
Submitted:
21 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Aims. In a male Italian cohort (initially aged 40-59, n=1712) followed-up during 61 years and reaching practical extinction, the natural history of major CVD mortality categories including coronary heart disease (CHD), stroke and other Heart Diseases of Uncertain Etiology (HDUE, including congestive heart failure) were studied along with their risk factor relationships.
Methods and Results. Cox models were run with 12 covariates measured at entry as possible predictors. About 93% of all CVD deaths were covered by the 3 major groups selected here (N=751): 37.4% of them were diagnosed as CHD, 30.6% as stroke and 28.5 % as HDUE. CHD declined in the last 20 years of follow-up, while a sharp increase of HDUE mortality was seen. Baseline mean levels of serum cholesterol were 209.6, 204.2 and 198.0 mg/dl respectively for CHD, stroke and HDUE deaths: the multivariable coefficients of serum cholesterol were positive and significant for CHD (p<0.0001) and stroke (p=0.0203) and not significant for HDUE (p=0.3467). In Fine-Gray models, the algebraic signs of cholesterol coefficients were opposite for CHD versus the other mortality categories (t=3.13). The predictive performances of remaining risk factors were varied whereas that of Cox models was not very good, probably due to the attrition phenomenon and possible competing risks.
Conclusion. Large differences in natural history and risk factors were found comparing the 3 CVD conditions, potentially indicating different etiologies and pointing to the need of not mixing them up in a grouped CVD category.
Keywords:
lifetime CVD mortality
; risk factors
; CVD natural history
Introduction
The cohorts of middle-aged men belonging to the Italian Rural Areas (IRA) of the Seven Countries Study of Cardiovascular Diseases (SCS) have reached a practical extinction after 61 years of follow-up since only 3 men (out the initial 1712) are still alive. This prompted the idea to describe the time trends of mortality and other characteristics across major groups of cardiovascular diseases (CVD) occurred during the lifespan of those men. We also tried to explain potential differences by considering the influence of risk factors associated with those CVD groups.
In previous analyses on shorter follow-up periods [1-3] but also on different cohorts of the SCS [4-6], we focused on coronary heart disease (CHD) versus a group of ill-defined heart diseases that we called Heart Diseases of Uncertain Etiology (HDUE, including congestive heart failure) and large differences from CHD were observed. For the purpose of the present analysis, the groups of CHD and HDUE were contrasted to stroke being another major component of CVD. It is important to note that the current Literature does not concentrate on these group differences, apart those of a clinically defined group of congestive heart failure (CHF), so that discussing outcomes in a practically extinct population-based series becomes quite critical for the time-trend understanding and the natural history of these conditions comparatively.
Material And Methods
Study population. The analysis was run in the pool of two cohorts of middle-aged men (40-59 years old) belonging to the IRA of the Seven Countries Study of Cardiovascular Diseases (SCS). The defined samples included a total of 1735 men and 1712 were examined at start in 1960 (participation rate of 98.7%). More information is available elsewhere [7].
Mortality data. Follow-up for life status, mortality and causes of death was extended for 61 years and only one man was lost to follow-up after 50 years when he was aged 91 years while 3 men were still alive. Causes of death were allocated by reviewing and combining information from death certificates, interim examinations, hospital and medical records, interviews with physicians and relatives of the deceased and any other witnesses of fatal events. Causes of death were determined by a single coder (AM) following defined criteria, and employing the 8th Revision of the WHO-ICD (ICD-8) [8]. In the presence of multiple causes and uncertainty about the principal cause, a hierarchical preference was adopted with violence, cancers, coronary heart disease, stroke and other in that order [9].
The end-points of this analysis were the following groups of cardiovascular diseases:
1) CHD including cases of myocardial infarction, acute ischemic attacks, and sudden coronary death occurring within 2 hours from onset of symptoms, after the exclusion of other possible causes (ICD-8 codes 410, 411, 412, 413, 795); cases with only mention or evidence of chronic coronary heart diseases (part of ICD-8 code 412) or classified as other ischemic heart disease (ICD-8 Coded 414) were not included in this group for reason given elsewhere [1,2], but healed myocardial infarction was retained in this group;
2) Stroke including any type of cerebrovascular diseases (ICD-8 codes 430-438);
3) among other types of CVD we selected and created a large subgroup on heart disease of uncertain etiology (HDUE) including symptomatic heart disease (ICD-8 code 427) (thus CHF in 62% of this group), hypertensive heart disease, usually poorly documented (ICD-8 codes 400-404) (13%), and cases vaguely quoted as chronic or other types of coronary heart disease, (ICD code 412, 414) in the absence of any evidence of typical coronary syndromes (25%); usually they were manifested as heart failure, arrhythmia and blocks.
All other rare or etiologically defined cardiovascular disease were not included in this analysis.
Risk factors. A large number of potential risk factors were measured but for the purpose of this analysis only 12 were selected, to be conservative and taking into account their role shown in previous analyses run on shorter follow-up periods [7].
There were: a) age in years, approximated to the nearest birthday; b) family history of heart attacks, among closed relatives (0=no; 1 = yes); c) cigarettes smoked on average per day (n/day), which was adopted as a metrics since preliminary analyses showed that in the long run ex-smoker had a risk rather similar to the non-smokers (both group being classified with zero cigarettes); d) body mass index (kg/m2) following the technique reported in the WHO Cardiovascular Survey Methods ( the WHO Manual) [10]; e) subscapular skinfold thickness (in mm) following the technique reported in the WHO Manual [10]; f) arm circumference (in mm) following the technique reported in the WHO Manual [10] with the crude measurement cleaned for the contribution of subcutaneous tissue using a formula that included the tricipital skinfold thickness [11]; g) systolic blood pressure (mmHg) measured in supine position at the end of a physical examination, using a mercury sphygmomanometer, following the technique reported in the WHO Manual [10] having the average of two measurements taken one minute apart as analytical variable; h) heart rate (beats/min) derived from a resting ECG; i) vital capacity (in L/m2) following the technique reported in the WHO Manual [10] having the best of two attempts used for analysis; l) serum cholesterol (mg/dl) measured in casual blood samples following the technique by Anderson and Keys [12]; m) urine glucose (yes=1; no=0) measured by uristix in casual urine samples, definite presence used as a proxi of diabetes; n) prevalence of major cardiovascular diseases at entry (0=no; 1 = yes) as defined by the SCS criteria [13].
Baseline data were collected in 1960 before the era of the Helsinki Declaration and acceptance was implied with participation at entry examinations while only later oral informed consent was obtained in view of collecting follow-up data.
Statistical Analysis. A descriptive statistic was computed for death rates of the CVD end-points during 61 years and Kaplan-Meier curves were produced for each CVD group.
A simplified description of mortality trends was created computing death rates for each CVD group in 3 time-blocks of about 20 years whose denominator was made by subjects alive at the beginning of each time-block. For each CVD group age at death was computed.
Cox proportional hazards models were solved with 3 cardiovascular end-points and 12 risk factors as covariates. For each end-point, calibration was computed (proportion of cases in quintile classes of estimated risk).
To test the possible competing risks, the Fine-Gray procedure was used to challenge CHD mortality versus all other causes of death (that is all causes other than CHD). Two models were solved, one with CHD as primary event and the other causes as secondary event, another the other way round, both as a function of the risk factors previously used in Cox models.
Mean levels of baseline risk factors significantly predicting at least one CVD end-point were computed in men who died from any CVD in 3 subsequent time-periods of about 20 years and compared by ANOVA. Statistical significance was set at p value <0.05.
Results
In the 61-year follow-up, among the 1712 men examined at baseline there were 1708 deaths (99.8%), while 3 men were still alive with an age range of 102 to 106 years and one man was lost to follow-up after 50 years when he was aged 91 years. All types of CVD deaths covered 46% of total mortality while those considered for this analysis were 93% of all CVD deaths (N=727). Among them, 38.7% were diagnosed as CHD, 31.6% as stroke, and 28.5% as HDUE.
Kaplan-Meier curves showed a highly statistically significant difference (p<0.0001) among the 3 components of CVD mortality with a clear-cut and constant rightward displacement of the lifetime HDUE curve as compared to those of CHD and stroke (Figure 1).
On the other hand, the time-trends of the 3 major conditions showed large differences in the 20-year periods covering the whole follow-up. In fact, CHD death rate sharply increased between period 1 and 2, but largely decreased in period 3 losing its first rank position; death rates for stroke increased from period 1 to period 3, maintaining its second rank position; while death rates for HDUE continuously increased becoming the first ranking in the third time period (Figure 2). All this suggested that HDUE, beyond other characteristics, had a different natural history compared with the other two major CVD categories. Moreover, age at death was largely different across the CVD groups, i.e. 73.2 (±19.4) years for CHD, 75.2 (±10.6) years for stroke and 79.7 (±10.8) years for HDUE (ANOVA p<0.0001).
Mean levels of the selected risk factors at entry examination are reported in Table 2 where those related to the whole study population reflect the situation for men in Italian rural environments in the mid of last century. Among them, there were relatively high levels of blood pressure and cigarette consumption and relatively low levels of serum cholesterol. Prevalence of family heart attack was rather high but the vague term used in the questionnaire was preferred to a more technical term (like myocardial infarction) that could be difficult to understand those times.
Baseline mean levels of risk factors across CVD mortality groups did not show significant differences except for heart rate (p=0.0075), and serum cholesterol (p=0.0066).
Cox models showed a variety of combinations of significant risk factors for CHD, stroke and HDUE as based on hazard ratios and their 95% confidence intervals (Table 2, Table 3 and Table 4). In particular, significant risk factors for CHD were age, cigarette smoking, systolic blood pressure, serum cholesterol and vital capacity; for stroke age, systolic blood pressure, serum cholesterol, urine glucose and vital capacity; for HDUE age, cigarette smoking, systolic blood pressure and heart rate. Significant risk factors common to the three CVD end-points were only age and systolic blood pressure. Among risk factors used in these models we found a relatively high correlation and a collinearity problem between BMI and subscapular skinfold but, after removal of the latter, the new multivariable coefficients of risk factors were not significantly different from those of the original models.
The performance of the Cox models was estimated through the calibration procedure, reported in Table 6 for the 3 CVD end-points. Calibration was poor for all end-points since there was no clear trends in the proportion of cases distributed in quintile classes of estimated risk. We tried to find an explanation for the poor performance of the Cox models and Table 7 may contribute, at least partially. Using only risk factors with significant coefficients in at least one CVD end-point, mean levels were reported for those who died from any end-point in each time period of about 20 years. A definite trend occurred from time period 1 to time period 3, compatible with early deaths among those carrying unhealthy levels.

Table 5.
Cox model for HDUE deaths (N=216) in 61 years as a function of 12 risk factors.
| Variable | Delta | HR | 95% CI | P of coefficient |
|---|---|---|---|---|
| Age | 5 | 2.34 | 1.98 2.77 | <0.0001 |
| Family heart attack | 1 | 1.17 | 0.89 1.54 | 0.2663 |
| Cigarettes | 9 | 1.21 | 1.06 1.38 | 0.0052 |
| Body mass index | 4 | 0.95 | 0.70 1.30 | 0.7612 |
| Subscapular skinfold | 6 | 0.95 | 0.75 1.22 | 0.7014 |
| Arm circumference | 24 | 0.91 | 0.74 1.11 | 0.3426 |
| Systolic blood pressure | 20 | 1.36 | 1.16 1.58 | <0.0001 |
| Heart rate | 13 | 0.81 | 0.69 0.96 | 0.0145 |
| Vital capacity | 0.24 | 0.92 | 0.78 1.09 | 0.3329 |
| Serum cholesterol | 40 | 1.07 | 0.93 1.23 | 0.3467 |
| Urine glucose | 1 | 1.72 | 0.89 3.32 | 0.1037 |
| CVD prevalence | 1 | 1.74 | 0.91 3.33 | 0.0950 |
Units of measurement as from Table 2; HR = Hazard ratio; 95%CI = confidence intervals. Delta for computation of HR roughly corresponding to 1 standard deviation for continuous variables. Significance in bold.
Findings of the competing risks by Fine-Gray procedure (Table 8) suggested that serum cholesterol was the critical risk factor in competition between CHD and other causes with a large positive and significant coefficient in the first model and a negative non-significant coefficient in the second model. On the other hand, age played a different role with positive higher level of coefficient in the second model.
Discussion
The study based on a follow-up of 61 years in a cohort of middle-aged men showed large differences across mortality from 3 major CVD conditions, i.e. CHD, HDUE (mostly composed of CHF) and stroke that related to several aspects of natural history and prediction thus suggesting that different diseases might be implicated and that etiology, mainly of HDUE, is still largely unknown but different from CHD. Although it was authoritatively suggested to base conclusions more on effect size, direction, plausibility, consistency, repeatability and clinical or practical utility rather than statistical significance [14] there are occasions, like the opposite sign (and thus direction) seen in this study for the predictive capacity of cholesterol versus CHD or other causes of death in the competing risk approach (Table 8), that deserve special attention as a statistical divergence, which is an important result presented. There are moreover, several other characteristics that were different across the 3 CVD mortality end-points used in this analysis, that is, death rates, mortality time-trends, age at death, baseline levels of some risk factors and long-term risk factor predictive power. In particular, CHD was the most common condition. It declined in the last 20 years of follow-up, while during the same period there was a sharp increase of HDUE (including in large proportions CHF) mortality. Age at death was significantly lower for CHD, higher for HDUE and intermediate for stroke. The latter result in the IRA cohorts was recently confirmed in another 8 cohorts of the SCS [15].
Baseline mean levels of serum cholesterol were higher for those who died from CHD, lower for those who died from HDUE, intermediate for those who died from stroke, while it was significantly predictive (with a positive coefficient) of CHD events and stroke events and not predictive for HDUE events. In particular, a further novel finding in this analysis was the significant positive coefficient of serum cholesterol predicting stroke mortality since in previous analyses on shorter follow-up periods this was not found [16]. It is possible that in the late years more thrombotic events added up but this conclusion remains uncertain since in the majority of cases we were unable to segregate thrombotic from hemorrhagic stroke.
All these important differences explicitly point to the fact that when comparing CHD with HDUE we are probably looking at different diseases, what might also be concluded if CHD is compared, by Fine-gray model that takes competition into account, to all other causes of death whereby a major risk factor such as cholesterol has a divergent role. As a consequence, it may not be appropriate to pool those 3 conditions into a single CVD end-point, simply because they relate to the same anatomical-physiological system although sharing the role of age and systolic blood pressure as significant risk factors, as is commonly but inappropriately done in composite end-point analyses in the current Literature. A Cox model including all CVD conditions (not reported in detail) may make sense in view of identifying risk factors that probably share at least some of the various end-points and for general preventive purposes. However, this does not help to improve the understanding of possible etiologies of the single conditions that, for certain aspects, remain different diseases.
The hypothesis was made of an important explanatory contribution of competing risks, a concept already documented on the same material using the 50-year follow-up data [17,18]. In other words, those with high cholesterol (and possibly other risk factors) are hit by a CHD event at younger age while the others (relatively protected) become more exposed to other types of events that finally occur but years later and at older ages. This likely explains part of the significant rightward displacement of the Kaplan-Meier curve for HDUE as compared to CHD and stroke (Figure 1) and the different age at death mainly comparing CHD with HDUE.
Some coefficients of major risk factors were smaller than in models run in the past for shorter follow-up period [7,16]. This can be explained by the fact that during the first periods subjects with higher levels were eliminated opening the chance to people with lower levels of risk factors to reach the disease status. In fact, the poor performance of the Cox models could partly be explained by the attrition phenomenon consisting in the early drop-out of subjects with worse risk factor levels. As a consequence, those dying later were usually carrying better levels of risk factors, contributing to dilute the magnitude of multivariable coefficients. This seems a universal phenomenon but probably enhanced by the lifelong follow-up that we have here.
Changes of risk factors level during the follow-up might also influence the multivariable coefficients. By sure there has been a sharp decline of cigarette smoking, a definite increase of blood pressure and a sizeable increase of serum cholesterol, but from previous analyses we know that the baseline risk factor levels were predictive for at least 40 years when tested in partitioned blocks of follow-up time [19].
It was almost impossible to find in the Literature studies really comparable to this one in terms of follow-up duration, practically extinction of the cohort and dealing with the same groups of CVD mortality with well-defined groups based on the international classification of diseases. The only “key word” providing somewhat similar analyses and references were “lifetime CVD risk”. Many studies claim to have estimated the lifetime risk of CHD but almost all have simply applied to their data a lifetime Framingham risk score [20]. Actually, they do not deserve a direct mention since they simply produced theoretical estimates applying an external score to their baseline data.
On the other hand, the Framingham score [20] was based on the use of total and HDL cholesterol, systolic and diastolic blood pressure, smoking habits and body mass index, all transformed into a variable number of discrete classes. The lifetime exposure was actually stopped at the age of 95 years and the overall death rate of the observed cohort was of about 30%. Moreover, the assumption was made that those reaching the age of 75 years could be considered as “dead” although the majority of them died later. In fact, the concept of "lifetime” was interpreted in a substantially arbitrary way and the analytical approach had nothing to do with our approach where a cohort was followed-up until practical extinction (99.8%).
Other contributions based on the Framingham study dealing with the same general problem were mainly devoted to numerical estimates of lifelong CVD incidence-mortality based on incomplete follow-up [21], including a specific analysis dedicated to CHF (in people without and with previous myocardial infarction) [22] and another to stroke [23]. The same authors made comparisons of 10 years versus lifelong events prediction [24,25] concluding that a new specific approach should be developed.
A huge analysis was conducted in the US pooling several large studies with data collected from 1964 through 2008 and exploiting the predictive role of blood pressure, smoking habits, diabetes and serum cholesterol and posing the age limit of 95 years. The outcome, defined by a pool of different major CVD, was predicted with largely different probabilities depending on the combination of high-low levels of the considered risk factors [26].
A Swedish study based on a risk factor population screening of 92,000 adults aged 40, 50 and 60 years, covered a maximum follow-up of 25 years [27]. Measured risk factors were serum cholesterol, smoking habits, blood pressure, body mass index, physical activity, self-reported health, education and marital status, all considered in discrete classes and combining them to determine 3 different risk profiles. The end-points were the occurrence of CHD, stroke, CHF and a pool of CVD. There was a coherence between the risk profiles and the so-called lifetime risk of CHD, but not for stroke and CHF, suggesting that this study had some similarity with our findings. However, the authors did not comment this aspect and simply said that the distinction between specific CVD events was not a relevant problem since the real problem is the prevention through action on risk factors. This conclusion has a practical sense, but excludes any attention for possible differences across various CVD types and their possible etiology, alike what we tried here.
A Chinese study published in 2015 involved almost 22,000 adults aged 35-84 where a few risk factors were measured and the follow-up was extended for 18 years [28] with pooled CVD events as end-point. The estimate of lifetime CVD risk, with limit posed at the age of 80 years, showed the ability of a few risk factors to segregate high from low risk for CVD events.
In 3 large meta-analyses run on the same population studies, but separately exploring different risk factors, it was impossible to identify a subgroup of common heart diseases, outside CHD (that is somewhat similar to those we call HDUE) since they were usually pooled with other vascular diseases preventing the possibility to describe carefully their characteristics [29-31].
It is clear that genomics analyses may improve long-term risk prediction and some contributions start to be of great interest [32] but this aspect could obviously not be considered in our data collected in the mid of last century.
Finally, we have more recently investigated in the context of 10 cohorts of 9,063 middle-aged men of the Seven Countries Study followed for 60 years to extinction whether competing risks of CHD mortality versus other causes of death, comparatively assessed by Fine-Gray versus Cox models, might help explaining why regions with initially high serum cholesterol have higher mortality from CHD and lower from stroke and HDUE, while the reverse is found for those with initially lower serum cholesterol [33]. There were 5 important conclusions that lead support to the results presented here: 1) CHD mortality is bound to different risk factor relationships when put in competition with all other causes of death and with the sum of HDUE and stroke; 2) competing risk analyses (by Fine-Gray methods) are needed to assess risk factor capabilities in specific outcome types of CVD since they are different depending on outcome types considered (CHD versus HDUE plus stroke ); 3) there are important differences among predictive covariates, in terms of presence/absence and opposition of the coefficients’ algebraic sign when the inversion is performed of primary versus the secondary outcome in case of Fine-Gray, what is much less evident or absent by Cox which point to the need of a certain power, namely number of enrolled individuals, in order to assess these aspects; 4) the changing algebraic sign of country coefficients, treated in the study as dummy variables, comparing direct versus inverse models might suggest a possible “ecologic“ interpretation of the Fine-Gray analysis; 5) it is clear that individual outcomes of CVD should not be summed-up or equated, which should be considered in all future investigations.
A major strength of the present study is the practical extinction of the original cohort and the extremely long duration of follow-up that with detailed diagnosis of outcome results, what has few if no comparative examples in the Literature. However, these results cannot be extended to women that were not included since at starting of the Seven Countries Study it was estimated that the low incidence of heart disease would have requested too large groups to be enrolled, unacceptable financial and organizational requirements in early sixties. It is extremely important to underline that composite end-point analyses of CVD mortality have the inherent risk to distort the relations among factors and outcomes to the extent that, at least, CHD versus HDUE (or also possibly the sum of HDUE and stroke) and versus all other causes of death should be considered, not mixing them up for a composite end-point analysis of CVD, like mostly done in the Literature. Moreover, there might be predictive differences in the analyzed covariates when a cohort presents around 39% of CHD deaths versus lower or higher proportions, which depends, among other factors also on the respective proportions of stroke and HDUE. This fact has important consequences for epidemiology, public health and clinical practice since the potential different etiology between CHD and HDUE (largely composed of CHF) points to the need of dissecting these causes in large ongoing and future investigations also separating stroke from the other components of CVD [34] and certainly not addressing composite end-points just to unduly increase the power of studies which is done more than often [35] and may have unpredictable consequences depending on the analyzed cohorts.
Author Contributions
Conceptualization, Paolo Emilio Puddu, Paolo Piras, Alessandro Menotti; Methodology and Analysis, Paolo Emilio Puddu, Paolo Piras; Writing – original draft, Paolo Emilio Puddu, Alessandro Menotti. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The board of directors of the various institutions involved in data collections (2 in this case) were de facto playing the role of ethical committee approving the execution of the study on the basis of the local existing legislation by the date this investigation started.
Informed Consent Statement
Baseline measurements were taken before the era of the Helsinki Declaration and approval was implied in participation, while verbal or written consent was obtained for collection of follow-up data.
Data Availability Statement
The original data are not publically available. However, research projects are evaluated centrally by an ad hoc committee.
Acknowledgments
The authors acknowledge the pioneer role of the late Vittorio Puddu and the late Flaminio Fidanza who were the initiators of the Italian participation to the Seven Countries Study of Cardiovascular Diseases.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Menotti A, Puddu PE. Lifetime prediction of coronary heart disease and heart disease of uncertain etiology in a 50-year follow-up population study. Int J Cardiol 2015; 196: 55-60. [CrossRef]
- Puddu PE, Menotti A. Natural history of coronary heart disease and heart disease of uncertain etiology: findings from a 50-year population study. Int J Cardiol 2015; 197: 260-264. [CrossRef]
- Menotti A, Puddu PE, Maiani G, Catasta G. Lifestyle behaviour and lifetime incidence of heart diseases. Int J Cardiol 2015; 201: 293-299. [CrossRef]
- Menotti A, Blackburn H, Seccareccia F, Kromhout D, Nissinen A, Karvonen M, et al. Relationship of some risk factors with typical and atypical manifestations of coronary heart disease. Cardiology 1998; 89: 59-67. [CrossRef]
- Menotti A, Lanti M, Nedeljkovic S, Nissinen A, Kafatos A, Kromhout D. The relationship of age, blood pressure, serum cholesterol and smoking habits with the risk of typical and atypical coronary heart disease death in the European cohorts of the Seven Countries Study. Int J Cardiol 2005; 106: 157-163. [CrossRef]
- Menotti A, Puddu PE, Lanti M, Kromhout D, Tolonen H, Parapid B, et al. Epidemiology of typical coronary heart disease versus heart disease of uncertain etiology (atypical) fatalities and their relationships with classic coronary risk factors. Int J Cardiol 2013; 168: 3963-3967. [CrossRef]
- Menotti A, Puddu PE. How the Seven Countries Study contributed to the launch and development of cardiovascular epidemiology in Italy. A historical perspective. Nutr Metab Cardiovasc Dis 2020; 30: 368-383. [CrossRef]
- WHO: International classification of diseases. Eight revision. Geneva, World Health Org, 1965.
- Kromhout D, Menotti A, Blackburn H. Prevention of coronary heart disease. Diet, lifestyle and risk factors in the Seven Countries Study. Kluwer Publ. Norwell Ma, USA and Dordrecht, NL, 2002: 1-267.
- Rose G, Blackburn H. Cardiovascular survey methods. Geneva, World Health Organization, 1968.
- Hemsfield SB, MacManus C, Smith J, Stevens V, Nixon DW. Anthropometric measurement of muscle mass: revised equations for calculating bone-free arm muscle area. Am J Clin Nutr 1982; 36:680-690. [CrossRef]
- Anderson JT, Keys A. Cholesterol in serum and lipoprotein fractions: its measurement and stability. Clin Chem 1956; 2:145-159. [CrossRef]
- Keys A, (ed) Blackburn H, Menotti A, Buzina R, Mohacek I, Karvonen MJ, et al. Coronary heart disease in seven countries. Circulation 1970, 41, suppl 1: 1-211. [CrossRef]
- Wasserstein RL, Schirm AL, Lazar NA. Moving to a world beyond “p <0.05”. Am Statistician 2019; 73: 1-19. [CrossRef]
- Menotti A, Puddu PE, Kafatos AG, Tolonen H, Adachi H, Jacobs DR Jr. Cardiovascular mortality in 10 cohorts of middle-aged men followed-up 60 years until extinction: The Seven Countries Study. J Cardiovasc Dev Dis 2023; 10: 201. [CrossRef]
- Menotti A, Lanti M, Maiani G, Kromhout D. Forty-year mortality from cardiovascular diseases and their risk factors in men of the Italian rural areas of the Seven Countries Study. Acta Cardiol 2005; 60: 521-531. [CrossRef]
- Puddu PE, Piras P, Menotti A. Competing risks and lifetime coronary heart disease incidence during 50 years of follow-up. Int J Cardiol 2016; 219: 79-83. [CrossRef]
- Puddu PE, Piras P, Menotti A. Lifetime competing risks between coronary heart disease mortality and other causes of death during 50 years of follow-up Int J Cardiol 2017; 228: 359-363. [CrossRef]
- Menotti A, Puddu PE. Risk factors measured in middle-aged men predicting coronary events in geriatric age. Int J Cardiol 2016; 222: 1116-1121. [CrossRef]
- Llyod-Jones DM, Leip EP, Larson MG, D’Agostino RB, Beiser A, Wilson PWF et al. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation 2006; 113: 791-798. [CrossRef]
- Lloyd-Jones DM, Larson MG, Beiser A, Levy D. Lifetime risk of developing coronary heart disease. Lancet 1999; 353:89-92. [CrossRef]
- Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, et al. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation 2002; 106: 3068-3672. [CrossRef]
- Seshadri S, Wolf PA. Lifetime risk of stroke and dementia: current concepts, and estimates from the Framingham Study. Lancet Neurol 2007; 12: 1106-1114. [CrossRef]
- Lloyd-Jones DM, Wilson PWF, Larson MG, Beise A, Leip EP, D’Agostino RB et al. Framingham risk score and prediction of lifetime risk for coronary heart disease. Am J Cardiol 2004; 94: 20-24. [CrossRef]
- Lloyd-Jones, DM. Short-term versus long-term risk for coronary artery disease: implications for lipid guidelines. Curr Opin Lipidol 2006; 6: 619-625. [CrossRef]
- Wilkins JT, Ning H, Berry J, Zhao L, Dyer AR, Lloyd-Jones DM. Lifetime risk and years lived free of total cardiovascular disease. JAMA 2012; 308:1795-1801. [CrossRef]
- Stenling A, Haggstrom C, Norberg M, Norstrom F. Lifetime risk predictions for cardiovascular diseases: competing risks analyses on a population-based cohort in Sweden. Atherosclerosis 2020; 312: 90-98. [CrossRef]
- Wang Y, Liu J, Wang W, Wang M, Qi Y, Xie W et al. Lifetime risk for cardiovascular disease in a Chinese population: the Chinese Multi-Provincial Cohort Study, Eur J Prev Cardiol 2015; 22: 380-388. [CrossRef]
- Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360: 1903-1913. [CrossRef]
- Prospective Studies Collaboration. Blood cholesterol and vascular mortality by age, sex and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55000 vascular deaths. Lancet 2007; 370: 1829-1839. [CrossRef]
- Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900,000 adults: collaborative analyses of 57 prospective studies. Lancet 2009; 373:1083-1096. [CrossRef]
- Abraham G, Havulinna AS, Bhalala OG, Byars, De Livera AM, Yetukuri L et al. Genomic prediction of coronary heart disease. Eur Heart J 2016; 37: 3267-3278. [CrossRef]
- Puddu PE, Piras P, Kafatos A, Adachi H, Tolonen H, Menotti A. Competing risks of coronary heart disease mortality versus other causes of death in 10 cohorts of middle-aged men of the Seven Countries Study followed for 60 years to extinction. J Cardiovasc Dev Dis 2023; 10: 482. [CrossRef]
- Puddu PE, Menotti A. Heart diseases of uncertain etiology: a new definition of heart failure for epidemiological studies. J Cardiovasc Dev Dis 2023; 10: 132. [CrossRef]
- Jacobs DR Jr, Woo JG, Sinaiko AR, Daniels SR, Ikonen J, Juonala M, et al. Childhood cardiovascular risk factors and adult cardiovascular events. N Engl J Med 2022; 386: 1877-1888. [CrossRef]
Figure 1.
Lifelong Kaplan-Meier curves of CHD, stroke and HDUE until practical extinction of the 1712 men of the IRA cohort of whom 1708 were dead by 61 years.
Figure 1.
Lifelong Kaplan-Meier curves of CHD, stroke and HDUE until practical extinction of the 1712 men of the IRA cohort of whom 1708 were dead by 61 years.
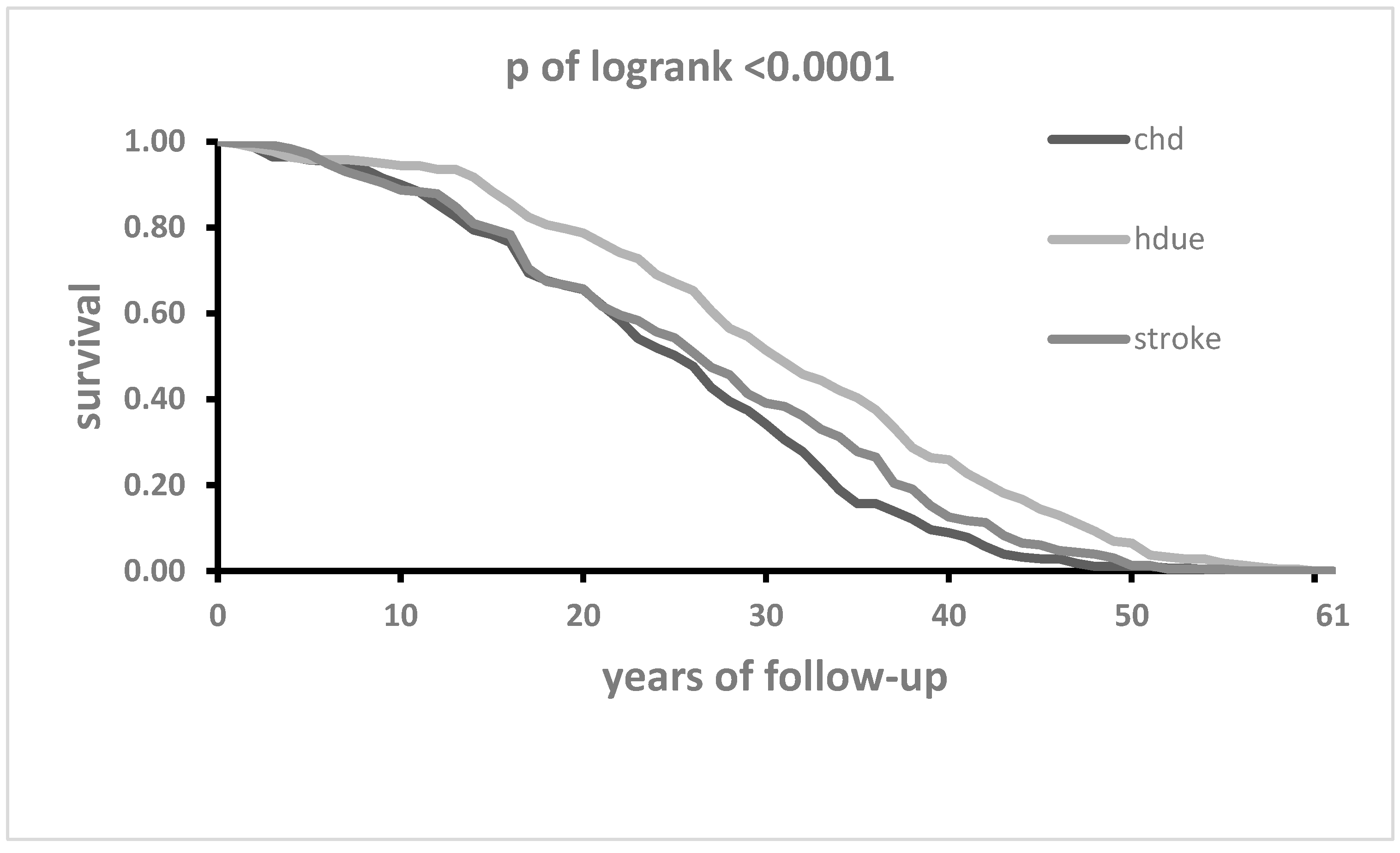
Figure 2.
Death rates from CHD, HDUE and stroke in 3 time-periods up to 61 years of follow-up.
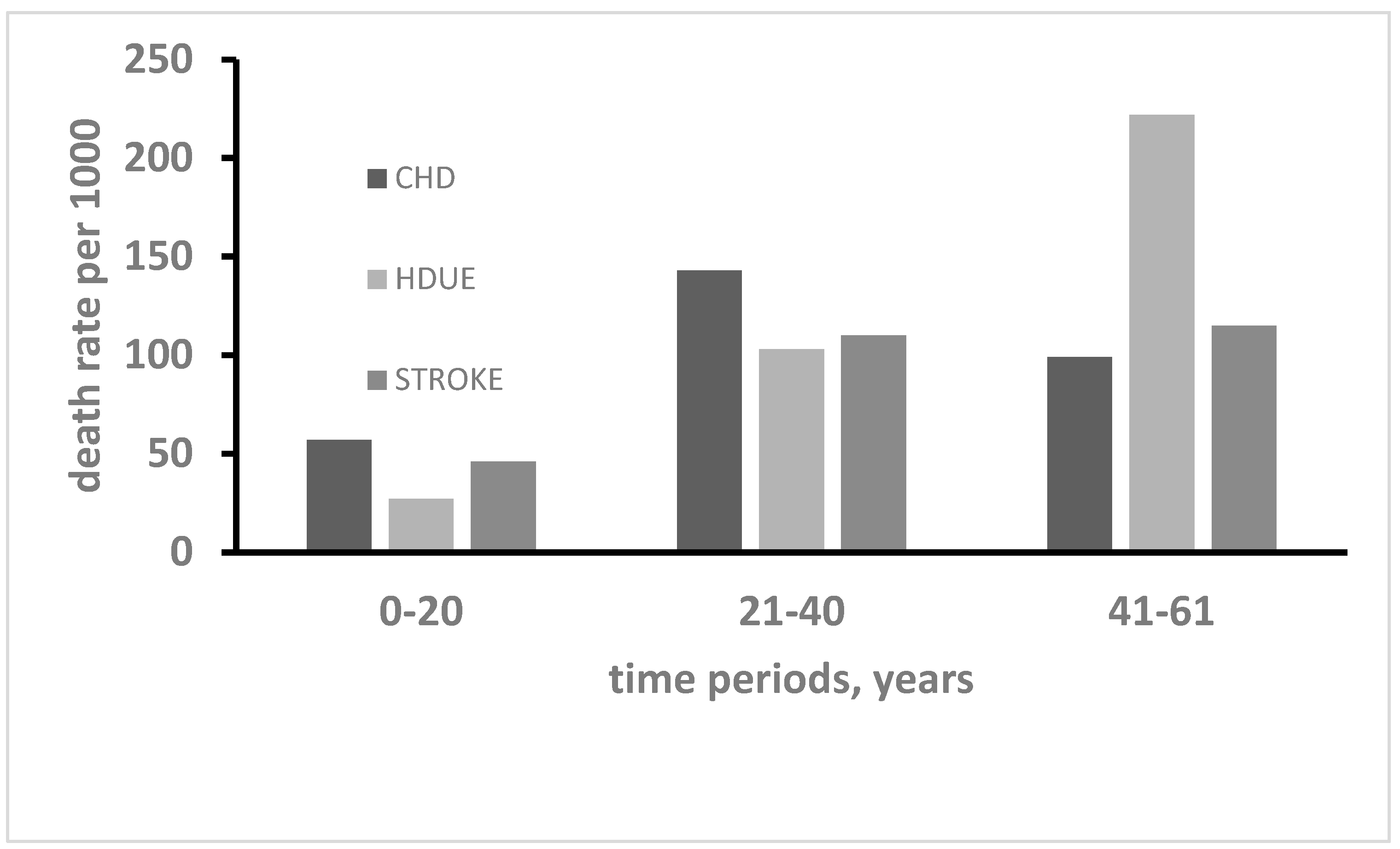
Table 1.
Death rates in 61 years from all-causes and selected CVD in 1712 men first examined in 1960.
Table 1.
Death rates in 61 years from all-causes and selected CVD in 1712 men first examined in 1960.
| Causes of death | N | Rate per 1000 |
Proportion % within selected groups of CVD |
|---|---|---|---|
| All causes | 1708 | 998 | ---- |
| All cardiovascular diseases CVD | 785 | 459 | ---- |
| Selected sub groups of CVD | |||
| Coronary heart disease | 281 | 164 | 38.7 |
| Stroke | 230 | 134 | 31.6 |
| Heart disease of uncertain etiology | 216 | 126 | 29.7 |
| Pool of selected groups of CVD | 727 | 425 | 100.0 |
Table 2.
Mean values at entry examination of selected risk factors distributed in the initial sample and in three classes of CVD mortality.
Table 2.
Mean values at entry examination of selected risk factors distributed in the initial sample and in three classes of CVD mortality.
| Risk Factor | Overall (N=1712) | CHD | Stroke | HDUE | P of ANOVA |
|---|---|---|---|---|---|
| Age, years | 49.1 (5.1) | 49.0 (5.1) | 49.7 (5.0) | 49.5 (5.2) | 0.4144 |
| Family heart attack (0-1), % (*) | 40.3 (1.8) | 40.9 (2.9) | 40.4 (3.2) | 39.4 (3.3) | 0.9380 (**) |
| Cigarettes, N/day | 8.7 (0.5) | 8.9 (9.4) | 7.4 (8.8) | 8.0 (8.9) | 0.1627 |
| Body mass index, kg/m2 | 25.2 (3.7) | 25.8 (3.7) | 25.3 (3.7) | 25.0 (3.7) | 0.0579 |
| Subscapular skinfold, mm | 11.8 (5.8) | 12.7 (6.2) | 12.1 (6.3) | 11.4 (5.7) | 0.0664 |
| Arm circumference, mm | 268.6 (23.6) | 270.0 (23.1) | 269.6 (23.6) | 268.7 (22.8) | 0.8503 |
| Systolic blood pressure, mmHg | 143.6 (21.0) | 146.4 (21.8) | 145.0 (21.9) | 142.7 (20.5) | 0.1638 |
| Heart rate, beats/min | 71.3 (12.9) | 71.7 (12.7) | 71.6 (12.4) | 68.4 (13.7) | 0.0075 |
| Vital capacity, L/m2 | 1.65 (0.24) | 1.63 (0.25) | 1.63 (0.23) | 1.67 (0.24) | 0.1736 |
| Serum cholesterol, mg/dl | 201.6 (40.8) | 209.6 (42.2) | 204.4 (38.8) | 198.0 (39.3) | 0.0066 |
| Urine glucose (0-1), % (*) | 5.1 (0.8) | 4.6 (1.3) | 6.1 (1.6) | 4.6 (1.4) | 0.7071 (**) |
| CVD prevalence (0-1), % (*) | 4.7 (0.8) | 4.6 (1.3) | 4.8 (1.4) | 4.6 (1.4) | 0.9958 (**) |
ANOVA across the three CVD mortality end-points; (*) Proportions % and (Standard error); (**) Chi squared test; Significance in bold.
Table 3.
Cox model for CHD deaths (N=281) in 61 years as a function of 12 risk factors.
| Variable | Delta | HR | 95% CI | P of coefficient |
|---|---|---|---|---|
| Age | 5 | 1.41 | 1.23 1.61 | <0.0001 |
| Family heart attack | 1 | 1.18 | 0.87 1.50 | 0.1814 |
| Cigarettes | 9 | 1.18 | 1.06 1.32 | 0.0034 |
| Body mass index | 4 | 1.16 | 0.91 1.48 | 0.2232 |
| Subscapular skinfold | 6 | 0.95 | 0.78 1.15 | 0.6067 |
| Arm circumference | 24 | 0.87 | 0.74 1.03 | 0.1135 |
| Systolic blood pressure | 20 | 1.36 | 1.20 1.54 | <0.0001 |
| Heart rate | 13 | 0.99 | 0.99 1.13 | 0.9396 |
| Vital capacity | 0.24 | 0.84 | 0.73 0.96 | 0.0094 |
| Serum cholesterol | 40 | 1.27 | 1.13 1.42 | <0.0001 |
| Urine glucose | 1 | 1.06 | 0.60 1.90 | 0.8335 |
| CVD prevalence | 1 | 1.50 | 0.85 2.64 | 0.1619 |
Units of measurement as from Table 2. HR = Hazard ratio; 95%CI = confidence intervals. Delta for computation of HR roughly corresponding to 1 standard deviation for continuous variables. Significance in bold.
Table 4.
Cox model for stroke deaths (N=230) in 61 years as a function of 12 risk factors.
| Variable | Delta | HR | 95% CI | P of coefficient |
|---|---|---|---|---|
| Age | 5 | 1.71 | 1.50 2.03 | <0.0001 |
| Family heart attack | 1 | 1.14 | 0.87 1.49 | 0.3323 |
| Cigarettes | 9 | 1.03 | 0.90 1.18 | 0.6414 |
| Body mass index | 4 | 0.95 | 0.72 1.26 | 0.7200 |
| Subscapular skinfold | 6 | 0.97 | 0.78 1.22 | 0.8092 |
| Arm circumference | 24 | 0.95 | 0.80 1.16 | 0.6730 |
| Systolic blood pressure | 20 | 1.28 | 1.10 1.48 | 0.0009 |
| Heart rate | 13 | 1.05 | 0.91 1.22 | 0.4740 |
| Vital capacity | 0.24 | 0.85 | 0.73 0.98 | 0.0306 |
| Serum cholesterol | 40 | 1.17 | 1.02 1.34 | 0.0203 |
| Urine glucose | 1 | 1.82 | 1.04 3.19 | 0.0370 |
| CVD prevalence | 1 | 1.51 | 0.81 2.81 | 0.1912 |
Units of measurement as from Table 2. HR = Hazard ratio; 95%CI = confidence intervals. Delta for computation of HR roughly corresponding to 1 standard deviation for continuous variables. Significance in bold.
Table 6.
Calibration of Cox models with proportion of total cases distributed in quintile classes of estimated risk (Q1, Q2, Q3, Q4, Q5), for 3 CVD end-points.
Table 6.
Calibration of Cox models with proportion of total cases distributed in quintile classes of estimated risk (Q1, Q2, Q3, Q4, Q5), for 3 CVD end-points.
| End-point | Q 1 | Q2 | Q3 | Q4 | Q5 | Ratio Q5/Q1 | P of chisquared |
|---|---|---|---|---|---|---|---|
| Coronary heart disease | 16.0 | 16.3 | 21.0 | 24.2 | 22.4 | 1.4 | 0.4298 |
| Stroke | 16.5 | 18.7 | 22.6 | 21.3 | 20.9 | 1.3 | 0.8498 |
| Heart disease of uncertain etiology | 19.0 | 17.1 | 18.0 | 21.8 | 24.1 | 1.3 | 0.8576 |
Table 7.
Mean level of baseline risk factors significantly predicting at least one CVD end-point in men who died from any CVD in subsequent time periods.
Table 7.
Mean level of baseline risk factors significantly predicting at least one CVD end-point in men who died from any CVD in subsequent time periods.
| Variable | Time period 1 Year 0 to 20 |
Time period 2 Year 21 to 40 |
Time period 3 Year 41 to 61 |
P of ANOVA | |||
|---|---|---|---|---|---|---|---|
| mean | SD | mean | SD | mean | SD | ||
| Age | 51.6 | 4.9 | 49.3 | 4.7 | 44.6 | 3.2 | <0.0001 |
| Cigarettes | 9.2 | 9.5 | 8.8 | 9.3 | 4.9 | 7.4 | <0.0001 |
| Systolic blood pressure | 155.9 | 25.6 | 141.8 | 17.4 | 134.1 | 15.5 | <0.0001 |
| Heart rate | 74.3 | 14.8 | 69.7 | 12.0 | 67.7 | 10.7 | <0.0001 |
| Vital capacity | 1.55 | 0.25 | 1.66 | 0.23 | 1.75 | 0.22 | <0.0001 |
| Serum cholesterol | 210.6 | 40.6 | 205.6 | 40.3 | 190.7 | 38.2 | <0.0001 |
| Urine glucose* | 7.3 | 2.1 | 4.5 | 1.2 | 1.7 | 1.2 | 0.0626 ** |
Unit of measurement as from Table 2; * proportion (%) and standard error; ** p of chi squared.
Table 8.
Fine-Gray models for the evaluation of competing risks of CHD versus other causes (all other than CHD) mortality as a function of 12 risk factors.
Table 8.
Fine-Gray models for the evaluation of competing risks of CHD versus other causes (all other than CHD) mortality as a function of 12 risk factors.
| CHD (as primary) versus OTHER CAUSES |
OTHER CAUSES (as primary) versus CHD |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk factor | coefficient | P value | HR | 95% CI | coefficient | P value | HR | 95% CI | t-test | |||
| Age | -0.0150 | 0.2390 | 0.93 | 0.82 | 1.05 | 0.0461 | <0.0001 | 1.26 | 1.19 | 1.34 | -4.31** | |
| Family heart attack | 0.1244 | 0.3102 | 1.13 | 0.89 | 1.44 | -0.0069 | 0.9044 | 0.99 | 0.89 | 1.11 | 0.97 | |
| Cigarettes | 0.0035 | 0.5592 | 1.03 | 0.93 | 1.15 | 0.0066 | 0.0258 | 1.06 | 1.01 | 1.12 | -0.46 | |
| BMI $ | 0.0210 | 0.5170 | 1.09 | 0.84 | 1.40 | 0.0052 | 0.7414 | 1.02 | 0.90 | 1.16 | 0.44 | |
| Subscapular skinfold | 0.0053 | 0.7582 | 1.03 | 0.84 | 1.26 | -0.0138 | 0.1012 | 0.92 | 0.83 | 1.02 | 1.00 | |
| Arm circumference | -0.0011 | 0.7486 | 0.97 | 0.83 | 1.15 | -0.0024 | 0.1488 | 0.94 | 0.87 | 1.02 | 0.34 | |
| Systolic blood pressure | 0.0063 | 0.0490 | 1.13 | 1.00 | 1.29 | 0.0014 | 0.4296 | 1.03 | 0.96 | 1.11 | 1.32 | |
| Heart rate | -0.0038 | 0.4354 | 0.95 | 0.84 | 1.08 | 0.0037 | 0.1444 | 1.05 | 0.98 | 1.12 | -137 | |
| Vital capacity | -0.2883 | 0.2984 | 0.93 | 0.82 | 1.06 | -0.1117 | 0.4124 | 0.97 | 0.91 | 1.02 | -0.57 | |
| Serum cholesterol | 0.0042 | 0.0042 | 1.18 | 1.05 | 1.33 | -0.0009 | 0.1972 | 0.96 | 0.91 | 1.02 | 3.13* | |
| Urine glucose | -0.0736 | 0.8104 | 0.93 | 0.51 | 1.70 | 0.1772 | 0.2342 | 1.19 | 0.89 | 1.60 | -0.74 | |
| CVD prevalnce | 0.0464 | 0.8776 | 1.05 | 0.58 | 1.89 | -0.0040 | 0.9840 | 1.00 | 0.70 | 1.41 | 0.15 | |
Units of measurement as from Table 2. HR: hazards ratios (with delta as used in Table 3, Table 4 and Table 5); t-test = test T between coefficients of the two models; $= corresponding coefficients in absence of subscapular skinfold and arm circumference, separately considered (10 degrees of freedom instead of 12) due to collinearities with BMI, were respectively: 0.02264 (p=0.160, HR 1.09, 95% CI 0.96-1.24) and -0.01991 (p=0.03, HR 0.92, 95% CI 0.86-0.99) whereas the results for the remaining covariates were globally unchanged. **P<0.0001; *P=0.0018.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



