
Submitted:
21 December 2023
Posted:
25 December 2023
You are already at the latest version
Abstract
Extramedullary hematopoiesis is a compensatory response in chronic hemolytic anemia, such as thalassemia, and can lead to spinal cord compression. This case report describes a 36-year-old woman with β-thalassemia who presented with lower extremity motor deficiency, pelvic paresthesia, and bladder dysfunction. The patient had a history of low back pain, bilateral lower limb weakness, and poor compliance with iron chelation therapy. MRI revealed compression of the spinal cord due to extramedullary hematopoiesis. Surgical intervention was not feasible, and the patient underwent hypertransfusion and iron chelation therapy. Neurological symptoms improved, but urinary retention persisted. The patient continues to receive iron chelation treatment and undergoes transfusions. Extramedullary hematopoiesis is a common complication in thalassemia and requires an individualized treatment approach.
Keywords:
extramedullary hematopoiesis
; chronic hemolytic anemia
; thalassemia
; blood transfusions
; radiation therapy
; surgical decompression
; hydroxyurea therapy
Introduction
Extramedullary hematopoiesis (EMH) is a compensatory response seen in chronic hemolytic anemia, specifically thalassemia, and can result in spinal cord compression. EMH compression of the spinal cord is a rare complication in thalassemia and commonly presents with paraparesis and sensory disability. This case report describes the presentation and management of a patient with β-thalassemia who developed neurological symptoms due to extramedullary hematopoiesis.
Case Presentation
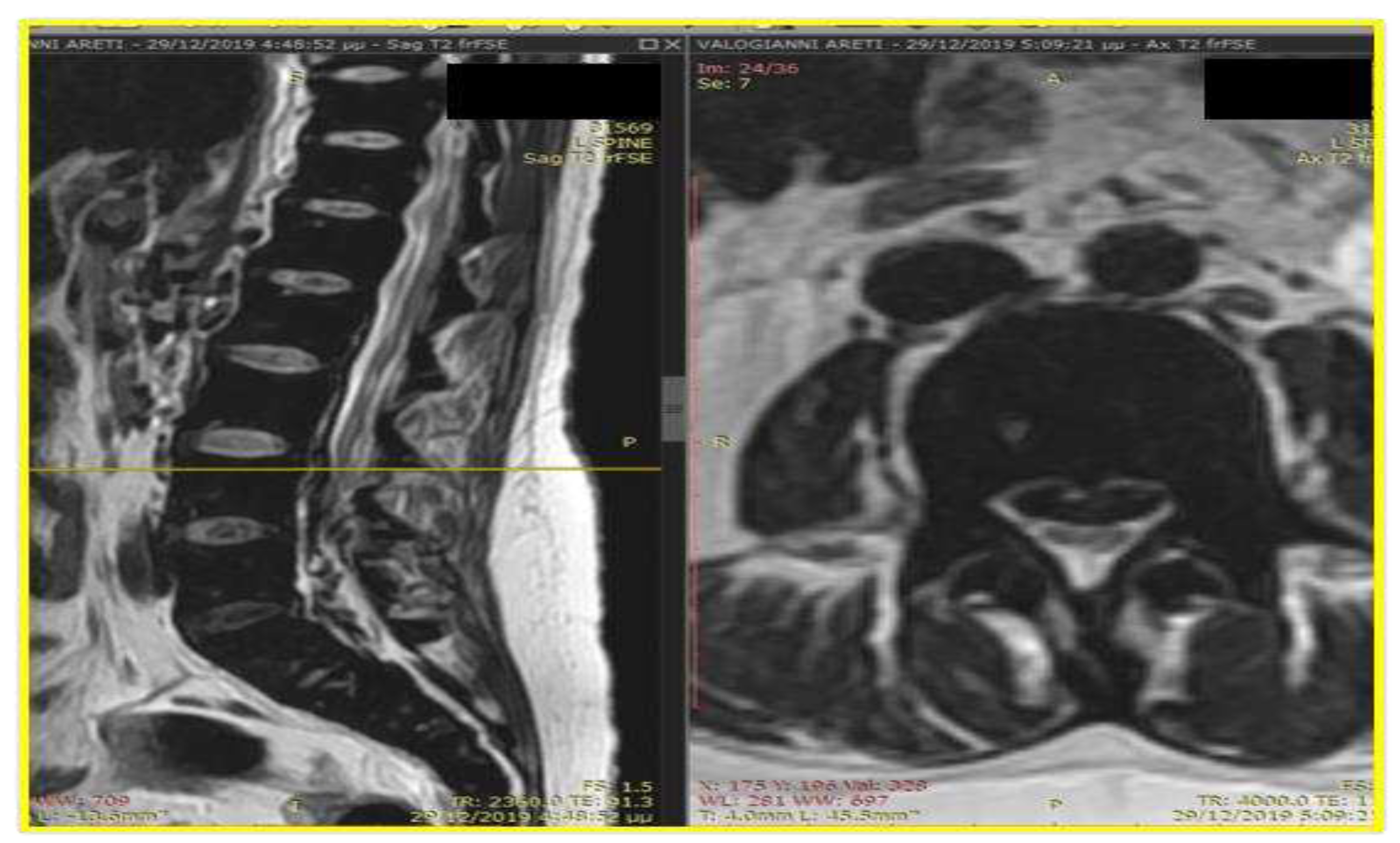
A 36-year-old Greek woman with β-thalassemia (IVSI-n1/-44bp del) had an abrupt history of lower extremity motor deficiency, pelvic paresthesia, and bladder dysfunction. She has been complaining of low back pain over the past six months, which has been steady over the last month. She has also reported bilateral lower-limb weakness. The patient was on a > 9.5 g/dl hemoglobin initiation systematic transfusion schedule every 15 days as per guidelines and iron chelation with desferrioxamine/deferiprone with poor compliance to the therapy. The mean Hb was 10 g/dL, and the mean ferritin level was 8500 μg/L, with a maximum value of 12200 μg/L. Her myocardial T2* value was estimated to be 5 milliseconds, and liver T2* value was estimated to be 1 millisecond, which correlates with a high iron concentration in the liver (20 mg/g dry tissue). On admission, vitals were temperature 37°C, blood pressure 110/70 mm Hg, respiratory rate 16/min, heart rate 90 per min, and saturation 99% on room air. A physical examination revealed hepatosplenomegaly and a heart murmur. On admission, a neurological exam showed that both legs had trouble flexing and extending the plantar fascia, and both Achilles tendon reflexes were not working properly. The patient also had full urinary retention and sensory cauda equina syndrome at the S3 level. The patient underwent an emergency MRI: The findings can be summarized as follows: In the T2 sequence, there is a low signal in the anterior epidural space, along with an inhomogeneous signal in the T1 sequence. These findings suggest compressive effects on the dura at the level of O2, extending to the posterior parts of the spinal canal until the final segment. Additionally, a segment of this compression seems to extend along the course of the midline fissures on the right side, specifically at the levels of O5-I1 and I1-I2, causing mild compressive effects on the nerve roots. In the GRE sequence, there is a low signal in a segment of the above-mentioned distribution, raising strong suspicion of hemosiderin deposition. (Figure 1 and Figure 2). In the fat-suppressed T2 sequence, there is a diffuse increase in signal, indicating edema, in the soft tissues at the level of the midline fissures in the posterior elements and the soft tissues between the ligamentum flavum and the dura at the level of the intervertebral foramina. Additionally, there is edema in the epidural space. As the duration of the symptoms was over 24 hours, the surgical approach was rejected because it couldn't be classified as an emergency. Local radiation was suggested to the patient, but she refused because she was planning a pregnancy shortly. The patient underwent hypertransfusion protocols during hospitalization to maintain hemoglobin levels at 12 mg/dl, 24-hour intravenous iron chelation with desferrioxamine at a dosage of 100 mg/kg, although the deferiprone dosage remained stable at 70 mg/kg, and hydroxyurea was initiated at 20 mg/kg following approval. The patient reported that the neurological manifestations of mobility and sensitivity improved steadily, and he was discharged from the hospital but without restoring urination, leading to self-catheterization. She continued the same subcutaneous iron chelation treatment with desferrioxamine at a dosage of 80 mg/kg. Severe aplasia occurred two months after hydroxyurea induction, and both deferiprone and hydroxyurea were discontinued until complete hematological recovery. The patient reappeared with aplasia during an effort to retake hydroxyurea, and it was decided to stop permanently. The MRI findings six months after the first appearance of symptoms showed a decrease in mass and iron deposition (Figure 3 and Figure 4). Intensive iron chelation continued in the patient with a combination of deferiprone and defesferoxamine resulting in a decreased iron load. The patient continued the transfusions every 15 days, intending to achieve hemoglobin levels above 10 g/dl. Patient's neurological recovery in the sensory and motor parts has been completed, although there has been a small improvement in neurogenic bladder dysfunction.
Discussion
Extramedullary hematopoiesis has been documented as a frequent compensatory reaction to chronic hemolytic anemia in many hematologic disorders, such as thalassemia, myelofibrosis, or after irradiation of the bone marrow. Extramedullary hematopoiesis is more common in men (5:1 male/female ratio). The incidence among Thalassemia intermedia patients with extramedullary hematopoiesis may reach up to 20% compared to polytransfused Thalassemia Major patients to roughly 1% incidence. In 11–15% of patients with extramedullary hematopoiesis, a paraspinal location for hematopoietic tissue occurs [1,2].
The most frequent sites are the thoracic region and, to a lesser extent, the lumbar region. The mechanism for this predisposition is unspecified, but though in the thoracic area, the subarachnoid space and the spinal canal are narrow, small intraspinal hematopoietic tissue can cause spinal compression at this level, unlike other regions of the cord in which such tissues must reach larger sizes to cause symptoms by exerting excessive pressure on the spinal cord. Foci of extramedullary hematopoiesis may occur in almost any organ [2,3]. The involvement of the organ often includes splenomegaly, hepatomegaly, lymphadenopathy, pleural, pericardial, or abdominal effusions, or gastrointestinal or genitourinary tract or lung involvement, leading to symptoms such as dysuria and respiratory distress. Central nervous system involvement may be associated with increased intracranial pressure, sensory impairment, and motor and sensory impairment, including cord compression. Almost all organs in fetal life are involved in hematopoiesis [4]. This path usually stops after birth. Preservation of extramedullary hematopoietic connective tissue and the ability to form red blood cells in ineffective erythrocytosis in long-term chronic anemia Extramedullary foci have been proposed to be some remnants of embryonic hematopoietic cells stimulated during chronic anemia and hypoxia. Extramedullary hematopoiesis, histologically, has in the erythroid and myeloid series immature and mature cells and dilated sinusoids that produce red cell precursors that are inactive and vulnerable to several fatty tissues and fibrosis in a stable state or extensive iron deposits [5]. In our case, although from an early age she was on a transfusion program, the patient developed extramedullary hematopoiesis, which had a significant accumulation of iron overload into the foci as described in the magnetic resonance. While history and physical evaluations can help, the most important diagnostic assessment remains radiographic imaging, which extends differential diagnosis and confirms the presence of hematopoietic tissue. The lesion may appear on magnetic resonance imaging with massive iron deposition in patients treated with blood transfusions. Recent active hematopoietic lesions have rich neovascularization, while adipose tissue and iron deposition have older lesions that are inactive [6,7,8,9]. Multiple blood transfusions to suppress the production of erythropoietin, radiation therapy to stop the development of overgrown marrow tissue, surgical decompression, or a combination of all of the above have been included in the intervention options. Due to the infrequency of this condition, the relative advantage of one treatment over another has not been established. Adequate blood transfusion in thalassemic patients reduces inefficient hematopoiesis by helping to reduce the massive development of extramedullary hematopoiesis [10,11]. Hypertransfusion therapy complications are not uncommon, and these should be taken into account and prevented where possible. The target hemoglobin level is usually >10 g/dl. Moreover, hypertransfusion therapy can be both diagnostic and therapeutic at the same time, as only edema and cord compression secondary to extramedullary hematopoiesis respond to this treatment technique. In the literature, a good response and follow-up assessment of transfusions for the treatment of spinal cord compression resulting from extramedullary hematopoiesis have been published. The main response primarily results from a decrease in the blood flow to all these tissues, even before a reduction in mass volume can even be observed. Surgical decompression is a recommended technique for handling extramedullary masses, as immediate mass decompression can be achieved. Surgery, however, has many disadvantages, including the risk of bleeding due to mass vascularization. Another limitation is the choice of incomplete resection and the high recurrence rate after surgical removal. Also, immediate, complete resection of hematopoietic masses, as these masses play a key role in maintaining an adequate hemoglobin level, can lead to clinical compensation and deterioration. Extramedullary hematopoietic tissue is very sensitive to radiation in studies, and some trials have shown a good response to radiation, with a marked decrease in mass size and rapid neurological improvement. Dosages reported in the literature range from 900 to 3,500 cGy. Moreover, following radiation therapy, recovery is usually complete. The main disadvantages of radiotherapy are the lack of documented histologic diagnosis and the drop of bone marrow activity related to radiation exposure. HU is a ribonucleotide reductase inhibitor that was first approved as a HbF modulator for clinical use in patients with sickle cell anemia, and its effects have also been extensively studied in patients with beta-thalassemia. It has major clinical and laboratory hematological effects in thalassemia intermedia patients with few side effects [13]. In combination with transfusion or radiotherapy, HU is also commonly used for the treatment of EMH. Our patient was started on a blood hypertransfusion. She received 10 units of packed RBC (2 units/week), she started to feel improvement after four units, and her neurologic symptoms disappeared after the 10th unit. Repeated neurologic examination was normal except for the persistence of slight brisk reflexes of the right knee and Achilles tendon. The hemoglobin level at that time was 15 g/dL. Hydroxyurea therapy has been introduced to increase the effectiveness of transfusion suppression of erythropoiesis in patients without further expansion of extramedullary hematopoiesis. Transfusion combined with HU is an effective therapeutic modality in these patients, especially when blood hypertransfusions may cause adverse effects such as alloimmunization of red cell antigens and iron overload. Treatment started at 5 mg/kg per day and gradually increased to 10 mg/kg per day, but the patient developed bone marrow aplasia with leukopenia and thrombocytopenia, leading to the discontinuation of treatment. Laminectomy is currently recommended in patients with an acute presentation who does not respond to adequate radiotherapy or transfusion [14].
Conclusion
Extramedullary hematopoiesis, although rare, is a significant complication of chronic hemolytic anemias. Prompt diagnosis and appropriate intervention are essential for managing this condition effectively. Treatment options such as blood transfusions, radiation therapy, surgical decompression, and hydroxyurea therapy can help alleviate symptoms and improve patient outcomes. Further research is needed to establish the most advantageous treatment approach for different cases of EMH.
Author Contributions
All authors equally contributed to data collection and writing of the current manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of Data and Materials
All data are available upon request.
Conflict of Interest Statement
The authors report no conflicts of interest in this work.
References
- Haidar, R.; Mhaidli, H.; Taher, A.T. Paraspinal extramedullary hematopoiesis in patients with thalassemia intermedia. European Spine Journal 2010, 19, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Taher, A.; Vichinsky, E.; Musallam, K.; Cappellini, M.D.; Viprakasit, V. Guidelines for the management of non-transfusion dependent thalassemia (NTDT). 2014. [Google Scholar]
- Bolaman, Z.; et al. Intrathoracic extramedullary hematopoiesis resembling posterior mediastinal tumor. The American journal of medicine 2002, 112(9), 739–741. [Google Scholar] [CrossRef] [PubMed]
- Zherebitskiy, V.; Morales, C.; Del Bigio, M.R. Extramedullary hematopoiesis involving the central nervous system and surrounding structures. Human pathology 2011, 42(10), 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; et al. The mechanisms of pathological extramedullary hematopoiesis in diseases. Cellular and Molecular Life Sciences 2020, 77, 2723–2738. [Google Scholar] [CrossRef] [PubMed]
- Malla, S.; et al. Marrow outside marrow: imaging of extramedullary hematopoiesis. Clinical Radiology 2020, 75(8), 565–578. [Google Scholar] [CrossRef] [PubMed]
- Kalchiem-Dekel, O.; Greenbaum, U. Extramedullary hematopoiesis in β-thalassemia. Mayo Clinic Proceedings 2015, 90(11). [Google Scholar] [CrossRef] [PubMed]
- Moulopoulos, L.A.; Koutoulidis, V. Bone marrow MRI; Springer Verlag, 2016. [Google Scholar]
- Subahi, E.A.; et al. Comprehensive Review: Extramedullary Hematopoiesis in Patients with Beta Thalassemia Major (transfusion dependent thalassemia). Blood 2021, 138, 4163. [Google Scholar] [CrossRef]
- Ata, F.; et al. Protocol for extramedullary hematopoiesis in patients with transfusion-dependent β-thalassemia (TDT): A systematic review. Health Science Reports 2021, 4(4), e429. [Google Scholar] [CrossRef] [PubMed]
- Betts, M.; et al. Systematic literature review of the burden of disease and treatment for transfusion-dependent β-thalassemia. Clinical Therapeutics 2020, 42(2), 322–337. [Google Scholar] [CrossRef] [PubMed]
- Doctor, P.N.; Merchant, R.; Pandey, A.K. Paraspinal extramedullary hematopoiesis in beta thalassemia Intermedia treated with low dose radiotherapy. 2020; 452–454. [Google Scholar]
- Cianciulli, P.; et al. Hydroxyurea therapy in paraparesis and cauda equina syndrome due to extramedullary hematopoiesis in thalassemia: improvement of clinical and hematological parameters. European journal of hematology 2000, 64(6), 426–429. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.H.; et al. Combined radiotherapeutic and surgical management of a spinal cord compression by extramedullary hematopoiesis in a patient with hemoglobin E beta-thalassemia. Acta haematologica 1994, 91(3), 154–157. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
In the T2 sequence, there is a low signal in the anterior epidural space, along with an inhomogeneous signal in the T1 sequence. These findings suggest compressive effects on the dura at the level of O2, extending to the posterior parts of the spinal canal until the final segment. Additionally, a segment of this compression seems to extend along the course of the midline fissures on the right side, specifically at the levels of O5-I1 and I1-I2, causing mild compressive effects on the nerve roots.
Figure 1.
In the T2 sequence, there is a low signal in the anterior epidural space, along with an inhomogeneous signal in the T1 sequence. These findings suggest compressive effects on the dura at the level of O2, extending to the posterior parts of the spinal canal until the final segment. Additionally, a segment of this compression seems to extend along the course of the midline fissures on the right side, specifically at the levels of O5-I1 and I1-I2, causing mild compressive effects on the nerve roots.
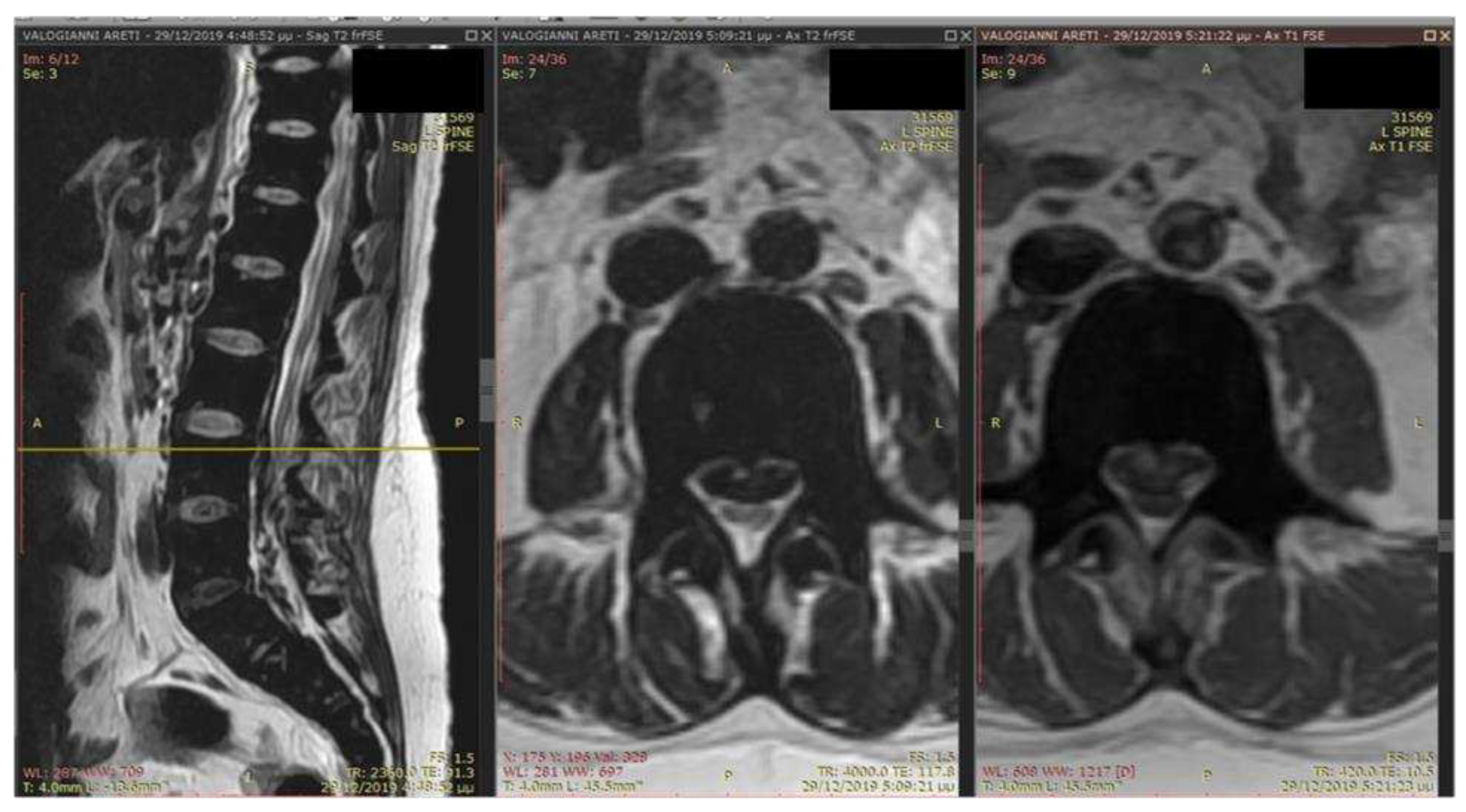
Figure 2.
In the T2 sequence, there is a low signal in the anterior epidural space, along with an inhomogeneous signal in the T1 sequence. These findings suggest compressive effects on the dura at the level of O2, extending to the posterior parts of the spinal canal until the final segment. Additionally, a segment of this compression seems to extend along the course of the midline fissures on the right side, specifically at the levels of O5-I1 and I1-I2, causing mild compressive effects on the nerve roots.
Figure 2.
In the T2 sequence, there is a low signal in the anterior epidural space, along with an inhomogeneous signal in the T1 sequence. These findings suggest compressive effects on the dura at the level of O2, extending to the posterior parts of the spinal canal until the final segment. Additionally, a segment of this compression seems to extend along the course of the midline fissures on the right side, specifically at the levels of O5-I1 and I1-I2, causing mild compressive effects on the nerve roots.

Figure 3.
The MRI findings six months after the first appearance of symptoms showed a decrease in mass and iron deposition.
Figure 3.
The MRI findings six months after the first appearance of symptoms showed a decrease in mass and iron deposition.

Figure 4.
The MRI findings six months after the first appearance of symptoms showed a decrease in mass and iron deposition.
Figure 4.
The MRI findings six months after the first appearance of symptoms showed a decrease in mass and iron deposition.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



