
Submitted:
20 December 2023
Posted:
25 December 2023
You are already at the latest version
Abstract
Cancer patients undergoing major interventions face numerous challenges, including the adverse effects of cancer and the side effects of treatment. Cancer rehabilitation is vital in ensuring cancer patients have the support they need to maximise treatment outcomes and minimise treatment-related side effects and symptoms. The Active Together service is a multi-modal rehabilitation service designed to address critical support gaps for cancer patients. The service is located and provided in Sheffield, UK, an area with higher cancer incidence and mortality rates than the national average. The service aligns with local and regional cancer care objectives and aims to improve clinical and quality of life outcomes of cancer patients by using lifestyle behaviour change techniques to address their physical, nutritional, and psychological needs. This paper describes the design and initial implementation of the Active Together service, highlighting its potential to support and benefit cancer patients.
Keywords:
Exercise prescription
; exercise
; physical activity
; psychology
; nutrition
; cancer
; oncology
; rehabilitation
; prehabilitation
; barriers
Introduction
Cancer rehabilitation (including prehabilitation) is central to high-quality cancer care 1. It enables patients to prepare well for treatment, maximise outcomes from treatment, and minimise treatment-related side effects and symptoms 1 leading to enhanced quality of life. The demand for rehabilitation services will continue to grow as the population ages and more people are diagnosed and survive cancer 2. As cancer transitions from a terminal disease to a long-term health condition 3, there is a need for lifestyle support through cancer rehabilitation services (including prehabilitation) to be integrated into the cancer care continuum 4.
Within the growing population of cancer survivors, two significant health concerns exist. The first is the concern regarding cancer recurrence and mortality. The second is the persistent adverse effects of cancer and its treatment 5. There is increasing evidence that physical activity, psychological, and nutritional state are related to prognosis and survival after cancer 6. Observational studies have indicated that insufficient physical activity and poor nutrition are associated with disease-related outcomes such as recurrence, death from cancer, and overall mortality 7,8. Evidence now highlights that regular exercise and a healthy diet before, during and after treatment decreases length of stay, the severity of treatment-related adverse side effects and is associated with a reduced risk of cancer recurrence and comorbid conditions such as cardiovascular disease and diabetes 9. Meeting the physical activity guidelines following a cancer diagnosis is associated with a 21-35% lower risk of cancer recurrence, a 28-44% reduced risk of cancer-specific mortality and a 25-48% reduced risk of all-cause mortality 10.
Multi-Modal Cancer Rehabilitation
Rehabilitation was cited as a central element of cancer care and a vital theme of the Achieving World-Class Outcomes Strategy 11. The NHS Long Term Plan states the need to provide cancer patients with personalised care, including needs assessment, a care plan and health and well-being information and support 12. However, rehabilitation (including prehabilitation) is not routinely offered to cancer patients.
Numerous attempts have been made to define “cancer rehabilitation” 13. Herbert Dietz classified cancer rehabilitation into four categories that align with the different stages of the cancer journey: 1) preventative, 2) restorative, 3) supportive, and 4) palliative 14. More recently, Silver and colleagues defined cancer rehabilitation as “medical care that should be integrated throughout the oncology care continuum and delivered by trained rehabilitation professionals who have it within their scope of practice to diagnose and treat patients’ physical, psychological and cognitive impairments to maintain or restore function, reduce symptom burden, maximise independence and improve quality of life in this medically complex population” 13.
The volume of cancer rehabilitation studies has grown substantially over the last two decades 15. However, the availability of rehabilitation services for cancer patients remains minimal in many countries 1,16,17. Only 1 in 200 cancer patients is estimated to have access to cancer rehabilitation services 18. Just 9% of hospitals in the United Kingdom, 6% in Canada, 19% in Australia, and 1% of hospitals in the United States offer exercise-based cancer rehabilitation services 18.
One of the critical barriers to the routine provision of cancer rehabilitation is the lack of funding, and where funding is available, it is often short-term and reliant on charitable organisations 1. Multi-centre trials 19 and services 20 evaluating prehabilitation and rehabilitation have begun in the UK. These programmes aim to assess cancer rehabilitation on a large scale as part of accepted clinical practice in the NHS 20. This paper describes the development of a multi-modal cancer rehabilitation (including prehabilitation) service in Sheffield, UK and the approach to embedding it within routine clinical practice.
The Cancer Landscape in Sheffield
South Yorkshire (Sheffield, Rotherham, Barnsley, and Doncaster) has a catchment population of approximately 1.4 million people, with over 580,000 residing in Sheffield. There are over 8,000 new cancer diagnoses per year in South Yorkshire, and in Sheffield alone, 3,038 new diagnoses per year 21. South Yorkshire has a higher incidence (624 new cancer diagnoses for every 100,000 people per year) 21 of cancer and higher cancer mortality rates (270 people in every 100,000 died from cancer each year) than the national average 21 with similar one-year survival rates (71.5% compared to the national average of 72.3%) 22. Sheffield has one of only four dedicated cancer centres in England with a world-leading reputation as a centre of excellence in cancer treatment, care and pioneering services for patients with late treatment consequences. Patients across South Yorkshire and North Derbyshire receive oncological care from Weston Park Cancer Centre, part of Sheffield Teaching Hospitals (the primary provider of acute cancer services for the South Yorkshire region). Cancer services and pathways are organised through the local Cancer Alliance, part of the recently established South Yorkshire (SY) Integrated Care Board (ICB). The ICB aims to integrate provision of health services across different organisations, including hospitals and community-based services, physical and mental health, and health and social care 23. The SY and Bassetlaw (SYB)Cancer Alliance is one of 19 alliances across England. The SYB Cancer Alliance is responsible for coordinating and delivering key national and regional cancer priorities as part of the ICB. These priorities arose from the Cancer Taskforce’s recommendations11 and were drawn from health inequalities data for the geographical population. Despite the infrastructure in SYB, historically, people with a cancer diagnosis had no equitable access to rehabilitation services. The Active Together service aims to address this critical support gap, while aligning with the local and regional cancer care objectives of the SYB Cancer Alliance.
Development of the Active Together Service
The Active Together service has been co-produced by cancer patients, clinical and professional stakeholders, and academics over a 2-year period. The service has also been informed by our previous work in cancer rehabilitation 24,25, where we identified the critical factors needed to create a model of exercise support for cancer patients 26,27. These include time during consultations to discuss rehabilitation, sufficient knowledge of the benefits of rehabilitation for cancer patients, and trust in the services that professionals refer patients to 26-28. We have also discussed the challenges that services face in terms of the financial sustainability of services29.
The programme of co-production involved meaningful and extensive consultation with patients, health professionals, professional leaders, commissioners, and academic experts to consider what a rehabilitation (including prehabilitation) service could look like, how to shape it to meet the contextual needs of Sheffield and what elements are crucial in delivering an impactful and sustainable service. Error! Reference source not found. displays the different groups and professional roles that engaged in the co-production process.

Table 1.
Professional roles involved in the development discussions.
| Professional role category 1 (clinical) | Number |
|---|---|
| Anaesthetist | 4 |
| Surgeon | 6 |
| Clinical nurse specialist | 4 |
| Oncologist | 4 |
| Exercise medicine consultant | 2 |
| Physiotherapist | 5 |
| Occupational therapist | 1 |
| Dietitian | 4 |
| Clinical psychologist | 3 |
| Total | 29 |
| Professional role category 2 (non clinical) | |
| Researcher | 2 |
| Fitness professional | 3 |
| Charitable sector (Cancer Support Centre, Cavendish Centre) | 2 |
| Other (cancer alliance, prehabilitation lead) | 4 |
| Total | 11 |
In total, 40 professionals supported the design process. Patient and professional groups and leaders communicated that the critical components of rehabilitation services included accessibility, safety, location, expertise, and capacity. The engagement of clinical teams across tumour groups was also deemed essential to foster buy-in from the programme's start. One key finding was the range of expertise required to deliver an effective multi-modal rehabilitation (including prehabilitation) programme. However, there were insufficient levels of allied health professional (AHP) capacity within existing teams (i.e., physiotherapists, occupational therapists, dietitians) to deliver a high-quality service. This was also the case for clinical psychologists and exercise professionals. Therefore, additional staff would need to be funded, recruited, and trained.
Patients should be at the centre of any discussions about their care 30, and so we ensured meaningful engagement was prioritised with patients throughout the design process. We held informal patient discussion groups to understand ‘what mattered most’ to patients and included patients in our project steering group. We held co-design sessions where prompts and service prototypes were used to tease out key service design features. We also created patient personas using insight from patient narratives to help guide service design. Personas create a shared and persistent view of the potential user, which can be referred to when making design decisions 31. The personas were particularly valuable in ensuring the service did not exacerbate existing inequalities. In total, 18 cancer patients supported the design process.
The Content of the Active Together Service
Active Together is an evidence-based, person-centred, multi-modal rehabilitation (including prehabilitation) service for people with a cancer diagnosis. Active Together provides support that spans the rehabilitation continuum and covers preventive rehabilitation (prehabilitation) following diagnosis, maintenance rehabilitation (during treatment), restorative (immediately post-treatment) and supportive rehabilitation (after treatment and discharge). The service aims to improve patient, clinical and patient-reported outcomes such as fatigue, physical fitness before surgery, treatment-related side effects, treatment tolerance, postoperative complications, survival rates, and quality of life.
Referral
All patients with a primary diagnosis of lung, colorectal, or upper gastrointestinal (UGI) cancer, aged ≥18 years and scheduled for curative treatment in Sheffield, are referred to Active Together following diagnosis. Referrals are completed by HCPs (i.e., oncologists, cancer nurse specialists, and AHPs) from cancer services at STH. HCPs have previously identified the time taken to complete referral processes for services as a potential barrier to engagement 26. Therefore, the Active Together service's referral process is deliberately simple, making the process easier for HCPs and ensuring the patient can access support quickly. Once a referral has been made, a member of the Active Together team contacts the patient by telephone within 48 hours and books the patient an initial assessment with a physiotherapist. This appointment will occur within seven days to both maximise the prehabilitation window and lower the risk of patient disengagement. Behaviour change principles underpin the initial contact telephone call with the patient and follow an ‘ask, advise, assist’ structure 32. The consultation provides an opportunity to explore with the patient their attitude, motivation, and understanding of the benefits of engaging in the service. It is also an opportunity to empower patient choice, enhance patient control to enable patient action 32.
The Initial Patient Needs’ Assessment
Patients attend an initial assessment with a specialist physiotherapist at Sheffield Hallam University’s Advanced Wellbeing Research Centre (AWRC) or at combined health and physical activity centres in Sheffield (i.e., Move More Centres discussed below). During this initial assessment, each patient completes physical, nutritional, and psychological screening assessments to determine the level of support required in each area. A personalised care plan is then offered per the universal, targeted, and specialised model advocated in the prehabilitation guidance33. Patients may have different levels of need for each element (i.e., physical, nutritional, and psychological).
A screening algorithm is used to determine the patient’s level of need for each rehabilitation element. The screening algorithm was developed through consultation with professionals in each area (physiotherapists, dietitians, and clinical psychologists) and academics. Additionally, recommendations from the existing literature on the screening process were incorporated, such as appropriate screening tools and how to determine the level of intervention required 6,33. Error! Reference source not found. shows the measures used to determine the patient’s level of need in each area. Each measure is entered into the screening algorithm, which determines the patient’s need using a traffic light system of green, indicating low complexity, amber indicating moderate complexity, and red indicating high complexity (Error! Reference source not found.). The patient's level of need identified during this initial assessment determines the support they will receive and who delivers it. The patient’s need is reassessed at key time points throughout the patient’s treatment pathway, and the support provided is adjusted accordingly.
Table 2.
Measures used to determine the patient’s level of need.
| Rehabilitation discipline | Measure |
|---|---|
| Physical activity needs criteria |
|
| Nutritional needs criteria |
|
| Psychological needs criteria |
|
Table 3.
Patient level of need matrix.
|
Patient need (Support provided) |
Intervention for each level of need (What?, Who?, Where?) |
|
Low complexity/need (Universal) Patient is healthy, with no additional physical, nutritional and/or psychological risk factors and requires no specialist support. |
What? |
Physical activity
| |
| Who? | |
Physical activity
| |
| Where? | |
| |
|
Moderate complexity/need (Targeted) Patient has some physical, nutritional and/or psychological risk factors and requires monitoring and some specialist support and monitoring. |
What? |
Physical activity
| |
| Who? | |
Physical activity
| |
| Where? | |
| |
|
High complexity/need (Specialist) Patient has significant physical, nutritional and/or psychological risk factors and requires frequent specialist support. |
What? |
Physical activity
Access to dietitian 1 x per week telephone or face-face) Psychological Alleviate distress from cancer and prepare patients psychologically for treatment | |
| Who? | |
Physical activity
| |
| Where? | |
|
Active Together Service Delivery Style and Behaviour Change Approach
Initiating and maintaining a healthier lifestyle is complicated, and patients often require support to succeed 34. The quality of this support can be enhanced by utilising behaviour change theory as part of the design of a complex intervention 35. Despite this, rarely do interventions in the cancer rehabilitation context adequately describe the content and approach to behaviour change as part of their intervention 36, with some exceptions 37,38. The behavioural change content of the Active Together programme, including the style of intervention delivery, has been developed using the behaviour change wheel39 to target specific behaviours and identify the most appropriate behaviour change techniques (BCT’s) to support lifestyle change amongst people with a cancer diagnosis.
As a key part of the behaviour change wheel, intervention functions were chosen to drive the desired changes 39. The Active Together service includes six intervention functions: education, training, persuasion, enablement, modelling, and environmental restructuring. These functions aim to empower patients and provide them with the necessary tools and support 39. For example, education is provided to patients about the benefits of regular exercise, nutrition, and psychological well-being. Training is provided to equip patients with the skills and knowledge necessary to perform the exercises effectively and safely. Enablement ensures patients can access necessary resources, such as exercise equipment or supportive programmes, to facilitate behaviour change.
After determining the appropriate intervention functions, the next step was selecting specific behaviour change techniques (BCTs) aligned with the chosen functions. The Behaviour Change Taxonomy 40 provides a comprehensive list of 93 BCTs, allowing the Active Together service to tailor its approach to suit patients' individual needs. For example, previous studies have demonstrated the importance of promoting self-efficacy as part of cancer recovery 41, which might include the promotion of mastery of behaviours such as exercise 42, setting achievable goals 43, and the inclusion of graded tasks, helping promote lifestyle change 38. Error! Reference source not found. shows the multi-modal BCTs used in the Active Together service aligned with the intervention functions, with examples describing how they are applied within the service.
To promote patient empowerment and control, all patient interactions within the Active Together service are i) delivered in a motivational interviewing (MI) style 44, adopting the principles of collaboration, compassion, evocation, and acceptance (known as the spirit of MI) and ii) incorporate the “What Matters to You?” approach, a method of implementing patient-centred care and shared decision-making 45. Practitioners who deliver the Active Together service have received training to deliver the intervention and associated behaviour change techniques, with competencies assessed via a process evaluation described in a forthcoming publication.
Table 4.
Multi-modal behaviour change techniques used in Active Together aligned with intervention functions.
Table 4.
Multi-modal behaviour change techniques used in Active Together aligned with intervention functions.
| Intervention function | Behaviour Change Technique (BCT no. (BCTTv1)) | Example of application within the multi-modal Active Together service |
|---|---|---|
| Education | Information about emotional consequences (5.6) |
|
| Feedback on behaviour (2.2) |
|
|
| Self-monitoring of behaviour (2.3) |
|
|
| Reduce negative emotions (11.2) |
|
|
| Information about health consequences (5.1) |
|
|
| Persuasion | Credible source (9.1) |
|
| Information about emotional consequences (5.6) |
|
|
| Feedback on behaviour (2.2) |
|
|
| Verbal persuasion and capability (15.1) |
|
|
| Training | Demonstration of the behaviour (6.1) |
|
| Instruction on how to perform a behaviour (4.1) |
|
|
| Feedback on behaviour (2.2) |
|
|
| Self-monitoring of behaviour (2.3) |
|
|
| Graded tasks (8.7) |
|
|
| Behavioural practice/rehearsal (8.1) |
|
|
| Biofeedback (2.6) |
|
|
| Environmental restructuring | Adding objects to the environment (12.5) |
|
| Reduce negative emotions (11.2) |
|
|
| Modelling | Demonstration of the behaviour (6.1) |
|
| Enablement | Goal setting (behaviour) (1.1) |
|
| Goal setting (outcome) (1.3) |
|
|
| Adding objects to the environment (12.5) |
|
|
| Problem-solving (1.2) |
|
|
| Action planning (1.4) |
|
|
| Self-monitoring of behaviour (2.3) |
|
|
| Generalisation of target behaviour (8.6) |
|
|
| Review behaviour goal(s) (1.5) |
|
|
| Review outcome goal(s) (1.7) |
|
|
| Social support (emotional) (3.3) |
|
Phases of the Rehabilitation Continuum
Phase 1: Prehabilitation
Cancer prehabilitation is a process on the continuum of care that occurs between the time of cancer diagnosis and the beginning of acute treatment 46. Patients enter the Active Together service prehabilitation phase after the initial needs assessment. The duration of the prehabilitation phase will depend on how soon after diagnosis the patient enters the service and how long after diagnosis the patient begins their acute cancer treatment. As a result, the degree to which a patient's physical and psychological health can be improved before the start of treatment will vary between individuals. Even in cases where the prehabilitation phase is very short (≤2 weeks), it is hoped that the advice and support provided during the prehabilitation phase will bring about changes in behaviour that can be continued during and after treatment, enabling people to live well beyond their treatment 33.
To reduce the risk of patients contracting COVID-19, adaptations to programmes and procedures are made in line with NHS COVID and infection control policies at the time. Patients are also given guidance and nutritional supplements to support them from a dietetic perspective, as well as access to paper-based or online materials and regular phone calls with Active Together staff to support their psychological well-being.
Phase 2: Maintenance Rehabilitation
During their acute treatment, patients enter the maintenance phase of Active Together. Although evidence suggests that physical activity is safe and feasible during cancer treatment47, participation has been shown to reduce significantly 48. During the maintenance phase, the service aims to support patients in maintaining their current physical, nutritional and psychological status as much as possible, supporting them to cope with any distress caused by cancer and its treatment whilst reducing the impact of any treatment-related side effects 47. The duration of the maintenance phase will depend on the type and duration of the treatment patients receive. Each patient receives a personalised exercise plan that can be completed in various settings depending on patient preference (gym setting, park or open space, at home). Active Together will maintain contact with them via telephone or text or email, depending on patient preference.
Phase 3: Restorative Rehabilitation
Following the patient's acute clinical treatment, they enter the restorative rehabilitation phase of the Active Together pathway. The restorative phase aims to support the patient in achieving optimal function following acute treatment49. At the start of the restorative phase, the patient repeats their initial needs assessment. The outcome of this review determines the patient’s prescribed exercise programme, nutrition plan, and psychological/behaviour change support strategies. The restorative rehabilitation phase can last up to 12 weeks following the end of the cancer treatment, depending on individual patient needs. The emphasis in the restorative phase is on helping individuals to return to their pre-treatment levels of health and well-being. This is achieved by setting functional goals involving strength and fitness within the context of what matters most to the patient (e.g., return to work or being able to play with their grandchildren).
Phase 4: Supportive Rehabilitation
The final phase of the Active Together programme is supportive rehabilitation, which aims to empower patients to achieve optimal health and well-being while living with long-term health conditions 50. The supportive phase can last up to 12 weeks, depending on individual patient needs and might involve referring patients to existing community exercise schemes such as walking groups. This phase culminates with a final assessment of patient outcomes, with the goal that the patient will have surpassed their pre-diagnosis fitness levels and can self-manage their physical, nutritional, and psychological well-being.
Active Together Workforce
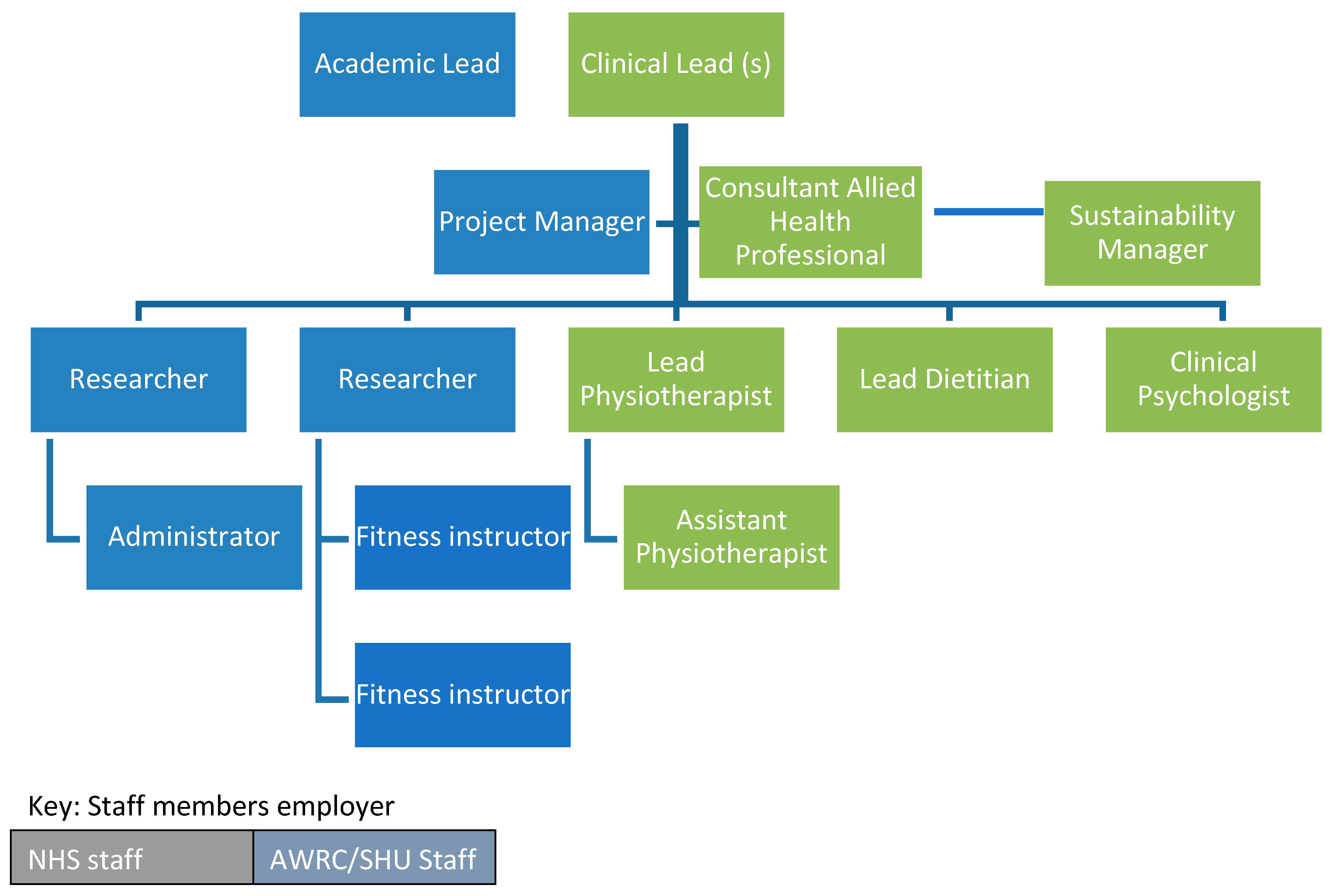
Rehabilitation (including prehabilitation) guidance from Macmillan Cancer Support states that rehabilitation should be delivered by a multidisciplinary team 33. Led by academics at Sheffield Hallam University and supported by professional leaders and clinicians at STH, funding was secured from Yorkshire Cancer Research to recruit the core Active Together team. This team consists of a consultant AHP, two physiotherapists, a dietitian, a clinical psychologist, two researchers with expertise in cancer exercise prescription and health behaviour change, two fitness instructors, a project manager, and an administrator. The team also includes a sustainability manager whose role is to explore the long-term future of the service (this role was funded by the SYB Cancer Alliance). Figure 1 shows the staffing structure of the Active Together service.
A clinical advisory group (CAG) was established to support Active Together's design, development, and ongoing implementation. The purpose of the CAG is to provide clinical leadership and governance oversight to ensure the successful delivery of Active Together. Responsibilities of the CAG include addressing service issues and risks and their resolution. The CAG comprises clinical leads from each cancer pathway, medical specialists from cancer services, including anaesthetists, surgeons, oncologists, senior nursing and AHP leads, academic leads for the programme and patient representatives.
The programme development stakeholder discussion groups stressed that any service must be delivered outside of the hospital setting. As part of the city-wide ‘Move More’ strategy 51, which adopts a whole system approach to increasing population physical activity, Sheffield has three Move More centres that co-locate health care services with exercise opportunities as part of a patient's recovery and rehabilitation 52,53. These centres currently deliver 100,000 clinical appointments per year, and the AWRC is a fourth centre taking the capacity up to 120,000. The AWRC and the three Move More centres include NHS clinical consulting rooms, education and training facilities and exercise facilities within a leisure and sports facility. Located across the city in communities of high economic disadvantage, the three centres enable the co-location of patients, researchers, clinicians, allied health professionals, and sports and exercise medicine specialists, providing an ideal hub and spoke model to deliver an equitable service for patients across the city 54.
Pilot Phase
Implementation of Active Together began in January 2022, and a pilot phase of the service was undertaken to set up, test and refine processes and procedures between February and June 2022. By June 2022, 112 patients receiving treatment in Sheffield had been referred to the service. Of those referred, 79 (71%) agreed to attend their initial assessment. Reasons for not wanting to attend include work commitments, travel arrangements to get to AWRC for assessment, not currently feeling psychologically ready, and patients feeling that they are already managing their health sufficiently. Of the 79 who attended their initial appointment, 100% engaged in the programme, suggesting initial acceptability for people diagnosed with cancer in Sheffield. Most referrals have been male (60%); the average age of the service users is 68 years. For upper GI, the mean age of patients entering the service is 65 years (range = 36 - 84 years), with 76% male. For colorectal patients, the mean age is 69 years (range = 35 - 89 years), with 53% male. For lung, the average age of patients entering the service is 69 years (range = 45 - 88 years), with 51% male. Initial participant feedback on the service has generated positive support for Active Together. Since completing the pilot phase in June 2022, the service has been running at full capacity. A robust process and outcome evaluation has been embedded into the service (described in a forthcoming publication), and the service will be continually refined based on the results.
Conclusion
Cancer rehabilitation (including prehabilitation) is vital in ensuring patients have the support they need to maximise treatment outcomes and side effects associated with cancer and its treatment. Although there is growing evidence of the importance of rehabilitation, the availability of services across England is sporadic 1. We identified an unmet need for cancer rehabilitation (including prehabilitation) in Sheffield and are addressing this by implementing the Active Together service. The service was co-designed using insight from previous research 26, service delivery 24, and robust stakeholder engagement, which prioritised the voice of patients. Robust evaluation is now needed to evidence the service’s acceptability and effectiveness.
Acknowledgements
The authors express gratitude to all people who have helped design and deliver the Active Together Service. We express thanks to the patients currently engaging in the service. The authors also thank Macmillan Cancer Support for funding the design phase of the service, and Yorkshire Cancer Research for funding the ongoing implementation and delivery of the service.
Conflict of Interest
The authors declare no competing interests.
References
- Integrated care system guidance for cancer rehabilitation A guide to reducing variation and improving outcomes in cancer rehabilitation in london. 2019.
- Rehabilitation. www.who.int Web site. Updated 2021. Accessed 01/07/, 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation.
- Pizzoli, S.F.M.; Renzi, C.; Arnaboldi, P.; Russell-Edu, W.; Pravettoni, G. From life-threatening to chronic disease: Is this the case of cancers? A systematic review. Cogent psychology 2019, 6(1). Available online: http://www.tandfonline.com/doi/abs/10.1080/23311908.2019.1577593. [CrossRef]
- Silver, J.K. Integrating rehabilitation into the cancer care continuum. PM & R 2017, 9 (9 Suppl 2), S291–S296. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1016/j.pmrj.2017.07.075. [CrossRef] [PubMed]
- Cormie, P.; Trevaskis, M.; Thornton-Benko, E.; Zopf, E.M. Exercise medicine in cancer care. Australian Journal of General Practice. 2020, 49, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Stout, N.L.; Brown, J.C.; Schwartz, A.L.; et al. An exercise oncology clinical pathway: Screening and referral for personalized interventions. Cancer. 2020, 126, 2750–2758. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Hamaue, Y.; Fukushima, T.; Tanaka, T.; Fu, J.B.; Nakano, J. Effect of exercise on mortality and recurrence in patients with cancer: A systematic review and meta-analysis. Integrative Cancer Therapies 2020, 19, 153473542091746–1534735420917462. Available online: https://journals.sagepub.com/doi/full/10.1177/1534735420917462. [CrossRef]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutrition Reviews. 2016, 74, 737–748. Available online: https://wwwncbinlmnihgov/pubmed/27864535. [CrossRef] [PubMed]
- Cormie, P.; Atkinson, M.; Bucci, L.; et al. Clinical oncology society of australia position statement on exercise in cancer care. Medical Journal of Australia. 2018, 209, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Trevaskis, M.; Thornton-Benko, E.; Zopf, E.M. Exercise medicine in cancer care. Australian journal of general practice. 2020, 49, 169–174. Available online: https://search.informit.org/documentSummary;dn=053010821856031;res=IELIAC. [CrossRef]
- Achieving world-class cancer outcomes: Taking the strategy forward.. 2016. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/05/cancer-strategy.pdf.
- NHS. The NHS long term plan.. 2019:61.
- Silver, J.K.; Raj, V.S.; Fu, J.B.; Wisotzky, E.M.; Smith, S.R.; Kirch, R.A. Cancer rehabilitation and palliative care: Critical components in the delivery of high-quality oncology services. Support Cancer Care 23, 3633–3643. [CrossRef]
- Dietz, J.H. Adaptive rehabilitation in cancer. Postgraduate medicine. 1980, 68, 145–153. Available online: http://wwwtandfonlinecom/doi/abs/101080/00325481198011715495. [CrossRef]
- Sleight, A.G.; Gerber, L.H.; Marshall, T.F. A systematic review of functional outcomes in cancer rehabilitation research. Archives of physical medicine and rehabilitation 2022. Available online: https://www.ncbi.nlm.nih.gov/pubmed/35104445. [CrossRef] [PubMed]
- Julie KSilver Nicole LStout Jack Fu Mandi Pratt-Chapman Pamela, J. Hajlock, Raman Sharma. The state of cancer rehabilitation in the united states. Journal of Cancer Rehabilitation 2018, 1, 1–8. Available online: https://doaj.org/article/51b8ea8ec4ac4199a905469fa35c5394.
- Smith, S.R.; Zheng, J.Y.; Silver, J.; Haig, A.J.; Cheville, A. Cancer rehabilitation as an essential component of quality care and survivorship from an international perspective. Disability and rehabilitation. 2020, 42, 8–13. Available online: https://wwwtandfonlinecom/doi/abs/101080/0963828820181514662. [CrossRef] [PubMed]
- Dennett, A.; Peiris, C.; Shields, N.; Taylor, N. From cancer rehabilitation to recreation: A coordinated approach to increasing physical activity. Physical Therapy. 2020, 100, 2049–2059. [Google Scholar] [CrossRef] [PubMed]
- Grimmett, C.; Bates, A.; West, M. SafeFit trial: Virtual clinics to deliver a multimodal intervention to improve psychological and physical well-being in people with cancer. protocol of a COVID-19 targeted non-randomised phase III trial. BMJ Open, 2021; 11. [Google Scholar] [CrossRef]
- Moore, J.; Merchant, Z.; Rowlinson, K. Implementing a system-wide cancer prehabilitation programme: The journey of greater manchester's ‘Prehab4cancer’. European journal of surgical oncology. 2021, 47, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Cancer incidence. Cancer Data Web site. Accessed 16/02/, 2022. Available online: https://www.cancerdata.nhs.uk/incidence_and_mortality.
- Local Cancer Intelligence. Survival in NHS sheffield CCG. Macmillan Cancer Support Web site. Available online: https://lci.macmillan.org.uk/England/03n/survival.
- Charles, A. Integrated care systems explained: Making sense of systems, places and neighbourhoods. Kings Fund. 2021.
- Humphreys, L.; Crank, H.; Frith, G.; Speake, H.; Reece, L.J. Bright spots, physical activity investments that work: Active everyday, sheffield’s physical activity service for all people living with and beyond cancer. British journal of sports medicine. 2019, 53, 837–838. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, L.; Frith, G.; Humphreys, H. Evaluation of a city-wide physical activity pathway for people affected by cancer: The active everyday service. Support Care Cancer. 2023, 31, 101. Available online: https://link.springer.com/article/10.1007/s00520-022-07560-y. [CrossRef] [PubMed]
- Humphreys, L.; Crank, H.; Dixey, J.; Greenfield, D.M. An integrated model of exercise support for people affected by cancer: Consensus through scoping. Disability and rehabilitation. 2020, 44, 1113–1122. Available online: http://wwwtandfonlinecom/doi/abs/101080/0963828820201795280. [CrossRef]
- Robinson, R.; Crank, H.; Humphreys, H.; Fisher, P.; Greenfield, D.M. Time to embed physical activity within usual care in cancer services: A qualitative study of cancer healthcare professionals’ views at a single centre in england. Disability and Rehabilitation 2022, 1. [Google Scholar] [CrossRef]
- Robinson, R.; Crank, H.; Humphreys, H.; Fisher, P.; Greenfield, D.M. Allied health professional's self-reported competences and confidence to deliver physical activity advice to cancer patients at a single centre in england. Disability and rehabilitation 2022, 1–7. Available online: https://www.tandfonline.com/doi/abs/10.1080/09638288.2022.2143580. [CrossRef] [PubMed]
- Dennett, A.M.; Zappa, B.; Wong, R.; Ting, S.B.; Williams, K.; Peiris, C.L. Bridging the gap: A pre-post feasibility study of embedding exercise therapy into a co-located cancer unit. Support Care Cancer. 2021, 29, 6701–6711 https://linkspringercom/article/101007/s00520. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.M.; Street, R.L. The values and value of patient-centered care. Annals of family medicine. 2011, 9, 100–103. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S1544170911600450. [CrossRef]
- Jacob, R.; Wong, M.L.; Hayhurst, C.; Watson, P.; Morrison, C. Designing services for frequent attenders to the emergency department: A characterisation of this population to inform service design. Clinical medicine (London, England). 2016, 16, 325–329. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27481374. [CrossRef] [PubMed]
- Webb, J.; Foster, J.; Poulter, E. Increasing the frequency of physical activity very brief advice for cancer patients. development of an intervention using the behaviour change wheel. Public Health. 2016, 133, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Macmillan Cancer Support, Royal College of Anaesthetists, National Institute for Health Research. Principles and guidance for prehabilitation within the management and support of people with cancer.. 2019.
- Ormel, H.L.; van der Schoot, G.G.F.; Sluiter, W.J.; Jalving, M.; Gietema, J.A.; Walenkamp, A.M.E. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psycho-Oncology. 2018, 27, 713–724. Available online: https://www.narcis.nl/publication/RecordID/oai:pure.rug.nl:publications%2F1846a8d8-34b6-4f97-a2ba-27499602a66a. [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.A. A new framework for developing and evaluating complex interventions: Update of medical research council guidance. BMJ, 2021; 374, n2061. [Google Scholar] [CrossRef]
- Grimmett, C.; Bradbury, K.; Dalton, S.O. The role of behavioral science in personalized multimodal prehabilitation in cancer. Frontiers in psychology 2021, 12, 634223. Available online: https://www.narcis.nl/publication/RecordID/oai:tilburguniversity.edu:publications%2F98562b1f-7b34-4e73-8abf-64d8d5ed2419. [CrossRef] [PubMed]
- McCourt, O.; Fisher, A.; Ramdharry, G. PERCEPT myeloma: A protocol for a pilot randomised controlled trial of exercise prehabilitation before and during autologous stem cell transplantation in patients with multiple myeloma. BMJ Open. 2020, 10, e033176. [Google Scholar] [CrossRef]
- Turner, R.R.; Steed, L.; Quirk, H. Interventions for promoting habitual exercise in people living with and beyond cancer. Cochrane database of systematic reviews. 2018, 2018, CD010192. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010192.pub3. [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science : IS. 2011, 6, 42. Available online: https://www.narcis.nl/publication/RecordID/oai:cris.maastrichtuniversity.nl:publications%2F1f2b8c2a-86b8-42b3-b106-2f2a5387283d. [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. ann behav med. 2013, 46, 81–95. Available online: https://link.springer.com/article/10.1007/s12160-013-9486-6. [CrossRef]
- Foster, C.; Breckons, M.; Cotterell, P. Cancer survivors’ self-efficacy to self-manage in the year following primary treatment. J Cancer Surviv. 2015, 9, 11–19. Available online: https://link.springer.com/article/10.1007/s11764-014-0384-0. [CrossRef] [PubMed]
- Wechsler, S.; Fu, M.R.; Lyons, K.; Wood, K.C.; Wood Magee, L.J. The role of exercise self-efficacy in exercise participation among women with persistent fatigue after breast cancer: A mixed-methods study. Physical therapy. 2023, 103, 1. Available online: https://wwwncbinlmnihgov/pubmed/36222153. [CrossRef] [PubMed]
- Johansson, E.; Larsen, J.; Schempp, T.; Jonsson, L.; Winterling, J. Patients' goals related to health and function in the first 13 months after allogeneic stem cell transplantation. Support Care Cancer. 2012, 20, 2025–2032. Available online: https://link.springer.com/article/10.1007/s00520-011-1310-x. [CrossRef] [PubMed]
- Miller, W.; Rollnick, S. Motivational interviewing: Preparing people for change. New York: Guildford; 2002.
- Olsen, C.F.; Debesay, J.; Bergland, A.; Bye, A.; Langaas, A.G. What matters when asking, “what matters to you?” — perceptions and experiences of health care providers on involving older people in transitional care. BMC Health Services Research. 2020, 20, 317. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32299424. [CrossRef]
- Silver, J.; Baima, J. Cancer prehabilitation: An opportunity to decrease treatment-related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. American journal of physical medicine & rehabilitation. 2013, 92, 715–727. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23756434. [CrossRef]
- Ormel, H.L.; van der Schoot, G.G.F.; Sluiter, W.J.; Jalving, M.; Gietema, J.A.; Walenkamp, A.M.E. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psycho-oncology (Chichester, England). 2018, 27, 713–724. Available online: https://www.narcis.nl/publication/RecordID/oai:pure.rug.nl:publications%2F1846a8d8-34b6-4f97-a2ba-27499602a66a. [CrossRef]
- Wong, J.N.; McAuley, E.; Trinh, L. Physical activity programming and counseling preferences among cancer survivors: A systematic review. The international journal of behavioral nutrition and physical activity. 2018, 15, 48. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29879993. [CrossRef]
- Parke, S.C.; Ng, A.; Martone, P. Translating 2019 ACSM cancer exercise recommendations for a physiatric practice: Derived recommendations from an international expert panel. PM & R 2548. Available online: https://search.proquest.com/docview/2548409171. [CrossRef]
- Cuthbert, C.A.; Farragher, J.F.; Hemmelgarn, B.R.; Ding, Q.; Mckinnon, G.P.; Cheung, W.Y. Self-management interventions for cancer survivors: A systematic review and evaluation of intervention content and theories. Psycho-Oncology 2019, 28, 2119. [Google Scholar] [CrossRef] [PubMed]
- Copeland, R.J. The move more plan - A framework for increasing physical activity in sheffield 2015-2020. 2020.
- Speake, H.; Copeland, R.J.; Till, S.H.; Breckon, J.D.; Haake, S.; Hart, O. Embedding physical activity in the heart of the NHS: The need for a whole-system approach. Sports Med. 2016, 46, 939–946. Available online: https://link.springer.com/article/10.1007/s40279-016-0488-y. [CrossRef] [PubMed]
- Copeland, R.J.; Lowe, A. How our pioneering new healthcare model is helping people stay active. Available online: https://www.shu.ac.uk/research/in-action/projects/move-moreUpdated 2021. Accessed 01/07/, 2023.
- Speake, H.; Copeland, R.J.; Till, S.H.; Breckon, J.D.; Haake, S.; Hart, O. Embedding physical activity in the heart of the NHS: The need for a whole-system approach. Sports Medicine. 2016, 46, 939–946. Available online: http://link.springer.com/10.1007/s40279-016-0488-y. [CrossRef] [PubMed]
Figure 1.
Active Together staffing structureService delivery setting.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



