
Submitted:
20 December 2023
Posted:
21 December 2023
You are already at the latest version
Abstract
Abstract: Intra-abdominal abscesses (IAA) may commonly arise following complicated gastrointestinal tract infections and, on occasion, from infections within the urinary system. Many of these IAA are initiated as a consequence of post-surgical complications. These abscesses have a substantial risk of morbidity and mortality. As a result, it is crucial to diagnose and treat them promptly to minimise these adverse outcomes. Therefore, radiological modalities play a vital role in diagnosing, localising, and detecting associated complications of IAA, as sometimes other investigations could be less reliable and non-specific. Radiological modalities are pivotal in achieving an accurate diagnosis, localising the abscesses, and identifying associated complications. This is especially important since alternative investigative methods may be misleading in certain situations. Radiological techniques such as ultrasound scans (USS), contrast-enhanced computed tomography (CECT), and even magnetic resonance imaging (MRI) are immensely helpful in diagnosing these conditions. These imaging tools guide clinicians in determining the most appropriate patient management strategies. In this article, we compile a case series involving tubo-ovarian abscess, appendicular abscess, diverticular abscess and infected walled-off pancreatic necrosis, paying particular attention to radiological features in the diagnosis. Furthermore, we reviewed the existing literature to delineate characteristic radiological features related to the cases we discussed.
Keywords:
Intra-abdominal abscesses
; Tubo-ovarian abscess
; Appendicular abscess
; diverticular abscess
; Infected walled-off pancreatic necrosis.
Introduction:
Abscesses are localised collections of pus caused by suppuration buried in a tissue, an organ, or a confined space. They are one of the morphological forms of acute inflammation [1]. Abscesses can be formed in almost every body site, including the brain, soft tissues, lungs, intra-abdominal, and pelvic organs [2]. Intra-abdominal abscesses (IAA) are classified as intraperitoneal vs retroperitoneal, spontaneous vs post-operative and primary vs secondary [3]. IAA commonly arises following infections of the gastrointestinal tract and occasionally following infections from the urinary system. Most of the IAA are post-surgical and account for about 70% of IAA [4]. Besides, intra-abdominal infections are liable to complicate by spreading beyond the primary organ of infection, forming abscesses. This process is predisposed by comorbidities, such as diabetes mellitus, intravenous drug abuse, and immunosuppression, including those with HIV infection [5,6,7,8]. The IAA has a substantial risk of increased morbidity and mortality. Hence, a high index of suspicion, close follow-up, and improved methods for early diagnosis are mandatory [9]. In the prompt diagnostic workup, radiological modalities such as ultrasound scans (USS), contrast-enhanced computed tomography (CECT), and even magnetic resonance imaging (MRI) are vital [9]. Four such cases of intra-abdominal abscesses are described in this article, paying particular attention to characteristic radiological features in the diagnosis.
Case-1:
A 43-year-old mother of three children presented with fever, anorexia, and pelvic pain for three weeks. She had odourless, whitish vaginal discharge and deep dyspareunia for two weeks. On examination, she was afebrile, and her vital signs were normal. Moderate cervical excitation was elicited on transvaginal examination. On bimanual pelvis examination, about 6 cm mass of cystic nature was noted in the left adnexa. She had neutrophil leukocytosis with an increased C-reactive protein (CRP) of 62 mg/dL and a marginally elevated CA125 of 42 units/mL. Her transvaginal ultrasound examination showed a well-defined cystic mass with internal thick echogenic material and a small amount of free fluid in her pouch of Douglas. The CECT abdomen and pelvis showed a unilocular collection measuring 6.2 cm x 6.1 cm x 5.5 cm in the left adnexa adjacent to the uterus, with a small amount of free fluid in the pelvis. (Figure 1a and Figure 1b) The rest of the abdomen was unremarkable. The diagnosis of left adnexal tubo-ovarian abscess (TOA) was made based on history and clinical, biochemical, and radiological findings. She underwent a laparoscopic hysterectomy with bilateral salpingo-oophorectomy and extensive adhesiolysis. She completely recovered after the surgery and a course of intravenous and oral antibiotics.
Case 2:
A 35-year-old woman presents with a gradually increasing severity of high fever, continuous right lower abdominal pain, nausea, and vomiting for six days. On examination, she was febrile with a temperature of 39oC. She was tachycardic with a blood pressure of 100/60 mmHg. Significant tenderness in the right iliac fossa associated with guarding and rigidity was noted in the abdominal examination. She had neutrophil leukocytosis with an elevated CRP of 82 mg/dL. A provisional diagnosis of acute or ruptured appendicitis with abscess formation was made. The abdominal ultrasonography showed a moderately localised fluid collection with surrounding echogenic fat in the right iliac fossa. Based on clinical, biochemical, and ultrasonography findings, it was diagnosed as a localised abscess, probably due to the ruptured appendix. Her CECT abdomen detected a thick-walled moderate-size fluid collection measuring 8.7 cm x 6.4 cm x 6.2 cm inferior to the caecum. (Figure 2a and Figure 2b) Multiple internal gas locules were also noted. The wall of the collection was enhanced with contrast. A collapsed appendix adjacent to the collection and surrounding inflammatory fat stranding were also noted. There is no evidence of right paracolic, subhepatic, or subdiaphragmatic fluid collections. Adjacent caecal and terminal ileal walls were thickened. The lesion was diagnosed as a ruptured appendix with a localised abscess formation and surrounding soft tissue inflammation. The abscesses were drained via an ultrasound-guided pigtail insertion under local anaesthesia, and 350 ml of pus were drained over three days. The pigtail catheter was removed after five days of insertion. Simultaneously, intravenous antibiotics were instituted. The patient made an uneventful recovery and was discharged on day 6 with oral antibiotics. The patient underwent an interval appendicectomy seven months later.
Case 3:
A 62-year-old man with no significant medical history presented with moderate left lower abdominal pain, a low-grade fever, and altered bowel habits for one week. On examination, he was febrile with a temperature of 38°C. Blood pressure of 140/90 mmHg with a pulse rate of 90 beats/min. On his abdominal examination, moderate tenderness was noted in the left iliac fossa without significant guarding or rigidity. He had leukocytosis with 90% neutrophilia and was mildly anaemic, with a haemoglobin level of 9.1 mg/dl. He had an elevated CRP of 69.2 mg/dL. His abdominal ultrasound scanning showed a small fluid collection (10 mm x 15 mm) deep to the maximum tenderness of the pelvis with surrounding echogenic inflamed fat adjacent to the sigmoid colon and urinary bladder.
Localised thickening of the sigmoid colonic wall was also noted, with no dilatation of bowel loops. No free fluid was observed in the abdomen. The pericolic abscess was diagnosed based on clinical examination, basic investigations, and image findings. Upon advice by the surgical team, CECT of the abdomen and pelvis was performed with rectal contrast for further evaluation. It showed a small fluid collection (10.2 mm x 13.0 mm x 15.0 mm) with significant thick fat stranding adjacent to the medial wall of the sigmoid colon, making an inflammatory mass. Significant localised luminal narrowing associated with wall oedema was also noted in affected bowel segments. An inflammatory mass adhered to the urinary bladder wall without intervening fat planes. The rest of the colon was not dilated and showed a few scattered uncomplicated diverticula (Figure 3a and Figure 3b) The CT diagnosis was mesosigmoid diverticular abscess (Hinchey classification, stage Ib). The patient was managed conservatively with intravenous antibiotics, and regular follow-ups were done ultrasonically. The symptoms resolved after a week, and the patient fully recovered.
Case 4:
A 42-year-old man with chronic alcohol abuse and poorly controlled diabetes was admitted with generalised abdominal pain, a high fever, and significant weight loss. He has had three hospital admissions due to abdominal pain over the past 18 months, which were managed as episodes of acute pancreatitis. On examination, he was febrile, with a temperature of 39.40C. His blood pressure was 100/70 mmHg with a pulse rate of 100 beats/min. Central abdominal tenderness and guarding were elicited. He had neutrophil leukocytosis and thrombocytosis with a platelet count of 527 × 109/L and a serum amylase level of 109 U/L. His initial abdominal ultrasonography showed multiple ill-defined intercommunicating fluid collections with thick internal echogenic material at the splenic hilar region. CECT abdomen with oral water and rectal contrast revealed numerous intercommunicating fluid collections (Figure 4a and Figure 4b) in the region of the tail of the pancreas (5.8 cm 6.3 cm x 3.7cm), superiorly extended to the left sub-diagrammatic region, and inferiorly communicating with a collection (2.2 cm x 3.7 cm x 2.9 cm) located anterior to the oedematous body of the pancreas. Multiple gas locules were also noted within the collection, and an air-fluid level was noted in the non-dependent location of the collection. No evidence of intra-pancreatic abscesses, calcifications, pancreatic duct dilatation, splenic artery aneurysm formation, splenic vein thrombosis, or free fluid in the abdomen was noted. Ultrasound-guided FNA confirmed this as an infected collection. After considering clinical, biochemical, and radiological findings, the final diagnosis was made as infected wall-off pancreatic necrosis (WOPN). Ultrasound-guided active aspiration with saline irrigation was performed using a large-bore cannula in the intensive care unit, and passive drainage was allowed with 14-F pigtail catheter insertion using the Selinger technique. The patient completely recovered after an extended stay in the intensive care unit and the surgical ward.
Discussion:
IAA are diverse and carry high mortality and morbidity if timely diagnosis and treatment are not instituted [9,4]. However, clinical features are nonspecific, and basic blood investigations are not characteristic of IAA [10,11,12]. Nevertheless, imaging plays a pivotal role in their diagnosis [4]. In addition, image-guided interventions enable microbiological sampling for definitive aetiological diagnosis with a specific ABST pattern directing targeted antibiotic therapy [13].
Tubo-ovarian abscess:
A tubo-ovarian abscess is a complex inflammatory pelvic pathology that occurs as a complication of untreated pelvic inflammatory disease in premenopausal women [14]. It is described as a walled-off pus involving the fallopian tube and or ovary because of an ascending polymicrobial infection from the lower genital tract [15]. Suspected TOA can be identified on imaging with transabdominal or transvaginal sonography, CECT, or MRI. The USS has become the best and most used initial imaging modality in TOA due to its inherited advantages, high sensitivity (93%), and specificity (98%) [15,16]. Ultrasonically, TOAs are characterised by a unilateral or bilateral complex adnexal cystic mass, thick irregular walls, and multiple internal coarse echoes that likely represent pus with cellular debris [17]. There may be partial septation within the collection. Mild to moderate pelvic free fluid with echogenic debris may also be seen in complicated individuals. The transvaginal examination may better delineate the lesions and exhibit pelvic tenderness over the affected adnexal area [17]. However, ultrasound appearances can mimic endometrioma, hemorrhagic cysts, dermoid cysts, or other cystic ovarian neoplasms. In patients with an uncertain diagnosis, even after proper history, physical examination, laboratory results, and preliminary ultrasonography, a CECT or MRI of the abdomen and pelvis can be performed to evaluate the suspected TOA further. In CECT, TOA may appear as a unilocular or multilocular cystic lesion with moderately attenuated internal fluid. There may be incomplete internal septa and solid areas. Further, TOA abscesses may have a thick, irregular, and heterogeneously enhancing wall [18]. Most of these findings will be shared with endometriomas. However, the multi-layered appearance of the cyst wall may indicate an inflammatory process with the cyst [19]. Identifying a pus-filled fallopian tube with an enhanced thick wall facilitates distinguishing TOA from a neoplastic lesion or endometrioma [20]. Internal gas locules, though rare, are a reliable indicator of a TOA. Other radiological signs to indicate an inflammatory process are perilesional fat standings, thickening of the uterosacral ligaments and mesosalpinx, and increased attenuation of the presacral and para-ovarian fat secondary to inflammation [20,21]. MRI can be used to distinguish between endometrioma and TOA because it reliably identifies or excludes the blood components of the lesion. The purulent content of a TOA usually appears hypointense in T1W and hyperintense in T2W images. However, this signal intensity may vary according to its hemorrhagic and protein content. Fluid within TOA usually shows diffusion restriction on DWI images, intense enhancement of the wall of the collection, and perilesional inflammatory stranding with intravenous Gadolinium. Laparoscopy is still considered the gold standard for diagnosing TOA in some centers. Undoubtedly, it gives the added advantage of concurrent cyst drainage and taking fluid for cultures where necessary [21]. Even so, the rapid development of sonographic and CECT technology allows operators to diagnose correctly and may be used to image guide percutaneous drainage of the abscess with minimal morbidity and mortality. In the first case described here, image-guided drainage was not performed due to inadequate, safe access to the lesion. Further, in this case, TOA was unilocular and confined to single adnexa without significant adnexal inflammatory changes. This could have been due to the sub-acute nature of the illness.
Appendicular abscess
An appendiceal abscess (AA) is a walled-off inflammatory collection adjacent to the appendix due to the inflamed appendix's perforation or peri-appendiceal inflammation due to aggravation of appendicitis [22]. It occurs in 2–6% of patients with acute appendicitis [23]. Appendicular abscesses are mainly diagnosed using USS and CECT. USG is undoubtedly an initial imaging modality due to its inherited advantages, especially since it is pivotal in resource-poor settings. Sonography has a sensitivity of 56 to 94% and a specificity of 47 to 95% [24]. Most appendicular abscesses show an ill-defined hypoechoic unilocular or multilocular fluid collection with internal echogenic debris covered by an irregularly thick wall. In addition, perilesional echogenic fat and free fluid in the right iliac fossa and pelvis may be detected. There may be a communication of the appendiceal lumen with the abscess, air in the appendix wall, and relatively low or absent tenderness with transducer compression [25]. The CT has better diagnostic power than the USS in the diagnosis of appendicitis, with a sensitivity of 98-100%, a specificity of 91-99%, a PPV of 92-98%, and an NPV of 95-100% [26]. In the CECT abdomen, AA appears as a localised fluid collection in the right iliac fossa region, confined by an enhanced thick wall.
Furthermore, abscesses may contain relatively dense material with internal gas shadows and calcification due to appendicoliths. The appendicular abscess remains localised if peri appendiceal fibrous adhesions develop before rupture [27]. These adhesions and perilesional fat standing are better visualised by CT [28]. As a result of the mass effect of the abscess, adjacent bowel loops may be compressed or displaced [28]. In the management of AA, image-guided percutaneous pigtail drainage is one option when the abscess diameter is >4cm [29,30]. It avoids surgery and related complications, shorter hospital stays, a lower cost, and temporising surgical procedures for extremely ill patients [31]. The case presented here also showed typical CT image findings, and it was managed with ultrasound-guided pigtail drainage followed by an interval appendectomy seven months later.
Diverticular abscesses
Diverticular abscesses (DA) are localised paracolic inflammatory collections as one of the complications of diverticulitis [32]. Clinical examination and laboratory findings are significantly inaccurate in defining many aspects of diverticular disease. Therefore, radiological findings are important in diagnosing the disease and its complications, including DA. Imaging modalities useful in diagnosing DA are barium enema, USS, CECT, and MRI [33]. As a traditional imaging technique, barium enema has low sensitivity and specificity in diagnosing diverticular disease and related complications compared to modern cross-sectional images [34]. Indeed, barium studies are not recommended for acute diverticulitis [33]. To reduce unnecessary radiation exposure, sonography is a widely available, non-invasive tool to diagnose diverticular abscesses, especially in premenopausal women and young patients [35]. Further, ultrasound is important in image-guided therapeutic interventions and follow-up of patients. A DA may appear as an anechoic cystic collection with internal hyperechoic debris and pockets of air locules deep to the maximum tender point in the abdomen [35]. CT scans with intravenous and intrarectal contrast are considered the imaging of choice for diverticulitis because it has a high sensitivity of up to 97% and a specificity reaching 100% [36,37]. Based on CT findings, Kaiser et al. described in 2005 the modified Hinchey classification of diverticulitis with five stages in diverticular disease, which has prognostic and potentially therapeutic importance [38]. (Table 1)
However, in 2015, Sartelli et al. proposed a new simple classification and possible treatment strategies based on CT findings, the clinical conditions of the patient, and the presence of comorbidities. This classification has allowed us to decide on acute diverticulitis's non-operative and operative management [39]. According to this classification, oral or intravenous antibiotics manage patients with acute diverticulitis and DA <4 cm. Image-guided percutaneous drainage is recommended for DA >4 cm, and a surgical approach is proposed for more complicated individuals, such as those with pneumoperitoneum [39]. The value of MRI in diagnosing diverticular diseases is still debated. According to Heverhagen et al., sensitivity is 94%, and specificity is 88% in diagnosing acute diverticulitis, with an interesting figure of diagnostic accuracy being better in younger than older patients [40].
Infected walled-off pancreatic necrosis
According to the revised Atlanta classification, various complications of acute pancreatitis, such as acute peripancreatic fluid, pancreatic pseudocyst, acute necrotic collections, and walled-off necrosis, can be differentiated [41]. Cross-sectional imaging based on this new classification avoids the confusion in terminology used over the last 20 years [41]. Pancreatic pseudocyst (PPC) is defined as localized enzyme-rich fluid collection surrounded by a non-epithelialized fibrous wall and occurs in 10-20 % of patients with acute pancreatitis [42]. Walled-off pancreatic necrosis (WOPN) is an encapsulated pancreatic or peripancreatic collection containing necrotic tissue debris and occurs in 1–9% of patients with acute pancreatitis [43]. Pancreatic pseudocysts and WOPN have sequelae of disease that take >4 weeks to mature into wall-off collections [41]. Any collection can be infected or remain sterile during the disease process, and infections are more commonly seen within necrotic collections [44]. Secondary infection of the WON can be associated with a high mortality rate of up to 30%–39% [45]. Therefore, prompt diagnosis of infected WOPN is mandatory to determine management options. Apart from deteriorating signs of infection, objective assessment of collection with imaging is vital. An ongoing infection can be assumed when intra-cystic gas locules or air-fluid levels are due to gas-forming organisms, which can be assured with CECT. However, the presence of gas-forming organisms can be reliably obtained using FNA of the collections and cultures of organisms. Other CECT findings, which are more suggestive of walled-off necrosis over pseudocyst, are more significant in size, extended into the paracolic or retrocolic space, an irregular wall, fat density internal debris, thick or multiple septations, and pancreatic parenchymal irregularities [46]. The accuracy rate for distinguishing WOPN from infected PPC using the evidence is about 80% [46]. Necrotic components of the infected collection are better identified on ultrasonography and T2W MRI than on CT [47]. Ultrasonography and CT are essential during guided FNA and inserting an image-guided pigtail catheter when indicated [48].
The case presented here also showed extensive intercommunicating collections with dense internal material and gas locules. Image-guided FNA followed by culture confirmed the collection as infected WOPN. This collection was managed with active and passive pigtail drainage.
USS
USS is the first imaging modality to diagnose most IAA [10,49], and it is a versatile technique owing to its easy access, portability, non-invasiveness, low cost, and absence of ionising radiation [50]. Therefore, evaluating the disease progress with subsequent scans is useful in patient follow-up [49]. However, USS findings are highly operator-dependent and need high expertise. USS findings are less reliable in obese subjects and when there is overlying bowel gas [50].
CT
CT scanning has a high sensitivity and specificity compared to USS in diagnosing IAA [50]. However, it carries a very high level of ionising radiation, and there is a risk of contrast allergy [50] and contrast-induced nephropathy [51]. Its affordability is lower than that of USS due to its relatively high cost. Therefore, the patient should be hemodynamically stable to undergo CT scanning [49].
MRI
MRI allows better demonstration of the extent of the disease, characterisation of the lesion, and making specific diagnoses than USS or CT scanning. Also, it does not carry the risks of ionising radiation, as seen in CT [52]. However, MRI is time-consuming and more costly than CT or USS and requires patient cooperation in certain instances. Also, MR contrast media-gadolinium has a risk of developing nephrogenic systemic fibrosis in patients with renal insufficiency [52].
Conclusion:
In conclusion, ultrasonography plays a vital role as the first imaging modality in diagnosing a variety of intra-abdominal abscesses. CECT abdomen and MRI better characterise the diagnosis. Imaging-guided interventions in intra-abdominal abscesses play an essential role in managing these patients, which will significantly reduce the morbidity and mortality of patients.
Author Contributions
SRS formulated the concept, designed the review, conducted the literature review, and wrote the manuscript. PDA conducted the literature review and wrote the manuscript. All authors reviewed the manuscript.
Funding
This review received no external funding.
Availability of data and materials
Acquired DICOM medical images during the current review are available from the corresponding author upon reasonable request. The subject’s identifying information was removed in radiology images.
Acknowledgements
The author acknowledges the Management and Radiographers of Leesons Hospital, Ragama, Sri Lanka.
Conflicts of Interest
The authors declare no conflict of interest.
Ethical Approval:
Ethical approval was not considered, as our work is a narrative review. However, we have secured informed consent to publish radiological images from each patient (Image numbers: Figure 1, Figure 2, Figure 3 and Figure 4). Table 1: Credit has been provided, and the reference is mentioned at the end of the table caption. Additionally, we have intentionally removed identifying information from the radiology images. Consent was obtained in the local and English language, and fully completed consent forms are available upon request.
References
- Kumar V, Abbas AK, Aster JC. Robbins Basic Pathology. 10th ed. Kumar V, Abbas AK, Aster JC, editors. Philadelphia, PA: Elsevier - Health Sciences Division; 2021.
- Zammitt N, Sandilands E. Essentials of Kumar and clark’s clinical medicine. 7th ed. London, England: Elsevier Health Sciences; 2021.
- Schein M. Management of intra-abdominal abscesses. In: Holzheimer RG, Mannick JA, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt; 2001.
- Mehta NY, Lotfollahzadeh S, Copelin II EL. Abdominal Abscess. [Updated 2022 Dec 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519573/.
- Zimmermann L, Wendt S, Lübbert C, Karlas T. Epidemiology of pyogenic liver abscesses in Germany: Analysis of incidence, risk factors and mortality rate based on routine data from statutory health insurance. United European Gastroenterol J. 2021 Nov;9(9):1039-1047. [CrossRef]
- Abbas MT, Khan FY, Muhsin SA, Al-Dehwe B, Abukamar M, Elzouki AN. Epidemiology, clinical features and outcome of liver abscess: a single reference center experience in Qatar. Oman Medical Journal. 2014 Jul;29(4):260. [CrossRef]
- Okafor CN, Onyeaso EE. Perinephric Abscess. 2022 Aug 22. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan.
- Saiki J, Vaziri ND, Barton C. Perinephric and intranephric abscesses: a review of the literature. West J Med. 1982 Feb;136(2):95-102.
- Altemeier WA, Culbertson WR, Fullen WD, Shook CD. Intra-abdominal abscesses. Am J Surg. 1973 Jan;125(1):70-9. [CrossRef]
- Adhikari S, Blaivas M, Lyon M. Role of bedside transvaginal ultrasonography in the diagnosis of tubo-ovarian abscess in the emergency department. J Emerg Med. 2008 May;34(4):429-33. [CrossRef]
- Mayer D, Malfertheiner P, Kemmer TP, Stanescu A, Kuhn K, Büchler M, Ditschuneit H. Wertigkeit von Sonographie und Computertomographie im Nachweis von zystischen Veränderungen bei chronischer Pankreatitis [The value of ultrasound and computerized tomography in detection of cystic changes in chronic pancreatitis]. Z Gastroenterol. 1992 Oct;30(10):709-12.
- Snyder MJ. Imaging of colonic diverticular disease. Clin Colon Rectal Surg. 2004 Aug;17(3):155-62. [CrossRef]
- Sirinek KR. Diagnosis and treatment of intra-abdominal abscesses. Surgical infections. 2000 Apr 1;1(1):31-8. [CrossRef]
- Munro K, Gharaibeh A, Nagabushanam S, Martin C. Diagnosis and management of tubo-ovarian abscesses. The Obstetrician & Gynaecologist. 2018 Jan;20(1):11-9. [CrossRef]
- Chappell CA, Wiesenfeld HC. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess. Clinical obstetrics and gynecology. 2012 Dec 1;55(4):893-903. [CrossRef]
- Lambert MJ, Villa M. Gynecologic ultrasound in emergency medicine. Emergency Medicine Clinics. 2004 Aug 1;22(3):683-96. [CrossRef]
- Velcani A, Conklin P, Specht N. Sonographic features of tubo-ovarian abscess mimicking an endometrioma and review of cystic adnexal masses. Journal of Radiology Case Reports. 2010;4(2):9. [CrossRef]
- Krivak TC, Cooksey C, Propst AM. Tubo-ovarian abscess: diagnosis, medical and surgical management. Comprehensive therapy. 2004 Jun;30:93-100. [CrossRef]
- Eo H, Choi HJ, Kim SH, Jung SI, Park BK, Kim SH. Differentiation of tuboovarian abscess from endometriosis: CT indicators. Journal of the Korean Radiological Society. 2005 Oct 1;53(4):273-7. [CrossRef]
- Foti PV, Tonolini M, Costanzo V, Mammino L, Palmucci S, Cianci A, Ettorre GC, Basile A. Cross-sectional imaging of acute gynaecologic disorders: CT and MRI findings with differential diagnosis-part II: uterine emergencies and pelvic inflammatory disease. Insights Imaging. 2019 Dec 20;10(1):118. [CrossRef]
- Bennett GL, Slywotzky CM, Giovanniello G. Gynecologic causes of acute pelvic pain: spectrum of CT findings. Radiographics. 2002 Jul;22(4):785-801. [CrossRef]
- Kobayashi S, Makizumi R, Nakahara K, Tsukikawa S, Miyajima N, Otsubo T. Appendiceal abscesses reduced in size by drainage of pus from the appendiceal orifice during colonoscopy: A Report of Three Cases. Case Reports in Gastroenterology. 2014 Dec 1;8(3):364-70. [CrossRef]
- Andersson RE, Petzold MG. Nonsurgical treatment of appendiceal abscess or phlegmon: a systematic review and meta-analysis. Annals of surgery. 2007 Nov 1;246(5):741-8. [CrossRef]
- Akingboye AA, Mahmood F, Zaman S, Wright J, Mannan F, Mohamedahmed AYY. Early versus delayed (interval) appendicectomy for the management of appendicular abscess and phlegmon: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021 Aug;406(5):1341-1351. [CrossRef]
- Abu-Yousef MM. Ultrasonography of the right lower quadrant. Ultrasound Quarterly. 2001 Dec 1;17(4):211-25. [CrossRef]
- Lane MJ, Liu DM, Huynh MD, Jeffrey Jr RB, Mindelzun RE, Katz DS. Suspected acute appendicitis: nonenhanced helical CT in 300 consecutive patients. Radiology. 1999 Nov;213(2):341-6. [CrossRef]
- Leite NP, Pereira JM, Cunha R, Pinto P, Sirlin C. CT evaluation of appendicitis and its complications: imaging techniques and key diagnostic findings. InPresented at the 2004 Dec 6. [CrossRef]
- Hopkins KL, Patrick LE, Ball TI. Imaging findings of perforative appendicitis: a pictorial review. Pediatr Radiol. 2001 Mar;31(3):173-9. [CrossRef]
- Macari M, Balthazar EJ. The acute right lower quadrant: CT evaluation. Radiologic Clinics. 2003 Nov 1;41(6):1117-36. [CrossRef]
- Hogan MJ. Appendiceal abscess drainage. Techniques in vascular and interventional radiology. 2003 Dec 1;6(4):205-14. [CrossRef]
- Van Sonnenberg E, Wittich GR, Casola G, Neff CC, Hoyt DB, Polansky AD, Keightley A. Periappendiceal abscesses: percutaneous drainage. Radiology. 1987 Apr;163(1):23-6. [CrossRef]
- McCafferty MH, Roth L, Jorden J. Current management of diverticulitis. Am Surg. 2008 Nov;74(11):1041-9. [CrossRef]
- Tursi A, Scarpignato C, Strate LL, Lanas A, Kruis W, Lahat A, Danese S. Colonic diverticular disease. Nat Rev Dis Primers. 2020 Mar 26;6(1):20.
- Andeweg CS, Wegdam JA, Groenewoud J, van der Wilt GJ, van Goor H, Bleichrodt RP. Toward an evidence-based step-up approach in diagnosing diverticulitis. Scand J Gastroenterol. 2014 Jul;49(7):775-84. [CrossRef]
- Mazzei MA, Cioffi Squitieri N, Guerrini S, Stabile Ianora AA, Cagini L, Macarini L, Giganti M, Volterrani L. Sigmoid diverticulitis: US findings. Critical Ultrasound Journal. 2013 Dec;5(1):1-7. [CrossRef]
- Jacobs DO. Diverticulitis. New England Journal of Medicine. 2007 Nov 15;357(20):2057-66.
- Klarenbeek BR, de Korte N, van der Peet DL, Cuesta MA. Review of current classifications for diverticular disease and a translation into clinical practice. International journal of colorectal disease. 2012 Feb;27:207-14. [CrossRef]
- Kaiser AM, Jiang JK, Lake JP, Ault G, Artinyan A, Gonzalez-Ruiz C, Essani R, Beart Jr RW. The management of complicated diverticulitis and the role of computed tomography. Official journal of the American College of Gastroenterology| ACG. 2005 Apr 1;100(4):910-7.
- Sartelli M, Moore FA, Ansaloni L, Di Saverio S, Coccolini F, Griffiths EA, Coimbra R, Agresta F, Sakakushev B, Ordoñez CA, Abu-Zidan FM. A proposal for a CT driven classification of left colon acute diverticulitis. World journal of emergency surgery. 2015 Dec;10(1):1-1. [CrossRef]
- Heverhagen JT, Sitter H, Zielke A, Klose KJ. Prospective evaluation of the value of magnetic resonance imaging in suspected acute sigmoid diverticulitis. Diseases of the colon & rectum. 2008 Dec;51:1810-5. [CrossRef]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013 Jan;62(1):102-11. [CrossRef]
- Memiş A, Parildar M. Interventional radiological treatment in complications of pancreatitis. Eur J Radiol. 2002 Sep;43(3):219-28. [CrossRef]
- Stamatakos M, Stefanaki C, Kontzoglou K, Stergiopoulos S, Giannopoulos G, Safioleas M. Walled-off pancreatic necrosis. World Journal of Gastroenterology: WJG. 2010 Apr 4;16(14):1707. [CrossRef]
- Foster BR, Jensen KK, Bakis G, Shaaban AM, Coakley FV. Revised Atlanta Classification for Acute Pancreatitis: A Pictorial Essay. Radiographics. 2016 May-Jun;36(3):675-87. [CrossRef]
- Bugiantella W, Rondelli F, Boni M, Stella P, Polistena A, Sanguinetti A, Avenia N. Necrotizing pancreatitis: A review of the interventions. International journal of surgery. 2016 Apr 1;28:S163-71. [CrossRef]
- Zhao K, Adam SZ, Keswani RN, Horowitz JM, Miller FH. Acute pancreatitis: revised Atlanta classification and the role of cross-sectional imaging. American Journal of Roentgenology. 2015 Jul;205(1):W32-41. [CrossRef]
- Türkvatan A, Erden A, Türkoğlu MA, Seçil MU, Yüce G. Imaging of acute pancreatitis and its complications. Part 2: complications of acute pancreatitis. Diagnostic and Interventional Imaging. 2015 Feb 1;96(2):161-9. [CrossRef]
- Sion MK, Davis KA. Step-up approach for the management of pancreatic necrosis: a review of the literature. Trauma surgery & acute care open. 2019 May 1;4(1):e000308. [CrossRef]
- Caraiani C, Yi D, Petresc B, Dietrich C. Indications for abdominal imaging: When and what to choose?. Journal of ultrasonography. 2020 Apr 1;20(80):43-54. [CrossRef]
- Leite NP, Pereira JM, Cunha R, Pinto P, Sirlin C. CT evaluation of appendicitis and its complications: imaging techniques and key diagnostic findings. InPresented at the 2004 Dec 6. [CrossRef]
- Tao SM, Wichmann JL, Schoepf UJ, Fuller SR, Lu GM, Zhang LJ. Contrast-induced nephropathy in CT: incidence, risk factors and strategies for prevention. European radiology. 2016 Sep;26:3310-8. [CrossRef]
- Xiao B, Zhang XM. Magnetic resonance imaging for acute pancreatitis. World Journal of Radiology. 2010 Aug 8;2(8):298. [CrossRef]
Figure 1.
(a,b): Axial and sagittal contrast-enhanced CT scan of the abdomen showed a left-sided moderate-size tubo-ovarian abscess (white arrows) with a small amount of pelvic free fluid.
Figure 1.
(a,b): Axial and sagittal contrast-enhanced CT scan of the abdomen showed a left-sided moderate-size tubo-ovarian abscess (white arrows) with a small amount of pelvic free fluid.
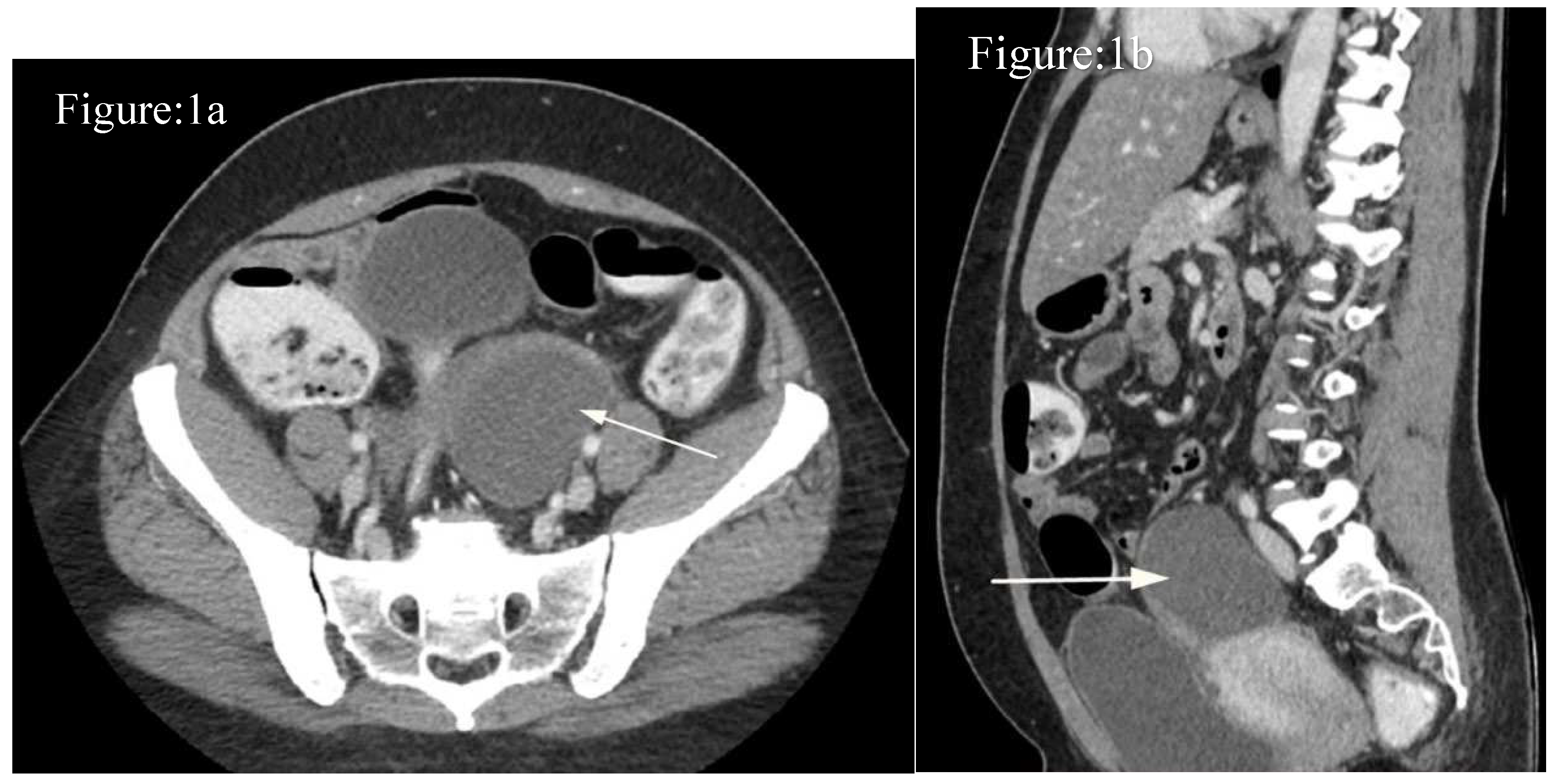
Figure 2.
(a,b): Axial and sagittal contrast CT scan of the abdomen demonstrates a moderate-size appendicular abscess (asterisk).
Figure 2.
(a,b): Axial and sagittal contrast CT scan of the abdomen demonstrates a moderate-size appendicular abscess (asterisk).
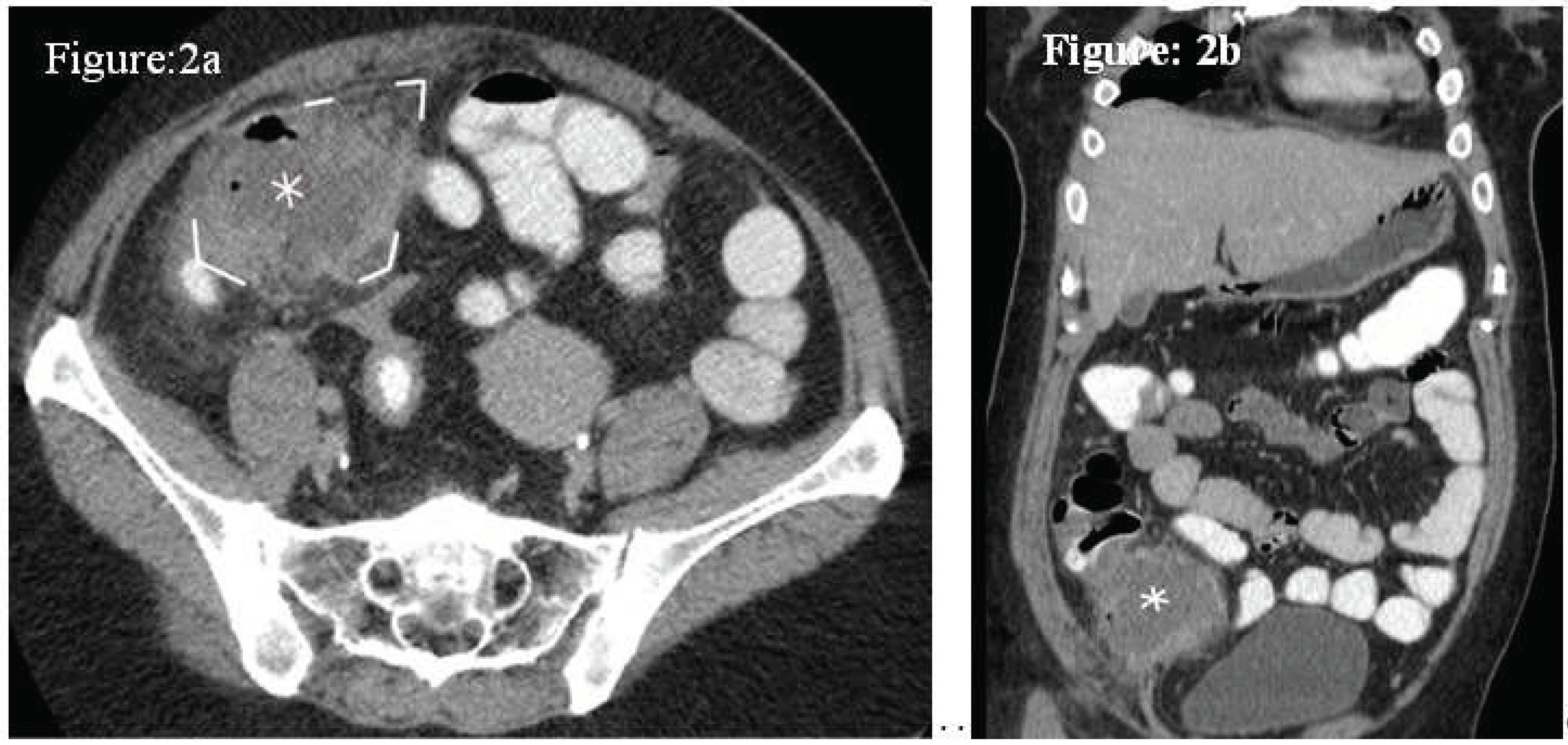
Figure 3.
(a,b): Axial and sagittal contrast-enhanced axial CT scans of the abdomen show a mesosigmoid diverticular abscess (Hinchey classification, stage Ib) (white arrows). The inflammatory mass appeared adherent to the urinary bladder wall.
Figure 3.
(a,b): Axial and sagittal contrast-enhanced axial CT scans of the abdomen show a mesosigmoid diverticular abscess (Hinchey classification, stage Ib) (white arrows). The inflammatory mass appeared adherent to the urinary bladder wall.
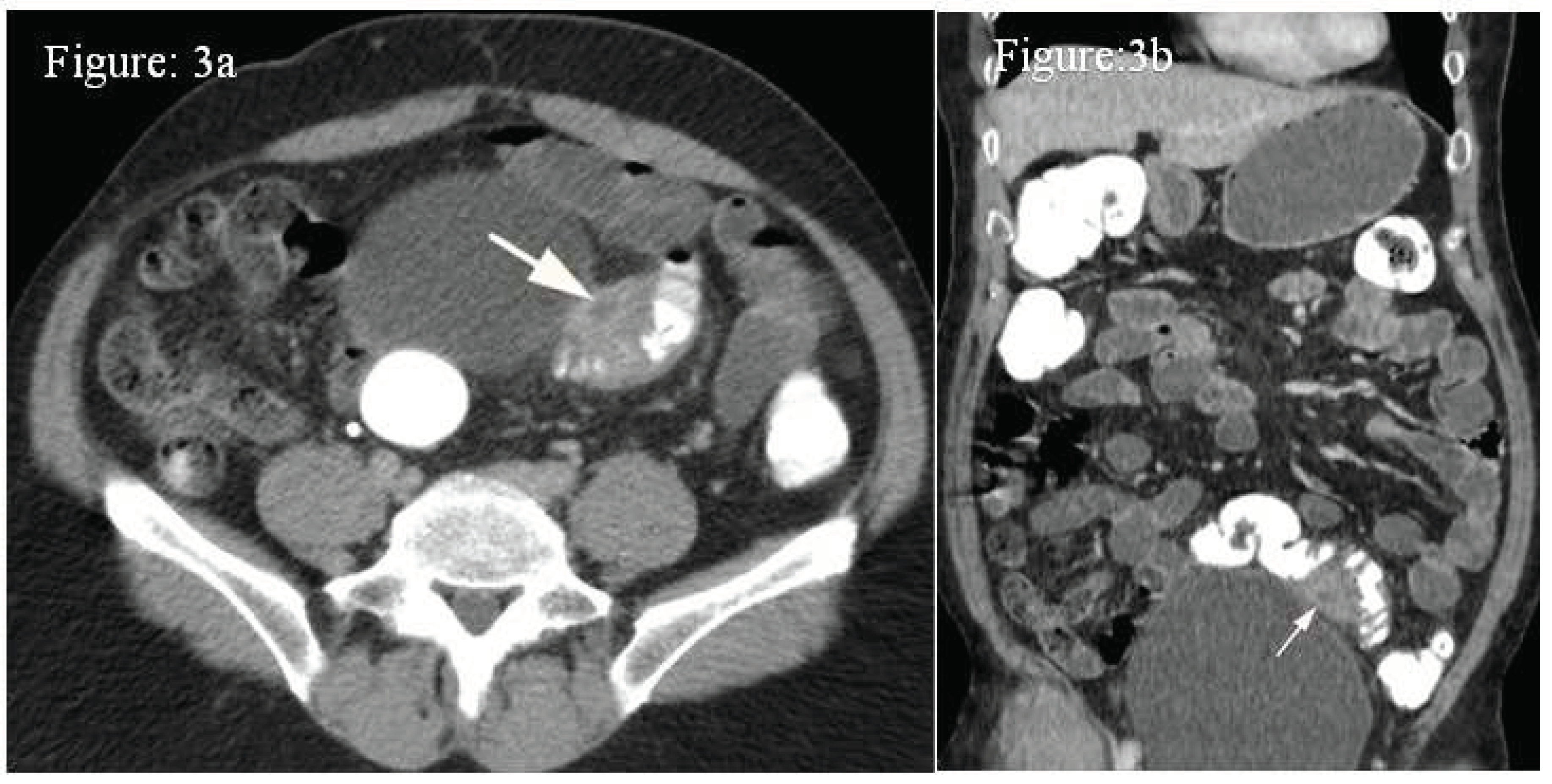
Figure 4.
(a,b): Axial and sagittal contrast-enhanced axial CT scans of the abdomen show an ill-defined intercommunicating infected pancreatic pseudocyst at the splenic hilar region (white arrows) extending superiorly and inferiorly.
Figure 4.
(a,b): Axial and sagittal contrast-enhanced axial CT scans of the abdomen show an ill-defined intercommunicating infected pancreatic pseudocyst at the splenic hilar region (white arrows) extending superiorly and inferiorly.
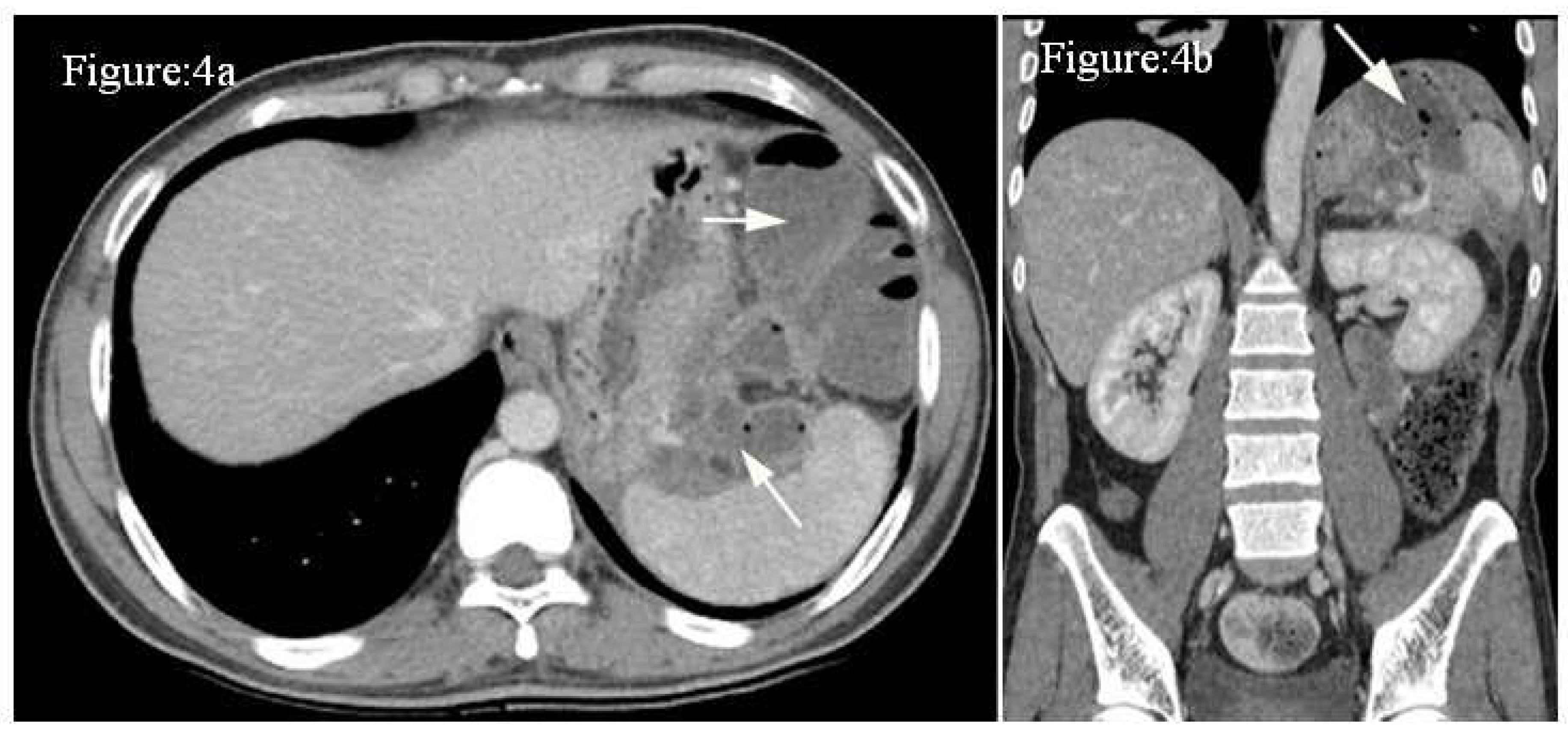

Table 1.
Classification modified by Kaiser et al. (CT findings).
| 0 | Diverticuli ± colonic wall thickening |
| Ia | Colonic wall thickening with pericolic soft tissue changes |
| Ib | Ia changes + pericolic or mesocolic abscess. |
| II | Ia changes + distant abscess (generally deep in the pelvis or interloop regions) |
| III | Free gas associated with localised or generalised ascites and possible peritoneal wallthickening |
| IV | Same findings as III |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



