
Submitted:
22 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Cervical cancer remains a major public health problem. Despite the screening programs, cervical cancer is the second most commonly diagnosed cancer. Most of the cases occur in less developed countries, and it is the third leading cause of cancer death among females. In 2000–2007, the five-year relative survival rate for European women diagnosed with cervical cancer was 62%.[1] Standard treatment for locally advanced cervical cancer reveals external beam radiotherapy (EBRT) with concurrent chemotherapy followed by image-guided adaptive brachytherapy (IGABT) boost [2, 3]. In the last years, the Gynaecological (GYN) working group composed of Group Européen de Curiethérapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) has developed new recommendations for the treatment of cervical cancer based on IGABT. The treatment plan includes 3-dimensional (3D) imaging based on magnetic resonance imaging (MRI) or computed tomography (CT), adaptive to the target volume and organ at risk [4–6]. The brachytherapy insertion is made under anaesthesia. At the time of the application insertion, the ultrasound is used to guide the dilatation of the uterine canal and assess the depth of the uterine cavity. In this paper, we review the data available in international literature about the use of ultrasound (US) in brachytherapy treatment of cervical cancer.
Keywords:
cervical cancer
; brachytherapy
; ultrasound
; image guided adaptive brachytherapy
1. Introduction
Brachytherapy was used for the first time in the treatment of gynaecological malignancies in 1960. Since then, brachytherapy has been constantly an integrated part of the cervical cancer treatment plan. Brachytherapy, following concurrent chemo radiotherapy, is an integral part of the standard of care for cervical cancer. Advances in the last decade have increased the dose to the target volume and limited the doses to the organs at risk (OAR), with the introduction of the dose volume histogram analyses. These developments have led to the improvement of the technique from 2-dimensional (2D) to 3-dimensional (3D) through IGABT based on MRI or CT. For many radiation oncologists around the word, IGABT represents the standard practice for cervical cancer, irrespective of the form of MRI or CT. The GYN GEC-ESTRO working group developed the concepts of target volume in the era of 3D and after that International Commission on Radiation Units and Measurements (ICRU) reported the recommendations and supported the implementation of the IGABT technique in many institutions. This technique has many benefits: the guided placement of the applicator, optimization of the treatment planning, without compromising target coverage, and decreasing the dose to OAR [4,5,6,7,8,9,10,11].
Outcomes data utilization of IGABT allows target volume dose escalation, whilst decreasing the dose to normal tissue. Doses over 80 Gy in a biologically equivalent dose of 2 Gy per fraction for D90 of high-risk clinical target volume (CTVHR) show a local control in the 90% range. In retro-EMBRANCE study which included 592 patients, the local control rate at 95% for a D90 to the CTVHR was over 92 Gy [4,9].
With the implementation and development of the image-guided adaptive brachytherapy techniques in cervical cancer patients, the application of radiation inserts was also reviewed. For the safety of the applicator insertion, transabdominal ultrasound (TAUS) is used. Ultrasound (US) is a method that allows guiding the dilatation of the uterine canal, measuring the depth of the uterine cavity and the safely placing the applicator.
TAUS is simple to use, not expensive, and achieved without great effort. TAUS gives treatment precision, reproducibility, and adaptability to each case. There are some brachytherapy planning systems that integrated US as the unique modality of imaging. US is used at the time of applicator insertion and at treatment planning for cervical cancer, prostate cancer, and anal canal cancer. It is also useful in placing brachytherapy catheters in skin cancer, breast cancer, and head and neck cancers.
Imaging advances such as 3D-US and contrast US are superior to traditional US, giving us greater accuracy of brachytherapy guidance. According to van Elburg [12], 3DTVUS imaging enhances the visualisation of tumours and vaginal walls during gynaecologic perineal template interstitial needle implantation. This imaging technique has been found to be effective in assessing implants in a surgical setting, based on feedback from primary users and a small group of initial patients.
Considering the current practice of the US in brachytherapy in various cancer sites, and the extreme situation of cervical cancer in Romania, which occupies the second place in Europe both as mortality and incidence rate [13], we conducted a review of international databases in order to find relevant material and evaluate the role of US in brachytherapy treatment cervical cancer. In Romania, the combination between the low level of knowledge about cervical cancer and specific preventive methods, the perceived cost of diagnostic and therapeutic procedures (despite the fact that in Romania access to healthcare is free and the state provides new drugs, therapies and screening measures through national programs free of charge [14,15,16,17,18,19,20,21]) and the non-functional national screening and HPV-vaccination programs leads to an extremely low number of women being screened or HPV-vaccinated [22]. This situation is well known and is responsible for the diagnosis of most cases in advanced stages [23] where radiotherapy plays a predominant role. Cervical cancer and other HPV-related diseases remain important health issues worldwide [24], determining the World Health Organization (WHO) to reiterate its recommendation for HPV vaccinations to be included in national immunization programs and for adequate screening programs.
2. Materials and Methods
In 27 July 2023, we conducted a survey of international data base PubMed for materials relevant to IGABT in cervical cancer. The advanced search function was used and the following combination of keywords/phrases and Boolean operators were used: (((image guided brachytherapy or image guided adaptive brachytherapy or ultrasound guided brachytherapy or transabdominal ultrasound guided brachytherapy or IGABT)) AND (cervical or cervix)) AND (tumour or tumour or malignancy or cancer). We placed no filters for language, type of research item, year of publication or text availability. The search returned 766 results, published between 1994 and 2023 – 29 presented case reports or series of cases, 93 presented data from clinical trial or studies, 6 were clinical guidelines or recommendations, and 115 were literature reviews, systematic reviews and meta-analyses. Other searches were conducted on 27 July 2023 and 14 December 2023 using the same parameters as before on www.sciencedirect.com (returned 4 results) and www.scopus.com (returned 583 results – 334 articles, 70 books or book chapters and 145 reviews).
3. Results
Brachytherapy is the radiotherapy technique that offers the most conformal dose distribution, through the applicator of the source in contact with the target volume. Brachytherapy has been for a very long time, before the development of the external radiation techniques and of surgical procedures, an important therapeutic for various deep-seated tumours of soft tissue, head and neck region or breast [25]. Although, the role brachytherapy occupies has slowly and steadily decreased over the years, it continues to play a key role in the treatment of cervical cancers. Given the current situation of cervical cancer in Romania [26], there is a renewed interest for brachytherapy and its easily affordable and available options.
The radiation method, first described in the early 1900s, was based on the approximation of target volume by using a regular shape and pre-calculated tabular data for the position of applicators, source strength and time of exposure. Although, an adequate radiation dose was delivered to the target volume, the organs at risk (OAR) were exposed to higher doses than necessary; the method had a limited planning possibility by usage of two-dimensional X-ray projection images which allowed for limited correction of source positioning [25]. Over the years, different predictive dosimetry systems for both interstitial and intracavitary brachytherapy were developed (Manchester, Manchester-Paterson-Parker, Quimby, Stockholm, Memorial, Fletcher and Paris), but the fundament was nothing more than clinical experience and simple dose calculation. These systems did not take into account tumour response to radiation and tumour volume extension and delineation, leading either to under dosing part of the target volume, or to a higher load on the surroundings OAR [27,28]. But even with all these limitations they constituted an important step forward towards standardizing brachytherapy treatments and provide a way of validating new advances in radiation therapy as they are introduced [29,30]. Among the technologies validated using historical dosimetry systems that provided huge improvements in the treatment especially for tumours requiring very high doses of radiation (like cervical or prostate cancers), we can name delivery systems such as after loads, applicator technology, 3-D visualization using modern imaging with 3D target volume determination and various computerized algorithms for dose calculation [25].
Advances in the last decade have increased the dose to the target volume and limited the doses to the organs at risk (OAR), with the introduction of the dose volume histogram analyses and the incorporation of various imaging techniques (magnetic resonance - MRI, computer tomography - CT, ultrasound - US and even Positron emission tomography) have led to the improvement of brachytherapy and the birth of IGABT and facilitated the transition between two-dimensional to three-dimensional [31]. This led to a better understanding of target volume topography [25] and the individualization of treatment planning [32,33,34,35] and reporting [36].
For locally advanced cervical cancer brachytherapy remains essential. In low-middle income countries (LMIC), where most of the burden associated with the disease occurs, the integration of the image modality for guidance of brachytherapy is extremely dependent of existing infrastructure and resources [37] (that do not always provide access to MRI or CT). In LMIC, X-rays remains the most used image-guidance modality for insertion of applicator and for ensuring the safe and correct placement of the applicator in the uterine canal. Although not credited with the same accuracy and characteristics as MRI, CT or other sophisticated imaging modalities (Table 1. Comparison between imaging modalities used for treatment planning in cervical cancer) and not yet recommended in guidelines for use in conformal planning [38,39], ultrasound guidance has a wider availability and can enhance cervical cancer treatment planning especially in its state-of-the-art form (3-dimensional contrast enhanced ultrasound) and improve outcomes [40], but does require specialized training [41,42].

Table 2.
Comparison between imaging modalities, used for treatment planning, in cervical cancer.
| Imaging modality | X-ray | Ultrasound | Tomography | Magnetic resonance | Positron emission tomography |
|---|---|---|---|---|---|
| Soft-tissue resolution | Poor | Good | Good@ | Excellent | Good |
| Geometric accuracy | Good | Good | Good* | Good# | Excellent |
| Image quality | Protocol dependent | Operator and protocol dependent | Sequence and protocol dependent | Sequence and protocol dependent& | Sequence and protocol dependent& |
| Artifacts | Metal | Multiple types and causes | Multiple types and causes | Multiple types and causes | Multiple types and causes |
| Slice orientation | Single planar | Multi planar | Trans axial | Multi planar | Trans axial |
| Usage in cervical cancer | Yes | Yes | Yes | Yes | Rarely used |
| Accurate visualization and reconstruction of brachytherapy applicators | Yes | Yes | Yes | Yes | Yes |
| Type of applicators | Metal or plastic with metal X-ray guides | Metal, plastic | Metal, Plastic | Metal%, Plastic | Metal, Plastic |
| Possibility of radiation dose calculation | No | NA | Yes | NA | Yes |
| Portability (potential for intraoperative use) | Yes | Yes | Sometimes available | Sometimes available | No |
| Time to obtain image | Seconds | Minutes | Seconds | Hour | Hours |
| Availability | Low | Low | Medium | High | High |
| Cost of equipment | Low | Low | High | High | High |
| Cost of scan | Low | Low | High | High | High |
@ can be enhanced by use of contrast; *but relies human factor for accurate focalization of region of interest; # the accuracy decreases away from the magnet core; & requires adequate patient cooperation; % limited types of metal due to MRI safety issues; NA – no data available, but studies are underway to produce electron density estimates for applications for radiotherapy.
Regarding the association between different methods of treatment monitoring, the existing imaging combination strategies primarily include MRI/CT, US/CT, MRI/US, and MRI/PET. The use of two imaging tools may be employed for the purpose of guiding applicator implantation, reconstructing applicators, contouring target and organs at risk (OAR), optimising dosage, evaluating prognosis, and more. This approach offers a more appropriate selection of imaging for brachytherapy, according to a study signed by Zhang [43].
4. Discussion
US in brachytherapy practice is an image guidance modality, with the following advantages: portable, cheap, and easy to use. The US allowed the precision, conformal, reproducible, and adaptive treatments.
The US gives information about the different echogenicity of the tissues, helping to delineate the tumours and to distinguish the surrounding normal tissues. In the new planning system brachytherapy used the US as the single method of imaging.
European Society for Radiotherapy and Oncology (ESTRO) acknowledges the importance of the US as an imaging method in the brachytherapy process for the next three steps: image-assisted temporary treatment planning, image-guided application, and image-assisted final treatment planning. Nevertheless, the use of imaging in the brachytherapy technique has four steps. To those recognized by ESTRO is added image image-assisted quality control.
The current use of the US in brachytherapy is in different types of cancer but with great interest in the incoming in gynaecological cancer [44]. Gynaecological brachytherapy used the US since 1970. The US was successfully integrated into the treatment planning for intracavitary application [44,45,46].
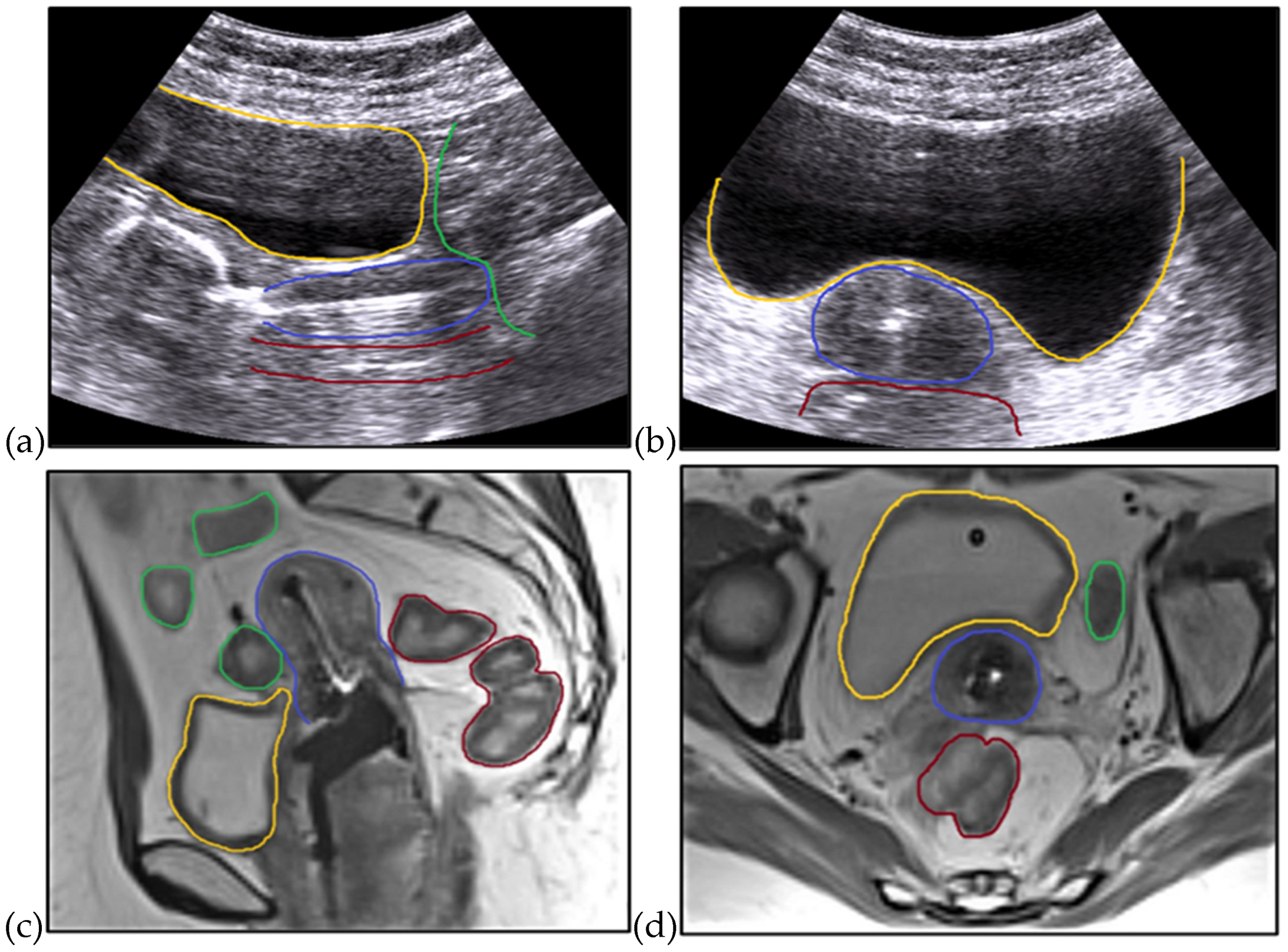
TAUS is used in real-time at the time of brachytherapy insertion for placement of uterine tandem and ovoids and allows the measurement of thickness. This method offers high probability and safety in the application of tandem and ovoids and provides information about placing the applicator in various sections (Figure 1).
The information provided through the US can be corroborated with orthogonal radiographs for the calculation of the dosimetry for the bladder and the real-time calculation of the surrounding organs.
Brachytherapy insertion consists of placing the applicator in the cervix and in the uterine cavity. When the application is made without guidance, a suboptimal application can occur.
This can lead to inadequate tumour coverage, poor local control, and higher doses to the organs at risk. It can also result a uterine perforation, which is not desirable. Although not a common practice, the US guidance of the brachytherapy application reduces these risks of improper placement. The radiation oncologist ensures that the uterus is not perforated. The resistance feels at the bottom of the uterus it is a landmark that the applicator/tandem is in the uterine cavity. The risk of uterine perforation at blind insertion reported in studies was 2–4%.
Following some studies, the further risk factors associated with inadequate tandem insertion have been reported: age over 60 years, history of surgery, cervix with distorted anatomy, retroverted uterus, and tumour growth. Moreover, after receiving initial pelvic and tumour irradiation with external beam radiation therapy (EBRT), the vagina and/or Endocervical canal might become completely blocked due to subsequent tissue fibrosis. Between 30% and 88% of women will have stenosis to some extent, with total stenosis occurring in up to 11% of patients. This makes it difficult and risky to reach the uterine canal for the insertion of brachytherapy applicators. Addley [47] used a combination of real-time ultrasonography and direct hysteroscopy guidance to successfully insert the IUBT applicator in a patient with stage IIa1 SCC cervix. This patient had previously had a failed insertion attempt because to severe narrowing of the Endocervical canal. The performed study further illustrated the safe navigation of post-radiation alterations, hence preventing morbidity caused by procedural problems and guaranteeing a satisfactory conclusion.
The real-time verification technique with the US is made at the time of the applicator insertion. TAUS helps to measure the size, shape, and thickness of the cervix, uterus, and tumour invasion. The guidance of the tandem placement with US reduces the risk of uterine perforation and increases the local control. Even if the utilization of this method gives benefits for application insertion in brachytherapy cervical cancer, in America is used only in 42%. In the developing countries, it is much less used [38,48,49,50,51,52].
The first experiences reported about the use of US in gynaecological treatment were in interstitial brachytherapy. The study included 12 patients and the authors related the utility of US identifying the target and the organs at risk [53].
Further another group reported the practice of transrectal ultrasound (TRUS) in placing the needles to the tumour volume, without perforating the rectum or bladder [54]. Investigators from other groups show the safety and usefulness of the placement of the needles at the brachytherapy insertion with the US.
Mahantshetty et al. reported their experience in the use of TAUS and they established a correspondence between the US and MRI on the treatment planning [55].
In a study of 292 cervical cancer patients, the US was used as the only method that assists the guidance and the treatment plan in intracavitary cervical brachytherapy. The five-year local control was 87.5% and no significant toxicity was reported [46].
The GEG-ESTRO claims that the US can be used for needle placement and the delineation of CTVHR. However, the US cannot be used safely in treatment planning in complicated interstitial brachytherapy. The Vienna team maintains that in the future TRUS could become a method of delineation of CTVHR [46].
Trans-cervical endo sonography (TRACE) is a recent concept described for use in pre-planning, real-time guidance, and treatment planning in cervical cancer patients treated with IGABT. This concept can bring additional information to existing imaging methods [56].
Brachytherapy is a radiotherapy technique that delivers a high dose of radiation, considered to be a rival of the new radiotherapy techniques such as intensity-modulated radiotherapy (IMRT) and stereotactic body radiotherapy. It can also be an alternative to external radiation.
In order to compete with modern radiotherapy techniques, delivering high doses of radiation in contact with the tumour, limiting the dose to surrounding organs, and limiting movement uncertainties, brachytherapy must be done according to recommendations using modern imaging in the guidance and application of brachytherapy.
However, there are several risks of the brachytherapy technique: the risk of moving the needles from the time of application to the time of treatment, the presence of metallic needles caused by visible CT, which is difficult to delimitate the tumour volume, and the risk of bleeding by perforating vessels near the tumour. To avoid the presence of artefacts caused by metal needles on CT, MRI compatible applicators and metal needles are recommended.
In thin patients, the bowel is lowered into the pelvis and it is often difficult to obtain a good image due to artefacts and it is more difficult to identify the cervix and uterus. In this situation, it is considered that the bladder is filled with serum so that there is no risk of damage to the bowel in case of uterine perforation.
During TAUS, in order to achieve the best possible image and to bring the uterus into a vertical position, the bladder is filled with physiological serum. The amount of serum introduced into the bladder can vary from 200 ml to 500 ml. In patients with a retroverted uterus, the bladder will be filled with a larger amount of serum 400-500 ml to bring the uterus into a vertical position. Depending on the position of the uterus identified in the US, the bladder filling is decided. The images obtained with the US are axial and sagittal sections.
As for obese patients, there are also limitations, and images offered by the US have reduced visibility. In the case of patient with a history of subtotal hysterectomy, it is important to obtain the best possible US image because there is a higher risk of perforation.
For interstitial BT, US guidance is important when inserting the needles at the level of the parameters but also paravaginal, avoiding pushing the needles into the bladder or bowel. Guiding the needles for interstitial brachytherapy at the parameters can also bring information, especially in the situation where the ureters are dilated, these are visible on ultrasound.
Several practitioners have studied the usefulness of the US for applicator insertion and brachytherapy treatment for cervical cancer, but there is no defined protocol in this regard.
The utility of TRUS for treatment planning in cervical cancer was evaluated by the Vienna working group. The images obtained with TRUS identify the target volume at the time of brachytherapy. They discovered that there are limitations regarding the focal distance and the visual field obtained with the endorectal probes [57,58].
In a research conducted by Hu [56], the efficacy and safety of ultrasound-CT guided 3D intracavitary and interstitial brachytherapy (US-CT-3D-IGBT) were investigated for the treatment of large cervical tumour cases accompanied by haemorrhage.
Pintakham [60] conducted a research to assess the dosimetry comparison of brachytherapy treatment planning using two different methods: a volume-based plan using computed tomography (CT) and a point-based plan utilising transabdominal ultrasonography (TAUS) in CT datasets for brachytherapy. The findings indicated that the point-based plan implemented by TAUS demonstrated superior values for both targets and organs at risk compared to the volume-based plan executed by CT. TAUS’s point-based strategy resulted in a proximity of D98 to HR-CTV.
Brachytherapy in prostate cancer used US imaging to plan treatment before application, in real-time at the time of needle insertion, correlated with CT planning, which led to the progress of the treatment planning of brachytherapy based on imaging. This concept was later used in other type of cancers. The US has been used in brachytherapy to guide the placement of needles and for the treatment plan when combined with other imaging modalities.
US imaging evolution such as 3D US, contrast-enhanced US, and high-frequency US entered practice with diagnostic, interventional, and therapeutic roles. In 3D interventional procedures, the US offers the benefit of precision and the possibility of visualization in several planes. The 3D US decreases the necessity of the operator and increases the reproducibility.
US imaging is not that hard to learn and handle. In an Indian study in which 2-month surgery residents were trained in US abdominal manoeuvring, compared to radiology residents they accumulated similar knowledge [57].
While there are standards for brachytherapy dosage and fractionation regimes, there is a scarcity of data on actual practice patterns. The objective of a recent research by Hsieh [62] to assess the current use of cervical cancer brachytherapy in the United States and its correlation with patient demographics and facility features.
The use of 3D US in cervical cancer as a unique practice for treatment planning is limited, due to difficult visualization of organs at risk and low reproducibility. There are still studies to validate some of these challenges in cervical cancer and in other types of cancer. Given the progress made in prostate cancer, scientific advances will overcome these technical limitations [58].
The use of 3D printing is viable in brachytherapy and tele therapy for both electron and photon treatments due to the enhanced treatment delivery quality resulting from higher dose administration to target volumes. The previous research signed by Lee [64] highlighted the possibility of decreasing the need for repeat computed tomography (re-CT) and successfully achieved time efficiency for both patients and oncologists.
Another important factor in the discussion about brachytherapy is its non-uniform use, influenced by various factors. Kumar’s research [65] indicated that there is a noticeable decline in the use of brachytherapy (BT) for cervical cancer. This decline has resulted in a fall in both local control and overall survival rates. Furthermore, numerous national and state-based registries have found a significant discrepancy in both the availability of healthcare services and the use of BT boost among patients with cervical cancer in the United States.
Regarding the future perspectives in which concerns brachytherapy and cervical cancer, we mention the existence of two clinical trials. The first one [66] entitled “Phase 0 Clinical Trial of Molecular Biomarkers in Women With Uterine Cervix Cancer” is a phase 0 clinical trial investigating molecular biomarkers in women diagnosed with uterine cervix carcinoma. Women get standard radio-chemotherapy treatment followed by brachytherapy. Obtaining blood samples is necessary to identify the presence of deoxyribonucleotides, human papillomavirus DNA, and circulating tumour cells. Another research, entitled” Comparison of Clinical Response and Toxicity of Hypo-fractionated Chemo radiation With Standard Treatment in Patients with Uterine Cervix Cancer” is developed in the following scientific context: the treatment for uterine cervix cancer involves definitive therapy by the use of concurrent chemo radiation, which combines external beam irradiation and chemotherapy, followed by high dose rate brachytherapy. Therapy time may be decreased by raising the dosage per fraction of therapy which can minimize expenses and patient exposure. The study aims to establish the non-inferiority of hypo fractionated radiation in comparison to conventional treatment.
5. Conclusions
Brachytherapy is one of the most conformal radiotherapy techniques. With the implementation of the IGABT technique in the world, the use of US during applicator insertion has also developed, bringing multiple advantages and improving the quality of the implants. In terms of benefits, we mention: the precision of the brachytherapy insertion, the guidance of the dilatation of the uterine canal, the measurement of the depth of the uterine cavity, noticing the changes in the position of the uterus, and, of course, the placement of the applicator and needles. The use of US in brachytherapy for cervical cancer can help define the treatment volumes and the treatment plan, especially in LMIC, where more sophisticated imaging guidance modalities are not always available to clinicians. In this review, we want to highlight the importance of practical use of the US in brachytherapy for cervical cancer, as an integrated part of a successful treatment. In the future, the IGABT technique will be extended to more institutions, and, therefore, incorporating the US in brachytherapy treatment for cervical cancer could improve the local control of the disease and also reduce toxicity.
Author Contributions
Conceptualization, E.M., L.S. and D.S.; methodology, E.M., E.C. and S-O.I.; software, D.L., M.A. and I.P.; validation, L.S., D.S., B.G. and S-O.I.; investigation, D.L., C.C. and M.A.; resources, C.C. and V.R.; writing—original draft preparation, E.M.; writing—review and editing, E.C., S-O.I. and V.R.; supervision, E.C. and L.S.; project administration, E.M. and L.S.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable since this study is a narrative review of literature. The photographs presented are part of the personal collection of Elena Manea.
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no conflict of interest.
References
- L. A. Torre, F. Bray, R. L. Siegel, J. Ferlay, J. Lortet-Tieulent, and A. Jemal, “Global cancer statistics, 2012,” CA Cancer J Clin, vol. 65, no. 2, pp. 87–108, Mar. 2015. [CrossRef]
- Z. Li, S. Yang, L. Liu, and S. Han, “A comparison of concurrent chemoradiotherapy and radiotherapy in Chinese patients with locally advanced cervical carcinoma: a multi-center study,” Radiat Oncol, vol. 9, no. 1, Sep. 2014. [CrossRef]
- H. Lukka et al., “Concurrent cisplatin-based chemotherapy plus radiotherapy for cervical cancer - A meta-analysis,” Clin Oncol, vol. 14, no. 3, pp. 203–212, 2002. [CrossRef]
- K. Tanderup, P. J. Eifel, C. M. Yashar, R. Pötter, and P. W. Grigsby, “Curative radiation therapy for locally advanced cervical cancer: Brachytherapy is NOT optional,” International Journal of Radiation Oncology Biology Physics, vol. 88, no. 3. Elsevier Inc., pp. 537–539, Mar. 01, 2014. [CrossRef]
- R. Pötter et al., “Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer,” Radiotherapy and Oncology, vol. 100, no. 1, p. 116, Jul. 2011. [CrossRef]
- C. Haie-Meder et al., “Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV,” Radiotherapy and Oncology, vol. 74, no. 3, pp. 235–245, Mar. 2005. [CrossRef]
- T. P. Hellebust et al., “Recommendations from Gynaecological (GYN) GEC-ESTRO working group: Considerations and pitfalls in commissioning and applicator reconstruction in 3D image-based treatment planning of cervix cancer brachytherapy,” Radiotherapy and Oncology, vol. 96, no. 2, pp. 153–160, Aug. 2010. [CrossRef]
- A. N. Viswanathan et al., “American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part II: High-dose-rate brachytherapy,” Brachytherapy, vol. 11, no. 1, pp. 47–52, Jan. 2012. [CrossRef]
- J. C. A. Dimopoulos et al., “Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV) - Basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy,” Radiotherapy & Oncology, 2012.
- R. Pötter et al., “Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy - 3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology,” Radiotherapy and Oncology, vol. 78, no. 1, pp. 67–77, Jan. 2006. [CrossRef]
- K. Tanderup et al., “Image guided intensity modulated External beam radiochemotherapy and MRI based adaptive BRAchytherapy in locally advanced CErvical cancer EMBRACE-II,” 2015. Accessed: Oct. 27, 2022. [Online]. Available: https://www.embracestudy.dk/UserUpload/PublicDocuments/EMBRACE II Protocol.pdf.
- D. Van Elburg et al., “Clinical implementation of 3D transvaginal ultrasound for intraoperative guidance of needle implant in template interstitial gynecologic high-dose-rate brachytherapy,” Brachytherapy, Nov. 2023. [CrossRef]
- World Health Organization, “Cancer Today.” Accessed: Jun. 05, 2023. [Online]. Available: https://gco.iarc.fr/today/home.
- M. Gherghe et al., “Quantitative Analysis of SPECT-CT Data in Metastatic Breast Cancer Patients—The Clinical Significance,” Cancers (Basel), vol. 14, no. 2, Jan. 2022. [CrossRef]
- Tr. Pãtrascu, H. Doran, E. Catrina, O. Mihalache, D. Degeratu, and G. Predescu, “Tumori sincrone ale tractului digestiv,” Chirurgia (Bucur), vol. 0, no. 1, Feb. 2010.
- C. Cirimbei, V. Rotaru, E. Chitoran, and S. Cirimbei, “Laparoscopic Approach in Abdominal Oncologic Pathology, Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25-27 September 2018,” Proceedings of the 35th Balkan Medical Week, Athens, Greece. Accessed: Jul. 20, 2023. [Online]. Available: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700043.
- V. Rotaru, E. Chitoran, C. Cirimbei, S. Cirimbei, and L. Simion, “Preservation of Sensory Nerves During Axillary Lymphadenectomy, Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25-27 September 2018,” Proceedings of the 35th Balkan Medical Week, Athens, Greece. Accessed: Jul. 20, 2023. [Online]. Available: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700045.
- L. Simion et al., “Simultaneous Approach Of Colo-Rectal And Hepatic Lesions In Colo-Rectal Cancers With Liver Metastasis - A Single Oncological Center Overview,” Chirurgia (Bucur), vol. 118, no. 3, 2023.
- L. Simion et al., “Indocyanine Green (ICG) and Colorectal Surgery: A Literature Review on Qualitative and Quantitative Methods of Usage,” Medicina (B Aires), vol. 59, no. 9, p. 1530, Aug. 2023. [CrossRef]
- L. Simion et al., “Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis,” Diagnostics, vol. 13, no. 6. MDPI, Mar. 01, 2023. [CrossRef]
- L. Simion et al., “Breast Reconstruction Following Mastectomy for Breast Cancer or Prophylactic Mastectomy-Therapeutic Options and Results,” 2023. [CrossRef]
- L. Simion et al., “A Decade of Therapeutic Challenges in Synchronous Gynecological Cancers from the Bucharest Oncological Institute,” Diagnostics, vol. 13, no. 12, p. 2069, Jun. 2023. [CrossRef]
- L. Simion et al., “Inequities in Cervical Cancer Screening and HPV Vaccination Programs and Their Impact on Incidence/Mortality Rates and the Severity of Disease in Romania,” Jul. 2023. [CrossRef]
- C. E. Condrat, L. Filip, M. Gherghe, D. Cretoiu, and N. Suciu, “Maternal HPV infection: Effects on pregnancy outcome,” Viruses, vol. 13, no. 12. MDPI, Dec. 01, 2021. [CrossRef]
- D. Berger, S. Van Dyk, L. Beaulieu, T. Major, and T. Kron, “Modern Tools for Modern Brachytherapy,” Clin Oncol, Aug. 2023. [CrossRef]
- L. Simion et al., “Inequities in Screening and HPV Vaccination Programs and Their Impact on Cervical Cancer Statistics in Romania,” 2023. [CrossRef]
- R. Vojtíšek, F. Mouryc, D. Čechová, R. Ciprová, J. Ferda, and J. Fínek, “[MRI based 3D brachytherapy planning of the cervical cancer - our experiences with the use of the uterovaginal Vienna Ring MR CT applicator],” Klin Onkol, vol. 27, no. 1, pp. 45–51, 2014. [CrossRef]
- C. Onal et al., “Comparison of conventional and CT-based planning for intracavitary brachytherapy for cervical cancer: target volume coverage and organs at risk doses,” J Exp Clin Cancer Res, vol. 28, no. 1, p. 95, 2009. [CrossRef]
- W. Y. Song, J. L. Robar, B. Morén, T. Larsson, Å. Carlsson Tedgren, and X. Jia, “Emerging technologies in brachytherapy,” Phys Med Biol, vol. 66, no. 23, p. 23TR01, Nov. 2021. [CrossRef]
- T. P. Hellebust, “Place of modern imaging in brachytherapy planning,” Cancer/Radiothérapie, vol. 22, no. 4, pp. 326–333, Jun. 2018. [CrossRef]
- INTERNATIONAL ATOMIC ENERGY AGENCY, “The Transition from 2-D Brachytherapy to 3-D High Dose Rate Brachytherapy,” The Transition from 2-D Brachytherapy to 3-D High Dose Rate Brachytherapy, pp. 1–33, 2015, Accessed: Aug. 28, 2023. [Online]. Available: https://www.iaea.org/publications/10705/the-transition-from-2-d-brachytherapy-to-3-d-high-dose-rate-brachytherapy.
- H. Zhang et al., “Clinical implementation, logistics and workflow guide for MRI image based interstitial HDR brachytherapy for gynecological cancers,” J Appl Clin Med Phys, vol. 20, no. 11, pp. 37–49, Nov. 2019. [CrossRef]
- A. Torresin et al., “Review of potential improvements using MRI in the radiotherapy workflow,” Z Med Phys, vol. 25, no. 3, pp. 210–220, Sep. 2015. [CrossRef]
- H. Kim et al., “Workflow and efficiency in MRI-based high-dose-rate brachytherapy for cervical cancer in a high-volume brachytherapy center,” Brachytherapy, vol. 17, no. 5, pp. 753–760, Sep. 2018. [CrossRef]
- M. Arenas et al., “Individualized 3D scanning and printing for non-melanoma skin cancer brachytherapy: A financial study for its integration into clinical workflow,” J Contemp Brachytherapy, vol. 9, no. 3, pp. 270–276, Jun. 2017. [CrossRef]
- ICRU, “Prescribing, Recording, and Reporting Brachytherapy for Cancer of the Cervix,” 10.1093/jicru_ndw027, vol. 13, no. 1–2, pp. 1-10, Apr. 2013. [CrossRef]
- M. Abdel-Wahab, E. Zubizarreta, A. Polo, and A. Meghzifene, “Improving Quality and Access to Radiation Therapy—An IAEA Perspective,” Semin Radiat Oncol, vol. 27, no. 2, pp. 109–117, Apr. 2017. [CrossRef]
- W. Small, J. B. Strauss, C. S. Hwang, L. Cohen, and J. Lurain, “Should Uterine Tandem Applicators Ever Be Placed Without Ultrasound Guidance? No: A Brief Report and Review of the Literature,” International Journal of Gynecologic Cancer, vol. 21, no. 5, pp. 941–944, Jul. 2011. [CrossRef]
- M. C. Jacobsen et al., “Contemporary image-guided cervical cancer brachytherapy: Consensus imaging recommendations from the Society of Abdominal Radiology and the American Brachytherapy Society,” Brachytherapy, vol. 21, no. 4, pp. 369–388, Jul. 2022. [CrossRef]
- S. van Dyk et al., “Clinical outcomes from an innovative protocol using serial ultrasound imaging and a single MR image to guide brachytherapy for locally advanced cervix cancer,” Brachytherapy, vol. 15, no. 6, pp. 817–824, Nov. 2016. [CrossRef]
- E. Tharavichitkul et al., “Intermediate-term results of trans-abdominal ultrasound (TAUS)-guided brachytherapy in cervical cancer,” Gynecol Oncol, vol. 148, no. 3, pp. 468–473, Mar. 2018. [CrossRef]
- S. van Dyk, S. Kondalsamy-Chennakesavan, M. Schneider, D. Bernshaw, and K. Narayan, “Assessing changes to the brachytherapy target for cervical cancer using a single MRI and serial ultrasound,” Brachytherapy, vol. 14, no. 6, pp. 889–897, Nov. 2015. [CrossRef]
- Z. Zhang, N. Zhang, and G. Cheng, “Application of three-dimensional multi-imaging combination in brachytherapy of cervical cancer,” Radiologia Medica, vol. 128, no. 5, pp. 588–600, May 2023. [CrossRef]
- R. Banerjee and M. Kamrava, “Brachytherapy in the treatment of cervical cancer: a review,” Int J Womens Health, pp. 6–555, 2014. [CrossRef]
- S. Van Dyk, K. Narayan, R. Fisher, and D. Bernshaw, “Conformal Brachytherapy Planning for Cervical Cancer Using Transabdominal Ultrasound,” Int J Radiat Oncol Biol Phys, vol. 75, no. 1, pp. 64–70, Sep. 2009. [CrossRef]
- K. Narayan, S. van Dyk, D. Bernshaw, P. Khaw, L. Mileshkin, and S. Kondalsamy-Chennakesavan, “Ultrasound guided conformal brachytherapy of cervix cancer: Survival, patterns of failure, and late complications,” J Gynecol Oncol, vol. 25, no. 3, pp. 206–213, 2014. [CrossRef]
- S. Addley, M. Persic, R. Kirke, and S. Abdul, “Combined direct hysteroscopic and real-time ultrasound guidance facilitating safe insertion of intra-uterine brachytherapy applicator for locally advanced cervical cancer with significant endocervical stenosis: A novel collaborative approach,” Gynecol Oncol Rep, vol. 47, Jun. 2023. [CrossRef]
- M. T. M. Davidson, J. Yuen, D. P. D’Souza, J. S. Radwan, J. A. Hammond, and D. L. Batchelar, “Optimization of high-dose-rate cervix brachytherapy applicator placement: The benefits of intraoperative ultrasound guidance,” Brachytherapy, vol. 7, no. 3, pp. 248–253, Jul. 2008. [CrossRef]
- A. N. Viswanathan and B. A. Erickson, “Three-Dimensional Imaging in Gynecologic Brachytherapy: A Survey of the American Brachytherapy Society,” Int J Radiat Oncol Biol Phys, vol. 76, no. 1, pp. 104–109, Jan. 2010. [CrossRef]
- R. Y. Kim, D. S. Levy, D. J. Brascho, and K. D. Hatch, “Uterine Perforation During Intracavitary Application Prognostic Significance in Carcinoma of the Cervix,” Radiology, vol. 147, pp. 249–251, 1983.
- M. D. Rotmensch, M. D. Waggoner, and M. D. Quiet, “Ultrasound Guidance for Placement of Difficult Intracavitary Implants,” Gynecol Oncol, vol. 54, no. 2, pp. 159–162, 1994. [CrossRef]
- I. Sahinler et al., “Tandem application with transvaginal ultrasound guidance,” Int J Radiat Oncol Biol Phys, vol. 59, no. 1, pp. 190–196, May 2004. [CrossRef]
- R. G. Stock, K. Chan, M. Terk, J. K. Dewyngaert, N. N. Stone, and P. Dotting, “A new technique for performing Syed-Neblett template interstitial implants for gynecologic malignancies using transrectal-ultrasound guidance,” Int J Radiat Oncol Biol Phys, vol. 37, no. 4, pp. 819–825, Mar. 1997. [CrossRef]
- D. N. Sharma, G. K. Rath, S. Thulkar, S. Kumar, V. Subramani, and P. K. Julka, “Use of transrectal ultrasound for high dose rate interstitial brachytherapy for patients of carcinoma of uterine cervix,” J Gynecol Oncol, vol. 21, no. 1, pp. 12–17, Mar. 2010. [CrossRef]
- U. Mahantshetty et al., “Trans-abdominal ultrasound (US) and magnetic resonance imaging (MRI) correlation for conformal intracavitary brachytherapy in carcinoma of the uterine cervix,” Radiotherapy and Oncology, vol. 102, no. 1, pp. 130–134, Jan. 2012. [CrossRef]
- P. Petric and C. Kirisits, “Potential role of TRAns Cervical Endosonography (TRACE) in brachytherapy of cervical cancer: Proof of concept,” J Contemp Brachytherapy, vol. 8, no. 3, pp. 215–220, 2016. [CrossRef]
- N. Nesvacil, M. P. Schmid, R. Pötter, G. Kronreif, and C. Kirisits, “Combining transrectal ultrasound and CT for image-guided adaptive brachytherapy of cervical cancer: Proof of concept,” Brachytherapy, vol. 15, no. 6, pp. 839–844, Nov. 2016. [CrossRef]
- S. van Dyk, P. Khaw, M. Y. Lin, D. Chang, and D. Bernshaw, “Ultrasound-guided Brachytherapy for Cervix Cancer,” Clin Oncol, vol. 33, no. 9, pp. e403–e411, Sep. 2021. [CrossRef]
- Y. Hu, Y. Jin, D. Wang, and Y. Luo, “Observation of hemostatic effectiveness and safety of ultrasound-CT guided 3D intracavitary and interstitial brachytherapy in the treatment of larger cervical cancer with bleeding: A retrospective study,” Medicine, vol. 102, no. 37, p. E34904, Sep. 2023. [CrossRef]
- C. Pintakham, E. Tharavichitkul, S. Wanwilairat, and W. Nobnop, “Comparative dosimetry of brachytherapy treatment planning between a volume-based plan by CT and a point-based plan by TAUS in CT datasets for brachytherapy,” J Radiother Pract, vol. 22, no. 2, Nov. 2023. [CrossRef]
- S. Sridhara, K. V. Rana, S. Naware, G. Singh, K. Nagare, and G. Gupta, “Ultrasound training in surgical residency: Is it feasible?,” Medical Journal of Dr. D.Y. Patil University, vol. 7, no. 3, pp. 284–288, May 2014. [CrossRef]
- K. Hsieh et al., “Dose and fractionation regimen for brachytherapy boost in cervical cancer in the US,” Gynecol Oncol, vol. 180, pp. 55–62, Jan. 2024. [CrossRef]
- P. St-Amant, W. Foster, M. A. Froment, P. Noel, S. Aubin, and L. Beaulieu, “PD-0180: Use of 3D-ultrasound for cervical cancer brachytherapy: an imaging technique to improve contouring,” Radiotherapy and Oncology, vol. 115, p. S89, Apr. 2015. [CrossRef]
- W. Lee and 李蘊恩, “Implementation of 3D printing in photon, electron radiotherapy and brachytherapy,” 2023, Accessed: Dec. 15, 2023. [Online]. Available: http://hub.hku.hk/handle/10722/335584.
- R. Kumar et al., “Disparities in brachytherapy utilization in cervical cancer in the United States: A comprehensive literature review,” Gynecol Oncol, vol. 179, pp. 79–84, Dec. 2023. [CrossRef]
- “Study Details | Clinical Trial of Molecular Biomarkers in Women With Uterine Cervix Cancer | ClinicalTrials.gov.” Accessed: Dec. 15, 2023. [Online]. Available: https://www.clinicaltrials.gov/study/NCT05462951?cond=Cervical%20Cancer&intr=brachytherapy&rank=1.
Figure 1.
Example of a case where the Fletcher applicator was used. Sagittal (a) and axial (b) view with the applicator in the uterine canal on transabdominal ultrasound and sagittal (c) and axial (d) pelvic MRI. The general concepts that we have to take in consideration regarding the intracavitary brachytherapy insertion are demonstrated. It is beneficial to measure the uterine canal and limit the risk of perforation, especially when it comes to the organs at risk (a, b). The relation between the organs at risk can be identified more clearly on MRI images (c, d). Organs at risk are: bladder (yellow), rectum (brown) bowel (green). During brachytherapy insertion, the bladder is filled with 400 ml of serum to bring the uterus (blue) in a vertical position (a, b), while at MRI, the bladder is filled with 50 ml of serum (c, d). The applicator is fixed using vaginal gauze packing.
Figure 1.
Example of a case where the Fletcher applicator was used. Sagittal (a) and axial (b) view with the applicator in the uterine canal on transabdominal ultrasound and sagittal (c) and axial (d) pelvic MRI. The general concepts that we have to take in consideration regarding the intracavitary brachytherapy insertion are demonstrated. It is beneficial to measure the uterine canal and limit the risk of perforation, especially when it comes to the organs at risk (a, b). The relation between the organs at risk can be identified more clearly on MRI images (c, d). Organs at risk are: bladder (yellow), rectum (brown) bowel (green). During brachytherapy insertion, the bladder is filled with 400 ml of serum to bring the uterus (blue) in a vertical position (a, b), while at MRI, the bladder is filled with 50 ml of serum (c, d). The applicator is fixed using vaginal gauze packing.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



