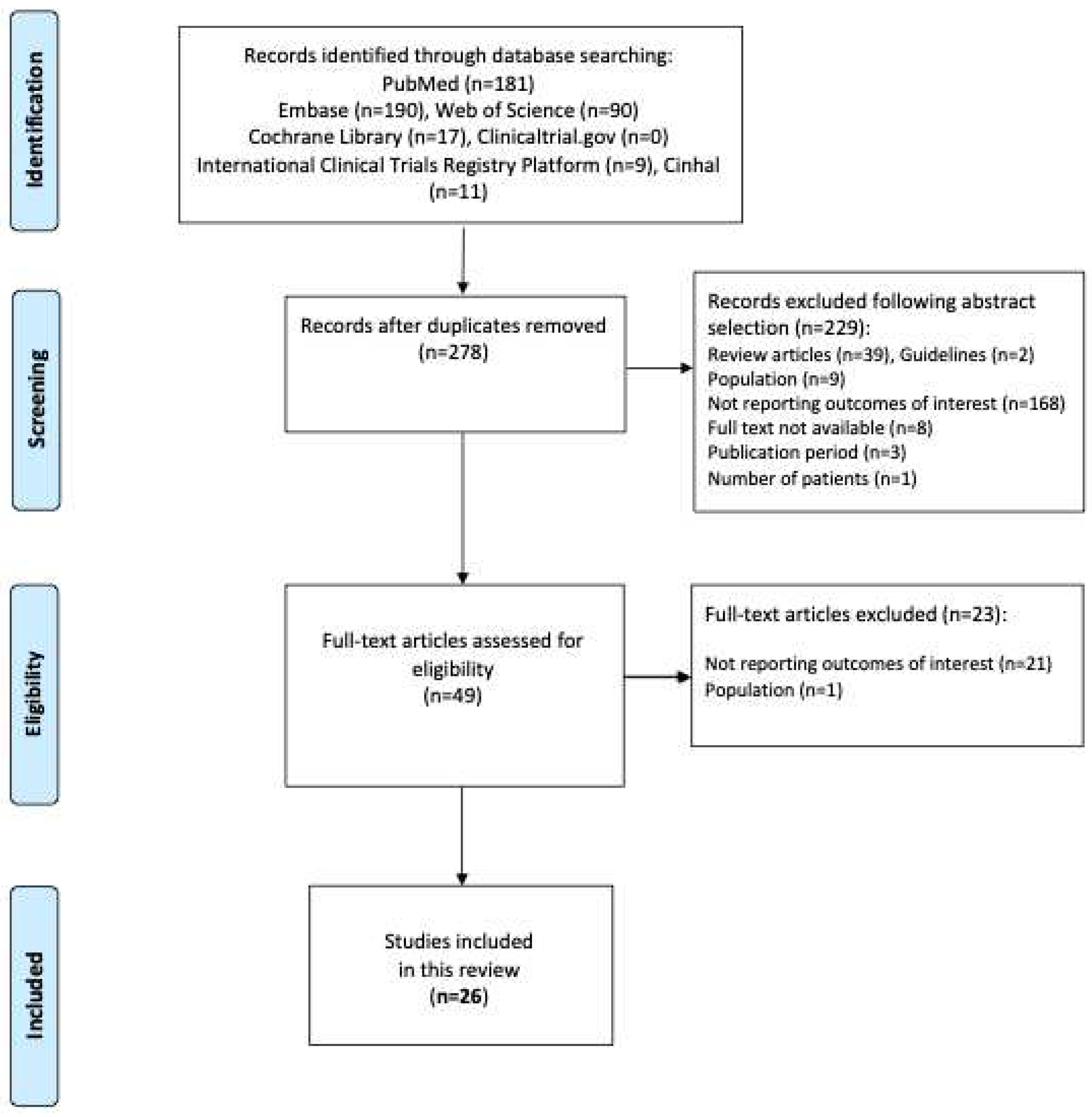
Table 1.
Literature analysis after PICOS selection: summary of the studies and grading of evidence by the GRADE system.
Table 1.
Literature analysis after PICOS selection: summary of the studies and grading of evidence by the GRADE system.
| References | Main objective | Study design | Population and comparator | Methods | Outcomes | Results | Study limitations and Level of evidence |
|---|---|---|---|---|---|---|---|
| Smith DF . et al. [16] |
Post-op WT and demographic risk factors |
Retrospective | 115 children with TA (85 had surgery for OSA; 30 for RT) Pre-op BMI z-score: 0.98±1.5 Age: 1-18y (7.2± 4.3y) Follow up: 6 m Period: 2008-2011 Region: USA |
Chart review | HT, WT, BMIz changes: pre-op vs post-op Risk factors: age, gender, race |
BMIz increased from 0.98±1.5 to 1.21±1.25 (p=0.0009) No difference by surgical indication, gender, race Younger age (<6 years) was a significant predictor of postoperative weight gain (p=0.015) |
Retrospective Moderate- |
| Huang YS et al. [17] |
Efficacy of TA in children with OSA | Prospective | 88 children with OSA underwent TA Pre-op BMI z-score: -0.7± 1.0 Age: 6-12y (8.9± 2.7y) Follow up: 36 m Period: 2007-2010 Region: Taiwan |
Medical history, physical examination | BMIz pre-op vs post-op | BMIz increased not significantly from -0.7±1.0 to -0.33±0.98 at 24 m (p> 0.05) | No control group Selection bias (no Obese by choice) Moderate |
| Koycu A et al. [18] |
Effect of TA on muscle and fat composition | Prospective | 30 prepubertal children with TA or A only vs 28 controls Pre-op BMIz 0.09±1.09 Age: 3-9y (5.0±1.2) Follow up: 6 m Period: 2013-2014 Region: Turkey |
Questionnaire at 0 and 6 m post-op Growth and body composition data at 0 and 6 m with bioelectrical impedance analysis (BIA) |
Dietary habits and physical activity HT and WT z-scores, body fat and muscle mass, BMI z-scores, basal metabolic scores |
At 6 m, in both groups: increased body muscle mass vs baseline (P < 0.05) The relative BMIz (relBMI), pre-post intervention, increased significantly (p=0.018) only in the patient group No change (pre-post) in body fat mass, body fat %, HT z-scores, WT z-scores and BMIz Children with TA (n=14): BMIz improved significantly (P < 0.05), whereas children who underwent A alone (n=16) had no significant change in BMI after surgery The number of OW and Ob children did not change significantly in either group (P < 0.05) BMIz were similar at the end of 6 m in the three groups |
Small sample size Low |
| Inja RR et al. [19] |
Effect of T on swallowing | Prospective | 29 with TA and 2 T only Pre-op WT: 25.4± 12.4 Kg Age: 4-14y (8.3±2.9) Follow up: 3 m Period: not reported Region: South India |
WT at 0, 1 and 3 m post-op | WT | The increase in the WT post-op (+3 m) was 26.9±12.7 (vs pre-op visit, p value < 0.001) |
Small sample size Short f/up No control group HT and BMI and z-scores not evaluated. Low |
| Elnashar I et al. [20] |
Effect of T on the serum IGF-1 in patients undergoing T | Prospective | 50 children with T (24 because of obstructive symptoms and 25 because of RT) Pre-Op BMI: n.a. Age: 4.5-10y Follow up: 3 m Period: 2013-2014 Region: Egypt |
IGF-1 pre-op and 3 m post-op |
IGF-1 levels | In the obstructive group there was an increase in IGF-1 (P < 0.0001), but not in the infection group (P = 0.0883) The pre-op IGF-1 levels in the obstructive group was less than that in the infective group (p=0.026), whereas the post-op IGF-1 level was higher in the obstructive group than in the infective group (0.01) |
Short f/up No control group HT, WT, BMI not evaluated. Low |
| Costa Pinto R et al. [21] |
Effect of TA on WT and HT | Retrospective | 29 children with TA Pre-op WT 29.1±17.4 Kg, HT 122±27.1cm Age:3-13y Follow up: 4 months Period: not reported Region: Brazil |
WT and HT pre-op and 4 m post-op | WT and HT | WT: from 29,1±17,4 kg to 32,8±18,7 kg (p<0,0001). HT: from 122±27,1cm to 125±25,4 (p<0,0001) Pre-scholar, Scholar, Adolescent age WT and HT increase not significant. |
Small sample size Short f/up Retrospective No z-score Low |
| Beauchamp MT et al. [22] |
Effect of T or TA on BMIz | Retrospective | 1751 children with T or TA Age 3-11 y Groups for WT: (383 Ob, 266 Ow, 1041 Nw and 61 Uw) Groups for age: “young” (ages 3-5y) and “older” (ages 6-11y) Follow up: 24m Period: 2004-2017 Region: USA |
Data from medical records |
Change in BMIz trajectories pre-op vs post-op Predictors: age at time of surgery and gender |
Age at time of surgery and gender were not significant predictors of BMIz change Children with Ow/Ob decreased in BMIz, whereas children with Uw or Nw experienced an increase in BMIz. |
Retrospective Wide range period Moderate |
| Ha EK et al. [23] |
Effect of TA on BMIz and HTz | Prospective | 3172 children with TA and 31,663 in the control group Age: 34-69 m Follow up: 66-71 m Period: 2008-2009 Region: Korea |
Physical measurement by a primary clinician | BMI, WT and HT | TA was related to increased WT and HT in the operation group vs the control group. Shortly after TA, WT and BMIz increased significantly in the operation group (0.41±0.02) vs control group (0.18±0.01; p<0.001); a significant increase in HT z-score was observed more than 1 y after TA. |
Moderate |
| Han SC et al. [24] |
Effect of TA on change in growth-for-age | Retrospective | 206 prepubertal children with TA; 167 Nw; 19 Uw; and 20 Ob Age: 3-10 y Follow up: 12m Period: 2011-2014 Region: Seoul |
OSA-18 questionnaire, symptom questionnaire. Data from medical records |
Change in HT, WT, BMIz pre-op vs post-op Factors affecting the change in growth after TA |
After TA, HTz, WTz, and BMIz all increased both in 167 Nw patients and 19 Uw patients (p value < 0.05). In 20 Ob patients, only HTz increased (p value = 0.028). The multiple regression test showed that the sleep disturbance domain of OSA-18 was positively correlated with HT z-score change (p value = 0.041), and age was negatively correlated with WT z-score change (p value = 0.016). Pre-op BMIz was negatively correlated (p value = 0.019) and adenoid grade was positively correlated (p value = 0.023) with BMIz change. |
Retrospective Small number of patients in the Uw and Ob group Moderate |
| Kim JY et al. [25] |
Effect of TA on behavior in children with sleep-disordered breathing (SDB) | Prospective | 170 children who underwent TA and 150 controls BMI pc: 57.1 ± 30.7 Age 5–11 y Follow up: 15.4 ± 2.7 m Period: 2013-2014 Region: South Korea |
Standardized questionnaires for parental sleep-related breathing disorder (SRBD); clinical assessments | Change in HT, WT, BMI pc | Significant increase in BMI pc (p<0.001) and percentage of Ow (p<0.05) after surgery compared to controls | Moderate |
| Voora RS et al. [26] |
Impact of T on obesity in Pediatric Patients With SDB |
Retrospective | 560 (of the cohort of 1153) had available follow-up BMI data. They underwent T or TA due to SDB (87.8%) or (12.2%) for recurrent tonsillitis (RT). Age: 2.0-19.5 y (7.6±4.0 y) Follow up: 6m (50-605 d) Period: 2016-2017 Region: USA |
HT, WT, BMI pre-op and post-op | Change in BMI pc pre-op vs post-op | Higher post-op BMI pc Post-op BMI pc strongly correlated to higher pre-op BMI pc (P <0.001), as well as younger age (P <0.001), male sex (P = 0.0005), and SDB as a surgical indication (P = 0.003). |
Retrospective Limited % of patients with available follow-up BMI data Wide f/up period Low |
| Hsu WC et al. [27] |
Impacts of WT status on surgical outcomes and shifts of WT status after TA in children with OSA |
Prospective | 161 children with OSA who underwent TA. Children were divided into four WT status groups (24 Uw, 79 Nw, 22 Ow and 36 Ob), based on age and gender corrected BMI Age: 7.0±3.4 y Follow up: 6 m Period: 2009-2011 Region: Taiwan |
Demographic data, clinical symptoms, and physical examinations | Change in WT pre-op vs post-op | 54% (13/24) of the Uw children gained WT and shifted to Nw. Nw group had a 9% (7/79) shift to Ow status and 4% (3/79) shift to Uw. The Ow group had a 27% (6/22) shift to Ob and a 14% (3/22) shift to Nw status. Most Ob children (92%, 33/36) remained Ob after TA, with only 8% (3/36) shifting to Ow status |
No control group Moderate |
| Koren D et al. [28] |
Impact of TA upon Ob and metabolic outcomes in children with OSA |
Retrospective | 69 children with moderate-severe baseline OSA who underwent TA Age: 6.33 ±2.04y (3.8-12.2) Follow up: 7.9±3.1 m (range, 2.2-12.2 m) Period: n.a. Region: USA |
Baseline and at follow up overnight PSG anthropometric and Metabolic measurements |
BMIz, insulin, glucose, HOMA-IR, McAuley index, total-HDL-LDL cholesterol, triglycerides | BMIz increased significantly (from 1.43±0.78 to 1.52±0.62, p<0.001) whereas fasting plasma insulin and HOMA-IR were significantly lower and McAuley index trended toward being higher, indicating improved insulin resistance. HDL was significantly higher and total cholesterol/HDL and LDL/HDL ratios significantly lower, indicating more favorable lipoprotein profiles. |
Retrospective Short follow up per some patients Wide age distribution and range of f/up Low |
| Karalok ZS et al. [29] |
Impact of T or TA on serum leptin and plasma ghrelin levels in children | Prospective | 31 patients with T or TA 29 age and sex-matched healthy control children Age: 5.70 ± 2.37y Follow up: 12m Period: 2010 Region: Turkey |
Auxologic evaluation and biochemical investigations | WT, HT, BMI, IGF-1, IGFBP-3, HOMA-IR, leptin, and ghrelin | 1y post-op, HTz (p = 0.001) and WTz (p = 0.004) were significantly increased in both groups. No changes in BMIz (p = 0.105) were observed Pre-Op leptin levels were significantly higher in patients than controls (p < 0.001). IGF-1, IGFBP-3, HOMA-IR, and ghrelin values were not significantly different between the groups. 1-year post-op, IGF-1 (p = 0.001) and IGFBP-3 (p = 0.001) were significantly increased, while ghrelin (p < 0.001) was significantly decreased; leptin levels were also significantly higher than pre-op values (p = 0.036). |
Small sample size Low |
| Moghaddam YJ et al. [30] |
Impact of TA on IGF-1 and ghrelin in children | Prospective | 40 pre-pubertal children with AT hypertrophy, SDB, snoring, open mouth breathing and growth retardation Age: 6.57 ± 1.28 y Follow up: 12 m Period: 2010-2011 Region: Iran |
Auxologic evaluation and biochemical investigations | WT, HT, BMI percentiles, IGF-1, ghrelin | WT, HT, and BMI percentiles were increased significantly post-op (P < 0.001). Serum IGF-1 and ghrelin levels increased significantly post-op vs pre-op (P < 0.001). | Small sample size No control group Low |
| S YB et al. [31] |
Influence of TA on WT | Prospective | 45 children divided in 2 groups: 28 (5-10y) 17 (11-15y) Mean age 9.32y ±n.a Follow-up: 6m Period: n.a. Region: India |
Growth data . |
Change in HT, WT pre and post op | No significant change in WT between two groups and between pre op and post op phasis | Small sample size No control group Low |
| Czechowicz et al. [32] |
Changes in WT, HT, BMIz, before and after TA | Retrospective | 815 children with TA Pre-op WT pc 1st-60th: 342 pt 61st-80th 142 pt 81st-99th 259 pt < 1st 11 pt, > 99th 61 pt Pre-op BMI z-score: n.a. Age: < 18y < 4y: 206 4-8y: 338 > 8y: 199 Follow up: 18m Period: 2007-2012 Region: Stanford, California |
Pre- and post-op WT and HT | HT, WT, BMIz changes: pre-op vs post-op | Mean WT pc increased by 6.3 pc points (p< 0.001) No significant changes in HT pc. Weight percentile plateaued 1 year after surgery, with 90% of gain occurring by 41⁄2 to 6 months. Mean BMI pc increased from 64 to 72 (p < 0.001) Lower BMI at the time of surgery (1st-80th pc) was a significant predictor of post-op WT gain (p < 0.001); no significant increase in BMI pc in those with higher BMI (81st-99th) African-American children had higher WT pc increase (p < 0.001) Tendency to greatest increases in WT in younger population (< 4y: mean increase of 10.7 points; children >8 years had a smaller increase: 3.8 points). |
Retrospective Moderate |
| Lewis TL et al. [33] |
Association between WT gain and TA | Retrospective | 154 children with TA; 182 as control group Study populations divided into 3 groups: Nw (BMI < 85°c), Ow (85°-95°c), Ob (> 95°c) Pre-op BMI pc: Nw 45.7, OW 90, Ob 96.7 Age: 2-16y (mean: Nw 4.9, Ow 6.6, Ob 8.3) Follow up: 6-24 months Period: 2010-2011 Region: USA |
Pre- and post-op WT, HT, BMIz | WT, HT, BMIz Risk factors: Baseline WT, age, gender, ethnicity, indication for surgery |
WT gain in TA group significantly increased at 6, 12, 18, 24 months (p 0.01, < 0.001, < 0.001, 0.002 respectively) HT changes significantly different at 24 months (TA + 1.8 cm, p 0.04) Ob: significant WT gain at 12, 18, 24 m (p <0.001); significant increased HT at 6-12 m Nw: significant WT gain at 12 months (p 0.02) Ow: no differences BMIz significantly higher in Ob at 24 m Differences not affected by age, gender, ethnicity, indication for surgery |
Retrospective Incomplete follow-up data Nw in TA group significantly younger than controls Moderate |
| Katz ES et al. [34] |
WT gain post-TA | RCT (CHAT) | 396: 204 children with OSA underwent TA; 192 watchful waiting control group Pre-op BMI pc: Nw: 48.3%, Ow: 14.9% Ob: 32.7% Uw: 4.5% Age: 5 - 9.9 y (6.57±1.43 in the TA group) Follow up: 7m Period: 2008-2011 Region: USA |
Pre- and post-op WT, HT, BMIz | WT, HT, BMIz Risk factors: Baseline WT, age, gender, ethnicity, indication for surgery |
WTz and BMIz increase (0.13 vs 0.31) in both the groups, greater with TA (p< 0.0001) A greater proportion of Ow randomized to TA developed Ob compared with controls (52% vs 21%; P=0 .05) Race and gender were not significantly associated with BMIz change |
Statistical model did not consider variability of baseline WT status (Kirkham et al.) Low |
| Jensen AM et al. [35] |
Determine if TA increases the risk of Ob | Re-analysis of RCT (CHAT) | 396: 204 children with OSA underwent TA; 192 watchful waiting control group Pre-op BMI pc: Nw: 48.3%, Ow: 14.9% Ob: 32.7% Uw: 4.5% Age: 5 - 9.9 y (6.57±1.43 in the TA group) Follow up: 7m Period: 2008-2011 Region: USA |
Pre- and post-op %BMI pc 95 (as a percentage of the 95th percentile) | %BMI pc 95 Baseline WT, Age, sex, race, Sleep apnea |
Utilizing a linear mixed-effects model accounting for the variability of baseline weight status, OSA resolution status, and time, no significant association between AT and %BMIp95 was found WT significantly increased in the TA group, especially in Uw at baseline (p=0.01). No gender difference. Resolution of OSA was associated with a decreased weight trajectory (p <0.001) |
High |
| Kirkham et al. [36] |
Effect of TA on BMIz Factors influencing post-op growth |
Reanalysis of RCT (CHAT) CHAT: children 5-9.9 yrs with OSA (proven by PSG) |
396: 204 children with OSA underwent TA 192 watchful waiting control group Pre-op BMI pc: Nw: 48.3%, Ow: 14.9% Ob: 32.7% Uw: 4.5% Age: 5 - 9.9 y (6.57±1.43 y in the TA group) Follow up: 7m Period: 2008-2011 Region: USA |
Pre- and post-op BMIz |
WT, HT, BMIz Baseline WT, Age, Sleep apnea, maternal BMI |
A similar percentage of children in both arms experienced undesirable WT gain (45% TA vs 41% watchful waiting). Regression models excluding children who were Uw at baseline: there was no longer a significant effect of TA on BMIz (different from Katz 2014) |
High |
| Al Abdulla A et al. [37] |
WT gain post-TA | Retrospective | 240 children Age: 1-15 (7.45±2.89y) Pre-operative BMI 22.35±3.98 Kg/m2 Follow up: 6m Period: 2018-2019 Region: Saudi Arabia |
Pre- and post-op BMI | WT, HT, BMI, and classification in Uw, Nw, Ow, Ob according to percentile cut-off | Significant difference in mean WT and BMI at 1-6 months post-op (p<0.0001) Positive linear correlation between WT and BMI at 6 m |
Retrospective No z-scores calculation Low |
| AlAbdullah ZA et al. [38] |
Impact of TA on growth | Prospective | 53 children underwent T. 52 controls Age: 2-14 y Pre-operative BMIz -0.30 ± 2.06 Follow up: 12m Period: 2012-2015 Region: Saudi Arabia |
Pre- and post-op BMIz | WT, HT, BMI, BMIz | BMIz in the study group increased compared to controls, but this gain was not statistically significant (p= 0.053) | Moderate |
| Kevat A et al. [39] |
Impact of TA on growth trajectories in children with OSA | RCT | 126 children with OSA randomly assigned to -early TA (within 2 m) -routine (12 m) Age: 49.46±8.44 m 48.97±8.23 m pre-operative BMIz 0.22 (-0.43-0.97) BMIz 0.56 (-0.24-1.21) Follow up: 2y Period: 2018-2019 Region: Australia |
BMIz pre-op and at 12-24 m | WTz, HTz, BMIz | Significant increase in BMIz in the 12 months after TA -early surgery group (0-12m): median 0.4, IC95 0.1-0.8 - routine surgery group (12-24m) median 0.45, IC 95 0.1–0.8, but not from 0–12 months (preoperative time) Findings for WTz, were like the findings for BMIz HTz: not significant change between different time points or intervention groups. |
High |
| Nachalon Y et al. [13] |
Impact of TA on growth in children with OSA | Prospective | 16 children with OSA Age: 23±6 m Follow up: 5±2 m Period: 2013 Region: Israel |
Pre- and post-op WT, HT, BMIz Caloric intake questionnaire |
HT, WT, C-reactive protein, IGF-1 | Increase in HT, WT (P < 0.001 for both) WTz, BMI and BMIz (P = 0.002). Increased caloric intake after TA (P < 0.001), with increased protein and decreased fat intake. The decrease in C-reactive protein levels correlated with the increase in WT in boys (P < 0.05, adjusted for caloric intake). |
Small sample size No control group Low |
| Au CT et al. [40] |
Impact of T or TA on growth | RCT | 71 pre-pubertal children with OSA 35 with early surgical intervention (18TA, 17T) 36 watchful waiting Age: 6-11y (8.4±1.6) Follow up: 10.5±2.2 m Period: 2010-2018 Region: Hong Kong |
Pre- and post-op WT, BMIz, waist circumference z-score | WT, BMIz, waist circumference z-score | The intervention group had a higher baseline waist circumference z score (p = 0.063) The intervention group had significantly greater increase in WT +3.3±2.1 vs +2.2±1.5 kg, p = 0.014 BMI z score remained similar at baseline and follow-up for both groups Waist circumference z score increased significantly in the control group (p<0.05) |
Wide f/up range High |
Abbreviations: adenotonsillectomy (TA), adenoidectomy (A), tonsillectomy (T), obstructive sleep apnea (OSA), recurrent tonsillitis (RT), pre-operative (pre-op), post-operative (post-op), polysomnography (PSG), height (HT), height z-score (HTz), weight (WT), weight z-score (WTz), body mass index (BMI), BMI z-score (BMIz), percentile (pc), Overweight (Ow), Obese (Ob), Normal weight (Nw), Underweight (Uw), recurrent tonsillitis (RT), n.a. not available, sleep-disordered breathing (SDB), day (d), month (m), year (y), Randomized controlled trial (RCT), Childhood Adenotonsillectomy trial (CHAT).Among the selected studies, 5 were RCTs, 12 were prospective, and nine were retrospective. The number of children enrolled in the studies who underwent tonsillectomy (with or without adenoidectomy) was between 16 and 3172: in eight (8) studies, participants were ≤ 50, in thirteen (13) were comprised between 51 and 300, and in five (5) studies were more than 300. The follow-up period lasted from 3 to 36 months (we analyzed up to 24 months by design of the review).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



